Embed Size (px)
Citation preview

.
GRAMPIAN UNIVERSITY HOSPITALS NHS TRUST
ACCOUNTS 2003-2004

Contents
1 Directors’ Report
8 Statement of NHS Trust Board Members’ Responsibilities
9 Statement of The Chief Executive’s Responsibilities as The Accountable Officerof The Grampian University Hospitals NHS Trust
10 Statement on Internal Control
11 Report of the Auditor
13 Operating Cost StatementSummary of Resource Outturn
14
15
Statement of Recognised Gains and Losses
Balance Sheet
16 Cash Flow Statement
17 Notes to the Accounts
40 Accounts Direction

1
Grampian University Hospitals NHS Trust
Directors’ Report
Foreword
These accounts have been prepared by the NHS Trust under section 86(1B) of the National HealthService (Scotland) Act 1978 in the form which the Scottish Ministers have directed.
Short History of the Trust
The Trust was established on 1 April 1999 following the merger of Aberdeen Royal Hospitals NHSTrust, parts of Grampian Healthcare NHS Trust and parts of Moray Health Services NHS Trust. TheTrust owns and manages Aberdeen Royal Infirmary, Aberdeen Maternity Hospital, the RoyalAberdeen Children’s Hospital, Tor-na-Dee Hospital, Roxburghe House, Woodend Hospital,Woolmanhill Hospital and the Raeden Centre (all in Aberdeen) and Dr Gray’s Hospital in Elgin. TheTrust provides acute care to patients from a wide area including the whole of Grampian, the islands ofOrkney and Shetland and provides some services to the residents of Highland and Tayside as well asto the offshore oil industry. The Trust serves a population of 525,000.
Role of Trust Management Team
Following the publication of the Scottish Health Plan by the Scottish Executive in December 2000, 15single Unified NHS Boards were established in October 2001 to replace the separate structures ofNHS Health Boards and Trusts. NHS Trusts remained as legal entities within the local NHS systemand retained their existing operational autonomy with Trust Management Teams taking on the role ofthe Trust Board.
Trust Dissolution
In March 2003, the Scottish Health Department published Partnership for Care, Scotland’s HealthWhite Paper. This required NHS Boards to bring forward proposals by April 2004, at the latest, todissolve NHS Trusts in Scotland. On 31 March 2004, Grampian University Hospitals NHS Trust wasformally dissolved when Grampian Health Board, commonly known as NHS Grampian, took over itsactivities and assets and liabilities.
This change is in support of the development of integrated, decentralised healthcare services withinNHS Grampian, as detailed in the White Paper. By removing unnecessary organisational and legalbarriers, NHS Grampian staff will be empowered to plan and deliver improved healthcare serviceswithin a framework of clear strategic direction and rigorous performance management.
Principal activities and review of the year
2003/04 was again a very productive year in terms of the clinical activity undertaken by the Trust.During the year, 100,443 inpatient episodes of care were performed. There were also 19,313 daycase attendances and 459,823 outpatient attendances. A key task for the Trust was again to meetwaiting time targets for inpatient and day case treatments that are set by the Scottish Executive HealthDepartment (SEHD). At the end of March 2004, the Trust had achieved its overall waiting time targetfor the year with no inpatient or day cases waiting longer than nine months for treatment. The Trust,working in conjunction with NHS Grampian and the local authorities, also met the SEHD target for thenumber of delayed discharges at 31 March 2004.

2
The Trust received funding to take forward a number of initiatives in 2003/04 including:-
♦ Implementation of the low pay agreement in order to provide all NHS staff with an agreedminimum wage.
♦ Opening of the Oaks Hospice for the provision of palliative care in Elgin.♦ A range of initiatives around winter planning to prevent delayed discharges such as a community
geriatrician and continued bed capacity at Aberdeen Royal Infirmary.♦ The implementation of the nationally agreed Coronary Heart Disease / Stroke Strategy within NHS
Grampian.♦ Provision of additional capacity both within the Trust and through use of the private sector to
ensure that waiting time guarantees are achieved.♦ Making available a number of new and expensive drugs for treatment of chronic diseases in areas
such as Oncology, Gastroenterology, Ophthalmology and Rheumatalogy.♦ Modernisation of the Audiology service.♦ Preparation for the “Agenda for Change” pay modernisation programme due to be implemented in
October 2004.
The Trust has also been involved (in conjunction with the Health Board) in planning the provision ofspecialist services on a North of Scotland basis by dealing with fellow Health Boards and Trusts inHighland, Tayside and the Islands. The aim of this co-operation is to ensure the continued stability ofcritical services by making use of all available resource on a regional basis.
The major construction project for the year was the completion of the new Royal Aberdeen Children’sHospital, which became operational in January 2004. It now provides a state of the art facility for thewhole of the North of Scotland. Thanks to the generosity of the people of the North East and North ofScotland, the Archie Foundation Fundraising Campaign raised £5million, £2million in excess of theiroriginal fundraising target. These monies were used to fund additional support for the new hospital onareas such as play facilities and improvements to the hospital’s arts environment.
Work is also well advanced on the relocation of Roxburghe House to the Cornhill site in Aberdeen.This project is being jointly funded by the NHS, the New Opportunities Fund and Macmillan CancerRelief. Major investments were also made in 2003/04 in the purchase of new medical equipment andIT systems.
As in the past, the Trust continues to provide high quality patient care in a cost effective manner. Arecent exercise covering the 2002/03 financial year carried out by the national Information & StatisticsDivision of the NHS highlighted that the cost base of the Trust was 12% lower than for an averageTrust providing a similar level of activity. This track record means that the Trust is well placed to addvalue and become an integral part of a single system NHS Grampian.
Financial targets
The Scottish Executive requires NHS Trusts to achieve two financial targets on an annual basis.These are:
• To break even taking one year with another, i.e. net resource outturn should not exceed theRevenue Resource Limit; and
• To stay within the Capital Resource Limit

3
Performance against financial targets
Limit as setby NHS
Board
ActualOutturn
Variance(Over)/Under
£000 £000 £000
Revenue Resource limit 276,847 277,520 (673)
Capital Resource Limit 7,226 7,226 -
The variance of £673,000 was mainly a result of the costs of the new contract for consultant medicalstaff and the ongoing costs of the new deal for junior medical staff.
NHS Grampian has a Financial Recovery Plan in place to achieve repayment of the deficit, as part ofan agreement with the Scottish Executive Health Department.
Fixed assets and capital expenditure
The Trust invested £7.6 million during the year on items of capital expenditure, which includes £3.8million spent on medical equipment, £2.7 million on the final phase of the new Royal AberdeenChildren’s Hospital and £0.6 million on the replacement Roxburghe House, the Breast ScreeningCentre and the new theatre development.
Going forward, NHS Grampian will continue to face severe pressures on its capital programme withbids for essential projects exceeding the level of funding available. Additional funding is thereforerequired if the condition of the buildings and equipment is to be maintained to an acceptable standard.
Payment policy
The Trust is required by the Scottish Executive Health Department to report on compliance with theCBI prompt payment code. The code states that responsible organisations should:-
- have a clear and consistent policy of paying bills in accordance with the contract;- ensure that finance and purchasing departments are aware of this policy and adhere to it;- agree payment terms at the outset of a deal and adhere to them;- not extend or alter payment terms without prior agreement;- provide suppliers with clear guidance on payment procedures; and- ensure that there is a system for dealing quickly with complaints and disputes and advise
suppliers without delay when invoices or parts of invoices are contested.
It is Trust policy to adhere to this code. In 2003/04 the average credit taken was 36.9 days (2002/03:32.6 days). 42% of invoices by value and 41% by volume were paid within 30 days.
Research and Development
As a major teaching hospital, the Trust seeks to encourage research and development at all levels.There is a Research and Development Office run by a Director of Research and Development tofacilitate this. Expenditure on research and development in 2003/04 was £5.848 million.

4
Trust Board
Under the terms of the Scottish Health Plan, NHS Trusts concentrated on delivering their operationalresponsibilities within the local NHS system: this was primarily the responsibility of the Trust’sexecutive management.
In 2003/04, the full Trust Management Team comprised the Chair, two non-executives and fiveexecutive posts. References in the accounts to the Board refer to the Trust Management Team.
The following served as members of the Trust Board during the year:
Non-executive members
Professor Stephen Logan, ChairmanMrs Sue RobertsonProfessor Valerie Maehle
Executive members
Mr Alec Cumming Chief ExecutiveDr Donald Ross Medical Director (Retired 30 September 2003)Dr Roelf Dijkhuizen Acting Medical Director to 30 September 2003Dr Roelf Dijkhuizen Medical Director (Appointed 1 October 2003)Mr Alan Gall Director of FinanceMr David Benton Director of Nursing & QualityMs Mary Dowling Director of Human Resources (on career break from 1 April 2003)Mr Gordon Morrice Director of Human Resources (appointed 1 April 2003)
Up to 30 September 2003, Dr Donald Ross spent one day per week on his role as Medical Director ofthe Trust. The remainder of his time related to his role as Director of Clinical Health Informatics forNHS Grampian.
Corporate Governance
The Trust Board met regularly throughout the year to progress the business of the Trust. The Boardhad adopted a schedule of matters reserved for its decision and was supported by the work of sub-committees reporting to the Board.
Membership of committees could be populated from across the whole local NHS system and couldinclude members of the executive team and others with expertise relevant to the function of thecommittee. The main functions of the Committees, together with membership as at 31 March 2004,were as follows:
Audit Committee
The Audit Committee met as a combined committee for NHS Grampian. Its main duties included:
- the regular review of the role, function and performance of the Trust’s Internal Audit Service;- the review of external audit arrangements;- the review and monitoring of adherence to the Trust’s Standing Orders and Standing Financial
Instructions; and- ensuring that effective internal control systems were maintained and corporate governance
matters were observed.
Membership: Mr David Sutherland (Chair), Professor Valerie Maehle, Councillor Edward Aldridge,Mrs Anne Campbell, and Mr Angus Gordon.

5
Remuneration Committee
The Remuneration Committee continued to meet at Trust level. Its main duties were:
- to agree all terms and conditions of employment for Executive Directors of the Trust;- to monitor arrangements for the pay and conditions of service of senior managers, being those
reporting to Executive Directors and other Directors;- to regularly review the Trust’s policy for the remuneration and performance of senior
managers in the light of guidance issued by the Scottish Executive.
Membership: Professor Stephen Logan (Chair), Professor Valerie Maehle, Mrs Sue Robertson.
Clinical Governance Committee
The Clinical Governance Committee continued to meet at Trust level. Its main duties were:
- to oversee the clinical governance of the Trust; and- to assure the Trust Board that the arrangements for clinical governance were effective.
Membership: Mrs Sue Robertson (Chair) and Professor Valerie Maehle. Co-opted members:Professor Marion Hall and Mrs Susan Kinsey.
Endowment Committee:
The Endowment Committee continued to meet at Trust level. Its main duties included:
- to determine and set policies and investment objectives for Endowments;- the approval of Endowment Fund budgets;- the approval of the audited annual accounts; and- to ensure probity of expenditure.
Membership: Mr George McIntyre (chair), Professor Stephen Logan, Mr Alec Cumming, Mr Alan Galland Mr Gordon Stephen.
Risk Management Committee
The Risk Management Committee operated at Trust level in 2003/04. Its main duties included:
- to achieve, in partnership with staff, evidenced improvements in risk management throughoutthe Trust;
- to ensure that risk management was properly co-ordinated and effective performancemanagement thereof was in place; and
- to advise the Trust Management Team of significant risks and associated developments asthey arose.
Membership: Mr Alec Cumming (Chair), Mr Gordon Morrice, Dr Roelf Dijkhuizen, Dr ElizabethRobertson, Mr David Benton, Mr Alan Gall, Ms Ros Watkinson and Mr Wayne Gault.
6
Staff Governance Committee.
The main responsibility of the Staff Governance Committee was to oversee the implementation of thefive staff governance standards and achieve exemplar employer status in NHS Grampian.
The five standards entitle staff to be: Well informed;Appropriately trained;Involved in decisions that affect them;Treated fairly and consistently; andProvided with an improved and safe working environment.
Membership: Mrs Anne Campbell (Chair), Mrs Barbara Bruce, Mrs Margaret Burns, Councillor KateDean, Mr George Esson, Mr Angus Gordon, Professor Stephen Logan, Mrs Susan Robertson, MrJames Royan.
The Trust Board has adopted the codes of conduct and accountability for the NHS. The Trust Boardmembers’ responsibilities in relation to the accounts are set out on page 8.
Human Resources
The Trust employs 6,574 whole time equivalent staff.
The Trust continued to make progress in terms of its Human Resources (HR) strategy, peoplemanagement, organisational development, and partnership working with staff. New strategies havebeen developed for Learning and Development, Workforce Planning, Pay Modernisation and RiskManagement.
Staff development is a key responsibility and is sustained by Performance Appraisal, PersonalDevelopment Plans and Learning Plans linked to Service Plans.
A major responsibility of HR is supporting organisational change which continued as NHS Grampianmoved to a single system. Change is a constant and although staff respond extremely well to neworganisational arrangements and changing roles and relationships, this does add to the existingworkplace pressures.
The Staff Governance Action Plan (based on the 5 Standards: being informed, appropriately trained,involved, treated fairly and consistently, and provided with an improved and safe work environment)has been audited with positive outcomes in most areas.
A second Staff Survey was conducted in November 2003 and the results are being reflected in anupdated Action Plan.
Introduction and/or harmonisation of Staff Policies is an ongoing area of work.
Pay Modernisation is a major new area of work. This involves new contracts for Consultants and GPsto be implemented around April 2004 and preparation for Agenda for Change, a new policy for allother staff.

7
Register of Interests of Trust Board Members
The register of interests of Trust Board members is held at Trust Headquarters, Foresterhill House,Ashgrove Road West, Aberdeen and can be inspected by members of the public by contacting theTrust Board Secretary. The Non Executive Trustees were free from any business or otherrelationship, which could interfere with the exercise of their judgement.
Appointment of Auditor
The Public Finance and Accountability (Scotland) Act 2000 places personal responsibility on theAuditor General for Scotland to decide who is to undertake the audit of each health body in Scotland.For the financial years 2001/02 to 2003/04 the Auditor General appointed Peter Johnston, ChiefAuditor in Audit Scotland’s West Region, to undertake the audit of Grampian University Hospitals NHSTrust. The general duties of the auditors of health bodies, including their statutory duties, are set outin the Code of Audit Practice issued by Audit Scotland and approved by the Auditor General.
The internal auditors of the Trust for the period to 30 September 2003 were Deloitte & Touche. On 1October 2003, PricewaterhouseCoopers LLP were appointed as internal auditors for the period to 31March 2004.
Post balance sheet events
On 1 April 2004, the assets and liabilities and undertakings of the Grampian University Hospitals NHSTrust transferred to Grampian Health Board. The Grampian University Hospitals NHS Trust wasdissolved on 31 March 2004. Following the transfers of assets and liabilities, all financial transactionsfor the Grampian University Hospitals NHS Trust after 31 March 2004 were taken on by GrampianHealth Board. The assets and liabilities of Grampian University Hospitals NHS Trust reported in theseaccounts will be brought into account from the start of the financial year within the accounts ofGrampian Health Board for the year ended 31 March 2005.
Mr James RoyanChairman DateGrampian Health Board
Mr Alexander SmithInterim Chief Executive DateGrampian Health Board

8
STATEMENT OF NHS TRUST BOARD MEMBERS’RESPONSIBILITIES
The National Health Service (Scotland) Act 1978 requires Grampian University Hospitals NHS Trust toprepare accounts for each financial year which give a true and fair view of the state of affairs of theNHS Trust and of its income and expenditure for that period. In preparing those accounts, the Trustboard members are required to (a) select suitable accounting policies and then apply themconsistently, (b) make judgements and estimates that are reasonable and prudent, (c) state whetherapplicable accounting standards have been followed, subject to any material departures disclosed andexplained in the accounts, and (d) prepare the accounts on the going concern basis unless it isinappropriate to presume that Trusts will continue to operate.
The Trust board members are responsible for ensuring proper accounting records are maintainedwhich disclose with reasonable accuracy at any time the financial position of the Trust and enablethem to ensure that the accounts comply with the National Health Service (Scotland) Act 1978 and therequirements of the Scottish Executive Health Department. They are also responsible forsafeguarding the assets of the Trust and hence taking reasonable steps for the prevention anddetection of fraud and other irregularities.
The Grampian University Hospitals NHS Trust ceased on 31 March 2004 and its operations, assetsand liabilities were transferred to Grampian Health Board on 1 April 2004. As members of GrampianHealth Board, we confirm that the above responsibilities have been discharged during the period 1April 2003 to 31 March 2004 and in preparing the accounts.
...................................................................................... Mr James RoyanChairmanGrampian Health Board
...................................................................................... Mr Alan GallDirector of FinanceGrampian Health Board

9
STATEMENT OF THE CHIEF EXECUTIVE’S RESPONSIBILITIES ASTHE ACCOUNTABLE OFFICER OF THE GRAMPIAN UNIVERSITYHOSPITALS NHS TRUST
Under Section 15 of the Public Finance and Accountability (Scotland) Act, 2000, the PrincipalAccountable Officer (PAO) of the Scottish Executive has appointed me as Accountable Officer ofGrampian University Hospitals NHS Trust.
This designation carries with it, responsibility for the propriety and regularity of financial transactionsunder my control, and for the economical, efficient and effective use of resources placed at the Trust’sdisposal.
I am responsible for ensuring proper records are maintained and that the Accounts are preparedunder the principles and in the format directed by Scottish Ministers.
To the best of my knowledge and belief, I have properly discharged my responsibilities as accountableofficer as intimated in the Departmental Accountable Officers letter to me of the 25th July 2000.
………………………………………………… Mr Alec CummingChief ExecutiveGrampian University Hospitals NHS Trust
31 March 2004 Date

10
GRAMPIAN UNIVERSITY HOSPITALS NHS TRUST
STATEMENT ON INTERNAL CONTROL
As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports theachievement of the Trust’s policies, aims and objectives, set by Scottish Ministers, whilst safeguarding the publicfunds and assets for which I am personally responsible, in accordance with the responsibilities assigned to me.
The system of internal control is designed to manage rather than eliminate the risk of failure to achieve the Trust’spolicies, aims and objectives; it can therefore only provide reasonable and not absolute assurance ofeffectiveness.
The system of internal control is based on an ongoing process designed to identify the principal risks to theachievement of the Trust’s policies, aims and objectives, to evaluate the nature and extent of those risks and tomanage them efficiently, effectively and economically. I can confirm that we have taken the necessary action toimplement guidance from Scottish Executive Finance and that the following processes have been in placethroughout the year ended 31 March 2004.
• A Trust Management Team which meets regularly to consider the plans and strategic direction of theorganisation;
• Periodic reports from the chairman of the audit committee, to the board, concerning internal control;• Regular reports by internal audit which include the Head of Internal Audit’s independent opinion on the
adequacy and effectiveness of the system of internal control together with recommendations forimprovement;
• Establishment of key performance and risk indicators, including a risk register;• As part of the performance management arrangements, regular reports from managers on the steps they
are taking to manage risks in their areas of responsibility including progress reports on key projects; and• Continued our programme of risk awareness training for all staff.
The Trust Management Team has been committed to ensuring that the risk management process continues to bereviewed and developed and that risk management is a key element of the corporate planning and decisionmaking process of the Trust. The Trust has an established Risk Management Committee which meets regularlyto ensure ongoing development of the effectiveness and operation of the Trust’s overall risk managementprocess.
The Audit Committee and the Trust Management Team receive regular reports from managers on the steps theyare taking to manage risks in their areas of responsibility including progress reports on key projects.
The Trust’s internal auditors also submit regular reports to the Audit Committee which include the Head of InternalAudit’s independent opinion on the adequacy and effectiveness of the Trust’s system of internal control togetherwith recommendations for improvement.
I can also confirm that the Trust complies with the minimum internal financial controls as set down inMEL(1993)83.
My review of the effectiveness of the system of internal control is informed by the work of the internal auditors andthe executive managers within the Trust who have responsibility for the development and maintenance of theinternal control framework, and comments made by the external auditors in their management letters and otherreports.
………………………………………………… Mr Alec CummingChief ExecutiveGrampian University Hospitals NHS Trust
31 March 2004 Date

11
INDEPENDENT AUDITOR’S REPORT
To the members of Grampian NHS Board, the Scottish Parliament and the Auditor General for Scotland
I have audited the financial statements on pages 13 to 39 under the National Health Service (Scotland) Act 1978. Thefinancial statements have been prepared under the historical cost convention, as modified by the revaluation of certainfixed assets, and in accordance with the accounting policies set out on pages 17 to 20.
This report is made solely to the parties to whom it is addressed in accordance with the Public Finance andAccountability (Scotland) Act 2000 and the Code of Audit Practice approved by the Auditor General for Scotland and forno other purpose, as set out in paragraph 43 of the Statement of Responsibilities of Auditors and of Audited Bodiesprepared by Audit Scotland, dated July 2001.
Respective responsibilities of the Board Members, Accountable Officer and Auditor
As described on pages 8 and 9 the Board and the Accountable Officer of the NHS Trust are normally responsible for thepreparation of the financial statements in accordance with the National Health Service (Scotland) Act 1978 and directionsmade thereunder. The Accountable Officer is also responsible for ensuring the regularity of expenditure and income.The Board and Accountable Officer are also normally responsible for the preparation of the Directors’ Report. Themembers of Grampian NHS Board have confirmed that the aforementioned responsibilities have been discharged duringthe period from 1 April 2003 to 31 March 2004 and in preparing the accounts. My responsibilities, as independentauditor, are established by the Public Finance and Accountability (Scotland) Act 2000 and the Code of Audit Practiceapproved by the Auditor General for Scotland, and guided by the auditing profession’s ethical guidance.
I report my opinion as to whether the financial statements give a true and fair view and are properly prepared inaccordance with the National Health Service (Scotland) Act 1978 and directions made thereunder and whether, in allmaterial respects, the expenditure and income shown in the financial statements were incurred or applied in accordancewith any applicable enactments and guidance issued by the Scottish Ministers. I also report if, in my opinion, the NHSTrust has not kept proper accounting records, or if I have not received all the information and explanations I require formy audit.
I review whether the statement on page 10 complies with the guidance issued by the Scottish Executive HealthDepartment ‘Corporate governance: Statement on Internal Control’. I report if, in my opinion, the statement does notcomply with the guidance or if it is misleading or inconsistent with other information I am aware of from my audit. I amnot required to consider whether the statement covers all risks and controls, or form an opinion on the effectiveness ofthe NHS Trust’s corporate governance procedures or its risk and control procedures.
I read the Directors’ Report published with the financial statements and consider the implications for my report if Ibecome aware of any apparent misstatements or material inconsistencies with the financial statements.
Basis of audit opinions
I conducted my audit in accordance with the Public Finance and Accountability (Scotland) Act 2000 and the Code ofAudit Practice, which requires compliance with relevant United Kingdom Auditing Standards issued by the AuditingPractices Board.
An audit includes examination, on a test basis, of evidence relevant to the amounts, disclosures and regularity ofexpenditure and income shown in the financial statements. It also includes an assessment of the significant estimatesand judgements made by the Board of the NHS Trust and the Accountable Officer in the preparation of the financialstatements and of whether the accounting policies are appropriate to the NHS Trust’s circumstances, consistentlyapplied and adequately disclosed.
I planned and performed my audit so as to obtain all the information and explanations which I considered necessary inorder to provide me with sufficient evidence to give reasonable assurance that the financial statements are free frommaterial misstatement, whether caused by fraud or other irregularity or error, and that, in all material respects, theexpenditure and income shown in the financial statements were incurred or applied in accordance with any applicableenactments and guidance issued by the Scottish Ministers. In forming my opinion, I also evaluated the overall adequacyof the presentation of information in the financial statements.
The Trust was dissolved on 31 March 2004 and on 1 April 2004, the assets and liabilities and undertakings of the Trusttransferred to Grampian Health Board. The assets, liabilities, results and cash flows of the Trust reported in thesefinancial statements will be brought into account within the financial statements of Grampian Health Board from thestart of the financial year ending 31 March 2005.

12
Opinions
Financial statementsIn my opinion the financial statements give a true and fair view of the state of affairs of the Grampian University HospitalsNHS Trust as at 31 March 2004 and of its net operating cost, recognised gains and losses and cash flows for the yearthen ended and have been properly prepared in accordance with the National Health Service (Scotland) Act 1978 anddirections made thereunder.
RegularityIn my opinion, in all material respects, the expenditure and income shown in the financial statements were incurred orapplied in accordance with any applicable enactments and guidance issued by the Scottish Ministers.
Failure to Comply with a Statutory Requirement
I draw attention to the Trust’s performance for the year ended 31 March 2004 against its statutory financial target tobreak even taking one year with another i.e. the Trust’s net resource outturn should not exceed the Revenue ResourceLimit (RRL). In 2003/04 the Trust’s net resource outturn exceeded the RRL by £0.673m.
Grampian Health Board has a financial recovery plan in place to achieve repayment of the deficit to the ScottishExecutive Health Department by 31 March 2006.
Peter Johnston CA CPFAChief AuditorAudit ScotlandBallantyne House84 Academy StreetINVERNESSIV1 ILU
6 July 2004

13
OPERATING COST STATEMENT FOR THE YEAR ENDED 31 MARCH 2004
2003-04 2002-03Note £000 £000
Clinical Services CostsHospital and Community HealthServices
2,3 205,310 178,108
Total Clinical Services Costs 205,310 178,108
Non Clinical Costs 2,3 87,694 89,466
Effect of Revaluation of Property 4 89 7,278(Profit) on disposal of fixed assets 5 (1,669) (736)
GROSS OPERATING COSTS 291,424 274,116
Less: Miscellaneous Income 6 (13,807) (13,730)Less: Interest Receivable 7 (97) (153)
NET OPERATING COSTS 277,520 260,233
SUMMARY OF RESOURCE OUTTURN FOR THE YEAR ENDED 31 MARCH 2004
Net Operating Costs (as above) 277,520 260,233Brought forward Income and Expenditure Balance - 5,199Net Resource Outturn 277,520 265,432Revenue Resource Limit 276,847 260,233Excess against Revenue Resource Limit (673) (5,199)
The excess of £5,199,000 against the Revenue Resource Limit, as reported for 2002/03, wastransferred to Grampian Health Board in 2003/04 and is reflected in Grampian Health Board’saccounts for 2003/04.

14
STATEMENT OF RECOGNISED GAINS AND LOSSES FOR THE YEAR ENDED 31 MARCH 2004
2003-04 2002-03£000 £000
Net Gain on revaluation of tangible fixed assets 14,468 10,915
Increases in the Donated Asset Reserve due to receipt of donated assets 3,881 1,201
Reduction in the Donated Asset Reserve due to the depreciation of fixed assets (471) (471)
Losses due to impairment of donated assets (as writtenoff in reserves) - (59)
Total gains and losses recognised in the financial year 17,878 11,586
Prior period adjustment (2,205) -
Total recognised gains and losses for the year 15,673 11,586

15
BALANCE SHEET AS AT 31 MARCH 2004
As at As at31/3/2004 31/3/2003
Note £000 £000FIXED ASSETSIntangible assets 9 8 -Tangible assets 10 230,647 215,716
230,655 215,716
Debtors falling due after more than one year 12 534 491
CURRENT ASSETSStocks and work in progress 11 2,854 2,915Debtors 12 9,483 7,315Cash at bank and in hand 146 1,127
12,483 11,357
CREDITORS:Amounts falling due within one year 13 (31,420) (23,049)
NET CURRENT (LIABILITIES) (18,937) (11,692)
TOTAL ASSETS LESS CURRENT LIABILITIES 212,252 204,515
PROVISIONS FOR LIABILITIES AND CHARGES 14 (685) (860)
211,567 203,655
FINANCED BY:CAPITAL AND RESERVES
General Fund 19 166,737 176,465Revaluation reserve 15 34,441 20,453Donated Asset Reserve 15 10,389 6,737
211,567 203,655
Signed on behalf of the board on 6 July 2004
Mr Alexander Smith Mr Alan GallInterim Chief Executive Director of FinanceGrampian Health Board Grampian Health Board

16
CASH FLOW STATEMENT FOR THE YEAR ENDED 31 MARCH 2004
2003-04 2003-04 2002-03 2002-03Note £000 £000 £000 £000
Net cash (outflow) from operating activities 16.1 (267,000) (252,566)
Capital Expenditure
Payments to acquire tangible fixed assets (12,656) (14,779)Receipts from sale of fixed assets 1,769 1,330
Net cash (outflow) from capital expenditure (10,887) (13,449)
Net cash (outflow) before Financing (277,887) (266,015)
Financing:Funding 277,887 266,015Movement in general fund working capital (981) 1,013Cash drawn down 276,906 267,028
Net cash inflow from financing 276,906 267,028
(Decrease)/Increase in cash (981) 1,013

17
NOTES TO THE ACCOUNTS
1. ACCOUNTING POLICIES
These accounts have been prepared in accordance with the Resource Accounting Manual issued by HMTreasury. The particular accounting policies adopted by the NHS Trust are described below. They havebeen applied consistently in dealing with items considered material in relation to the accounts.
a. Going Concern
The accounts are prepared on the going concern basis, which provides that the entity will continue inoperational existence for the foreseeable future.
Grampian University Hospitals NHS Trust was formally dissolved on 31 March 2004 when GrampianHealth Board, commonly known as NHS Grampian, took over its activities and assets and liabilities.The Going Concern Concept has been applied to the provision of patient care services formerlycarried out by Grampian University Hospitals NHS Trust following guidance on the application of FRS18 contained in the Resource Accounting Manual. Assets and liabilities of the Trust were transferred toNHS Grampian on 1 April 2004 at the values recorded in the accounts of the Trust for the year ended31 March 2004.
b. Accounting Convention
The accounts are prepared on a historical cost basis modified to reflect changes in the value of fixedassets at their value to the business by reference to their current costs.
c. Funding
Most of the expenditure of the Trust is met from funds advanced by Scottish Health Boards withinapproved revenue and capital resource limits. Cash drawn down to fund expenditure within theselimits will be credited to the general fund.
Miscellaneous Income represents all other income receivable by the Trust.
d. Fixed Assets
i. Capitalisation
All assets falling into the following categories are capitalised:
intangible assets which can be valued, are capable of being used in a Trust’s activities for more thanone year and have a replacement cost equal to or greater than £5,000;
tangible assets which are capable of being used for a period which could exceed one year, and havea cost equal to or greater than £5,000;
assets of lesser value may be capitalised where they form part of a networked computer systempurchased at approximately the same time, and cost over £5,000 in total, or where they are part ofthe initial costs of equipping a new development and total over £5,000.
ii. Valuation
Fixed assets are valued as follows:
Operational land, buildings and their installations and fittings, and external works are assessed withinexisting use on the basis that the occupation will continue for the foreseeable future, unless otherwisestated.
For non-specialised properties, where there is direct market evidence, the value is assessed at openmarket value for the existing use.
For specialised properties, where there is no market evidence within existing use, the value isassessed by using a depreciated replacement cost approach.

18
Non-operational properties which are surplus to requirements are assessed at open market value foralternative use.
All land and building assets within the NHS in Scotland are revalued at not more than 5 yearlyintervals. Between valuations an appropriate index is applied to arrive at a current cost. Thebuildings index is based on the All in Tender Price Index published by the Building Cost InformationService (BCIS). The land index is based on the residential building land values reported in theProperty Market Report published by the Valuation Office.
The last professional revaluation took place as at 31st March 2004 and is reflected in these accounts.The valuations are carried out in accordance with the Royal Institute of Chartered Surveyors (RICS)Appraisal and Valuation Manual insofar as these terms are consistent with the agreed requirements ofthe Scottish Executive Health Department.
Equipment is valued at estimated net replacement cost or the recoverable amount. The estimatednet replacement cost is the replacement value of the asset as new, less the accumulateddepreciation. The recoverable amount will only be used when the decision has been made to disposeof the asset.
Assets in the course of construction are valued at current cost. This is calculated as the level ofexpenditure incurred to which an appropriate index is applied to arrive at a current value.
To meet the underlying objectives established by the Scottish Executive Health Department thefollowing accepted variations of the RICS Appraisal and Valuation Manual have been required:
Specialised operational assets have been valued on a replacement rather than a modern substitutebasis;
No adjustment has been made to the cost figures of operational assets in respect of dilapidations;and
Additional alternative Open Market Value figures have only been supplied for operational assetsscheduled for imminent closure and subsequent disposal.
Impairment
Losses in value reflected in valuations are described as impairments. These are accounted for inaccordance with Financial Reporting Standard 11. Where these relate to the consumption ofeconomic benefits, they are charged to the operating cost statement.
Reductions in value that relate to fluctuations in market prices, or other reasons not involving loss ofeconomic benefit, are first charged to the revaluation reserve insofar as it is represented by thoseassets, and that part of the loss is recognised in the Statement of Recognised Gains and Losses.Further losses, beyond the level of the revaluation reserve relating to that asset, are charged to theoperating cost statement, except where it can be demonstrated that the recoverable amount is greaterthan the revalued amount, in which case the fall in value below recoverable amount is recognised inthe Statement of Recognised Gains and Losses, and ultimately in the Revaluation Reserve.
iii. Depreciation and Amortisation
Depreciation is charged on each main class of tangible asset as follows:
Freehold land and assets in the course of construction are not depreciated. Buildings, installations,and fittings are depreciated on their current value over the estimated remaining life of the asset asadvised by the appointed valuer. The actual remaining lives of the building elements are assessed inthe context of the maximum useful lives for building elements.
Equipment is depreciated on current cost over the estimated life of the asset.
Depreciation is charged on a straight-line basis.

19
The following asset lives have been used:
Useful Life
Buildings (Structure) 31-75
Buildings (Engineering) 15-35
Moveable engineering plant and equipment andlong life medical equipment
10
Furniture and medium life medical equipment 5-10
Mainframe information technology installations 7
Vehicles and soft furnishings 7
Office, information technology, short life medicaland other equipment
5
iv. Donated Assets
Donated assets are capitalised at their valuation on receipt and are valued and depreciated asdescribed above.
The value of donated assets and the donated element of part donated assets is reflected in a DonatedAsset Reserve which is credited with the value of the original donation and debited/credited followingany subsequent revaluation; an amount equal to the depreciation charge is released from this reserveeach year to the operating cost statement.
v. Leasing
Rentals under operating leases are charged on a straight-line basis.
vi. Intangible Assets
Intangible assets, such as software licenses, are capitalised when they are capable of being used in aTrust’s activities for more than one year, they can be valued and they have a cost of at least £5,000.
Intangible fixed assets held for operational use are valued at historical cost and are depreciated overthe estimated life of the asset on a straight-line basis. The carrying value of intangible assets isreviewed for impairments at the end of the first full year following acquisition and in other periods ifevents or changes in circumstances indicate the carrying value may not be recoverable.
Purchased computer software licences are capitalised as intangible fixed assets where expenditure ofat least £5,000 is incurred. They are amortised over the shorter term of the licence and their usefuleconomic lives.
e. Stocks and Work in Progress
Stocks and work in progress are valued at the lower of cost and net realisable value. This isconsidered to be a reasonable approximation to current cost due to the high turnover of stocks.
Work in progress comprises goods in intermediate stages of production. Partially completed contractsfor patient services are not accounted for as work in progress.
20
f. Debtors and Creditors
Debtors and Creditors have been assessed on the basis of goods and services supplied or receivedup to and including 31st March 2004 for which payment had not been received or made by that date.
g. Research and Development
Research and development expenditure is charged against income in the year in which it is incurred,except insofar as it relates to a clearly defined project, the benefits from which can reasonably beregarded as assured. Expenditure so deferred is limited to the value of future benefits and isamortised through the operating cost statement on a systematic basis over the period expected tobenefit from the project.
h. Medical and Clinical Negligence Costs
Both medical and clinical negligence costs are treated as operating expenses, to the extent that theyare payable by the Trust. Where a settlement is likely it is provided for within the accounts. Wherethe prospect of settlement is uncertain, the amount should be estimated and disclosed as a contingentliability.
i. Pensions
The Trust contributes to the NHS Superannuation Scheme for Scotland. Contributions aredetermined on the basis of recommendations made by the Government Actuary. The pension costcharged to the operating cost statement is based on an actuarial assessment of the cost to be borneby the Trust.
j. Related Party Transactions
FRS 6 requires disclosure of material related party transactions. As the majority of NHS incomederives from related party transactions each transaction will not therefore be disclosed separately.Note 6 “Miscellaneous Income” however shows income received from each category of Health Bodyand Note 2 identifies total expenditure with other NHS bodies.
k. Liquid Resources
Deposits and other investments that are readily convertible into known amounts of cash at or close totheir carrying amounts are treated as liquid resources in the cashflow statement.
Investments which are not accessible within 24 hours without loss of interest but which do not maturein a period greater than one year are classified as current asset investments in the balance sheet andas liquid resources in the cashflow statement.
l. Value Added Tax
Most of the activities of the Trust are outside the scope of VAT and, in general, output tax does notapply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevantexpenditure category or included in the capitalised purchase cost of fixed assets. Where output tax ischarged or input VAT is recoverable, the amounts are stated net of VAT.
m. Losses and Special Payments
Operating expenditure includes certain losses which would have been made good through insurancecover had the NHS not been bearing its own risks. Had the NHS provided insurance cover, theinsurance premiums would have been included as normal revenue expenditure.

21
2. OPERATING EXPENSES
2.1 Operating expenses comprise the following elements:2003-04 2003-04 2002-03 2002-03
£000 £000 £000 £000
Clinical Services - HCH 205,310 178,108
Total Clinical Services 205,310 178,108
Non Clinical Costs Hotel Services 14,004 13,038
Other Services 29,714 28,129
Transport, Travel & Subsistence 2,442 1,671
Premises 17,433 17,863
Depreciation 10,804 11,213
Cost of Capital 6,723 11,538
Clinical/Medical Negligence 300 266
Research & Development 5,848 5,298
Other 426 450
Total Non Clinical Costs 87,694 89,466
TOTAL 293,004 267,574
Other expenses include £91,000 (2002-03: £97,000) payable to Audit Scotland to secure the externalaudit of the Trust.
Total operating expenses includes £15,815,000 (2002-03: £12,913,000) payable to other NHS bodies.
2.2 Operating expenses include the following amounts in respect of hire and operating lease rentals :
2003-04 2002-03£000 £000
Other operating leases 177 210
At 31 March 2004, the Trust amounts due in the next year under operating leases were asfollows:
Other Leases Other Leases31 March 2004 31 March 2003
£000 £000Operating leases which expire:- Within 1 year - 31- Between 1 and 5 years 166 150- After 5 years 43 -
TOTAL 209 181

22
2.3 Senior Employees' Remuneration2003-04 2002-03 £000 £000
Trustees’ RemunerationNon-Executive Members 37 36Executive Members’ Salaries 454 502Other emoluments 32 41
TOTAL 523 579
Total of taxable benefits to board members 8 8

23
Remuneration of:
Salary(Bands of
£5,000)
Realincrease
inpension
at age 60(bands of
£5,000)
Totalaccruedpension
at age 60at 31/3/04(bands of
£5,000)
CashEquivalent
TransferValue
(CETV) at 31March 2003
£000
CashEquivalent
TransferValue
(CETV) at 31March 2004
£000
RealIncrease in
CETV inyear
(bands of£5,000)
SuperannuationService at
31 March 2004No. of Years
Benefits inkind£000
Chairman- Professor S Logan 20-25 - - - - - n/a -
Chief Executive- Mr A Cumming (see note 1) 110-115 0-5 35-40 633 680 10-15 28 5
Medical Director- Dr D Ross (up to 30/9/03)
(see note 1)65-70 0-5 55-60 1,077 n/a n/a n/a -
- Dr R Dijkhuizen (from1/10/03) (see note 1)
110-115 0-5 15-20 216 257 10-15 13 -
Director of Finance- Mr A Gall (see note 1) 70-75 0-5 5-10 106 132 15-20 9 3
Director of Nursing & Quality- Mr D Benton (see note 1) 80-85 0-5 0-5 19 34 5-10 2 -
Director of Human Resources- Ms M Dowling (up to
31/3/03)25-30 0-5 15-20 205 n/a n/a 16 -
- Mr G Morrice (from 1/4/03) See note 2
Non-Executive Trustees:Professor V Maehle 5-10 - - - - - n/a -
Mrs S Robertson 5-10 - - - - - n/a -

24
Remuneration of:
Salary(Bands of
£5,000)
Realincrease
inpension
at age 60(bands of
£5,000)
Totalaccruedpension
at age 60at 31/3/04(bands of
£5,000)
CashEquivalent
TransferValue
(CETV) at 31March 2003
£000
CashEquivalent
TransferValue
(CETV) at 31March 2004
£000
RealIncrease in
CETV inyear
(bands of£5,000)
SuperannuationService at
31 March 2004No. of Years
Benefits inkind£000
Other Senior Employees:Associate Facilities Director- Mr J Ferguson (see note 1) 60-65 0-5 20-25 350 380 5-10 32 2
Director of CorporateCommunications- Mr A Reid (up to 24/8/03)
(see note 1)25-30 0-5 10-15 191 n/a n/a n/a 3
Head of Service Development- Mr G Smith (see note 1) 70-75 0-5 15-20 204 234 10-15 21 -
Assistant Chief Executives:Mr W Chisholm 75-80 0-5 25-30 365 409 15-20 30 2
Mrs F Grant 50-55 0-5 15-20 215 245 10-15 28 1
Ms D Grant 85-90 0-5 10-15 128 155 10-15 11 3
Miss K Simcock 60-65 0-5 5-10 48 61 5-10 7 -
Note 1 Mr A Gall was also Director of Finance for Grampian Primary Care NHS Trust. His total remuneration in respect of the two directorships is disclosed above;
Prior to his retirement on 30 September 2003, Dr D Ross spent one day per week in his role as Medical Director of the Trust. The remainder of his time related to hisrole as Director of Clinical Health Informatics for NHS Grampian. His total remuneration is disclosed above.
Dr R Dijkhuizen was Acting Medical Director for the period to 30 September 2003. His remuneration for this period is included above.
The remit for Mr J Ferguson, Mr A Reid and Mr G Smith covered all of NHS Grampian, which included Grampian University Hospitals NHS Trust, Grampian PrimaryCare NHS Trust and Grampian Health Board. Their total remuneration is disclosed above.
Mr A Cumming and Mr D Benton also held positions as executive directors of Grampian Health Board. Their total remuneration is disclosed above.
Professor S Logan also holds a post as a non-executive trustee of Grampian Health Board. His total remuneration is disclosed above.
Note 2 Mr G Morrice, Director of Human Resources, is also the Human Resources and Organisational Learning Director for Grampian Primary Care NHS Trust. Hisremuneration and pension entitlement are disclosed in the accounts of that body.
Note: Staff pension benefits are provided through the NHS Superannuation Scheme for Scotland. Details of the scheme can be found in Note 18.

25
Prior Year Comparative Figures2002-2003
Remuneration of:
Salary(Bands of
£5,000)
Realincrease
inpension
at age 60(bands of
£5,000)
Totalaccrued
pension atage 60 at
31/3/03(bands of
£5,000)
CashEquivalent
TransferValue
(CETV) at 31March 2003
£000
SuperannuationService at
31 March 2003No. of Years
Benefits inkind£000
Chairman- Professor S Logan (from 1/11/02)
5-10 - - - n/a -
- Dr H Fullerton OBE(to 30/9/02)
10-15 - - - n/a -
Chief Executive- Mr A Cumming (see Note 1)
110-115 0-5 35-40 633 27 5
Medical Director- Dr D Ross (see Note 1)
45-50 5-10 55-60 1,077 36 -
Acting Medical Director- Dr R Dijkhuizen
105-110 0-5 15-20 216 12 -
Director of Finance- Mr A Gall (see Note 1)
65-70 0-5 5-10 106 8 3
Director of Nursing & Quality- Mr D Benton (see Note 1)
75-80 0-5 0-5 19 1 -
Director of Human Resources- Ms M Dowling (see Note 1)
80-85 0-5 10-15 205 15 -
Acting Director of HumanResources- Mr E Rennie (from 4/7/02 to31/3/03) (see Note 1)
45-50 0-5 20-25 n/a n/a -
Non-Executive Trustees:
Professor V Maehle 5-10 - - - n/a -
Mrs S Robertson 5-10 - - - n/a -

26
Remuneration of:
Salary(Bands of
£5,000)
Realincrease
inpension
at age 60(bands of
£5,000)
Totalaccrued
pension atage 60 at
31/3/03(bands of
£5,000)
CashEquivalent
TransferValue
(CETV) at 31March 2003
£000
SuperannuationService at
31 March 2003No. of Years
Benefits inkind£000
Other Senior Employees:
Associate Facilities Director- Mr J Ferguson (see Note 1)
60-65 0-5 20-25 350 31 2
Director of CorporateCommunications- Mr A Reid (see Note 1)
60-65 0-5 10-15 191 15 2
Head of Service Development- Mr G Smith (see Note 1)
65-70 0-5 15-20 204 20 -
Assistant Chief Executives:
Mr W Chisholm 70-75 0-5 20-25 365 29 3
Mrs F Dodds 45-50 0-5 15-20 215 27 1
Ms D Grant 80-85 0-5 5-10 128 10 3
Miss K Simcock 60-65 0-5 0-5 48 6 -

27
Note 1 For these Directors and Senior Employees, their remuneration covered responsibilities on a NHSGrampian wide basis as follows:
Mr A Gall was appointed Acting Director of Finance for Grampian Primary Care NHS Trust on 1 June2002, and became Director of Finance with effect from 1 January 2003. His total remuneration inrespect of the two directorships is disclosed above.
Dr D Ross spent one day per week in his role as Medical Director of the Trust and retired in October2003. The remainder of his time related to his role as Director of Clinical Health Informatics for NHSGrampian. His remuneration in relation to his role as Medical Director is disclosed above.
With effect from January 2003, the remit for Mr J Ferguson, Mr A Reid and Mr G Smith covered all ofNHS Grampian, which includes Grampian University Hospitals NHS Trust, Grampian Primary CareNHS Trust and Grampian Health Board. Their total remuneration is disclosed above.
Mr A Cumming and Mr D Benton also held positions as executive directors of Grampian HealthBoard. Their total remuneration is disclosed above.
Professor S Logan also holds a post as a non-executive trustee of Grampian Health Board. His totalremuneration is disclosed above.
From April 2002, Ms M Dowling was appointed Director Designate, Human Resources, with a remitcovering all of NHS Grampian as part of the integration of all non-clinical support services. Thisnecessitated an ‘acting-up’ arrangement in Human Resources and Mr E Rennie took on the role ofActing Director of Human Resources from July 2002 to March 2003.
It is not possible to disclose the Cash Equivalent Transfer Values of directors and senior employees at 31March 2002 as this information is not available from the Scottish Public Pensions Agency.
3. STAFF DETAILS
3.1 Average number of employees2003-04 2002-03
Total Cost Total CostNo. £000 No. £000
Medical & Dental 859 68,245 806 55,297
Nursing & Midwifery 3,019 70,049 2,906 66,082
Professions Allied to Medicine 497 14,839 440 12,974
Ancillaries 862 13,240 921 12,902
Management & Administration 810 16,473 831 16,498
Professional & Technical 518 12,222 447 10,153
Board Members 9 661 10 622
TOTAL 6,574 195,729 6,361 174,528

28
3.2 Segmentation of staff costs2003-04 2002-03
£000 £000
Salaries and wages 172,752 154,352
Social security costs 12,867 10,175
Other pension costs 7,831 7,197
Agency and recharged staff 2,279 2,804
TOTAL 195,729 174,528
3.3 The following numbers of employees received remuneration (excluding pension contributions)falling within the following ranges:
2003-04 2002-03No. No.
Clinicians£50,001-£55,000 66 44£55,001-£60,000 55 38£60,001-£65,000 36 48£65,001-£70,000 49 47£70,001-£75,000 46 40£75,001-£80,000 48 40£80,001-£85,000 34 30£85,001-£90,000 25 18£90,001-£95,000 26 17£95,001-£100,000 7 7£100,001-£105,000 13 13£105,001-£110,000 13 6£110,001-£115,000 5 6£115,001-£120,000 4 1£120,001-£125,000 3 3£125,001-£130,000 2 2£130,001-£135,000 5 1£135,001-£140,000 2 1£140,001-£145,000 1 -£145,001-£150,000 1 1£150,001-£155,000 1 -£165,001-£170,000 - 1
Other£50,001-£55,000 13 6£55,001-£60,000 4 3£60,001-£65,000 2 -£65,001-£70,000 2 -£70,001-£75,000 1 -£80,001-£85,000 1 -

29
4. EFFECT OF REVALUATION OF PROPERTY
Impairment of Fixed Assets 2003-04 2002-03£000 £000
Value Written off Asset:
Written off through OCS 89 7,278
5. (PROFIT) ON DISPOSAL OF FIXED ASSETS
(Profit) on disposal of fixed assets is made up as follows:
2003-04 2002-03£000 £000
Profit on disposal of land and buildings (1,669) (731)Profit on disposal of plant and equipment - (5)
TOTAL (1,669) (736)
6. MISCELLANEOUS INCOME
2003-04 2002-03£000 £000
Income from ActivitiesNHSScotland Bodies: NHS Trusts 527 504Non-NHS: Private Patients 1,175 1,314 RTA Income 638 607 Other Income from Activities 97 169
2,437 2,594Other Operating IncomeTransfers from the Donated Asset Reserve in respectof depreciation on donated assets
471 471
Contributions in respect of clinical/medical negligenceclaims - 5
Other 10,899 10,660
TOTAL 13,807 13,730
Of the above, £5,262,000 (2002-03 £5,098,000) is derived from other NHS bodies.

30
7. INTEREST RECEIVABLE2003-04 2002-03
Interest receivable consists of: £000 £000
Interest on bank deposits 97 153
8. COST OF CAPITAL CHARGE
The Trust is charged a Cost of Capital Charge on average relevant net assets. The charge is made at theGovernment’s standard rate, as determined by HM Treasury. The rate is currently 3.5%.
The average relevant net assets is the simple average of the opening and closing relevant net assets,calculated as follows:
1/4/2003 31/3/2004£000 £000
Total net assets (total capital and reserves before write down ofequipment) 203,655 211,567
LESS: Donated assets (Donated Asset Reserve) (6,737) (10,389)
Revaluation of Fixed Assets - (14,469)
OPG Account Balance (1,110) (110)
General Fund Creditor 1,127 146
Capital charges control account balance 513 -
RELEVANT NET ASSETS 197,448 186,745
Average relevant net capital = 197,448+186,745 = £192,096 (2002-2003 £192,303)2
The 3.5% Cost of Capital is thus:
Average relevant net assets of £192,096 x 3.5% = £6,723
9. INTANGIBLE FIXED ASSETS
Intangible fixed assets held at the balance sheet date comprise the following elements:
Software Total£000 £000
Cost Valuation:As at 1 April 2003 - -
Additions 8 8
At 31 March 2004 8 8
Net Book Value at 1 April 2003 - -
Net Book Value at 31 March 2004 8 8
31
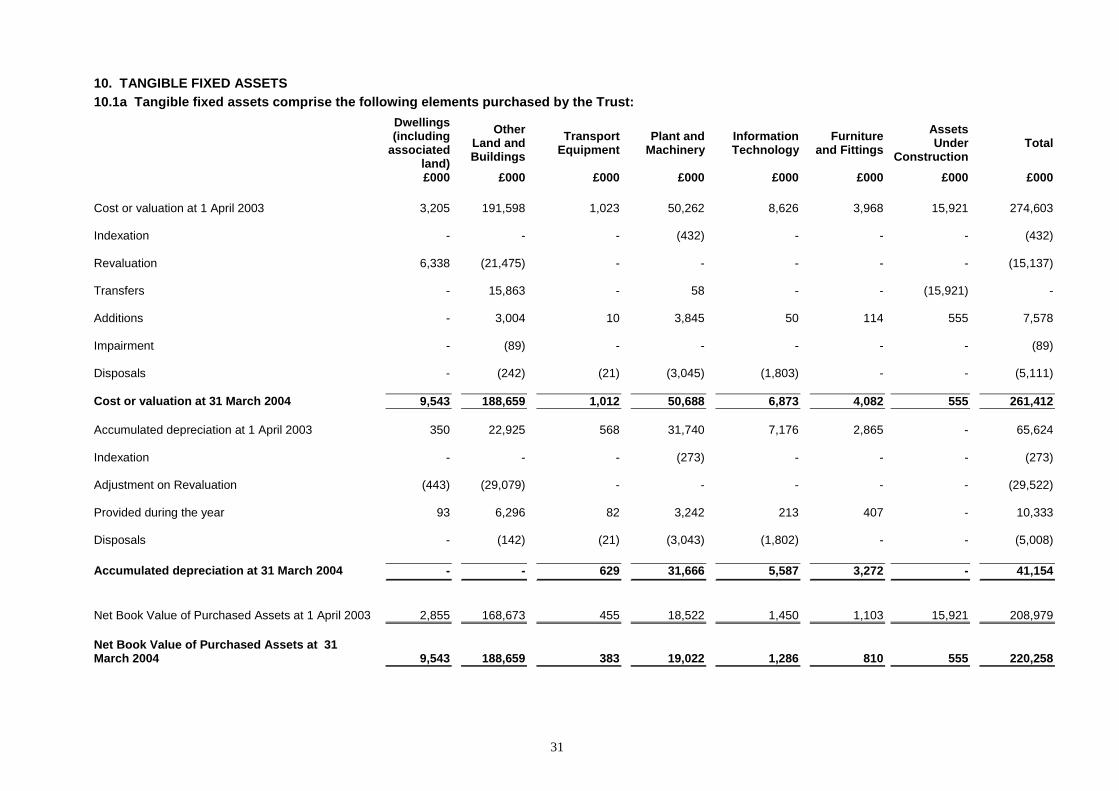
10. TANGIBLE FIXED ASSETS10.1a Tangible fixed assets comprise the following elements purchased by the Trust:
Dwellings(including
associatedland)
OtherLand andBuildings
TransportEquipment
Plant andMachinery
InformationTechnology
Furnitureand Fittings
AssetsUnder
ConstructionTotal
£000 £000 £000 £000 £000 £000 £000 £000
Cost or valuation at 1 April 2003 3,205 191,598 1,023 50,262 8,626 3,968 15,921 274,603
Indexation - - - (432) - - - (432)
Revaluation 6,338 (21,475) - - - - - (15,137)
Transfers - 15,863 - 58 - - (15,921) -
Additions - 3,004 10 3,845 50 114 555 7,578
Impairment - (89) - - - - - (89)
Disposals - (242) (21) (3,045) (1,803) - - (5,111)
Cost or valuation at 31 March 2004 9,543 188,659 1,012 50,688 6,873 4,082 555 261,412
Accumulated depreciation at 1 April 2003 350 22,925 568 31,740 7,176 2,865 - 65,624
Indexation - - - (273) - - - (273)
Adjustment on Revaluation (443) (29,079) - - - - - (29,522)
Provided during the year 93 6,296 82 3,242 213 407 - 10,333
Disposals - (142) (21) (3,043) (1,802) - - (5,008)
Accumulated depreciation at 31 March 2004 - - 629 31,666 5,587 3,272 - 41,154
Net Book Value of Purchased Assets at 1 April 2003 2,855 168,673 455 18,522 1,450 1,103 15,921 208,979
Net Book Value of Purchased Assets at 31March 2004 9,543 188,659 383 19,022 1,286 810 555 220,258

32
10.1b Tangible fixed assets comprise the following elements donated to the Trust:
Dwellings(including
associatedland)
Other Landand
BuildingsTransport
EquipmentPlant
andMachinery
InformationTechnology
FurnitureAnd
Fittings
AssetsUnder
ConstructionTotal
£000 £000 £000 £000 £000 £000 £000 £000
Cost or valuation at 1 April 2003 - 4,534 54 3,758 97 36 1,179 9,658Indexation - - - (36) - - - (36)Revaluation (461) - - - - - (461)Additions - 3,466 11 404 - - - 3,881Transfers - 1,179 - - - - (1,179) -Disposals - - - (90) - - - (90)
Cost or valuation at 31 March 2004 - 8,718 65 4,036 97 36 - 12,952
Accumulated depreciation at 1 April 2003 - 547 25 2,259 75 15 - 2,921Provided during the year - 170 6 283 9 3 - 471Indexation - - - (22) - - - (22)Adjustment on revaluation - (717) - - - - - (717)Disposals - - - (90) - - - (90)
Accumulated depreciation at 31 March 2004 - - 31 2,430 84 18 - 2,563
Net Book Value of Donated Assets at 1 April 2003 - 3,987 29 1,499 22 21 1,179 6,737
Net Book Value of Donated Assets as at 31 March 2004 - 8,718 34 1,606 13 18 - 10,389
Total Tangible Fixed Assets
Net Book Value at 1 April 2003 2,855 172,660 484 20,021 1,472 1,124 17,100 215,716
Net Book Value at 31 March 2004 9,543 197,377 417 20,628 1,299 828 555 230,647
Net book value of land included above
At 1 April 2003 174 8,621
At 31 March 2004 228 29,194

33
Of the total net book value at 31 March 2004, £1,910,000 related to land valued at open market value,and £nil related to buildings, installations and fittings valued at open market value.
10.2 Revaluation of Properties
A valuation of all properties, as at 31 March 2004, was carried out by The Valuation Office Agency,Chartered Surveyors. The valuation was the regular five year process and the effect of the valuation isshown below:
The total impact was an increase in value of £14,885,000, of which £14,540,000 was credited to therevaluation reserve (see note 15) and £89,000 was charged to the Operating Cost Statement.
10.3 Capital Commitments2004 2003£000 £000
Contracted 2,378 10,377
Included within contracted capital commitments is:• £1.4million (2003: £3.4million) relating to the construction of the replacement Roxburghe House
which is scheduled to open in June 2004; and• £0.5million (2003: nil) for a replacement tunnel washer for the laundry on the Foresterhill site.
This is expected to be operational by June 2004.
11. STOCKS AND WORK IN PROGRESS2004 2003£000 £000
Raw materials and consumables 2,854 2,915
34
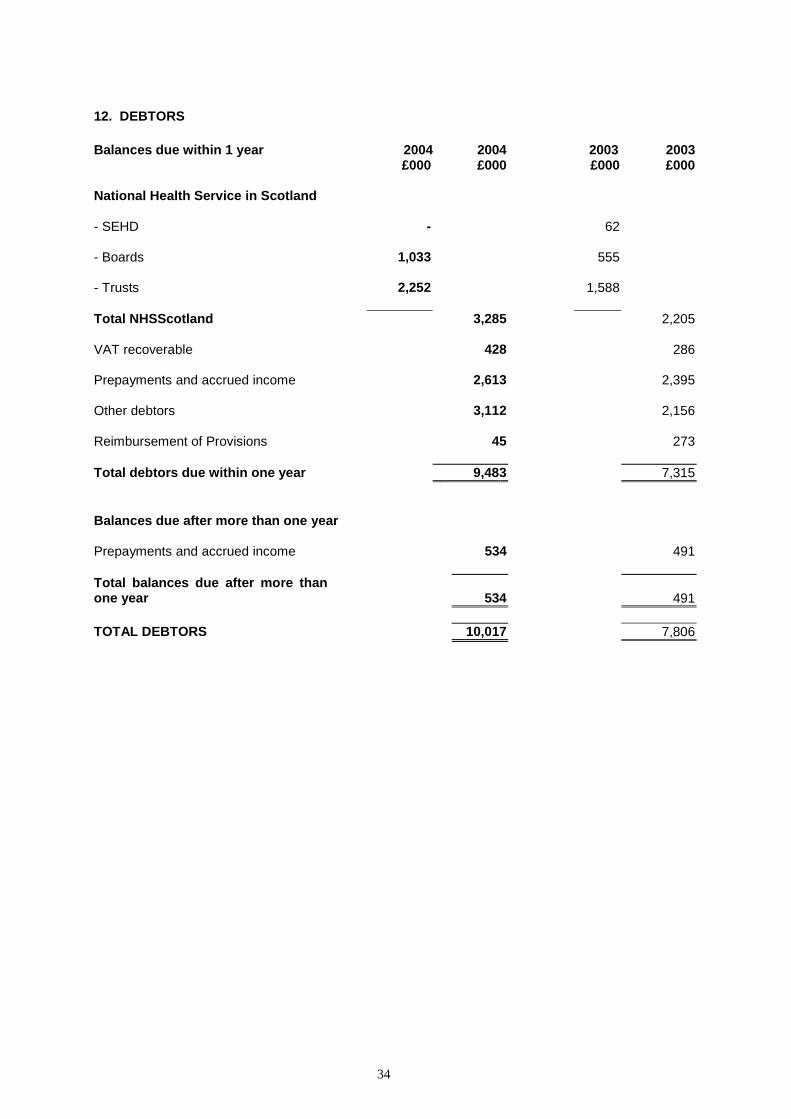
12. DEBTORS
Balances due within 1 year 2004 2004 2003 2003£000 £000 £000 £000
National Health Service in Scotland
- SEHD - 62
- Boards 1,033 555
- Trusts 2,252 1,588
Total NHSScotland 3,285 2,205
VAT recoverable 428 286
Prepayments and accrued income 2,613 2,395
Other debtors 3,112 2,156
Reimbursement of Provisions 45 273
Total debtors due within one year 9,483 7,315
Balances due after more than one year
Prepayments and accrued income 534 491
Total balances due after more thanone year 534 491
TOTAL DEBTORS 10,017 7,806

35
13. CREDITORS: AMOUNTS FALLING DUE WITHIN ONE YEAR
2004 2004 2003 2003£000 £000 £000 £000
National Health Service in Scotland
-SEHD - 513
-Boards 807 572
-Trusts 3,615 3,995
Total NHSScotland 4,422 5,080
General Fund Creditor 146 1,127
Trade Creditors 7,527 6,696
Accruals 12,551 3,794
Payments received on account 980 1,116
Income Tax & Social Security 4,414 3,824
Other creditors 1,380 1,314
VAT - 98
Total 31,420 23,049
14. PROVISIONS FOR LIABILITIES AND CHARGES
Pension and Clinical/Similar Medical
Obligations Negligence Total£000 £000 £000
As at 1 April 2003 214 646 860
Arising during the year 39 218 257
Utilised during the year (40) (164) (204)
Reversed Unutilised - (228) (228)
As at 31 March 2004 213 472 685

36
15. MOVEMENTS ON RESERVES
The movements on reserves in the year comprised the following:
RevaluationReserve
DonatedAsset
Reserve£000 £000
As at 1 April 2003, as previously stated 22,658 6,737
Prior period adjustment (2,205) -
As at 1 April 2003, as restated 20,453 6,737
Indexation/revaluation of fixed assets 14,226 242
Transfer of realised element to general fund (238) -
Additions of donated assets - 3,881
Depreciation of donated assets - (471)
As at 31 March 2004 34,441 10,389

37
16. NOTES TO THE CASH FLOW STATEMENT
16.1 Reconciliation of operating cost to operating cash flows
2003-04 2002-03£000 £000
Net operating cost (277,520) (260,233)
Adjustments for Non Cash Items: Effect of revaluation of property 89 7,278 (Profit) on disposal of fixed assets (1,669) (736) Total Non Cash Items (279,100) (253,691)
Adjustments for movement in working capital Decrease/(increase) in stocks 61 (574) (Increase) in debtors (2,192) (2,150) Increase in creditors 14,406 3,433 (Decrease)/increase in provisions (175) 416Net decrease in working capital 12,100 1,125
Net cash outflow from operating activities (267,000) (252,566)
16.2 Analysis of changes in net cash
Opening Cash Other ClosingBalance Flows non cash Balance
1 April 2003 movements 31 March 2004£000 £000 £000 £000
Cash at bank and in hand 1,127 (981) - 146
TOTAL 1,127 (981) - 146
17. CONTINGENT LIABILITIES
The following contingent losses have not been accrued:
Nature £000
A number of claims for clinical negligence against the Trust which the CentralLegal Office of the Scottish Executive Health Department estimates there is amedium risk of the Trust having to make a settlement.
£2,404
There are also further claims for negligence against the Trust that the Central Legal Office of theScottish Executive Health Department estimates there is a low risk of the Trust having to make asettlement.

38
18. PENSIONS
The Trust participates in the National Health Service Superannuation Scheme for Scotland, which is anotional defined benefit scheme where contributions are credited to the Exchequer and the balance inthe account is deemed to be invested in a portfolio of Government securities. The pension cost isassessed every five years by the Government Actuary; details of the most recent actuarial valuation canbe found in the separate statement of the Scottish Public Pensions Agency (SPPA).
The National Health Service Superannuation Scheme for Scotland is a multi-employer scheme wherethe share of the assets and liabilities applicable to each employer is not identified. The Trust willtherefore account for its pension costs on a defined contribution basis as permitted by FinancialReporting Standard 17.
For 2003-04, normal employer contributions of £7,676,000 were payable to the SPPA at the rate of5.5% of total pensionable salaries (prior year £6,892,000 at a rate of 5.5%). In addition, during theaccounting period the Trust incurred additional costs of £155,000 (prior year £305,000) arising from theearly retirement of staff. The most recent actuarial valuation discloses a balance of £934 million to bemet by future contributions from employing authorities. As a consequence of the valuation, employerssuperannuation contributions increased to 14% on 1 April 2004.
At 31 March 2004, the balance sheet included provisions of £213,000, accruals of £763,000 andprepayments of £nil in respect of pension costs. The equivalent values at 31 March 2003 were£214,000, £858,000 and £nil, respectively.
The scheme provides benefits on a “final salary” basis at a normal retirement age of 60. Annualbenefits are normally based on 1/80th of the best of the last three years pensionable pay for each yearof service. In addition, a lump sum equivalent to three years’ pension is payable on retirement.Members pay contributions of 6% (5% for manual staff) of pensionable earnings. Pensions areincreased in line with Retail Prices Index.
On death, pensions are payable to the surviving spouse at a rate of half the member’s pension. Ondeath in service, the scheme pays a lump-sum benefit of twice pensionable pay and also provides aservice enhancement on computing the spouse’s pension. The enhancement depends on length ofservice and cannot exceed 10 years. Child allowances are payable according to the number ofdependant children and whether there is a surviving parent who will get a scheme widow/ widower’spension. Medical retirement is possible in the event of serious ill health. In this case, pensions arebrought into payment immediately where the member has more than 2 years service. Where serviceexceeds 5 years, the pension is calculated using specially enhanced service, with a maximumenhancement of 10 years.
Members aged 50 or above may take voluntary early retirement and receive a reduced pension.Alternatively, if the employer agrees to this the member will be able to retire on the full pension andlump sum which they have earned.

39
19. RECONCILIATION OF MOVEMENT IN GENERAL FUND
£000 £000General Fund as at 1 April 2003 Public Dividend Capital 180,149 Other (3,684) Total 176,465
Opening General Fund Creditor 1,127Add Cash drawn down 276,906Less Closing General Fund (Creditor) (146)Net Funding 277,887Net Operating Cost (277,520)Depreciation due to SEHD (10,333)Transfer of realised element of revaluation reserve 238
Net (decrease) in General Fund (9,728)
General Fund at 31 March 2004 Public Dividend Capital 180,149 Other (13,412)
Total 166,737
20. VOLUNTARY CONTRIBUTIONS
During the year the Trust received financial support from various voluntary sources includingendowment funds.
When these funds were used for capital purposes, the associated asset has been included in theaccounts and disclosed in the notes as a donated asset. Voluntary contributions which were usedfor revenue purposes are excluded from both the accounts and the notes to the accounts.
The Trust's endowment funds are a recognised charity and prepare an annual report and accountsin accordance with the appropriate legislation.
21. PRIOR YEAR ADJUSTMENT
Changes that have been made to the Prior Year figures from the published annual accounts are:
Asset RevaluationThe prior year adjustment relates to a transfer between the Revaluation Reserve and the GeneralFund for assets re-valued in 2002/03.
PrincipleStatement
NoteNumber
As stated inPrior YearAccounts
£000Adjustment
£000
Re-stated inCurrent Year
Accounts£000
Balance Sheet 15 22,658 (2,205) 20,45319 174,260 2,205 176,465





























