Embed Size (px)
Citation preview
Grand Rounds PresentationNURS 4340
Shannon Arender
February 14th, 2008
Collaboration of client management
NursesDoctorsRespiratory therapistsPhysical therapistsPeersInstructor
Client demographics
27 years oldCaucasian female5’3’’, 123 IbsNo religious affiliationDivorced1 child, 7 years old
+ Risk Factors
Congenial diseasePersistent heavy tobacco use, 1 pack per
day since age 14Complete noncompliance with medical
therapy
Events leading to hospitalization
Discontinued Interferon Gamma injectionsAdmitted 1/2/2008 to Vanderbilt Received argon ablation therapyLeft against medical adviceAdmitted to St. Thomas 1/7/2008Transferred to CCU from 7th floor after
sneaking to smoke a cigarette which resulted in patient being intubated
Medical Diagnosis
Congenital squamous papillomatosis of the trachea, larynx, and lung with presumed tracheoesophageal (TE) fistula
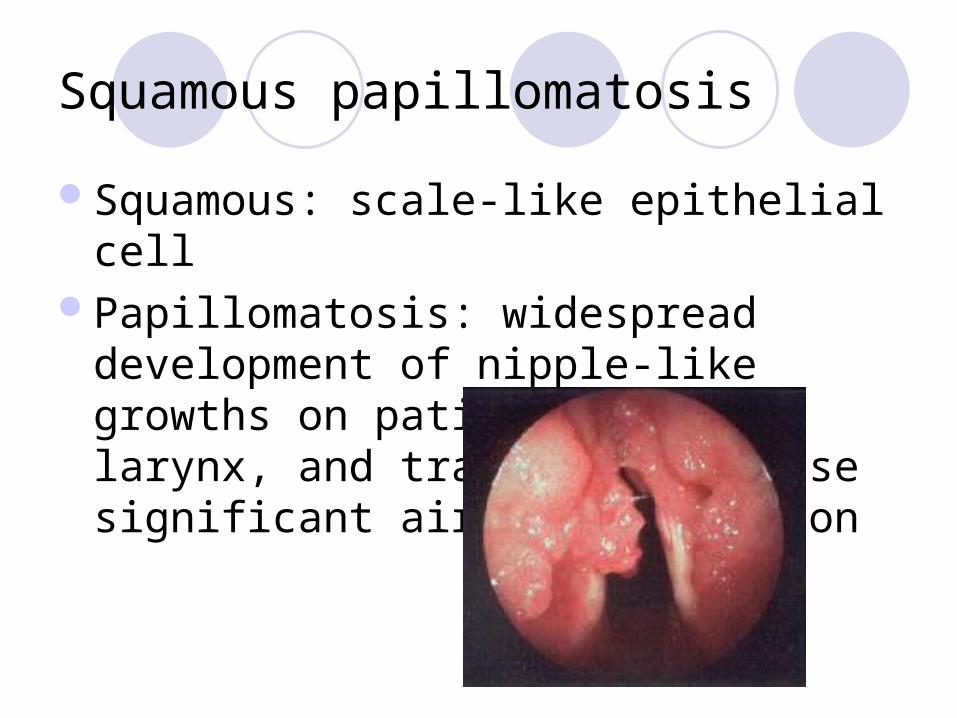
Squamous papillomatosis
Squamous: scale-like epithelial cellPapillomatosis: widespread development
of nipple-like growths on patient’s lungs, larynx, and trachea that cause significant airway obstruction
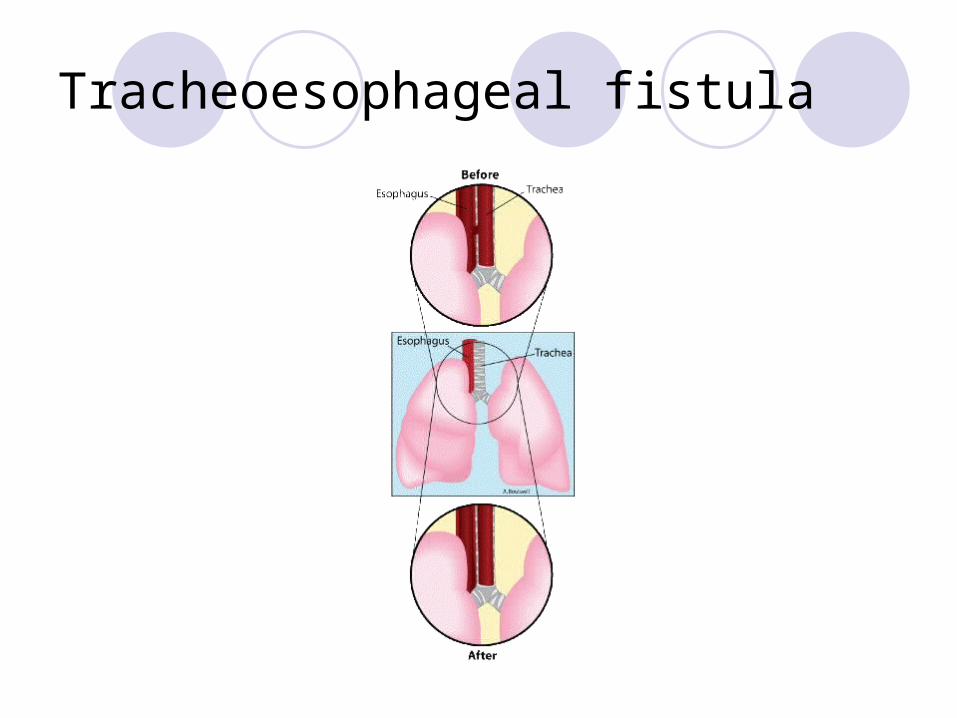
Tracheoesophageal fistula
A congenital malformation in which there is an abnormal tubelike passage between the trachea and esophagus
Puts the patient at risk for aspiration pneumonia and breathing problems
Tracheoesophageal fistula
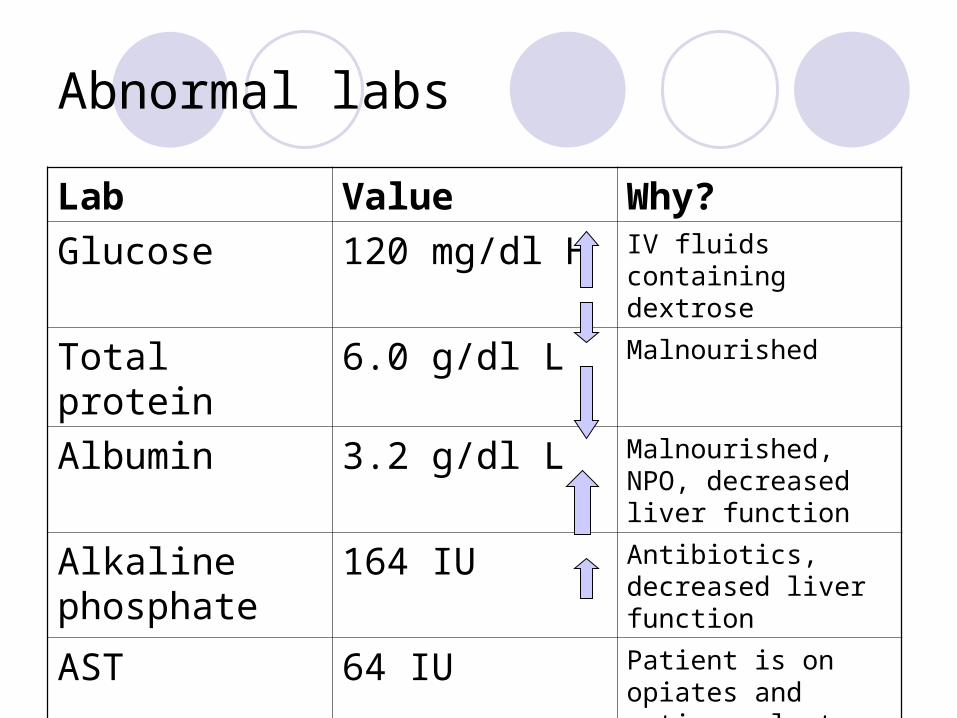
Abnormal labs
Lab Value Why?
Glucose 120 mg/dl H IV fluids containing dextrose
Total protein 6.0 g/dl L Malnourished
Albumin 3.2 g/dl L Malnourished, NPO, decreased liver function
Alkaline phosphate
164 IU Antibiotics, decreased liver function
AST 64 IU Patient is on opiates and anticoagulants, decreased liver function
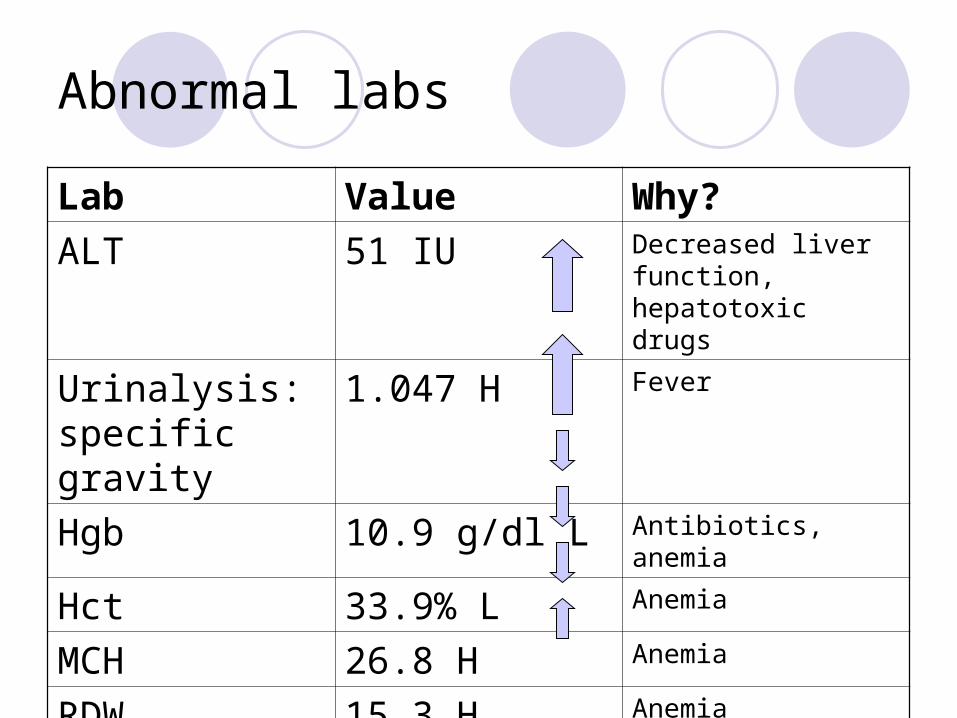
Abnormal labs
Lab Value Why?
ALT 51 IU Decreased liver function, hepatotoxic drugs
Urinalysis: specific gravity
1.047 H Fever
Hgb 10.9 g/dl L Antibiotics, anemia
Hct 33.9% L Anemia
MCH 26.8 H Anemia
RDW 15.3 H Anemia
Diagnostic tests
CT scan of neck for soft tissue Confirmed diagnosis of tracheoesophageal
fistula Seen at level of lower cervical esophagus
X-RAY- video fluoroscopic swallow Done post recent laser therapy for TE fistula Patient was unable to handle secretions, had
one episode of frank aspiration
Diagnostic tests
X-RAY- lung Extensive abnormalities found in lungs Numerous masses, many that contain cavities Range in size from less than 1 cm up to 4 cm Lower lobes are the most severely affected
X-RAY- performed to verify PICC placement All findings are consistent with clinical diagnosis of TE
fistula and papillomatosis
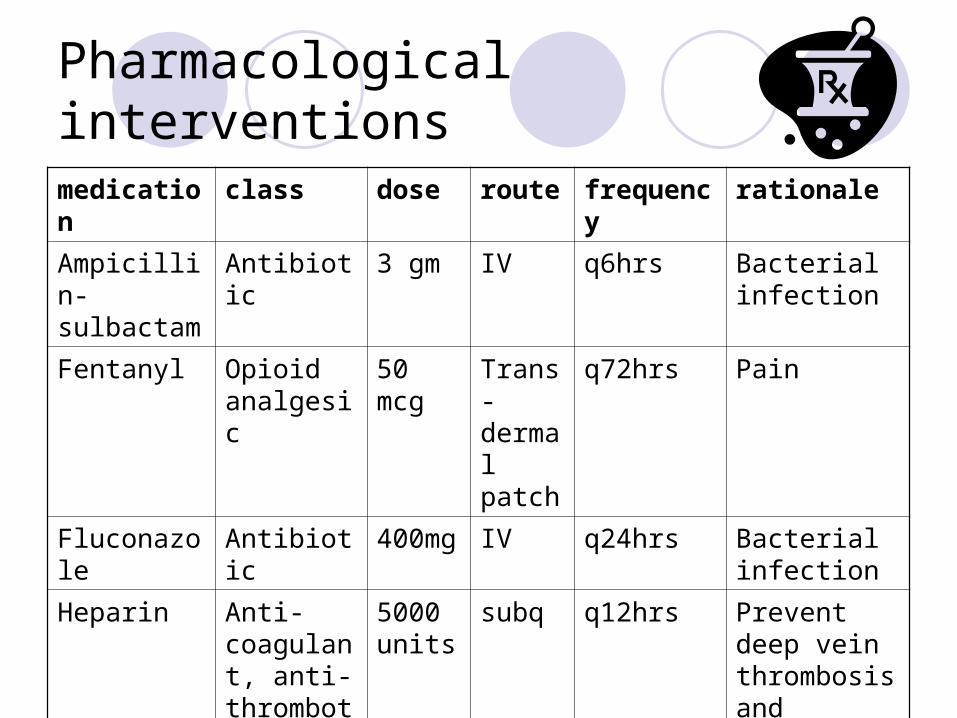
Pharmacological interventions
medication class dose route frequency rationale
Ampicillin-sulbactam
Antibiotic 3 gm IV q6hrs Bacterial infection
Fentanyl Opioid analgesic
50 mcg
Trans-dermal patch
q72hrs Pain
Fluconazole Antibiotic 400mg IV q24hrs Bacterial infection
Heparin Anti-coagulant, anti- thrombotic
5000 units
subq q12hrs Prevent deep vein thrombosis and pulmonary embolism
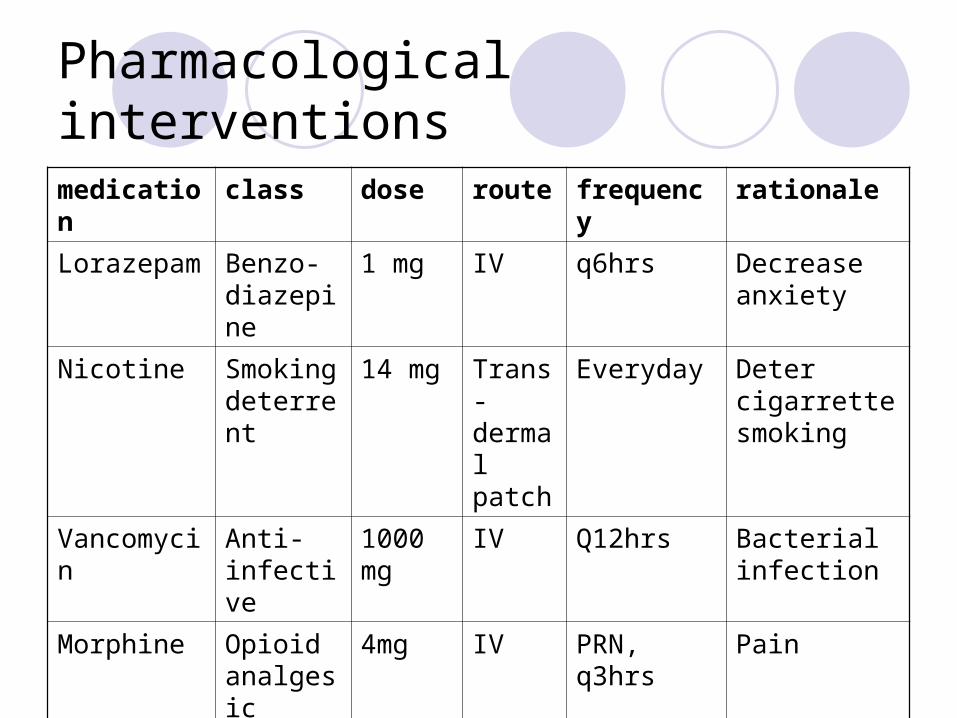
Pharmacological interventions
medication class dose route frequency rationale
Lorazepam Benzo-diazepine
1 mg IV q6hrs Decrease anxiety
Nicotine Smoking deterrent
14 mg Trans- dermal patch
Everyday Deter cigarrette smoking
Vancomycin Anti-infective
1000 mg
IV Q12hrs Bacterial infection
Morphine Opioid analgesic
4mg IV PRN, q3hrs Pain
Insulin regular (Novolin R)
Anti-diabetic
Based on BG
Subq
inj
q4hrs Control blood sugar
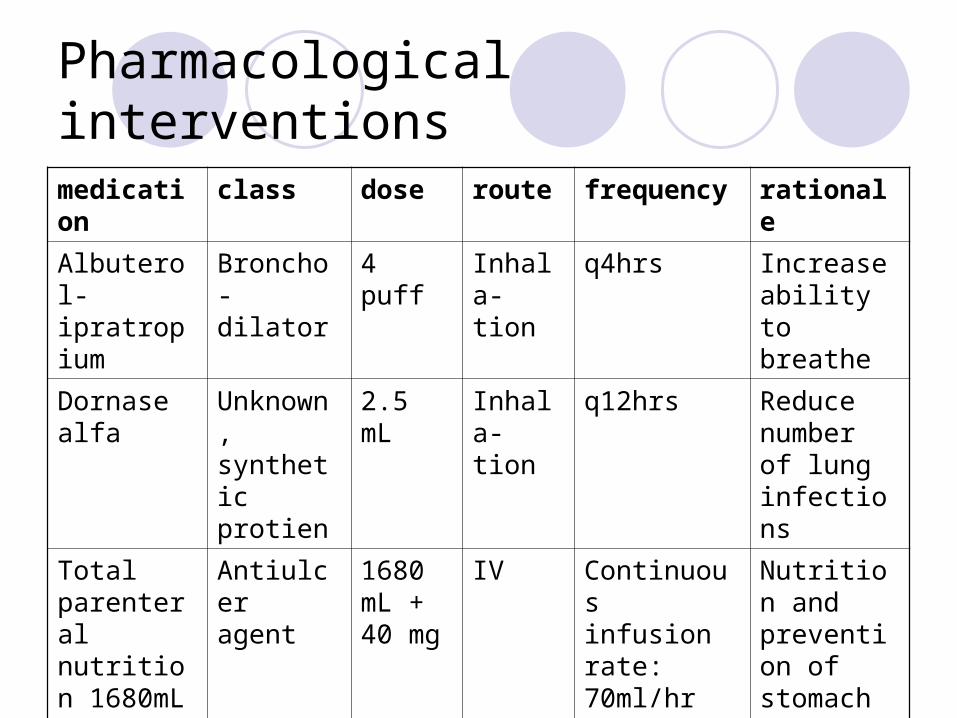
Pharmacological interventions
medication class dose route frequency rationale
Albuterol-ipratropium
Broncho-dilator
4 puff Inhala-tion
q4hrs Increase ability to breathe
Dornase alfa
Unknown, synthetic protien
2.5 mL Inhala-tion
q12hrs Reduce number of lung infections
Total parenteral nutrition 1680mL + famotidine 40 mg
Antiulcer agent
1680 mL + 40 mg
IV Continuous infusion rate: 70ml/hr
Nutrition and prevention of stomach ulcers
Head to Toe Assessment
Neurological Alert and awake Oriented x 3 Pupil reaction equal and brisk
Psychosocial Anxious Agitated as a result of new tracheostomy and
inability to communicate
Head to Toe Assessment
Integumentary Skin pink, dry, warm Nail pink and intact Surgical incision on neck, medial, edges
approximate, steri-strips present, intact, no drainage
Braden skin integrity: score: 18
Head to Toe Assessment
Pulses Jugular vein distention: 3+ (normal) Brachial, radial, and dorsal pedal pulses: 3+ No edema present Capillary refill < 3 seconds
Musculoskeletal Upright posture Generalized weakness in all extremities
Head to Toe Assessment
Respiratory AP diameter: 1:1 Breath sound diminished in all lobes Slight wheezing in upper lobes Tracheostomy collar with 4L oxygen
Cardiovascular NSR with sinus tachycardia No abnormal heart sounds
Head to Toe Assessment
Gastrointestinal Mucous membranes moist, pink, intact with no
lesions present Difficulty swallowing Hypoactive bowel sounds No abdomen distention or tenderness
Urinary Indwelling foley, gravity, intact Concentrated, amber colored urine
Paraphernalia
Nasogastric tube Connected to continuous low suction Bloody drainage
PEG tube Intact gravity
Paraphernalia
PIV access-peripheral intravascular access IV lock Left antecubital No complications No drainage
VAD- vascular access device Triple lumen Peripherally inserted central catheter Right upper arm No complications No drainage
Vital signs
Blood pressure: 118/70Heart rate: 99Temperature: 101.4˚FRespirations: 23SpO2: 95%Pain: 10, chronic, continuous
Nursing diagnosis priority #1
Ineffective airway clearance related to new tracheostomy and endotracheal tube as manifested by decreased ability to cough and thick, bloody secretions.
Goal: The patient will remain an open airway free of secretions, and secretions are easily moved.
Nursing diagnosis priority #1
Interventions Assess for ETT suctioning Watch for harsh breath sounds and audible secretions Suction patient as needed Reposition patient frequently
Outcome The ability to maintain a clear airway will require several
days until the new tracheostomy heals and secretions decrease.
Nursing diagnosis priority #2
Risk of pulmonary infection related artificial airway as manifested by a new tracheostomy and endotracheal tube, and a temperature of 101.4˚F.
Goal: Patient will remain free of infection.
Nursing diagnosis priority #2
Interventions: Monitor temperature q4hrs Monitor color, consistency, and odor of secretions Use sterile technique for suctioning Provide oral care q2hrs Monitor patient for increased breathing effort Administer Ampicillin-sulbactam q6hrs, Fluconazole
q24hrs, and Vancomycin q12hrs Outcome:
Patient remained free of pulmonary infection and a white blood cell count within normal range.
Nursing diagnosis priority #3
Impaired verbal communication related to mute state when the ET tube is in place as manifested by not being able to speak.
Goal: The client will be able to communicate with health team providers in order to have basic needs met.
Nursing diagnosis priority #3
Interventions: Keep a pencil and paper readily available Be patient and willing to spend time
communicating
Evaluation: Patient was able to write down feelings and communicate to the healthcare team. Her anxiety and frustration was decreased.
Nursing research
Tracheal Suctioning of Adults with an Artificial Airway
Evidence based practice including the effects of suctioning, suctioning techniques, oxygenation, suctioning patient subgroups, summary of evidence, and recommendations
Participants were adult patients (>15 years) in the acute care setting with an endotracheal tube or tracheostomy tube
Nursing research
Purpose Review suction interventions that are currently
employed in the nursing management of patients with an artificial airway
Results Suctioning is a potentially harmful procedure
and should only be done when a thorough assessment of the patient established the need for such a procedure
References
Emedicine by WebMD.(2008). Recurrent Respiratory Papillomatosis. Retrieved February 11, 2008, from http://www.emedicine.com/med/topic2535.htm
Ignatavivius, D.D. & Workman, M.L.(2006). Medical-Surgical nursing: Critical Thinking for Collaborative care.(5th ed.) Vol. I. Philadelphia, PA: W.B. Saunders.
Thompson, L.(2000). Tracheal Suctioning of Adults with an Artificial Airway. Johanna Briggs Institute for Evidence Based Nursing and Midwifery Vol. 4(4). Australia: Blackwell Science-Asia.
Sole, M.L., Klein, D.G., & Moseley, M.J.(2005). Introduction to Critical Care Nursing.(4th ed.) St. Louis, MO: Elsevier Saunders.