Embed Size (px)
Citation preview

SYMPOSIUM: NEPHROLOGY
Haemolytic uraemicsyndromeAmrit Kaur
Larissa Kerecuk
AbstractHaemolytic uraemic syndrome (HUS) the commonest cause of acute renal
failure (ARF) in children. It is categorized by a triad of clinical features,
haemolytic anaemia, thrombocytopenia and ARF. HUS is subdivided in to
two broad categories, typical, usually diarrhoea positive D þ HUS (more
than 90% of cases) most commonly caused by Shiga toxin (Stx)-producing
Escherichia coli (STEC; also called verotoxin, VTEC). Atypical, usually
diarrhoea negative D � HUS or aHUS (approximately 5% of cases).
Clinical spectrum of HUS is initiated by intestinal colonization of STEC.
Histological appearance of HUS shows widespread thrombotic microangi-
opathy (TMA) in renal glomeruli, the gastrointestinal tract, the brain, and
the pancreas. Intraluminal thrombosis occurs leading to partial or
complete obstruction of the vessel lumen.
The aim of this review is to summaries the latest development and
understanding of this condition. Focussing on epidemiology, pathophys-
iology and disease course. An emphasis on the diagnosis, management
and follow-up of HUS has also been taken.
Keywords acute renal failure; haemolytic uraemic syndrome;
pneumococcal haemolytic uraemic syndrome; shigatoxin; thrombotic
microangiopathy
How common? UK and worldwide
The overall incidence of haemolytic uraemic syndrome (HUS) in
UK and Ireland is 0.71 per 100,000 children under 16 years of
age. Prospective surveillance study of childhood HUS from 1997
to 2001 in UK and Ireland showed the highest incidence rates
were in Scotland (1.56 per 100,000). This difference could be
secondary to the relative population densities of livestock and
humans and reliance on private water supplies in rural areas.
The prevalence of HUS has remained unchanged since 1985.
The incidence is similar across Europe, Australia and North
America. A large outbreak occurred in Germany this year with
the strain E. Coli 0104:H4. Argentina is reported to have the
highest incidence worldwide, 22 per 100,000.
Amrit Kaur MB ChB MRCPCH BSc Hons is a Nephrology Specialist Registrar in
Birmingham Children’s Hospital, Steelhouse Lane, Birmingham UK.
Conflict of interest: none declared.
Larissa Kerecuk MBBS BSc MRCPCH FRCPCH is a Consultant Paediatric
Nephrologist at Birmingham Children’s Hospital, Steelhouse Lane,
Birmingham, UK. Conflict of interest: none declared.
PAEDIATRICS AND CHILD HEALTH 22:8 332
Definition
Swiss haematologist Conrad von Gasser first described HUS in
1955. He used the term to describe the combined symptoms of
diarrhoea, haemolytic anaemia, thrombocytopenia and acute
renal failure (ARF), which he observed in five children. This
description is still valid today however HUS is further subdivided
into two broad categories:
� Typical, usually diarrhoea positive D þ HUS (more than
90% of cases)
� Atypical, usually diarrhoea negative D � HUS or aHUS
(approximately 5% of cases)
Please refer to Table 1 for common causes of each category.
The D þ HUS is the most common cause of ARF in childhood.
Haemolytic anaemia is defined as a haemoglobin level <10
g/dlitre and fragmented erythrocytes on blood film, thrombocy-
topenia with a platelet count <150 � 109/litre, and ARF with
serum creatinine greater than the age-related range (more than
97th percentile) or glomerular filtration rate (GFR) <80 mlitre/
min/1.73 m2 by the Schwartz formula.
Epidemiology
The incidence of HUS is greatest in children under 5 years old
and then peaks again in the elderly. Studies suggest greatest risk
of developing HUS is in areas with high density of cattle. There is
a seasonal variation with majority of cases occurring in the
summer months.
Infections with Shiga toxin (Stx)-producing Escherichia coli
(STEC; also called verotoxin, VTEC) is the greatest risk factor.
E. coli 0157:H7 is the most prevalent serotype of STEC associated
with human disease worldwide. STEC colonizes animals without
causing disease. STEC are not part of the normal human gut flora
and transmission occurs mainly through ingestion of infected
food or water, person to person spread and animal contact.
Contaminated ground beef, unpasteurized milk products, vege-
tables, drinking water and petting of farm animals have been the
source of infection in previous outbreaks. Isolated cases can also
occur. Inoculation with 100 organisms is sufficient enough to
cause disease. The incubation period is 1e8 days, although
asymptomatic infection may occur. Shedding of the bacterium
may persist for more than 3 weeks after infection.
Approximately 10% of children exposed to STEC will develop
gastrointestinal symptoms. Of these children, 3e7% (isolated
cases) or up to 20% in outbreaks will develop HUS.
Pathology, pathogenesis and applied physiology
Understanding of the pathogenesis of HUS allows the clinician
a logical approach and explanation of the presenting symptoms
and complications seen in severe HUS.
Histological appearance of HUS shows widespread thrombotic
microangiopathy (TMA) in renal glomeruli, the gastrointestinal
tract, the brain, and the pancreas. TMA describes the process of
vessel wall thickening, namely at arteriolar-capillary junction,
with swelling or detachment from the basement membrane.
Intraluminal thrombosis occurs leading to partial or complete
obstruction of the vessel lumen. Thrombosis can also be seen in
the hilum of the glomeruli and interlobular arteries. Cortical
necrosis can occur in extreme cases.
� 2012 Elsevier Ltd. All rights reserved.
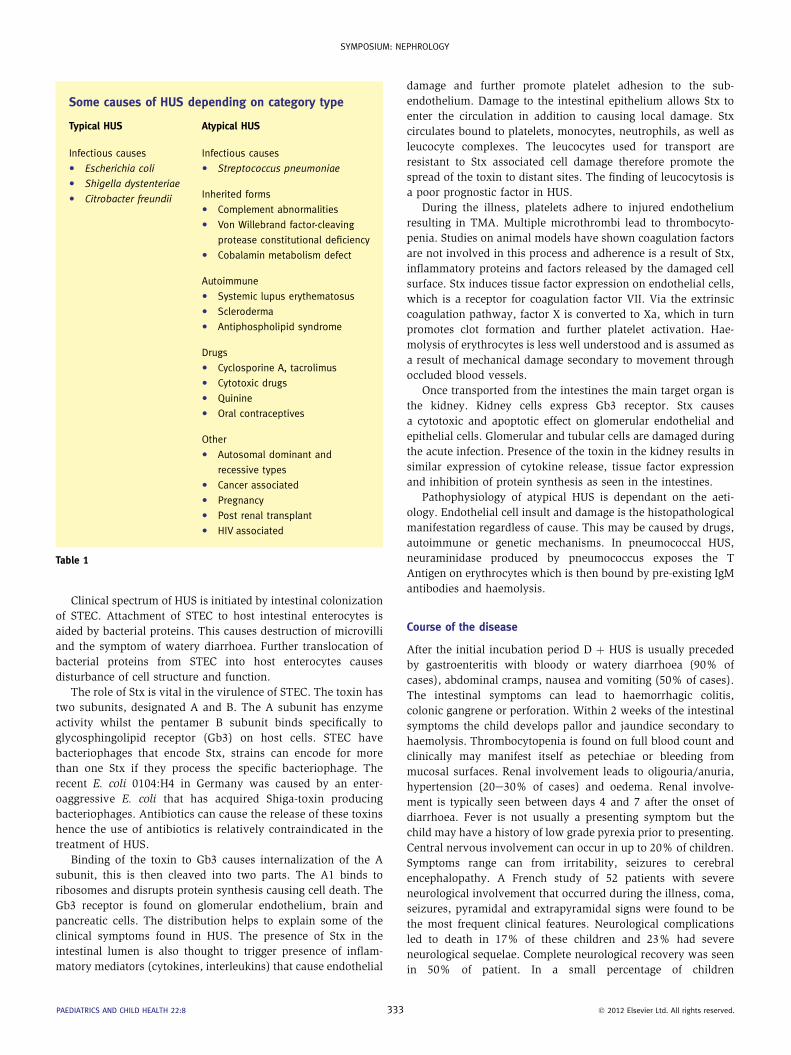
Some causes of HUS depending on category type
Typical HUS Atypical HUS
Infectious causes
C Escherichia coli
C Shigella dystenteriae
C Citrobacter freundii
Infectious causes
C Streptococcus pneumoniae
Inherited forms
C Complement abnormalities
C Von Willebrand factor-cleaving
protease constitutional deficiency
C Cobalamin metabolism defect
Autoimmune
C Systemic lupus erythematosus
C Scleroderma
C Antiphospholipid syndrome
Drugs
C Cyclosporine A, tacrolimus
C Cytotoxic drugs
C Quinine
C Oral contraceptives
Other
C Autosomal dominant and
recessive types
C Cancer associated
C Pregnancy
C Post renal transplant
C HIV associated
Table 1
SYMPOSIUM: NEPHROLOGY
Clinical spectrum of HUS is initiated by intestinal colonization
of STEC. Attachment of STEC to host intestinal enterocytes is
aided by bacterial proteins. This causes destruction of microvilli
and the symptom of watery diarrhoea. Further translocation of
bacterial proteins from STEC into host enterocytes causes
disturbance of cell structure and function.
The role of Stx is vital in the virulence of STEC. The toxin has
two subunits, designated A and B. The A subunit has enzyme
activity whilst the pentamer B subunit binds specifically to
glycosphingolipid receptor (Gb3) on host cells. STEC have
bacteriophages that encode Stx, strains can encode for more
than one Stx if they process the specific bacteriophage. The
recent E. coli 0104:H4 in Germany was caused by an enter-
oaggressive E. coli that has acquired Shiga-toxin producing
bacteriophages. Antibiotics can cause the release of these toxins
hence the use of antibiotics is relatively contraindicated in the
treatment of HUS.
Binding of the toxin to Gb3 causes internalization of the A
subunit, this is then cleaved into two parts. The A1 binds to
ribosomes and disrupts protein synthesis causing cell death. The
Gb3 receptor is found on glomerular endothelium, brain and
pancreatic cells. The distribution helps to explain some of the
clinical symptoms found in HUS. The presence of Stx in the
intestinal lumen is also thought to trigger presence of inflam-
matory mediators (cytokines, interleukins) that cause endothelial
PAEDIATRICS AND CHILD HEALTH 22:8 333
damage and further promote platelet adhesion to the sub-
endothelium. Damage to the intestinal epithelium allows Stx to
enter the circulation in addition to causing local damage. Stx
circulates bound to platelets, monocytes, neutrophils, as well as
leucocyte complexes. The leucocytes used for transport are
resistant to Stx associated cell damage therefore promote the
spread of the toxin to distant sites. The finding of leucocytosis is
a poor prognostic factor in HUS.
During the illness, platelets adhere to injured endothelium
resulting in TMA. Multiple microthrombi lead to thrombocyto-
penia. Studies on animal models have shown coagulation factors
are not involved in this process and adherence is a result of Stx,
inflammatory proteins and factors released by the damaged cell
surface. Stx induces tissue factor expression on endothelial cells,
which is a receptor for coagulation factor VII. Via the extrinsic
coagulation pathway, factor X is converted to Xa, which in turn
promotes clot formation and further platelet activation. Hae-
molysis of erythrocytes is less well understood and is assumed as
a result of mechanical damage secondary to movement through
occluded blood vessels.
Once transported from the intestines the main target organ is
the kidney. Kidney cells express Gb3 receptor. Stx causes
a cytotoxic and apoptotic effect on glomerular endothelial and
epithelial cells. Glomerular and tubular cells are damaged during
the acute infection. Presence of the toxin in the kidney results in
similar expression of cytokine release, tissue factor expression
and inhibition of protein synthesis as seen in the intestines.
Pathophysiology of atypical HUS is dependant on the aeti-
ology. Endothelial cell insult and damage is the histopathological
manifestation regardless of cause. This may be caused by drugs,
autoimmune or genetic mechanisms. In pneumococcal HUS,
neuraminidase produced by pneumococcus exposes the T
Antigen on erythrocytes which is then bound by pre-existing IgM
antibodies and haemolysis.
Course of the disease
After the initial incubation period D þ HUS is usually preceded
by gastroenteritis with bloody or watery diarrhoea (90% of
cases), abdominal cramps, nausea and vomiting (50% of cases).
The intestinal symptoms can lead to haemorrhagic colitis,
colonic gangrene or perforation. Within 2 weeks of the intestinal
symptoms the child develops pallor and jaundice secondary to
haemolysis. Thrombocytopenia is found on full blood count and
clinically may manifest itself as petechiae or bleeding from
mucosal surfaces. Renal involvement leads to oligouria/anuria,
hypertension (20e30% of cases) and oedema. Renal involve-
ment is typically seen between days 4 and 7 after the onset of
diarrhoea. Fever is not usually a presenting symptom but the
child may have a history of low grade pyrexia prior to presenting.
Central nervous involvement can occur in up to 20% of children.
Symptoms range can from irritability, seizures to cerebral
encephalopathy. A French study of 52 patients with severe
neurological involvement that occurred during the illness, coma,
seizures, pyramidal and extrapyramidal signs were found to be
the most frequent clinical features. Neurological complications
led to death in 17% of these children and 23% had severe
neurological sequelae. Complete neurological recovery was seen
in 50% of patient. In a small percentage of children
� 2012 Elsevier Ltd. All rights reserved.
SYMPOSIUM: NEPHROLOGY
cardiomyopathy and pancreatitis may also be a feature. Please
refer to Table 2 for a list of clinical features associated with each
system involved.
Duration of symptoms to recovery is variable, usually 1e3
weeks after onset. Onset of improvement is depicted by a rise in
platelet count. Haematological improvement is followed by renal
function recovery.
Diagnosis, history and physical examination
In order to make the diagnosis a standard paediatric history
together with emphasis on fluid balance is essential. Specifically
ask about gastrointestinal symptoms and losses. Toleration of
oral fluids and micturition should be documented. Exploration of
ingestion of infected food products, farm animal contact and
person to person spread is essential.
Examination should include height, weight and body surface
area calculation. Vital signs including blood pressure must be
measured. In view of potential complications of HUS, the
cardiovascular, respiratory, abdominal, and central nervous
systems should be examined, paying particular attention to
hydration status and acute abdominal signs. Regular examina-
tion during hospital admission is essential to allude to clinical
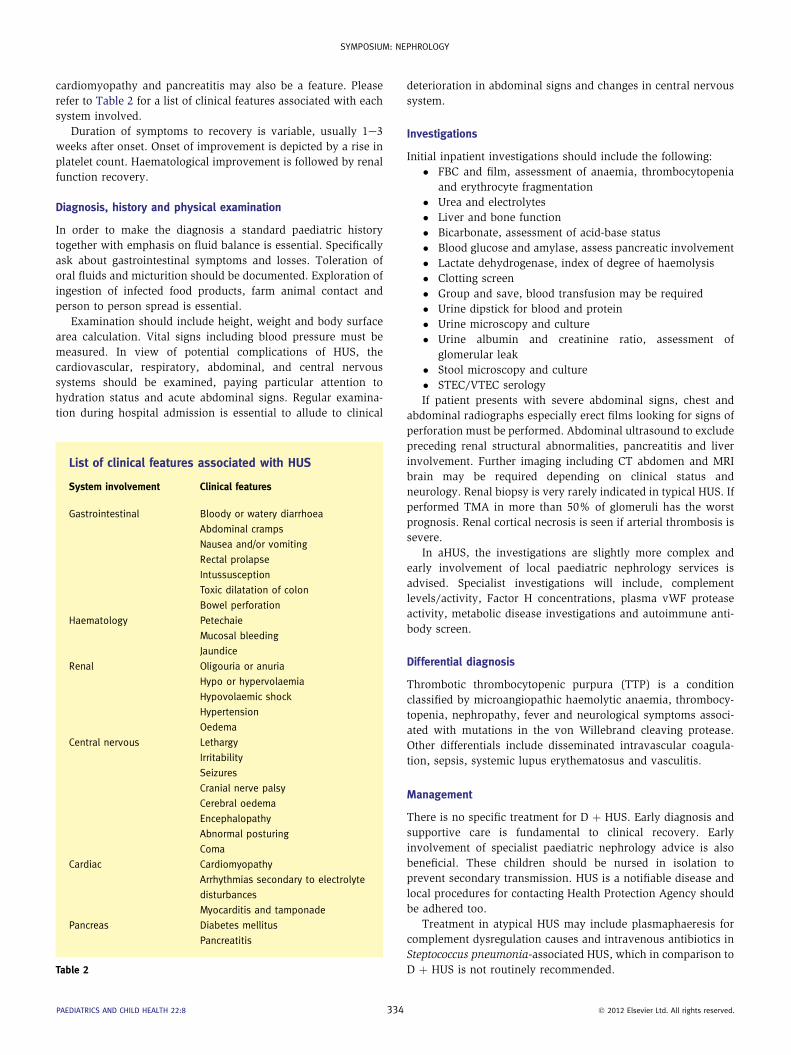
List of clinical features associated with HUS
System involvement Clinical features
Gastrointestinal Bloody or watery diarrhoea
Abdominal cramps
Nausea and/or vomiting
Rectal prolapse
Intussusception
Toxic dilatation of colon
Bowel perforation
Haematology Petechaie
Mucosal bleeding
Jaundice
Renal Oligouria or anuria
Hypo or hypervolaemia
Hypovolaemic shock
Hypertension
Oedema
Central nervous Lethargy
Irritability
Seizures
Cranial nerve palsy
Cerebral oedema
Encephalopathy
Abnormal posturing
Coma
Cardiac Cardiomyopathy
Arrhythmias secondary to electrolyte
disturbances
Myocarditis and tamponade
Pancreas Diabetes mellitus
Pancreatitis
Table 2
PAEDIATRICS AND CHILD HEALTH 22:8 334
deterioration in abdominal signs and changes in central nervous
system.
Investigations
Initial inpatient investigations should include the following:
� FBC and film, assessment of anaemia, thrombocytopenia
and erythrocyte fragmentation
� Urea and electrolytes
� Liver and bone function
� Bicarbonate, assessment of acid-base status
� Blood glucose and amylase, assess pancreatic involvement
� Lactate dehydrogenase, index of degree of haemolysis
� Clotting screen
� Group and save, blood transfusion may be required
� Urine dipstick for blood and protein
� Urine microscopy and culture
� Urine albumin and creatinine ratio, assessment of
glomerular leak
� Stool microscopy and culture
� STEC/VTEC serology
If patient presents with severe abdominal signs, chest and
abdominal radiographs especially erect films looking for signs of
perforation must be performed. Abdominal ultrasound to exclude
preceding renal structural abnormalities, pancreatitis and liver
involvement. Further imaging including CT abdomen and MRI
brain may be required depending on clinical status and
neurology. Renal biopsy is very rarely indicated in typical HUS. If
performed TMA in more than 50% of glomeruli has the worst
prognosis. Renal cortical necrosis is seen if arterial thrombosis is
severe.
In aHUS, the investigations are slightly more complex and
early involvement of local paediatric nephrology services is
advised. Specialist investigations will include, complement
levels/activity, Factor H concentrations, plasma vWF protease
activity, metabolic disease investigations and autoimmune anti-
body screen.
Differential diagnosis
Thrombotic thrombocytopenic purpura (TTP) is a condition
classified by microangiopathic haemolytic anaemia, thrombocy-
topenia, nephropathy, fever and neurological symptoms associ-
ated with mutations in the von Willebrand cleaving protease.
Other differentials include disseminated intravascular coagula-
tion, sepsis, systemic lupus erythematosus and vasculitis.
Management
There is no specific treatment for D þ HUS. Early diagnosis and
supportive care is fundamental to clinical recovery. Early
involvement of specialist paediatric nephrology advice is also
beneficial. These children should be nursed in isolation to
prevent secondary transmission. HUS is a notifiable disease and
local procedures for contacting Health Protection Agency should
be adhered too.
Treatment in atypical HUS may include plasmaphaeresis for
complement dysregulation causes and intravenous antibiotics in
Steptococcus pneumonia-associated HUS, which in comparison to
D þ HUS is not routinely recommended.
� 2012 Elsevier Ltd. All rights reserved.

SYMPOSIUM: NEPHROLOGY
General considerations
The majority of all children with D þ HUS develop some degree
of renal impairment. Approximately two thirds will require renal
replacement therapy (RRT). Those children who do not require
dialysis, fluid management is key to a successful outcome.
Regular assessment of hydration status, twice daily weight, strict
fluid balance and regular electrolyte measurements including
blood sugar must be routine. Daily fluid replacement regimen
should include insensible losses (400 mlitres/m2/day) plus total
24 h urine output, emphasis is on maintaining euvolaemia in the
acute phase. Choice of intravascular fluid replacement should be
governed by plasma electrolytes.
Packed red cell transfusion may be required in those with
a haemoglobin less than 7 g/dlitre or symptomatic anaemia.
Careful monitoring is required in view of potential fluid overload
and hyperkalaemia secondary to blood transfusion.
Platelet transfusions are generally not required. If count is
particularly low (less than 10 � 109/litre), episodes of active
bleeding or pre-operative correction, transfusions may be given.
Careful monitoring and treatment of hypertension should not
be overlooked in the management of these children. In the acute
phase, if hypertension persists after fluid overload has been dealt
with, antihypertensive therapy should be started with calcium-
channel blockers. Once, renal function has improved and if
hypertension is persistent, angiotensin converting enzyme
inhibitors (ACEi) and angiotensin II receptor blockers (ARBs) are
particularly useful especially if there is also proteinuria. Seizures
in central nervous disease should be managed in accordance
with advance paediatric life support (APLS) algorithms ensuring
that electrolyte, metabolic abnormalities and intracranial lesions
have been excluded.
Renal replacement therapy
RRT is required in those children who are fluid overloaded in
presence of oliguria, correction of electrolyte or acid-base
disturbances and symptomatic uraemia. Common electrolyte
disturbance include hyperkalaemia and hyponatraemia. Fluid
overload can lead on to pulmonary oedema and myocardial
insufficiency. The type of RRT offered is governed by clinical and
logistic factors. Peritoneal dialysis (PD) has the advantage of
avoiding large volume imbalances. Disadvantages include the
need for surgical placement of PD catheter. This may not be
possible in view of acute abdominal signs or impede ultrafiltra-
tion during acute enterocolitis. Haemodialysis (HD) has the
advantages of potentially being available without the need for
abdominal surgery however central venous catheters must be
placed in order to perform HD. Disadvantages include the need
for anticoagulation, haemodynamic instability and additional
loss of blood and platelets in the extracorporeal circulation.
Continuous haemofiltration can be instituted in cases of hae-
modynamic instability.
Renal transplant in D þ HUS is rare. If transplant is required
recurrence of the disease in the transplanted kidney is again rare
(approximately 1%) and transplantation can be performed
without increased risk of failure.
Other treatments
Nutritional support and early involvement of dietetic support is
particularly important to prevent a catabolic state during
PAEDIATRICS AND CHILD HEALTH 22:8 335
protracted illnesses. Antimotility agents and nonsteroidal anti-
inflammatory analgesics (NSAIDs) are not recommended in the
management of D þ HUS. Antimotility agents have been asso-
ciated with higher rates of HUS and NSAIDs increase the risk of
gastrointestinal bleeding and reduce renal perfusion thereby
affecting GFR.
Antibiotics are not recommended as part of the treatment.
Experimental data has shown certain classes of antibiotics,
trimethoprim, sulfamethoxazole, and quinolones stimulate the
bacterial Shiga toxin expression and release. Other studies have
shown antibiotic administration does not increase the risk of HUS.
In view of the disparity between studies the general consensus is
not to administer antibiotics as part of routine management.
Plasma infusions and therapeutic plasma exchange have no
proven beneficial role in D þ HUS although there are limited
studies to support the use of plasma exchange in D þ HUS with
central nervous system involvement.
Future treatment options
Anti-Shiga toxin antibodies have been shown to prevent HUS in
animals. The monoclonal antibodies are intended to neutralize
the circulating Stx. Healthy adults have been exposed to mono-
clonal antibodies, no serious adverse events were reported. In
2003 a randomized, double blind, placebo-controlled study was
initiated in Canada and Argentina. Children with STEC positive
stools were randomized. Children were treated within 72 h of the
onset of bloody diarrhoea and then followed up for 4 months.
The study concentrated on the safety and pharmokinetics of the
humanized monoclonal antibody (Urtoazumab) as a therapy
against paediatric patients infected with Shiga toxin. The study
showed no serious adverse effects of administering the mono-
clonal antibody and there was no evidence of human antibodies
against the monoclonal antibody after treatment. No comment
was made on the clinical benefit of administering Urtoazumab in
paediatric patients with D þ HUS.
Eculizimab is a monoclonal antibody against complement
factor 5 and has been used in the recent DþHUS outbreak in
Germany with anedoctal beneficial reports. However, a RCT is
required to establish its usefulness in this setting.
Prognosis and explanation to patient
D þ HUS generally has a good prognosis. Early recognition and
treatment including dialysis has improved disease outcomes.
Acute mortality rate is 5e10% in D þ HUS. Long term complica-
tions after initial disease are seen in approximately 25% of
patients. Complications include persistent proteinuria, arterial
hypertension, neurological impairment, diabetes mellitus, and
chronic renal failure. End stage renal failure occurs in 1.8% of
these children.
Poor prognostic factors for long term renal complications
include;
� leucocytosis gt; 20 � 109/litre with neutrophilia
� shock during acute illness
� anuria for more than 2 weeks
� dialysis for more than 4 weeks is unlikely to lead to full
renal recovery
� hypertension
� persistent proteinuria
� 2012 Elsevier Ltd. All rights reserved.

Practice points
C HUS is the combined symptoms of diarrhoea, haemolytic
anaemia, thrombocytopenia and acute renal failure (ARF).
Typical HUS, usually diarrhoea positive DþHUS (more than 90%
of cases), atypical HUS, usually diarrhoea negative D � HUS or
aHUS (approximately 5% of cases)
C The D þ HUS is the most common cause of ARF in childhood
C E. coli 0157:H7 is the most prevalent serotype of STEC asso-
ciated with human disease worldwide
C Approximately 10% of children exposed to STEC will develop
gastrointestinal symptoms. Of these children, 3e7% (isolated
cases) or up to 20% in outbreaks will develop HUS
C Histological appearance of HUS shows widespread thrombotic
microangiopathy (TMA) in renal glomeruli, the gastrointestinal
tract, the brain, and the pancreas
C Duration of symptoms to recovery is variable, usually 1e3
weeks after onset. Onset of improvement is depicted by a rise
in platelet count
C There is no specific treatment for Dþ HUS. RRT is required in those
childrenwhoarefluidoverloaded inpresenceofoliguria, correction
of electrolyte or acid-base disturbances and symptomatic uraemia
C Long term complications after initial disease are seen in
approximately 25% of patients
SYMPOSIUM: NEPHROLOGY
� central nervous involvement
� severe colitis and/or rectal prolapse
� cortical necrosis and TMA (more than 50% glomeruli
involved) on renal biopsy
� atypical HUS
It is important to follow up cases of even mild HUS. In a study
in which 130 children with D þ HUS not requiring dialysis during
the acute illness, 3.8% and 11.5% had proteinuria or hyperten-
sion, respectively. Nearly one fifth had microalbuminuria after
12 years from the onset of disease.
In D � HUS, renal prognosis is significantly worse, with
nearly half of children developing end-stage renal failure (ESRF)
and a quarter dying in the acute period. Renal transplantation in
D þ HUS children has low recurrence risk of original illness. In
D � HUS depending on the aetiology, recurrence of illness in
transplanted organ may be extremely high especially in factor
deficiencies.
Follow up
Subsequent medical follow up after the initial admission will
depend on the severity of the disease. Those who have had
a milder form of HUS should be seen soon after discharge and
then annually to monitor for hypertension and proteinuria. This
service can be offered by the local paediatrician or general
practioner. Early referral to paediatric nephrologist is recom-
mended should the annual review highlight a concern.
Of those children that have had a more protracted illness, they
will remain under the care of the paediatric renal services and
other specialists depending on the complications of their illness.
Prevention
Hygienic measures are themost important factor in preventing the
disease. Avoiding ingestion of contaminated food by assuring
thorough cooking ofmeat products, correct pasteurization of dairy
products, and vegetables/fruit to be washed thoroughly. Young
children should avoid consumption of unpasturized food prod-
ucts. It seems extreme to prohibit the petting of farm animals,
however hand washing should be encouraged afterwards.
Person to person spread amongst children who attend nursery
again can be limited by ensuring adequate hand hygiene during
toileting.
Early involvement of the Health Protection Agency once a case
has been diagnosed is paramount in ascertaining the epidemiology
of the current case and prevent spread amongst the public. A
FURTHER READING
Ariceta G, Besbas N, Johnson S, et al. Guideline for the investigation and
initial therapy of diarrhea-negative hemolytic uremic syndrome.
Pediatric Nephrology April 2009; 24: 687e96.
Bitzan M, Schaefer F, Reymond D. Treatment of typical (enteropathic)
hemolytic uremic syndrome. Seminars in Thrombosis & Hemostasis
September 2010; 36: 594e610.
PAEDIATRICS AND CHILD HEALTH 22:8 336
Garg AX, Suri RS, Barrowman N, et al. Long-term renal prognosis of
diarrhea-associated haemolytic uremic syndrome. JAMA September
10, 2003; 290: 1360e70.
Gianviti A, Tozzi AE, De Petris L. Risk factors for poor renal prognosis in
children with hemolytic uremic syndrome. Pediatric Nephrology
December 2003; 18: 1229e35.
Karpman D. Haemolytic uraemic syndrome and thrombotic thrombocy-
topenic purpura. Current Paediatrics 2002; 12: 569e74.
KarpmanD, Sartz L, Johnson S. Pathophysiology of typical hemolytic uremic
syndrome. Seminars in Thrombosis andHemostasis 2010; 36: 575e85.
Lynn RM, O’Brien SJ, Taylor CM, et al. Childhood hemolytic uremic
syndrome, United Kingdom and Ireland. Emerging Infectious Diseases
April 2005; 11: 590e6.
Nathanson S, Kwon T, Elmaleh M, et al. Acute neurological involvement in
diarrhea-associated hemolytic uremic syndrome. Clinical Journal of
The American Society of Nephrology July 2010; 5: 1218e28.
Rees L, Webb NJA, Brogan PA. Haemolytic uraemic syndrome. In: Oxford
specialist handbooks in paediatrics: paediatric nephrology. Oxford:
Oxford University Press, 2007. 384e391.
Scheiring J, Andreoli SP, Zimmerhacki LB. Treatment and outcome of
Shiga-toxin-associated hemolytic uremic syndrome (HUS). Pediatric
Nephrology 2008; 23: 1749e60.
Scheiring J, Rosales A, Zimmerhackl LB. Today’s understanding of the
haemolytic uraemic syndrome. European Journal of Pediatrics January
2010; 169: 7e13.
Waters AM, Kerecuk L, Luk D, et al. Hemolytic uremic syndrome associated
with invasive pneumococcal disease: the United kingdom experience.
Journal of Pediatrics August 2007; 151: 140e4.
� 2012 Elsevier Ltd. All rights reserved.


![Atypical haemolytic uraemic syndrome (aHUS) - eculizumab ...Atypical haemolytic uraemic syndrome (aHUS) - eculizumab [ID703] | Guidance and guidelines | NICE](https://img.pdfslide.us/doc/110x75/5ed0f8912b6d4e0fbe17d4a1/atypical-haemolytic-uraemic-syndrome-ahus-eculizumab-atypical-haemolytic.jpg)