Embed Size (px)
Citation preview

Gruppo Infermieri del GIFC
Strategies for infection control adopted in the
Italian CF Centers
Silvana Ballarin, RN Filippo Festini, RN BA
Carmen Loganes, RN
on behalf of the Italian Cystic Fibrosis Nurses’ Group
www.infermieri-fc.net
aims of the survey
•to evaluate the measures adopted by the Italian CF Centers to prevent and control infections sustained by respiratory pathogens in CF patients
•to provide data for a future possible Italian consensus on this issue
Although the way CF patients get in contact with respiratory pathogens such as PA or BC, has not been completely explained, healthcare settings seem to play a role in determining the risk for patients of contracting infection.
Segregation, reduction of overcrowding, behavioral rules for caregivers and patients and other measures have showed to be effective in reducing the risk, in some cases.
Standardized questionnaire, sent to all 21 Regional centers (15 mixed, 3 adult, 3 pediatric) and 7 local CF Services.
24 questions
materials and methods
results
Answers from 16 Regional Centers (11 mixed, 3 adult, 2 pediatric) and 5 local services.
=3363 patients
(88.9% of Italian CF population)
Regional Centers Local Services
Torino C.pediatrico Livorno
Torino C.adulti Roma OPBG
Milano C. pediatrico
Cerignola
Milano C. adulti Messina
Verona Catania
Trieste
Genova
Parma
Cesena
Firenze
Ancona
Gualdo Tadino
Napoli C. adulti
Potenza
Soverato
Palermo
Results will be presented both as number of Centers and as % of patients followed
7 Centers (51.7% pts): non-shared healthcare setting
14 Centers (48.3% pts): healthcare settings in common with other services and diseases
•Airways culture is usually performed every 3 months in 18 Centers. (1 Center less frequently, 2 Centers more frequently).
•In 15 Centers (84.7% pts) all caregivers are aware of pathogens present in last culture of patients they are taking care of.
•10 Centers (50.6%) have a written protocol about the infection control issue.
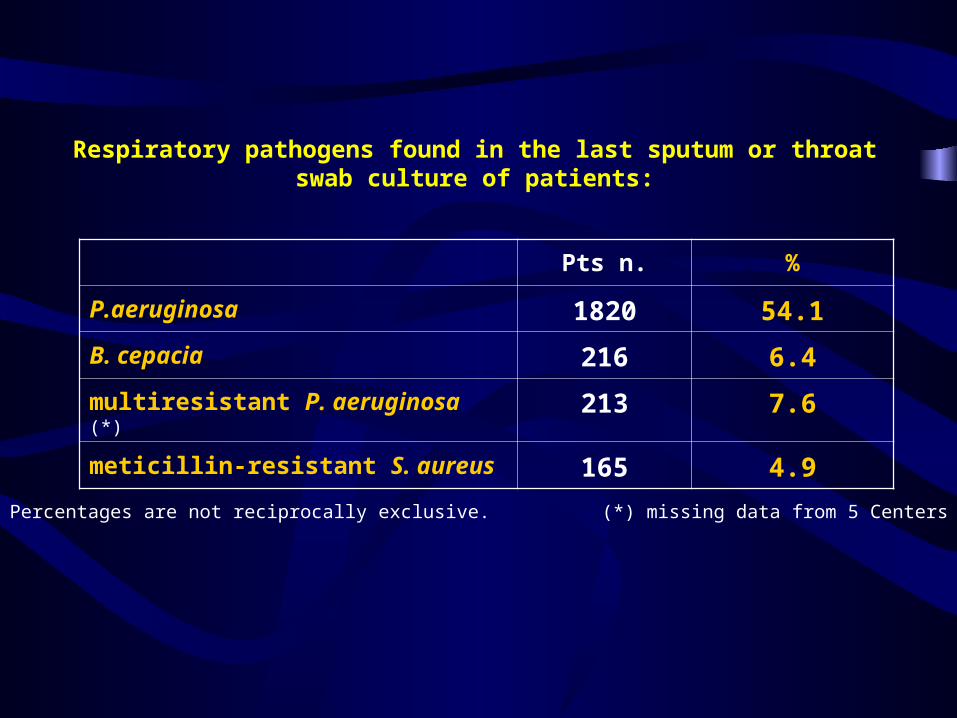
Pts n. %
P.aeruginosa 1820 54.1
B. cepacia 216 6.4
multiresistant P. aeruginosa (*)
213 7.6
meticillin-resistant S. aureus 165 4.9
Respiratory pathogens found in the last sputum or throat swab culture of patients:
Percentages are not reciprocally exclusive. (*) missing data from 5 Centers
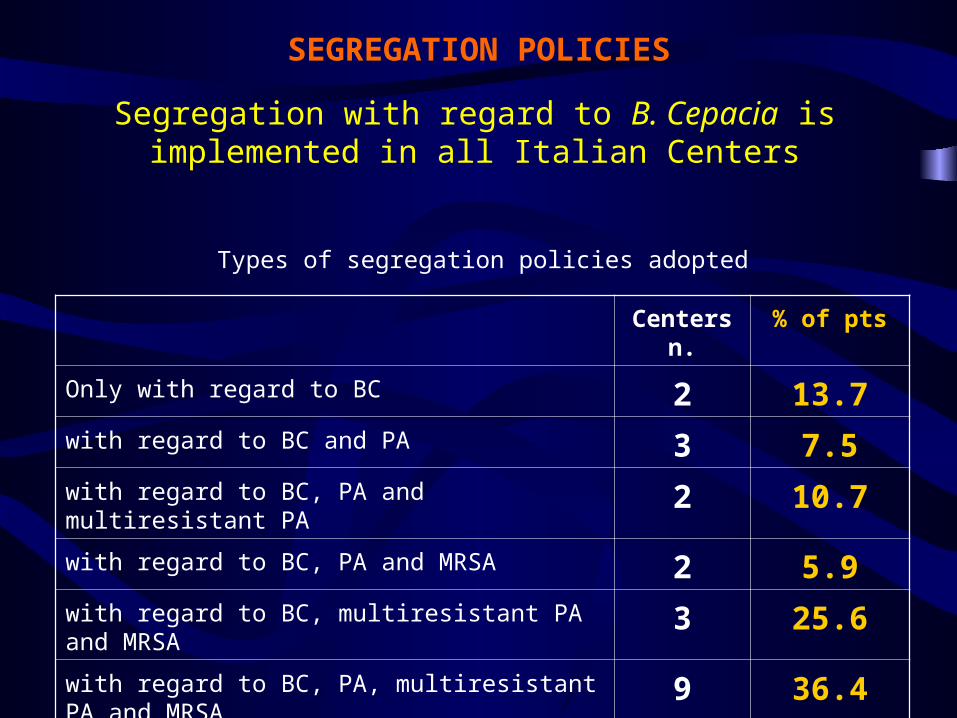
SEGREGATION POLICIES
Segregation with regard to B. Cepacia is implemented in all Italian Centers
Centers n.
% of pts
Only with regard to BC 2 13.7with regard to BC and PA 3 7.5with regard to BC, PA and multiresistant PA 2 10.7with regard to BC, PA and MRSA 2 5.9with regard to BC, multiresistant PA and MRSA
3 25.6
with regard to BC, PA, multiresistant PA and MRSA
9 36.4
Types of segregation policies adopted
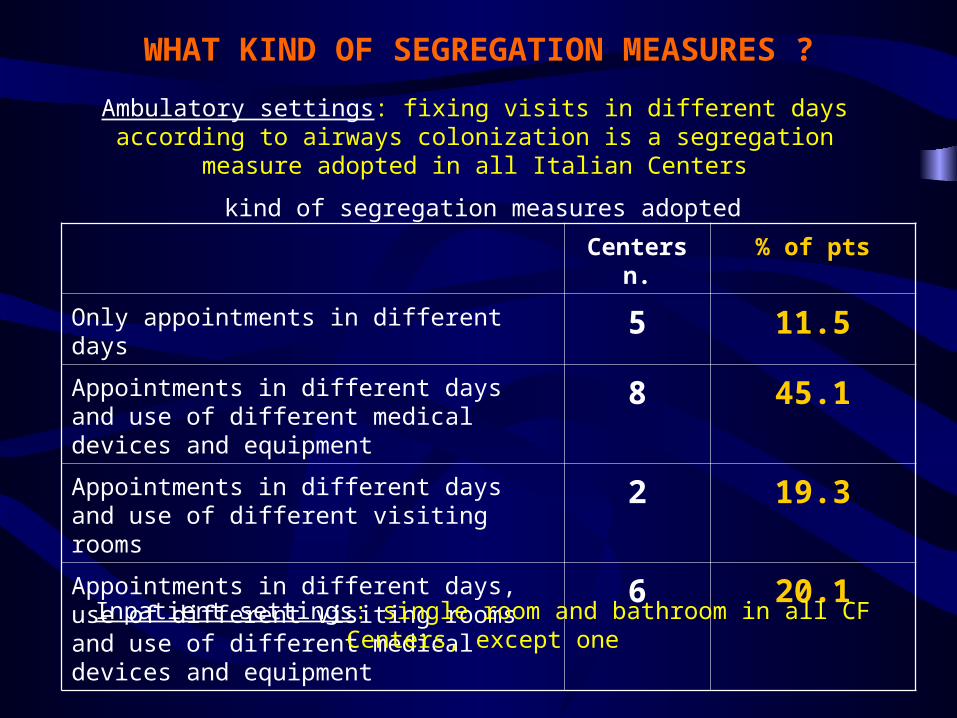
WHAT KIND OF SEGREGATION MEASURES ?
Ambulatory settings: fixing visits in different days according to airways colonization is a segregation measure adopted in all Italian
Centers
Centers n.
% of pts
Only appointments in different days 5 11.5Appointments in different days and use of different medical devices and equipment
8 45.1
Appointments in different days and use of different visiting rooms
2 19.3
Appointments in different days, use of different visiting rooms and use of different medical devices and equipment
6 20.1
kind of segregation measures adopted
Inpatient settings: single room and bathroom in all CF Centers, except one
STAFF HYGIENIC PRACTICES
Frequent hands washing: all Centers
Hands disinfection: 13 Centers (73.5% of pts)
Use of disposable gowns and gloves: (only for assisting some types of pts i.e. with BC or MRSA)
13 Centers (74.2% pts)
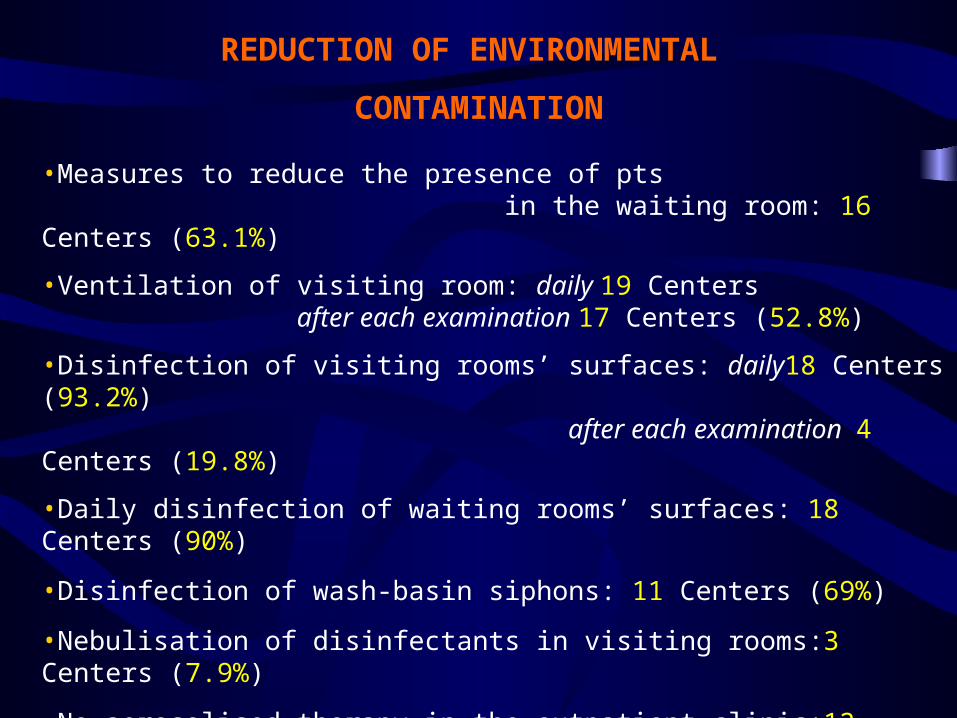
REDUCTION OF ENVIRONMENTAL
CONTAMINATION
•Measures to reduce the presence of pts in the waiting room: 16 Centers (63.1%)
•Ventilation of visiting room: daily 19 Centers after each examination 17 Centers (52.8%)
•Disinfection of visiting rooms’ surfaces: daily18 Centers (93.2%) after each examination 4 Centers (19.8%)
•Daily disinfection of waiting rooms’ surfaces: 18 Centers (90%)
•Disinfection of wash-basin siphons: 11 Centers (69%)
•Nebulisation of disinfectants in visiting rooms:3 Centers (7.9%)
•No aerosolised therapy in the outpatient clinic:12 Centers (51.4%)
•No toys, books etc. in the waiting room:15 Centers (71.9%)
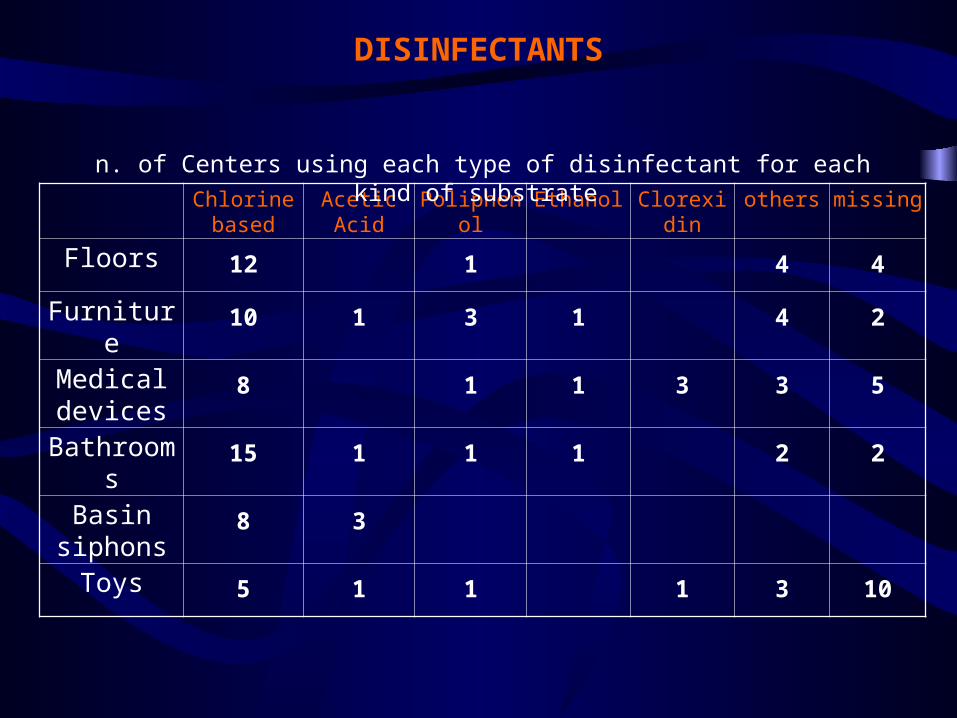
DISINFECTANTS
Chlorine based
Acetic Acid
Poliphenol
Ethanol Clorexidin
others missing
Floors 12 1 4 4
Furniture 10 1 3 1 4 2
Medical devices
8 1 1 3 3 5
Bathrooms
15 1 1 1 2 2
Basin siphons
8 3
Toys 5 1 1 1 3 10
n. of Centers using each type of disinfectant for each kind of substrate
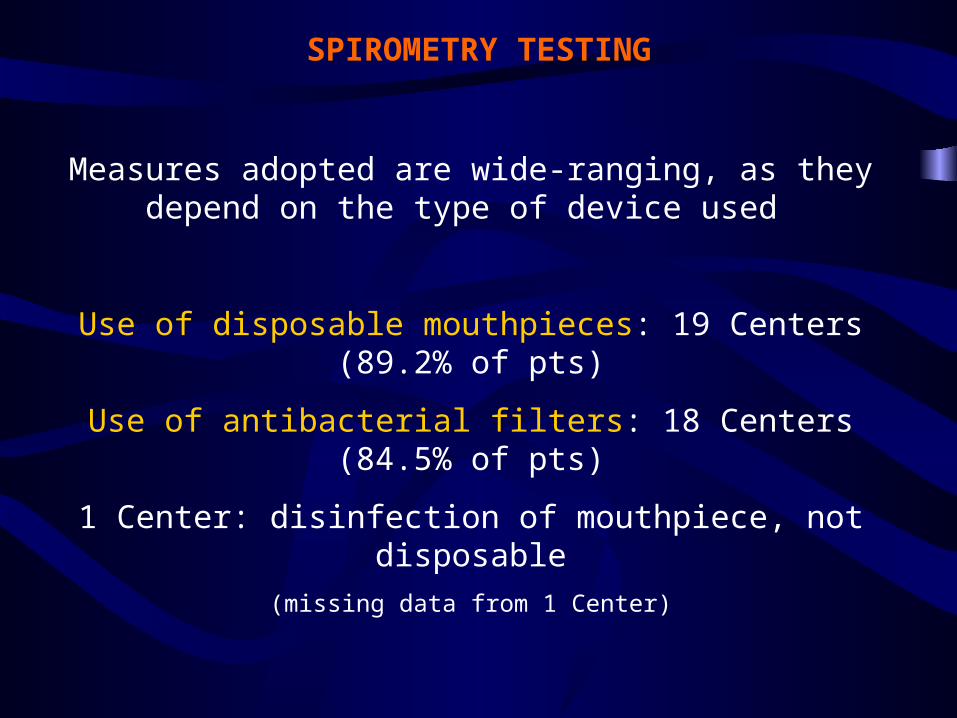
SPIROMETRY TESTING
Measures adopted are wide-ranging, as they depend on the type of device used
Use of disposable mouthpieces: 19 Centers (89.2% of pts)
Use of antibacterial filters: 18 Centers (84.5% of pts)
1 Center: disinfection of mouthpiece, not disposable(missing data from 1 Center)
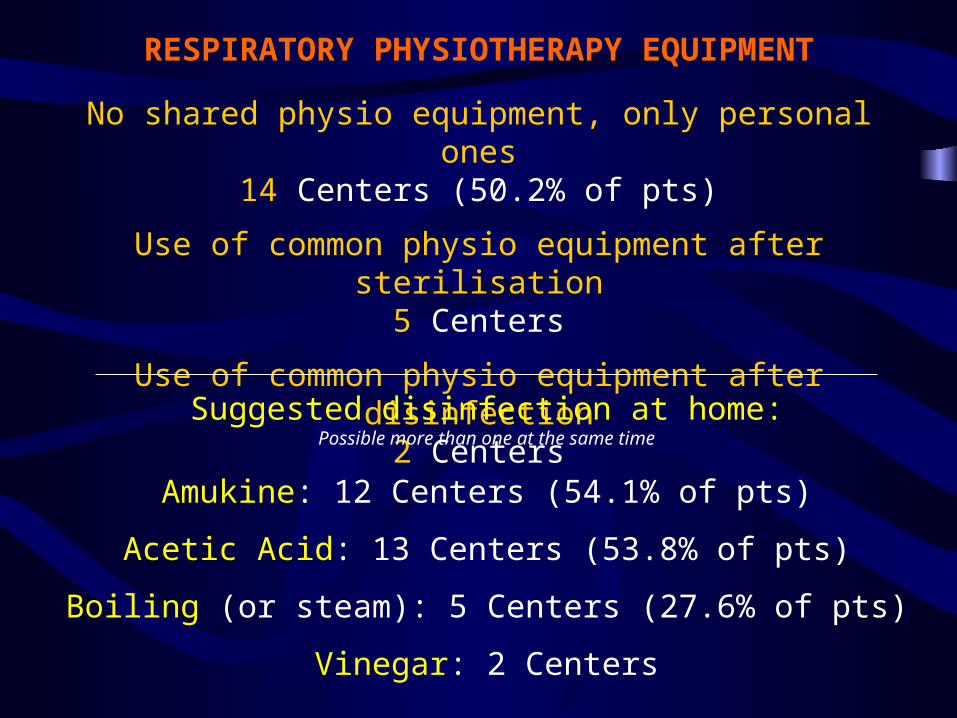
RESPIRATORY PHYSIOTHERAPY EQUIPMENT
No shared physio equipment, only personal ones14 Centers (50.2% of pts)
Use of common physio equipment after sterilisation5 Centers
Use of common physio equipment after disinfection2 Centers
Suggested disinfection at home:Possible more than one at the same time
Amukine: 12 Centers (54.1% of pts)
Acetic Acid: 13 Centers (53.8% of pts)
Boiling (or steam): 5 Centers (27.6% of pts)
Vinegar: 2 Centers
AEROSOL THERAPY EQUIPMENT
No shared A.T. equipment, only personal ones14 Centers (56.7% of pts)
Use of common A.T. equipment after sterilisation3 Centers
Use of common A.T. equipment after disinfection4 Centers
Suggested disinfection at home:Possible more than one at the same time
Amukine: 12 Centers (54.1% of pts)
Acetic Acid: 13 Centers (53.8% of pts)
Boiling (or steam): 6 Centers (35.1% of pts)
ENVIRONMENTAL MICROBIOLOGIC
SURVEILLANCE
Periodical cultures of specimens from the environment of healthcare setting
are performed in 7 Centers (45.7% of pts).
Occasional or periodical cultures on staff members (hands etc.)
are performed in 5 Centers (43.1%)
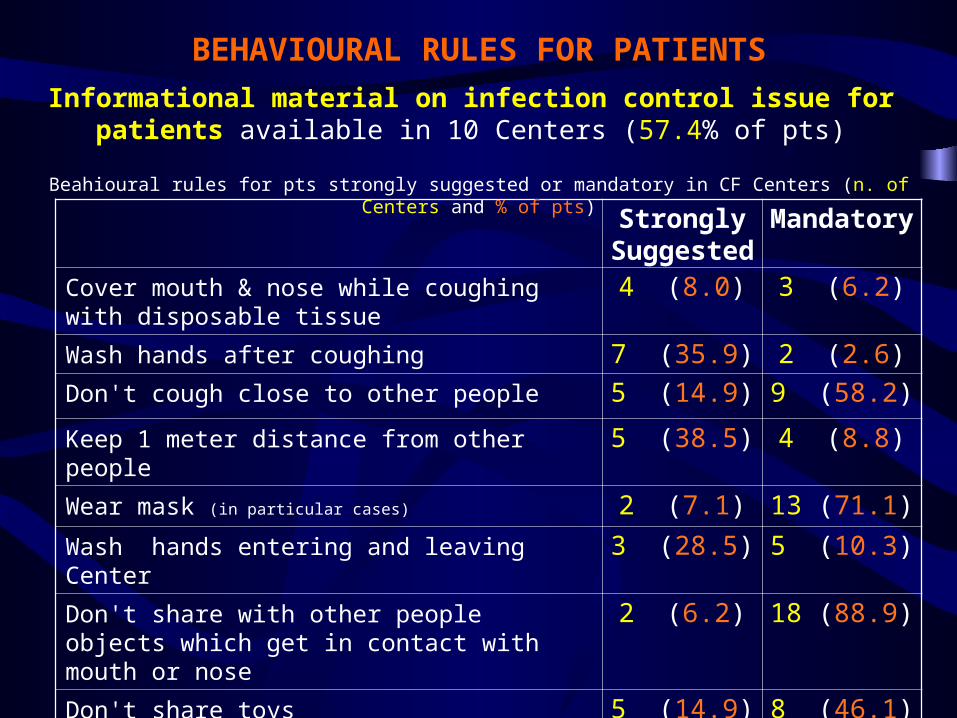
BEHAVIOURAL RULES FOR PATIENTS
Informational material on infection control issue for patients available in 10 Centers (57.4% of pts)
StronglySuggeste
d
Mandatory
Cover mouth & nose while coughing with disposable tissue
4 (8.0) 3 (6.2)
Wash hands after coughing 7 (35.9) 2 (2.6)
Don't cough close to other people 5 (14.9) 9 (58.2)
Keep 1 meter distance from other people 5 (38.5) 4 (8.8)
Wear mask (in particular cases) 2 (7.1) 13 (71.1)
Wash hands entering and leaving Center 3 (28.5) 5 (10.3)
Don't share with other people objects which get in contact with mouth or nose
2 (6.2) 18 (88.9)
Don't share toys 5 (14.9) 8 (46.1)
Don't see other Cf individuals in everyday life
6 (22.4) 4 (20.5)
Beahioural rules for pts strongly suggested or mandatory in CF Centers (n. of Centers and % of pts)
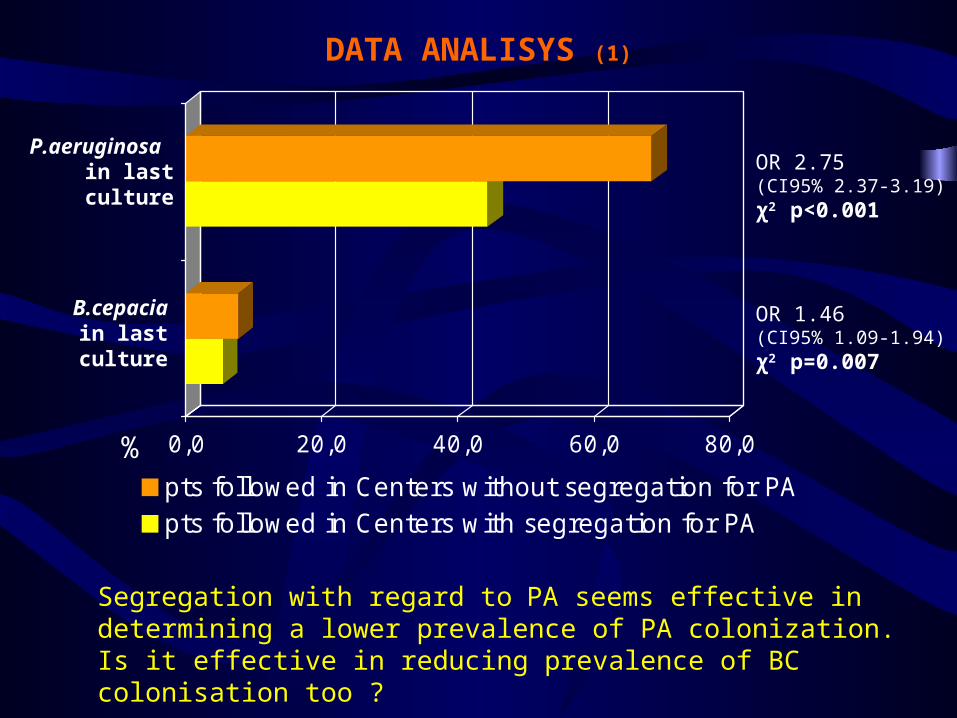
DATA ANALISYS (1)
0,0 20,0 40,0 60,0 80,0%pts followed in Centers without segregation for PApts followed in Centers with segregation for PA
OR 2.75 (CI95% 2.37-3.19)χ2 p<0.001
OR 1.46 (CI95% 1.09-1.94)χ2 p=0.007
Segregation with regard to PA seems effective in determining a lower prevalence of PA colonization. Is it effective in reducing prevalence of BC colonisation too ?
P.aeruginosa in last
culture
B.cepacia in last
culture
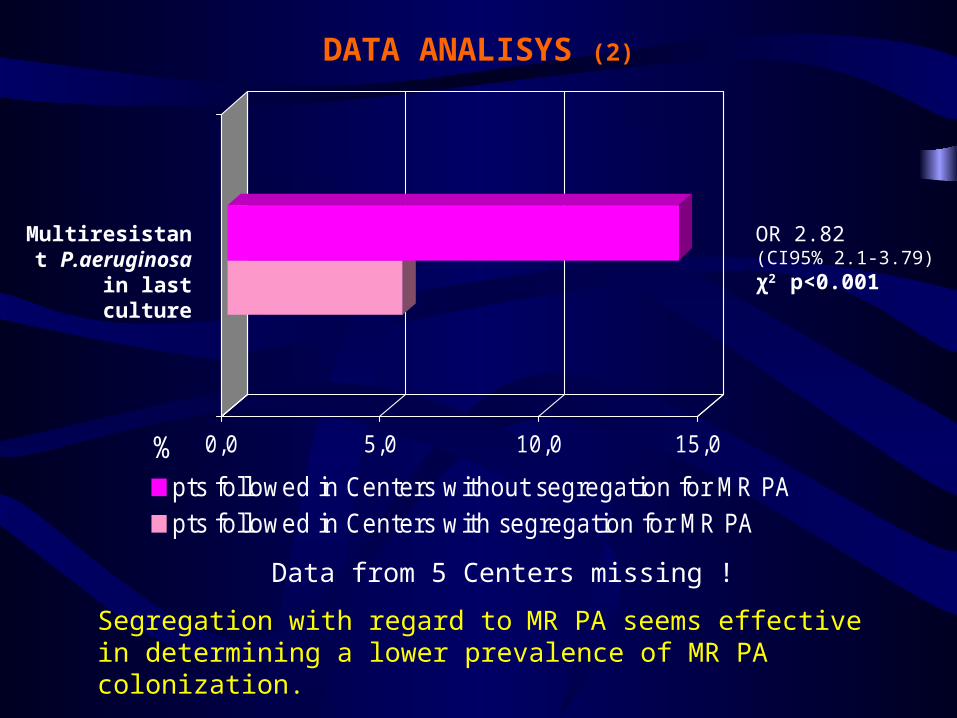
DATA ANALISYS (2)
0,0 5,0 10,0 15,0%pts followed in Centers without segregation for MR PApts followed in Centers with segregation for MR PA
OR 2.82 (CI95% 2.1-3.79)χ2 p<0.001
Multiresistant P.aeruginosa in last culture
Data from 5 Centers missing !
Segregation with regard to MR PA seems effective in determining a lower prevalence of MR PA colonization.
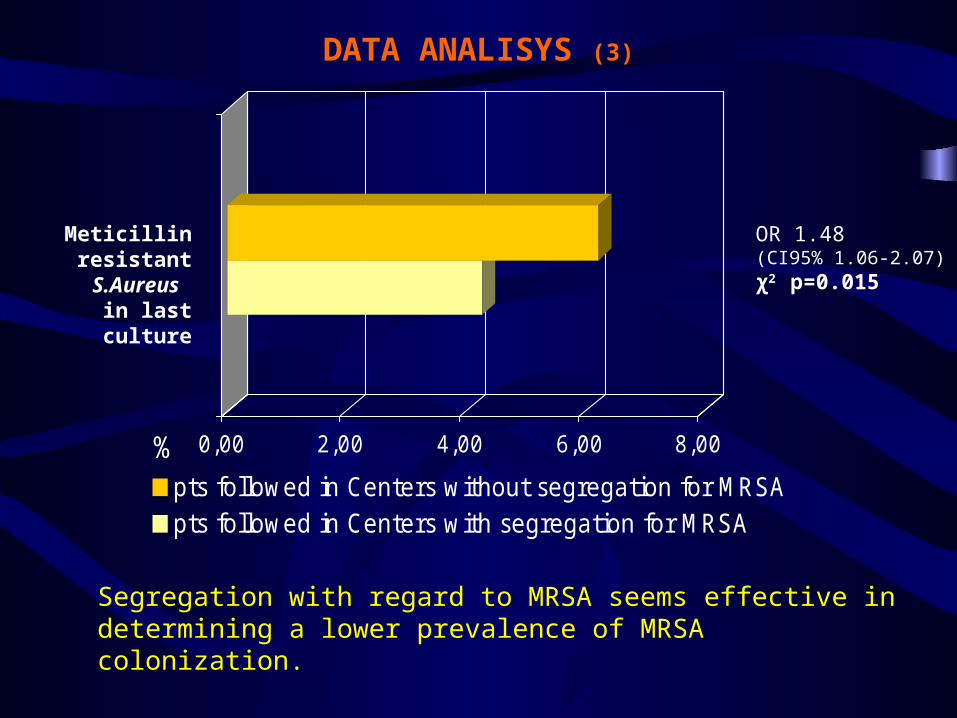
DATA ANALISYS (3)
0,00 2,00 4,00 6,00 8,00%pts followed in Centers without segregation for MRSApts followed in Centers with segregation for MRSA
OR 1.48 (CI95% 1.06-2.07)χ2 p=0.015
Meticillin resistant
S.Aureus in last culture
Segregation with regard to MRSA seems effective in determining a lower prevalence of MRSA colonization.
DATA ANALISYS (4)
No correlation between the prevalence of each single pathogen
in each CF Center and :
- Number of patient followed by each Center
- Number of yearly visits performed in the outpatient Clinic
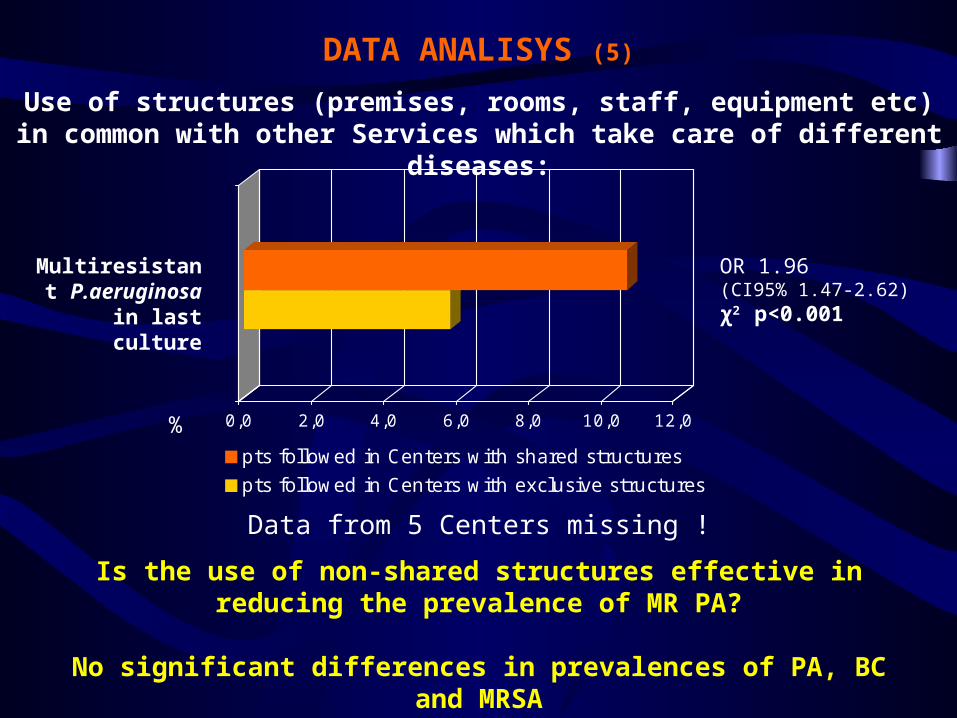
DATA ANALISYS (5)
Use of structures (premises, rooms, staff, equipment etc) in common with other Services which take care of different
diseases:
0,0 2,0 4,0 6,0 8,0 10,0 12,0%
pts followed in Centers with shared structures
pts followed in Centers with exclusive structures
OR 1.96 (CI95% 1.47-2.62)χ2 p<0.001
Multiresistant P.aeruginosa in last culture
Data from 5 Centers missing !
Is the use of non-shared structures effective in reducing the prevalence of MR PA?
No significant differences in prevalences of PA, BC and MRSA
DATA ANALISYS (6)
Comparison with 2001 CFF Registry data:
Higher prevalence of P.aeruginosa in USA than in Italy
(58.8% vs. 54.1%, χ2 p<0.001)
Higher prevalence of B.cepacia in Italy than in USA(6.4% vs.3.1%, χ2 p<0.001)
DISCUSSION (1)
•In general, policies and measures adopted by Italian Centers seem effective in controlling infections from respiratory pathogens in CF patients.
•Nonetheless in a few Centers some measures are still being used whose inefficacy has been proved (e.g. environmental nebulisation of disinfectant) or which put patients at serious risk of contamination (e.g. use of shared AT devices after simple disinfection).
DISCUSSION (2)
•Many factors are involved in and concur to the prevention and control of infection from respiratory pathogens in CF:Characteristics of the CF Center’s structureType of segregation policy adoptedMeasures of segregation adoptedProtocolos of disinfection usedStaff members’ hygienic practicesBehavioural rules suggested to patients
•A local policy for infection control should consider as many factors as possible among the above mentioned, considering available resources.
•Many CF Centers staffs have complained of the shortage of structural, logistic and human resources available, which seems to be an important barrier to an effective infection control.
SUGGESTIONS
•Adopt a written protocol for prevention and control of infections from respiratory pathogens, which takes into account the resources available locally.
•Provide that all staff members are aware of the airways microbiological status of the CF patients they are assisting.
•Consider the implementation of regular environmental microbiological controls.
•Program a Consensus on national guidelines about prevention and control of infections

Gruppo Infermieri del GIFC
www.infermieri-fc.net
Italian Cystic Fibrosis Nurses’ Group