Embed Size (px)
DESCRIPTION
presentation on sepsis
Citation preview
Epidemiology of neonatal sepsis
CAMILLA BRIMBLE, SOPHIE BARRETT, MATTHEW BYOTT, SHERIN CHACKO, SAM GOULD, HANNAH BROOKS, ABDUL ABDULLAH,
RABAB AHMAD
What is the definition of ‘sepsis’?•Sepsis is the condition that develops following an infection/insult and is accompanied by SIRS symptoms
•SIRS stands for Systemic Inflammatory Response syndrome. Under the 1992 guidelines, SIRS is diagnosed by two or more of the following conditions:
oBody temperature >38°C or <36°C
oHeart rate higher than 90 bpm
oRespiratory rate higher than 20/min, or PaCO₂ lower than 32mmHg
oWBC count > 12,000 cells/μl or < 4,000/ μl
•Sepsis = SIRS + confirmed infection
•Newer ‘PIRO’ system for staging sepsis
460-370BC
Hippocrates
979-1037
Ibn Sina
1688-1738
Hermann Boerhave
1818-1865
Semmelweis
1822-1895
Lois Pasteur
1867-1936
H.Lennhartz
WWII
1967 onwards
1827-1912
Joseph Lister
Early Onset Sepsis:Definition: Neonatal early-onset sepsis (EOS) is defined as blood or cerebrospinal fluid culture-proven bacterial infection of the newborn occurring in the first 7 days of life (Mukhopadhyay and Puopolo 2012).
Of newborns with early-onset sepsis, 85% present within 24 hours, 5% present at 24-48 hours, and a smaller percentage present within 48-72 hours. Onset is most rapid in premature neonates.
The microorganisms most commonly associated with early-onset sepsis include the following:
-Group B Streptococcus (GBS)-Escherichia Coli-Coagulase-negative Staphylococcus-Hameophilus influenzae -Listeria monocytogenes
(Anderson-Berry 2014)
The overall incidence of EOS in the United States was 3-4 cases per 1000 live births just prior to the first Centers for Disease Control and Prevention (CDC) guideline recommending the use of intrapartum antibiotic prophylaxis (IAP) to prevent perinatal Group B Streptococcus (GBS) disease (1-4)
With the widespread use of intrapartum antibiotic therapies the incidence of neonatal early onset sepsis has declined.
Currently the incidence of GBS-specific EOS has declined to 0.3-0.4 cases per 1000 live births, and overall EOS incidence has declined to 0.8-1.0 cases per 1000 live births
(Mukhopadhyay and Puopolo 2012)
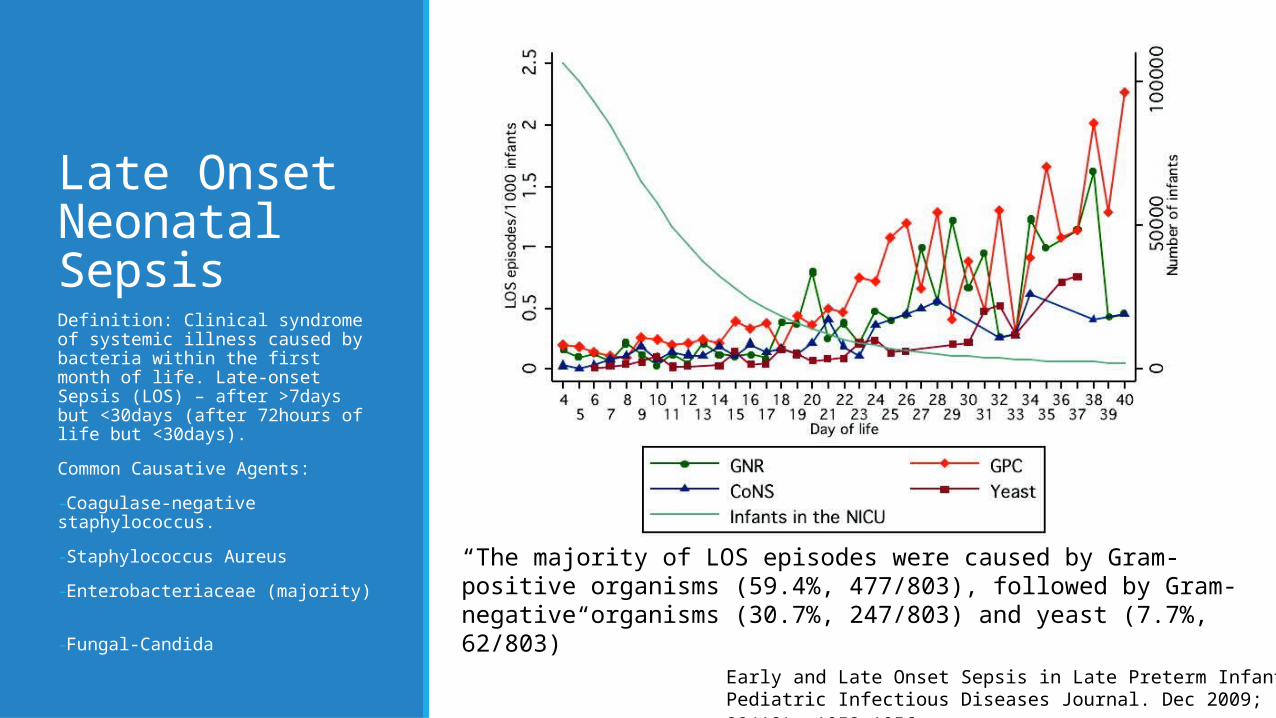
Late Onset Neonatal SepsisDefinition: Clinical syndrome of systemic illness caused by bacteria within the first month of life. Late-onset Sepsis (LOS) – after >7days but <30days (after 72hours of life but <30days).
Common Causative Agents:
-Coagulase-negative staphylococcus.
-Staphylococcus Aureus
-Enterobacteriaceae (majority)
-Fungal-Candida
“The majority of LOS episodes were caused by Gram-positive organisms (59.4%, 477/803), followed by Gram-negative organisms (30.7%, 247/803) and yeast (7.7%, 62/803)”
Early and Late Onset Sepsis in Late Preterm Infants - Pediatric Infectious Diseases Journal. Dec 2009; 28(12): 1052–1056.
Vaginal Microflora and Sepsis•It is estimated that 30-40% of infections resulting in neonatal sepsis deaths are transmitted at the time of childbirth and have early onset of symptoms
•This can be due to the vagina microflora, if a mother is known to have vaginosis she may be treated with antibiotics
•Even if a mother does not have vaginosis standard care to treat newborns’ eyes with topical erythromycin or a similar antibiotic to prevent bacterial infection, showing that the mothers flora may cause infection in infants
•Group B streptococcus, part of the normal vaginal flora in about 25% of women, is a leading cause of neonatal sepsis, mothers ideally should be treated with antibiotics at 35-37 weeks of gestation if this is the case
•If a baby is premature, antibiotics may have not already been administered
•Other bacterial species may be transmitted from the mother to child in vaginal birth such as E.coli and Staphylococcal species, also responsible for causing sepsis
•GBS, Escherichia. coli, Haemophilus influenzae, and Listeria monocytogenes and are most likely to have been acquired transplacentally, by ascending or intrapartum infection
Vaginal Vs Caesarean Births•GBS risk is reduced when a C-section is planned, no antibiotics are required
•The risk is still high in an emergency C-section if the mothers waters have already broken
•Infectious outcomes among 497 women, who were undergoing elective repeat cesarean delivery and 492 who attempted vaginal birth after cesarean (VBAC).
•Rates of both suspected and confirmed neonatal sepsis were significantly lower in the elective repeat cesarean group (2% versus 5%, P<0.05 for suspected sepsis, and 0% versus 1% P<0.05 for proven sepsis
•Although sepsis rates for the child are reduced, sepsis rates for the mother may increase
•The reduction of contact to the vaginal flora is most likely the main reason for a reduced neonate sepsis rate in elective C-section
Neonatal Sepsis in developing countries
●99% of the approximate 1 million annual neonatal deaths happen developing countries, at least 50% of which are from home births or community settings.
●Access to appropriately-trained health workers and high-quality services is limited.
●Current recommendations of hospitalization and parenteral therapy for managing neonatal infections are inadequate.
●Under-recognition of illness, delay in care seeking at the household level, and lack of access to both appropriately trained health workers and to high quality services to manage neonatal sepsis.
●Late onset sepsis is complicated by a higher percentage of Gram-negative bacteria and greater antimicrobial resistance among the organisms.
●Evidence shows newborns in developing countries often don’t receive required healthcare which contributes to the increased mortality in neonates and that this is associated with an increase in mortality.
●Potential sociocultural issues can be a factor.
●Likelihood of infection is increased due to other additional risk factors.
●Unsafe birthing practices are common in developing countries which increase the risk of neonatal sepsis.
●Health education is a possible preventative intervention for improving neonatal health.
●Issues with the supply and quality of antimicrobials in certain developing areas.
Risk of neonate in Britain becoming infected with Group B Streptococcus
• 1 in 1,000 when the mother is not known to be a carrier.
• 1 in 400 when the mother is known to be carrying Group B Streptococcus during pregnancy.
• 1 in 300 when the mother is carrying the bacteria during delivery.
• 1 in 100 when the mother has previously had a baby infected with Group B Streptococcus.
If the mother is known to have Group B Streptococcus bacteria and is given the antibiotics then the risk to the baby is reduced significantly:
• 1 in 8,000 when the mother is known to be carrying GBS during pregnancy.
• 1 in 6,000 when the mother is carrying GBS during delivery.
• 1 in 2,000 when the mother has previously had a baby infected with GBS.
Preterm neonates are 3-15 times more likely to die from GBS infection. 83% of deaths from sepsis are neonates born preterm.
Summary1. Sepsis is a condition arising from a proven infection alongside SIRS
2. From history, much of the knowledge gained about sespsis was based on cases of sepsis in pregnant women – Childbirth was a large risk for sepsis and death.
3. Studies are still underway however it seems neonatal sepsis is at a lower rate when birth occurs via C-Sections due to decreased contact with the mothers flora
4. Group B streptococci are a major cause of early onset sepsis but through the use of intrapartum antibiotic prophylaxis, incidence has significantly decreased.
References Anderson-Berry A (2014). Neonatal Sepsis. Medscape [Online]. Available at http://emedicine.medscape.com/article/978352-overview. [Accessed 9th November 2014]
Borton.C. (2013). Congenital, Perinatal and Neonatal Infections.Available: http://www.patient.co.uk/doctor/congenital-perinatal-and-neonatal-infections. Last accessed 12/11/14.
Blencowe.H , Cousens.S, Mullany.LC, Lee.ACC, Kerber.K, Wall.S,Darmstadt.GL,Lawn.JE. (2011). Clean birth and postnatal care practices to reduce neonatal deaths from sepsis and tetanus: a systematic review and Delphi estimation of mortality effect. BMC Public Health. 11 (3), s11.
German Sepsis Society. (unknown). Sepsis History. Available: http://www.sepsis-gesellschaft.de/DSG/Englisch/Disease+pattern+of+Sepsis/Sepsis+History?sid=zlqSveCVbkfoVuJIVE91yM&iid=2. Last accessed 11/11/14.
Levy, M et al.. (2003). 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Intensive Care Med. 29 (1), 530-538
Mukhopadhyay S and Puopolo K (2012). Risk Assessment in Neonatal Early-Onset Sepsis. Pubmed [Online]. Available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3782302/. [Accessed 10th November 2014]
Paediatrics(2012). Neonatal Sepsis. Available: http://www.paediatrics.co.uk/nicu/neonatal-sepsis. Last accessed 11th Nov 2014.
Patel, SJ Saiman, L. (2010). Antibiotic resistance in neonatal intensive care unit pathogens: mechanisms, clinical impact, and prevention including antibiotic stewardship. Clinics in Perinatology. 37 (3), 547-563.
Oddie, S. (2002). Risk factors for early onset neonatal group B streptococcal sepsis: case-control study. British Medical Journal. 325:308
Singore.C, Klebanoff.M. (2008). Neonatal Morbidity and Mortality After Elective Cesarean Delivery. NIHPA author manuscripts. 35 (2), 361.
Vergnano S, Menson E, Kennea N, Embleton N, Russell AB, Watts T, Robinson MJ, Collinson A, Heath PT (2011). Neonatal infections in England: the NeonIN surveillance network. Pubmed [Online]. Available at: http://www.ncbi.nlm.nih.gov/pubmed/20876594 [Accessed 10th November 2014].
Waters, D et al. (2011). aetiology of community-acquired neonatal sepsis in low- and middle-income countries. Available: http://www.jogh.org/documents/issue201102/JGH2-6_A1_Waters.pdf. Last accessed 14th Nov 2014.
Zaidi, A et el. (2009). Pathogens Associated With Sepsis in Newborns and Young Infants in Developing Countries. The Pediatric Infectious Disease Journal. 28 (1), 10-18.






![Sepsis neonatal [autoguardado]](https://img.pdfslide.us/doc/110x75/58e75b911a28ab4a278b506b/sepsis-neonatal-autoguardado.jpg)