Embed Size (px)
Citation preview
The American Journal of Drug and Alcohol Abuse, 2013; 39(3): 217–218Copyright © Informa Healthcare USA, Inc.ISSN: 0095-2990 print/1097-9891 onlineDOI: 10.3109/00952990.2013.773335
LETTER TO THE EDITOR
Hand Sanitizer Intoxication Following a Crude Extraction Method
Michael A. Darracq, M.D., M.P.H.1,2, Nasim Ghafouri, Pharm.D.2, Amadeo Pesce, Ph.D.3, andF. Lee Cantrell, Pharm.D.2
1Department of Emergency Medicine, University of California, San Diego, San Diego, CA, USA, 2California PoisonControl System, San Diego Division, San Diego, CA, USA, 3Millenium Laboratories, San Diego, CA, USA
Ethanol-based hand sanitizers are recommended bymany public health authorities as an alternative to wash-ing for hand hygiene (1,2). Widespread availability hasgiven rise to a concerning trend. In recent years, therehave been an increasing number of intentional inges-tions of ethanol-based hand sanitizers (3), some ofwhich have occurred in controlled settings such as hos-pitals (4) and prisons (5). We report the case of a severehand sanitizer intoxication which occurred in a psychia-tric facility.
A 40-year-old patient in a locked psychiatric facilitywas found to be minimally responsive in her room alongwith two empty 1L bags of hand sanitizer. Emergencymedical services (EMS) was contacted and the patientwas intubated en route to the emergency department dueto a decreased level of consciousness and respiratorydepression. She was previously observed in her usualstate of health. Vital signs were within normal limitsupon arrival and during hospitalization. Due to the historyof exposure, a blood ethanol concentration was obtainedand was measured at 382 mg/dL. A head CT and otherlaboratory findings including renal and liver function,chemistry panel, blood count, and blood gas analysiswere unremarkable. The patient was admitted to the inten-sive care unit for supportive care and was successfullyextubated after approximately 24 hours with baseline men-tal status. Upon questioning, the patient reported mixingthe hand sanitizer gel with table salt, then running itthrough a sock to remove all salt and solids, thus leavinga consumable liquid. This was her first use of this product.She denied any other co-ingestants.
We performed a reproduction of the described extrac-tion process to determine how effectively ethanol can beisolated. This method has been previously describedonline (6–8). Two tablespoons of table salt (NaCl)
were added to two tablespoons of hand sanitizer gel(62% ethyl alcohol) and then filtered through a cottoncheesecloth to produce a clear, colorless liquid. Ethanolconcentrations of the hand sanitizer gel and post-extraction liquid were analyzed using the Nicotinamideadenine dinucleotide (protonated) (NADH)-generatingenzymatic method. The post-distillation product yieldedroughly 30%more ethanol per volume than the parent handsanitizer gel (5278 vs 4084 mg/dL).
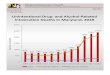
Gormley described 68,712 intentional exposures toalcohol-based hand sanitizers reported to the NationalPoison Database System between 2005 and 2009 withan average increase of 1894 new cases per year (3).Clinicians and facility administrators need to be awareof the potential for misuse of these products as intox-icants and take measures to limit their availability to at-risk populations. Additionally, manufacturers and distri-butors should consider developing tamper-resistantdispensers in an attempt to minimize large quantityingestions.
REFERENCES
1. Boyce JM, Pittet D. Guideline for hand hygiene in health-caresettings: Recommendations of the Healthcare Infection ControlPractices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. MMWR Recomm Rep 2002;51:1–45.
2. Joint Commission.Comprehensive Accreditation Manual forHospitals (CAMH). Oakbrook Terrace, IL: Joint Commissionon Accreditation of Healthcare Organizations, 2006.
3. Gormley NJ, Bronstein AC, Rasimas JJ, Pao M, Wratney AT,Sun J, Austin HA, Suffredini AF. The rising incidence ofintentional ingestion of ethanol-containing hand sanitizers.Crit Care Med 2012; 40(1):290–294.
Address correspondence to Michael A. Darracq, M.D., M.P.H., 4374 Arcadia Drive, San Diego, CA 92103, USA. Tel: þ619 299 9849.E-mail: [email protected]
217
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
9/14
For
pers
onal
use
onl
y.

4. Bookstaver PB, Norris LB, Michels JE. Ingestion of handsanitizer by a hospitalized patient with a history of alcoholabuse. Am J Health Syst Pharm 2008; 65(23):2203–2204.
5. Doyon S, Welsh C. Intoxication of a prison inmate with anethyl alcohol-based hand sanitizer. N Engl J Med 2007;356(5):529–530.
6. Grimm G. How to Use Salt to Separate Purell. Available athttp://www.ehow.co.uk/how_7504498_use-salt-separate-purell.html. Last accessed on January 7, 2012.
7. The Drink Nation. Kids Are Drinking Hand Sanitizer.Available at http://thedrinknation.com/articles/read/7386-Kids-Are-Drinking-Hand-Sanitizer. Last accessed onJanuary 7, 2012.
8. CBS New York. Dangerous Trend: Teens Drinking HandSanitizer, Equivalent to 120 Proof Liquor. Available at http://newyork.cbslocal.com/2012/04/24/dangerous-trend-teens-drinking-hand-sanitizer-to-get-drunk/. Last accessed on January 7,2012.
218 M. A. DARRACQ ET AL.
Am
J D
rug
Alc
ohol
Abu
se D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y SU
NY
Sta
te U
nive
rsity
of
New
Yor
k at
Sto
ny B
rook
on
10/2
9/14
For
pers
onal
use
onl
y.