Upload
verghese17
View
225
Download
0
Embed Size (px)
Citation preview
8/10/2019 Guide to Mental Health Act
1/87
Guidelines to theMental Health
(Compulsory Assessment andTreatment) Act 1992
8/10/2019 Guide to Mental Health Act
2/87
Disclaimer While every care has been taken in the preparation of the information in this document,users are reminded that the Ministry of Health cannot accept any legal liability for anyerrors or omissions or damages resulting from reliance on the information contained inthis document.
Please note that these guidelines are not intended as a substitute for informed legalopinion. Any concerns individuals may have should be discussed with appropriate legaladvisors.
Published with the permission of the Director !eneral of Health, pursuant tosection "#$%a& of the Mental Health %'ompulsory Assessment and (reatment& Act "))*.
'itation+ Ministry of Health. *$"*. Guidelines to the Mental Health (Compulsory Assessment and Treatment) Act 1992. Wellington+ Ministry of Health.
Published in ovember *$"* by theMinistry of Health
P- o/ 0$"#, Wellington 1"20, ew 3ealand45 )67 $ 267 #6#07 0 %book&
45 )67 $ 267 #6#0) * %online&HP 02**
(his document is available at www.health.govt.n8
8/10/2019 Guide to Mental Health Act
3/87
Contents
4ntroduction
" 5ection *+ Definitions"." 9Mental disorder:".* 9;it to be released from compulsory status:
".# 9Person in charge:".2 9Principal caregiver:
* 5ection 2+
8/10/2019 Guide to Mental Health Act
4/87
1 Part *+ 'ompulsory treatment orders1." 5cope of a community treatment order1.* =esidence reCuirements under community treatment orders1.# (erms of a community treatment order
1.2 oluntary admissions during the term of a community treatment order1.0 'ompulsory admissions during the term of a community treatment order1.1 -verseas and domestic travel during the term of a community treatment
order1.6 4npatient treatment orders1.7 4npatient leave1.) =elease from compulsory treatment order
1."$ =eassessment following release from compulsory treatment order1.""
8/10/2019 Guide to Mental Health Act
5/87
"" Part 1+ =ights of patients and proposed patients""." 5ection 12+ !eneral rights to information"".* 5ection 10+ =espect for cultural identity "".# 5ection 11+ =ight to treatment
"".2 5ection 16+ =ight to be informed about treatment"".0 5ection 17+ ;urther rights in case of visual or audio recording"".1 5ection 1)+ =ight to independent psychiatric advice"".6 5ection 6$+ =ight to legal advice
"".7 5ection 6"+ =ight to company and seclusion"".) 5ection 6*+ =ight to receive visitors and make telephone calls""."$ 5ections 6# and 62+ =ight to receive?send letters and postal articles""."" 5ection 60+ 'omplaint about a breach of rights
""."* =ights of proposed patients""."# =ights under the ew 3ealand ill of =ights Act "))$
"* Part 6+ =eviews and Budicial enCuiries"*." Duty to conduct clinical review of patients"*.* Applications to the Mental Health =eview (ribunal"*.# Mental Health =eview (ribunal reviews of patients
"*.2 Appeal against Mental Health =eview (ribunal decision
"# Part 7+ 'onsent for young people and involvement offamily?wh@nau
"2 Part "$+ se of force"2.7 5ection ""2+ eglect or ill treatment of patients or proposed patients
Appendi/ "+ -ther guidelines and documents published by theMinistry of Health
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* v
8/10/2019 Guide to Mental Health Act
6/87
ist of ;igures;igure "+ 'ompulsory assessment and treatment;igure *+ Process for making compulsory treatment orders;igure #+ 'linical and Budicial review of patients under compulsory treatment orders
;igure 2+ 'linical and Budicial review of special patients acCuitted by reason ofinsanity
;igure 0+ 'linical and Budicial review of special patients found unfit to stand trial;igure 1+ 'linical and Budicial review of restricted patients
vi !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
7/87
Introduction(hese guidelines are intended to support the effective and lawful use of the MentalHealth %'ompulsory Assessment and (reatment& Act "))* %referred to hereafter as 9the Act: or 9the MH%'A(& Act:&. (he purposes of the Act may be described as being to+
define the circumstances in which compulsory assessment and treatment may occur
ensure that both vulnerable individuals and the public are protected from harm
ensure that the rights of patients and proposed patients are protected
ensure that assessment and treatment occur in the least restrictive mannerconsistent with safety
provide a legal framework consistent with good clinical practice promote accountability for actions taken under the Act.
(he Act is not a comprehensive framework for mental health treatment. 4t shouldinstead be thought of as an entry point to services for people e/periencing a mentalillness which causes or may cause serious harm to themselves or others. 'ompulsorytreatment under the Act provides an opportunity for a person e/periencing a seriousmental illness to begin to live well in the community and take self ownership of theirhealth care. (his is promoted through a focus on regular collaborative consultation between compulsory patients and clinicians, and the statutory presumption in favour of
minimally restrictive treatment in the community.
o piece of legislation can be framed in such a way that all circumstances that canpossibly arise are precisely covered. 4f there is uncertainty as to the 9correct:interpretation, any action taken should be taken in good faith, be consistent with thespirit and intent of the Act, and reflect best clinical practice. 4n practice, especially inurgent circumstances, situations may arise where adherence to a literal interpretationof the Act may compromise the safety and wellbeing of the individual, staff or public. 4fthe Act can be interpreted in two ways, literally or purposively %that is, in a mannerconsistent with its purpose&, then the purposive interpretation should be preferred.
(he Act gives specific powers to enable compulsory assessment and treatment to occurand in limited circumstances permits the use of reasonable force in e/ercising suchpowers. A clinician, member of the Police or any other person should be able to Bustifytheir actions in terms of the powers conferred by this Act or other legislation orauthority.
(he Ministry of Health has issued a range of guidance material to assist clinicians andadministrators to best fulfil their statutory roles, and to assist in the appointment ofsuitable candidates to statutory roles. (he following guidance documents should beread in conBunction with these guidelines+
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 1
8/10/2019 Guide to Mental Health Act
8/87
Guidelines for the Role and unction of !irectors of Area Mental Health "er#ices %Ministry of Health *$"*&
Guidelines for the Role and unction of !uly Authorised $fficers %Ministry ofHealth *$"*&
Competencies for the Role and unction of Responsi%le Clinicians under the Mental Health (Compulsory Assessment and Treatment) Act 1992 %Ministry ofHealth *$$"&
Guidelines for Medical &ractitioners usin' "ections 11 and 11 A of the Mental Health (Compulsory Assessment and Treatment) Act 1992 %Ministry of Health*$$$&.
A full list of related Ministry of Health publications is contained in Appendi/ ".
2 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
9/87
1 ection 2! De"initions
1#1 $Mental disorder%
Mental disorder , in relation to any person, means an abnormal stateof mind %whether of a continuous or an intermittent nature&,characterised by delusions, or by disorders of mood or perception or volition or cognition, of such a degree that it F%a& poses a serious danger to the health or safety of that person or of
othersG or%b& seriously diminishes the capacity of that person to take care of
himself or herselfG Fand mentally disordered , in relation to any such person, has acorresponding meaning. "
(he central criteria for initiating and continuing compulsory assessment and treatmentis that a person is or appears to be mentally disordered . (he 'ourt of Appeal discussedthe definition of 9mental disorder: at length in its decision in aitemata Health # Attorney*General .* (he following general points can be inferred from that case.
(he definition of 9mental disorder: is based on phenomena rather than diagnosis. # (he Act avoids reference to any particular mental or psychiatric illness. 4nstead, it
provides a number of symptom clusters that might indicate an 9abnormal state ofmind:. (hese are 9delusions, or disorders of mood or perception or volition orcognition:.
(he language of the 9mental disorder: definition seeks to avoid the debate over thedifference between mental illness and behavioural disorders. A person with a severepersonality disorder e/hibiting any of the phenomena identified in the 9mentaldisorder: definition may well Cualify for compulsory treatment under the Act,despite not having a mental illness according to clinical definitions.
" 5ection *%"& of the MH%'A(& Act.* %*$$"& *" ;= 3 *"1G *$$"I 3; = ""**.# 9Phenomena: are abnormalities of specific areas of mental functioning %psychopathology&
that may be observed. (he presence of individual abnormal phenomena does not necessarily indicate a specific illness or diagnosis. 9Diagnosis: is an attempt to identify an illness, basednot only on the presence of patterns of psychopathological abnormalities, but also on the basis of the cause %aetiology&, time course %history& and outcome %prognosis& of the disorder.Diagnosis may be relevant to the definition in terms of assessing whether the disorder of
mind is of a continuous or intermittent nature %for a fuller account refer to Dawson E. "))1.Psychopathology and 'ivil 'ommitment 'riteria . Medical +a, Re#ie, . 2+ 1*F7#&.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* &
8/10/2019 Guide to Mental Health Act
10/87
(he part of the definition of 9mental disorder: concerning the nature of a person:sabnormal state of mind, ending with the word 9cognition:, is commonly referred to asthe 9first limb: of the definition. (he part of the definition concerning the severity of theperson:s condition is referred to as the 9second limb:.
1#1#1 $A'normal state o" mind%
Whether or not a person has an 9abnormal state of mind: is determined wholly by thepresence of one or more of the phenomena provided in the 9mental disorder: definition.'linicians should not measure whether, taken as a whole, a person has an obBectivelyabnormal state of mind compared with that of the average person, but whether anyphenomena indicating an abnormal state of mind as described at ".".# are present.
1#1#2 $ hether o" a continuous or an intermittent nature%
(he definition of 9mental disorder: specifically includes intermittent disorders. (hisreflects an allowance for a fluctuating intensity of the phenomena characterising anabnormal state of mind. =emission and relapse of phenomena may occur during thecourse of a person:s recovery. (here is no reCuirement that the phenomena on whichthe finding of mental disorder is based must necessarily be present at the time ofe/amination, or at the time that the application is made. (here are times when it may be appropriate to continue or even initiate compulsory treatment during a period ofremission. 'ompulsory treatment may be appropriate in some cases for a person whoappears to currently be well if the person has previously demonstrated+ repeated or prolonged episodes of illness
severe conseCuences during phases of illness, such as severe violence to self orothers
early loss of insight during an episode of illness, with a pattern of failing to be able totake the necessary steps to halt the development of illness
changeable insight into the nature of their mental illness that results in an inabilityto maintain a consistent decision to seek appropriate treatment.
(he definition of mental disorder incorporates intermittently present phenomena,allowing continuing compulsory treatment during periods of remission to provide formore intensive overview and the possibility of early intervention to prevent relapse.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
11/87
1#1#& $Characterised 'y delusions* or 'y disorders o" mood orperception or volition or co+nition%
An abnormal state of mind must be characterised by one or more of these phenomena.(hese may be abnormal for the individual, compared to what is normal for the
individual %as is the case in an acute illness, for e/ample&, or abnormal in terms ofpopulation norms.
Particular care must be taken to ensure that the state of mind is 9abnormal: in terms ofthe individual:s cultural norms. (hese may include M@ori spiritual beliefs or other belief systems. ;or e/ample, in Re MMG ,2 the applicant believed in witchcraft and wasa member of a community of witches, which included the applicant:s mother.
(he 'ourt of Appeal in aitemata Health described in passing the phenomena in thedefinition of 9mental disorder: as words in ordinary use, although their application isheavily dependent upon the assessment of clinicians. (his means that colloCuial uses of those words are not sufficient to bring someone under the Act, but that phenomena arenot strictly limited to their clinical definitions. ;or e/ample, when a person is describedas 9deluded: in the ordinary use of that term, it does not follow that the person has9delusions: for the purposes of the Act. However, the 'ourt suggested that a severepersonality disorder that led to an e/ceptionally disturbed view of the world couldfeasibly be taken to be a disorder of cognition or perception. 0
(his has been followed in some subseCuent cases 1 but Cuestioned in others. 6 4t should be noted that the 9mental disorder: definition was not directly at issue in theaitemata Health case, and so the 'ourt:s statements are advisory and not strictly
binding. (he Ministry regards the law in this area as unsettled, and cautions againstundue e/pansion of the psychiatric understanding of the disorders that can give rise toan abnormal state of mind.
5everal of the phenomena described in the mental disorder definition F delusions,disorders of mood and disorders of perception F are well defined clinical concepts. (heconcepts of 9disorder of volition: and 9disorder of cognition: are not well definedclinically and are open to interpretation, as e/plained below. (he following e/planationsare intended to provide guidance.
2 Re MMG % MH=( 017?)7&, "7 ovember "))7. (he Mental Health =eview (ribunal%MH=(& considered the applicant:s beliefs this factor, but the applicant was neverthelessconsidered to have fulfilled the criteria of the first limb of the mental disorder definition.
0 aitemata Health at 6*I.1 ;or e/ample, in a later case concerning Mr H % Re RCH *$$*I 3; = 2"#&, the Mental
Health =eview (ribunal %MH=(& accepted the view that H:s severe personality disordercreated overvalued ideas to the e/tent that it constituted a disorder of cognition. 4n Re GT+ %MH=( ""?$)2, 6 December *$""& aspects of a person:s severe personality disorder wereconsidered disorders of mood, volition and perception.
6 5ee Re RCH %MH=( "*?$#), #$ April *$"*&.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* ,
8/10/2019 Guide to Mental Health Act
12/87
Disorders o" volition
9 olition: means the power to consciously choose or will, and includes the power to acton or abstain from acting on that choice or will .7
A disorder of volition may include+ catatonic e/citement or withdrawal depressive stupor passivity phenomena and command hallucinations amotivational syndrome in maBor psychosis.
(hese are e/amples of absent or changed volition that occur in the conte/t of a maBormental illness. =are states such as conversion disorders, sleep walking and epilepticautomatism may also be disorders of volition.
(here are many other circumstances where volition may be seen as abnormal. (heseare within the areas of disorders of impulse control. Here, a person is aware of theiractions and potential outcomes and has normal reality testing, but acts according to animpulse or desire for some reason. -ne of the difficulties here is the conflict between anirresistible impulse and an impulse not resisted. 4t is e/tremely difficult to Budgeclinically whether someone is able to resist an urge, but chooses not to, or is trulyunable to resist. Whether these should be included as disorders of volition is, therefore,arguable.
8/10/2019 Guide to Mental Health Act
13/87
Bustified when a person is affected by a condition that impairs or affects their ability tochoose, with serious or dangerous conseCuences. 4n general, conditions such aspsychose/ual disorders and anti social personality disorder will not be considered anabnormal state of mind, unless particularly severe or complicated by another conditionsuch as a disorder of mood, perception or cognition, delusions or intellectual disability.
Disorders o" co+nition
9'ognition: includes the processes involved in perceiving, knowing, recalling, thinking,learning, evaluating and understanding, and includes the mental process of obtaining,organising and utilising sensory and perceptual information, remembering paste/periences, and making plans or strategies. )
9'ognition: can also refer to a thought. (he potential difficulties with the use of the term9disorder of cognition: are primarily the confusion between cognition as a process andcognition as a thought. 4t is inappropriate to define 9cognition: as a thought rather thana process to include people with deviant but non delusional thoughts in the scope of the Act. 4f cognition is seen as the process of thinking, perceiving and recalling, then theuse of this concept should not spread e/cessively beyond that intended by Parliament.
Disorders of cognition clearly include+ slowing of cognition in depressive states increased rate of cognition in manic states disorganisation or disruption of thought process in psychotic states cognitive changes in dementia and other acCuired organic mental disorders.
A disorder of cognition can be seen to embrace the thought disorder commonly notedduring psychosis, namely disorganised or illogical thought processes of a very severedegree, as well as poverty of thought or absence of thought that can occur in somemarked psychotic states. As the terminology has been different %9cognition: versus9thought:&, some psychiatrists have been uncertain whether formal thought disorder isembraced by a disorder of cognition. 4n the Ministry:s view it is. ;ormal thoughtdisorder may be the only mental state abnormality in some manifestations ofpsychosis. 4t may also cover+ obsessional rumination in obsessive compulsive disorder disordered self perception such as in eating disorders an/iety disorders with recurrent ruminations.
4t is rarely appropriate to compulsorily treat conditions characterised only by recurrentdangerous thoughts such as inappropriate se/ual desires or violent fantasies. (o becompulsorily treated, such conditions should be characterised by a lack of control overacting on such thoughts of such severity as to constitute a disorder of #olition . Withoutsuch a volitional disorder, such persons will rarely present a sufficient danger to thesafety of others to satisfy the definition of mental disorder.
)
!orland-s llustrated Medical !ictionary %#*nd ed *$"*&, Mos%y-s !ictionary of Medicine/ 0ursin' and Health &rofessions %"st Australian and ew 3ealand ed *$$1&.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* .
8/10/2019 Guide to Mental Health Act
14/87
8/10/2019 Guide to Mental Health Act
15/87
5erious danger to the safety of the person in Cuestion may arise if a person:sargumentative or confrontational demeanour, which is a result of an abnormal state ofmind, makes the person likely to be the victim of violence from others. "" 4t may alsoarise if a particularly vulnerable person has a history of being se/ually e/ploited whenaffected by an abnormal state of mind. "* (here may also be a serious danger to thesafety of a person if an abnormal state of mind leads to suicidal ideation.
When considering a serious danger to the health of others, both physical andpsychological health should be considered ."# A person with an erotomanic fi/ationmight constitute a serious danger to the mental health of others. 4n Re C ,"2 where there was evidence that a person:s obsessional attachment and stalking behaviour had causedgreat an/iety and fear to his victim and her family, but there had been no physicalthreats, the MH=( held that 9there is clear and uneCuivocal evidence to show that theI behaviour poses and continues to pose a serious danger to the psychological health ofthe victim and her family:. A parent with custody of their child may present a seriousdanger to the physical or mental health of that child if not subBect to compulsorytreatment. "0
5erious danger to the health of the person in Cuestion may occur if the person has achronic illness such as diabetes and is unable to manage their condition due to anabnormal state of mind. (he clinician should also consider whether the risk of mentalhealth deterioration, as the result of lack of treatment, might constitute a seriousdanger to the health or safety of the person. =epeated acute bouts of mental illness may contribute to the overall deterioration of that person:s condition.
4f a person does not have the capacity to make decisions related to their physical health,
compulsory treatment under the Act should not be initiated for the purpose of treatingphysical health problems. (he appropriate course of action is to seek a treatment orderor an order appointing a welfare guardian under the Protection of Personal andProperty =ights Act ")77.
1#1#- $ eriously diminishes the capacity o" that person to ta e careo" himsel" or hersel"%
5elf care is not limited to the basic necessities of survival %activities of daily living suchas food, shelter, hygiene and medication& but includes 9the multiplicity of other needssuch as achieving financial security, maintaining proper social relationships,
maintaining stable accommodation and seeking out ... the assistance of others ...concerning health and lifestyle:. "1 5elf care has been said to embrace all of 9the highercomple/ities of modern living: "6 and the 9ability to cope adeCuately in the community:. "7
"" As considered in Re TR MH=( $7?""2, ") August *$$7."* Re MH=( ""?$*6, *" April *$""."# 5ee Re R ! "))0I 3; = *7."2 "))1I 3; = 01*."0 Re TR ."1 !ecision 324596 MH=( #*2?)0, "2 Eune "))0."6 Re A7HM MH=( $7?""$, *0 August *$$7."7 !ecision 324596 .
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 9
8/10/2019 Guide to Mental Health Act
16/87
5elf care is not simply that which is in the 9best interests: of a person, if they behave insome way that makes them a nuisance to others. ") or does it include provision for 9thecapacity to find happiness in life and fulfil potential:G *$ these are considered to beprivate and individual matters independent of any mental disorder.
5elf care can also be regarded as those essential functions that can be 9reasonablyreadily provided or addressed by others:. *" (he degree of outside care available to aperson is a relevant factor in the mental disorder test. 4f the support of wh@nau orfriends is present to adeCuately fill the functional gap created by diminished capacity,or to lessen the risks posed to self or others so that they are no longer 9serious:, a person who is otherwise mentally disordered may be released from compulsory care. **
(he test of diminished capacity is neither wholly subBective nor wholly obBective. AsubBective test of diminished capacity may unfairly target people of high economic worth, education or social status. Although that person:s capacity for self care may beseriously diminished by a mental illness, they may still cope adeCuately in thecommunity. An obBective test, on the other hand, may target persons with a belowaverage capacity independent of any abnormal state of mind, such as those with anintellectual or physical disability, or frailty due to age. 4n Re C ,*# the court described ami/ed obBective?subBective test of a 9minimum standard of effective self care for aperson of the patient:s circumstances and background:.
'apacity for self care is 9uniCue to the individual having regard to both intrinsic ande/trinsic considerations, that is to say, the Cualities and characteristics of theindividual, together with the features of their social, and material environment:. *2 (his
approach recognises a person:s uniCue skills and talents. Despite this, a certainminimum capacity has been generally considered sufficient in all but the moste/ceptional cases, as there is a 9broad commonality: between the minimum capacities of most members of the community. *0
4t is appropriate to primarily enCuire as to whether a person meets an obBective baselevel of capacity for self care. However, diminished capacity has sometimes beenestablished when a person has feasible goals reCuiring a high level of functioning, suchas running a business, *1 working as a doctor *6 or attending university. *7
") Re " C MH=( $*?$#*, 2 ovember *$$**$ Re A7HM.*" Re A7HM.** Re TRT MH=( $)?$67, "2 August *$$).*# D' Auckland, 'A( "#*?)), *7 August *$$$, (horburn D'E.*2 Re 8 MH=( ""?"#), "7 Eanuary *$"*.*0 Re A7HM.*1 Re T MH=( $6?$#6, *6 April *$$6.*6 Re A AA MH=( $7?$"*, 6 Euly *$$7.*7 Re A7HM.
13 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
17/87
1#1#. Head in4ury
A person may be compulsorily treated due to a mental disorder arising from a headinBury. As mentioned above at ".", the definition of mental disorder under the Act isdeliberately stated in terms of phenomena rather than diagnoses. (he Act reCuires an
abnormal state of mind characterised by one or more phenomena, including 9disorderof cognition:. (his applies irrespective of whether the disorder results from a diagnosisof mental illness %in the narrow sense& or any other cause, such as traumatic braininBury, hypo/ia, to/icity or dementia.
5ection 2 of the Act contains the only reference to diagnosis. (his specifically e/cludescertain conditions %such as intellectual disability& as a sole reason for invokingcompulsory assessment procedures. (here is no clause in the Act that e/cludes headinBury as the basis of its application.
1#2 $5it to 'e released "rom compulsory status%(he Act defines 9fit to be released from compulsory status: to mean 9no longer mentallydisordered and fit to be released from the reCuirement of assessment or treatment:under the Act.
(he 'ourt of Appeal in aitemata Health held that the correct interpretation of thisprovision was that fitness to be released automatically follows when a person is nolonger mentally disordered. 4f a person remains mentally disordered, it follows thatthey are therefore not fit to be released.
4n spite of that interpretation, necessity of compulsory treatment remains a relevantconsideration when determining whether a person is mentally disordered. When it isnot necessary to maintain a compulsory treatment order, due to good compliance withmedication, for e/ample, the severity criteria in the second limb of the mental disorderdefinition may no longer be met, even if the person:s abnormal state of mind is stillpresent under the first limb. (he person will therefore be fit to be released fromcompulsory status.
1#& $/erson in char+e%(he Act defines the person in charge of a hospital or a service to be the chief e/ecutiveofficer.
>nder section )) the person in charge of a hospital may delegate their powers underthe Act to another person who is suitably Cualified, often the Director of Area MentalHealth 5ervices %DAMH5&. (he delegation must be in writing, and any revocation of thedelegation must also be in writing. 4t is recommended that the power to admit or detaina patient or proposed patient only be delegated to a person who has a clinical background, such as members of a psychiatric crisis team and?or designated staff in anacute psychiatric unit.
(he authority to admit and detain a patient or proposed patient to a hospital is grantedto the person in charge of the hospital under section ""#. (o avoid any risk of unlawful
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 11
8/10/2019 Guide to Mental Health Act
18/87
detention, this authority should be delegated to a person normally present at thehospital.
1# $/rincipal care+iver%(he Act defines the 9principal caregiver: to mean 9the friend of the patient or themember of the patient:s family group or wh@nau who is most evidently and directlyconcerned with the oversight of the patient:s care and welfare:. (he fact that the patientdoes not give the name of the principal caregiver, or does not authorise, or even forbids,the principal caregiver being contacted, does not affect the statutory duty to send theprincipal caregiver a copy of the certificate of preliminary %section "$%2&%a&%iv&&, further%section "*%0&%d&& and final %section "2A%*&%c&& assessment, and a copy of a certificate of clinical review that states that the patient is not fit to be released from compulsorystatus %section 61%6&%b&%iii&&.
(he Privacy Act "))# does not affect the clear statutory duty of notification in thesecircumstances, *) nor does the Health 4nformation Privacy 'ode or the 'ode of Healthand Disability 5ervices 'onsumers: =ights %the 'ode of =ights&.
;or many patients, there is no dispute as to who the 9principal caregiver: is. 4f there isdoubt or disagreement, the viewpoints that need to be considered are those of+ the patient spouse or partners the family?wh@nau friends of the patient health professionals in the service other parties concerned with the care of the patient, for e/ample, prison staff.
4f the patient is competent to make a decision about who is the principal caregiver,their advice as to who the principal caregiver is should be accepted. (his informationmay also have been given in an advance directive.
8/10/2019 Guide to Mental Health Act
19/87
4t is important to note that more than one principal caregiver may be appointed. #$
#$ Re HM ")))I 3; = 707.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 1&
8/10/2019 Guide to Mental Health Act
20/87
2 ection ! 67clusion criteria5ection 2 of the Act prohibits compulsory assessment and treatment by reason only ofa person:s political, religious or cultural beliefs, their se/ual preference, criminal ordelinCuent behaviour, substance abuse or intellectual disability. However, section 2does not prohibit assessment and treatment of patients who have a mental disorder butmight otherwise fit within one of the section 2 categories. 4n Re H ,#" Eudge 4nglissummarised the position.
-nce the 'ourt has found that the patient is mentally disordered withinthe definitionI, it is irrelevant for the purposes of parts 4 and 44 that thestate of the mental disorder e/ists because the patient is also intellectuallydisabled. (here is no logic in terms of the scheme and purpose of the Act inpreventing a person, that is mentally disordered to a degree where acompulsory treatment order is reCuired, from being compulsorily treatedmerely because the conseCuences of his mental disorder are heightened byhis intellectual disability. (he true purpose of section 2%e& is to prevent it being too readily assumed from a state of intellectual disability that theremust also be a state of mental disorder as that term is defined %y thestatute . 4 have italicised the last words to make it clear while intellectualdisability may, in its nature, involve some degree of mental disorder in ageneral sense, it may not involve mental disorder in the specialisedstatutory sense.
(he e/clusion factors in section 2 reflect an attempt to indicate the limits of theimposition of compulsory treatment. 4t is clearly improper for people to be detained ina psychiatric hospital for their political, religious and cultural beliefs, or se/ualpreference %sections 2%a& and 2%b&&.
'ompulsory treatment should be confined to those with a maBor mental disturbance,not a disagreement with the 5tate. (his is the rationale for section 2%c& of the Act, whiche/cludes criminal or delinCuent behaviour. 'onflicts of these types between theindividual and society are best reserved for the criminal Bustice system. Psychiatry:sethical position in the treatment of people e/periencing mental illness is undermined if
it becomes an agent of 5tate control for groups of people who society may find irksome.
5ection 2%d& of the Act, which e/cludes substance abuse as a sole reason for compulsory assessment and treatment, is discussed below at *.". 5ection 2%e& of the Act e/cludesthe application of the Act on the grounds of intellectual disability alone, and isdiscussed below at *.*.
#" Re H :Mental Health; %"))#& "$ ;= 3 2**.
1 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
21/87
oth substance abuse and intellectual disability may contribute to a person:s abnormalstate of mind. 5o long as substance abuse or intellectual disability is not the sole causeof a person:s abnormal state of mind, an assessing clinician or Budge may legitimatelyconsider dangers that arise as a result of any aspect of that person:s abnormal state ofmind, including dangers that arise due to a person:s compulsive substance use orintellectual disability, when determining whether a person is mentally disordered.
2#1 u'stance a'use5ection 2%d& of the Act specifically e/cludes substance abuse as a sole basis for theapplication of procedures for compulsory assessment and treatment under the Act. utthe presence of substance abuse does not preclude the use of the Act if the criteria for9mental disorder: are otherwise met.
(he following are e/amples of the types of situation in which mental disorder may arise
in the conte/t of substance abuse. When an into/icated individual displays suicidal behaviour, or threatens suicide or
self harm, it may be appropriate to utilise the Act. 4t may be reasonable to form the belief that someone who is threatening suicide or acting in a suicidal manner may bementally disordered, no matter how into/icated they are.
(he acute effects of into/ication may present as a mental disorder, for e/ample theeffects of hallucinogenic drugs may mimic psychotic symptoms. Persons in such astate will often meet the lower threshold for assessment and treatment under Part "of the ActG that is, there will be reasonable grounds to believe that they are mentallydisordered until the cause of their symptoms becomes apparent %see 0." below&.
Mental disorder may arise as the conseCuence of long term substance abuse, fore/ample the cognitive impairment of a Jorsakoff:s psychosis. 4f there is a mentaldisorder, irrespective of its underlying causation, the Act may apply.
4ndividuals who have a 9dual diagnosis: or 9co morbidity: of a mental disorder and asubstance abuse disorder at the same time present particular difficulties for clinicalmanagement. An individual who is mentally disordered can be made subBect to theprovisions of the Act, irrespective of whether they also have a co e/isting substanceuse disorder.
(he terms of a community treatment order or leave from an inpatient order, should
specify whether abstinence from drugs or alcohol is a condition of the order. (hecontinuing abuse of drugs by an individual who is subBect to a compulsory treatmentorder, particularly if this is associated with disturbance of behaviour, may be sufficientgrounds for readmission or reassessment.
(he Alcoholism and Drug Addiction Act ")11 provides a legislative basis forcompulsorily detaining people in order to treat them for an alcohol or substancedependence problem. (hat Act should be used if compulsory treatment for suchproblems is reCuired. (reatment of alcohol or drug abuse should never be the primaryreason for compulsory treatment under the Mental Health %'ompulsory Assessmentand (reatment& Act "))*.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 1,
8/10/2019 Guide to Mental Health Act
22/87
2#2 Intellectual disa'ility 5ection 2%e& of the Act specifically e/cludes intellectual disability as a sole basis for theapplication of procedures for compulsory assessment and treatment under the Act. utthe presence of intellectual disability does not preclude the use of the Act if the criteriafor 9mental disorder: are otherwise met.
8/10/2019 Guide to Mental Health Act
23/87
& 8espect "or cultural andpersonal ri+hts
5ections 0 and 1 reCuire powers to be e/ercised with respect for a person:s culture,language and beliefs. (he use of the word 9person: in sections 0 and 1 indicates thatsection 0 applies to all people before they become proposed patients, and once they become proposed patients and patients. (he reCuirements of sections 0 and 1 of the Actmean that staff need to know how to access the services of an interpreter andappropriate cultural advisors, often at short notice. Mental health services should balance their responsibilities under sections 0 and 1 of the Act with the need to ensurethat the overall goal of proper care for a patient or proposed patient is notunnecessarily hindered.
ection ,! Cultural identity
#1 ection ,(2)(a) $proper reco+nition o" the importance andsi+ni"icance to the person o" the person%s ties ith his or her"amily* h:nau* hap;* i i* and "amily +roup%
5ection 0%*&%a& reCuires that family?wh@nau relationships be encouraged if they are beneficial to a person:s wellbeing. ;amily?wh@nau should be encouraged to provide
information about the person, in terms of that individual:s history, and feedback on any changes noticed when the person is on leave or in the company of family?wh@naumembers. 4t is important at a very early stage of the compulsory assessment andtreatment process to involve family?wh@nau and to continue to do so throughout thecourse of treatment.
(he relationship between the person and their family?wh@nau may change over time. A person who refuses contact with family?wh@nau may change their mind and the wishesof family?wh@nau should be considered whenever possible %see section 6A&.
ote that the Privacy Act does not preclude information from being provided byfamily?wh@nau members and does not always prevent family?wh@nau members andother caregivers from being provided with information about the person #* for e/ample if+ disclosure was one of the purposes for which the information was collected ##
there is a serious and imminent threat of self harm by the person #2
the person is being discharged into the care of family?wh@nau.
#* 5ee Ministry of Health. "))1, n
8/10/2019 Guide to Mental Health Act
24/87
'linicians should alert a person:s family?wh@nau about aspects of the person:s illness ifthey are e/pected to be a part of their support group. ;or e/ample, clinicians shouldprovide information about the person:s medication needs and any kinds of behaviourthey should be concerned about.
#2 ection ,(2)(c) $proper respect "or the person%s cultural andethnic identity* lan+ua+e* and reli+ious or ethical 'elie"s%
ote that section 10 of the Act affirms that 9every patient is entitled to be dealt with in amanner that accords with the spirit and intent of section 0:. (his reCuirement isreinforced by =ight "%#& of the 'ode of Health and Disability 5ervices 'onsumers:=ights %the 'ode of =ights&. 4t should be incorporated into the assessment andmanagement of the individual by ensuring that cultural assessment is a key componentof assessment.
ection -!
8/10/2019 Guide to Mental Health Act
25/87
and their main source of communication. (hey see themselves as a distinct culture, ande/perience uniCue pressures that affect their mental health. #0 Mental health servicesshould be responsive to people, patients and proposed patients who are Deaf byensuring that a competent interpreter is available to them, and by ensuring that staffmembers are aware that a Deaf individual:s culture surrounding their deafness hasspecific relevance and meaning.
A registered ew 3ealand 5ign anguage interpreter is considered to be a competentinterpreter for the Deaf. An updated list of registered ew 3ealand 5ign anguageinterpreters can be obtained from regional Deaf Association offices or the 5ignanguage 4nterpreters Association of ew 3ealand %5 4A 3&.
#0 Ministry of Health. "))6. Mo#in' or,ard . Wellington+ Ministry of Health 2*F2#.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 19
8/10/2019 Guide to Mental Health Act
26/87
ection .A! Consultation ith "amily= h:nau
5ection 6A of the Act reCuires a medical practitioner or responsible clinician to consult with family or wh@nau during the compulsory assessment and treatment process unlessit is not in the best interests of the patient or proposed patient, or it is not reasonablypracticable. 'omprehensive guidelines for consultation with family and wh@nau can befound in the Ministry of Health publication n#ol#in' amilies> Guidance 0otes .#1
(he purpose of consultation with family?wh@nau is to+
strengthen family?wh@nau involvement in the compulsory assessment andtreatment process enhance the family?wh@nau contribution to the patient or proposed patient:s
subseCuent care go some way towards addressing family?wh@nau concerns about information
sharing and treatment options help facilitate ongoing family?wh@nau involvement in MH%'A(& Act processes such
as clinical reviews of treatment or court hearings.
When a medical practitioner or responsible clinician is deciding whether family? wh@nau consultation is in the best interests of the patient or proposed patient, theymust first consult the patient or proposed patient. A medical practitioner or responsibleclinician must apply the relevant parts of these guidelines when deciding+ when and how to consult family?wh@nau or the patient or proposed patient whether consultation with family?wh@nau is reasonably practicable whether consultation with family?wh@nau is in the best interests of the patient or
proposed patient.
'onsultation with family?wh@nau is an ongoing process. 4t is recommended that amedical practitioner or responsible clinician consults or attempts to consult+ when making significant treatment decisions at each Buncture in the compulsory assessment and treatment process when considering discharge from the compulsory assessment and treatment process when developing a relapse prevention plan.
#1 =oyal Australian and ew 3ealand 'ollege of Psychiatrists. *$$$. n#ol#in' amilies>Guidance notes> Guidance for in#ol#in' families and ,h?nau of mental health
consumers5tan'ata ,hai ora in care/ assessment and treatment processes . Wellington+Ministry of Health.
23 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
27/87
'onsultation may reCuire the medical practitioner or responsible clinician to disclose apatient:s or proposed patient:s personal and health information to family?wh@nau. (hisis particularly necessary when developing a treatment, discharge or relapse preventionplan in which family?wh@nau will be involved in maintaining a person:s wellness in thecommunity. (he disclosure of information for the purposes of consultation undersection 6A is not a breach of the Privacy Act "))# or Health 4nformation Privacy 'ode. #6
However, it is desirable to discuss the consultation process with the patient or proposedpatient in advance, so they understand the purpose of consultation and the e/tent to which information will be shared.
'onsultation at the different stages of the compulsory assessment and treatmentprocess is likely to assist the responsible clinician in making decisions at those stages. 4tmay also increase family?wh@nau awareness of and?or involvement in, andcontribution to, court hearings under the Act. 4f a person has presented to mentalhealth services at a late stage of their illness, when the likelihood of successfulconsultation has been diminished due to strained family relationships, it may be beneficial to encourage re engagement with family members as the person becomes well.
(he names of family?wh@nau members consulted should be recorded on the initialassessment record form, and the nature of the consultation recorded in the patient:s orproposed patient:s clinical file.
(he medical practitioner or responsible clinician should obtain a patient:s or proposedpatient:s consent to consult family?wh@nau whenever possible, but patient consent isnot always reCuired, such as when a patient is acutely unwell or lacks capacity to
consent. (he reCuirement to consult does not mean a patient or proposed patientforfeits their right to confidential care and treatment. Patients: and proposed patients:rights and the protection of those rights continue to be paramount and a maBorphilosophical tenet of the Act.
(he section 6A reCuirement to consult does not mean all family?wh@nau concernsabout the compulsory assessment and treatment of the patient or proposed patient willnecessarily be addressed. 4t is possible the reCuirement will raise family?wh@naumembers: e/pectations about the e/tent of their role in clinical decision making andinvolvement in daily decisions about the care of their family?wh@nau member.evertheless, the reCuirement to consult should ensure the medical practitioner or
responsible clinician makes more informed decisions.
Where family?wh@nau have been consulted to develop a treatment, discharge orrelapse prevention plan in which they will be involved in a person:s continuing care, aclinician may share a copy of the plan with those wh@nau members most closelyinvolved in delivering that care. (his is a permitted disclosure of information for thepurpose for which it was collected. #7
#6 5ee sections 6 and 0# of the Privacy Act "))#.#7 Health 4nformation Privacy 'ode "))2, rule ""%c&.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 21
8/10/2019 Guide to Mental Health Act
28/87
#1 ho must consult5ection 6A places the reCuirement to consult clearly and directly on the medicalpractitioner or responsible clinician. However, other clinical staff %such as a DA-, caremanager or cultural worker& may, because of a pre e/isting relationship with thepatient or proposed patient and family?wh@nau, have important roles in facilitating theconsultation.
#2 ho to consult
#2#1 De"inin+ $"amily= h:nau%
Definitions and understandings of family?wh@nau vary and are informed by differentcultural backgrounds and practices. Almost always, the most important perspective fordefining family?wh@nau is that of the patient or proposed patient.
(he following definition is only one of many possible definitions, but the Ministry ofHealth recommends medical practitioners and responsible clinicians use it to helpavoid confusion and for consistency across the country.
#2#2 8ecommended de"inition
9;amily?wh@nau: means a set of relationships a patient or proposed patient defines asfamily?wh@nau. 4t is not limited to relationships based on blood ties, and may includeany of the following+ the spouse or partner of the patient or proposed patient relatives of the patient or proposed patient a mi/ture of relatives, friends and others in a support network only non relatives of the patient or proposed patient. #)
A patient:s or proposed patient:s definition of family?wh@nau may differ from thisrecommended definition. 4f the patient or proposed patient is competent to decide whotheir family?wh@nau is, then their definition must be accepted.
(he Act reCuires compulsory notifications at various stages of the assessment andtreatment process to welfare guardians and to principal caregivers. 5uch persons
should be regarded as family?wh@nau for the purposes of consultation undersection 6A, in addition to other family?wh@nau members. ote that 9principal caregiver:is more closely defined than family?wh@nau %see ".2 above&.
#2#& /rior competently e7pressed ishes
(here are a number of ways in which a patient or proposed patient may have e/pressedtheir wishes as to who to consult when they become unable to make decisions, what
#) =oyal Australian and ew 3ealand 'ollege of Psychiatrists. *$$$. n#ol#in' amilies>Guidance notes> Guidance for in#ol#in' families and ,h?nau of mental health
consumers5tan'ata ,hai ora in care/ assessment and treatment processes . Wellington+Ministry of Health.
22 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
29/87
treatment they do or do not want in such situations, or who can make decisions ontheir behalf in certain circumstances. (hese include+ crisis or treatment plans %see 5tandard #.0 of the Health and !isa%ility "er#ices
(Core) "tandards @ Continuum of ser#ice deli#ery % 35 7"#2.".#+*$$7& advance directives %see 'ode of Health and Disability 'onsumers: =ights& enduring power of attorney %see Part ) of the Protection of Personal and Property
=ights Act ")77& personal orders under the Protection of Personal and Property =ights Act ")77,
including appointment of a welfare guardian.
'linicians should take steps to give effect to prior competently e/pressed wishes whenreasonably practicable and clinically indicated.
#2# Decidin+ disputed de"initions o" "amily= h:nau4n cases of doubt or dispute, the DAMH5 is responsible for deciding+ whether the patient or proposed patient is sufficiently competent to determine who
is their family?wh@nau who the patient:s or proposed patient:s family?wh@nau is for the purposes of
section 6A.
(he DAMH5 will make this decision based on advice from the responsible clinician,medical practitioner or key worker.
4f the patient or proposed patient identifies as M@ori, the DAMH5 should seek advicefrom M@ori health workers and cultural support staff. (he DAMH5 should consultother knowledgeable parties, for e/ample, the patient:s or proposed patient:s usualgeneral practitioner, key worker, M@ori health worker, kaum@tua, cultural supportstaff, M@ori consumer advisory groups, M@ori advisory committee, other M@oriproviders of services to the patient or proposed patient, or a district inspector.
4n urgent circumstances, the medical practitioner completing sections "$ and "" of the Act is responsible for making this decision for the purposes of the Act.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 2&
8/10/2019 Guide to Mental Health Act
30/87
#& hat consultation is
# De"inition o" $consultation%
4n practical terms, consultation in this conte/t describes a clinical activity, which seeksto engage family?wh@nau in a therapeutic process. 'onsultation is a two way ongoingprocess.
'onsultation does not reCuire the parties to agree and does not reCuire negotiationstowards agreement. However, negotiations and agreement might occur as the tendencyin consultation is for the parties to work towards consensus. 2$
Meaningful consultation has been described by the courts to consist of the followingstages and may occur in a variety of ways, including in person or by phone %including by teleconference&. (he party reCuired to consult+
begins consultation in the formative stages of a process by notifying affected orinterested parties of a proposed %not final& decision or action provides the affected or interested parties with a reasonable amount of time in
which to respond to the notification %which will depend on the urgency of thedecision or action&
may have a working plan in mind that they inform the affected or interested partiesabout, but must keep an open mind and be ready to change or start afresh shouldthat be reCuired
provides the affected or interested parties with a reasonable opportunity to form andstate their views in a safe and open environment
considers properly the representations of the affected or interested parties beforedeciding what will be done
notifies the affected or interested parties of the outcomes of the consultation.
# Decidin+ a'out consultation
A medical practitioner or responsible clinician must consult the patient or proposedpatient to ascertain their views about consultation with family?wh@nau. (hepractitioner or clinician should also give the patient or proposed patient an opportunity to respond to their provisional findings. 4t is important that a medical practitioner orresponsible clinician does not close their mind to alternatives before consultationoccurs.
A patient or proposed patient may refuse permission for a medical practitioner orresponsible clinician to consult family?wh@nau. 4n this situation it is up to thepractitioner or clinician to then decide whether consulting family?wh@nau would be inthe best interests of the patient or proposed patient %see 2.0." below&.
4f the circumstances are urgent, a medical practitioner or responsible clinician muststill consult with the patient or proposed patient to seek their views about the
2$ ellin'ton Airport # Air 0e, ealand "))#I " 3 = 16".
2 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
31/87
consultation. However, given the urgency the clinician may decide it is not in the bestinterests of the patient or proposed patient or not reasonably practicable to consultfamily?wh@nau at that time. (his does not preclude the practitioner or clinician fromcommunicating with the family?wh@nau at the earliest possible opportunity after adecision has been made and before further action is taken.
# Ho to consult
# #1 General comment
A medical practitioner or responsible clinician who consults family?wh@nau must usetheir discretion to decide how much information to disclose to the family?wh@nau. (hepractitioner or clinician must consider how much information the family?wh@nauneeds to make informed and useful responses to the proposed course of assessment ortreatment. (he practitioner or clinician may have a working plan in mind, but must
keep an open mind and be ready to change or start afresh if this is reCuired.
;or consultation to be meaningful it must occur before the medical practitioner orresponsible clinician makes a decision. Discussions after a decision are no longerconsultation but rather information sharing.
'onsulting family?wh@nau as part of the assessment and treatment process is generally ongoing to allow views to change as new information is e/changed. 4f a significantperiod has elapsed or new information has come to light since a consultation, themedical practitioner or responsible clinician should not rely on that consultation butconsult afresh.
;urther consultation may be particularly relevant when the patient moves from thecare of one clinician to another. (he practitioner or clinician should outline the likelychanges and the opportunities family?wh@nau will have to consult the new clinician orattend future meetings or court hearings.
# #2 M:ori
;amily?wh@nau involvement will often be important for M@ori. As a principal source of strength, support, security and identity, wh@nau plays a central role in the wellbeing ofM@ori individually and collectively. (he emphasis the Act places on the individualpatient or proposed patient conflicts with the 9wh@naungatanga: concept ofinterdependence and the interconnectedness between all members of the wh@nau,including the tangata whai ora. 2"
A medical practitioner or responsible clinician should not make decisions about M@oriindividual interests and?or wh@nau interests solely. Whenever possible they shouldinvolve M@ori health workers, kaum@tua, cultural support staff, tangata whai oraadvocacy services, M@ori advisory committees or other M@ori providers of services totangata whai ora.
2" 9(angata whai ora: means 9the one who is seeking wellness:.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 2,
8/10/2019 Guide to Mental Health Act
32/87
(o implement section 6A appropriately and to ensure mental health staff workeffectively with wh@nau, staff may need+ specific training resources appropriate cultural e/pertise support within the organisation.
M@ori do not all share the same views and practices.
8/10/2019 Guide to Mental Health Act
33/87
(o determine a patient:s or proposed patient:s best interests, a medical practitioner orresponsible clinician must consider all relevant clinical or personal information, whichincludes+
the mental state of the patient or proposed patient the patient:s or proposed patient:s competence to make decisions about their care
any advance directives the patient or proposed patient may have made
why the patient or proposed patient wants their family?wh@nau e/cluded
the patient:s or proposed patient:s clinical and family?wh@nau history
any previous contact the patient or proposed patient has had with other mentalhealth service providers
the likelihood of the family?wh@nau having information not available from other
sources.
4f family?wh@nau will be providing the ongoing care of a discharged patient, it willnormally be in the patient:s best interests that family?wh@nau be consulted and havethe appropriate treatment information disclosed to them.
4f the medical practitioner or responsible clinician decides consulting family?wh@nau isnot in the patient:s or proposed patient:s best interests, they must take into accountthat+ they may still seek information from the family?wh@nau
the family?wh@nau may continue to provide information to the practitioner orclinician the family?wh@nau may be given information that was collected for the purpose of
being disclosed to the family?wh@nau the family?wh@nau may be given information if the practitioner or clinician
considers it will prevent a serious threat to the life or health of the patient orfamily?wh@nau members.
#,#2 $8easona'ly practica'le%
(he term 9reasonably: brings a measure of obBectivity to a decision+ with knowledge ofthe same facts, would a reasonable, responsible clinician make the same decisionK
(he term 9practicable: has been considered in other Burisdictions in relation tofamily?wh@nau involvement in mental health care. 2* 4t acknowledges that, for variousreasons, there are circumstances in which we must be content with less than the ideal,and the degree of compromise calls for Budgement and common sense.
(hus when considering whether consultation is 9not reasonably practicable: the medicalpractitioner or responsible clinician needs to consider obBectively whether consultationis feasible. (hey may consider+2* R (on the application of ) # Bristol City Council *$$0I
8/10/2019 Guide to Mental Health Act
34/87
whether the situation is urgent %such as if the patient or proposed patient is acutelyunwell and the clinician needs to act Cuickly&
the time it will take to contact family?wh@nau members as well as the time reCuiredfor family?wh@nau members to form their views
any other disadvantage.
A medical practitioner or responsible clinician needs to balance the disadvantages ofconsultation with the potential benefits to the patient or proposed patient.
;or assessments occurring after hours, the time of day is not necessarily a reason fornot consulting family?wh@nau. An after hours assessment would invariably be anurgent assessment and family?wh@nau consultation may be highly relevant to theimmediate safety and risk issues.
ikewise, resource constraints %such as a lack of clinician time& will rarely of themselves Bustify a 9not reasonably practicable: decision. >rgency combined with resourceconstraints may limit the time available for consultation but will not in most casesmake it 9not reasonably practicable:.
2 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
35/87
, /art 1! The compulsoryassessment process
4f less restrictive mental health interventions have failed, and a person appears to bementally disordered, compulsory assessment under Part " of the Act may beappropriate.
Any person can make an application for assessment under section 7 of the Act,provided they meet the criteria in sections 7A and 7 . However, as the applicationprocess is a comple/ and significant intervention, the Ministry recommends thatanyone concerned about a person:s mental health contact a crisis assessment team andseek the assistance of a duly authorised officer %DA-&. DA-s are appointed to e/ercisecertain powers under the Act relating to the compulsory assessment and treatment ofpeople e/periencing mental health issues in the community. (he Ministry maintains alist of mental health crisis phone numbers on its website. 2#
!uidance relating to the e/ercise of DA- powers, particularly in relation to thecompulsory assessment process, is contained in the Ministry of Health publicationGuidelines for the Role and unction of !uly Authorised $fficers %Ministry of Health*$"*&.
,#1 Threshold "or application "or compulsoryassessment
(he Act reCuires a lower threshold for initial application for compulsory assessment,than for making a compulsory treatment order. >nder section 7 %2&%b& of the Act, a medical practitioner must 9consider that there
are reasona%le 'rounds for believing that the person may %e sufferin' from amental disorder: before issuing a medical certificate to accompany an application forcompulsory assessment.
>nder section "$ of the Act, the medical practitioner issuing a certificate ofpreliminary assessment must consider that there are 9 reasona%le 'rounds for believing that the proposed patient is mentally disordered:.
>nder section "* of the Act, the responsible clinician issuing a certificate of furtherassessment must consider that 9there remain reasona%le 'rounds for believing thatthe patient is mentally disordered:.
2#
www.health.govt.n8?yourhealth topics?health care services?mental health services?crisisassessment teams
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* 29
http://www.health.govt.nz/yourhealth-topics/health-care-services/mental-health-services/crisis-assessment-teamshttp://www.health.govt.nz/yourhealth-topics/health-care-services/mental-health-services/crisis-assessment-teamshttp://www.health.govt.nz/yourhealth-topics/health-care-services/mental-health-services/crisis-assessment-teamshttp://www.health.govt.nz/yourhealth-topics/health-care-services/mental-health-services/crisis-assessment-teams8/10/2019 Guide to Mental Health Act
36/87
efore issuing a certificate of final assessment making an application for acompulsory treatment order under section "2%2&, the responsible clinician mustconsider that a patient 9 is not fit to be released from compulsory status:. ;ollowingaitemata Health , this means that the responsible clinician must believe that thepatient is mentally disordered.
efore a compulsory treatment order can be issued under section *6%"& of the Act,the court must 9consider whether or not the patient is mentally disordered:, andunder section *6%#& if the court considers that the patient is mentally disordered, itmust determine whether or not, having regard to all the circumstances of the case, itis necessary to make a compulsory treatment order.
(he test of 9reasonable grounds for believing: may be derived both from the responsibleclinician:s e/amination of the patient and?or from information given by caregivers,family?wh@nau and third parties.
(he significance of this difference is that whereas there is a high threshold reCuired before a compulsory treatment order can be imposed by the court, including not onlythe presence of mental disorder but also of the necessity of an order, a clinician can actto invoke compulsory assessment on much less certainty. (here is thus the capacity tocompulsorily detain and assess in cases when there is some doubt, but if the assessingclinician feels it is prudent to err on the side of caution.
4f the responsible clinician becomes concerned at any time that there may have beeninsufficient grounds for compulsory assessment, the ne/t stage of the compulsoryassessment process should be undertaken. A new assessment will cure earlier legalflaws if the validity of the patient:s detention is called into Cuestion, 22 thereforepreventing a successful application for a writ of habeas corpus.
22 B # Auc land !HB *$"$I 3'A 1#*G *$""I 3A= "#0.
&3 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
37/87
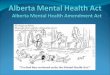
5i+ure 1! Compulsory assessment and treatment
Application formSection 8A
Medical certificateSection 8B
Application for assessmentSection 8
Assessment examinationSection 9
Certificate of preliminary assessmentSection 10
Does patientappear to bementally disordered?
Section 10(1)
Does patientappear to be
mentally disordered?Section 1 (1)
!s t"e patientmentally disordered?
Section 1#(1)
$elease fromcomp%lsory stat%s
&irst period ofassessment andtreatment (fi'e days)
Section 11
Certificate of f%rt"erassessment
Section 1
Second period ofassessment and
treatment (1# days)Section 1
Certificate of finalassessment
Section 1#
Application forcomp%lsory treatment
order
&inal period of assessment and treatmentpendin application (1# days)
Section 1*
+es ,o
+es
+es
,o
,o
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* &1
8/10/2019 Guide to Mental Health Act
38/87
,#2 Applications "or assessment! the role o" dulyauthorised o""icers
A medical certificate under section 7 of the Act must be obtained before an
application for assessment can be completed under section 7A of the Act, although inpractice an application will normally be initiated before a section 7 certificate isissued. -nce an application is made, a duly authorised officer %DA-& may take allreasonable steps to facilitate an assessment e/amination under section 2$%*&%a&.
4f no application for assessment has yet been made, and there are reasonable groundsfor believing a person may be mentally disordered, under section #7%2&%d&%i& a DA- cantake all reasonable steps to take the person to a medical practitioner for an e/aminationif less restrictive options of facilitating a medical e/amination have been e/hausted.
4f necessary, a DA- can under section 2" of the Act reCuest Police assistance to take a
proposed patient to a nominated place for the purposes of an e/amination undersection "$ of the Act. 5ervices should refer to the Memorandum of >nderstanding between the ew 3ealand Police and the Ministry of Health, which provides guidanceto members of the Police and health professionals administering the provisions of the Act, as well as any local agreements made under the Memorandum of >nderstanding.
More detailed guidance about DA- powers can be found in the Ministry of Healthpublication Guidelines for the Role and unction of !uly Authorised $fficers %Ministry of Health *$"*&.
,#& Assessment e7aminations5ection )%"& of the Act states that the DAMH5 or a DA- 9shall make the necessaryarrangements for the proposed patient to undergo an assessment e/aminationforthwith:. (his means that the DAMH5 or DA- must take reasonable steps to act on acompleted application. 5ection )%*& of the Act provides details about thesearrangements. (his includes a reCuirement to give the proposed patient a written noticee/plaining the purpose of the e/amination and detailing the place, time and the personconducting the e/amination %section )%*&%c&&.
(he DAMH5 or DA- may not always be able to perform these functions personally but
must ensure that necessary arrangements are made appropriate to the circumstances,including the urgency of the situation. ;or e/ample, if a medical practitioner is actingunder section ""$ of the Act %powers of medical practitioner where urgent assessment isreCuired&, a phone call to the DA- or DAMH5 is sufficient to decide who will carry outthe assessment and where. (he DA- can ask the medical practitioner to give thesection )%*&%c& notice to the proposed patient and e/plain what is to occur and theirrights %see chapter ""&.
&2 !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
39/87
ote that written information can be given on any paper, not necessarily the usual formused under section ) of the Act. 4n an emergency, the proposed patient should be givenas much detail as practicable, but it may not be practicable to give full written details.(he clinician must make a reasonable Budgement as to how much disclosure ispracticable in the circumstances.
4n making the necessary arrangements for an assessment e/amination undersection )%"& of the Act, a DA- may contact other health services %such as a generalpractitioner& to obtain information relevant to the assessment. (he collection of suchinformation by DA-s, and its disclosure to DA-s by health services, is permitted bylegislation related to information privacy %the Health 4nformation Privacy 'ode "))2,the Privacy Act "))# and the Health Act ")01&. 20
4f the proposed patient is assessed as not being mentally disordered, the DA- and otherclinical staff of the mental health service concerned should take whatever further actionis reCuired to assist the individual who has been assessed. (his assistance will normallyinclude+ the continuing provision of services to a patient who accepts them voluntarily assistance with transport from the place of assessment %if the person has been
transported to the assessment&.
,# ection 9(2)(d) e7planation o" notice o" assessment
4t is mandatory for an e/planation of the purpose of the assessment to take place in thepresence of a support person under section )%*&%d&. While non compliance with thissection has previously resulted in applications for habeas corpus being granted, 21 the'ourt of Appeal has indicated that such a breach is insufficient to warrant nullificationof the assessment process by granting the writ if the assessor has attempted to comply with the reCuirement .26
An assessor must offer to organise the attendance of a support person known to theapplicant, such as a family member, caregiver or friend, if such a person is available. 4fno such person is available, an independent person not involved in the application orassessment and treatment process should be engaged. (his should not be a mentalhealth professional.
20 5ection **; of the Health Act ")01 states that a provider who holds health informationmust disclose that information to another person who is providing or is to provide health ordisability services to a person.
21 eenan # !AMH" *$$1I * 3 = 06*G Chu # !istrict Court at ellin'ton *$$1I 3A=6$6.
26 "estan # !AMH"/ aitemata !istrict Health Board *$$6I " 3 = 616.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* &&
8/10/2019 Guide to Mental Health Act
40/87
Provided this process is undertaken in good faith, it is unlikely to preBudice the validityof the application as other opportunities for clinical and Budicial reassessment areavailable under the Act. 27 4f a proposed patient strongly indicates that they do not wantto comply with the reCuirement, their right to privacy should be respected. 2) Additionally, there may be situations where it would be unsafe to engage a supportperson.
,# ection 9(&) assessment e7amination to 'e conducted 'y amedical practitioner
5ection )%#& of the Act describes the Cualifications necessary to perform an assessmente/amination. (he person must be a medical practitioner who is either a psychiatristapproved by the DAMH5 or, if no psychiatrist is 9reasonably available:, some othermedical practitioner who is 9suitably Cualified: to conduct the assessment e/aminationin the opinion of the DAMH5.
9Psychiatrist: is defined within section * of the Act as 9a medical practitioner whosescope of practice includes psychiatry:. A medical practitioner holding 9scope of practice:in any specialty must have completed vocational training and completed a postgraduate Cualification approved for or relevant to the scope of practice. 0$ =egistrars areregistered in a general scope of practice and do not fall under this definition.
9=easonably available: is not defined within the Act. (he e/pertise that is 9reasonablyavailable: in a well staffed urban centre may be very different to that in a more isolatedrural area. evertheless, some consistency in the matter is e/pected. When consideringthe e/pertise that is 9reasonably available:, the following conte/t should be considered+ who is able to be called the geographical location, or how far away the psychiatrist is the normal duty roster the clinical demands of the situation.
Practically, it may be too onerous for the DAMH5 to consider the comple/ity of allassessments being undertaken, but if a less e/perienced practitioner is assessing a casethat they %or other members of the multidisciplinary team& feel is comple/ orparticularly fraught, the circumstances and appropriateness of the medical practitionerundertaking this assessment should be discussed with a DAMH5.
27 "estan , paragraphs 2*IF 00I.2) "estan , paragraph 02I.0$
Medical 'ouncil. *$"". 95copes of practice:. >= + www.mcn8.org.n8?get registered?scopesof practice %accessed " -ctober *$"*&.
& !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
http://www.mcnz.org.nz/get-registered/scopes-of-practicehttp://www.mcnz.org.nz/get-registered/scopes-of-practicehttp://www.mcnz.org.nz/get-registered/scopes-of-practicehttp://www.mcnz.org.nz/get-registered/scopes-of-practice8/10/2019 Guide to Mental Health Act
41/87
(he Ministry considers situations where a psychiatrist would not be reasonablyavailable might include+ after hours when there is no psychiatrist scheduled on the duty roster %for e/ample
in small DH s where the duty rosters are populated by registrars and Medical
-fficers %5pecial 5cale&& when the psychiatrist is absent for other reasons %such as ill health& and cannot be
replaced by another psychiatrist when the psychiatrist is involved in other urgent work that means they are unable to
attend the assessment in a timely manner and they cannot be replaced by anotherpsychiatrist
when the psychiatrist is too far away to be able to attend the assessment in a timelymanner %for e/ample in DH s which cover a large geographical area&.
Whenever possible %and particularly in the last two e/amples& the medical practitionerconducting the assessment should discuss the particulars of the case over the telephone with the psychiatrist.
95uitably Cualified: is not defined, but as a minimum reCuirement the medicalpractitioner %such as a psychiatric registrar or medical officer& should have at least two years: e/perience in psychiatry. 4n a more difficult case that reCuires a fine degree of Budgement, a more e/perienced senior practitioner with a greater level of e/pertise isneeded.
4t should be kept in mind that the person in charge of a hospital has the power to detaina person at a hospital for a ma/imum period of si/ hours under section ""#%"& of the Act. 4f the proposed patient can be safely detained, it is preferable to detain them untilthe most suitable practitioner becomes available within a si/ hour period.
,#& 8eassessment "ollo in+ release "rom compulsory assessment
5ection "$%#& of the Act notes that a further application under section 7A of the Actmay be made at some time in the future. (here may be circumstances in which afurther application is reCuired very soon after the first assessment. (here is no timelimit specified. A reapplication should be Budged on the clinical and other informationto hand. 4t should take into account the previous assessment made under section "$%#&
of the Act, and the circumstances of the assessment that found the individual not to bementally disordered at that time.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* &,
8/10/2019 Guide to Mental Health Act
42/87
,# 5urther assessment and treatment periods(he first and second periods of assessment and treatment are defined in the Act. (hefirst period of assessment and treatment begins on the date that the patient receives anotice under section ""%"& of the Act and ends when five full days have passed, or earlierif the patient is reassessed for the purposes of section "* of the Act before that date. (hesecond period of assessment begins when a patient receives the notice under section "#of the Act and ends when "2 full days have passed, or earlier if the patient is reassessedfor the purposes of section "2 of the Act before that date. ;ollowing the initialassessment e/amination, all assessment and treatment decisions will be made by theresponsible clinician assigned to the patient by the DAMH5.
oth sections "" and "# of the Act refer to the assessment and treatment periods as9commencing with the date on which the patient receives the notice and ending on theclose of the LLI day after that date:. (he five and "2 day periods should be calculatede/clusive of the day on which the notice is given to the patient. 0" 4t is thereforerecommended that the interpretation in the following e/ample be adopted.
Day $ F (he day on which the notice is given to the patient+ " Eanuary Day 0 F (he end of the fifth day+ 1 Eanuary
(his facilitates the management and appropriate assessment of individuals who receivenotice of the compulsory assessment late in the day.
4f, at any time during the first period %section ""%1&& or second period %section "#%1&&,the responsible clinician considers that the patient is not mentally disordered and istherefore fit to be released from compulsory status, they must be immediately
discharged. 4f there are good clinical reasons for truncating the five or "2 dayassessment periods, it is not necessary to let them run their full course.
,#, ?eave durin+ the assessment and treatmentprocess
5ections ""%0& and "#%0& of the Act enable a responsible clinician to allow a patientsubBect to compulsory inpatient assessment a short period of controlled leave %9trialleave:& in the community, or to allow leave on compassionate grounds %such as toattend a tangi&. 5ection "#%0& also applies when a responsible clinician has made an
application for a compulsory treatment order.
4f the leave is for eight hours or less between 7 am and "$ pm, the Act reCuires it to berecorded %along with the terms and conditions of leave& in the patient:s clinical records%sections ""%0&%a& and "#%0&%a&&. (he patient:s contact details while on leave should also be recorded.
4f overnight leave is granted it must be recorded in the clinical records %as with dayleave&, and the patient and the person in charge of the hospital must be given a writtennotice %sections ""%0&%b& and "#%0&%b&&.
0" Re ! "))1I 3; = 6"#.
&- !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
43/87
(he written notice should include+ the day that leave was granted length of leave when the patient is e/pected to return from leave the patient:s contact details any terms and conditions attached to the leave.
,#- ection 1 ! Certi"icate o" "inal assessment5ection "2%2& of the Act governs the process of applying to the court for a compulsorytreatment order. (he opinion that the patient is not fit to be released from compulsorystatus 0* must be personally formed by the responsible clinician.
An application for a compulsory treatment order should be accompanied by reportsfrom the responsible clinician and other health professionals involved in the care of thepatient. (his facilitates the timeliness of hearings and enables the Budge to determine whether any further information is reCuired before the date for the hearing is set. A Budge is reCuired to consider the evidence of both the responsible clinician and 9at leastone other health professional involved in the case: when deciding whether to make acompulsory treatment order %section "7%2&&.
A second health professional:s evidence should do more than merely address the legalcriteria of the Act. 4t should instead provide a comprehensive global view of thepatient:s health problems. (he second health professional will most often be aregistered mental health nurse. !uidance for nurses on report writing is provided in theew 3ealand 'ollege of Mental Health urses publication Guidelines for Mental
Health 0ursin' Assessment and Reports % 3'MH , Eanuary *$"*& available on the'ollege website %http+??www.n8chmn.org.n8&.
(he responsible clinician must primarily address the criteria for compulsory treatmentunder the Act. (he responsible clinician:s and other health professionals: reportsshould collectively include+ comments on the patient:s history of contact with mental health services, including
severity of illness and response to treatment issues of alcohol and?or drug use previous admissions under the Mental Health Act ")1), Mental Health %'ompulsory
Assessment and (reatment& Act "))*, 'riminal Eustice Act ")70, 'riminalProcedure %Mentally 4mpaired Persons& Act *$$#, 4ntellectual Disability%'ompulsory 'are and =ehabilitation& Act *$$#, or the Alcoholism and Drug Addiction Act ")11
comments on cultural issues %including advice on whether a cultural assessment has been undertaken&
advice on family?wh@nau and social support
0* 5ee Re +B "))2I 3; = 1$.
!uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))* &.
8/10/2019 Guide to Mental Health Act
44/87
proposals for treatment, including information on community services %if applyingfor a community compulsory treatment order&
Bustification of how the patient comes within the definition of 9mental disorder:
any known specific risk issues
issues likely to be challenged in a defended hearing. 0#
-ther relevant material %such as reports prepared for previous hearings& may also beincluded. At this stage it should be determined whether or not the patient will reCuirethe services of an interpreter.
;ollowing the final assessment, the patient may be held for up to "2 days after the timeat which the second period would have e/pired %section "0%"&&. (his means that thema/imum period for which a person can be held for assessment consists of a five dayfirst period, a "2 day second period and "2 day final period, totalling ## days. (his
period may only be e/tended by the order of a court %section "0%*&&.
,#. ection 1-! 8evie 'y a 4ud+e5ection "1 of the Act allows the patient to reCuest a Budge to review the patient:scondition while the assessment process is in progress. 4f the Budge is 9satisfied: that thepatient is fit to be released from compulsory status, the Budge discharges the patientforthwith and brings the process to an end. 4f not, the process of assessment continues.;urthermore, it falls to the person seeking the review and seeking discharge to satisfythe Budge that the patient is fit to be discharged. 4n such a review, the Budge is unlikelyto have available the same amount of evidence as would be obtained at a full hearing.(he process outlined in section "1 of the Act can be invoked at any point after acertificate of preliminary assessment reCuiring further assessment and treatment of thepatient has been issued.
A Budge has limited discretion in deciding whether or not to grant a review of a patient:scondition. A Budge can refuse to grant a review if a patient has had a previous reviewand there is evidence that there has been no change in the patient:s condition%section "1%"'&&.
A Budge is reCuired to consider the evidence of both the responsible clinician and 9at
least " other health professional involved in the case: when determining an applicationfor review %section "1%2&&. (he second health professional will most often be aregistered mental health nurse. !uidance for nurses on report writing is provided at 0.1above and in the ew 3ealand 'ollege of Mental Health urses publication Guidelines for Mental Health 0ursin' Assessment and Reports % 3'MH , Eanuary *$"*&available on the 'ollege website %www.n8chmn.org.n8&.
0# 5tephen Mc'arthy and Dr 5andy 5impson. MayFEune "))1. Runnin' a case under the
Mental Health Act 1992 and related le'islation. Paper presented at ew 3ealand aw5ociety 5eminar, pp "2F"1.
& !uidelines to the Mental Health %'ompulsory Assessment and (reatment& Act "))*
8/10/2019 Guide to Mental Health Act
45/87
- /art 2! Compulsorytreatment orders
A compulsory treatment order is made by a court under section *7 of the Act. 5uch anorder will only be made when a patient is mentally disordered and the court considersthat the order is necessary. (his is the only time at which the necessity of an order isconsidered separately from the Cuestion of whether the person is mentally disordered, but necessity of treatment remains relevant to whether or not a person is mentallydisordered in other conte/ts %see ".* above&.
A compulsory treatment order will be made if the responsible clinician applies to thecourt under section "2%2&, and a ;amily 'ourt Eudge considers that the patient ismentally disordered and that an order is necessary %section *6&. An order will be eithera community treatment order or, if the patient cannot be adeCuat