Embed Size (px)
Citation preview

HALILOL RAHMAN
National Poison Centre
Universiti Sains Malaysia
Animal Toxinology

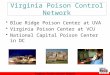
0 100 200 300 400 500
Snake
Spider/Scorpion/Centipe…
Insect
Jellyfish
Other marine toxin
Plant
Bacteria/Fungi/Algae
Other natural toxin
Unknown natural toxin
418
119
36
30
54
74
157
23
4
Number of cases
NATURAL TOXIN poisoning (2006-2014)

SNAKE BITE

Case
• 5 year old girl was brought to ED with alleged snake bite over her left leg
• Occurred at 2pm and arrived to ED at 3pm
• Child was playing near her house in Paya Jaras when she was suddenly bitten by a small cobra like snake
• No bleeding at site
• Left lower leg becomes painful and tender

• Noted 2 bite marks over Lt lateral erythematous skin changes surrounding it measuring 5x5cm
• Her left leg was not oedematous
• Pulses were palpable, able to move her toes, sensation intact
• The left leg was splinted for immobilization

• Admission to ward, noted 6 hours after bite , Lt lower foot was swollen and had bluish discoloration
• Swelling was increasing ,tender++,
• FBC :TW 9, Hb 12.3, PLT 256, PT/ApTT normal
• She was also having spiking temperature

• At 11pm, she was administered 1 vile of monovalent cobra antivenom
• Subsequenlty started on IV Augmentin
• On the following day, noted that swelling was static and fever was slowly subsiding
• BP remains stable
• Serial FBC and coagulation profile remains normal
• Child remains alert and comfortable

After 8 hours

• At D3 of bite, swelling has reduced and child was able to move her lower limbs
• She was also able to ambulate
• Currently still in ward awaiting swelling to resolve
• No systemic involvement subsequently

Introduction
• From 1978 to 2000, there were 55000 cases of snakebites recorded in the hospitals in Malaysia
• The mortality rate of snakebite in Malaysia is only 0.3 per 100000 population but the local necrotic effects of some venoms can cause prolonged morbidity or even crippling deformity

• not all snakes are venomous
• In Malaysia there are approximately 40 species of venomous snakes (18 land snakes, all 22 of sea snakes) belonging to two families:
- Elapidae – have short, fixed front fangs. The family includes cobras, kraits, coral snakes and sea snakes.
- Viperidae – have a triangular shaped head and long, retractable fangs. eg; the Malayan pit vipers are common in the northern part of Peninsular Malaysia but are not found in Sabah and Sarawak


Elapidae
Ismail AK., et al. Image gallery of land snakes of medical significance in Malaysia. 2013

Elapidae
Ismail AK., et al. Image gallery of land snakes of medical significance in Malaysia. 2013
Banded krait (Bungarus fasciatus) Red-headed krait (Bungarus flaviceps)
Banded coral (Calliophis intestinalis lineata ) Blue coral (Calliophis bivirgatus)

Naja sumatrana
Naja kaouthia
Ophiophagus hannah

Elapidae
Ismail AK., et al. Image gallery of land snakes of medical significance in Malaysia. 2013
Spitting cobra, Naja sumatrana
King cobra, Ophlophagus hannah
Monocled cobra Naja kaouthia

©Yati
Ophiophagus hannah, King Cobra


Laticaudinae/Hydrophiinae
(Sea-Krait/Sea Snakes)
©Grismer
Beaked Sea Snakes, Enhydrina schistosa
Common Sea Krait, Laticauda colubrina
Common Sea Krait, Laticauda colubrina


Viperidae Sumatran pit viper, Trimeresurus (Parias) sumatranus
Cameron pit viper Trimeresurus (Popeia) nebularis
Ismail AK., et al. Image gallery of land snakes of medical significance in Malaysia. 2013
White-lipped green pit viper, Trimersurus (Cryptelytrops) albolabris

Viperidae
Malayan pit viper, Calloselasma rhodostoma Mountain pit viper, Ovophis convictus
Ismail AK., et al. Image gallery of land snakes of medical significance in Malaysia. 2013

Local symptoms in the bitten part
• fang marks
• local pain
• local bleeding
• bruising
• lymph node enlargement
• lymphangitis (raised red lines tracking up the bitten limb)
• inflammation (swelling, redness, heat)
• Blistering
• local infection, abscess formation
• necrosis

Generalized (systemic)
symptoms and signs General
• Nausea, vomiting, malaise, abdominal pain, weakness, drowsiness,
prostration
Cardiovascular (Viperidae)
• Visual disturbances, dizziness, faintness, collapse, shock,
hypotension, cardiac arrhythmias, pulmonary oedema, conjunctival
oedema (chemosis)
Bleeding and clotting disorders (Viperidae)
• Traumatic bleeding
• Spontaneous systemic bleeding
Neurological (Elapidae, Russell’s viper)
• Drowsiness, abnormalities of taste and smell, “heavy” eyelids,
ptosis, paralysis, difficulty in swallowing secretions, respiratory and
generalised flaccid paralysis.

Bleeding and clotting disorders (Viperidae)
Neurological (Elapidae, Russell’s viper)

MANAGEMENT OF SNAKE BITES

General Measures
• Adequate reassurance
• Immobilize patient, particularly the bitten limb
• Treat local lesion
• Treat shock
• Tetanus prophylaxis
• Specific antivenom given
• Admit and observe all bitten patients for at least
24 hours.

Recommended First Aid
Methods
• Reassure the victim who may be very anxious
• Immobilize the bitten limb with a splint or sling
(any movement or muscular contraction may increase the absorption of venom into the blood stream and lymphatics)
• Consider PRESSURE-IMMOBILISATION for some elapid bites
• Avoid any interference with the bite wound
(may introduce infection, increase absorption of the venom, and increase bleeding)

Most Traditional First Aid Methods should be discouraged
THEY DO MORE HARM THAN GOOD !
Some proved useless or even dangerous
For examples: • tying tight bands (tourniquet around the limb)
• attempt to suck out the venom out of the wound
• topical application of chemicals, herbs or ice-pack at the site of the bite or in the bitten limb
• making local incision, or punctures, etc.

Pressure-Immobilisation
Method
• To slow down the absorption of venom from the site of
the bite, BECAUSE
Bites by neurotoxin elapids (cobras, king cobras, kraits
or sea snakes) may lead to the rapid development of life-
threatening respiratory paralysis
SHOULD NOT be used for
viper bites because of the
danger of increasing the local
effects of the necrotic venom.

Antivenom treatment
• What is antivenom?
Immunoglobulin from the serum or plasma of a
horse or sheep that has been immunized with
the venoms of one or more species of snakes.
2 types : monovalent or polyvalent
• Dose in both adult and children is the same.
• Contraindication

What antivenom is available in
Malaysia?
Monovalent Antivenom • King Cobra antivenin
• Cobra antivenin
• Banded Krait antivenin
• Malayan Pit Viper antivenin
• Green Pit Viper antivenin;
– Sabah pit viper, Sumatran pit viper, Bornean palm pit viper, Kinabalu pit viper
Polyvalent Antivenom • Hemato polyvalent snake antivenin
• Malayan pit viper, white-lipped green pit viper and Siamese Russell’s viper
• Neuro polyvalent snake antivenin
• King Cobra, Monocled cobra, Banded Krait, Malayan Krait

Indications for antivenom
Recommended if a patient with proven or suspected snake bite, develops one or more of the following signs:
Local Envenoming
Local swelling in more than half of the bitten limb
Swelling after bites on the digits
Rapid extension of swelling beyond wrist or ankle within a few hours of bite
on the hands or feet
Development of an enlarged tender lymph node draining the bitten limb
Systemic Envenoming
Haemostatic abnormalities
Neurotoxic signs
Cardiovascular abnormalities
Acute Renal failure
Haemoglobin-/myoglobin-uria
Other supporting laboratory evidence of systemic envenoming (e.g., ↓ platelet count, etc.,)

Antivenom administration
• The snake species is identified (use monovalent/mono-specific antivenom)
• The snake species is unidentified (use Neuro-polyvalent or Hemato-polyvalent antivenom)
• Adrenaline drawn up in readiness before antivenom is administered (IM 0.5 mg for adults and IM 0.01mg/kg body weight for children (0.1% solutions, 1 in 1,000 dilution, 1mg/ml).
• Method: Intravenous infusion. - Reconstitute freeze-dried antivenom with the solution supplied or
10ml WFI. - Gently swirl (never shake) to dissolve the freeze-dried antivenom. - Further dilute with 5-10ml of NS or D5% per kg body weight for
children or 250-500ml NS or D5% for adult). - Infuse the antivenom mixture starting slow (1 to 2 ml/min) over
10-15 min then increased to a higher rate if no reaction to complete within a period of one hour or earlier.
• Closely observe patient during and for at least one hour AFTER completion of intravenous infusion. Serially chart vital signs and clinical progression

Antivenom reactions


CENTIPEDE
• Centipede bites usually cause only local irritation
local burning pain, erythema, vesiculation, itching,
and swelling
Treatment:
Application of ice
IV bupivacaine
Topical corticosteroids or antihistamines
Tetanus prophylaxis

SCORPION
• 2 species commonly found in Malaysia – Asian forest scorpion (Heterometrus longimanus)
– Malaysian Forest Scorpion (Heterometrus spinifer)
• Usually cause only local irritation
• Pain, swelling, redness and numbness
Treatment:
Application of ice
IV bupivacaine
Topical corticosteroids or antihistamines
Tetanus prophylaxis

Honeybees, bumblebees, yellow jacket hornets, wasps,
• Envenomation may cause allergic reactions, local effects, or
systemic poisoning.
– Nonallergic local reaction
– Toxic reactions
– Hypersensitivity reactions
Hymenoptera stings

Hymenoptera stings: symptoms
Nonallergic local reaction: – pain, irritation, itching, and redness at the site of the sting
– Symptoms generally resolve within a few hours
– Stings in the mouth or throat may be especially dangerous because local edema may cause respiratory obstruction.
Toxic reactions:
• Manifestations include edema, fatigue, vomiting, diarrhea, headache, hyporeflexia, slurred speech, hypertension, tachycardia, hypotension, seizures, coma, rhabdomyolysis, and acute renal failure.
• Delayed toxic reactions are rare, but do occur. (onset: 1 – 13 days)
- Patients with multiple stings may experience delayed toxicity,
- Such patients are asymptomatic after a massive bee envenomation, with normal initial laboratory results,
- but later develop laboratory evidence of hemolysis, coagulopathy, thrombocytopenia, rhabdomyolysis, liver dysfunction, and disseminated
intravascular coagulation.


Hymenoptera stings: symptoms
Home management :.
• Manually remove the sting shafts with their commonly attached
venom sacs as soon as possible
– use a key, piece of cardboard or other blunt-edged device.
– Avoid squeezing the stinger or venom sac.
• Local application of ice packs at the sting site for 15 minutes every
30 minutes may decrease the intensity of swelling.
• Over the counter antihistamines may reduce pruritus and swelling.
Observation criteria in hospital:
• Patients with multiple stings, and those with evidence of or a history
of anaphylaxis should be referred to a healthcare facility
• For severe toxicity: supportive treatment

0 100 200 300 400 500
Snake
Spider/Scorpion/Centipe…
Insect
Jellyfish
Other marine toxin
Plant
Bacteria/Fungi/Algae
Other natural toxin
Unknown natural toxin
418
119
36
30
54
74
157
23
4
Number of cases
NATURAL TOXIN poisoning (2006-2014)

Catfish 19%
Ciguatoxin 3%
Unknown fish sting 2%
Jellyfish 36%
Leach 1%
Lion fish 1%
Mystus sp 1%
Stingray 6%
Stone fish 5%
Scorpion fish 1%
Saxitoxin 2%
Brevetoxin 2%
Tetrodotoxin (puffer fish)
10%
Tetrodotoxin (horseshoe crab)
7%
Unknown marine toxin 4%
PERCENTAGE OF FRESH WATER/MARINE TOXINS POISONING CASES REFERRED FOR ENQUIRY TO
NATIONAL POISON CENTRE (2006-2014) Frequency %
Catfish 16 19.0
Ciguatoxin 2 2.4
Unknown fish sting 2 2.4
Jellyfish 30 35.7
Leach 1 1.2
Lion fish 1 1.2
Mystus sp 1 1.2
Stingray 5 6.0
Stone fish 4 4.8
Scorpion fish 1 1.2
Saxitoxin 2 2.4
Brevetoxin 2 2.4
Tetrodotoxin (puffer fish)
8 9.5
Tetrodotoxin (horseshoe crab)
6 7.1
Unknown marine toxin
3 3.6
Total 84 100.0


There are three main classes of jellyfish that pose a threat to humans
• Scyphozoans
• Cubozoans
• Hydrozoans



Venom properties Jellyfish has stinging mechanism in the form of venom – containing nematocyst. Different species have different content of toxin. The nematocysts may discharge dermatonecrotic ,neurotoxic, hemolytic factors and/or cardiotoxins. Stinging mechanism Nematocysts are stinging cells, that with an appropriate stimulus may trigger a tubule (a harpoon like structure) to eject and penetrate into the surface where it is anchored, and release venom. Nematocysts are extremely stable and can remain active even when the coelenterate has died and is dried.

• Clinical management is specific for the symptoms of serious envenomation: to provide analgesia, reduce hypertension, and provide specific drug therapy to manage severe symptoms.
• It may include advanced life support, antivenom administration, and management of both systemic and regional vascular problems.
• Antivenom is available for Chironex fleckeri stings and has been used with success in other chirodropid envenomations. However, this antivenom is currently NOT available in Malaysia.



Catfish venoms have been shown to display neurotoxic and hemolytic properties and can produce a variety of additional effects. Exact venom components vary from species to species; the toxic mechanism of many species has not been fully elucidated.

Types of catfish in Malaysia

Acute
effect of
catfish
sting

Management of Catfish
Envenomation

The scientific family name refers to the four large teeth, fused into an upper and lower plate. This is a unique characteristic of puffer fish that helps us to identify it in poisoning cases.
The toxin found in pufferfish is known as TETRODOTOXIN or TTX



Dried fish-roes - Xenopterus naritus

Grilled Yellow Pufferfish




Horseshoe crab
Carcinoscorpius rotundicauda
Another source of TTX


Pufferfish poisoning cases in Malaysia
Year Case Sources
1985 Puffer fish poisoning: Four case reports, Sabah Med. J. Malaysia. 40 (1), 31-34.
1987 Nine fatal cases of puffer fish poisoning in Sabah Med. J. Malaysia. 42 (3), 199-200.
1997 A Unique Case of Tetrodotoxin Poisoning, Terengganu
Articles
2008 Two cases of food poisoning due to consumption of puffer in Johor ( 2 dies)
Local newspaper
2009 Fishermen dies in Terengganu after eating puffer fish
Local newspaper
2009 3 admitted to HUS after eating puffer fish bought from fish monger in Buntal, Kuching.
Jabatan Kesihatan Bahagian Kuching

For Your Kind Attention
THANK YOU