Embed Size (px)
Citation preview
Great Debates in Vascular Medicine
Pro: Iliac vein lesions/obstruction should
always be treated PRIOR to lower
extremity superficial vein ablation for
patients with venous leg ulcers
Mitchell Silver DO FACC FSVM RPVI
Director, Center for Critical Limb Care
Ohio Health Heart and Vascular
Columbus, Ohio
PI-
422002-A
A S
EP
2016
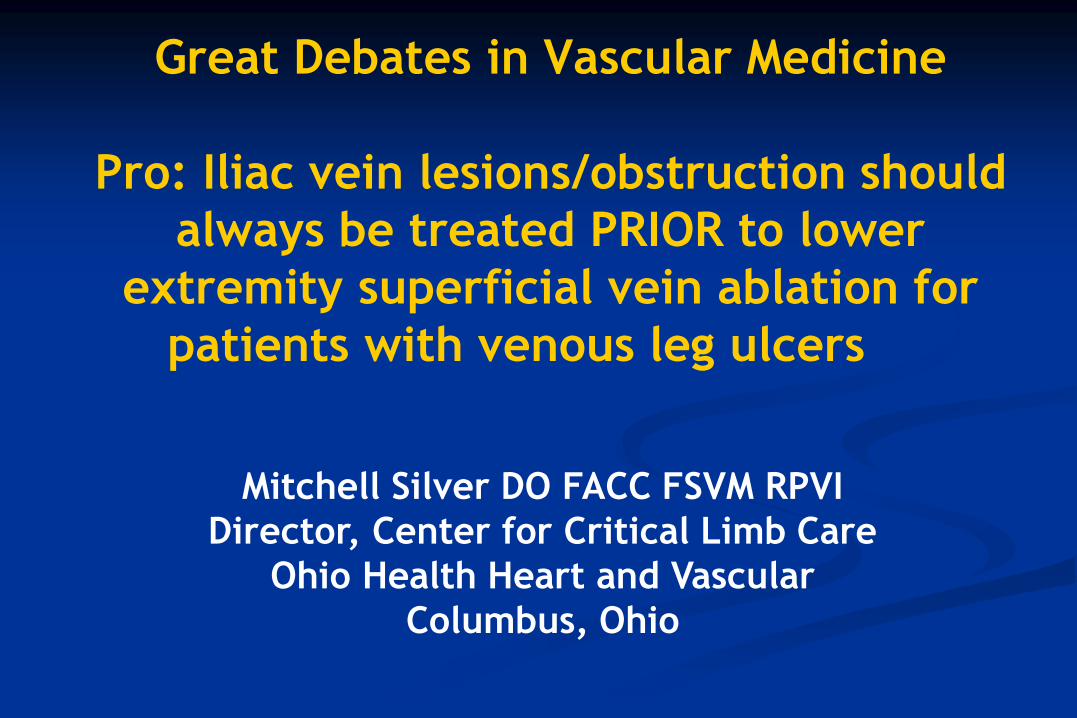
The Real World
Fix the Ulcer vs Fix the Patient…..
64 year old male
Venous stasis ulcer for 2 years
Venous claudication
Recurrent stasis cellulitis
Chronic leg pain/ache with standing
Recurrent swelling
Very low score on quality of life
questionnaire
>> CTA CHRONIC LEFT COMMON ILIAC VEIN OCCLUSION
PI-
422002-A
A S
EP
2016
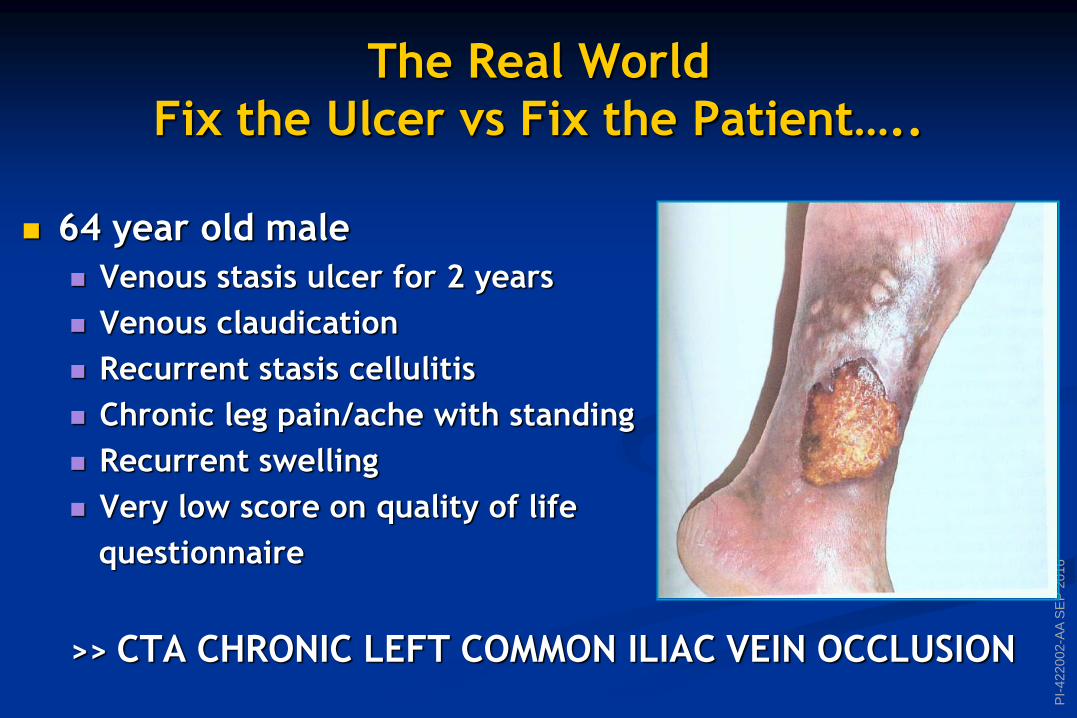
Superficial Vein Ablation
May Heal the Ulcer ???
BUT WHAT ABOUT THE PATIENT ???
PI-
422002-A
A S
EP
2016
This is Simple Physiology…..
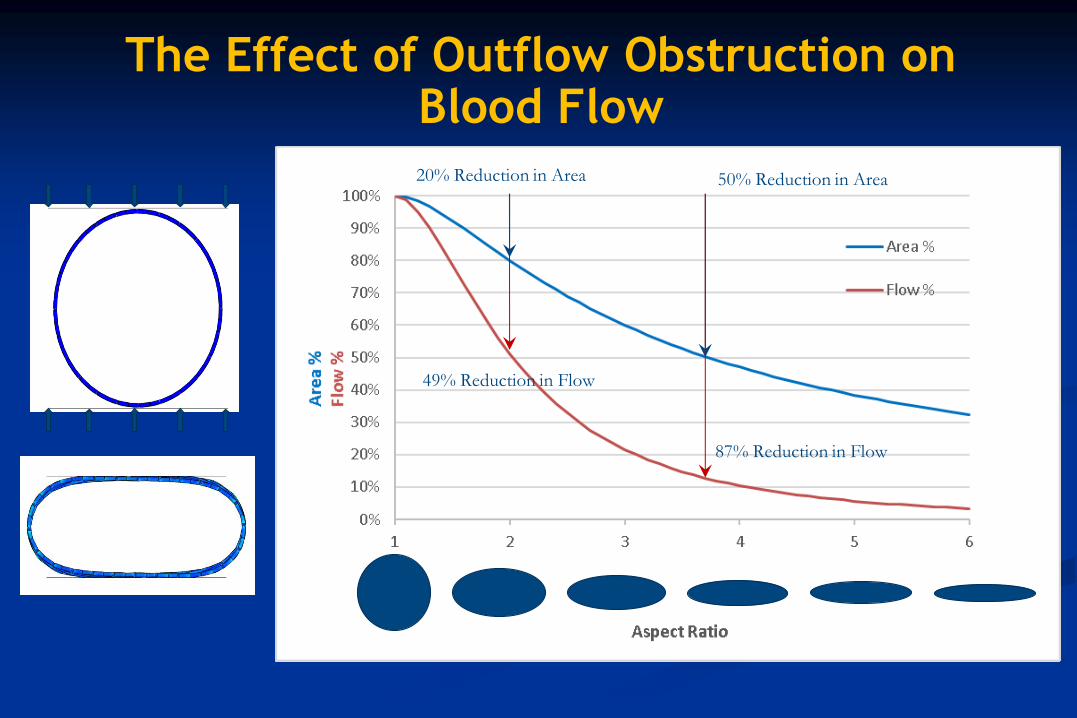
The Effect of Outflow Obstruction on Blood Flow
20% Reduction in Area 50% Reduction in Area
49% Reduction in Flow
87% Reduction in Flow
PI-
422002-A
A S
EP
2016
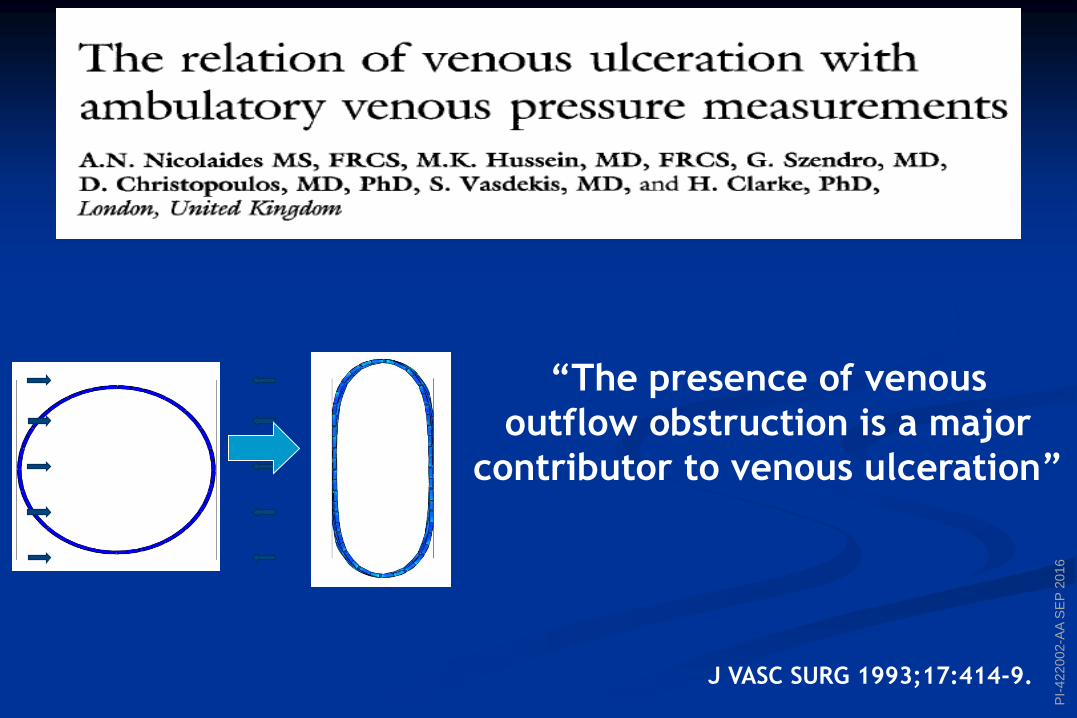
J VASC SURG 1993;17:414-9.
“The presence of venous
outflow obstruction is a major
contributor to venous ulceration”
PI-
422002-A
A S
EP
2016
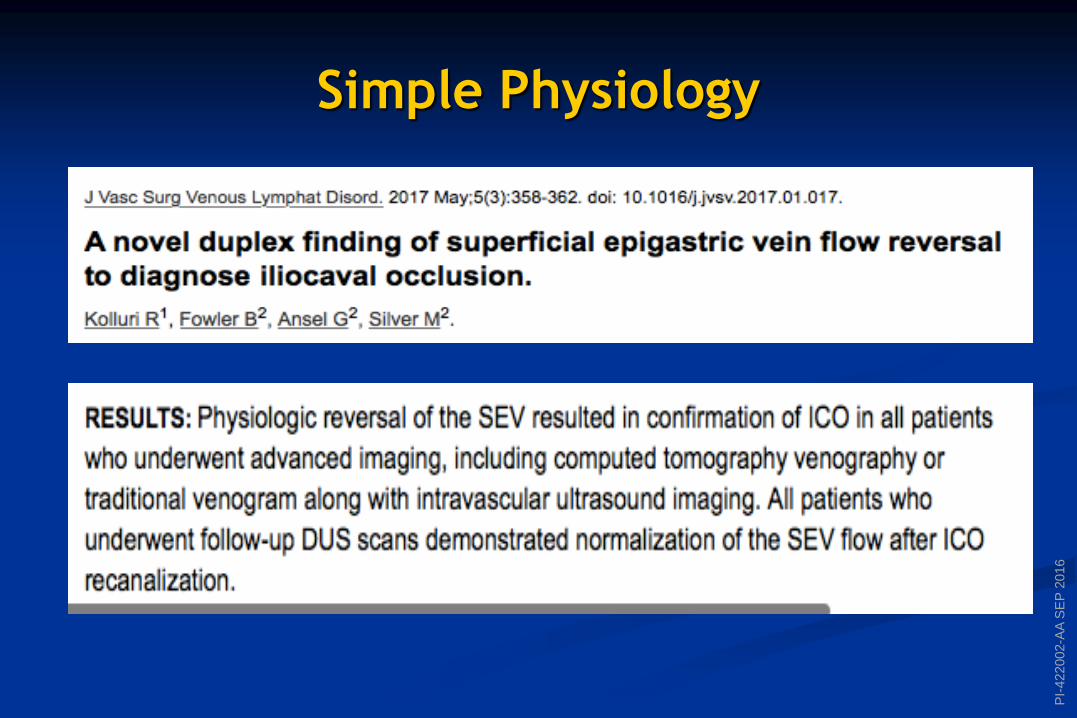
Simple Physiology
PI-
422002-A
A S
EP
2016
The Facts from the Evidence – Venous Ulcers
Etiology, Anatomy, Pathophysiology
Venous outflow obstructions are found in combination with
reflux in 55% of symptomatic patients.
This combination leads to the higher levels of venous
ambulatory pressure and more severe symptoms then when
either condition is present alone.
The authors recommend that when significant obstruction is
localized above the inguinal ligament, the obstruction
should be treated before any concomitant reflux.
McDaniel HB, Marston WA, Farber MA, et al. Recurrence of chronic venous ulcers on the
basis of clinical, etiologic, anatomic, and pathophysiologic criteria and air
plethysmography. J Vasc Surg. 2002;35:723-728.
PI-
422002-A
A S
EP
2016
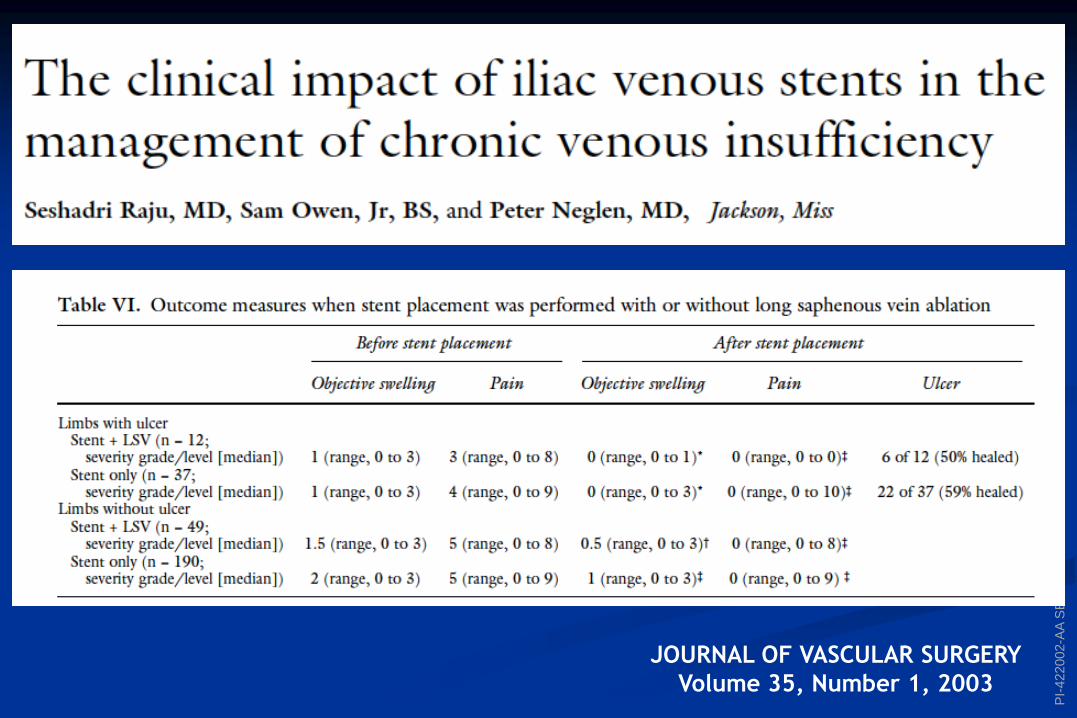
JOURNAL OF VASCULAR SURGERY
Volume 35, Number 1, 2003
PI-
422002-A
A S
EP
2016
“THE MESSAGE”
Significant iliofemoral venous obstruction should be
treated, whether associated with reflux or not, in
patients with venous stasis ulceration.
When obstruction is shown with reflux, the obstruction
should be treated first.
JOURNAL OF VASCULAR SURGERY
Volume 35, Number 1, 2003
PI-
422002-A
A S
EP
2016
The CONCLUSION
Iliocaval intervention alone may be sufficient
to treat patients with combined significant
reflux of both CFV and GSV.
PI-
422002-A
A S
EP
2016
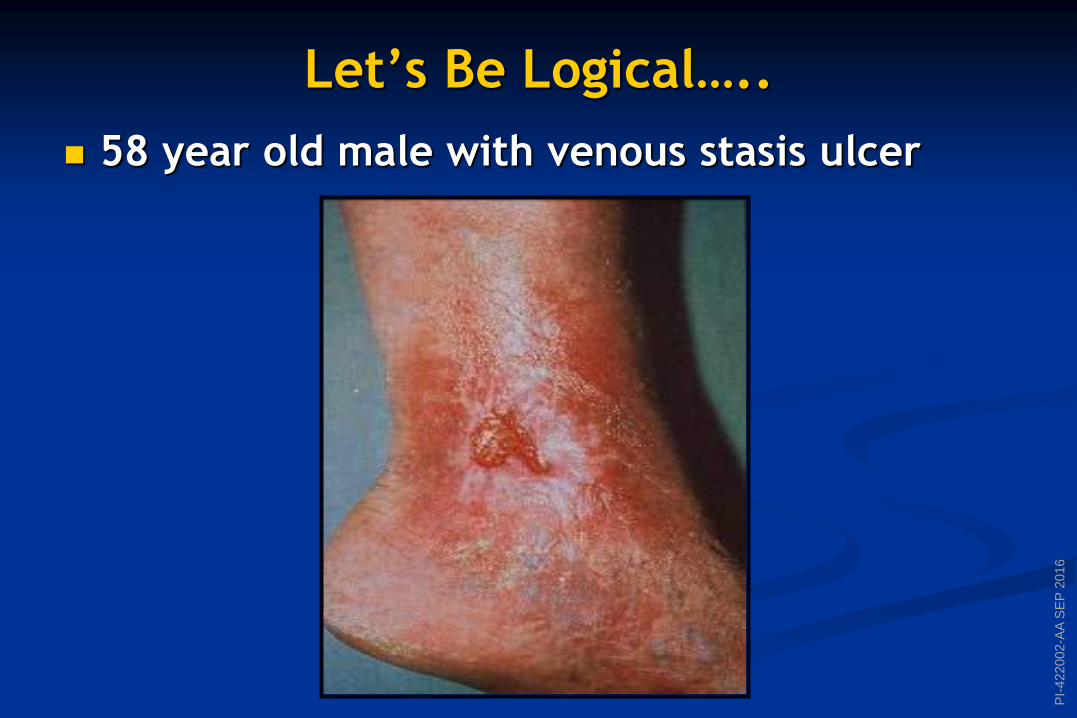
Let’s Be Logical…..
58 year old male with venous stasis ulcer
PI-
422002-A
A S
EP
2016
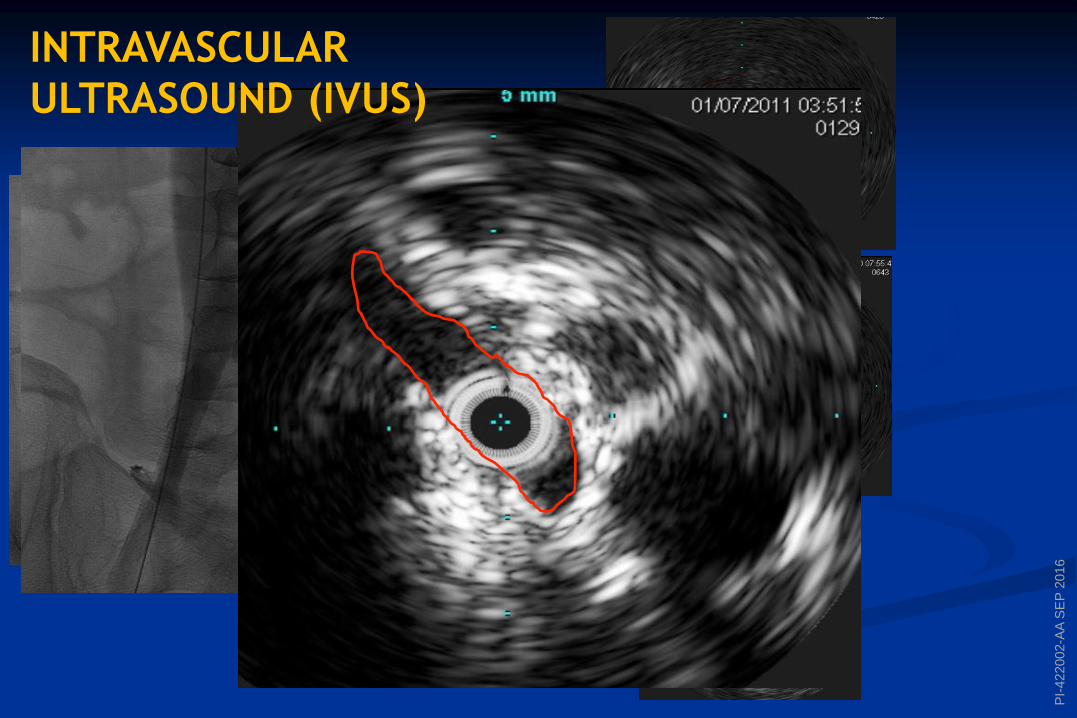
INTRAVASCULAR
ULTRASOUND (IVUS)
PI-
422002-A
A S
EP
2016
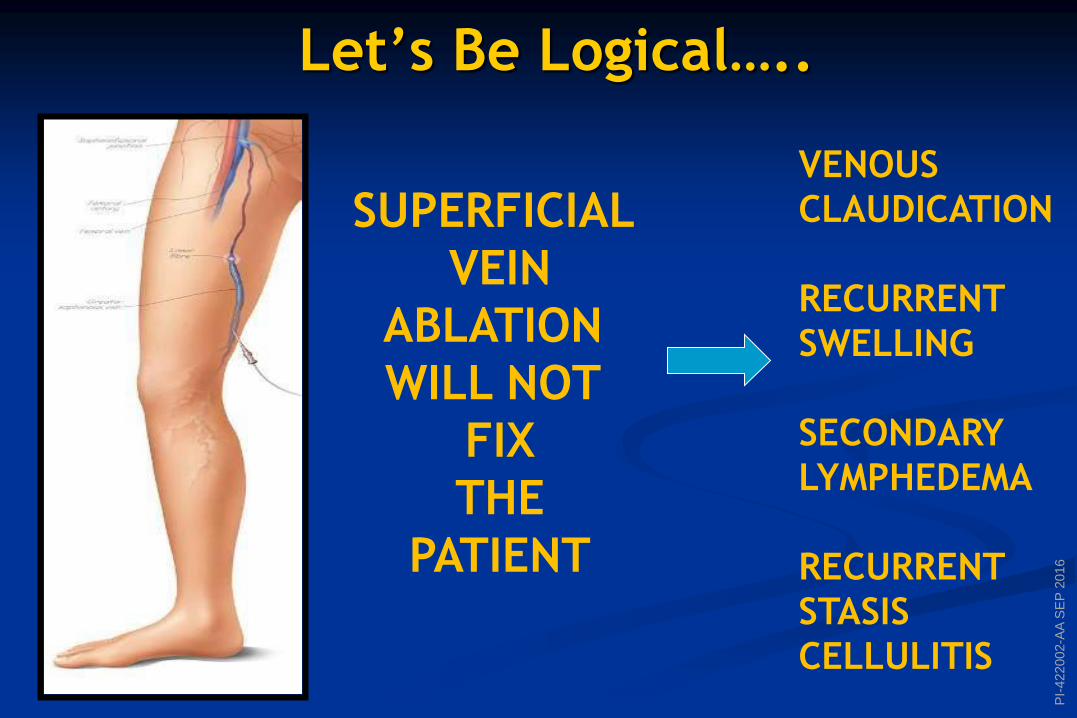
Let’s Be Logical…..
SUPERFICIAL
VEIN
ABLATION
WILL NOT
FIX
THE
PATIENT
VENOUS
CLAUDICATION
RECURRENT
SWELLING
SECONDARY
LYMPHEDEMA
RECURRENT
STASIS
CELLULITIS
PI-
422002-A
A S
EP
2016
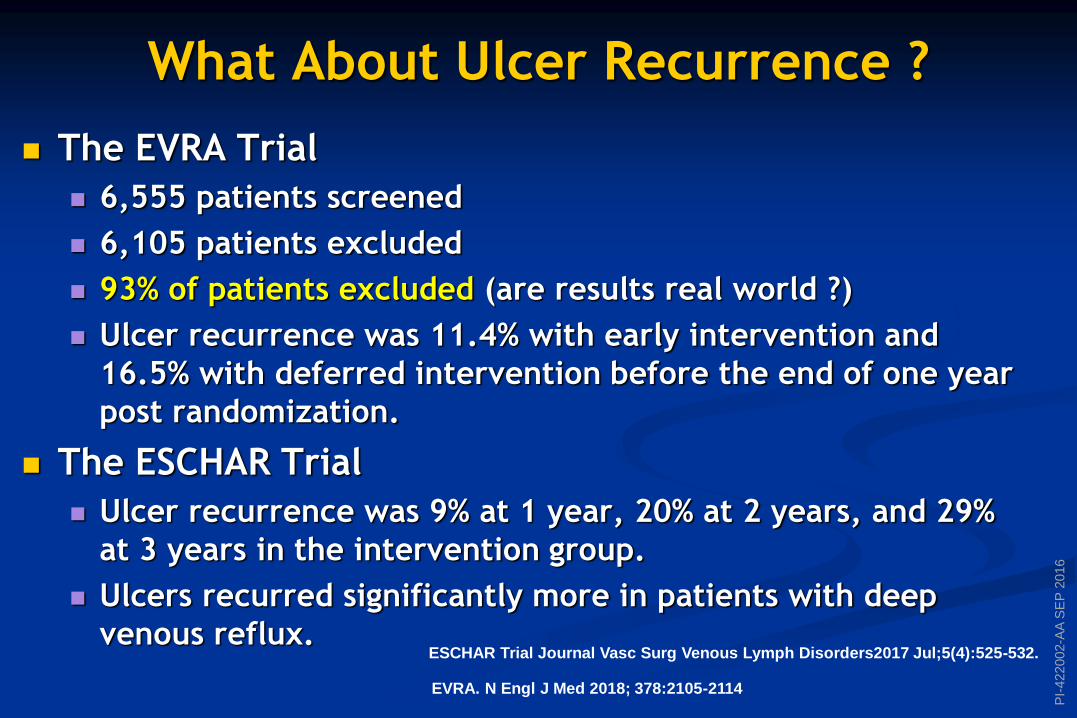
What About Ulcer Recurrence ?
The EVRA Trial
6,555 patients screened
6,105 patients excluded
93% of patients excluded (are results real world ?)
Ulcer recurrence was 11.4% with early intervention and
16.5% with deferred intervention before the end of one year
post randomization.
The ESCHAR Trial
Ulcer recurrence was 9% at 1 year, 20% at 2 years, and 29%
at 3 years in the intervention group.
Ulcers recurred significantly more in patients with deep
venous reflux.
ESCHAR Trial Journal Vasc Surg Venous Lymph Disorders2017 Jul;5(4):525-532.
EVRA. N Engl J Med 2018; 378:2105-2114
PI-
422002-A
A S
EP
2016
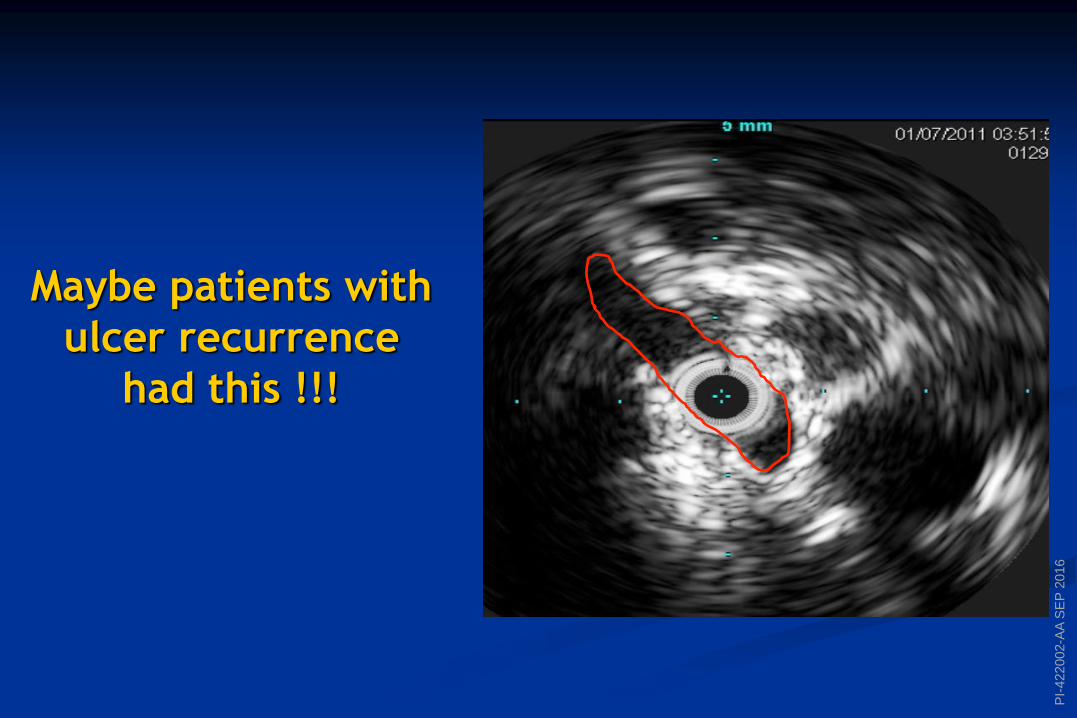
Maybe patients with
ulcer recurrence
had this !!!
PI-
422002-A
A S
EP
2016
THEY PROBABLY DID…
Incidence of and risk factors for iliocaval venous
obstruction in patients with active or healed venous
leg ulcers.
37% of imaging studies demonstrated obstruction of at
least 50%, and 23% had obstruction of >80%.
Risk factors that were found to be independently
associated with a significantly higher incidence of >80%
obstruction included female gender (P = .023), a medical
history of DVT (P = .035), and reflux in the deep venous
system (P = .035)
YOU DON’T KNOW UNLESS YOU LOOK !!!
Marston W. J Vasc Surg 2011 May;53(5):1303-8.

PI-
422002-A
A S
EP
2016
REBUTTAL
PI-
422002-A
A S
EP
2016
PI-
422002-A
A S
EP
2016
PI-
422002-A
A S
EP
2016
PI-
422002-A
A S
EP
2016
PI-
422002-A
A S
EP
2016
The Evidence
McDaniel HB, Marston WA, Farber MA, et al. Recurrence of chronic venous ulcers on the
basis of clinical, etiologic, anatomic, and pathophysiologic criteria and air plethysmography.
J Vasc Surg. 2002;35:723-728.
Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr. The site of residual abnormalities in
the leg veins in long-term follow-up after deep vein thrombosis and their relationship to
the development of the post-thrombotic syndrome. Int Angiol. 1996;15:14-19.
Johnson BF, Manzo RA, Bergelin RO, Strandness DE Jr. Relationship between changes in the
deep venous system and the development of the postthrombotic syndrome after an acute
episode of lower limb deep vein thrombosis: a one- to six-year follow-up. J Vasc Surg.
1995;21:307-312
Alimi YS, DiMauro P, Fabre D, Juhan C. Iliac vein reconstructions to treat acute and
chronic venous occlusive disease. J Vasc Surg. 1997;25:673-681.
O’Sullivan GJ, Semba CP, Bittner CA, et al. Endovascular management of iliac vein
compression (May-Thurner) syndrome. J Vasc Interv Radiol. 2000;11:823-836.
PI-
422002-A
A S
EP
2016
There is increasing support for the beneficial effect of superficial
vein ablation on the healing rate and recurrence of venous leg
ulcers.
The ulcer recurrence rate is, however, markedly increased by the
presence of deep reflux even after superficial reflux ablation.
A cumulative recurrence rate at 4 to 5 years is reported to be
67% to 100%, and 6% to 28% in limbs with and without deep
involvement, respectively.
Thus, deep venous insufficiency appears to be a major
determinant for ulcer recurrence.
The Facts from the Evidence








![Agenesis of common iliac vein encroaching development of … · 2020-06-20 · Agenesis of common iliac vein 23 vein embolization and sampling of renal and adrenal veins [14]. Ruggeri](https://img.pdfslide.us/doc/110x75/5fa85145ea725f20c15155f3/agenesis-of-common-iliac-vein-encroaching-development-of-2020-06-20-agenesis-of.jpg)