-
Using Computer Modeling to Help Identify Patient Subgroupsin
Clinical Data Repositories
Gregory F. Cooper', M.D., Ph.D., Bruce G. Buchanan2,
Ph.D.,Mehmet Kayaalp1, M.D., M.S., Melissa Saul3, John K. Vries4,
M.D.
'Center for Biomedical Informatics, University of
Pittsburgh2Department of Computer Science, University of
Pittsburgh3University of Pittsburgh Medical Center Health
System
4University of Pittsburgh School of Medicine
OBJECTIVE: The ability to accurately and efficientlyidentify
patient cases of interest in a hospitalinformation system has many
important clinical,research, educational and administrative uses.
Theidentification of cases of interest sometimes can bedifficult.
This paper describes a two-stage method forsearching for cases of
interest.DESIGN: First, a Boolean search is performed usingcoded
database variables. The user classifies theretrieved cases as being
of interest or not. Second,based on the user-classified cases, a
computer modelof the patient cases of interest is constructed.
Themodel is then used to help locate additional cases.These cases
provide an augmented training set forconstructing a new computer
model of the cases ofinterest. This cycle of modeling and
userclassification continues until halted by the user.MEASUREMENTS:
This paper describes a pilotstudy in which this method is used to
identify therecords of patients who have venous thrombosis.RESULTS:
The results indicate that computermodeling enhances the
identification of patient casesof interest.
INTRODUCTION
A hospital information system (HIS) can greatlyfacilitate
retrospective studies of patient cases. Withsuch a system,
researchers also can identify potentialparticipants in prospective
clinical studies. Both usesof a HIS require the identification of
patientsubgroups of interest. The more accurately andefficiently
such subgroups of patients can beidentified, the better.
The accurate and efficient identification of patientsubgroups of
interest extend beyond research studiesto include clinical,
educational and administrativeuses. For example, one educational
application wouldbe the identification of interesting patient cases
foruse in teaching medical students.
If a patient subgroup can be defined by arelatively small and
simple combination of coded datafields in a HIS (e.g., ICD-9 codes,
laboratory values,and patient demographic variables), then finding
therelevant hospital records is relatively straightforward.The task
becomes considerably more challenging,however, when a simple
Boolean combination of datafields does not readily locate all the
patient cases of
interest. In such situations, it may be necessary toperform more
complex searches that involve codedinformation and possibly
unstructured information(e.g., free-text history and physical
examinations,radiology reports, and discharge summaries). Thispaper
describes a semi-automated technique that isintended to assist
users in performing these morecomplex searches.
BACKGROUND
We are using the MARS (Medical ARchival System)hospital
information system at the University ofPittsburgh Medical Center
[1], which contains a richstore of both coded and free-text
clinical information.This section describes a current method that
iscommonly used in identifying patient subgroups inMARS.
Patient subgroups are often identified in MARSas a team effort
by MARS staff and users. Wecharacterize here a typical
collaboration. The user(e.g., a researcher) first describes the
target populationto the staff member, and through a discussion,
theyrefine the description to construct an initial MARSquery.
Typically the staff and user first identify a setof patient
reference cases, which are patient records inMARS that match the
study criteria. These casesoften are obtained using a Boolean
search of MARS.The reference cases are reviewed by the staff
memberto get an idea of the search terms to use in
findingadditional relevant records, which we call
recordmatches.
After developing a refined search query inconsultation with the
user, the staff member performsthe search and reviews the results
with the user. Ifthere are too many records to review
exhaustively,then a sample of the records is reviewed. Through
thisprocess, a set of record matches is assembled. Areview of these
records often provides additional hintsabout how to further refine
the search query, which isrun, and the cycle repeats.
The search and review cycle terninates when theuser is satisfied
with the set of record matches thathave been found. The union of
the reference cases andall record matches constitute the set of
records thatdefine the patient cases of interest to be used
infurther analyses.
1091-8280/98/$5.00 © 1998 AMIA, Inc. 180
-
There are two labor-intensive aspects to theprocess of
constructing a patient subgroup of interest:(a) constructing
complex search criteria beyond theinitial Boolean search, and (b)
reviewing the retrievedresults of searches to identify record
matches andrefine the queries further. We propose a method
tofacilitate these two steps for the staff and user team,which for
brevity we generically call the user. Thecurrent paper focuses
primarily on the first step.
COMPUTER-ASSISTEDIDENTIFICATION OF PATIENT
SUBGROUPS
In this section, we provide an overview of our basicapproach to
using computer modeling to help identifypatient subgroups in MARS.
Figure 1 provides aschematic sumnary of the approach. We currently
arein the process of implementing and integrating all thesteps in
this approach.
The reference cases hold important clues to thepatient features
that distinguish the patient subgroupof interest from the other
patients with records inMARS. We are investigating the use of
computermodeling methods to characterize explicitly
thosedistinguishing clues. The reference cases are used aspositive
instances in a training set. Negativeinstances are either provided
directly by the user or arerandomly selected from the entire set of
MARSrecords if it is highly unlikely that a random hospitalrecord
satisfies the study criteria. The training setcontaining positive
and negative instances is used toconstruct a computer model. The
variables in themodel can represent both coded and free-text
patientdata, although initially we are using only coded data.
The computer model contains a set of patientfeatures (clues)
that characterize approximately thepatient subgroup of interest.
Conceptually, eachpatient record in MARS is compared to the model
todetermine a numeric score that indicates how closelythe record
and the model match (in practice, theimplementation can be more
efficientcomputationally). The most closely matching recordsare
presented to the user, sorted in descending order oftheir scores.
As outlined in Figure 1, the user reviewsrecords in the order they
appear in the sorted list, andin the process indicates record
matches, until the yieldof matches becomes so low that he or she
stops thereview. To help maintain confidentiality, theserecords
contain no explicit patient or clinicianidentifiers (e.g., name,
address, social securitynumber); currently we perform this
de-identificationprocess manually, but we plan to investigate
methodsfor automating it. We hypothesize that (a) thisselective
review of the records will be significantlyfaster than the current
more manual process ofreviewing records, and (b) more record
matches will
be found using the system than are found usingcurrent methods.
The current paper describes apreliminary study that provides a step
towardaddressing these hypotheses.
The records that are marked by the user asmatches or non-matches
become part of a growingtraining set of patient records. The
augmented trainingset is used to learn a new, refined computer
model,and the cycle of search and review continues.Ultimately, the
user will decide to terminate thesearch and review process. At that
point the union ofthe reference cases and all record matches become
thestudy set that is exported for use.
RELATED RESEARCH
Conceptually, the basic methodology presented in thecurrent
paper is closely related to relevance feedbackresearch in
information retrieval [2]. In relevancefeedback, a user performs an
initial search andclassifies a sample of the retrieved
documentsregarding whether or not they are of interest.
Thisfeedback is used to re-weight and possibly expand thesearch
terms that are then used in subsequentretrievals. Other related
research is being pursued bymachine-learning researchers [3].
The line of research we are pursuing isdistinguished along two
basic ways from most of theprior work on relevance feedback. First,
we areinterested in using a highly heterogeneous collectionof
information in the electronic medical record,including free text of
several types (e.g., dictatedhistory and physical examinations,
surgical pathologyreports, and discharge summaries) as well as a
varietyof types of coded information (e.g., demographicinformation,
patient charge codes (see below), andlaboratory results). The
current paper focuses onlearning models using patient charge codes;
it servesas a baseline study for future extensions that
involvemodeling with additional information in the
electronicmedical record. Second, we are interested in applyinga
wide variety of statistical and machine-learningmethods for
modeling. Some of these methods (e.g.,neural networks and Bayesian
networks) are able tomodel multivariate interactions among
features. Byusing a simple Bayes classification model, the
currentpaper serves as a baseline for planned investigationsthat
use more sophisticated modeling techniques.
EXPERIMENTAL METHODS
This section describes a pilot study that involves
theidentification of those patients in the intensive careunit with
a venous thrombosis (VY). The primarygoal of the original study was
to eventually locatejust those patients with a deep venous
thrombosis.
181
-
New cases of interest(new record matches) user indic
are in the
cases are added to thetraining set
cases are model istransferred Cases of constructed
interestfor training [
4 user decides to stop _searching for more cases
Finalcases of interest(de-identified)
cates which casessubgroup of interest
model
Possible new cases ofinterest (de-identified)
patientidentifiers are
s removed from
RS case recordss Possible
--00 new casesIof interestI
MARSdatabase
Figure 1. An outline of a method for identifying patient
subgroups that uses computer modeling.
We investigated an approach in which initial cases ofVT are
obtained by a simple search of coded featuresof the total study
population. The question is whetherthere are other cases of VT that
computer modelingcan help a user efficiently locate.
The total study population consists of allpatients admitted to
two medical ICUs at theUniversity of Pittsburgh Medical Center
HealthSystem (UPMC-HS) between January 1, 1993 andDecember 31,
1995. There were a total of 3020patients. Of these, 124 patients
were identified ashaving VT, based on being assigned one or more
ofthe following ICD-9 codes at discharge: other venousthrombosis
(ICD-9 code 453), Budd-Chiari syndrome(453.0), thrombophlebitis
migrans (453.1), vena cavasyndrome (453.2), renal vein thrombosis
(453.3),venous thrombosis nec (453.8), and venousthrombosis nos
(453.9). An ICU specialist reviewedthe MARS patient records and
verified that the recordssupport a VT diagnosis.
In the current experiment, we randomly dividedthe 124 VT cases
into two parts. A total of 74 caseswere placed in a training
dataset. For the purpose ofour study, we imagine that this dataset
contains allthe cases found by a Boolean search of the ICD-9codes;
suppose, for example, that the ICD-9 coding ofrecords had been less
complete, and only 74 caseswere coded as VT. We use the remaining
50 cases as atest dataset. We investigate to what extent
computermodeling can help efficiently locate some or all ofthose 50
cases without using ICD-9 codes; so, forexample, if the ICD-9
coding had been incomplete,we are investigating the extent to which
the uncoded50 cases could be located by means other than theICD-9
codes.
Of the 3020 ICU patient cases, we randomlyselected 1802 cases
for use in preliminaryexperiments that investigated model
construction
methods. To avoid testing bias, in performing thefinal
experiment reported here, we used only theremaining 1218 cases
(3020 - 1802). These 1218cases contained 50 VT cases, as
mentionedpreviously; none of these 50 cases appeared in the1802
cases used in preliminary experiments. Thefraction of VT cases in
the entire set of 3020 isapproximately 4 percent. Likewise, the
fraction of VTcases in the set of 1218 cases is approximately
4percent; thus, our evaluation dataset of 1218 casesprovides an
unbiased sample of the original patientpopulation of 3020
cases.
We used patient charge codes as the features(variables) with
which to construct computer modelsof VT cases. A charge code is a
single item charged toa patient during his or her hospitalization.
Forexample, the code 33001371 is used to represent acharge for
"warfarin sodium S mg tablet". There areapproximately 45,000
distinct items that can becharged at UPMC-HS. Among the 3020 cases
in ourstudy database, only 7035 distinct charge codesappeared.
Since charge codes can be very specific, andthus lead to small
sample sizes, we augmented these7035 charge code features with 1081
abstract features.In the current pilot study, an abstract feature
wascreated for each unique first word within the chargecode
descriptions; as an example, the abstract chargecode heparin
corresponds to the disjunction of allcharge codes whose
descriptions begin with the word"heparin". For the current study,
we choose to usecharge codes because (a) they represent many of
theactions taken in caring for patients, and thus, are arich source
of clinical information, and (b) they aresufficiently voluminous
and complex in theirorganization that using them in a structured
Booleansearch would be difficult for most users. Werepresented a
given charge code as a binary variable.The value of a charge code
is set to true if the given
182
Initialcases ofinterest(thereferencecases)
-
charge was made at any time during a patient'shospitalization;
otherwise, the value was set to false.
We used a simple Bayes system as a statisticalmodel, because it
is simple to code, efficient to learnand apply, and it often
performs well in practice. Asimple Bayes system assumes that
features (e.g.,charge codes) are independent conditioned on
adiagnosis (e.g., VT). Although this assumptionusually is not
valid, simple Bayes models have beenshown to be robust to
violations of the assumptionwhen the models are used for
classification [4]. Thatis not to say that improvements cannot be
made byusing more sophisticated models, which we intend todo in
future research.
Suppose that d represents a diagnosis orprediction (e.g., VT).
Let d' denote that d is bound tosome particular value (e.g., VT=
present). Let fidenote a feature (e.g., a charge for a 5 mg
warfarintablet) that is bound to some particular value (e.g.,either
bound to the value true orfalse). Let F denote aset of n features,
each of which is bound to somevalue. A simple Bayes model computes
theprobability of d' given F as follows:
nP(d')HP(fi d')
P(d' F) = i=l (1)n
(P(d) P(fi d))d i=l
where n is the number of features in the model andthe sum is
taken over all the values of d (e.g., d =present and d = absent).
For any specific values offand d, we estimated the term P (Jf d)
as(freq(fi, d) + 1)/(freq(d) + 2), wherefreq(f, d) is thenumber of
times that f. and d co-occur in the trainingdatabase. Similarly, we
estimated P(d) as(freq(d) + 1)/(N + 2), where N is the total
numberof cases in the training database. When the samplesize is
small, these estimates are less extreme than aremaximum likelihood
estimates based on the simpleratios freq(fi,d)/freq(d) and
freq(d)/N.
When there are a large number of features, simpleBayes models
often have better predictive performanceif feature selection is
applied. Thus, rather than usemany thousands of charge codes in
Equation 1, asearch method is applied to select a relatively
smallnumber of features that are highly predictive of thediagnosis.
We used a simple feature selection method:in Equation 1 we only
used those features with thevalue true in at least one case in the
training set.
Initially (cycle 0) we started with a training setcontaining 74
cases of patients known to have hadVT and 74 cases known not to
have had VT. Theseconstitute the reference cases denoted in Figure
1.Following the figure, a simple Bayes model was
constructed from those 148 cases. This model wasapplied to the
1218 cases in the test set and aprobability of VT was computed for
each case usingEquation 1. The probabilities were sorted
indescending order. We assumed that a user would bewilling to
review the 40 most probable VT cases andclassify each case as VT or
not. In actual practice,such a review would involve the user
examining theMARS record of each of the 40 patients to
assesswhether the patient had experienced VT. Such anexamination
could involve looking at structuredinformation (e.g., laboratory
values) or free text (e.g.,discharge summaries). In our experiments
wesimulated the assessments that a user would give. Wewere able to
do so because we assume that among the3020 cases the only ones with
VT were those 124cases described above.
We repeated this cycle of 40 patients for 10cycles. We stopped
after 10 cycles because it seemsunlikely that a user would be
willing to review morethan 400 cases.
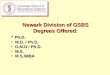
RESULTS
Figure 2 shows the key results. The x axis representsthe number
of cycles taken in Figure 1. In a singlecycle, the 40 most probable
VT cases (outside thetraining set) are presented to the user
forclassification. The y axis shows the total number ofVT cases
found, which is equal to the 74 referencecases plus the new record
matches as verified by theuser.
Figure 2. A plot of the total number of VTcases located as a
function of the modeling cycle.
The upper line in Figure 2 is the maximumperformance that could
be achieved; since only 40cases are selected in each cycle, the
maximum numberof cases that can be identified just after the first
cycleis 40 + 74 = 114. The line containing triangles
183
1249 . . . ....
104 -- -le -
'94 I*/ @*-*e**
.89
84 A Bw us* @ *.se
740 1 2 3 4 5 6 7 8 9 1[0
cycl
-
shows the performance of applying the methoddescribed in the
previous section. The lower line isthe performance that would be
expected whenrandomly selecting 40 patient cases (from outside
thetraining set) during each cycle; this performancecorresponds to
randomly searching through the ICUpatients in search of VT cases
beyond the original 74.
DISCUSSION
The results in Figure 2 indicate that computermodeling is
helping locate VT cases that are notincluded in the original set of
74 reference cases. Inthe first cycle, 7 new VT cases are included
amongthe 40 cases presented to the user. Based on VThaving a prior
probability of 4 percent in this dataset,we would expect to find
only 1 or 2 VT cases in arandom sample of 40 cases. The performance
ofcomputer modeling continues at about the same rate,until the
fourth cycle. A plausible interpretation isthat as more and more VT
cases are discovered, theremaining cases become relatively fewer
and aretherefore more difficult to locate; thus, the slopebegins to
flatten at about the fourth cycle. Also, themost apparent VT cases
are likely to be located in theearly cycles, leaving the more
difficult cases for latercycles. Another factor is that we
presently are usingonly charge codes as model features. We intend
toexpand the features modeled to include demographicinformation,
ICD-9 codes, and DRG codes; we thenplan to investigate the extent
to which theseadditional features change the system's
performance.
In the present study, we have assumed that all2896 (i.e., 3020 -
124) cases that are not known to beVT are in fact not VT. As a
check on thatassumption, we plan to have an ICU specialistexamine
cases of VT that are predicted by the systemand that are not among
the 124 cases alreadyestablished to be VT. We are interested in the
fractionof those cases that the specialist designates as beingVT
cases. The larger the fraction the better. As asupplementary check,
we also plan to select afeasible-sized random sample of the 2896
cases andpresent these to the specialist for evaluation. Fromthe
fraction designated by the specialist as VT caseswe can estimate
the total number of VT cases withinthe entire dataset of 3020
cases.
In the near term, we also plan to expand ourinvestigation to the
identification of other patientsubgroups. In the longer term, our
plans include therepresentation of features that are extracted from
freetext in the medical record (e.g., the dischargesummary). Our
emphasis in representing free textwill be to explore relatively
simple methods that willbe computationally tractable on a database
the size ofMARS. For example, one basic approach is to mapfree-text
phrases into UMLS Metathesaurus conceptsusing available mapping
tools. Each identifiedconcept represents one variable that
characterizes a
part of the free-text report. We also will explore awide variety
of statistical and machine-learningmodels, including neural
networks, Bayesiannetworks, and rule-based systems. We plan to
providea web interface that will allow a user to perform aninitial
set of Boolean queries on coded features, thenextend the search for
patient cases using computermodeling. The interface will permit the
user toexamine and directly alter the model, if desired. Anaudit
trail will be maintained of all user decisionsregarding
classification of cases in order to documentfor each case the
user's justification for it being ofinterest or not.
When the overall search system is sufficientlymature, we plan to
perform a randomized, controlexperiment with a wide variety of
users and searchtasks in order to compare the computer
modelingapproach to the current approach. The primary metricswe
anticipate using are the total patient cases ofinterest that are
found using each approach (casecapture), the total amount of user
and staff timeexpended in obtaining those cases, and the
users'assessments of the utility of the case capture giventhe total
expended time.
Acknowledgments
We thank Dr. Michael Donahoe for his help indefining the dataset
that we used in the pilot studyreported here. We thank Dr. Charles
Friedman forhelpful comments on the design and development ofthis
project. This research was supported in part byIAIMS grant
I-G08-LM06625 from the NationalLibrary of Medicine to the
University of Pittsburgh.
References
1. Yount RJ, Vries JK, Councill CD. The MedicalArchival System:
An information retrieval systembased on distributed parallel
processing.Information Processing Management 1991;27:379.
2. Hannan D. Relevance feedback and other querymodification
techniques. In: Frakes WB, Baeza-Yates R, eds. Information
Retrieval: DataStructures and Algorithms. Englewood Cliffs,
NJ:Prentice Hall, 1992: 241-263.
3. Nigam K, McCallum A, Thrum S, Mitchell T.Learing to classify
text from labeled and unlabeleddocuments. National Conference on
ArtificialIntelligence (AAAI), 1998.
4. Domingos P. Pazzani M. On the optimality of thesimple
Bayesian classifier under zero-one loss.Machine Learning
1997;29:103-130.
184