Embed Size (px)
Citation preview

Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 1 of 13
Guideline Title Emergency Resternotomy in ICU Summary1: This guideline outlines the process for managing patients who require emergency resternotomy in ICU. The key to the successful resuscitation of cardiac arrest in these patients is the need to perform emergency resternotomy early, especially in the context of tamponade or haemorrhage, where external chest compressions may be ineffective.
Approved by: ICU Medical Director
Publication (Issue) Date: September 2014 Next Review Date: September 2017 Replaces Existing Guideline: Emergency chest re-opening in ICU_ 2011 Previous Review Dates: 2006, 2011
1. Background Information4:
Patients returning to ICU post cardiac surgery are at increased risk of arrhythmias, acute cardiac tamponade, haemorrhage, and coronary artery spasm in the first 24 hours which in turn can lead to clinical haemodynamic instability. Cardiac arrest following cardiac surgery can occur in the immediate post-operative phase. The specific causes of cardiac arrest, such as tamponade, hypovolaemia, myocardial ischaemia, tension pneumothorax, or pacing failure are all potentially reversible. The key to the successful resuscitation of cardiac arrest in these patients is the need to perform emergency resternotomy early, especially in the context of tamponade or haemorrhage, where external chest compressions may be ineffective.
2. Introduction: The risk addressed by this policy:
Patient Safety
The Aims / Expected Outcome of this policy:
Staff caring for patients who require emergency resternotomy in ICU will have the knowledge and skills to respond in a timely manner, activate CTOT and manage and stabilise the patient appropriately.
Related Standards or Legislation
NSQHS Standard 1 Governance Related Policies
LH_PD_2011 Management of Arrhythmias
LH_GL2013 CTOT (Cardiothoracic Operating Theatre Team) Activation
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 2 of 13
3. Policy Statement: All care provided within Liverpool Hospital will be in accordance with infection
prevention/control, manual handling and minimisation and management of aggression guidelines.
Once the decision is made to open the chest a CTOT needs to be activated by dialing 666 and stating CTOT to ICU and bed number.
Advanced Life Support must be implemented if the patient has a life threatening arrhythmia.
The chest reopening and emergency arrest trolleys must be taken to the bed area Staff must be allocated specific roles (at the start of the shift staff in the ICU are
allocated roles in case of potential emergency resternotomy). Staff involved in the management must wear appropriate PPE -eye protection, mask,
gown and gloves at all times Any sponges or gauze used in the procedure must be x-ray detectable, counted and
recorded on OT count sheet There must be two high suction outlets with canisters and tubing in bed area.
4. Principles / Guidelines
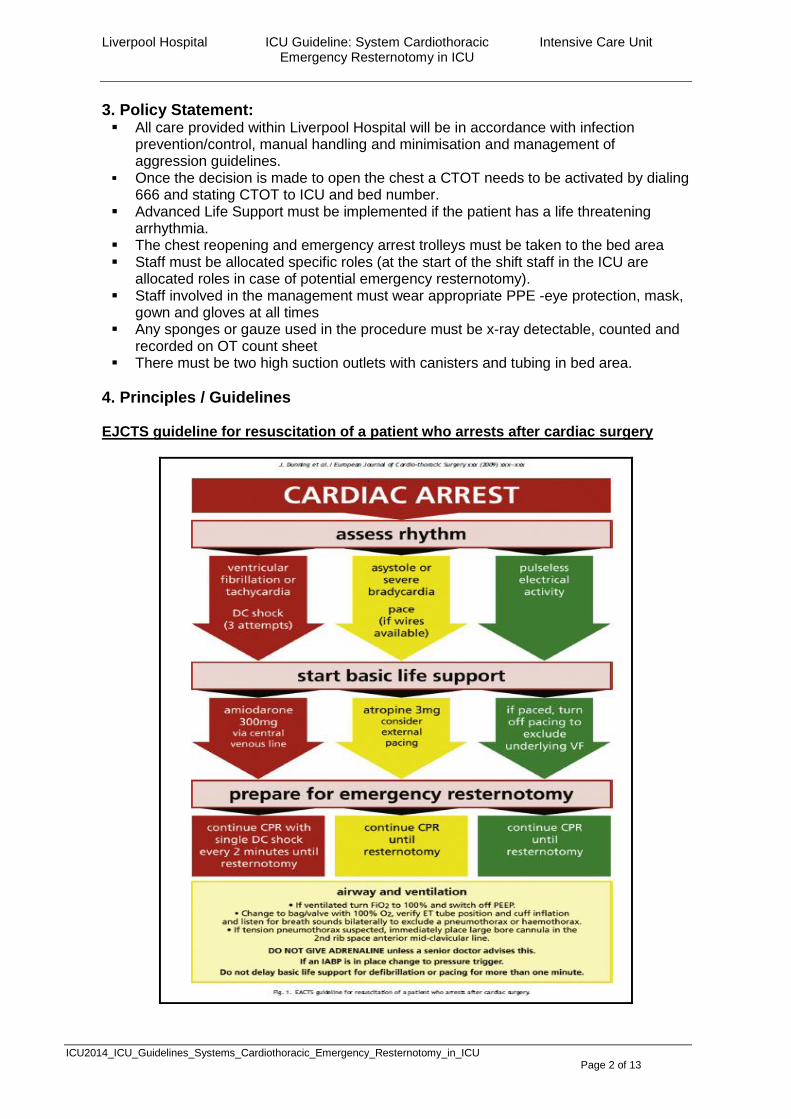
EJCTS guideline for resuscitation of a patient who arrests after cardiac surgery

Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 3 of 13
Patients who arrest post cardiac surgery will require immediate CPR as per the ALS guidelines. CPR procedure will vary depending if the patient has a closed or open sternum (refer to the process below).
Shockable rhythms will also require immediate defibrillation. A CTOT should be activated by dialing 666.
CPR on a post – op cardiothoracic patient with a closed sternum1,2,3 Activate CTOT by dialing 666. In the post cardiac surgery ICU, a witnessed and monitored VF/VT arrest should be
treated immediately with 3 quick successive stacked defibrillation attempts1 Three failed defibrillations should trigger the need for emergency resternotomy Commence Cardiac compressions on patient with no output Sternotomy patients need less pressure to generate cardiac output and this should be
done gently using arterial pressure trace as a guide. Adrenaline 1mg should be administered if no output. If patient has an output Adrenaline
should be administered cautiously 100mcg-200mcg IV after the 2nd defibrillation Amiodarone 300mg given after 3rd defibrillation See management of Arrhythmias Guideline for detailed management of arrhythmias. CPR on Post op Cardiothoracic patient with an Open Sternotomy 1, 2, 3
Activate CTOT by dialing 666. In the post cardiac surgery ICU, a witnessed and monitored VF/VT arrest should be
treated immediately with 3 quick successive stacked defibrillation attempts1 Adrenaline 1mg should be administered if no output. If patient has an output Adrenaline
should be administered cautiously 100mcg-200mcg IV after the 2nd defibrillation Amiodarone 300mg given after 3rd defibrillation Prepare patient and equipment for Medical staff to open sternal wound dressing Internal cardiac massage should only be delivered with a two- hand (‘clapping”)
technique The wrists of the Medical Officer are placed together at the apex of the heart, and the
heart is squeezed together between the two open palms in a rhythmic motion. The thumb of each hand is maintained adjacent the first finger to avoid inadvertently pushing them into the heart. (See Figure 1 below)
Internal cardiac defibrillation is performed with the defibrillator initially set at 20joules, using the internal defibrillation paddles.
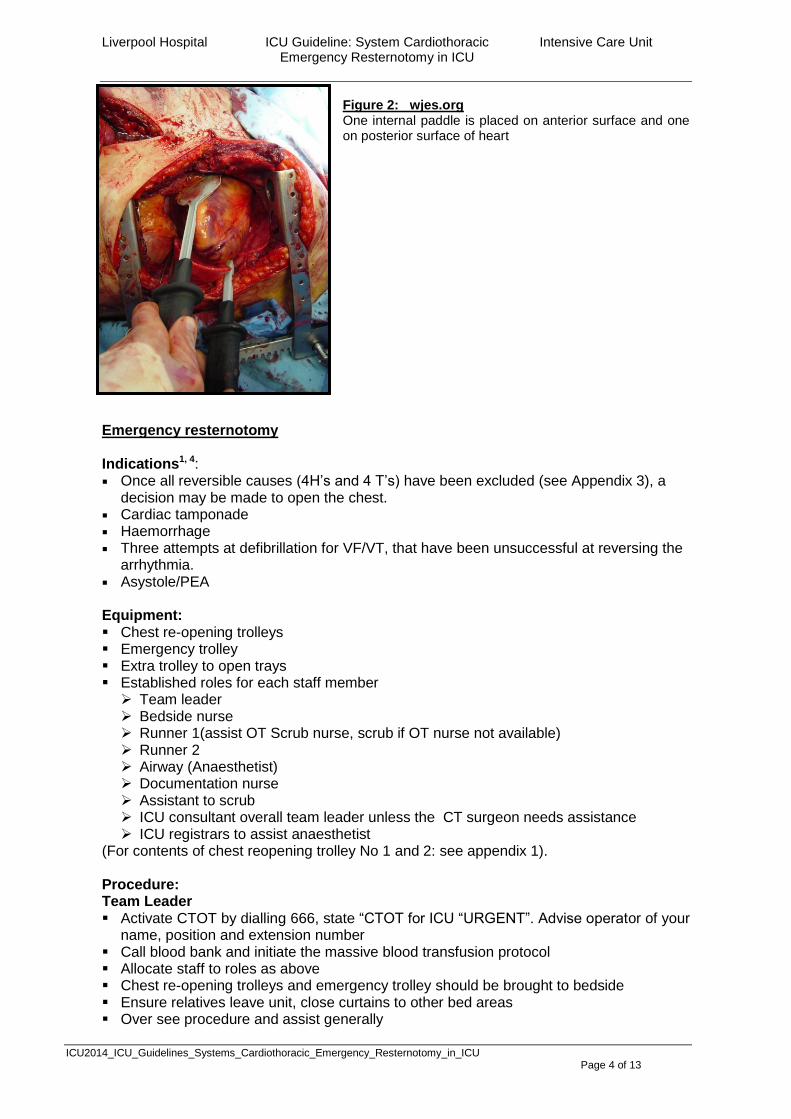
Repeat defibrillation is performed, as needed, at 20 to 50 joules. One of the internal paddles is placed on the anterior (ventral) surface of the heart and
the other is placed on the posterior (dorsal) surface of the heart. See Figure 2 As with external defibrillation, all personnel should be well away from the patient prior to
defibrillation to prevent inadvertent electric shock and avoid blood splatter Continue as per ARC guidelines until Cardiothoracic team arrive
Figure 1: Open chest cardiac massage is performed with the heart compressed between the palms of both hands. Cardiac compression with one hand should be avoided because the pulmonary outflow tract is vulnerable to penetration by the thumb uptodate 2013
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 4 of 13
Figure 2: wjes.org One internal paddle is placed on anterior surface and one on posterior surface of heart
Emergency resternotomy Indications1, 4: Once all reversible causes (4H’s and 4 T’s) have been excluded (see Appendix 3), a
decision may be made to open the chest. Cardiac tamponade Haemorrhage Three attempts at defibrillation for VF/VT, that have been unsuccessful at reversing the
arrhythmia. Asystole/PEA Equipment: Chest re-opening trolleys Emergency trolley Extra trolley to open trays Established roles for each staff member Team leader Bedside nurse Runner 1(assist OT Scrub nurse, scrub if OT nurse not available) Runner 2 Airway (Anaesthetist) Documentation nurse Assistant to scrub ICU consultant overall team leader unless the CT surgeon needs assistance ICU registrars to assist anaesthetist
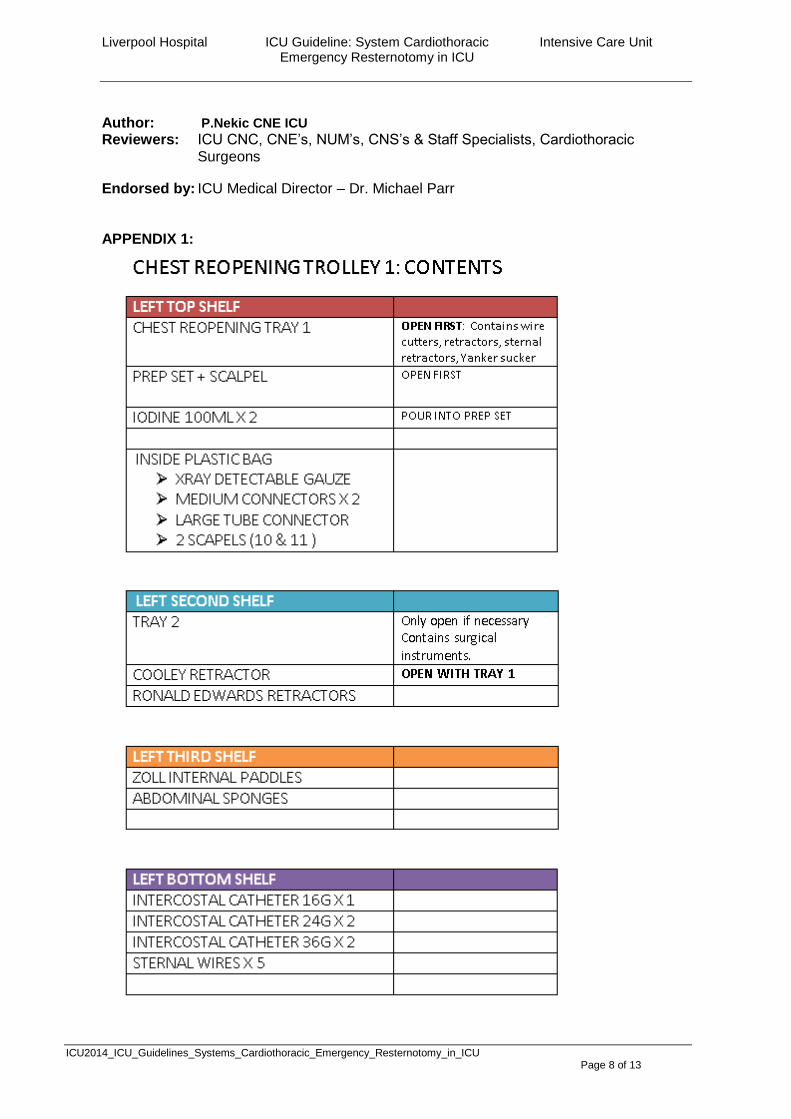
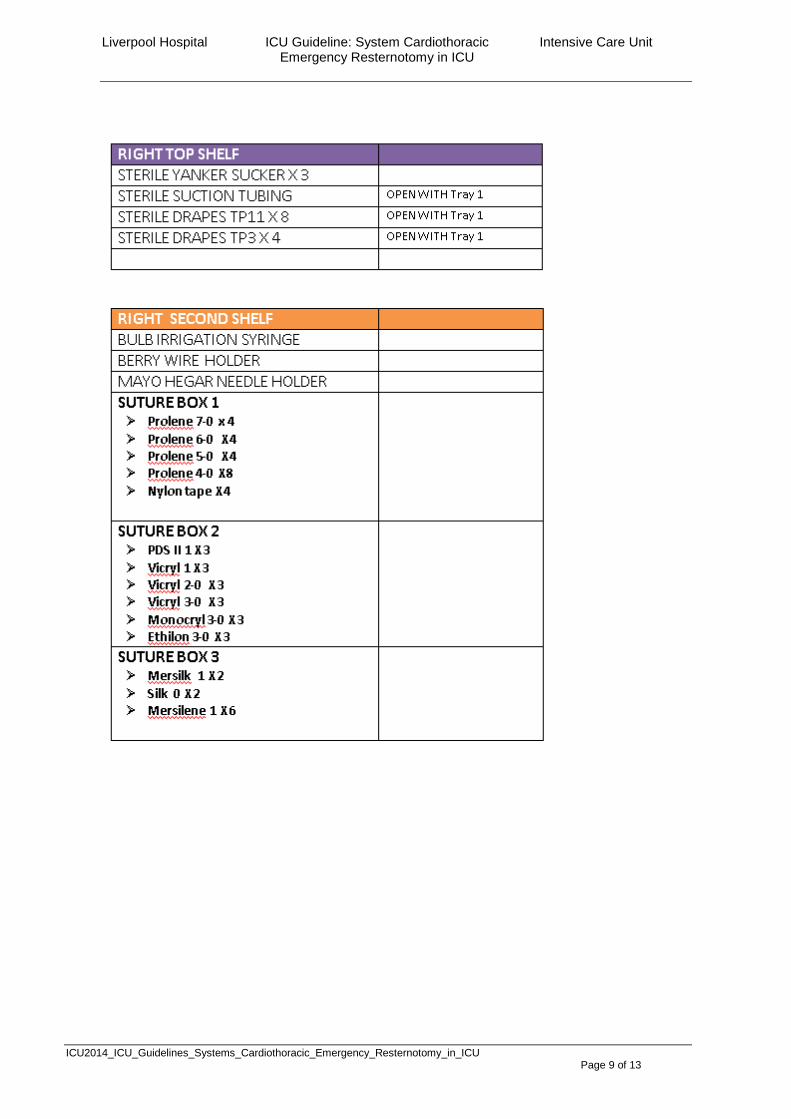
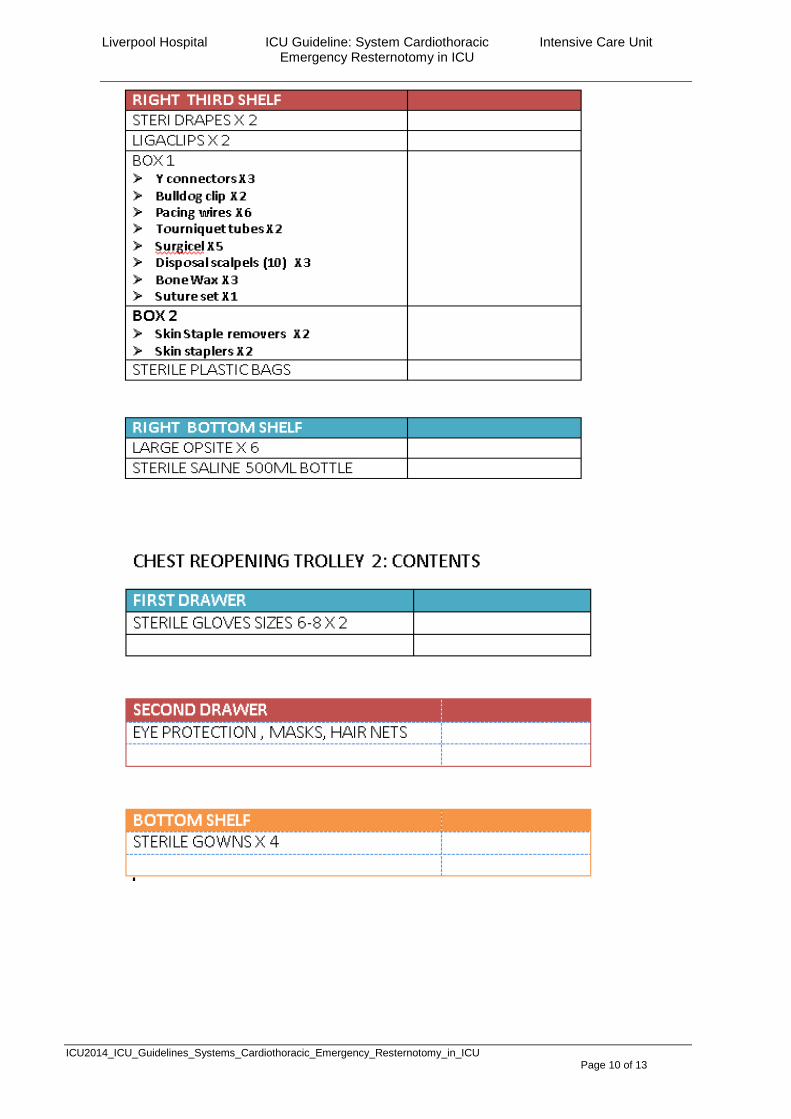
(For contents of chest reopening trolley No 1 and 2: see appendix 1). Procedure: Team Leader Activate CTOT by dialling 666, state “CTOT for ICU “URGENT”. Advise operator of your
name, position and extension number Call blood bank and initiate the massive blood transfusion protocol Allocate staff to roles as above Chest re-opening trolleys and emergency trolley should be brought to bedside Ensure relatives leave unit, close curtains to other bed areas Over see procedure and assist generally

Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 5 of 13
Bedside Nurse Stay with patient at all times Assist with ALS measures Put on gown gloves apron Prepare bed area Move bed for access Adjust bed height Ensure high suction x 2 is available Clear unnecessary equipment
Prepare patient Administer 100% Fi02 Position patient supine Remove sternal dressing Move ECG electrodes away from sternum Isolate lines for IV drugs, blood products, sedation Assist anaesthetist Maintain patient comfort and safety, observe for signs of pain, maintain sterile field.
Runner 1: scrub and gown if OT scrub nurse not in unit Stay close to bed area Identify to surgeon that you are Runner 1 and that you will be helping to open trays If OT scrub nurse not available set up as scrub nurse On spare sterile draped trolley, open gowns, gloves and drapes, scalpel, preparation
tray and pour in betadine. Open sterile suction tubing and yankuers Open chest opening tray number 1 (See Appendix 1) Open sterile gauze and ensure that they are counted and documented on count sheet Remaining equipment is opened as required Open chest tray number 2 only if necessary (see Appendix 1) Assist as required until patient is stabilised and /or returned to theatres Ensure chest reopening trays are returned to CSSD for cleaning Restock all trolleys Ensure relatives are informed of patients condition Runner 1: for patient with no cardiac output: If patient has no cardiac output and the chest reopening cannot wait for normal draping procedure as above, the procedure is: Dressing removed from chest and betadine poured over chest Knife to surgeon Drapes over top and bottom of wound while surgeon is cutting skin Sterile suction opened and connected Wire cutters to surgeon Retractors to surgeon Once patient is stable more drapes can be put over patient Runner 2 Obtain any equipment that is needed that is not in bed area e.g. balloon pump, blood
products, drugs, fluids Help prepare equipment Connects unsterile end of suction tubing to suction If OT staff unavailable step up to Runner 1 Documentation nurse All documentation Drugs, fluids, blood products OT count sheet
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 6 of 13
Once procedure is completed ensure correct documentation of drugs, gauzes and instruments is attended
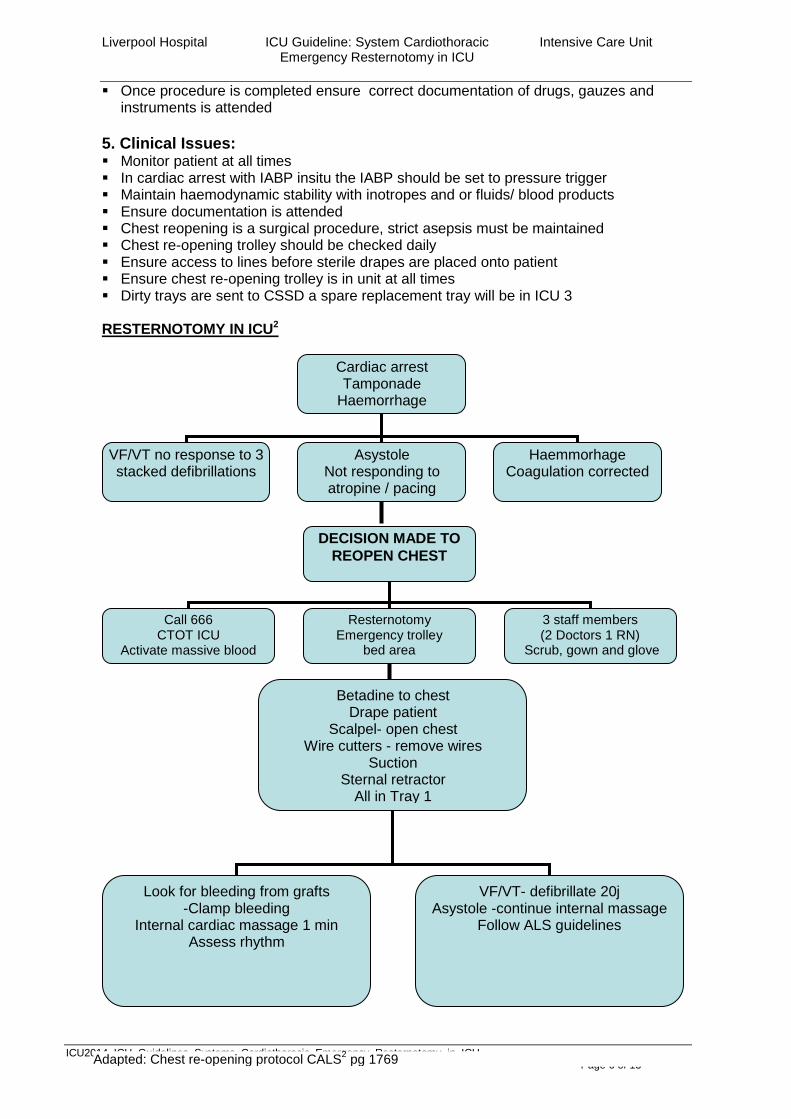
5. Clinical Issues: Monitor patient at all times In cardiac arrest with IABP insitu the IABP should be set to pressure trigger Maintain haemodynamic stability with inotropes and or fluids/ blood products Ensure documentation is attended Chest reopening is a surgical procedure, strict asepsis must be maintained Chest re-opening trolley should be checked daily Ensure access to lines before sterile drapes are placed onto patient Ensure chest re-opening trolley is in unit at all times Dirty trays are sent to CSSD a spare replacement tray will be in ICU 3 RESTERNOTOMY IN ICU2
Cardiac arrest Tamponade
Haemorrhage
VF/VT no response to 3 stacked defibrillations
Asystole Not responding to atropine / pacing
Haemmorhage Coagulation corrected
DECISION MADE TO
REOPEN CHEST
Call 666 CTOT ICU
Activate massive blood transfusion protocol
Resternotomy Emergency trolley
bed area
3 staff members (2 Doctors 1 RN)
Scrub, gown and glove
Betadine to chest Drape patient
Scalpel- open chest Wire cutters - remove wires
Suction Sternal retractor
All in Tray 1
Look for bleeding from grafts -Clamp bleeding
Internal cardiac massage 1 min Assess rhythm
VF/VT- defibrillate 20j Asystole -continue internal massage
Follow ALS guidelines
Adapted: Chest re-opening protocol CALS2 pg 1769
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 7 of 13
6. Performance Measures All incidents are documented using the hospital electronic reporting system: IIMS and managed appropriately by the NUM and staff as directed.
Definitions: Cardiac tamponade: is defined as the compression of all cardiac chambers due to increased pericardial or mediastinal pressure from fluid/blood. This limits the normal functioning of the heart and ventricular filling is disrupted. Clinical presentation: Decrease BP, elevation of diastolic pressures may causes a narrow pulse pressure Increased CVP, PAP, PAWP Tachycardia Sudden cessation of bleeding from chest drains when they were previously bleeding Widened mediastinum on CXR Chest pain Cyanosis Neck vein distention Haemorrhage Characterised by chest drain output of > 100mls /hour Causes Post bypass coagulopathies Graft rupture / leaking Inadequate heparin reversal Thrombolytic therapy, platelet inhibitors used for stenting Impaired platelet function Prolonged hypothermia Hypertension immediately post- op Loosening of clips or sutures Sites of bleeding IMAs, cannulation sites, vascular anatomises, pleural or pericardial fat Sternal wire sites, coronary veins, edge of pericardium Signs of bleeding Increase in drain output > 100ml/hr Tachycardia Hypotension Decrease cardiac output Decrease in filling pressures Widened mediastinum on CXR
7. References / Links 1. European Resuscitation Council guidelines 2010. J. Soar et al. / Resuscitation 81 (2010) 1417–
1418
2. The Cardiac Surgery Advanced Life Support Course (CALS): Delivering Significant Improvements in Emergency Cardiothoracic Care. Joel Dunning, PhD, Jay Nandi, MRCSEd, Sharil Ariffin, FRCA, John Jerstice, FRCA, Deborah Danitsch, MS, and Adrian Levine, FRCS. Ann Thorac Surg 2006; 81:1767–72) 2006 by The Society of Thoracic Surgeons
3. Guideline for resuscitation in cardiac arrest after cardiac surgery. Joel Dunning t al.European Journal Cardiothoracic Surgeons 2009. doi:10.1016/j.ejcts.2009.01.033
4. Cardiac Tamponade. Brian D Hoit, MD. uptodate 2014
5. Resuscitative thoracotomy: technique. uptodate2014
6. LH_GL2013 CTOT (Cardiothoracic Operating Theatre Team) Activation guideline
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 8 of 13
Author: P.Nekic CNE ICU Reviewers: ICU CNC, CNE’s, NUM’s, CNS’s & Staff Specialists, Cardiothoracic
Surgeons
Endorsed by: ICU Medical Director – Dr. Michael Parr APPENDIX 1:
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 9 of 13
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 10 of 13
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 11 of 13
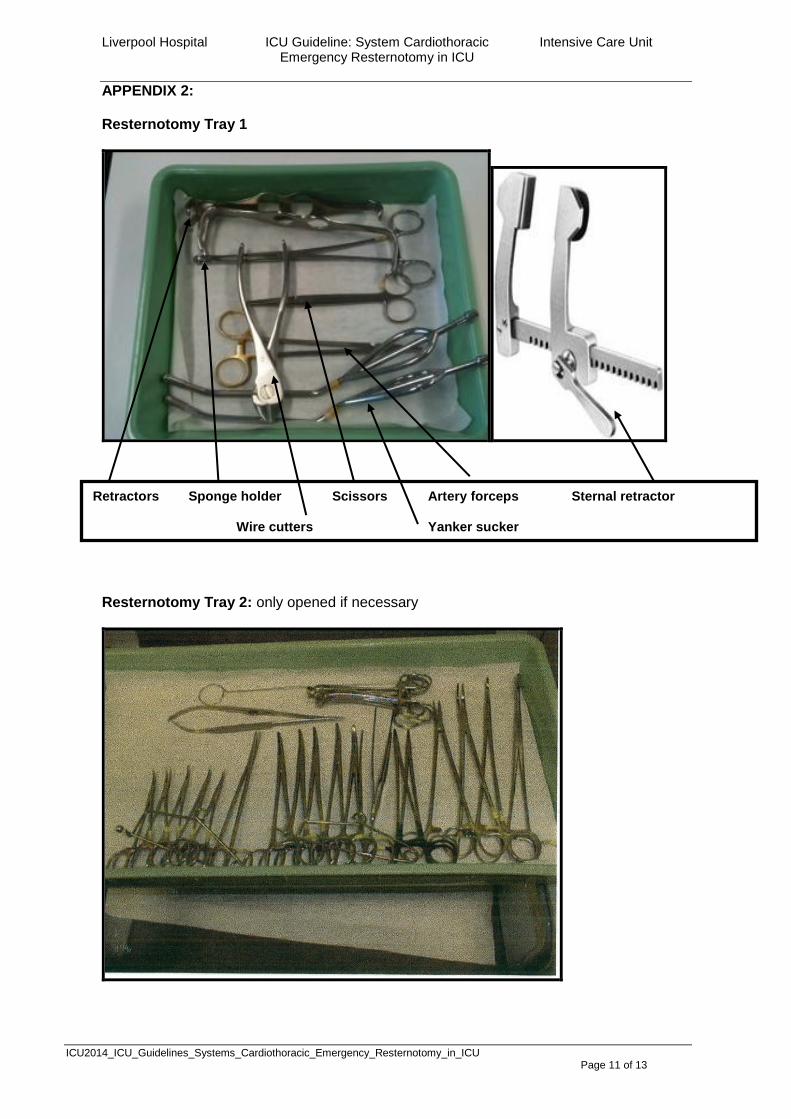
APPENDIX 2: Resternotomy Tray 1
Resternotomy Tray 2: only opened if necessary
Retractors Sponge holder Scissors Artery forceps Sternal retractor Wire cutters Yanker sucker

Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 12 of 13
APPENDIX 3: Management of Reversible Causes 4H’s
4 H’s MANAGEMENT Hypoxia Check airway
Insert guedals, ETT, LMA surgical airway to maintain airway
Check oxygenation and ventilation
Hypovolaemia Massive blood loss. Replacement of blood with:
- Crystalloid/ Colloid - Blood Products Anaphylaxis:
Management of ABC - Adrenaline (IMI, S/C) - Anti histamine - Steroid - Consider IV therapy
Hypo/Hyperkalaemia Hypokalaemia Potassium of less than 3.5mmol/L Replace Potassium
Hyperkalaemia IV calcium, 10 mls 10% CaCl2, up to 3 ampoules, each
over 5 minutes hyperventilation: CO2 + H2O H2CO3 H+ + HCO3- 50 grams 50 % Glucose + 10 units Actrapid over 10-15
minutes. ( Check your hospital policy) NaHCO3 to correct acidosis Nebulised Salbutamol
Hypo/Hyperthermia Hypothermia Active core re-warming Warmed humidified oxygen Warmed intravenous fluids Peritoneal lavage Extracorporeal warming Pleural lavage
Hyperthermia Cooling Blankets Cooling packs or Ice to head, axilla, chest, groin and
legs Cooled IV fluids
Liverpool Hospital ICU Guideline: System Cardiothoracic Intensive Care Unit Emergency Resternotomy in ICU
ICU2014_ICU_Guidelines_Systems_Cardiothoracic_Emergency_Resternotomy_in_ICU Page 13 of 13
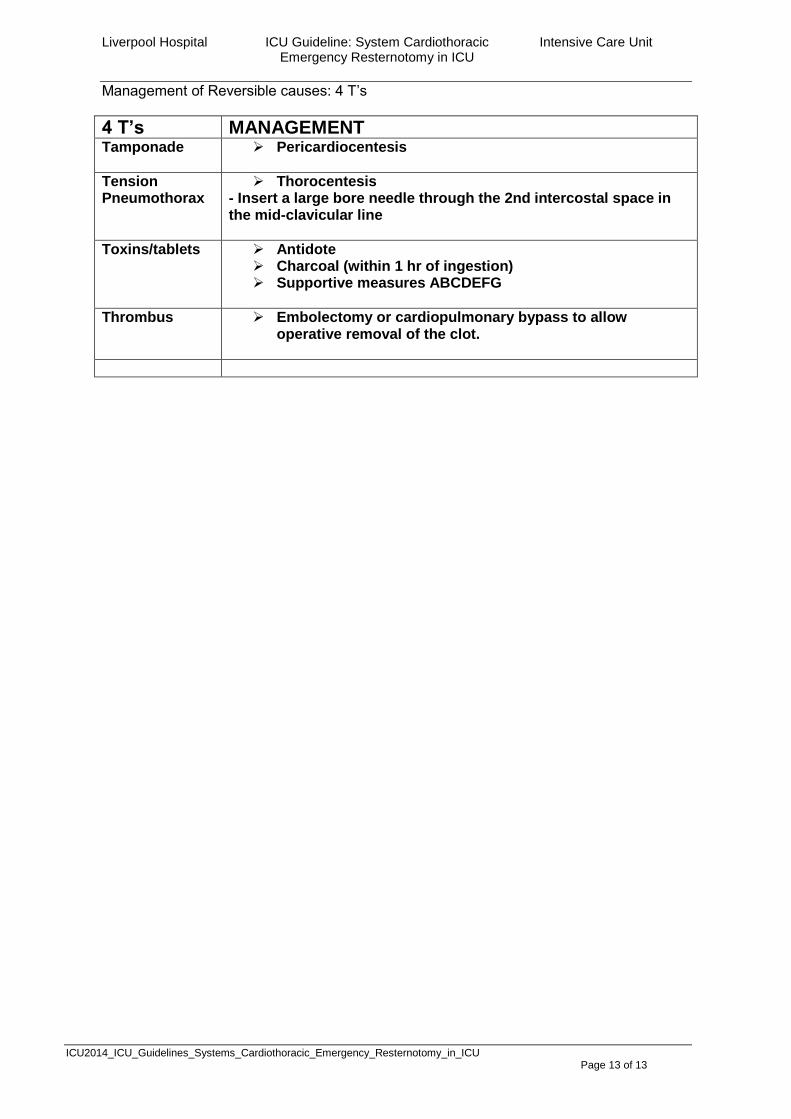
Management of Reversible causes: 4 T’s
4 T’s MANAGEMENT Tamponade Pericardiocentesis
Tension Pneumothorax
Thorocentesis - Insert a large bore needle through the 2nd intercostal space in the mid-clavicular line
Toxins/tablets Antidote Charcoal (within 1 hr of ingestion) Supportive measures ABCDEFG
Thrombus Embolectomy or cardiopulmonary bypass to allow operative removal of the clot.





























