Embed Size (px)
Citation preview

HAMILTON NIAGARA HALDIMAND BRANT LOCAL HEALTH INTEGRATION NETWORK
CLINICAL SERVICES PLANNING PROJECT
PLANNING ADVISORY GROUP MEETING GUIDE
ONCOLOGY
1. June, 2009

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
1. Complete Template #1. Describe the strengths and challenges within the existing health care system in addressing population health care needs for the PAG’s patient/client population. Primers for discussion: ‘Summary of Community Values and Preferences’ (Appendix A), ‘Criteria for PAG Service Delivery Models’ (Appendix B) and ‘Guiding Principles for PAG Service Delivery Models’ (Appendix C).
Template #1: Strengths and Challenges within the Current System in Addressing Population Needs PAG Name
PAG Facilitator
Strengths Challenges Ontario Cancer Plan - 3 Year Plan refreshed annually 14 Regional Cancer Plans are aligned with the provincial goals and deliverables
and are monitored provincially by CCO and regionally by the Regional Cancer Program
In HNHB, Regional Cancer Program Priorities & Planning Committee has representatives from key organizations across the LHIN providing cancer services. RCP RVP Chair with Director Accountability
Cancer System Quality Index – produced annually in April by the Quality Council. Set of 39 indicators that are used in planning services provincially and regionally. Indicators cover continuum of care from prevention through to palliative care
Quarterly reporting system to CCO for wait times and quality indicators Commitment to a Regional Cancer Program vision statement that was developed in
2003: “Equal access to a coordinated system of high quality cancer services across the continuum of care, from prevention and early detection through to palliative care, across the region”
Regional Medical and Administrative Leads identified for Systemic, Radiation, Surgery and Palliative Care Program. Memorandum of Understanding among CCO, HHS/JCC and NHS for integration and planning of cancer services for the development of the Walker Family Cancer Centre (WFCC) (2013)
Integrated Cancer Planning Steering Committee to oversee development of cancer services in Niagara in collaboration with the JCC
Regional Cancer Program accredited by CCHSA in 2004 & 2008 (areas of strength across the LHIN for cancer services from prevention, screening, diagnostics,
Increasing age of the population and corresponding increase in demand for services (largest population of seniors aged 65+ for all LHINs)
risk factors associated with cancer are high within the LHIN (e.g. Smoking rates, consumption of fruit and vegetables, physical activity, obesity rates)
LHIN has higher proportion of population with less than high school education compared to Ontario – a key determinant of health. One in five live in poverty
Reaching the large Aboriginal population – both on and off the reserve - for prevention, screening and care as survival data is worse across all DSTs even after accounting for age and treatment differences
Limited funding to address cancer prevention Uptake to cancer screening programs
o OBSP – overall 64% eligible population screened, but still _% of screening takes place outside of the organized screening program
o Cervical – plateaued at 72% eligible population screened, no population based recruitment strategy, no coordination with Public Health/schools/primary care regarding Gardasil eligible women
o Colorectal 22% eligible population screened – rolling out FOBT for average risk and colonoscopy for high risk – reduced CCO funding for incremental volumes
Screening being conducted both inside/outside organized screening o Uncertainty with quality indicators outside organized screening programs o CCO funds hospitals that meet criteria for colonoscopy (not IHFs)
Impact of digital mammography for breast screening sites (women may choose not to go to a facility with film screen mammography)
FINAL 2 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
treatment, palliative care, & survivorship across the LHIN Rationalization of services of high acuity (30, 40) to sites with expertise and capacity
o Integrated Model for JCC & WFCC for systemic & radiation therapy with complex cases to JCC (see model page)
o Surgical oncology services (see model page) o Adolescent & young adult oncology o Pediatric oncology o Rare tumours requiring combined modality therapy o Palliative care shared care team regional model with 3 levels of care (see
model page) Development of the Department of Oncology, McMaster University Strong academic and research mission Training and research will be at 2 sites (St. Catharines & Hamilton) for physicians
and nurses Medical Physics and Radiation Therapists will continue to have their training in the
short term in Hamilton through McMaster University and Mohawk College Strong clinical, Health Services and Knowledge Translation Research Groups Enhancing interdisciplinary activity for shared learning, management of clinical
cases, and knowledge and skills through: o 11 multidisciplinary disease site teams with regional, clinical and academic
mandate o Implementation of multidisciplinary case conferencing (MCC) by Disease Site
Team (DST) across LHIN (institutional and regional) o Educational opportunities through shared regional rounds, disease site specific
workshops, training programs for undergraduates and post graduate specialties, including Medical & Radiation Oncology and Palliative Care
o Telementoring to improve surgical skills and introduce new techniques/technologies (e.g. laparoscopic colectomy)
Commitment from University and Hospital to build a Cancer Research Institute Development of a Functional Program for a new Research Tower Hamilton is the home of evidence-based medicine which influences the approach
to Clinical Practice Development of a LHIN wide IM/IT strategy and Regional Cancer Informatics
Strategy o Dedicated Cancer Informatics Unit o Regional Cancer Program Informatics Plan – implementation of computerized
Early detection and timely diagnosis of lung cancer Shortage of health care providers across the cancer system (e.g. family physicians,
GPOs, palliative care physicians, pharmacists, medical oncologists, mammo technologists, physicists etc.)
Need for interprofessional expertise across the system to build capacity for cancer care services (i.e., importance of access to pharmacists for unfunded drugs, social work, dieticians, etc) across community clinics
Ability to garner additional APP positions based on workload data (e.g. medical oncologist positions through ONTMOA, palliative care physicians through new APP with the Division of Palliative Care, Department of Family Medicine)
Lack of funding models (incremental + base) to support care close to home Lack of educational resources to support standardized education (e.g. chemo
nursing certification & recertification), policies & procedures Lack of funding models to support resource intensive cancer surgery Drug Funding – funded and unfunded drugs. JCC has small budget to pay for
unfunded drugs that meet established criteria. Community Oncology clinics do not have budgets for unfunded drugs creating an access issue
Role for more navigational models (e.g. McMillan Nursing Model in UK , APN Palliative Care role) to coordinate and integrate care across continuum
Access to care – creating a truly integrated cancer program with JCC and WFCC with funding models for cancer centres and community oncology clinics to deliver care close to home. Challenge in rural communities where physical proximity to services is a barrier (e.g. examples of variation in referral rates as well as decreased utilization (e.g. prostate radiation) across the LHIN
Generally low utilization rates for radiation treatment across the LHIN compared to expected rates
Acute care facilities are having difficulty with patient flow and access to care due to long waits for non-acute care (ALC), resulting in long ED wait times, cancelled scheduled surgical care and high costs due to high inpatient census and the associated staffing
Wait times that do not yet meet targets – surgery (specific issues related to GU and Prostate), radiation and systemic therapy
Access to family physicians all areas designated under-serviced – critical for referral into the cancer system and especially for palliative patients
Understanding the role of the family physician in cancer services and supporting family physician’s needs (e.g., lack of tools including web-based tools to guide
FINAL 3 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
physician order entry (CPOE) across all systemic therapy sites. System that enables primary care providers to access information on optimal diagnostic work-up, referral mechanisms, appropriate follow-up care including supportive/palliative care; supports movement of patients, treatment plans (systemic and radiation) between 2 cancer centres and community oncology clinics, palliative care shared care teams, Community Care Access Centres (CCAC) etc.
Strong collaborative partnerships across the LHIN (e.g. Community Oncology Program developed in St. Catharines in 1981 , development of the OBSP began in Hamilton in the late 80’s)
Strong partnerships with family physicians, radiologists, surgeons and pathologists across LHIN with the OBSP for breast screening and assessment (13 screening sites and 6 assessment sites plus 2 in progress) Most screening sites linked to rapid diagnostic assessment clinics
Building on the family physician partnerships to implement the letter of invitation recruitment strategy for the ColonCancerCheck Program
Higher proportion of rostered (FHTs) Family Physicians in LHIN than elsewhere in Ontario. These practices support cancer screening strategies
Successful implementation of Advanced Practice Models to increase capacity for cancer care services (e.g. APNs - Research Centre of Excellence (JCC, McMaster, CCO, Amgen partnership). APT (Can Well Initiative with YMCA), AMRT, Nurse Endoscopy Pilot Project for Flexi-Sigmoidoscopy)
Nurse Navigator Model in OBSP to link screening to diagnostic assessment and treatment
Aboriginal Navigator role to increase access to cancer services (especially cancer screening), support navigation across the cancer system and improve outcomes (survival)
Cancer Surgery Network established in 2006. Surgical Oncology Leaders receiving stipends to advance CCO quality agenda
Established Communities of Practice (CoP) focused on the quality of cancer surgery for Breast and Colorectal patients. The CoP model is expanding to Urologists in the LHIN to improve GU and Prostate cancer surgery
Increasing surgical capacity across the LHIN through wait time funding Excellent collaboration with pathologists for synoptic pathology reporting Commitment to provision of clinical trials as a standard of care across the LHIN Increasing capacity for palliative care across the LHIN though collaboration with
diagnostic work-up, “just-in-time” information/communication tools etc.) ending in e-referral
Lack of central access point for many cancer services (e.g., colonoscopy) Different information management systems across the region Increasing patient and family expectations regarding access to care and
information about treatment options Access to diagnostic testing for family doctors delays diagnosis Shift in delivery of thoracic malignant surgery in Niagara. Risk of losing general
thoracic surgical skills in Niagara as thoracic oncology moves to Hamilton. Consider benefits and risks of a centralized model that has clinical merit for oncology but not for non-oncology. Challenge in developing a partnership model that works for the patient population
Inadequate resources in the community for palliative care in different areas across the LHIN (e.g., Palliative Care Teams, hospice)
o Projecting the need for an additional 5 palliative care teams in the LHIN (for a total of 9 teams)
Challenge of partial implementation of ESAS, PCC across the LHIN Palliative care is more than end-of-life care. Need to incorporate palliative care
earlier in the trajectory of cancer services (e.g. palliative care consultation in medical oncology clinic visit for specific DSTs)
Need to foster patient self-management to address growing prevalence issue CCAC model is a challenge to the LHIN
o Frequent turn over of service providers o Inexperienced nursing staff increases ER visits o Issues with supporting vascular access devices in the community and care for
devices being shifted to the JCC Current potential and future issue with medical isotopes and impact on wait time
for cancer diagnostics
FINAL 4 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
HNHB Hamilton Hospice Palliative Care Network, implementation of Tertiary Palliative Care Unit (TAPCU) at Henderson Hospital, partial implementation of the Ontario Cancer System Management Collaborative (ESAS, PPC) across the LHIN
4 Interdisciplinary Palliative Care Teams in the LHIN Regional Networks for Prevention & Early Detection, Supportive Care (currently
being revised as PsychoOncology Network), Palliative Care, Pharmacy, Aboriginal, Community Oncology)
Development of Patient Education Network to increase awareness and access to cancer prevention, screening & treatment options (e.g. web based tools to access evidence-based information)
Survivorship initiatives (Life After Breast Cancer, Out of the Shadows, Lymphoma the Journey Forward, Bright Run etc).
FINAL 5 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
2. Complete Template #2: Describe the leading factors that are most likely to increase or decrease the demand for health care by the PAG’s patient/client population by 2013. For each of these factors, indicate whether it will have a modest or significant impact on the future demand for health care. And, list factors that may influence the demand for care beyond 2013
Template #2: Factors Most Likely to Increase or Decrease the Future Demand for Health Care: PAG Name: Oncology
Describe the Factor that will increase or decrease the demand for health care by 2013:
Will this factor have a modest or significant impact on future demand for health care?
1. Increase in Incidence & Prevalence of Cancer 70 % increase in incidence from 1990 to 2020 Doubling of prevalence in next 10 years. More people living longer with cancer (chronic disease) Drivers of increase include aging population, population growth and small increase in risk In the next 10+ years, 44% men and 39% of women are expected to develop cancer
Significant
2. Risk Factors for Cancer Higher in HNHB LHIN
Smoking 27.8% compared to Ontario 22.6% Alcohol 25.8% compared to Ontario 20.3% Overall 90% target for increase fruit and vegetable intake (43.9%), and increase physical activity (51.4%) Obesity 20.3 % compared to Ontario 16.8%
Significant – higher lung cancer rates & use of alcohol than province
FINAL 6 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Oncology
Describe the Factor that will increase or decrease the demand for health care by 2013:
Will this factor have a modest or significant impact on future demand for health care?
3. Determinants of Health
Large Aboriginal population (on and off reserve) – lower SES (poorer overall survival for all DSTs.) LHIN has higher proportion of population with less than high school education compared to Ontario One in 5 live in poverty in LHIN
Significant
4. Uptake of Cancer Screening Breast (64%), Cervical (72%), Colorectal (22%) Potential to decrease mortality through population-based organized screening
Significant
5. Timely Access To Diagnostic Assessment Development of Diagnostic Assessment Units for Breast (6 sites in LHIN affiliated with OBSP plus 2 sites in progress),
Lung (1 at St. Joe’s partnering with Niagara), need Colorectal and Prostate. Planning for Thoracic at LHIN level in partnership with Niagara.
Significant
FINAL 7 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Oncology
Describe the Factor that will increase or decrease the demand for health care by 2013:
Will this factor have a modest or significant impact on future demand for health care?
6. Timely Access to Cancer Treatment Wait times for Surgery, Radiation & Systemic Therapy Access to Palliative Care Resources (e.g., CCAC support, hospice)
Significant
7. Access to a Family Physician Number of people without a family doctor-impacts on preventative care, referral into the system for screening/diagnostics,
ongoing care and palliative care
Significant
8. Access to Hospice Palliative Care To address pain and symptom management, psychosocial and bereavement needs in the community and prevent
unnecessary ED and hospital admissions Inadequacy of tertiary palliative care resources and need to integrate into acute care management
Significant
9. Lack of Funding Support Available for Community Care/Patient Flow To treat patients close to home To enable patients to return home/LTC/etc after treatment
Significant
10. Increased Radiation Utilization As access to health care providers improves, radiation rates should increase Currently our LHIN treats 34.9% of cases at any time during the course of their illness against a provincial target of 48% IMRT – more complex treatment requires more time to treat impacting on wait times
Significant
FINAL 8 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Oncology
Describe the Factor that will increase or decrease the demand for health care by 2013:
Will this factor have a modest or significant impact on future demand for health care?
11. New Drugs New drugs for previously untreated indications (e.g. maintenance therapy for Non-small cell lung cancer) and a larger
population requiring these treatments
Significant
12. Less invasive surgery Less invasive minimal access surgery may mean more patients are eligible for surgery LOS in hospital may be shorter
Significant
13. Survivorship Issues for cancer patients that survive and develop late effects related to earlier treatment Outline expectations for patients around treatment and follow-up o “Prescription for Survivorship” o Link back to family physician for follow-up o Need to promote self-care o Psychosocial - increase in demand for supportive care staff, JCC and Region
Significant
14. Increase collaboration between oncologists & family doctors Enhance engagement of family doctors in diagnostic work-up, well-patient follow-up and palliative care Foundation of clinical care should be family practice Link with Family Health Teams
Significant
15. Increased research and translation of research findings To optimize ability to design innovative care delivery models To detect and treat cancer; to improve the experience of cancer patients within existing resources To train the health care professionals of tomorrow
Significant
FINAL 9 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name: Oncology
Describe the Factor that will increase or decrease the demand for health care by 2013:
Will this factor have a modest or significant impact on future demand for health care?
16. Improve the integration of clinical information systems linking providers and patients. Access to clinical information will increase uptake of treatment The impact of email – consultation fee for electronic consultation
Significant
What factors are expected to influence the demand for health care beyond 2013?
Incidence and prevalence Increasing use of molecular markers to tailor treatments for patients
FINAL 10 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
3. Complete Template #3. Describe the key components of an ideal service delivery model for the PAG’s target population. An ideal service delivery model will be informed by, and reflect the following key inputs: Community Values and Preferences (Appendix A) Criteria for PAG Service Delivery Models (Appendix B) Guiding Principles for PAG Service Delivery Models (Appendix C) Leading Practices in Service Delivery Models (Section 2 of PAG binder) Local Planning Principles and Models (Section 3 of PAG binder) Other examples of ‘best practice’ approaches to service delivery brought forward by PAG members.
a. For each component, describe the associated programs and services b. Identify clinical and non-clinical interdependencies (e.g., DI, lab, other programs/services, other PAGs) c. Describe required linkages to community services
Template #3: Components of an Ideal Service Delivery Model PAG Name PAG Facilitator
Component of service delivery model
Services associated with this component of the model
Clinical and non-clinical interdependencies (e.g., DI, lab, other programs/services, other PAGs)
Linkages to community services
Health Promotion/Disease Prevention
Smoking Cessation Healthy Lifestyles – increasing fruits and
vegetables, increasing physical activity, decreasing alcohol
Cancer screening for early detection
DI, GI, Primary Care, Lab
Family Physicians, Public Health, Community Health Centres
Family Physicians, Public
Health, Community Health Centres
Screening programs,
(breast, cervical, colorectal) affiliated services in community hospitals and Independent Health Facilities
FINAL 11 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Component of service delivery model
d with this component of Clinical and non-clinical interdependencies (e.g., DI, lab, other
o ces, other PAGs) Linkages to community
rServices associatethe model pr grams/servi se vices
Primary Care
Prevention Cancer Screening Diagnostic Assessment Supportive Care Cancer Treatment Palliative Care
DI, GI, Lab DI, Lab, Surgery Social work, navigators, dieticians,
psychosocial DI, Lab, Surgery ED
Community Health Centres Community X-ray, Lab,
Hospital JCC, Hospital Hospice, PC beds, LTC,
Hospital
Pre-hospital Care
Diagnostics as above
Acute Hospital Care
Surgery Complications of Treatment Pain & Symptom Management Acute Palliative Care
DI, Lab CCAC
Hospitals CCAC
FINAL 12 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Component of service delivery model
Services associated with this component of the model
Clinical and non-clinical interdependencies (e.g., DI, lab, other programs/services, other PAGs)
Linkages to community services
Non-acute Hospital Care
Post-Hospital Care
Recovery from Treatment Palliative Care
Home care services
CCAC Family Physician, Family Health Teams (FHTs) Community Health Centres
Community-based Acute Care
Recovery from Treatment Pain & Symptom Management Palliative Care
Home care services
CCAC Family Physicians, Family Health Teams (FHTs) Community Health Centres
Community-based Non-Acute Care
Palliative Care
Home Care Services Access to 24/7 on-call
Shared Care Teams
FINAL 13 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name PAG Facilitator
Component of service delivery model
Servon-clinical ncies (e.g., DI, lab, other
PAGs) ices associated with this component of
the model
Clinical and ninterdependeprograms/services, other
Linkages to services
community
Ambulatory Clinics
Delivery of Systemic Therapy & Radiation (new and follow-up visits in community) at JCC and community clinics.
Development of Walker Family Cancer
Centre including 3 radiation bunkers in Niagara
Palliative Care Ambulatory Clinics
DI, Lab DI, Lab, Surgery Home Care Services
CCAC Family Physicians Family Health Teams
(FHTS) Community Health Centres
Self monitoring tools and resources for patients surviving with cancer as a chronic disease
Medication Reconciliation
Edmonton Symptom Assessment Scale
(ESAS) Tool Advanced Care Plan Protocol
Hospice, Palliative Care beds, Long Term Care, Hospital, Community Care Access
Centres, JCC Family Physicians Family Health Teams
(FHTS) Community Health Centres
FINAL 14 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
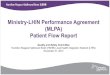
Diagram of Ideal Service Delivery Model:
FINAL 15 of 39
Prevention
Screening
Diagnosis
Government Policy Primary Care, Public Health Hospitals IHFs
Primary Care DAUs, Hospitals IHFs Labs
Surgery Radiation Therapy
Palliative Care
JCC (Level 1), new WFCC (Level 2), Joe Brant & Brantford (Level 3) Radiation new & follow-up Joseph Brant, Brantford, NHS Primary Care Oncologists Palliative Care
Systemic Therapy
Community Hospitals (e.g. general breast, colorectal) Tertiary Hospitals (e.g. Thoracic, Gyne Onc, Hepatobiliary) Primary Care Surgeons Palliative Care
Survivorship
JCC, Hospitals, Primary Care, CCAC Hospice, St. Peter’s, LTC Primary Care Oncologists Palliative Care
Community based support services CCS Community Health centres
09/10 Priority Themes
Family Schools Media Occupational Health Work Place Environment Education
CANCER PATIENT/FAMILY JOURNEY
End-of-Life Transitional Care
Strengthen the Regional Cancer Program
Facilitate Access to Care
Decrease Demand for Services

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
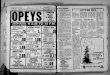
HNHB: Proposed Model for the Full Integration of Systemic & Radiation Therapy Services Among the JCC, Walker Family Cancer Centre and Community Oncology Satellite and Affiliate Clinics * ◊
FINAL 16 of 39
Regional Systemic & Radiation Therapy
Program
Brantford General Hospital Satellite
Level 3 Facility • DST • increase to 5 days per week • Radiation Oncology Clinics •Surgical Oncology
Walker Family Cancer Centre Level 2 Facility (2013)
Academic Education and Research (Clinical Trials) Radiation Surgical Oncology
Joseph Brant Memorial Hospital Satellite
Level 3 Facility DST Radiation Oncology Clinics Surgical Oncology
* Includes the implementation of the Disease Site Team (DST) Model across the LHIN, multidisciplinary case conferencing, plus a regional cancer informatics system to support care across the continuum. ◊ Definitions of Level1, 2, 3 (appendix)
Juravinski Cancer Centre
Level 1 Facility
Welland Affiliate
Follow up
Niagara Falls Affiliate
Follow up sys
Surgical Oncology
Referrals to Brantford General Hospital & JCC Community Oncology Clinic as appropriate
Haldimand Norfolk
Primary Academic, Early Drug Development, Basic Research, Complex Multidisease Management Education & Research (Clinical Trials) Tertiary & Quaternary Radiation
Brachytherapy IMRT Cyberknife

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Definitions of Level of Care
Level 1 (ICP) Academic institutions with teaching and research responsibilities Experimental Investigational New Drug (IND) Program (IND phase 1 and or 2 trials with highly developed clinical trials infrastructure,
e.g., participate in the National Cancer Institute of Canada Clinical Trials Group (NCIC-CTG) IND program and Princess Margaret Hospital/National Institute of Health (PMH/NIH) new drug consortium)
Responsible for training future health care professionals, including oncologists (subspecialty residents and fellows) Level 2 (ICP) Systemic therapy given at an ICP with radiation therapy services and capable of providing most complex systemic therapies,
including concurrent head and neck chemoradiation and/or radiolabelled conjugates Limited teaching and research capabilities Level 3 (Affiliate) Systemic therapies given under direct supervision of an on-site staff medical oncologists, hematologist, or gynecologic oncologist Limited teaching and research responsibilities Level 4 (Satellite) Provides ambulatory facilities, nursing, pharmacy, and physician support for the administration of low-risk to high-risk, intravenous
systemic therapy under the direction of an oncologist from an ICP or affiliate level 3 institution Systemic therapies given under the supervision of a physician with appropriate training in oncology Require access to specialized services and providers with a formalized linkage to the RSTP.
FINAL 17 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL 18 of 39
Regional Cancer Surgery Model
St. Joseph’s Thoracic HPB (proposed
move)) Prostate Head & Neck Endocrine Sarcoma Ophthalmology
Hamilton Health Sciences Gyne-Henderson CNS-General HPB – Henderson Sarcoma
Brantford General Hospital
Joseph Brant Memorial Hospital
Norfolk General Hospital
West Haldimand General Hospital
Haldimand War Memorial Hospital
West Lincoln Memorial Hospital
Niagara Health System
Thoracic (moving)
St. Catharines General Hospital
Greater Niagara General Hospital
Thoracic
HPB
Proposed Model for the Delivery of Cancer Surgery - Draft
Welland General Hospital

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Proposed Model for the Delivery of Supportive and Palliative Care, and End-of-Life Services
FINAL 19 of 39
Specialist Expertise Concentration Interventional Management Pharmacological
Management BOOST Discharge Program
Needs exceed that of primary care providers
Exacerbations of symptoms ↓ coping
Largest Group of patients Chronic disease Cancer
Complex Needs All domains
Phys/psych/social/spiritual
↑↑ personal care ↓↓ coping
Regional Tertiary Acute Palliative Care Unit at Henderson * see addendum
Support Primary Care Providers Consultation Follow-up Direct care
Collaborative Care plans
Basic Palliative Care (BPC) core competencies Identify problems Manage according to
Symptom Management guidelines (SMG)
Know when to refer
Consultation to 10 and 20 levels
Training & Education Research into Best
Practices
Leve
l of P
atie
nt N
eed
& E
xper
tise
Nee
ded
to
Patient Needs Provider Role
Community Teams
Patient in the Home
Primary Care 1st level HPC Expertise
Tertiary Level Specialist
HPC Consult Teams
Larger Hospitals Community
Advanced PC Teams
2nd Level HPC Care
Community Care Teams PC MD PC APN
Community Hospitals Hospices
Levels of Care
Regional TAPCU
CCAC Palliative Care Program
Family Care FoundationsPatient/Family Flow through Levels of Care

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
* Addendum: Regional Tertiary Acute Palliative Care Unit – Henderson General Hospital – 6 beds to 15 beds 2010 Regional Role Provides intensive care in symptom control for patients whose needs can’t be met elsewhere
o Physical e.g. pain, dyspnea, neurologic, obstruction o Psychiatric/psychologic e.g. depression, delirium o Social e.g. difficulties managing at home, family support o Spiritual
Expertise in interventional modalities e.g., intrathecal catheters, kyphoplasty, radiation therapies, neurosurgery Expertise in pharmacologic interventions e.g., lidocaine and ketamine infusions, methadone initiation and teaching
Local Role Palliative care consults and integration into ICU Care at Henderson Step down care to ICU at Henderson, surgical oncology
Teaching Mandatory two week rotation on unit for oncology residents, Palliative Care Fellows Nursing expertise: partnering with CCAC as training site for community nurses managing patients in home, community hospitals wishing to
increase level expertise in nursing ward staff, FHT nursing staff
Research Best practices in palliative care health services delivery models in supportive and palliative care Boost Discharge Program Better outcomes through safe transitions – 4 core elements
o Medication reconciliation in hospital and at home o Primary nurse telephone follow-up within 48 hours o Home visit by MD within 14 days o Liaison with CCAC home team and patients family physician
FINAL 20 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Regional Models of Care for Palliative Cancer Care: Recommendations for the Organization and Delivery of Palliative Cancer Care in Ontario (Cancer Care Ontario)
Recommendation 1: Each region should have three levels of palliative cancer care available: Primary, Secondary and Tertiary
Recommendation 2: Each region should have a mix of services that are patient focused, based on the patient’s needs, as opposed to prognosis, and optimizes outcomes for patients.
Recommendation 3: All regional cancer programs should offer a tertiary level of expertise to maximize access to specialist palliative care services throughout the cancer centre, hospital and the region
Recommendation 4: Common screening, assessment tools and guides to practice should be implemented in all levels of care in each region (e.g., ESAS, Palliative Performance Scale, Collaborative Care Plans and Symptom Management Guides to Practice)
Recommendation 5: Standardized Education, Training and Health Human Resource Planning should be implemented
Recommendation 6: The Regional Palliative Care Program should continue to work with the End-of-Life Networks to establish formal linkages amongst palliative care providers in different settings of care
Recommendations 7: Each Regional Cancer Program should address interprofessional and intraprofessional collaboration within the integrated cancer program and regional cancer program, as collaborative practice is essential for the effective delivery of palliative care in any care setting and between settings of care
Recommendation 8: A mixture of structure, process, and outcome indicators should be established for palliative care services to identify if symptoms are improving, whether services are accessible and whether there is equitable distribution of services across the province
Recommendation 9: An appropriate number of designated palliative care beds within the acute care and non-acute care sector including complex continuing care, residential hospice and LTC should be established based on current benchmarks and projected
FINAL 21 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
need
The recommendations were developed to accommodate long-range needs and take into account the projected increase in palliative cancer care treatment over the next decade due to a growing and aging population. The successful implementation of the model is intended to create sustainable, accessible, quality care and improve patient outcomes
The model provides a comprehensive regional and provincial framework for regional cancer programs and inpatient hospitals to achieve high quality care and services when delivering palliative care treatment in Ontario
FINAL 22 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL 23 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL 24 of 39
Vision of HPC Integration
LTC Homes
CCAC–General CM Nurses
Hospital–Acute bed
Tertiary Interventions
Hospice
Tertiary Level Expertise
Secondary Level Expertise
Primary Level Expertise
Hospital – CCC beds
P & S Consultants
1ry Care Physician PC Physicians
Shared Care Teams, nurse navigator
CCAC – PC CM PC Nurses, APN
Mentored PCP
LTC Homes
Hospital–PC bed Hospital-Surgery
Hospital–ER
Other Comprehensive Palliative Care Services (SW, psychospiritual, bereavement, Rx, funeral directors)
Hospital--Consults
Hospital-Cancer Ctr Hospital-Cancer Ctr Hospital-Cancer Ctr

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Regional Cancer Program – 2009/10 Regional Priorities
Priority #1: Strengthen the Regional Cancer Program
Description of Regional Priority, including Deliverables and Timelines
1. Continue to engage regional partners around the Regional Systemic Therapy Plan. Continue planning for Walker Family Cancer Center in Niagara, add 1 Breast Clinic to Brantford. Develop additional GPO resources in Brantford and Burlington. 2. Meet CCO compliance targets for safe delivery of systemic therapy. 3. Implement process to certify and recertify all regional oncology nurses in the safe handling of cytotoxic drugs. 4. Engage more regional participants in MCC videoconferencing. 5. Continue annual Regional Oncology Nursing and Pharmacy Retreat. 6. Strengthen the Regional Pharmacy Network. 7. Development of Regional Psychosocial Oncology Network. 8. Continue pathology reporting. 9. Continue stage capture including non-ICP hospitals. 10. Standardize regional diagnostic workup for lung cancer and establish assessment process for Niagara. Develop formal plan for consolidation of hepatobiliary. 11. Continue work for common clinical information systems for HHS/NHS cancer program and LHIN. 12. Continue implementation of Regional Cancer Informatics Strategy. 13. Implement Regional Education Network. 14. Continue to strengthen and develop relationships with the HNHB HPC Network 15. Launch Cancer Research Institute
Which CSQI indicator is this tied to?
Cancer data capture (treatment), Cancer data capture (diagnosis), completeness of pathology reporting, stage capture.
What is the Program Level Performance Indicator
Brantford breast cancer patients will receive systemic therapy close to home. Standard high quality model of care across region. Wait times are decreased. Organizational model for Walker FCC confirmed and leads recruited. Pharmacy Network goals achieved. Surgical Oncology Network goals achieved.
FINAL 25 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
What is the year-end 2009/10 target for this program level?
C1S volumes will be achieved. C1R volumes will be a challenge to achieve.
Compliance with CCO targets for all regional performance indicators.
What CCO Support may be required (i.e., non-financial)
Support for medical oncologist positions for LHIN, especially in Niagara. Funding models that address base funding in community to increase care close to home. Ability to count cases done in community. Support for minimal access surgery.
Priority #2: Facilitates Access to Effective Diagnosis and High Quality Care
Description of Regional Priority, including Deliverables and Timelines
1. Develop plans (systemic and radiation) for the Walkers Family Cancer Centre through the integrated partnership model. 2. Consolidate Hematology Program to Henderson Hospital. 3. Strengthen patient access to excellent clinical trials as a standard of care across the LHIN. 4. Increased use of ESAS for all tumor types. 5. Develop strategies through Henderson Innovation and Learning to facilitate end of life care in the most appropriate settings and reduce emergency admissions. 6. Continue to integrate palliative medicine,practices and education into additional DSTs. 7. Cost Functional Program for new OBSP Hub, Develop capital and operational budgets. Secure funding. 8. Support fundraising efforts for CIBC - Breast Assessment Centre (BAC). 9. Continued development and implementation of Lung DAU at St. Joseph's. 10. Support for St. Joe’s proposal for Diagnostic Assessment Program – Lung, Colon & Prostate 11. Develop strategies to correct underutilization of radiotherapy in Brantford, Burlington, Norfolk. 12. Develop joint JCC, St. Joseph's, Brantford GU and Prostate Clinics (surgical and radiation). 13. Increase referrals to Aboriginal Navigator for supportive care services; increase breast and colorectal screening on Six Nations reserve through CCO Primary Care Pilot Project. 14. Increase Medical and Radiation Oncology Human Resources. 15. Basadur process improvements (should we be tying our process improvements to a named consultant? - chemosuite/pharmacy development of scheduling grid, patient registration and clinic operations, lab staffing requirements.
FINAL 26 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
16. Strengthen regional, clinical and research leadership role of Disease Site Teams 17. Collaborate with CCO-ACCU on Aboriginal Cultural Identification pilot. 18. Develop strategy to train all LHIN surgeons on breast cancer sentinel node biopsy. 19. Continue training of general surgeons in laparoscopic colectomy via telementoring 20. Consolidate Hepatobilray surgery to a single site 19. Provide access to decision support tools to support best practice. 20. Develop advanced practice oncology nursing through new Centre of Research Excellence.
FINAL 27 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Which CSQI Indicator is this tied to?
Wait times for systemic and radiation therapy. End-of-Life Care ESAS Screening Patient Satisfaction Pain Management Wait time to breast assessment Standards for thoracic surgery and hepatobilray surgery
What is the Program Level Performance Indicator
Increase roll-out of OCSMC across LHIN Process improvements for new patient referrals and clinic implemented. Implement pharmacy and chemo grid. Begin detailed operational planning for CIBC-BAC.
Complete ACCU pilot project.
What is the year-end 2009/10 target for this program level?
Achieve wait time targets for both Radiation and Systemic Therapy
What CCO Support may be required (i.e., non-financial)
Continued support for data to drive decision-making at the regional level.
Priority #3: Decrease Demand for Cancer Treatment Services
Description of Regional Priority, including Deliverables and Timelines
1. Continue regional public lecture series focusing on cancer prevention. 2. Plan and implement a Cancer Prevention Conference. 3. Develop plan to implement JCC RNAO Best Practices Smoking Cessation Model more broadly across the LHIN including Community Oncology Clinics. 4. LHIN-wide initiative to make all hospitals smoke-free and move towards the Ottawa Heart Institute Model to support the inpatient population 5. Convert all hospital non-OBSP screens to OBSP screens. 6. Continue to increase initial screening volumes at all sites through collaboration with FPs. 7. Increase uptake of FOBT with FP pilot target sites including FP serving Aboriginal population. 8. Increase capacity for colonoscopy through LHIN-wide participation in process improvement strategies. 9. Collaborate with OBSP and FP to increase cervical screening.
FINAL 28 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
10. Continue to develop cancer genetics program for breast, ovarian and colorectal. 11. Collaborate with CCS and regional partners on sun exposure initiative.
Which CSQI Indicator is this tied to?
FOBT rates, cervical screening rates, mammography rates, obesity rates, smoking rates, diet and physical activity. Specific indicators related to Aboriginal initiatives. Sun exposure.
What is the Program Level Performance Indicator
Increased collaboration of chronic disease partners around common messaging and initiatives for increased screening and decrease risk factors, including specific initiatives with Aboriginal partners. CAR hospitals apply for OBSP affilation (Hagersville, Dunnville) and new initiatives with IHF increase initials and overall screening levels. Increase population with FOBT screening through FP pilot including Aboriginal population.
Increased colonoscopy capacity.
What is the year-end 2009/10 target for this program level?
OBSP hub and regional projections achieved. Grimsby, Hagersville and Dunnville become OBSP sites. Non-OBSP screens decrease and OBSP initial screens increase. Recruit IHF in Niagara. Review opportunities for affiliation with other IHFs. Regional colonoscopy incremental volumes and WTs achieved. Continue flexi-sig pilot project. Increase in cervical cancer screening rates.
What CCO Support may be required (i.e., non-financial)
Increased funding for incremental colonoscopy volumes. Increased support for administrative activity to roll out CCC program.
FINAL 29 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL 30 of 39
RReeggiioonnaall CCaanncceerr PPrrooggrraamm Hamilton, Niagara, Haldimand, Brant
Local Health Integration Network
2 HHS & St. Joe’s+ Colonoscopy Volume Sites
•HHS •St. Joe’s •St. Catharines •Burlington •Brantford •Simcoe
2013)

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Template #4. Assess and Describe the PAG service delivery model using the HNHB LHIN Criteria PAG Name
Domain Criteria Assessment Description Strategic Fit Alignment with LHIN
priorities for health improvement
Regional Cancer Plan is in alignment with CCO’s Ontario Cancer Plan 2008-2011 and with LHIN priority for health improvement. Regional vision is equal and timely access to a coordinated system of high quality cancer services across the continuum of care from prevention through palliative care. The model is care close to home across the region with 30 and 40 services consolidated for a few sites (e.g. gyneoncology, sarcoma, at JCC. Building capacity for care close to home with regional plans for cancer screening, systemic therapy, radiation therapy and palliative care. Wait time funding to increase throughput for surgery and colonoscopy volumes.
Alignment with trends in health care needs and system transformation
Ontario Cancer Plan and Regional Cancer Plan built on data showing 70% increase in cancer incidence from 1990 to 2020 and a doubling of prevalence in 10 years. Plans to include decreasing demand for services through prevention and early detection, and strengthening Regional Cancer Programs to increase access to care and development of a new Cancer Centre in the LHIN (Niagara). Palliative ALC population needs to move towards ‘home first’ approach requiring greater support from CCAC palliative care community-based shared care teams in providing end-of-life care. Development of Adolescent and Young Adult Program to address unmet needs
Health status (clinical outcomes & QOL)
Planning for Provincial and regional cancer services is based on an analysis of the regional profile, modifiable risk factor data, incidence & prevalence trends, Cancer System Quality Index data and current capacity issues/challenges. Regional priorities are developed in consultation with CCO and are aligned with provincial targets. Monitoring guideline concordance, survival rates by DST
Population Health
Prevalence Ontario Cancer Plan and Regional Cancer Plan address increases in incidence and prevalence of cancer. Cancer is becoming more of a chronic disease as more people are living longer with cancer due to early detection and improvements in treatment. The number of people living with cancer will double in the next 10 years. By 2020, 450,000 people will be living with cancer in Ontario; 40,000 in this LHIN
FINAL 31 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
Domain Criteria Assessment Description
Health promotion & disease prevention
Cancer System Quality Indicators (CSQI) address key targets for Prevention (rates for obesity, smoking, vegetable and fruit intake, physical activity and alcohol), and Access (uptake for screening – breast, colorectal, cervical as well as a composite score for women for cancer screening completeness).
Client-focus Development of an Ontario Cancer Plan was based on data including the Cancer System Integration Committee Report in 2003. At that time, Cancer services were not client-focused across the continuum of care. Integration of all Regional Cancer Centres with their host hospital in June 2004 began the integration and coordination of care across cancer centres, hospitals and community/regional partners. Formal Regional Cancer Programs were developed with CSQI and Quarterly Reporting to CCO. Indicators include measures of patient satisfaction. Specific programming in key areas including Aboriginal (e.g. Patient Navigator) and cancer screening (e.g. hard to reach populations in collaboration with Public Health). All screening program materials are available in multiple languages (including resources for French language population in LHIN). Still need more attention to this area. The proposed model is driving change to increase the client focus by providing more services closer to home, increasing the human resources capacity to provide care consistent with best practice guidelines or highly specialized care in tertiary centres to maximize patient outcomes.
System Values
Partnerships Long history (over 25 years) of partnership for the delivery of cancer services across the LHIN to increase care close to home. Community Oncology Clinics for systemic and radiation therapy (new and follow-up visits) in Niagara, Brantford and Burlington. Breast Screening delivered at 9 hospitals, colonoscopy incremental volumes at 6 hospitals, and surgical volumes at 2 hospitals (with corresponding systemic therapy volumes at 2 hospitals) Implementation of the Ontario Cancer Symptom Management Collaborative at the regional level through the JCC, CCACs and LTC partners. Partnerships with HNHB Hospice Palliative Care Network, Community Based Shared Care Teams. Partnerships with Aboriginal community both on and off reserve to increase cancer screening rates to improve current poor survival rates. CCO Pilot site for Aboriginal Indicators studies to link identifiers to cancer data. Strengthen partnerships with patients to maximize self-care Build capacity for academic/education research to address need for Human Resources
FINAL 32 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
Domain Criteria Assessment Description Use of standard protocols beyond hospitals (e.g. community care, urgent care etc) MCC with partnering institutions Mentorships Supportive Care partnership with YMCA (CanWell), Wellwood, Wellspring, Aboriginal Network and all
Regional Networks previously listed
Community Engagement The Regional Cancer Plan reflects community values and preferences for access (goal and major deliverables in plan), efficiency (multiple process improvement initiatives (e.g. colonoscopy pilot), quality care (CSQI) and engagement (public reporting, town halls)
Innovation Innovation and Advanced Practice Models for APNs (Centre of Research Excellence for APN), APT & AMRT, Nurse Endoscopy.
Recruitment strategies with family physicians for cancer screening (OBSP, FOBT and Nurse Endoscopy)
“Alternate Day Chemo” to increase care close to home. (The first systemic therapy visit is at the JCC with treatment given in community).
Dose Banding – to expedite preparation of chemotherapy by pharmacy services and thereby decrease patient waiting times in the chemo suite.
Aboriginal Navigator role to address access, cultural sensitivity and support. Clinical Decision Support Tools – breast, lung, GI Regional Survey of Family Physicians to understand and support their role in providing cancer services Developing proposal for dissemination of clinical algorithms for diagnostic imaging in cancer care for
family physicians using PDAs on desk-top computers Canwell – exercise program for cancer patients in partnership with the YMCA
Equity Equity of Access is a key deliverable in Regional Cancer Plan. Reviewing variation in utilization of cancer services across LHIN (e.g. radiation plan is addressing lower utilization rates in Haldimand, Norfolk and Brant, breast screening plan works with public health to address hard-to-reach populations, FOBT and colonoscopy mapping project etc.)
FINAL 33 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
PAG Name
Domain Criteria Assessment Description
Efficiency (operational) Multiple process improvement initiatives to expedite flow within the cancer centre including Basadur project (e.g. Lab, Chemo, Pharmacy, Clinic Scheduling), PDSAs (e.g. Admission Avoidance, Oncology Response Team), projects with Industrial Engineering University of Toronto (colonoscopy, surgery) and a relative demand model working with the ALC Palliative population to expedite patient flow out of acute care. Information access is a key initiative. HHS-led LHIN initiatives with regional cancer informatics.
Access Indicators monitoring cancer screening (breast, cervical, colorectal, composite score for women), breast cancer test wait times, cancer treatment wait times and End-of-Life Care wait times. See CSQI April 2009 Report (attached).
Quality Administrative Leadership for Quality at the regional level. Cancer System Quality Index Report – produced annually in April by the Cancer Quality Council of Ontario. Quality Councils are embedded in Executive Committees at JCC and Henderson Hospital. Development of HNHB Cancer Quality Index
Sustainability
Cancer services funded by CCO. Mismatch between increase in cancer volumes and dollars for cancer at the ambulatory level and decreasing budget at the hospital level. CCO addressing funding models to support more care close to home for Systemic Therapy (i.e., community hospitals like Brantford and Joseph Brant do not receive additional operational dollars to support increasing the number of patients who would be eligible to receive chemotherapy close to home.
System Performance
Integration
CCO launched a major research initiative to develop a tool to measure cancer services integration. The goal was to monitor and improve cancer system performance. The tool includes measures of clinical, functional and vertical system integration. CCO has conducted 3 provincial surveys of all 14 RCPs. HNHB LHIN ranked 1st in the 1st 2 surveys and 3rd in the 3rd survey.
FINAL 34 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
4. Complete Template #5. Describe the pre-requisites, enablers and challenges to implementation of the ideal service model.
Template #5: Description of Pre-requisites, Enablers and Challenges to Implementation: Category Pre-requisites Enablers Challenges Policy/legislation Cancer system data
Quality guidelines and standards
Clinical pathways/care maps
Legislative authority – CCO is a provincial agency governed by the Cancer Act.
Ontario Cancer Registry (OCR)
Centre of Excellence-Based
Medicine – influence policy Cancer Quality Council of
Ontario
Challenges specific to
Aboriginal population re: unique identifiers and ability to link to OCR
Resources (e.g., human, fiscal, capital, etc.)
Workload data and standards related to incidence and prevalence for all Health Care Providers (HCP)
Alternate Payment Plans for med onc/rad onc/surg onc/gyne onc/palliative care
Alternate Models of cancer service delivery (e.g. APNs, APT, AMRT, GPOs)
Schools/Training Programs
Systemic therapy plan identifies med onc workload issues across region
Shortage of HCP across the board impacts on access and ability to provide care in a timely fashion (e.g. family physicians, GPOs, palliative care physicians, nurses, pharmacists, mammo techs etc.)
Inequity in access to supportive care resources across LHIN (e.g. social work, dieticians, chaplaincy)
Funding to Radiation Therapy
FINAL 35 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Adequate budget to fund
cancer services across continuum of care from prevention through to palliative care
Capital equipment funding
through CCO adequate to deliver state-of-the art cancer services
Capital equipment on hospital
side is seriously out of date and no funds for capital call. A lot of this equipment is important for cancer diagnostics and treatment (e.g. interventional suite, PET/CT, state of the art Ultrasound, MRI etc)
Adequate drug budget
for alternate roles. Funding Models Incremental dollars to
increase capacity CCO funding for “in-house”
capital equipment (e.g. radiation, mammography)
New Drug Funding Formula
School and graduate Medical Physics training program doesn’t match expenses
Nurse Endoscopy role being piloted without budget support at the hospital level
Inadequate funding and
programming allocated to prevention to reduce demand for services
Ability to move care close to home impacted by lack of funding at the operational level
Mismatch in increasing cancer dollars and decreasing hospital budget dollars
Inadequate funding on
“hospital-side of the house” for DI and Lab
Inequity in access to
unfunded drugs across region
FINAL 36 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
Community readiness
Transparency in planning, decision-making and delivery of cancer services
CSQI CCO RCP Performance
Report Cards
Funding to move care close to home
Always need for more communication and engagement (including web-based and electronic tools) across all HCPs to improve access, use of resources, process for referrals, and quality
Services
Right care at the right place at the right time
Defining roles and accountability for cancer services across LHIN
Capacity for increased services
Funding for tertiary level services at JCC and funding for care close to home (systemic, radiation, supportive/palliative care)
Increased interdisciplinary care teams
Care paths/planning Outreach for specific
populations (e.g. Aboriginal) Adequate resources (HR and
funding) to support care in the community
Electronic medical record Regional Cancer Informatics Telemedicine
Challenge for funding increased cancer services close to home
MOH funding dual streams for screening (OBSP/non-OBSP, CCC program FOBT forum)
Currently no funding for colonoscopy outside hospital system.
Enhanced health promotion and prevention initiatives
Patient referrals to Aboriginal Navigator
CCAC RFP process – high-turnover of staff, inexperienced staff increases referrals to ED
Time to implement IM/IT strategy
Partnerships/linkages
Willingness to collaborate to improve access and quality
Memoranda of Understanding Innovation funding Quality indicators and
reporting to CCO Performance Management
targets for Quality Reporting
One year CCO contracts create uncertainty for planning purposes
Pilot projects without plan for longer term funding if the pilot is successful – potential
FINAL 37 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
to CCO impact on hospital budgets Knowledge transfer and
disease pathway management uptake
FINAL 38 of 39

HNHB LHIN Clinical Services Planning Project, Planning Advisory Group Meeting Guide
FINAL 39 of 39
Appendix D: Meeting #1: PAG Meeting Summary Form: PAG Meeting Summary Form Meeting #1 – May 19, 2009
PAG Name: Oncology PAG Facilitator: Carol Rand
Summary of PAG progress Template to be populated by Carol Rand based on Regional Cancer Plan 09/10 draft document and supporting materials General discussion of “out-of-the box” thinking across the continuum of care from prevention through to palliative care.
Outstanding questions or Issues for follow-up Timeframe issues
e.g., Ont – Palliative Care Think Tank Information and questions to be communicated to other PAG(s) Other comments Pleased with engagement and discussion at 1st meeting