Embed Size (px)
Citation preview

GuillainGuillain--BarrBarréé Syndrome and Influenza Syndrome and Influenza VaccineVaccine
James J. Sejvar, MD; Lawrence B. Schonberger, MD, MPHJames J. Sejvar, MD; Lawrence B. Schonberger, MD, MPHDivision of Viral and Rickettsial DiseasesDivision of Viral and Rickettsial Diseases
National Center for Zoonotic, Vectorborne, and Enteric DiseasesNational Center for Zoonotic, Vectorborne, and Enteric DiseasesCenters for Disease Control and PreventionCenters for Disease Control and Prevention
Dina Pfeifer, MD, MScDina Pfeifer, MD, MScDepartment of Immunization, Vaccines, and BiologicalsDepartment of Immunization, Vaccines, and Biologicals
World Health OrganizationWorld Health Organization
GuillainGuillain--BarrBarréé Syndrome (GBS)Syndrome (GBS)
•• ImmuneImmune--mediated polyradiculoneuropathymediated polyradiculoneuropathy•• Acute Acute –– subacute subacute ““ascendingascending”” limb weakness with decreased limb weakness with decreased
reflexesreflexes•• Cranial nerve palsies, respiratory failureCranial nerve palsies, respiratory failure
•• Several potential mechanisms hypothesizedSeveral potential mechanisms hypothesized•• Humoral or cellular immune response to antigenic stimulus, Humoral or cellular immune response to antigenic stimulus,
resulting in attack on nerve selfresulting in attack on nerve self--proteinsproteins•• Numerous infectious agents and immunizations temporally Numerous infectious agents and immunizations temporally
associatedassociated•• Strongest association with Strongest association with Campylobacter jejuniCampylobacter jejuni infection infection ––
““molecular mimicrymolecular mimicry””•• Incidence increases with age, particularly over 50Incidence increases with age, particularly over 50•• Characteristic clinical, laboratory, electrodiagnostic featuresCharacteristic clinical, laboratory, electrodiagnostic features•• Outcome generally favorableOutcome generally favorable
•• Case fatality 5 Case fatality 5 –– 10%10%•• Neurologic sequelae in 20%Neurologic sequelae in 20%•• Older age with worse prognosisOlder age with worse prognosis

GBS and Influenza Vaccine: MethodsGBS and Influenza Vaccine: Methods
•• All available literature reviewed (limited to controlled studiesAll available literature reviewed (limited to controlled studies))•• Use of swineUse of swine--antigen containing influenza vaccines, including antigen containing influenza vaccines, including
A/NJ/76 (H1N1), used preA/NJ/76 (H1N1), used pre-- and postand post--1976 assessed1976 assessed•• Archived WHO, CDC, CBER recordsArchived WHO, CDC, CBER records
•• AFEB recordsAFEB records•• Personal communicationsPersonal communications
•• Comparison data on virologic, molecular characteristics of Comparison data on virologic, molecular characteristics of A/NJ/79 influenza virus, current A/CA/09 virus, other SWA/NJ/79 influenza virus, current A/CA/09 virus, other SW--OI OI virusesviruses
•• Best available data for Best available data for ““backgroundbackground”” rates of GBSrates of GBS: : •• 1.0 1.0 –– 1.7 / 100,000 population / year 1.7 / 100,000 population / year in developed countriesin developed countries•• When possible, published rates converted to incidence / When possible, published rates converted to incidence /
100,000 for comparison100,000 for comparison
GBS and A/NJ/76 (H1N1) VaccineGBS and A/NJ/76 (H1N1) Vaccine
•• 1976: human1976: human--toto--human transmission of swinehuman transmission of swine--origin H1N1 origin H1N1 influenza virus on US military baseinfluenza virus on US military base•• 40 million doses of vaccine among US civilians, military40 million doses of vaccine among US civilians, military•• Influenza epidemic never materializedInfluenza epidemic never materialized
•• ““ClusterCluster”” of GBS cases noted though AE surveillance early of GBS cases noted though AE surveillance early in campaignin campaign•• Campaign discontinued Dec. 16, 1976Campaign discontinued Dec. 16, 1976
•• Subsequent assessment of US civilians by CDC, state Subsequent assessment of US civilians by CDC, state health depts.health depts.•• Active, national caseActive, national case--finding between December 16, finding between December 16,
1976 and Jan 31, 19771976 and Jan 31, 1977•• GBS among adult vaccinees compared to nonGBS among adult vaccinees compared to non--vaccinees vaccinees
((““expectedexpected”” rate)rate)

1. Based on 8 controlled assessments, 1. Based on 8 controlled assessments, A/NJ/76 (H1N1) influenza vaccine associated A/NJ/76 (H1N1) influenza vaccine associated with increased risk of GBS in adultswith increased risk of GBS in adults
•• RR of RR of 7.67.6 (95% CI 6.7 (95% CI 6.7 –– 8.6)8.6)
•• Reporting rate of Reporting rate of 8.6 cases / 100,0008.6 cases / 100,000 / yr/ yr•• NonNon--vaccinees: 1.7 / 100,000 / yrvaccinees: 1.7 / 100,000 / yr
•• Attributable risk of Attributable risk of 0.95 / 100,0000.95 / 100,000 vaccineesvaccinees
•• Features consistent with biological plausibilityFeatures consistent with biological plausibility•• Risk concentrated within first 6 weeks of Risk concentrated within first 6 weeks of
vaccination (peak at week 2 vaccination (peak at week 2 –– 3)3)
•• Not a lotNot a lot-- or manufactureror manufacturer-- specific phenomenonspecific phenomenon
•• Several reSeveral re--analyses with same conclusionsanalyses with same conclusions
2. There are limited data on GBS risk among 2. There are limited data on GBS risk among other populations receiving vaccine.other populations receiving vaccine.
•• U.S. MilitaryU.S. Military•• A/NJ/76 formulation (bivalent) same as civilian, but higher doseA/NJ/76 formulation (bivalent) same as civilian, but higher dose (1.0 ml (1.0 ml
vs. 0.5 ml); also received B vaccinevs. 0.5 ml); also received B vaccine•• Single study: Single study: ““no increased risk of the magnitude reported by CDCno increased risk of the magnitude reported by CDC””; ;
limitations in data*limitations in data*•• No additional controlled data No additional controlled data
•• Use of A/NJ/76 vaccine outside USUse of A/NJ/76 vaccine outside US
•• UK: ? Anecdotal reports, but no confirmationUK: ? Anecdotal reports, but no confirmation
•• Canada: 800,000 doses of monovalent and bivalent vaccine distribCanada: 800,000 doses of monovalent and bivalent vaccine distributeduted•• Limited mechanisms to detect risk of GBS; small population of Limited mechanisms to detect risk of GBS; small population of
vaccineesvaccinees
•• NetherlandsNetherlands•• 2.4 million doses apparently delivered2.4 million doses apparently delivered•• None apparently usedNone apparently used
*Johnson, D. Arch Neurol 1982;39:21

3. There are limited data on risk of GBS 3. There are limited data on risk of GBS from swinefrom swine--antigenantigen--containing influenza containing influenza vaccines prevaccines pre----19761976
•• 1955 1955 –– 1969: Swine antigen (A/swine/Iowa/1976/31 H1N1) 1969: Swine antigen (A/swine/Iowa/1976/31 H1N1) routinely incorporated into U.S. military vaccinesroutinely incorporated into U.S. military vaccines
•• 1956 1956 –– 1959: same antigen incorporated in some civilian 1959: same antigen incorporated in some civilian vaccinesvaccines
•• No suggestion of increased riskNo suggestion of increased risk•• Limited passive surveillance infrastructureLimited passive surveillance infrastructure•• No systematic assessmentsNo systematic assessments•• In limited exposed population, no risk of sufficient In limited exposed population, no risk of sufficient
concern enough to be reported to public health concern enough to be reported to public health authorities or publishedauthorities or published
•• Swine antigens not used since 1976 (Netherlands 1977?)Swine antigens not used since 1976 (Netherlands 1977?)
4. Most data suggest little, if any, significant 4. Most data suggest little, if any, significant risk of GBS following subsequent influenza risk of GBS following subsequent influenza vaccines vaccines
•• Association between other influenza vaccine formulations and GBSAssociation between other influenza vaccine formulations and GBS less clearless clear•• 9 9 wellwell--designed,designed, controlled assessments between 1977 and 2009controlled assessments between 1977 and 2009•• Two suggesting a small but statistically significant increase inTwo suggesting a small but statistically significant increase in risk of GBSrisk of GBS
•• Lasky et al*: Lasky et al*: •• increased risk following influenza vaccine for combined 1992increased risk following influenza vaccine for combined 1992--93 and 93 and
19931993--94 seasons (RR 1.7; 95% CI 1.0 94 seasons (RR 1.7; 95% CI 1.0 –– 2.4; AR 0.06 / 100,000 2.4; AR 0.06 / 100,000 vaccinations); vaccinations);
•• no such risk with each season separately. no such risk with each season separately. •• Juurlink et al#: Juurlink et al#:
•• increased risk of GBS following presumed influenza vaccination increased risk of GBS following presumed influenza vaccination over over period of 1993 period of 1993 –– 2004 (RR 1.45, 95% CI 1.05 2004 (RR 1.45, 95% CI 1.05 –– 1.99)1.99)
•• No increase in incidence of hospital admissions for GBS followinNo increase in incidence of hospital admissions for GBS following g universal influenza vaccination in Ontario in 2000.universal influenza vaccination in Ontario in 2000.
•• Differences in methodologies, case ascertainment methods, analysDifferences in methodologies, case ascertainment methods, analyseses•• No clear, consistent associationNo clear, consistent association•• Potential GBS risk likely outweighed by influenzaPotential GBS risk likely outweighed by influenza--associated morbidity / mortality associated morbidity / mortality
in any particular seasonin any particular season
*N Engl J Med 1998;339:1797 #Arch Int Med 2006;166:2217

5. Biological data on possible mechanisms 5. Biological data on possible mechanisms for association of GBS and A/NJ/76 (H1N1) for association of GBS and A/NJ/76 (H1N1) vaccine are largely absentvaccine are largely absent
•• No association with particular human leukocyte No association with particular human leukocyte antigen (HLA) haplotypes antigen (HLA) haplotypes
•• A/NJ/76 vaccine, A/NJ/76 vaccine, but also other formulationsbut also other formulations, , induces antiinduces anti--myelin ganglioside antibodies in myelin ganglioside antibodies in mice mice (Nachamkin et al. 2008)(Nachamkin et al. 2008)•• Provides biological basis, but significance Provides biological basis, but significance
unclearunclear
•• No robust data suggesting a biological basis for No robust data suggesting a biological basis for associationassociation
*Kaslow et al. Neurology 1987;37:685 #J Infect Dis 2008;198:226
6. There are both molecular and antigenic 6. There are both molecular and antigenic similarities and differences between A/NJ/76 similarities and differences between A/NJ/76 (H1N1) and 2009 A/H1N1 viruses(H1N1) and 2009 A/H1N1 viruses
•• A/NJ/76 (HswN1): A/NJ/76 (HswN1): ““classicalclassical”” swine influenza virusswine influenza virus•• All gene segments derived from viruses since 1930All gene segments derived from viruses since 1930
•• 2009 A/H1N1: novel combination of gene segments2009 A/H1N1: novel combination of gene segments•• 6 genes 6 genes –– ““triple reassortanttriple reassortant””; gene segments from ; gene segments from
swine H1N1, North American avian and human swine H1N1, North American avian and human H3N2H3N2
•• NA, M NA, M –– Eurasian lineage of Hsw1N1 virusesEurasian lineage of Hsw1N1 viruses•• HA antigenically and genetically different from HA antigenically and genetically different from
A/NJ/76A/NJ/76•• Biological properties of 2009 A/H1N1 HA and NA not Biological properties of 2009 A/H1N1 HA and NA not
fully characterizedfully characterized

Conclusions (1)Conclusions (1)
•• A/NJ/76 (H1N1) influenza vaccine associated with increased A/NJ/76 (H1N1) influenza vaccine associated with increased risk of GBS in adults 6 risk of GBS in adults 6 -- 8 weeks following vaccine in US 8 weeks following vaccine in US civilianscivilians•• Reasons unknownReasons unknown•• No clear biological explanationNo clear biological explanation
•• Data on risk of GBS following other swineData on risk of GBS following other swine--antigen antigen containing vaccines too limited to allow for conclusionscontaining vaccines too limited to allow for conclusions
•• Most data suggest little or no risk of GBS following Most data suggest little or no risk of GBS following subsequent influenza vaccinessubsequent influenza vaccines
•• A/NJ/76 (H1N1) and 2009 A(H1N1) viruses differ A/NJ/76 (H1N1) and 2009 A(H1N1) viruses differ virologically and antigenicallyvirologically and antigenically•• Without biological underpinning for 1976 event, unclear Without biological underpinning for 1976 event, unclear
what significance any similarities might have on risk of what significance any similarities might have on risk of vaccinevaccine
Conclusions (2)Conclusions (2)
•• 1976: No significant influenza disease1976: No significant influenza disease
•• 2009: Already associated with morbidity 2009: Already associated with morbidity and mortalityand mortality•• Future epidemiology, potential virulence Future epidemiology, potential virulence
unknownunknown
•• Risk in 1976 may have been acceptable in Risk in 1976 may have been acceptable in the setting of significant influenzathe setting of significant influenza--associated diseaseassociated disease

AcknowlegmentsAcknowlegments
•• John D Grabenstein, RPh, PhD Col (ret) USA; Senior John D Grabenstein, RPh, PhD Col (ret) USA; Senior Director, Adult Vaccine Medical Affairs, Merck Vaccines & Director, Adult Vaccine Medical Affairs, Merck Vaccines & Infectious Diseases.Infectious Diseases.
•• Philip K. Russell, M.D.Major General (ret) USAPhilip K. Russell, M.D.Major General (ret) USA
•• Teresa Hammett, Division of Viral and Rickettsial Diseases, Teresa Hammett, Division of Viral and Rickettsial Diseases, Centers for Disease Control and PreventionCenters for Disease Control and Prevention
•• Dr. Cathy Parker, Biologics and Genetic Therapies Dr. Cathy Parker, Biologics and Genetic Therapies Directorate Health CanadaDirectorate Health Canada
•• Dr. Mair Powell, Medicines and Healthcare products Dr. Mair Powell, Medicines and Healthcare products Regulatory Agency, United Kingdom of Great Britain & Regulatory Agency, United Kingdom of Great Britain & Northern IrelandNorthern Ireland
•• Dr. Bettie Voordouw, Medicines Evaluation Board, Dr. Bettie Voordouw, Medicines Evaluation Board, Netherlands.Netherlands.
Additional SlidesAdditional Slides

GBS and Influenza IllnessGBS and Influenza Illness
•• Case reports of GBS following influenza / Case reports of GBS following influenza / ILIILI
•• No substantial evidence of strong No substantial evidence of strong associationassociation•• No seasonal pattern of GBSNo seasonal pattern of GBS•• No increase in GBS following large No increase in GBS following large
epidemicsepidemics•• Several reports suggest risk, but data Several reports suggest risk, but data
conflictingconflicting
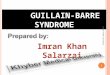
VaccineVaccine--Associated Neurologic Associated Neurologic DiseaseDisease
Neurologic AE
NeurotropicPost-ImmunizationImmune-Mediated
Central Nervous System
Central NervousSystem
Peripheral NervousSystem
“Idiosyncratic”

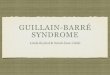
““PhylogenyPhylogeny”” of GBSsof GBSs
Guillain-BarréSyndromes
Acute InflammatoryDemyelinating Type
(AIDP)
Acute motor axonalType (AMAN)
Fisher syndrome
(Secondary axonalDegeneration)
Acute motor andSensory axonal type
(AMSAN)

GuillainGuillain--BarrBarréé SyndromeSyndrome
•• Acute inflammatory demyelinating polyradiculopathyAcute inflammatory demyelinating polyradiculopathy----most common form of GBS in North America, Europemost common form of GBS in North America, Europe•• Primarily axonal form more common in developing Primarily axonal form more common in developing
worldworld
•• Incidence 0.5 Incidence 0.5 –– 4 / 100,000, depending on study design; 4 / 100,000, depending on study design; incidence increases with ageincidence increases with age
•• Demyelination > axonal damage; cross Demyelination > axonal damage; cross -- reactive epitopes reactive epitopes on peripheral myelin sheath or axonson peripheral myelin sheath or axons
•• Various structural glycoproteins on myelin / axons Various structural glycoproteins on myelin / axons induce antigenic responseinduce antigenic response
•• Antecedent viralAntecedent viral--like illness or immunization reported in like illness or immunization reported in over 2/3over 2/3
GBSGBS
•• Acute Acute –– subacute onset of weaknesssubacute onset of weakness–– evolve over days to weeksevolve over days to weeks•• MostMost–– maximal deficit within 2 weeksmaximal deficit within 2 weeks•• HypoHypo-- or areflexiaor areflexia
•• ““AscendingAscending”” weaknessweakness——legs to arms; generally symmetriclegs to arms; generally symmetric
•• Sensory abnormalitiesSensory abnormalities•• Ascending pain or dysesthesiasAscending pain or dysesthesias•• Objective numbness generally absentObjective numbness generally absent
•• Autonomic dysfunctionAutonomic dysfunction•• Tachy / bradycardia, hypotension, arrhythmiasTachy / bradycardia, hypotension, arrhythmias
•• Cytoalbuminologic dissociation Cytoalbuminologic dissociation –– elevated CSF protein in elevated CSF protein in absence of pleocytosisabsence of pleocytosis
•• Characteristic electrophysiologic profile Characteristic electrophysiologic profile –– reduced conduction reduced conduction velocities and decreased amplitudes indicative of demyelinationvelocities and decreased amplitudes indicative of demyelination
•• Fisher Syndrome: Fisher Syndrome: ““ataxia, areflexia, ophthalmoplegiaataxia, areflexia, ophthalmoplegia””

GBS and Glycoconjugate AntibodiesGBS and Glycoconjugate Antibodies
•• Gangliosides: glycosphingolipids in plasma membrane of Gangliosides: glycosphingolipids in plasma membrane of tissuestissues•• Major surface molecules of PNS & CNS tissuesMajor surface molecules of PNS & CNS tissues
•• Strong association of antiganglioside antibodies with GBS; Strong association of antiganglioside antibodies with GBS; thought to play a role in pathogenesisthought to play a role in pathogenesis•• AntiAnti--GM1: AMANGM1: AMAN•• AntiAnti--GQ1b: FSGQ1b: FS
•• Natural infection with certain serotypes of Natural infection with certain serotypes of Campylobacter Campylobacter jejunijejuni associated with GBSassociated with GBS•• CrossCross--reactive antibodies to gangliosides and reactive antibodies to gangliosides and C. jejuniC. jejuni
lipopolysaccharide moieties lipopolysaccharide moieties •• Biological plausibility?Biological plausibility?
GBSGBS
•• Outcome generally favorable; complete recovery Outcome generally favorable; complete recovery with or without treatmentwith or without treatment•• Advanced age, mechanical ventilation Advanced age, mechanical ventilation
associated with poorer outcomeassociated with poorer outcome
•• Treatment modifies disease progression and Treatment modifies disease progression and outcomeoutcome•• Intravenous immune globulin (IVIG)Intravenous immune globulin (IVIG)•• PlasmapheresisPlasmapheresis•• Corticosteroids contraindicatedCorticosteroids contraindicated

GBS vs. CIDPGBS vs. CIDP
GBSGBS CIDPCIDPAntibodiesAntibodies AIDP: VariableAIDP: Variable
AMAN: GM1AMAN: GM1FS: GQ1bFS: GQ1b
No antibodiesNo antibodies
Antecedent eventAntecedent event 70%70% NoneNone
CourseCourse MonophasicMonophasic Relapsing / remittingRelapsing / remitting
TreatmentTreatment IVIG, PLEXIVIG, PLEX Steroids, IVIG, PLEXSteroids, IVIG, PLEX
PathologyPathology Axonal and demyelinatingAxonal and demyelinating DemyelinatingDemyelinating
Differentiation between GBS and CIDP requires longitudinal follow-up to identify relapses and remissions
GBS and VaccinesGBS and VaccinesInfluenzaInfluenza•• 1976 swine influenza: small but significant risk for GBS (1 1976 swine influenza: small but significant risk for GBS (1
additional case / 100,000 vaccinees) 1 additional case / 100,000 vaccinees) 1 –– 6 weeks post6 weeks post--immunizationimmunization•• IOM: IOM: ““evidence favors a causal association...evidence favors a causal association...””
•• Association between other influenza vaccine formulations and Association between other influenza vaccine formulations and immunizations less clearimmunizations less clear•• 19 19 wellwell--designed,designed, controlled studies in the literature between controlled studies in the literature between
1977 and 20091977 and 2009•• 22 (Lasky et al., 1998 [flu]; Kinnunen et al., 1989 [OPV]) (Lasky et al., 1998 [flu]; Kinnunen et al., 1989 [OPV])
suggest slightly increased risk...(maximal odds ratio 1.7)suggest slightly increased risk...(maximal odds ratio 1.7)•• No clear, consistent associationNo clear, consistent association
•• Biological data: swine influenza vaccine, Biological data: swine influenza vaccine, but also other but also other formulationsformulations, induces anti, induces anti--myelin ganglioside antibodies in mice myelin ganglioside antibodies in mice (Nachamkin et al. 2008)(Nachamkin et al. 2008)•• Provides biological basis, but significance unclearProvides biological basis, but significance unclear
![Guillain-Barré Syndrome 28 and Related DisordersGuillain-Barré syndrome (GBS), also known as Landry-Guillain-Barré-Strohl syndrome, was described in 1916 [ 1, 2 ] . GBS is usually](https://img.pdfslide.us/doc/110x75/5f334ccc3207631439633ebc/guillain-barr-syndrome-28-and-related-disorders-guillain-barr-syndrome-gbs.jpg)