Embed Size (px)
Citation preview
5.14.13
GRAND ROUNDS
CASE
64 y.o AAF with h/o HTN, DM, HLD , MGUS referred by PMD for uncontrolled resistant hypertension, new renal failure (Cr of 1.5), hematuria and proteinuria • Per patient systolic BP in last 3 months in the range of 200s to 250s requiring
multiple antihypertensives • LE swelling for last 3 months • Periorbital swelling and facial puffiness on waking up • Decrease exercise tolerance, DOE, orthopnea, fatigue • Noted urine to be frothy but denied increased frequency and hematuria ROS: Negative for fever, chills, chest pain, cough, headache, blurry vision, arthralgias, myalgias, rash, recent infections
PMHx
• HTN
• DM
• HLD
• MGUS( dx in 2011)
Meds: ASA 81 mg, Losartan 100 mg daily, Chlorthalidone 25 mg daily, Simvastatin 80 mg daily, Atenolol 75 mg daily
FHx: HTN and DM
SHx: Denies smoking or recreational drug use. Occassional Etoh
PE: VS: 194/85 HR 83 RR 20 T 97.7 So2 99% HEENT: pale conjunctiva, sclera anicteric, periorbital edema Lungs: L left basilar rales Heart: RRR, normal S1S2 Abd: soft, nt, nd, bs+ve LE: 2+ pitting edema up to knees b/l Skin: no rashes
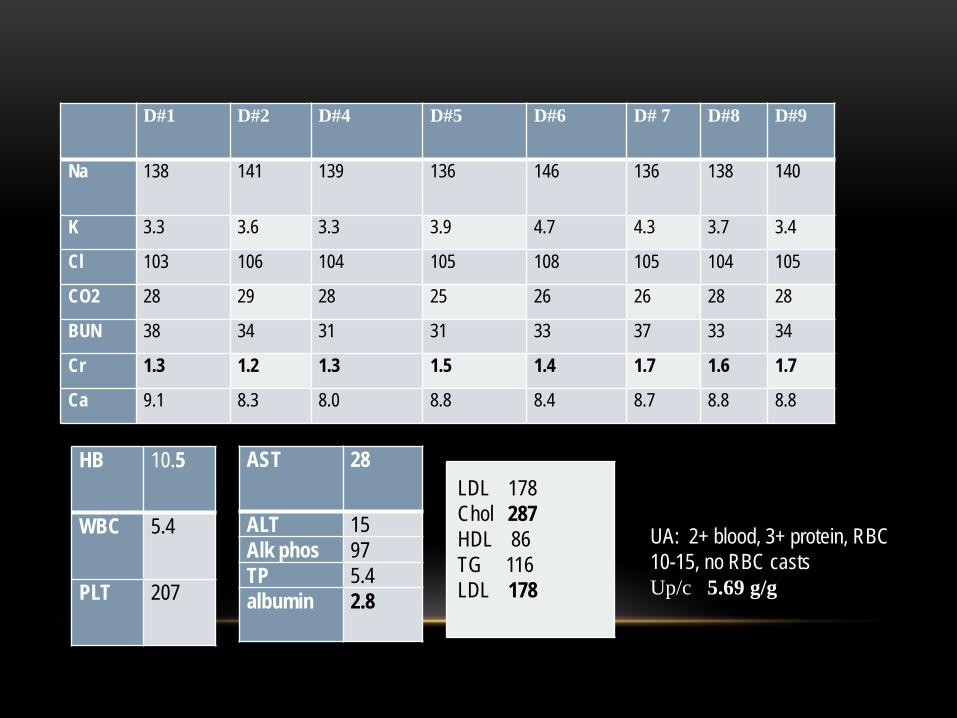
D#1 D#2 D#4 D#5 D#6 D# 7 D#8 D#9
Na 138 141 139 136 146 136 138 140
K 3.3 3.6 3.3 3.9 4.7 4.3 3.7 3.4
Cl 103 106 104 105 108 105 104 105
CO2 28 29 28 25 26 26 28 28
BUN 38 34 31 31 33 37 33 34
Cr 1.3 1.2 1.3 1.5 1.4 1.7 1.6 1.7
Ca 9.1 8.3 8.0 8.8 8.4 8.7 8.8 8.8
UA: 2+ blood, 3+ protein, RBC 10-15, no RBC casts Up/c 5.69 g/g
AST 28
ALT 15 Alk phos 97 TP 5.4 albumin 2.8
HB 10.5
WBC 5.4
PLT 207
LDL 178 Chol 287 HDL 86 TG 116 LDL 178
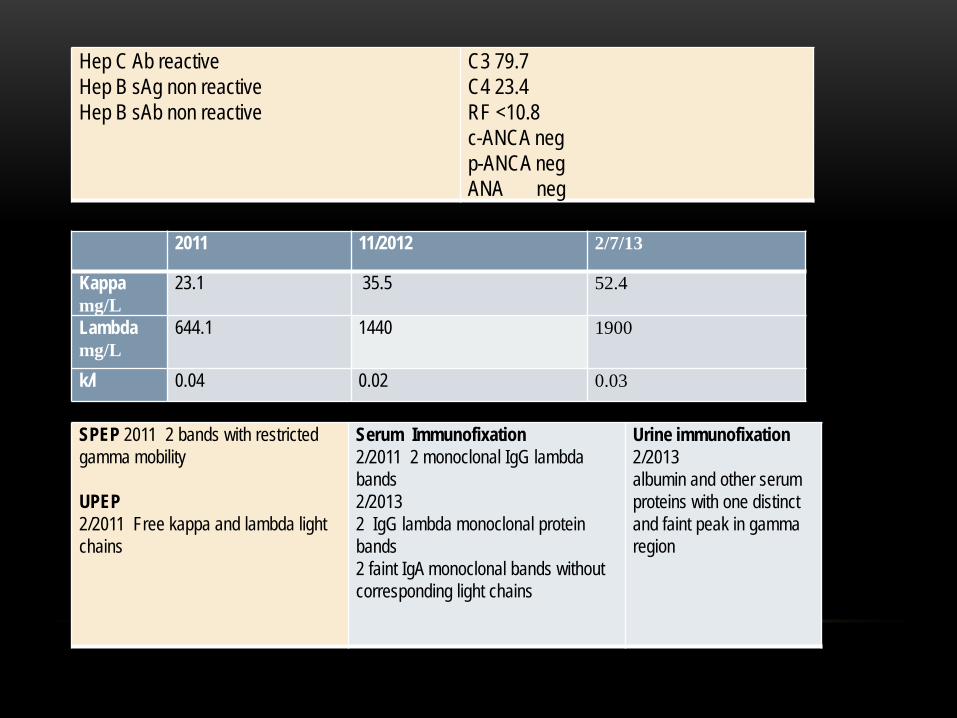
SPEP 2011 2 bands with restricted gamma mobility UPEP 2/2011 Free kappa and lambda light chains
Serum Immunofixation 2/2011 2 monoclonal IgG lambda bands 2/2013 2 IgG lambda monoclonal protein bands 2 faint IgA monoclonal bands without corresponding light chains
Urine immunofixation 2/2013 albumin and other serum proteins with one distinct and faint peak in gamma region
Hep C Ab reactive Hep B sAg non reactive Hep B sAb non reactive
C3 79.7 C4 23.4 RF <10.8 c-ANCA neg p-ANCA neg ANA neg
2011 11/2012 2/7/13
Kappa mg/L
23.1 35.5 52.4
Lambda mg/L
644.1 1440 1900
k/l 0.04 0.02 0.03
Renal Ultrasound • Right kidney 9.9 cm left kidney 10.2 cm • Increased echogenicity • Few right renal cysts the largest 15 x11 mm in the mid pole • There is no hydronephrosis or calculi
• CXR: cardiomegaly, no effusions • 2 D echo: Concentric LVH ef 65%, impaired relaxation pattern, small
pericardial effusion, epicardial thickening
DIFFERENTIAL DIAGNOSIS Nephrotic syndrome, hypertension, renal insufficiency
FSGS
Amyloidosis
MIDD
MPGN
Thrombotic microangiopathy
IF
- 3 glomeruli with nodular sclerosis
- There is linear GBM, bowmans capsule and tubular BM staining for lambda
EM
- 2 glomeruli with nodular sclerosis
- GBM within normal thickness
-No subepithelial or sub endothelial immune complex deposits
-Near complete foot process effacement
-Marked increase in mesangial matrix in a nodular pattern
-Tubular basements ate thickened and show focal
-No evidence of amyloid fibrils
RENAL BIOPSY • Diagnosis: Light Chain deposition disease
LM: 4/38 glomeruli globally sclerotic
-Diffuse, moderate to marked increase increase in mesangial matrix and cellularity in a nodular pattern
-Glomeruli show lobular pattern
-GBM appear irregular with focal corrugation and splitting
-There is endocapillary hypercellularity
-Arterioles show mild hyalinosis, Interlobular arteries show very mild intimal fibrosis
-Congo red stain for amyloid negative
LIGHT CHAIN DEPOSITION DISEASE • LCDD is one manifestation of monoclonal immunoglobulin deposition disease in the
kidney, first reported in 1973 and confirmed by Randall et al who published in 1976 the first description of LCDD
• The incidence of LCDD in patients with plasma cell dyscrasia is approximately 5%
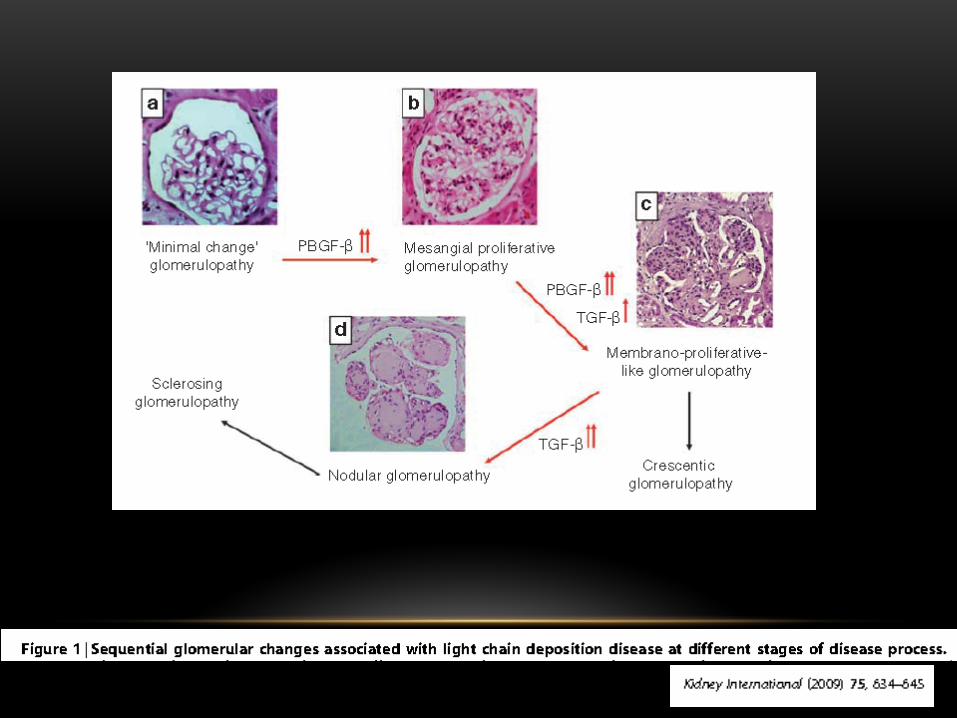
• Nodular glomerulosclerosis is the classical lesion in LCDD
• Mesangial nodularity results from increased deposition of extracellular matrix proteins and monotypic light chains most commonly kappa
• Deposits are neither fibrillar nor congo red positive
• Ultrastructurally deposits are seen as punctate granular electron dense material, which is typically present in subendothelial glomerular areas and in the mesangium.
CLINICAL FEATURES OF LCDD • MIDD most often occur in the sixth and seventh decades of life, but patients in 20s and
90s have been reported
• Renal involvement is a constant feature and renal failure often dominate the clinical presentation
• Nephrotic syndrome in 30-50% of cases
• proteinuria <1 g/day in 25%
• Hematuria 29- 67%
• Hypertension is variable
• 60% of cases progress to ESRD
J Am Soc Nephrol 12: 1558–1565, 2001
… • Extrarenal manifestations- Liver and cardiac involvement are the most common
• Hepatomegaly with mild alterations in LFT’s are the most usual presentation, but several patients develop hepatic insufficiency and portal hypertension, and of them die of hepatic failure
• Cardiac manifestations include restrictive cardiomyopathy and MI from light chain deposition in the coronary vasculature
• Other manifestations include cerebral infarction and hemorrhage, peripheral neuropathy and mononeuritis muliplex. Adrenal insufficiency has also been reported
J Am Soc Nephrol 12: 1558–1565, 2001
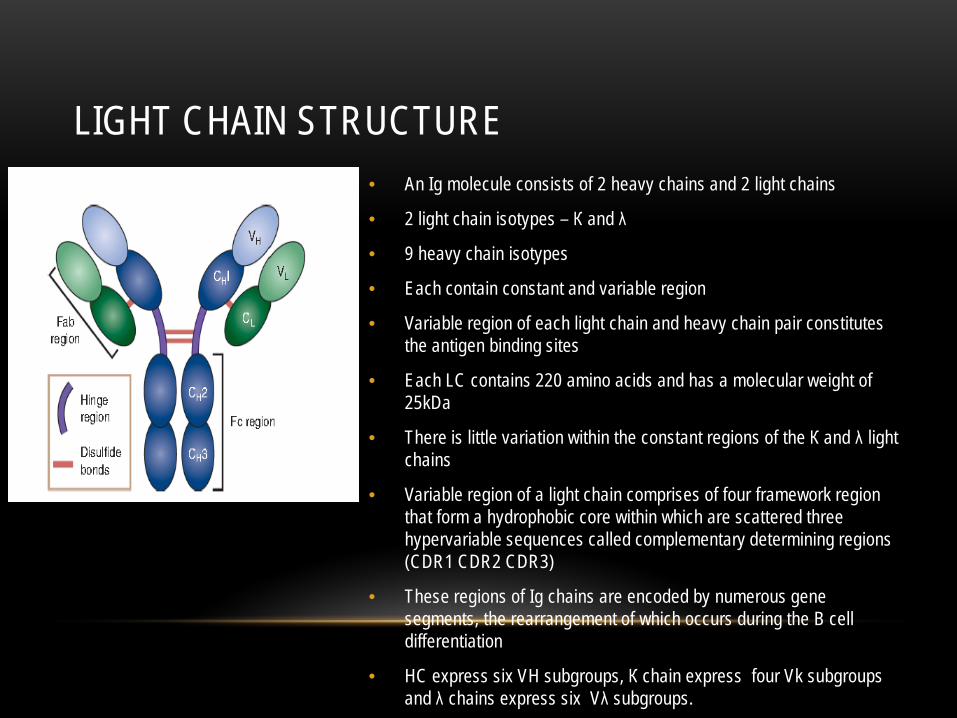
LIGHT CHAIN STRUCTURE • An Ig molecule consists of 2 heavy chains and 2 light chains
• 2 light chain isotypes – К and λ
• 9 heavy chain isotypes
• Each contain constant and variable region
• Variable region of each light chain and heavy chain pair constitutes the antigen binding sites
• Each LC contains 220 amino acids and has a molecular weight of 25kDa
• There is little variation within the constant regions of the К and λ light chains
• Variable region of a light chain comprises of four framework region that form a hydrophobic core within which are scattered three hypervariable sequences called complementary determining regions (CDR1 CDR2 CDR3)
• These regions of Ig chains are encoded by numerous gene segments, the rearrangement of which occurs during the B cell differentiation
• HC express six VH subgroups, К chain express four Vk subgroups and λ chains express six Vλ subgroups.
LIGHT CHAIN PRODUCTION, DISTRIBUTION AND RENAL HANDLING • Approximately 500 mg of free light chains is produced by the normal
lymphoid system • 80% of FLC is extravascular • Two thirds of light chain production is kappa ( К/λ 1.8:1) • Light chains are filtered and catabolized by the kidney in proximal tubule,
such that only approximately 1 to 10 mg of polyclonal light chains normally appear in the urine
• Internalization in PTECs occurs through rapid and saturable megalin and cubilin receptor mediated endocytosis in clathrin coated pits
WHY DO SOME CLONAL FLC CAUSE KIDNEY INJURY • FLCs isolated from patients with PCD and renal injury have a greater potential to self
aggregate and form higher molecular weight aggregates under physiological conditions than FLCs from patients with PCD but without kidney injury
• Mice injected with FLCs from patients with renal lesions developed similar renal lesions to the patients indicating that specific clones of FLCs cause distinct transferrable patterns of injury
• In LCDD, Kappa light chains occur in approximately 80% of cases.
• VКIV variability subgroup was overrepresented in patients with LCDD. This subgroup features a longer CDR1 loop that contains some hydrophobic residues
• Data in this study support a single receptor present on mesangial cells for both LCDD and AL-LCs
• This receptor resides in the caveolae present on the plasma membrane of HMCs and is overexpressed when HMCs are incubated with G-LCs not tubulopathic LCs
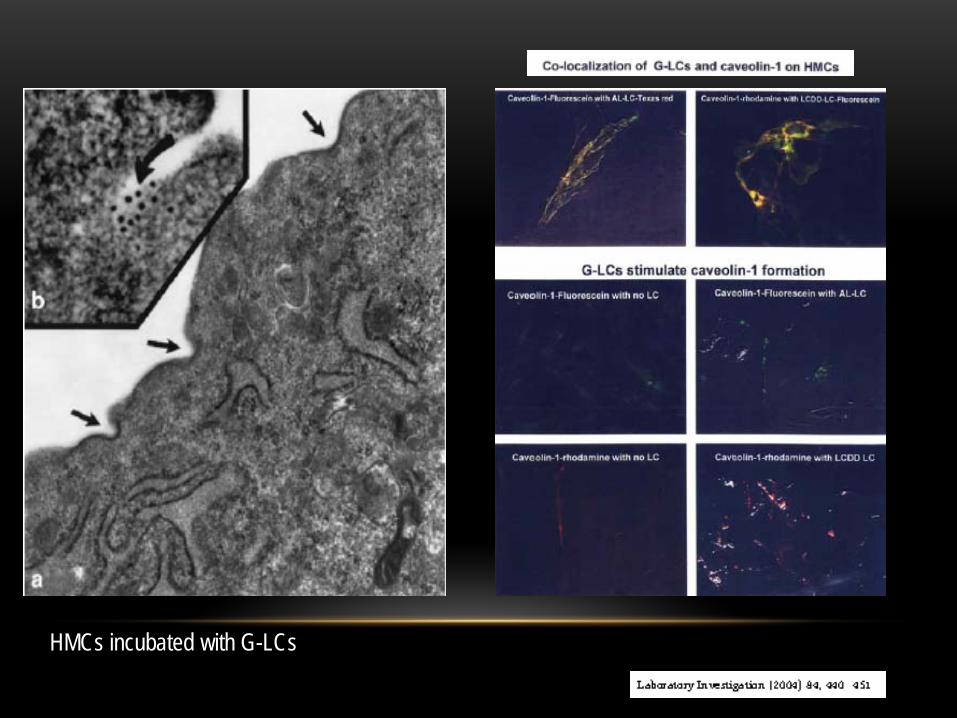
HMCs incubated with G-LCs
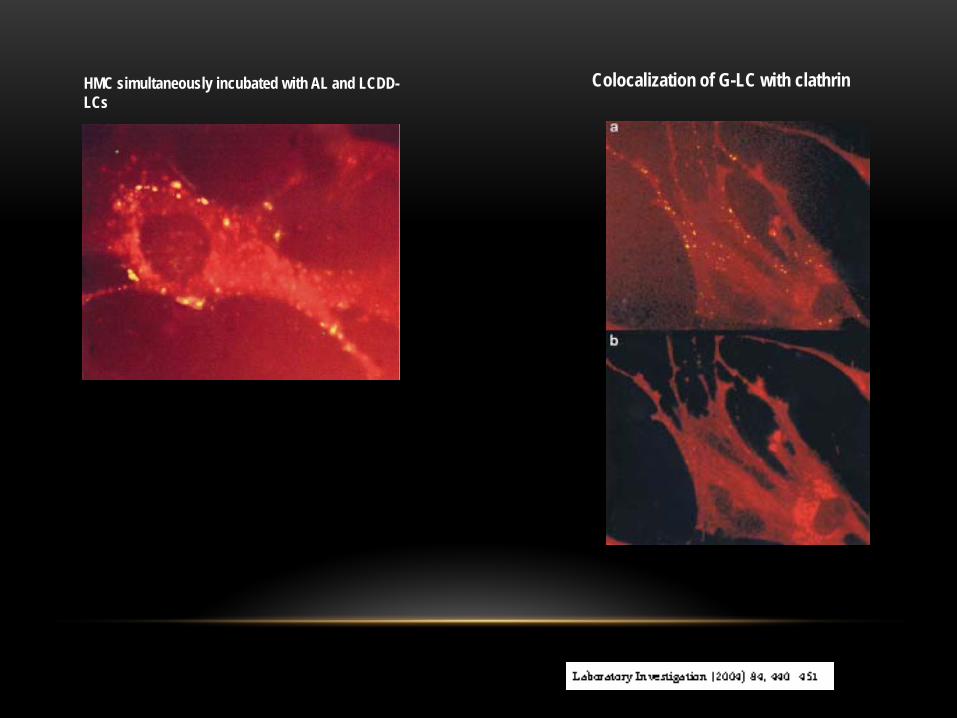
HMC simultaneously incubated with AL and LCDD-LCs
Colocalization of G-LC with clathrin
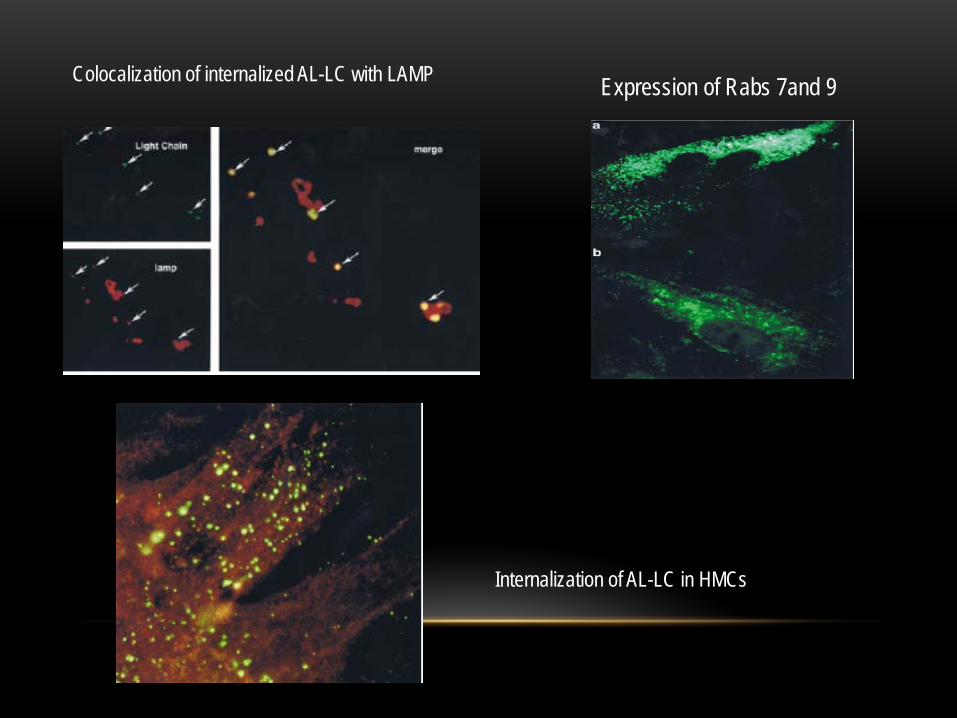
Colocalization of internalized AL-LC with LAMP Expression of Rabs 7and 9
Internalization of AL-LC in HMCs
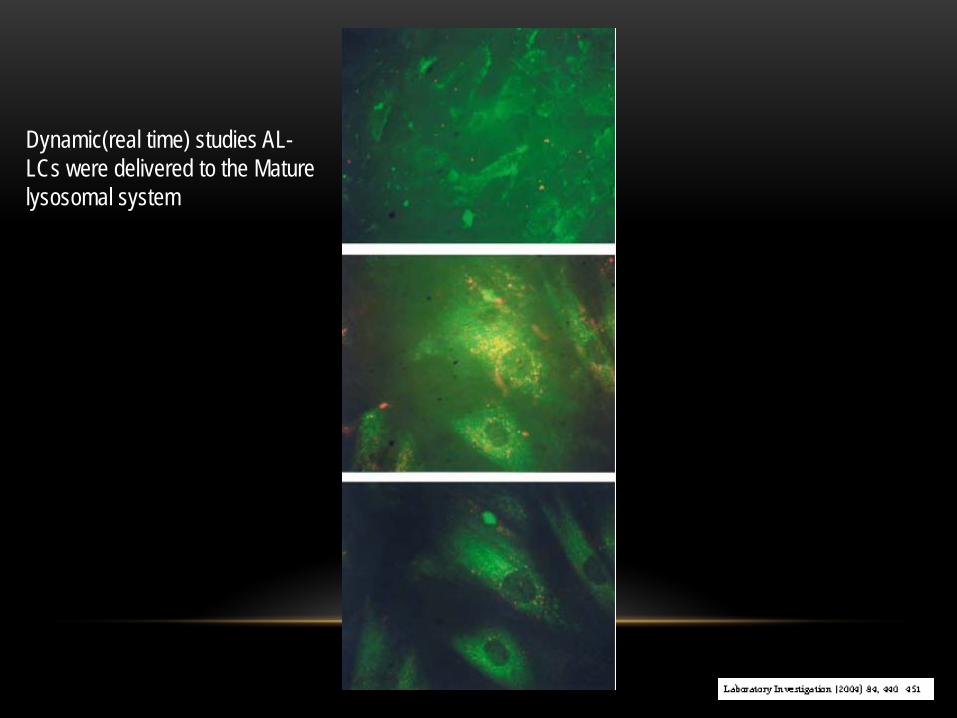
Dynamic(real time) studies AL-LCs were delivered to the Mature lysosomal system
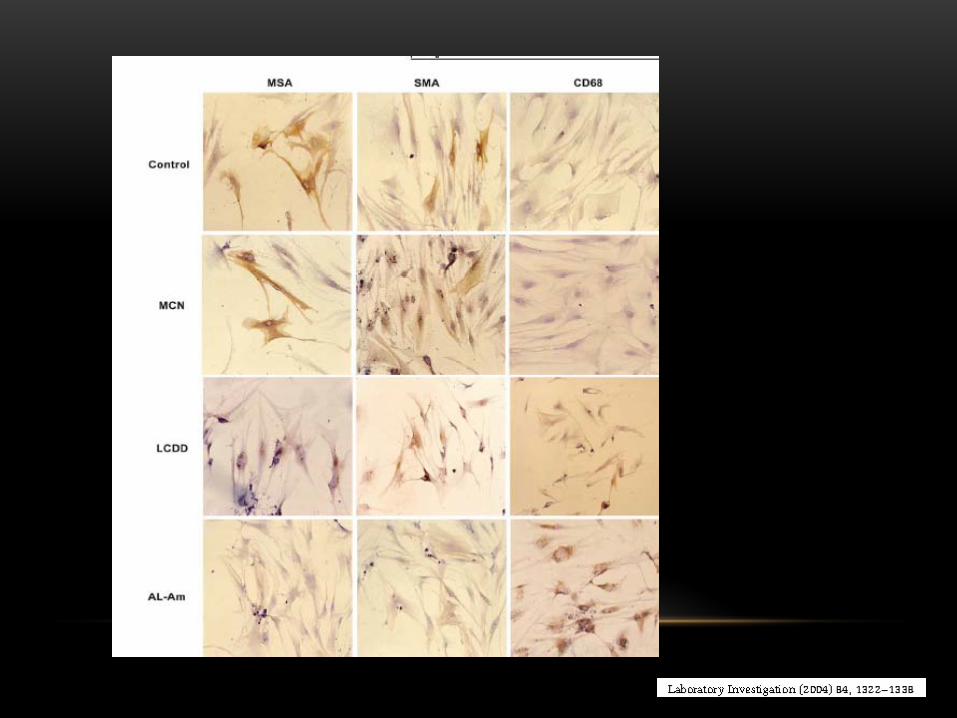
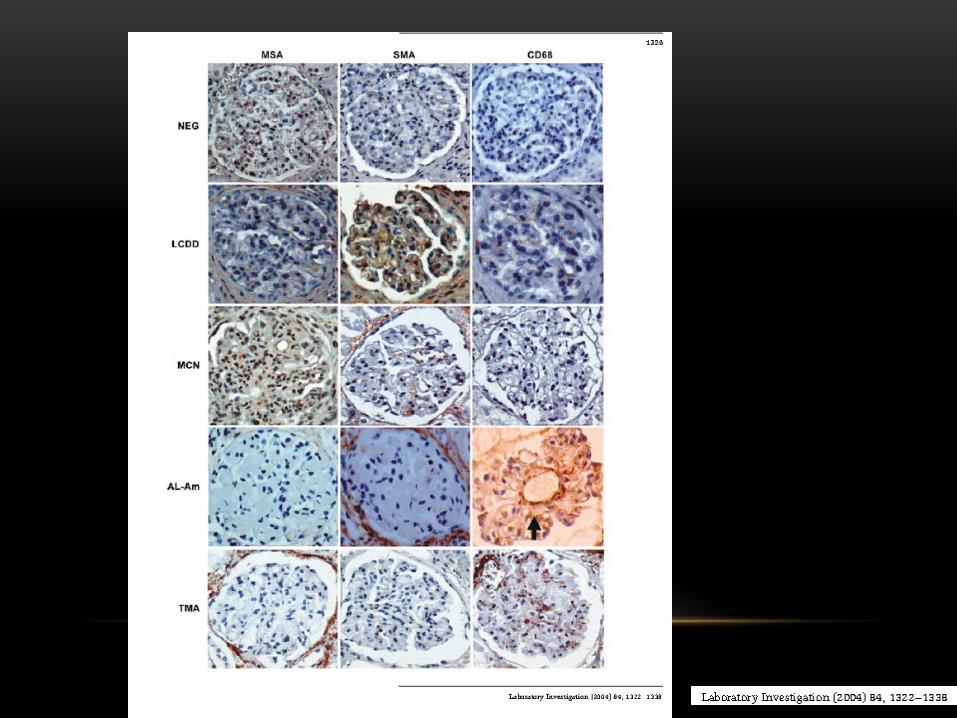
• HMCs are injured by abnormal light chains with plasma cell dyscrasia.
• Consequently these mesangial cells undergo phenotypic transformation
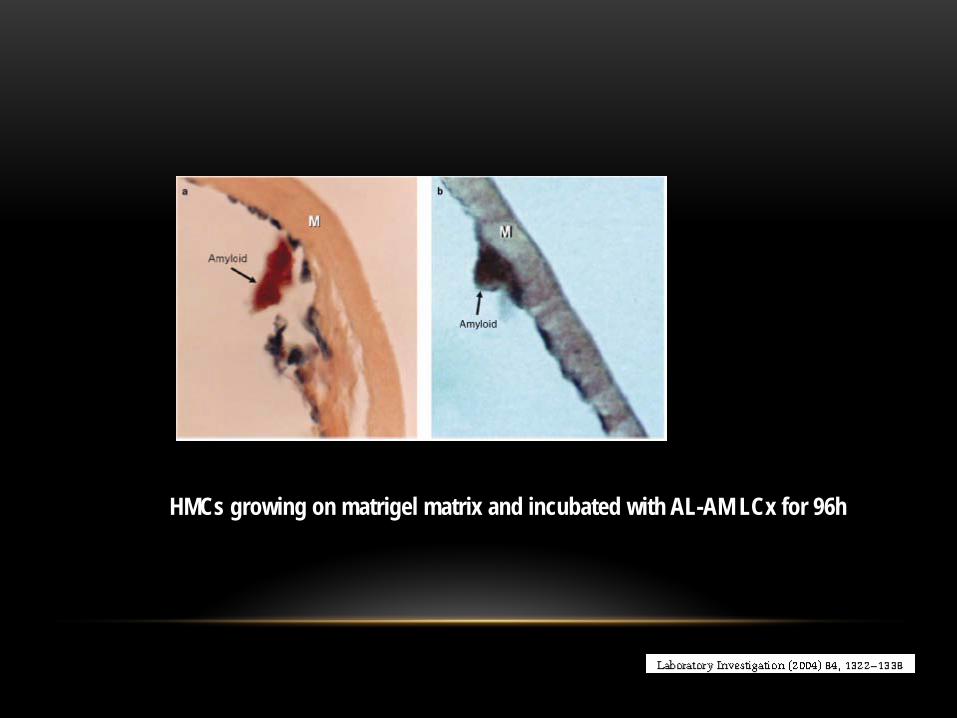
HMCs growing on matrigel matrix and incubated with AL-AM LCx for 96h
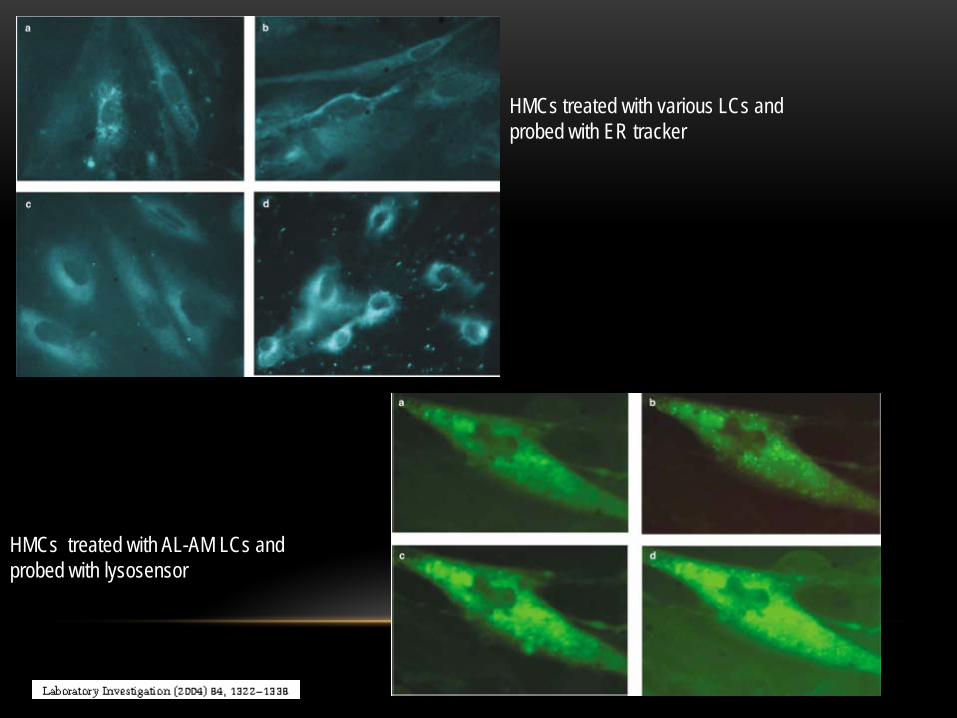
HMCs treated with various LCs and probed with ER tracker
HMCs treated with AL-AM LCs and probed with lysosensor
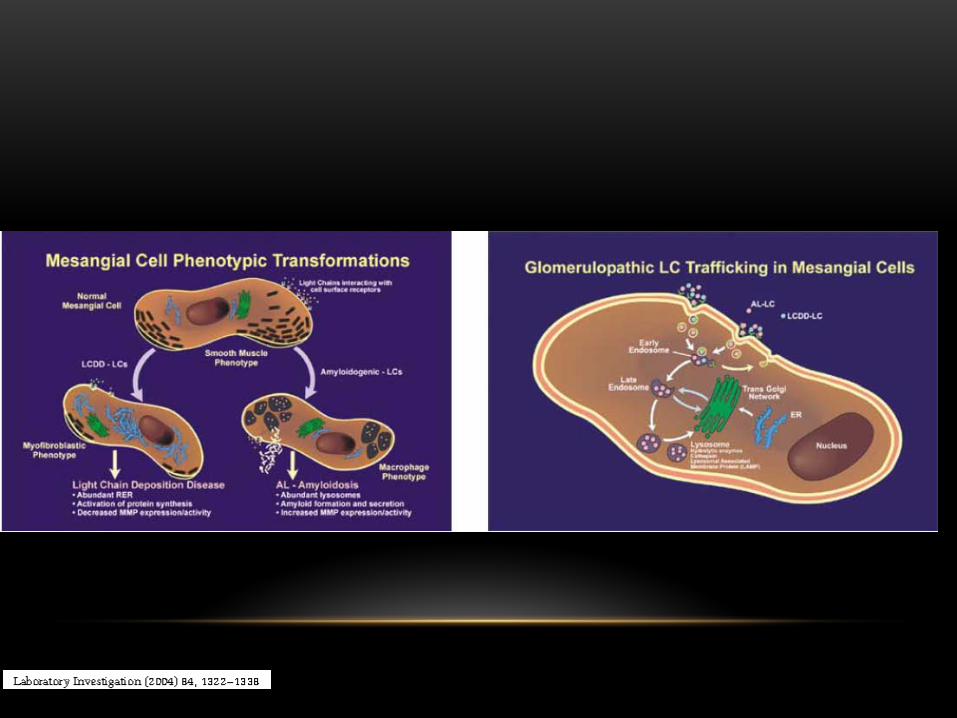


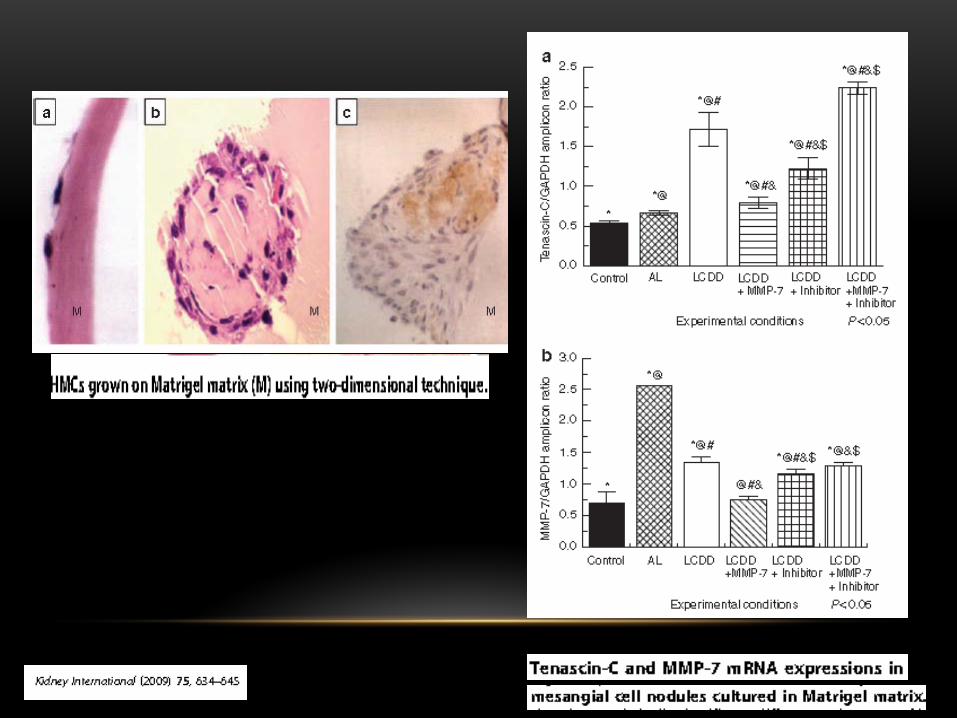
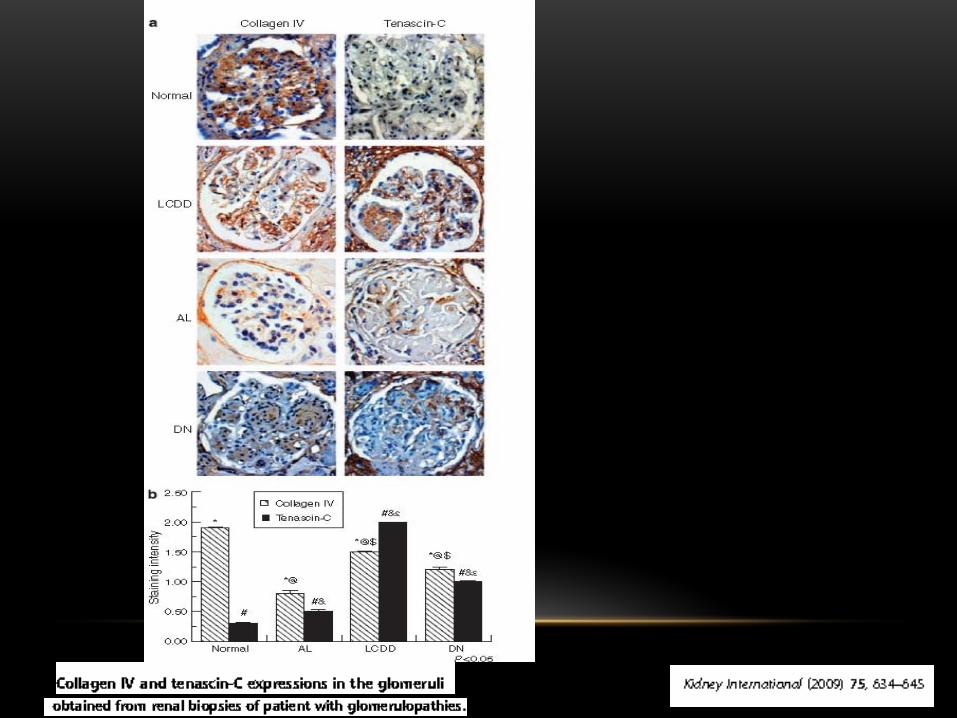
• Nodular glomerulosclerosis results from increased deposition of extracellular matrix proteins and monotypic light chains
• Inability of mesangial cells to degrade abnormal levels of Tenascin C-along with increased expression of some growth factors such as PDGF and TGF-ß is crucial to the pathogenesis of LCDD
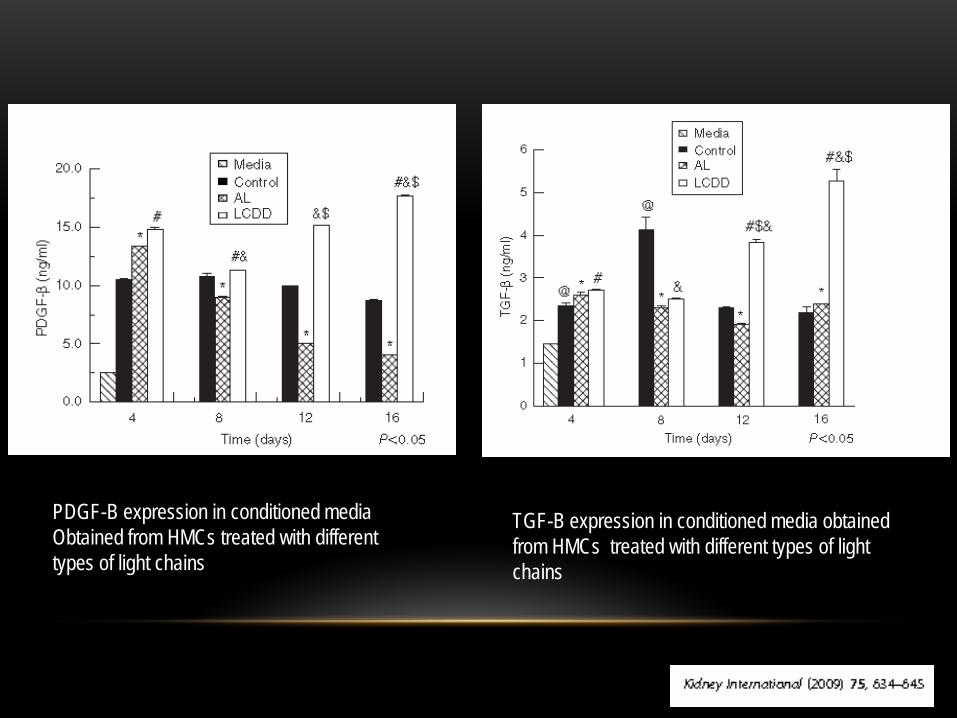
PDGF-B expression in conditioned media Obtained from HMCs treated with different types of light chains
TGF-B expression in conditioned media obtained from HMCs treated with different types of light chains
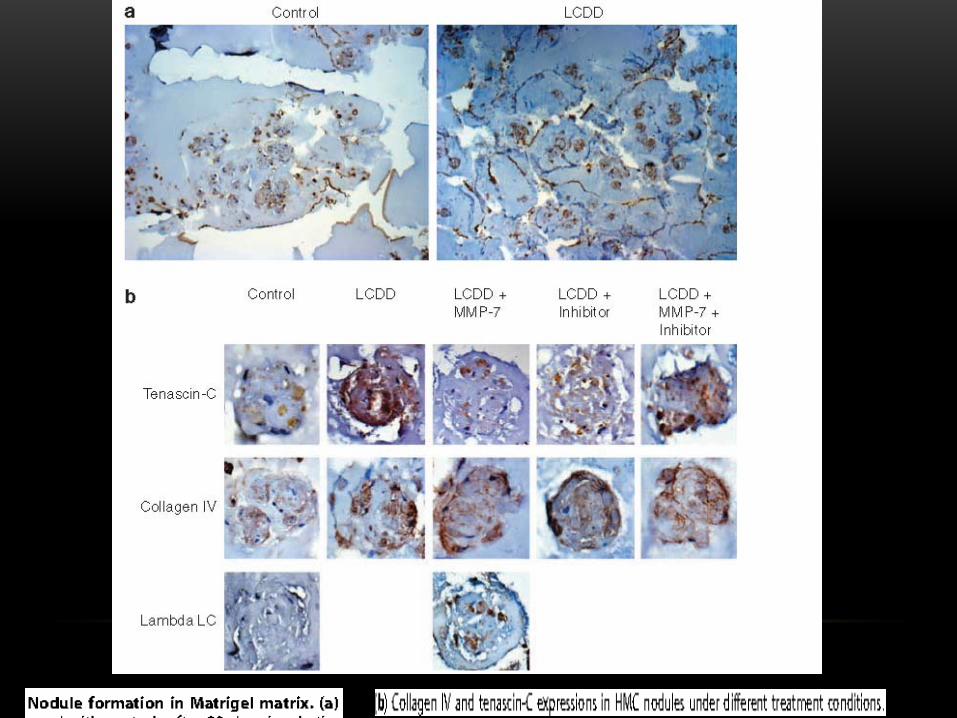
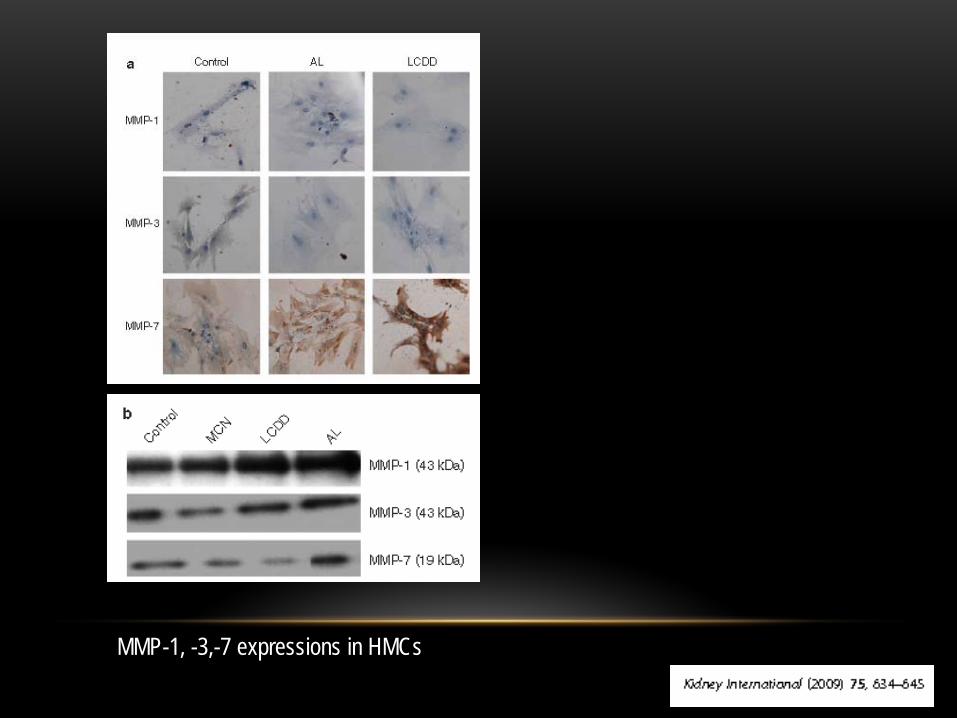
MMP-1, -3,-7 expressions in HMCs