Embed Size (px)
Citation preview

478
HYPOADRENOCORTICISM
Defi nitionHypoadrenocorticism (Addison’s disease) arises from defi cient secretion of mineralocorticoids (aldosterone) and gluco-corticoids by the adrenal gland.
Causes and Pathophysiology
I. Naturally occurring, primary hypoadrenocorticism is usually caused by immune-mediated destruction of the adrenal cortex in cats and dogs.
II. Lymphoma of the adrenal glands is a cause of Addison’s disease in cats.
III. Secondary hypoadrenocorticism results when the pituitary gland produces inadequate amounts of adrenocorticotro-pic hormone (ACTH).A. Secondary to chronic steroid therapyB. Associated with tumors, trauma, or congenital defects
of the pituitary gland IV. Hypoadrenocorticism associated with glucocorticoid defi -
ciency only is termed atypical Addison’s disease.A. Secondary hypoadrenocorticism is always atypical.B. Primary hypoadrenocorticism is atypical in the early
stages of the disease, before destruction of the zona glomerulosa.
Clinical Signs
I. Signalment (Kintzer and Peterson, 1997)A. Young female dogs (70%) of any breedB. Reported in families of Leonbergers and standard
poodles (Smallwood and Barsanti, 1995)C. Young cats of any breed or sex
II. Historical fi ndings (Table 45-1)A. Gastrointestinal (GI) signs: intermittent vomiting,
anorexia, diarrhea, melena, weight lossB. General signs: lethargy, depression, weaknessC. Miscellaneous signs: hair loss, polyuria/polydipsia (PU/
PD), waxing and waning courseD. Hypoadrenal crisis: any of the GI, general, and mis-
cellaneous signs plus collapse, hypothermia, shaking III. Physical examination fi ndings (Box 45-1)
A. Acute addisonian crisis1. Weak pulses2. Bradycardia
3. Prolonged capillary refi ll time4. Severe mental depression5. Profound muscle weakness
B. Features increasing the index of suspicion of hypo-adrenocorticism1. Normal or slow heart rate in the presence of circu-
latory shock2. Previous response to corticosteroid or fl uid therapy3. Waxing and waning course of disease before col-
lapse
Diagnosis
I. Serum biochemical abnormalitiesA. Classic electrolyte abnormalities: hyponatremia, hyper-
kalemia, hypochloremiaB. Sodium: potassium ratios <27:1 suggestiveC. Prerenal azotemia and hyperphosphatemiaD. Hypercalcemia in 30% of cases (Peterson and Feinman,
1982)E. Metabolic acidosisF. Animals with glucocorticoid defi ciency only
1. No classic electrolyte imbalances2. Possible hypoglycemia
II. Complete blood count (CBC)A. Mild normocytic normochromic (nonregenerative)
anemia (masked by dehydration)B. The absence of a stress leukogram
1. Important feature of atypical hypoadrenocorticism2. Atypical hypoadrenocorticism likely with increased
eosinophil or lymphocyte count III. Urinalysis
A. Urine specifi c gravity is frequently low owing to medullary washout and decreased medullary blood fl ow.
B. Hormonal assays are required to differentiate between hypoadrenocorticism and renal failure.
IV. Electrocardiography (ECG) and radiographyA. ECG fi ndings: prolonged QRS complex, decreased R
wave amplitude, increased T wave amplitude (“spiked” T waves), prolonged or absent P waves, heart block, and sinoatrial standstill
B. Thoracic radiography: microcardia, narrowed vena cava, hypoperfused lungs, rarely megaesophagus
V. Dynamic adrenal testing (Table 45-2)
C H A P T E R 45
Diseases of the Adrenal Gland
| Deborah S. Greco
Ch045-X3949.indd 478 8/3/07 5:54:36 PM

CHAPTER 45 | Diseases of the Adrenal Gland 479
A. With ACTH response test serum samples are obtained before and at 30 minutes (cats) and 1 hour (cats and dogs) after IV administration of synthetic ACTH (co-syntropin 0.5 mg/kg IV, IM).
B. Baseline and post-ACTH cortisol concentrations are usually low or undetectable.
VI. Endogenous plasma ACTH
A. Collect blood in an ethylenediamine tetraacetic acid (EDTA) tube, separate, and store in plastic before the administration of any corticosteroids.
B. Primary hypoadrenocorticism has endogenous ACTH concentrations usually >100 pg/mL as a result of loss of negative feedback to the pituitary gland.
TABLE 45-1
Clinical Signs and Abnormal Laboratory Findings in Dogs and Cats with Primary Hypoadrenocorticism (Addison’s Disease)
CATS (%) DOGS (%) (n = 10) (n = 225)
Clinical Signs
Lethargy 100 95Anorexia 100 90Weight loss 100 50Dehydration 88 45Weakness 75 75Slow capillary refi ll time 63 30Weak pulses 50 20Vomiting 25 75Polyuria/polydipsia 25 25Bradycardia 13 18Diarrhea — 40Waxing/waning course — 40Previous response to therapy — 35Hypothermia — 35Shaking — 27Melena — 15Painful abdomen — 8Hair loss — 5
Laboratory Findings
Hyperkalemia 100 95Hyponatremia 100 80Hypochloremia 100 40Azotemia 100 85Hyperphosphatemia 88 85Metabolic acidosis — 40Increased ALT/AST — 30Hyperbilirubinemia — 20Hypercalcemia 13 30Hypoglycemia — 17Anemia 25 25Eosinophilia 20 13Lymphocytosis 38 10Urine specifi c gravity < 1.030 — 75
Data from Kintzer PP, Peterson ME: Treatment and long-term follow-up of 205 dogs with hypoadrenocorticism. J Vet Intern Med 11:43, 1997; Peterson ME, Greco DS, Orth DR: Hypoadrenocorticism in ten cats. J Vet Intern Med 3:55, 1989.
ALT, Alanine transaminase; AST, aspartate transaminase.
Box 45-1
Comparison of the Clinical Features of Typical and Atypical Hypoadrenocorticism
Typical Hypoadrenocorticism Atypical Hypoadrenocorticism
PathogenesisLate primary adrenal Early primary adrenal
insufficiency insufficiencySecondary adrenal insufficiency
(ACTH deficiency)
Signalment
Young (<5 years) Young (<5 years)Dogs: female; cats: either sex Dogs: femaleStandard poodles, Leonbergers Any breed
Clinical Signs
Weakness AnorexiaLethargy LethargyDepression DepressionVomiting VomitingDiarrhea Chronic diarrheaAnorexia Waxing and waning coursePrevious response to therapy Previous response to therapyCollapse Hair lossShock Hypothermia Shaking Polydipsia/polyuria Painful abdomen Melena Hair loss
Laboratory Findings
Lack of stress leukogram Lack of stress leukogramEosinophilia EosinophiliaHyponatrema LymphocytosisHyperkalemia HypoglycemiaHypochloremia Na+:K+ ratio < 27 Azotemia Hypercalcemia Metabolic acidosis Hypoglycemia
Endocrine Testing
Decreased cortisol before Decreased cortisol beforeand after ACTH and after ACTH
High endogenous ACTH Secondary: low endogenous ACTH
ACTH, Adrenocorticotropin hormone.
Ch045-X3949.indd 479 8/3/07 5:54:36 PM

480 SECTION 6 | Endocrine and Metabolic System
C. Secondary hypoadrenocorticism demonstrates the fol-owing:1. Decreased endogenous ACTH concentrations
(<20 pg/mL)2. Diminished exogenous ACTH response3. Possibly normal baseline cortisol and post-ACTH
cortisol concentrations
Differential Diagnosis
I. Infl ammatory bowel disease II. Intestinal parasitism: Trichuris vulpis III. Bilious vomiting syndrome IV. Acute renal failure V. Other causes of hypercalcemia VI. Postrenal azotemia
Treatment
I. Therapy of acute adrenal crisisA. Fluid therapy and stabilization of electrolytes with
0.9% NaCl at shock doses (see Chapter 132)B. Glucocorticoid replacement
1. Dexamethasone sodium phosphate 2 to 4 mg/kg IV (no interference with the cortisol assay)
2. Prednisolone sodium succinate 15 to 20 mg/kg IVC. Correction of life-threatening hyperkalemia
1. Regular insulin (0.06 to 0.12 U/kg IV) and glucose (4 mL of 50% dextrose/unit insulin IV)
2. 10% calcium gluconate 0.4 to 1.0 mL/kg IV over 10 to 20 minutes; maximum 10 mL
D. Prevention and treatment of GI hemorrhage1. Treat shock aggressively, because GI hemorrhage
occurs after poor intestinal perfusion.
2. Treatment includes blood transfusion and GI pro-tectants, such as sucralfate 0.5 to 1 g/25 kg PO TID to QID (dogs).
E. Correction of metabolic acidosis1. Metabolic acidosis often resolves after fl uid therapy.2. Severe acidosis (pH <7.1) is treated with sodium
bicar bonate 0.5 mEq/kg IV for 1 to 2 doses.F. Treatment of any hypoglycemia: slow IV bolus of 50%
dextrose (0.5 to 1.0 mL/kg) II. Maintenance therapy
A. Mineralocorticoid supplementation1. Oral fl udrocortisone acetate 0.02 mg/kg PO SID2. Desoxycorticosterone pivalate (DOCP) 1.5 to
2.2 mg/kg IM, SC every 25 daysB. Prednisone supplementation (0.22 mg/kg) with DOCP
1. Administer 0.2 to 0.4 mg/kg PO SID to QOD to dogs on fl udrocortisone.
2. When DOCP is used, give 50% of prednisone dose required by fl udrocortisone-treated dogs.
3. Provide additional prednisone (double dose) during periods of stress.
C. Injectable medication for affected cats1. Methylprednisolone acetate (Depo-Medrol) 10 mg
IM every 3 to 4 weeks2. DOCP 12.5 mg IM every 3 to 4 weeks
Monitoring of Animal
I. Measure serum electrolytes every 3 weeks until optimum dosage and interval of administration are determined.
II. DOCP injections are usually required every 25 to 40 days in dogs, and every 30 days in cats.
III. Serum potassium often remains slightly elevated (4.5 to 5.2 mEq/L) in clinically controlled animals.
TABLE 45-2
Protocols for Dynamic Adrenal Function Testing in Dogs and Cats
SCREENING TEST PROTOCOL NORMAL VALUES
Corticotropin (ACTH) stimulation test Cosyntropin Dog: 0.5 U/kg aqueous corticotropin IV, IM Pre: 1-4 mg/dL (28-110 nmol/L) Serum samples at 0 and 1 hr Post-ACTH: <20 mg/dL (550 nmol/L) Cat: 1/2 vial aqueous corticotropin IV, IM Serum samples at 0, 30, 60 min ACTH gel* 2.2 U/kg corticotropin gel IM (max 20 U in dog) Same as for Cosyntropin Serum samples at 0 and 2 hr in dog Serum samples at 0, 1, 2 hr in catEndogenous ACTH Single plasma sample (may be collected before 20-80 pg/mL (4.4-17.6 pmol/L) screening test and frozen for later analysis) Collect in EDTA Vacutainer (with aprotinin) Centrifuge and store in plastic Ship at 4° C (or frozen if not collected in aprotinin)
ACTH, Adrenocorticotropic hormone; max, maximum; EDTA, ethylenediamine tetraacetic acid.
*Effi cacy of compounded gels vary (Kemppainen RJ, Behrend EN, Busch KA: Use of compounded adrenocorticotropin hormone (ACTH) for adrenal function testing in dogs. J Am Anim Hosp Assoc 41:368, 2005).
Ch045-X3949.indd 480 8/3/07 5:54:37 PM
CHAPTER 45 | Diseases of the Adrenal Gland 481
HYPERADRENOCORTICISM
Defi nitionThe clinical syndrome of hyperadrenocorticism, or Cushing’s syndrome, arises with chronic and/or excessive exposure to glucocorticoids.
Causes and Pathophysiology
I. Pituitary-dependent hyperadrenocorticism (PDH) (Feldman and Nelson, 1996)A. Approximately 85% of affected dogs and 90% of
affected cats have PDH.B. Pituitary microadenomas (70%) and macroadenomas
(30%) cause excessive endogenous ACTH secretion, with secondary adrenal hyperplasia.
II. Adrenal tumors (Feldman and Nelson, 1996)A. Approximately 15% of animals with hyperadreno-
corticism have adrenal tumors.B. Of those tumors, 50% are malignant.
III. Iatrogenic hyperadrenocorticismA. Prolonged or excessive glucocorticoid administrationB. Results in chronic negative feedback to the pituitary,
decreased endogenous ACTH, and secondary adrenal atrophy
Clinical Signs
I. SignalmentA. Middle-aged to older dogs or cats (7 to 12 years)B. PDH: miniature poodle, dachshund, boxer, Boston
terrier, beagleC. Adrenal tumors: large-breed dogs, female (3:1) pre-
dilection II. Common historical and clinical signs
A. PU/PDB. Polyphagia, picaC. Heat intolerance, pantingD. Lethargy, muscle weaknessE. Obesity, abdominal enlargement or “pot belly” ap-
pearanceF. Recurrent urinary tract infectionsG. Cutaneous manifestations (see Chapter 87)
III. Uncommon clinical manifestations of hyperadreno-corticismA. HypertensionB. Pulmonary thromboembolismC. Testicular atrophy in males, clitoral hypertrophy in
femalesD. Congestive heart failureE. Prostatomegaly in castrated male dogsF. Perianal adenoma in a female or castrated male dogG. Bronchial calcifi cationH. Corneal ulceration (nonhealing)I. Cranial cruciate rupture (small dog)J. BlindnessK. Behavior changes: “steroid rage” in catsL. PseudomyotoniaM. Polyneuropathy and myopathy
Diagnosis
I. Minimum databaseA. Serum biochemistry profi le
1. Increased serum alkaline phosphatase (SAP), usually >1000 IU/L (except in cats)
2. Increased alanine transaminase3. Hypercholesterolemia4. Hyperglycemia5. Decreased blood urea nitrogen
B. CBC changes1. Nucleated red blood cells2. Erythrocytosis3. Stress leukogram4. Basophilia
C. Urinalysis fi ndings1. Bacteriuria without pyuria2. ± Glycosuria3. Hyposthenuria or minimally concentrated urine4. ± Proteinuria
II. Screening tests (Table 45-3)A. Low-dose dexamethasone suppression (LDDS) test
1. The LDDS is an extremely sensitive test (92% to 95%) (Feldman, 1983a).
2. Only 5% to 8% of dogs with PDH exhibit sup -pressed cortisol concentrations at 8 hours (i.e., 5% to 10% false negatives).
3. Some (30%) dogs with PDH exhibit suppression at 3 to 4 hours, followed by “escape” of suppression at 8 hours; this pattern is diagnostic for PDH, and makes further testing unnecessary.
4. The major disadvantage of the LDDS test is the lack of specifi city in dogs with nonadrenal illness; over 50% of dogs with nonadrenal illness have a positive LDDS test (Box 45-2) (Kaplan and Peterson, 1995).
B. Modifi ed high-dose dexamethasone suppression (HDDS) test1. Dexamethasone 0.1 mg/kg IV2. Used to screen cats for hyperadrenocorticism
C. ACTH (corticotropin) stimulation test1. ACTH stimulation test has a sensitivity of approxi-
mately 80% to 85% for the diagnosis of naturally occurring hyperadrenocorticism (Peterson et al., 1982).
2. Specifi city is higher than the LDDS test, and only 15% of dogs with nonadrenal disease showed an exaggerated response to ACTH stimulation.
3. Adrenal tumors are diffi cult to diagnose using the ACTH stimulation test.
4. Cortisol samples are collected at 30 and 60 minutes post-ACTH injection in cats.
D. Urine cortisol: creatinine ratio (UCCR)1. The UCCR is a highly sensitive (99%) screening test
with few false-negative results (Feldman and Mack, 1992; Mack et al., 1994).
2. The test is not specifi c for hyperadrenocorticism, because dogs with moderate to severe nonadrenal illness may also have elevated ratios.
Ch045-X3949.indd 481 8/3/07 5:54:37 PM

482 SECTION 6 | Endocrine and Metabolic System
3. Collect three samples at home to decrease the prob-ability of stress-associated false-positive results.
4. An increased UCCR is followed by an ACTH stimulation test or an LDDS test.
E. SAP isoenzyme1. Advantages of SAP isoenzyme determination: wide
availability, low cost2. Disadvantages
a. Elevations possibly induced by small amounts of exogenous steroids (e.g., ocular preparations)
b. Low specifi city (<44%)c. Affected by stress and nonadrenal diseasesd. Questionable quality of some assayse. No differentiation between endogenous and ia -
trogenic hyperadrenocorticismF. Dogs suffering from adrenal sex steroid excess may have
negative ACTH stimulation and LDDS tests because serum cortisol concentrations are normal.1. Excessive cortisol precursors may be present.2. Increases in progesterone, 17-OH-progesterone,
androstenedione, testosterone, and estrogens may require dynamic adrenal testing using the ACTH stimulation test and measurement of sex steroids (in addition to cortisol).
III. Differentiation tests (see Table 45-3)A. HDDS
1. ACTH secretion is suppressed maximally in dogs with functioning adrenal tumors; therefore, serum cortisol concentrations remain elevated.
2. In dogs with PDH, high doses of dexamethasone suppress ACTH and cortisol secretion.
3. Some animals with pituitary macroadenomas (15% to 50% of dogs with PDH) do not suppress on the HDDS test (Mack and Feldman, 1990).
B. Endogenous plasma ACTH concentrations1. Reliable method of discriminating between PDH
and adrenal tumors2. Tumors: low to undetectable ACTH concentrations3. PDH: normal to elevated ACTH concentrations
C. Diagnostic imaging of the pituitary and/or the adrenal glands1. Survey radiographs of 30% to 50% of dogs with
adrenal tumors show a mineralized adrenal mass (Pennick et al., 1988).
2. Abdominal ultrasonography is a more sensitive method of identifying tumors, liver metastasis, or vena caval invasion.
3. Abdominal ultrasonography helps to identify adrenomegaly in dogs with PDH.
4. Computed tomography and/or magnetic resonance imaging of the brain and/or abdominal cavity may demonstrate unilateral or bilateral adrenal enlarge-ment and pituitary adenomas (Box 45-3).
Differential Diagnosis
I. Cutaneous lesions (see Chapter 87)A. HypothyroidismB. Adrenal sex steroid excess
TABLE 45-3
Protocols for Screening and Differentiation Tests for Hyperadrenocorticism
PROTOCOL NORMAL VALUES
Screening Tests
Low-dose dexamethasone 1. 0.015 mg/kg dexamethasone solution (Azium) IV, IM Pre: 1-4 mg/dL (28-110 nmol/L) suppression test 2. 0.01 mg/kg dexamethasone sodium phosphate IV 3 hr: < 1.5 mg/dL (40 nmol/L) Samples at 0, 3-4 and 8 hr 8 hr: < 1.5 mg/dL (40 nmol/L)Corticotropin (ACTH) 1. 0.5 U/kg aqueous corticotropin IV Pre: 1-4 mg/dL (28-110 nmol/L) stimulation test Samples at 0 and 1 hr Post-ACTH: <20 mg/dL (550 nmol/L) 2. 2.2 U/kg corticotropin gel IM (max 20 U in dogs) Samples at 0 and 2 hrUrine cortisol: creatinine ratio Single urine sample, voided or collected by cystocentesis Dependent on laboratoryAlkaline phosphatase isoenzyme Single serum sample < 150 U/L SAP should be at least 2-3 times greater than normal
Differentiation Tests
High-dose dexamethasone 1. 1 mg/kg dexamethasone sodium IV Suppression to < 1.5 mg/dL suppression test 2. 0.1 mg/kg dexamethasone sodium phosphate IV (40 nmol/L) at 8 hr Samples at 0 and 8 hrEndogenous ACTH Single plasma sample (may be collected before 20-80 pg/mL (4.4-17.6 pmol/L) screening test and frozen for later analysis) Collect in EDTA Vacutainer (with aprotinin) Centrifuge and store in plastic Ship at 4° C (or frozen if not collected in aprotinin)
ACTH, Adrenocorticotropin; max, maximum; SAP, serum alkaline phosphatase; EDTA, ethylenediamine tetraacetic acid.
Ch045-X3949.indd 482 8/3/07 5:54:37 PM
CHAPTER 45 | Diseases of the Adrenal Gland 483
C. Growth hormone defi ciency II. PU/PD
A. Renal diseaseB. Liver diseaseC. PyometraD. HypoadrenocorticismE. HypercalcemiaF. Diabetes mellitusG. Diabetes insipidus: central, nephrogenic
Treatment and Monitoring
I. Mitotane (Lysodren) for PDHA. Normal induction protocol
1. Dosage is 25 to 50 mg/kg/day PO for 5 to 10 days.2. Monitor appetite and water consumption.
3. Discontinue if adverse effects occur (e.g., vomiting, anorexia, weakness).
4. Assess effectiveness using ACTH stimulation tests (Figure 45-1).
B. Production of hypoadrenocorticism1. Mitotane 50 mg/kg/day PO for 30 days causes com-
plete destruction of the adrenal cortex; then the animal is managed as an Addisonian case.
2. Physiological doses of prednisolone at 0.2 mg/kg day PO SID are subsequently given.
C. Slow induction protocol1. For cases with dermatological conditions only2. Low dose of mitotane 25 mg/kg PO weekly for
1 monthD. Monitor mitotane therapy with ACTH response tests
1. Goal is for post-ACTH cortisol concentrations to be in the normal range (1 to 5 mg/dL, or 25 to 150 nmol/L)
2. Measure at termination of the induction period (7 to 10 days).
3. Monitor electrolytes weekly for evidence of mineralo-corticoid defi ciency (hypoadrenocorticism).
4. Measure at the end of 1 month if the reduced dosage protocol is used.
E. Maintenance therapy
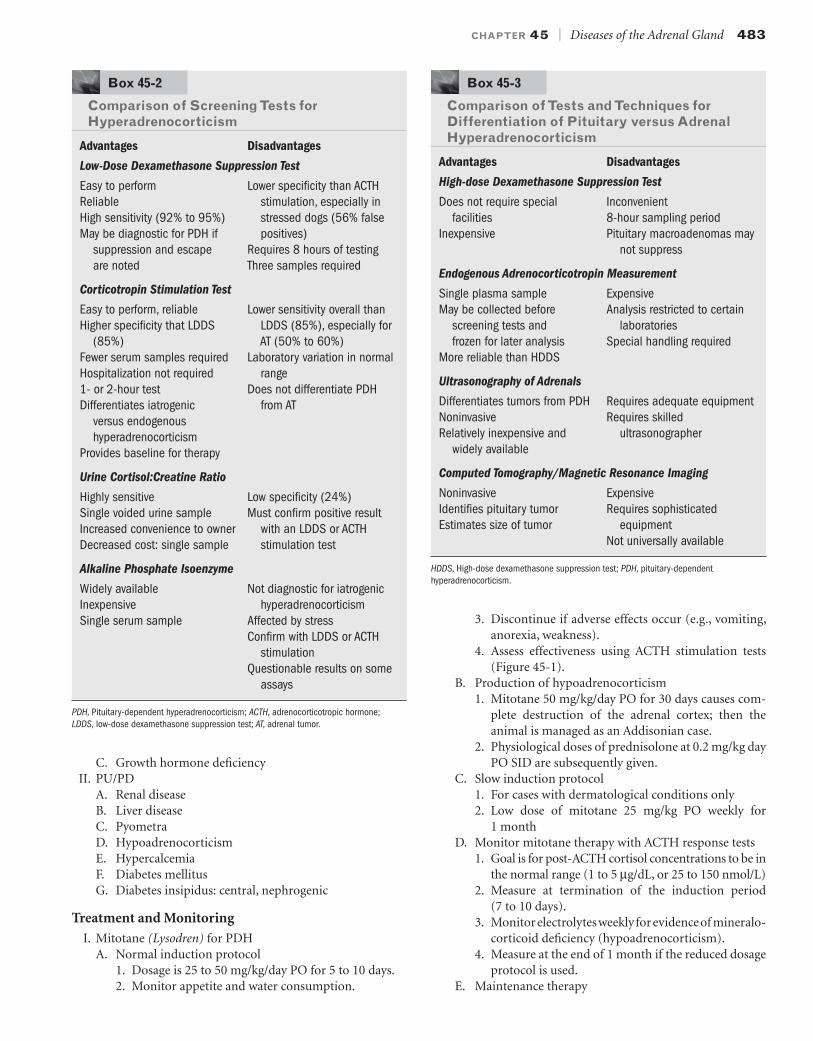
Box 45-2
Comparison of Screening Tests for Hyperadrenocorticism
Advantages Disadvantages
Low-Dose Dexamethasone Suppression Test
Easy to perform Lower specificity than ACTHReliable stimulation, especially inHigh sensitivity (92% to 95%) stressed dogs (56% falseMay be diagnostic for PDH if positives)
suppression and escape Requires 8 hours of testingare noted Three samples required
Corticotropin Stimulation Test
Easy to perform, reliable Lower sensitivity overall thanHigher specificity that LDDS LDDS (85%), especially for
(85%) AT (50% to 60%)Fewer serum samples required Laboratory variation in normalHospitalization not required range1- or 2-hour test Does not differentiate PDHDifferentiates iatrogenic from AT
versus endogenous hyperadrenocorticism
Provides baseline for therapy
Urine Cortisol:Creatine Ratio
Highly sensitive Low specificity (24%)Single voided urine sample Must confirm positive resultIncreased convenience to owner with an LDDS or ACTHDecreased cost: single sample stimulation test
Alkaline Phosphate Isoenzyme
Widely available Not diagnostic for iatrogenicInexpensive hyperadrenocorticismSingle serum sample Affected by stress Confirm with LDDS or ACTH
stimulation Questionable results on some
assays
PDH, Pituitary-dependent hyperadrenocorticism; ACTH, adrenocorticotropic hormone; LDDS, low-dose dexamethasone suppression test; AT, adrenal tumor.
Box 45-3
Comparison of Tests and Techniques for Differentiation of Pituitary versus Adrenal Hyperadrenocorticism
Advantages Disadvantages
High-dose Dexamethasone Suppression Test
Does not require special Inconvenientfacilities 8-hour sampling period
Inexpensive Pituitary macroadenomas may not suppress
Endogenous Adrenocorticotropin Measurement
Single plasma sample ExpensiveMay be collected before Analysis restricted to certain
screening tests and laboratoriesfrozen for later analysis Special handling required
More reliable than HDDS
Ultrasonography of Adrenals
Differentiates tumors from PDH Requires adequate equipmentNoninvasive Requires skilledRelatively inexpensive and ultrasonographer
widely available
Computed Tomography/Magnetic Resonance Imaging
Noninvasive ExpensiveIdentifies pituitary tumor Requires sophisticatedEstimates size of tumor equipment Not universally available
HDDS, High-dose dexamethasone suppression test; PDH, pituitary-dependent hyperadrenocorticism.
Ch045-X3949.indd 483 8/3/07 5:54:37 PM

484 SECTION 6 | Endocrine and Metabolic System
1. Mitotane 50 mg/kg/wk PO is divided into two doses, 3 to 4 days apart.
2. ACTH stimulation tests are performed every 4 months.
3. Relapses are common within 12 months of initiating maintenance therapy.
F. Prolonged effects1. Mitotane causes adrenal necrosis and effects persist
for several days.2. Withdrawal does not result in immediate improve-
ment of side effects. II. Trilostane
A. It is a competitive 3b-hydroxysteroid dehydrogenase inhibitor that affects both the production of gluco-corticoids and aldosterone.
B. Duration of effect is approximately 20 hours in the dog, which is a major advantage in comparison to mitotane.
C. It has been used primarily for PDH, but it has also been used in a few dogs with functional adrenal tumors (Eastwood et al., 2001, 2003).
D. Some dogs respond to once daily administration.1. Starting dose is 6 mg/kg PO SID.2. ACTH response tests are performed 4 to 6 hours
after administration, which is thought to be the time of peak activity.
3. Goal for post-ACTH cortisol concentrations is 1 to 5 mg/dL (Alenza et al., 2006).
E. Some dogs do better on twice-daily administration.1. Clinical signs persist in some dogs on SID therapy,
probably because cortisol values rise toward the end of the day.
2. Starting dose is 3 mg/kg PO BID.3. ACTH response tests are performed 8 to 12 hours
post-pill to evaluate the drug’s duration and effects on cortisol reserves (Alenza et al., 2006).
4. Goal for post-ACTH cortisol concentrations is 2 to 10 mg/dL (Alenza et al., 2006).
5. Yorkshire terriers may require higher doses (Alenza et al., 2006).
6. Although BID administration is more expensive, side effects may be fewer.
F. ACTH response tests are performed 7 days, and 1, 3, and 6 months (or as needed) after starting therapy and dosage adjustments (Alenza et al., 2006).
G. Because of its inhibition of aldosterone synthesis, hyperkalemia is a common side effect, and electrolytes must be monitored in addition to ACTH response tests.
H. Other adverse effects include rare cases of acute death and prolonged hypoadrenocorticism (Eastwood and Elwood, 2003).
III. KetoconazoleA. Ketoconazole is a steroid inhibitor with a transient
effect in dogs.B. Initial dosage is 7.5 mg/kg PO BID.C. Increase dose slowly (over 3 weeks) to 15 mg/kg PO
BID.D. Ketoconazole is not often used, owing to its expense
and possible severe anorexia.E. Use is primarily before surgical adrenalectomy or
radiation therapy.F. Goal is for post-ACTH cortisol concentrations of 1 to
5 mg/dL (25 to 150 nmol/L). IV. l-Deprenyl (Anipryl)
A. Monoamine oxidase B inhibitor that increases hypothalamic dopamine concentrations
B. Initial dosage: 1 mg/kg/day POC. Used for PDH only; questionable effectivenessD. Indications
1. Mild hyperadrenocorticism: skin disease only2. Intolerance to other therapies
E. Laboratory monitoring unnecessary1. ACTH response tests do not return to normal.2. Use clinical response as a guide to therapy.
V. Surgical therapyA. Surgical treatment consists of unilateral (dogs with uni-
lateral tumors) or bilateral (cats with PDH) adrenal-ectomy (Anderson et al., 2001).
Initiate therapy at25-50 mg/kg/day for 7-10 days
Monitor waterand food consumption
At the end of 7-10 daysperform ACTH stimulation test
If signs of hypoadrenocorticism occur,perform an ACTH stimulation test
Desired response Excessive response Desired response Excessive response
Go to maintenence therapy of50 mg/kg/week divided
Continue induction for 3-5more days
Repeat ACTH stimulation test
Begin maintenance therapy of50 mg/kg/week divided
Rule out pituitary tumorwith an ACTH assay
Rule out mitotane toxicity(response to w/d of drug)
FIGURE 45-1 Outline for the treatment of hyperadrenocorticism with oral mitotane. ACTH, Adrenocorticotropic hormone; w/d, withdrawal.
Ch045-X3949.indd 484 8/3/07 5:54:38 PM

CHAPTER 45 | Diseases of the Adrenal Gland 485
B. Medical management during the intra- and post-operative periods is critical.
C. Mineralocorticoid (DOCP 2.2 mg/kg IM, SC every 25 days) and glucocorticoid (prednisone 0.2 mg/kg/day PO) supplementation are initiated immediately after adrenalectomy.
D. Complications following adrenalectomy are as follows:1. Dehiscence, poor wound healing2. Addisonian crisis3. Pituitary tumor enlargement with subsequent blind-
ness or seizures (Nelson’s syndrome) VI. Radiation therapy of pituitary tumors
A. Effective method of treatment with low morbidityB. Requires several months for PDH to subsideC. Expensive and time consuming (3 weeks)D. Good long-term results
PHEOCHROMOCYTOMA
Defi nition and Cause I. Pheochromocytoma is a tumor arising from chromaffi n
cells of the adrenal medulla that hypersecretes cate-cholamines.
II. Actual cause of the tumor is unknown.
Pathophysiology
I. Cats secrete predominantly norepinephrine; dogs secrete primarily epinephrine from the adrenal medulla.
II. Clinical signs result from overproduction of catechola-mines and from direct invasion of adjacent organs and structures.
III. This tumor is uncommon in dogs and extremely rare in cats.
Clinical Signs and Diagnosis
I. Signalment (Feldman and Nelson, 1996)A. Older dogs (mean age = 11 years)B. No sex predilectionC. Boxers, miniature poodles, and German shepherd dogs
predisposed II. Historical fi ndings
A. Signs may be chronic (present for >1 year) or acute (often fatal).
B. Thirty percent are identifi ed at necropsy (Feldman and Nelson, 1996).
C. Signs include dyspnea, whining, shaking, shivering, and pacing.
D. Signs may be constant or paroxysmal. III. Physical examination fi ndings
A. Tachyarrhythmias, weakness, systolic murmurB. ± Rales from pulmonary edemaC. Possible weight loss secondary to hypermetabolismD. Ascites, edema, abdominal mass and pain from the
tumor, local metastases, or bothE. Anorexia, vomiting, weight loss, diarrheaF. Hypertension from a1-mediated increased peripheral
vascular resistance
G. Epistaxis, pale mucous membranes, blindness, and hyperemic mucous membranes from hypertension
IV. Clinical pathologyA. CBC: nonregenerative anemia, hemoconcentration,
leukocytosisB. Serum biochemistries
1. Mild hyperglycemia, carbohydrate intolerance, and occasionally overt diabetes mellitus may occur from stimulation of hepatic glycogenolysis and gluco-neogenesis, inhibition of insulin secretion, and peripheral insulin resistance.
2. Other possible laboratory abnormalities include mild uremia, increased liver enzyme activity, hypo-albuminemia, and hypocalcemia.
C. Proteinuria: variable V. Radiographic and ultrasonographic fi ndings
A. Presence of abdominal mass on plain radiography: 30% of cases (Feldman and Nelson, 1996)
B. Ultrasonography superior to radiography for identifi -cation of adrenal glands
C. Calcifi cation of adrenal massD. Abnormal renal contour, displacementE. Generalized cardiomegalyF. Possibly pulmonary edema
VI. Arterial blood pressuresA. Normal canine values
1. Systolic: 148 ± 16 mm Hg (unstressed)2. Diastolic: 87 ± 8 mm Hg3. Mean: 102 ± 9 mm Hg
B. Hypertension: systolic >180 or diastolic >95 mm Hg in a nonazotemic, relaxed dog
C. Detectable hypertension in only 50%, owing to the episodic secretion of some tumors (Feldman and Nelson, 1996)
VII. Other diagnostic testingA. Plasma catecholamines levels >2000 pg/mL are diag-
nostic.B. On a clonidine suppression test, clonidine suppresses
catecholamine levels in normal animals, but not in those with pheochromocytomas (see Chapter 2).
C. Total excretion of urinary catecholamine and cate-cholamine metabolites for 24 hours may be deter-mined.1. Normal vanillylmandelic acid: <7.0 mg/day2. Normal metanephrine/normetanephrine: <1.3 mg/day3. Normal total urinary catecholamines: <250 mg/day
Treatment
I. Surgical removal of tumorA. It is the treatment of choice but is technically
demanding.B. Metastasis is present in 33% of cases at the time of
surgery (Feldman and Nelson, 1996). II. Anesthetic management
A. Phenoxybenzamine 0.2 to 1.5 mg/kg PO BID for 1 to 2 weeks before surgery
B. Propranolol 0.15 mg/kg PO TID, for tachycardia and severe hypertension, with phenoxybenzamine
Ch045-X3949.indd 485 8/3/07 5:54:38 PM

486 SECTION 6 | Endocrine and Metabolic System
C. Drugs to avoid: phenothiazines (hypotension), atro-pine (tachycardia), barbiturates for induction (arrhyth-mias), halothane (arrhythmias)
III. Medical, palliative therapyA. Phenoxybenzamine 0.2 to 1.5 mg/kg PO BIDB. Addition of propranolol for tachyarrhythmias
Monitoring of Animal
I. If hypertension does not resolve with excision of the mass, suspect an additional tumor.
II. In general, prognosis is fair to poor owing to diffi culties commonly associated with surgery and the likelihood of metastases.
BibliographyAlenza DP, Arenas C, Lopez ML et al: Long-term effi cacy of trilostane
administered twice daily in dogs with pituitary-dependent hyper-adrenocorticism. J Am Anim Hosp Assoc 42:269, 2006
Anderson CR, Birchard SJ, Powers BE et al: Surgical treatment of adrenocortical tumors: 21 cases (1990-1996). J Am Anim Hosp Assoc 37:93, 2001
Baily MQ: Use of x-ray computed tomography as an aid in localization of adrenal masses in the dog. J Am Vet Med Assoc 188:1046, 1986
Barker EN, Campbell S, Tebb AJ et al: A comparison of survival times of dogs treated with mitotane or trilostane for pituitary-dependent hyperadrenocorticism. J Vet Intern Med 19:810, 2005
Bartges JW, Nielson DL: Reversible megaesophagus associated with atypical primary hypoadrenocorticism in a dog. J Am Vet Med Assoc 201:889, 1992
Braddock JA, Church BD, Robertson ID et al: Trilostane treatment in dogs with pituitary-dependent hyperadrenocorticism. Aust Vet J 81:600, 2003
Burns MG, Kelly AB, Hornof WJ et al: Pulmonary artery thrombosis in three dogs with hyperadrenocorticism. J Am Vet Med Assoc 178:388, 1981
Capen CC, Martin SL, Koestner A: Neoplasms in the adenohypophysis of dogs: a clinical and pathologic study. Vet Pathol 4:301, 1967
Chastain CB, Franklin RT, Granham VK et al: Evaluation of the hypothalamic-pituitary-adrenal axis in clinically stressed dogs. J Am Anim Hosp Assoc 22:435, 1986
Chastain CB, Panciera D: Trilostane treatment of dogs with pituitary-dependent hyperadrenocorticism. Small Anim Clin Endocrinol 14:18, 2004
DiBartola SP, Johnson SE, Davenport DJ et al: Clinicopathologic fi ndings resembling hypoadrenocorticism in dogs with primary gastrointestinal disease. J Am Vet Med Assoc 187:60, 1985
Dorner JL, Hoffman WE, Long GB: Corticosteroid induction of an isoenzyme of alkaline phosphatase in the dog. Am J Vet Res 35:1457, 1974
Eastwood JM, Elwood CM: Prolonged hypoadrenocorticism in fi ve dogs treated with trilostane for pituitary-dependent hyperadreno-corticism (PDH). Proc Brit Small Anim Vet Assoc April:527, 2003
Eastwood JM, Elwood CM, Hurley KJ: Trilostane treatment of four dogs with functional adrenal neoplasia (abstract). Proc Eur Soc Vet Intern Med 11:185, 2001
Eastwood JM, Elwood CM, Hurley KJ: Trilostane treatment of a dog with functional adrenal neoplasia. J Small Anim Pract 44:126, 2003
Feldman BF, Feldman EC: Routine laboratory abnormalities in endo-crine disease. Vet Clin North Am Small Anim Pract 7:433, 1977
Feldman EC: Comparison of ACTH response and dexamethasone suppression as screening tests in canine hyperadrenocorticism. J Am Vet Med Assoc 182:505, 1983a
Feldman EC: Distinguishing dogs with functioning adrenocortical tumors from dogs with pituitary-dependent hyperadrenocorticism. J Am Vet Med Assoc 183:195, 1983b
Feldman EC, Mack RE: Urine cortisol: creatinine ratio as a screening test for hyperadrenocorticism in the dog. J Am Vet Med Assoc 200:1637, 1992
Feldman EC, Nelson RW: Canine and Feline Endocrinology and Reproduction. 2nd Ed. WB Saunders, Philadelphia, 1996
Graves TK, Schall WD, Refsal K et al: Basal and ACTH-stimulated plasma aldosterone concentrations are normal or increased in dogs with trichuriasis-associated pseudohypoadrenocorticism. J Vet Intern Med 8:287, 1994
Greco DS: Endocrine emergencies. Part II. Compend Contin Educ Pract Vet 19:23,1997
Joles JA, Mulnix JA: Polyuria and polydipsia. p. 1050. In Kirk RW (ed): Current Veterinary Therapy VI: Small Animal Practice. WB Saunders, Philadelphia, 1977
Kantrowitz BM, Nyland TG, Feldman EC: Adrenal ultrasonography in the dog: detection of tumors and hyperplasia in hyperadrenocor-ticism. Vet Radiol 27:91, 1986
Kaplan AJ, Peterson ME: Effect of desoxycorticosterone pivalate administration on blood pressure in dogs with primary hypoadreno-corticism. J Am Vet Med Assoc 206:327, 1995
Katherman KA, O’Leary TP, Richardson RC: Hyperadrenocorticism and diabetes in the dog. J Am Anim Hosp Assoc 16:705, 1980
Kemppainen RJ, Behrend EN, Busch KA: Use of compounded adreno-corticotropin hormone (ACTH) for adrenal function testing in dogs. J Am Anim Hosp Assoc 41:368, 2005
Kintzer PP, Peterson ME: Treatment and long-term follow-up of 205 dogs with hypoadrenocorticism. J Vet Intern Med 11:43, 1997
Langlais-Burgess L, Lumsden JH, Mackin A: Concurrent hypoadreno-corticism and hypoalbuminemia in dogs: a retrospective study. J Am Anim Hosp Assoc 31:307, 1995
Lifton SJ, King LG, Zerbe CA: Glucocorticoid defi cient hypoadreno-corticism in dogs: 18 cases (1986-1995). J Am Vet Med Assoc 209:2076, 1996
Ling GV, Stabenfeldt GH, Comer KM et al: Canine hyperadreno-corticism: pretreatment clinical and laboratory evaluation of 117 cases. J Am Vet Med Assoc 174:1211, 1979
Mack RE, Feldman EC: Comparison of two low-dose dexamethasone suppression protocols as screening and discrimination tests in dogs with hyperadrenocorticism. J Am Vet Med Assoc 197:1603, 1990
Mack RE, Feldman EC, Wilson SM: Diagnosis of hyperadrenocorticism in dogs. Compend Contin Educ Pract Vet 16:311, 1994
Medinger TL, Williams DA, Bruyette DS: Severe gastrointestinal tract hemorrhage in three dogs with hypoadrenocorticism. J Am Vet Med Assoc 202:1869, 1993
Neiger R, Ramsey I, O’Connor J et al: Trilostane treatment of 78 dogs with pituitary-dependent hyperadrenocorticism. Vet Rec 150:799, 2002
Parnell NK, Powell LL, Hohenhaus AE et al: Hypoadrenocorticism as the primary manifestation of lymphoma in two cats. J Am Vet Med Assoc 214:1208, 1999
Pennick DG, Feldman EC, Nyland TG: Radiographic features of canine hyperadrenocorticism caused by autonomously functioning adreno-cortical tumors: 23 cases (1978-1986). J Am Vet Med Assoc 192:1604, 1988
Peterson ME, Feinman JM: Hypercalcemia associated with hypoadren-ocorticism in 16 dogs. J Am Vet Med Assoc 181:802, 1982
Peterson ME, Gilbertson SR, Drucker WD: Plasma cortisol response to exogenous ACTH in 22 dogs with hyperadrenocorticism caused by adrenocortical neoplasia. J Am Vet Med Assoc 180:542, 1982
Peterson ME, Greco DS, Orth DR: Hypoadrenocorticism in ten cats. J Vet Intern Med 3:55, 1989
Ch045-X3949.indd 486 8/3/07 5:54:38 PM

CHAPTER 45 | Diseases of the Adrenal Gland 487
Peterson ME, Kintzer P: Pretreatment clinical and laboratory fi ndings in dogs with hypoadrenocorticism: 225 cases (1979-1993). J Am Vet Med Assoc 208:85, 1996
Ramsey I, McGrotty Y: The effect of trilostane on ACTH stimulation test performed at two different times post-treatment. Proc Eur Soc Vet Intern Med 11:184, 2001
Ruckstuhl NS, Nett CS, Reusch CE: Results of clinical examinations, laboratory tests, and ultrasonography in dogs with pituitary-dependent hyperadrenocorticism treated with trilostane. Am J Vet Res 63:506, 2002
Sadek D, Schaer M: Atypical Addison’s disease in the dog: a retrospective survey of 14 cases. J Am Anim Hosp Assoc 32:159, 1996
Shaker E, Hurvitz AI, Peterson ME: Hypoadrenocorticism in a family of standard poodles. J Am Vet Med Assoc 192:1091, 1988
Smallwood LJ, Barsanti JA: Hypoadrenocorticism in a family of Leonbergers. J Am Anim Hosp Assoc 31:301, 1995
Smiley LE, Peterson ME: Evaluation of a urine cortisol: creatinine ratio as a screening test for hyperadrenocorticism in dogs. J Vet Intern Med 7:163, 1993
Webb CB, Twedt DC: Acute hepatopathy associated with mitotane administration in a dog. J Am Anim Hosp Assoc 42:298, 2006
Wenger M, Ruckstuhl NS, Reusch CE: Effect of trilostane on serum concentrations of aldosterone, cortisol, and potassium in dogs with pituitary-dependent hyperadrenocorticism. Am J Vet Res 65:1245, 2004
White SD, Ceragioli KL, Bullock LP et al: Cutaneous markers of canine hyperadrenocorticism. Compend Contin Educ Pract Vet 4:446, 1989
Willard MD, Schall WD, McCaw DE at al: Canine hypoadrenocorti-cism: report of 37 cases and review of 39 previously reported cases. J Am Vet Med Assoc 180:59, 1986
Wilson SM, Feldman EC: Diagnostic value of the steroid-induced isoenzyme of alkaline phosphatase in the dog. J Am Anim Hosp Assoc 28:245, 1992
Ch045-X3949.indd 487 8/3/07 5:54:39 PM