Embed Size (px)
Citation preview

Incidence of stroke following thoracic endovascular aortic repair for descending
aortic aneurysm: A Systematic Review of the Literature with Meta-analysis
Regula S von Allmen1*, Brigitta Gahl2, Janet T Powell3
1 Clinic for vascular surgery, Kantonsspital St. Gallen, Rorschacherstrasse, St. Gallen,
Switzerland
2 Clinic for cardiovascular surgery, University Hospital Bern and University of Bern,
Switzerland
3 Vascular Surgery Research Group, Imperial College London, Charing Cross Campus,
London, UK
* Address for correspondence: Regula S von Allmen; [email protected]; clinic for
vascular surgery, Kantonsspital St. Gallen, Rorschacherstrasse, St. Gallen, Switzerland
Original article
Systematic review and Meta-analysis
Running head: Meta-analysis on stroke risk following TEVAR
This work has been presented as a poster at the annual conference of the European Society
of Vascular Surgery in Porto, Portugal 2015
Word count: 3609
Abstract: 282
1

Keywords
stroke; cerebrovascular event; TEVAR; endovascular; thoracic aortic aneurysms; systematic
review; meta-analysis
2

What this study adds
This is a comprehensive review including a meta-analysis looking specifically at the stroke
risk of patients undergoing thoracic endovascular aortic repair (TEVAR) for descending
thoracic aortic aneurysm, thus eliminating heterogeneity regarding patient selection as
effectively as possible. There is an indication that stroke risk is increased if the left
subclavian artery (LSA) is covered during the procedure without revascularisation. Such data
are important for informing patients of procedure risks and to increase research efforts
towards stroke prevention.
3
1
2
3
4
5
6
7
8

Abstract
Objectives: Stroke is an increasingly recognised complication following thoracic
endovascular aortic repair (TEVAR).The aim of this study was to synthesise systematically
the published data on perioperative stroke incidence during TEVAR for patients with
descending thoracic aneurysmal disease and assess the impact of left subclavian artery
(LSA) coverage on stroke incidence.
Data sources: A systematic review of English and German articles using MEDLINE and
EMBASE (2005–2015).
Review methods: A systematic review of studies looking at perioperative (in-hospital or
30day) stroke incidence following TEVAR for descending aortic aneurysm was performed,
including studies with ≥50 cases, published after January 2005. Pooled prevalence rate of
perioperative stroke and 95 per cent confidence interval (95% CI) was estimated using
random effect analyses. Heterogeneity was examined using I2 statistic.
Results: Of 215 studies identified, ten were considered suitable for inclusion. The included
studies enrolled a total of 2594 persons (61% were male) during 1997-2014 with a mean
weighted age of 71.8 (95% CI 71.1 to 73.6) years. The pooled prevalence rate for stroke was
4.1% (95% CI 2.9 to 5.5) with moderate heterogeneity between studies (I2=49.8%, P=0.04).
Five studies reported stroke incidences stratified by the management of the LSA; i.e.
uncovered versus covered and revascularised versus covered and not-revascularised. In
cases where the LSA remained uncovered, the pooled stroke incidence was 3.2% (95% CI
1.0 to 6.5). There was however, an indication that stroke incidence increased following LSA
coverage, to 5.3% (95% CI 2.6 to 8.6) in those with a revascularisation and 8.0% (95% CI
4.1 to 12.9) in those without revascularisation.
Conclusion: Stroke incidence is an important morbidity after TEVAR, and probably increases
if the LSA is covered during the procedure, particularly in those without revascularisation.
4
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
29
30
31
32
33

Introduction
Thoracic endovascular aortic repair (TEVAR) is regarded as a lower-risk treatment for a
variety of thoracic aortic conditions and thus, is the preferred treatment approach over open
repair in many cases.1, 2 Due to its minimal invasiveness compared to open repair, TEVAR
has gained widespread adoption and has also been propagated in official guidelines to be
applied at an even lower diameter aneurysm threshold than open repair.3 The endovascular
aortic repair technique likely meets the wish of patients for a rapid recovery. Associated
neurologic complications, however, interfere considerably with this wish; first, neurologic
events may be fatal in up to 33%4 and second, the consequences of neurologic events, i.e.
long-term disability and handicap are highly correlated with impaired physical health related
quality of life.5 The most dreaded neurologic complications are paraplegia and stroke. The
incidence of spinal cord ischaemia following TEVAR varies considerably across studies
between 0 to more than 10%6-11 and a considerable body of research has led to a reduction
in paraplegia rate.12 So far, the reduction of stroke during endovascular aortic interventions
has attracted less interest, apart from differential revascularisation strategies when left
subclavian artery (LSA) coverage is needed. The risk of stroke during TEVAR is not
surprising; atherosclerotic disease of the aortic arch is not only a recognised risk factor for
unprovoked stroke13, but also for neurologic events after open heart surgery or during carotid
artery stenting.14 A recent study looking at midterm outcomes after TEVAR in relation to
aortic pathology reported a more than two-fold higher early-term stroke incidence among
thoracic aortic aneurysm patients compared to those with an aortic dissection.15 This may be
a reflection of more advanced atherosclerotic disease among the aneurysm patients.
Therefore, new therapies might focus on plaque-stabilisation, e.g. utilisation of high dose
statins, to prevent stroke and on the evolvement of technical adjuncts (i.e. further
development of fusion imaging techniques), which would allow to reduce the time the
endograft dangles within the aortic arch causing plaque dislocation. However, before
5
34
35
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59

designing any such studies, it is essential to know the exact magnitude of the problem, i.e.
stroke incidence.
Therefore, the aim of this study was to synthesise the published data on stroke incidence
following TEVAR for descending thoracic aortic aneurysm in a systematic review.
6
60
61
62
63

Methods
Systematic review and protocol
The systematic review followed quality reporting guidelines set by the PRISMA (Preferred
Reporting Items for Systematic reviews and Meta-Analysis) group (http://www.prisma-
statement.org/).16 A review protocol including every step of the systematic review was
developed and approved by all authors.
Search strategy
Medline and EMBASE were initially searched up until the 16th February 2015, and
subsequently updated until 30th June 2016 using the following search terms in different
combinations; "Aorta, Thoracic/surgery"[Mesh], "Aorta, Thoracic/therapy"[Mesh], “stroke”,
“neurologic deficit”. Filters were used to restrict studies to human studies only and to articles
in English and German published 2005 onwards in order to focus on procedures with
technologically more advanced devices. In addition, reference lists of reviews were also
searched for further studies to be included.
Eligibility criteria, study selection
Potential studies were reviewed according to a set of eligibility criteria. The study participants
(minimum n=50, men or women) must have undergone TEVAR with indications being
separable between descending thoracic aortic aneurysms, traumatic aortic lesions and aortic
dissections. Studies were not excluded if penetrating aortic ulcers were not separable from
aneurysms. Studies on patients with connective tissue disease were excluded as well as
studies involving ascending aortic aneurysms. In addition, the following were also excluded:
review articles, studies where patient data were duplicated (in which case the most recent or
7
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
86
87

comprehensive study was used), editorials, letters and case reports. Study authors were
contacted in cases where outcome data could not easily be separated according to
underlying aortic pathology.
Data collection process
A data extraction form to identify variables in the eligible studies was designed. The following
were extracted: the study design (prospective, retrospective, case series, observational
studies with or without comparison group, registries, multicentre or single-centre), author
affiliation, date of publication, and country (where study was undertaken), year of publication,
recruitment period, inclusion and exclusion study criteria, baseline data including age, sex
and other cardiovascular risk factors (e.g. blood pressure, history of smoking, drugs (i.e.
statins), ischaemic heart disease, diabetes), type of endograft, information on coverage of
the LSA and on revascularisation strategies, outcomes (stroke incidence in hospital or within
30 days of intervention, mortality rate in hospital or within 30 days of intervention). Two
authors (RSvA, JTP) independently extracted data of the potentially eligible primary studies
and crosschecked their results. Any disagreements between the two reviewers were
discussed and finally settled by agreement.
For studies that failed to provide baseline variables (age separable by aortic pathology,
stroke incidence according to coverage of LSA) study authors were contacted for completion
and if these variables were not available the studies were excluded for these specific
analyses.
Estimation of perioperative stroke incidence
The reported overall mean stroke incidence either within 30 days or in-hospital (if 30-day
outcome was not reported) was extracted from each study. In studies that reported on LSA
8
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112

coverage, stroke incidences were extracted according to revascularisation strategy of the
LSA (uncovered versus covered and revascularised versus covered and non-
revascularised).
Study quality
The Newcastle-Ottawa Scale was used to assess the quality of the included studies using a
'star system' based on three broad perspectives: the selection of the study groups; the
comparability of the groups; and the ascertainment of either the exposure or outcome of
interest for cohort studies. The different items were adapted to the study question of interest
(supplemental material). None of the studies could score for representativeness of the
exposed cohort, however a star was given for selection of the non-exposed cohort if
information on previous stroke had been reported. Each study was given two points; one for
ascertainment of exposure because all information relied on surgical records and for
demonstration that the outcome of interests was not present at the start of the study.
Consequently, in the selection category, all studies were given 2-3 points. Regarding
comparability category, studies yielded 0-2 points. They were given one point if key factors
were controlled for, i.e. coverage of the LSA and another point if separable details were
given for thoracic aortic aneurysm patients relating to age and sex ratio. In the final category
‘Outcome’ all studies yielded 1-3 points: Assessment of follow up was scored with one point
if a good quality assessment for stroke was applied (i.e. by imaging, diagnosed by
specialised neurologist). All the studies were given one point for the item ‘was follow-up long
enough for outcomes to occur’ because the outcome of interest was a postoperative event
and was an inclusion criterion. Studies with no patients lost to follow up for the early
postoperative primary outcome were given one point for ‘adequacy of follow up of cohorts’.
Taken together, all studies could receive a score of minimum 3 to maximum 8 points. The
9
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137

quality of reporting was independently analysed by two authors (RSvA and JTP);
disagreement were solved by consensus.
Statistical analysis
All analyses were conducted using STATA 12 (StataCorp, College Station, Texas, USA).
Meta-analysis estimates such as weighted summary proportions were generated in random
effects meta-analyses model17 and heterogeneity was assessed using the I2 test.18 We follow
Higgins et al. in quantifying heterogeneity by I2 into low (25%), moderate (50%), and high
(75%).18 The pooled estimates were calculated using the Freeman-Tukey double arcsine
transformation 19 and standard continuity correction (0.5) for zero events was used to
stabilise variances. The confidence intervals were based on the Wilson score method using
asymptotic variance.20
If means for age were not reported (one out of ten studies), the mean was approximated
using the median.21 If the range was quoted in place of standard deviation, it was converted
to standard deviation according to the recommendations of Hozo et al.21 In studies that
reported interquartile ranges, this was first converted to standard deviations (sd) using the
formula sd=IQR/1.35.21 The same was applied to the estimation of maximum aneurysm
diameter.
Three studies (Clough et al.22, Maldonado et al.23 and Patterson et al.15) reported separate
stroke incidences for the three different management strategies of the LSA, e.g. uncovered,
covered plus revascularisation and covered without revascularisation. Two further studies
reported separate stroke incidences for the two treatments, where LSA has been covered,
e.g. with and without revascularisation (Makaroun et al.24 and Fossaceca et al.25). For a
comparison of the stroke incidences following these strategies, we calculated risk ratios
using all available data, thus including the three or the five studies, respectively.
10
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162

An alternative funnel plot was constructed using study size instead of the inverse of standard
error on the y-axis due to the acknowledged risk of potentially misleading funnel plots for
non-comparative meta-analyses when traditionally constructed, which may be particularly
true for low or high proportional outcomes.25 In such circumstances, plot asymmetry could be
mistakenly interpreted as presence of a publication bias, whereas it has been proven that it
may have been caused by scale artefact due to correlations between outcome measures
and measure of precision.25
A sensitivity analysis for study size (≤ 150 versus >150 patients) was performed, with respect
to the primary endpoint to further investigate the possibility of a publication bias.
11
163
164
165
166
167
168
169
170
171

Results
Identification of relevant studies
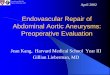
A total of 215 study titles were identified by the initial search strategy after removing
duplicate entries and of these 139 titles were excluded after title screening (Figure 1). A total
of 76 potential papers were selected. In the next stage, full records were reviewed. Of the
eligible publications, 66 were excluded for one or more of the following reasons: too few
patients (n=12); no original data or case reports (n=21); Studies with duplicated data/patients
(n=8); data not separable for descending thoracic aneurysms (n=22); reporting on occlusive
cerebrovascular disease (n=1); reporting on open repair only (n=1); stroke not being an
outcome (n=1). Ten studies were identified as potentially eligible for inclusion in the
systematic review and meta-analysis.15, 22-24, 26-30 Included studies are summarised in Table 1.
Data extraction: study characteristics
The publication dates of the ten potentially eligible studies for the meta-analysis ranged from
2005 to 2015 with patient recruitment from 1997 to 2014. Of these, six were prospective
studies (no randomised trials) and four were retrospective. Additional data from the study
authors were obtained for 2 studies.
Post-operative stroke was an outcome measure in all studies, defined as an event within 30
days for all except for the study from Clough et al.22, which reported in-hospital events only.
The diagnosis of stroke, stroke severity and fatality were reported inconsistently in the ten
included studies.
The included studies reported on 2594 persons with study sizes ranging from 53 to 823
patients. Sex ratio and age were extracted in all but two studies (Buth et al.27, Illig et al.31),
but in those that did, the proportion of men ranged from 58 to 85% of the study population.
12
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195

Mean or median age was extractable from all studies apart from the studies of Buth et al.27
and Illig et al.31, in which age was not separable for descending aortic aneurysm. The mean
study age ranged from 70-75 years resulting in a mean weighted age of 71.8 (95% CI 71.1
to 73.6).
All but two studies (Makaroun et al.24 and Illig et al.31) also included patients with
symptomatic thoracic aortic aneurysms, but the proportion with symptomatic lesions varied
considerably across studies from 6% (Patterson et al.15) to 43% (Andrassy et al.26)
Other patient characteristics, such as history of smoking, prevalence of diabetes, arterial
hypertension, proportion of participants with ischaemic heart disease and use of statins as
well as maximum aneurysm diameter were reported inconsistently across the ten studies
(Table 2). Information on thoracic aneurysm diameter and use of statin therefore were not
included.
Study quality according to the modified Newcastle-Ottawa Scale
Total quality score across all ten studies ranged from 4 to 8 (Table 1). A retrospective study
with the lowest sample size (Fossaceca et al.29) yielded the lowest quality score, while a
prospective phase 2 multi-centre study (Makaroun et al.24) achieved the highest quality
score. The majority (nine out of ten) scored a minimum five points indicating that most
studies were of at least moderate quality.
Prevalence rate of stroke
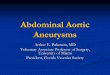
The pooled prevalence rate for stroke was 4.1% (95% CI 2.9 to 5.5) with moderate
heterogeneity between studies (I2=49.8%, P=0.04). The point prevalence of stroke within the
ten studies ranged between 0 to 7.2%. The largest study (Maldonado et al23) published the
13
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
215
216
217
218
219

highest mean stroke incidence of 7.2% (95% CI 5.6 to 9.1). The corresponding forest plot is
shown in Figure 2, in which studies are sorted by study size.
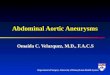
The funnel plot, Figure 3, showed some evidence of bias: it was asymmetrical with respect
to a vertical line in the middle of the plot, and the points closer to the horizontal line were
shifted to the left, indicating that smaller studies reported lower stroke incidences. In a
sensitivity analysis stratifying studies by size, smaller studies with ≤ 150 patients had a
stroke incidence of 2.03% (95% CI 1.0 to 4.1) with low heterogeneity (I2 = 0.0%), whereas
larger studies reported a pooled stroke incidence of 5.4% (95% CI 3.0 to 6.9) with moderate
heterogeneity (I2 = 45.7%). Overall there was a small overlap of the confidence intervals
and significant heterogeneity between the groups (P = 0.021) with moderate overall
heterogeneity (I2 = 49.8%).
Stroke incidenceassociated with the management of the left subclavian artery during TEVAR
The three studies, that reported strokes stratified by the management of the LSA (Clough et
al.22, Maldonado et al.23 and Patterson et al.15); i.e. uncovered versus covered and
revascularised versus covered and not-revascularised, provided data on 1686 patients. In
these patients, the overall stroke incidence was 6.3% (95% CI 5.2 to 7.5). Two further
studies (Makaroun et al24 and Fossaceca et al.29) reported strokes separately for the two
treatments; i.e. revascularised versus covered and not-revascularised, providing data on 195
patients with five strokes. Overall stroke incidence across all the five studies was 4.9% (95%
CI 3.2 to 7.0).
In cases where the LSA remained uncovered, the pooled stroke incidence was 3.2% (95%
CI 1.0 to 6.1). There was, however, an indication for an increased pooled stroke incidence
following LSA coverage, with 5.3% (95% CI 2.6 to 8.6) for those with a revascularisation
versus 8.0% (95% CI 4.1 to 12.4) in those without revascularisation. The pairwise
comparison of the stroke incidence per treatment, using all available, information showed a
14
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245

risk ratio (RR) of covered and revascularised versus uncovered of 1.4 (95% CI 0.8 to 2.2), I2
= 37.4%. The RR of the two covered strategies without versus with revascularisation was
0.77 (95% CI 0.39 to 1.5), I2 = 38.9%. For those without revascularisation, the RR of covered
cases versus uncovered was 1.7 (95% CI 1.0 to 2.6), I2 = 79.9% showing a lower risk for
patients without LSA coverage. The corresponding forest plots are shown in supplemental
material.
Mortality rate
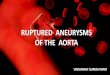
30-day mortality was available from nine studies and yielded a pooled mortality rate of 4.3%
(95% CI 1.9 to 7.5), but with high heterogeneity between the studies (I2=89.4%, P < 0.001).
Buth et al.27 did not report mortality. The corresponding forest plot is shown in Figure 4.
15
246
247
248
249
250
251
252
253
254
255
256

Discussion
This systematic review, with meta-analysis, focused on post-operative stroke
incidencefollowing TEVAR for descending aortic aneurysms and has shown that stroke
affects at least one in every 25th patient, with an increased risk after coverage of the LSA
without revascularisation. Overall stroke incidenceoccurred in 4.1% of patients with a slightly
lower rate in cases where the LSA remained uncovered (3.2%), with an indication for an
increased stroke incidence following LSA coverage, with stroke in 5.3% patients after LSA
revascularisation rising to 8% in patients where the LSA was covered without
revascularisation. The larger studies reported higher stroke incidences.
A recent narrative review from Waterford et al.32 of stroke incidence following TEVAR
for various aortic pathologies focused on how stroke incidence varied with management of
the LSAstroke incidence. Their heterogeneous patient selection, together with inclusion of
duplicate patient data make generalisation of their findings difficult. In contrast, we restricted
our study to TEVAR for descending thoracic aortic aneurysms only. stroke incidenceWe
included fewer studies and less patients, partly because we restricted the aortic pathology
and excluded (according to protocol) small studies and those with duplicate patients. For
stroke incidence we still observed moderate heterogeneity with an I2 of 49.8% with smaller
studies reporting a lower stroke incidence, with lower heterogeneity. In a subgroup analysis
Waterford et al. reported pooled stroke incidence following TEVAR for all thoracic
aneurysms and found an overall increased stroke risk of 4.3% compared to TEVAR for
dissections (3.2%, P=0.043). Our review found a similar stroke risk of 4.1%, even though we
focused only on descending thoracic aneurysms and included two studies (Clough et al.22
and Maldonado et al.23) with 1016 patients, which had higher stroke incidences of 7.2 and
6.2%, respectively.
Waterford et al. stroke incidenceacknowledged that there are different approaches to
revascularise the LSA, some of which were associated with more extensive stentgraft
16
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282

coverage of the aortic arch, thus covering other supraaortic vessel branches. There is
evidence that stroke risk increases with the involvement of the aortic arch,33 probably due to
an increased risk of embolisation from a diseased arch. By including only descending
thoracic aortic aneurysms, we minimised this problem. Waterford et al.32 reported a stroke
incidence of 7.4% with LSA coverage compared to 4% in patients with devices deployed
distally to the LSA. In their review LSA coverage without revascularisation was associated
with a stroke incidence of 5.6%, while stroke incidence was 3.1% in those with LSA
revascularisation, but this difference did not reach statistical significance. In our review, we
observed a similar trend with a stroke incidence of 3.2% in uncovered situations compared
to an increased stroke incidence of 5.3% in those with covered and revascularised LSA and
8.0% in non-revascularised cases, a trend confirmed by another recent meta-analysis
looking specifically at revascularisation strategies in LSA coverage.34 Since we have
provided some evidence of publication bias, with the smaller studies reporting lower stroke
incidence, our inclusion of two larger studies (not included by Waterford), is likely to be an
important contributor to the higher stroke risks, which we report. On a real life population
basis, the stroke incidence may be even higher. The need for LSA coverage is an obvious
indicator for a more extensive procedure being associated with a higher adverse event rate.
A recent Cochrane database review also concluded that optimal management of LSA
coverage in TEVAR is still unknown.34
It has been suggested that strokes following LSA coverage were mainly due to
haemodynamic problems as a result of a compromised vertebral circulation. Ullery et al.35
looked specifically at stroke distribution in a series of 530 patients undergoing TEVAR for a
variety of aortic conditions. The risk of stroke in the posterior circulation was 6 times higher
in cases with LSA coverage (OR 6.11, 95% CI 1.15; 32.3) associated with increased
mortality (33% versus 0%) and a lower complete recovery rate (75% versus 17%) compared
to patients with a stroke in the anterior circulation.35 Revascularisation of the LSA seems a
17
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308

logical procedure to prevent particularly stroke in the posterior circulation. The present data
however cannot confirm that the stroke risk is significantly reduced by LSA revascularisation.
Other preventive measures towards mitigation of perioperative procedure-related
cerebral events, apart from LSA revascularisation, have not been investigated. The main
cause of cerebral lesions seems from embolisation of aortic debris from intravascular
manipulations, which is intrinsic to the procedure. The overall risk of embolisation is
significant, with a neuroimaging study identifying new cerebral lesions in almost two third of
patients following TEVAR.36 This risk is well known for many endovascular interventions that
are associated with navigation of the aortic arch with guidewires, catheters and even
delivery-systems and new mainly clinically undetected cerebral lesions have been reported
in up to 50% after carotid artery stenting37 and in more than 80% of cases following
transfemoral aortic valve implantation.38 This could be a particularly important research topic
for the future as this is a common feature for all endovascular treatment modalities with
aortic arch navigation and since long-term sequelae of such silent brain lesions are still
unknown.
Certain limitations of this review need to be acknowledged. First, some of the included
studies were not of very good quality. Second, reporting of stroke was heterogeneous not
formally requiring a radiological or specialised neurological assessment in all studies. Thus,
clinically less apparent strokes could have been underreported. Third, only insufficient data
relating to study subgroups, i.e. sex, were available, so that such relevant confounders might
have remained unrecognised. Fourth, we also may have included few patients with a
penetrating aortic ulcer (PAU), as this pathology was not always clearly separable from
aneurysms in the earlier publications. Whilst this might have introduced a certain bias as
patients with aortic ulcers show heavy atherosclerotic burden and are probably more prone
to dislodgment of embolic material, in the Illig study31 all the strokes occurred in the
aneurysm patients and none in the excluded PAU patients. Finally, although this study
strived to reduce heterogeneity by including descending aortic aneurysms only, moderate
18
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335

heterogeneity was found. This may be due to case-mix problems with smaller studies
including only easy cases whilst more complex cases were included in the larger and
multicentre studies.
In conclusion, stroke incidence is an important morbidity after TEVAR and more research is
needed to reduce the risk in the future, particularly where the LSA is to be covered.
Importantly, information on the actual stroke risk needs to be incorporated into patient
information sheets.
19
336
337
338
339
340
341
342

Conflicts of interests:
None
20
343
344

References
1. Glade GJ, Vahl AC, Wisselink W, Linsen MA, Balm R. Mid-term survival and costs of
treatment of patients with descending thoracic aortic aneurysms; endovascular vs. open
repair: a case-control study. Eur J Vasc Endovasc Surg. 2005;29(1):28-34.
2. Fattori R, Tsai TT, Myrmel T, Evangelista A, Cooper JV, Trimarchi S, et al.
Complicated acute type B dissection: is surgery still the best option?: a report from the
International Registry of Acute Aortic Dissection. JACC Cardiovasc Interv. 2008;1(4):395-
402.
3. Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, et al.
2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering
acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task
Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of
Cardiology (ESC). Eur Heart J. 2014;35(41):2873-926.
4. Gutsche JT, Cheung AT, McGarvey ML, Moser WG, Szeto W, Carpenter JP, et al.
Risk factors for perioperative stroke after thoracic endovascular aortic repair. Ann Thorac
Surg. 2007;84(4):1195-200; discussion 200.
5. Patel MD, Tilling K, Lawrence E, Rudd AG, Wolfe CD, McKevitt C. Relationships
between long-term stroke disability, handicap and health-related quality of life. Age Ageing.
2006;35(3):273-9.
6. Greenberg RK, Lu Q, Roselli EE, Svensson LG, Moon MC, Hernandez AV, et al.
Contemporary analysis of descending thoracic and thoracoabdominal aneurysm repair: a
comparison of endovascular and open techniques. Circulation. 2008;118(8):808-17.
7. Feezor RJ, Martin TD, Hess PJ, Jr., Daniels MJ, Beaver TM, Klodell CT, et al. Extent
of aortic coverage and incidence of spinal cord ischemia after thoracic endovascular
aneurysm repair. Ann Thorac Surg. 2008;86(6):1809-14; discussion 14.
21
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368

8. Conrad MF, Ye JY, Chung TK, Davison JK, Cambria RP. Spinal cord complications
after thoracic aortic surgery: long-term survival and functional status varies with deficit
severity. J Vasc Surg. 2008;48(1):47-53.
9. Gravereaux EC, Faries PL, Burks JA, Latessa V, Spielvogel D, Hollier LH, et al. Risk
of spinal cord ischemia after endograft repair of thoracic aortic aneurysms. J Vasc Surg.
2001;34(6):997-1003.
10. Matsuda H, Fukuda T, Iritani O, Nakazawa T, Tanaka H, Sasaki H, et al. Spinal cord
injury is not negligible after TEVAR for lower descending aorta. Eur J Vasc Endovasc Surg.
2010;39(2):179-86.
11. Drinkwater SL, Goebells A, Haydar A, Bourke P, Brown L, Hamady M, et al. The
incidence of spinal cord ischaemia following thoracic and thoracoabdominal aortic
endovascular intervention. Eur J Vasc Endovasc Surg. 2010;40(6):729-35.
12. Etz CD, Weigang E, Hartert M, Lonn L, Mestres CA, Di Bartolomeo R, et al.
Contemporary spinal cord protection during thoracic and thoracoabdominal aortic surgery
and endovascular aortic repair: a position paper of the vascular domain of the European
Association for Cardio-Thoracic Surgerydagger. Eur J Cardiothorac Surg. 2015;47(6):943-
57.
13. Amarenco P, Cohen A, Tzourio C, Bertrand B, Hommel M, Besson G, et al.
Atherosclerotic disease of the aortic arch and the risk of ischemic stroke. N Engl J Med.
1994;331(22):1474-9.
14. Kastrup A, Groschel K, Schnaudigel S, Nagele T, Schmidt F, Ernemann U. Target
lesion ulceration and arch calcification are associated with increased incidence of carotid
stenting-associated ischemic lesions in octogenarians. J Vasc Surg. 2008;47(1):88-95.
15. Patterson B, Holt P, Nienaber C, Cambria R, Fairman R, Thompson M. Aortic
pathology determines midterm outcome after endovascular repair of the thoracic aorta:
report from the Medtronic Thoracic Endovascular Registry (MOTHER) database. Circulation.
2013;127(1):24-32.
22
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
385
386
387
388
389
390
391
392
393
394
395

16. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al. The
PRISMA statement for reporting systematic reviews and meta-analyses of studies that
evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
17. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials.
1986;7(3):177-88.
18. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-
analyses. BMJ. 2003;327(7414):557-60.
19. Freeman MF, Turkey JW. Transformations related to the angular and the square
root. Annals of Mathematical Statistics 1950;21:607-11.
20. Newcombe RG. Two-sided confidence intervals for the single proportion: comparison
of seven methods. Stat Med. 1998;17(8):857-72.
21. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median,
range, and the size of a sample. BMC Med Res Methodol. 2005;5:13.
22. Clough RE, Patel AS, Lyons OT, Bell RE, Zayed HA, Carrell TW, et al. Pathology
specific early outcome after thoracic endovascular aortic repair. European journal of vascular
and endovascular surgery : the official journal of the European Society for Vascular Surgery.
2014;48(3):268-75.
23. Maldonado TS, Dexter D, Rockman CB, Veith FJ, Garg K, Arko F, et al. Left
subclavian artery coverage during thoracic endovascular aortic aneurysm repair does not
mandate revascularization. Journal of vascular surgery. 2013;57(1):116-24.
24. Makaroun MS, Dillavou ED, Kee ST, Sicard G, Chaikof E, Bavaria J, et al.
Endovascular treatment of thoracic aortic aneurysms: results of the phase II multicenter trial
of the GORE TAG thoracic endoprosthesis. J Vasc Surg. 2005;41(1):1-9.
25. Hunter JP, Saratzis A, Sutton AJ, Boucher RH, Sayers RD, Bown MJ. In meta-
analyses of proportion studies, funnel plots were found to be an inaccurate method of
assessing publication bias. J Clin Epidemiol. 2014;67(8):897-903.
23
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421

26. Andrassy J, Weidenhagen R, Meimarakis G, Rentsch M, Jauch KW, Kopp R.
Endovascular versus open treatment of degenerative aneurysms of the descending thoracic
aorta: a single center experience. Vascular. 2011;19(1):8-14.
27. Buth J, Harris PL, Hobo R, van Eps R, Cuypers P, Duijm L, et al. Neurologic
complications associated with endovascular repair of thoracic aortic pathology: Incidence
and risk factors. a study from the European Collaborators on Stent/Graft Techniques for
Aortic Aneurysm Repair (EUROSTAR) registry. Journal of vascular surgery.
2007;46(6):1103-10; discussion 10-1.
28. Chaikof EL, Mutrie C, Kasirajan K, Milner R, Chen EP, Veeraswamy RK, et al.
Endovascular repair for diverse pathologies of the thoracic aorta: an initial decade of
experience. Journal of the American College of Surgeons. 2009;208(5):802-16; discussion
16-8.
29. Fossaceca R, Guzzardi G, Cerini P, Parziale G, Stanca C, Micalizzi E, et al.
Endovascular treatment of thoracic aortic aneurysm: a single-center experience. Ann Vasc
Surg. 2013;27(8):1020-8.
30. Matsumura JS, Cambria RP, Dake MD, Moore RD, Svensson LG, Snyder S, et al.
International controlled clinical trial of thoracic endovascular aneurysm repair with the Zenith
TX2 endovascular graft: 1-year results. J Vasc Surg. 2008;47(2):247-57; discussion 57.
31. Illig KA, Ohki T, Hughes GC, Kato M, Shimizu H, Patel HJ, et al. One-year outcomes
from the international multicenter study of the Zenith Alpha Thoracic Endovascular Graft for
thoracic endovascular repair. J Vasc Surg. 2015;62(6):1485-94 e2.
32. Waterford SD, Chou D, Bombien R, Uzun I, Shah A, Khoynezhad A. Left Subclavian
Arterial Coverage and Stroke During Thoracic Aortic Endografting: A Systematic Review.
Ann Thorac Surg. 2016;101(1):381-9.
33. Melissano G, Tshomba Y, Bertoglio L, Rinaldi E, Chiesa R. Analysis of stroke after
TEVAR involving the aortic arch. Eur J Vasc Endovasc Surg. 2012;43(3):269-75.
24
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447

34. Hajibandeh S, Hajibandeh S, Antoniou SA, Torella F, Antoniou GA. Meta-analysis of
Left Subclavian Artery Coverage With and Without Revascularization in Thoracic
Endovascular Aortic Repair. J Endovasc Ther. 2016;23(4):634-41.
35. Ullery BW, McGarvey M, Cheung AT, Fairman RM, Jackson BM, Woo EY, et al.
Vascular distribution of stroke and its relationship to perioperative mortality and neurologic
outcome after thoracic endovascular aortic repair. Journal of vascular surgery.
2012;56(6):1510-7.
36. Kahlert P, Eggebrecht H, Janosi RA, Hildebrandt HA, Plicht B, Tsagakis K, et al.
Silent cerebral ischemia after thoracic endovascular aortic repair: a neuroimaging study. Ann
Thorac Surg. 2014;98(1):53-8.
37. Bonati LH, Jongen LM, Haller S, Flach HZ, Dobson J, Nederkoorn PJ, et al. New
ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid
stenosis: a substudy of the International Carotid Stenting Study (ICSS). Lancet Neurol.
2010;9(4):353-62.
38. Kahlert P, Knipp SC, Schlamann M, Thielmann M, Al-Rashid F, Weber M, et al.
Silent and apparent cerebral ischemia after percutaneous transfemoral aortic valve
implantation: a diffusion-weighted magnetic resonance imaging study. Circulation.
2010;121(7):870-8.
25
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465

Figure Legend
Figure 1 PRISMA flow diagram
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow
diagram showing an overview of the study selection process
Figure 2 The effect size for the overall risk of stroke (within 30 days or in-hospital)
after thoracic endovascular aortic repair of descending artic aneurysms including the
95% confidence intervals.
Author, date, risk of stroke as a weighted summary proportion (95% CI) are shown. Studies
are listed by study size.
Figure 3 Funnel plot asymmetry used to determine publication bias
In this alternative Funnel plot, study size was used on the y-axis due to the acknowledged
risk of potentially misleading funnel plots for non-comparative meta-analyses when
traditionally constructed. The plot shows some evidence of bias with smaller studies
reporting a lower rate of strokes.
Figure 4
The effect size for the overall mortality (within 30 days or in-hospital) after thoracic
endovascular aortic repair of descending aortic aneurysms including the 95%
confidence intervals.
Author, date, risk of mortality as weighted summary proportion (95% CI) are shown.
26

Studies are listed by study size.
27

Figure 1
28
Studies included in qualitative and
quantitative synthesis (n= 10)
Full-text articles excluded (n=66) - Low number size, n=12
- No unique results*, n=21- Same patient population,
n=8- No separable data for
dTAA, n=22- Occlusive disease, n=1
Full-text articles assessed for eligibility
(n=76)
Records excluded (n =139)
Records screened (n=215)
Records after duplicates removed (n=215)
Additional records identified through other sources
(n=1)
Identificatio
Eligibility
Included
Screening
Records identified through database searching
(n=293)
Author replies (n=3)
466

29
467

Figure 2
30
468

Figure 3
31
469
470
471
472
473
474
475
476
477
478
479
480
481
482

Figure 4
32
483
484
485