Embed Size (px)
Citation preview

Hand and leg dominance: Do they really affect limb muscle strength?
Joseph A. Balogun and Ayodele T. Onigbinde
The aim of this study was to compare the strength of selected muscle groups in 32 right- and 32 left-limb dominant subjects. Using standard procedures, we measured the isometric strength of hand grip, elbow flexion, knee extension and knee flexion. Each subject's hand grip strength ratio (GSR) was calculated. T h e results revealed that our right- and left-limb dominant subjects were comparable in age, weight, height and body adiposity. However, the left-limb dominant subjects exhibited stronger left-hand grip and left knee extensor strength than their right-limb dominant counterparts. Similarly, the right-limb dominant subjects exhibited greater right elbow flexor muscle strength than their left-limb dominant counterparts. The GSR for the right- and left-limb dominant subjects was similar. We recommend that separate grip strength, knee extensor and elbow flexor norms be established for right- and left-limb dominant subjects.
~~ ~~
I NTRO D U CTI 0 N
The human cortex is divided into left and right cerebral hemispheres; however, these hemi- spheres are not exact mirror images of one another. One of the hemispheres exerts domin- ance over the other, and the dominant cerebrum is concerned mainly with verbal, linguistic, arith- metic, calculative and analytical functions, whereas the other is concerned with non-verbal, geometric, spatial, visual, pattern, musical and synthetic functions (Chusid, 1979). Further- more, cerebral dominance manifests itself in hand (handedness) and leg dominance (legged- ness). Thus, right-handed individuals are left
J. A. Balogun, A. 1. Onigbinde, Department of Medical Rehabilitation, Faculty of Health Sciences, Obafemi Awolowo University, Ile-lfe, Oyo State, Nigeria (Reptint requests to JAB, School of Physical Therapy. Texas Woman's University. Houston, Texas 77030, USA) Accepted for publication September 1991
hemisphere dominant, whereas 1efi.-handed indi- viduals are right hemisphere dominant (Daube, Sandok, Reagan and Westmorelarid, 1978).
Handedness is the preferential use of one hand over the other for everyday activities; leg- gedness is the preferential use of one leg over the other (Kellor et al, 1971). The dominance ofone limb over the other is acquired ;is a result of developmental sequence and adaptation (Gesch- wind and Galaburda, 1985). About 90% of adults exhibit more strength and dexterity with their right hand than with their left, and such handedness is commonly associated with ipsila- teral leggedness (Daube et al, 1978). In medical rehabilitation, it is common practice to employ the same normative data (e.g. grip strength) for both left- and right-limb dominant subjects (Kellor et al, 1971; Mathiowetz et al, 1985; Mathiowetz, Wiemer and Federman, 1986). To validate this practice, we believe i t i:i necessary to design a prospective study to compare the muscle strength of right- and left-limb dominant sub- jects.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.

90 PHYSIOTHERAPY THEORY AND PRACTICE
There have been few studies that have com- pared the muscular strength of right- and left- limb. dominant subjects, and their findings have often been contradictory. Some studies have not reported any significant difference in the grip strength of right- and left-hand dominant sub- jects (Ager, Olivett and Johnston, 1984; Full- wood, 1986; Matthiowetz et al, 1985, 1986), whereas others (Schmidt and Toews, 1970; Bur- meister, Flat and Weiss, 1974; Nwuga, 1983) have found that most left-hand dominant sub- jects are stronger in both hands than their right- hand dominant counterparts. A major research design shortcoming with the above studies was the wide disparity in the number of left- and right-hand dominant subjects employed. Simi- larly, i t is not stated whether the right- and left- hand dominant subjects were matched for other relevant variables (e.g. age, height, weight) which are known to affect grip strength (Balo- gun, Akinloye and Adenlola, 1991 b).
Leggedness is known to play an important role in the pattern of human gait (Gunderson et al, 1989). Many studies have reported differences in kinematic and electromyographic functions between the dominant and non-dominant limbs during ambulation (Hannah, Morrison and Chapman, 1984; Arsenault, Winter and Eng, 1986). In the same vein, some studies which have compared the musclestrength of the lower extre- mities have found significant differences between the strength of the dominant and non-dominant lower-extremity muscles (Goslin and Charteris, 1979; Miyashita and Kaneshisa, 1979; Wyatt and Edwards, 1981). In contrast, other studies have not reported any significant differences between the strength of the dominant and non- dominant limbs (Gillian, Sady and Freedson, 1979; Costain and Williams, 1984; Holmes and Alderink, 1984; Onuoha, 1990). The influence of leg dominance on the strength of the muscles of the lower extremities remains relatively unex- plored.
It is nav generally recognised that absolute muscle strength is not the critical factor in assess- ing the performance and integrity of a limb. For example, the ratio of the grip strength of the dominant to the non-dominant hand is con- sidered the key to an accurate evaluation of grip
strength .and grip loss (Toews, 1964; Patterson, 1965; Schmidt and Toews, 1970; Lunde, Brewer and Garcia, 1971). The ratio varies only slightly with age and sex and it is a useful parameter in the evaluation of patients with upper-extremity disabilities (Thorngren and Werner, 1979). To the best of our knowledge, there have been no studies that have compared the dominant:non- dominant hand grip strength ratio of right- and left-limb dominant subjects. Therefore, the aims of this study were to compare:
1. The isometric strength of hand grip, elbow flexion, knee extension and knee flexion of right- and left-limb dominant subjects.
2. The , dominant:non-dominant hand grip strength ratio of right- and left-limb domin- ant subjects.
METHOD
Subjects
Altogether, 64 healthy male undergraduate stu- dents at Obafemi Awolowo University were re- cruited for the study. The mean ( f SD) physical characteristics of the subjects were as follows: age 22.8f 2.2 years (range 18-28 years), height I 7 4 f 7 cm (range 142-188 cm), weight 63 f 5 kg (range 54-74 kg). Some of the subjects were involved in recreational activities, but not one of them was an elite athlete. All of the subjects gave informed consent prior to testing. The subjects were split into left- and right-limb dominant groups based on preference during daily activi- ties. Limb dominance was ascertained after a brief interview, in which the following questions were asked: Which hand/leg would you preferen- tially use for (1) writing, (2) eating, (3) sweep- ing, (4) cutting grass, (5) throwing a ball, (6) holding a tennis racket, (7) opening or closing doors and window shutters, and (8) kicking a ball while playing soccer? If a subject favoured one hand over the other when replying to questions 1-7, then that hand was considered dominant. The response to question 8 dictated which leg was dominant. We found those subjects who were right-hand dominant to be also right-leg
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.

PHYSIOTHERAPY THEORY AND PRACTICE 91
T8bh 1 Tho mean (tSD) physic81 characteristics of the subjocts ( ~ 6 4 )
Variable Right-limb dominant Left-limb dominant
( ~ 3 2 ) (n=32) t P
23.2i2.2 175i6 62*4 20il
22.3t2.2 1.51 0.136 174i8 0.67 0.505 63*5 -0.79 0.453 21 12 -1.46 0.149
dominant; similarly, those subjects who were left-hand dominant were also left-leg dominant. None of the subjects was ambidextrous.
Of the 64 subjects, 32 were left-limb domin- ant and 32 were right-limb dominant. The two groups were matched (PcO.05) for age, height, weight and body adiposity (Table 1). Those subjects with a previous history of injury to the upper or lower extremities were excluded.
Research design
A purposive sampling technique (Polit and Hungler, 1978) was employed in this study. Because of the low percentage (3%) of left-limb dominant subjects in the Nigerian population (Balogun, Adenlola and Akinloye, 1991c), we contacted known left-limb dominant subjects in our university community and sought their con- Sent to participate in the study. In addition, we recruited right-limb dominant subjects of com- parable age and anthropometric parameters from the same community.
Procedure
The age of each subject was recorded and his weight and height measured on a stadiometer (Seca, Prazision frr die Gesindheit, Germany). Subsequently, we measured the isometric strength of hand grip, elbow flexion, knee exten- sion and knee flexion of both extremities using standardised procedures. For each measurement, two trials were carried out, the highest reading being used in the data analysis. The subjects were
wight adjusted for height and is an objecthe measure of
verbally motivated during the test and were provided with the isometric forces for the mus- cles being tested at the end of each trial. Ad- equate intervals of rest were allowed between measurements, and all measurements were undertaken for each subject within a week. The different muscle strength measurements were taken in random order and all of the measure- ments were taken by the same researcher (ATO) to control for inter-researcher variability.
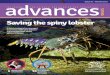
The grip strength of each subject was measured using a hand grip dynamometer (Takei Kiki Kogyo, Japan) following the proto- col described by Balogun and Onigbinde (1991). Prior to each measurement, the subjects assumed the erect position with the shoulder joint adducted and neutrally rotated, and the elbow and wrist joints fully extended (Fig. 1). They were instructed to exert their maximal effort and the dynamometer was properly adjusted to en- able the subjects to maintain a firm grip. Subse- quently, the subjects were cued to pull the handle of the dynamometer as hard as possible and to hold it in place for about Ssec. We have pre- viously investigated the psychometric properties of the hand dynamometer employed in this study, and found the measurements to be both reliable (rz0.91; P<O.OI) and valid ( ~ 0 . 9 7 ; P<O.O01) when the output of the dynamometer was compared to standard weights (Balogun and Onigbinde, 1991).
We measured the elbow flexor isometric force using a cable tensiometer. While in a sitting position, each subject’s elbow joint was fully extended and the forearm supinated. The limb being tested was placed on a table positioned in front of the subject. The distal end of the cable
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.

92 PHYSIOTHERAPY THEORY AND PRACTICE
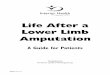
tensiometer was anchored to a wooden bar dir- ectly facing the subject. The fully extended arm gripped the proximal end of the cable tensi- ometer (Fig. 2). During each measurement, the subject was instructed to bend the elbow joint by pulling the proximal end of the cable tensi- ometer.
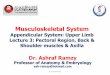
The knee extensor isometric force was measured with a cable tensiometer while sitting on a testing table with a backrest, following the procedures described by Richard and Currier (1977). The subject’s hip was maintained at 120” extension and the knee positioned in 60” flexion. An ankle cuff was affixed and attached to the cable tensiometer (Fig. 3). The other end of the tensiometer was anchored to the base of the testing table. The peak isometric force (kgQ was recorded when the subject was instructed to ‘pull’ during knee extension.
To measure the knee flexor isometric force, the subject lay in the prone position with his legs
slightly projecting beyond the edge of the testing table (Fig. 4). A cuff was attached just proximal to the ankle joint and hooked to the cable tensiometer, the base of which was affixed to the testing table. Compensatory movement was pre- vented during measurement by stabilising the subject’s hip joints. The maximal isometric force (kgf) was recorded as the subject bent his knee in response to the command ‘pull’.
In a recent study, Balogun, Adesinasi and Marzouk (submitted) found the readings of the cable tensiometer used in the present study to be highly reproducible (r=0.90) and valid (s=O.999) when calibrated against known weights.
Following data collection, the grip strength ratio (GSR) was calculated for each subject using:
dominant hand grip force (kgf) GSR= non-dominant hand grip force (kgf)
Statistical analysis
Using paired t-test inferential statistics, we deter- mined significant differences in the dependent variables between right- and left-limb dominant subjects. The level of significance was set at P < 0.05. We determined the percentage of the subjects with GSR values ( 1 ) less than 1.0, (2) equal to 1.0 and (3) greater than 1.0. The statistical analyses were performed on an IBM 370 computer with the aid of the Statistical Package for Social Scientists (SPSS).
RESULTS
The results of the paired t-test used to evaluate differences in the strength of the various muscle groups revealed that the left-limb dominant subjects exhibited a stronger left-hand grip (P<O.OOI) and stronger left knee extensors ( P < 0.05) than their right-limb dominant coun- terparts. However, the right-limb dominant sub- jects exhibited stronger right elbow flexor muscle
Fig. 1 Measurement of hand grip strength with the strength (p<0.05) than the left-limb dominant Takei Kiki Kogyo dynamometer. subjects (Table 2).
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.

PHYSIOTHERAPY THEORY AND PRACTICE 93
Fig. 2 Measurement of elbow flexor isometric strength with a cable tensiometer.
Fig. 3 Measurement of knee extensor isometric strength with a cable tensiometer.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.

94 PHYSIOTHERAPY THEORY AND PRACTICE
The grip strength ratio for the right- and left- limb dominant subjects was not statistically signi- ficant. The percentage distribution of the GSR was similar for both groups. The majority (> 80%) of both the right- and left-limb domin- ant subjects had a GSR greater than 1.0, with only a few subjects having a GSR less than 1.0 (Table 3).
D I SCUSSIO N
One of the primary objectives of this study was to compare absolute muscular strength with han- dedness and leggedness. Both groups of subjects - right- and left-hand dominant - were compar- able for age and anthropometric indices (Table 1) . Thus, any significant differences in the iso- metric muscle strength of the two groups cannot be attributed to variation in these factors. We
Fig. 4 Measurement of knee flexor isometric strength with a cable tensiometer.
did find significant differences in the isometric hand grip, knee extensor and elbow flexor strength of the two groups. Our findings suggest that the usual practice of employing the same normative data for right- and left-limb dominant subjects when making clinical decisions (Gillian et al, 1979; Goslin and Charteris, 1979; Holmes and Alderink, 1974; Kellor et al, 1971; Mathiowetz et al, 1989) can be misleading. Based on our find- ings, we recommend that separate grip strength, knee extensor and elbow flexor norms be estab- lished for right- and left-limb dominant subjects. In agreement with the findings of other related studies (Bechtol, 1954; Schmidt and Toews, 1970; Thorngren and Werner, 1979), the majority of our subjects ( > 80%) exhibited greater grip strength in their dominant hand when compared to their non-dominant hand. This suggests that the practice in medical rehabilitation whereby physical therapists compare the grip strength of the limb of interest with the contralateral limb as a criterion reference is unjustified.
A second concern of this study was to compare the grip strength ratio of right- and left-limb dominant subjects. We found no significant dif- ferences in the GSR of the two groups. A GSR of 1 .O indicates that the grip strength of both hands is equal; a GSR of less than 1 .O indicates that the non-dominant hand is stronger than the domin- ant hand; finally, a GSR greater than 1.0 indi- cates that the dominant hand is stronger than the non-dominant hand. The mean GSR value obtained in the present study of male university students (1.1 1 f 0.13) is comparable to that reported by Lunde et a1 in 1972 for female universitystudents (1.14f0.19). Our mean GSR value was, however, slightly higher than the 1.030 f 0.054 reported by Schmidt and Toews (1970) for male factory workers aged 18-62 years, and the 1.07 f 0.1 1 reported by Thorngren and Werner (1979) for both men and women aged 21-65 years.
The above findings suggest that GSR is affec- ted by the ageing process. It is, however, known that the GSR remains fairly constant when repeated measures are taken within an interval of some weeks (Thorngren and Werner, 1979). Thus, the GSR is a useful and reliable means of evaluating grip strength.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.

PHYSIOTHERAPY THEORY AND PRACTICE 95
Table 2 Comparison of the mean (*SO) muscle strength indices for the subjects (n=6/)
VariaMe
Right-limb dominant ( n= 32)
Left-limb dominant (n-32) t
Right-hend grip force (kgf) Left-hand grip force (kgf) Right dbow flexor force (kgf) Left elbow flexor force (kgf) Right knee ( U t O B m force (kgf) Left knee extensol force (kgf) Right knee flexor force (kgf) Left knee fleuror force (kgf) Grip strength ratio (GSR)'
48.5i7.6
28.7i6.5 26.7 * 6.0 56.8t7.2 52.7 18.1 30.3i5.7 2 8 . 3 6 9 1.1 2i0.15
43.8i7.8 46.4 t 6.8 50.3t6.3 25.5t4.8 28.2t4.8 54.5t5.0 59.3t4.3 28.1 t4.3 31.0t5.6 1.09*0.10
1.18 -3.66
2.25 -1.10
1.23 -2.22
1.76 -1.87
0.99
P
0.243 0.001 0.028 0.275 0.224 0.030 0.084 0.067 0.325
'GSR fa both groupr-1.11 tO.13.
Table 3 Distribution of the grip strength ratio (OSR) bv categories
Right-hand dominant Left-hand dominant Both groups combined ( ~ 3 2 ) (n- 32) (n=W
Muscle strength index Freq. % Freq. % Fm. %
~ ~ ~~~
Grater than 1 .O 26 81.3 28 87.5 54 84.4 Eqwk 1 .O 4 12.6 4 12.5 8 12.5 Less than 1.0 2 6.2 0 0.0 2 3.1
References
Ager CL, Olivett BL, Johnston CL 1984 Grasp and pinch strength in children 5 to 12 years old. American Journal of Occupational Therapy 38: 107- 1 I3
EMG profile in human locomotion. American Journal of Physical Medicine 6 5 1-16
Balogun JA, Metid CO, Manouk DK (submitted) The efkcts of wobble board exercise training program on static balance performance and strength of lower a m i t y murla . Physiotherapy Canada
Balogun JA, Oaigbinde TA 1991 Intratater reliability and validity of the Takei Kiki Kosyo hand grip dynamometer. Journal of Physical Therapy Science 3 5 5 4 0
strength: Effects of tating posture and elbow position. Archives of physical Medicine and Rehabilitation 7 2 280-283
strength as a function ofage, height, body weight and Quetelet index. Physiotherapy Theory and Practice 7: 111-119
Balogun JA, Adenlola SA, Akinloye AA 1991c Grip strength normative data for the Harpenden dynamometer. Journal of Orthopaedic and Sports Physical Therapy I 4 155-160
k h t o l CO 1954 Grip tat: The use of a dynamometer with adjustable handle spacings. Journal of Bone and Joint Surgery 36A: 820-824
Anenault AB, Winter DA, Eng P 1986 Bilateralkm of
Balogun JA, Akomolafe CT, Amusa LO 1991a Grip
Balogun JA, Akinloye AA, Adenlola SA 1991 b Grip
Burmeister LE, Flat AE, Weiss MW 1974 Site and strength development of the hand in elementary school children. Iowa State Service for Crippled Children, Iowa City, Iowa
Chusid JG 1979 Correlative neuroanatomy and functional neurology, 17th edn, pp9-10. Lange Medical Publications, Los Altos, Calif.
Costain R, Williams A K 1984 Isokinetic qiradriceps and hamstring toque lev& of adolescent female soccer players. Journal of Orthopaedic and Sports Physical Therapy 5: 198-200
Dauk JR, Sandok RA. Reagan TJ. Westmoreland BF 1978 Medical neuroscience, pp379-382. Little Brown, Boston, Mass.
Fullwood D 1986 Australian norms for hand and finger strength of boys and girls aged 5-1 2 years. Australian Occupational Therapy Journal 33: 26-36
Gachwind N, Galaburda MD 1985 Cerebral lateraliration: Biological mechanism. m i a t i o n and pathology. A hypothesis and a programme for research. Archives of Neurology 42: 428-455
Gillian T, Sady S. Freedson P 1979 Isokinetic torque lev& for high school football playen. Archives of Physical Medicine and Rehabilitation 60: 110-1 14
Gorlin BR, Chaneris J 1979 Isokinetic dynamomeq: Normative data for clinical use in lower extremity (knee) cases. Scandinavian Journal of Rehabilitation Medicine I I : 105-109
Gundemon LA, Valle DR, Barr AE, Danoff JV, Stanlage SJ, Mackler LS 1989 Bilateral analysis of the knee and ankle during gait: An examination of the relationship
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.

96 PHYSIOTHERAPY THEORY AND PRACTICE
between lateral dominance and symmetry. Physical Therapy 69: 6-50
Hannah RE, Morrison JB, Chapman AE 1984 Kinetic symmetry of the lower limbs. Archives of Physical Medicine and Rehabilitation 65: 155-158
characteristics of the quadriceps femoris and hamstring muscles in high school students. Physical Therapy 64: 914-918
Kellor M, Frost J, Silberberg N, Iversen I, Cummings R 1971 Hand strength and dexterity. American Journal of Occupational Therapy 25: 77-83
Lunde KB, Brewer WD, Garcia PA 1972 Grip strength of college women. Archives of Physical Medicine and Rehabilitation 53: 491493
Mathiowetz V, Kashman N, Volland G, Weber K, Dowe M, Roger S 1985 Grip and pinch strength: Normative data for children. Archives of Physical Medicine and Rehabilitation 66: 69-72
pinch norms for 6-19 year olds. American Journal of Occupational Therapy 40: 705-71 1
Miyashita M, Kaneshisa H 1979 Dynamic peak torque related to age, sex and experience. Research Quarterly in Exercise and Sport 50: 249-255
Holmes JR, Alderink G 1984 Isokinetic strength
Mathiowetz V, Wiemer DM, Federman SM 1986 Grip and
Nwuga GO 1983 A study of the relationship between grip strength and manual dexterity in central nervous system intact adults. Journal of the Nigerian Society of Physiotherapy 8: 30-32
Onuoha ARA 1990 Comparison of quadriceps and hamstring functions in college-age students. Physiotherapy 76: 172-1 76
preplacement evaluation. Industrial Medical Surgery 34: 555-557
Polit D, Hungler B 1978 Nursing research: Principles and methods. WB Lippincott, Philadelphia, Penn.
Richard G, Currier DP 1977 Back stabilization during knee strengthening exercise. Physical Therapy 57: 1013-1015
Schmidt RJ, Toews JV 1970 Grip strength as measured by the Jamar dynamometer. Archives of Physical Medicine
' and Rehabilitation 57: 321-327 Thorngren KG, Werner C O 1979 Normal grip strength.
Acta Orthopaedica Scandinavica 50: 255-259 Toews JV 1964 A grip strength study among steel workers.
Archives of Physical Medicine and Rehabilitation 45: 413417
Wyatt MP, Edwards AM 1981 Comparison ofquadriceps and hamstring torque values during isokinetic exercise. Journal of Orthopaedic and Sports Physical Therapy 3: 48-56
Patterson H M 1965 Grip measurement as a part of the
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y Y
ork
Uni
vers
ity L
ibra
ries
on
11/0
6/14
For
pers
onal
use
onl
y.