Embed Size (px)
Citation preview

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 113
SURGICAL TECHNIQUE
Acute Surgical Management of Hand Burns
Winston T Richards MD Edward Vergara Dawood G Dalaly DOLoretta Coady-Fariborzian MD David W Mozingo MD
A hand represents 3 of the total body surface area The hands are involved in close to 80of all burns The potential morbidity associated with hand burns can be substantial Imagine a
patient carrying a pan of 1047298aming cooking oil to the doorway or someone lighting a room-sized
pile of leaves and branches doused with gasoline It is clear how the hands are at risk in these
common scenarios Not all burn injuries will require surgical intervention Recognizing the
need for surgery is paramount to achieving good functional outcomes for the burned hand
The gray area between second- and third-degree burns tests the skill and experience of every
burnhand surgeon Skin anatomy and the size of injury dictate the surgical technique used to
close the burn wound In addition to meticulous surgical technique preoperative and post-
operative hand therapy for the burned hand is essential for a good functional outcome
Recognizing the burn depth is paramount to developing the appropriate treatment plan for any
burn injury This skill requires experience and practice In this article we present an approachto second- and third-degree hand burns (J Hand Surg Am 201439(10)2075e2085
Copyright 2014 by the American Society for Surgery of the Hand All rights reserved)
Key words Burn injury hand acute surgery
H
AND EXPOSURE TO THE ENVIRONMENT makes it
vulnerable to burn injuries that have a high
potential for morbidity In addition differ-
ences in the natural history of second- and third-degree
burns are important in their surgical management
Second-degree burns heal with minimal scarring
whereas deeper wounds develop thick restrictive scars
if not treated surgically Excision and grafting of burn
wounds also has the potential to create restrictive
scars Surgical intervention on a super 1047297cial burn may
create a poor result where observation would not This
difference in the healing process highlights the need
for accurate recognition of second- and third-degree
burns a skill that requires clinical experience1
A large burn is life-threatening and the hands as-
sume lower priority during treatment Preserving
hand function in these situations requires hand ther-
apy during the resuscitation and burn wound
debridement phases and the use of skin substitutes or
allograft to cover the wounds until donor sites have
healed Edema management through limb elevation
orthosis fabrication and dressings is an important
adjunct in this process This highlights the critical
function of the occupational t herapy service in the
management of hand burns2e4
SURGICAL ANATOMY
Skin has 2 distinct layers the epidermis and the
dermis These layers measure 005 to 15 mm for the
epidermis and 03 to 30 mm for the dermis Hair
follicles are present in varying concentrations their
base is in the deep dermis and they have an epithelial
lining Sebaceous glands and sweat glands lined with
epithelium reside in the dermal layer also Glabrous
From the Department of Acute Care Surgery Department of Surgical Critical Care and the
Department of Plastic and Reconstructive Surgery University of Florida at Shands Medical
Center and the Department of Physical and Occupational Therapy Shands Medical CenterGainesville FL
Received for publication June 13 2014 accepted in revised form July 22 2014
No bene1047297ts in any form have been received or will be received related directly or
indirectly to the subject of this article
Corresponding author Winston T Richards MD Department of Acute Care Surgery
University of Florida at Shands Medical Center 1600 SW Archer Rd Gainesville FL 32608
e-mail Winstonrichardssurgeryu1047298edu
0363-5023143910-0035$36000httpdxdoiorg101016jjhsa201407032
2014 ASSH r Published by Elsevier Inc All rights reserved r 2075
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 213
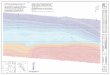
skin is naturally hairless and covers the palms and
soles (Fig 1)
Recognition of burn depth is exceptionally dif 1047297-
cult Unevenness in burn injuries skin pigmentation
discoloration from soot adherent clothing blisters
dressings and topical treatments all change the
appearance of burn wounds confounding the accu-
rate identi1047297cation of burn depth In addition burn
wounds tend to progress and demarcate over 24 to
48 hours adding uncertainty to the initial evaluation
FIGURE 1 A cartoon representing the structure of intact skin Notice the dermal capillary bed and nerve endings which 1047297gure promi-
nently in differentiating second- and third-degree burns Also note the epithelial lining of the hair follicles and sweat glands which allow
for rapid healing of super 1047297cial burns (Reprinted with permission from Duffy BJ McLaughlin PM Eichelberger MR Assessment triage
and early management of burns in children Clinical Pediatric Emergency Medicine 7(2)82e93 Copyright 2006 Elsevier Inc)
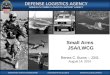
FIGURE 2 A super 1047297cial second-degree hand burn A The wound bed is moist and painful and blanches when compressed B The
blisters have been removed and the wound bed is bleeding after minor debridement
2076 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 313
Accurate diagnosis involves serial examinations over
the 1047297rst 48 hours and early wound debridement
removing loose detritus material under sedation
Burn wounds involve the epidermis dermis and
even subcutaneous structures Super 1047297cial second-de-gree burns involve the epidermis and super 1047297cial
dermis They are typically blistered and moist The
nerve endings are intact making them painful to light
touch and the dermal capillary beds are present
blanching on palpation Routinely they heal in 2 to 3
weeks when epithelial cells surrounding the dermal
appendages (hair sebaceous glands and sweat
glands) proliferate and 1047297ll in the burned area
Second-degree burns involving the deep dermis
have few epithelial structures intact They take longer
than 2 to 3 weeks to heal and have an increased risk for
hypertrophic scarring Topical antimicrobial dress-
ings applied to deep second-degree burns allow us
to determine their depth and time to heal Subse-
quently they may require skin grafting Third-
degree burns involve the skinrsquos full thickness
destroying the dermal appendages and leaving no
nests of epidermal cells to proliferate Dermal ves-
sels and super 1047297cial veins may be thrombosed and
visible and the skin is leathery dry desiccated or
carbonized Tangential excision and grafting or
excision and primary closure are the treatments of
choice for these burns (Figs 2e4)
INDICATIONS AND CONTRAINDICATIONS
Burn depth size and time to heal drive the indications
for surgical intervention Super 1047297cial second-degree
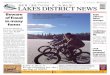
FIGURE 3 Examples of deep second-degree burns A A step-off is present between the wound bed and the unburned skin B C A thick
sloughing serum and cream cover a pale wound bed with hemorrhage in the dermis
FIGURE 4 Third- and fourth-degree burns on a hand A The skin is leathery discolored and dry Escharotomies (arrow) released the
constricting circumferential burn B The repose of the resting 1047297ngers suggests burn injury with rupture of the underlying tendons
(transverse arrow 1047297ngers extended) and coagulation of the forearm muscles (oblique arrow 1047297ngers 1047298exed) in this electrical injury
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2077
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 413
burns that heal with time and topical antimicrobials
avoid a donor site and the scarring associated with
tangential excision and grafting The indications for
surgical excision are deep dermal burns that have not
healed in 2 weeks and third- or fourth-degree burnsA relative contraindication to burn wound excision
on the hand occurs in patients with a large total body
surface area (TBSA) burn Survival depends on
excising and grafting the largest burn areas 1047297rst Once
those donor sites have healed one can then harvest a
split-thickness skin graft (STSG) to cover the hands
Temporizing approaches available in this situation
include enzymatic debridement dermal substitutes
allograft and cultured cells allowing coverage of the
hand burns while treating the larger burn wound
Several articles report no difference in the outcome of
late versus early excision of hand burns provided one
continues therapy by means of judicious functional
orthosis fabrication and mainta ining range of motion
(ROM) to wrist and 1047297ngers56
Optimum timing for excision and grafting of burnwounds on the hands is a complex problem often
complicated by extensive burns Shortly after the pa-
tient is resuscitated and the wounds are well demar-
cated one may excise third- and fourth-degree
burn injuries Observation of second-degree burns
while using topical antimicrobial creams or dressings
allows time to determine the depth of injury We then
excise and graft large wounds that granulate or remain
open after 2 weeks In addition aggressive hand
therapy routines before and after surgery improve
hand function1
FIGURE 5 A Weck knife (Tele1047298ex Medical Research Triangle Park NY) used at our institution This knife has a straight razor blade
and multiple 1047297xed guards ranging from 0004 to 0012 inch in depth A Blade and knife handle separate B Blade inserted into handle
and guard in place for right-handed use
FIGURE 6 A deep-second and third-degree burn wound before A and after B surgical debridement Note the pink moist wound bed with
punctate hemorrhage Arrows show hemorrhage Electrocautery was used on the larger bleeding capillaries prior to applying an STSG
Arrows also show sites to cauterize
2078 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 513
SURGICAL TECHNIQUE
A major advance in the treatment of burn wounds
was the introduction of tangential excision and
grafting This involves serial excision of thin layers
of burned skin exposing healthy tissue followed by
closing the wound with a skin graft
Weck knives used for excision have a 1047297xed guard
from 0004 to 0012 inch in depth Multiple passes of
the knife used in a sawing fashion at a slight angle to the
surface uncovers healthy tissue A useful excision
technique involves holding traction and countertraction
on the wound while passing the knife over the burn
FIGURE 7 A deep second-degree burn after 2 weeks under Xenograft (pigskin Brennen Medical LLC St Paul MN) The wound had
not completely healed and required excision and grafting A Before debridement B After debridement with the Versajet and hemostasis
with electrocautery We removed small nests of epithelial cells (arrow in A shows small healed area that was removed for uniform
coverage) from the center of the wound to provide a uniform wound bed for grafting (arrow in B shows uniform wound bed)
FIGURE 8 This super 1047297cial second-degree burn was debrided and then covered with Xenograft The proximal graft was secured with
staples and the distal graft on the 1047297ngers was secured with Dermabond (EthiconJohnson amp Johnson Somerville NJ) skin adhesive A
After debridement B Xenograft in place
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2079
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 613
In addition to the standard knives the Versajet
(Smith amp Nephew Wound Management Hull UK) is
a recently developed adjunct This system uses a
high-pressure jet of water to remove thin layers of
tissue with each pass Used in conjunction with sharp
debridement it smoothens out the wound surface and
is useful on complicated contours in the burn wound
(Fig 5)
A moist glistening surface identi1047297es successful
debridement A healthy dermal capillary bed reveals
punctate bleeding when unroofed As the excision
progresses in depth the space between capillaries
becomes wider When determining the adequacy of
debridement the presence of thrombosed vessels and
tissue hemorrhage suggest further excision Normal-
appearing fat has a yellow wet appearance to it and
healthy muscles once exposed will contract whenstimulated Tourniquet use during this process makes
identifying the level of debridement more dif 1047297cult but
reduces blood loss (Figs 6 7)
Tourniquet use allows more time to debride a
complex wound area on thehand and1047297ngers Elevating
the limb for 2 minutes prior to in1047298ation instead of
exsanguinating with an Esmarch bandage leaves
enough residual blood in the capillaries to evaluate the
depth of excision When using an Esmarch bandage
prior to debridement partial de1047298ation of the tourniquet
may reveal areas that need further excision Finally if the depth of excision is uncertain apply allograft to the
wound as a test If this graft becomes adherent then
there is potential for successful autograft application
otherwise repeat the debridement in several days
Grafting may be performed with xenograft (animal
skin most often pigskin) allograft (cadaver skin
obtained through a tissue bank) or autograft the
patient rsquos own skin Each of these biological coverings
has a speci1047297c place in the acute management of
hand burns In addition skin substitutes and burn
woundespeci1047297c dressings may be used
FIGURE 9 A This third-degree burn wound was excised and covered with allograft Notice the difference in pigmentation B We
covered the larger surface area on the forearm and upper arm with an STSG in a 21 mesh pattern during this operation We removed theallograft in 2 weeks when the patient rsquos donor sites had healed
FIGURE 10 A Third-degree hand burn wound B STSG sheet
graft with hash marks (arrow) A 11 mesh pattern in the STSG
and limited separation of the interstices produces the same effect
2080 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 713
Xenograft (pigskin) (Brennen Medical LLC St
Paul MN) covers super 1047297cial second-degree burns It
seals the wound from the environment allowing it to
epithelialize Allograft cadaver skin (AlloSource
Centennial CO) is useful in the management of large
burn injuries We excise the hand burn as soon as
possible and use allograft as a temporary biological
dressing Allograft adheres to the excised wound in a
fashion similar to that of autografted skin In 3 weeks
the cadaver skin separates from the wound bed
FIGURE 11 Example of the use of a dermal substitute
A At this stage the Integra (Integra Life Sciences Plainsboro NJ) has engrafted
on the wound bed as evidenced by the red color of the material B After removing the silicone layer and light debridement of the wound
we applied an STSG
TABLE 1 Dermal Substitutes and Burn-Speci1047297c Wound Dressings With a Description of Their Components
Primary Uses and Company Information
Skin
Substitute Components Primary Use Company Information
Xenograft Porcine Skin Super 1047297cial second-degree burns
temporary covering
Brennen Medical LLC 1290 Hammond
Rd St Paul MN 55110-5959
Biobrane Nylon mesh silicone and
type 1 porcine collagen
Super 1047297cial second-degree burns
temporary covering
Smith amp Nephew Wound Management
PO Box 81 101 Hessle Rd Hull
HU3 2BN UK
Allograft Full-thickness
cadaver skin
Deep second- and third-degree burns
temporary covering
AlloSource 6278 South Troy Circle
Centennial CO 80111
AlloDerm Cadaver dermis Third-degree burns combined with
thin STSG Wound closure
LifeCell Corporation 95 Corporate Dr
Bridgewater NY 08807
Integra Silicone collagen
chondroitin-6-sulfate
Third-degree burns combined with
thin STSG Wound closure
Two-stage procedure
Integra Life Sciences 311 Enterprise Dr
Plainsboro NJ 08536
Matriderm Collagen elastin Third-degree burns combined with
thin STSG Wound closure
Dr Oto Suwelack Skin and Health
Care AG Josef-Suwelack-Strasse 48727
Billerbeck Germany
Oasis Porcine small intestinal
submucosa
Second degree burns as a dressing
Wound closure
Smith amp Nephew Wound Management
3909 Hulen St Fort Worth TX 76107
Primatrix Fetal bovine dermis Second- and third-degree burns
may be combined
with STSG Wound closure
TEI Biosciences 100 Winter St Waltham
MA 02451
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2081
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 213
skin is naturally hairless and covers the palms and
soles (Fig 1)
Recognition of burn depth is exceptionally dif 1047297-
cult Unevenness in burn injuries skin pigmentation
discoloration from soot adherent clothing blisters
dressings and topical treatments all change the
appearance of burn wounds confounding the accu-
rate identi1047297cation of burn depth In addition burn
wounds tend to progress and demarcate over 24 to
48 hours adding uncertainty to the initial evaluation
FIGURE 1 A cartoon representing the structure of intact skin Notice the dermal capillary bed and nerve endings which 1047297gure promi-
nently in differentiating second- and third-degree burns Also note the epithelial lining of the hair follicles and sweat glands which allow
for rapid healing of super 1047297cial burns (Reprinted with permission from Duffy BJ McLaughlin PM Eichelberger MR Assessment triage
and early management of burns in children Clinical Pediatric Emergency Medicine 7(2)82e93 Copyright 2006 Elsevier Inc)
FIGURE 2 A super 1047297cial second-degree hand burn A The wound bed is moist and painful and blanches when compressed B The
blisters have been removed and the wound bed is bleeding after minor debridement
2076 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 313
Accurate diagnosis involves serial examinations over
the 1047297rst 48 hours and early wound debridement
removing loose detritus material under sedation
Burn wounds involve the epidermis dermis and
even subcutaneous structures Super 1047297cial second-de-gree burns involve the epidermis and super 1047297cial
dermis They are typically blistered and moist The
nerve endings are intact making them painful to light
touch and the dermal capillary beds are present
blanching on palpation Routinely they heal in 2 to 3
weeks when epithelial cells surrounding the dermal
appendages (hair sebaceous glands and sweat
glands) proliferate and 1047297ll in the burned area
Second-degree burns involving the deep dermis
have few epithelial structures intact They take longer
than 2 to 3 weeks to heal and have an increased risk for
hypertrophic scarring Topical antimicrobial dress-
ings applied to deep second-degree burns allow us
to determine their depth and time to heal Subse-
quently they may require skin grafting Third-
degree burns involve the skinrsquos full thickness
destroying the dermal appendages and leaving no
nests of epidermal cells to proliferate Dermal ves-
sels and super 1047297cial veins may be thrombosed and
visible and the skin is leathery dry desiccated or
carbonized Tangential excision and grafting or
excision and primary closure are the treatments of
choice for these burns (Figs 2e4)
INDICATIONS AND CONTRAINDICATIONS
Burn depth size and time to heal drive the indications
for surgical intervention Super 1047297cial second-degree
FIGURE 3 Examples of deep second-degree burns A A step-off is present between the wound bed and the unburned skin B C A thick
sloughing serum and cream cover a pale wound bed with hemorrhage in the dermis
FIGURE 4 Third- and fourth-degree burns on a hand A The skin is leathery discolored and dry Escharotomies (arrow) released the
constricting circumferential burn B The repose of the resting 1047297ngers suggests burn injury with rupture of the underlying tendons
(transverse arrow 1047297ngers extended) and coagulation of the forearm muscles (oblique arrow 1047297ngers 1047298exed) in this electrical injury
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2077
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 413
burns that heal with time and topical antimicrobials
avoid a donor site and the scarring associated with
tangential excision and grafting The indications for
surgical excision are deep dermal burns that have not
healed in 2 weeks and third- or fourth-degree burnsA relative contraindication to burn wound excision
on the hand occurs in patients with a large total body
surface area (TBSA) burn Survival depends on
excising and grafting the largest burn areas 1047297rst Once
those donor sites have healed one can then harvest a
split-thickness skin graft (STSG) to cover the hands
Temporizing approaches available in this situation
include enzymatic debridement dermal substitutes
allograft and cultured cells allowing coverage of the
hand burns while treating the larger burn wound
Several articles report no difference in the outcome of
late versus early excision of hand burns provided one
continues therapy by means of judicious functional
orthosis fabrication and mainta ining range of motion
(ROM) to wrist and 1047297ngers56
Optimum timing for excision and grafting of burnwounds on the hands is a complex problem often
complicated by extensive burns Shortly after the pa-
tient is resuscitated and the wounds are well demar-
cated one may excise third- and fourth-degree
burn injuries Observation of second-degree burns
while using topical antimicrobial creams or dressings
allows time to determine the depth of injury We then
excise and graft large wounds that granulate or remain
open after 2 weeks In addition aggressive hand
therapy routines before and after surgery improve
hand function1
FIGURE 5 A Weck knife (Tele1047298ex Medical Research Triangle Park NY) used at our institution This knife has a straight razor blade
and multiple 1047297xed guards ranging from 0004 to 0012 inch in depth A Blade and knife handle separate B Blade inserted into handle
and guard in place for right-handed use
FIGURE 6 A deep-second and third-degree burn wound before A and after B surgical debridement Note the pink moist wound bed with
punctate hemorrhage Arrows show hemorrhage Electrocautery was used on the larger bleeding capillaries prior to applying an STSG
Arrows also show sites to cauterize
2078 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 513
SURGICAL TECHNIQUE
A major advance in the treatment of burn wounds
was the introduction of tangential excision and
grafting This involves serial excision of thin layers
of burned skin exposing healthy tissue followed by
closing the wound with a skin graft
Weck knives used for excision have a 1047297xed guard
from 0004 to 0012 inch in depth Multiple passes of
the knife used in a sawing fashion at a slight angle to the
surface uncovers healthy tissue A useful excision
technique involves holding traction and countertraction
on the wound while passing the knife over the burn
FIGURE 7 A deep second-degree burn after 2 weeks under Xenograft (pigskin Brennen Medical LLC St Paul MN) The wound had
not completely healed and required excision and grafting A Before debridement B After debridement with the Versajet and hemostasis
with electrocautery We removed small nests of epithelial cells (arrow in A shows small healed area that was removed for uniform
coverage) from the center of the wound to provide a uniform wound bed for grafting (arrow in B shows uniform wound bed)
FIGURE 8 This super 1047297cial second-degree burn was debrided and then covered with Xenograft The proximal graft was secured with
staples and the distal graft on the 1047297ngers was secured with Dermabond (EthiconJohnson amp Johnson Somerville NJ) skin adhesive A
After debridement B Xenograft in place
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2079
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 613
In addition to the standard knives the Versajet
(Smith amp Nephew Wound Management Hull UK) is
a recently developed adjunct This system uses a
high-pressure jet of water to remove thin layers of
tissue with each pass Used in conjunction with sharp
debridement it smoothens out the wound surface and
is useful on complicated contours in the burn wound
(Fig 5)
A moist glistening surface identi1047297es successful
debridement A healthy dermal capillary bed reveals
punctate bleeding when unroofed As the excision
progresses in depth the space between capillaries
becomes wider When determining the adequacy of
debridement the presence of thrombosed vessels and
tissue hemorrhage suggest further excision Normal-
appearing fat has a yellow wet appearance to it and
healthy muscles once exposed will contract whenstimulated Tourniquet use during this process makes
identifying the level of debridement more dif 1047297cult but
reduces blood loss (Figs 6 7)
Tourniquet use allows more time to debride a
complex wound area on thehand and1047297ngers Elevating
the limb for 2 minutes prior to in1047298ation instead of
exsanguinating with an Esmarch bandage leaves
enough residual blood in the capillaries to evaluate the
depth of excision When using an Esmarch bandage
prior to debridement partial de1047298ation of the tourniquet
may reveal areas that need further excision Finally if the depth of excision is uncertain apply allograft to the
wound as a test If this graft becomes adherent then
there is potential for successful autograft application
otherwise repeat the debridement in several days
Grafting may be performed with xenograft (animal
skin most often pigskin) allograft (cadaver skin
obtained through a tissue bank) or autograft the
patient rsquos own skin Each of these biological coverings
has a speci1047297c place in the acute management of
hand burns In addition skin substitutes and burn
woundespeci1047297c dressings may be used
FIGURE 9 A This third-degree burn wound was excised and covered with allograft Notice the difference in pigmentation B We
covered the larger surface area on the forearm and upper arm with an STSG in a 21 mesh pattern during this operation We removed theallograft in 2 weeks when the patient rsquos donor sites had healed
FIGURE 10 A Third-degree hand burn wound B STSG sheet
graft with hash marks (arrow) A 11 mesh pattern in the STSG
and limited separation of the interstices produces the same effect
2080 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 713
Xenograft (pigskin) (Brennen Medical LLC St
Paul MN) covers super 1047297cial second-degree burns It
seals the wound from the environment allowing it to
epithelialize Allograft cadaver skin (AlloSource
Centennial CO) is useful in the management of large
burn injuries We excise the hand burn as soon as
possible and use allograft as a temporary biological
dressing Allograft adheres to the excised wound in a
fashion similar to that of autografted skin In 3 weeks
the cadaver skin separates from the wound bed
FIGURE 11 Example of the use of a dermal substitute
A At this stage the Integra (Integra Life Sciences Plainsboro NJ) has engrafted
on the wound bed as evidenced by the red color of the material B After removing the silicone layer and light debridement of the wound
we applied an STSG
TABLE 1 Dermal Substitutes and Burn-Speci1047297c Wound Dressings With a Description of Their Components
Primary Uses and Company Information
Skin
Substitute Components Primary Use Company Information
Xenograft Porcine Skin Super 1047297cial second-degree burns
temporary covering
Brennen Medical LLC 1290 Hammond
Rd St Paul MN 55110-5959
Biobrane Nylon mesh silicone and
type 1 porcine collagen
Super 1047297cial second-degree burns
temporary covering
Smith amp Nephew Wound Management
PO Box 81 101 Hessle Rd Hull
HU3 2BN UK
Allograft Full-thickness
cadaver skin
Deep second- and third-degree burns
temporary covering
AlloSource 6278 South Troy Circle
Centennial CO 80111
AlloDerm Cadaver dermis Third-degree burns combined with
thin STSG Wound closure
LifeCell Corporation 95 Corporate Dr
Bridgewater NY 08807
Integra Silicone collagen
chondroitin-6-sulfate
Third-degree burns combined with
thin STSG Wound closure
Two-stage procedure
Integra Life Sciences 311 Enterprise Dr
Plainsboro NJ 08536
Matriderm Collagen elastin Third-degree burns combined with
thin STSG Wound closure
Dr Oto Suwelack Skin and Health
Care AG Josef-Suwelack-Strasse 48727
Billerbeck Germany
Oasis Porcine small intestinal
submucosa
Second degree burns as a dressing
Wound closure
Smith amp Nephew Wound Management
3909 Hulen St Fort Worth TX 76107
Primatrix Fetal bovine dermis Second- and third-degree burns
may be combined
with STSG Wound closure
TEI Biosciences 100 Winter St Waltham
MA 02451
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2081
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 313
Accurate diagnosis involves serial examinations over
the 1047297rst 48 hours and early wound debridement
removing loose detritus material under sedation
Burn wounds involve the epidermis dermis and
even subcutaneous structures Super 1047297cial second-de-gree burns involve the epidermis and super 1047297cial
dermis They are typically blistered and moist The
nerve endings are intact making them painful to light
touch and the dermal capillary beds are present
blanching on palpation Routinely they heal in 2 to 3
weeks when epithelial cells surrounding the dermal
appendages (hair sebaceous glands and sweat
glands) proliferate and 1047297ll in the burned area
Second-degree burns involving the deep dermis
have few epithelial structures intact They take longer
than 2 to 3 weeks to heal and have an increased risk for
hypertrophic scarring Topical antimicrobial dress-
ings applied to deep second-degree burns allow us
to determine their depth and time to heal Subse-
quently they may require skin grafting Third-
degree burns involve the skinrsquos full thickness
destroying the dermal appendages and leaving no
nests of epidermal cells to proliferate Dermal ves-
sels and super 1047297cial veins may be thrombosed and
visible and the skin is leathery dry desiccated or
carbonized Tangential excision and grafting or
excision and primary closure are the treatments of
choice for these burns (Figs 2e4)
INDICATIONS AND CONTRAINDICATIONS
Burn depth size and time to heal drive the indications
for surgical intervention Super 1047297cial second-degree
FIGURE 3 Examples of deep second-degree burns A A step-off is present between the wound bed and the unburned skin B C A thick
sloughing serum and cream cover a pale wound bed with hemorrhage in the dermis
FIGURE 4 Third- and fourth-degree burns on a hand A The skin is leathery discolored and dry Escharotomies (arrow) released the
constricting circumferential burn B The repose of the resting 1047297ngers suggests burn injury with rupture of the underlying tendons
(transverse arrow 1047297ngers extended) and coagulation of the forearm muscles (oblique arrow 1047297ngers 1047298exed) in this electrical injury
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2077
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 413
burns that heal with time and topical antimicrobials
avoid a donor site and the scarring associated with
tangential excision and grafting The indications for
surgical excision are deep dermal burns that have not
healed in 2 weeks and third- or fourth-degree burnsA relative contraindication to burn wound excision
on the hand occurs in patients with a large total body
surface area (TBSA) burn Survival depends on
excising and grafting the largest burn areas 1047297rst Once
those donor sites have healed one can then harvest a
split-thickness skin graft (STSG) to cover the hands
Temporizing approaches available in this situation
include enzymatic debridement dermal substitutes
allograft and cultured cells allowing coverage of the
hand burns while treating the larger burn wound
Several articles report no difference in the outcome of
late versus early excision of hand burns provided one
continues therapy by means of judicious functional
orthosis fabrication and mainta ining range of motion
(ROM) to wrist and 1047297ngers56
Optimum timing for excision and grafting of burnwounds on the hands is a complex problem often
complicated by extensive burns Shortly after the pa-
tient is resuscitated and the wounds are well demar-
cated one may excise third- and fourth-degree
burn injuries Observation of second-degree burns
while using topical antimicrobial creams or dressings
allows time to determine the depth of injury We then
excise and graft large wounds that granulate or remain
open after 2 weeks In addition aggressive hand
therapy routines before and after surgery improve
hand function1
FIGURE 5 A Weck knife (Tele1047298ex Medical Research Triangle Park NY) used at our institution This knife has a straight razor blade
and multiple 1047297xed guards ranging from 0004 to 0012 inch in depth A Blade and knife handle separate B Blade inserted into handle
and guard in place for right-handed use
FIGURE 6 A deep-second and third-degree burn wound before A and after B surgical debridement Note the pink moist wound bed with
punctate hemorrhage Arrows show hemorrhage Electrocautery was used on the larger bleeding capillaries prior to applying an STSG
Arrows also show sites to cauterize
2078 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 513
SURGICAL TECHNIQUE
A major advance in the treatment of burn wounds
was the introduction of tangential excision and
grafting This involves serial excision of thin layers
of burned skin exposing healthy tissue followed by
closing the wound with a skin graft
Weck knives used for excision have a 1047297xed guard
from 0004 to 0012 inch in depth Multiple passes of
the knife used in a sawing fashion at a slight angle to the
surface uncovers healthy tissue A useful excision
technique involves holding traction and countertraction
on the wound while passing the knife over the burn
FIGURE 7 A deep second-degree burn after 2 weeks under Xenograft (pigskin Brennen Medical LLC St Paul MN) The wound had
not completely healed and required excision and grafting A Before debridement B After debridement with the Versajet and hemostasis
with electrocautery We removed small nests of epithelial cells (arrow in A shows small healed area that was removed for uniform
coverage) from the center of the wound to provide a uniform wound bed for grafting (arrow in B shows uniform wound bed)
FIGURE 8 This super 1047297cial second-degree burn was debrided and then covered with Xenograft The proximal graft was secured with
staples and the distal graft on the 1047297ngers was secured with Dermabond (EthiconJohnson amp Johnson Somerville NJ) skin adhesive A
After debridement B Xenograft in place
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2079
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 613
In addition to the standard knives the Versajet
(Smith amp Nephew Wound Management Hull UK) is
a recently developed adjunct This system uses a
high-pressure jet of water to remove thin layers of
tissue with each pass Used in conjunction with sharp
debridement it smoothens out the wound surface and
is useful on complicated contours in the burn wound
(Fig 5)
A moist glistening surface identi1047297es successful
debridement A healthy dermal capillary bed reveals
punctate bleeding when unroofed As the excision
progresses in depth the space between capillaries
becomes wider When determining the adequacy of
debridement the presence of thrombosed vessels and
tissue hemorrhage suggest further excision Normal-
appearing fat has a yellow wet appearance to it and
healthy muscles once exposed will contract whenstimulated Tourniquet use during this process makes
identifying the level of debridement more dif 1047297cult but
reduces blood loss (Figs 6 7)
Tourniquet use allows more time to debride a
complex wound area on thehand and1047297ngers Elevating
the limb for 2 minutes prior to in1047298ation instead of
exsanguinating with an Esmarch bandage leaves
enough residual blood in the capillaries to evaluate the
depth of excision When using an Esmarch bandage
prior to debridement partial de1047298ation of the tourniquet
may reveal areas that need further excision Finally if the depth of excision is uncertain apply allograft to the
wound as a test If this graft becomes adherent then
there is potential for successful autograft application
otherwise repeat the debridement in several days
Grafting may be performed with xenograft (animal
skin most often pigskin) allograft (cadaver skin
obtained through a tissue bank) or autograft the
patient rsquos own skin Each of these biological coverings
has a speci1047297c place in the acute management of
hand burns In addition skin substitutes and burn
woundespeci1047297c dressings may be used
FIGURE 9 A This third-degree burn wound was excised and covered with allograft Notice the difference in pigmentation B We
covered the larger surface area on the forearm and upper arm with an STSG in a 21 mesh pattern during this operation We removed theallograft in 2 weeks when the patient rsquos donor sites had healed
FIGURE 10 A Third-degree hand burn wound B STSG sheet
graft with hash marks (arrow) A 11 mesh pattern in the STSG
and limited separation of the interstices produces the same effect
2080 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 713
Xenograft (pigskin) (Brennen Medical LLC St
Paul MN) covers super 1047297cial second-degree burns It
seals the wound from the environment allowing it to
epithelialize Allograft cadaver skin (AlloSource
Centennial CO) is useful in the management of large
burn injuries We excise the hand burn as soon as
possible and use allograft as a temporary biological
dressing Allograft adheres to the excised wound in a
fashion similar to that of autografted skin In 3 weeks
the cadaver skin separates from the wound bed
FIGURE 11 Example of the use of a dermal substitute
A At this stage the Integra (Integra Life Sciences Plainsboro NJ) has engrafted
on the wound bed as evidenced by the red color of the material B After removing the silicone layer and light debridement of the wound
we applied an STSG
TABLE 1 Dermal Substitutes and Burn-Speci1047297c Wound Dressings With a Description of Their Components
Primary Uses and Company Information
Skin
Substitute Components Primary Use Company Information
Xenograft Porcine Skin Super 1047297cial second-degree burns
temporary covering
Brennen Medical LLC 1290 Hammond
Rd St Paul MN 55110-5959
Biobrane Nylon mesh silicone and
type 1 porcine collagen
Super 1047297cial second-degree burns
temporary covering
Smith amp Nephew Wound Management
PO Box 81 101 Hessle Rd Hull
HU3 2BN UK
Allograft Full-thickness
cadaver skin
Deep second- and third-degree burns
temporary covering
AlloSource 6278 South Troy Circle
Centennial CO 80111
AlloDerm Cadaver dermis Third-degree burns combined with
thin STSG Wound closure
LifeCell Corporation 95 Corporate Dr
Bridgewater NY 08807
Integra Silicone collagen
chondroitin-6-sulfate
Third-degree burns combined with
thin STSG Wound closure
Two-stage procedure
Integra Life Sciences 311 Enterprise Dr
Plainsboro NJ 08536
Matriderm Collagen elastin Third-degree burns combined with
thin STSG Wound closure
Dr Oto Suwelack Skin and Health
Care AG Josef-Suwelack-Strasse 48727
Billerbeck Germany
Oasis Porcine small intestinal
submucosa
Second degree burns as a dressing
Wound closure
Smith amp Nephew Wound Management
3909 Hulen St Fort Worth TX 76107
Primatrix Fetal bovine dermis Second- and third-degree burns
may be combined
with STSG Wound closure
TEI Biosciences 100 Winter St Waltham
MA 02451
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2081
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 413
burns that heal with time and topical antimicrobials
avoid a donor site and the scarring associated with
tangential excision and grafting The indications for
surgical excision are deep dermal burns that have not
healed in 2 weeks and third- or fourth-degree burnsA relative contraindication to burn wound excision
on the hand occurs in patients with a large total body
surface area (TBSA) burn Survival depends on
excising and grafting the largest burn areas 1047297rst Once
those donor sites have healed one can then harvest a
split-thickness skin graft (STSG) to cover the hands
Temporizing approaches available in this situation
include enzymatic debridement dermal substitutes
allograft and cultured cells allowing coverage of the
hand burns while treating the larger burn wound
Several articles report no difference in the outcome of
late versus early excision of hand burns provided one
continues therapy by means of judicious functional
orthosis fabrication and mainta ining range of motion
(ROM) to wrist and 1047297ngers56
Optimum timing for excision and grafting of burnwounds on the hands is a complex problem often
complicated by extensive burns Shortly after the pa-
tient is resuscitated and the wounds are well demar-
cated one may excise third- and fourth-degree
burn injuries Observation of second-degree burns
while using topical antimicrobial creams or dressings
allows time to determine the depth of injury We then
excise and graft large wounds that granulate or remain
open after 2 weeks In addition aggressive hand
therapy routines before and after surgery improve
hand function1
FIGURE 5 A Weck knife (Tele1047298ex Medical Research Triangle Park NY) used at our institution This knife has a straight razor blade
and multiple 1047297xed guards ranging from 0004 to 0012 inch in depth A Blade and knife handle separate B Blade inserted into handle
and guard in place for right-handed use
FIGURE 6 A deep-second and third-degree burn wound before A and after B surgical debridement Note the pink moist wound bed with
punctate hemorrhage Arrows show hemorrhage Electrocautery was used on the larger bleeding capillaries prior to applying an STSG
Arrows also show sites to cauterize
2078 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 513
SURGICAL TECHNIQUE
A major advance in the treatment of burn wounds
was the introduction of tangential excision and
grafting This involves serial excision of thin layers
of burned skin exposing healthy tissue followed by
closing the wound with a skin graft
Weck knives used for excision have a 1047297xed guard
from 0004 to 0012 inch in depth Multiple passes of
the knife used in a sawing fashion at a slight angle to the
surface uncovers healthy tissue A useful excision
technique involves holding traction and countertraction
on the wound while passing the knife over the burn
FIGURE 7 A deep second-degree burn after 2 weeks under Xenograft (pigskin Brennen Medical LLC St Paul MN) The wound had
not completely healed and required excision and grafting A Before debridement B After debridement with the Versajet and hemostasis
with electrocautery We removed small nests of epithelial cells (arrow in A shows small healed area that was removed for uniform
coverage) from the center of the wound to provide a uniform wound bed for grafting (arrow in B shows uniform wound bed)
FIGURE 8 This super 1047297cial second-degree burn was debrided and then covered with Xenograft The proximal graft was secured with
staples and the distal graft on the 1047297ngers was secured with Dermabond (EthiconJohnson amp Johnson Somerville NJ) skin adhesive A
After debridement B Xenograft in place
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2079
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 613
In addition to the standard knives the Versajet
(Smith amp Nephew Wound Management Hull UK) is
a recently developed adjunct This system uses a
high-pressure jet of water to remove thin layers of
tissue with each pass Used in conjunction with sharp
debridement it smoothens out the wound surface and
is useful on complicated contours in the burn wound
(Fig 5)
A moist glistening surface identi1047297es successful
debridement A healthy dermal capillary bed reveals
punctate bleeding when unroofed As the excision
progresses in depth the space between capillaries
becomes wider When determining the adequacy of
debridement the presence of thrombosed vessels and
tissue hemorrhage suggest further excision Normal-
appearing fat has a yellow wet appearance to it and
healthy muscles once exposed will contract whenstimulated Tourniquet use during this process makes
identifying the level of debridement more dif 1047297cult but
reduces blood loss (Figs 6 7)
Tourniquet use allows more time to debride a
complex wound area on thehand and1047297ngers Elevating
the limb for 2 minutes prior to in1047298ation instead of
exsanguinating with an Esmarch bandage leaves
enough residual blood in the capillaries to evaluate the
depth of excision When using an Esmarch bandage
prior to debridement partial de1047298ation of the tourniquet
may reveal areas that need further excision Finally if the depth of excision is uncertain apply allograft to the
wound as a test If this graft becomes adherent then
there is potential for successful autograft application
otherwise repeat the debridement in several days
Grafting may be performed with xenograft (animal
skin most often pigskin) allograft (cadaver skin
obtained through a tissue bank) or autograft the
patient rsquos own skin Each of these biological coverings
has a speci1047297c place in the acute management of
hand burns In addition skin substitutes and burn
woundespeci1047297c dressings may be used
FIGURE 9 A This third-degree burn wound was excised and covered with allograft Notice the difference in pigmentation B We
covered the larger surface area on the forearm and upper arm with an STSG in a 21 mesh pattern during this operation We removed theallograft in 2 weeks when the patient rsquos donor sites had healed
FIGURE 10 A Third-degree hand burn wound B STSG sheet
graft with hash marks (arrow) A 11 mesh pattern in the STSG
and limited separation of the interstices produces the same effect
2080 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 713
Xenograft (pigskin) (Brennen Medical LLC St
Paul MN) covers super 1047297cial second-degree burns It
seals the wound from the environment allowing it to
epithelialize Allograft cadaver skin (AlloSource
Centennial CO) is useful in the management of large
burn injuries We excise the hand burn as soon as
possible and use allograft as a temporary biological
dressing Allograft adheres to the excised wound in a
fashion similar to that of autografted skin In 3 weeks
the cadaver skin separates from the wound bed
FIGURE 11 Example of the use of a dermal substitute
A At this stage the Integra (Integra Life Sciences Plainsboro NJ) has engrafted
on the wound bed as evidenced by the red color of the material B After removing the silicone layer and light debridement of the wound
we applied an STSG
TABLE 1 Dermal Substitutes and Burn-Speci1047297c Wound Dressings With a Description of Their Components
Primary Uses and Company Information
Skin
Substitute Components Primary Use Company Information
Xenograft Porcine Skin Super 1047297cial second-degree burns
temporary covering
Brennen Medical LLC 1290 Hammond
Rd St Paul MN 55110-5959
Biobrane Nylon mesh silicone and
type 1 porcine collagen
Super 1047297cial second-degree burns
temporary covering
Smith amp Nephew Wound Management
PO Box 81 101 Hessle Rd Hull
HU3 2BN UK
Allograft Full-thickness
cadaver skin
Deep second- and third-degree burns
temporary covering
AlloSource 6278 South Troy Circle
Centennial CO 80111
AlloDerm Cadaver dermis Third-degree burns combined with
thin STSG Wound closure
LifeCell Corporation 95 Corporate Dr
Bridgewater NY 08807
Integra Silicone collagen
chondroitin-6-sulfate
Third-degree burns combined with
thin STSG Wound closure
Two-stage procedure
Integra Life Sciences 311 Enterprise Dr
Plainsboro NJ 08536
Matriderm Collagen elastin Third-degree burns combined with
thin STSG Wound closure
Dr Oto Suwelack Skin and Health
Care AG Josef-Suwelack-Strasse 48727
Billerbeck Germany
Oasis Porcine small intestinal
submucosa
Second degree burns as a dressing
Wound closure
Smith amp Nephew Wound Management
3909 Hulen St Fort Worth TX 76107
Primatrix Fetal bovine dermis Second- and third-degree burns
may be combined
with STSG Wound closure
TEI Biosciences 100 Winter St Waltham
MA 02451
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2081
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 513
SURGICAL TECHNIQUE
A major advance in the treatment of burn wounds
was the introduction of tangential excision and
grafting This involves serial excision of thin layers
of burned skin exposing healthy tissue followed by
closing the wound with a skin graft
Weck knives used for excision have a 1047297xed guard
from 0004 to 0012 inch in depth Multiple passes of
the knife used in a sawing fashion at a slight angle to the
surface uncovers healthy tissue A useful excision
technique involves holding traction and countertraction
on the wound while passing the knife over the burn
FIGURE 7 A deep second-degree burn after 2 weeks under Xenograft (pigskin Brennen Medical LLC St Paul MN) The wound had
not completely healed and required excision and grafting A Before debridement B After debridement with the Versajet and hemostasis
with electrocautery We removed small nests of epithelial cells (arrow in A shows small healed area that was removed for uniform
coverage) from the center of the wound to provide a uniform wound bed for grafting (arrow in B shows uniform wound bed)
FIGURE 8 This super 1047297cial second-degree burn was debrided and then covered with Xenograft The proximal graft was secured with
staples and the distal graft on the 1047297ngers was secured with Dermabond (EthiconJohnson amp Johnson Somerville NJ) skin adhesive A
After debridement B Xenograft in place
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2079
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 613
In addition to the standard knives the Versajet
(Smith amp Nephew Wound Management Hull UK) is
a recently developed adjunct This system uses a
high-pressure jet of water to remove thin layers of
tissue with each pass Used in conjunction with sharp
debridement it smoothens out the wound surface and
is useful on complicated contours in the burn wound
(Fig 5)
A moist glistening surface identi1047297es successful
debridement A healthy dermal capillary bed reveals
punctate bleeding when unroofed As the excision
progresses in depth the space between capillaries
becomes wider When determining the adequacy of
debridement the presence of thrombosed vessels and
tissue hemorrhage suggest further excision Normal-
appearing fat has a yellow wet appearance to it and
healthy muscles once exposed will contract whenstimulated Tourniquet use during this process makes
identifying the level of debridement more dif 1047297cult but
reduces blood loss (Figs 6 7)
Tourniquet use allows more time to debride a
complex wound area on thehand and1047297ngers Elevating
the limb for 2 minutes prior to in1047298ation instead of
exsanguinating with an Esmarch bandage leaves
enough residual blood in the capillaries to evaluate the
depth of excision When using an Esmarch bandage
prior to debridement partial de1047298ation of the tourniquet
may reveal areas that need further excision Finally if the depth of excision is uncertain apply allograft to the
wound as a test If this graft becomes adherent then
there is potential for successful autograft application
otherwise repeat the debridement in several days
Grafting may be performed with xenograft (animal
skin most often pigskin) allograft (cadaver skin
obtained through a tissue bank) or autograft the
patient rsquos own skin Each of these biological coverings
has a speci1047297c place in the acute management of
hand burns In addition skin substitutes and burn
woundespeci1047297c dressings may be used
FIGURE 9 A This third-degree burn wound was excised and covered with allograft Notice the difference in pigmentation B We
covered the larger surface area on the forearm and upper arm with an STSG in a 21 mesh pattern during this operation We removed theallograft in 2 weeks when the patient rsquos donor sites had healed
FIGURE 10 A Third-degree hand burn wound B STSG sheet
graft with hash marks (arrow) A 11 mesh pattern in the STSG
and limited separation of the interstices produces the same effect
2080 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 713
Xenograft (pigskin) (Brennen Medical LLC St
Paul MN) covers super 1047297cial second-degree burns It
seals the wound from the environment allowing it to
epithelialize Allograft cadaver skin (AlloSource
Centennial CO) is useful in the management of large
burn injuries We excise the hand burn as soon as
possible and use allograft as a temporary biological
dressing Allograft adheres to the excised wound in a
fashion similar to that of autografted skin In 3 weeks
the cadaver skin separates from the wound bed
FIGURE 11 Example of the use of a dermal substitute
A At this stage the Integra (Integra Life Sciences Plainsboro NJ) has engrafted
on the wound bed as evidenced by the red color of the material B After removing the silicone layer and light debridement of the wound
we applied an STSG
TABLE 1 Dermal Substitutes and Burn-Speci1047297c Wound Dressings With a Description of Their Components
Primary Uses and Company Information
Skin
Substitute Components Primary Use Company Information
Xenograft Porcine Skin Super 1047297cial second-degree burns
temporary covering
Brennen Medical LLC 1290 Hammond
Rd St Paul MN 55110-5959
Biobrane Nylon mesh silicone and
type 1 porcine collagen
Super 1047297cial second-degree burns
temporary covering
Smith amp Nephew Wound Management
PO Box 81 101 Hessle Rd Hull
HU3 2BN UK
Allograft Full-thickness
cadaver skin
Deep second- and third-degree burns
temporary covering
AlloSource 6278 South Troy Circle
Centennial CO 80111
AlloDerm Cadaver dermis Third-degree burns combined with
thin STSG Wound closure
LifeCell Corporation 95 Corporate Dr
Bridgewater NY 08807
Integra Silicone collagen
chondroitin-6-sulfate
Third-degree burns combined with
thin STSG Wound closure
Two-stage procedure
Integra Life Sciences 311 Enterprise Dr
Plainsboro NJ 08536
Matriderm Collagen elastin Third-degree burns combined with
thin STSG Wound closure
Dr Oto Suwelack Skin and Health
Care AG Josef-Suwelack-Strasse 48727
Billerbeck Germany
Oasis Porcine small intestinal
submucosa
Second degree burns as a dressing
Wound closure
Smith amp Nephew Wound Management
3909 Hulen St Fort Worth TX 76107
Primatrix Fetal bovine dermis Second- and third-degree burns
may be combined
with STSG Wound closure
TEI Biosciences 100 Winter St Waltham
MA 02451
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2081
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 613
In addition to the standard knives the Versajet
(Smith amp Nephew Wound Management Hull UK) is
a recently developed adjunct This system uses a
high-pressure jet of water to remove thin layers of
tissue with each pass Used in conjunction with sharp
debridement it smoothens out the wound surface and
is useful on complicated contours in the burn wound
(Fig 5)
A moist glistening surface identi1047297es successful
debridement A healthy dermal capillary bed reveals
punctate bleeding when unroofed As the excision
progresses in depth the space between capillaries
becomes wider When determining the adequacy of
debridement the presence of thrombosed vessels and
tissue hemorrhage suggest further excision Normal-
appearing fat has a yellow wet appearance to it and
healthy muscles once exposed will contract whenstimulated Tourniquet use during this process makes
identifying the level of debridement more dif 1047297cult but
reduces blood loss (Figs 6 7)
Tourniquet use allows more time to debride a
complex wound area on thehand and1047297ngers Elevating
the limb for 2 minutes prior to in1047298ation instead of
exsanguinating with an Esmarch bandage leaves
enough residual blood in the capillaries to evaluate the
depth of excision When using an Esmarch bandage
prior to debridement partial de1047298ation of the tourniquet
may reveal areas that need further excision Finally if the depth of excision is uncertain apply allograft to the
wound as a test If this graft becomes adherent then
there is potential for successful autograft application
otherwise repeat the debridement in several days
Grafting may be performed with xenograft (animal
skin most often pigskin) allograft (cadaver skin
obtained through a tissue bank) or autograft the
patient rsquos own skin Each of these biological coverings
has a speci1047297c place in the acute management of
hand burns In addition skin substitutes and burn
woundespeci1047297c dressings may be used
FIGURE 9 A This third-degree burn wound was excised and covered with allograft Notice the difference in pigmentation B We
covered the larger surface area on the forearm and upper arm with an STSG in a 21 mesh pattern during this operation We removed theallograft in 2 weeks when the patient rsquos donor sites had healed
FIGURE 10 A Third-degree hand burn wound B STSG sheet
graft with hash marks (arrow) A 11 mesh pattern in the STSG
and limited separation of the interstices produces the same effect
2080 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 713
Xenograft (pigskin) (Brennen Medical LLC St
Paul MN) covers super 1047297cial second-degree burns It
seals the wound from the environment allowing it to
epithelialize Allograft cadaver skin (AlloSource
Centennial CO) is useful in the management of large
burn injuries We excise the hand burn as soon as
possible and use allograft as a temporary biological
dressing Allograft adheres to the excised wound in a
fashion similar to that of autografted skin In 3 weeks
the cadaver skin separates from the wound bed
FIGURE 11 Example of the use of a dermal substitute
A At this stage the Integra (Integra Life Sciences Plainsboro NJ) has engrafted
on the wound bed as evidenced by the red color of the material B After removing the silicone layer and light debridement of the wound
we applied an STSG
TABLE 1 Dermal Substitutes and Burn-Speci1047297c Wound Dressings With a Description of Their Components
Primary Uses and Company Information
Skin
Substitute Components Primary Use Company Information
Xenograft Porcine Skin Super 1047297cial second-degree burns
temporary covering
Brennen Medical LLC 1290 Hammond
Rd St Paul MN 55110-5959
Biobrane Nylon mesh silicone and
type 1 porcine collagen
Super 1047297cial second-degree burns
temporary covering
Smith amp Nephew Wound Management
PO Box 81 101 Hessle Rd Hull
HU3 2BN UK
Allograft Full-thickness
cadaver skin
Deep second- and third-degree burns
temporary covering
AlloSource 6278 South Troy Circle
Centennial CO 80111
AlloDerm Cadaver dermis Third-degree burns combined with
thin STSG Wound closure
LifeCell Corporation 95 Corporate Dr
Bridgewater NY 08807
Integra Silicone collagen
chondroitin-6-sulfate
Third-degree burns combined with
thin STSG Wound closure
Two-stage procedure
Integra Life Sciences 311 Enterprise Dr
Plainsboro NJ 08536
Matriderm Collagen elastin Third-degree burns combined with
thin STSG Wound closure
Dr Oto Suwelack Skin and Health
Care AG Josef-Suwelack-Strasse 48727
Billerbeck Germany
Oasis Porcine small intestinal
submucosa
Second degree burns as a dressing
Wound closure
Smith amp Nephew Wound Management
3909 Hulen St Fort Worth TX 76107
Primatrix Fetal bovine dermis Second- and third-degree burns
may be combined
with STSG Wound closure
TEI Biosciences 100 Winter St Waltham
MA 02451
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2081
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 713
Xenograft (pigskin) (Brennen Medical LLC St
Paul MN) covers super 1047297cial second-degree burns It
seals the wound from the environment allowing it to
epithelialize Allograft cadaver skin (AlloSource
Centennial CO) is useful in the management of large
burn injuries We excise the hand burn as soon as
possible and use allograft as a temporary biological
dressing Allograft adheres to the excised wound in a
fashion similar to that of autografted skin In 3 weeks
the cadaver skin separates from the wound bed
FIGURE 11 Example of the use of a dermal substitute
A At this stage the Integra (Integra Life Sciences Plainsboro NJ) has engrafted
on the wound bed as evidenced by the red color of the material B After removing the silicone layer and light debridement of the wound
we applied an STSG
TABLE 1 Dermal Substitutes and Burn-Speci1047297c Wound Dressings With a Description of Their Components
Primary Uses and Company Information
Skin
Substitute Components Primary Use Company Information
Xenograft Porcine Skin Super 1047297cial second-degree burns
temporary covering
Brennen Medical LLC 1290 Hammond
Rd St Paul MN 55110-5959
Biobrane Nylon mesh silicone and
type 1 porcine collagen
Super 1047297cial second-degree burns
temporary covering
Smith amp Nephew Wound Management
PO Box 81 101 Hessle Rd Hull
HU3 2BN UK
Allograft Full-thickness
cadaver skin
Deep second- and third-degree burns
temporary covering
AlloSource 6278 South Troy Circle
Centennial CO 80111
AlloDerm Cadaver dermis Third-degree burns combined with
thin STSG Wound closure
LifeCell Corporation 95 Corporate Dr
Bridgewater NY 08807
Integra Silicone collagen
chondroitin-6-sulfate
Third-degree burns combined with
thin STSG Wound closure
Two-stage procedure
Integra Life Sciences 311 Enterprise Dr
Plainsboro NJ 08536
Matriderm Collagen elastin Third-degree burns combined with
thin STSG Wound closure
Dr Oto Suwelack Skin and Health
Care AG Josef-Suwelack-Strasse 48727
Billerbeck Germany
Oasis Porcine small intestinal
submucosa
Second degree burns as a dressing
Wound closure
Smith amp Nephew Wound Management
3909 Hulen St Fort Worth TX 76107
Primatrix Fetal bovine dermis Second- and third-degree burns
may be combined
with STSG Wound closure
TEI Biosciences 100 Winter St Waltham
MA 02451
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2081
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 813
secondary to in1047298ammation If the allograft initially
adheres to the wound bed then the wound is well
vascularized and bacterial colonization is minimal
When appropriate donor sites become available to
harvest remove the allograft and replace it with a
skin graft (Figs 8 9)
Harvest autograft from nonburned areas for the
treatment of acute burn injuries Choose donor sites
from areas covered by clothing The thighs buttocks
and 1047298anks are good donor sites for covering the
hands 1047297ngers and wrists with sheet grafts Smooth
out bony prominences in a donor site with clysis (ie
in1047297ltration of saline or dilute epinephrine solution to
level out the donor surface to facilitate dermatome
use) Using the widest dermatome guard limits the
number of graft-to-graft seams A sheet graft or 11
meshed graft offers good cosmetic results Meshed
skin grafts are useful in extensive burn injuries where
donor sites are limited When using a meshed graft on
the hand limited stretching of the interstices willlimit the ldquowaf 1047298edrdquo appearance of the healed grafts
STSG harvested at a thickness of 0012 inch pro-
vide well-healing donor sites and a 1047298exible graft with
minimal scar contracture Increasing the thickness of
the donated skin increases the 1047298exibility of the healed
graft reduces contracture at the grafted site but in-
creases the time to donor site healing Full-thickness
skin grafts (FTSG) provide the most 1047298exible grafting
material for a full-thickness burn wound on the hand
They also require primary closure or skin graft closure
of the donor site A prospective randomized controlledtrial of STSG thicknesses of 0015 inch or 0025 inch
did not show a signi1047297cant difference in function once
the wounds healed7
(Fig 10)
Dermal substitutes are available for use in deep
burns Integra is a bilayer material of silicone and
collagenchondroitin-6-sulfate This material provi-
des a moisture- preserving covering and a neodermal
layer Small capillary vessels invade the collagen
layer engrafting the material Once the layer is
adequately vascularized at around 21 days remove
the silicone layer prepare the surface and cover it
FIGURE 12 Example of the dressing process used for hand burns after grafting A Xenograft applied to a second-degree burn wound B
Nonstick layer of wound veil applied over the grafts C Fingers wrapped individually with gauze for a secure dressing with some
1047298exibility for the patient to participate in therapy activities
FIGURE 13 Picture highlights the obvious difference between
the palmar glabrous skin and the FTSG used to revise scar
contractures on this palm
2082 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 913
FIGURE 14 A Hypertrophic scarring on the dorsal hand involving the eponychial folds B Scarring in the 1047297rst webspace which limitsthumb function The hypertrophic scarring noted in these 2 cases represents a complication of hand burns that may occur despite
adequate debridement and skin grafting Scar excision and repeat grafting or grafting with dermal substitutes are effective treatments for
this problem
FIGURE 15 Web space syndactyly is another hand burn complication encountered when treating hand burns The 1047297rst case A rep-
resents a low-grade syndactyly B Markings for a planned Z-Plasty to release the second web space C This patient has an almost
complete syndactyly D Intraoperative picture of the dorsal skin 1047298ap resurfacing the web space E Completed closure of the repair with
FTSGs secured with absorbable sutures
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2083
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1013
with a thin STSG (0008 inch) This 2-part process
which creates a neodermal layer covered by epithe-
lium results in a thick pliable covering over the
wound with limited scarring Dermal substitutes are
useful in the management of large burn wounds
where donor sites are limited on the dorsum of the
hand for deep burns involving the subcutaneous tis-
sue and for scar revision surgery They are dif 1047297cult
to use because the wound bed must be absolutely
clean and well debrided with minimal bacterial
colonization Integra may be meshed in a 11 Bren-nen mesher (Brennen Medical LLC St Paul MN)
and secured in place with a wound VAC negative-
pressure system (Kinetic Concepts Inc San Anto-
nio TX) to control egress of 1047298uids from the wound
and enha nce the apposition of the graft to the wound
surface89
(Fig 11 Table 1)
The 1047297nal critical piece of surgical management of
a burn wound is the dressing This process secures
the grafts in position and protects them from minor
trauma Appropriate dressing techniques allow for
control of 1047298
uids leaking from the wound and decreaselocal edema Wrapping the 1047297ngers individually and
providing some 1047298exibility in the dressing will allow
the patient to begin early therapy Our current prac-
tice is to apply wound veil (DeRoyal Powell TN) a
nonstick dressing to the grafts and wrap them with
Kling (Johnson amp Johnson New Brunswick NJ)
gauze Our nursing staff applies 5 sulfamylon so-
lution to the gauze every 8 hours Once the grafts
have become adherent to the wound bed we then
switch the dressing to wound veil with bacitracin or
mupirocin (Bactroban) ointments (Fig 12)
PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough un-
derstanding of the effects of burn injury on anatom-
ical structures and the rehabilitation implications of
both pre- and postsurgical intervention Ongoing
communication and collaboration within the burn
team is essential to the successful management of the
burned hand (Appendix A available on the Journal rsquos
Web site at wwwjhandsurgorg)
PEARLS AND PITFALLS
Recognizing second-degree burns that will heal
without scarring is key to achieving good outcomes for
hand burns Waiting 2 to 3 weeks while the woundheals and the patient performs therapy helps in these
dif 1047297cult to assess injuries Adding donor site morbidity
and graft scarring to a wound that might have
healed well is a major pitfall Accurate and thorough
debridement of appropriate wounds is another im-
portant point to achieving good wound healing
Glabrous skin is the smooth hairless skin on the
palms of the hands and soles of the feet An STSG
harvested from the instep of the foot makes a suitable
graft for a small injury on the palm of the hand A
small graft from the thenar or hypothenar eminence
FIGURE 16 A Before debridement and postgrafting case pictures for the patient presented in the video B The graft is being trimmed
and secured
2084 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1113
can cover a small area on the palmar surface of the
1047297ngers An advantage of this technique is to supply
skin with similar characteristics to the wound and
avoid pigment differences and the possibility of hair
growth on the palm (Fig 13)
COMPLICATIONS
Graft failure web space syndactyly 1047298exion or exten-
sion contractures secondary to scarring epithelial
shelves pits and sinuses all represent complications of
burn injuries to the hands In addition mallet and
boutonniere deformities may represent a complication
of the severity of the wound or aggressive debridement
of the burn wound from either damage to tendons or
stretch attenuation There are multiple approaches for
their treatment (Figs 14 15)
CASE ILLUSTRATION
A 44-year-old woman with history of right breast
cancer and lumpectomy sustained burns to her right
arm right hand and left arm after a grease 1047297re 4 days
prior to presentation She initially received silver sul-
fadiazine (Silvadene) cream and pain medicine at an
outside hospital However she returned to that hospital
with purulent drainage fevers nausea and vomiting
After antibiotic treatment she transferred to our fa-
cility for de1047297nitive management of her burns The
following videos highlight her treatment (Fig 16
Videos 1 2 [available on the Journal rsquos Web site at
wwwjhandsurgorg])
REFERENCES
1 Tredget EE Nedelec B Scott PG Ghahary A Hypertrophic scars
keloids and contractures The cellular and molecular basis for ther-
apy Surg Clin North Am 199777(3)701e730
2 Petro JA Salisbury RE Rehabilitation of the burn patient Clin Plast
Surg 198613(1)145e149
3 Sheridan RL Hurley J Smith MA et al The acutely burned hand
management and outcome based on a ten-year experience with 1047
acute hand burns J Trauma 199538(3)406e
4114 Barillo DJ Harvey KD Hobbs CL Mozingo DW Ciof 1047297 WG
Pruitt BA Prospective outcome analysis of a protocol for the surgical
and rehabilitative management of burns to the hands Plast Reconstr
Surg 1997100(6)1442e1451
5 Omar MT Hassan AA Evaluation of hand function after early
excision and skin grafting of burns versus delayed skin grafting a
randomized clinical trial Burns 201137(4)707e713
6 Mohammadi AA Bakhshaeekia AR Marzban S et al Early excision
and skin grafting versus delayed skin grafting in deep hand burns (a
randomized clinical controlled trial) Burns 201137(1)36e41
7 Mann R Gibran NS Engrav LH et al Prospective trial of thick vs
standard split-thickness skin grafts in burns of the hand J Burn Care
Rehabil 200122(6)390e392
8 Lou RB Hickerson WL The use of skin substitutes in hand burns
Hand Clin 200925(4)497e
5099 Ryssel H Germann G Kloeters O Gazyakan E Radu CA Dermal
substitution with Matriderm() in burns on the dorsum of the hand
Burns 201036(8)1248e1253
10 Moore ML William DS Richard RL Rehabilitation of the burned
hand In Klein MB ed Hand Clinics Hand Burns Vol 25 no 4
Philadelphia WB Saunders 2009529e554
11 Kowalske K Outcome assessment after hand burns In Klein MB
ed Hand Clinics Hand Burns Vol 25 no 4 Philadelphia WB
Saunders 2009557e561
12 Smith MA Munster AM Spence RJ Burns of the hand and upper
limbmdasha review Burns 199824(6)493e505
13 Nakamura DY Occupational therapy principles for the burn patient
In Sood R ed Achauer and Sood rsquos Burn Surgery Reconstruction
and Rehabilitation Philadelphia Elsevier 2006370e387
14 Macintyre L Baird M Pressure garments for use in the treatment of hypertrophic scarsmdasha review of the problems associated with their
use Burns 200632(1)10e15
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085
J Hand Surg Am r Vol 39 October 2014
S u r g i c a l T e c h n i q u e
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1213
APPENDIX A PERIOPERATIVE MANAGEMENT
Functional recovery of the burned hand is achieved
through early and ongoing intervention both before
and after surgery Many of the anticipated issues in
the postoperative recovery process are the same as
those in the acute phase of injury pain edema skin
and joint contracture joint and sensory impairments
loss of skin integrity and impaired functional hand
use The burn therapist must have a thorough under-
standing of the effects of burn injury on anatomical
structures and the rehabilitation implications of both
pre- and postoperative intervention to joint tendon
and soft tissue structures10
Ongoing communication
and collaboration between the occupational therapist
and the burn team is essential to the successful
management of the burned hand
Dressings
After surgery dressings provide protection whilefacilitating edema reduction Dressings should not
hinder primary goals for proper positioning and
orthosis fabrication As the wounds heal dressings
should be decreased as much as possible to allow for
the most effective positioning and orthosis fabrication
as well as to allow for greater active and passive ROM
of the hand If possible remove dressings during
stretching exercise and ROM sessions to achieve and
record true ROM limits Removing and reapplying
dressings with rehabilitation treatment also serves to
ensure that wounds are evaluated frequently so that
any negative changes are found early on
Positioning and orthosis fabrication
Positioning and orthosis fabrication of the hand is
instr umental throughout all phases of the burn pro-
cess1112
The goal of ongoing postoperative posi-
tioning and orthosis fabrication is to protect and
optimize healing Individualized plans for positioning
and orthosis fabrication need constant management to
accomm odate for changes throughout the healing
process11 Elevating the distal extremity above the
heart coupled with extension of the elbow facilitatespromotion of increased venous return reducing
vascular pressures in the extremity and allowing for
greater freedom of ROM and protection of structures
in the acute postoperative phase Proper positioning
and orthosis fabrication also promotes elongation
forces on healing tissues to prevent contracture and
improve functional hand outcomes It is generally
accepted that for any burned body part allowing the
position of comfort allows for position of contrac-
ture10
There are many approaches to orthosis fabri-
cation of the hand by therapists but the principles for
preserving joint and tendon function along with pre-
venting scar contracture deformity are the same When
fabricating an orthosis for dorsal hand burns the
antideformity position is generally accepted The
orthosis is fabricated with the hand in the intrinsic plus
position placing the wrist in extension the meta-
carpophalaneal (MCP) joints in 1047298exion the proximal
interphalangeal (PIP) and distal interphalangeal (DIP) joints in extension and the thumb in palmar abduction
to preserve the web space With palmar hand burns
the goal is to preserve 1047297nger extension at the MCP
PIP and DIP joints along with thumb radial abduc-
tion Circumferential hand burns require managing
dorsal and volar positioning and orthosis fabrication
techniques that will allow for the best functional
outcomes10
Positioning and orthosis fabrication goals
may change as the hand undergoes the healing pro-
cess and continual management is necessary to pro-
mote the best postoperative outcomes
Active and passive ROM
Treatment plans for hand burns must incorporate
ROM techniques to promote skin elongation joint
function and muscle and tissue strengthening Active
ROM is generally preferred over passive ROM
however a combination of both active ROM active
assisted ROM and passive ROM is often needed for
achieving full potential of recovery1112
Tissue
elongation pliability and joint articulation are
necessary to prevent scar contracture and achieve
maximal hand function Because scar contraction is a constant 24-hour process exercise should be done
frequently throughout the day and multiple exercise
sessions are preferred over a singular intense session
The patient should be taught ROM and strengthening
exercises as soon as possible Patients actively
engaged in their own ROM and exercise programs
will have increased success in the overall return of
function13
Between exercise sessions positioning
and orthosis fabrication plans must continue Evalu-
ation of orthosis fabrication and positioning should
occur frequently to help maintain andor facilitateROM programs Dynamic components to orthosis
fabrication may provide low load stress and elonga-
tion of tissues over time promoting increases in hand
ROM Ultimately the therapist must progress the
patient to be an active and compliant participant in the
rehabilitation process No prescribed treatment plan
will be successful if the patient participates only when
the therapist is present13
The patient must continue to
perform stretching exercise and ROM between
therapy sessions to achieve the greatest functional
outcome
2085e1 ACUTE SURGICAL MANAGEMENT OF HAND BURNS
J Hand Surg Am r Vol 39 October 2014
S ur gi c al Tec h ni que
892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e

892019 Hand Burns 2014
httpslidepdfcomreaderfullhand-burns-2014 1313
Several methods are used to assess hand function
and include individual joint active ROM passive
ROM total active motion total passive motion
pinch and grip strength sensation and dexterity
Whereas all of these are important to assess hand
function no single assessment can comprehensively
predict functional outcome in the long term11
At
present the correlation between these objectivemeasurements and hand function has not been
clearly de1047297ned Another measure of hand function is
more qualitative in nature but may provide a more
meaningful measure of ldquofunctionrdquo The patient rsquos
own self-report of activities of daily living inde-
pendence and ability to return to work should be
explored by the occupational therapist and be a
driving factor in setting goals in the rehabilitation
process The occupational therapist is instrumental
not only in optimizing hand function after surgery
but also in the reintegration of the patient to thecommunity and return to work Incorporating both
objective and qualitative measur es of hand function
will facilitate the best outcomes13
Compression garments
Compression is often introduced early in the acute
phase of the burn to control edema and this continues
after surgery The amount of compression will vary
depending on the skin integrity and overall ability of
the hand to tolerate pressure This early process can
also serve to normalize the concept of compression
for the patient as a vital part of the healing process10
Typically compression for the purpose of scar con-
trol starts when a majority of wounds are healed and
the skin is at a point that can tolerate the wearing of
garments Scar compression garments are typically in
the pressure range of 25 to 30 mm Hg and can beboth commercially available and custom fabricated to
therapist measurements14
The compression garment
may fail to provide even pressure owing to its
inability to completely conform to the hand Most
often these areas are in the web spaces between
digits in the palm and at the volar and dorsal wrist It
may be necessary to apply inser ts to keep pressure as
even as possible in all areas10
Manufacturers of
custom compression garments can often incorporate
foam or silicon inserts to selected areas Garments are
typically prescribed with a wear schedule of at least 23 hd1014
Garments are replaced periodically
throughout the 12- to 18-month scar maturation
phase The prescription of constant wear damages the
garment rsquos integrity and compromises the initial
pressures needed to affect scar tissue Assessing the
hand measurements regularly ensures proper garment
1047297tting with anticipated changes in edema skin
integrity ROM and development of hypertrophic
scar14
ACUTE SURGICAL MANAGEMENT OF HAND BURNS 2085e2
J H d S A V l O b
S u r g i c a l T e c h n i q u e