Embed Size (px)
Citation preview
HCAP & HAPPamela Charity, MD
Cathryn Caton, MD, MS
OBJECTIVES
Define pneumonia
Define HAP and review the characteristics
Define HCAP
Diagnosing HCAP and HAP
Treatment of HCAP and HAP
Review treatment algorithm
PNEUMONIA
Fever Leukocytosis Infiltrate on CXR
HOSPITAL ACQUIRED PNEUMONIA
Category of pneumonia that occurs 48 hours or more after admission
Encompasses
healthcare associated pneumonia and
ventilator associated pneumonia
HOSPITAL ACQUIRED PNEUMONIA
Time of onset
Is an epidemiologic variable and
Risk factor for specific pathogens and
Affects outcomes
HOSPITAL ACQUIRED PNEUMONIA
Early onset Within first 4 days Better prognosis More likely to be caused by antibiotic-sensitive
bacteria
Above is true unless patient Received prior antibiotics Have had prior hospitalization within 90 days
Greater risk for colonization and infection with MDR pathogens
HOSPITAL ACQUIRED PNEUMONIA
Late onset
5 days or more
More likely to be caused by MDR pathogens risk factors for MDR
Antimicrobial therapy in preceding 90 days Presence of risk factors for HCAP Immunosuppresive disease/therapy
Increased morbidity and mortality
HEALTHCARE ASSOCIATED PNEUMONIA
Category of pneumonia in patients with recent close contact with the health care system
Hospitalized for 2 or more days within last 90 days
Resides in nursing home or long-term care facility
Received recent IV antibiotic therapy, chemotherapy, or wound care within past 30 days
Hemodialysis
MAKING THE DIAGNOSIS
History – this will determine the classification of pneumonia
Physical exam findings
Laboratory data
Radiographic findings
Antibiotics should be initiated within 4 hours of making the diagnosis.
CHOOSING EMPIRIC ANTIBIOTICS
HCAP and HAP are treated similarly Think about multi-drug resistant pathogens
Gram Neg Pseudomona Aeruginosa – some are only sensitive to
polymyxin B Serratia Marcescens Klebsiella Enterobacter Acinetobacter
Gram Positive MRSA VRE
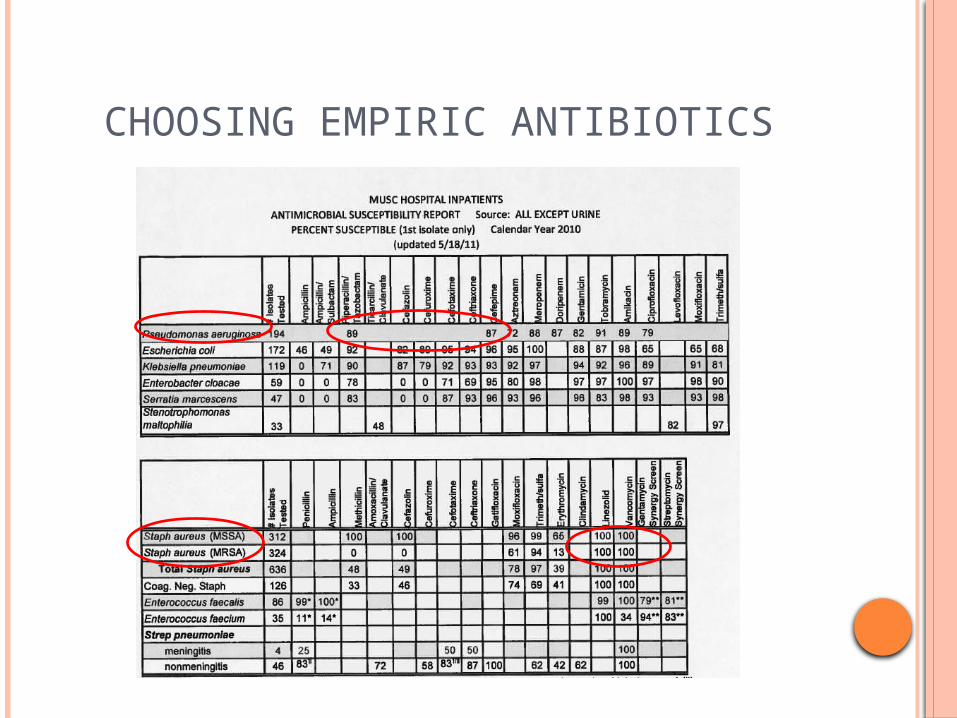
CHOOSING EMPIRIC ANTIBIOTICS
DE-ESCALATION OF ANTIBIOTIC THERAPY
This may be appropriate if Clinical improvement at 48-72 hours Cultures are positive Treat for 7-8 days and reassess patient Single agent such as moxifloxacin may be
appropriate
May stop antibiotics if clinical improvement at 48-72 hours and cultures are negative
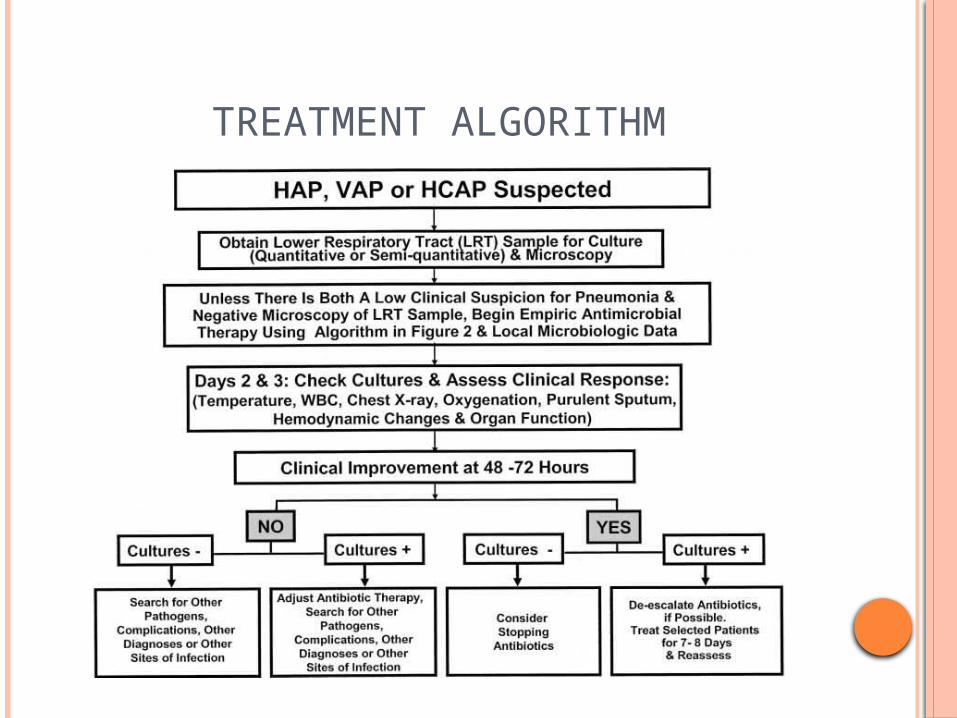
TREATMENT ALGORITHM
REFERENCES
ATS/IDSA GuidelinesAm J Respir Crit Care Med Vol 171. pp 388-
416, 2005