Embed Size (px)
Citation preview
Growth Hormone Replacement Therapy: Interpreting Guidelines for Clinical Practice
Pinchas Cohen, MDDean, USC Davis School, Adjunct Professor of Pediatric Endocrinology
Growth Hormone Replacement Therapy: Interpreting Guidelines for Clinical Practice
• History of growth hormone (GH) consensus statements & clinical guidelines
• Value of GH consensus statements & clinical guidelines
• Review of key GH statements & clinical guidelines
• Future of guidelines and statements on GH therapy
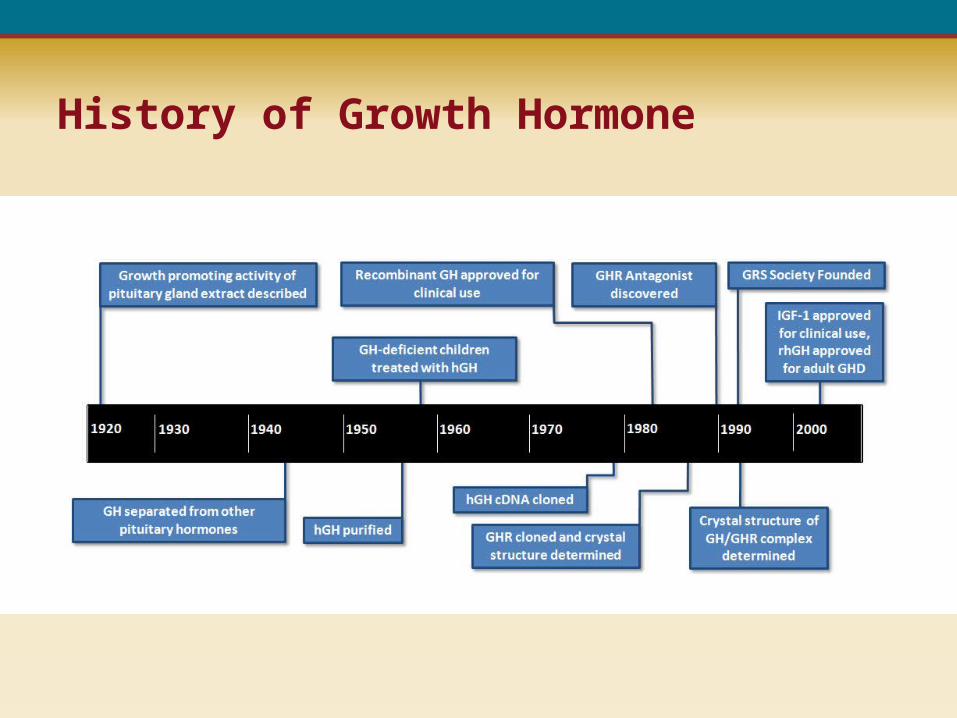
History of Growth Hormone
Why Consensus Statements
• Needs from the community
• Emerging standard of care
• New studies and data change practices
• New controlled trials
• New FDA approved indications
• Unpublished clinical experience
• Unpublished registry data
• Geographical variability in clinical practice
• Changing payer climate
• Litigious environment
Who is Served by Consensus Statements
The pediatric endocrine community:
•FDA approvals were broad and lacked specific guidance
•De facto, these guidelines establish a standard of care
•Protect doctors who follow guidelines from frivolous lawsuits
•Establishing the basis for dialogue with payers
Patients:
•Providing detailed guidelines on the approach to diagnosis, treatment, and monitoring of growth disorders
•Establish best unbiased proven practices for effective treatment
The First GH Consensus Statement - 1990
Issues and concerns:
• Industry sponsored
• Driven by a single drug company
• No involvement of learned societies
A New Era in Consensus Statements
1992 – Growth Hormone Research Society (GRS) founded:
• Developed a philosophy for support of the GH field
• Recognized need for unbiased guidelines
• Developed independence from commercial influence
• Established a tradition of consensus workshops
• Worked with other societies
GRS Consensus Statements 1998-2005 • Consensus guidelines for the diagnosis and treatment of adults with
growth hormone deficiency: summary statement of the Growth Hormone Research Society workshop on adult growth hormone deficiency.J Clin Endocrinol Metab. 1998;83:379–381.
• Consensus guidelines for the diagnosis and treatment of growth hormone (GH) deficiency in childhood and adolescence: summary statement of the GH Research Society. J Clin Endocrinol Metab. 2000;85:3990–3993.
• Critical evaluation of the safety of recombinant human growth hormone administration: statement from the Growth Hormone Research Society. J Clin Endocrinol Metab. 86:2001;1868–1870.
• Biochemical assessment and long-term monitoring in patients with acromegaly: statement from a joint consensus conference of the Growth Hormone Research Society and The Pituitary Society. J Clin Endocrinol Metab. 2004;89:3099–3102.
• Consensus statement on the management of the GH-treated adolescent in the transition to adult care. Eur J Endocrinol.2005;152:165–170.
GRS Consensus Statements 2007-2013• Management of the child born small for gestational age through to adulthood:
a consensus statement of the International Societies of Pediatric Endocrinology and the Growth Hormone Research Society. J Clin Endocrinol Metab.2007;92:804–810.
• Consensus guidelines for the diagnosis and treatment of adults with GH deficiency II: a statement of the GH Research Society in association with ESPE and LWPES. Eur J Endocrinol.2007;157:695–700.
• Consensus statement on the diagnosis and treatment of children with idiopathic short stature: a summary of the Growth Hormone Research Society, the LWPES and ESPE workshop. J Clin Endocrinol Metab.2008;93:4210–4217.
• Statement by the Growth Hormone Research Society on the GH/IGF-I axis in extending health span. J Gerontol A Biol Sci Med Sci.2009;64A:1039–1044.
• Consensus statement on the standardization and evaluation of growth hormone and insulin-like growth factor assays. Clin Chem.201;57:555–559.
• Growth Hormone Research Society workshop summary: consensus guidelines for recombinant human growth hormone therapy in Prader-Willi syndrome. J Clin Endocrinol Metab.2013 Mar 29. [Epub ahead of print]
Goals of Consensus Workshops
1. Ultimate goal: to serve patients and doctors
2. Aim: to set a standard in a field fraught with controversy
3. Final product: consensus statement
4. Consumers of the statement: clinicians, payers, regulators
5. Address the key issues outlined in the questions posed
6. Define an INTERNATIONAL perspective
7. Not to focus on important items outside the defined scope
• Based on the NIH consensus model
• Evidence review of published (and unpublished) data on the topic in the first part of the workshop
• A set of questions addressing unresolved issues in the diagnosis and management of the condition are circulated
• Succinct review lectures and focused presentations of relevant topics were given by invited experts
• Breakout sessions discuss specific topics
• Discussions are reviewed and summarized
• Consensus document is written and reviewed in real time
Structure of Consensus Workshops
Representation in Consensus Workshops
Example – ISS consensus
• 32 experts• 15 countries• 8 professional societies• 6 industry observers
Most of the funding came in the form of grants from participating organizations, such as GRS, LWPES, and ESPE as well as small unrestricted educational grants from several supporting industry members of GRS.
ISS = idiopathic short stature.
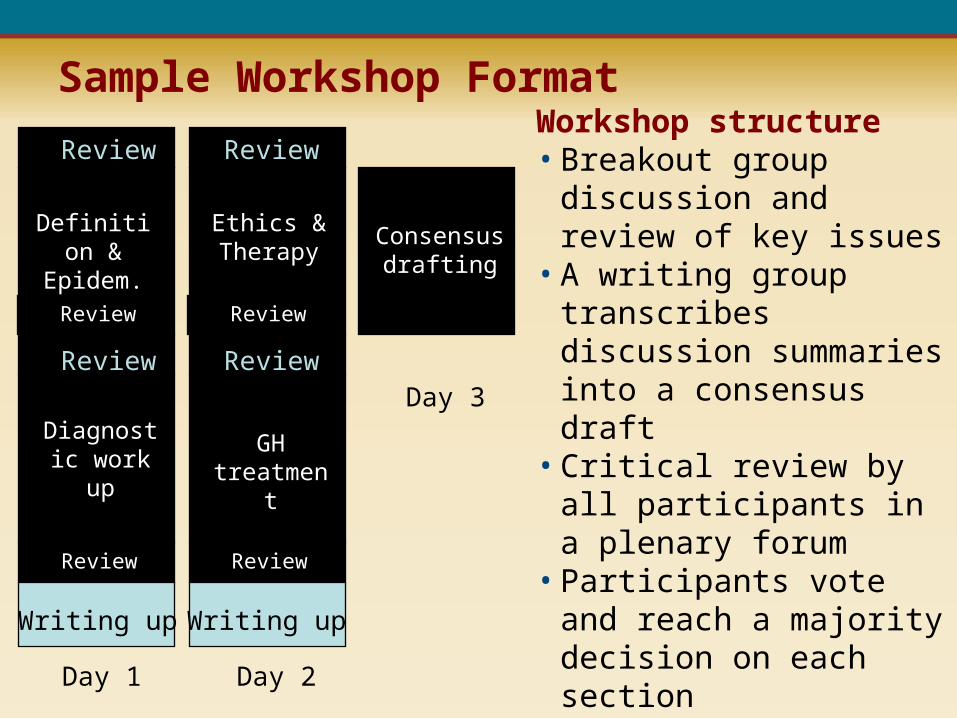
Sample Workshop Format
Definition & Epidem.
Diagnostic work up
Review
Writing up
Ethics & Therapy
GH treatment
Review
Writing up
Consensusdrafting
Day 1 Day 2
Day 3
Review Review
Review Review
Review Review
Workshop structure• Breakout group discussion
and review of key issues• A writing group transcribes
discussion summaries into a consensus draft • Critical review by all
participants in a plenary forum • Participants vote and reach a
majority decision on each section • They are sent a polished draft
for additional comments and give signed approval to the final revision
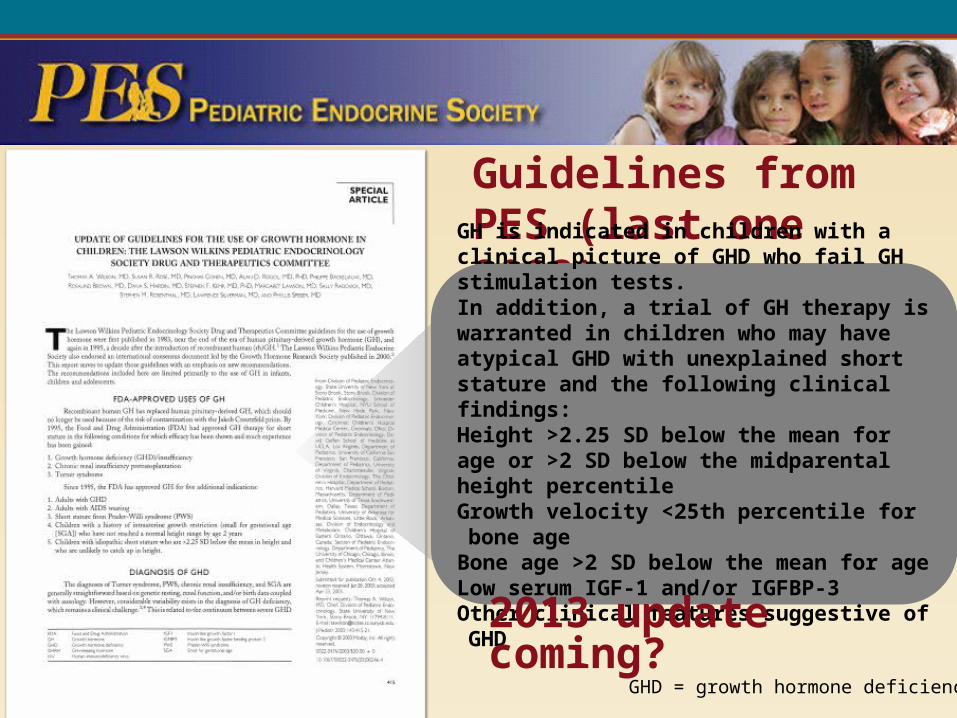
Limited GH Guidelines from PES (last one 2003)
GH is indicated in children with a clinical picture of GHD who fail GH stimulation tests. In addition, a trial of GH therapy is warranted in children who may have atypical GHD with unexplained short stature and the following clinical findings: Height >2.25 SD below the mean for age or >2 SD below the midparental height percentileGrowth velocity <25th percentile for bone ageBone age >2 SD below the mean for ageLow serum IGF-1 and/or IGFBP-3Other clinical features suggestive of GHD
2013 update coming?GHD = growth hormone deficiency.
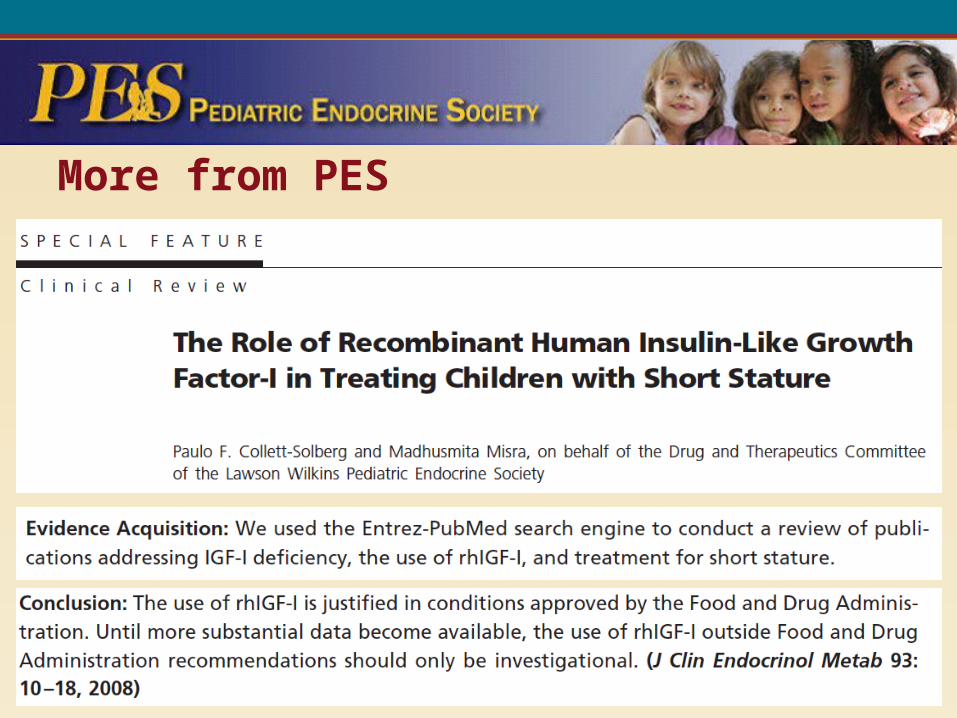
More from PES
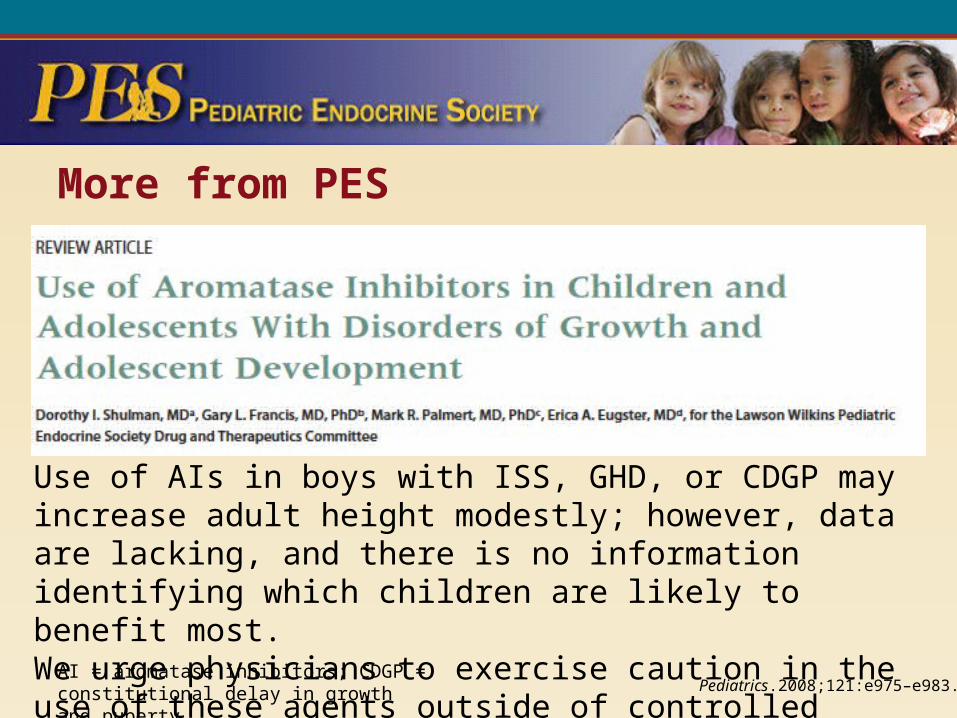
More from PES
Use of AIs in boys with ISS, GHD, or CDGP may increase adult height modestly; however, data are lacking, and there is no information identifying which children are likely to benefit most.We urge physicians to exercise caution in the use of these agents outside of controlled clinical trials.
AI = aromatase inhibitors; CDGP = constitutional delay in growth and puberty. Pediatrics.2008;121:e975–e983.

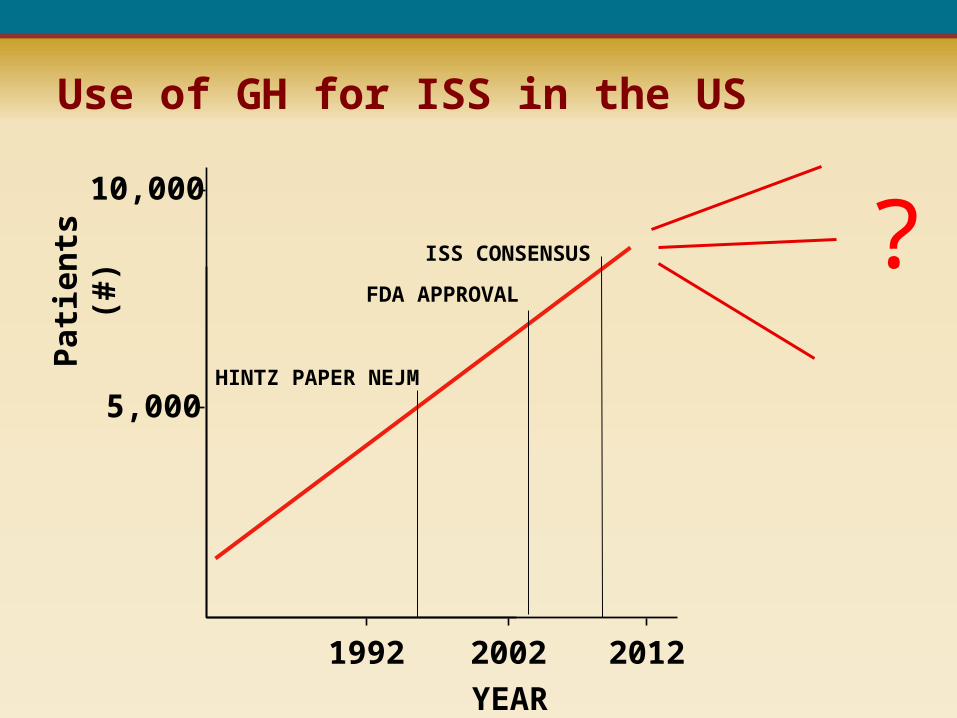
Use of GH for ISS in the US
5,000
1992
YEAR
2002
Pat
ien
ts (
#)
2012
10,000
FDA APPROVAL
HINTZ PAPER NEJM
?ISS CONSENSUS
Normal at Any Cost: Tall Girls, Short Boys,
and the Medical Industry's Quest to Manipulate Height. Susan Cohen. 2009.
A Backlash?
Consensus Statement on the Diagnosis and Treatment of
Children with Idiopathic Short Stature: A Summary of the Growth Hormone Research Society, the Lawson Wilkins Pediatric Endocrine Society and the European Society for
Paediatric Endocrinology Workshop.
J Clin Endocrinol Metab.2008; 93:4210–4217.
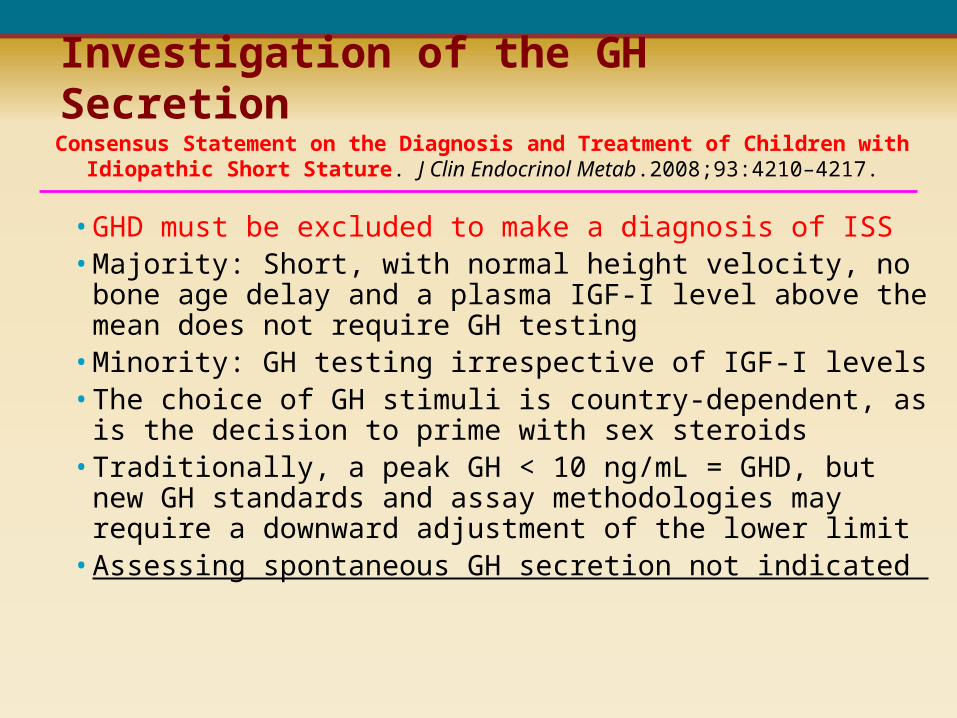
• GHD must be excluded to make a diagnosis of ISS• Majority: Short, with normal height velocity, no bone age
delay and a plasma IGF-I level above the mean does not require GH testing
• Minority: GH testing irrespective of IGF-I levels• The choice of GH stimuli is country-dependent, as is the
decision to prime with sex steroids• Traditionally, a peak GH < 10 ng/mL = GHD, but new GH
standards and assay methodologies may require a downward adjustment of the lower limit
• Assessing spontaneous GH secretion not indicated
Investigation of the GH SecretionConsensus Statement on the Diagnosis and Treatment of Children with Idiopathic Short
Stature. J Clin Endocrinol Metab.2008;93:4210–4217.
• Auxological: FDA approved < -2.25 SDS (1.2 percentile)
• Expert opinions range from - 2 SDS to – 3 SDS
• Optimal age for initiating treatment is 5 years to early puberty
• There are no accepted biochemical criteria for initiating GH
• Psychological: weigh the degree of short stature and the coping capacity of the child
Criteria for Treating Children with ISSConsensus Statement on the Diagnosis and Treatment of Children with Idiopathic Short
Stature. J Clin Endocrinol Metab.2008;93:4210–4217.
• Successful 1st year response: delta height SDS > 0.3; a HV increment >3 cm/year; HVSDS > +1
• Emerging tools: prediction modeling/specific charts
• Serial IGF-I to assess efficacy, safety and compliance, and as tool for adjusting the GH dose
• No other biochemical tests are routinely recommended in GH-treated ISS patients
• If after 1-2 years, plus higher doses of GH, growth rate is still inadequate, GH should be stopped and alternative therapies could be entertained
Response to GH Treatment
First-Year Growth Responses to Daily GH in ISS
Female Male
Age at baseline Age at baseline
Fir
st-y
ear
hei
ght
velo
city
(cm
/yr)
0
2
4
6
8
10
12
14
16
2 3 4 5 6 7 8 9 10 11 12 13 14
Mean HV +1 SDMean HVMean HV –1 SDMean Pretreatment HV
Fir
st-y
ear
hei
ght
velo
city
(cm
/yr)
0
2
4
6
8
10
12
14
16
2 3 4 5 6 7 8 9 10 11 12 13 14
n=842 n=2318
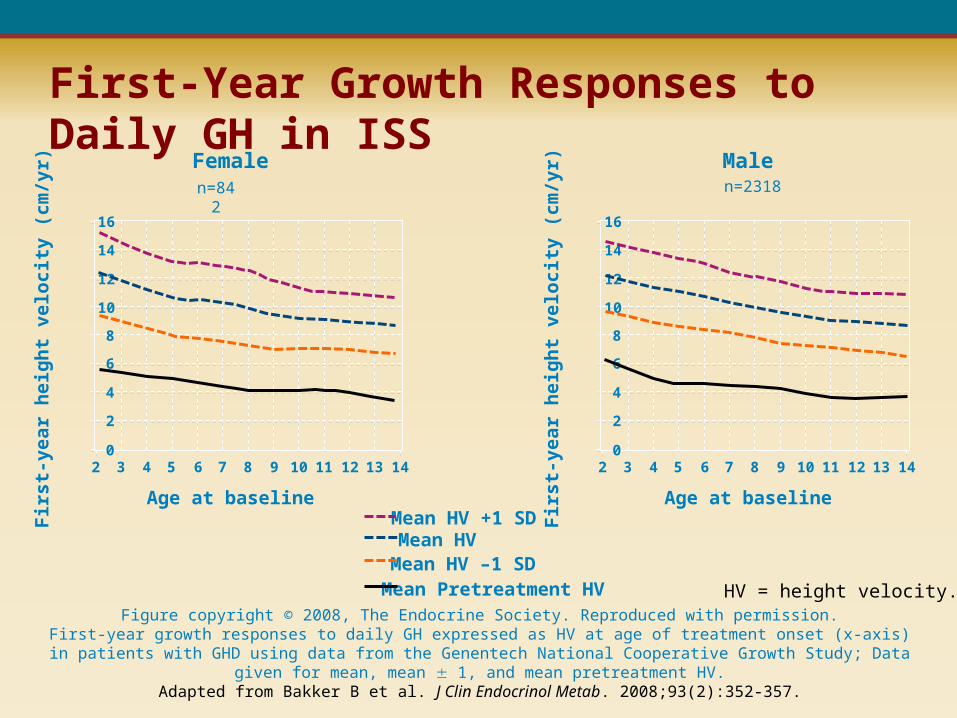
Figure copyright © 2008, The Endocrine Society. Reproduced with permission.First-year growth responses to daily GH expressed as HV at age of treatment onset (x-axis) in patients with GHD using data from the
Genentech National Cooperative Growth Study; Data given for mean, mean 1, and mean pretreatment HV.Adapted from Bakker B et al. J Clin Endocrinol Metab. 2008;93(2):352-357.
HV = height velocity.
• Dosage is usually selected and adjusted by weight
• If the growth response is considered inadequate, the dose may be increased
• There are no definitive data concerning the long-term safety of doses higher than 70 mcg/kg/day in ISS
• IGF-I levels may be helpful in assessing compliance and GH sensitivity; levels that are consistently elevated (>2.5 SDS) should prompt consideration of GH dose reduction
GH Treatment Adjustment Strategies
Consensus Statement on the Diagnosis and Treatment of Children with Idiopathic Short Stature. J Clin Endocrinol Metab.2008;93:4210–4217.
Two schools of thought:
1. Treatment should stop when near adult height is achieved (HV < 2 cm/year, and/or BA > 16- boys / 14- girls).
2. Therapy can be discontinued when height is in the “normal” adult range (> – 2 SDS), or as in Australia, the 10th percentile or the 50th percentile
Stopping therapy is influenced by patient/family satisfaction and cost-benefit analysis
Duration of GH Treatment Consensus Statement on the Diagnosis and Treatment of Children with Idiopathic Short
Stature. J Clin Endocrinol Metab.2008;93:4210–4217.
BA = bone age.
Care of Turner Syndrome (Led from the NIH)
`̀
Care of the Child with SGA
Consensus Statement• Diagnosis should be based on accurate
anthropometry at birth• At-risk children: early neurodevelopment
evaluation and intervention• Endocrine and metabolic disturbances are
infrequent• 10% lack “catch-up” growth• GH therapy can increase linear growth in
those lacking catch-up growth• For severe growth retardation (-2.5 SD, 2-
4 yr), start GH at 35-70 μg/kg/d• SGA associated with coronary disease
and stroke later in life• Presently, inadequate evidence to
recommend routine surveillance outside normal clinical practice
Consensus Statement• Diagnosis should be based on accurate
anthropometry at birth• At-risk children: early neurodevelopment
evaluation and intervention• Endocrine and metabolic disturbances are
infrequent• 10% lack “catch-up” growth• GH therapy can increase linear growth in
those lacking catch-up growth• For severe growth retardation (-2.5 SD, 2-
4 yr), start GH at 35-70 μg/kg/d• SGA associated with coronary disease
and stroke later in life• Presently, inadequate evidence to
recommend routine surveillance outside normal clinical practice
SGA = small for gestational age.
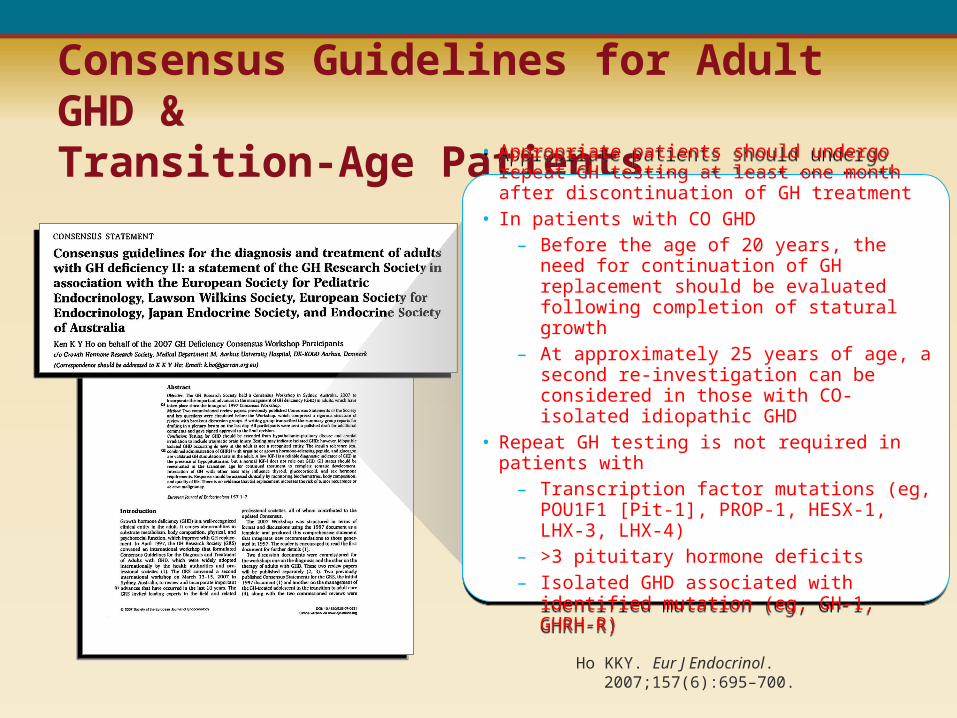
Consensus Guidelines for Adult GHD &Transition-Age Patients
Ho KKY. Eur J Endocrinol. 2007;157(6):695–700.
• Appropriate patients should undergo repeat GH testing at least one month after discontinuation of GH treatment
• In patients with CO GHD – Before the age of 20 years, the need for
continuation of GH replacement should be evaluated following completion of statural growth
– At approximately 25 years of age, a second re-investigation can be considered in those with CO-isolated idiopathic GHD
• Repeat GH testing is not required in patients with– Transcription factor mutations (eg, POU1F1 [Pit-1],
PROP-1, HESX-1, LHX-3, LHX-4)– >3 pituitary hormone deficits– Isolated GHD associated with identified mutation
(eg, GH-1, GHRH-R)
• Appropriate patients should undergo repeat GH testing at least one month after discontinuation of GH treatment
• In patients with CO GHD – Before the age of 20 years, the need for
continuation of GH replacement should be evaluated following completion of statural growth
– At approximately 25 years of age, a second re-investigation can be considered in those with CO-isolated idiopathic GHD
• Repeat GH testing is not required in patients with– Transcription factor mutations (eg, POU1F1 [Pit-1],
PROP-1, HESX-1, LHX-3, LHX-4)– >3 pituitary hormone deficits– Isolated GHD associated with identified mutation
(eg, GH-1, GHRH-R)
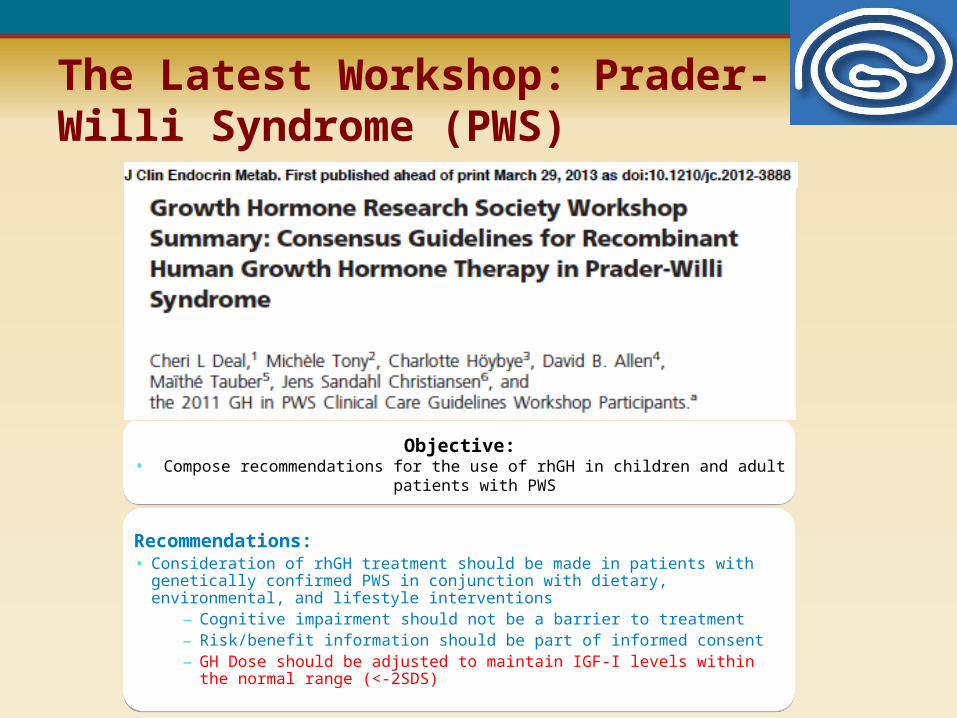
Objective:• Compose recommendations for the use of rhGH in children and adult patients with PWS
Objective:• Compose recommendations for the use of rhGH in children and adult patients with PWS
Recommendations:• Consideration of rhGH treatment should be made in patients with genetically confirmed PWS in
conjunction with dietary, environmental, and lifestyle interventions– Cognitive impairment should not be a barrier to treatment– Risk/benefit information should be part of informed consent– GH Dose should be adjusted to maintain IGF-I levels within the normal range (<-2SDS)
Recommendations:• Consideration of rhGH treatment should be made in patients with genetically confirmed PWS in
conjunction with dietary, environmental, and lifestyle interventions– Cognitive impairment should not be a barrier to treatment– Risk/benefit information should be part of informed consent– GH Dose should be adjusted to maintain IGF-I levels within the normal range (<-2SDS)
The Latest Workshop: Prader-Willi Syndrome (PWS)
Reviews on Consensus Statements and Clinical Guidelines
The Actual Utility of Clinical Guidelines
• Leverage industry: (eg, the diagnostic companies now provide better assays and express values as SDS)
• Dealing with rogue practices & off-label use of GH/IGF
• Feedback and citations (eg, ISS consensus cited > 50 times; safety consensus cited >30 times)
Future of Guidelines and Consensus Statements
• GH safety, take-2 (2014)
• IGFD (2015)
• Emerging issues? (audience suggestions?)
A Managed Care View of Growth Hormone Replacement Therapy:Plan Perspectives
Michael Fine, MDSenior Medical DirectorHealth Net of CaliforniaWoodland Hills, California
Can Managed Care afford health care reform?
Can Managed Care afford not to have reform?
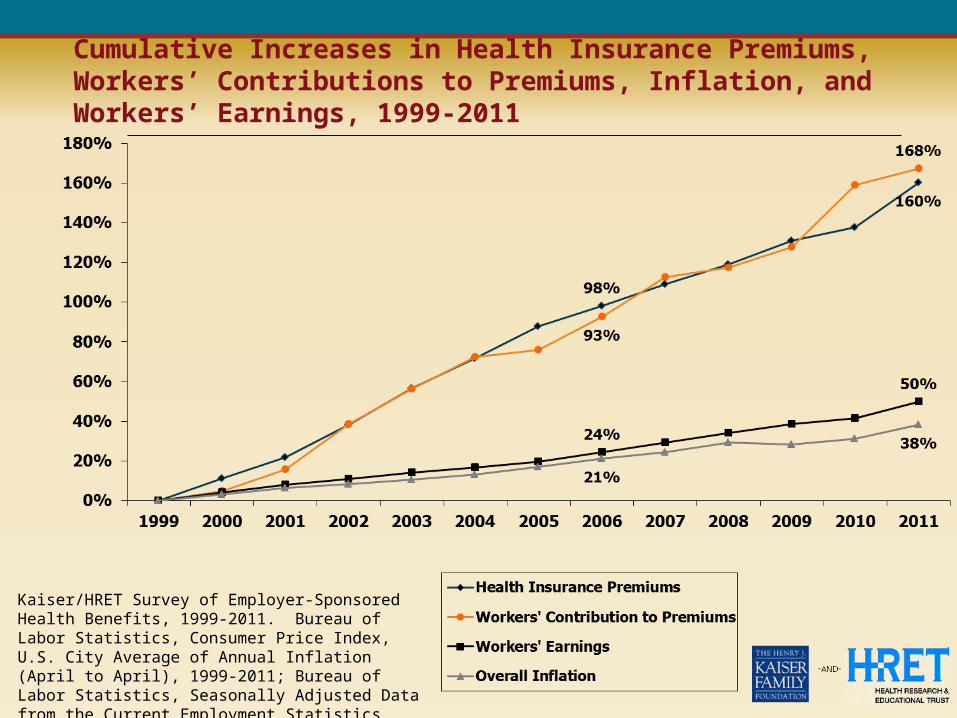
Cumulative Increases in Health Insurance Premiums, Workers’ Contributions to Premiums, Inflation, and Workers’ Earnings, 1999-2011
Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2011. Bureau of Labor Statistics, Consumer Price Index, U.S. City Average of Annual Inflation (April to April), 1999-2011; Bureau of Labor Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey, 1999-2011 (April to April).
Who is paying for healthcare?
Who is paying for growth hormone?
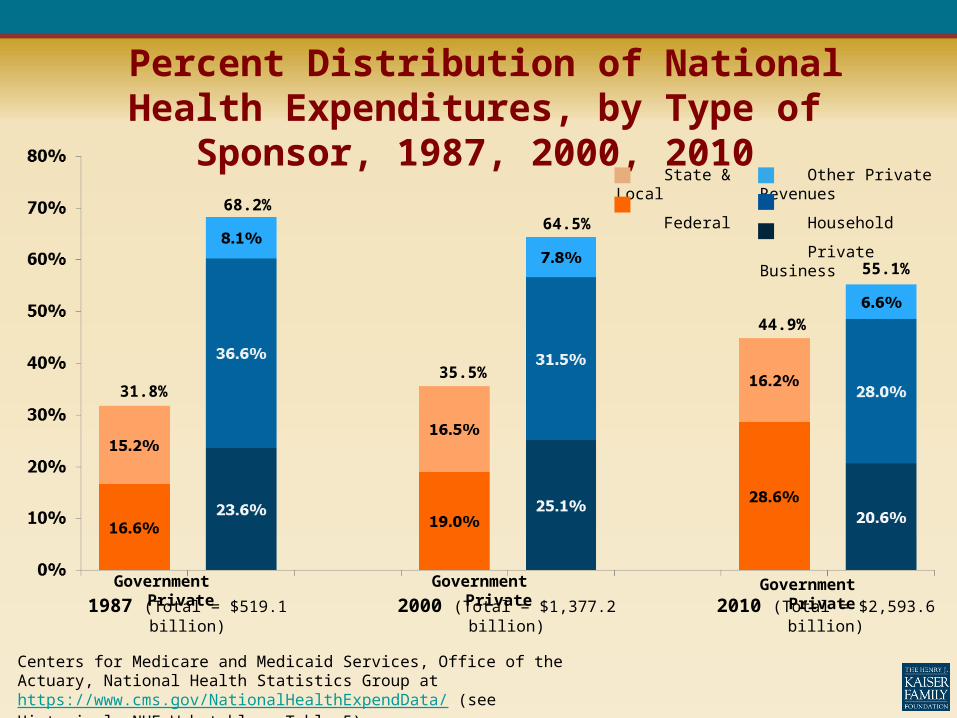
Percent Distribution of National Health Expenditures, by Type of Sponsor, 1987, 2000, 2010
Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group at https://www.cms.gov/NationalHealthExpendData/ (see Historical; NHE Web tables, Table 5).
Government Private1987 (Total = $519.1 billion)
Government Private
Government Private2000 (Total = $1,377.2
billion)
31.8%
68.2%
35.5%
64.5%
44.9%
55.1%
2010 (Total = $2,593.6 billion)
State & Local Other Private Revenues
Federal Household
Private Business
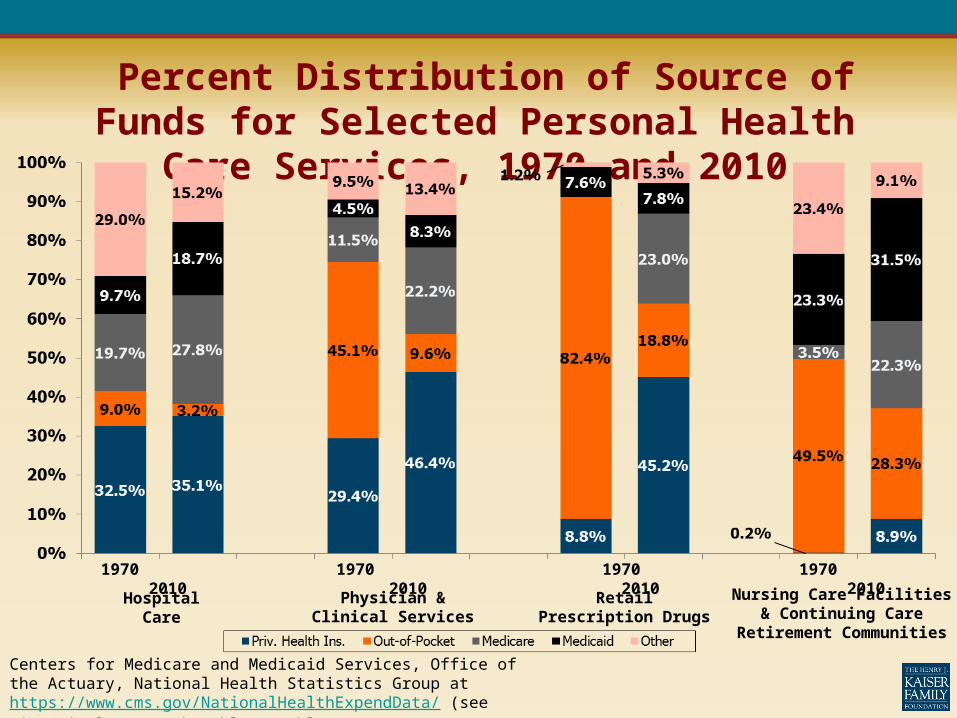
Percent Distribution of Source of Funds for Selected Personal Health Care Services, 1970 and 2010
1970 2010 1970 2010 1970 2010 1970 2010
Hospital Care Physician & Clinical Services
Retail Prescription Drugs Nursing Care Facilities & Continuing Care Retirement
Communities
Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group at https://www.cms.gov/NationalHealthExpendData/ (see Historical; NHE Web tables, Tables 7, 8, 11, 12).
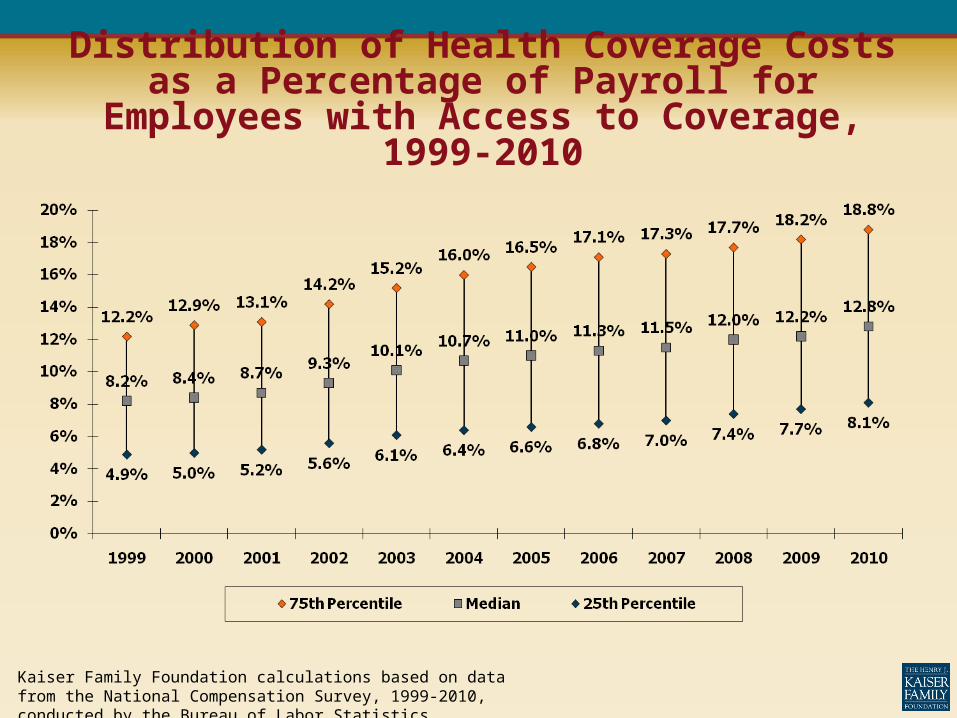
Distribution of Health Coverage Costs as a Percentage of Payroll for Employees with Access to
Coverage, 1999-2010
Kaiser Family Foundation calculations based on data from the National Compensation Survey, 1999-2010, conducted by the Bureau of Labor Statistics.
Who will sign up for the healthcare exchanges?
Kaiser Family Foundation calculations using data from U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey (MEPS), Household Component, 2009.
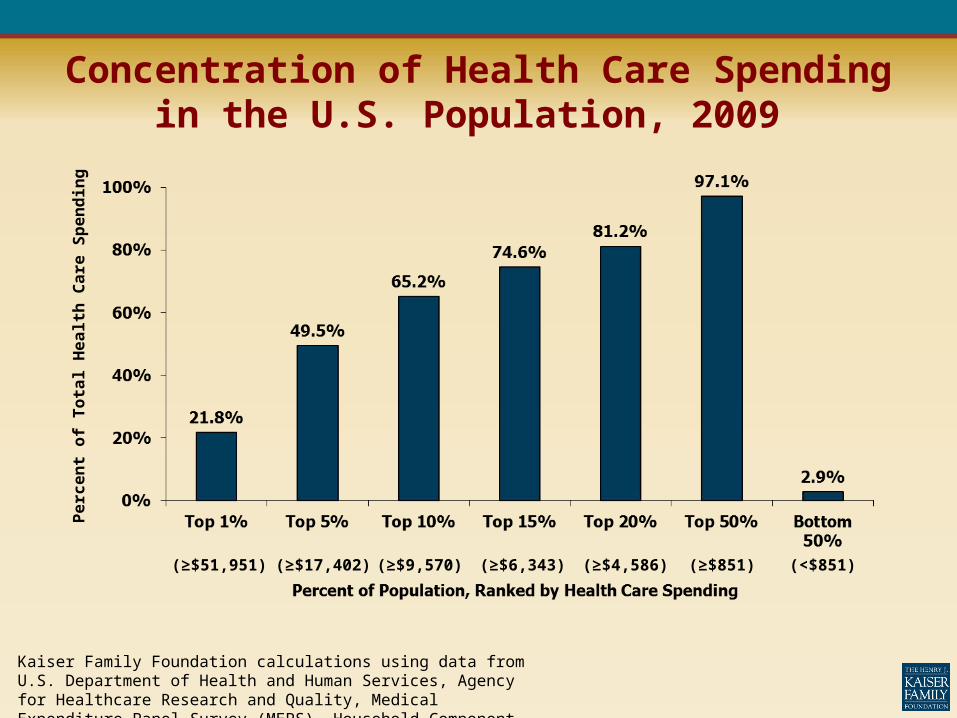
Concentration of Health Care Spending in the U.S. Population, 2009
(≥$51,951)
(≥$17,402)
(≥$9,570) (≥$6,343) (≥$4,586) (≥$851) (<$851)
Perc
en
t of
Tota
l H
ealt
h C
are
Sp
en
din
g
Is the management of growth hormones a priority for managed
care organizations (MCOs)?
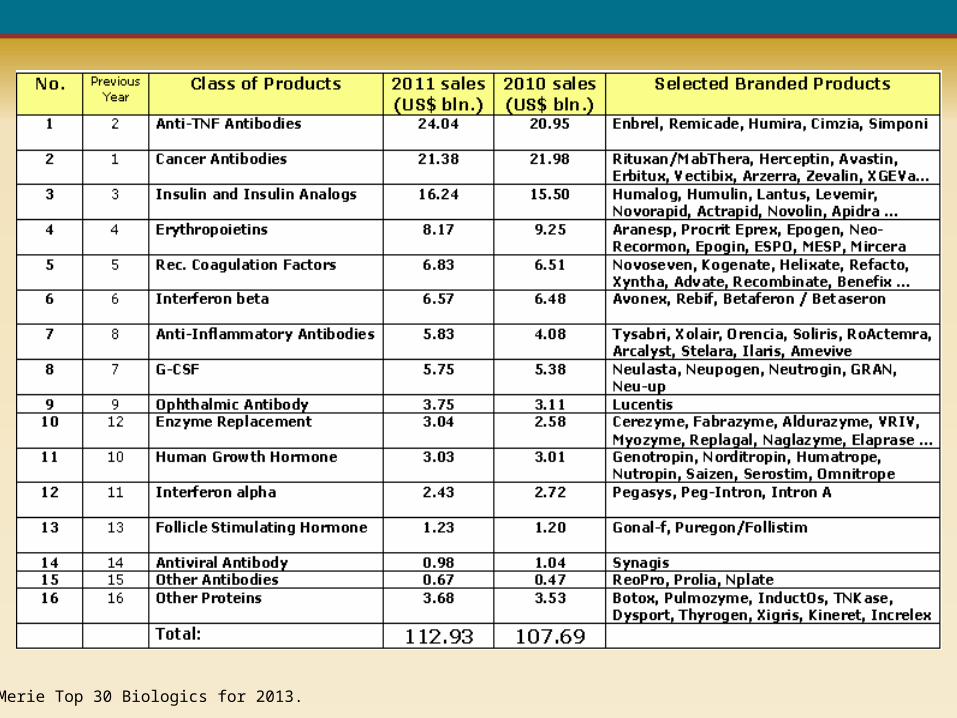
La Merie Top 30 Biologics for 2013.
Drug Cost Trends
• Drug overall cost trends = 2.6%
• Specialty drug cost trend = 17.1%
• Growth hormone class trend = 6.6%
Express Scripts. Drug Trend Report 2011.
Express Scripts. Drug Trend Report 2011.
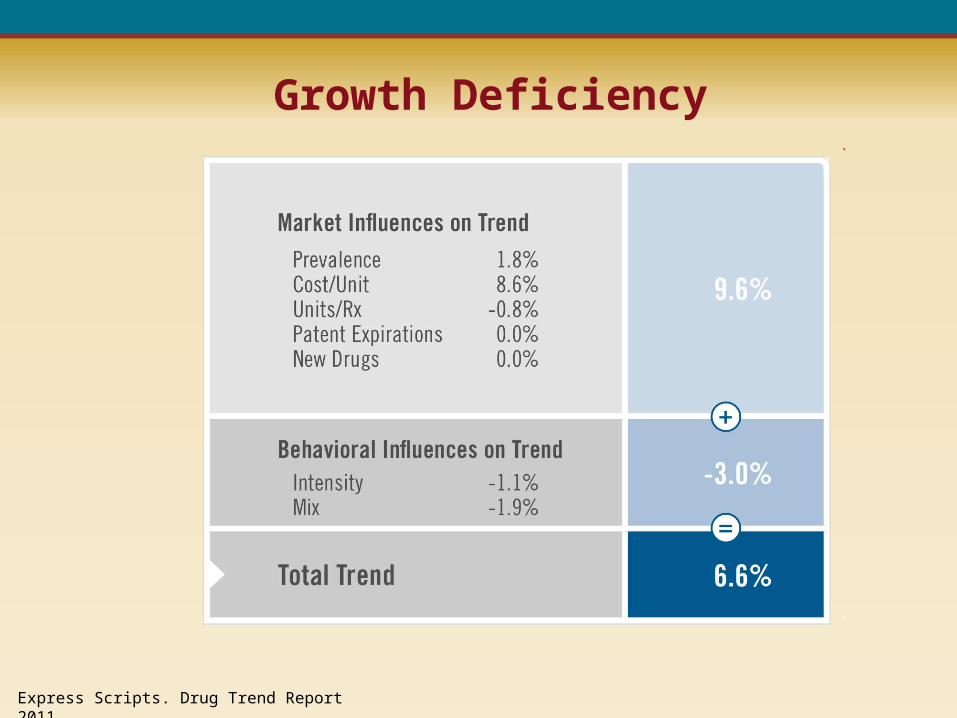
Growth Deficiency
Growth Hormone Product Trends
• Despite a decrease in the use of growth hormone medications in 2011, drug trend for the class still was up 6.6%, due to increased cost.
• Double-digit growth was seen in the cost of several older brands of growth hormones.
• Large utilization increases for the newer somatropin formulations, Nutropin AQ® NuSpin™ (approved in 2009) and Norditropin® FlexPro® (approved in 2010), contributed to higher utilization trend in 2011.
• Cost for Norditropin FlexPro actually dropped considerably, however, and cost for Nutropin AQ NuSpin rose only moderately.
• Cost trends for two biosimilar growth hormones, Omnitrope® and Tev-Tropin®, were down significantly (by 21.6% and 13.8%, respectively). Utilization of each, however, increased more than 100% in 2011.
Express Scripts. Drug Trend Report 2011.
MCO Management of Growth Hormone
• Benefit Design
• Utilization Management
• Cost Management
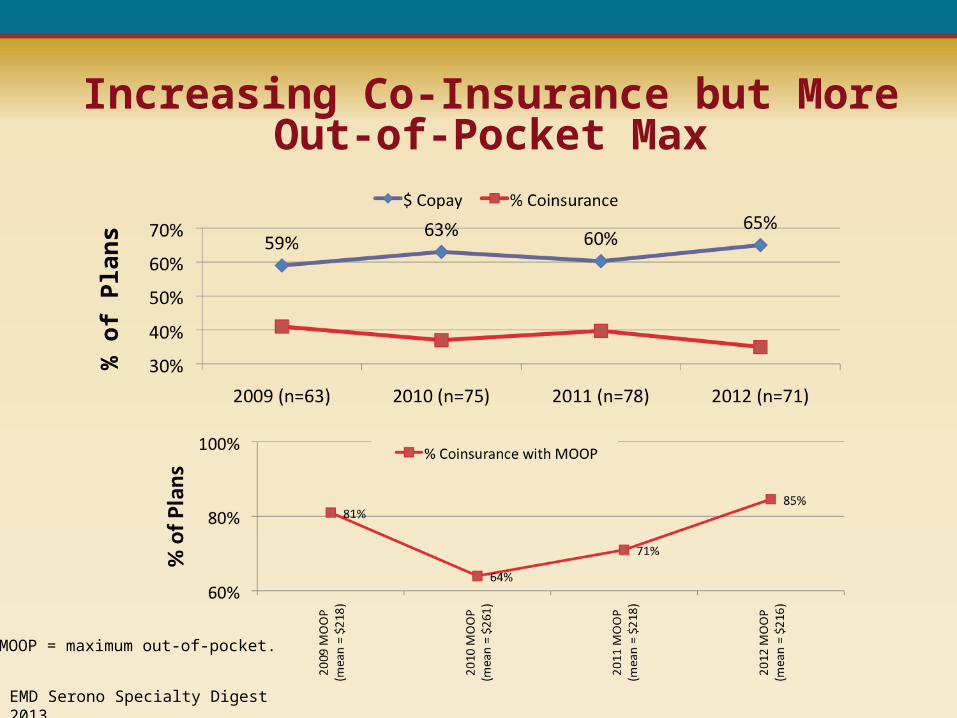
Increasing Co-Insurance but More Out-of-Pocket Max
EMD Serono Specialty Digest 2013.
% o
f Pla
ns
MOOP = maximum out-of-pocket.
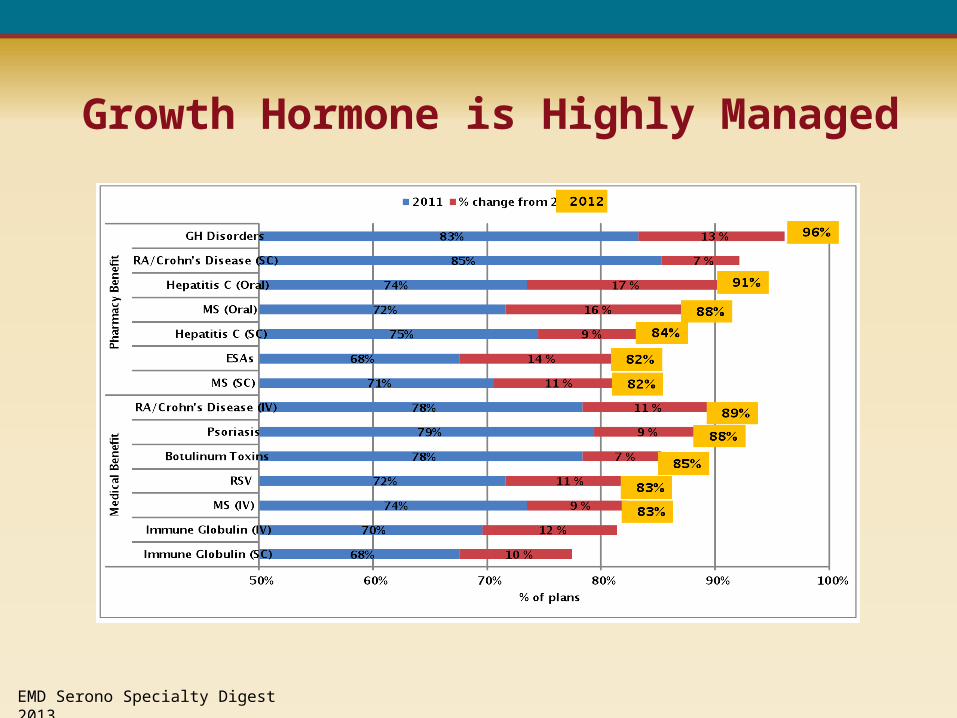
Growth Hormone is Highly Managed
EMD Serono Specialty Digest 2013.
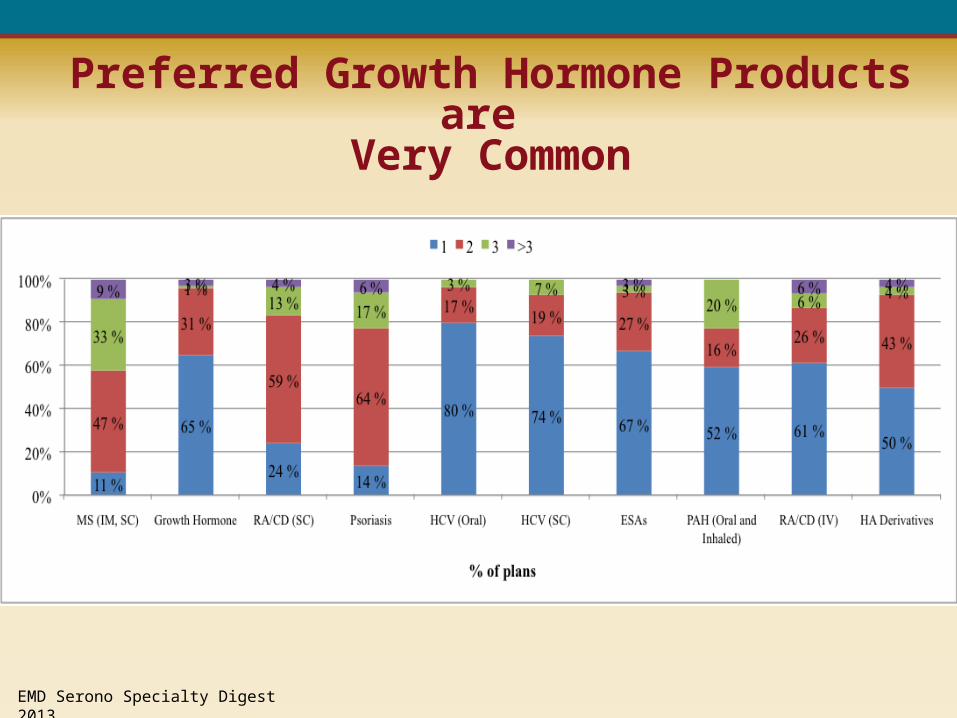
Preferred Growth Hormone Products are Very Common
EMD Serono Specialty Digest 2013.
One Plan’s Approach
• All human growth hormone products are therapeutically equivalent.
• The use of preferred brand growth hormones is appropriate.
• Growth hormones are interchangeable and can be used for any FDA-approved indication, even off-label.
• All growth hormone products require prior authorization.
• Specialty pharmacy is mandatory.
• Continued authorization for treatment in children requires demonstration of adequate growth response.
Approved Indications
• Growth hormone deficiency in children and adolescents
• Growth hormone deficiency in adults
• Idiopathic short stature syndrome
• Small for gestational age
• SHOX (short stature homeobox-containing gene) deficiency
• Chronic renal failure in pre-transplantation children
• Prader-Willi syndrome, Turner syndrome, Noonan syndrome
• Therapy of infantile hypoglycemia
• Central nervous system tumor treated with radiation
• Short-bowel syndrome
Growth Hormone Deficiency in Children
• Two (2) pharmacologic provocation tests (insulin, clonidine, arginine, levodopa, glucagon) with a result < 10 ng/mL
• Patients who do not meet stimulation test criteria < 10ng/mL on both tests or whose stimulation tests are discordant can be approved for a 6 month trial of growth hormone if the other criteria for growth hormone deficiency have been met and both IGF-1 and IGFBP-3 levels are below the normal range for gender and age
• Diagnosis by a pediatric endocrinologist
• The patient's baseline height must be > 2 standard deviations [SD] below the mean forgender and age (which corresponds to < 2.3 percentile)
• Growth rate is such that the patient is unlikely to attain an adult height in the normal range - 59 inches for girls and 63 inches or boys (ie, growth velocity below the 25th percentile or, alternatively, in children aged <3 years, pretreatment growth velocity < 7cm per year and for children aged 3 years and older growth velocity < 4 cm per year measured accurately for at least one year)
Idiopathic Short Stature Syndrome
• The patient's baseline height must be > 2.25 standard deviations [SD] below the mean for gender and age (which corresponds to < 1.2 percentile)
• The epiphyses must be open
• Growth rate is such that the patient is unlikely to attain an adult height in the normal range - 59 inches for girls and 63 inches for boys (ie, growth velocity below the 25th percentile or, alternatively, in children aged < 3 years, pretreatment growth velocity < 7cm per year and for children aged 3 years and older growth velocity < 4 cm per year measured accurately for at least one year measured accurately for at least one year)
Small for Gestational Age
• Child was born small for gestational age, defined as birth weight or length 2 or more standard deviations below the mean for gestational age
• Child must be at least two years old
• The patient's baseline height must be > 2 standard deviations [SD] below the mean for gender and age (which corresponds to < 2.3 percentile)
Continuation Criteria for hGH RX in Children
• Increased growth rate by two cm over baseline in first year or one cm over baseline in 6 months for those patients undergoing a 6-month trial
• Continued growth rate exceeds 2.5 cm/year• For treatment of growth hormone deficiency child's
height remains below median adult height (5'10"for males, 5'5" for females) and mid-parental height
• For non-growth hormone deficiency treatment, the child' height continues to be >2.25 standard deviations below the normal adult height for gender (5' 3" for a male, 4' 11” for a female)
Adults with Growth Hormone Deficiency
• Pharmacologic provocation tests (insulin, clonidine, arginine, levodopa, glucagon) with a result <10 ng/ml with RIA (Radioimmunoassay) or <2.5ng/ml with IRMA (Immunoradiometric assay)
• Hypothalmic or pituitary disease
• Significant clinical symptoms related to growth hormone deficiency such as fatigue, poor endurance, poor sense of well being persist despite maximizing treatment of other hormonal disorders, mood disorders, and medical illness
• Patient has multiple pituitary hormone deficiencies resulting from structural hypothalamic/pituitary disease, radiation, defined CNS pathology, cranial radiation, trauma, pituitary surgery, or genetic defect affecting the GH axis with low IGF-1 and low IGFBP-3
Growth Hormone Utilization Management Challenges 2013
• Adolescents in transition
• Adults with growth hormone deficiency
• HIV wasting
Future Landscape
• The growth hormone class is stable, with no late-phase medications in the pipeline.
• More patient access under the Affordable Care Act• Increase utilization in transition and adult patients• More utilization management especially concerning
discontinuation and dose adjustment• Parity of drug benefits under the medical and pharmacy
benefits• Value based pricing• Accountable Care Organizations (ACOs)• Biosimilars
Value-Based Payment Methodologies
Approach to payment to providers that includes incentives for achieving identified quality standards and cost management targets
Accountable Care Organization (ACO)
As defined by the Affordable Care Act (ACA), ACOs are provider-based organizations (medical groups, hospitals that employ physicians, integrated delivery systems, physician- hospital organizations, and independent practice associations) that take responsibility for the health care needs of a defined population, e.g., Medicare patients.
Challenges for Success of ACOs
• Misalignment of physician and hospital incentives
• Absence of value based payment methodologies
• Need for greater integration of physicians and hospitals
• Absence of sufficient competition in some areas
Practical Considerations for the Use of Growth Hormone Replacement Therapy in a Managed Care Environment
Clifford A. Bloch, MDPediatric Endocrine Associates, P.C.Greenwood Village, Colorado
Clinical Professor of PediatricsUniversity of Colorado School of Medicine
Short Stature: Why Should We Care?
• Many attempts to discredit us as endocrinologists
• “Short stature is a cosmetic issue.”
• “There are no psychosocial consequences of being short.”
• “Use of growth hormone is unethical in today’s environment in which healthcare resources are already stretched.”
We Should Care Because:
• Short stature is a symptom that may be a marker of an underlying disease.
• Failure to evaluate a child with short stature under certain circumstances is a violation of the standard of care.
• Failure to diagnose may result in an adverse outcome for the child and expose the physician to potential malpractice litigation.
We Should Care Because:
• The reason why most kids are referred is because the parents and kids are concerned.
• There is nothing unethical about practicing evidence-based medicine!
• Since we, as physicians, do not set or fix the price of growth hormone (GH), we cannot be responsible for stretching the scarce resources, as long as we follow the “on label” indications for use.
Why Are Parents and Kids Concerned?
A. Something is wrong with the child.
B. The child is being teased at school.
C. The child’s younger sibling is as tall or taller
D. The child feels inadequate in class.
E. The child is struggling to keep up with the other kids in sports.
F. When a teenage boy answers the phone, the caller mistakes him for his sister or mother.
G. All of the above.
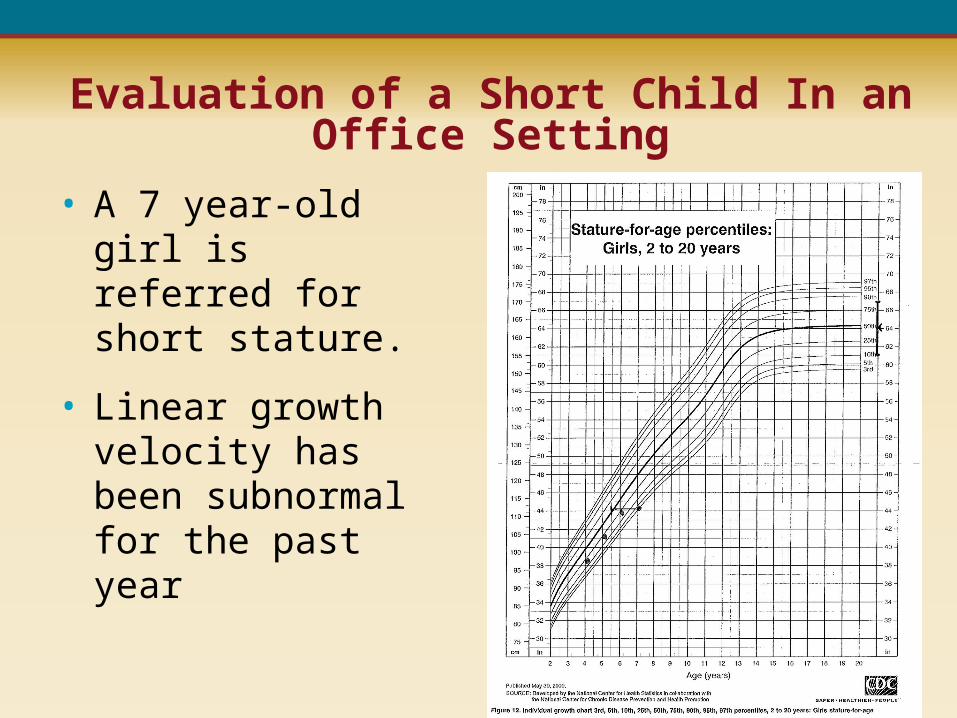
Evaluation of a Short Child In an Office Setting
• A 7 year-old girl is referred for short stature.
• Linear growth velocity has been subnormal for the past year
Evaluation of a Short Child In an Office Setting• A 7 year-old girl is referred for short stature.• Linear growth velocity has been subnormal for the past
year• Prenatal, natal and postnatal history are unremarkable• Mid-parental height at 50th percentile• Physical exam reveals a morphologically normal,
prepubertal female, with proportionate short stature• Her dental age is delayed.• Thyroid is normal• Optic funduscopy and visual fields are normal
Evaluation of a Short Child In an Office Setting
• Bone age is delayed by 1 ½ years
• Lab investigations: Blood is drawn in the office for a screening evaluation. In compliance with the recommendations of Medicaid and the American Medical Association (AMA), only the necessary tests are ordered.
Lab Investigations
1. CBC or Hgb + Hct?
2. ESR?
3. Electrolyte panel or creatinine?
4. CO2 content?
5. Biochemistry panel 22?
6. Calcium, phos, alk phos?
7. AST, ALT?
8. IgA, TTG IgA AB’s?
9. TSH or thyroid panel?
10. Karyotype?
11. IGF-1, IGFBP-3?
CBC = complete blood count, Hgb = hemoglobin blood, Hct = hematocrit, ESR = erythrocyte sedimentation rate, CO2 = carbon dioxide, phos = phosphorus, alk phos = alkaline phosphatase, AST = aspartate aminotransferase, ALT = alanine aminotransferase, IgA = immunoglobulin A, TTG = tissue transglutaminase, AB = antibody, TSH = thyroid stimulating hormone, IGF-1 = insulin-like growth factor 1, IGFBP-3 = insulin-like growth factor-binding protein 3.
Would you do a sed rate, and if so, what are you looking for?
A. Yes, I am looking for possible JRA or inflammatory bowel disease.
B. No, the child is asymptomatic and these diseases are uncommon in this age group.
Would you do a sed rate, and if so, what are you looking for?
A. Yes, I am looking for possible JRA or inflammatory bowel disease.
B. No, the child is asymptomatic and these diseases are uncommon in this age group.
Would you check full electrolyte panel, including BUN, creatinine, Na, K, Cl, and CO2 content or would you just check creatinine?
A. Full electrolyte panel
B. Creatinine only, because RTA and Bartter syndrome are unlikely to present at this age, and there is no reason to suspect electrolyte abnormalities in an asymptomatic 7-year-old.
Would you check a biochemistry-22 panel or would you just cherry pick tests like Ca, Phos, Alk phos, AST, ALT?
A. Biochemistry panel-22
B. Selected tests only
Would you check a biochemistry-22 panel or would you just cherry pick tests like Ca, Phos, Alk phos, AST, ALT?
A. Biochemistry panel-22
B. Selected tests only
Would you check IgA and TTG IgA AB’s in this girl, who has no weight loss or steatorrhea?
A. Yes, this is a routine part of my screen in all children with growth failure of any kind.
B. No, I only check these in children who are symptomatic.
Would you check IgA and TTG IgA AB’s in this girl, who has no weight loss or steatorrhea?
A. Yes, this is a routine part of my screen in all children with growth failure of any kind.
B. No, I only check these in children who are symptomatic.
Would you check a TSH with reflex free T4 or thyroid panel [free T4 and TSH]?
A. TSH only, because this is what is recommended by the AMA for screening for hypothyroidism
B. Thyroid panel, because I am screening for primary or central hypothyroidism
Would you check a karyotype in this girl?
A. Yes. All short girls ought to be karyotyped, as short stature may be the only manifestation of Turner syndrome.
B. No. Abrupt linear growth failure and a delayed bone age point to an acquired cause for growth failure.
Would you check a karyotype in this girl?
A. Yes. All short girls ought to be karyotyped, as short stature may be the only manifestation of Turner syndrome.
B. No. Abrupt linear growth failure and a delayed bone age point to an acquired cause for growth failure.
Office-Based Growth Hormone Testing
• Despite the controversy about the value of GH testing, the repeatability of GH testing, the variation in assay methodologies, etc., most 3rd party payers require documentation of GH deficiency in the setting of a high index of clinical suspicion.
• If GH testing is to be done in an office setting, it needs to be done safely, using standardized tests.
• To be reimbursed for the drugs used for testing, the medication needs to be administered parenterally.
What do you think of GH testing in an office setting?
A. I do not do GH testing, because it is unreliable.
B. GH testing is too risky to be done in an office setting.
C. GH testing is safe in an office setting with glucagon and arginine as the pharmacologic stimuli.
What do you think of GH testing in an office setting?
A. I do not do GH testing, because it is unreliable.
B. GH testing is too risky to be done in an office setting.
C. GH testing is safe in an office setting with glucagon and arginine as the pharmacologic stimuli.
Office-Based Growth Hormone Testing
• Since 2 tests are required to increase the positive predictive value of the results, we choose glucagon, followed by arginine.
• We reject insulin, because of its high risk.
• We reject clonidine and L-dopa, because they are oral agents.
• We have a designated testing room, replete with, supplies, an infusion pump for the arginine, O2, suction, and a crash cart.
• Room includes a DVD player and TV.
Growth Hormone Authorization
• Results are collated and documented in a table.
• They are interpreted, and the diagnosis of GH deficiency is made.
• This is followed by a 1 mcg cortrosyn [ACTH] stim test in the office, and a hypothalamic-pituitary, focused MRI scan, pre- and post contrast in an outpatient MRI facility.
• [Sometimes the ACTH stim test is done at the same time as the GH stim testing.]
ACTH = adrenocorticotropic hormone, MRI = magnetic resonance imaging.

Reimbursement for the Costs of GH Testing
• Nursing time - 96365 [1st hr] + 96366 [x4]• IV supplies - Bundled into nursing charge• IV pump - E0781• Heparin flush - J1642• Drugs
– Arginine - J3490
– Glucagon - J1610
• Physician time - E&M code
E&M = evaluation and management.
Reimbursement for the Costs of ACTH Testing
• Nursing time - 96365 [1st hr] + 96366 [x1]• IV supplies - Bundled into nursing charge• Heparin flush - J1642• Drugs
– Cortrosyn - J0833
• Physician time - E&M code
Should cranial MRI scans with contrast and conscious sedation be done in an outpatient facility?
A. No. They should always be done in an inpatient facility where pediatric anesthesia is available.
B. They could be done in an outpatient facility as long as there are facilities and staff available to deal with complications.
Should cranial MRI scans with contrast and conscious sedation be done in an outpatient facility?
A. No. They should always be done in an inpatient facility where pediatric anesthesia is available.
B. They could be done in an outpatient facility as long as there are facilities and staff available to deal with complications.
How do you choose the brand of GH?
A. I have a rotation of brands.
B. I only use a few brands of my choice.
C. I use the preferred brand that is on formulary for the patient’s insurance carrier.
D. I let my nurse or MA choose the brand before writing a prescription.
How do you choose the brand of GH?
A. I have a rotation of brands.
B. I only use a few brands of my choice.
C. I use the preferred brand that is on formulary for the patient’s insurance carrier.
D. I let my nurse or MA choose the brand before writing a prescription.
Authorization of GH Therapy
• The letter with the results and documentation of GH deficiency and recommendations for GH therapy is submitted to insurance for authorization.
• We complete a patient demographic form and make a copy of the insurance card and submit them to a company that performs a “Pharmacy Benefits Investigation” [PBI].
• Within 24 hrs, we receive a report indicating which brands of GH are preferred by the patient’s insurance company and/or pharmacy benefits manager [PBM], and the patient co-payments for each.
Commencement of GH Therapy
• The physician selects the brand of GH that is most advantageous, financially, for the patient and his/her family.
• A prescription is written and submitted with a “Statement of Medical Necessity” [SMN] to the case manager of GH company, requesting a “rapid start.”
• A limited supply of “free” drug is shipped to the patient.
• Once drug is received, patient is instructed to call our office to schedule GH teaching for their GH start.
Who does the teaching for the GH start?
A. We have the GH company or a nursing agency send a nurse to do the teaching at the patient’s home.
B. We have our own staff do the teaching at our facility.
Who does the teaching for the GH start?
A. We have the GH company or a nursing agency send a nurse to do the teaching at the patient’s home.
B. We have our own staff do the teaching at our facility.
Commencement of GH Therapy• Patient and family receive teaching at our office,
provided by a medical assistant, with full discussion about anticipated response and known side-effects
• Patient and family also meet with physician
• Follow-up is scheduled in 3 months
• Sometime in the 3 month interval, the family and our office will hear from the insurance company about approval or denial of therapy.
• Patient has the option of continuing with therapy at the family’s own expense if coverage is denied by insurance
GH therapy is denied, because “GH is not a covered benefit.” How do you respond?
A. I write a letter of appeal and am willing to do a “peer-to-peer” conference call
B. I tell the patient’s family that they will need to apply for assistance or bear the costs of therapy themselves
GH therapy is denied, because “GH is not a covered benefit.” How do you respond?
A. I write a letter of appeal and am willing to do a “peer-to-peer” conference call
B. I tell the patient’s family that they will need to apply for assistance or bear the costs of therapy themselves
Continued GH Therapy
• Unlike previous times, we do not typically write letters of appeal if the reason for the denial is that GH therapy is “not a covered benefit.”
• Only if GH therapy is a covered benefit for the diagnosis that is submitted, and insurance issues a denial, based upon erroneous interpretation of the rationale for the diagnosis, do we write a letter of appeal.
• Repeat SMN’s are submitted upon request by the PBM or insurance, with updated information.
Continued GH Therapy• Visits are scheduled every 3 months.• Usual standards of care are followed, including
documentation and communication with the primary care physician.
• Prescriptions are given to the patient/family, who are expected to submit them to their pharmacy.
• It is the patient’s responsibility to notify us of any changes in their insurance.
• If the insurance formulary changes, a new SMN is completed by us and sent together with a new prescription.
• Patient returns for re-teaching regarding the new GH delivery system.
Criteria for Discontinuation (D/C) of GH Therapy• Unless the patient requests to D/C therapy early or
there are financial issues, side effects, etc., GH therapy is continued to near-final height.
• It is my practice to D/C therapy after we document a linear growth velocity of <0.5 cm every 3 months over 2 successive visits, assuming good compliance with therapy.
• We also document a near-mature/mature bone age.
• All GH deficient patients undergo repeat GH testing after a washout period, following D/C of GH.
Do you perform repeat GH testing in children with idiopathic, isolated GH deficiency upon completion of growth?
A. Not usually
B. Only in selected cases, where the diagnosis of GH deficiency was made in early childhood, outside of the period of physiologic, pre-pubertal growth deceleration
C. Yes, in most or all children with idiopathic, isolated GH deficiency
D. Never, because GH testing is a waste of time
Do you perform repeat GH testing in children with idiopathic, isolated GH deficiency upon completion of growth?
A. Not usually
B. Only in selected cases, where the diagnosis of GH deficiency was made in early childhood, outside of the period of physiologic, pre-pubertal growth deceleration
C. Yes, in most or all children with idiopathic, isolated GH deficiency
D. Never, because GH testing is a waste of time
Panel Discussion
Is there any consensus on the use of growth hormone in inflammatory bowel disease?
If a patient is growth hormone deficient by stimulation test, why would you consider their height?
And why would you consider their velocity of growth?
Why don’t you just treat them?
What should be the appropriate trajectory for the reduction in the price of growth hormone over time?
How do we bill for physician time when we do growth hormone stimulation tests if we don’t see the patient?
There are long-acting growth hormones in early stage development now that probably will be available in a few years.
How will they be handled?