Embed Size (px)
Citation preview
1
GuyanaHIVCaseSurveillance
SystemStandardOperatingProceduresManual
May2013
Surveillance Unit Ministry of Health Lot 1 Brickdam
Georgetown, Guyana
2
Table of Contents
Foreword ........................................................................................................................................................ 4
Glossary of Terms ........................................................................................................................................... 5
I. Mission Statement ................................................................................................................................. 7
II. Introduction ........................................................................................................................................... 8
A. Purpose of the Standard Operating Procedures Manual ................................................................... 8
B. Intended Users ................................................................................................................................... 8
C. Organizational Chart .......................................................................................................................... 8
D. Updated HIV Case Surveillance System and Form ........................................................................... 10
E. HIV Case Definitions ......................................................................................................................... 10
III. HIV Case Reporting ........................................................................................................................... 12
A. Definition of HIV Case Based Surveillance ....................................................................................... 12
B. HIV Case Surveillance Form (HCSF) .................................................................................................. 12
C. Testing Procedures and Reportable Events ..................................................................................... 18
D. Reporting Sources ............................................................................................................................ 19
E. Reporting Procedures ...................................................................................................................... 19
F. Description of Data Flow Diagram for Guyana’s HIV Case Surveillance System .............................. 22
G. Program Specific Data Flow Diagrams ............................................................................................. 27
IV. Security and Confidentiality ............................................................................................................. 35
A. Training............................................................................................................................................. 36
B. Standards for Monitoring and Evaluating the HIV Case Surveillance System .................................. 36
Appendix A1: WHO clinical staging of HIV infection for adults and adolescents with confirmed HIV
infection ....................................................................................................................................................... 40
Appendix A2: WHO clinical staging of HIV infection for children with confirmed HIV infection ................. 42
Appendix B: Guide for Constructing the PUID on the HIV Case Surveillance Form (HCSF) ......................... 43
Appendix C: HIV Case Surveillance Form (HCSF) .......................................................................................... 46
3
Appendix D: HCSF Completion Procedures .................................................................................................. 47
Appendix E: HCSF Initial Review Procedures ............................................................................................... 53
Appendix F: HCSF Secondary Review Procedures ........................................................................................ 55
Appendix G: Data Entry Procedures ............................................................................................................. 58
Appendix H: Matching Procedures .............................................................................................................. 60
4
Foreword
Epidemiological surveillance is amajorpublichealth strategy inpreventionandcontrolofHIV in
developinganddevelopedcountries.TheMinistryofHealth(MOH),inpartnershipwiththeCenters
forDisease Control and Prevention (CDC) and theNational Alliance of State and Territorial AIDS
Directors(NASTAD)hasdevelopedthefollowingguidancetoprovidethenecessaryproceduresto
ensure a strong integrated HIV Case Surveillance System at the national level. HIV surveillance
cannotbedoneinisolation.Hence,keystakeholdersfrombothpublicandprivatesectors,andthe
national HIV prevention monitoring and evaluation programmes were involved in the effort to
improvethequalityandstandardsoftheHIVCaseSurveillanceSystem.
The strengthening of the HIV Case Surveillance System will serve to efficiently and accurately
monitor theHIV epidemic over time by providing information onpersons affected byHIV in our
society.Additionally,thequalityinformationobtainedfromthecasebasedHIVSurveillanceSystem
is used to organize, plan, and implement programs in response to the HIV pandemic. Hence, the
upgradedHIVsurveillanceinformationinformsresourceallocation,andadvocacygroups;measures
the burden and impact on health services; and provides information for developing broad based
strategiestomitigateagentsthatimpactHIVinGuyana.
_______________________________
Dr.ShamdeoPersaud
ChiefMedicalOfficer
5
GlossaryofTerms
AIDS AcquiredImmunodeficiencySyndrome
ANC AntenatalCareorAntenatalClinic
ART Antiretroviraltherapy
C&T CareandTreatment
CDC CentersforDiseaseControlandPrevention
CD4 CD4Tcells
CMO ChiefMedicalOfficer
DOB DateofBirth
EDB ElectronicHIVSurveillanceDataBase
ELISA EnzymeLinkedImmunosorbentAssay
HCSF HIVCaseSurveillanceForm
HIV HumanImmunodeficiencyVirus
HIV+ HIVpositive
HIV‐ HIVnegative
MARPS MostatRiskPopulations
M&E MonitoringandEvaluation
MCHMaternalChildHealth
MOH MinistryofHealth
MSM MenwhohaveSexwithMen
NAPS NationalAIDSProgrammeSecretariat
NASTAD NationalAllianceofStateandTerritorialAIDSDirectors
NGO Non‐GovernmentalOrganization
PII PersonallyIdentifyingInformation
PLWH PeopleorPersonLivingwithHIV
PMTCT PreventionofMother‐to‐ChildTransmission(ofHIV)
PUID PatientUniqueIdentifier
RHO RegionalHealthOfficer

6
SOP StandardOperatingProcedures
UNAIDS JointUnitedNationsProgrammeforHIV/AIDS
VCT VoluntaryCounsellingandTesting
WHO WorldHealthOrganization
7
I. MissionStatement
Theaimof theMinistryofHealth is to improvethephysical, socialandmentalhealthstatusofall
Guyanese by ensuring that health services are accessible, acceptable, affordable, timely and
appropriate as possible given available resources and enhancing the effectiveness of health
personnelthroughcontinuingeducation,trainingandmanagementsystems.
Toachievesuchgoalsoneof thecomponentsof theNationalHealthSectorStrategy2008‐2012 is
the strengthening of strategic information, developing a capacity to lead relevant data collection,
analysisanduseinplanning,managementandevaluationatalllevels.
8
II. Introduction
A. PurposeoftheStandardOperatingProceduresManual
Thisproceduralmanual(referredtoasSOPhenceforth)iscomprehensiveinscope,andintendedtoprovidenecessaryinformationandguidancefortheimplementation,managementandutilizationofthenationalHIVcasesurveillancesystemacrossvoluntarycounselingandtesting,HIVcareandtreatment,antenatalcare(includingpreventionofmothertochildtransmission(PMTCT))programsandlaboratoriesandtheBloodBank.ThisincludesclearanddescriptiveinstructionsandrolesandresponsibilitiesforthecompletionoftheHIVcasesurveillanceform(HCSF),submissionofHCSFformstotheappropriateadministrativeunit,dataentryandreporting.
B. IntendedUsers
TheSOPshouldbereferencedandutilizedbyanyandallclinicalstaffparticipatinginHIVtesting,careandthecompletionandtransportationoftheHCSF.Additionally,thisSOPisintendedforusebyNationalAIDSProgrammeSecretariat(NAPS)staff,MinistryofHealth(MoH)StatisticalUnitstaff,MoHSurveillanceUnit staff,MoHMaternalChildHealth (MCH)staffworking in theANCprogramandMoHManagementInformationSystemsUnit(MISU).
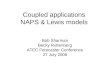
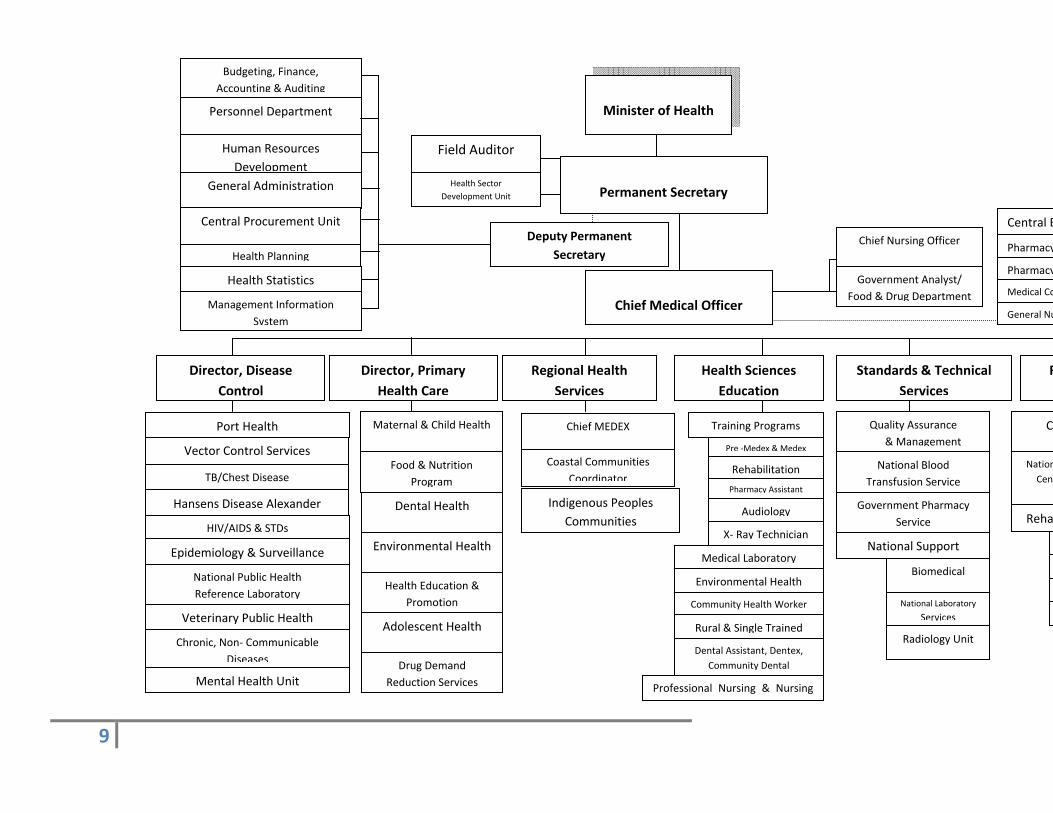
C. OrganizationalChart
TheMinistryofHealthcomprisessevenprogrammes,eachwithvariousnumbersofsub‐programs.Sixunitsarespecifically identifiedtomanageHIVsurveillanceandprogramdata; theSurveillanceUnit, Health Statistics Unit, Management Information Systems Unit, Voluntary Counseling andTesting(VCT),PreventionofMother‐to‐ChildTransmission(PMTCT)atantenatalclinics,andCareandTreatment(C&T).Togethertheseunitsworkcollaborativelytocoordinateandsupportalldatacollection, management, analysis and dissemination of HIV surveillance and program data. TheSurveillanceUnitcoordinates theprocedures forHIVsurveillancedataandworkswith theHealthStatisticsunittoproducehighqualityandreliabledatareportsandanalyses.
TheNationalAIDSProgrammeSecretariat(NAPS)islocatedwithintheDiseaseControlprogramanditoverseestheHIVpreventionandcareprogramsandit istheprimarystakeholdertoensureHIVsurveillancereportsareusedforprogramplanninganddecisionmaking.
Figure1:OrganizationalChart
9
Minister of Health
Permanent Secretary
Chief Medical Officer
Health Planning
Human Resources
Development
General Administration
Central Procurement Unit
Field Auditor
Management Information
System
Director, Disease
Control
Director, Primary
Health Care
Health Sciences
Education
Chronic, Non‐ Communicable
Diseases
HIV/AIDS & STDs
Mental Health Unit
Epidemiology & Surveillance
Port Health
Vector Control Services
TB/Chest Disease
Hansens Disease Alexander
Maternal & Child Health
Adolescent Health
Food & Nutrition
Program
Dental Health
Environmental Health
Quality Assurance
& Management
National Public Health
Reference Laboratory
Biomedical
National Blood
Transfusion Service
Veterinary Public Health
Personnel Department
Government Analyst/
Food & Drug Department
Central B
Pharmacy
General Nu
Medical Co
Chief Nursing Officer Pharmacy
C
Nation
Cent
Reha
Coastal Communities
Coordinator
Indigenous Peoples
Communities
Training Programs
Budgeting, Finance,
Accounting & Auditing
Health Sector
Development Unit
Pre ‐Medex & Medex
Rehabilitation
Pharmacy Assistant
Audiology
X‐ Ray Technician
Community Health Worker
Dental Assistant, Dentex,
Community Dental
Rural & Single Trained
Professional Nursing & Nursing
Environmental Health
Medical Laboratory
Health Education &
Promotion
Drug Demand
Reduction Services
Health Statistics
Government Pharmacy
Service
Chief MEDEX
National Support
National Laboratory
Services
Radiology Unit
Standards & Technical
Services
R
Deputy Permanent
Secretary
Regional Health
Services
10
D. UpdatedHIVCaseSurveillanceSystemandForm
In order to facilitate the scaling up of access to antiretroviral therapy (ART), in 2007 theWorldHealthOrganization(WHO)revisedHIVcasedefinitionsforsurveillanceofHIVandtheclinicalandimmunologicalclassificationofHIV‐relateddiseasesintoauniversalfour‐stagesystemthatincludessimplified standardized descriptors of clinical staging events1. The 2007 WHO HIV surveillancerecommendationscall forrevisingthecasedefinitionsto includeallstagesofHIV infectionandtoreplace AIDS case reporting with reporting of persons with advanced and severe HIV disease(clinicalstages3and4).TherearefourWHOclinicalstages:stage1(asymptomatic),stage2(mildsymptoms),stage3(advancedsymptoms),andstage4(severesymptoms,previouslyreferredtoasAIDS). In the light of these revisions, Ministry of Health revised and upgraded the HIV casesurveillance reporting form and the current HIV case reporting system to strengthen HIV casesurveillanceinGuyana.TheupgradedMoHHIVSurveillanceSystem:
MonitorstheHIVepidemicovertimebyrequiringreportingofallHIVinfectedpersonsfromeachsitewheretheypresentfortestingorcare&treatmentaswellasadditionalreportsonpersonsdiagnosedwithadvancedand/orsevereHIVinfectionorwhohavedied
Tracksindividualclientdiseaseprogressionfrompointofdiagnosisthroughstage3and4 IdentifiesthecareandtreatmentneedsofHIV‐infectedindividuals DeterminesthecharacteristicsandexposurecategoriesofpersonswithHIVinfection Determines the region’s disease burden that is attributable to HIV by measuring HIV
prevalence InformstheburdenandimpactofHIVonhealthservices ProvidesdatafordevelopingandmonitoringHIVpreventionprograms,toinformadvocacy
groups,resourceallocation,programplanning,andmonitoringandevaluationofprograms.
MeasurestrendsinmortalityamongHIV‐infectedpersons
E. HIVCaseDefinitions
TheHIVcasedefinitionsforHIVinfectionandadvancedHIVareinaccordancewiththe2007WHOcasedefinitions1:
1 World Health Organization 2007. WHO case definitions of HIV for surveillance and revised clinical staging and immunological classification of HIV‐related disease in adults and children.
11
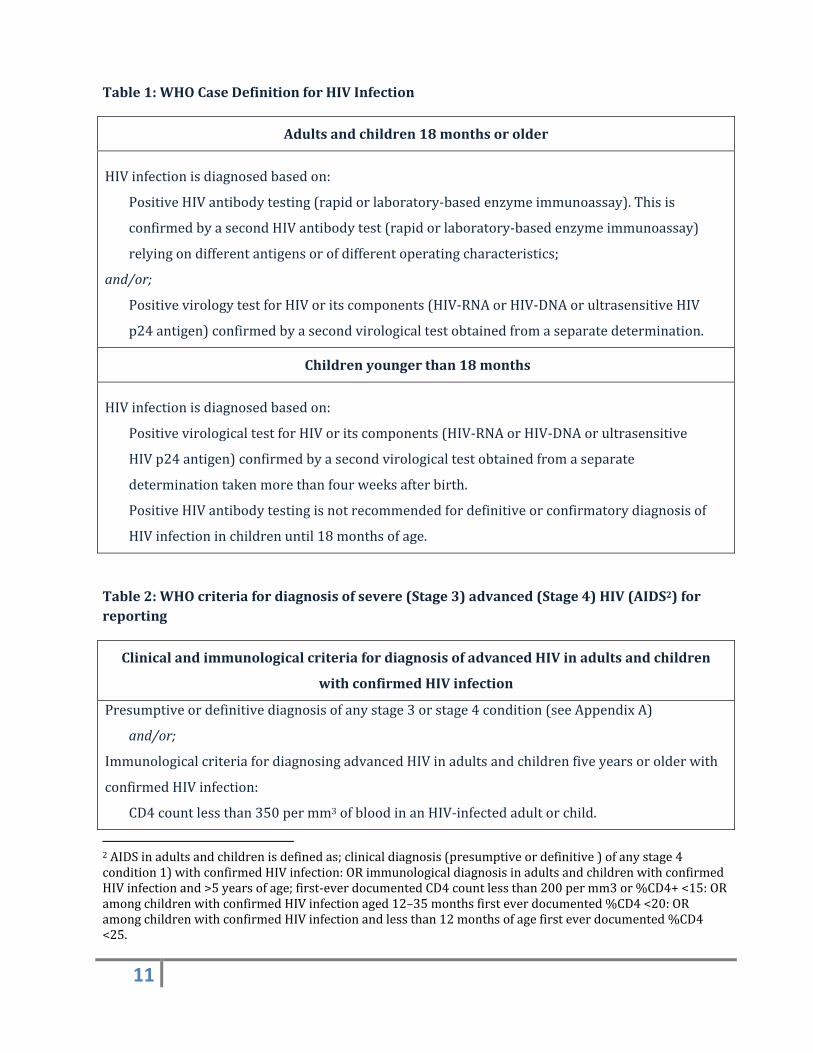
Table1:WHOCaseDefinitionforHIVInfection
Adultsandchildren18monthsorolder
HIVinfectionisdiagnosedbasedon:
PositiveHIVantibodytesting(rapidorlaboratory‐basedenzymeimmunoassay).Thisis
confirmedbyasecondHIVantibodytest(rapidorlaboratory‐basedenzymeimmunoassay)
relyingondifferentantigensorofdifferentoperatingcharacteristics;
and/or;
PositivevirologytestforHIVoritscomponents(HIV‐RNAorHIV‐DNAorultrasensitiveHIV
p24antigen)confirmedbyasecondvirologicaltestobtainedfromaseparatedetermination.
Childrenyoungerthan18months
HIVinfectionisdiagnosedbasedon:
PositivevirologicaltestforHIVoritscomponents(HIV‐RNAorHIV‐DNAorultrasensitive
HIVp24antigen)confirmedbyasecondvirologicaltestobtainedfromaseparate
determinationtakenmorethanfourweeksafterbirth.
PositiveHIVantibodytestingisnotrecommendedfordefinitiveorconfirmatorydiagnosisof
HIVinfectioninchildrenuntil18monthsofage.
Table2:WHOcriteriafordiagnosisofsevere(Stage3)advanced(Stage4)HIV(AIDS2)forreporting
ClinicalandimmunologicalcriteriafordiagnosisofadvancedHIVinadultsandchildren
withconfirmedHIVinfection
Presumptiveordefinitivediagnosisofanystage3orstage4condition(seeAppendixA)
and/or;
ImmunologicalcriteriafordiagnosingadvancedHIVinadultsandchildrenfiveyearsorolderwith
confirmedHIVinfection:
CD4countlessthan350permm3ofbloodinanHIV‐infectedadultorchild.
2AIDSinadultsandchildrenisdefinedas;clinicaldiagnosis(presumptiveordefinitive)ofanystage4condition1)withconfirmedHIVinfection:ORimmunologicaldiagnosisinadultsandchildrenwithconfirmedHIVinfectionand>5yearsofage;first‐everdocumentedCD4countlessthan200permm3or%CD4+<15:ORamongchildrenwithconfirmedHIVinfectionaged12–35monthsfirsteverdocumented%CD4<20:ORamongchildrenwithconfirmedHIVinfectionandlessthan12monthsofagefirsteverdocumented%CD4<25.
12
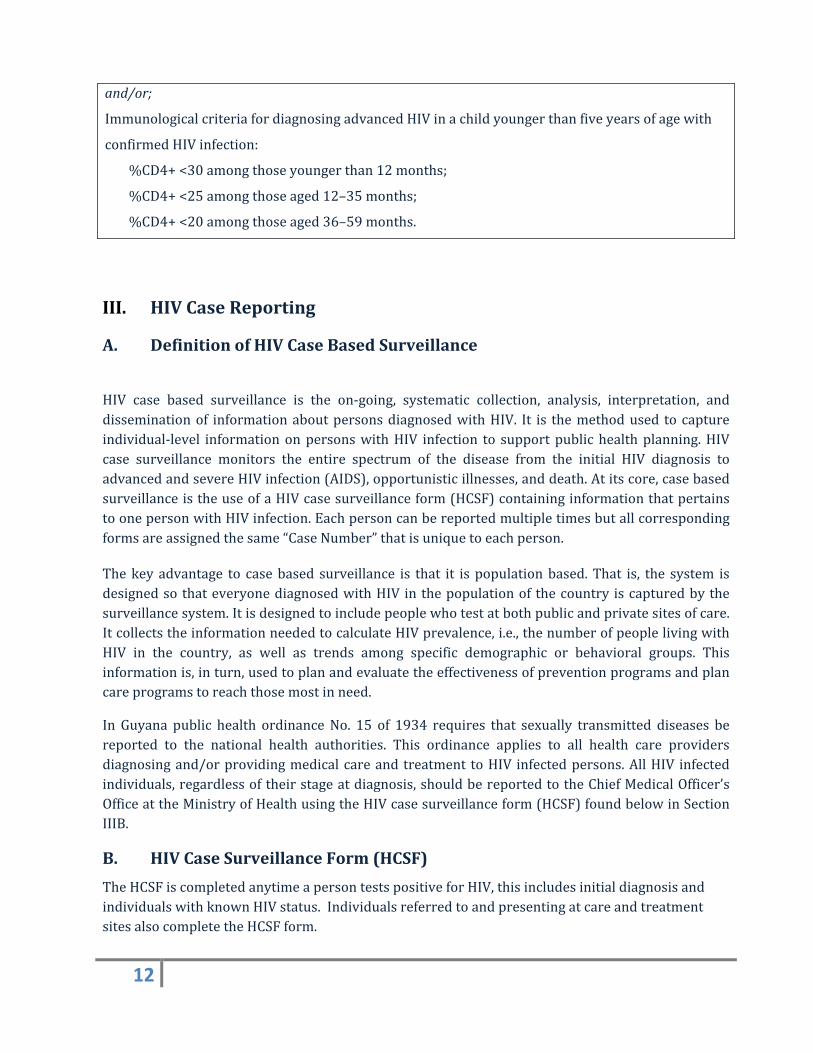
and/or;
ImmunologicalcriteriafordiagnosingadvancedHIVinachildyoungerthanfiveyearsofagewith
confirmedHIVinfection:
%CD4+<30amongthoseyoungerthan12months;
%CD4+<25amongthoseaged12–35months;
%CD4+<20amongthoseaged36–59months.
III. HIVCaseReporting
A. DefinitionofHIVCaseBasedSurveillance
HIV case based surveillance is the on‐going, systematic collection, analysis, interpretation, anddisseminationof informationaboutpersonsdiagnosedwithHIV. It is themethodused tocaptureindividual‐level informationonpersonswithHIV infection to supportpublichealthplanning.HIVcase surveillance monitors the entire spectrum of the disease from the initial HIV diagnosis toadvancedandsevereHIVinfection(AIDS),opportunisticillnesses,anddeath.Atitscore,casebasedsurveillanceistheuseofaHIVcasesurveillanceform(HCSF)containinginformationthatpertainstoonepersonwithHIVinfection.Eachpersoncanbereportedmultipletimesbutallcorrespondingformsareassignedthesame“CaseNumber”thatisuniquetoeachperson.
Thekeyadvantage to casebased surveillance is that it ispopulationbased.That is, the system isdesignedso thateveryonediagnosedwithHIV in thepopulationof thecountry iscapturedbythesurveillancesystem.Itisdesignedtoincludepeoplewhotestatbothpublicandprivatesitesofcare.ItcollectstheinformationneededtocalculateHIVprevalence,i.e.,thenumberofpeoplelivingwithHIV in the country, as well as trends among specific demographic or behavioral groups. Thisinformationis,inturn,usedtoplanandevaluatetheeffectivenessofpreventionprogramsandplancareprogramstoreachthosemostinneed.
In Guyana public health ordinanceNo. 15 of 1934 requires that sexually transmitted diseases bereported to the national health authorities. This ordinance applies to all health care providersdiagnosingand/orprovidingmedicalcareandtreatment toHIV infectedpersons.AllHIV infectedindividuals,regardlessoftheirstageatdiagnosis,shouldbereportedtotheChiefMedicalOfficer’sOfficeattheMinistryofHealthusingtheHIVcasesurveillanceform(HCSF)foundbelowinSectionIIIB.
B. HIVCaseSurveillanceForm(HCSF)
TheHCSFiscompletedanytimeapersontestspositiveforHIV,thisincludesinitialdiagnosisandindividualswithknownHIVstatus.IndividualsreferredtoandpresentingatcareandtreatmentsitesalsocompletetheHCSFform.
13
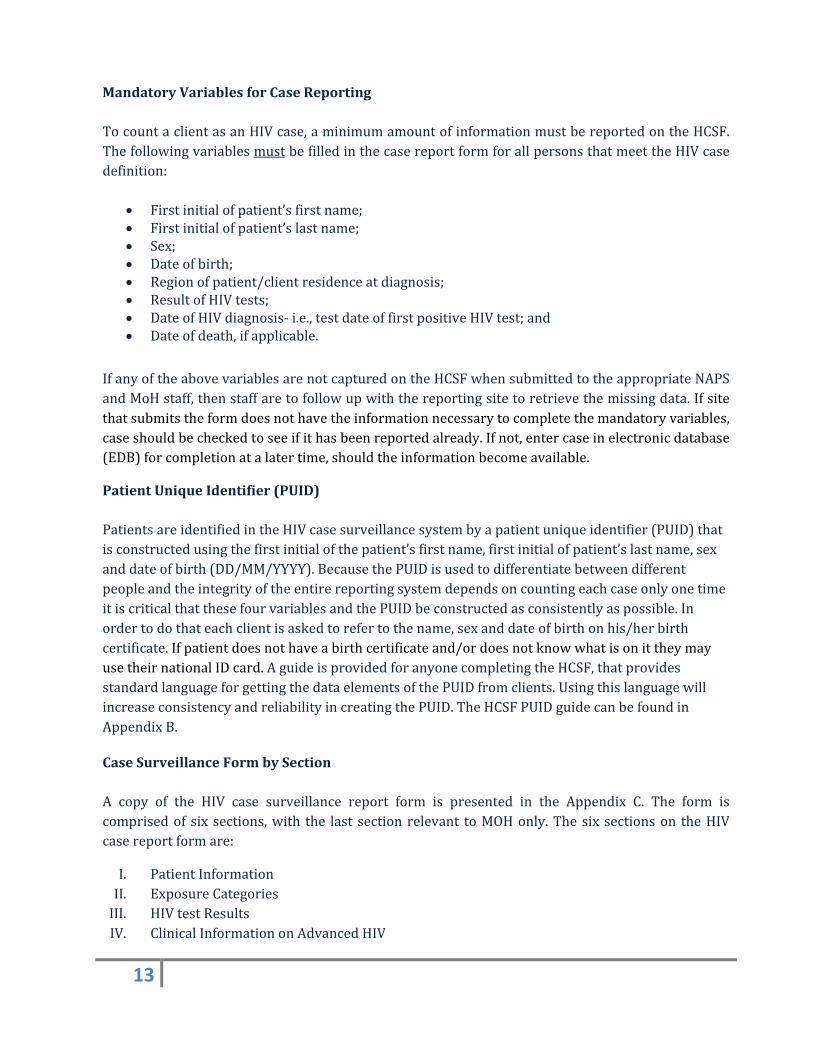
MandatoryVariablesforCaseReporting
TocountaclientasanHIVcase,aminimumamountofinformationmustbereportedontheHCSF.ThefollowingvariablesmustbefilledinthecasereportformforallpersonsthatmeettheHIVcasedefinition:
Firstinitialofpatient’sfirstname; Firstinitialofpatient’slastname; Sex; Dateofbirth; Regionofpatient/clientresidenceatdiagnosis; ResultofHIVtests; DateofHIVdiagnosis‐i.e.,testdateoffirstpositiveHIVtest;and Dateofdeath,ifapplicable.
IfanyoftheabovevariablesarenotcapturedontheHCSFwhensubmittedtotheappropriateNAPSandMoHstaff,thenstaffaretofollowupwiththereportingsitetoretrievethemissingdata.Ifsitethatsubmitstheformdoesnothavetheinformationnecessarytocompletethemandatoryvariables,caseshouldbecheckedtoseeifithasbeenreportedalready.Ifnot,entercaseinelectronicdatabase(EDB)forcompletionatalatertime,shouldtheinformationbecomeavailable.
PatientUniqueIdentifier(PUID)
PatientsareidentifiedintheHIVcasesurveillancesystembyapatientuniqueidentifier(PUID)thatisconstructedusingthefirstinitialofthepatient’sfirstname,firstinitialofpatient’slastname,sexanddateofbirth(DD/MM/YYYY).BecausethePUIDisusedtodifferentiatebetweendifferentpeopleandtheintegrityoftheentirereportingsystemdependsoncountingeachcaseonlyonetimeitiscriticalthatthesefourvariablesandthePUIDbeconstructedasconsistentlyaspossible.Inordertodothateachclientisaskedtorefertothename,sexanddateofbirthonhis/herbirthcertificate.Ifpatientdoesnothaveabirthcertificateand/ordoesnotknowwhatisonittheymayusetheirnationalIDcard.AguideisprovidedforanyonecompletingtheHCSF,thatprovidesstandardlanguageforgettingthedataelementsofthePUIDfromclients.UsingthislanguagewillincreaseconsistencyandreliabilityincreatingthePUID.TheHCSFPUIDguidecanbefoundinAppendixB.
CaseSurveillanceFormbySection
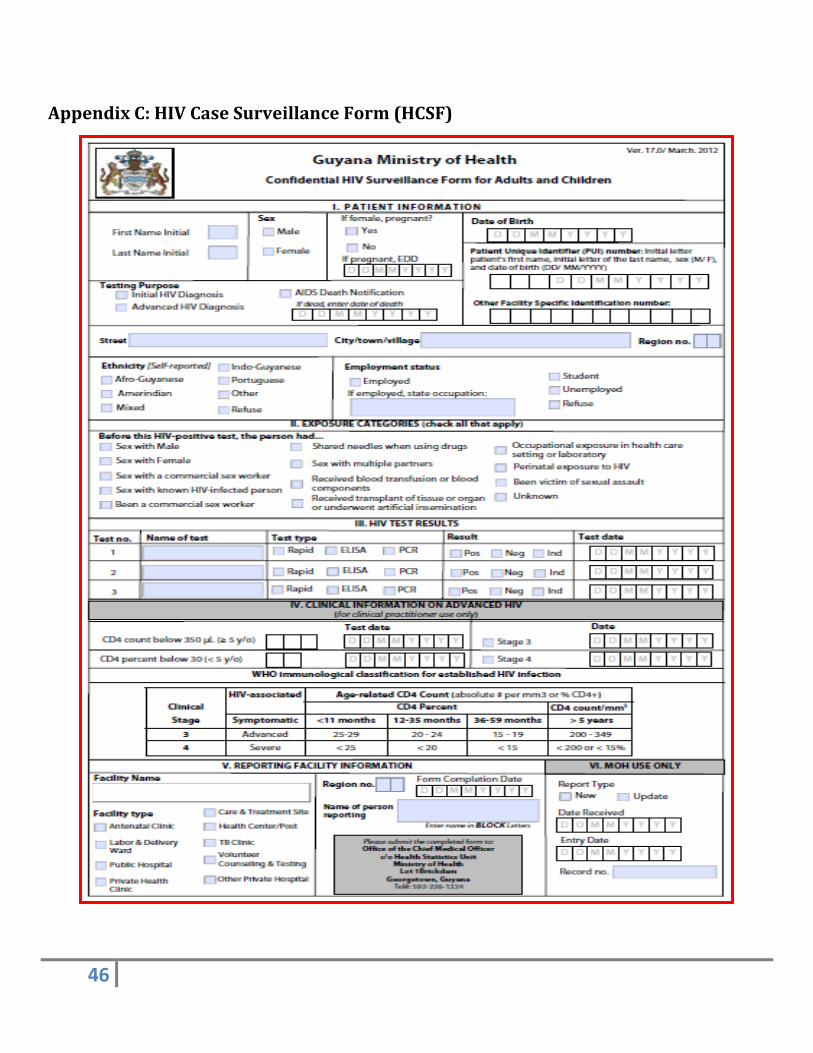
A copy of the HIV case surveillance report form is presented in the Appendix C. The form iscomprisedof six sections,with the last sectionrelevant toMOHonly.Thesix sectionson theHIVcasereportformare:
I. PatientInformationII. ExposureCategoriesIII. HIVtestResultsIV. ClinicalInformationonAdvancedHIV
14
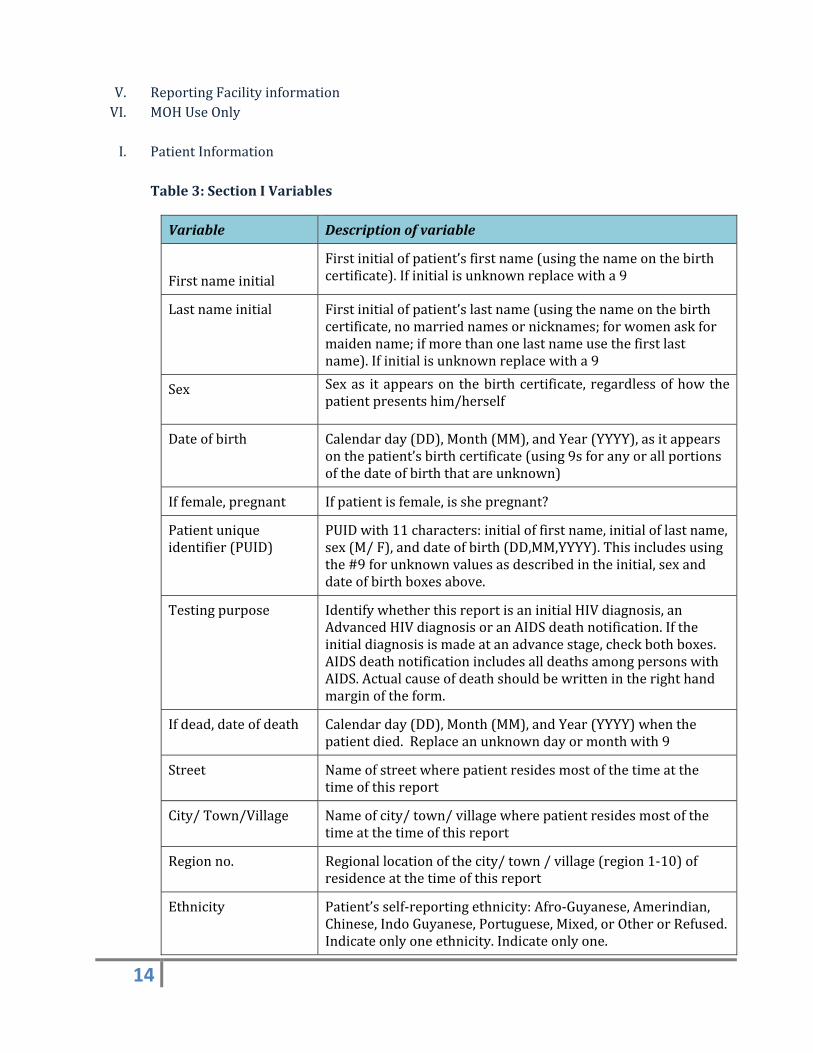
V. ReportingFacilityinformationVI. MOHUseOnlyI. PatientInformation
Table3:SectionIVariables
Variable Descriptionofvariable
Firstnameinitial
Firstinitialofpatient’sfirstname(usingthenameonthebirthcertificate).Ifinitialisunknownreplacewitha9
Lastnameinitial Firstinitialofpatient’slastname(usingthenameonthebirthcertificate,nomarriednamesornicknames;forwomenaskformaidenname;ifmorethanonelastnameusethefirstlastname).Ifinitialisunknownreplacewitha9
Sex Sexas itappearson thebirthcertificate, regardlessofhowthepatientpresentshim/herself
Dateofbirth Calendarday(DD),Month(MM),andYear(YYYY),asitappearsonthepatient’sbirthcertificate(using9sforanyorallportionsofthedateofbirththatareunknown)
Iffemale,pregnant Ifpatientisfemale,isshepregnant?
Patientuniqueidentifier(PUID)
PUIDwith11characters:initialoffirstname,initialoflastname,sex(M/F),anddateofbirth(DD,MM,YYYY).Thisincludesusingthe#9forunknownvaluesasdescribedintheinitial,sexanddateofbirthboxesabove.
Testingpurpose IdentifywhetherthisreportisaninitialHIVdiagnosis,anAdvancedHIVdiagnosisoranAIDSdeathnotification.Iftheinitialdiagnosisismadeatanadvancestage,checkbothboxes.AIDSdeathnotificationincludesalldeathsamongpersonswithAIDS.Actualcauseofdeathshouldbewrittenintherighthandmarginoftheform.
Ifdead,dateofdeath Calendarday(DD),Month(MM),andYear(YYYY)whenthepatientdied.Replaceanunknowndayormonthwith9
Street Nameofstreetwherepatientresidesmostofthetimeatthetimeofthisreport
City/Town/Village Nameofcity/town/villagewherepatientresidesmostofthetimeatthetimeofthisreport
Regionno. Regionallocationofthecity/town/village(region1‐10)ofresidenceatthetimeofthisreport
Ethnicity Patient’sself‐reportingethnicity:Afro‐Guyanese,Amerindian,Chinese,IndoGuyanese,Portuguese,Mixed,orOtherorRefused.Indicateonlyoneethnicity.Indicateonlyone.
15
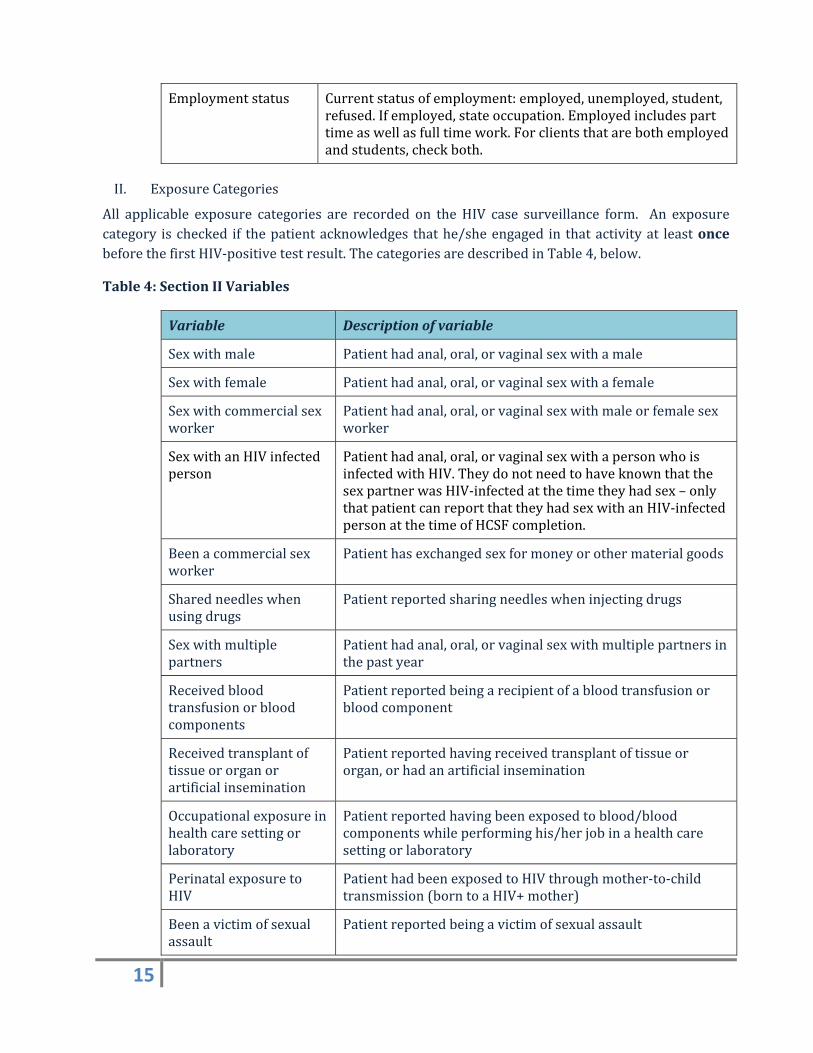
Employmentstatus Currentstatusofemployment:employed,unemployed,student,refused.Ifemployed,stateoccupation.Employedincludesparttimeaswellasfulltimework.Forclientsthatarebothemployedandstudents,checkboth.
II. ExposureCategories
All applicable exposure categories are recorded on theHIV case surveillance form. An exposurecategory ischecked if thepatientacknowledges thathe/sheengaged in thatactivityat leastoncebeforethefirstHIV‐positivetestresult.ThecategoriesaredescribedinTable4,below.
Table4:SectionIIVariables
Variable Descriptionofvariable
Sexwithmale Patienthadanal,oral,orvaginalsexwithamale
Sexwithfemale Patienthadanal,oral,orvaginalsexwithafemale
Sexwithcommercialsexworker
Patienthadanal,oral,orvaginalsexwithmaleorfemalesexworker
SexwithanHIVinfectedperson
Patienthadanal,oral,orvaginalsexwithapersonwhoisinfectedwithHIV.TheydonotneedtohaveknownthatthesexpartnerwasHIV‐infectedatthetimetheyhadsex–onlythatpatientcanreportthattheyhadsexwithanHIV‐infectedpersonatthetimeofHCSFcompletion.
Beenacommercialsexworker
Patienthasexchangedsexformoneyorothermaterialgoods
Sharedneedleswhenusingdrugs
Patientreportedsharingneedleswheninjectingdrugs
Sexwithmultiplepartners
Patienthadanal,oral,orvaginalsexwithmultiplepartnersinthepastyear
Receivedbloodtransfusionorbloodcomponents
Patientreportedbeingarecipientofabloodtransfusionorbloodcomponent
Receivedtransplantoftissueororganorartificialinsemination
Patientreportedhavingreceivedtransplantoftissueororgan,orhadanartificialinsemination
Occupationalexposureinhealthcaresettingorlaboratory
Patientreportedhavingbeenexposedtoblood/bloodcomponentswhileperforminghis/herjobinahealthcaresettingorlaboratory
PerinatalexposuretoHIV
PatienthadbeenexposedtoHIVthroughmother‐to‐childtransmission(borntoaHIV+mother)
Beenavictimofsexualassault
Patientreportedbeingavictimofsexualassault
16
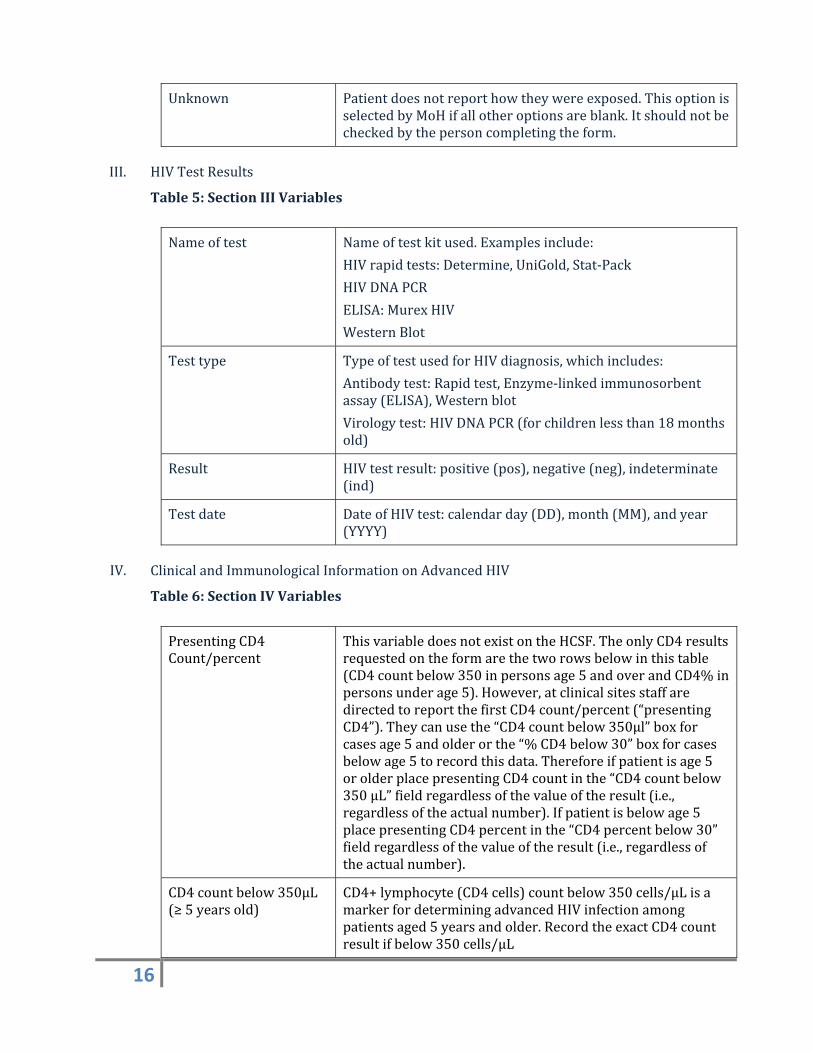
Unknown Patientdoesnotreporthowtheywereexposed.ThisoptionisselectedbyMoHifallotheroptionsareblank.Itshouldnotbecheckedbythepersoncompletingtheform.
III. HIVTestResults
Table5:SectionIIIVariables
Nameoftest Nameoftestkitused.Examplesinclude:
HIVrapidtests:Determine,UniGold,Stat‐Pack
HIVDNAPCR
ELISA:MurexHIV
WesternBlot
Testtype TypeoftestusedforHIVdiagnosis,whichincludes:
Antibodytest:Rapidtest,Enzyme‐linkedimmunosorbentassay(ELISA),Westernblot
Virologytest:HIVDNAPCR(forchildrenlessthan18monthsold)
Result HIVtestresult:positive(pos),negative(neg),indeterminate(ind)
Testdate DateofHIVtest:calendarday(DD),month(MM),andyear(YYYY)
IV. ClinicalandImmunologicalInformationonAdvancedHIV
Table6:SectionIVVariables
PresentingCD4Count/percent
ThisvariabledoesnotexistontheHCSF.TheonlyCD4resultsrequestedontheformarethetworowsbelowinthistable(CD4countbelow350inpersonsage5andoverandCD4%inpersonsunderage5).However,atclinicalsitesstaffaredirectedtoreportthefirstCD4count/percent(“presentingCD4”).Theycanusethe“CD4countbelow350µl”boxforcasesage5andolderorthe“%CD4below30”boxforcasesbelowage5torecordthisdata.Thereforeifpatientisage5orolderplacepresentingCD4countinthe“CD4countbelow350µL”fieldregardlessofthevalueoftheresult(i.e.,regardlessoftheactualnumber).Ifpatientisbelowage5placepresentingCD4percentinthe“CD4percentbelow30”fieldregardlessofthevalueoftheresult(i.e.,regardlessoftheactualnumber).
CD4countbelow350µL(≥5yearsold)
CD4+lymphocyte(CD4cells)countbelow350cells/µLisamarkerfordeterminingadvancedHIVinfectionamongpatientsaged5yearsandolder.RecordtheexactCD4countresultifbelow350cells/µL
17
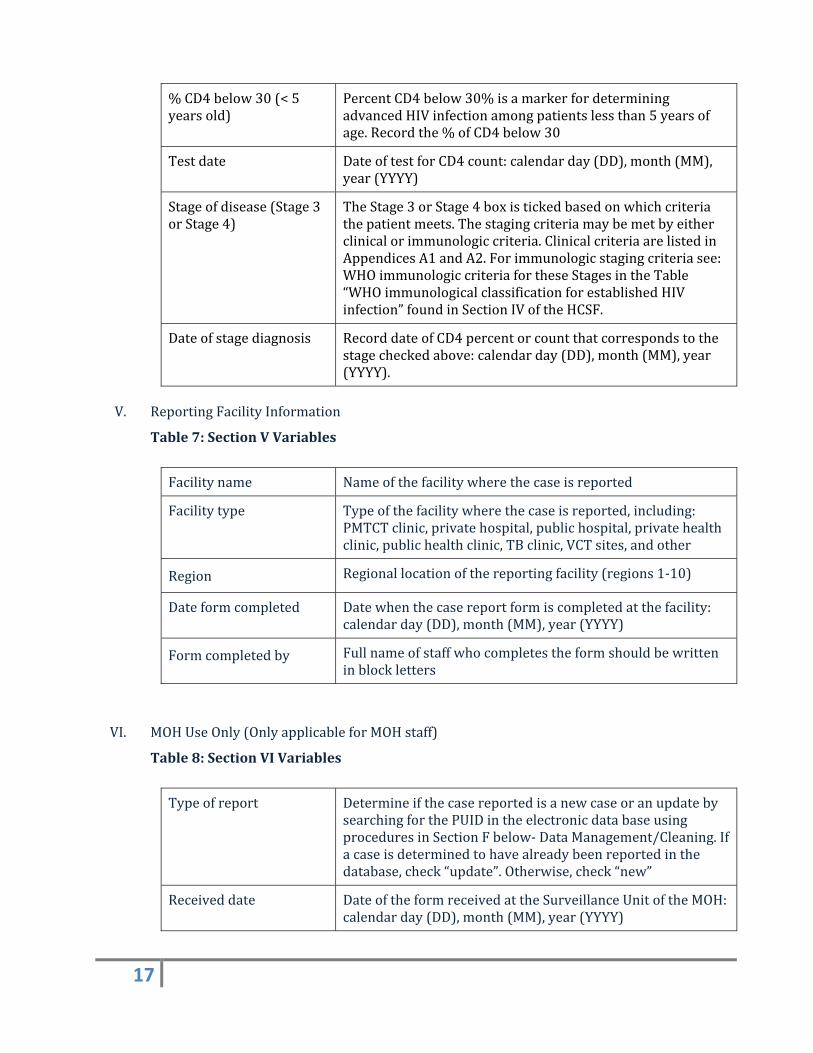
%CD4below30(<5yearsold)
PercentCD4below30%isamarkerfordeterminingadvancedHIVinfectionamongpatientslessthan5yearsofage.Recordthe%ofCD4below30
Testdate DateoftestforCD4count:calendarday(DD),month(MM),year(YYYY)
Stageofdisease(Stage3orStage4)
TheStage3orStage4boxistickedbasedonwhichcriteriathepatientmeets.Thestagingcriteriamaybemetbyeitherclinicalorimmunologiccriteria.ClinicalcriteriaarelistedinAppendicesA1andA2.Forimmunologicstagingcriteriasee:WHOimmunologiccriteriafortheseStagesintheTable“WHOimmunologicalclassificationforestablishedHIVinfection”foundinSectionIVoftheHCSF.
Dateofstagediagnosis RecorddateofCD4percentorcountthatcorrespondstothestagecheckedabove:calendarday(DD),month(MM),year(YYYY).
V. ReportingFacilityInformation
Table7:SectionVVariables
Facilityname Nameofthefacilitywherethecaseisreported
Facilitytype Typeofthefacilitywherethecaseisreported,including:PMTCTclinic,privatehospital,publichospital,privatehealthclinic,publichealthclinic,TBclinic,VCTsites,andother
Region Regionallocationofthereportingfacility(regions1‐10)
Dateformcompleted Datewhenthecasereportformiscompletedatthefacility:calendarday(DD),month(MM),year(YYYY)
Formcompletedby Fullnameofstaffwhocompletestheformshouldbewritteninblockletters
VI. MOHUseOnly(OnlyapplicableforMOHstaff)
Table8:SectionVIVariables
Typeofreport DetermineifthecasereportedisanewcaseoranupdatebysearchingforthePUIDintheelectronicdatabaseusingproceduresinSectionFbelow‐DataManagement/Cleaning.Ifacaseisdeterminedtohavealreadybeenreportedinthedatabase,check“update”.Otherwise,check“new”
Receiveddate DateoftheformreceivedattheSurveillanceUnitoftheMOH:calendarday(DD),month(MM),year(YYYY)
18
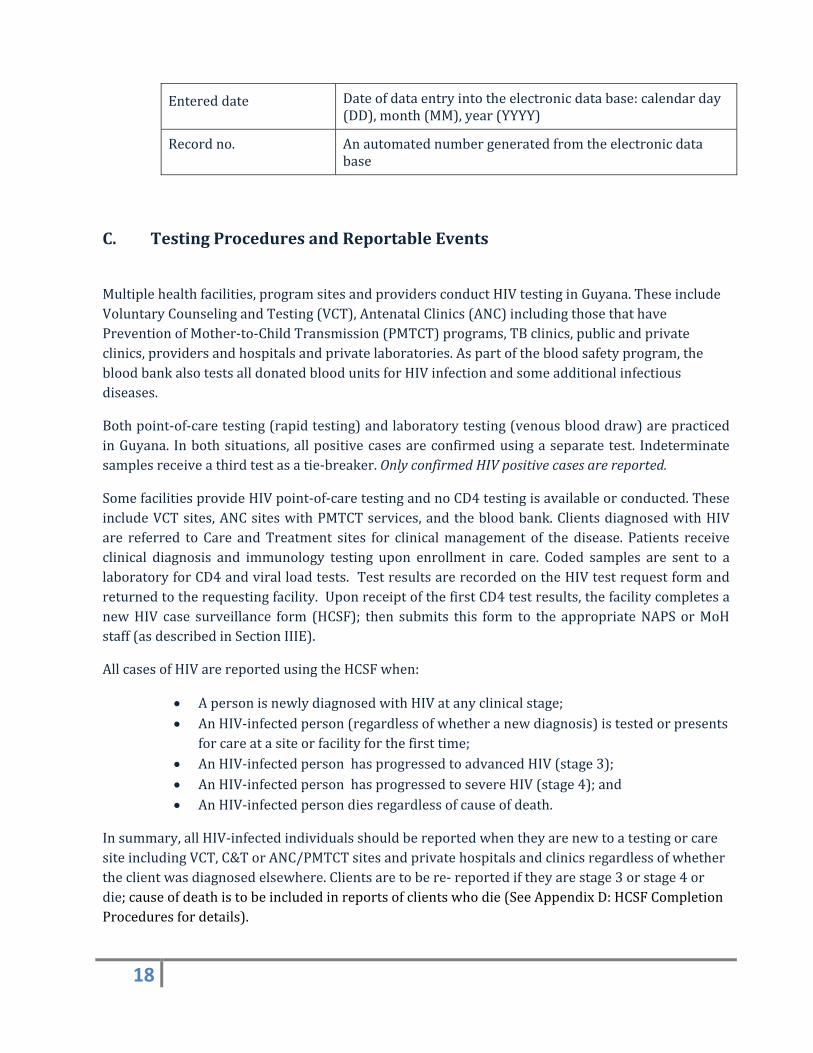
Entereddate Dateofdataentryintotheelectronicdatabase:calendarday(DD),month(MM),year(YYYY)
Recordno. Anautomatednumbergeneratedfromtheelectronicdatabase
C. TestingProceduresandReportableEvents
Multiplehealthfacilities,programsitesandprovidersconductHIVtestinginGuyana.TheseincludeVoluntaryCounselingandTesting(VCT),AntenatalClinics(ANC)includingthosethathavePreventionofMother‐to‐ChildTransmission(PMTCT)programs,TBclinics,publicandprivateclinics,providersandhospitalsandprivatelaboratories.Aspartofthebloodsafetyprogram,thebloodbankalsotestsalldonatedbloodunitsforHIVinfectionandsomeadditionalinfectiousdiseases.
Bothpoint‐of‐caretesting(rapidtesting)andlaboratorytesting(venousblooddraw)arepracticedinGuyana. Inbothsituations,allpositivecasesareconfirmedusingaseparatetest. Indeterminatesamplesreceiveathirdtestasatie‐breaker.OnlyconfirmedHIVpositivecasesarereported.
SomefacilitiesprovideHIVpoint‐of‐caretestingandnoCD4testingisavailableorconducted.TheseincludeVCTsites,ANCsiteswithPMTCTservices,andthebloodbank.ClientsdiagnosedwithHIVare referred to Care andTreatment sites for clinicalmanagement of the disease. Patients receiveclinical diagnosis and immunology testing upon enrollment in care. Coded samples are sent to alaboratoryforCD4andviralloadtests.TestresultsarerecordedontheHIVtestrequestformandreturnedtotherequestingfacility.UponreceiptofthefirstCD4testresults,thefacilitycompletesanewHIV case surveillance form (HCSF); then submits this form to the appropriateNAPSorMoHstaff(asdescribedinSectionIIIE).
AllcasesofHIVarereportedusingtheHCSFwhen:
ApersonisnewlydiagnosedwithHIVatanyclinicalstage; AnHIV‐infectedperson(regardlessofwhetheranewdiagnosis)istestedorpresents
forcareatasiteorfacilityforthefirsttime; AnHIV‐infectedpersonhasprogressedtoadvancedHIV(stage3); AnHIV‐infectedpersonhasprogressedtosevereHIV(stage4);and AnHIV‐infectedpersondiesregardlessofcauseofdeath.
Insummary,allHIV‐infectedindividualsshouldbereportedwhentheyarenewtoatestingorcaresiteincludingVCT,C&TorANC/PMTCTsitesandprivatehospitalsandclinicsregardlessofwhethertheclientwasdiagnosedelsewhere.Clientsaretobere‐reportediftheyarestage3orstage4ordie;causeofdeathistobeincludedinreportsofclientswhodie(SeeAppendixD:HCSFCompletionProceduresfordetails).
19
D. ReportingSources SourcesofHIVCaseSurveillanceReportForms
WiththesystemofHIVservicesdescribedabove,thefollowingarelocationswherepeoplearetestedforHIVand,therefore,aresourcesofHIVcasereports:
VCTsites ANCsiteswithandwithoutPMTCTservices TBclinics CareandTreatmentSites Publicandprivatehospitals Privateprovidersandclinics Privatelaboratories
AteachofthesesitespersonswhoconductHIVtestingareresponsibleforcompletingtheHIVCaseSurveillanceForm(HCSF)forallpersonsdiagnosedwithHIV.EachsiteisthenrequiredtosubmitallHCSFtotheMoH/NAPS(dataflowdescribedindetailinSectionIIIEbelow.InadditiontothesesourcesofHIVcasereports,theNationalPublicHealthLaboratoryConductsCD4testingandprovidestheresultstorequestingclinicalstaffwhoincludetheCD4resultsinSectionIVoftheHCSF.
• DeathRegistry
ObtainingreportsofdeathonpersonspreviouslyreportedwithHIVisessentialtoaccuratelymeasurethenumberofpeoplelivingwithHIVinGuyana.AmatchwillbeconductedannuallytoobtainvitalstatusofpersonsreportedwithHIVtoproducethemostreliableup‐to‐datecountofpersonslivingwithHIVinGuyana.AmatchtoobtaincauseofdeathusingverifiedICD‐10codesisconductedeverytwoyears.AprocedureforthisisinAppendixG.ReportsonHIVrelateddeathsarealsoacquiredwhen:
1. Sitescallclientsintheeventtheymissanappointment,onlytofindouttheclientdied;
2. VeryillclientsaresenttotheHospice,whothenreporttothereferringsiteintheeventtheclientdies;
3. Familymembersinformsitewhentheclientsdie;and
4. OutreachOfficerreceivesthisinformationwhenoutinthefieldscheckinguponclients.
E. ReportingProceduresTheprogramareasatNAPS/MoHresponsibleforprocessingHCSFsfromvariouspartsofthehealthsectorareasfollows:
20
• VCTsites–sendreportstoVCTstaffatNAPS ANCsiteswithandwithoutPMTCTservices‐sendreportstoPMTCTstaffatMoH TBclinics‐sendreportstoVCTstaffatNAPS CareandTreatmentSites‐sendreportstoC&TstaffatNAPS Publicandprivatehospitals‐sendreportstoVCTstaffatNAPS Privateproviders,laboratoriesandclinics‐sendreportstoVCTstaffatNAPS
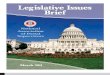
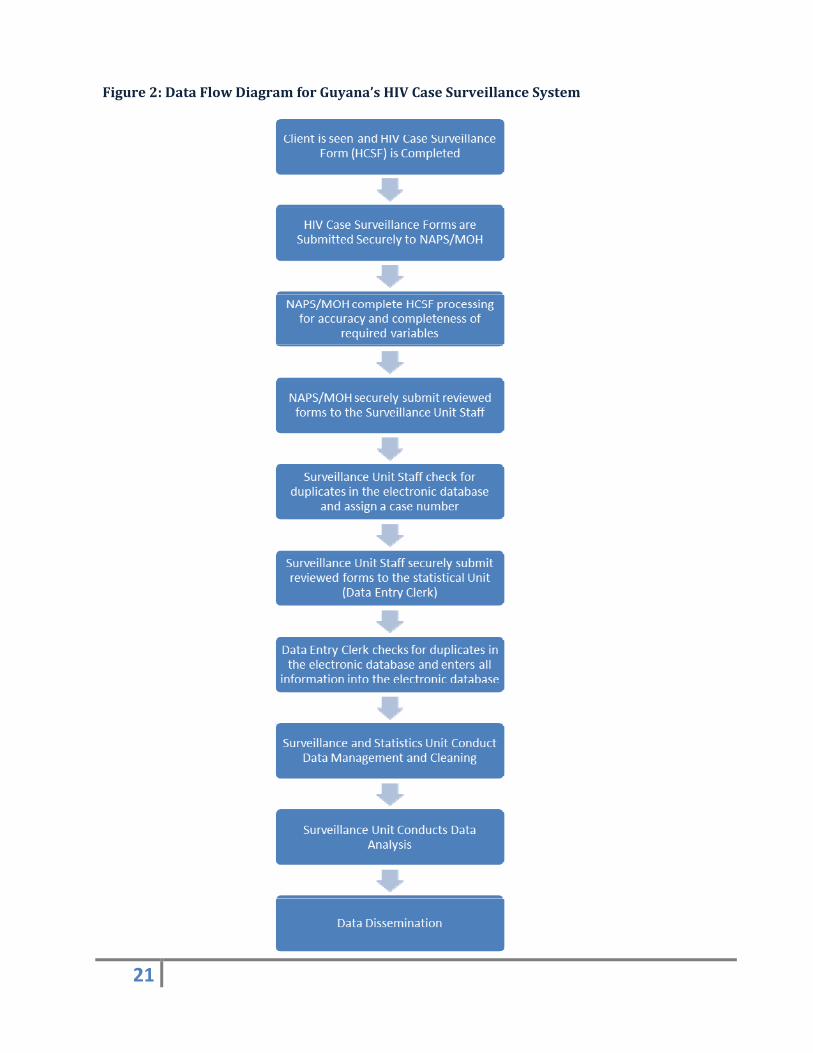
ThedataflowforHIVcasereportingbetweenthesiteslistedaboveandNAPSandMoHthroughtodatacleaning,analysisanddisseminationisdepictedinthedataflowdiagrambelow.Thisoverviewofthedataflowdiagramisfollowedbythreemorespecificdataflowdiagramsfor:1)VCT,2)C&Tand3)antenatalclinics.
21
Figure2:DataFlowDiagramforGuyana’sHIVCaseSurveillanceSystem
22
F. DescriptionofDataFlowDiagramforGuyana’sHIVCaseSurveillanceSystem
TheHIVCaseSurveillanceProcessincludesthestepsdescribedbelow.
1. DistributionofHIVCaseSurveillanceForms(HCSFs)
o NAPS distributes HIV Case Surveillance Forms to all sites conducting HIV testingexceptANCsites
o MoHPMTCTUnitdistributestheHIVCaseSurveillanceFormstoallANCsites
2. CompletionoftheHIVCaseSurveillanceForm(HCSF)
o ThecompletionoftheHCSFoccursat:
VCTsites
ANCsitesincludingthosewithPMTCTPrograms
C&Tsites
TBclinics
Healthcareproviders(publicandprivate)
Laboratories
Bloodbank
o RefertoSectionIIIBabovefordetaildescriptionofSectionsItoVIoftheHCSF
o SitesthatobtainCD4countresultsfromthelabarerequiredtocompleteSectionsI‐V.
o PMTCTandVCTarerequiredtocompleteSectionsI‐IIIandV.
o After forms are completed they are submitted for HCSF processing as listed inSection3belowwithin4‐weeksofpatientdiagnosis.However,everyeffortshouldbemadetosubmittheHCSFasquicklyaspossible.
o Questions regarding the completion of the HCSF should be directed to theSurveillanceUnitattheMinistryofHealth
3. HCSFSubmissiontoUnitsConductingHCSFProcessing
o AftercompletingtheHCSF:
VCT and C&T sites are responsible for securely transporting forms in a
timelyandsecuremannertoNAPS
23
PMTCTsitesareresponsibleforsecurelytransportingformsinatimelyand
securemannertoMCH
o PrivatefacilitiessubmitHCSFstovisitingEpi‐nursesinatimelyandsecuremanner.
EpiNursesareresponsibleforsecurelytransportingformsinatimelymannertothe
SurveillanceUnit.
4. HCSFProcessing
o HCSFProcessingiscompletedasfollows: NAPSVCT andC&Tunits andMoHPMTCT are responsible for completing
the following tasks as outlined in the HSCF Initial Review Procedures, inAppendixD:
Writedateofreceiptinthelefthandmargin,andinitial Ensurethatthemandatoryvariablesarecompleted Identifymissing,questionable,orincompletevariables,andfollowup
with the person who completed the form onsite to obtain missingvariables
EpidemiologicalNurses return formswithmissing, questionable, orincomplete variables, and follow up with personnel at the privatefacilitywhocompletedtheform/s.
After initial quality checks all HCSFs should be submitted to theSurveillanceUnitwithin aweek of receipt byNAPSorMoH staff. Ifcontactneedstobemadewithpersoncompletingtheformtoclarifyinformation every attempt should be made to submit form to theSurveillanceUnitwithintwoweeksofreceipt
Ministry of Health Surveillance Unit completes the following tasks asoutlinedintheHCSFSecondaryReviewProcedures,inAppendixE: Writedateofreceiptinthelefthandmargin,andinitial De‐duplicationusingtheelectronicdatabase CompletetheReportTypevariableasNeworUpdateinSectionVI AssigneachuniquepersonasequentialCaseNumber Forms should be submitted to Statistical Unit staff for data entry
withinaweekofreceipt
5. DataEntryo MinistryofHealthStatisticalUnitDataEntryClerkcompletesthefollowingtasksas
outlinedinDataEntryProceduresinAppendixF: CompleteDateReceivedandEntryDateinSectionVIofHCSF De‐duplicationusingtheelectronicdatabase Formsshouldbeenteredandfiledwithinaweekofreceipt.
24
6. DataManagementandCleaning
o The Statistical Unit facilitates datamanagement and cleaning on a quarterly basis.Thisincludescompletionofthefollowingtasks:
1. Statistical Unit Officer develops and runs a standard analytic program thatproduces lists of cases with potential duplicates as well as suspect,inconsistentor incompletedemographicordiagnostic information,orotherquestionableordiscrepantdata.
2. Establishes data cleaning schedule and routines (i.e., what computerprograms are used and what potential discrepancies are checked‐ forexample‐duplicates).IntheinitialphaseoftheHIVcaseSurveillanceSystemthese activities will be conducted monthly to any significant or obviouserrors.Oncethenumberoferrorsdecreasesaquarterlyschedulewillthenbeestablished.
3. Generatesalistofpotentialduplicates.
4. SubmitsresultstotheSurveillanceUnitStaffonamonthlybasis.
o TheSurveillanceUnitthencompletesthedatamanagementandcleaningprocessbycompletingthefollowingtasks:
1. PullpaperHCSFsandcomparethemwiththeinformationintheelectronicdatabasetoidentifyanydiscrepanciesandfollowupwithappropriatestafftorectify.
7. DataAnalysis
o This section contains a list of commonly used reports. However, it should not beconsideredastaticlist.Whatiscontainedinthereportsandhowfrequentlytheyarerunisadjustedinresponsetotheeffectiveutilizationofdataforprogramplanning,developmentandmonitoring.Additionalreportswillbeneededas thesurveillancesystemmaturesandthedataareusedtoplanandevaluatepreventionprogramsandplanforcareofpeoplelivingwithHIVAIDS(PLWH).Examplesoffuturereportstoconsiderare:
• Compareregionof facilitywithregionofpatient residence toquantifyhowmuch testing of PLWH is being done outside of the patient’s region ofresidence. You can use this type of analysis to decide where more testingservicesmaybeneeded.
• Analyzeoccupationbyregionofresidencetoassistwiththedevelopmentoftargetedpreventionprograms
25
• Measure howmany people are tested that do not go into care by sex, age,region,occupation,etc.
• MeasuretimebetweentestingandentrytoC&T
o TwiceayeartheSurveillanceUnitrunsthefollowingreports:
Numberofi)newlydiagnosedHIVcases,ii)prevalent(living)HIVcases,iii)advancedHIVcases(stage3),iv)severeHIVcases(Stage4),v)cumulativecasesandvi)deaths,stratifiedby:
o Agegroupatdiagnosis,Forexample: <1 year 1‐4 years 5‐12 years 13‐14 years 15‐19 years 20‐24 years 25‐29 years 30‐34 years 35‐39 years 40‐44 years 45‐49 years ≥ 50
Unknowno Sexo Regionofresidenceatdiagnosiso Race/Ethnicity
o Onceayear,theSurveillanceUnitrunsthefollowingreports:
Total number and percent of newly diagnosed HIV cases, advanced HIV cases(stage3),andsevereHIVcases(stage4).AllreportedHIVcasesstratifiedby:
o Agegroupandsexo Region and sex (may not be applicable for all areas, depending on
morbidity)o Ethnicityandsexo Exposurecategoryandsexo Exposurecategoryandethnicity(maynotbeapplicableforallcategories,
dependingonmorbidity) TrendsinnewlydiagnosedHIVcases,advancedHIVcasesanddeaths,stratified
byagegroup,sex,raceandexposurecategory.Inordertominimizetheinfluenceofreportingdelayontrendssuchanalysesisconductedoncasesreportedsixormore months before the analysis date. This decreases the likelihood that thetrendsarebasedonincompletedata.
8. DataDissemination
26
o Dataisdistributedtothefollowingentities:
NAPS VCT and C&T for the purpose of planning and evaluating preventionprograms, planning care programs, program management, monitoring andevaluation
MoH PMTCT for the purpose of program management, monitoring andevaluation
Stakeholders (i.e. MoH, NAPS, funders, partners) for policy and protocoldevelopment
TheNAPSwebsiteforpublicaccess
27
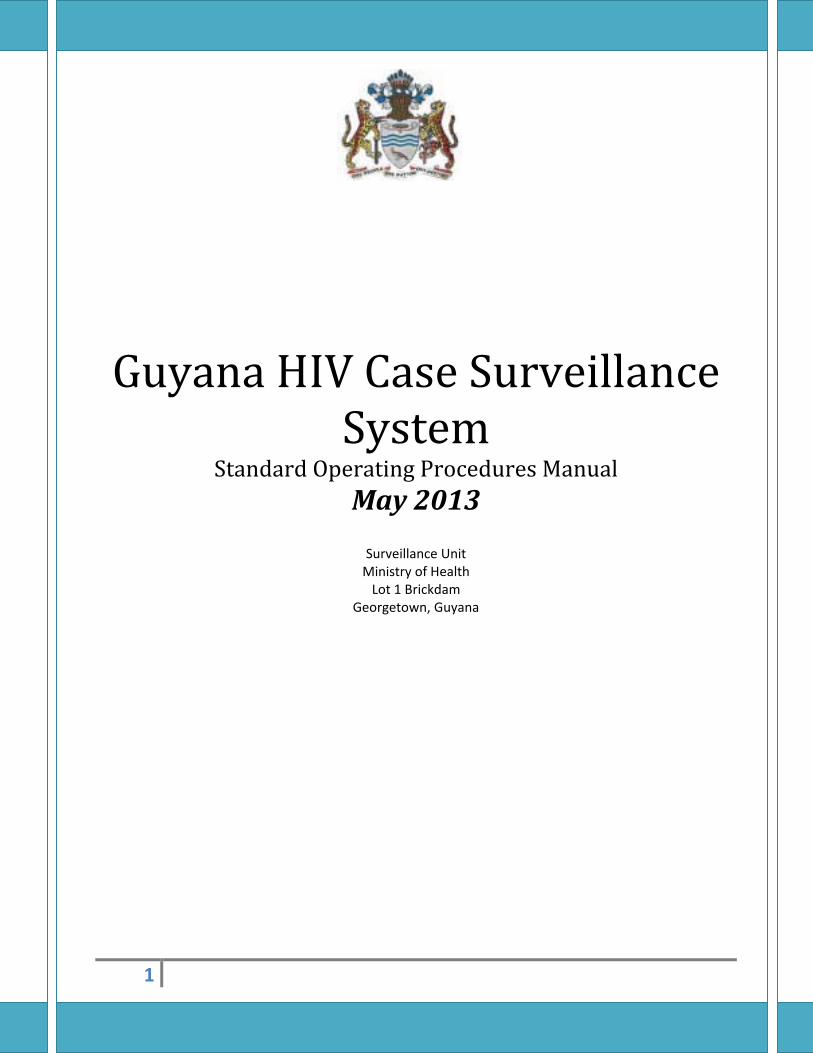
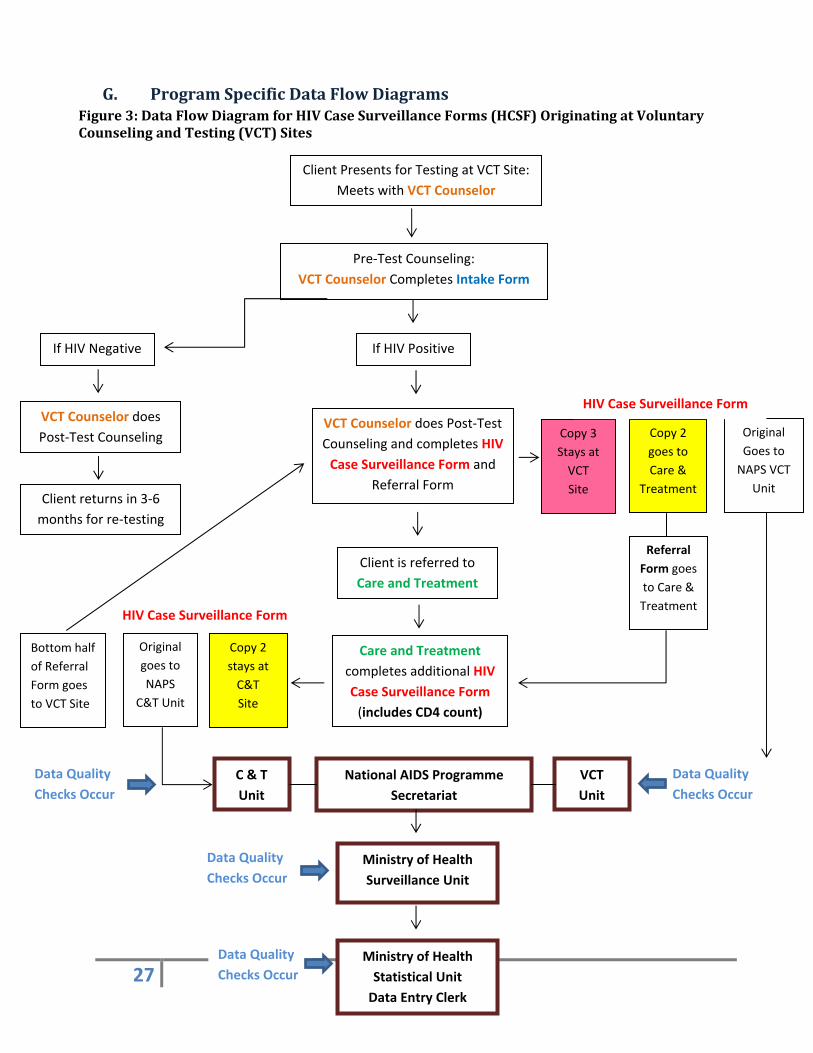
G. ProgramSpecificDataFlowDiagramsFigure3:DataFlowDiagramforHIVCaseSurveillanceForms(HCSF)OriginatingatVoluntaryCounselingandTesting(VCT)Sites
Client Presents for Testing at VCT Site:
Meets with VCT Counselor
Pre‐Test Counseling:
VCT Counselor Completes Intake Form
If HIV Negative If HIV Positive
VCT Counselor does
Post‐Test Counseling
Client returns in 3‐6
months for re‐testing
VCT Counselor does Post‐Test
Counseling and completes HIV
Case Surveillance Form and
Referral Form
Original
Goes to
NAPS VCT
Unit
Copy 2
goes to
Care &
Treatment
Copy 3
Stays at
VCT
Site
Client is referred to
Care and Treatment
Care and Treatment
completes additional HIV
Case Surveillance Form
(includes CD4 count)
Original
goes to
NAPS
C&T Unit
Copy 2
stays at
C&T
Site
National AIDS Programme
Secretariat
Ministry of Health
Surveillance Unit
Referral
Form goes
to Care &
Treatment
HIV Case Surveillance Form
Bottom half
of Referral
Form goes
to VCT Site
HIV Case Surveillance Form
C & T
Unit
VCT
Unit
Ministry of Health
Statistical Unit
Data Entry Clerk
Data Quality
Checks Occur
Data Quality
Checks Occur
Data Quality
Checks Occur
Data Quality
Checks Occur
28
DescriptionofDataFlowDiagramforHIVCaseSurveillanceForms(HCSF)OriginatingatVoluntaryCounselingandTesting(VCT)Sites
ClientistestedforHIVatVCTsite:1. ClientpresentsforTestingataVCTsite.2. VCTcounselorconductspre‐testcounselingandcompletesanIntakeForm.3. VCTcounselorconductstherapidHIVtestalgorithm(twoparalleltests):
i. IfbothtestresultsindicatetheclientisHIVnegative,theVCTcounselorconductspost‐testcounselingandencouragestheclienttoreturnin3‐6monthsforre‐testing.
ii. IfbothtestresultsindicatetheclientisHIVpositive,VCTcounselorcontinueswithStep4,describedbelow.Ifonetestispositiveandtheotherisnegativeanothertestisimmediatelyconductedatthetestingsite.Ifthe“tie‐breaker”testispositive,theclientisreferredtocareandtreatment.Ifthetie‐breakertestisnegative,theclientiscounseledandadvisedtoreturnforadditionaltestinginthreemonths.
IfclientisdeterminedtobeHIVpositive:4. VCTcounselorconductspost‐testcounselingandcompletesthefollowingforms:
ReferralForm TriplicateHIVCaseSurveillanceForm(HCSF)
Originalcopy(white)oftheHCSFissenttotheNAPSVCTUnitsothatthemostlegiblecopyisavailablefordataentrytominimizedataentryerrors.
Copy#2(yellow)oftheHCSFandthereferralformareeithergiventothepatient,whopresentsittoCare&TreatmentorgiventotheCaseNavigatorwhopresentsboththeclientandcopyofHCSFtoCareandTreatment(C&T).
Copy#3(pink)remainsattheVCTreportingsite5. VCTcounselorreferstheclienttoaC&Tsite,andinstructstheclienttobringCopy#2
(yellow)oftheHCSFandtheReferralForm(perforated)withthemwhentheyenrollinC&T.WhenclientisreferredtoCare&Treatment:
6. ClientpresentsatC&TsitewithCopy#2(yellow)oftheHCSFandtheReferralForm.7. C&TstaffcompletesanewduplicateHIVCaseSurveillanceForm(HCSF)atintake:
C&TstaffrecordspresentingCD4countinSectionIVoftheHCSFatthetimeclientpresentsandchecksStage3orStage4,ifapplicable,basedoncurrentimmunologicstatusand/orclinicaldiagnoses(SeeWHOimmunologiccriterialistedinSectionIVoftheHCSFortheclinicalcriteriainAppendixA)
Original(white)copyoftheHCSFissenttotheNAPSC&TUnit Copy#2(yellow)oftheHCSFremainsattheC&Tsite
8. C&TstaffpresentsthebottomhalfoftheperforatedreferralformandsendsitbacktotheVCTsitethatreferredthepatient.ThisallowstheVCTstafftoknowthatthepatientenrolledinC&T.
NationalAIDSProgrammeSecretariat(NAPS)
9. TheNAPSVCTUnitreceivestheoriginalcopy(white)oftheHCSFthattheVCTcounselorcompletedattheVCTsiteforeachHIVpositiveclient.
29
i. NAPSVCTUnitstaffwritesthedatereceivedandhis/herinitialsintheleftmarginofeachHCSFthathe/shereceives
ii. NAPSVCTUnitstaffdoesaqualitycheckoneachHCSFthathe/shereceives(SeeHCSFInitialReviewProcedurefordetails)
iii. NAPSVCTUnitstaffsubmitsallHCSFstotheMinistryofHealthSurveillanceUnit10. TheNAPSC&TUnitreceivestheoriginalcopy(white)oftheHCSFthattheC&Tstaff
completedattheC&TsiteforeachHIVpositiveclient:i. NAPSC&TUnitstaffwritesthedatereceivedandhis/herinitialsintheleftmarginof
eachHCSFthathe/shereceivesii. NAPSC&TUnitstaffdoesaqualitycheckoneachHCSFthathe/shereceives(See
HCSFInitialReviewProcedurefordetails)iii. NAPSC&TUnitstaffsubmitsallHCSFstotheMinistryofHealthSurveillanceUnit
MinistryofHealth(MoH)11. MinistryofHealthSurveillanceUnitreceives2originalsoftheHCSFforeachHIVpositive
clientthatenterscare,onefromtheNAPSVCTUnitandonefromtheNAPSC&TUnit:i. MoHSurveillanceUnitstaffwritesthedatereceivedandhis/herinitialsintheleft
marginofeachHCSFthathe/shereceivesii. MoHSurveillanceUnitstaffchecksallHCSFsagainsttheelectronicdatabaseto
ensurethattherearenoduplicates(SeeHCSFSecondaryReviewProcedurefordetails)
iii. MoHSurveillanceUnitstaffassignseachuniquepersonaCaseNumber(SeeHCSFSecondaryReviewProcedurefordetails)
iv. MoHSurveillanceUnitstaffsubmitsallHCSFstotheMinistryofHealthStatisticalUnit(DataEntryClerk)
12. MinistryofHealthStatisticalUnit(DataEntryClerk):i. TheDataEntryClerkcompletes“DateReceived”and“EntryDate”fieldsinSectionVI
ofeachHCSFreceivedii. TheDataEntryclerkchecksallHCSFsagainsttheelectronicdatabasetoensurethat
therearenoduplicates(seeDataEntryProcedurefordetails)iii. TheDataEntryclerkentersthecaseintotheelectronicdatabaseandrecordsthe
“RecordNumber”generatedbytheElectronicDatabaseontheHCSF
30
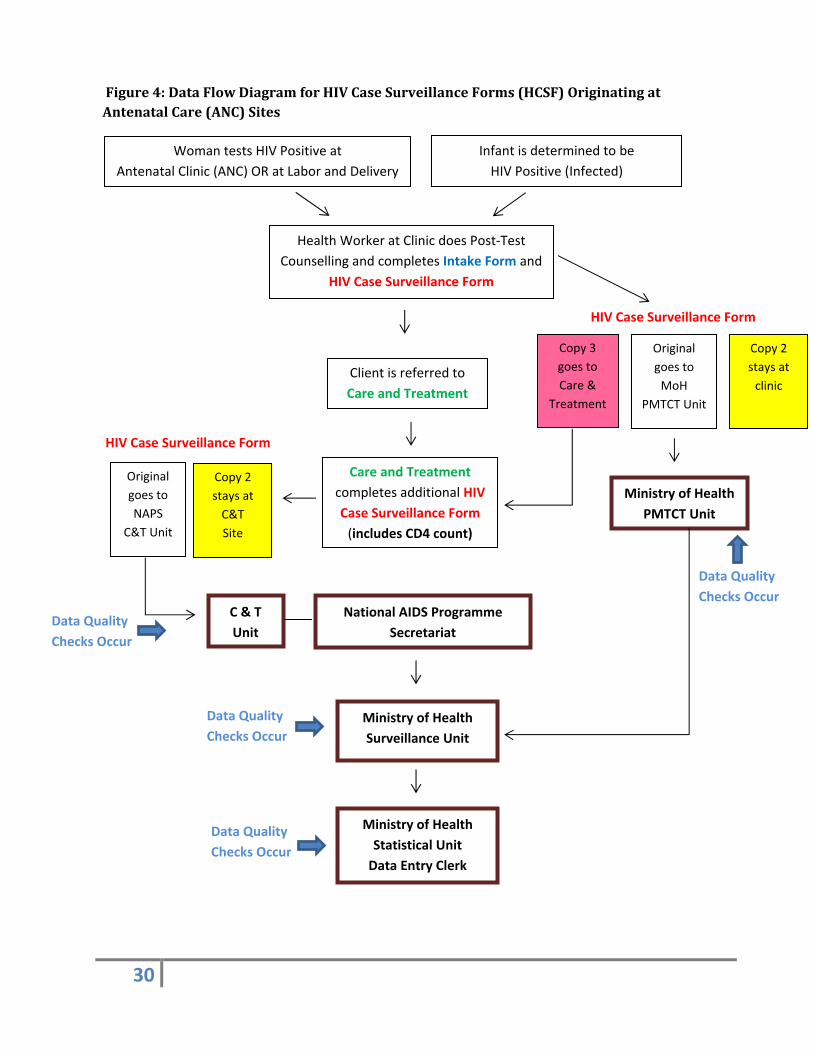
Figure4:DataFlowDiagramforHIVCaseSurveillanceForms(HCSF)OriginatingatAntenatalCare(ANC)Sites
Woman tests HIV Positive at
Antenatal Clinic (ANC) OR at Labor and Delivery
Health Worker at Clinic does Post‐Test
Counselling and completes Intake Form and
HIV Case Surveillance Form
Original
goes to
MoH
PMTCT Unit
Copy 2
stays at
clinic
Copy 3
goes to
Care &
Treatment
Client is referred to
Care and Treatment
Care and Treatment
completes additional HIV
Case Surveillance Form
(includes CD4 count)
Original
goes to
NAPS
C&T Unit
Copy 2
stays at
C&T
Site
National AIDS Programme
Secretariat
Ministry of Health
Surveillance Unit
HIV Case Surveillance Form
HIV Case Surveillance Form
C & T
Unit
Ministry of Health
Statistical Unit
Data Entry Clerk
Data Quality
Checks Occur
Data Quality
Checks Occur
Data Quality
Checks Occur
Data Quality
Checks Occur
Infant is determined to be
HIV Positive (Infected)
Ministry of Health
PMTCT Unit
31
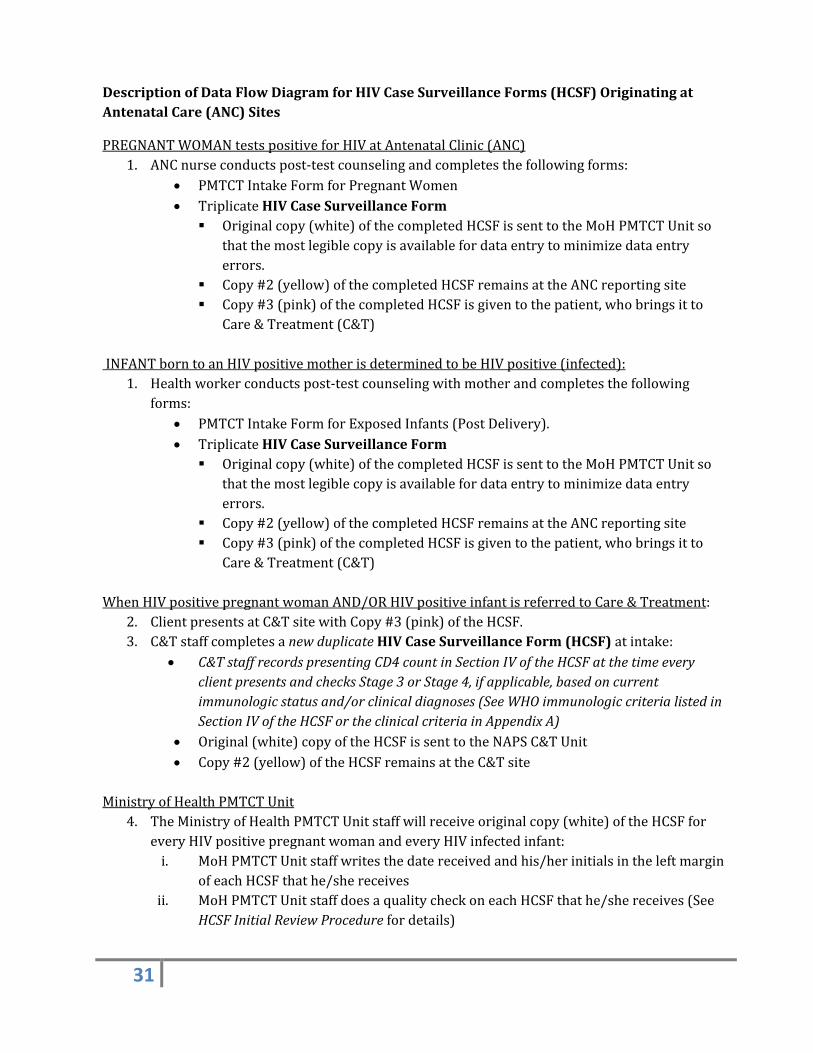
DescriptionofDataFlowDiagramforHIVCaseSurveillanceForms(HCSF)OriginatingatAntenatalCare(ANC)Sites
PREGNANTWOMANtestspositiveforHIVatAntenatalClinic(ANC)1. ANCnurseconductspost‐testcounselingandcompletesthefollowingforms:
PMTCTIntakeFormforPregnantWomen TriplicateHIVCaseSurveillanceForm Originalcopy(white)ofthecompletedHCSFissenttotheMoHPMTCTUnitso
thatthemostlegiblecopyisavailablefordataentrytominimizedataentryerrors.
Copy#2(yellow)ofthecompletedHCSFremainsattheANCreportingsite Copy#3(pink)ofthecompletedHCSFisgiventothepatient,whobringsitto
Care&Treatment(C&T)INFANTborntoanHIVpositivemotherisdeterminedtobeHIVpositive(infected):
1. Healthworkerconductspost‐testcounselingwithmotherandcompletesthefollowingforms:
PMTCTIntakeFormforExposedInfants(PostDelivery). TriplicateHIVCaseSurveillanceForm Originalcopy(white)ofthecompletedHCSFissenttotheMoHPMTCTUnitso
thatthemostlegiblecopyisavailablefordataentrytominimizedataentryerrors.
Copy#2(yellow)ofthecompletedHCSFremainsattheANCreportingsite Copy#3(pink)ofthecompletedHCSFisgiventothepatient,whobringsitto
Care&Treatment(C&T)WhenHIVpositivepregnantwomanAND/ORHIVpositiveinfantisreferredtoCare&Treatment:
2. ClientpresentsatC&TsitewithCopy#3(pink)oftheHCSF.3. C&TstaffcompletesanewduplicateHIVCaseSurveillanceForm(HCSF)atintake:
C&TstaffrecordspresentingCD4countinSectionIVoftheHCSFatthetimeeveryclientpresentsandchecksStage3orStage4,ifapplicable,basedoncurrentimmunologicstatusand/orclinicaldiagnoses(SeeWHOimmunologiccriterialistedinSectionIVoftheHCSFortheclinicalcriteriainAppendixA)
Original(white)copyoftheHCSFissenttotheNAPSC&TUnit Copy#2(yellow)oftheHCSFremainsattheC&Tsite
MinistryofHealthPMTCTUnit
4. TheMinistryofHealthPMTCTUnitstaffwillreceiveoriginalcopy(white)oftheHCSFforeveryHIVpositivepregnantwomanandeveryHIVinfectedinfant:i. MoHPMTCTUnitstaffwritesthedatereceivedandhis/herinitialsintheleftmargin
ofeachHCSFthathe/shereceivesii. MoHPMTCTUnitstaffdoesaqualitycheckoneachHCSFthathe/shereceives(See
HCSFInitialReviewProcedurefordetails)
32
iii. MoHPMTCTUnitstaffrecordsthePMTCTcodesinthemarginofeachHCSFthathe/shereceives
iv. PMTCTunitthensubmitsHCSFtotheSurveillanceUnit.MinistryofHealth(MoH)
5. MinistryofHealthSurveillanceUnitreceivestwooriginalsoftheHCSFforeachHIVpositiveclientthatenterscare,onefromthePMTCTUnitandonefromtheNAPSC&TUnit:i. MoHSurveillanceUnitstaffwritesthedatereceivedandhis/herinitialsintheleft
marginofeachHCSFthathe/shereceivesii. MoHSurveillanceUnitstaffchecksallHCSFsagainsttheelectronicdatabaseto
ensurethattherearenoduplicates(SeeHCSFSecondaryReviewProcedurefordetails)
iii. MoHSurveillanceUnitstaffassignseachuniquepersonaCaseNumber(SeeHCSFSecondaryReviewProcedurefordetails)
iv. MoHSurveillanceUnitstaffsubmitsallHCSFstotheMinistryofHealthStatisticalUnit(DataEntryClerk)
6. MinistryofHealthStatisticalUnit(DataEntryClerk):v. TheDataEntryclerkcompletes“DateReceived”and“EntryDate”fieldsinSectionVI
ofeachHCSFreceivedvi. TheDataEntryclerkchecksallHCSFsagainsttheelectronicdatabasetoensurethat
therearenoduplicates(seeDataEntryProcedurefordetails)vii. TheDataEntryclerkenterscaseintotheelectronicdatabaseandrecordsthe
“RecordNumber”generatedbytheElectronicDatabaseontheHCSF
33
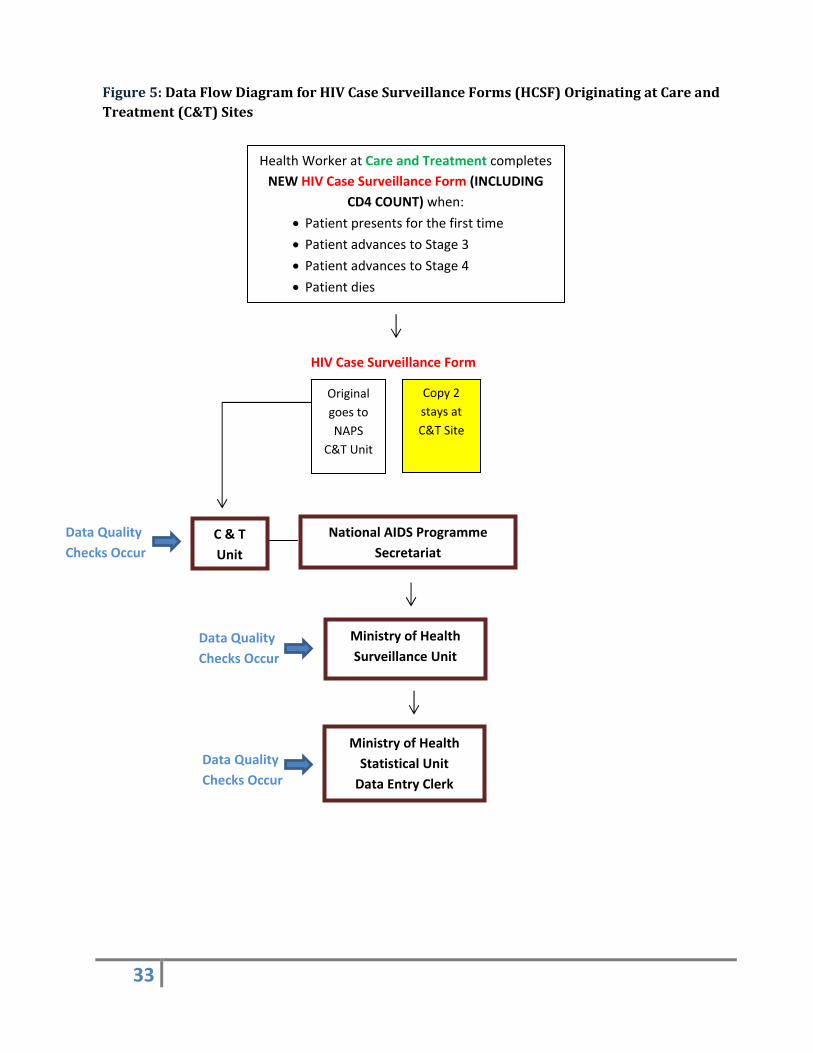
Figure5:DataFlowDiagramforHIVCaseSurveillanceForms(HCSF)OriginatingatCareandTreatment(C&T)Sites
Health Worker at Care and Treatment completes
NEW HIV Case Surveillance Form (INCLUDING
CD4 COUNT) when:
Patient presents for the first time
Patient advances to Stage 3 Patient advances to Stage 4 Patient dies
Original
goes to
NAPS
C&T Unit
Copy 2
stays at
C&T Site
National AIDS Programme
Secretariat
Ministry of Health
Surveillance Unit
HIV Case Surveillance Form
C & T
Unit
Ministry of Health
Statistical Unit
Data Entry Clerk
Data Quality
Checks Occur
Data Quality
Checks Occur
Data Quality
Checks Occur
34
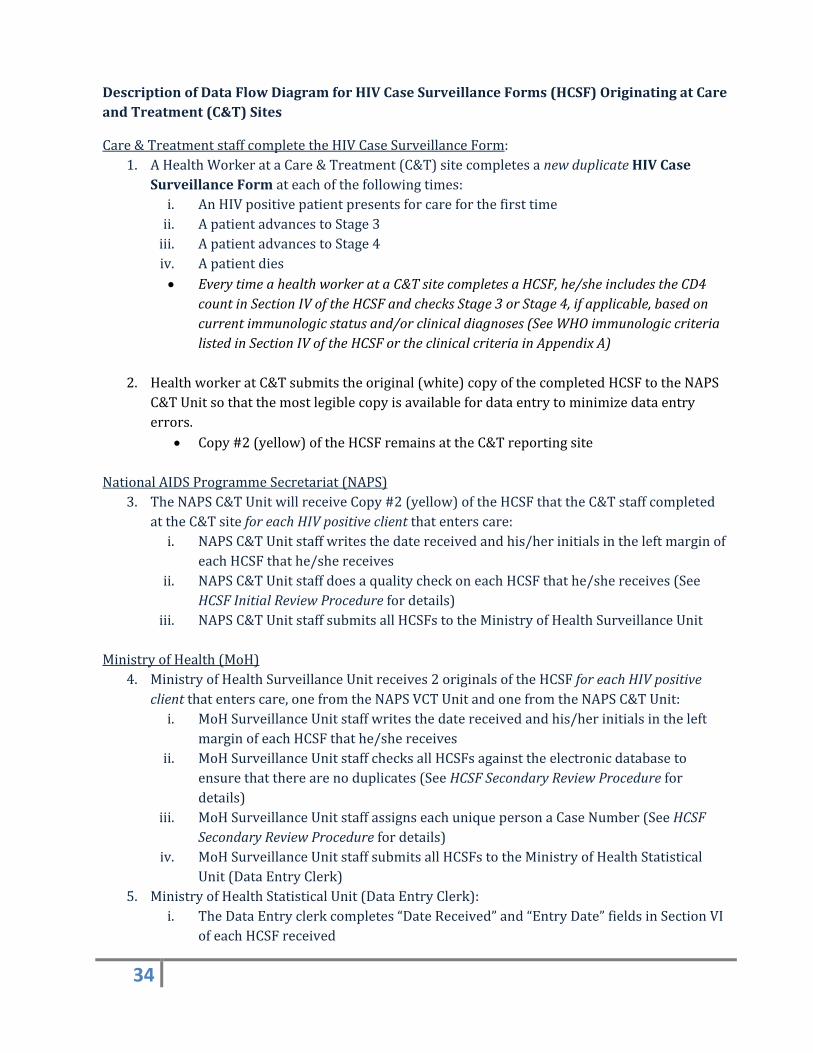
DescriptionofDataFlowDiagramforHIVCaseSurveillanceForms(HCSF)OriginatingatCareandTreatment(C&T)Sites
Care&TreatmentstaffcompletetheHIVCaseSurveillanceForm:1. AHealthWorkerataCare&Treatment(C&T)sitecompletesanewduplicateHIVCase
SurveillanceFormateachofthefollowingtimes:i. AnHIVpositivepatientpresentsforcareforthefirsttimeii. ApatientadvancestoStage3iii. ApatientadvancestoStage4iv. Apatientdies EverytimeahealthworkerataC&TsitecompletesaHCSF,he/sheincludestheCD4
countinSectionIVoftheHCSFandchecksStage3orStage4,ifapplicable,basedoncurrentimmunologicstatusand/orclinicaldiagnoses(SeeWHOimmunologiccriterialistedinSectionIVoftheHCSFortheclinicalcriteriainAppendixA)
2. HealthworkeratC&Tsubmitstheoriginal(white)copyofthecompletedHCSFtotheNAPSC&TUnitsothatthemostlegiblecopyisavailablefordataentrytominimizedataentryerrors.
Copy#2(yellow)oftheHCSFremainsattheC&TreportingsiteNationalAIDSProgrammeSecretariat(NAPS)
3. TheNAPSC&TUnitwillreceiveCopy#2(yellow)oftheHCSFthattheC&TstaffcompletedattheC&TsiteforeachHIVpositiveclientthatenterscare:i. NAPSC&TUnitstaffwritesthedatereceivedandhis/herinitialsintheleftmarginof
eachHCSFthathe/shereceivesii. NAPSC&TUnitstaffdoesaqualitycheckoneachHCSFthathe/shereceives(See
HCSFInitialReviewProcedurefordetails)iii. NAPSC&TUnitstaffsubmitsallHCSFstotheMinistryofHealthSurveillanceUnit
MinistryofHealth(MoH)4. MinistryofHealthSurveillanceUnitreceives2originalsoftheHCSFforeachHIVpositive
clientthatenterscare,onefromtheNAPSVCTUnitandonefromtheNAPSC&TUnit:i. MoHSurveillanceUnitstaffwritesthedatereceivedandhis/herinitialsintheleft
marginofeachHCSFthathe/shereceivesii. MoHSurveillanceUnitstaffchecksallHCSFsagainsttheelectronicdatabaseto
ensurethattherearenoduplicates(SeeHCSFSecondaryReviewProcedurefordetails)
iii. MoHSurveillanceUnitstaffassignseachuniquepersonaCaseNumber(SeeHCSFSecondaryReviewProcedurefordetails)
iv. MoHSurveillanceUnitstaffsubmitsallHCSFstotheMinistryofHealthStatisticalUnit(DataEntryClerk)
5. MinistryofHealthStatisticalUnit(DataEntryClerk):i. TheDataEntryclerkcompletes“DateReceived”and“EntryDate”fieldsinSectionVI
ofeachHCSFreceived
35
ii. TheDataEntryclerkchecksallHCSFsagainsttheelectronicdatabasetoensurethattherearenoduplicates(seeDataEntryProcedurefordetails)
iii. TheDataEntryclerkenterscaseintotheelectronicdatabaseandrecordsthe“RecordNumber”generatedbytheElectronicDatabaseontheHCSF
IV. SecurityandConfidentiality
HIVcontinues tobeassociatedwithsocial stigmaandanybreachof confidentialityposes risksofsocial, mental, economic and physical harm to HIV infected individuals. To ensure theconfidentialityofHIV infectedpatients, their informationmustbekept in secured areas and staffmust rigorously protect patient confidentiality. HIV case surveillance data collection, storage,transmission and use should follow procedures to protect any personally identifying information(PII). The policies below apply to any location where patient information is kept: clinics,laboratories,hospitals,NAPSandMoHoffices.
PersonallyIdentifyingInformation(PII)
PII is more than name. It includes any information that could potentially identify anindividual. On the HCSF PII includes initials of first and last name, date of birth and allcomponentsofthepatientaddress.
ThereforeanyHCSFthathasanyPIIwillbeprotectedasifithadthepatientnameonit.
PhysicalDataStorage
AllpaperHIVcasereportformsthatcontainanyPII,includingthosethatremaininthereportingfacilityandatMOH,mustbefiledandstoredinasecureplacesuchasalockedfilingcabinetthatcannotbeaccessedbyun‐authorizedstaffnorpatientsinthewaitingareaoranyothermembersofthegeneralpublic.
FormscontainingPIImustnotbeleftoutondesksorinanunsecuredfilefolderorenvelopewhenthepersonworkingatthedeskleaves.
IfsomeonecomesovertothedeskofanemployeeworkingwithformswithPIItheymustbecovered.
TransportingConfidentialInformation
WhentransportingcompletedHCSFstheymustbeplacedinasealedenvelopeandplacedinthetrunkorothercoveredareaofthevehicle.
Anystopsbetweenthefacilitycompletingtheformsandthedestinationshouldbekepttoaminimum.Workerstransportingthedatashoulddiscusswiththeirsupervisorwhethertheformsaremoresecurebeingbroughtwiththeemployeeorkeptinthevehicle.
ElectronicDataStorage
36
Electronicdatabaseshouldbepasswordprotectedandaccessedusingapasswordsecured.computerthatisbackeduponaserverandcannotbeaccessedbyun‐authorizedstaff
Datamustbebackedupregularly.OathsofConfidentiality
AllemployeeswithaccesstoPIIshouldreadandsigntheconfidentialityoathuponobtainingaccesstoPIIandannually.
SecurityandConfidentialityTraining
AllHIVhealthcareprovidersandMoHandNAPSstaffwhohaveaccesstoorworkwithHCSFsorotherformswithpersonallyidentifyinginformationshouldbetrainedonconfidentialityandsecurityprocedures.
Anannualtrainingshouldbeheld,thatincludesre‐signingtheoath.BreachProcedures
Aprocessforidentifyingandinvestigatingbreachesinsecurityandconfidentialityincludes:o Formsforreportingbreachesandproceduresforcompletingthemshouldbe
developed.o Consequencesforviolatingconfidentialityandsecurityshouldbedeveloped,and
staffeducatedontheramificationsforviolatingpoliciesandprocedures.
A. Training
SitesthatcompleteHCSFaretrainedminimallyonanannualbasis.Suchtrainingcanbeconductedinpersonoranonlinetrainingforsitestoaccessdirectly.PointstobecoveredinsuchtrainingsareoutlinedinHCSFCompletionProceduresinAppendixHandshouldincludeadherencetosecurityandconfidentialityprocedures.
B. StandardsforMonitoringandEvaluatingtheHIVCaseSurveillanceSystem
HIV case reporting data needs to maintain minimum quality standards to ensure the system isresponsiveandrelevanttoreflectwhoislivingwithanddyingfromHIV.Thequalityofthedataisregularly monitored, and results used to strengthen the relevant components through training.Periodic evaluation of the HIV case surveillance system includes measures for timeliness,completenessofreporting,andvalidity.TheseanalysesarerunbytheMoHStatisticalUnitOfficerandreviewedbytheSurveillanceUnit.
ThepurposesofmonitoringandevaluatingtheHIVcasesurveillancesystemaretodetermine:
37
Completeness:tomeasurewhatproportionofthediagnosedHIVcasesarecaptured; Timeliness:tomeasurehowsooncasesarereportedafterdiagnosis;and Validity:toevaluatetheaccuracyofdatareported.
Completeness
CompletenessofreportingreferstotheproportionofalltrueHIVpositivecasesthatarereportedtothe MoH. In order to monitor completeness, additional case finding methods should be found.Exampleswouldinclude1)listsofHIVdischargecodesfromplaceswherepeoplewithHIVreceivecare and 2) programmonitoring data from VCT, C&T and PMTCT to compare to the number ofuniqueHCSFsreceivedmonthlybythedesignatedunit(SeeIIEabove).
Because patients may not get into care once they are diagnosed, completeness measures areconducted on diagnostic tests not usingmeasures such as CD4 tests that are only conducted onpersonsincare.NPHRLregistriesareperiodicallyreviewedtoassessthecompletenessofreportingofpersonswhopresentforcare.
InadditiontodeterminingthecompletenessoftheHIVsurveillancesystem,staffwhoprocessforms(SeeIIEabove)followupwiththecorrespondingfacilityoncasesnotfoundintheHIVsurveillancedatabasestohavetheHCSFcompleted.
Timeliness
Timelinessmeasures the timebetweendiagnoseandreportedtoMoH.Timeliness ismeasuredbytwomethods:
1. Median timebetweendiagnosisofHIVor advanced/severeHIV andHIV case report formreceivedbytheunitdesignatedinIIEabove.
2. ProportionofthereportedcasesthatarereceivedbytheunitdesignatedinIIEabovewithinthreemonths,sixmonthsandtwelvemonthsofdiagnosis.
Standards
ThestandardsthattheHIVcasesurveillancesystemstrivestoachieveare:
66%ofcasesreportedwithinsixmonthsofdiagnosis 85%ofcasesreportedwithintwelvemonthsofdiagnosis
BelowarethestepsneededtocalculatetimelinessofHIVreporting,whichrequirestheuseofdateofdiagnosisanddatecaseisfirstreceivedbytheunitdesignatedinIIEabove.
Step1:Calculatecompletenessofreportingat12monthsafterthediagnosis.Ifcompletenessis≥85%,thengotoStep2.
Step2:Calculatetime(numberofmonths)fromdiagnosistoreport:
=(reportdate)‐(diagnosisdate)
=[(yearofreport)*12)+month]‐[((yearofdiagnosis)*12)+month]
38
Forexample,thereportdateisMay2004andthediagnosisdateisNovember2003.Thetimeinterval(inmonths)is:
[(2004*12)+5]‐[(2003*12)+11]=6months
Step3:Determinethenumberofcaseswithatimetoreport≤6months.
Step4:Calculatetimelinessofcasereporting:
NumberofcasesdiagnosedwithinayearandreportedwithinsixmonthsofdiagnosisNumberofcasesdiagnosedandreportedforthatdiagnosisyear
Validity
Validity measures the extent to which the information 1) on the case report form matchesinformationinthepatientrecordatthehealthcarefacilityaswellas2)intheelectronicdatabasematcheswhatisontheHCSF.
I. Casesurveillanceform/healthcarefacilitydatavalidity
Thevalidityof the information recordedon theHCSFcompared towhat is recorded in thepatient’s VCT or C&T or othermedical record can be measured by re‐abstracting data onpreviously reported cases and comparing the information contained in theoriginal and re‐abstractedforms.
Step1:Staffnotpreviouslyinvolvedwiththedataorsitedoesthere‐abstractioncheck.Thisperson works for the national surveillance program and is familiar with the casereport forms and methods for reviewing clinic records, abstracting data andcompletingthecasereportform.
Step2:Arandomsampleofcasesatasiteischosen‐5%chosenrandomlyifstaffinglevelsallow.
Step3:Atthesite,gobacktopatientrecordsorregistryforpersonschosenasthesample.CompleteanewHCSF.Besuretoonlyreviewthedatathatwasavailableatthetimeof the initial report and to exclude data received since the initial report wascompleted.
Step4:Comparetheinformationontheoriginalformandtheonecompletedduringthere‐abstractionphase.
Step5:Recordthediscrepanciesandsummarizeaccuracyforeachvariable.
II. Casesurveillanceform/electronicdatabasevalidity
ThevalidityoftheinformationenteredintotheelectronicdatabasecomparedtowhatisrecordedontheHCSFcanbemeasuredbyre‐enteringthedataonasampleofHCSFs.Thespecificmethodfor
39
doing this depends on how the EDB is structured. Ideally one would be able to re‐enter it andidentifyitasre‐entrysoitdoesnotoverwritetheoriginalform.Step1:Selectastaffpersonfamiliarwiththeformanddataentrytoperformthisstep.OneofthestafffromtheSurveillanceUnitinvolvedinthesecondaryreviewoftheformswouldbeideal.Step2:Randomlyselect5%ofenteredcases(ifstaffinglevelsallow)Step32:Re‐entertheform‐methodstobedeterminedafterconsultingwithMISUAlternativetoStep3:VisuallycomparewhatisontheHCSFwithwhathasbeenentered.Step4:Calculate theproportionsof errors for eachdata field. Separateout errors thatwill affecthowthedataareanalyzedfromthosethatshouldbecorrectedbutwhichhaveless impactonthedatareports.
40
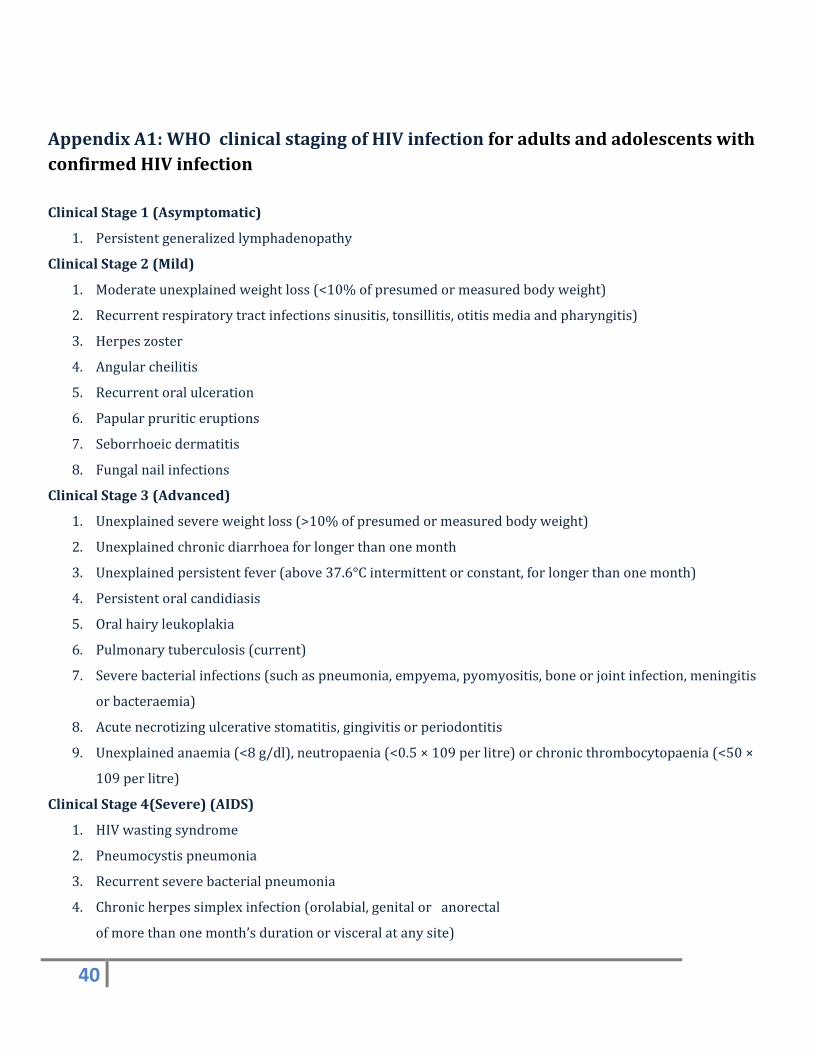
AppendixA1:WHOclinicalstagingofHIVinfectionforadultsandadolescentswithconfirmedHIVinfection
ClinicalStage1(Asymptomatic)
1. Persistentgeneralizedlymphadenopathy
ClinicalStage2(Mild)
1. Moderateunexplainedweightloss(<10%ofpresumedormeasuredbodyweight)
2. Recurrentrespiratorytractinfectionssinusitis,tonsillitis,otitismediaandpharyngitis)
3. Herpeszoster
4. Angularcheilitis
5. Recurrentoralulceration
6. Papularpruriticeruptions
7. Seborrhoeicdermatitis
8. Fungalnailinfections
ClinicalStage3(Advanced)
1. Unexplainedsevereweightloss(>10%ofpresumedormeasuredbodyweight)
2. Unexplainedchronicdiarrhoeaforlongerthanonemonth
3. Unexplainedpersistentfever(above37.6°Cintermittentorconstant,forlongerthanonemonth)
4. Persistentoralcandidiasis
5. Oralhairyleukoplakia
6. Pulmonarytuberculosis(current)
7. Severebacterialinfections(suchaspneumonia,empyema,pyomyositis,boneorjointinfection,meningitis
orbacteraemia)
8. Acutenecrotizingulcerativestomatitis,gingivitisorperiodontitis
9. Unexplainedanaemia(<8g/dl),neutropaenia(<0.5×109perlitre)orchronicthrombocytopaenia(<50×
109perlitre)
ClinicalStage4(Severe)(AIDS)
1. HIVwastingsyndrome
2. Pneumocystispneumonia
3. Recurrentseverebacterialpneumonia
4. Chronicherpessimplexinfection(orolabial,genitaloranorectal
ofmorethanonemonth’sdurationorvisceralatanysite)
41
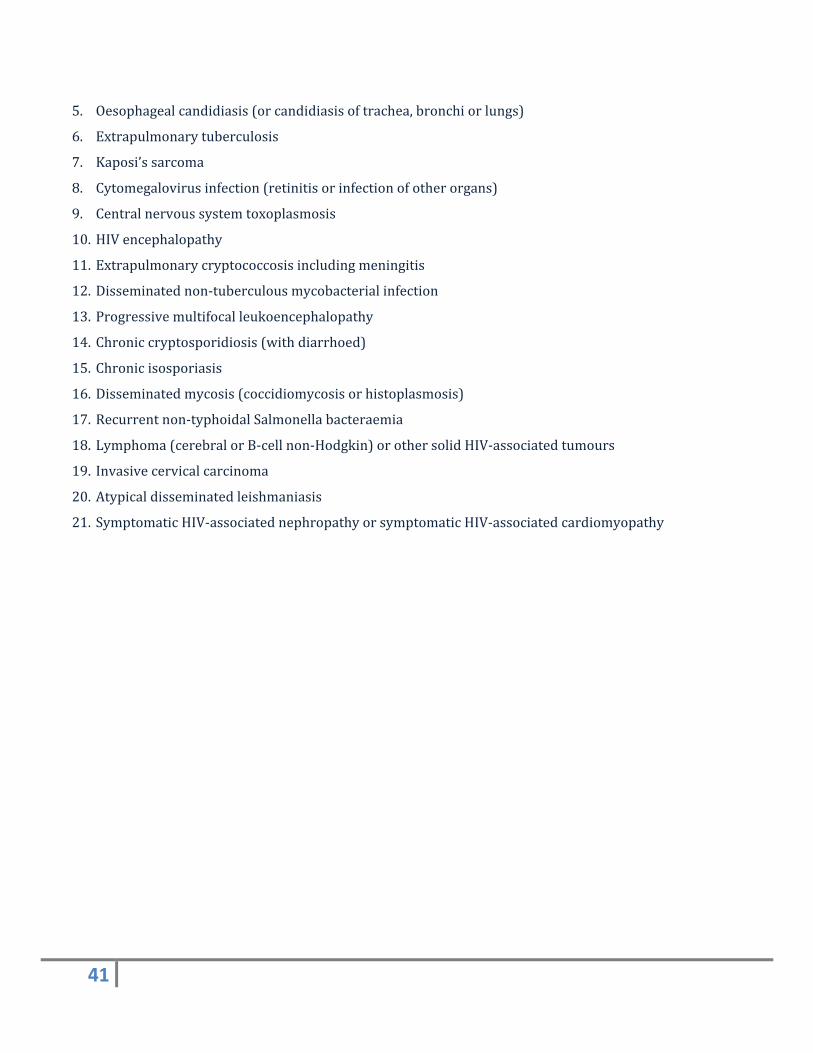
5. Oesophagealcandidiasis(orcandidiasisoftrachea,bronchiorlungs)
6. Extrapulmonarytuberculosis
7. Kaposi’ssarcoma
8. Cytomegalovirusinfection(retinitisorinfectionofotherorgans)
9. Centralnervoussystemtoxoplasmosis
10. HIVencephalopathy
11. Extrapulmonarycryptococcosisincludingmeningitis
12. Disseminatednon‐tuberculousmycobacterialinfection
13. Progressivemultifocalleukoencephalopathy
14. Chroniccryptosporidiosis(withdiarrhoed)
15. Chronicisosporiasis
16. Disseminatedmycosis(coccidiomycosisorhistoplasmosis)
17. Recurrentnon‐typhoidalSalmonellabacteraemia
18. Lymphoma(cerebralorB‐cellnon‐Hodgkin)orothersolidHIV‐associatedtumours
19. Invasivecervicalcarcinoma
20. Atypicaldisseminatedleishmaniasis
21. SymptomaticHIV‐associatednephropathyorsymptomaticHIV‐associatedcardiomyopathy
42
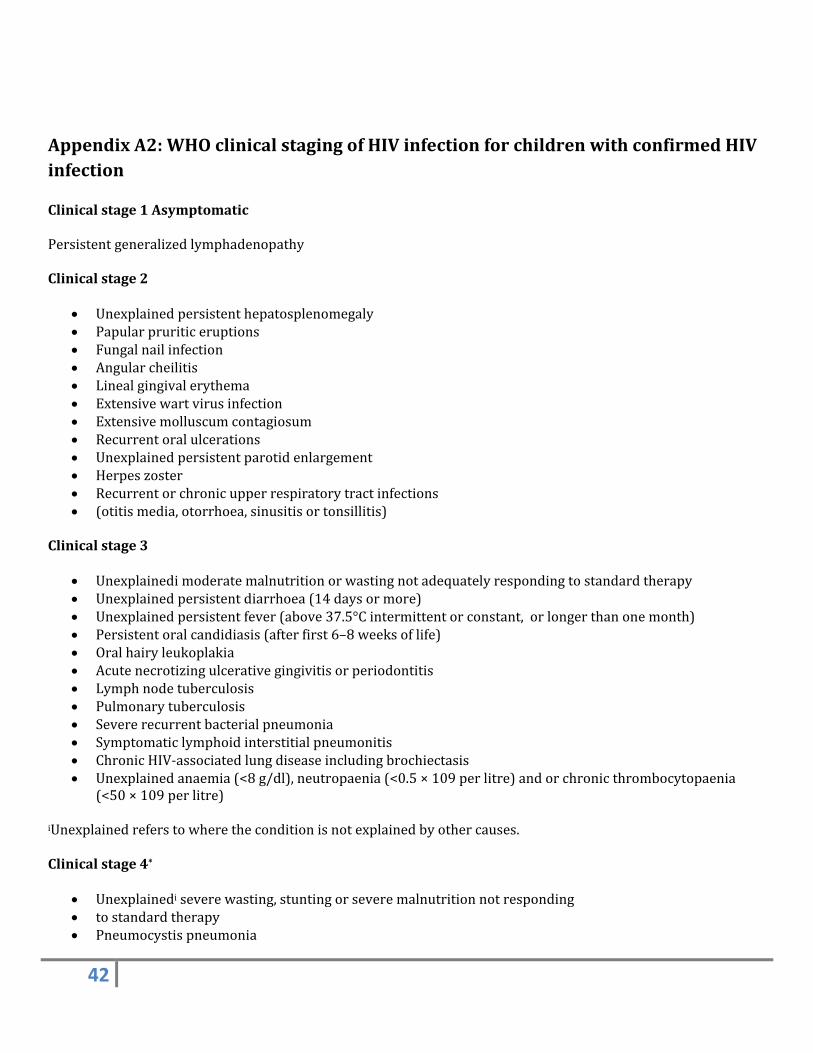
AppendixA2:WHOclinicalstagingofHIVinfectionforchildrenwithconfirmedHIVinfectionClinicalstage1AsymptomaticPersistentgeneralizedlymphadenopathyClinicalstage2
Unexplainedpersistenthepatosplenomegaly Papularpruriticeruptions Fungalnailinfection Angularcheilitis Linealgingivalerythema Extensivewartvirusinfection Extensivemolluscumcontagiosum Recurrentoralulcerations Unexplainedpersistentparotidenlargement Herpeszoster Recurrentorchronicupperrespiratorytractinfections (otitismedia,otorrhoea,sinusitisortonsillitis)
Clinicalstage3
Unexplainedimoderatemalnutritionorwastingnotadequatelyrespondingtostandardtherapy Unexplainedpersistentdiarrhoea(14daysormore) Unexplainedpersistentfever(above37.5°Cintermittentorconstant,orlongerthanonemonth) Persistentoralcandidiasis(afterfirst6–8weeksoflife) Oralhairyleukoplakia Acutenecrotizingulcerativegingivitisorperiodontitis Lymphnodetuberculosis Pulmonarytuberculosis Severerecurrentbacterialpneumonia Symptomaticlymphoidinterstitialpneumonitis ChronicHIV‐associatedlungdiseaseincludingbrochiectasis Unexplainedanaemia(<8g/dl),neutropaenia(<0.5×109perlitre)andorchronicthrombocytopaenia
(<50×109perlitre)iUnexplainedreferstowheretheconditionisnotexplainedbyothercauses.Clinicalstage4*
Unexplainediseverewasting,stuntingorseveremalnutritionnotresponding tostandardtherapy Pneumocystispneumonia
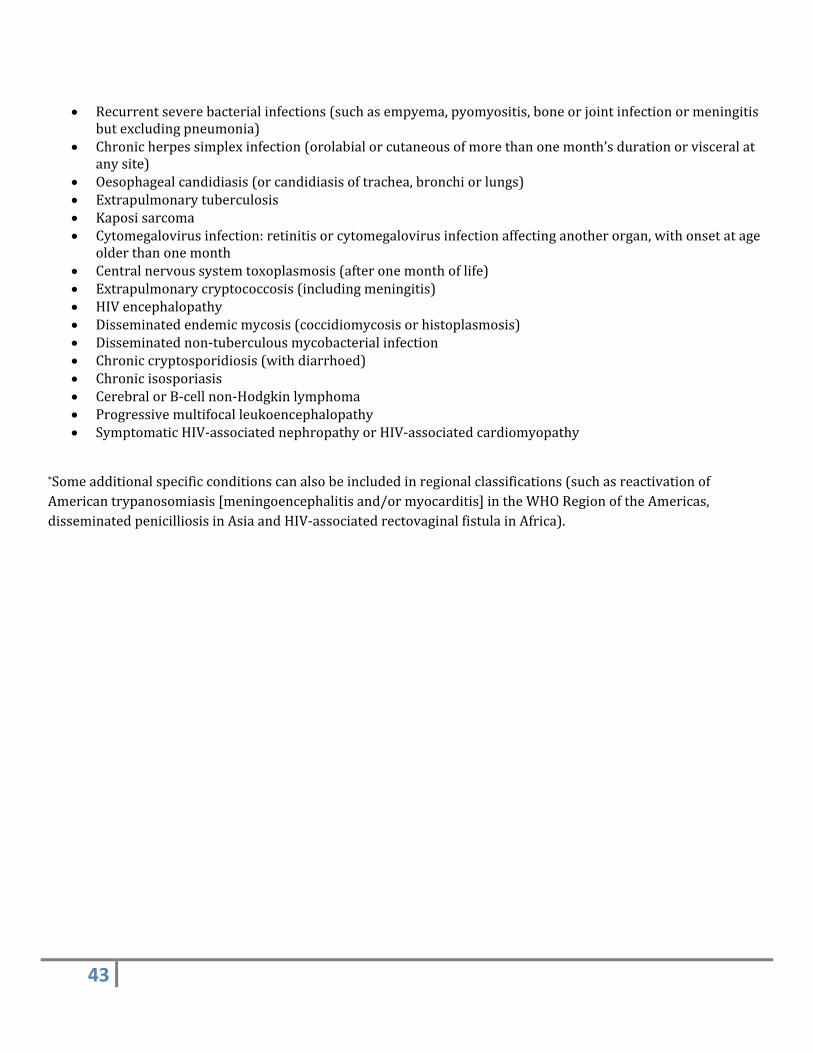
43
Recurrentseverebacterialinfections(suchasempyema,pyomyositis,boneorjointinfectionormeningitisbutexcludingpneumonia)
Chronicherpessimplexinfection(orolabialorcutaneousofmorethanonemonth’sdurationorvisceralatanysite)
Oesophagealcandidiasis(orcandidiasisoftrachea,bronchiorlungs) Extrapulmonarytuberculosis Kaposisarcoma Cytomegalovirusinfection:retinitisorcytomegalovirusinfectionaffectinganotherorgan,withonsetatage
olderthanonemonth Centralnervoussystemtoxoplasmosis(afteronemonthoflife) Extrapulmonarycryptococcosis(includingmeningitis) HIVencephalopathy Disseminatedendemicmycosis(coccidiomycosisorhistoplasmosis) Disseminatednon‐tuberculousmycobacterialinfection Chroniccryptosporidiosis(withdiarrhoed) Chronicisosporiasis CerebralorB‐cellnon‐Hodgkinlymphoma Progressivemultifocalleukoencephalopathy SymptomaticHIV‐associatednephropathyorHIV‐associatedcardiomyopathy
*Someadditionalspecificconditionscanalsobeincludedinregionalclassifications(suchasreactivationofAmericantrypanosomiasis[meningoencephalitisand/ormyocarditis]intheWHORegionoftheAmericas,disseminatedpenicilliosisinAsiaandHIV‐associatedrectovaginalfistulainAfrica).
44
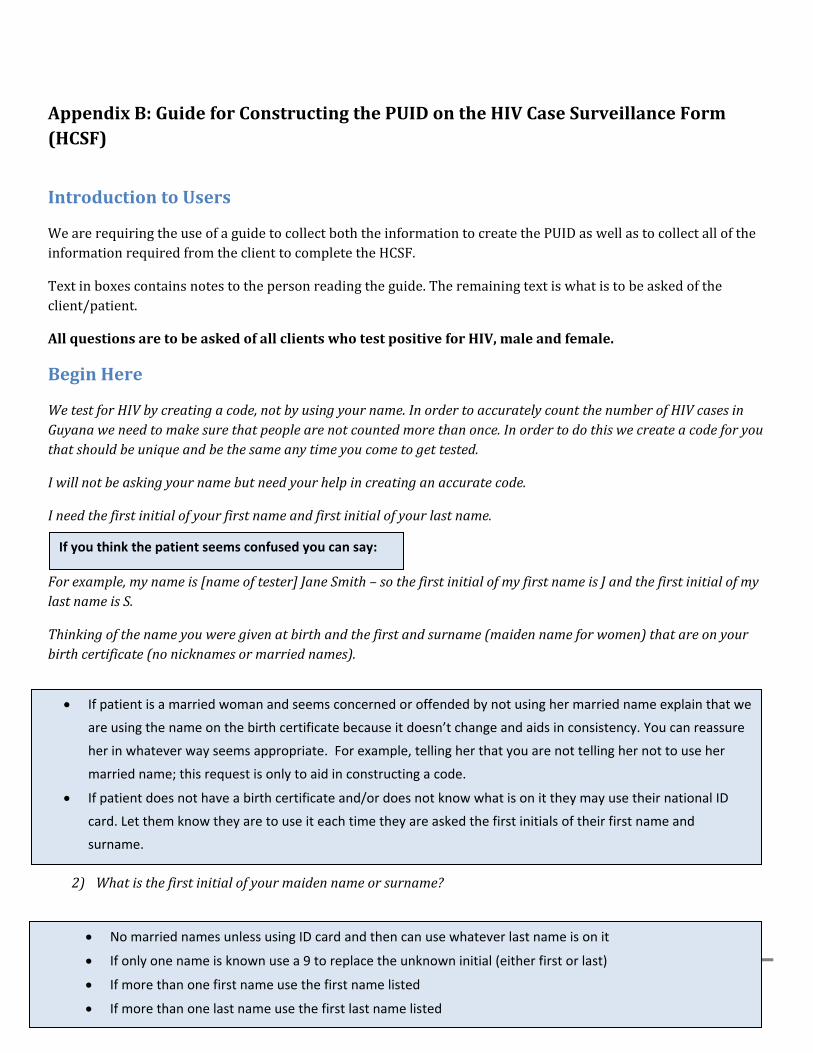
AppendixB:GuideforConstructingthePUIDontheHIVCaseSurveillanceForm(HCSF)
IntroductiontoUsers
WearerequiringtheuseofaguidetocollectboththeinformationtocreatethePUIDaswellastocollectalloftheinformationrequiredfromtheclienttocompletetheHCSF.
Textinboxescontainsnotestothepersonreadingtheguide.Theremainingtextiswhatistobeaskedoftheclient/patient.
AllquestionsaretobeaskedofallclientswhotestpositiveforHIV,maleandfemale.
BeginHere
WetestforHIVbycreatingacode,notbyusingyourname.InordertoaccuratelycountthenumberofHIVcasesinGuyanaweneedtomakesurethatpeoplearenotcountedmorethanonce.Inordertodothiswecreateacodeforyouthatshouldbeuniqueandbethesameanytimeyoucometogettested.
Iwillnotbeaskingyournamebutneedyourhelpincreatinganaccuratecode.
Ineedthefirstinitialofyourfirstnameandfirstinitialofyourlastname.
Forexample,mynameis[nameoftester]JaneSmith–sothefirstinitialofmyfirstnameisJandthefirstinitialofmylastnameisS.
Thinkingofthenameyouweregivenatbirthandthefirstandsurname(maidennameforwomen)thatareonyourbirthcertificate(nonicknamesormarriednames).
1) Whatisthefirstinitialofyourfirstname?
2) Whatisthefirstinitialofyourmaidennameorsurname?
If you think the patient seems confused you can say:
If patient is a married woman and seems concerned or offended by not using her married name explain that we
are using the name on the birth certificate because it doesn’t change and aids in consistency. You can reassure
her in whatever way seems appropriate. For example, telling her that you are not telling her not to use her
married name; this request is only to aid in constructing a code.
If patient does not have a birth certificate and/or does not know what is on it they may use their national ID
card. Let them know they are to use it each time they are asked the first initials of their first name and
surname.
No married names unless using ID card and then can use whatever last name is on it
If only one name is known use a 9 to replace the unknown initial (either first or last)
If more than one first name use the first name listed
If more than one last name use the first last name listed
45
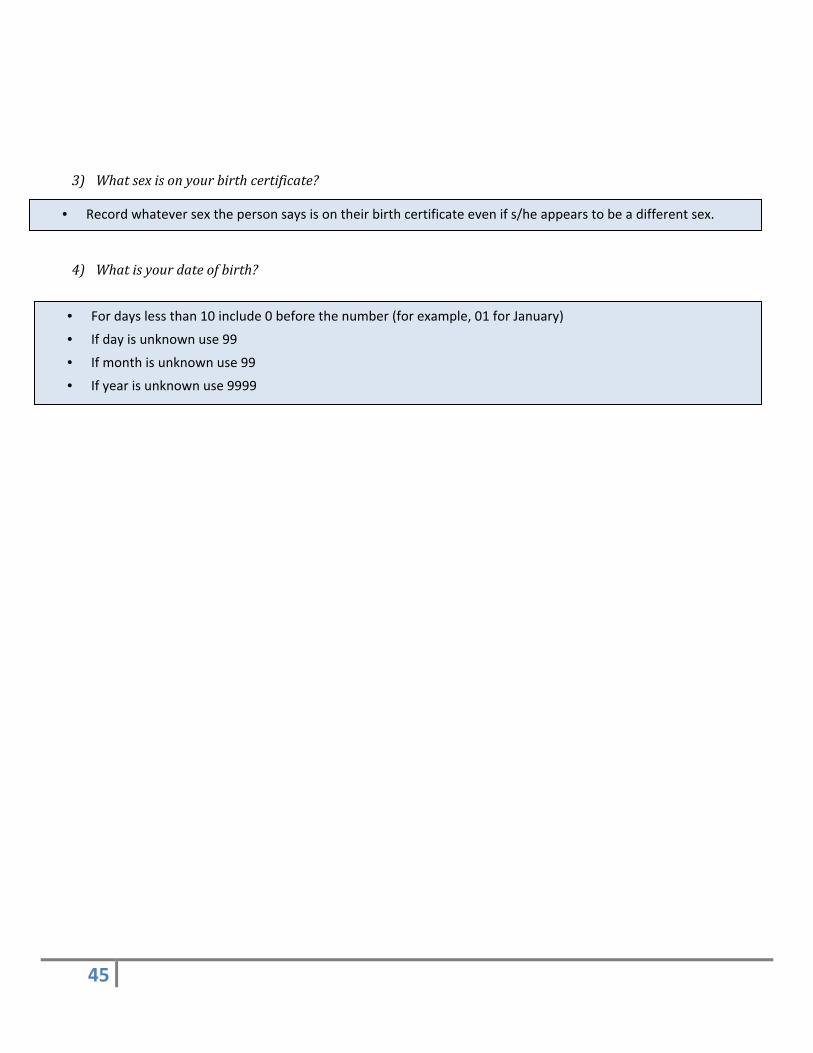
3) Whatsexisonyourbirthcertificate?
4) Whatisyourdateofbirth?
• For days less than 10 include 0 before the number (for example, 01 for January)
• If day is unknown use 99
• If month is unknown use 99
• If year is unknown use 9999
• Record whatever sex the person says is on their birth certificate even if s/he appears to be a different sex.
46
AppendixC:HIVCaseSurveillanceForm(HCSF)
47
AppendixD:HCSFCompletionProcedures
HIVCaseSurveillanceFormCompletionProceduresTheseproceduresareforanyonecompletingtheHIVcasesurveillanceform(HCSF)forreportingorupdatingacaseofHIV.ThereareeightmandatoryvariablesthatmustbecompletedforMoHtocountthecaseofHIV.Thesearelistedbelow.However,itisexpectedthatallvariableswillbecompletedbypersonsreportingorupdatingacaseofHIV.Thesevariablesarelistedonthetablebelow.
MandatoryVariables
Firstinitialofpatient’sfirstnameFirstinitialofpatient’slastnameSexDateofBirthRegionofpatient/clientresidenceatdiagnosisResultofHIVtestsDateofHIVdiagnosisdefinedastestdateoffirstpositiveHIVtestDateofdeath,ifapplicable
PatientsareidentifiedintheHIVcasesurveillancesystembyapatientuniqueidentifier(PUID)thatisconstructedusingthefirstinitialofthepatient’sfirstname,firstinitialofpatient’slastname,sexanddateofbirth(DD/MM/YYYY).BecausethePUIDisusedtodifferentiatebetweendifferentpeopleandtheintegrityoftheentirereportingsystemdependsoncountingeachcaseonlyonetimeitiscriticalthatthesefourvariablesandthePUIDbeconstructedasconsistentlyaspossible.Inordertodothateachclientisaskedtorefertothename,sexanddateofbirthonhis/herbirthcertificate.Ifpatientdoesnothaveabirthcertificateand/ordoesnotknowwhatisonittheymayusetheirnationalIDcard.AguideisprovidedinAppendixBoftheSOPwithquestionsthataretobeaskedoftheclientseverytimeaPUIDisbeingconstructed.Inordertoincreasethelikelihoodthatthisinformationwillbeusedconsistentlyregulartrainingonusingtheguide,includingroleplaysareconductedannually,socounselorscanpracticeintegratingthequestionsintothecounselingsession.
Regardlessofwhichnameisusedthereshouldbenoblanksinthenameinitialfieldsandtheseinitialsmustbelegible.SexasitappearsonthebirthcertificateshouldberecordedontheHCSF,regardlessofhowthepatientpresentshim/herself.ThereshouldbenoblanksintheSexfield.
DateofBirthisasitappearsonthebirthcertificate.ThereshouldbenoblanksintheDateofBirthFieldsandalldigitsmustbelegible:
i. Fordayslessthan10include0beforethenumber(forexample,01forJanuary)ii. Ifdayisunknownuse99iii. Ifmonthisunknownuse99iv. Ifyearisunknownuse9999
48
I.PATIENTINFORMATION
Variable Descriptionofvariable
Firstnameinitial FirstInitialofpatient’sfirstname(usingthenameonthebirthcertificate).Ifinitialisunknownreplacewitha9
Lastnameinitial FirstInitialofpatient’slastname(usingthenameonthebirthcertificate,nomarriednamesornicknames;forwomenaskformaidenname;ifmorethanonelastnameusethefirstlastname).Ifinitialisunknownreplacewitha9
Sex Sexas itappearson thebirthcertificate, regardlessofhowthepatientpresentshim/herself
DateofBirth CalendarDay(DD),Month(MM),andYear(YYYY)whenthepatientwasbornasrecordedonthebirthcertificate(using9sforanyorallportionsofthedateofbirththatareunknown)
IfFemale,Pregnant Ifpatientisfemale,isshepregnant?
PatientUniqueIdentifier(PUID)
PUIDwith11characters:initialoffirstname,initialoflastname,sex(M/F),anddateofbirth(DD,MM,YYYY).Thisincludesusingthe#9forunknownvaluesasdescribedintheinitial,sexanddateofbirthboxesabove.
Testingpurpose IdentifywhetherthisreportisaninitialHIVdiagnosis,anAdvancedHIVdiagnosisoranAIDSdeathnotification.Iftheinitialdiagnosisismadeatanadvancedstage,checkbothboxes.AIDSdeathnotificationincludesalldeathsamongpersonswithAIDS.Actualcauseofdeathshouldbewrittenintherighthandmarginoftheform.
Ifdead,dateofdeath CalendarDay(DD),Month(MM),andYear(YYYY)whenthepatientdied(using9sforanyorallportionsofthedateofdeaththatareunknown)
Street Nameofstreetwherepatientresidesmostofthetimeatthetimeofthisreport
City/Town/Village Nameofcity/town/villagewherepatientresidesmostofthetimeatthetimeofthisreport
Regionno. Regionallocationofthecity/town/village(region1‐10)ofresidenceatthetimeofthisreport
Ethnicity Patient’sself‐reportingethnicity:Afro‐Guyanese,Amerindian,Chinese,Info‐Guyanese,Portuguese,Mixed,orOtherorRefused.CHECKONLYONE
EmploymentStatus Currentstatusofemployment:employed,unemployed,student,refused.Ifemployed,stateoccupation.Employedincludesparttimeaswellasfulltimework.Forclientsthatarebothemployed
49
andstudents,checkboth.
II.EXPOSURECATEGORIES:AllapplicableexposurecategoriesarerecordedontheHIVcasesurveillanceform.Anexposurecategoryischeckedifthepatientacknowledgesthathe/sheengagedinthatactivityatleastoncebeforethefirstHIV‐positivetestresult.Thecategoriesareasfollows:
Variable Descriptionofvariable
Sexwithmale Patienthadanal,oral,orvaginalsexwithamale
Sexwithfemale Patienthadanal,oral,orvaginalsexwithafemale
Sexwithcommercialsexworker
Patienthadanal,oral,orvaginalsexwithmaleorfemalesexworker
SexwithanHIVinfectedperson
Patienthadanal,oral,orvaginalsexwithapersonwhoisinfectedwithHIV.TheydonotneedtohaveknownthatthesexpartnerwasHIV‐infectedatthetimetheyhadsex–onlythatpatientcanreportthattheyhadsexwithanHIV‐infectedpersonatthetimeofHCSFcompletion.
Beenacommercialsexworker
Patienthasexchangedsextoreceivemoneyorothermaterialgoods
Sharedneedleswhenusingdrugs
Patientreportedsharingneedleswheninjectingdrugs
Sexwithmultiplepartners
Patienthadanal,oral,orvaginalsexwithmultiplepartnersinthepastyear
Receivedbloodtransfusionorbloodcomponents
Patientreportedbeingarecipientofbloodtransfusionorbloodcomponent
Receivedtransplantoftissueororganorartificialinsemination
Patientreportedhavingreceivedtransplantoftissueororgan,orhadanartificialinsemination
Occupationalexposureinhealthcaresettingorlaboratory
Patientreportedhavingbeenexposedtoblood/bloodcomponentswhileperforminghis/herjobinahealthcaresettingorlaboratory
PerinatalexposuretoHIV
PatienthadbeenexposedtoHIVthroughmother‐to‐childtransmission(borntoaHIV+mother)
Beenavictimofsexualassault
Patientreportedbeingavictimofsexualassault
Unknown Patientdoesnotreporthowtheywereexposed.ITSHOULDNOTBECHECKEDBYTHEPERSONCOMPLETINGTHE
50
FORM.ThisoptionisselectedbyMoHifallotheroptionsareblank.
III.HIVTESTRESULTS
Nameoftest Nameoftestkitused.Examplesinclude:
HIVrapidtests:Determine,UniGold,Stat‐Pack
HIVDNAPCR
ELISA:MurexHIV
WesternBlot
Testtype TypeoftestusedforHIVdiagnosis,whichincludes:
Antibodytest:Rapidtest,Enzyme‐linkedimmunosorbentassay(ELISA),Westernblot
Virologytest:HIVDNAPCR(forchildrenlessthan18monthsold)
Result HIVtestresult:positive(pos),negative(neg),indeterminate(ind)
Testdate DateofHIVtest:calendarday(DD),month(MM),andyear(YYYY).Ifspecimencollectiondateisdifferentfromdatetestwasrun,recordspecimencollectiondate

51
IV.CLINICALINFORMATIONONADVANCEDHIV(forclinicalpractitioneruseonly)
PresentingCD4Count/percent
ThisvariabledoesnotexistontheHCSF.TheonlyCD4resultsrequestedontheformarethetworowsbelow.However,atclinicalsitesstaffaredirectedtoreportthefirstCD4count/percent(“presentingCD4”).Theycanusethe“CD4countbelow350µl”boxforcasesage5andolderorthe“%CD4below30”boxforcasesbelowage5torecordthisdata.Thereforeifpatientisage5orolderplacepresentingCD4countinthe“CD4countbelow350µL”fieldregardlessofthevalueoftheresult(i.e.,regardlessoftheactualnumber).Ifpatientisbelowage5placepresentingCD4percentinthe“CD4percentbelow30”fieldregardlessofthevalueoftheresult(i.e.,regardlessoftheactualnumber).
CD4Countbelow350µL(≥5yearsold)
CD4+lymphocyte(CD4cells)countbelow350cells/µLisamakerforadvancedHIVinfectionamongpatientsaged5yearsandolder.RecordtheexactCD4countresultifbelow350cells/µL
%CD4below30(<5yearsold)
PercentCD4below30%isamarkerfordeterminingadvancedHIVinfectionamongpatientslessthan5yearsofage.Recordthe%ofCD4below30
TestDate DateoftestforCD4count:calendarday(DD),month(MM),year(YYYY).Ifspecimencollectiondateisdifferentfromdatetestwasrunrecordspecimencollectiondate
Stageofdisease(Stage3orStage4)
TheStage3orStage4boxistickedbasedonwhichcriteriathepatientmeets.Thestagingcriteriamaybemetbyeitherclinicalorimmunologiccriteria.ClinicalcriteriaarelistedinAppendicesA1andA2intheSOP.Forimmunologicstagingcriteriasee:WHOimmunologiccriteriafortheseStagesintheTable“WHOimmunologicalclassificationforestablishedHIVinfection”foundinSectionIVoftheHCSF.
Dateofstagediagnosis RecorddateofCD4percentorcountthatcorrespondstothestagecheckedabove:calendarday(DD),month(MM),year(YYYY)
52
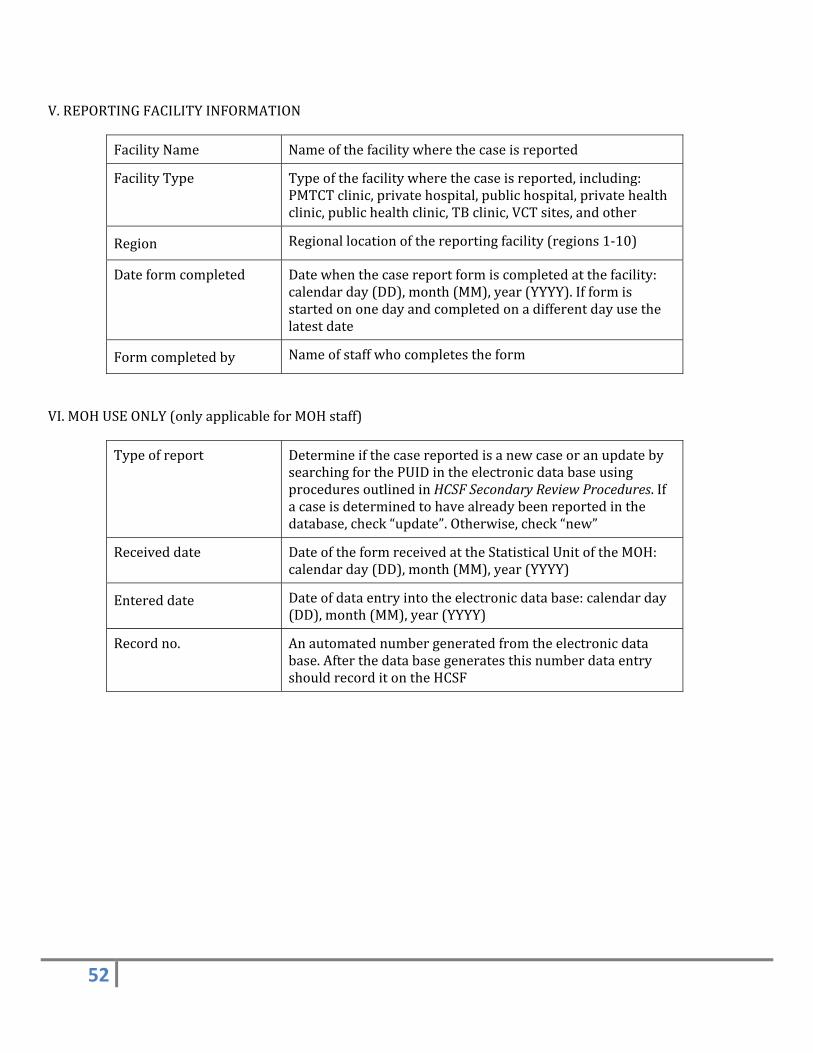
V.REPORTINGFACILITYINFORMATION
FacilityName Nameofthefacilitywherethecaseisreported
FacilityType Typeofthefacilitywherethecaseisreported,including:PMTCTclinic,privatehospital,publichospital,privatehealthclinic,publichealthclinic,TBclinic,VCTsites,andother
Region Regionallocationofthereportingfacility(regions1‐10)
Dateformcompleted Datewhenthecasereportformiscompletedatthefacility:calendarday(DD),month(MM),year(YYYY).Ifformisstartedononedayandcompletedonadifferentdayusethelatestdate
Formcompletedby Nameofstaffwhocompletestheform
VI.MOHUSEONLY(onlyapplicableforMOHstaff)
Typeofreport DetermineifthecasereportedisanewcaseoranupdatebysearchingforthePUIDintheelectronicdatabaseusingproceduresoutlinedinHCSFSecondaryReviewProcedures.Ifacaseisdeterminedtohavealreadybeenreportedinthedatabase,check“update”.Otherwise,check“new”
Receiveddate DateoftheformreceivedattheStatisticalUnitoftheMOH:calendarday(DD),month(MM),year(YYYY)
Entereddate Dateofdataentryintotheelectronicdatabase:calendarday(DD),month(MM),year(YYYY)
Recordno. Anautomatednumbergeneratedfromtheelectronicdatabase.AfterthedatabasegeneratesthisnumberdataentryshouldrecorditontheHCSF
53
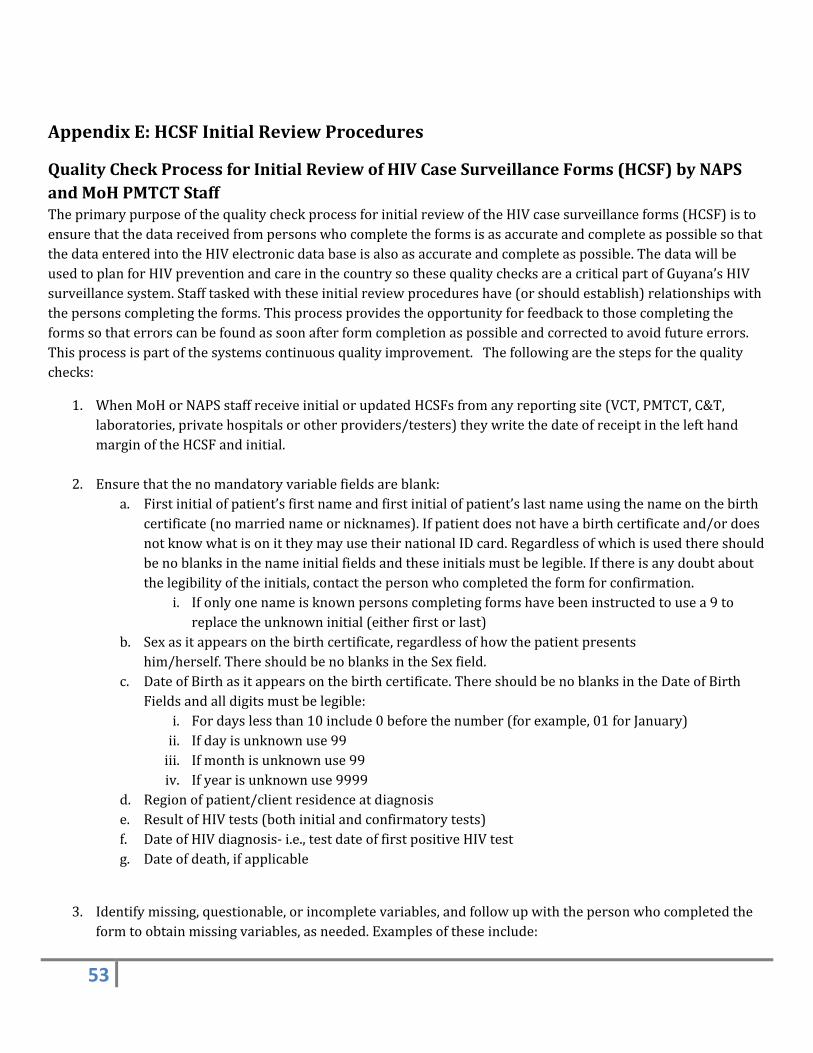
AppendixE:HCSFInitialReviewProcedures
QualityCheckProcessforInitialReviewofHIVCaseSurveillanceForms(HCSF)byNAPSandMoHPMTCTStaffTheprimarypurposeofthequalitycheckprocessforinitialreviewoftheHIVcasesurveillanceforms(HCSF)istoensurethatthedatareceivedfrompersonswhocompletetheformsisasaccurateandcompleteaspossiblesothatthedataenteredintotheHIVelectronicdatabaseisalsoasaccurateandcompleteaspossible.ThedatawillbeusedtoplanforHIVpreventionandcareinthecountrysothesequalitychecksareacriticalpartofGuyana’sHIVsurveillancesystem.Stafftaskedwiththeseinitialreviewprocedureshave(orshouldestablish)relationshipswiththepersonscompletingtheforms.Thisprocessprovidestheopportunityforfeedbacktothosecompletingtheformssothaterrorscanbefoundassoonafterformcompletionaspossibleandcorrectedtoavoidfutureerrors.Thisprocessispartofthesystemscontinuousqualityimprovement.Thefollowingarethestepsforthequalitychecks:
1. WhenMoHorNAPSstaffreceiveinitialorupdatedHCSFsfromanyreportingsite(VCT,PMTCT,C&T,laboratories,privatehospitalsorotherproviders/testers)theywritethedateofreceiptinthelefthandmarginoftheHCSFandinitial.
2. Ensurethatthenomandatoryvariablefieldsareblank:a. Firstinitialofpatient’sfirstnameandfirstinitialofpatient’slastnameusingthenameonthebirth
certificate(nomarriednameornicknames).Ifpatientdoesnothaveabirthcertificateand/ordoesnotknowwhatisonittheymayusetheirnationalIDcard.Regardlessofwhichisusedthereshouldbenoblanksinthenameinitialfieldsandtheseinitialsmustbelegible.Ifthereisanydoubtaboutthelegibilityoftheinitials,contactthepersonwhocompletedtheformforconfirmation.
i. Ifonlyonenameisknownpersonscompletingformshavebeeninstructedtousea9toreplacetheunknowninitial(eitherfirstorlast)
b. Sexasitappearsonthebirthcertificate,regardlessofhowthepatientpresentshim/herself.ThereshouldbenoblanksintheSexfield.
c. DateofBirthasitappearsonthebirthcertificate.ThereshouldbenoblanksintheDateofBirthFieldsandalldigitsmustbelegible:
i. Fordayslessthan10include0beforethenumber(forexample,01forJanuary)ii. Ifdayisunknownuse99iii. Ifmonthisunknownuse99iv. Ifyearisunknownuse9999
d. Regionofpatient/clientresidenceatdiagnosise. ResultofHIVtests(bothinitialandconfirmatorytests)f. DateofHIVdiagnosis‐i.e.,testdateoffirstpositiveHIVtestg. Dateofdeath,ifapplicable
3. Identifymissing,questionable,orincompletevariables,andfollowupwiththepersonwhocompletedtheformtoobtainmissingvariables,asneeded.Examplesoftheseinclude:
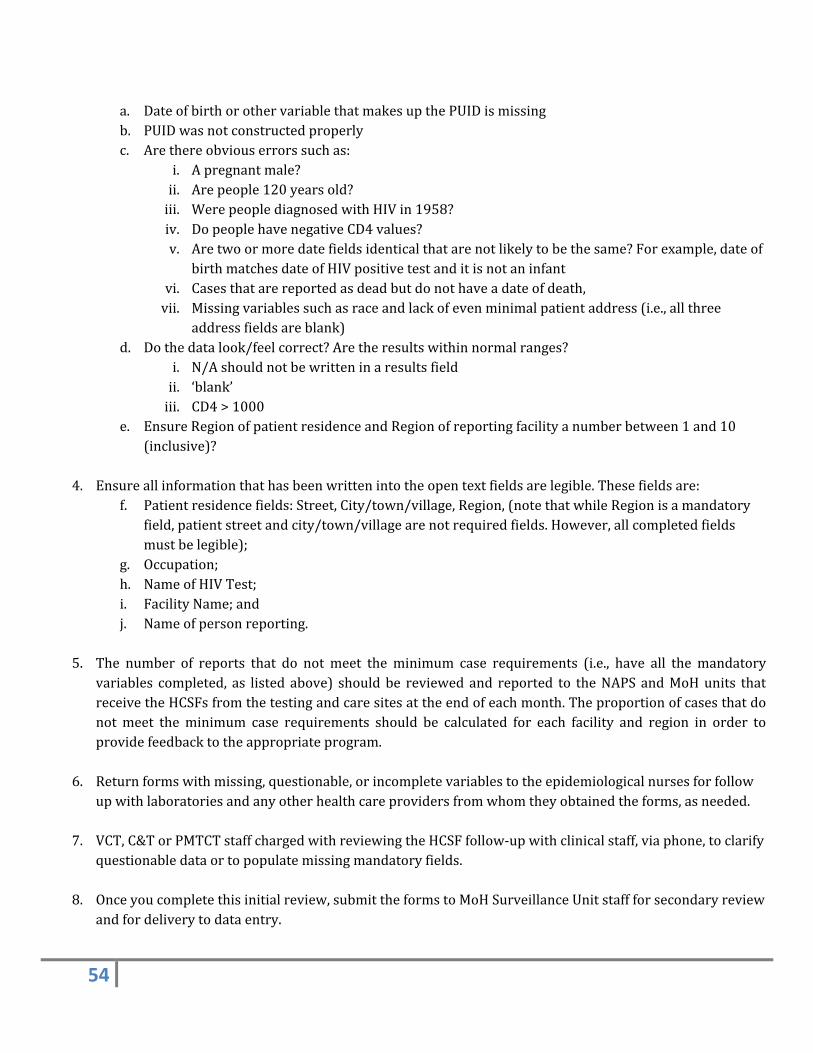
54
a. DateofbirthorothervariablethatmakesupthePUIDismissingb. PUIDwasnotconstructedproperlyc. Arethereobviouserrorssuchas:
i. Apregnantmale?ii. Arepeople120yearsold?iii. WerepeoplediagnosedwithHIVin1958?iv. DopeoplehavenegativeCD4values?v. Aretwoormoredatefieldsidenticalthatarenotlikelytobethesame?Forexample,dateof
birthmatchesdateofHIVpositivetestanditisnotaninfantvi. Casesthatarereportedasdeadbutdonothaveadateofdeath,vii. Missingvariablessuchasraceandlackofevenminimalpatientaddress(i.e.,allthree
addressfieldsareblank)d. Dothedatalook/feelcorrect?Aretheresultswithinnormalranges?
i. N/Ashouldnotbewritteninaresultsfieldii. ‘blank’iii. CD4>1000
e. EnsureRegionofpatientresidenceandRegionofreportingfacilityanumberbetween1and10(inclusive)?
4. Ensureallinformationthathasbeenwrittenintotheopentextfieldsarelegible.Thesefieldsare:
f. Patientresidencefields:Street,City/town/village,Region,(notethatwhileRegionisamandatoryfield,patientstreetandcity/town/villagearenotrequiredfields.However,allcompletedfieldsmustbelegible);
g. Occupation;h. NameofHIVTest;i. FacilityName;andj. Nameofpersonreporting.
5. The number of reports that do not meet the minimum case requirements (i.e., have all themandatory
variables completed, as listed above) shouldbe reviewedand reported to theNAPSandMoHunits thatreceivetheHCSFsfromthetestingandcaresitesattheendofeachmonth.Theproportionofcasesthatdonotmeet theminimum case requirements should be calculated for each facility and region in order toprovidefeedbacktotheappropriateprogram.
6. Returnformswithmissing,questionable,orincompletevariablestotheepidemiologicalnursesforfollowupwithlaboratoriesandanyotherhealthcareprovidersfromwhomtheyobtainedtheforms,asneeded.
7. VCT,C&TorPMTCTstaffchargedwithreviewingtheHCSFfollow‐upwithclinicalstaff,viaphone,toclarifyquestionabledataortopopulatemissingmandatoryfields.
8. Onceyoucompletethisinitialreview,submittheformstoMoHSurveillanceUnitstaffforsecondaryreviewandfordeliverytodataentry.
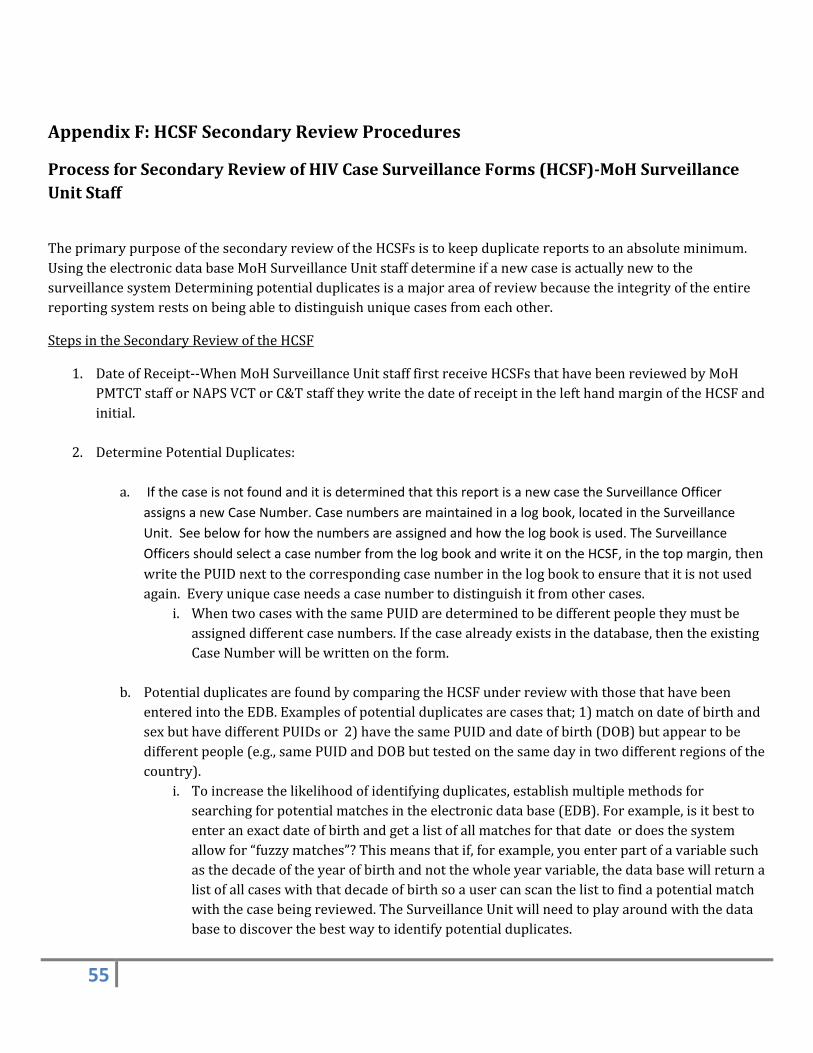
55
AppendixF:HCSFSecondaryReviewProcedures
ProcessforSecondaryReviewofHIVCaseSurveillanceForms(HCSF)‐MoHSurveillanceUnitStaff
TheprimarypurposeofthesecondaryreviewoftheHCSFsistokeepduplicatereportstoanabsoluteminimum.UsingtheelectronicdatabaseMoHSurveillanceUnitstaffdetermineifanewcaseisactuallynewtothesurveillancesystemDeterminingpotentialduplicatesisamajorareaofreviewbecausetheintegrityoftheentirereportingsystemrestsonbeingabletodistinguishuniquecasesfromeachother.
StepsintheSecondaryReviewoftheHCSF
1. DateofReceipt‐‐WhenMoHSurveillanceUnitstafffirstreceiveHCSFsthathavebeenreviewedbyMoHPMTCTstafforNAPSVCTorC&TstafftheywritethedateofreceiptinthelefthandmarginoftheHCSFandinitial.
2. DeterminePotentialDuplicates:
a. If the case is not found and it is determined that this report is a new case the Surveillance Officer
assigns a new Case Number. Case numbers are maintained in a log book, located in the Surveillance
Unit. See below for how the numbers are assigned and how the log book is used. The Surveillance
Officers should select a case number from the log book and write it on the HCSF, in the top margin, thenwritethePUIDnexttothecorrespondingcasenumberinthelogbooktoensurethatitisnotusedagain.Everyuniquecaseneedsacasenumbertodistinguishitfromothercases.
i. WhentwocaseswiththesamePUIDaredeterminedtobedifferentpeopletheymustbeassigneddifferentcasenumbers.Ifthecasealreadyexistsinthedatabase,thentheexistingCaseNumberwillbewrittenontheform.
b. PotentialduplicatesarefoundbycomparingtheHCSFunderreviewwiththosethathavebeenenteredintotheEDB.Examplesofpotentialduplicatesarecasesthat;1)matchondateofbirthandsexbuthavedifferentPUIDsor2)havethesamePUIDanddateofbirth(DOB)butappeartobedifferentpeople(e.g.,samePUIDandDOBbuttestedonthesamedayintwodifferentregionsofthecountry).
i. Toincreasethelikelihoodofidentifyingduplicates,establishmultiplemethodsforsearchingforpotentialmatchesintheelectronicdatabase(EDB).Forexample,isitbesttoenteranexactdateofbirthandgetalistofallmatchesforthatdateordoesthesystemallowfor“fuzzymatches”?Thismeansthatif,forexample,youenterpartofavariablesuchasthedecadeoftheyearofbirthandnotthewholeyearvariable,thedatabasewillreturnalistofallcaseswiththatdecadeofbirthsoausercanscanthelisttofindapotentialmatchwiththecasebeingreviewed.TheSurveillanceUnitwillneedtoplayaroundwiththedatabasetodiscoverthebestwaytoidentifypotentialduplicates.
56
3. Iftwocasesmatchon1)PUID,2)dateofbirth3)reportingsiteandtestdatetheyareprobablythesameperson.However,lookatotherinformation,suchasregionofresidence,toassistindeterminingwhetherthetwocasesarethesamepersonordifferentpeople.
4. IfaSurveillanceOfficerorotherpersondoingsecondaryreviewdiscoversthattwocasesinthedatabasehavethesameCaseNumberbuttheyhavereasontobelievethattheyaredifferentpeoplethenoneofthemisassignedanewCaseNumber(selectedfromtheCaseNumberLogBook,seebelow).ThenewnumberiswrittenbothontheHCSFandchangedinthedatabaseforALLHCSFformsthathavetheCaseNumberthatmatchesanothercase.Conversely,iftwocaseshavedifferentCaseNumbersbuttheyappeartobethesamepersonthenoneoftheCaseNumbersmustbedeletedsothattheeachHCSFforthissinglepersoncanbeassignedthesameCaseNumber.AllchangesmadeintheEDBarealsochangedontheHCSF,initialedanddated.DonotreusedeletedCaseNumbers,itisapotentialcauseoferrorandthereisnoneedtodoso.
5. OnceitisdeterminedthatthecasebeingreviewedmatchesonealreadyinthedatabasecheckReportTypeinSectionVIoftheHCSFasUpdateandwritetheexistingCaseNumberonthecurrentcase’sHCSF.IfitisdeterminedthattherearenomatchesintheEDBcheckReportTypeinSectionVIoftheHCSFasNewandselectanewCaseNumberfromtheCaseNumberLogBook(seebelow).
AssigningSequentialCaseNumbersUsingtheCaseNumberLogBook
UsingalogbooktoassignCaseNumbersmeansthateither:1)allstaffconductingthistaskmustbeinclosephysicalproximitysothatthelogbookiseasilyaccessibleor2)eachofficewithstaffwhoassignCaseNumbersaregivenaseriestousesothatseparateofficesarenotassignedthesamenumber.Forexample,eachofficethatassignscasenumbershasitsownlogbookandnumberseries.Anexampleofnumberserieswouldbenumbersthatstartwith100,000,200,000,etc.IfthereisonlyonelocationthattheCaseNumbersarebeingassignedthenjustselectastartingnumberandassignthemsequentially.Thelogbookissimplyawaytokeeptrackofwhichnumbershavebeenused.Onceitisdeterminedwhatseriesofnumberstouseandthefirstoneisassignedtheremainingnumbersareassignedsequentially.IfthefirstCaseNumberis500,000,thenextoneis500,001,500,002,etc.Examplesofwaysthesenumbersareassigned/used:
1. If,uponusingthelogbook,oneofthestaffdiscoversthatoneofthesequentialnumberswasmistakenlyskippednocorrectiveactionisneeded.
2. If500,103isassignedtoacaseanditislaterdeterminedthatitisthesamepersonascasenumber500,077thenthenumber500,103isdeletedfromtheforminthedatabaseandnotreused.Thecasethathad500,103assignedhasthenumber500,077enteredintotheEDBasitsCaseNumber.
a. CaseNumber500,054islaterdeterminednottobeHIV‐infected.TheHCSFisdeletedfromthedatabaseandthenumber500,054isnotreused.
Suggestedcolumnheadingsforthelogbookare:
CaseNumber.....PUID....Dateofbirth……..StaffName....DateCaseNumberIssued
57
Thereasonsfortheseheadingsare:
1. CaseNumber‐tokeeptrackoftheissuednumberssotheyarenotusedmorethanonce.Thenumbershavenoinherentmeaningsoifoneisskippedthereisnoproblem.It’simportantistouseeachnumberonlyonce.
2. PUIDandDOB‐toidentifywhichpatientisassignedthenumber.ThishelpsifmorethanonepersonisassigningCaseNumbersandtwoformsforthesamepersonarewithtwodifferentstaff.WhengoingtoassignaCaseNumberifthePUIDandDOBarealreadyassignedanumberstaffpersonscanconsultwitheachothertomakesureeachindividualpersonisassignedthesameCaseNumber
3. Staffname‐tobeabletoidentifywhotookaparticularnumberasinthesituationin2)above.
4. DateCaseNumberIssued.
SelectingOccupation
InordertoanalyzetheoccupationvariablealistofoccupationsofinteresthasbeendevelopedbyNAPSandMoH.
Upon secondary review the Surveillance Unit staff select themost appropriate occupation based on what was
writtenontheHCSFandwritethatanywhereintheEmploymentStatusboxontheHCSF.Itwillbeenteredusinga
matchinglistthatisfoundinadropdownmenuintheelectronicdatabase.
58
AppendixG:DataEntryProcedures
DataEntryProcedures‐StatisticalUnitDataEntryClerkThepurposeof thedataentryprocedures is toensurethatdataareentered inasystematicwaythatminimizes
errors.DataentryisconductedbytheMoHStatisticalUnitDataEntryClerkassignedandtrainedforthistaskafter
the initial and secondary review processes have been completed. The Data Entry Clerk repeats the search for
duplicatestoconfirmwhatwasfoundduringthesecondaryreviewprocedure(AppendixF).ReasonsthattheData
EntryClerkmightfindaduplicatethatwasnotfoundduringsecondarydatareviewinclude:1)apriorformonthe
patientmayhavebeenawaitingdataentrysotheformwasnotintheEDBatthetimethattheEDBwassearched
forduplicatesduringsecondaryreview,and2)asstaffbecomemorefamiliarwiththeEDBtheymaydeveloptheir
ownmethods of searching for duplicates so the two processes conducted by two different people can produce
differentresults.
1. RecordDateReceivedandEntryDateinSectionVIMOHUSEONLY
2. Checkforduplicatesusingtheelectronicdatabase(EDB).SeeHCSFSecondaryReviewProceduresfor
methodsfordeterminingpotentialduplicates.
3. EntertheHCSFinformationintheEDBasanewcaseifnoexistingrecordforthepatient,orupdatethe
patient’srecordifacasealreadyexist
4. EntereachvariableasitappearsontheHCSFanddirectanyquestionstotheMoHSurveillanceUnit.
5. Once data entry has begun this procedure document should include specific directions for any and all
variablesthatrequiremoredetailedexplanations.Examplesinclude:
o Entering occupation using the information written on the form by those conducting secondary
reviewintheSurveillanceUnitusingadropdownmenu.
o Wheretoenter“presentingCD4count”sinceitisnotspecifiedontheform/EDB
o Wheretoentercauseofdeaththatshouldbewritteninrighthandmarginof formwhenpersons
arebeingreportedashavingdied.
o Whattoenterifmorethanoneraceischecked
o WhattowriteontheHCSFiftheEDBcalculatesaPUIDthatdoesnotmatchtheonewrittenonthe
HCSF.
o WhattodoifthefacilitynamewrittenontheHCSFisnotincludedinthedropdownmenuinthe
EDB
6. RecordtherecordnumbergeneratedbytheelectronicdatabaseinSectionVIMOHUSEONLY.
59
7. OncetheHCSFisenteredintothedatabase,storehardcopyinalockedfilecabinetinaroomwithlimited
access.
60
AppendixH:MatchingProcedures
ProcessforMatchingofHIVCaseSurveillanceForms(HCSF)
MatchingProcedures
DatabasematchescanefficientlyaddvaluableinformationtotheHIVregistrywithouttheinformationbeingreportedonanHCSFandmanuallyenteredintotheHIVregistry.Thetwomostprominentexamplesarelaboratorydataanddeathinformation.
Iflabdata–CD4andviralloadresults‐canbeelectronicallymatchedtotheHIVregistryandtheresultsuploadedtotheHIVregistry,thesystemprovidesvaluableinformationonproportionofpersonswhopresentforcare,stayincareandtrendsinCD4countandviralloadvalues.Suchanalysescanbefurtherbrokendownbydemographicvariablestohelptargetservices.BecauseGuyanaisusingthePUIDinsteadofname‐basedreporting,itmaybedifficulttoidentifyrecordsatthelaboratoryandconductsuchamatch.
DeathRegistryMatchProcedure
ThepurposeofthismatchistofindouthowmanypeoplelivingwithHIVinGuyanahavedied.ItisonlybydoingthisthatthesurveillancesystemcanaccuratelymeasurehowmanypeoplearelivingwithHIVinthecountry.Withoutconductingthismatchonaregularbasis(e.g.,annuallyoreverytwoyears)surveillancesystemwilloverestimatethenumberoflivingcases.
AssumingthattheinformationfromtheRegistrationofDeathformisinanelectronicdatabaseandusingthesoftwareintheHIVelectronicdatabasethatcreatesthePUID,createthesamePUIDusingtheinformationfromtheRegistrationofDeathform.Thisformasksformaidennamesothesoftwareshouldpullthefirstinitialofthelastnamefromthatfieldforwomen.SinceweareaskingformaidennamewhenthePUIDiscreatedinVCTandothersettingsthiswillincreasethelikelihoodthatthesamePUIDisbeingusedinbothsystems.
OncethePUIDhasbeencreatedfortheyear(s)thatyouwishtomatchwiththeHIVdatabaseyoucanusethePUID,dateofbirthandsextofindthosepersonswithHIVwhohaveadeathregistrationform.ThematchisasoftwareprogramthatidentifiescasesthatareinboththeHIVelectronicdatabaseandthedeathregistry.AlistofcasesidentifiedasinbothdatabasesisproducedthatincludesthePUID,dateofbirthandsex,dateofdeathandallthecauseofdeathinformationavailablefromthedeathregistry.ASurveillanceOfficerreviewsthelisttoconfirmthatthesematchesdorepresentthesameperson.Oncethatisconfirmedtheinformationthatthepersonhasdied,dateofdeathandcause(s)ofdeathisuploadedintotheHIVEDB.Underlyingcausesofdeath(diseaseorconditionleadingdirectlytodeath,antecedentcausesgivingrisetodeathandothersignificantconditionscontributingtodeath)aresearchedforHIV‐relatedassociatedcausesofdeath.ThisgivesaminimumnumberofHIV‐relateddeathsforaparticularyear.
ThismatchisparticularlyimportantforcapturingdeathsamongHIV‐infectedpersonswhoneveraccessedcareordidsoonlysporadicallyand/oratmultiplelocations.
EvaluationoftheDeathRegistryMatch
61
Evaluationofthedeathregistrymatchisaccomplishedinatleasttwoways:
1) Selectasampleofdeathsfoundfromthematchthatareamongpeoplewhoattendedcareclinics.NotifytheclinicthatthepatienthasdiedandconfirmthatthepatienthasnotbeenseentheresincethedateofdeathobtainedfromtheRegistrationofDeathform
2) SelectasampleofdeathsfoundfromverbalreportsorHCSFreportsofdeathsandseeifthedeathregistrymatchidentifiedthepersonashavingdiedthatyear.
Thismatchisconductedannuallyandevaluatedthoroughlyusingaslargeanddiverseasampleaspossible.Samplediversityisbasedondifferentregionsofthecountryanddifferentsitesofdeath.