Embed Size (px)
Citation preview

Dysfunctional growth is currently treated with daily injections of a recombinant form of human growth hormone, which is inconvenient and, if not appropriately treated, can trigger other hormonal disorders. Professor Dr Primus-E Mullis, Dr Vibor Petkovic and their collaborators hope to find alternative, more accessible therapies to improve the lives of patients with this condition
To start, could you describe the objectives of your current research?
Our research is focused on human growth hormone (GH), from production to secretion. Besides describing clinical disorders causing autosomal recessively inherited isolated GH deficiencies (IGHD-I), our recent scientific investigations have centred on the autosomal dominant isolated GHD (IGHD-II) forms, in which the secretion of ill-folded GH is of great interest. Of major importance to any clinician involved in endocrinology, it also causes combined pituitary-derived hormonal deficiency over time. These patients need to be monitored all their lives.
One of our aims is to rescue the altered hormonal system in IGHD-II. In such disorders, the secretion of wild-type GH (wt-GH) is directly affected by an increasing amount of a shorter GH variant produced, for example, as the consequence of a splice-site mutation in the GH1-gene. We are working on strategies to decrease the expression of this shorter variant to rescue wt-GH secretion.
We also investigate the secretory pathway of GH at the molecular and cellular levels. After RNA transcription, GH needs to be translated and folded, enter the secretory pathway, and be correctly packed in the secretory granules for normal secretion. It is known that zinc plays an important role in this process and our preliminary data suggests that the same
holds true for various zinc transporters in the GH secretory pathway that
are responsible for maintaining zinc dynamics.
What is the role of GH in human physiology?
As the name suggests, GH plays an essential role in postnatal somatic growth. It additionally controls many physiological processes such as bone mineralisation; sugar and lipid metabolism; protein synthesis; and immune system stimulation. It is an anabolic hormone, which explains its misuse in doping in sport.
Are there distinct clinical features in patients suffering from IGHD-II?
Patients with IGHD-II may vary substantially in severity of GHD. For instance, patients with GH1-gene splice-site mutations are thought to be more severely affected – and are younger and shorter at diagnosis – than those with missense mutations causing the disorder.
The affected subjects present with low but detectable serum GH levels, height deficit, muscular hypotonia, reduced lean body mass, frontal bossing, hypogonadism and 40-50 per cent of patients may have an anterior pituitary hypoplasia, in addition to an ectopic posterior pituitary gland.
How do splicing mutations in GH occur?
Most splicing mutations within the GH1-gene are genetically inherited. Individuals affected by IGHD-II occur in every generation in an affected family.
GH1 splice-site mutations mostly occur within the first six nucleotides of intron 3
Growth hormone deficiencies
DRS
PRI
MU
S-E
MU
LLIS
AN
D V
IBO
R PE
TKO
VIC
50 INTERNATIONAL INNOVATION

A growing problemDetailed explorations of the genetic bases of stunted growth in children by paediatric endocrinologists at the Bern Inselspital aim to discover safe, accessible therapies for helping them to achieve normal height
GROWTH HORMONE (GH) is a significant factor in human physiology. Important external factors influence GH levels, including stress, sleep, exercise and food intake. GH is secreted from the anterior pituitary gland at the base of the brain and released in the bloodstream under regulation of two hypothalamic peptides: GH-releasing hormone (GHRH), which is stimulatory, and GH- inhibiting factor (GHIF), which has an inhibitory effect. GH normally regulates its own expression and production by both direct and indirect feedback mechanisms, but on occassion this process can be disrupted.
DEFICIENCY
GH deficiency (GHD) occurs when the pituitary gland cannot produce enough GH to support normal growth and/or other GH-based functions. Patients can be born with this condition, although GHD may also occur later in life. For example, GHD may present in adult patients who have had a tumour, cyst or surgery in the pituitary gland area.
There are two genetic forms of isolated GHD (IGHD): type I (IGHD-I) and -II, both of which derive from an alteration in the GH1-gene. IGHD-II is autosomal dominantly whereas IGHD-I is autosomal recessively inherited. In contrast to
nonsense, missense and deletion mutations that characterise IGHD-I, the majority of IGHD-II mutations described so far affect the splicing of the GH1-gene.
YEARS OF RESEARCH
Professor Dr Primus-E Mullis, Dr Vibor Petkovic and their collaborators at the Children’s Hospital – part of the University Hospital in Bern (Inselspital) – have explored both IGHD-I and IGHD-II, with support from the Swiss National Science Foundation, since 1989. Combining clinical and academic research techniques, they have studied many GH1-gene mutations over the years, as well as alterations within the gene that affect growth and development.
The GH1-gene consists of five exons and four introns, enabling transcription of five variants through alternate splicing mechanisms. Mullis has come to the conclusion that incorrect splicing mechanisms give rise to the form which he and his laboratory currently study – IGHD-II: “Several reports describe various missense or splice enhancer mutations in the GH1-gene leading to IGHD-II, but the disorder is mainly caused by mutations that affect the correct splicing of the GH1-gene, which leads to the production of varying amounts of GH,” Mullis asserts.
and result in skipping of exon 3 during splicing of the GH1-gene. This leads to production of the harmful 17.5-kDa GH variant. Importantly, the amount produced depends directly on the position of the splice-site mutation; so only a slight reduction of it may help to rescue the secretory system, resulting in full recovery from the condition, as we have shown with mice. At the cellular level, 17.5-kDa GH is retained in the endoplasmic reticulum and disrupts the Golgi complex, impairs both GH and other hormonal trafficking, and blocks the secretion of wt-GH.
What is the result of GH1-gene mutations?
GH1-gene mutations may lead to IGHD-I, depending on the location within the GH1-gene. GH may not be produced and, therefore, the children do not secrete any GH. Such children, when treated with recombinant GH (rhGH), may develop antibodies against it and growth is stunted after a few months.
Point mutations that occur in and around exon 3 lead to the production of various amounts of the 17.5-kDa GH isoform, which directly affect normal secretion of wt-GH and are considered the main cause of IGHD-II. Further, secretory granules containing the GH-R183H variant as the result of a missense mutation are not secreted as effectively as those containing wt-GH, finally resulting in its reduced secretion. In addition, by causing structural changes and, therefore, incorrect folding of the GH molecule, P89L missense mutation, leads to profound and early disturbances in the early secretory pathway. In other cases, the mechanism is more complex, as in the GH-R178H mutation, which results in reduced secretion, possibly by disrupting zinc-dependent dimerisation and packaging of GH in granules. In conclusion, any GH1-gene alteration may lead to a specific but different secretory defect within its secretion pathway. Therefore, it is of importance to study any mutation at the functional level as it may change its clinical impact dramatically.
Mullis hopes that his work will lead to the development of better,
longer-acting treatments for growth hormone deficiency
WWW.RESEARCHMEDIA.EU 51
DRS PRIMUS-E MULLIS AND VIBOR PETKOVIC

CLINICAL, GENETIC AND CELLULAR ANALYSIS OF SHORT STATURE CAUSED BY GENES AFFECTING GROWTH HORMONE (GH) SECRETION RESULTING IN ISOLATED GH DEFICIENCY (IGHD) AND STEPS TOWARDS A RESCUE OF THIS DISORDER
OBJECTIVES
• To elucidate the lifecycle of growth hormone (GH) – from production to secretion
• To decrease the expression of the harmful shorter GH variant resulting in the rescue of wild-type GH secretion to treat autosomal dominant isolated GH deficiency sufferers
KEY COLLABORATORS
Switzerland: Dr Vibor Petkovic, Maria Miletta, Andrée Eblé, Dr Nuria Camats, Professor Dr Christa E Flück, University of Bern; Dr Souzan Salemi, Universitäts Spital Zürich; Dr Didier Lochmatter, University of Bonn; Gaby Hofer, University Children’s Hospital, Bern • Germany: Dr Martin Bidlingmaier, Universität München, Munich; Professor Dr Michael Ranke, Professor Dr Gerhard Binder, Universitätsklinikum Tübingen; Professor Dr Roland Pfäffle, Universitäts-Kinderklinik Leipzig • USA: Professor Dr John Phillips II, Vaderbilt-Ingram Cancer Center, Nashville; Professor Dr Roberto Salvatori, Johns Hopkins University, Baltimore • France: Professor Dr Paul Czernichow, Hospital Robert Debré, Paris • UK: Professor Dr Peter Hindmarsh, Professor Dr Mehul Dattani, Professor Dr Iain Robinson, University College Hospital, London; Professor Dr David Dunger, University of Cambridge
FUNDING
Swiss National Science Foundation • Oncosuisse • NovoNordisk • Pfizer • Merck-Serono • Eli-Lilly • Sandoz
CONTACT
Professor Dr Primus-E Mullis Principal Investigator
Paediatric Endocrinology, Diabetology & Metabolism University Children’s Hospital Inselspital CH-3010 Bern, Switzerland
T +41 31 632 9552 E [email protected]
http://p3.snf.ch/project-121998
PROFESSOR DR PRIMUS-E MULLIS studied Medicine at the universities of Fribourg, Bern and Vienna. He then trained in paediatrics and paediatric endocrinology and diabetology in Chur, Lucerne, Bern and London. Since 2000, he has been a full Professor of Paediatrics and the Head of the Division of Paediatric Endocrinology/Diabetology & Metabolism at the University Children’s Hospital in Bern. He served for more than 10 years on the Scientific Board of the Swiss National Science Foundation, is a member of the Swiss Academy of Medical Sciences and is the recipient of many prestigious awards (Swiss Paediatric Association, European Society for Paediatric Endocrinology, Cloetta-Foundation, etc.)
The amount of the harmful mutant GH produced, known as the 17.5-kDa GH variant, relative to the correctly spliced GH 22-kDa wild-type (wt-GH) form, is directly dependent on the position of the splice-site mutation, which occurs in and around exon 3. The mutation can cause complete exon 3 skipping; disrupting the GH secretory pathway and impairing both wt-GH and other pituitary-derived hormone trafficking.
Mullis and his laboratory use in vivo and in vitro methods to elucidate whether the quantity of damaging GH secreted induces specific GHD impacts, ie. whether this affects symptoms presented by patients, such as varying pituitary size; age and speed of onset; and severity of deficiency: “Our recent data suggests that the variable phenotype of IGHD-II may reflect a threshold- and dose-dependency effect of the amount of the 17.5-kDa GH variant,” Mullis elaborates.
CURRENT THERAPEUTIC STATUS
Recombinant GH (rhGH) to boost GH levels is currently the only therapy licenced for IGHD-II. A child with GHD needs to be injected daily with rhGH from diagnosis until they reach their adult height at 16-18 years old, which is tiresome for children and teenagers. For some, daily injections are required for life. Unfortunately, while the therapy is effective, the 17.5- kDa isoform has some toxic effects on the pituitary gland, which can eventually lead to other hormonal deficiencies.
Pharmaceutical companies are working on developing alternatives: an rhGH form that is long-lasting and entails one injection a week drugs which can be administered without injection and hormones that release GH gradually. Mullis’ preferred strategy for patients with GH1 splicing defects that lead to IGHD-II is to target the harmful isoform and so make wt-GH predominant over it, considering the obvious correlation between the clinical severity of the disorder and the relative amount of 17.5-kDa GH.
EXPERIMENTAL METHODS
Mullis’ team explores all possible GH1-gene mutations, using molecular and cellular analysis, as each mutation may have a different impact on GH production and secretion. The researchers also look into other possibilities to explain GHD; for example, if a child appears to have GHD but it is apparent that GH is being secreted, further analysis of whether and how GH is binding to its receptor, and of its subsequent signalling capacities, will be conducted.
In vitro models that the group uses are based on rat or mouse pituitary tumour cell lines to study GH synthesis, secretion and regulation. These cell lines store hormones in secretory granules and secrete them upon stimulation, mirroring natural human GH processes. To examine and compare the effect of a specific human GH1 mutation with that of wt-GH on secretion and the secretory pathway, the scientists express both variants in these cells and then compare their intracellular production and extracellular
secretion. Using confocal microscopy they also carry out detailed studies of the co-localisation of wt-GH or mutant GH within the specific intracellular compartments of the secretory pathway, ie. the endoplasmic reticulum, the Golgi complex and the secretory granules. This technique allows them to investigate situations such as where the mutant GH displays reduced secretion, enabling detection of the stage at which a defect may occur.
RESEARCH FOCI
With a view to defining the mechanism of action of new GH mutations, the laboratory carries out computational analyses. One such looks at GH variants using simulations of their molecular dynamics to distinguish the potential implications of ligand- and sequence-based disruptions.
“One of our key goals is to elucidate the exact storage form of GH in secretory granules and the underlying conditions and mechanisms,” Mullis reveals. The role of zinc and specific zinc transporters in GH storage and secretion in IGHD is a key area of analysis for his laboratory at present.
TOWARDS TREATMENT
Ultimately, Mullis hopes that his work will lead to the development of better, longer-acting treatments for GHD. His laboratory is working on developing compounds that could replace rhGH and still promote growth efficiently. Mullis is particularly looking for a compound that uses different pathways from GH and could be administered other than by injection.
He is also looking into whether it might be possible to engineer a form of GH that could be inhaled or swallowed instead. Using their in vitro cell-based IGHD system, the group is testing the possibility of using different pharmacological agents to adjust alternate GH splicing, and so reduce the amount of 17.5-kDa GH isoform produced following splice-site mutations. “Our final goal is to rescue wt-GH secretion, which could open up new avenues for therapies to cure IGHD,” he reveals. Through these varied and in-depth examinations, it is hoped that Mullis and his collaborators may one day provide the key to curing this devastating condition.
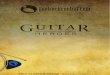
Subcellular colocalisation of wt- and mutant forms of GH with different cell organelles. Cells were fixed and immuno-labelled with either primary antibodies against GH, (wt – first panel, and P89L – last panel), or against Myc (del32-71 – second panel, and R183H – third panel) and with a primary antibody against one of the cell organelles.
52 INTERNATIONAL INNOVATION
INTELLIGENCE