-
A Guide to Clinical Managementand Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
WHO Western Pacific RegionPUBLICATION
ISBN-13 978 92 9061 525 5
-
A Guide to Clinical Managementand Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
-
[ ii ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
WHO Library Cataloguing in Publication Data
A Guide to clinical management and public health response for
hand, foot and mouth disease (HFMD)
1.Hand,footandmouthdiseaseepidemiology.2.Hand,footandmouthdiseasepreventionandcontrol.
3.Diseaseoutbreaks.4.EnterovirusA,Human.I.RegionalEmergingDiseaseInterventionCenter.
ISBN9789290615255(NLMClassification:WC500)
World Health Organization 2011
All rights reserved.Publications of theWorldHealthOrganization
can be obtained fromWHOPress,WorldHealth
Organization,20AvenueAppia,1211Geneva27,Switzerland(tel.:+41227913264;
fax:+41227914857;e-mail:
[email protected]).RequestsforpermissiontoreproduceortranslateWHOpublicationswhetherforsaleorfor
noncommercialdistributionshouldbeaddressedtoWHOPress,attheaboveaddress(fax:+41227914806;e-mail:
[email protected]).ForWHOWesternPacificRegionalPublications,requestforpermissiontoreproduceshouldbe
addressedtothePublicationsOffice,WorldHealthOrganization,RegionalOfficefortheWesternPacific,P.O.Box2932,
1000,Manila,Philippines,(fax:+6325211036,e-mail:[email protected]).
Thedesignationsemployedandthepresentationofthematerialinthispublicationdonotimplytheexpressionofany
opinionwhatsoeveronthepartoftheWorldHealthOrganizationconcerningthelegalstatusofanycountry,territory,
cityor areaorof its authorities,or concerning thedelimitationof
its frontiersorboundaries.Dotted linesonmaps
representapproximateborderlinesforwhichtheremaynotyetbefullagreement.
Themention of specific companies or of certainmanufacturers
products does not imply that they are endorsed or
recommendedby theWorldHealthOrganization inpreference toothersof
a similarnature that arenotmentioned.
Errorsandomissionsexcepted,thenamesofproprietaryproductsaredistinguishedbyinitialcapitalletters.
All
reasonableprecautionshavebeentakenbytheWorldHealthOrganizationtoverify
the informationcontained in
thispublication.However,thepublishedmaterialisbeingdistributedwithoutwarrantyofanykind,eitherexpressed
orimplied.Theresponsibilityfortheinterpretationanduseofthemateriallieswiththereader.Innoeventshallthe
WorldHealthOrganizationbeliablefordamagesarisingfromitsuse.
-
[ iii ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Contents
Acknowledgements.......................................................................................v
Acronyms.......................................................................................................vi
Introduction...................................................................................................1Developingtheguide.........................................................................................1
Section1:Epidemiology................................................................................31.1Overview......................................................................................................3
1.2Descriptiveepidemiology............................................................................4
1.3Seroepidemiologicalstudy...........................................................................10
Section2:Virology........................................................................................152.1Overview......................................................................................................15
2.2Virusreceptor..............................................................................................18
2.3Recombination..............................................................................................18
2.4ReservoirofEV71.......................................................................................18
Section3:LaboratoryDiagnosis...................................................................213.1Overview......................................................................................................21
3.2Laboratorysafety.........................................................................................21
3.3Clinicalsamples...........................................................................................21
3.4Laboratorydiagnosismethods.....................................................................22
Section4:PathogenesisinEV71Infection...................................................284.1Overview......................................................................................................28
4.2Virusneuro-virulencefactors......................................................................28
4.3Hostfactors..................................................................................................29
4.4Pathologicalfindings....................................................................................30
-
[ iv ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
Section5:ClinicalFeaturesandCaseManagement.....................................355.1Casedefinitions...........................................................................................35
5.2Differentialdiagnosis...................................................................................39
5.3Clinicalassessmentandmanagement........................................................39
Section6:PreventionandControlMeasures...............................................466.1Overview......................................................................................................46
6.2PreventionMeasures:RecommendationsandRationale............................47
6.3FutureConsiderations.................................................................................51
Appendix1:SummaryofepidemiologicfindingsofHFMDfrom
surveillancedatainWesternPacificRegion(since1997)............................54
Appendix2:Benefitsandlimitations
ofspecificpreventionandcontrolmeasures.................................................62
-
[ v ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Acknowledgements
This document was jointly developed by the World Health
OrganizationRegional Office for the Western Pacific and the
Regional Emerging DiseasesIntervention(REDI)Centre.Its
developmentwas coordinated byDr SatokoOtsu, (WHORegionalOffice for
theWestern Pacific) and Dr Zarifah Hussain Reed (REDI Centre) with
support
fromDrChinKeiLee(WHOChina),DrLeVanTuan(WHOVietNam),DrHarpalSingh(WHOMalaysia),andDrWeigongZhou(CentersforDiseaseControlandPrevention,UnitedStatesofAmerica).
The following individuals contributed to chapters as lead
writers, advisers or peerreviewers:
Dr Jane Cardosa, Dr Jeremy Farrar, Dr Feng Zijian, Dr Wakaba
Fukushima,Dr Gao Zifen, Dr Truong Huu Khanh, Ms Keiko Kumatani, Dr
Raymond LinTzer Pin, Dr Tzou-Yien Lin, Dr Ching-Chuan Liu, Dr Peter
Charles McMinn,Dr Lam Yen Minh, Dr Revathy Nallusamy, Dr Nguyen Thi
Hien Thanh,Dr Ooi Mong How, Dr Hiroyuki Shimizu, Dr Tom Solomon, Ms
Maria Takechi,DrPhanVanTu,DrWongKumThong,DrDustinChen-FuYang.
ThanksarealsoduetoDrRuthFoxwellforprovidingtechnicalandeditorialoversight,andMsRhiannonCookforprovidingeditorialadviceandcontributingtothefinalizationofthepublication.
-
[ vi ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
Acronyms
ANS AutonomicnervoussystemBSL BiosafetylevelCA
CoxsackievirusACNS CentralnervoussystemCODEHOP
ConsensusdegeneratehybridoligonucleotideprimerCPE
CytopathiceffectCSF CerebrospinalfluidCT ComputedtomographycAMP
cyclicadenosinemonophosphateECMO
Extra-corporealmembraneoxygenationEV EnterovirusHA HerpanginaHEV
HumanenterovirusH&E HaematoxylinandeosinstainHFMD
Hand,footandmouthdiseaseHLA HumanleukocyteantigenIgM
ImmunoglobulinMIFA IndirectimmunofluorescenceassayIL
InterleukinIVIG IntravenousimmunoglobulinMCP
MonocytechemoattractantproteinMIG
MonokineinducedbyinterferongammaPDE PhosphodiesterasePSGL
HumanP-selectinglycoproteinligandRD HumanrhabdomyosarcomacellsRNA
RibonucleicacidRT-LAMP
Reversetranscriptionloop-mediatedisothermalamplificationRT-PCR
ReversetranscriptionpolymerasechainreactionSCARB
HumanscavengerreceptorclassBSD StandarddeviationUTR
UntranslatedregionVTM Virustransportationmedium
-
[ 1 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Introduction
Hand,footandmouthdisease(HFMD)isacommoninfectiousdiseasecausedby
a group of enteroviruses, including Coxsackievirus A16 (CA16)
andEnterovirus71(EV71). InfectionwithEV71 isofparticularconcernas
itcancauseseverediseaseinchildren,sometimesresultingindeath.Overthelastdecade,manyoutbreaksofHFMDhavebeenreportedincountriesoftheWestern
Pacific Region, including Japan,Malaysia and Singapore, and across
China.The incidence of HFMD, particularly that caused by EV71
infection, appears to
beincreasingacrosstheRegion.Thishaspromptedconcernsthat,withoutintervention,thepublichealthimpactandspreadofthediseasewillcontinuetointensify.
Thispublicationhasbeendevelopedtosupportthetreatment,preventionandcontrolofHFMD.It
is
intendedasaresourceforcliniciansworkingwithHFMDcasesonaregularbasis,aswellaspublichealthpersonnelwhoareresponsibleforpreventingandrespondingtooutbreaksofHFMD.ItdrawsonthemostrecentscientificliteratureandcapturesthecurrentunderstandingandexperiencesofinternationalexpertsworkingonHFMD.
Developing the guide
In2008and2009,epidemiological,diagnosticandclinicalissuesrelatingtoHFMDwerereviewedanddiscussedatthreeinternationalmeetings.Thosemeetingsemphasizedthe
importanceofestablishingstandardizedsurveillancesystems that are
supportedby laboratorydiagnosis,developing investigationand
responsestrategies forHFMDoutbreaks,and furtheringresearch
intothebestclinicalmanagement forHFMD. Inparticular, it was
suggested that standardized case definitions and guidelines
forclinicalmanagementofseverecaseswereneededtoassistintheoverallcontrolandmanagementofEV71-associatedHFMD.
TheWorldHealthOrganization(WHO)WesternPacificRegionalOffice,incoordinationwith
the Regional Emergency Diseases Intervention (REDI) Centre,
subsequentlyorganizedaninformalconsultativemeetingonHFMDinMarch2010inKualaLumpur,Malaysia.Seventeenregionalandinternationalexpertsattendedthemeeting.Findingswere
summarized and recommendations developed in the areas of:
surveillance,epidemiology and burden of disease; characterization
of etiological agents and
-
[ 2 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
transmission; pathogenesis; laboratory diagnosis; clinical
features andmanagement;andpreventionandcontrol.
In July 2010, theREDICentre invited 10 clinicalmanagement
experts to a
furthermeetingonHFMDinSingaporetoreviewthedraftguidancedocumentandconsolidateup-to-dateknowledgeandexperiencesontheclinicalmanagementofHFMDcausedbyEV71.
TheresultingdocumentfromtheabovetwomeetingshasbeenreviewedbyexpertswithinandoutsidetheWesternPacificRegion,andconsensusreachedonthecontentofeachchapter.
The support of all thosewho contributed to development of this
guide is gratefullyacknowledged.
-
[ 3 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Section 1: Epidemiology
1.1 Overview
Many small and large outbreaks associatedwith EV71 infection
have
beenreportedthroughouttheworldsincetheearly1970s(1,2).Childrenhavebeenmostcommonlyaffectedinthoseoutbreaks,andclinicalmanifestationofcaseshasbeenmostlytypicalofHFMD,withfever,skineruptionsonhandsandfeet,andvesiclesinthemouth.However,casesinvolvingthecentralnervoussystem(CNS)and/orpulmonaryoedemahavealsobeenobserved(3).
In the Western Pacific Region, widespread epidemics have been
reported in manycountries,
includingAustralia,BruneiDarussalam,China,
Japan,Malaysia,Mongolia,theRepublicofKorea,Singapore,andVietNam.Severalcountrieshavealsoreportedfatalcases,withsevereCNSdiseaseorpulmonaryoedema.In2009,forexample,anoutbreak
inmainlandChina involved 1 155 525 cases, 13 810 severe cases and
353deaths.
LessisknownregardingthedescriptiveepidemiologyofHFMDorEV71infectionincountriesoutsidetheWesternPacificRegion.AlthoughdozensoffatalitieswithCNSinvolvementwerereportedduringEV71outbreaksinBulgariain1975andHungaryin1978,therehavebeenfewfatalcasesreportedoverthelastthreedecades.Arecentlongitudinal
study fromNorway suggested asymptomatic circulation of EV71 in
thecommunity.
Information regarding the recent seroepidemiology of EV71 in the
Western PacificRegion is limited.A cross-sectional study in
Singapore indicated that, following
thedeclineofmaternalantibodies,theseroprevalenceforEV71increasedatanaveragerateof12%peryearinchildrenfromtwotofiveyearsofage,andreachedasteadystateofapproximately50%inthoseagedfiveyearsorolder.Similarresultsusingthreegroupsofstoredserawerefoundinacross-sectionalstudyperformedinTaiwan(China).TwootherseroepidemiologicalstudiesinTaiwan(China)indicatedthat,followingadecreasein
the circulation of EV71 in the community, an accumulation of
susceptible
youngchildrenmayhavecontributedtothelarge-scaleepidemicthatoccurredtherein1998.
-
[ 4 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
1.2 Descriptive epidemiology
DiseaseassociatedwithEV71infectionwasfirstdescribedbySchmidtandcolleaguesin1974,whoreportedon20patientswithCNSdisease,includingonefatalityinCalifornia,UnitedStatesofAmerica,between1969and1972(1).SubsequentoutbreaksassociatedwithEV71infectionwerereportedinNewYork,UnitedStatesofAmerica,in1972and1977(4-6),Australiain1972-1973and1986(7,8),Swedenin1973(9),Japanin1973and1978(10-13),Bulgariain1975(14,15),Hungaryin1978(16,17),Francein1979(18),HongKong(China)
in1985(19),andPhiladelphia,UnitedStatesofAmerica in1987(20). During
those outbreaks,EV71 caused awide spectrumof diseases,
includingHFMD, aseptic meningitis, encephalitis, paralysis, acute
respiratory symptoms andmyocarditis.
Thoseoutbreaksreportedbetween1974andthemid-1990smaybeclassifiedaseitherbenignorsevereinnature(21).Fortheformer,typicalexamplesincludethelargeoutbreaks
inJapan in1973and1978,
involving3296and36301cases,respectively.Although cases involving
CNS were observed during those outbreaks, including anumberof
fatalities,clinicalmanifestationofcaseswasmostlytypicalofHFMD(10-13).ThatwasalsothecasefortheoutbreakinAustraliain1986,althoughnofatalitieswere
reported (8). Reports of other outbreaks, however, have contained
significantcomponentsofCNSdisease.AlargeepidemicinBulgariain1975,involving705casesandincludingalargenumberoffatalities,wasinitiallythoughttorepresentpoliomyelitisorencephalitisandwasnotcharacterizedasHFMD(14).AsimilarepidemicofacuteCNSdiseaseinHungaryin1978showedthatonlyfourcaseswereclassifiedasHFMDamong323caseswithEV71infection(17)
Inthelate1990s,twowidespreadcommunityoutbreaksassociatedwithEV71infectionoccurred;thefirstinSarawak,Malaysia,in1997,andthesecondinTaiwan(China)in1998,with2628and129106casesreported,respectively(22,23).
Althoughclinicalmanifestations during those outbreaks were mostly
typical of HFMD, a cluster
ofdeathsamongyoungchildrenwasidentified.Caseswithrapidlyprogressiveandfatalpulmonaryoedema/haemorrhagewerealsoobservedforthefirsttime
Numerous Member States in the Western Pacific Region have since
experiencedlargeHFMDepidemics associatedwithEV71 infection. Several
countries have
alsoreportedsubstantialnumbersofdeaths.Thefollowingsectionpresentsthedescriptiveepidemiologyofanumberofthoseepidemics.Inaddition,findingsfromthesurveillancedataofselectedcountriesintheWesternPacificRegionsince1997aresummarizedinAnnex1.
Australia
Between February and September 1999, 14 cases of EV71-associated
neurologicaldiseasewere
identifiedatahospitalduringacommunity-wideoutbreakofHFMDin
-
[ 5 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Perth,WesternAustralia.Twelve(86%)ofthe14childrenwerelessthanfouryearsofage(24).
AnoutbreakofHFMDduetoEV71occurredinSydneyinthesummerof20002001.Approximately
200 children presented to hospital, including nine
patientswithCNSdisease and five with pulmonary oedema. EV71 was
identified in all patients withpulmonaryoedema(25).
Brunei Darussalam
Brunei Darussalam experienced its firstmajor reported outbreak
of EV71 betweenFebruaryandAugust2006. More than1681childrenwere
reportedlyaffected,withthreedeathsresultingfromsevereneurologicaldisease.EV71wasisolatedinsamplesfrom34ofatleast100patientsdiagnosedwithHFMDorherpangina(HA),includingtwopatientswhodiedasaresultofsevereneurologicalcomplications(26).
China
Between March and May 2007, an outbreak of HFMD occurred in
Linyi
City,ShandongProvince,China.By22May2007,1149caseshadbeenreportedthroughacountrywide
disease-reporting system in mainland China. The majority of
thosepatients(84.4%)wereyoungerthanfiveyearsofage.Eleven(0.9%)oftheHFMDcaseswereclassifiedassevere,presentingwithneurologicalcomplications.
Three
(0.3%)children(agedthreeyearsoryounger)diedduringtheoutbreak.Atotalof233clinicalspecimenswere
collected from105 hospitalized patients, including 11
patientswithsevereHFMD.Amongthose,55(52.4%),includingsixseverecases,wereconfirmedtobeEV71infections(27).
Between1Januaryand9May2008,61459HFMDcasesand36deathswerereportedthrough
Chinas disease reporting system. However, prior to 2May 2008,
HFMDwasnotcategorizedasanotifiablediseaseandreportingofHFMDreliedonvoluntaryreportssubmittedbyclinicians.ThenumberofreportedcasesincreasedsharplyafterthediseasewasdesignatedasaclassCnotifiabledisease,withcasesbeingreportedfromnearly
all provinces.The five provinceswith the highest numbers of
reportedcaseswereGuangdong(11374),Anhui(9235),Zhejiang(6134),Shandong(4566)andHenan(3230).Childrenyoungerthanfiveyearsofageaccountedfor92%ofreportedHFMDcases.Among582samplestested,EV71accountedfor54.5%ofcases(28).
More detailed studies of the 2008 outbreakwere reported
fromFuyangCity,AnhuiProvince,where6049caseswere
reportedbetween1March and9May 2008.
Ofthose,353(5.8%)weresevereand22werefatal(casefatalityrate:0.4%).Amongthereportedcases,themale-to-femaleratiowas1.9:1andtheagerangedfrom28daysto18years,with78%ofthecasesbeingthreeyearsofageoryounger.Epidemiologicalinvestigation
revealed no contact between the 22 fatal cases, but
environmentalinvestigationofthehouseholdsofthefatalcasesrevealedpoorhygieneandsanitary
-
[ 6 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
conditions. The
initiallyhighcase-fatalityrate(2.9%(18/610)between1Marchand23April2008)wasattributedto:rapiddiseaseprogression;lateclinicalpresentation;and
limited localmedical capacity. The case-fatality rate decreased
considerably (to0.07% (4/5439) for the period between 24April and
9May 2008) once the
etiologyofthediseasewasknownandearlytreatmentwasprovidedtoseverepatients.Thatwasattributedtoenhancedsurveillanceandimplementationofpreventionandcontrolmeasures(28).Itshouldbenotedthat,duringtheoutbreak(asof2May2008),HFMDwasdesignatedasaclassCnotifiabledisease.
In2009,thenumberofHFMDcasesnotifiedinmainlandChinaamountedto1155525,including13810(1.2%)severecasesand353(0.03%)deaths.Themale-to-femaleratiowas1.8:1.Ofthosecases,93%werefiveyearsofageoryounger,and75%werethreeyearsofageoryounger.ThecaseswerewidelydistributedacrossChinaandincludedbothclinicallydiagnosedandlaboratory-confirmedcases.Forthelaboratory-confirmedcases,EV71wasresponsiblefor41%ofthecases,81%oftheseverecasesand93%ofthedeaths.
Taiwan (China)
In Taiwan (China), HFMD/HA has been included in the national
sentinel-physicianreporting systemsince3March1998due to
theprevalenceofHFMD/HAcases. In1998,129106HFMD/HAcaseswerereported
in twowavesbetween29Marchandtheendoftheyear.
Theyincluded405(0.3%)patientswithseveredisease,mostofwhomwerefiveyearsofageoryounger.Seventy-eight(19.6%)patientswithseverediseasedied,71(91%)ofthemfiveyearsofageoryounger.Ofthepatientswhodied,65(83%)hadpulmonaryoedemaorpulmonaryhaemorrhage.EV71wasfoundin44of59(75%)isolatesfrompatientswithsevereinfectionswhosurvived,while34of37(92%)isolatesfrompatientswhodiedwerepositiveforEV71(23).Furthersmalleroutbreaksoccurredin2000and2001,involving291and389severecasesand41and55fatalities,respectively
(41). Sentinel physician surveillance data for 2000 and 2001
indicatedsimilar levels of diseasewere caused byCA16 andEV71 (17.1%
and 18.2% versus15.5%and15%,respectively).
EV71wasassociatedwith47.3%(26/545)ofcasesin2000andwasthedominantstrainassociatedwithfatalitiesin2001(25/41,61%).
Between1998and2005,thenumberofsevereHFMD/HAcasesperyearrangedfrom35to405.Ofthe1548severecasesidentifiedduringtheeight-yearperiod,93%werefouryearsofageoryounger,and75%weretwoyearsofageoryounger.Themale-to-femaleratiowas1.5:1.Atotalof245fatalcaseswerereportedduringthesameperiod.EV71positivityratesamongthefatalcasesrangedfrom11%to100%ineachyear(42-44).Thenumberofseverecasesanddeaths,respectively,were:11and0in2006;12and2in2007;373and14in2008;and29and2in2009.
-
[ 7 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Japan
Approximately2400paediatricclinicsparticipatedinthesentinelsurveillancesystemin
Japan between 1993 and 1998,with an average of 36.5 cases ofHFMD
reportedper sentinel site annually (29). Since 1999, approximately
3000 paediatric
clinicshaveparticipatedinthesentinelsurveillancenetwork,withanaverageof42.7casesofHFMD
reported per sentinel site between1999 and 2005.Large-scale
outbreaksoccurredin2000and2003,withthenumbersofreportedcases(casespersentinelsite)205365(68.96)and172659(56.78),respectively.Approximately90%oftheHFMDcaseswereagedfiveyearsofageoryounger(30).
HFMD is also included in the InfectiousAgentsSurveillance system
in Japan. TheInfectious Agents Surveillance reports are derived
from approximately 10% of
thesentinelclinicsandallthesentinelhospitalsinthenetwork.EV71wasfoundtobetheprimary
causative agentofHFMDepidemics inboth2000and2003 (30).
AlthoughthereisnosurveillancesystemforsevereorfatalcasesofHFMDinJapan,suchcaseshavebeenidentifiedthroughcase-seriesfromhospitalsduringepidemicperiodsinthecommunity.
In1997, threedeathsofyoungchildren fromHFMDorEV71
infectionwereidentifiedinOsakaprefecture(30).Inthesummerof1997,12patients,agedtwoweeks
to six years,with serologically confirmedEV71 infections,were
hospitalizedin Otsu city as a result of CNS involvement (31).
Between June and August 2000,30 caseswithHFMD complicated byCNS
involvementwere hospitalized
inHyogoprefecture.Onepatientagedtwoyearsdiedasaresultofpulmonaryoedemacausedbybrainstemencephalitis.EV71was
isolated fromnine (69%)of 13 faecal
samples,includingasamplefromthefatalcase(32).Anationwidequestionnairesurveyfound272complicatedcaseswithHFMDduringtheperiod2000-2002.Ofthese,226casesoccurredin2000,32in2001,and14in2002.Therewerefourcasesinvolvingsequelaeandonefatalcasereportedin2000(52).
Malaysia
InSarawak,Malaysia,awidespreadcommunityoutbreakofHFMD,primarilycausedbyEV71infection,beganinearlyApril1997.From1Juneto30August1997,atotalof2628caseswerereportedtotheSarawakStateDepartmentofHealth.Duringtheoutbreak,889childrenwerehospitalized,including39patientswithasepticmeningitisoracuteflaccidparalysis.
Atotalof29previouslyhealthychildrenyoungerthansixyearsofage(median,1.5years;range,0.55.9years;male-to-femaleratioof1.9:1)diedofrapidlyprogressivecardiorespiratoryfailure.EV71wasisolatedinsamplesfromsixofthefatalcases(22).Laterin1997,anoutbreakinvolving4625hospitaladmissionsoccurredinpeninsularMalaysia,resultingin11fatalcases(35).
AsentinelsurveillanceprogrammeforHFMDwassubsequentlyestablishedinSarawakinMarch1998.BetweenMarch1998andJune2005,4290specimenswerecollectedfrom
2950 children, with a male-to-female ratio of 1.4:1. During that
period, two
-
[ 8 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
largeoutbreakswereidentifiedinSarawak,in2000and2003.EV71wasthedominantenterovirus
serotype of the isolates in both years (36). The sentinel
surveillanceprogrammeinSarawakisongoing,withtwomoreoutbreaksidentified:thefirstin2006andthesecondin2008/2009.
Mongolia
OfficialreportingofHFMDinMongoliabeganin2008,with3210casesreportedduringthatyear.Caseswereequallydistributedbetweenthecapitalcityandtheprovinces.Amongthe245samplesinvestigated,102(41.6%)werepositiveforEV71(37).
Republic of Korea
TheincidenceofHFMD/HAincreasedintheRepublicofKoreaduring2000,withanoutbreakofHFMD/HAinChejuProvince.WhiletheactualnumberofcasesofHFMD/HAisunknown,nofatalitywasassociatedwiththeoutbreak(33).
AsentinelsurveillancesystemforEVinfectionwasinitiatedin2005.BetweenJanuary2008and30October2009,719suspectedcasesofHFMDorHA(200casesin2008and519casesin2009)wereidentified,includingonefatalcaseresultingfromsevereneurological
complications and two cases resulting in a comatose
state.Enteroviruswasdetectedin447(62.2%)cases.Ofthose,enteroviralgenotypewasidentifiedin218cases(53casesin2008and165casesin2009).In2008,themostcommonpathogendetectedwasCA10
(18 cases; 34.0%),while, in 2009,EV71was themost
commonpathogendetected(91cases;55.2%)(34).
Singapore
AlargeepidemicofHFMDcausedbyEV71infectionoccurredinSingaporebetweenSeptemberandOctober2000,with3790casesreportedandthreedeaths.Ofthe104patientswhowereclinicallydiagnosedwithHFMDandwhosesamplesyieldedatleastonevirus,EV71wasthemostcommonlyisolatedvirus(73%)(38).
ReportingHFMDsubsequentlybecamemandatoryinOctober2000.Intheseven-yearperiodfrom2001through2007,nationwideepidemicsofHFMDwereobservedin2002(16228reportedcases),2005(15256reportedcases),2006(15282reportedcases)and2007(20003reportedcases).Theage-specificannualincidenceratewashighestin
those aged 04 years, ranging from1640.5 to 5975.5 per 100 000
population
andaccountingfor62.2%to74.5%ofreportedcases.DuringtheEV71-associatedHFMDepidemicinMarchandApril2006,1.8%ofthecaseswerehospitalized.Thatratewasmorethantwiceashighas
inthoseepidemicscausedbyCA16(betweenMarchandApril2005,0.8%ofcaseswerehospitalized,andbetweenAprilandMay2007,0.7%ofcaseswerehospitalized).
-
[ 9 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
InasmalleroutbreakinJanuaryandFebruary2001,5187caseswerereported,includingthreeHFMD-associateddeaths.Ofthefatalcases,onewasagedfouryears,whiletheothertwowereboth11monthsofage(39).
BetweenlateMarchandMay2008,anationwideepidemicofEV71-associatedHFMDoccurred.Inthefirst24weeksof2008,thenumberofreportedHFMDcaseswas15030,atwo-foldincreasecomparedwiththesameperiodin2006(themostrecentEV71-associatedepidemicpriorto2008).Fortheepidemicperiodfromweek8toweek24in2008,EV71constituted33.2%ofthesamplestested.EV71positivitywassignificantlyhigherduringthe2008epidemicperiodthanin2006(40).
Viet Nam
InsouthernVietNam,anoutbreakofacuteencephalitisassociatedwithHFMDwasreportedinHoChiMinhCityin2003.In2005,764childrenwerediagnosedwithHFMDinHoChiMinhCitythroughsentinelsurveillanceatthelargestpaediatrichospital,withmostcases(96.2%)beingfiveyearsofageoryounger.AllpatientsprovidedspecimensandHEVwas
isolated from 411 patients. Of those, 173 (42.1%)were identified
asEV71,and214(52.1%)asCA16.OfthosepatientswithEV71infections,51(29.3%)werecomplicatedbyacuteneurologicaldiseaseandthree(1.7%)werefatal(45).
In20062007,sentinelsurveillanceatthesamehospitalreported305casesdiagnosedas
neurological disease, of which 36 cases (11%), and three deaths
(0.01%), wereassociatedwithEV71.
In2007,2008and2009, thenumbersofreportedand
fatalcaseswere:5719and23,10958and25,and10632and23,respectively.Themajorityofthecaseswereinthesouthernpartofthecountry.
In northern Viet Nam, EV71/C4 has only been identified in one
patient with acuteencephalitis since 2003. Between 2005 and 2007,
EV71/C5 was identified in
sevenpatientswithacuteflaccidparalysis.Allcaseswereunderfiveyearsofage.During2008,88casesofHFMDwerereportedfrom13provinces.Theresultsofvirusisolationfromthe88casesconfirmedthat33
(37.5%) isolateswereenterovirus-positive,
includingnine(27.3%)withEV71,23(69.7%)withCA16,andonewithCA10.Nosevereorfatalcaseswerereported.Themajorityofcaseswereunderfiveyearsofage.
Countries outside the Western Pacific Region
Less is known regarding the descriptive epidemiology of HFMD or
EV71 infectionin countries outside theWestern Pacific Region. In
TheNetherlands, only
severe,hospitalizedcasesofEV71infectionarereportedaspartof
thenationalsurveillancesystem.Whilebetween1963and2008therewasnoindicationofEV71-relatedfatalities,58casesofEV71infectionrequiringhospitalizationwerereportedin2007aftera21-yearperiodoflowendemicity(46).
-
[ 10 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
In the United Kingdom, there is evidence of continuous
circulation of EV71,
withEV71isolatedeachyearfrom1998to2006,exceptfor2003.Of32patientswithEV71infectionaccompaniedbyneurologicalcomplicationsand/orcutaneousmanifestationsduringthateight-yearperiod,onehadfatalencephalitis(47).
AlongitudinalstudyfromNorway,conductedbetweenSeptember2001andNovember2003,indicatedasymptomaticcirculationofEV71.Atotalof113healthyinfantsfromtheageofthreemonthswererecruitedtoprovidemonthlystoolsamplesandclinicaldataupuntiltheageof28months.PrevalenceofEV71instoolsamplesshowedthatEV71wascirculatingwidelybetweenOctober2002andOctober2003.However,datafromasurveillance/registersystemshowednocorrespondingincreaseinthenumberofhospitalizedpatientswithencephalitis,HFMDorHAwithintheagegroupduringthesameperiod(48).
1.3 Seroepidemiological study
Recent data regarding the seroepidemiology of EV71 in theWestern
Pacific
Regionarelimited.InSingapore,aserologicalsurveywasconductedatapaediatricclinicattheNationalUniversityHospitalthatincludedallchildrenbornatthehospitalorthoseaged12yearsoryoungerbroughtforroutinevisitsandvaccinationsbetweenJuly1996andDecember1997,givingatotalof856children.Antibodyprevalenceincordbloodsuggestedthat44%ofmothershadantibodiestoEV71.NoneofthechildrentestedhadmaternalantibodiestoEV71afteronemonth,andantibodieswerefoundinonlyoneofthe124samplesfromchildrenaged1-23months.Inchildrenagedfromtwotofiveyears,theseropositiverateincreasedatanaverageof12%peryear.Insamplesfromchildrenfiveyearsofageandolder,theage-specificseroprevalencesteadiedatapproximately50%(49).
Anothercross-sectionalstudycarriedoutinTaiwan(China)examinedseroprevalenceratesforEV71byusingamicro-neutralizingassaytotestthreegroupsofstoredseracollectedin1994,1997and1999.Regardlessoftheperiodfromwhichthespecimensweretaken,theseropositiverateswererelativelyhigh(38%-44%)ininfantsyoungerthan
sixmonthsof age. The rates declined to 0%-15% in infants
age7-11months,increasedgraduallythereafteruntiltheageofsix,andreachedaplateauatabout50%inchildrenolderthansixyearsofage(50).
Two seroepidemiological studies have contributed to the
understanding of
factorsunderlyingtheHFMDoutbreakinTaiwan(China)in1998.Inacross-sectionalstudy,neutralizing
antibodies toEV71were assayed for 539 subjectswho provided
serumsamples for vaccine trials or health examinations in
twohospitals between July andDecember 1997. Age-specific
EV71-seropositive rates before the outbreak
wereinverselyrelatedtoage-specificmortalityratesandsevere-caseratesinthecommunityduringtheoutbreak(r=-0.82and-0.93,respectively)(51).Alongitudinalstudywasalsoconductedusingserumsamplesfromabirthcohortstudyof81healthychildren
-
[ 11 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
whoprovidedyearlybloodsamplesbetween1988and1998.Thestudyfoundthattheyearly
incidence ofEV71 seroconversionwas 3%-11%between 1989 and 1997,
andthat68%of childrenhad serological evidenceofEV71
infectionby1997. However,comparedwith previous years, the
seroconversion rate forEV71was relatively
lowbetween1994and1997.TherarityofEV71infectionbetween1994and1997suggestsdecreasedcirculationofEV71inthecommunity.Anaccumulationofsusceptibleyoungchildrenmaythereforehavecontributedtothe
large-scaleepidemicthatoccurredin1998(44,50).
References
1.
SchmidtNJ,LennetteEH,HoHH.Anapparentlynewenterovirusisolatedfrompatientswith
diseaseofthecentralnervoussystem.JournalofInfectiousDiseases,1974,Mar,129(3):304
309.
2.
SolomonT,etal.Virology,epidemiology,pathogenesisandcontrolofenterovirus71.Lancet
InfectiousDiseases,2010,10(11):778790.
3. Ooi MH, et al. Clinical features, diagnosis and management of
human enterovirus 71
infection.LancetNeurology,2010,9(11):10971105.
4.
DeibelR,GrossLL,CollinsDN.Isolationofanewenterovirus(38506).Proceedingsofthe
SocietyforExperimentalBiologyandMedicine,1975Jan,148(1):203207.
5. ChonmaitreeT, et al. Enterovirus 71 infection: report of an
outbreakwith two cases of
paralysisandareviewoftheliterature.Pediatrics,1981,Apr,67(4):489-493.
6. Goldberg F, Weiner LB. Cerebrospinal fluid white blood cell
counts and lactic acid
dehydrogenaseinEnterovirustype71meningitis.ClinicalPediatrics(Philadelphia),1981,
May,20(5):327-330.
7.
KennettML,etal.Enterovirustype71infectioninMelbourne.BulletinoftheWorldHealth
Organization,1974,51(6):609-615.
8. GilbertGL,etal.Outbreakofenterovirus71 infection
inVictoria,Australia,withahigh
incidenceofneurologicinvolvement.PediatricInfectiousDiseaseJournal,1988,Jul,7(7):484-
488.
9. Blomberg J, et al. Letter: New enterovirus type associated
with epidemic of aseptic
meningitisand-orhand,foot,andmouthdisease.Lancet,1974,Jul13,2(7872):112.
10. Tagaya I, Tachibana K. Epidemic of hand, foot and mouth
disease in Japan, 19721973:
differenceinepidemiologicandvirologicfeaturesfromthepreviousone.JapaneseJournal
ofMedicalScienceandBiology,1975,Aug,28(4):231234.
11. HagiwaraA,TagayaI,YoneyamaT.Epidemicofhand,
footandmouthdiseaseassociated
withenterovirus71infection.Intervirology,1978,9(1):6063.
-
[ 12 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
12. Ishimaru Y, et al. Outbreaks of hand, foot, and mouth
disease by enterovirus 71. High
incidence of complication disorders of central nervous system.
Archives of Disease in
Childhood,1980,Aug,55(8):583588.
13.
TagayaI,TakayamaR,HagiwaraA.Alarge-scaleepidemicofhand,footandmouthdisease
associated with enterovirus 71 infection in Japan in 1978.
Japanese Journal of Medical
ScienceandBiology,1981,Jun,34(3):191196.
14. Shindarov LM, et al. Epidemiological, clinical, and
pathomorphological characteristics
of epidemic poliomyelitis-like disease caused by enterovirus 71.
Journal of Hygiene,
Epidemiology,MicrobiologyandImmunology,1979,23(3):284295.
15. Chumakov M, et al. Enterovirus 71 isolated from cases of
epidemic poliomyelitis-like
diseaseinBulgaria.ArchivesofVirology,1979,60(3-4):329340.
16. WorldHealthOrganization.Virusdiseasessurveillance,1979.
17.
NagyG,etal.Virologicaldiagnosisofenterovirustype71infections:experiencesgained
duringanepidemicofacuteCNSdiseasesinHungaryin1978.ArchivesofVirology,1982,
71(3):217227.
18.
WorldHealthOrganization.Enterovirustype71surveillance,1979.
19. Samuda GM, et al. Monoplegia caused by Enterovirus 71: an
outbreak in Hong Kong.
PediatricInfectiousDiseaseJournal,1987,Feb,6(2):206-208.
20.
HaywardJC,etal.Outbreakofpoliomyelitis-likeparalysisassociatedwithenterovirus71.
PediatricInfectiousDiseaseJournal,1989,Sep,8(9):611616.
21. HoM. Enterovirus 71: the virus, its infections and
outbreaks. Journal of Microbiology,
ImmunologyandInfection,2000,Dec,33(4):205216.
22.
ChanLG,etal.Deathsofchildrenduringanoutbreakofhand,foot,andmouthdiseasein
Sarawak,Malaysia:clinicalandpathologicalcharacteristicsofthedisease.FortheOutbreak
StudyGroup.ClinicalInfectiousDiseases,2000,Sep,31(3):678683.
23.
HoM,etal.Anepidemicofenterovirus71infectioninTaiwan.TaiwanEnterovirusEpidemic
WorkingGroup.NewEnglandJournalofMedicine,1999,Sep23,341(13):929935.
24.
McMinnP,etal.Neurologicalmanifestationsofenterovirus71infectioninchildrenduringan
outbreakofhand,foot,andmouthdiseaseinWesternAustralia.ClinicalInfectiousDiseases,
2001,Jan15,32(2):236242.
25. Nolan MA, et al. Survival after pulmonary edema due to
enterovirus 71 encephalitis.
Neurology,2003,May27,60(10):16511656.
26.
AbuBakarS,etal.Enterovirus71outbreak,Brunei.EmergingInfectiousDiseases,2009,
Jan,15(1):7982.
-
[ 13 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
27.
ZhangY,etal.Anoutbreakofhand,foot,andmouthdiseaseassociatedwithsubgenotype
C4 of human enterovirus 71 in Shandong,China. Journal
ofClinicalVirology, 2009,Apr,
44(4):262-267.
28. Report on the hand, foot, and mouth disease in Fuyang City,
Anhui Province and the
preventionandcontrolinChina.Beijing,ChineseCenterforDiseaseControlandPrevention
andtheofficeoftheWorldHealthOrganizationinChina2008.
29.
TaniguchiK,etal.OverviewofinfectiousdiseasesurveillancesysteminJapan,1999-2005.
JournalofEpidemiology,2007,Dec,17Suppl:S313.
30. Hand, foot andmouth disease, 2000-2003, Japan.
InfectiousAgents SurveillanceReport.
200425(9):224225.
31.
KomatsuH,etal.OutbreakofsevereneurologicinvolvementassociatedwithEnterovirus
71infection.PediatricNeurology,1999,Jan,20(1):1723.
32.
FujimotoT,etal.Outbreakofcentralnervoussystemdiseaseassociatedwithhand,foot,and
mouthdiseaseinJapanduringthesummerof2000:detectionandmolecularepidemiologyof
enterovirus71.MicrobiologyandImmunology,2002,46(9):621627.
33.
JeeYM,etal.GeneticanalysisoftheVP1regionofhumanenterovirus71strainsisolated
inKoreaduring2000.ArchivesofVirology,2003,Sep,148(9):17351746.
34. RyuWS, et al. Clinical and etiological characteristics of
enterovirus 71-related diseases
duringarecent2-yearperiodinKorea.JournalofClinicalMicrobiology,2010,Jul,48(7):2490
2494.
35.
ShekharK,etal.Deathsinchildrenduringanoutbreakofhand,footandmouthdiseasein
PeninsularMalaysia-clinicalandpathologicalcharacteristics.Medical
JournalofMalaysia,
2005,Aug,60(3):297304.
36.
PodinY,etal.Sentinelsurveillanceforhumanenterovirus71inSarawak,Malaysia:lessons
fromthefirst7years.BMCPublicHealth,2006,6:180.
37. Report of the Second Meeting on Vaccine Preventable Diseases
Reference Laboratory
NetworksintheWesternPacificRegion.22-26February2010,Manila,Philippines.Manila,
WHORegionalOfficefortheWesternPacific,2010
38. ChanKP,etal.Epidemichand,
footandmouthdiseasecausedbyhumanenterovirus71,
Singapore.EmergingInfectiousDiseases,2003,Jan,9(1):7885.
39.
AngLW,etal.Epidemiologyandcontrolofhand,footandmouthdiseaseinSingapore,2001-
2007.Annals,AcademyofMedicine,Singapore,2009,Feb,38(2):106112.
40.
Epidemiologicalnewsbulletin,MinistryofHealth,Singapore.2008,34(4).
41. Lin TY, et al. Enterovirus 71 outbreaks, Taiwan: occurrence
and recognition. Emerging
InfectiousDiseases,2003,Mar,9(3):291293.
42.
ChenKT,etal.Epidemiologicfeaturesofhand-foot-mouthdiseaseandherpanginacaused
byenterovirus71inTaiwan,1998-2005.Pediatrics,2007,Aug,120(2):e244252.
-
[ 14 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
43.
ChenSC,etal.Aneight-yearstudyofepidemiologicfeaturesofenterovirus71infectionin
Taiwan.AmericanJournalofTropicalMedicineandHygiene,2007,Jul,77(1):188191.
44.
ChangLY.Enterovirus71inTaiwan.PediatricsandNeonatology,2008,Aug,49(4):103112.
45. TuPV, et al.Epidemiologic and virologic investigation of
hand, foot, andmouth disease,
southernVietnam,2005.EmergingInfectiousDiseases,2007,Nov,13(11):17331741.
46.
vanderSandenS,etal.Epidemiologyofenterovirus71intheNetherlands,1963to2008.
JournalofClinicalMicrobiology,2009,Sep,47(9):28262833.
47. BibleJM,etal.Molecularepidemiologyofhumanenterovirus71
intheUnitedKingdom
from1998to2006.JournalofClinicalMicrobiology,2008,Oct,46(10):31923200.
48.
WitsoE,etal.AsymptomaticcirculationofHEV71inNorway.VirusResearch,2007,Jan,
123(1):1929.
49.
OoiEE,etal.Seroepidemiologyofhumanenterovirus71,Singapore.EmergingInfectious
Diseases,2002,Sep,8(9):995997.
50. Lu CY, et al. Incidence and case-fatality rates resulting
from the 1998 enterovirus 71
outbreakinTaiwan.JournalofMedicalVirology,2002,Jun,67(2):217223.
51. Chang LY, et al. Risk factors of enterovirus 71 infection
and associated hand, foot, and
mouthdisease/herpanginainchildrenduringanepidemicinTaiwan.Pediatrics,2002,Jun,
109(6):e88.
52.SuzukiY,etal.Riskfactorsforseverehandfootandmouthdisease.PediatricsInternational
2010Apr;52(2):2037
-
[ 15 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Section 2: Virology
2.1 Overview
ThemajoretiologicalagentsthatcauseHFMDarethehumanenterovirusesspeciesA(HEV-A),particularlycoxsackievirusA16(CA16)andenterovirus71(EV71).
Thesebelong to the genus Enterovirus within the family
Picornaviridae. Other
HEV-Aserotypes,suchasCoxsackievirusA6andCoxsackievirusA10,arealsoassociatedwithHFMDandherpangina.
While all these viruses can causemild disease in
children,EV71hasbeenassociatedwithneurologicaldiseaseandmortalityinlargeoutbreaksintheAsiaPacificregionoverthelastdecade(14).
Enteroviruses are small viruseswith virions that are about 30 nm
in diameter
andcomposedoffourstructuralproteinscalledVP1,VP2,VP3andVP4.VP1isthemajorcapsidproteinonthesurfaceofthevirion,whileVP4isnotexposedonthesurface.Serotypingofhumanenteroviruseshastraditionallybeenbasedonneutralizationtestsusing
specific antiserum pools: as such they are directed particularly at
serologicalresponsestotheVP1protein.Morerecently,dueinparttolimitedaccesstoserotypingantisera
and improved accessibility tomolecular technology, there has been
amovetowardsusingmoleculartypingmethods.ThegeneencodingVP1isthetargetgenemostoftenusedinmoleculartypingmethodsforenteroviruses.
It isforthisreasonthat a wealth of genetic sequence data on EV71 is
available, enabling the
geneticclassificationofvirusstrainsincommoncirculation(57).
Ribonucleic acid (RNA) viruses, such as the enteroviruses,
generate
evolutionarychangesfairlyrapidly.Labels(genogroups)canbeappliedtoclustersofepidemiologicallyrelatedEV71strains,generallythosewithuptoa5%nucleotidedifferenceintheVP1region.
These genogroup divisions have no known significance for any
enterovirusotherthanbeingaconvenientlabeltoreflectviralsequenceclusteringwithinaseaofgeneticdiversity.ItisimportanttonotethatthereisnotyetevidenceofanyassociationbetweenvirulenceandparticulargenogroupsorsubgenogroupsofEV71.
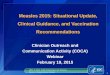
Figure 1 on the succeeding page shows a phylogenetic tree
containing the
threegenogroupsofEV71:genogroupsA,BandC.TheprototypeEV71virusisBrCr,isolatedinCaliforniain1969.ThisistheonlysampledvirusofgenogroupA(8).
-
[ 16 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
Figure 1: Circulating genotypes of HEV71 between 1970 and
2010
HEV71 - circulating genotypes, 1970 - present
White Dendrograms:Worldwide, 1970-1995*C1 has continued to
circulate in the Asia-Pacific region to the presentColoured
Dendrograms:Asia-Pacific, 1997-present
A (BrCr)
C1* Singapore 2000, Sarawak WA 2001 & 2005, Vietnam 2005
C2 Taiwan 1998 WA 1999
C3 Korea 2000
C4 China & Korea, 2004, Vietnam 2005
C5 Vietnam, 2005-06
B1
B2
B3 1997-99
B4 2000-01
B5 2003,2006
B6 2006
Southeast Asia
1997-2006
SubgenogroupB1wascirculatingintheUnitedStatesofAmerica,Europe,JapanandAustraliainthe1970s,whilesubgenogroupB2wassampledmainlyintheUnitedStatesinthe1980s.In1997,whenthefirstofseveralrecentandlargeAsiaPacificoutbreaksofEV71occurredinSarawak,Malaysia,themajorcirculatingviruswasaBgenogroupvirus
thatwas clearlydistinct from thegenogroupBviruses
thathadbeensampledinthe1970sand1980s.ThiswasthennamedsubgenogroupB3.TheviruswasalsofoundintheMalaysianpeninsulaandinSingapore(1,2).
In1998, another largeoutbreakofEV71HFMDoccurred in
theAsiaPacific
region,thistimeinTaiwan(China).ThemajorcirculatingviruswasfromsubgenogroupC2.ThissubgenogrouphadalsobeenfoundinJapanandwasassociatedwithanoutbreakinPerth,WesternAustralia,in1999,wheregenogroupB3viruseswerealsocirculating.InTaiwan(China)in1998,subgenogroupB4viruseswerealsosampledand,by2000,thoseviruseshadbeenassociatedwithlargeoutbreaksthroughouttheregion,includinginJapan,MalaysiaandSingapore,aswellasinTaiwan(China),wheresubgenogroupB4virusesreplacedtheC2viruses.InSarawak,Malaysia,subgenogroupB4wasreplacedbysubgenogroupB5in2003,andthishassinceremainedthedominantsubgenogroup.SubgenogroupB5virusesarealsoimportantcirculatingvirusesinJapan,SingaporeandTaiwan(China)(13,921).
-
[ 17 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
SubgenogroupC1 viruseswere sampled inNorth America in the 1970s
and
1980s.Throughoutthe1990s,anduptothepresentday,theyhavebeenconsistentlyidentifiedinmanypartsoftheworld,includinginAustralia,Japan,Malaysia,NewZealand,Norway,ThailandandtheUnitedKingdom,Despitebeingfoundincirculationinmanycountries,however,thesubgenogroupC1viruseshavenotcausedlargeoutbreaksduringthelasttwodecades.ThesubgenogroupC2virusesthatwerereplacedbyB4virusesinTaiwan(China)by2000havecontinuedtobeidentifiedinJapan,SingaporeandThailandoverthelastfewyears.
VietNambegan investigatingEV71 in2005. It is interesting tonote
that,
althoughC1andC4virusesdocirculateinVietNam,thedominantsubgenogrouphasbeen,andremains,C5(22).ThatsubgenogroupemergedinTaiwan(China)in2006.
AsimilarsituationexistsinChina,wherethesingledominantsubgenogroupC4causedmajoroutbreaksin2008and2009(23,24).ThatsubgenogroupwassampledinChinaandJapaninthelate1990sandearly2000sandwasdominantinTaiwan(China)in2004and2005.It
iscurrentlycirculatinginJapan,theRepublicofKorea,Taiwan(China),ThailandandVietNam.TheRepublicofKorearecordedasubgenogroupC3clusterofcasesin2000,whenB4virusesweredominantelsewhereintheregion(25).
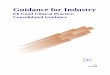
Figure2illustratesthetemporaldistributionofthedifferentsubgenogroupsofEV71circulating
in various countries in the region. The figure includes data
generatedfollowing the enhanced surveillance activities in
operation in many countries
since1997.Itisthereforeimportanttonotethattherearegapsintheknowledgeregardingcirculatingstrainspriortothatperiod.
Figure 2: Recorded prevalence of EV71 subgenogroups in the
Asia-Pacific region
AreaYear
1970s 1980 s 1990s 2000 -2004 2005 -2009
Malaysia
Taiwan
Australia
Japan
Singapore
China
Vietnam
Korea
Mongolia
Thailand
New Zealand
Area-
B1 C2 C4B2
B3
B4
B5
C3
C5
C2B4
C4B5
C4
C1 C4
C2
C1C2 B4
B3 B4C1
B5
B3B4
C4B5C1
C1C2
C4
B5
C5
C5
C1
C1
C2
B1
B2
C2
C2
-
[ 18 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
2.2 Virus receptor
Nishimura (26), Yamayoshi (27) and Yang (28), with their
colleagues, recentlyindependently demonstrated that human
P-selectin glyprotein ligand-1
(PSGL-1),humanscavengerreceptorclassB,member2(SCARB2),andsialic-acid-linkedglycansactasfunctionalreceptorsforEV71byusingdifferenthumancell
linesanddifferentcloning strategies. Identification of three
structurally and functionally differentreceptors for EV71may
provide valuable insights into themolecular basis of
EV71infection,includingHFMDandvariousneurologicaldiseases.
2.3 Recombination
Aswithotherenteroviruses,recombinationhasbeenobservedinseveralEV71fieldisolates
(2932). It has been observedmost frequently in the 5UTR
(untranslatedregion)and3UTRregions;ithasrarelybeenidentifiedinthestructuralproteingeneregion.
Although theeffect of recombinationon thevirulenceor
transmissibility
ofEV71isunknown,laboratorystudieshaveshownthatreplacementofthe3halfofthegenomeofanon-recombinantEV71fieldisolatewithonederivedfromaHEV-Bspeciesvirussignificantly
improvesgrowth
incellculturecomparedwithanon-recombinantstrain(33).
2.4 Reservoir of EV71
EV71replicatesintheintestinaltractandistypicallyshedforbetweentwoandfourweeks,andsometimesforaslongas12weekspost-infection.Replicationalsooccursintheupperrespiratorytractandthevirushasbeenrecoveredfromthroatswabsforuptotwoweekspost-infection.Thustransmissioncanincludefaecal-oralandrespiratorysecretions
through direct person-to-person contact, droplets or fomites.
Factorsthataffectthetransmission include
levelofhygiene,waterquality,andtheextentofcrowding(34).
Ingeneral,theenteroviruseshaveadistinctseasonalpatternofcirculationthatvariesbygeographicarea.Intropicalandsubtropicalcountries,circulationtendstobeyearround,withmoreoutbreaksintherainyseason.
References
1. McMinn P, et al. Phylogenetic analysis of enterovirus 71
strains isolated during linked
epidemics inMalaysia,Singapore, andWesternAustralia.
JournalofVirology,2001,Aug,
75(16):77327738.
2. CardosaMJ, et al. Molecular epidemiology of human enterovirus
71 strains and recent
outbreaks in the Asia-Pacific region: comparative analysis of
the VP1 and VP4 genes.
EmergingInfectiousDiseases,2003,Apr,9(4):461468.
-
[ 19 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
3.
ShimizuH,etal.Molecularepidemiologyofenterovirus71infectionintheWesternPacific
Region.PediatricsInternational,2004,Apr,46(2):231235.
4. Bible JM, et al. Genetic evolution of enterovirus 71:
epidemiological and pathological
implications.ReviewsinMedicalVirology,2007,NovDec,17(6):371379.
5. Nix WA, Oberste MS, Pallansch MA. Sensitive, seminested PCR
amplification of VP1
sequences for direct identification of all enterovirus serotypes
from original clinical
specimens.JournalofClinicalMicrobiology,2006,Aug,44(8):26982704.
6. Oberste MS, et al. Improved molecular identification of
enteroviruses by RT-PCR and
ampliconsequencing.JournalofClinicalVirology,2003,Apr,26(3):375377.
7.
ObersteMS,etal.Comparisonofclassicandmolecularapproachesfortheidentificationof
untypeableenteroviruses.JournalofClinicalMicrobiology,2000,Mar,38(3):11701174.
8.
BrownBA,etal.Molecularepidemiologyandevolutionofenterovirus71strainsisolated
from1970to1998.JournalofVirology,1999,Dec,73(12):99699975.
9.
TeeKK,etal.Evolutionarygeneticsofhumanenterovirus71:origin,populationdynamics,
natural selection, and seasonal periodicity of the VP1 gene.
Journal of Virology, Apr,
84(7):33393350.
10. HuangSW,et al.Reemergenceofenterovirus71 in2008 in
taiwan:dynamicsofgenetic
and antigenic evolution from 1998 to 2008. Journal of Clinical
Microbiology, 2009, Nov,
47(11):36533662.
11.
IwaiM,etal.GeneticchangesofcoxsackievirusA16andenterovirus71isolatedfromhand,
foot,andmouthdiseasepatientsinToyama,Japanbetween1981and2007.JapaneseJournal
ofInfectiousDiseases,2009,Jul,62(4):254259.
12.
MizutaK,etal.Cross-antigenicityamongEV71strainsfromdifferentgenogroupsisolated
inYamagata,Japan,between1990and2007.Vaccine,2009,May21,27(24):31533158.
13.
KungSH,etal.Geneticandantigenicanalysesofenterovirus71isolatesinTaiwanduring
1998-2005.ClinicalMicrobiologyandInfection,2007,Aug,13(8):782787.
14.
HosoyaM,etal.Geneticdiversityofenterovirus71associatedwithhand,footandmouth
diseaseepidemicsinJapanfrom1983to2003.PediatricInfectiousDiseaseJournal,2006,
Aug,25(8):691694.
15.
PodinY,etal.Sentinelsurveillanceforhumanenterovirus71inSarawak,Malaysia:lessons
fromthefirst7years.BMCPublicHealth,2006,6:180.
16.
LinKH,etal.EvolutionofEV71genogroupinTaiwanfrom1998to2005:anemergingof
subgenogroupC4ofEV71.JournalofMedicalVirology,2006,Feb,78(2):254262.
17. Sanders SA, et al. Molecular epidemiology of enterovirus 71
over two decades in an
Australianurbancommunity.ArchivesofVirology,2006,May,151(5):10031013.
18.
MizutaK,etal.Frequentimportationofenterovirus71fromsurroundingcountriesintothe
localcommunityofYamagata,Japan,between1998and2003.JournalofClinicalMicrobiology,
2005,Dec,43(12):61716175.
-
[ 20 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
19.
FujimotoT,etal.Outbreakofcentralnervoussystemdiseaseassociatedwithhand,foot,and
mouthdiseaseinJapanduringthesummerof2000:detectionandmolecularepidemiologyof
enterovirus71.MicrobiologyandImmunology,2002,46(9):621627.
20. ChuPY,etal.Molecularepidemiologyofenterovirus71
inTaiwan.ArchivesofVirology,
2001,146(3):589600.
21.
ShimizuH,etal.Enterovirus71fromfatalandnonfatalcasesofhand,footandmouthdisease
epidemics in Malaysia, Japan and Taiwan in 1997-1998. Japanese
Journal of Infectious
Disease,1999,Feb,52(1):125.
22. TuPV, et al.Epidemiologic and virologic investigation of
hand, foot, andmouth disease,
southernVietnam,2005.EmergingInfectiousDiseases,2007,Nov,13(11):17331741.
23.
YangF,etal.Enterovirus71outbreakinthePeoplesRepublicofChinain2008.Journalof
ClinicalMicrobiology,2009,Jul,47(7):23512352.
24.
ZhangY,etal.Anoutbreakofhand,foot,andmouthdiseaseassociatedwithsubgenotype
C4 of human enterovirus 71 in Shandong,China. Journal
ofClinicalVirology, 2009,Apr,
44(4):262267.
25.
JeeYM,etal.GeneticanalysisoftheVP1regionofhumanenterovirus71strainsisolated
inKoreaduring2000.ArchivesofVirology,2003,Sep,148(9):17351746.
26. Nishimura Y, et al. Human P-selectin glycoprotein ligand-1
is a functional receptor for
enterovirus71.NatureMedicine,2009,Jul,15(7):794797.
27.
YamayoshiS,etal.ScavengerreceptorB2isacellularreceptorforenterovirus71.Nature
Medicine,2009,Jul,15(7):798801.
28.
YangB,ChuangH,YangKD.Sialylatedglycansasreceptorandinhibitorofenterovirus71
infectiontoDLD-1intestinalcells.VirologyJournal,2009,6:141.
29. ChenX, et al.Analysis of recombination andnatural selection
inhumanenterovirus71.
Virology,2010,Mar15,398(2):251261.
30.
DingNZ,etal.Appearanceofmosaicenterovirus71inthe2008outbreakofChina.Virus
Research,2009,Oct,145(1):157161.
31.
HuangSC,etal.Appearanceofintratypicrecombinationofenterovirus71inTaiwanfrom
2002to2005.VirusResearch,2008,Feb,131(2):250259.
32. Yoke-Fun C, AbuBakar S. Phylogenetic evidence for
inter-typic recombination in the
emergenceofhumanenterovirus71subgenotypes.BMCMicrobiology,2006,6:74.
33.
PhuektesP.DevelopmentofareversegeneticssystemforHumanenterovirus71(HEV71)
and the molecular basis of its growth phenotype and adaptation
to mice. PhD Thesis,
MurdochUniversity,Australia.2009.
34.
OoiEE,etal.Seroepidemiologyofhumanenterovirus71,Singapore.EmergingInfectious
Diseases,2002,Sep,8(9):995997.
-
[ 21 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Section 3: Laboratory Diagnosis
3.1 Overview
Rapid identification of the causative agent of HFMD,
particularly whether there isEV71 infection, can help
clinicalmanagement by focusing attention on the
possiblecomplications.WhenpatientspresentwithothermanifestationsofEV71,suchasCNSdiseaseorcardiovascularcollapse,rapidvirologicaldiagnosisisevenmorehelpfulbecauseofthebroaddifferentialforthoseconditionsandthespecifictreatmentsavailable(1).IdentificationoftheagentsresponsibleforoutbreaksofHFMDisalsoimportantwithregardstopredictingtheseverityoftheoutbreakandinitiatingappropriatepublichealthinterventions.
Aswithotherenteroviruses, confirmatorydiagnosishas
traditionallybeenbasedoncellcultureandvirusisolationandidentification,bothofwhicharetime-consumingandresource-intensive.Modernmoleculartechniqueshavebeendevelopedandarenowinuseinsomelaboratories.Effectiveandaccuratevirologicaldiagnosisdependsonthecorrecttimingandcollectionofappropriateclinicalspecimens,andtheirtransporttothelaboratoryunderoptimalconditions.Thisrequiresclosecooperationbetweenlaboratoryexperts,epidemiologistsandclinicians.
3.2 Laboratory safety
Toensuresafehandlingofclinicalsamplesandinfectiousmaterials,laboratoriesshouldfollowthenecessarybiosafety,chemical,fireandelectricalsafetyrequirementstoprotectstaff,thecommunityandtheenvironment(2).Thedirectorsandallstaffofdiagnosticlaboratories
should be familiar with international and local biosafety
requirements,includingsafehandlingandtransportationofclinicalsamplesandinfectiousmaterials,including
goodmicrobiological techniques and basic biosafety level of the
facilities,normallyBSL-2forprimaryisolation(3).
3.3 Clinical samples
Throatandvesicle(ifavailable)swabsamplesinvirustransportationmedium(VTM)areconsideredtobethemostusefulspecimensintermsoftherateofvirusdetectionofHFMD(4)andintermsofbothinpatientandoutpatientavailability.
EV71canbeshedinthestoolforseveralweeksandstool(rectalswab)samplesarealsoappropriateclinicalspecimensforvirusdetectionand/orisolation.
-
[ 22 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
The risk of recent coincidental infection, rather than casual
infection, should beconsidered forsomeclinicalsamples,particularly
forstoolsamples. Vesicle isolatesare the most useful, because they
always represent current systemic infection (4).Given
thepotentialnumberofsamples, from largenumbersofpatients,
laboratoriescanbecomeoverwhelmed.
To increase the possibility of enterovirus detection, collecting
throat swab samplesforallpatientsplusswabsfromat leasttwovesiclesor
fromtherectumforpatientswithnovesiclesisrecommended.ThevirusdetectionratesofEV71andCA16fromcerebrospinalfluid(CSF)samplesareratherlow(lessthan5%)(4,5).However,CSFsamples
are useful for virus detection of other enteroviruses, particularly
forHEV-B-associated aseptic meningitis. Serum samples from
inpatients may be useful
forserologicaldiagnosis,butthereliabilityofserologicaltestsforEV71infectionrequirescarefulevaluation.
3.4 Laboratory diagnosis methods
Asforotherenterovirusinfections,includingpoliomyelitis,confirmeddiagnosesbasedoncellculture,virusisolationandidentificationofenterovirusesisstillthestandardmethodforlaboratorydiagnosis.Whilevirusisolatesareneededforfurthermolecularcharacterizations
of EV71, virus isolation and identification are generally
laboriousand time-consumingandsuchmethodsarenotpractical
forclinicaldecision-making.Although rapid
laboratorydiagnosticmethodsusing clinical specimens are
available,standardizationofthemethodsandcomparativeevaluationofthereliabilityoftherapidtestsarestillneeded.
Virus isolation
Someclinicalspecimensrequireappropriatepre-treatment(completemixing,filtration,chloroformtreatment)beforeinoculation.Anumberofhumanandnon-humanprimatecelllinesareavailableforvirusisolationandidentificationofenteroviruses.Ofthesecelllines,RD(humanrhabdomyosarcomacells)andVero(Africangreenmonkeykidneycells)cellshavebeenwidelyusedforvirusisolationofEV71andCA16becauseoftheirrelativelyhighsensitivityandtheapparentcytopathiceffect(CPE)
inducedbyEV71andCA16.RDcellsareavailable
fromtheGlobalPolioLaboratoryNetworkand thequalitycontrolof thecells
is routinelycarriedoutaccording to
thePolioLaboratoryManual(3)toensuresensitivityagainstpolioviruses.Thequalityofcellculturesusedinvirologicalinvestigationisimportantforthestandardizationofenterovirusisolationanditscharacterization.
It is important to use several different human and non-human
primate cell lines
toincreasethepossibilityofvirusisolationincellcultures.Additionalcelllines(includingMRC-5,HEL,HeLa,
L20B) can also be used for virus isolation of EV71 and other
-
[ 23 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
enteroviruses, including polioviruses. Although the
receptor-specificities of
EV71isolatesandtheotherHEV-Astrainswouldneedtobecharacterized,mousecelllinesexpressing
functional cellular receptors for EV71 (human P-selectin
glycoproteinligand-1 andhuman scavenger receptor classB,member
2)would beuseful for
theselectiveisolationofEV71and/orCA16fromclinicalspecimens(6,7).Sucklingmice(less
than 48 hours old) are still useful for virus isolation of
someHEV-A isolates,particularly forclinicalsamples
fromherpanginacases (8). However,virus
isolationandidentificationusingsucklingmiceistime-consumingandrequiresspecifichumanandequipmentresources.
Identification of virus isolates
Neutralization test
Following virus isolation in cultured cells, the serotype of
EV71 and CA16 isolatescan be identified by a conventional
neutralization test with a qualified type-specificantiserum. The
type-specific antisera against HEV-A strains, including EV71
andCA16,arenotcommerciallyavailableandthesupplyofin-houseantiseraisthereforegenerally
limited. The neutralization test is still a reliablemethod for
enterovirusidentification,butitcantakeuptoaweek(57days)tocompletetheassay.
Reverse transcription polymerase chain reaction (RT-PCR) and
sequencing
Following virus isolation in cultured cells, reverse
transcription polymerase
chainreaction(RT-PCR)amplificationofviralRNAandsequencingofthedeoxyribonucleicacid(DNA)amplicons,usingvariousgenetargets(5untranslatedregion[5UTR],VP1,VP4/VP2
genes), have been widely used for molecular identification of
enterovirusisolates. The advantage of the RT-PCR and sequencing
strategy is the universaldetection and amplification of enterovirus
gene targets, regardless of the
serotypesandgenotypesofenteroviruses,possibly
includingnewlyemergedvariantsandnewserotypesof enteroviruses (911).
While sequencingof the shorterVP4 region
(orVP4pluspartialVP2)issufficientforregularsurveillance,confirmationofthedataformolecular
epidemiological research should use theVP1 region of the
genome.Thisis also important as theVP1gene is themostexposedand
immunodominantof thecapsid proteins and is thereforemost likely to
change in response to
immunogenicpressure(12,13).TheRT-PCRandsequencingstrategymaydependonroutineaccessto
the sequencing facility at diagnostic laboratories and requires
higher installationandrunningcosts. Specific trainingactivities for
laboratoryexpertsand
techniciansonmolecularidentificationofenterovirusesareneededtominimizetheriskofcross-contaminationandtoensurethereliabilityofidentification,includingsequenceanalysisanddatamanagement.
EV71-specific RT-PCR
Following virus isolation in cultured cells,RT-PCR amplification
of viralRNAusingEV71-specific primers is useful for themolecular
identification of EV71 (14). The
-
[ 24 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
EV71-specific RT-PCR amplification is a rapid and simple
identificationmethod andrequires lower installation and running
costs. EV71-specific primers should
berevisedaccordingtothesequencesofnewlyemergingEV71genogroupsandvariantsto
maintain the reliability of the EV71-specific RT-PCR test (14).
General trainingactivities for laboratory technicians on RT-PCR are
needed tominimize the risk ofcross-contamination.
Indirect immunofluorescence assay
Indirectimmunofluorescenceassay(IFA)testsusinganti-EV71monoclonalantibodiescan
provide rapid, presumptive EV71 identification. The IFAmethod is
technicallysimpleandrapid,andtheantibodiesarecommerciallyavailable(15),althoughrelativelyexpensivetopurchase.
Rapid diagnosis directly from clinical samples
Nested RT-PCR
Targeting of conserved 5UTR has been widely used for the
universal detection ofenteroviruses. However, 5UTR RT-PCR methods
are inappropriate for serotype-specific detection and
identification of EV71. Technical improvement of
RT-PCRmethodsbasedontheVP1regionhasenabledpartialVP1sequencingusingconsensus-degenerate
hybrid oligonucleotide primer (CODEHOP) with a high sensitivity
andbroader specificity for all known enterovirus serotypes (16).
Enteroviruses
canthereforebeidentifiedbyVP1sequencesderivedfromtheCODEHOPPCRproductsdirectlyfromclinicalsamples.MultiplexRT-PCRmethodshavebeendevelopedfortheidentificationofEV71andCA16(17)andforthespecificdetectionofEV71andCA16directlyfromclinicalsamples(18).
Real-time PCR
Real-timeRT-PCRsystemshaverecentlybecomeavailabletodiagnosticlaboratoriesforrapidandspecificdetectionofanumberofviralinfectiousdiseases.One-tubereal-time
RT-PCR systems can reduce the risk of cross-contamination when
comparedwithconventionalRT-PCR,particularlynestedPCRsystems.WhileseveraldifferentEV71-specificreal-timeRT-PCRsystemshavebeenreported(1921)thereliabilityofsuchsystemsneedstobeaddressedusingdifferentgenogroupsofEV71,CA16,HEV-Astrains,
and clinical samples. In general, EV71-specific real-time RT-PCR
primersand probes should be revised according to the sequences of
newly identified
EV71genogroupsandvariantstomaintainthereliabilityofEV71-specificreal-timeRT-PCR.
New diagnostic approaches
InadditiontoEV71-specificreal-timeRT-PCRsystems,severalotherpromisingoptionsforrapidandconvenient(bedside)diagnosisareunderinvestigation.
Althoughrapidviralantigen-detectionkitsusing
immunochromatographyarecommerciallyavailablefor a number of viral
infectious diseases, EV71 antigen-detection kits have not yet
-
[ 25 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
beendeveloped,mainlyduetothelowsensitivityfromclinicalsamples(22).Whilethereversetranscriptionloop-mediatedisothermalamplification(RT-LAMP)methodcanbeusedasarapidandsensitiveisothermaldetectionmethodforenteroviruses,itisnotspecifictocertainserotypes(genotypes)ofenterovirus(23).
Evaluation of the reliability of new laboratory diagnostic
methods
To encourage the development of rapid and convenient (bedside)
diagnostic kits
forEV71infectionintheregion,astandardizedevaluationsystemtocomparethesensitivityand
specificity of diagnostic methods is critical. For the evaluation
of
molecularidentificationmethods,establishmentofanEV71strainbank,containingallavailableEV71subgenogroups(A,B1-B5,C1-C5,plusnewlyemerginggenogroups),shouldbeconsidered.Linkingthistoaqualityassurancesystemandnetworkingoflaboratorieswouldensurestandardsforidentificationofenterovirusesandtheirsubgroupscanbeappliedinthefuture.
Molecular epidemiological analysis (genotyping) of EV71
strains
A powerful tool for tracking the circulation of EV71 strains is
the
molecularcharacterizationofEV71genomes(genotyping).BycomparingtheextentofgeneticchangesthatareobservedbetweenEV71strains,thegeographicandevolutionaloriginofaviruscanbedetermined.
BaseduponacapsidVP1sequencedatabaseofEV71strains,itispossibletodeveloprapidapproachestotrackingtheregionaltransmissionand
current prevalence ofEV71 strains (see the section onVirology). For
detailedmolecularepidemiological analysisofEV71strains,
theentireVP1sequenceshouldbedeterminedandanalysed,
althoughpartialVP1sequencingwouldbesufficient
togenotypeeachEV71isolate.
Serological analysis
Testingforneutralizingantibodiesagainstenterovirusesisnotrecommendedforroutineuseinthediagnosisofenterovirusinfections.Pairedserumsamplesarecollectedforserologicaldiagnosisofcertainserotypesofenterovirus,but
interpretationofserumantibodytitersissometimesdifficult.Ontheotherhand,theneutralizingtestagainstEV71
would be useful for evaluating of immunity levels for EV71
infection withincommunities (23,24),aswellas
formonitoringthecross-reactivityofserumamongdifferentgenogroupsofEV71(25).
SerumsamplesfrominpatientscouldbeusefulfortherapidimmunoglobulinM(IgM)detectionofEV71
(22,26),but thespecificityandsensitivityofserological tests
forEV71infectionremainsanareawherecarefulevaluationisneeded.
-
[ 26 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
References
1. Ooi MH, et al. Clinical features, diagnosis and management of
human enterovirus 71
infection.LancetNeurology,2010,9(11):10971105
2.
Laboratorybiosafetymanual,3rdedition.Geneva,WorldHealthOrganization,2004.
3.
Poliolaboratorymanual,4thedition.Geneva,WorldHealthOrganization,2004.
4.
OoiMH,etal.Evaluationofdifferentclinicalsampletypesindiagnosisofhumanenterovirus
71-associated hand-foot-and-mouth disease. Journal of Clinical
Microbiology, 2007, Jun,
45(6):18581866.
5. ChanKP,etal.Epidemichand,
footandmouthdiseasecausedbyhumanenterovirus71,
Singapore.EmergingInfectiousDiseases,2003,Jan,9(1):7885.
6. Nishimura Y, et al. Human P-selectin glycoprotein ligand-1 is
a functional receptor for
enterovirus71.NatureMedicine,2009,Jul,15(7):794797.
7.
YamayoshiS,etal.ScavengerreceptorB2isacellularreceptorforenterovirus71.Nature
Medicine,2009,Jul,15(7):798801.
8.
ShimaT,etal.Enterovirusdetectionstatusfrompatientswithherpanginaandhand,foot
andmouthdiseaseinKanagawaPrefecture,Japan.JapaneseJournalofInfectiousDisease,
2007,Feb,60(1):6364.
9.
ObersteMS,etal.TypingofhumanenterovirusesbypartialsequencingofVP1.Journalof
ClinicalMicrobiology,1999,May,37(5):12881293.
10.
ObersteMS,etal.Molecularevolutionofthehumanenteroviruses:correlationofserotype
withVP1sequenceandapplicationtopicornavirusclassification.JournalofVirology,1999,
Mar,73(3):19411948.
11.
BrownBA,etal.Molecularepidemiologyandevolutionofenterovirus71strainsisolated
from1970to1998.JournalofVirology,1999,Dec,73(12):99699975.
12. CardosaMJ, et al. Molecular epidemiology of human
enterovirus 71 strains and recent
outbreaks in the Asia-Pacific region: comparative analysis of
the VP1 and VP4 genes.
EmergingInfectiousDiseases,2003,Apr,9(4):461468.
13. PereraD,et al.Acomparisonof theVP1,VP2,andVP4regions
formolecular typingof
humanenteroviruses.JournalofMedicalVirology,2010,Apr,82(4):649657.
14. PereraD,et al. Incorrect identificationof
recentAsianstrainsofCoxsackievirusA16as
humanenterovirus71:improvedprimersforthespecificdetectionofhumanenterovirus71
byRTPCR.BMCInfectiousDiseases,2004,May4;4:11.
15. APNET. [cited 2010 July 30]; Available from:
http://sydney.edu.au/medicine/apnet/
diagnostics/index.php.
-
[ 27 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
16. Nix WA, Oberste MS, Pallansch MA. Sensitive, seminested PCR
amplification of VP1
sequences for direct identification of all enterovirus serotypes
from original clinical
specimens.JournalofClinicalMicrobiology,2006,Aug,44(8):26982704.
17. Chiueh TS, et al. Multiplex Reverse
Transcription-semi-nested PCR for Differentiating
Enterovirus71,CoxsackievirusA16,andpoliovirusesfromotherenteroviruses.Journalof
MedicalSciences,2001,21(6):277282.
18.
ChenTC,etal.Combiningmultiplexreversetranscription-PCRandadiagnosticmicroarray
to detect and differentiate enterovirus 71 and coxsackievirus
A16. Journal of Clinical
Microbiology,2006,Jun,44(6):22122219.
19. TanEL,etal.Specificdetectionofenterovirus71directly
fromclinicalspecimensusing
real-time RT-PCR hybridization probe assay. Molecular and
Cellular Probes, 2006, Apr,
20(2):135140.
20.
TanEL,etal.Rapiddetectionofenterovirus71byreal-timeTaqManRT-PCR.Journalof
ClinicalVirology,2008,Jun,42(2):203206.
21. XiaoXL,et al.Simultaneousdetectionofhumanenterovirus71
andcoxsackievirusA16
in clinical specimens bymultiplex real-time PCRwith an internal
amplification control.
ArchivesofVirology,2009,154(1):121125.
22. Wu H-S (Centers for Disease Control, Taiwan[China]).
Personal communication to H.
Shimizu,2010.
23.
AritaM,etal.Developmentofareversetranscription-loop-mediatedisothermalamplification
(RT-LAMP)systemforahighlysensitivedetectionofenterovirusinthestoolsamplesof
acuteflaccidparalysiscases.BMCInfectiousDiseases,2009,9:208.
24.
OoiEE,etal.Seroepidemiologyofhumanenterovirus71,Singapore.EmergingInfectious
Diseases,2002,Sep,8(9):995997.
25.
MizutaK,etal.Cross-antigenicityamongEV71strainsfromdifferentgenogroupsisolated
inYamagata,Japan,between1990and2007.Vaccine,2009,May21,27(24):31533158.
26. Wang SY, et al. Early and rapid detection of enterovirus 71
infection by an IgM-capture
ELISA.JournalofVirologicalMethods,2004,Jul,119(1):3743.
-
[ 28 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
Section 4: Pathogenesis in EV71 Infection
4.1 Overview
There is very little information concerning the pathology of
uncomplicated EV71-associatedHFMDandherpangina.
Inamousemodel,theviruswasshowntoinfectskin, suggesting that human
skin or oralmucosa lesions could also be the result
ofdirectinfectionofsquamouscells(1).Whileitispossiblethatpathologicalchangesareconfinedtoskinrashesandoral
lesions,there isa lackof informationavailable
fromskinororalmucosabiopsies.
The neurovirulence factors of EV71 in human infections are still
unknown. So
far,thereisnoconvincingevidenceofspecificvirusgenomemutationsthatmayfacilitateinfectionofthehumancentralnervoussystem(CNS).Otherfactors,suchashigherinitialinfectivedosesleadingtoseveredisease,arealsopossible.Certaincytokines,chemokines,
alterations of cell mediated immunity and human leukocyte
antigen(HLA) subtypes appear tobe associatedwith ahigher
incidenceof
cardiopulmonarycomplications.Therelationshipbetweenpathogenesisanddistributionofviralentryreceptors(scavengerreceptorB2,P-selectinglycoproteinligand-1andsialicacid-linkedglycans)andhostfactors,suchasgenderandagegroup,isunknown.
ThepathologicalfindingsintheCNSinfatalcasesofEV71arestereotypedandconsistof
neuronophagia, perivascular cuffing, focal oedema and infiltration
of
inflammatorycells.Viralcytolysisappearstobeanimportantmechanismforneuronaldamage.Themost
severe inflammation is found in thehypothalamus,brain stem, spinal
cordandcerebellardentatenucleus.Medullaryinflammationandfindingsinthelungsandheartareconsistentwithneurogenicpulmonaryoedemaasacauseofdeath.AnimalstudiesconfirmsomeofthehumanautopsyfindingsandsuggestthatmotorpathwaysmayplayanimportantroleinviraltransmissionintheCNS.
4.2 Virus neuro-virulence factors
Viral genome mutations
To date, no convincing evidence of specific virus genome
mutations that conferneurovirulenceinhumanshasbeenreported.
-
[ 29 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
However, clinical epidemiological evidence from outbreaks in
Perth, Australia, andSarawak, Malaysia, suggests that there may be
differences between genogroups
intermsofbiologicalbehaviourandvirulence(2).InPerth,in1999,subgroupsB3andC2werebothcirculating(3,4).
C2 viruses were linked to the 1998 epidemic in Taiwan (China)
and were almostexclusively isolated
fromchildrenwithsevereneurologicaldisease;onlyone
isolatecamefromacaseofuncomplicatedHFMD(3,4).Bycontrast,B3virusesthatweresimilartothosefromthe1997Sarawakepidemic,wereisolatedmainlyfromchildrenwithuncomplicatedHFMDorasepticmeningitis,orthosewithneurologicalcomplications,noneofwhomdied(5).IntwodiscreteepidemicsinSarawakinwhicheitherB4orB5viruseswerepredominant,
a studyof 277
childrenwithEV71-associatedHFMDshowedthatB4viruseswerelesslikelythanB5virusestocauseCNSinfectionorbepartofafamilycluster(6).
More extensive virological surveillance and genetic analysis
from the region mayprovide further evidence of potential genetic
determinants of virulence. Animalstudies, however, have
demonstrated that there are four co-expressed
mutationsderivedfromtheSabinpoliovirustype1attenuatedEV71inbothcynomolgusmonkeys(7)andinnon-obesediabetic/severecombinedimmunodeficient(NOD/SCID)mice(8).A3Dpolymerasegenemutationhasbeenshowntointroduceatemperature-sensitivephenotypeincellcultureandanattenuationofvirulenceinnewbornmice(9).
Other factors
Otherfactors,suchashigherinfectivevirusdosesleadingtomoresevereillness,arepossibleandshouldbeinvestigatedfurther.
4.3 Host factors
Immunopathology
There have been relatively few studies of the human immune
response to EV71infection. Induction of specific cytokines and
chemokines has been associated
withcertainadverseoutcomesofEV71infection,mostnotablypulmonaryoedema.Abnormalelevationofcytokinesmaybeonemechanismforpulmonaryoedemainfatalcases.Inatleasttwostudies,cerebrospinalfluidlevelsofinterleukin(IL)-6werefoundtoberaisedin
caseswith pulmonary oedema (10, 11). Higher levels of
interferongammawerealsofoundincerebrospinalfluidinsimilarcases(11).LevelsofIL-6,tumournecrosisfactoralpha,IL-1beta(12)andIL-10(11)werealsofoundtobehigherintheserumofpulmonaryoedemacases.Furthermore,levelsofchemokines,IL-8,interferoninducedprotein(IP-10),monocytechemoattractantprotein(MCP-1)andmonokineinducedbyinterferongamma(MIG)werefoundtobehigherinserum,andMIGinbothserumandcerebrospinalfluidinpulmonaryoedema(13).
-
[ 30 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
Withregardstocell-mediatedimmunity,areductionofTlymphocytesandNKcellshasbeenreportedinpatientswithpulmonaryoedema(14).Anotherstudydemonstratedreducedproductionofinterferongamma,IL-1beta,IL-6andmacrophageinflammatoryprotein-1alphainstimulatedperipheralmononuclearcellsinpatientswithpulmonaryoedema(15).
HLA-A33isreportedtobeassociatedwithsusceptibilitytoEV71infection,particularlyinAsianpopulationswheretheHLAprevalence(17%-35%)ishigherthaninCaucasianpopulations.
In addition, HLA-A2 may possibly be linked to increased risk
ofcardiopulmonarycomplications(16).
Virus receptors on host target cells
In 2009, three receptors were identified that facilitate virus
entry into host
cells:scavengerreceptorB2(17)andP-selectinglycoproteinligand-1(18).Respectively,thosereceptorshavebeenreported
tobeubiquitouslyexpressedor limited to leukocytes.Whether
thepresenceorabsenceof thosereceptors inhuman tissuesmight
impactonviralpathogenesishasnotbeeninvestigated.
Similarly,viralreplicationsitesandviraltransmissionrouteswithinthebodymayberelatedtothepresenceorabsenceofreceptorsinsusceptibletissues.
Other host factors
Otherhost factorsthatmaybeimportant forsusceptibilityto
infectioncould includegender, as a higher incidence of severe
diseasehas been reported inmale
children.Moreover,therelativeimmaturityoftheinnateandadaptiveimmunesysteminchildrenagedbetweenoneandfiveyearscouldaccountforthehigherincidenceofneurologicalcomplicationsinthatagegroup.Evidenceforthisisstilllacking.
4.4 Pathological findings
Human autopsies
Autopsies conducted in mainland China, Malaysia, Singapore and
Taiwan (China)have been useful in improving understanding of the
pathogenesis of severe diseaseand theunderlyingpathological insult
leading todeath. The inflammatory
responseseeninEV71encephalomyelitisistypicalofviralencephalitides,thefeaturesofwhichinclude
neuronophagia, perivascular cuffing, focal oedema
andmacrophage/microgliainfiltration(Figure3)(19-22).Themainareasofinflammationappeartobelocalizedtothehypothalamus,brainstem,spinalcordandcerebellardentatenucleus.Althoughmildinflammationcanbeseeninthecerebralcortex(especiallythemotorcortex),itis
entirely absent from the anterior pontine nuclei and cerebellar
hemisphere.
Thetopographicdistributionofinflammationandvirussuggestsretrogradeperipheralmotornerveviral
spread into theCNS. Within theCNS,otherneuralpathways,
includingmotorpathways,couldbeinvolved(19).Viralantigens/RNAhavebeendemonstrated
-
[ 31 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
in neuronal body and processes (Figure 4), and inmacrophages
participating in
theneuronophagiaseenininflamedareas.Thisprovidesevidencethatneuronsarethemainviraltargetsandthatviralcytolysisisanimportantmechanismforneuronalinjury.Themechanismcouldinvolveapoptosis,asthevirusisabletoinduceapoptosisinneuronalandglialcellcultures
(23,24). Pathologicalevidenceofmedullary
inflammationanddestructionisconsistentwithneurogenicpulmonaryoedemaastheprimarycauseofdeath.
Lung findings at autopsywere found to be consistent with
interstitial
pneumonitis,pulmonaryoedemaandhaemorrhage,andmyocardialcongestion(20).Otherstudieshavefoundthat,apart
frompulmonaryoedema,therewasnoevidenceofpulmonaryinflammationorviralantigeninthelungparenchyma(25).Myocarditisandmyocardialinfectionaregenerallyabsent.
Thepathogenesisofdeathresulting
frompulmonaryoedemaaloneorpulmonaryoedemawithconcurrentpulmonaryhaemorrhageduringEV71infectionisnotcompletelyunderstood.Basedonthefindingsabove,however,myocarditisisunlikelytobethecauseofdeath.
Animal models
Monkey(26,27)andmousemodels(1,28-30)havebeenusedtostudytheneurovirulenceof
EV71. In such models, the CNS pathology has, so far, confirmed that
EV71
isneuronotropic.Amajordrawbackofthemonkeymodelsisthatmonkeysarerefractorytoinfectionbytheoralroute.
Figure 3:
Perivascularcuffingandparenchymal
infiltrationbyinflammatorycellsin
thehumanmedullainEnterovirus71
encephalomyelitis(Haematoxylinandeosin
stain(H&E),magnificationx10objective)
Figure 4:
Enterovirus71-infectedneuronshowing
cytoplasmicviralRNA(insituhybridization,
magnificationx40objective)
-
[ 32 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
InonemousemodelofEV71encephalomyelitis, thedistributionofvirus
infiltrationandinflammationwassimilartothatseeninhumanencephalomyelitis,suggestingthatmotor
pathways are important for viral transmission into and within the
CNS
(30).Viralantigenswerefoundintheskeletalmuscleandbrownfat,butthishasnotbeenreportedinhumanEV71infections.InfectivitystudiesshowthattheskeletalmusclesaremajorprimaryvirusreplicationsitesforEV71inmiceandthatmyositisisaprimarycauseofdeath(29,30).Thecurrentlyavailableanimalmodelscouldbeusedforfurtherinvestigationofdiseasepathogenesisandforanti-viraldrugandvaccinetesting.
References
1.
ChenYC,etal.Amurineoralenterovirus71infectionmodelwithcentralnervoussystem
involvement.JournalofGeneralVirology,2004,Jan,85(Pt1):6977.
2.
SolomonT,etal.Virology,epidemiology,pathogenesisandcontrolofentervirus71.Lancet
infectiousdiseases,2010:10(11):778790.
3. McMinn P, et al. Phylogenetic analysis of enterovirus 71
strains isolated during linked
epidemics inMalaysia,Singapore, andWesternAustralia.
JournalofVirology,2001,Aug,
75(16):77327738.
4.
McMinnPC.Anoverviewoftheevolutionofenterovirus71anditsclinicalandpublichealth
significance.FEMSMicrobiologyReviews,2002,Mar,26(1):91107.
5.
McMinnP,etal.Neurologicalmanifestationsofenterovirus71infectioninchildrenduringan
outbreakofhand,foot,andmouthdiseaseinWesternAustralia.ClinicalInfectiousDiseases,
2001,Jan15,32(2):236242.
6.
OoiMH,etal.Humanenterovirus71diseaseinSarawak,Malaysia:aprospectiveclinical,
virological,andmolecularepidemiologicalstudy.ClinicalInfectiousDiseases,2007,Mar1,
44(5):646656.
7. Arita M, et al. Temperature-sensitive mutants of enterovirus
71 show attenuation in
cynomolgusmonkeys.JournalofGeneralVirology,2005,May,86(Pt5):13911401.
8.
AritaM,etal.Cooperativeeffectoftheattenuationdeterminantsderivedfrompoliovirus
sabin1strainisessentialforattenuationofenterovirus71intheNOD/SCIDmouseinfection
model.JournalofVirology,2008,Feb,82(4):17871797.
9.
KungYH,etal.Introductionofastrongtemperature-sensitivephenotypeintoenterovirus
71byalteringanaminoacidofvirus3Dpolymerase.Virology,2010,Jan5,396(1):19.
10. Lin TY, et al. Different proinflammatory reactions in fatal
and non-fatal enterovirus 71
infections:implicationsforearlyrecognitionandtherapy.ActaPaediatrica,2002,91(6):632
635.
11. Wang SM, et al. Cerebrospinal fluid cytokines in enterovirus
71 brain stem encephalitis
andechovirusmeningitisinfectionsofvaryingseverity.ClinicalMicrobiologyandInfection,
2007,Jul,13(7):677682.
-
[ 33 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
12.
LinTY,etal.Proinflammatorycytokinereactionsinenterovirus71infectionsofthecentral
nervoussystem.ClinicalInfectiousDiseases,2003,Feb,36(3):269274.
13.
WangSM,etal.Acutechemokineresponseinthebloodandcerebrospinalfluidofchildren
withenterovirus71-associatedbrainstemencephalitis.JournalofInfectiousDiseases,2008,
Oct1,198(7):10021006.
14.
WangSM,etal.Pathogenesisofenterovirus71brainstemencephalitisinpediatricpatients:
rolesofcytokinesandcellularimmuneactivationinpatientswithpulmonaryedema.Journal
ofInfectiousDiseases,2003,Aug15,188(4):564570.
15.
ChangLY,etal.Statusofcellularratherthanhumoralimmunityiscorrelatedwithclinical
outcomeofenterovirus71.PediatricResearch,2006,Oct,60(4):466471.
16. Chang LY, et al. HLA-A33 is associated with susceptibility
to enterovirus 71 infection.
Pediatrics,2008,Dec,122(6):12711276.
17.
YamayoshiS,etal.ScavengerreceptorB2isacellularreceptorforenterovirus71.Nature
Medicine,2009,Jul,15(7):798801.
18. Nishimura Y, et al. Human P-selectin glycoprotein ligand-1
is a functional receptor for
enterovirus71.NatureMedicine,2009,Jul,15(7):794797.
19. Wong KT, et al. The distribution of inflammation and virus
in human enterovirus
71 encephalomyelitis suggests possible viral spread by neural
pathways. Journal of
NeuropathologyandExperimentalNeurology,2008,Feb,67(2):162169.
20.
ChongCY,etal.Hand,footandmouthdiseaseinSingapore:acomparisonoffatalandnon-
fatalcases.ActaPaediatrica,2003,Oct,92(10):11631169.
21.
YangY,etal.Neuropathologyin2casesoffatalenterovirustype71infectionfromarecent
epidemic in the Peoples Republic of China: a histopathologic,
immunohistochemical,
and reverse transcriptionpolymerase chain reaction
study.HumanPathology, 2009,Sep,
40(9):12881295.
22.
ShiehWJ,etal.Pathologicstudiesoffatalcasesinoutbreakofhand,foot,andmouthdisease,
Taiwan.EmergingInfectiousDiseases,2001,Jan-Feb,7(1):146148.
23.
LiML,etal.The3Cproteaseactivityofenterovirus71induceshumanneuralcellapoptosis.
Virology,2002,Feb15,293(2):386395.
24.
ShihSR,etal.ViralproteinsynthesisisrequiredforEnterovirus71toinduceapoptosisin
humanglioblastomacells.JournalforNeurovirology,2008,Jan,14(1):5361.
25. LumLC, et al. Fatal enterovirus 71 encephalomyelitis.
Journal of Pediatrics, 1998,Dec,
133(6):795798.
26. Nagata N, et al. Differential localization of neurons
susceptible to enterovirus 71 and
poliovirustype1inthecentralnervoussystemofcynomolgusmonkeysafterintravenous
inoculation.JournalofGeneralVirology,2004,Oct,85(Pt10):29812989.
-
[ 34 ]
A Guide to Clinical Management and Public Health Responsefor
Hand, Foot and Mouth Disease (HFMD)
27. Nagata N, et al. Pyramidal and extrapyramidal involvement in
experimental infection of
cynomolgusmonkeyswithenterovirus71.JournalofMedicalVirology,2002,Jun,67(2):207
216.
28.
WangYF,etal.Amouse-adaptedenterovirus71straincausesneurologicaldiseaseinmice
afteroralinfection.JournalofVirology,2004,Aug,78(15):79167924.
29.
ChuaBH,etal.Themolecularbasisofmouseadaptationbyhumanenterovirus71.Journal
ofGeneralVirology,2008,Jul,89(Pt7):16221632.
30. Ong KC, et al. Pathologic characterization of a murine model
of human enterovirus 71
encephalomyelitis. Journal of Neuropathology and Experimental
Neurology, 2008, Jun,
67(6):532542.
-
[ 35 ]
A Guide to Clinical Management and Public Health Response
for Hand, Foot and Mouth Disease (HFMD)
Section 5: Clinical F