-
8/6/2019 Hand Book of Evaluation
1/89
HANDBOOK FOR THE EVALUATION
OF THE
QUALITY OF LIFE IN THE SCHIZOPHRENIC
Department of Psychiatry
Clinical care service.
Chainama Hills College Hospital
Board of Management LUSAKA/ZAMBIA
1
-
8/6/2019 Hand Book of Evaluation
2/89
2
-
8/6/2019 Hand Book of Evaluation
3/89
Acknowledgement
We are grateful to the following persons for their various
contributions:
Dr M. Zulu, Executive Director - Chainama Hills College
Hospital Board of Management (CHCHBM), Lusaka -Zambia, for her
motherly heart with which she has been
attending to our various problems,
Dr P.C. Msoni, Consultant Psychiatrist -Director Clinical
Care, Chainama Hills College Hospital Board of
Management, for his cheerfulness, friendship
andunderstanding,
Pr Haworth, for his moral support as a good family father,
Pr Kinsala Ya Bassy - Neuropsychiatrist, Head of
Psychiatric Department, University of Kinshasa, for hisvaluable
scientific contribution to this work,
Mampinda Voltaire, Senior Customs Expert-COMESA and
Ankiba Nestor - Fuels & Lead Country Manager
EXXOMOBIL for their logistical support,
Dr Yassa Consultant Dermatologist - University Teaching
Hospital, Lusaka - Zambia, Dr Sheik- Registrar, CHCHBM,
Mr. Abraham Mulenga, Clinical Officer, CHCHBM and Dr
Tchikara Consultant Psychiatrist - Parirenyatwa Hospital,
Harare-Zimbabwe, for having facilitated and created in
various ways an enabling environment for my work,
3
-
8/6/2019 Hand Book of Evaluation
4/89
We would also like to extend our gratitude to all the
nurses,
clinical officers and general workers ofCHCHBM for their various
contributions to the realization of
this piece of work.
4
-
8/6/2019 Hand Book of Evaluation
5/89
The Authors
Dr J.Kaswa KASIAMA (MD)
Senior Lecturer, secretary of the department of Psychiatry,
in
charge of teaching,
Neuropsychiatrist
University of KinshasaFormer Deputy Director,
Neuro-Psycho-Pathological Center -
University of Kinshasa D.R.C.
Senior Registrar - Chainama Hills College Hospital Board of
Management
Department of Psychiatry, Lusaka - Zambia
Kawele Allan
Bsc Comp. Sc., MA Leadership and Org. Mgt., MCSE, CCAILecturer-
ICT
Katanga Methodist University,Evelyn Hone College,
UNZA-Cisco Centre
Lusaka-Zambia
5
-
8/6/2019 Hand Book of Evaluation
6/89
Pr. S. Mampunza Ma Miezi (MD)
Former Director, C.N.P.P., University of Kinshasa D.R.C
Professeur AgrgNeuropsychiatrist
Facult de mdecine - Universit de Kinshasa R.D.C.
Dr. Kaswa Kayomo M. (MD)
Clinical
Mycobacteriology Laboratory,
David Axeirod Institute
Albany, NY 121208
Science in the Pursuit of HealthUSA
Pr. Odimba BwanaFwambaKoshe E.,
MD MPH MGS MSC PHD of Paris,
Ordinary Professor, Former Dean School of Medicine Unilu
D.R.C.
6
-
8/6/2019 Hand Book of Evaluation
7/89
Consultant Surgeon / University Teaching Hospital, Lusaka -
Zambia
7
-
8/6/2019 Hand Book of Evaluation
8/89
8
-
8/6/2019 Hand Book of Evaluation
9/89
Foreword
Chainama Hills College Hospital Board of Management:
A third level psychiatric hospital, which has the mandate
toProvide:
- quality mental health services,
- training of primary health care providers
- impacting clinical psychiatric acumen to students from
health colleges and the university of Zambia,
- conducting research.The hospital was built in 1961 with the
bed capacity of 260
patients.
It was officially opened on the 20th June 1962
It consists of six wards, including a fee-paying ward.(A
ward), B and C wards as acute admission wards, E and F
9
-
8/6/2019 Hand Book of Evaluation
10/89
wards as rehabilitation wards male and female and children
respectively and L ward for forensic patients, Chainama east
in 1967,built to admit medical forensic patients.Since 1968 the
hospital had a bed capacity of 500 patients.
Suffering due to chronic diseases is often associated to
real-
life experience, that feeling that the patient has of
loosingcontrol over his own life, a feeling that is often
strengthened
by the fact that the entourage and the physicians do not
take
his personal impressions into account.
Indeed, the latters pay attention to clinical signs and
symptoms, whereas for the patient, leisure, joys of life
andactivities come first. Moreover, he complains about his
therapist who ignores his subjective experiences, which are
yet at the base of decisions concerning his treatment; a
breakdown can be brought about by the divergence betweenthe
clinician and the patients expectations.
The evaluation of the quality of life of the schizophrenic
(EQLS) patient is a complete self-evaluation measure made to
give a review of the aspects of the quality of life relating
to
health affected by schizophrenia.
Hopefully this handbook will serve as reference for the levelof
quality of life of the schizophrenic patients in our
psychiatry department.
10
-
8/6/2019 Hand Book of Evaluation
11/89
The handbook includes the following points:
Problems and objectives
SchizophreniaDevelopment of the evaluation scale of the quality
of life
Psychometric comparison of instruments
Constructing the questionnaire
Evaluation scale of the quality of life of the schizophrenic
(EQLS)Scoring formula
Handbook for the investigator
Conditions of administration
Dr SHEIK M.D.
Chainama Hills College Hospital Board of Management
11
-
8/6/2019 Hand Book of Evaluation
12/89
12
-
8/6/2019 Hand Book of Evaluation
13/89
TABLE OF CONTENTS
ACKNOWLEDGEMENT.3
THE AUTHORS5
FOREWORD.9
PagesCHAPTER I: Problems and objectives.......
. 17
The problem 18
Real-life experience and quality of life.. 20
What are we looking for?....... 23
Objectives... 24
CHAPTER II : Schizophrenia .... 27
Target population ... .. 28
Epidemiological definition. 29Taking charge of medical care
31
CHAPTER III : Development of the evaluation
of the quality of life 33
Quality of life in schizophrenia.... 34
Specific instruments ........ 36
Properties to be observed..... 37
CHAPTER IV : Psychometric comparison 45
Choice..... 46
Psychometric comparison of instruments... 49
CHAPTER V : Constructing the questionnaire.. . 51
13
-
8/6/2019 Hand Book of Evaluation
14/89
Stage I: Conception of the questionnaire.. 53
Stage II: Constructing the questionnaire...... 57
Stage III: Forming an evaluation scale of thequality of life of
the schizophrenic........... 58
CHAPTER VI : Evaluation scale of the quality
of life of theschizophrenic(EQLS)..... 59
Health.... 61Psychic symptoms ....... 61
Self-esteem / well-being.. 62
Relation with family..... 63
Social and love relationships .. 64
Leisure / creativity 64
Participation in community life ....... 65Religion. 68
Financial situation..... 67
Living conditions . 68
Autonomy.... 69
CHAPTER VII : Scoring formula............. 71For an item...
72
For a field... 72
For a scale. 73
CHAPTER VIII : The interviewershandbook.. 75
Age ....... 76
Sex........ 76
Residence in Zambia (province).. 76
Ethnic groups.... 77
Real-life experience and report. 79
14
-
8/6/2019 Hand Book of Evaluation
15/89
Stabilisation and report ........ 80
Typical questions . 81
CHAPTER IX : Condition of administration 83
The patients consent ........... 84
Enlightened free consentement... 84
Precautions to be taken ... 84
REFERENCES.. 87
15
-
8/6/2019 Hand Book of Evaluation
16/89
ZAMBI ETHNIC GROUPS
16
-
8/6/2019 Hand Book of Evaluation
17/89
- The problem- Real-life experience and quality of life
- What are we looking for?
- Objectives
17
PROBLEMS ANDOBJECTIVES
-
8/6/2019 Hand Book of Evaluation
18/89
CHAPTER I: PROBLEMS AND OBJECTIVES
The problem
During the last 50 years, care has evolved towards a
community pattern based on two main principles:
respect of basic rights of individuals suffering from
behavioural and mental disorders, resorting to most
moderninterventions and techniques, which, in the best of cases,
are
translated by a careful desinstitutionalisation supported by
health agents, consumers, families, progressive communities.
This is what the 14 / 9 / 1990 CARACAS declaration meant
at the Regional Conference on Restructuring Psychiatric Care
in Latin America (VENEZUELA), more precisely:restructuring based
on primary health care revision of the
hemogenic and centralizing role of the psychiatric hospital
KaswaPhoto : mental patients-CHAINAMA Hospital. LUSAKAimperative
preservation of the dignity of the person as well as
that of human rights.
Alas, as we all know, the world is far from being perfect.
18
-
8/6/2019 Hand Book of Evaluation
19/89
The mental patient image, perceptions and mental health
practices have not evolved and remain controversial or, lets
admit it, always problematic.Social perception of the mental
patient, as for other diseases,
leper yesterday, HIV/AIDS today, has certainly gone through
changes, but those changes are slow, marked by hesitations
and a feeling of discouragement. These developments are
perceived by the mental patient as oscillating between
almosttotal lack of interest and excessive and inhibitive sense
of
guilt.
During this period placed under the emblem of tolerance and
human rights, perhaps the time has come to introduce one of
the wishes of society, namely respect of differences that
could
exist in the way individuals are and think, especially if
thosedifferences are inherent to their diseases and to hazards
of
their existence.
Hence, should the mental disease not arouse contradictory
feelings today, divided between pity, compassion, fear,rejection
and hatred?
Nevertheless, despite the progress in the treatment and
effortsto improve how to take charge of mental patients, there
are
still many important unanswered questions!
What image does the mental patient have of himself?
What does his inner life conceal?
What does his silence mean?
Does his inner life organized so as to lead the subject to
theacceptance of himself, others and reality?
What are his living conditions?
Finally, how does he live himself and to what does his
quality
of life tally?
Such are the questions that certainly deserve a clear answer.
If
the patient does not say anything, be careful, for that does
not
19
-
8/6/2019 Hand Book of Evaluation
20/89
mean that nothing is happening. It is a question of his
invisible life, with a litany of complaints and reactions
externalized by loss of esteem and self-confidence,
increasinguncertainty about tomorrow (the future?) and somewhere
an
illusion of being still a human being. There is therefore
for
society a kind of air vent on the patients real-life
experience
by himself, on the way he conceives himself in reality,even
if
externally he shows restlessness, sadness and other
bodilyexpressions.
Real-life Experience and quality of life
Psychiatry equals madness is still too present in our minds.
A consensus emerges from all the literature: people
sufferingfrom serious mental incapacity have serious difficulties
to
live in society and they have trouble integrating a position
in
the framework of basic social institutions of our community
(family, work). Hence, the return to the fold, after
psychiatricconsultation shows a problematic feature with
numerous
obstacles. For the large public; the psychiatric hospitalremains
a stigmatized institution, to such extent that, after
staying for some time there, the mental patient is often
associated with the psychiatric hospital and he has to start
a
patient trajectory; a psychiatric carrier.
The prejudice is notonly considerable
and long lasting, but
it is even mediocre,
even after healing
(4).
20
-
8/6/2019 Hand Book of Evaluation
21/89
For the large public; the psychiatric hospital remains a
stigmatized
institution (Chainama Hospital-Lusaka/Zambia). Kaswa Photo
Henceforth, the patient has to fight exclusion all his life.
More often than not, confinement and isolation appear to be
the sole alternative.
Hence this bad self-real-life experience, the
non-satisfaction
of basic social and functional needs (18) are predictive
factors
of a bad quality life of subjects suffering from
severedisorders.
Today health is no longer defined as an absence of disease,
but as a complete state of physical, psychological and
social
welfare.
As for mental health, despite the social progress and progressin
present psychiatry, we cannot sum up in a clear and precise
definition the complexity of phenomena that are made up by
the whole of mental disorders.
Lets say that mental disease appears as a disorder that
affects
the thought, feelings, or behavior of a person to such
extent
that his conduct becomes incomprehensible and unacceptablefor
his entourage. Therefore, the individual is affected in his
personnel equilibrium as well as in relationships with other
people. According to the model used most frequently in
contemporary psychiatry, the biopsychosocial model, mental
disease does not presuppose any unidimensional cause butrather
an array or accumulation of factors of biological, psychological
and social nature that negatively affect the
individuals equilibrium.
Mental disease does not mean mental deficiency! The
latter is a state that limits a persons learning (3).
21
-
8/6/2019 Hand Book of Evaluation
22/89
The real-life experience is the perception of ones own
vulnerability, ones experience of disease, the subjects
internal perception, subject that is his own reference, his
ownwitness.
GOOD REAL-LIFE EXPERIENCE: the adaptive aspect of
health; which, according to us, is a relatively trouble free
mental state that enables the individual to function
asefficiently and for as long as possible in the environment
where he will be placed by chance or by choice.
The quality of life tends to replace the notion of good
health. The quality of life, from an individual point of
view,
is what one wishes on an new year day, not simple survival, but
what makes life to be good (health, love, success,
comfort; pleasure), in short happiness From Good health
at all cost, we have moved to a relativisation of the
physical,
mental, and social state of individuals. Each disease shows
itscharacteristics and therefore its consequences on the
quality
of life of the patient who is suffering from it.
Adaptation to the environment makes it necessary to
communicate with him. Optimal communication is the
harmony wanted by man with himself and with his
environment, hence with others. The difficulty comes from
the fact that other people are not static but they
changecontinually, hence the need of a dynamic adaptation. The
latter, according to each ones moments of life, environment,
culture, is set to enter a model of meaning of life that
associates actual real-life experience, received ideas and
the
imaginary. This meaning given to life encompasses
22
-
8/6/2019 Hand Book of Evaluation
23/89
biological, psychological and sociological aspects in a
given
cultural framework.
Quality of life is the perception that an individual has
about
his place in existence, in the context of culture and value
system in which he lives in relation with his objectives,
expectations, norms, and preoccupations. It is a very large
concept that is influenced in a complex manner by thesubjects
physical health; psychological state, level of
independence, social relations as well as his relation with
essential elements of his environment (W.H.O., 8. 1993). The
quality of life concept includes physical and psychological
health, the degree of autonomy, social relations, personal
options, and relationship with the environment. Health
andquality of life tie up and complete each other (8).
Only the subject can assess his quality of life. There is no
possible yardstick in this matter, no norm, no
standardization.
What are we looking for?
Certainly, misfortune and suffering cannot be measured;
however, we can imagine the impact of these troubles thanks
to instruments used to assess the quality of life (28). Living
is
also laughing, singing, crying, arguing, touching, going
out,
loving, sleeping, caring for ones body, enjoying life. We
think that it is a complex conception between physical
health,psychological state, believes and social relations (16).
Therefore we will try to demonstrate that, by helping the
schizophrenic to improve himself his real-life experience,
through information, education and communication, he will
change and his quality of life will improve. He would be, in
this way, the first person to unmaddenise psychiatry!
23
-
8/6/2019 Hand Book of Evaluation
24/89
Perception of his own vulnerability and of his experience of
the disease will greatly influence his quality of life, even
if,
after all, doctors are the people who determine the
treatment(2).
Thus, we turn towards a practical application for the
benefit
of the patient, that is:
Collecting reliable data that enable us to appraise the
relevance of some therapeutic momentum, indicating changesin the
fields of quality of life that are of interest to everybody,
the patient, the family, as well as the practitioner (26),
assess
the effects of our intervention on the perception by the
patient
of his state, evaluate the quality of life before and after
the
improvement of real-life experience by himself.
An interesting approach consists in setting, from the opinionof
our patients, a questionnaire on quality of life, adapted to
our sociocultural context (14).
Objectives
Improving and promoting the state of health of theschizophrenic
through changing his real-life experience of his
state and through reducing handicaps, distress and
discomfort,
in order to enable him to live better with his disease.
Learning to observe, to distinguish between the clinical
signs
and a mental dysfunction, to listen to the psychical
suffering
hidden behind behavioral disorders, to collect and canalizethat
anguish, at times unbearable, that the patients pass back
to us and to accompany the patient in view of a return to an
ordinary environment to live differently among other people.
Taking into consideration the perception by the patient of
his
own state of health by perfecting instruments for specific
24
-
8/6/2019 Hand Book of Evaluation
25/89
measurements adapted to our environment, and make
accessible the deep feeling of the patients and their
capacity
to satisfy their needs and desires which have often
remainedinaccessible by lack of appropriate means of
evaluation.
To consider henceforth, under a new day, mental health,
neglected for a long time, in the psychodynamic
comprehension of the caregiver-cared relationship anddemonstrate
the need to improve relationships between the
caregivers, the entourage and the patients.
Giving health professionals the means to know better the
extent of the mental health problems of the schizophrenics
for
whom they work, in the interest of better care in order
toimprove prevention, therapeutic capacity, rehabilitation and
reinsertion, and putting at the disposal of the community an
indicator that enables to spot patients presenting low levels
of
quality of life in order to develop more precociously help
andadapted medico-social support strategies.
To complete henceforth treatments aiming at curing through
specific care turned towards change of the mental patients
real-life experience by himself and his entourage and
through
development of the patients relational abilities; as well as
aptitudes to sociocultural and socio-professional exchanges
and thus get to not reinserting in the community the
stablechronic mental patient by means of a chemical strait
jacket,
which is equivalent to confinement in hospital, without any
reason.
25
-
8/6/2019 Hand Book of Evaluation
26/89
26
-
8/6/2019 Hand Book of Evaluation
27/89
- -Target population
- -Epidemiological definition
- -Taking charge of medical care
27
SCHIZOPHRENIA
-
8/6/2019 Hand Book of Evaluation
28/89
CHAPTER II: SCHIZOPHRENIA
Target population
Schizophrenia; often rejected, of apparently easy diagnosis,
is
costly and it has a deep influence on the patients existence
and subjective feeling of well-being. Suffering from an
incurable mental disease, the individual accepts its
socialconsequences daily. This pathology requires regular
hospitalisation, which causes heavy constraints for
patients,
who have little financial resources in general and often live
at
their parents near whom they are submitted to considerable
tension to the extent of being separated from them due to
chronicity and to a series of ever-present symptoms.Few of them
manage to break through some maturing stages
of the adult life such as marital life, having children or a
job
within which they can blossom. It is in this category that
we
should recruit, in a given period, all stabilized subjects
amonga population of schizophrenic outpatients, thus living
between
the hospital and their home, hospitalized at least twice, andwho
have all been diagnosed schizophrenics according to
DSM-IV criteria.
Stability will be an additional criterion for the choice, as
the
patient has to show coherence of speech, aptitude to answer
questions, lucidity and a beginning of adaptation to his
environment.
28
-
8/6/2019 Hand Book of Evaluation
29/89
Epidemiological definition
Schizophrenia is a group of psychoses that have a
commonsemiological core: dissociation.
It marks a dislocation of psychic life in different sectors
of
intelligence, thought, affectiveness, relationship life and
apprehension of reality.
Schizophrenia is a change of brain functioning that disturbsthe
thought and judgment process, sensorial perception and
capacity to interpret and react in an appropriate manner to
particular situations or stimuli are affected.
This symptomatology deeply affects the existence of the
individual. The high suicide rate translates the exceptional
nature of the schizophrenics feelings about their
life.(Lemperire, 1996).
Schizophrenia is a destabilizing chronic disease affecting
1%
of the population. Studies have demonstrated a prevalence of0.6
to 8.3 for 1000 inhabitants, about one per cent of the adult
population suffers from schizophrenia (Shur 1988).
29
-
8/6/2019 Hand Book of Evaluation
30/89
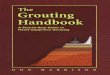
Source: O.M.S. J.M.S 2001
Number of schizophrenic patients in the world (in millions)
Photo Kaswa
The first symptoms usually appear between the age of 17 and
24 and can be mistaken for behaviors related to adolescence.Ben
Ismalwrites that deep social changes during the two last
decades and intense acculturation conflicts have caused
aspectacular progression of schizophrenia, mainly in urban
large cities.
In 1972, Lejri and Ammar also observed that schizophrenia
was developing more and more in favor of present family
constellation disturbances and the sense of unfulfilment of
families with physical or functional exclusion of one of thetwo
parents. On our part, should we emphasize the
importance of what we live in the cultures overlap, the
infinite increase in the number of scales of values and
society
patterns, conveyed, up to inside our homes, by media
invading through satellite dishes, cinemas, etc? Are these
contradictory models not at the origin of difficulties of
30
-
8/6/2019 Hand Book of Evaluation
31/89
identification involving individual fragility that it might
cause
at the cultural scission of the Self level
Taking charge of medical care
A few decades ago, healing at any cost preoccupied medicine
and chronically ill people were receiving less attention.
During the recent decades, the pharmacological approachprevailed
and had a significant importance. Usually; drugs
control positive symptoms (hallucinations, delirium); they
have no or little effect on negative symptoms (personality
disorder). If one can live without any drugs, one cannot
live without care. Modern man is no longer surviving, he
lives longer and now he wishes to live better. Even if diseaseis
invalidating, it should not be a nuisance (17). Taking
charge of schizophrenics entails a whole spectrum of
interventions that must include medicines, psychological
support, rehabilitation and reinsertion efforts.
Today, when a patient does not heal, the approach isdifferent;
one tries as hard as possible to maintain his
autonomy and quality of life (6).
31
-
8/6/2019 Hand Book of Evaluation
32/89
32
-
8/6/2019 Hand Book of Evaluation
33/89
- Quality of life in schizophrenia
- Specific instruments- Properties to be observed
33
DEVELOPMENT OFEVALUATION OF THE
QUALITY OF LIFE
-
8/6/2019 Hand Book of Evaluation
34/89
CHAPTER III: DEVELOPMENT OF THE
EVALUATION OF QUALITY OF LIFE
Quality of life in schizophrenia
This work develops a questionnaire for measuring the quality
of life of the schizophrenic through improvement of his life
by himself.Interest in the quality of life in schizophrenia has
grown,
between 1960 and 1970, with the desinstitutionalisation
movement (1). Since the eighties, a lot of effort has been
deployed to determine whether schizophrenic patients were
capable or not of assessing their own quality of life. (21).
In 1983, Lehman demonstrated that indicators of the quality
of life were reliable on patients suffering from chronic
psychiatric disorders. The author concludes that mental
health
does not alter significantly the answers of the
subjects.According to these results, quality of subjective life
is
measurable with these types of patients (20).
Other studies confirm these results (Voruganti and coll.
1998,
Lehman and coll., 1993, Franz and coll., 2001).
However Lehman observes that the mental health index and
subjective indicators of the quality of life are correlated.
Thus individuals suffering from mental disorders are
reallycapable of assessing their quality of life, but they also
have a
specific conception of their life.
Therefore, setting up a questionnaire from the patients
opinion seems to be an interesting approach to be
privileged.
We should not loose sight of the fact that data collected
are
34
-
8/6/2019 Hand Book of Evaluation
35/89
meaningful only if it is specified that it is the quality of
life
seen through an individual suffering from schizophrenia.
Indeed, his conception is to be distinguished from that whichis
accepted by most sane individuals or those suffering from
affection that is less weakening physically (14).
The presence of a therapeutic relationship is likely to help
the
patient to assess his quality of life (McAbe and coll.
1999).
35
-
8/6/2019 Hand Book of Evaluation
36/89
Specific instruments
Measuring instruments of the quality of life were elaboratedfrom
different health and disease models.
Thus, some instruments use a functional health model while
others use an experimental model, in the sense that they
take
into account the subjects experiences in relation to
disease.
(Cf. Costain and coll., 1993). Each instrument categorytackles
consumers problems from a different angle (10).
The choice of the instrument and the conception of the
survey/evaluation have an influence on the capacity to
detect
change between observed individuals. Many different types
of questionnaires were consulted. However, they were not all
appropriate for us for the following reasons:some were
considered too long (more than 100 items)
others should be completed by other experts others still had
a
very short view of the quality of life some were even
limited
in terms of their psychometric properties the system had tobe a
self-evaluation.
36
-
8/6/2019 Hand Book of Evaluation
37/89
Properties to be observed
Subjective measures are often constructed from self-administered
questionnaires. They relate to many health
factors, to perceptions, to attitudes in relation to health,
welfare, habits of life as well as to functional
limitations:
autonomy, sociability, incapacity. There are several sources
of chancy error that are necessarily linked to the conceptionand
application of the instruments. There is good reason to do
anything, at the planning stage, to increase the accuracy of
the
evaluation and to detect better the possibilities of error
(12).
Roughly, two types of errors in the answers have the effect
of
reducing coherence of the sets of data (reducing the level
of
reliability) and undermine the trust that one can have in
theresults obtained.
Firstly, there is non-systematic or chancy error, which
occurs
when the scores obtained by the subjects are influenced
bychance. This type of error decreases the accuracy of the
estimated value of a parameter by increasing the
unexplainedvariation in the whole lot of data.
When the whole lot of data is too vague, significant
differences that could be found there risk more passing
unnoticed.
Secondly, there is systematic error that occurs when there is
asystematic and unforeseen element that affects all the
observations in the same way and distorts conclusions.
The possibility of a systematic error compromises the
significance or validity of any important conclusion. Thus,
before designing a new measuring instrument of the quality
of
life, it is imperious to know some psychometric principles
in
37
-
8/6/2019 Hand Book of Evaluation
38/89
order to know that it is the patients quality of life that
is
really being measured (5). Though a complete analysis of
this
process extend beyond the framework of this document, weare
compelled to consult a good book on designing
investigation plans, and in the present case, Portney and
Watkins, 1993. Therefore it appeared important to us to
remind those principles here.
The quality of a scale of evaluation of the quality of life
is
defined by its degree of validity and reliability. Validity
concerns coherence of the scale with the whole lot of data
that
one possesses inside a field (external validity), but also
coherence of these figures with other figures taken in the
same population (internal validity). This validity, of course,
isthat of the degree of significance of the instrument and data
that it allows to obtain (15).
Questions such as what is really being measured?
What do the results mean?These results, do they apply to other
people?
The validity of an instrument or a method refers to its degree
of truth . Determining the significance or the truth
of a measurement is a complex question that supposes that
the
return of an instrument in relation to that of other
instruments
or criteria duly proved to establish to which extent it
fulfils
the expected function of the evaluation activity
(32).
Several types of validity can be counted, notably the
apparent
validity, content validity, construct validity, convergent
validity, and predictive validity (Weiner and Stewart, 1984,
Aiken, 1991). We shall look hereafter into the determination
of the apparent/content validity and converging/predictive
38
-
8/6/2019 Hand Book of Evaluation
39/89
validity since these are concepts that evaluators should
know
thoroughly.
Apparent validity and content validity: apparent validitymeans
the degree at which an instrument appears to ask
questions on a content that concerns both the measured
objective and the respondents experience. In other words, if
a
measuring instrument of the quality of life seems to have no
relationship with the respondents life experience, the
givenanswers have more risk of containing errors attributable
to
wrong interpretations or lack of motivation, possible source
of inattention on the part of the respondent. In addition,
less
relevant items can give rise to answers that are impossible
to
interpret. Such is the case for example when one asks a
group
of schizophrenic subjects questions relating to
theirsatisfaction with regard to their spouses when in fact very
few
of them are married.
The content validity is close to apparent validity, the
maindifference between the two being that, in the first case, it is
a
group of experts that examines the instrument and determinesat
which degree questions of an instrument are used to
measure the studied characteristics.
The convergence of views between people who are perfectly
familiar with a subject, concerning the content of an
instrument, contributes to validating its content (Streiner,
1993).It is frequent for the validity of an instrument to be
compromised when respondents have different interpretations
of the meaning of an item. For example, if the statement: To
what extent are you close to your family? is interpreted in
such a way that family members evoke for some
descendants and for others ascendants , data relating to
39
-
8/6/2019 Hand Book of Evaluation
40/89
the group become impossible to interpret. Hence the
necessity
to take into consideration interpretations to which items
could
give rise in people supposed to answer a questionnaire onquality
of life. Hence also the necessity to skim through the
instrument in order to determine the items and the scales
are
adapted to the understanding level of the respondents
(vocabulary, educational standard, etc.).
Construct validity: a theoretical concept that was created
to
explain and structure some aspects of knowledge [and
observations] (American Psychological Association, 1974,
p. 29).
Among the constructs used in measuring instruments of the
quality of life, there are the satisfaction, importance
andfunctioning in the fields of personal, family, social and
community life. The perfecting of measuring instruments or
scales that allow measuring properly such constructs is a
process said of construct validation. Measurements taken byusing
an instrument that has good construct validity will give
results in correlation with those of other instruments that
aretheoretically about the same constructs.
For example, if a researcher who tackles the quality of life
from an objective point of view elaborates a new measure of
the intellectual functioning, one could, in principle, expect
a
correlation between results obtained by means of that
instrument and those of other measurements duly tested
andvalidated of skilfulness, functioning and intellectual
efficiency.
Another method used commonly used to determine the
construct validity of an instrument is the validation
factorial
analysis. It is a statistical method that consists in assessing
the
40
-
8/6/2019 Hand Book of Evaluation
41/89
answers given to items of an instrument in order to
establish
if they regroup, as they should theoretically.
Thus, there should be strong correlation between items thatrely
on the global satisfaction construct. On the contrary,
correlation between items based on the physical functioning
construct and those that stake on global satisfaction should
not be too high.
External validity: a type of validity often taken for
granted
consists in knowing to what extent inferences made from
results describe the whole population. More precisely,
external validity refers to the adaptability between
instruments and methods on one hand, and the object of the
survey on the other hand.When one neglects to establish the
correlation between the
instrument and the measured objective, the significance of
any observation can be questioned and there is a risk of not
leading to any conclusion.If the results obtained by means of
these measurements are
often comparable from one instrument to the other, their
linkswith the effects due to processing are less obvious (19).
Reliability is the sensitivity and specificity of the scale,
that
is to say, the potential of data to vary according to
effective
variations of the phenomenon that one wants to observe.
As a reminder, reliability refers to coherence in the
collectionof data by means of a measuring instrument or method.
Our instruments internal coherence will be good if subjects
will answer in a coherent manner similar items of that same
instrument. We also consider the temporal coherence of the
instrument to be good when the same subjects, assessed twice
41
-
8/6/2019 Hand Book of Evaluation
42/89
(at different times), get essentially identical scores (the
studied characteristics do not change).
As the scale is formed of closely linked items, its
internalcoherence index, the Cronbach Alpha coefficient (9)
must
be satisfactory (> 80).
Reliability and validity are at the base of any measuring
activity, and it was necessary for us to properly grasp
theseconcepts as we wanted very much to take enlightened
decisions at the time of planning for the assessment project
implementation and analysis.
It is known that, the higher the number of items, the higher
its
reliability will be. Thus, all other factors being equal, a
questionnaire relating to quality of life that has less items
willbe less coherent than a longer instrument and it will give
rise
to more fluctuations in the scores obtained by the patients,
due to chance answers.
Apart from mathematical considerations, various reasons
explain why multiple category scales are in the whole
morecoherent than instruments that call on unique categories.
An
interesting theory was put forward to account for this
phenomenon, i.e. that multiple category instruments
generally
incite subjects to search their memories in order to find
relevant experiences that will guide their answers.
It seems that this search for relevant information elements
hasthe effect of reducing quick judgment and preconscious
thought impact that are only tangentially linked to the
prime
raison dtre of the question (Pavot and Denier, 1993a).
Another way of increasing the answers coherence is to ask
respondents to find and list fields that they think are the
most
important. (cf. Schedule for the Evaluation of Individuals
42
-
8/6/2019 Hand Book of Evaluation
43/89
Quality of Life see XXVI, chapter 5) or still attach the
categories back to their recent life experiences.
This way of proceeding has other advantages, for it enables usto
rapidly see to what extent the item is well understood by
the subject and whether it shows interest for him.
We did also proceed to doing test-retest reliability and
parallel form reliability.
Another mean of assessing the accuracy of a scale consists
indetermining to what extent two assessments made at two
different times using the same scale and with the same
subjects, match up, in other words, of establishing the
degree
of correlation between results.
Of course, we start here from the notion that the time
interval
must be sufficiently brief so that we have the insurance thatthe
measured characteristics do not change between the two
assessment sessions, but long enough to ensure that the
subjects do not answer from memory (30).
The test-retest trust coefficient indicates to what extent
answers to the same items are identical when the same test
isadministered to the same subjects at different times. In
general, the test-retest constancy index is slightly lower
than
the internal coherence index (Generally, a >0.75
coefficient
indicates sufficient test-retest constancy).
43
-
8/6/2019 Hand Book of Evaluation
44/89
44
-
8/6/2019 Hand Book of Evaluation
45/89
-
8/6/2019 Hand Book of Evaluation
46/89
CHAPTER IV: PSYCHOMETRIC COMPARISON
ChoiceWe had to consult several types of quality of life
assessing
instruments. We started from a table showing 28 instruments
on which their reliability and validity principles rested. It
was
not easy for us to determine the quality of instruments, the
trust coefficients varying according to the number of items.We
know that it is perhaps preferable, when we embark upon
an evaluation, to choose a short instrument, easy to
administer
and less accurate than a long, very stable and very reliable
indicator. Likewise, instruments that measure individuals
behaviour or symptoms are generally less homogenous, such
that their internal coherence is lower than scales composed
ofmore general and evaluative items. Before such panoply, each
of the rubrics of these instruments was examined in detail
to
enable us to make a choice (11).
This choice of the instrument depended on various factors:
the type of questionnaire,the fields of study,
questions for each field,
especially the necessary resources for its application.
All that should meet our objectives to such extent that a
realistic compromise was to be found between clinical
efficacy and learned assessment.Our decision were equally
influenced by the choice and
accessibility of psychometric analyses:
reliability and validity,
the method of data collection,
the characteristics of the items,
the approximate administration time.
46
-
8/6/2019 Hand Book of Evaluation
47/89
I any case, the relevance of our instrument; it does not
matter
the mode of administration, had to be appreciated according
to the usage that we wanted to make of it with ourrespondents
and according to whether or not the instrument
enabled us to get answers to the questions asked by the
study.
To avoid being confronted to the high cost of evaluation, we
proposed, as a solution, to resort to a self-administered
questionnaire and to automated systems of data collection
andinput in order to use computing to assess the quality of
life.
Thus, We decided to explore and analyse thoroughly three
evaluation tools of the chronic mental patients quality of
life,
more especially the schizophrenic, whose psychometric
qualities are tested.
These are:
S-QoL of Marseilles (1),
the SQLS of Oxford Outcomes (13) and
QL of Leyman. (21).The S-QoL
Recently the public health laboratory of the Marseilles schoolof
medicine, with the collaboration of PsycCLE (Cognition,
language and Emotions Psychology Research Center) and the
psychiatry service of the CHU of Timone developed a new
measuring instrument of quality of life specific to
schizophrenia that can be self-administered.
SQLS OXFORD OUTCOMES
In case of certain very frequently used instruments such as
the
Oxford Outcomes, we selected representative items among
about thirty that existed taking into account the interest
they
represented for the study population.
47
-
8/6/2019 Hand Book of Evaluation
48/89
LEHMAN (QL)
The method consists in collecting the opinion of the
interested
party on several aspects of his life in order to assess
theconsequences of harmful symptoms and disorders.
48
-
8/6/2019 Hand Book of Evaluation
49/89
Psychometric comparisons of instruments
APPLIED FIELDS OF LIFE
Measuringinstruments
Health
Symptoms
Financialsituation
Livingconditions
Family
Socialandloverelations
Leisure/
Creativity
Particip
ationtocommunity
life
Religion
Self-esteem/well-being
Sqo
L
* * * * * * * * *
SQ
Ls
* * * * *
QL
LE
HM
AN
* * * * * * * * * *
The three tools have in common, as far as psychometrics is
concerned:
Specificity of the chronic mental patient, the
schizophrenic,subjectivity, self-evaluation, reliability, validity,
feasibility,
satisfaction.
They are among the most recent and up to date; the fields of
life, the number and the types of items, as well as the time
required for the survey differ.
49
-
8/6/2019 Hand Book of Evaluation
50/89
We borrowed from some and from others, either some items
from SqoL and SQLS and fields from QL of LEHMAN,
which we adapted later to our sociocultural context.From these
tools, it is LEHMAN that seemed to deal
thoroughly with the question of fields of life registered by
the
Quality of life evaluation interview. That is how we are
going
to construct our questionnaire using the last instrument as
a
basis, to which we shall add some missing elements fromothers,
the whole thing has to be adapted to our population,
our sociocultural environment and to objectives of the
questionnaire, while attending to the common-core syllabus.
50
-
8/6/2019 Hand Book of Evaluation
51/89
51
Constructing thequestionnaire
-
8/6/2019 Hand Book of Evaluation
52/89
STAGES:
Stage I: Conception of the questionnaire
Stage II: Constructing the questionnaireStage III: Forming stage
of the evaluation scale of the quality
of life in the schizophrenic patient
52
-
8/6/2019 Hand Book of Evaluation
53/89
CHAPTER V: CONSTRUCTING THE
QUESTIONNAIRE
Quality of life evaluation instruments are standardised
tools.
The construction and analysis methodology of the
questionnaire is established and recognised by the
international community. One of the applications of these
new measurements is the assessment by the patientsthemselves of
their state of health (24).
We want to know if the schizophrenics are happy, the best is
to ask them. It is therefore a questionnaire that is designed
to
assess conditions in which people suffering from serious
mental diseases live, by examining subjective evaluationfactors,
subjectivity being a key dimension in measuring
quality of life. Hence, to make a good questionnaire, we
needed:
Help from patients at all stages of the elaboration of
thequestionnaire to witness, test, validate, and answer.
We needed and still need to look for specialists in quality
oflife measuring, expertise from psychiatrists, psychologists
and sociologists.
Time, it took us 18 months of continuous work;
STAGES
We planned for three stages in the development of our
questionnaire:
53
-
8/6/2019 Hand Book of Evaluation
54/89
Stage I: Conception of the questionnaire
Itemize problems that concern the individual withschizophrenia
and determine the fields of life (item
generation stage),
Create a questionnaire based on the development of the first
stage (revision of items and scale forming stage),
Test and appreciate the new development of the
questionnaire(construction validity test stage).
*Interview with patients at CHCHBM
It was agreed that some provisions for selecting the target
population and define modalities of collection
throughquestionnaires. The proposed project should take into
account:
the patients expectations
that the services done give him satisfactionthat he has access
to his rights
that he is closely associated with the project that concern
him;
While mental health professionals at CHCHBM put emphasis
on the handicap associated with pathology, the patients did
content themselves with more quibbling about on ordinary
dimensions, attached back to normal life; schizophrenics
defined quality of life by health, leisure, joy to live in
family.That probably is the reason why patients suffering from
chronic mental affection see their quality of life as more
correlated with psychosocial factors rather than with
factors
associated with pathology.
Generative items were realised by a panel formed of
psychiatrists, nurses, psychologists, medical social
workers,
54
-
8/6/2019 Hand Book of Evaluation
55/89
and administrative staff of the psychiatry department, from
individual interviews with ten patients of different
clinical
forms of schizophrenia, stabilised, under treatment and still
inhospitalisation at CHCHBM The interview with them was
held with a semi structured questionnaire.
Evaluative criteria rested on the patients cognitive or
emotional judgement, and students conducted the pilot test
at
the time of their end of cycle works. Here, it was a
self-assessment by the respondent.
55
-
8/6/2019 Hand Book of Evaluation
56/89
Definition of categories of evaluative dimensions.
We chose these fields to define the way in which eachrespondent
perceives his own quality of life.
It is:
Health, Psychic symptoms, Self-esteem/well-being, Relation
with family, Social and love relations, leisure/creativity,
participation to community life, Religion, Financial
situation,Living conditions.
1 Health:
Items or scales relating to physical functioning, precise
physical symptoms or the state of health.
Psychiatric symptoms:
Items or scales concerning symptoms associated with a state
of mind or a mental disorder.
3 Financial situation:
Items or scales concerning the respondents welfare
orsituation..
4 Living conditions:
Items or scales concerning the appropriate state or nature
of
the respondents life environment.
5 Family:
Items or scales deliberately aiming at family members and
not
other sources of social support in the respondents life.
6 Social/love relationships:
56
-
8/6/2019 Hand Book of Evaluation
57/89
Items or scales concerning the degree of social support
enjoyed by the respondent, emotionally or materially.
7 Leisure/creativity:
Items or scales concerning the quantity or the nature of the
respondents leisure or creative activities.
8 Participation in community life/productivity:
May be this is the most controversial grouping. These items
or scales concern the quantity, the degree or the nature of
participation in community life or employment activities.
Items were grouped on employment and community
participation because a lot of people suffering from chronic
mental diseases are not in full time employment,
nevertheless,they can devote themselves to other activities that
contribute
to the community good functioning.
9 Religion:Items and scales concerning formal or free practice
of a
religion, a cult, or a type of spirituality.
10 Self-esteem/well-being:
Items or scales concerning the patients emotional,
psychological or subjective state, including comprehensive
self-esteem, a feeling of psychological well-being,
contentment, optimism and the manner of looking at life.
57
-
8/6/2019 Hand Book of Evaluation
58/89
Stage II: Constructing the questionnaire
Setting up a questionnaire based on development of the
firststage (development of items and scale forming stage). This
stage takes place in Harare, ZIMBABWE.
The interviews took into account various factors: clinical
form, acute or chronic episode in hospitalization, as a
walking
case, first episode notion.
* Items
One hundred and sixteen items were chosen; after the first
analysis, we remained with 109 items (first version of the
questionnaire), then 92 at the end of a subsequent sorting
phase.
* Categories
The 92 items were grouped in eleven categories:
Health, Psychic symptoms, Self-esteem/well-being, Relationwith
family, social and love relations, Leisure/creativity,
Participation in community life, Religion, Financial
situation,Living conditions, Autonomy.
* Modalities of answers
Five modalities were retained (33):
Sevendays ago Answers
Questions Never
0
Rarely
1
Sometimes
2
Often
3
Always
4
58
-
8/6/2019 Hand Book of Evaluation
59/89
Stage III: Forming stage of an evaluation scale for the
quality of life of the schizophrenic
Inspired by the W.H.O. presentation (11), we went down
from 81 questions of the previous questionnaire to 44, of
which 4 per field. The 44 items were grouped in eleven
categories or fields of life:
Health, Psychic symptoms, Self-esteem/well-being, Relation
with family, social and love relations, Leisure/creativity,
Participation in community life, Religion, Financial
situation,
Living conditions, Autonomy.
The notion of subjectivity takes all its value when one
questions oneself about autonomy.Without autonomy, it is
impossible to go and work, to
establish stable relations with somebody, to project oneself
into the future. Any healthy person could think that freedom
of action is a positive and indispensable data of life.
59
-
8/6/2019 Hand Book of Evaluation
60/89
FIELDS OF LIFE
Health
Psychic symptoms
Self-esteem/well-being
Relation with family
Social and love relationsLeisure/creativity
Participation in community life
Religion
Financial situation
Living conditions
Autonomy
60
EQLSEVALUATION OF THEQUALITY OF LIFE OF
THE SCHOZOPHRENIC
-
8/6/2019 Hand Book of Evaluation
61/89
CHAPTER VI: EVALUATION OF
THE QUALITY OF LIFE OF THESCHIZOPHRENIC (EQLS)
INTERVIEWER ID N /_____/_____/_____/
DATE: /___/___/_____/
STARTINGTIME:/___/__/__/ PLACE:
/________________/
PARTICIPANT ID N: /_____/_____/_____/____
AGE: /______/
SEX: /_____ ETHNIC GROUP: /___ /
COMMUNE: /___ _/
STABILISATION /______/ REAL-LIFE EXPERIENCE:/______/
We are interested in knowing your quality of life during the
seven last days. Please answer all the rubrics by ticking a
box
for each rubric.
61
-
8/6/2019 Hand Book of Evaluation
62/89
-
8/6/2019 Hand Book of Evaluation
63/89
3. SELF-ESTEEM/WELL-BEING
D3.1 My whole being inspires me confidence.
Never
0
Rarely
1
Sometimes
3
Always
4
D3.2 My authority is respected in familyNever
0
Rarely
1
Someti
mes
3
Always
4
D3.3 I am comfortable in publicNever
0
Rarely
1
Someti
mes
3
Always
4
D3.4 I am satisfied with what I do
Never 0
Rarely1
Sometimes3
Always4
4. RELATION WITH FAMILY
D4.1 I am with my family
Never
0
Rarely
1
Sometimes
3
Always
4
D4.2 And the family listens to me
Never
0
Rarely
1
Sometimes
3
Always
4
Never
0
Rarely
1
Sometimes
3
Always
4
63
-
8/6/2019 Hand Book of Evaluation
64/89
D4.3 In case of difficulties, the family helps me
Never0
Rarely
1
Sometimes3
Always4
D4.4 I love my family members, and I am loved
Never
0
Rarely
1
Sometimes
3
Always
4
5. SOCIAL AND LOVE RELATIONSHIPS
D5.1 I have friends
Never
0
Rarely
1
Sometime
s
3
Always
4
D5.2 Friends visit me
Never0
Rarely
1
Sometimes3
Always4
D5.3 Beside that, I am sexually active
Never
0
Rarely
1
Sometime
s
3
Always
4
D5.4 I am satisfied with this sexual lifeNever
0
Rarely
1
Sometimes
3
Always
4
64
-
8/6/2019 Hand Book of Evaluation
65/89
6.LEISURE / CREATIVITY
D6.1 I visit friendsNever
0
Rarely
1
Sometimes
3
Always
4
D6.2 I do my shopping
Never
0
Rarely
1
Sometimes
3
Always
4
D6.3 In the evening, I like watching TV
Never
0
Rarely
1
Sometimes
3
Always
4
D6.4 At parties, I like dancing
Never
0
Rarely
1
Sometim
es
3
Always
4
7. PARTICIPATION IN COMMUNITY
LIFE/Productivity
D7.1 I attend events in the neighbourhood with friends
Never
0
Rarely
1
Sometim
es
3
Always
4
D7.2 And I like talking with people around me
Never
0
Rarely
1
Sometim
es
3
Always
4
65
-
8/6/2019 Hand Book of Evaluation
66/89
D7.3 I need to get information
Never
0
Rarely
1
Sometim
es3
Always
4
D7.4 I manage to fulfil my projects
Never
0
Rarely
1
Sometim
es
3
Always
4
8. RELIGION
D8.1 I believe in God
Never0
Rarely1
Sometimes
3
Always4
D8.2 I read the Bible, (the Koran), the word of God
Never
0
Rarely
1
Sometim
es
3
Always
4
D8.3 I go to a cult
Never
0
Rarely
1
Sometim
es
3
Always
4
D8.4 Prayer brings something to my life
Never
0
Rarely
1
Sometim
es3
Always
4
66
-
8/6/2019 Hand Book of Evaluation
67/89
9. FINANCIAL SITUATION
D9.1 I can pay for my transportNever
0
Rarely
1
Sometim
es
3
Always
4
D9.2 I buy my medicines aloneNever
0
Rarely
1
Sometim
es
3
Always
4
D9.3 I am capable of feeding myself
Never0
Rarely1
Sometimes
3
Always4
D9.4 I am satisfied with my financial situation
Never
0
Rarely
1
Sometim
es
3
Always
4
67
-
8/6/2019 Hand Book of Evaluation
68/89
10. LIVING CONDITIONS
D10.1 At home I have my own bedNever
0
Rarely
1
Sometim
es
3
Always
4
D10.2 At home, I have waterNever
0
Rarely
1
Sometim
es
3
Always
4
D10.3 In the neighborhood, I get along with my neighbors
Never0
Rarely1
Sometimes
3
Always4
D10.4 I live in a safe place and in security
Never
0
Rarely
1
Sometim
es
3
Always
4
68
-
8/6/2019 Hand Book of Evaluation
69/89
11. AUTONOMY
D11.1 I can live without medicinesNever
0
Rarely
1
Sometim
es
3
Always
4
D11.2 For dressing, I choose my clothes myselfNever
0
Rarely
1
Sometim
es
3
Always
4
D11.3 I can take my transport alone
Never0
Rarely1
Sometimes
3
Always4
D11.4 I am capable of doing a job
Never
0
Rarely
1
Sometim
es
3
Always
4
Thank you for your time
ENDING TIME /__/__/__/
69
-
8/6/2019 Hand Book of Evaluation
70/89
THE SCORE
for an item
for a domain
for a scale
70
SCORINGFORMULA
-
8/6/2019 Hand Book of Evaluation
71/89
CHAPTER VII: SCORING FORMULA
* The score (13)
for an item,
the value goes from 0 (the worse quality of life) to 4 (the
best quality of life) (1):
SCORE
0
1
2
3
4
ANSWERS
Never,
rarely,
sometimes,
often,
always
QUALITY
bad
bad enough
good
enough
goodexcellent
Percentage
(0 %)
(25 %)
(50 %)
(75 %)
(100 %)
For a field:
the sum of scores of items(from 1 to 4) ofD domain X 100
100 (the maximum score of an item) X 4(the number of items /
field)
For a scale:
The average of the sum of % of all D domains of the scale,
That is:
sum of % from D1 to D11
11
71
-
8/6/2019 Hand Book of Evaluation
72/89
AgeSex
Residence in Zambia (Province)
Ethnic groups
Real-life experience and ReportStabilisation and Report
Typical questions
72
Constructing thequestionnaire
-
8/6/2019 Hand Book of Evaluation
73/89
CHAPTER VIII:THE INTERVIEWERS HANDBOOK
I. AGE II. SEX
01. AGE: /--------/-------/ 02. SEX: /------/
01. 1. 15 - 25 02. 1. Male
01. 2. 26 - 36
02. 2. Female
01. 3. 37 - 47
01. 4. 48 - 58
01. 5. > 58
III. RESIDENCE IN ZAMBIA (Province)
03. PROVINCE : /--------/
03.1. Copperbelt
03.2. Central
03.3. Eastern
03.4. Luapula 03.5. Lusaka
03.6. Northern
03.7. North Western
03.8. Southern
03.9. Western
73
-
8/6/2019 Hand Book of Evaluation
74/89
-
8/6/2019 Hand Book of Evaluation
75/89
04.29. Sera
04.30. Soli
04.31. Swaka
04.32. Tonga
04.33. Tabwa
04.34. Totela
04.35. Tumbuka
04.36. Unga
04.37. Ushi
V. LANGUAGES
05.1. Bemba
05.2. Kaonde
05.3. Lozi
05.4. Luchazi-Mbunda
05.5. Lunda 05.6. Luvale
05.7. Luyana
05.8. Mambwe-Lungu
05.9. Mashi
05.10. Nkoya-Mwela
05.11. Nsenga
05.12. Nyanja 05.13 Nyika
05.14. Tonga
05.15.Tumbuka
75
-
8/6/2019 Hand Book of Evaluation
76/89
V. REAL-LIFE EXPERIENCE AND REPORT
REAL-LIFE EXPERIENCE /--------/
Good: > 75 %
Bad: 75 %
Awareness of disease /--------/
1. Yes
2. No
Accepts care /--------/
1. Yes
22. No
Feels he is a man like any other/--------/
1. Yes
2. No
There is still hope of recovering previous
capacities/--------/
1. Yes
2. No
76
-
8/6/2019 Hand Book of Evaluation
77/89
VI. STABILISATION AND REPORT
Stabilization /--------/Good: > 75 %
Bad: 75 %
Contact is good/---------/
1. Yes
2. No
Subdued clinical syndrome/-------/
1. Yes
2. No
Relation with entourage /-------/
1. Yes
2. No
Partial awareness of the state of sickness/-------/
1. Yes
2. No
77
-
8/6/2019 Hand Book of Evaluation
78/89
-
8/6/2019 Hand Book of Evaluation
79/89
* PATIENTS REAL-LIFE EXPERIENCE
Typical questions, report, observationyes = > 75 %
no = 75 %02.1.Awareness of illness (question)
Are you a mental patient?
Do you know the cause ?
Do you accept treatment?
Do you want to heal?
02.2. Accepts care (question)
Do you accept to come for consultation?
Do you accept to take your medicines?
Do you take medicines on your own?
Do you know the names of your medicines
02.3. Feels he is a man like others (question)Have you lost your
honor?
Are you ashamed?
Do you feel rejected?
Do you hide?
02.4. There is still hope of recovering previous capacities
(question)
Do you feel you are capable of working?Can you do your shopping
all alone?
Can you take your bus all alone?
Can you choose your food and clothes?
79
-
8/6/2019 Hand Book of Evaluation
80/89
-The patients consent
-Enlightened free consent
-Precautions to be taken
80
CONDITION OFADMINISTRATION
-
8/6/2019 Hand Book of Evaluation
81/89
CHAPTER IX: CONDITION OF ADMINISTRATION
The type of study chosen (research-action) makes theinvolvement
of field actors to be compulsory. Wherever the
investigation will take place, a preliminary sensitisation
of
health, social, administrative, and political partners must
be
carried out, on the mental illness, taking charge and what
we
intend to do. (3):
* The patients consent
The fact of entering a clinic means that one is agreeable to
the
medical contract and the hospitalisation. However, that is
not
the equivalent to accepting all subsequent medical
decisions.
The patients consent is indispensable before any
importantmedical action. He can refuse a diagnosis method, a
treatment, etc.* The enlightened free consent
In order to be able to approve or refuse a medical action,
thepatient will be accurately informed about the objectives of
the
action, its consequences and the methods to be employed.It is
only thanks to this information that the patient will be
able to give you his consent in full knowledge of the facts.
*Precautions to be taken
1. CREATE AN ATMOSPHERE OF TRUST
Reserve a warm, spontaneous, sincere welcome in which
youravailability to answer questions will be appreciated.
Remain
calm, avoid reactions based on fear or stereotypes, treat
the
person as a adult.
In order for the contacts to be more personal, give the
hand,
introduce yourself, ask the name, etc.
81
-
8/6/2019 Hand Book of Evaluation
82/89
-
8/6/2019 Hand Book of Evaluation
83/89
83
-
8/6/2019 Hand Book of Evaluation
84/89
84
REFERENCES
-
8/6/2019 Hand Book of Evaluation
85/89
REFERENCES
1. Auquier and coll.. Schizophrenia Quality ofLife (S-QoL),
2002.
2. Auricourt, Christian - Une mdecine de la
personne. - Espace thique, la lettre, 9-10. Dossier
spcial : Qualit de vie l'hpital et quipes
soignantes 1998.3. Auriol B.. Marginalit du malade mentale.
Rencontre, Cahiers du travailleurs Social, revue
du MCPS VIII, Automne 1979, N 31, pp. 51
59.
4. Baker, F. et Intagliata, J. Quality of life in the
evaluation of community support systems.Evaluation and Program
Planning, 5, 69-79.
1982.
5. Barry, M. M., Crosby, C. et Bogg, J..
Methodological issues in evaluating the qualityof life of
long-stay psychiatric patients. Journal
of Mental Health, 2, 43-56. 19936. Bech, P. Quality of life
measurement in chronic
disorders. Psychotherapy & Psychosomatics, 59,
1-10. 1993.
7. Blondeau, Dominique. - La qualit de vie. -
Ethique, 5, 83-97. 1992
8. Cella DF. Pain J.. Quality of life : concepts anddefinition.
Symptom Manage, 9 ; 186-192. 1989.
9. Cronbach LJ. Coefficient alpha and the internal
structure of tests, 16 : 297-334. Psychometrika
1951.
10. Crosby, C..Mental health research programs.
Health Services Research Unit (HSRU)
85
-
8/6/2019 Hand Book of Evaluation
86/89
University College of North Wales: Evaluation
of the strategy for mental illness services in
North Wales. Journal of Mental Health, 2, 85-88.1993
11. Fava, G. A.. Methodological and conceptual
issues in research on quality of life.
Psychotherapy & Psychosomatics, 54, 70-76.
1990.12. Gill TM, Feinstein AR. A critical appraisal of
the quality of life measurements, 272 : 619-
626. JAMA 1994.
13. Greg W, Diane W, Jenkinson C et coll. : The
Schizophrenia Quality of Life Scale. User
Manuel for the SQLS. SQLS Outcomes, Oxford1999.
14. Grard. - La qualit de vie et le discours des
malades. - 6me congrs national de la SFAP,
Lyon, 1998, 9 p.15. Hamon A. et Mesbah M. Fiabilit des
questionnaires dans le cadre du modle deRasch. XXXI mes Journes
de Statistique de
Grenoble, 5th Annual Conference of the
Internationnal Society for Quality of Life
Research, Baltimore. 1999.
16. Hirsch, Emmanuel. - Qualit de vie, qualit
d'une vie. - Espace thique, la lettre,. Dossierspcial : Qualit
de vie l'hpital et quipes
soignantes. 1998, 3-5.
17. Jasmin, Claude. - Longvit et qualit de vie :
dfis et enjeux. - Le Plessis Robinson :
Synthelabo, 1999.
86
-
8/6/2019 Hand Book of Evaluation
87/89
18. Jasnoski, M. B. The physical environment
affects quality of life based upon environmental
sensitivity. Journal of Applied DevelopmentalPsychology, 13,
139-142. 1992.
19. Jones, S. H., Thornicroft, G., Coffey, M. et
Dunn, G.. A brief mental health outcome scale:
Reliability and validity of the Global Assessment
of Functioning (GAF). British Journal ofPsychiatry, 166,
654-659. 1995.
20. Kring, A. M., Kerr, S. L., Smith, D. A. et
Neale, J. M.. Flat affect in schizophrenia does
not reflect diminished subjective experience of
emotion. Journal of Abnormal Psychology, 4,
507-517. 1993.21. Lehman A, Ward N, Linn L., Chronic mental
patients : the quality of life issue. Am J of
Psychiatry, 139 : 1271- 6. 1982.
22. Lehman A. The well-being of chronic mentalpatients assessing
their quality of life. Arch Gen
Psychiatry, 40369-738. 1983.23. Mac Gilp, D.. A quality of life
study of
discharged long-term psychiatric patients.
Journal of Advanced Nursing, 16, 1206-
1215.1991.
24. Mc Dowell, I. et Newell, C.. Measuring Health:
A Guide to Rating Scales and Questionnaires.New York: Oxford
University Press. 1987.
25. Mc Grath, J.. Quality of life: What is it? Why
use it ? Vocational and Rehabilitation Research
Institute (VRRI, Calgary, Alberta) Research
Document #409. 1992.
87
-
8/6/2019 Hand Book of Evaluation
88/89
26. Mc Sweeny, A. J. et Creer, T. L.. Health-
related quality-of-life assessment in medical
care. DM, January, 10-71. 1995.27. Peruselli Carlo. - Evaluating
a home palliative
care service : development of indicators for a
continuous quality improvment program. -
Journal of palliative care, 13, 3, 34-42. 1997.
28. RIOU, Sylvie. - Qualit de vie en mdecine :une nouvelle
exigence. - Impact mdecin hebdo,
305, 6-15. 1996.
29. Slaughter, J. G., Lehman, A. F. et Myers, C.
P.. Quality of life of severely mentally ill adults
in residential care facilities. Adult Residential
Care Journal, 5, 97-111. 1991.30. Thomas, G. M. et Feinstein, A.
R.. A critical
appraisal of the quality of life measurements.
Journal of the American Medical Association,
272, 619-626. 1994.31. Tierney, R.M. - Relationships between
relief
quality of life and satisfaction with hospice care.- Palliative
medicine, 5, 333-345. 1998.
32. Vansina, D: Introduction lthnographie du
Congo- ditions universitaires du Congo
C.R.I.S.P., 35 rue du Congs Bruxelles, 260 p.
33. Ware, J.E. fils. Standards for validating health
measures: Definition and content. Journal ofChronic Disease, 40
(6), 473-480. 1987.
34. Wilkinson et all. Uw kwaliteit van leven.
Vertaling SOLS, 2000.
88
-
8/6/2019 Hand Book of Evaluation
89/89
89