Embed Size (px)
Citation preview

Neurology® Clinical Practice Research
Guillain-Barré syndrome aftersurgical proceduresPredisposing factors and outcomeElanagan Nagarajan, MD; Mark Rubin, MD; Eelco F.M. Wijdicks, MD; Sara E. Hocker, MD
AbstractBackground: We sought to identify clinical associa-tions and potential triggers of Guillain-Barré syndrome(GBS) within 8 weeks of surgical procedures.Methods:We retrospectively reviewed consecutive patientsdiagnosed with GBS within 8 weeks of a surgicalprocedure between January 1995 and June 2014at Mayo Clinic. Postsurgical GBS was defined assymptom onset within 8 weeks of a surgical proce-dure. Patients with postsurgical GBSwere comparedwith patients who did not have a surgery or proce-dure prior to GBS onset to determine differences be-tween groups. Results: A total of 208 patients withGBS, median age 55 years (interquartile range[IQR] 41–68), were included. Thirty-one patients(15%) developed postsurgical GBS. Median dura-tion from the surgery or procedure to onset of firstGBS symptom was 19 days (IQR 11.1–37.5). Themain types of surgeries/procedures preceding GBSwere gastrointestinal, cardiac, and orthopedic. General anesthesia was used in 18 (58%)and conscious sedation in 13 (42%) patients. Among the 31 patients with postsurgicalGBS, 19 (61%) had a known diagnosis of malignancy. Autoimmune conditions were pres-ent in 9 (29%) patients. Additional triggering factors were identified in 11 (35.5%)patients. On univariate analysis, the factors that showed an association with postsurgicalGBS were age (p 5 0.003), malignancy (p , 0.0001), active malignancy (p 5 0.05),preexisting autoimmune disorder (p 5 0.001), and duration of hospital stay (p 5 0.015).On multivariate analysis, age (p 5 0.045), malignancy (p , 0.0001), and preexisting au-toimmune disorder (p 5 0.004) remained associated. Conclusions: Surgical proceduresantedated GBS in 15% of patients, which is unexpectedly high. History of malignancy or au-toimmune disease may predispose to development of postsurgical GBS. Neurol Clin Pract
2017;7:1–9
Department of Neurology (EN, EFMW, SEH), Mayo Clinic, Rochester, MN; Department of Neurology (MR),Northshore University Health System, Glenview, IL; and Department of Neurology, Mayo Clinic, Scottsdale, AZ.
Funding information and disclosures are provided at the end of the article. Full disclosure form informationprovided by the authors is available with the full text of this article at Neurology.org/cp.
Correspondence to: [email protected]
Neurology: Clinical Practice |||||||||||| February 2017 Neurology.org/cp 1
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Patients with Guillain-Barré syndrome (GBS) may recall a flu-like syndrome weeksbefore the onset of symptoms. Other antecedent events have been reported, in-cluding trauma, vaccination, blood transfusion, administration of chemotherapy, orsurgery. Two publications from Mayo Clinic and Massachusetts General Hospital
have reported surgical procedures as a trigger for GBS.1,2 Since these observations werepublished, 2 retrospective series noted an incidence of GBS after surgery of 5% and 9.5%,and multiple subsequent case reports have been published, most commonly in patients un-dergoing cardiovascular, gastrointestinal, or neurosurgical procedures.1–8 The first detailedstudy on postoperative polyneuritis reported that postsurgical GBS occurred as a result ofthe release of nerve antigen during the course of surgery. Further, the authors hypothesized anassociation with other host factors that caused a vigorous immunologic response, culminatingin the development of polyneuritis.1 Others have postulated that surgical stress induced theactivation of neuroendocrine stress axis and cell-mediated immunosuppression, which in turnmight promote infections resulting in the production of cross-reactive antibodies.9,10 Weaimed to understand whether patients who presented with GBS within 8 weeks of under-going a surgery or procedure are different from other patients developing GBS.
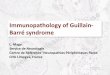
METHODSWe retrospectively reviewed medical records of patients diagnosed with GBS between January1995 and June 2014 at Mayo Clinic. We used the search terms acute demyelinating polyneur-opathy, Guillain-Barré syndrome, and Miller Fisher syndrome in the reason for admission,discharge diagnosis, body of the clinical documents, and problem list to identify patients. Allcharts were reviewed and only patients aged 18–90 years with GBS diagnosed on the basis ofdiagnostic criteria proposed in 1990 (figure 1) were included.11 We excluded patients who
Figure 1 Diagnostic criteria for Guillain-Barré syndrome
Patients with postsurgical GBS were comparedwith those with GBS and no prior surgery/procedure to determine the differencesbetween groups.
2 © 2016 American Academy of Neurology
Elanagan Nagarajan et al.
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

were diagnosed with GBS outside Mayo Clinic or were experiencing a recurrent episode ofGBS.
Variables collected included basic demographics, history of autoimmune disorders and ma-lignancy, other established GBS triggers, surgery/procedure type, type of anesthesia, number ofdays from the surgery/procedure to onset of GBS, details of treatment for the GBS episode,duration of hospital stay, and recurrence of GBS during follow-up. Active malignancy was de-fined as a diagnosis of cancer within 6 months of enrollment, any treatment for cancer withinthe previous 6 months, or documented recurrent or metastatic cancer.12 The study group wasdefined as those patients who developed postsurgical GBS, defined as GBS symptom onsetwithin 8 weeks of a surgery or procedure.3 Patients with postsurgical GBS were comparedwith those with GBS and no prior surgery/procedure to determine the differences betweengroups.
Standard protocol approvals, registrations, and patient consentsThis study was reviewed by and received approval from our institutional review board. Patientswho had not given consent to use their medical records for research were excluded.
Statistical analysisDescriptive summaries were reported using frequencies and percentages for categorical variablesand median and interquartile range (IQR) for continuous variables. Statistical significance wasset at the conventional 2-tailed a level of 0.05. Associations between the categorical variableswere assessed using the x2 test or Fisher exact test as appropriate and Kruskal-Wallis test wasused to compare the continuous variables as they were not normally distributed. Furtheranalysis was performed using the multivariate logistic regression. Variables with p valuesof ,0.05 were considered as candidate variables for multivariate regression. Since only 3variables could be analyzed simultaneously in the model (due to small size of the populationand to avoid overfitting), multiple models with all possible combinations of importantvariables were analyzed, before arriving at the final set of included variables. Odds ratioand 95% confidence intervals were used to quantify the strength of associations. All thestatistical analyses were performed using JMP 10.0.0 (SAS Institute Inc., Cary, NC).
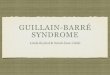
RESULTSWe identified 969 patients using our search terms, 208 of whom met inclusion criteria(figure 2). Median age was 55 years (IQR 41–68), and 120 (58%) were men. The demo-graphic details are presented in table 1. Thirty-one (15%) patients developed postsurgicalGBS. The median age of patients with postsurgical GBS was 63 years (IQR 57–71) and 20(65%) were men. Details of the surgeries and procedures are included in table 2. The mostcommonly used type of anesthesia was general in 18 (52%) patients, followed by conscioussedation in 13 (41.9%) patients. No patient developed GBS after a procedure in which theywere administered only spinal or local anesthesia. The median duration from the surgery orprocedure to the onset of GBS symptoms was 19 days (IQR 11–38).
Nineteen (61%) patients had an associated malignancy and 10 patients (52.6%) had activemalignancies. Gastrointestinal (5; 26%) and hematologic malignancies (5; 26%) were the mostcommon type, followed by prostate (3; 16%) and gynecologic cancer (3; 16%). Comorbid
Patients with postsurgical GBS were morelikely to have comorbid autoimmune conditionscompared to those who developed GBS withouta prior surgery.
Neurology: Clinical Practice |||||||||||| February 2017 Neurology.org/cp 3
Guillain-Barré syndrome after surgical procedures
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

autoimmune conditions were present in 9 (29%) patients with postsurgical GBS. Apart fromsurgical procedures, other triggers were identified in 11 (36%) patients, including chemother-apy in 5 (45%), blood transfusion in 4 (35%), and trauma and vaccination in 2 (7%) patientseach. Twenty (65%) patients were treated with IV immunoglobulin (IVIg), 8 (26%) with plas-mapheresis, and 2 (7%) received both IVIg and plasmapheresis. The median duration of hos-pital stay was 12 days (IQR 6–19). Five (16%) patients died during the hospital stay. Thecause of death is unknown in 2 patients, related to underling malignancy in 2 patients, andrelated to respiratory failure due to pneumonia in 1 patient. The median duration of follow-up after the diagnosis was 42 months (IQR 2–123). Sixteen patients underwent surgicalprocedures after the diagnosis of GBS and the median number of surgical procedures was 1(IQR 0–2). There were no recurrences of GBS in these patients.
On univariate analysis, the factors that were associated with GBS after a surgery or procedurewere age (p 5 0.003), malignancy (p , 0.0001), active malignancy (p 5 0.05), or preexistingautoimmune disorder (p 5 0.001) (table 3). On multivariate logistic regression analysis, age(p 5 0.05), malignancy (p , 0.0001), and preexisting autoimmune disorder (p 5 0.004)remained significant (table 4).
DISCUSSIONIn this large consecutive series of patients with GBS, we found that malignancy and comorbidautoimmune disease were strongly and independently associated with the development of post-surgical GBS, while older age was less strongly associated.
A positive history of autoimmune conditions was present in nearly 10% of the patients withpostsurgical GBS in our series. Patients with postsurgical GBS were more likely to have comor-bid autoimmune conditions compared to those who developed GBS without a prior surgery.Existing literature with regard to adult populations reported autoimmune conditions to be
Figure 2 Patient flow diagram
GBS 5 Guillain-Barré syndrome.
4 © 2016 American Academy of Neurology
Elanagan Nagarajan et al.
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Table 1 Demographic and clinical features of adults with Guillain-Barré syndrome
Demographics Values (total n 5 208)
Age, y, median (IQR) 55 (41.3–68)
Male, n (%) 120 (57.7)
Duration of hospital stay, d, median (IQR) 7 (4–16)
Mortality 5 (2.4)
Underlying malignancy, n (%) 46 (22.1)
GI carcinomas 10 (4.8)
Blood cancers 10 (4.8)
Skin cancer 7 (3.3)
Prostate cancer 5 (2.4)
Gynecologic cancer 5 (2.4)
Active cancer 22 (10.6)
Autoimmune conditions, n (%) 20 (9.6)
Ulcerative colitis 5 (2.4)
Type 1 DM 2 (1)
Sjögren syndrome 3 (1.5)
Giant cell arteritis 1 (0.5)
Addison disease (immune) 1 (0.5)
Sarcoidosis 1 (0.5)
Endometriosis 1 (0.5)
Autoimmune hepatitis 1 (0.5)
Immune-mediated thrombocytopenia 1 (0.5)
Antiphospholipid antibody syndrome 1 (0.5)
Graves disease 1 (0.5)
Rheumatoid arthritis 2 (1)
Treatment, n (%)
IVIg 125 (60.1)
Plasmapheresis 34 (16.3)
IVIg 1 plasmapheresis 15 (7.2)
Steroids 6 (2.9)
IVIg 1 Steroids 2 (0.9)
No treatment 26 (12.5)
Triggers, n (%) 32 (15.4)
Chemotherapy 10 (31.3)
Vaccination 8 (25)
Blood transfusion 5 (15.6)
Trauma 3 (9.4)
Recent surgery or procedure 31 (14.9)
Abbreviations: DM 5 diabetes mellitus; GI 5 gastrointestinal; IQR 5 interquartile range; IVIg 5 IVimmunoglobulin.
Neurology: Clinical Practice |||||||||||| February 2017 Neurology.org/cp 5
Guillain-Barré syndrome after surgical procedures
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

more prevalent in patients with GBS, accounting for 10%–14%. This finding was consistentwith the results of the present study and higher than the incidence of autoimmune disordersin the population at large.13,14 This might be attributed to the transient immunosuppression,which in turn caused an inflammatory response to the neurogenic protein in the peripheral
Table 3 Factors associated with patients developing Guillain-Barré syndrome (GBS) aftersurgery on univariate analysis
GBS without recentsurgery (n 5 177)
GBS aftersurgery (n 5 31) p Value
Age, y, median (IQR) 52 (40.5–66) 63 (57–71) 0.003
Male, n (%) 100 (56.5) 20 (64.5) 0.4
Malignancy, n (%) 27 (15.3) 19 (61.3) ,0.0001
Active malignancy, n (%) 10 (37.1) 12 (66.7) 0.05
Autoimmune, n (%) 11 (6.2) 9 (29) 0.001
Abbreviation: IQR 5 interquartile range.
Table 2 Details of surgeries and procedures
Surgery or procedure No. (%) (total n 5 31)
Gastrointestinal surgery 10 (32.1)
Colonoscopy with biopsy 4 (12.9)
Colectomy 3 (9.6)
Abdominal aneurysm repair 1 (3.2)
Cholecystectomy 1 (3.2)
Post biliary stenting 1 (3.2)
Cardiac surgery 5 (16.1)
Angioplasty with stenting 3 (9.6)
Coronary bypass surgery 1 (3.2)
AICD placement 1 (3.2)
Orthopedic surgery 4 (12.9)
Total knee replacement 2 (6.4)
Hip replacement 1 (3.2)
Bimalleolar fracture open reduction 1 (3.2)
Thoracic surgery 3 (9.6)
Lung lobectomy 1 (3.2)
Lung biopsy 2 (6.4)
Uro-gynecologic surgery 3 (9.6)
Urethral stent placement 2 (6.4)
Hysterectomy and salpingo-oophorectomy 1 (3.2)
Bone marrow biopsy 3 (9.6)
Transsphenoidal resection of pituitaryadenoma
1 (3.2)
Oral maxillofacial surgery 1 (3.2)
Septoplasty 1 (3.2)
Abbreviation: AICD 5 automatic implantable cardioverter defibrillator.
6 © 2016 American Academy of Neurology
Elanagan Nagarajan et al.
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

nervous system (PNS), thereby triggering GBS.15 Multiple previously published case reportshave documented the association between GBS and immunodeficiency and malignancy.16–21
A population-based study in patients with GBS concluded that cancer patients were moreprone to develop GBS, with a reported prevalence of 2.4 times higher when compared to thegeneral population.19 Interestingly, comorbid malignancy was an independent risk factor forthe development of postsurgical GBS in the present study when compared to the controlgroup. Still, there is no consensus about the association between postsurgical GBS andmalignancy or preexisting autoimmune disease. We presumed that the surgical procedurecaused exposure of nerve roots, followed by oncoantigen-mediated misdirection of autoim-mune response to epitopes present in the PNS.19 The other possibility considered wasimmune dysregulation secondary to the pharmacologic agents (e.g., halothane, enflurane,propofol, ketamine) used during the last few decades. Most of these drugs were lipid solubleand could interact with PNS myelin and initiate the cascade of immunologic process. Suchlipid-soluble drugs and trauma to the nerve root could cause demyelinating disorders in thesetting of transient immunosuppression.13 A third possibility is immunosuppression triggeringGBS, secondary to surgical procedure, underlying malignancy, or subclinical infections.
Other factors known to be associated with GBS include transplantation, Hodgkin disease,leukemia, infection, vaccination, and blood transfusion.16–21 Our study population was com-parable to previously published series with respect to the distribution of other triggeringfactors.
During the study period, more than 50,000 surgeries were performed under general anes-thesia and innumerable procedures were performed under conscious sedation at the institutionwhere the study was undertaken. The occurrence of GBS after a surgery or procedure was there-fore extremely rare and this was demonstrated earlier in large population studies.3,4,22
A surgery or procedure preceded the onset of GBS symptoms in 15% of patients in the pres-ent study, conducted over 18.5 years. In the Massachusetts General Hospital, a series of 169patients with GBS was observed from 1962 to 1978. About 10 patients with postsurgicalGBS were reported with postoperative wound infections or blood transfusions, and one patientwith cytomegalovirus infection. The findings of the present study were higher than what waspreviously reported with smaller study populations.3–5,22
One study reported an incidence of postsurgical GBS of 9.5%. Within a relatively small co-hort of 63 patients, 6 patients developed GBS within 6 weeks of a surgery. The affected groupincluded patients with exposure to general anesthesia during the surgical procedure only.4 Weincluded a large series of 208 patients who underwent both general and conscious sedation.Traditionally, most of the procedures were done under general anesthesia. However, over thelast 2 decades, due to advances in surgical techniques and anesthetic medications, higherprevalence of side effects associated with general anesthesia, and endotracheal intubation,most procedures such as colonoscopy, endotracheal biopsy, and laparoscopic surgeries wereperformed under conscious sedation.23–26 We presumed that the risk of nerve damage asso-ciated with procedures and transient immunosuppression remained the same, regardless of theduration of procedure and type of anesthetic medications used.
Table 4 Factors associated with patients developing Guillain-Barré syndrome after surgeryon multivariate analysis
Odds ratio 95% CI p Value
Age 1.03 1.001–1.06 0.045
Autoimmuneconditions
5.19 1.70–15.81 0.004
Malignancy 7.19 3.04–17.69 ,0.0001
Abbreviation: CI 5 confidence interval.
Neurology: Clinical Practice |||||||||||| February 2017 Neurology.org/cp 7
Guillain-Barré syndrome after surgical procedures
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

In addition, we included patients with symptom onset within 8 weeks from the onset ofa surgical procedure. These 2 factors probably accounted for the higher incidence of postsur-gical GBS in the current study. In another study, including pediatric and adult patients, 1,034patients developed GBS during the study period, among whom 52 (5%) experienced symptomonset within 8 weeks of a surgical procedure.3 In the abovementioned study, patients withother potential triggering factors for GBS occurring within 8 weeks of symptom onset werenot excluded. This aspect was similar to the present study.
Mortality rate was 16% among patients with postsurgical GBS. Deaths were predominantlynoticed during the acute and early plateau phase. Mortality was shown to be higher in cancerpatients who developed GBS when compared to the general population.19 In an earlier studyinvolving a large series of patients with GBS, the mortality rate was 2.8%–3.9% at 1 yearfollow-up. It was also observed that death occurred predominantly during the recoveryphase.27 We attributed this to the preexisting comorbid conditions and complications ofthe surgical procedures in these patients, since the mortality rate for the entire GBS series,including patients without an antecedent surgical procedure, was 2.4%.
The duration of hospital stay in patients with GBS after the surgical procedure was found tobe longer when compared to that in patients who did not undergo surgery. This might be dueto the time required for postoperative recovery. However, future studies should examine if thecourse of GBS would be more severe and prolonged in patients with antecedent surgery thanwithout.
We were not able to document the incidence and attributable risk in the study populationwithout an exact number of surgical procedures performed during the study period. Nonethe-less, patients developing GBS after a surgery or procedure represent a rare, distinct cohort withmore frequent history of malignancy and autoimmunity.
Surgical procedures antedated GBS in 15% of patients, which was unexpectedly high. Inmost instances, surgery does not predispose patients to new onset of quadriparesis within 8weeks of the procedure. In the event of such an occurrence, a search for malignancy or auto-immune disease may be warranted.
REFERENCES1. Arnason BG, Asbury AK. Idiopathic polyneuritis after surgery. Arch Neurol 1968;18:500–507.2. Wiederholt WC Mulder DW Lambert EH. The Landry-Guillain-Barré Strohl syndrome or polyra-
diculoneuropathy: historical review, report on 97 patients, and present concepts. Mayo Clin Proc1964;30:427.
3. Hurwitz ES, Holman RC, Nelson DB, Schonberger LB. National surveillance for Guillain-Barrésyndrome: January 1978-March 1979. Neurology 1983;33:150–157.
4. Gensicke H, Datta AN, Dill P, Schindler C, Fischer D. Increased incidence of Guillain-Barrésyndrome after surgery. Eur J Neurol 2012;19:1239–1244.
5. Ropper AH, Wijdicks EFM, Truax BT. Antecedent and associated illness, Guillain-Barré syndrome.In: Contemporary Neurology Series, vol 34. Philadelphia: FA Davis; 1991:71.
6. Algahtani H, Moulin DE, Bolton CF, Abulaban AA. Guillain-Barre syndrome following cardiacsurgery: difficult diagnosis in the intensive care unit. Neurosciences (Riyadh) 2009;14:374–378.
7. Chang CG, Helling TS, Black WE, Rymer MM. Weakness after gastric bypass. Obes Surg 2002;12:592–597.
8. Papantoni E, Sakorafas GH, Zouros E, Peros G. Guillain-Barré syndrome following total gastrecto-my/esophagectomy: a very rare and dramatic post-operative complication with a favourable outcome.ANZ J Surg 2010;80:858.
9. Hogan BV, Peter MB, Shenoy HG, Horgan K, Hughes TA. Surgery induced immunosuppression.Surgeon 2011;9:38–43.
10. Vucic S, Kiernan MC, Cornblath DR. Guillain-Barré syndrome: an update. J Clin Neurosci 2009;16:733–741.
11. Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain-Barré syndrome.Ann Neurol 1990;27(suppl):S21–S24.
12. Lee AY, Levine MN, Baker RI, et al. Low-molecular-weight heparin versus a coumadin for the preventionof recurrent venous thromboembolism in patients with cancer. N Engl J Med 2003;349:146–153.
8 © 2016 American Academy of Neurology
Elanagan Nagarajan et al.
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

13. Korn-Lubetzki I, Abramsky O. Acute and chronic demyelinating inflammatory polyradiculoneurop-athy: association with autoimmune diseases and lymphocyte response to human neuritogenic protein.Arch Neurol 1986;43:604–608.
14. Abramsky O, Korn-Lubetzky I, Teitelbaum D. Association with autoimmune diseases and cellularimmune response to the neuritogenic protein in Guillain-Barré syndrome. Trans Am Neurol Assoc1980;105:350–354.
15. Steiner I, Argov Z, Cahan C, Abramsky O. Guillain-Barré syndrome after epidural anesthesia: directnerve root damage may trigger disease. Neurology 1985;35:1473–1475.
16. Ozkan A, Taskapilioglu O, Bican A, et al. Hairy cell leukemia presenting with Guillain-Barre syn-drome. Leuk Lymphoma 2007;48:1048–1049.
17. Qureshi AI, Cook AA, Mishu HP, Krendel DA. Guillain-Barré syndrome in immunocompromisedpatients: a report of three patients and review of the literature. Muscle Nerve 1997;20:1002–1007.
18. Re D, Schwenk A, Hegener P, Bamborschke S, Diehl V, Tesch H. Guillain-Barré syndrome ina patient with non-Hodgkin’s lymphoma. Ann Oncol 2000;11:217–220.
19. Vigliani MC, Magistrello M, Polo P, Mutani R, Chiò A; Piemonte and Valled’Aosta Register forGuillain-Barré Syndrome. Risk of cancer in patients with Guillain-Barré syndrome (GBS): a popula-tion-based study. J Neurol 2004;251:321–326.
20. Brannagan TH III, Zhou Y. HIV-associated Guillain-Barré syndrome. J Neurol Sci 2003;208:39–42.21. El-Sabrout RA, Radovancevic B, Ankoma-Sey V, Van Buren CT. Guillain-Barré syndrome after solid
organ transplantation. Transplantation 2001;71:1311–1316.22. Sipilä JO, Soilu-Hänninen M. The incidence and triggers of adult-onset Guillain-Barré syndrome in
southwestern Finland 2004-2013. Eur J Neurol 2015;22:292–298.23. Lobo R, Kiernan T. The use of conscious sedation in elective external direct current cardioversion:
a single centre experience. BMJ Qual Improv Rep 2015;4. eCollection 2015.24. Rosati M, Bramante S, Conti F, Rizzi M, Frattari A, Spina T. Laparoscopic salpingo-oophorectomy in
conscious sedation. JSLS 2015;19.25. Grau-Talens EJ, Cattáneo JH, Giraldo R, Mangione-Castro PG, Giner M. Transcylindrical chole-
cystectomy under local anesthesia plus sedation: a pilot study. Endoscopy 2010;42:395–399.26. Sivalingam S, Tamm-Daniels I, Nakada SY. Office-based ureteral stent placement under local anes-
thesia for obstructing stones is safe and efficacious. Urology 2013;81:498–502.27. Van den Berg B, Bunschoten C, van Doorn PA, Jacobs BC. Mortality in Guillain-Barre syndrome.
Neurology 2013;80:1650–1654.
Received June 3, 2016. Accepted in final form August 11, 2016.
AUTHOR CONTRIBUTIONSE. Nagarajan was responsible for study design, study concept, data collection, data analysis, and draftingthe manuscript. M. Rubin was responsible for data collection and revision of the manuscript. E.F.M.Wijdicks was responsible for study concept and manuscript revision. S.E. Hocker was responsible forstudy design, study concept, drafting the manuscript, and manuscript revision.
ACKNOWLEDGMENTThe authors thank Dr. Tarun Singh for assistance with creating the tables and statistical review.
STUDY FUNDINGNo targeted funding reported.
DISCLOSURESE. Nagarajan and M. Rubin report no disclosures. E.F.M. Wijdicks receives publishing royalties frombooks published by Oxford University Press. S.E. Hocker serves on a scientific advisory board for SAGETherapeutics; has received speaker honoraria from the AAN and honoraria from Continuum; and servesas an Associate Editor for Frontiers in Neurology Education, on the editorial board of Journal of Strokeand Cerebrovascular Diseases, and as Review Editor for Frontiers in Stroke and Frontiers in Neurocriticaland Neurohospitalist Care. Full disclosure form information provided by the authors is available withthe full text of this article at Neurology.org/cp.
Neurology: Clinical Practice |||||||||||| February 2017 Neurology.org/cp 9
Guillain-Barré syndrome after surgical procedures
ª 2016 American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

DOI 10.1212/CPJ.0000000000000329 published online November 23, 2016Neurol Clin Pract
Elanagan Nagarajan, Mark Rubin, Eelco F.M. Wijdicks, et al. Guillain-Barré syndrome after surgical procedures: Predisposing factors and outcome
This information is current as of November 23, 2016
ServicesUpdated Information &
29.full.htmlhttp://cp.neurology.org/content/early/2016/11/23/CPJ.00000000000003including high resolution figures, can be found at:
Subspecialty Collections
http://cp.neurology.org//cgi/collection/guillainbarre_syndromeGuillain-Barre syndrome
http://cp.neurology.org//cgi/collection/autoimmune_diseasesAutoimmune diseasesfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://cp.neurology.org/misc/about.xhtml#permissionsits entirety can be found online at:Information about reproducing this article in parts (figures,tables) or in
Reprints
http://cp.neurology.org/misc/addir.xhtml#reprintsusInformation about ordering reprints can be found online:
Neurology. All rights reserved. Print ISSN: 2163-0402. Online ISSN: 2163-0933.since 2011, it is now a bimonthly with 6 issues per year. Copyright © 2016 American Academy of
is an official journal of the American Academy of Neurology. Published continuouslyNeurol Clin Pract