Embed Size (px)
DESCRIPTION
Grand Rounds. Joseph Reck VAMC Wilkes-Barre, PA November 3, 2006. Clinical Presentation. Seen in Texas six weeks ago; GAT- 54 Current Medications: Diamox 500mg b.id.; ran out 5d ago Cosopt b.id. Atropine b.id. Brimonidine b. id. Ocular history: - PowerPoint PPT Presentation
Citation preview
Grand RoundsGrand Rounds
Joseph Reck
VAMC Wilkes-Barre, PA
November 3, 2006
Clinical PresentationClinical Presentation
Seen in Texas six weeks ago; GAT- 54Seen in Texas six weeks ago; GAT- 54 Current Medications:Current Medications:
– Diamox 500mg b.id.; ran out 5d agoDiamox 500mg b.id.; ran out 5d ago– Cosopt b.id.Cosopt b.id.– Atropine b.id.Atropine b.id.– Brimonidine b. id.Brimonidine b. id.
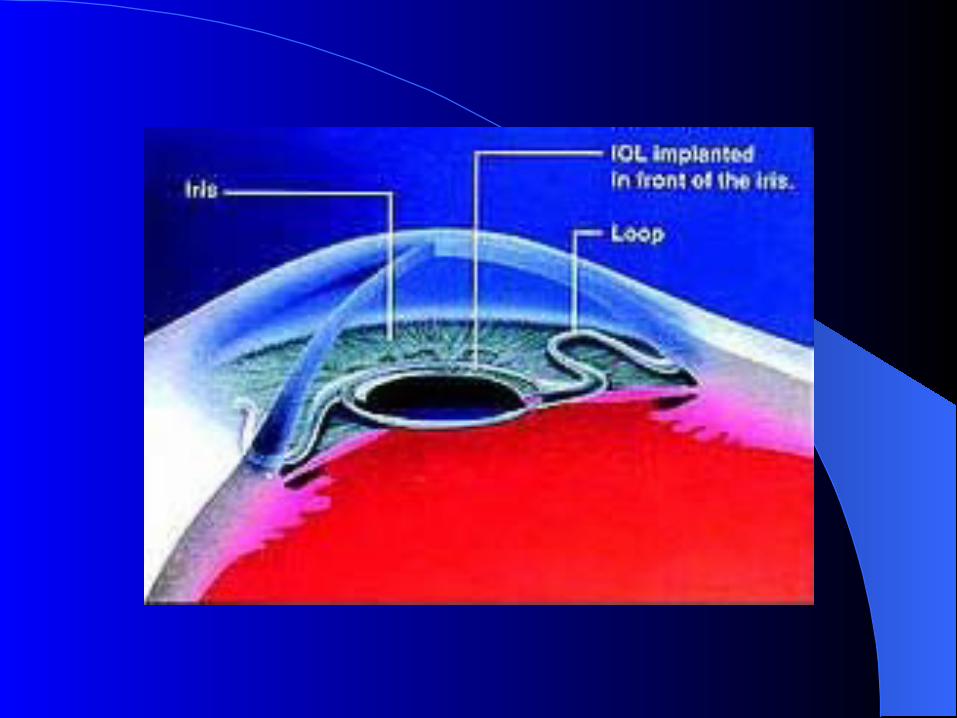
Ocular history:Ocular history:– Cataract extraction without implantation, 1983.Cataract extraction without implantation, 1983.– Anterior chamber IOL implantation, 1987.Anterior chamber IOL implantation, 1987.
Acuity and ExternalsAcuity and Externals
VA cc: O.D. 20/60, PH 20/40VA cc: O.D. 20/60, PH 20/40
O.S. 20/20O.S. 20/20
Pupils: O.D. pharm fixed; O.S. RRL –APDPupils: O.D. pharm fixed; O.S. RRL –APD EOM: Full and smooth, O.U.EOM: Full and smooth, O.U. Confrontation fields; Full, O.U.Confrontation fields; Full, O.U.
Clinical FindingsClinical Findings
Slit Lamp Exam:Slit Lamp Exam:– 1+ injection.1+ injection.– Diffuse microcysts and SPK.Diffuse microcysts and SPK.– 1+ AC Reaction.1+ AC Reaction.– Iris atrophy with exposed iris vessels near Iris atrophy with exposed iris vessels near
ACIOL haptic foot.ACIOL haptic foot.
TonometryTonometry
O.D. - O.D. - 5252 O.S.- O.S.- 1313
Uveitic GlaucomaUveitic Glaucoma
Unilateral, red eye.Unilateral, red eye.Pain and photosensitivity.Pain and photosensitivity.Corneal edema.Corneal edema.AC reaction.AC reaction.Increased IOP.Increased IOP.
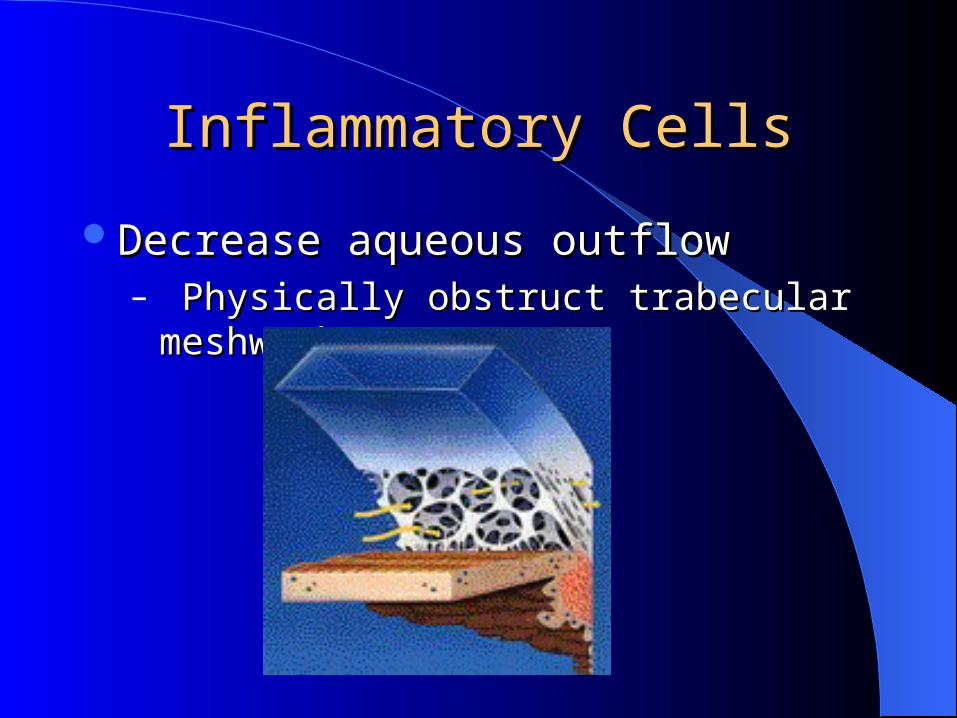
Inflammatory CellsInflammatory Cells
Decrease aqueous outflowDecrease aqueous outflow– Physically obstruct trabecular meshwork.Physically obstruct trabecular meshwork.
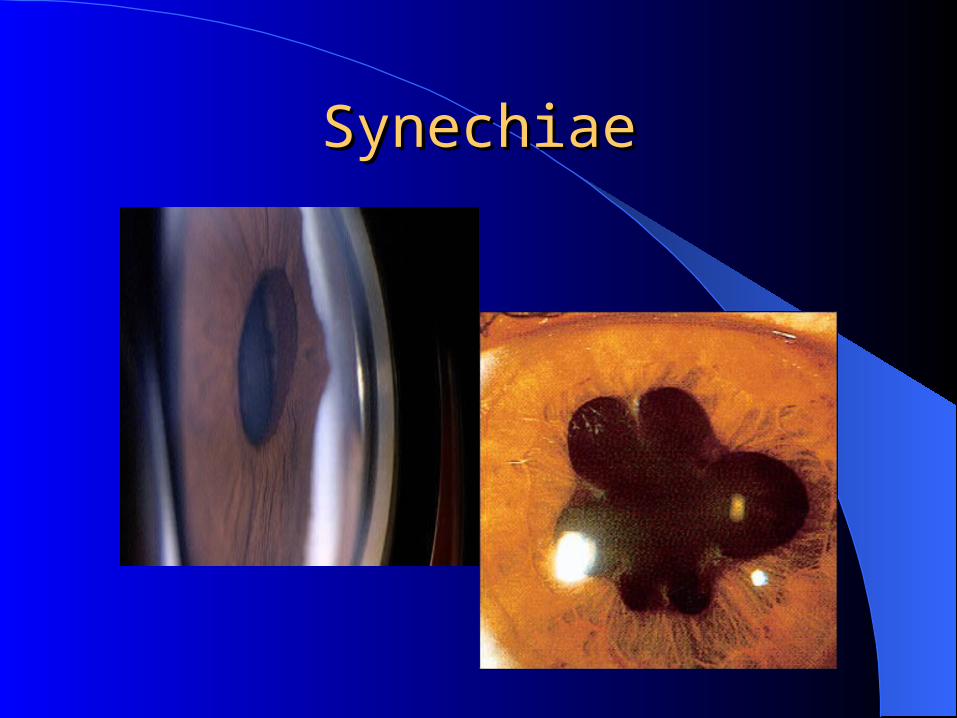
SynechiaeSynechiae
Inflammation, then PressureInflammation, then Pressure
Topical steroid.Topical steroid.– Pred Forte q15min; Pred Forte q15min;
then taper.then taper.
Strong cycloplegia.Strong cycloplegia.– Atropine 1% b.id.Atropine 1% b.id.
Break synechiae.Break synechiae.– Phenylephrine 10%.Phenylephrine 10%.
Beta-blockerBeta-blocker
Alpha-agonistAlpha-agonist
CAICAI
Avoid Prostaglandins.Avoid Prostaglandins.
Assessment/Plan:Assessment/Plan:
Lotemax q2hLotemax q2hAtropine t.id.Atropine t.id.Cosopt b.id.Cosopt b.id.Diamox 500mg, b.id.Diamox 500mg, b.id.
Follow-up in 1 week.Follow-up in 1 week.
One Week Follow-UpOne Week Follow-Up
VA cc: O.D. 20/100, PH 20/40VA cc: O.D. 20/100, PH 20/40
O.S. 20/20O.S. 20/20
GAT: O.D. 52, O.S. 12GAT: O.D. 52, O.S. 121+ AC Reaction1+ AC Reaction
Updated Treatment PlanUpdated Treatment Plan
Continue meds as scheduled.Continue meds as scheduled.– Add Alphagan t.id.Add Alphagan t.id.
Run full uveitis work-up.Run full uveitis work-up.
Follow-up next day.Follow-up next day.
Return VisitReturn Visit
Patient experiencing some pain.Patient experiencing some pain.VA cc: O.D. 20/80, ph 20/30VA cc: O.D. 20/80, ph 20/30
O.S. 20/20O.S. 20/20
GAT: O.D. 55, O.S. 11.GAT: O.D. 55, O.S. 11.1+ AC reaction.1+ AC reaction.
DifferentialDifferential
Unilateral increase in IOPUnilateral increase in IOP Steroid responseSteroid response PASPAS EndopthalmitisEndopthalmitis Chronic inflammationChronic inflammation Retained lens materialRetained lens material
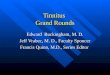
GonioscopyGonioscopy
Lens position in iris; not angleLens position in iris; not angle Small areas of synechiae.Small areas of synechiae. Small areas of bleeding.Small areas of bleeding. Peripheral rubeosis, superiorly.Peripheral rubeosis, superiorly. Dilated iris tissue rolled into angle. Dilated iris tissue rolled into angle. ACIOL haptics appear to have pushed peripheral ACIOL haptics appear to have pushed peripheral
iris directly into angleiris directly into angle
Discontinue Atropine.Discontinue Atropine.
UUVEITISVEITIS
GGLAUCOMALAUCOMA
HHYPHEMAYPHEMA
UGH SyndromeUGH Syndrome
Inflammation after anterior chamber IOL Inflammation after anterior chamber IOL implantation, caused by the haptics of the implantation, caused by the haptics of the IOL. IOL.
Misplaced or misdirected haptics from the Misplaced or misdirected haptics from the anterior chamber IOL erode the tissues of anterior chamber IOL erode the tissues of the angle, causing bleeding and the angle, causing bleeding and inflammation. inflammation.
UGH SyndromeUGH Syndrome
– Excessive lens movementExcessive lens movementSmall sizeSmall sizeDecentration or dislocationDecentration or dislocation
– Poorly manufactured edgesPoorly manufactured edges– Iris-clipped IOLIris-clipped IOL– Rigid, closed loop hapticsRigid, closed loop haptics
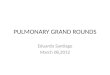
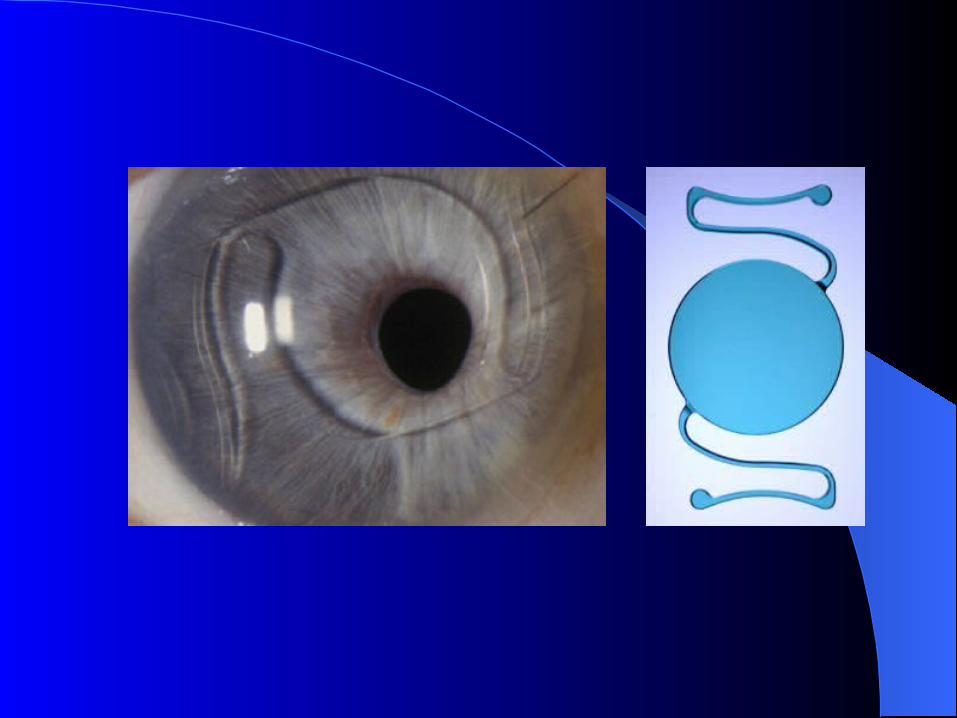
Open v. Closed LoopOpen v. Closed Loop
Open Loop IOLOpen Loop IOL-good finish/polish-good finish/polish
-easy to size-easy to size
-less area of contact-less area of contact
Closed Loop IOL Closed Loop IOL -difficult to fit-difficult to fit
-erosion chaffing-erosion chaffing
-large contact zone-large contact zone
-poorly finished/ sharp -poorly finished/ sharp edgesedges
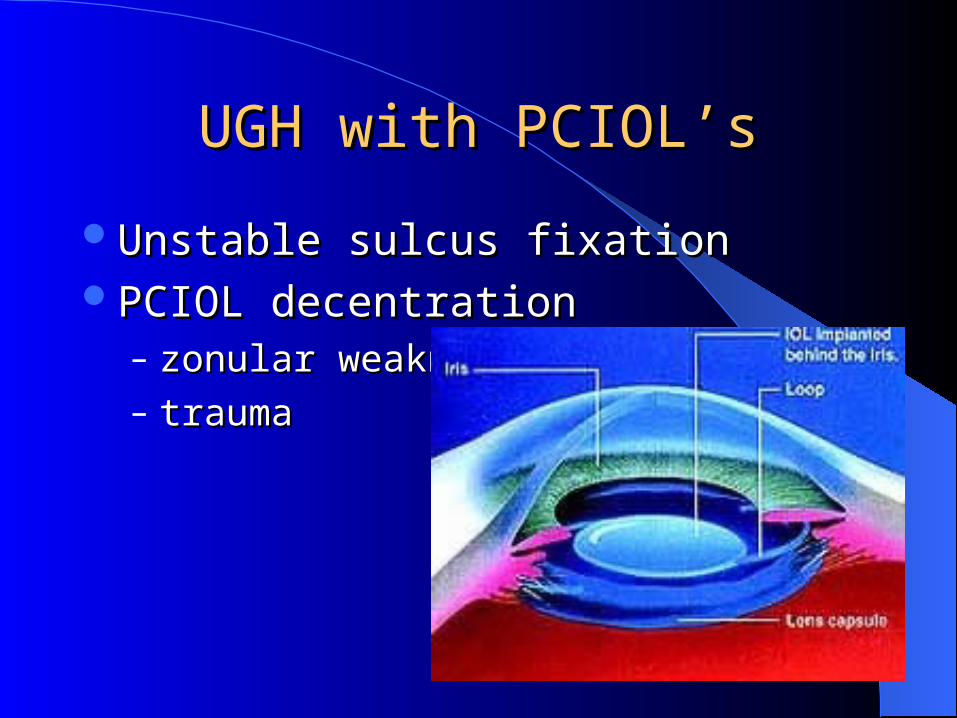
UGH with PCIOL’sUGH with PCIOL’s
Unstable sulcus fixationUnstable sulcus fixationPCIOL decentrationPCIOL decentration
– zonular weaknesszonular weakness– trauma trauma
UGH Etiology; UveitisUGH Etiology; Uveitis Activation of innate immunity.Activation of innate immunity. TheoriesTheories
– Cytokine and eicosanoid synthesis triggered by Cytokine and eicosanoid synthesis triggered by mechanical excoriation of the angle or iris by the mechanical excoriation of the angle or iris by the haptics or optichaptics or optic
– Plasma-derived enzymes (especially complement or Plasma-derived enzymes (especially complement or fibrin) activated by the surface of the IOLs fibrin) activated by the surface of the IOLs
– Adherence of bacteria and leukocytes to the IOL Adherence of bacteria and leukocytes to the IOL surfacesurface
– Toxicity caused by contaminants on the IOL surface Toxicity caused by contaminants on the IOL surface during manufacturing or implantationduring manufacturing or implantation
Post-Operative TimingPost-Operative Timing
UGH DevelopmentUGH Development– Usually weeks to months.Usually weeks to months.– Literature suggests 1-8 yrs.Literature suggests 1-8 yrs.
This patient; 1987 to 2006 – 19 years.This patient; 1987 to 2006 – 19 years.
Clinical SpectrumClinical Spectrum
Iris pigment epithelial defectsIris pigment epithelial defectsPigment dispersionPigment dispersionMicrohypemaMicrohypemaMacrohyphema IMacrohyphema IIncrease in IOPIncrease in IOP
Presenting SymptomsPresenting Symptoms
Intermittant blurringIntermittant blurring‘‘Redness’ to visionRedness’ to visionEye painEye painRed eyeRed eyePhotophobiaPhotophobia
UGH ComplicationsUGH Complications
Pseudophakic bullous keratopathyPseudophakic bullous keratopathyCorneal staining; recurrent hyphemaCorneal staining; recurrent hyphemaChronic inflammationChronic inflammationCystoid macular edemaCystoid macular edemaGlaucomaGlaucoma
UGH ManagementUGH Management
Bed rest with elevated head position to Bed rest with elevated head position to encourage hyphema settling encourage hyphema settling
Topical steroidTopical steroidReduce increased IOPReduce increased IOP
Ultimately, the lens may have to be Ultimately, the lens may have to be repositioned or removed.repositioned or removed.
UGH Treatment OptionsUGH Treatment Options
Observe, treat episodes individually.Observe, treat episodes individually.Pharmacologically reposition IOLPharmacologically reposition IOLIOL rotation IOL rotation IOL explanation +/- replacement.IOL explanation +/- replacement.
Patient ReturnsPatient Returns
VA cc: VA cc: O.D. 20/50, ph 20/30O.D. 20/50, ph 20/30
O.S. 20/20O.S. 20/20
GAT: 22, O.D.; 13 O.S.GAT: 22, O.D.; 13 O.S.2+ AC reaction.2+ AC reaction.
Patient scheduled for IOL removal.Patient scheduled for IOL removal.
STUDY:Indications for STUDY:Indications for IOL Explanation (FL)IOL Explanation (FL)
The majority of the removed IOLs were The majority of the removed IOLs were anterior chamber styles (53.9%), anterior chamber styles (53.9%), followed by iris-fixated lenses (33.7%)followed by iris-fixated lenses (33.7%)
The most common indications for The most common indications for surgery included:surgery included: Pseudophakic bullous keratopathy, 69%Pseudophakic bullous keratopathy, 69% UGH syndrome, 9%UGH syndrome, 9% IOL instability, 7%.IOL instability, 7%.
Surgical Timing with ACIOLSurgical Timing with ACIOL
Time between implantation and explanation Time between implantation and explanation with ACIOL complications:with ACIOL complications:– 1 to 8 years.1 to 8 years.
Surgical OutcomeSurgical Outcome
The poorest visual outcome was seen in The poorest visual outcome was seen in patients with the UGH syndrome.patients with the UGH syndrome.– 83% had a final acuity of 20/200 or 83% had a final acuity of 20/200 or
worse. worse. – Resolution of pain and inflammationResolution of pain and inflammation– Better control of their IOP as a result of Better control of their IOP as a result of
the surgery.the surgery.
1- Day Post-Operative1- Day Post-Operative
Surgery without incidentSurgery without incidentVA- 20/400, PH 20/100VA- 20/400, PH 20/100Some corneal edema; 3+ AC reaction.Some corneal edema; 3+ AC reaction.GAT- 13.GAT- 13.Continue with meds:Continue with meds:
– Cosopt b.id.Cosopt b.id. - Tobradex ung q.id.- Tobradex ung q.id.– Alphagan P b.id.Alphagan P b.id. - Atropine b.id.- Atropine b.id.– Diamox 500mg b.id.Diamox 500mg b.id.
Follow-UpsFollow-Ups
Seen on Day 2, 4, then 1 week, 2 week.Seen on Day 2, 4, then 1 week, 2 week.VA improves to 20/100 with pinhole and VA improves to 20/100 with pinhole and
+15D lens.+15D lens.Cornea improves; AC reaction diminishes Cornea improves; AC reaction diminishes
to grade 1.to grade 1.IOP in mid to low teens.IOP in mid to low teens.Continuing all meds.Continuing all meds.
3 Week Follow-Up3 Week Follow-Up
VA- 20/80VA- 20/80Refracts to 20/30.Refracts to 20/30.Trace AC reaction.Trace AC reaction.GAT- 13.GAT- 13.
SLOW taper off all meds.SLOW taper off all meds.
Review: Key PointsReview: Key Points
Be suspicious of misplaced IOLBe suspicious of misplaced IOL
ACIOL with UveitisACIOL with Uveitis
GonioscopyGonioscopy
THE END