Embed Size (px)
Citation preview
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 1/16
Guidelines for CHPS implementation, Eastern Region (DRAFT)
PART ONE
General Principles of CHPS
Definition
CHPS is the acronym for Community based Health Planning and Services
The CHPS concpet means three things: a process, a policy and a strategy.
PROCESS - All stakeholders in health participate in planning, implementation, monitoring &
evaluation of health service delivery at community & household levels. The fifteen (15) steps are
all important. One step does not need to be completed before moving to the next. Sometimes you
may have to go back to strengthen a step when you realise that it is weak.
The step are broadly grouped into two: strategic and operational planning phases.
The Strategic planning phase is when the DHMT and the other key stakeholders plan to zone the
district into CHPS zones and come sout with a district coverage plan which may be updated
every year. The following steps are important:
i. Situation analysis of the districtii. Consultations among stakeholders about the concept and the process and building
consensus on the zonal centresiii. Zoning of whole district into CHPS zones
iv. Prioritising zones for implementation based degree of need for proivding access to healthservices, commitment of the communities int he zones and availability of resources
Operational(Implementation) planning. This begins when it district has decided to establish a
particular demarcated CHPS zone.
The phase involves:
i. Community entry to further introduce the concept to all communities in the zones. It
involves conducting several meetings with the leadership and the communities of each of the different communities that consitute the zone.
ii. Training and preparing the CHO to take the job
iii. Formation of a representative zonal health committeeiv. Construction or finding a suitable accommodation for the CHO(s)
v. Conducting the community profile. It involves community mapping, house to houseregistration of population and collection of other household data, records review,
interviews of key people in the community, etc.
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 2/16
vi. Mobilising resources ± vii. Selection and training of health volunteers. Suitable existing volunteers may presented to
the community for endorsement or otherwise.viii. Launching the CHPS zone ± usually a big durbar attended by all the communities under
the zone, health committee members, volunteers, TBAs,DHMT, SDHT, district
assembly, other stakeholders.Main aim of this grand durbar are to: Introduce the CHO, health committee members and the volunteers and to indicate
the team are to start performing their duties fully. The calrification of the roles of the various stakeholders: CHO, health committee
members, volunteers, community members, sub-district health team, DHMT andthe district assembly.
K ey issues to discuss are the security of the CHO and the mechanisms, includingthe mode of financing, for referral and transportation of emergencies to the health
centre or hospital.
What is the implication of CHPS as a PROCESS?
It means the critical steps must be followed to install the CHPS. These are making the
communities to understand the concept and play their part; and the CHO well trained in the
process and carrying out the key activities that different CHPS from the ways they were
accustomed to.
POLICY ± It is a stated government policy as an integral part of the health system orgnaisation
in the country.
The stated CHPS policy goal is to improve health status of people living in Ghana by
empowering households & communities to produce good health for wealth creation.
The Policy objectives are:
i. Improve Access to health servicesii. Improve Efficiency and Responsiveness to client needs
What is the implication of CHPS as a POLICY?
Whait it means is that it district health managers or staff have not the option not to implement
CHPS. It is mandatory for district managers led by the district director of helth services to
explain the policy to all their staff and ensure its implementation.
STRATEGY ± It a unique way of organising and providing health care. It recognises the unique
resources available in communities and their role in promoting good health and participating in
the delivery of health care. It recognises the importance of health personnel living within
communities their unique leadership and empowering role.
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 3/16
CHPS encourages all stakeholders to work together to empower & make health services
accessible to households through participatory planning, resources mobilisation, implementation,
monitoring & evaluation of service delivery.
The strategic focus of CHPS Implementation:
Building partnerships & collaboration among govt agencies, development partners &
NGOs for synergy
Directing all efforts towards empowerment of households & communities for good health
& wealth creation by thier active participation.
What is the implication of CHPS as a STRATEGY?
CHPS as a strategy means that it need to be implemented as its designed to have the desired
effect. It is not the usual thing. It is doing things differently from what we were doning before.
PART TWO
Operationalisation of a CHPS Zone
The following a re CRTICAL STEPS in CHPS implementation once a Zone has been selected
for operationalisation:
i. Community entry (module 14)
ii. Establishment of CHPS zone health Committee
iii. Training of a CHO(s) for the zoneiv. Production of community profile (module 14)
v. Provision of living accommodation and working unit for the CHO
vi. Launching of CHPS zone.
Community entry involves:
1. Recognizing the community, its leadership & people: Identify community leaders and
contact persons and hold meetings to understand their problems, and the place of health in
their prioritisation.
2. Learning from the community in order to adopt the most appropriate processes to interact
and work with community members
3. Introducing the CHPS concept, its relevance and importance, and actions necessary to
realise better health for the people. This should involve the leadership of all the
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 4/16
communities under the zone. Separate meetings may be held first then followed by a
meeting with representatives from all the communities to decide on the critical issues of
zonal centre, how to provide the CHPS compound and the formation of the community
health committee.
Establishment of CHPS zone health Committee
The CHPS zone health committee, often called community health Committee (CHC), is an
important structure that must be put in place once the people in the zone support the
establishment of the CHPS zone.
Their roles are:
1. To act as the immediate liaison with Ghana Health Service through the CHO and2. Mobilisation of the people for the CHPS activities for their active participation in health
matters.
Their duties include the following:
1. Initially they mobilise the community and resources for the CHPS compound construction.2. They develop and ensure the implementation of community health plans to address
community health problems that require community action.3. They monitor the activities of the community volunteers.
4. They monitor the activities of the CHO.5. The monitor the security siutation of the CHO.
Production of community profile
This provide the necessary information for proper planning and working with the people. It starts
with the community entry when the your gather information about the communities and the
people.
Community mapping by walking through the communities in the zone and drawing a map of the
zone showing important landmarks, facilities, etc, is an important part of developing the profile.
The actual community profile activity involves the house to house visits to interview and record
all information on population demographics, available resources, economic and socio-cultural
elements. This provides the information for the community register which needs to regularly
updated as the CHO begins having the cyclical house to hosue visits.
Launching of CHPS zone.
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 5/16
Launching of the CHPS zone in the form of a community durbar invloving the whole population
of the zone¶s area is a critical acitivity that must always be carried out to mproperly usher in
CHPS to a community. The objectives of the launching are as follows:
1. To announce to the population of the catchment area about the commencement of activity
service delivery by the CHO and the volunteers2. To introduce the CHO, the volunteers and community health committee members.
3. To spell out the duties of the key stakeholders: community members, community healthcommittee, volunteers, community health officer, district assembly and its substructures,
Ghana Health Servcies at sub-district and district levels, etc.4. To spell out the types of services that can be provided by the CHO5. To start the process of establisning the community mechanism of referrals and how they
can be transported to the appropriate level.6. To acknowledge the contributions of other stakeholders for their contribution to the
establishment of the zone (e.g. NGOs, prominent natives from the area).
There is often merry making because it is the culmination of the tedious processes of moilsing
the community, resources and preparing the ground for the full operation of the zone.
However, the merry making should not be allowed to overshadow the objectives outlined
above. Usually the district political and zonal traditional and religious leardership are invited
and commencement may be delayed because of the numerous schedules of these busy people.
It is thereforoe often necessary for the DHMT to esnure that the some of the above objectives
are addressed by engaging the crowd in discussions about the issues before the formally
opening begins.
A Functional CHPS Zone
A CHPS zone is described as functional when he satisfies all the following criteria:
1. The availability of an annually updated CHPS zone profile and community registers;
2. There is a functioning CHPS zone Community Health Committee (CHC); and3. There is a trained and functional community health officer (CHO) responsible for the
zone.
1. The availability of an annually updated CHPS zone profile and community registers
The following information is available at the zonal office:
i. Zonal profile document with the following information: communities, demographic,
infrastructure, social, economic, religious, resources, communication, health problems, etcii. Map of the zone in relation to other CHPS zones
iii. Evidence of annual updating of profile, especially demographic data
2. There is a functioning CHPS zone Community Health Committee (CHC)
i. There is a list of membership of CHC representing the cross-section of the communitiesconstituting the zone;
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 6/16
ii. The CHC meets monthly or at least quarterly with evidence of minutes kept at zonaloffice; and
iii. There exists a current CHC work plan.
3. There is a trained and functional community health officer (CHO) responsible for
the zone.
i. The nurse has received the CHO trainingii. The CHO has been officially introduced to the all zone population in a public durbar iii. The CHO conducts:
Regular house to house visits for health promotion activities Hold monthly or at least quarterly community health durbars
These are the minimum standards for a CHPS zone to qualify to be designated a functional zone.
Please, note that the CHO reports should include these indicator activities.Any of these criteria if
not verifiable disqualifies the zone as functional.
Role of Community in CHPS
1. Provide CHPS compound, if capable, or assist in the construction.
2. Assist in the maintenance of the CHPS compound3. Provide security for CHO and the CHPS compound
4. Participate in the planning, organisation and delivery of health services
Role of the District Assembly
1. Assist communities that cannot provide CHPS compounds to construct and maintainCHPS compounds
2. Provide utility services such as safe water and electricity to the compound3. Assist in providing security to the CHPS compound and the CHO
4. Support to maintian the volunteer system5. Mobilise other resources to support CHPS activities
6. Monitor the CHPS implementation in the district.
Role of District and Regional HealthManagement Teams (DHMT/RHMT)
1. Plan and coordinate CHPS implementation
2. Carry out advocacy and community mobilisation for CHPS
3. Mobilise resources for CHPS implementation
4. Provide training and technical support to CHOs & SDHTs
5. Monitor, supervise and evaluate the implementation
Role of Sub-district Health Teams (SDHTs)
1. Participate in the planning and establishment of CHPS zones in sub-district
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 7/16
2. Mobilise communties for CHPS
3. Provide logistics support to CHOs
4. Supervise of CHOs
5. Provide technical support to CHOs
6. Monitor CHPS activities in the zones
Roles of the Community Health Officer (CHO)
The CHO plays three key roles: as aprimary healthcare service provider,community health
change agent and community health manager.
As health professional with primary healthcare service provider function. ± He/she provide
treatment for minor ailments, providing preventive and health promotion services, including
reproductive and child health and disease control, to households and communities.
As community health change agent ± He/she works with communities and households to
identify their health problems and find solutions for them. Through mutual learning households
are empowered in health matters, and the CHO¶s professional competencies, leadership and
social skills are further enhanced.
As a community health manager -
He/she lead in the planning of community health activities and manage the CHOactivities ± priroty setting, planning weekly, monthly iterineraries, implementation,
monitoring and evaluation (Module 1) He/she manages resources made available to him/her for health in the community. These
resources include, transport, equipment, transport, medicines, other logistics and time.
The Different Options for Training and Development of the Community
HealthOfficer (CHO)
1. Two weeks orientation training on core functions/duties prior to placement
This is mandatory before a CHN is assigned to a CHPS zone. The health worker is taken
through the two weeks core orientation training.
In some cases after this traing it may be necessary to also attach the person to a more
experienced CHO for some period before final placement.
2. Attachment to acquire adequate midwifery skills preferably in district hospital ( 2-3
months)
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 8/16
In a CHPS zone where there is no health facility with delivery services, that CHO should receive
some additional midwifery skills training, preferably 2 -3 months attachment in a hospital.
Periodic attachments and supervision is very important to build their skills and confidence.
3. Training on IMCI ± clinical & C-IMCI
All CHOs should be given the community IMCI training to enable them supervise volunteers.
Those CHOs who are required to treat minor ailments should be given clinical IMCI trainingis as
well.
4. HIV/AIDS counselling & testing training, including PMTCT
Now that PMTCT is to be implemented at all ANC service delivery points using the opt out
strategy, it goes without saying that the ANC module in the two weeks CHOs orientation course
should be updated to include PMTCT. The CHO may also be given the repscribed PMTCT
training.
DDHS should plan for CHOs to undergo HIV/AIDS counselling training to enhance their
counselling skills. Attachment to experienced counselling during counselling sessions should
also be promoted.
5. Family Planning counselling training
The provision of family planning services is an important activity of the CHO hence DDHS
should plan and organise family planning counselling training workshops for all CHOs
6. Adolescent sexual & reproductive health training
Adolescents are important segment of the population and CHOs should be trained on adolescent
health policy and service delivery and the reproductive health protocols.
7. IEC & Behaviour Change Communication(BCC) training
The work of the CHOs mainly hinges on IEC and BCC hence the need for them to acquire these
skills. They is therefore the need to take them through regular IEC and BCC training workshops
8. Working with Communities and social groups
CHOs skills in working with communities and social groups should be built through workshops
and seminars
9. Regular In-service training & updates on new services/new knowledge.
CHOs should be seen as key service providers who should be targeted whenever new service
areas are introduced or change of policy are made.
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 9/16
10. Regular CHO review meetings
The DDHS should organise monthly or quarterly meetings for CHOs to meet and share their
experiences and learn from each other. It is important for SDHT and DHMTs to participate in
these meetings to follow the CHPS implementation and address any misunderstanding and problems that they may have.
During these meeting each CHO should present their performance according to a format
developed by the DDHS, followed by questions and discussions. The meeting should end with
plans to address problems identified and spelling out actions to be carried at each level.
Critical Success Factors of CHPS Implementation -These elements should therefore be given greater
attention.
1. Well informed, dedicated and resource district director of health services who believes in the concept.
2. Effective supervisory support from DHMT to sub-districts and to CHPS zones.3. Early involvement of the communities in the CHPS process.4. Active CHPS zone health committee.
Challenges to CHPS Implementation
1. The concept of CHPS not understood by some stakeholders. This is not limited to
community members alone. Some health professional are themsleves ignorant and some
some extent sceptical. Everybody needs to try to understand the concept and how it can be
operationalsied to bring health benefits to households and communities, especially rural
and deprived communities.
2. Lack of suitable CHPS compounds. Many communities cannot provide CHPS compounds.
Some CHPS compounds that are constructed are without essential utilities such as safe
water, electricity and toilet facilities. Some structures have no living accommodation for
the CHO
3. Inadequate funds for CHPS activities ± for equipment, transport and recurrent activities.
Many CHPS zones are without the necessary equipment. Funding for the training of CHOs,CHCs and volunteers, and for social mobilisation and community durbars are insufficient.
4. Many CHOs do not ride motor bikes provided.
5. Weak supervision of CHPS implementation. DHMTs and sub-districts ar enot supervising
and monitoring the activities of the CHOs. Such CHOs are not motivated to stay at their
zones, hence numerous complains from community members from such zones.
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 10/16
PART THREE
Operations of the CHO
CHO Activities
Arising from the the three roles above the CHO is expected to carry out activities that fall under
the following broad areas:
A. Provide reproductive and child health (MCH) services
B. Carry disease surveillance and control activities
C. Manage minor ailments & referrals
D. Carry out social mobilisation and advocacy for health promotion and nutrition activities
E. Manage health programmes and resources
A. Providing Reproductive and child health (MCH) services including antenatal care,conducting deliveries, postnatal care, family planning counseling and services, EPI, growth
monitoring and promotion, etc
i. Provision of EPI services
ii. Provide ante-natal and post-natal care
iii. Family Planning services & counselling
iv. Distribution of Condoms & non-injectable FP
v. Counselling & BCC on STIs
vi. Carry out growth monitoring and promotion for under-five children
vii. Provide School health services to Day nurseries and schools in the catchment area with
assistance from the sub-district
viii. Promote regenerative health and nutrition among all age groups.
B. Carry out disease surveillance and control activities in the catchment area by:
i. Compiling and submitting communicable disease Form CD1 to the sub-district
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 11/16
ii. Investigating and reporting to the district on unusual events reported from thecommunities
iii. Notifying the district immediately of any disease outbreak iv. Ensure the implementation of community based disease control activities such:
y
ITN distribution and use
y Community Directed Treatment- filariasis, Vit A, deworming, etc
y Community based DOTS for Tuberculosis treatment
y Water and sanitation programmes
C. Treament of minor ailments/injuries
i. Treatment of uncomplicated malaria and fevers
ii. Treatment of simple cough and URTIs
iii. Treatment of simple diarrhoea
iv. First Aid for Burns, cuts, other home accidents
v. Blood pressure monitoring
vi. First Aid for spontaneous delivery
vii. Referral of all conditions beyond the scope of authority
D. Carry out social mobilisation and advocacy for health promotion and nutrition activities1. Home visits
They conduct house to house visits (routine home visits) ± regularly carried in a cycle of
monthly, every two months or quarterly. The purpose is inspection, understanding household
problems and assisting family members to solve them through counseling and health
education.They also conduct special home visits for specific purposes such as:
i. Follow up of malnourished children, PLWHA, TB patients, etcii. Tracing of defaulters in receiving services e.g. EPI, ANC, TB, Family Planning,
etciii. Home Based Care e.g. postnatal care at home, home delivery, DOTs, chronic
illness, etc.2. Holding of community health durbars.
3. Mobilising communities for health actions4. Holding health education sessions for target social groups
5. Provide support for community based volunteer workers:i. Participate in the selection and training of TBAs, CBDs, CBS volunteers, etc
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 12/16
ii. Monitor and supervise volunteersiii. Hold regular review meetings with volunteers
iv. Ensure volunteers¶ supplies are regularly replenished.E. Manage health programmes and resources
1. Develop annual plans; and draw weekly and monthly work itineraries
2. Manage resources provided to the CHPS zone for work.3. Participate in zonal health committee meetings and guide them in planning andimplementation of their activities
i. Participate in the following sub-district and district activities:ii. Planning and conduct of mop up exercises
iii. In-service trainingiv. Review meetings
v. Special celebrations and campaigns e.g. Malaria month, National NINs, SIAs, childhealth promotion week, integrated maternal and child health campaign, etc
4. Collaborate with TBAs and chemical sellers operating in the CHPS zone.5. Write reports on acitivities carried out
6. Compile and submit service reports to sub-district.
Conducting House to House Visits
Organising Community Health Durbars
Empowering Social Groups
CHPS Information System
CHO
Records
1. CHPS zone profile file
2. CHC membership3. CHC plans
4. Minutes of CHC Meetings5. CHO Monthly itinerary file
6. CHO Annual workplans file7. CHO monthly reports file
8. CHO Activity reports file
Sub-district level
1. File for information on each CHPS zone, which should include the following:i. Zone profile
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 13/16
ii. CHC membershipiii. CHC plans
iv. Minutes of CHC Meetingsv. CHO Monthly itinerary file
vi. CHO Annual workplans file
vii. CHO monthly reports fileviii. CHO Activity reports file
2.
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 14/16
IMPORTANT ANNEX INFORMATION
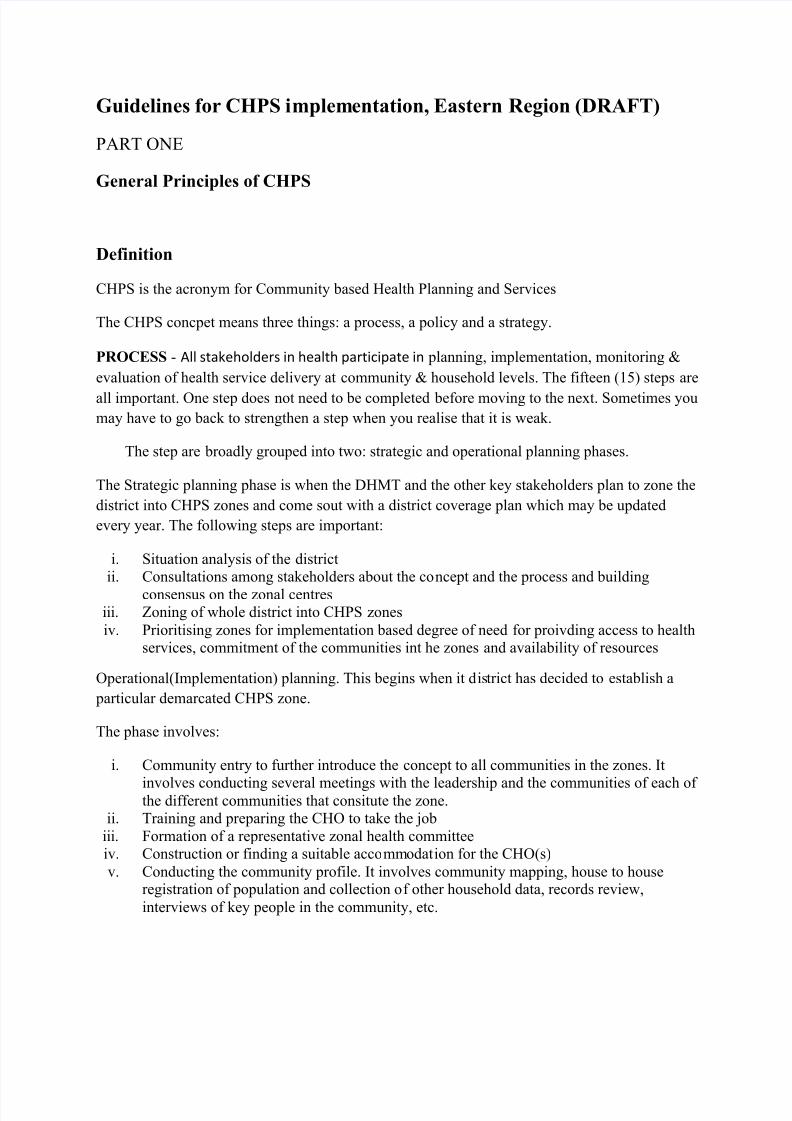
Fig 1: Focus of CHPS Strategy
¡ ¢
£ ¤ h¡
¥ ¦ £
¡ ¢
£ ¤ h¡
¥ ¦ £
§ ¡ ̈
¤ © ¤
§ ¡ ̈ ¤ ©
¤
¡ ¢
¤ £
¡
¢ ¤
£
!
"
#
$
%
&
%
' (
F $ ) 0
CHPS targets the households who arethe primary producers of health
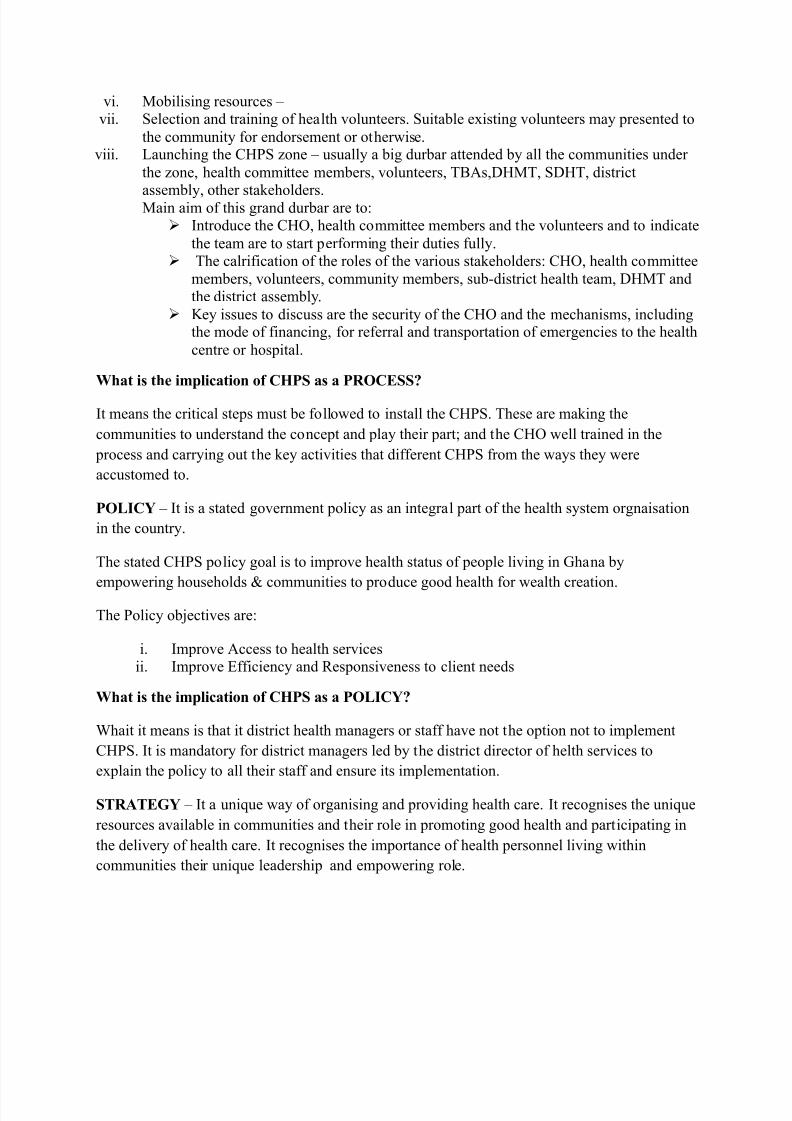
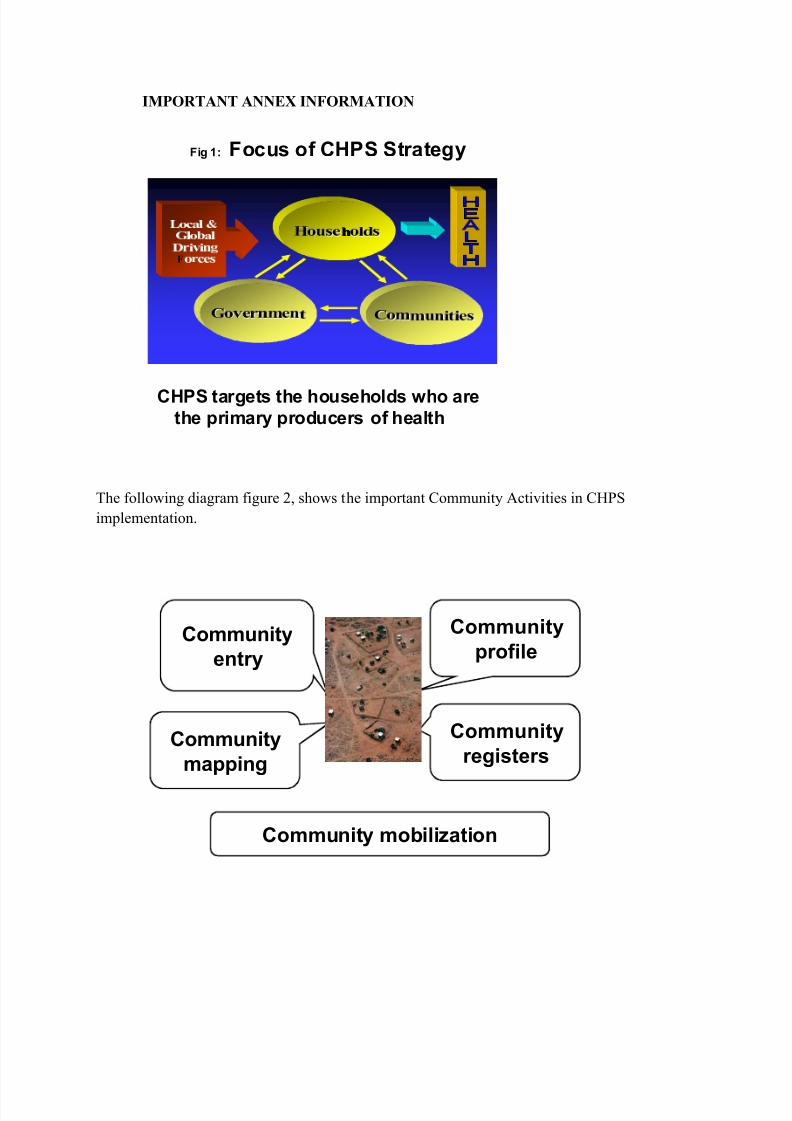
The following diagram figure 2, shows the important Community Activities in CHPS
implementation.
Community
entry
Community
mapping
Community
registers
Community
profile
Community mobilization
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 15/16
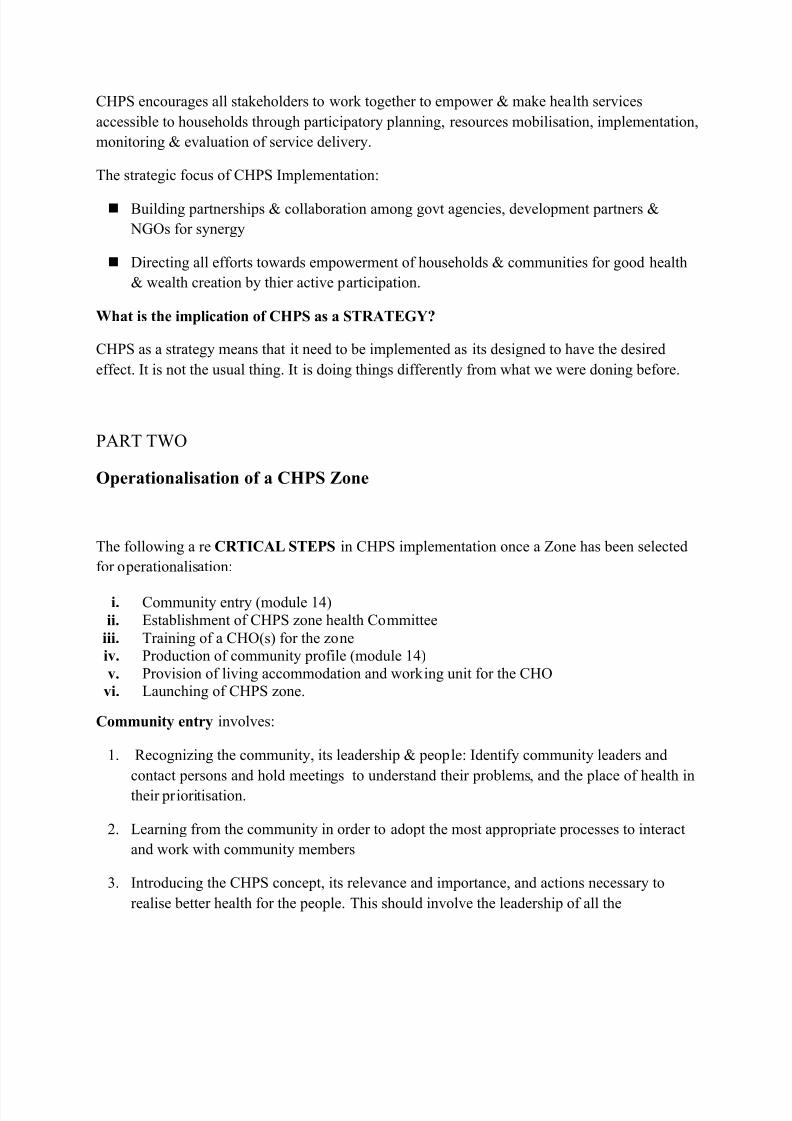
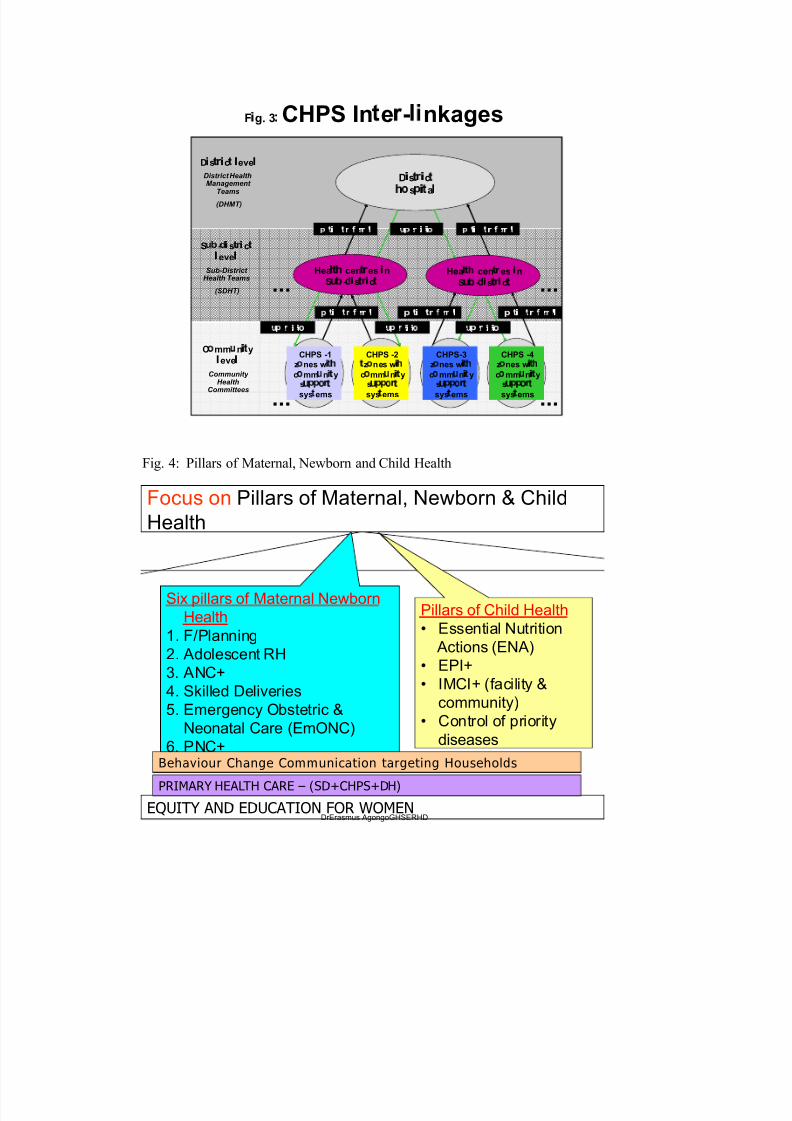
F 1 g. 3 2 CHPS In e - nkages
D3 s4 5 3
c 4 6 eve 6
District HealthManagement
Teams
(DHMT)
C7 mm 8 n3 4
y
6 eve 6
Community Health
Committees
S 8 9 - @ 3 s 4 5 3 c 4
6 eve 6
Sub-District Health Teams
(SDHT) ...
...
...
...
D A sB
C A cB
D
E
s F A
B
a G
s H I e P v Q s Q
R
n
sH I
e P v Q s Q
R
n
Hea6 4 S
cen4 5
es 3 n
S8 9
-@ 3
s4 5 3
c 4
CHPS -2T
zU
nes wV W
cU
mmX
nV T
ys
X Y Y U `
T
sysT
ems
CHPS -1z
U
nes wV T W
cU
mmX
nV T
ys
X Y Y U `
T
sysT
ems
Hea6 4 S
cen4 5
es 3 n
S8 9
-@ 3
s4 5 3
c 4
CHPS-3z
U
nes wV T W
cU
mmX
nV T
ys
X Y Y U `
T
sysT
ems
CHPS -4z
U
nes wV T W
cU
mmX
nV T
ys
X Y Y U `
T
sysT
ems
sH I
e P v Q s Q
R
n
I aa
Q ena
P eb
e P P a c I aa
Q ena
P eb
e P P a c
sH I
e P v Q s Q
R
n
I aa
Q ena
P eb
e P P a c I aa
Q ena
P eb
e P P a c I aa
Q ena
P eb
e P P a c
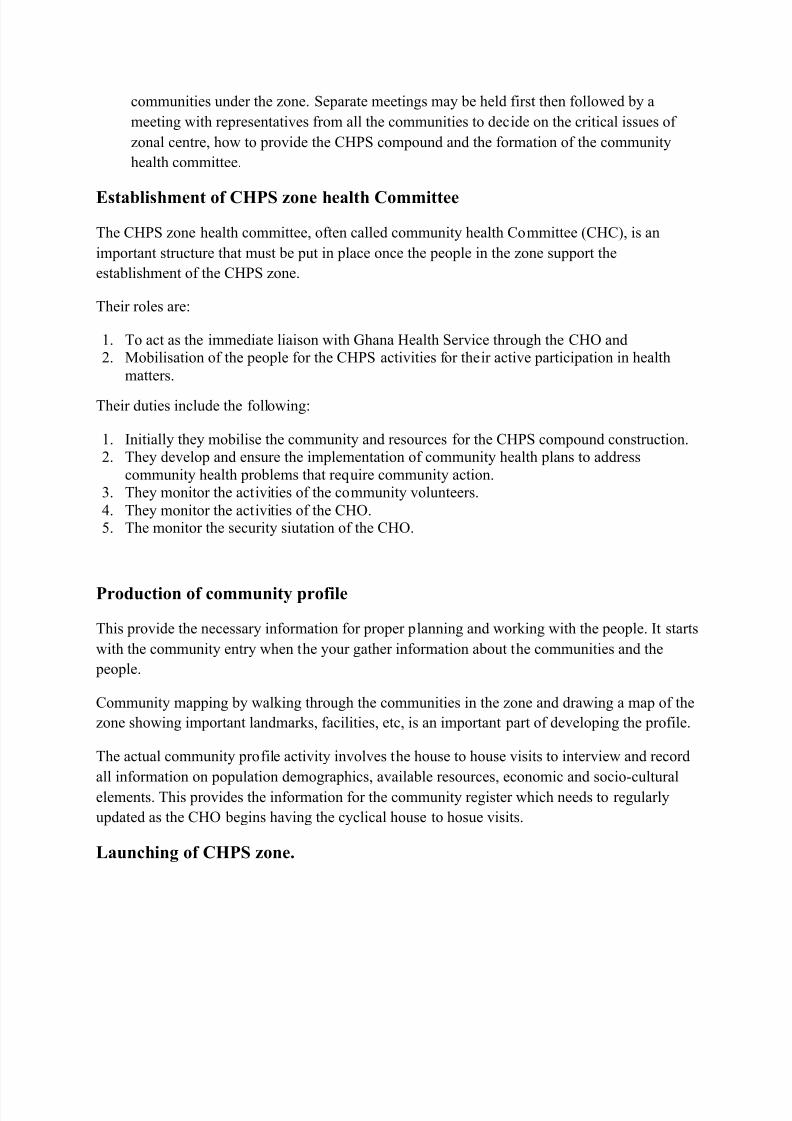
Fig. 4: Pillars of Maternal, Newborn and Child Health
Focus on Pillars of Maternal, Newborn & Child
Health
EQUITY AND EDUCATION FOR WOMEN
Behaviour Change Communication targeting Households
PRIMARY HEALTH CARE (SD+CHPS+DH)
Pillars of Child Health
Essential Nutrition
Actions (ENA)
EPI+
IMCI+ (facility &
community)
Control of priority
diseases
Six pillars of Maternal Newborn
Health
1. F/Planning
2. Adolescent RH
3. ANC+
4. Skilled Deliveries
5. Emergency Obstetric &
Neonatal Care (EmONC)
6. PNC+
DrErasmus AgongoGHSERHD
8/8/2019 Guidelines for CHPS Implementation
http://slidepdf.com/reader/full/guidelines-for-chps-implementation 16/16
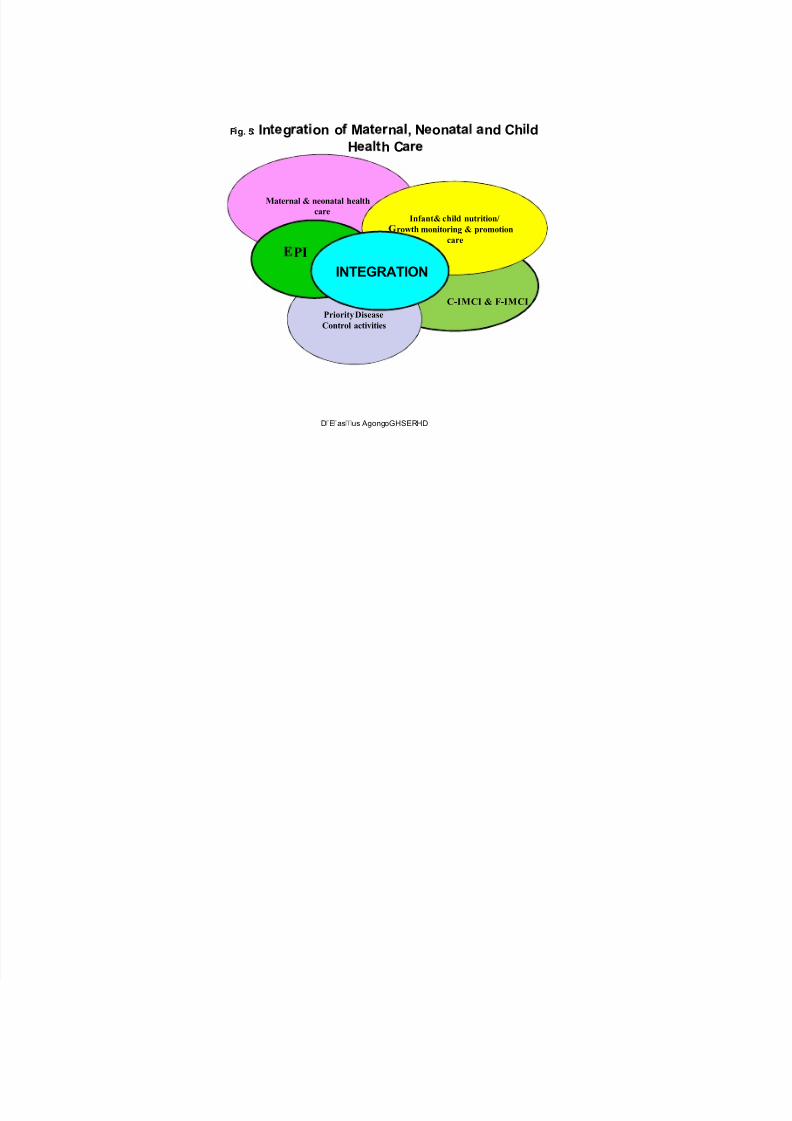
F d g. 5e In g on o M n , N on nd Ch d
H h C
Maternal & neonatal health
care
C-IMCI & F-IMCI
Priority Disease
Control activities
Infant& child nutrition/
f rowthmonitoring & promotion
care
PI
INTEGRATION
Dg
Eg
ash
us AgongoGHSERHD























![[Chps] best practices_manual__vol.vi_high_perform(book_fi.org)](https://img.pdfslide.us/doc/110x75/55c3fb68bb61eb6f198b45ef/chps-best-practicesmanualvolvihighperformbookfiorg.jpg)



