Embed Size (px)
Citation preview

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
HAB HIV Core Clinical Performance Measures for
Adult/Adolescent Clients: Group 1
Performance Measure: ARV Therapy for Pregnant Women
OPR-Related Measure: Yes www.hrsa.gov/performancereview/measures.htm
Percentage of pregnant women with HIV infection who are prescribed antiretroviral therapy
Numerator: Number of HIV-infected pregnant women who were prescribed antiretroviral therapy during the 2nd and 3rd trimester
Denominator: Number of HIV-infected pregnant women who had a medical visit with a provider with prescribing privileges1, i.e. MD, PA, NP at least once in the measurement year
Patient Exclusions:
1. Patients whose pregnancy is terminated 2. Pregnant patients who are in the 1st trimester and newly enrolled in care during last
three months of the measurement year
Data Element:
1. Is the client HIV-infected? (Y/N) a. If yes, is the client female? (Y/N)
i. If yes, was she pregnant during the reporting period? (Y/N) 1. If yes, was she on antiretroviral therapy during this
reporting period? (Y/N)
Data Sources:
• Ryan White Program Data Report, Section 5, Item 53 may provide data useful in establishing a baseline for this performance measure
• Electronic Medical Record/Electronic Health Record • CAREWare, Lab Tracker, or other electronic data base • Medical record data abstraction by grantee of a sample of records
National Goals, Targets, or Benchmarks for Comparison:
None available at this time.
Outcome Measures for Consideration:
° Rate of perinatal transmission in the measurement year ° Number of events of perinatal transmission in the measurement year
Basis for Selection and Placement in Group 1: Treatment recommendations for pregnant women infected with HIV-1 have been based on the belief that therapies of known benefit to women should not be withheld during pregnancy unless there are known adverse effects on the mother, fetus, or infant and unless these adverse effects outweigh the benefit to the woman. Antiretroviral therapy can reduce perinatal HIV-1 transmission by nearly 70%.2
Measure reflects important aspect of care that significantly impacts survival, mortality and hinders transmission. Data collection is currently feasible and measure has a strong evidence base supporting the use. US Public Health Service Guidelines: Health-care providers considering the use of antiretroviral agents for HIV-1 infected women during pregnancy must take into account two separate but related issues:
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
• Antiretroviral treatment of maternal HIV-1 infection, and • Antiretroviral chemoprophylaxis to reduce the risk for perinatal HIV-1 transmission
The benefits of antiretroviral therapy for a pregnant woman must be weighed against the risk of adverse events to the woman, fetus, and newborn. Although ZDV chemoprophylaxis alone has substantially reduced the risk for perinatal transmission, antiretroviral monotherapy is now considered suboptimal for treatment of HIV-1 infection, and combination drug regimens are considered the standard of care for therapy. Initial evaluation of an infected pregnant woman should include an assessment of HIV-1 disease status and recommendations regarding antiretroviral treatment or alteration of her current antiretroviral regimen. This assessment should include the following: • Evaluation of the degree of existing immunodeficiency determined by CD4 T-cell count, • Risk for disease progression as determined by the level of plasma RNA, • History of prior or current antiretroviral therapy, • Gestational age, and • Supportive care needs. Decisions regarding initiation of therapy should be the same for women who are not currently receiving antiretroviral therapy and for women who are not pregnant, with the additional consideration of the potential impact of such therapy on the fetus and infant. Further, use of ZDV alone should not be denied to a woman who wishes to minimize exposure of the fetus to other antiretroviral drugs and therefore, after counseling, chooses to receive only ZDV during pregnancy to reduce the risk for perinatal transmission.1
References/Notes: 1A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 2Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV-1 Transmission in the United States (http://aidsinfo.nih.gov/ContentFiles/PerinatalGL.pdf)
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
Performance Measure: CD4 T-Cell Count OPR-Related Measure: Yes www.hrsa.gov/performancereview/measures.htm
Percentage of clients with HIV infection who had 2 or more CD4 T-cell counts performed in the measurement year
Numerator: Number of HIV-infected clients who had 2 or more CD4 T-cell counts performed at least 3 months apart during the measurement year
Denominator: Number of HIV-infected clients who had a medical visit with a provider with prescribing privileges1, i.e. MD, PA, NP at least once in the measurement year
Patient Exclusions: 1. Patients newly enrolled in care during last six months of the year
Data Element:
1. Is the client HIV-infected? (Y/N) a. If yes, did the client have a CD4 count test conducted during the
reporting period? (Y/N) a. If yes, list the quarters of these tests
Data Sources:
• Electronic Medical Record/Electronic Health Record • CAREWare, Lab Tracker, or other electronic data base • HIVQUAL reports on this measure for grantee under review • Medical record data abstraction by grantee of a sample of records
National Goals, Targets, or Benchmarks for Comparison
IHI Goal: 90%2
National HIVQUAL Data: 3 2003 2004 2005 2006
Top 10% 87.2% 87.7% 90.3% 87.5% Top 25% 74.2% 78.0% 76.6% 78.8% Median* 61.0% 62.7% 63.9% 62.5%
*from HAB data base
Outcome Measures for Consideration
° Rate of opportunistic infections in the measurement year ° Rate of clients with progression to AIDS in the measurement year ° Mortality rates
Basis for Selection and Placement in Group 1:
The CD4 T-cell count plays a vital role in determining the staging of HIV disease and indicating the need for prophylaxis against opportunistic infections. It continues to be used in decisions regarding initiation or adjustment of antiretroviral treatment.
The most recent CD4 T-cell count is the strongest predictor of subsequent disease progression and survival, according to clinical trials and cohort studies data on patients receiving antiretroviral therapy.4
Measure reflects important aspects of care that significantly impacts survival and mortality. Data collection is currently feasible and measure has a strong evidence base supporting the use. US Public Health Service Guidelines: " In general, CD4 T-cell count should be determined every three to six months to (1) determine when to start antiretroviral in patients who do not meet the criteria for initiation; (2) assess immunologic response to
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
antiretroviral therapy; and (3) assess the need for initiating chemoprophylaxis for opportunistic infections." 3
References/Notes: Guidelines state that CD4 T-cell counts should be measured at least every 3-4 months depending on the stage of the disease. The timeframe of 6 months was determined by clinical expert consensus for the purpose of this measure, but can and should be measured at more frequent intervals if needed. 1A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 2IHI Measure reads, “Percent of Patients/Clients with a CD4 Count Test in the Past 4 Months” (http://www.ihi.org/IHI/Topics/HIVAIDS/HIVDiseaseGeneral/Measures/Percentof+patientswithaCD4counttestinthepast4months.htm) 3National HIVQUAL data looks at the percent of clients who have a CD4 T-cell count done every four months, not every six months. (http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf) 4Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-infected adults and adolescents. Department of Health and Human Services. December 1, 2007; 1-143. Available at http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed December 12, 2007.
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
Performance Measure: HAART OPR-Related Measure: Yes www.hrsa.gov/performancereview/measures.htm
Percentage of clients with AIDS who are prescribed HAART
Numerator: Number of clients with AIDS who were prescribed a HAART regimen1 within the measurement year
Denominator:
Number of clients who: • have a diagnosis of AIDS (history of a CD4 T-cell count below 200 cells/mm3 or
other AIDS-defining condition2), and • had at least one medical visit with a provider with prescribing privileges3, i.e. MD,
PA, NP in the measurement year. Patient Exclusions: 1. Patients newly enrolled in care during last three months of the measurement year
Data Element:
1. Is the client diagnosed with CDC-defined AIDS? (Y/N) a. If yes, was the client prescribed HAART during the reporting period?
(Y/N)
Data Sources:
• Ryan White Program Data Report, Section 2, Items 26 and 31 may provide data useful in establishing a baseline for this performance measure
• Electronic Medical Record/Electronic Health Record • CAREWare, Lab Tracker, or other electronic data base. • HIVQUAL reports on this measure for grantee under review • Medical record data abstraction by grantee of a sample of records
National Goals, Targets, or Benchmarks for Comparison
IHI Goal: 90%4
CDC and HIVRN data consistent that 80% of those in care “eligible for ARVs” on tx. This includes CD4<350 and not just AIDS.5,6
National HIVQUAL Data:7,8
2003 2004 2005 2006 Top 10% 100% 100% 100% 100% Top 25% 100% 100% 100% 100% Median* 100% 88.9% 95.7% 100%
*from HAB data base
Outcome Measures for Consideration:
° Rate of opportunistic infections in the measurement year ° Rate of HIV-related hospitalizations in the measurement year ° Mortality rates
Basis for Selection and Placement in Group 1: “Randomized clinical trials provide strong evidence of improved survival and reduced disease progression by treating symptomatic patients and patients with CD4 T-cells <200 cells/mm3.”9
Measure reflects important aspect of care that significantly impacts survival, mortality and hinders transmission. Data collection is currently feasible and measure has a strong evidence base supporting the use.
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
US Public Health Service Guidelines: “Antiretroviral therapy is recommended for all patients with history of an AIDS-defining illness or severe symptoms of HIV infection regardless of CD4 T-cell count.” 10
References/Notes: 1Many authorities recommend two baseline CD4 T-cell measurements before decisions are made to initiate antiretroviral therapy because of wide variations in results. The test should be repeated yet a third time if discordant results are seen. The optimal time to initiate antiretroviral therapy among asymptomatic patients with CD4 T-cell counts >200 cells/mm3 is unknown. This measure focuses strictly on the subset of patients for whom antiretroviral therapy is unequivocally recommended—those with a CD4 T-cell count below 200 cells/mm3 or history of another AIDS-defining condition. Asymptomatic patients with CD4 T-cell counts of 201–350 cells/mm3 should be offered treatment. For asymptomatic patients with CD4 T-cell of >350 cells/mm3 and plasma HIV RNA >100,000 copies/ml most experienced clinicians defer therapy but some clinicians may consider initiating treatment. (See reference 8 below) 2AIDS Defining conditions are noted in CDC. 1993 Revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR 1992;41(no. RR-17). (http://www.cdc.gov/mmwr/preview/mmwrhtml/00018871.htm) 3A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 4IHI Measure reads, “Percent of Patients with Appropriate ARV Therapy Management” http://www.ihi.org/IHI/Topics/HIVAIDS/HIVDiseaseGeneral/Measures/PercentofPatientswithAppropriateARVTherapyManagement.htm) 5 Gebo, JAIDS January 2005, vol. 38, pp. 96-103. 6 Teshale Abstract #167, CROI 2005. 7 The National HIVQUAL data may not be directly comparable due to varying exclusions. Indicator definitions can be accessed at http://www.hivguidelines.org/Content.aspx?PageID=53. 8http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf9”HAART, CD4<200” (http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf) 10Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-infected adults and adolescents. Department of Health and Human Services. December 1, 2007; p. 9. Available at http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed December 12, 2007.
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
Performance Measure: Medical Visits OPR-Related Measure: Yes www.hrsa.gov/performancereview/measures.htm
Percentage of clients with HIV infection who had two or more medical visits in an HIV care setting in the measurement year
Numerator: Number of HIV-infected clients who had a medical visit with a provider with prescribing privileges1, i.e. MD, PA, NP, in an HIV care setting2 two or more times at least 3 months apart during the measurement year
Denominator: Number of HIV-infected clients who had a medical visit with a provider with prescribing privileges at least once in the measurement year
Patient Exclusions: 1. Patients newly enrolled in care during last six months of the year
Data Element:
1. Is the client HIV-infected? (Y/N) a. Did the client have at least 2 medical visits in an HIV care setting
during the reporting period? (Y/N) i. If yes, list the quarters of these visits
Data Sources:
• Ryan White Program Data Report, Section 5, Items 42 and 43 may provide data useful in establishing a baseline for this performance measure
• Electronic Medical Record/Electronic Health Record • CAREWare, Lab Tracker, or other electronic data base • HIVQUAL reports on this measure for grantee under review • Medical record data abstraction by grantee of a sample of records
National Goals, Targets, or Benchmarks for Comparison
None available at this time.
Outcome Measures for Consideration
° Rate of HIV-related hospitalizations in the measurement year ° Rate of HIV-related emergency room visits in the measurement year ° Rate of opportunistic infections in the measurement year ° Mortality rates
Basis for Selection and Placement in Group 1: Clinicians should schedule routine monitoring visits at least every 4 months for all HIV-infected patients who are clinically stable.3,4
Greater experience among primary care physicians in the care of persons with AIDS improves survival. 5
Measure reflects important aspects of care that significantly impacts mortality. Data collection is currently feasible and measure has a strong evidence base supporting the use. US Public Health Service Guidelines: In general, patients with early-stage disease are seen at 3-month intervals to undergo routine medical evaluation and monitoring of CD4 T-cell count, viral load and CBC. During the initial evaluation more frequent visits are common because there is so much information to transmit. Visits should also be more frequent when therapy is introduced and when the CD4 T-cell count is <200 cells/mm3 because complications
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
are more likely.6 Multiple studies have demonstrated that better outcomes are achieved in patients cared for by a clinician with expertise. This has been shown in terms of mortality, rate of hospitalizations, compliance with guidelines, cost of care, and adherence to medications. The definition of expertise in these studies has varied, but most rely on the number of patients actively managed. Based on this observation, the Panel recommends HIV primary care by a clinician with at least 20 HIV-infected patients and preferably at least 50 HIV-infected patients. Many authoritative groups have combined the recommendation based on active patients, along with fulfilling ongoing CME requirements on HIV-related topics. 7 References/Notes: Guidelines state that routine monitoring of HIV-infected patients should occur at least every 3-4 months depending on the stage of the disease. 7 The timeframe of 6 months was determined by clinical expert consensus for the purpose of this measure, but CD4 T-cell counts can and should be measured at more frequent intervals if needed. 1A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 2An HIV care setting is one which received Ryan White HIV/AIDS Treatment Modernization Act of 2006 funding to provide HIV care and has a quality management program in place to monitor the quality of care addressing gaps in quality of HIV care. 3New York State Department of Health. Primary care approach to the HIV-infected patient. New York: New York State Department of Health; 2004. p. 8. http://www.hivguideliens.org/Content.aspx?pageID=257[Accessed November 27, 2007]. 4AETC National Resource Center. Clinical Manual for Management of the HIV-Infected Adult http://www.aidsetc.org/pdf/AETC-CM_071007.pdf [Accessed November 27, 2007]. 5Kitahata MM, Van Rompaey SE, Dillingham PW, Koepsell TD, Deyo RA, Dodge W, Wagner EH. Primary care delivery is associated with greater physician experience and improved survival among persons with AIDS. J Gen Intern Med. 2003 Feb;18(2):157-8.6Bartlett JG, Cheever LW, Johnson MP, Paauw DS [eds]. A Guide to Primary Care of People with HIV/AIDS. Rockville(MD): US Department of Health and Human Services, Health Resources and Services Administration, HIV/AIDS Bureau; 2004, p. 167. http://hab.hrsa.gov/tools/primarycareguide/. [Accessed November 27, 2007]. 7Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-infected adults and adolescents. Department of Health and Human Services. December 1, 2007; 1-143. Available at http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf. Accessed December 12, 2007.
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
Performance Measure: PCP Prophylaxis OPR-Related Measure: Yes www.hrsa.gov/performancereview/measures.htm
Percentage of clients with HIV infection and a CD4 T-cell count below 200 cells/mm3 who were prescribed PCP prophylaxis
Numerator: Number of HIV-infected clients with CD4 T-cell counts below 200 cells/mm3 who were prescribed PCP prophylaxis
Denominator:
Number of HIV-infected clients who: • had a medical visit with a provider with prescribing privileges1, i.e. MD, PA, NP at
least once in the measurement year, and • had a CD4 T-cell count below 200 cells/mm3
Patient Exclusions:
1. Patients with CD4 T-cell counts below 200 cells/mm3 repeated within 3 months rose above 200 cells/mm3
2. Patients newly enrolled in care during last three months of the measurement year
Data Element:
1. Is the client HIV-infected? (Y/N) a. If yes, was the CD4 T-cell count <200 cells/mm3? (Y/N)
i. If yes, was PCP prophylaxis prescribed? (Y/N) 1. If no, was the CD4 count repeated within 3 months? (Y/N)
a. If yes, did it remain below 200 cells/mm3? (Y/N) i. If yes, was PCP prophylaxis prescribed?
(Y/N)
Data Sources:
• Electronic Medical Record/Electronic Health Record • CAREWare, Lab Tracker, or other electronic data base • HIVQUAL reports on this measure for grantee under review • Medical record data abstraction by grantee of a sample of records
National Goals, Targets, or Benchmarks for Comparison:
IHI Goal: 95%2
National HIVQUAL Data3: 2003 2004 2005 2006
Top 10% 100% 100% 100% 100% Top 25% 100% 100% 100% 100% Median* 93.3% 90.9% 92.3% 94.4%
*from HAB data base
Outcome Measures for Consideration:
° Rate of PCP in the measurement year ° Mortality rates ° Cost savings
Basis for Selection and Placement in Group 1: Pneumocystis pneumonia (PCP) is the most common opportunistic infection in people with HIV. Without treatment, over 85% of people with HIV would eventually develop PCP. It is a major cause of mortality among persons with HIV infection, yet is almost entirely preventable and treatable. Pneumocystis almost always affects the lungs, causing a form of pneumonia. People with CD4 T-cell counts under 200 cells/mm3
July 2008

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 1
are at greatest risk of developing PCP. The drugs now used to prevent and treat PCP include TMP/SMX, dapsone, pentamidine, and atovaquone.4 Before the widespread use of primary PCP prophylaxis and effective ART, PCP occurred in 70%--80% of patients with AIDS. The course of treated PCP was associated with a mortality rate of between 20% and 40% in persons with profound immunosuppression. Approximately 90% of cases occurred among patients with CD4 T-cell counts <200 cells/mm3. 5
Measure reflects important aspect of care that significantly impacts survival and mortality. Data collection is currently feasible and measure has a strong evidence base supporting the use. US Public Health Service Guidelines:
HIV-infected adults and adolescents, including pregnant women and those on HAART, should receive chemoprophylaxis against PCP if they have a CD4 T-cell count <200 cells/mm3.6
References/Notes: 1A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 2 IHI Measure reads, “Percent of Patients with a CD4 Cell Count Below 200 cells/mm3 Receiving Pneumocystis Carinii Pneumonia (PCP) Prophylaxis” 3(http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf) 4 http://www.aidsinfonet.org/factsheet_detail.php?fsnumber=5155 Centers for Disease Control and Prevention. Treating opportunistic infections among HIV-infected adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV Medicine Association/Infectious Diseases Society of America. MMWR 2004;53(No. RR-15) ( http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5315a1.htm) 6 Centers for Disease Control and Prevention. Guidelines for Preventing Opportunistic Infections Among HIV-Infected Persons — 2002 Recommendations of the U.S. Public Health Service and the Infectious Diseases Society of America. MMWR 2002;51 (No. RR-8) (http://www.cdc.gov/mmwr/PDF/rr/rr5108.pdf or http://aidsinfo.nih.gov/ContentFiles/OIpreventionGL.pdf)
July 2008
HAB HIV Core Clinical Performance Measures: Adult/Adolescent Clients Group 2
HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 2
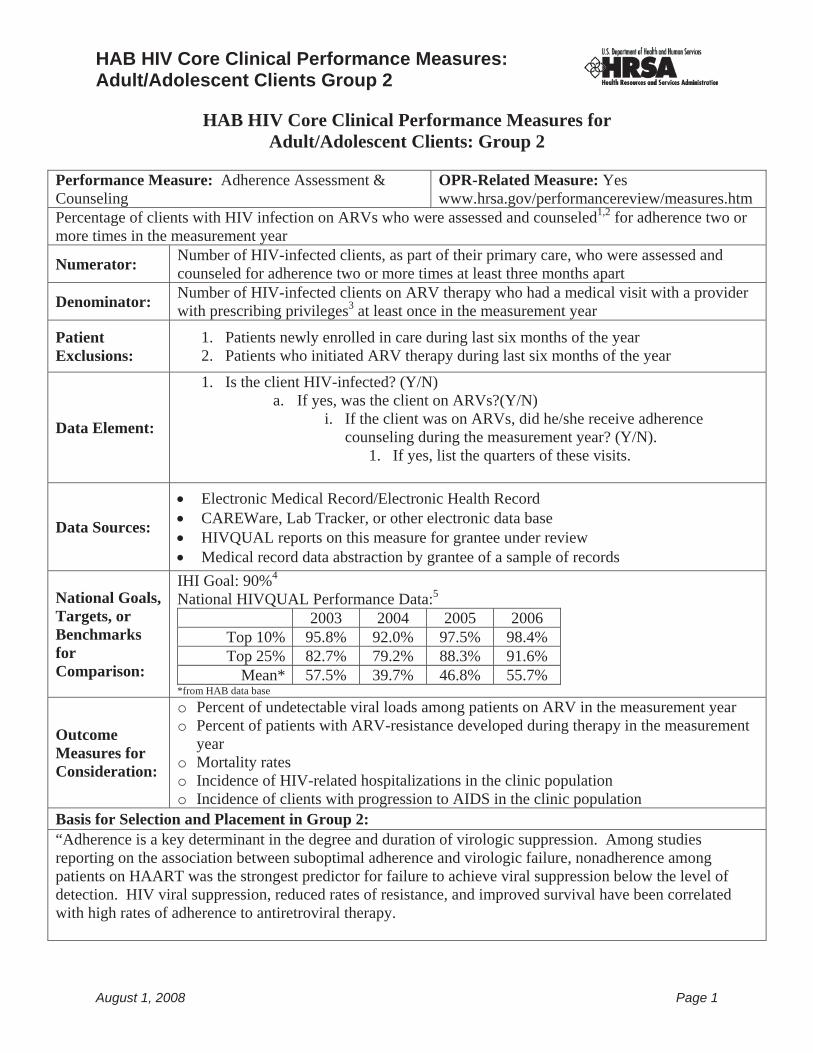
Performance Measure: Adherence Assessment & Counseling
OPR-Related Measure: Yes www.hrsa.gov/performancereview/measures.htm
Percentage of clients with HIV infection on ARVs who were assessed and counseled1,2 for adherence two or more times in the measurement year
Numerator: Number of HIV-infected clients, as part of their primary care, who were assessed and counseled for adherence two or more times at least three months apart
Denominator: Number of HIV-infected clients on ARV therapy who had a medical visit with a provider with prescribing privileges3 at least once in the measurement year
PatientExclusions:
1. Patients newly enrolled in care during last six months of the year 2. Patients who initiated ARV therapy during last six months of the year
Data Element:
1. Is the client HIV-infected? (Y/N) a. If yes, was the client on ARVs?(Y/N)
i. If the client was on ARVs, did he/she receive adherence counseling during the measurement year? (Y/N).
1. If yes, list the quarters of these visits.
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker, or other electronic data base HIVQUAL reports on this measure for grantee under review Medical record data abstraction by grantee of a sample of records
National Goals, Targets, or BenchmarksforComparison:
IHI Goal: 90%4
National HIVQUAL Performance Data:5
2003 2004 2005 2006Top 10% 95.8% 92.0% 97.5% 98.4%Top 25% 82.7% 79.2% 88.3% 91.6%
Mean* 57.5% 39.7% 46.8% 55.7%*from HAB data base
OutcomeMeasures for Consideration:
o Percent of undetectable viral loads among patients on ARV in the measurement year o Percent of patients with ARV-resistance developed during therapy in the measurement
yearo Mortality rates o Incidence of HIV-related hospitalizations in the clinic population o Incidence of clients with progression to AIDS in the clinic population
Basis for Selection and Placement in Group 2: “Adherence is a key determinant in the degree and duration of virologic suppression. Among studies reporting on the association between suboptimal adherence and virologic failure, nonadherence among patients on HAART was the strongest predictor for failure to achieve viral suppression below the level of detection. HIV viral suppression, reduced rates of resistance, and improved survival have been correlated with high rates of adherence to antiretroviral therapy.
August 1, 2008 Page 1

HAB HIV Core Clinical Performance Measures: Adult/Adolescent Clients Group 2
Prior to writing the first prescriptions, clinicians need to assess the patient’s readiness to take medication. Patients need to understand that the first regimen is the best chance for long-term success. Resources need to be identified to assist in success. Interventions can also assist with identifying adherence education needs and strategies for each patient.”6
Measure reflects important aspect of care that impacts HIV-related morbidity and focuses on treatment decisions that affect a sizable population. Although discussions of the importance of adherence to ARVs is important to begin prior to initiation of treatment, there is no standard of care for discussions to occur every 6 months for patients who may be years away from ARV treatment. US Public Health Guidelines:
"...adherence counseling and assessment should be done at each clinical encounter"7 (10/10/06)
References/Notes:1Assessment of adherence includes: 1) patient reports of adherence by: a) quantifiable scales, e.g. missed 3 out of 10 doses; b) qualitative scale, e.g. Likert scale; or 2) quantification such as pharmacy dispensing records, pill counts or direct observation therapy. 2Adherence counseling can be provided by any member of the multidisciplinary primary care team. 3A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 4IHI Measure reads, “Percent of Patients/Clients Assessed for Adherence to Antiretroviral (ARV) Therapy in the Past 4 Months” (http://www.ihi.org/IHI/Topics/HIVAIDS/HIVDiseaseGeneral/Measures/PercentofPatientsClientsAssessedforAdherencetoAntiretroviralARVTherapyinthePast4Months.htm)5(http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf)6Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents [April 7, 2005] (http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL04072005001.pdf)7Ibid
August 1, 2008 Page 2

HAB HIV Core Clinical Performance Measures: Adult/Adolescent Clients Group 2
Performance Measure: Lipid Screening OPR-Related Measure: NoPercentage of clients with HIV infection on HAART who had a fasting lipid panel1 during the measurement year
Numerator:Number of HIV-infected clients who:
were prescribed HAART, and had a fasting lipid panel in the measurement year
Denominator: Number of HIV-infected clients who are on HAART and who had a medical visit with a provider with prescribing privileges2 at least once in the measurement year
PatientExclusions: None
Data Element:
1. Is the client HIV-infected? (Y/N) a. If yes, was the client on HAART?(Y/N)
i. If the client was on HAART, did he/she have a fasting lipid panel during the measurement year? (Y/N)
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker, or other electronic data base HIVQUAL reports on this measure for grantee under review Medical record data abstraction by grantee of a sample of records
National Goals, Targets, or BenchmarksforComparison:
National HIVQUAL Data:3
2003 2004 2005 2006Top 10% 100% 100% 100% 100%Top 25% 100% 100% 97.9% 100%
Mean* 80.7% 79.1% 80.2% 84.7%*From HAB database
OutcomeMeasures for Consideration:
o Incidence of cardiovascular events in clinic population o Incidence of metabolic syndrome in the clinic population
Basis for Selection and Placement in Group 2: Changes in body shape, fat distribution & metabolism occur with frequency among HIV-infected patients, particularly those prescribed HAART. Metabolic changes that have been observed include hypertriglyceridemia, low high-density-lipoprotein (HDL) cholesterol and changes in LDL cholesterol.
Although rates of prevalence vary, studies have found the rate of prevalence for metabolic syndrome to be almost 25% in a population of patients taking HAART4, where metabolic syndrome is defined as the presence of at least 3 of the following: hypertriglyceridemia, low high-density lipoprotein cholesterol, hypertension, abdominal obesity or high serum glucose.5
All patients should receive a lipid profile at least once a year in order to monitor general health. For patients on HAART, lipid level monitoring is important to detect side effects and to identify patients who may require
August 1, 2008 Page 13
HAB HIV Core Clinical Performance Measures: Adult/Adolescent Clients Group 2
treatment.
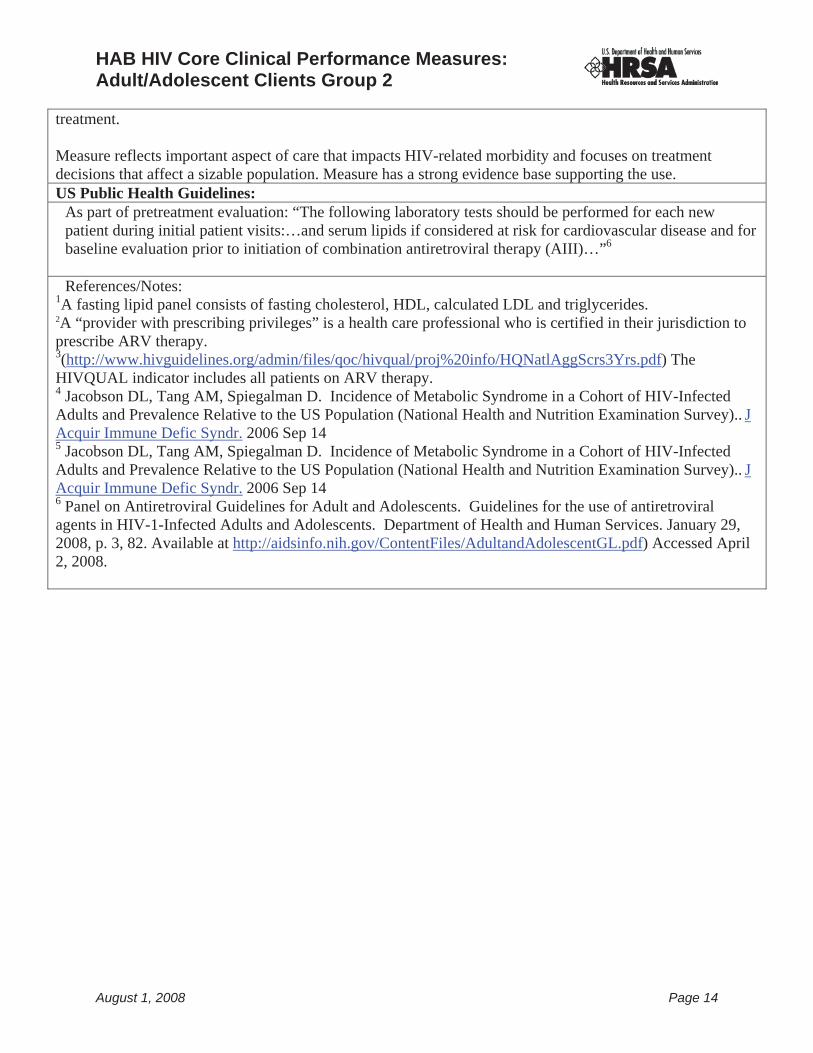
Measure reflects important aspect of care that impacts HIV-related morbidity and focuses on treatment decisions that affect a sizable population. Measure has a strong evidence base supporting the use. US Public Health Guidelines:
As part of pretreatment evaluation: “The following laboratory tests should be performed for each new patient during initial patient visits:…and serum lipids if considered at risk for cardiovascular disease and for baseline evaluation prior to initiation of combination antiretroviral therapy (AIII)…”6
References/Notes:1A fasting lipid panel consists of fasting cholesterol, HDL, calculated LDL and triglycerides. 2A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 3(http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf) The HIVQUAL indicator includes all patients on ARV therapy. 4 Jacobson DL, Tang AM, Spiegalman D. Incidence of Metabolic Syndrome in a Cohort of HIV-Infected Adults and Prevalence Relative to the US Population (National Health and Nutrition Examination Survey).. JAcquir Immune Defic Syndr. 2006 Sep 145 Jacobson DL, Tang AM, Spiegalman D. Incidence of Metabolic Syndrome in a Cohort of HIV-Infected Adults and Prevalence Relative to the US Population (National Health and Nutrition Examination Survey).. JAcquir Immune Defic Syndr. 2006 Sep 14 6 Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1-Infected Adults and Adolescents. Department of Health and Human Services. January 29, 2008, p. 3, 82. Available at http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf) Accessed April 2, 2008.
August 1, 2008 Page 14

HAB HIV Core Clinical Performance Measures: Adult/Adolescent Clients Group 2
Performance Measure: TB Screening OPR-Related Measure: No Percentage of clients with HIV infection who received testing with results documented for latent tuberculosis infection (LTBI) since HIV diagnosis
Numerator:Number of clients who received documented testing for LTBI with any approved test (tuberculin skin test [TST] or interferon gamma release assay [IGRA]) since HIV diagnosis
Denominator:
Number of HIV-infected clients who: do not have a history of previous documented culture-positive TB disease or previous documented positive TST or IGRA1; and had a medical visit with a provider with prescribing privileges2 at least once in the measurement year.
PatientExclusions None
Data Element:
1. Is the client HIV-infected? (Y/N) a. If yes, has the client ever had previous documented culture-positive TB
disease or previous documented positive TST or IGRA? (Y/N) i. If no, has the client ever been tested for LTBI with a TST or
IGRA since his/her HIV diagnosis? (Y/N) 1. If yes, are the results documented? (Y/N)
Data Sources:
Ryan White Program Data Report, Section 5, Item 47 may provide data useful in establishing a baseline for this performance measure
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker or other electronic data base HIVQUAL reports on this measure for grantee under review Medical record data abstraction by grantee of a sample of records.
National Goals, Targets, or BenchmarksforComparison
National HIVQUAL Data:3
2003 2004 2005 2006Top 10% 88.9% 91.7% 88.8% 92.2%Top 25% 77.4% 73.5% 74.8% 78.2%
Mean* 58.8% 56.0% 57.1% 56.2%*from HAB data base
OutcomeMeasures for Consideration
Incidence of TB disease in the clinic population
Basis for Selection and Placement in Group 2: HIV is the most important known risk factor for progression to TB disease from latent TB infection (LTBI) after exposure to infectious TB patients. There is a 2% to 8% TB risk per year within 5 years after LTBI for HIV-infected adults4,5 versus an 8% TB risk over 60 years for adults with LTBI but not HIV6. The TB risk for HIV-infected persons remains higher than for HIV-uninfected persons, even for HIV-infected persons who are taking antiretroviral medications.7,8 TB disease is an AIDS-defining opportunistic condition that can be deadly. McCombs found a 3 times adjusted odds of being diagnosed with TB at death and a 5 times adjusted
August 1, 2008 Page 19

HAB HIV Core Clinical Performance Measures: Adult/Adolescent Clients Group 2
odds of dying during TB treatment for HIV-infected TB patients compared with other patients from 1993 through 2001.9 Immunologic and virologic evidence now indicates that the host immune response to M.tuberculosis enhances HIV replication and might accelerate the natural progression of HIV infection.10
Providers should screen all HIV infected patients for TB and LTBI as soon as possible after HIV diagnosis. TB and LTBI testing should be conducted among HIV-infected persons regardless of duration of infection since they are at increased risk for progressing to TB disease. Thus, an HIV-infected person having a prior positive TST for which he/she did not complete treatment is still eligible for treatment. However, early identification and treatment of TB disease improves outcomes and reduces the risk of transmission. TB should be suspected in any patient who has had a persistent cough for more than 2 to 3 weeks, especially if the patient has at least one additional symptom, including fever, night sweats (sufficient to require changing of bed clothes or sheets), weight loss, or hemoptysis (coughing up blood). Identification of LTBI and completion of LTBI treatment reduces the risk of development of TB disease by 70 to 90 percent.11
Measure reflects important aspect of care that impacts HIV-related morbidity and mortality and focuses on treatment decisions that affect a sizable population. Measure has a strong evidence base supporting the use.US Public Health Guidelines: Guidelines for TB services for HIV-infected persons, such as those jointly published by the Public Health Service and the Infectious Diseases Society of America12 or by the Centers for Disease Control and Prevention (CDC)13 call for:
provision of a TST when HIV infection is first recognized,annual or periodic TSTs for HIV-infected persons who are initially TST-negative and belong to groups at substantial risk for TB exposure or if they experience immune reconstitution, chest radiographs and clinical evaluations to rule out active TB among those who are TST positive (reactions 5 mm) or who have symptoms (regardless of TST result), andLTBI treatment (once active TB has been excluded) for those having a positive TST or for those who are recent contacts of persons with infectious active TB14.
References/Notes:1Previous documented culture-positive TB disease or previous documented positive TST or IGRA occurred prior to HIV diagnosis. 2A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe ARV therapy. 3”PPD screening” (http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf4Markowitz N, Hansen NI, Hopewell PC, et al. Incidence of tuberculosis in the United States among HIV-infected persons. Annals of Internal Medicine. 1997;126:123-32. 5Selwyn PA, Hartel D, Lewis VA, et al. A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. New England Journal of Medicine. 1989;320:545-50.6Aronson NE, Santosham M, Comstock GW, et al. Long-term efficacy of BCG vaccine in American Indians and Alaska Natives: A 60-year follow-up study. Journal of the American Medical Association. 2004;291(17):2086-91.7The Antiretroviral therapy cohort collaboration. Incidence of tuberculosis among HIV-infected patients receiving highly active antiretroviral therapy in Europe and North America. Clinical Infectious Diseases. 2005;41:1772-1782.
August 1, 2008 Page 20

HAB HIV Core Clinical Performance Measures: Adult/Adolescent Clients Group 2
8Jones JL, Hanson DL, Dworkin MS, DeCock KM, and the Adult/Adolescent Spectrum of HIV Disease Group. HIV-associated tuberculosis in the era of highly active antiretroviral therapy. International Journal of TB and Lung Disease. 2000;4(11):1026-1031. 9McCombs SB. Tuberculosis mortality in the United States, 1993-2001. Oral presentation at CDC. Atlanta. December 2003. 10 Centers for Disease Control and Prevention. Prevention and treatment of tuberculosis among patients infected with human immunodeficiency virus: Principles of therapy and revised recommendations. MMWR Recomm Rep 1998 Oct 30;47(RR-20):1-58. 11American Thoracic Society/Centers for Diseases Control and Prevention/Infectious Diseases Society of America. Treatment of tuberculosis. Am J Respir Crit Care Med 2003;167:603-662 12 Centers for Disease Control and Prevention. Guidelines for Preventing Opportunistic Infections Among HIV-Infected Persons — 2002 Recommendations of the U.S. Public Health Service and the Infectious Diseases Society of America. MMWR 2002;51 (No. RR-8) (http://www.cdc.gov/mmwr/PDF/rr/rr5108.pdf or http://aidsinfo.nih.gov/ContentFiles/OIpreventionGL.pdf)13 Centers for Disease Control and Prevention. Prevention and treatment of tuberculosis among patients infected with human immunodeficiency virus: Principles of therapy and revised recommendations. MMWR Recomm Rep 1998 Oct 30;47(RR-20):1-58. 14Guidelines for the Investigation of Contacts of Persons with Infectious Tuberculosis Recommendations from the National Tuberculosis Controllers Association and CDC. MMWR December 16, 2005 / Vol. 54 / No. RR-15
August 1, 2008 Page 21

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
Performance Measure: Hepatitis/HIV Alcohol Counseling OPR-Related Measure: No Percentage of clients1 with HIV and Hepatitis B (HBV) or Hepatitis C (HCV) infection who received alcohol counseling2 within the measurement year
Numerator: Number of HIV-infected clients who received alcohol counseling
Denominator:
Number of HIV-infected clients who: were co-infected with HBV3 or HCV; andhad a medical visit with a provider with prescribing privileges4 at least once in the measurement period
PatientExclusions: None
Data Elements:
1. Is the client HIV-infected? (Y/N) a. If yes, is the client HBV or HCV-positive? (Y/N)
i. If yes, did the client receive alcohol counseling during the measurement year? (Y/N)
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker, or other electronic data base Medical record data abstraction by grantee of a sample of records Billing records
National Goals, Targets, or BenchmarksforComparison
None available at this time.
OutcomeMeasures for Consideration:
Hepatitis-related mortality rates in the clinic population
Basis for Selection and Placement in Group 3: Discussion of substance use allows the clinician to either provide counseling or make referrals to substance and alcohol treatment centers. A study of HIV positive veterans showed that hazardous drinking and alcohol diagnoses were associated with HIV disease progression and/or hepatic co-morbidity and anemia. It also concluded that alcohol problems are often missed by providers thus increasing the need for routine screening.5
Long-term studies of patients with chronic HCV infection show that between 2%-20% develop cirrhosis in 20 years. This rate of progression increases with older age, alcoholism and HIV infection.6
The measure is placed in Group 3 because the definition of “counseling” varies considerably across grantees.

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
The variation in definition impacts the feasibility of data collection. US Public Health Guidelines:
“All patients with HIV/HCV infection should be advised to avoid or limit alcohol consumption…”7
References/Notes:1 “Clients” refers to all clients aged 13 years and older. 2 For the purposes of this measure, alcohol counseling refers to counseling provided by the primary care team that emphasizes the need to avoid or limit alcohol intake due to the impact on the liver. 3 Markers of Hepatitis B infection include Hep B Surface Antigen, Hep B e Antigen, Hep B e Antibody or Hep B DNA. 4A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe medications. 5 Joseph Conigliaro, Adam J. Gordon, Kathleen A. McGinnis, Linda Rabeneck, and Amy C.; How Harmful Is Hazardous Alcohol Use and Abuse in HIV Infection: Do Health Care Providers Know Who Is at Risk?; Journal of Acquired Immune Deficiency Syndromes 33:521–525. 6 Centers for Disease Control and Prevention. Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents. June 18, 2008; 1-134.(http://aidsinfo.nih.gov/contentfiles/Adult_OI.pdf)
HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
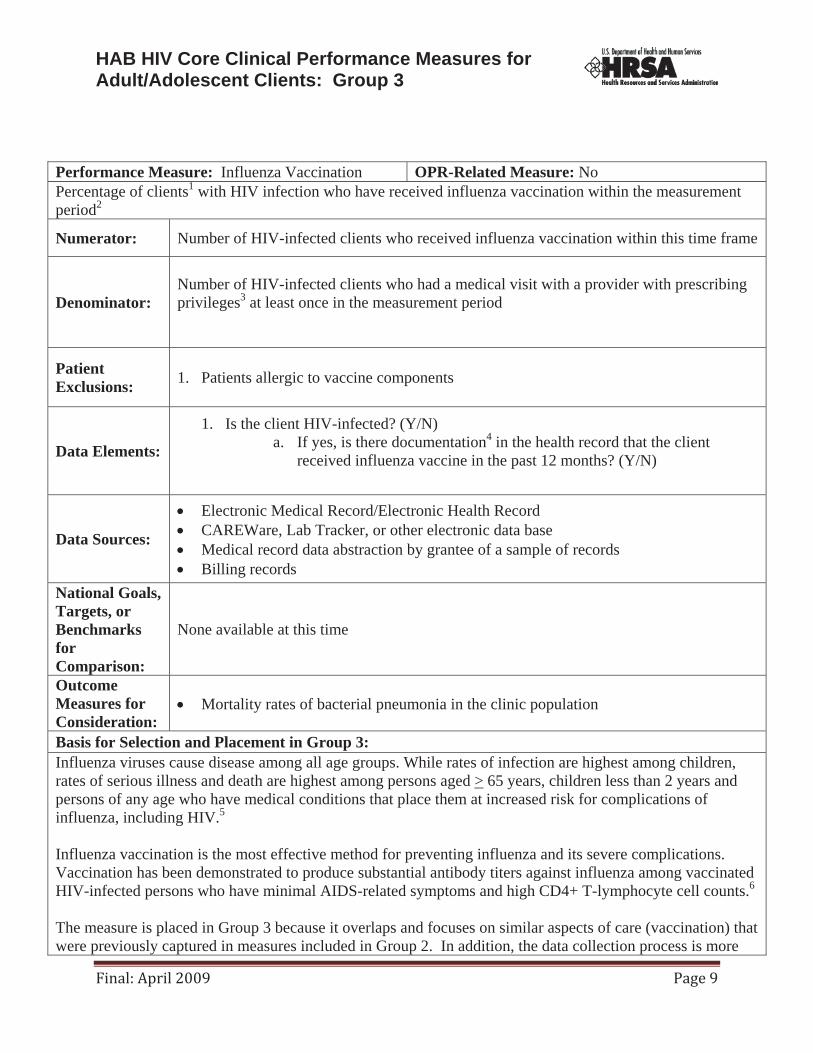
Performance Measure: Influenza Vaccination OPR-Related Measure: No Percentage of clients1 with HIV infection who have received influenza vaccination within the measurement period2
Numerator: Number of HIV-infected clients who received influenza vaccination within this time frame
Denominator:Number of HIV-infected clients who had a medical visit with a provider with prescribing privileges3 at least once in the measurement period
PatientExclusions: 1. Patients allergic to vaccine components
Data Elements:
1. Is the client HIV-infected? (Y/N) a. If yes, is there documentation4 in the health record that the client
received influenza vaccine in the past 12 months? (Y/N)
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker, or other electronic data baseMedical record data abstraction by grantee of a sample of records Billing records
National Goals, Targets, or BenchmarksforComparison:
None available at this time
OutcomeMeasures for Consideration:
Mortality rates of bacterial pneumonia in the clinic population
Basis for Selection and Placement in Group 3: Influenza viruses cause disease among all age groups. While rates of infection are highest among children, rates of serious illness and death are highest among persons aged > 65 years, children less than 2 years and persons of any age who have medical conditions that place them at increased risk for complications of influenza, including HIV.5
Influenza vaccination is the most effective method for preventing influenza and its severe complications. Vaccination has been demonstrated to produce substantial antibody titers against influenza among vaccinated HIV-infected persons who have minimal AIDS-related symptoms and high CD4+ T-lymphocyte cell counts.6
The measure is placed in Group 3 because it overlaps and focuses on similar aspects of care (vaccination) that were previously captured in measures included in Group 2. In addition, the data collection process is more

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
complex because of the timing of the vaccination.
US Public Health Guidelines:
“Annual vaccination against influenza is recommended for….adults and children who have immunosuppression (including immunosuppression caused by medications or by human immunodeficiency virus).”7
References/Notes: 1 “Clients” includes all clients aged 13 years and older. 2 Due to the unique nature of this measure, the measurement period runs from April 1-March 31. 3A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe medications. 4 Evidence of vaccination could include personal, school, physician, or immunization records or registries.5Centers for Disease Control and Prevention. Prevention and Control of Influenza: Recommendations from the Advisory committee on Immunization Practices (ACIP). MMWR 2007; 56(RR#6)[1-60]. Available at: http://www.cdc.gov/mmwr/PDF/rr/rr5606.pdf.6Ibid. 7Ibid.

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
Performance Measure: MAC Prophylaxis OPR-Related Measure: NoPercentage of clients1 with HIV infection with CD4 count < 50 cells/mm3 who were prescribed Mycobacterium avium Complex (MAC) prophylaxis2 within the measurement year
Numerator: Number of HIV-infected clients with CD4 count < 50 cells/mm3 who were prescribed MAC prophylaxis
Denominator:
Number of HIV-infected clients who had a: CD4 count < 50 cells/mm3 ; and medical visit with a provider with prescribing privileges3 at least once in the measurement year
PatientExclusions: 1. Patients who have disseminated MAC
Data Elements:
1. Is the client HIV-infected? (Y/N) a. If yes, was the CD4 count < 50 cells/mm3? (Y/N)
i. If yes, was MAC prophylaxis subsequently prescribed?
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker or other electronic data base HIVQUAL reports on this measure for grantee under review Medical record data abstraction by grantee of a sample of records Billing records
National Goals, Targets, or BenchmarksforComparison:
National HIVQUAL Data:4
2003 2004 2005 2006 2007 Top 10% 100% 100% 100% 100% 100% Top 25% 100% 100% 100% 100% 100%
Mean* 86.5% 84.7% 85.7% 83.1% 84.6% *from HAB data base
OutcomeMeasures for Consideration:
Incidence of MAC disease in the clinic population MAC-related mortality rates in the population assessed
Basis for Selection and Placement in Group 3: MAC disease is an opportunistic infection that can cause severe illness in people with advanced AIDS but rarely affects others. The risk of disseminated MAC (DMAC) is directly related to the severity of immunosuppression. DMAC typically occurs in persons with CD4 counts < 50 cells/mm3 and its frequency increases as the CD4 count declines. In the absence of antibiotic prophylaxis, DMAC occurs in up to 40% of AIDS patients with CD4 counts of < 50 cells/mm.5
The measure was placed in Group 3 because it focuses on similar aspects of care (prophylaxis) previously

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
captured in measures included in Groups 1 & 2.
US Public Health Guidelines:
“Adults and adolescents who have HIV infection should receive chemoprophylaxis against disseminated MAC disease if they have CD4 count < 50 cells/mm.3”6
References/Notes: 1 “Clients” includes all clients aged 13 years and older.2Current regimens for preventing MAC can be found at: Centers for Disease Control and Prevention. Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents. June 18, 2008; 1-134. (http://aidsinfo.nih.gov/contentfiles/Adult_OI.pdf)3A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe medications. 4 MAC Prophylaxis (http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf)5 National AIDS Education & Training Centers (2006). Clinical Manual for Management of the HIV-Infected Adult.6Centers for Disease Control and Prevention. Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents. June 18, 2008; 1-134. (http://aidsinfo.nih.gov/contentfiles/Adult_OI.pdf)

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
Performance Measure: Mental Health Screening
OPR-Related Measure: Yes www.hrsa.gov/performancereview/measures.htm
Percentage of new clients1 with HIV infection who have had a mental health screening
Numerator: Number of HIV-infected clients who received a mental health screening
Denominator:
Number of HIV-infected clients who: were new during the measurement year, and had a medical visit with a provider with prescribing privileges2 at least once in the measurement year
PatientExclusions: None
Data Elements:
1. Is the client HIV-infected? (Y/N) a. If yes, was the client new to the program during the
measurement year? (Y/N) i. If yes, did the client receive mental health screening
during the measurement year? (Y/N)
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker, or other electronic data base HIVQUAL reports on this measure for grantee under review
Medical record data abstraction by grantee of a sample of records Billing records
National Goals, Targets, or BenchmarksforComparison
National HIVQUAL Data:3
2003 2004 2005 2006 2007Top 10% 100% 100% 80.6% 86.7% 100% Top 25% 93.0% 89.5% 35.1% 52.4% 84.0%
Mean* 68.2% 58.5% 21.9% 28.1% 42.0% *from HAB data base
OutcomeMeasures for Consideration:
Rate of mental health referrals Mental health-related hospitalizations Rate of suicide in the clinic population Rate of mental health disorders being treated in the clinic population
Basis for Selection and Placement in Group 3: Patients living with HIV infection must often cope with multiple social, psychiatric, and medical issues. The ability to cope with these issues can dramatically impact management of the disease. The initial evaluation should include an assessment of substance abuse, economic factors, social

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
support, mental illness and co-morbidities. 4
The measure was placed in Group 3 because feasibility of data collection can vary considerably across grantees. US Public Health Guidelines: “Patients living with HIV infection must often cope with multiple social, psychiatric, and medical issues. Thus, the (initial) evaluation should also include assessment of substance abuse, economic factors, social support, mental illness, co-morbidities, and other factors that are known to impair the ability to adhere to treatment and to alter outcomes. Once evaluated, these factors should be managed accordingly."5
References/Notes: 1 “Clients” includes all clients aged 13 years and older. 2A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe medications. 3 The components of the mental health indicator were broken down and implemented for the 2005-2007 data. The Mental Health/Substance Use Subcommittee of the National HIVQUAL Clinical Advisory Committee include the following components for an annual Mental Health Screening for people with HIV: Cognitive function assessment, including mental status; Depression screening; Anxiety screening; Sleeping habits assessment; Appetite assessment; Domestic violence screening; Post Traumatic Stress Disorder screening; Psychiatric history (optional); Psychosocial assessment (optional). (http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf4Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents. Department of Health and Human Services. January 29, 2008; 1-128. (http://aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf)5Ibid

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
Performance Measure: Tobacco Cessation Counseling OPR-Related Measure: No Percentage of clients1 with HIV infection who received tobacco cessation counseling within the measurement year
Numerator: Number of HIV-infected clients who received tobacco cessation counseling
Denominator:
Number of HIV-infected clients who: used tobacco products within the measurement year; and had a medical visit with a provider with prescribing privileges2 at least once in the measurement year
PatientExclusions: 1. Patients who deny tobacco use throughout the measurement year
Data Elements:
1. Is the client HIV-infected? (Y/N) a. If yes, did the client use tobacco during the reporting period? (Y/N)
i. If yes, did the client receive tobacco cessation counseling during the measurement year? (Y/N)
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker, or other electronic data base HIVQUAL reports on this measure for grantee under review Medical record data abstraction by grantee of a sample of records Billing records
National Goals, Targets, or BenchmarksforComparison
National HIVQUAL Data:3
2003 2004 2005 2006 2007 Top 10% 100% 100% 100% 100% 100% Top 25% 93.3% 97.8% 98.4% 100% 100%
Mean* 69.3% 75.0% 76.8% 81.8% 83.8% * HAB database
OutcomeMeasures for Consideration:
Rate of head & neck and lung cancer Rate of tobacco use in the clinic population
Basis for Selection and Placement in Group 3: A recent study has shown that lung cancer rates are 2.7 times greater for people living with HIV.4 As tobacco use among HIV-infected patients poses significant health risks, tobacco-dependent patients should be provided assistance to enroll in smoking cessation programs. Various studies have shown that brief interventions by the clinician to encourage tobacco cessation and offer substitution programs can decrease smoking rates5 and tobacco use.6 Cessation reduces the risk of incidence or the progression of tobacco-related diseases and increases life expectancy.7,8,9 HIV care providers should provide cessation assistance in the form of counseling, pharmacotherapy or referral to cessation programs.

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
The measure was placed in Group 3 because the feasibility of data collection can vary considerably across grantees.US Public Health Guidelines:
“The U.S. Preventive Services Task Force strongly recommends that clinicians screen all adults for tobacco use and provide tobacco cessation interventions for those who use tobacco products.”10
References/Notes:1 “Clients” includes all clients aged 13 years and older. 2 A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe medications. 3Tobacco Use(http://www.hivguidelines.org/admin/files/qoc/hivqual/proj%20info/HQNatlAggScrs3Yrs.pdf)4Philips, Abs 8, CROI, Boston, 2008. 5 Page AR, Walters DJ, Schlegel RP, Best JA. Smoking cessation in family practice: The effects of advice and nicotine chewing gum prescription. Addict Behav 1986;11(4):443-6. 6 Demers RY, Neale AV, Adams R, Trembath C, Herman SC. The impact of physicians' brief smoking cessation counseling: A MIRNET study. J Fam Pract 1990;31(6):625-9. 7 Rigotti NA. Treatment of tobacco use and dependence. N Engl J Med 2002;346:506-512. 8 Lancaster T, Stead L, Silagy C, Sowden A. Effectiveness of interventions to help people stop smoking: findings from the Cochrane Library. BMJ 2000;321:355-8. 9 Methods, Successes, and Failures of Smoking Cessation Programs E B Fisher Jr,, E Lichtenstein, D Haire-Joshu, G D Morgan, H R Rehberg Annual Review of Medicine, February 1993, Vol. 44, Pages 481-513. 10 Agency for Healthcare Research and Quality. The Guide to Clinical Preventive Services: Recommendations of the U.S. Preventive Services Task Force, June 2006, p. 120.

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
Performance Measure: Toxoplasma Screening OPR-Related Measure: No Percentage of clients1 with HIV infection for whom Toxoplasma screening2 was performed at least once since the diagnosis of HIV infection3
Numerator: Number of HIV-infected clients who have documented Toxoplasma status in health record
Denominator: Number of HIV-infected clients who had a medical visit with a provider with prescribing privileges4 at least once in the measurement year
PatientExclusions: 1. Patients with known toxoplasmic disease, e.g. Toxoplasma gondii encephalitis
Data Elements:
1. Is the client HIV-infected? (Y/N) a. If yes, is there documentation of the client’s Toxoplasma status in the
health record? (Y/N)
Data Sources:
Electronic Medical Record/Electronic Health Record CAREWare, Lab Tracker or other electronic data base Medical record data abstraction by grantee of a sample of records Billing records
National Goals, Targets, or BenchmarksforComparison:
None available at this time
OutcomesMeasures for Consideration:
Toxoplasmosis-related mortality rates in the clinic population Incidence of Toxoplasmosis in the clinic population
Basis for Selection and Placement in Group 3: Toxoplasmic disease appears to occur almost exclusively because of reactivation of latent tissue cysts. Clinical disease is rare among patients with CD4 counts >200 cells/uL. The greatest risk is among patients with a CD4 cell count < 50/uL. HIV-infected patients with Toxoplasma gondii encephalitis (TE) are almost uniformly seropositive for anti-toxoplasma IgG antibodies.5
The measure is placed in Group 3 because it overlaps and focuses on similar aspects of care (prophylaxis) previously captured in measures included in Group 1. Certain geographic regions have lower rates of toxoplasmic disease. US Public Health Guidelines: “HIV-infected persons should be tested for immunoglobulin G (IgG) antibody to Toxoplasma soon after the diagnosis of HIV infection to deter latent infection with T. gondii (strength of recommendation: BIII).”6
“Toxoplasma-seronegative persons who are not taking a PCP prophylactic regimen known to be active

HAB HIV Core Clinical Performance Measures for Adult/Adolescent Clients: Group 3
against TE should be retested for IgG antibody to Toxoplasma when their CD4+ counts decline to <100/uL to determine whether they have seroconverted and are therefore at risk for TE (strength of recommendation: CIII).”7
References/Notes: 1 “Clients” refers to all clients aged 13 years and older. 2Toxoplasma screening refers to testing for the presence of anti-toxoplasma immunoglobulin G (IgG) antibodies to detect latent infection with Toxoplasma gondii.3Unless there is concern about ongoing exposure, annual re-screening is not generally recommended. 4A “provider with prescribing privileges” is a health care professional who is certified in their jurisdiction to prescribe medications. 5Centers for Disease Control and Prevention. Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents. June 18, 2008; 1-134. (http://aidsinfo.nih.gov/contentfiles/Adult_OI.pdf)6Ibid 7Ibid