Embed Size (px)
Citation preview
GRAM-POSITIVE BACILLI I
Spore-forming bacilli Non-spore-forming bacilli
Bacillus anthracis Corynebacterium diptheriae
Bacillus cereus Listeria monocytogenes
Actinomyces
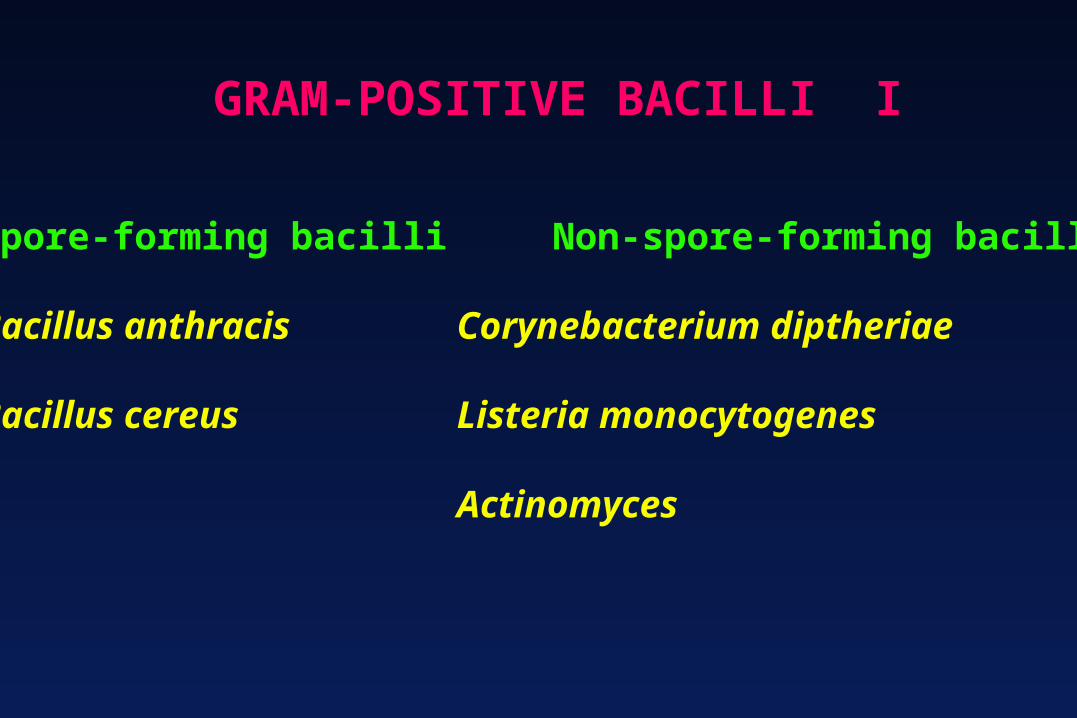
BACILLUS ANTHRACIS
1915 German agents in the US believed to have injected horses, mules and cattle with anthrax on their way to Europe during World War I
1937 Japan starts biological warfare program in Manchuria
1942 UK experiments with anthrax at Gruinard Island off the coast of Scotland (only recently decontaminated)
1943 United States begins developing anthrax weapons
1945 Anthrax outbreak in Iran kills 1 million sheep
1969 US biological weapons program ends

1972 International convention outlaws development and stokpiling of biological weapons
1978-80 Human anthrax epidemic in Zimbabwe infects 6,000 and killing 100
1979 Aaerosolized anthrax spores are released accidentally at a Soviet Union military facility, killing 68 people
1991 US troops vaccinated for anthrax in preparation for Gulf War
1995 Iraq admits it produced 8,500 liters of concentrated anthrax
1998 Anthrax vaccination approved by for all military service members

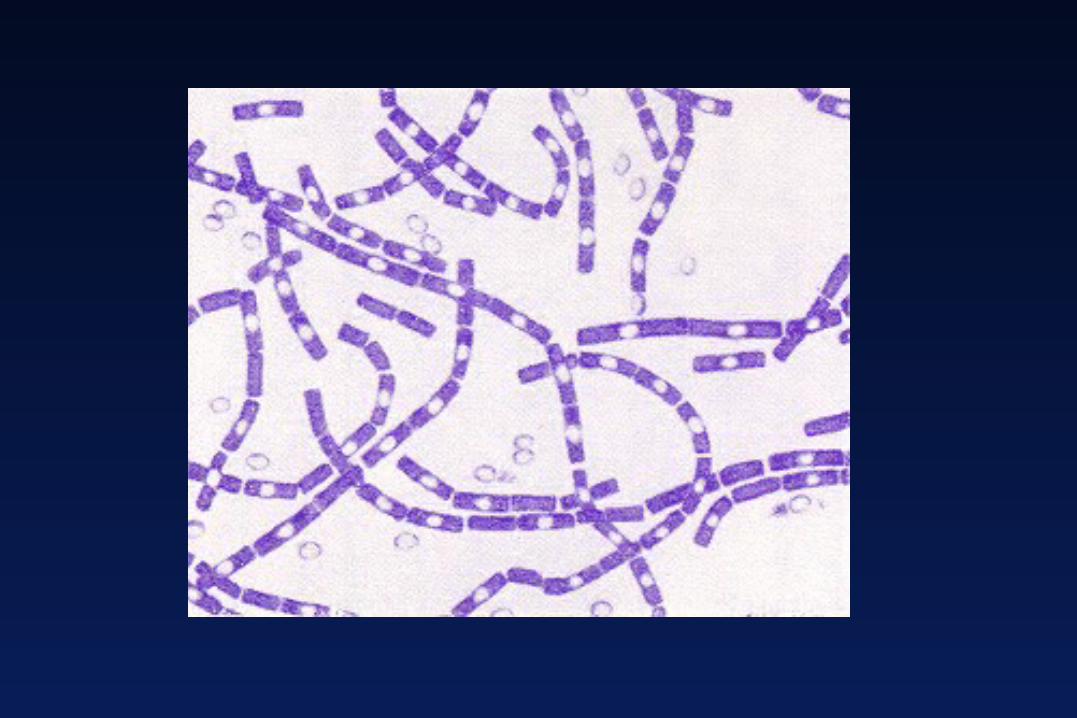
BACILLUS ANTHRACIS
Form spores aerobically
Prominent polypeptide capsule composed ofD-glutamate residues
Capsule is antiphagocytic
Antibodies against capsule are not protective
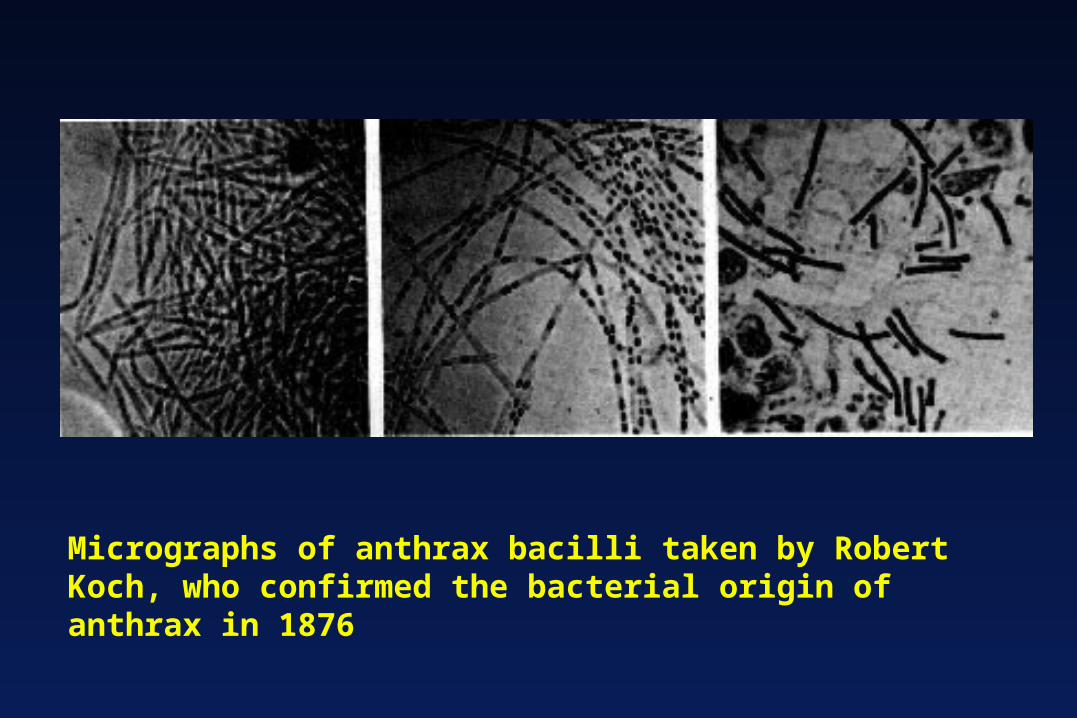
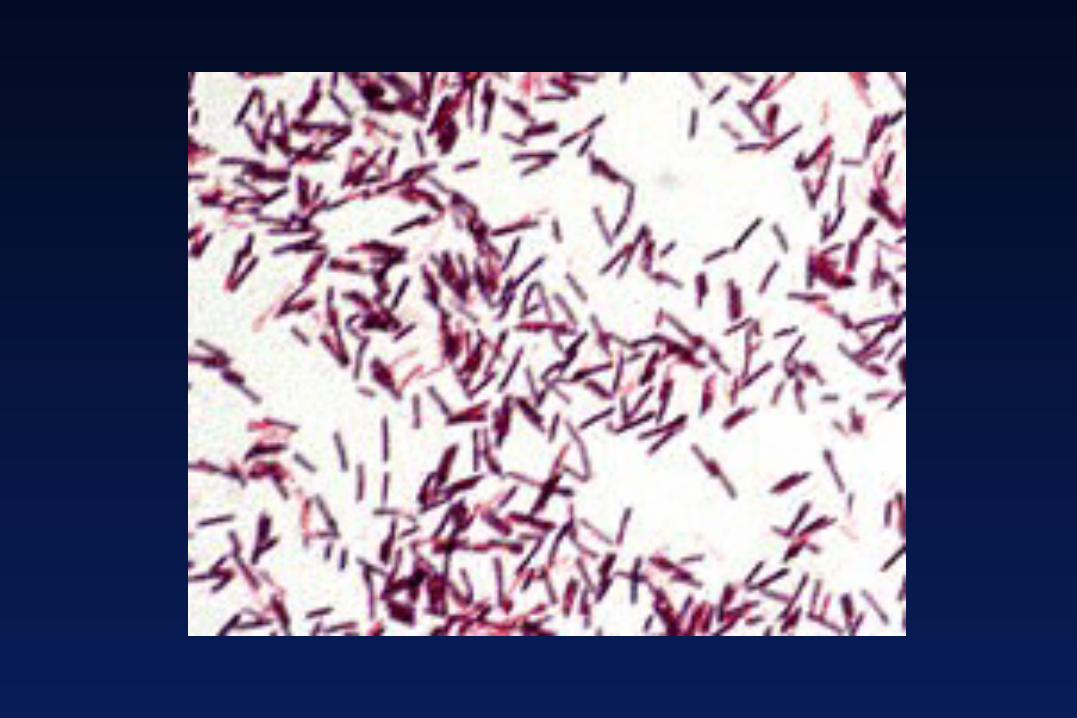
Micrographs of anthrax bacilli taken by Robert Koch, who confirmed the bacterial origin of anthrax in 1876
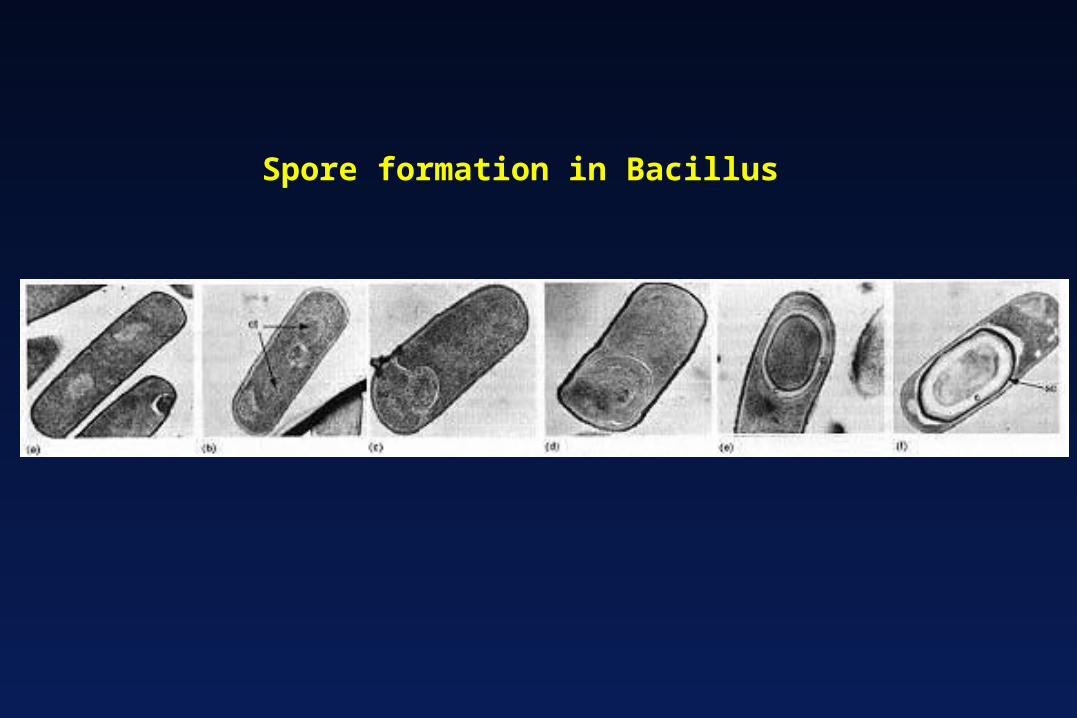
Spore formation in Bacillus

Mucoid type colonies of encapsulated Bacillus

Bacillus anthracis capsule visualized by India Ink negative stain

BACILLUS ANTHRACIS
Pathogenesis
Virulence factors:
Capsule composed of poly-D-glutamic acid
Anthrax toxin

“Anthrax toxin” consists of 3 proteins encoded by a large plasmid, pXO1
1. Protective antigen (PA)
2. Lethal factor (LF)
3. Edema factor (EF)
Non-toxic individually

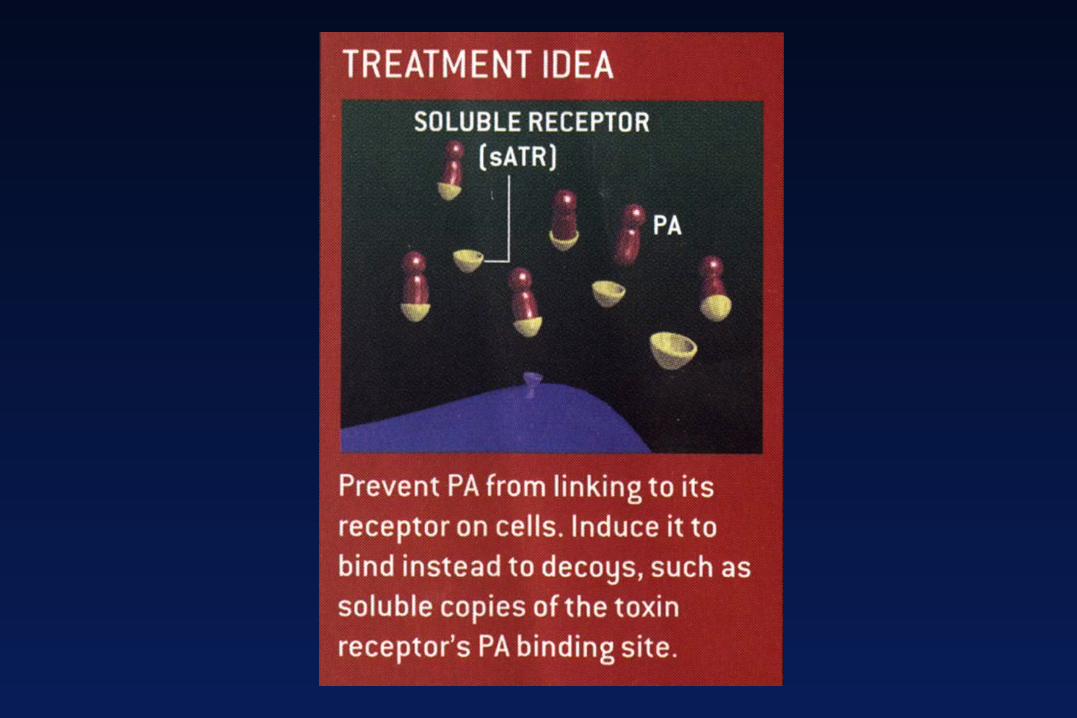
Protective antigen (PA) facilitates cell entry of the other toxins.
Binds to 2 types of receptors on cell surfaces:
Tumor endothelial marker 8 (TEM8) (anthrax toxin receptor) and Capillary morhpogenesis protein
Present on cells in the heart, brain, intestine, lung, skeletal muscle, pancreas, macrophages

After receptor binding, PA is cleaved by cellular proteases, and forms a heptameric “prepore”
LF or EF bind to the heptamer and are endocytosed
In the acidified endosome, the prepore transforms into a pore, releasing the factors into the cell

Lethal factor
A zinc metalloproteaseCleaves the phosphokinase that activates the
mitogen-activated protein kinase (MAPK) signal transduction pathway
Cleavage of phosphokinase inhibits cell growth 3. Edema factor: An adenylate cyclase dependent on protective antigen for binding and entry into the cell

Edema factor
An adenylate cyclase
Increases intracellular cAMP
Related to the enzyme produced by Bortedella pertussis and Pseudomonas aeruginosa




BACILLUS ANTHRACIS
Transmission
Through exposed skin or mucous membranes, from contaminated soil or infected animal products or by contact with sick animals
Inhalation: rare in humans, more common in herbivores

BACILLUS ANTHRACIS
Clinical syndromes
Cutaneous anthraxSpores entering abrasions in the skinPainless ulcer with a black eschar (scab)Local edemaCalled "malignant pustule"Can lead to death in 20% of patients if untreated
BACILLUS ANTHRACIS
Clinical syndromes
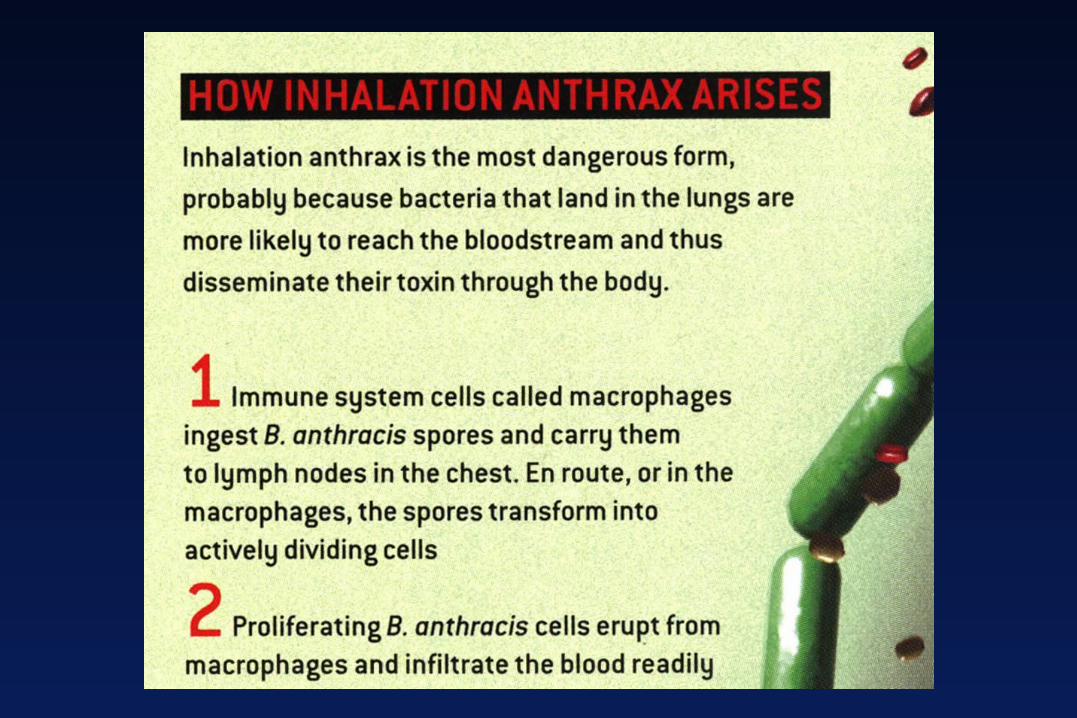
Inhalation anthrax(pulmonary anthrax, "Woolsorter's disease”)Initially appears like a viral respiratory illnessCan progress to diffuse pulmonary disease with
respiratory failureMortality rate is high (>95% if untreated)

Treatment and control
Early antibiotic treatment of anthrax is essentialCiprofloxacin is the drug of choice
Penicillin, doxycycline, erythromycin, or chloramphenicol may be used if susceptible
Vaccination of animal herds and people in endemic areas
Burning or burial of animals that die of anthrax
BACILLUS ANTHRACIS

BACILLUS CEREUS
Causes:
Food poisoningGastroenteritisOcular infectionsIntravenous catheter-mediated sepsis
BACILLUS CEREUS
Pathogenesis
Spores can survive in soil Heat stable enterotoxin: Acts as a superantigen
Causes gastroenteritis with vomiting
Heat labile enterotoxin: ADP-ribosylates a G protein > stimulates adenylate cyclaseCauses the diarrhea and fluid loss

Transmission and clinical syndromes
Ingestion (food poisoning)Emetic (vomiting) form caused by
contaminated riceHeat-resistant spores survive and germinate Nausea, vomiting, and abdominal cramps
Diarrheal formTransmitted via contaminated meat, vegetables
or sauces
BACILLUS CEREUS

Treatment & Prevention
Symptomatic treatment
Proper refrigeration of food
Rice should not be kept warm for long periods
BACILLUS CEREUS

BACILLUS
Bacillus species used in sterilization monitoring
B. stearothermophilus sporesMonitoring proper sterilization in an autoclave 121-132oC for 15 minThen placed in medium at 37oC to grow
B. subtilis sporesMonitoring sterilization by dry heat171oC for 1 h or 160oC for 2 h

CORYNEBACTERIUM DIPHTHERIAE
CORYNEBACTERIUM DIPHTHERIAE
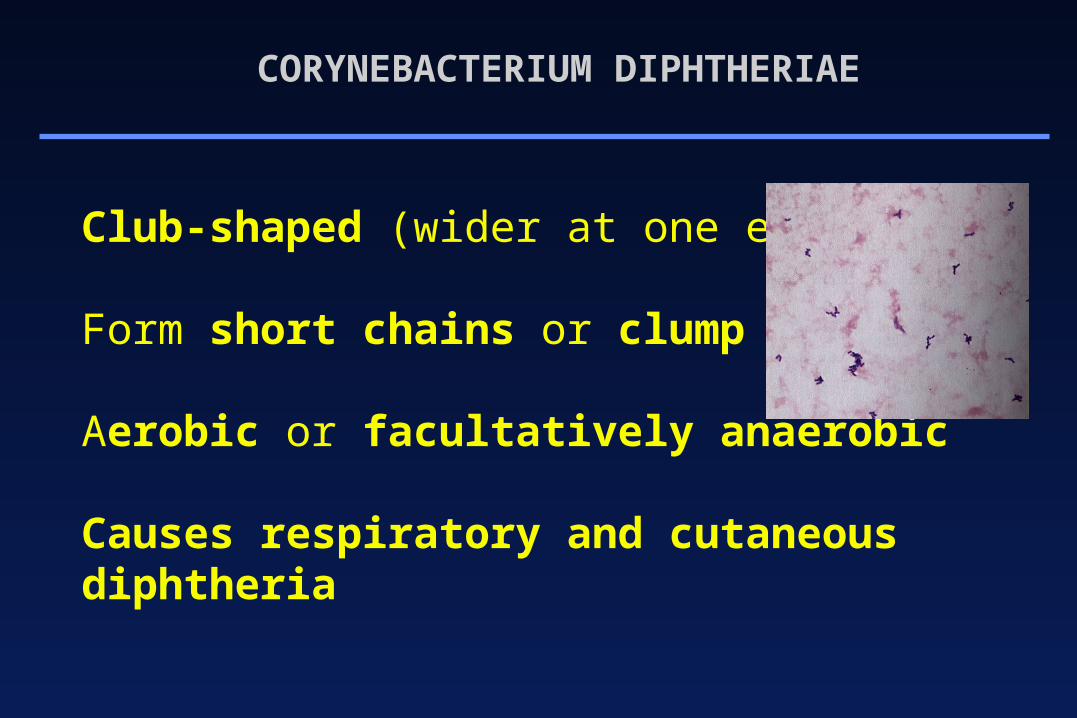
Club-shaped (wider at one end) rods
Form short chains or clump together
Aerobic or facultatively anaerobic
Causes respiratory and cutaneous diphtheria

CORYNEBACTERIUM DIPHTHERIAE
Pathogenesis
Exotoxin secreted by the bacterium
The "tox" gene introduced into strains ofC. diphtheriae by a lysogenic phage(beta phage)
CORYNEBACTERIUM DIPHTHERIAE
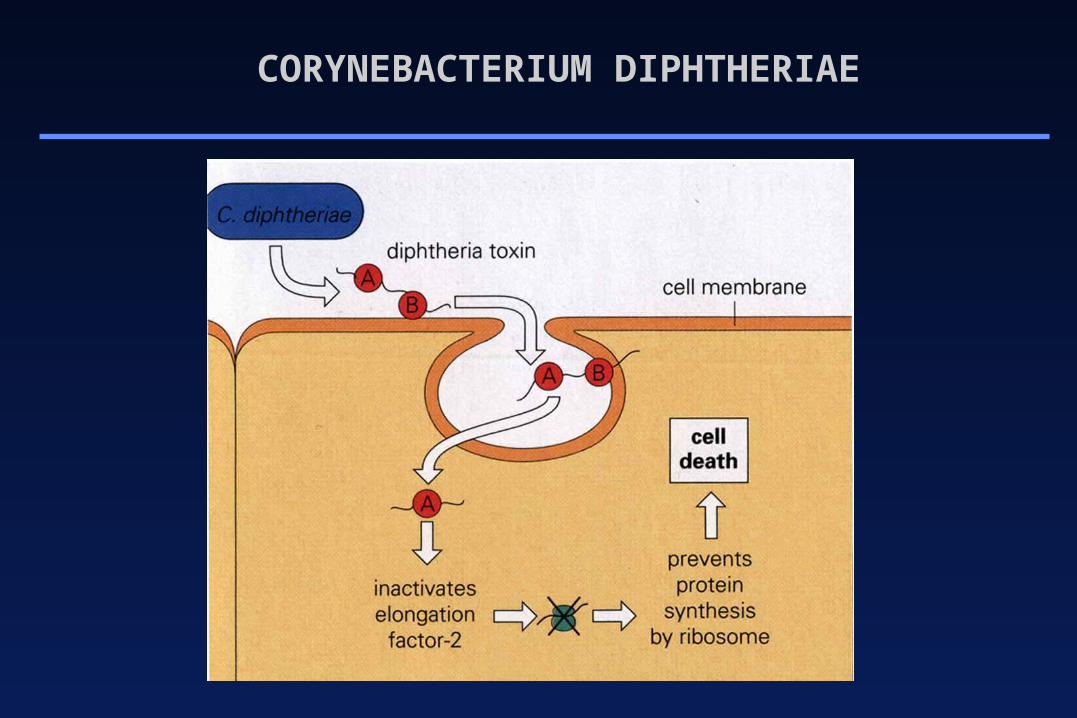
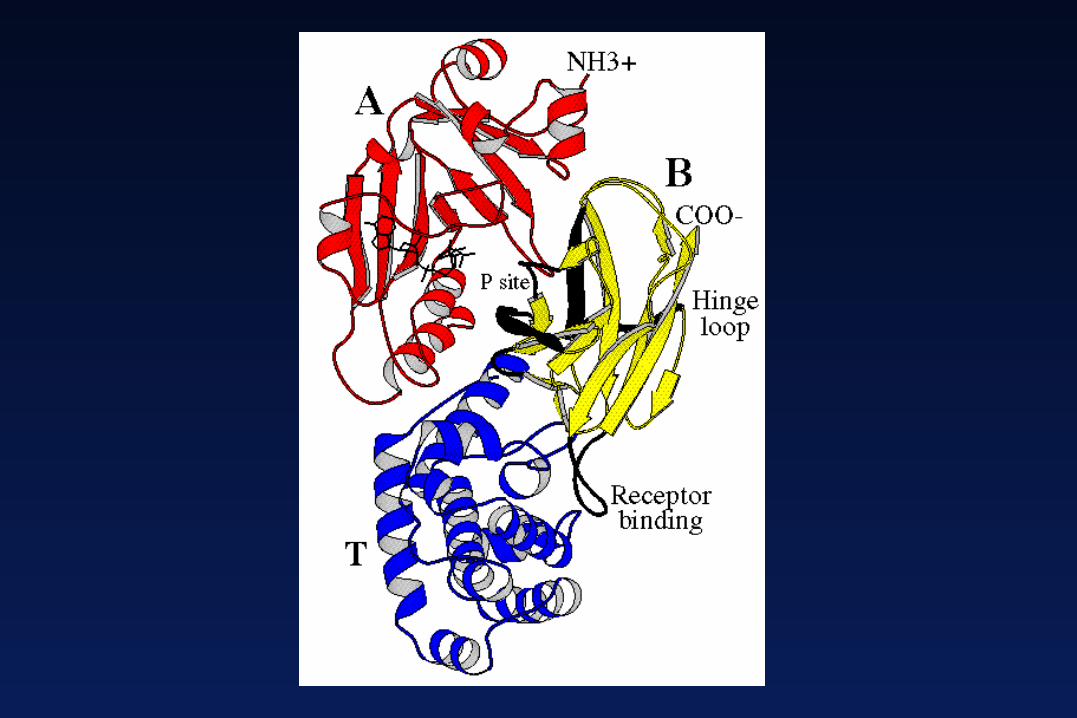
Exotoxin
B subunitreceptor binding domainmembrane translocation domain
A subunitADP-ribosylation of elongation factor 2 (EF-2)
CORYNEBACTERIUM DIPHTHERIAE

CORYNEBACTERIUM DIPHTHERIAE
CORYNEBACTERIUM DIPHTHERIAE
Transmission
Inhalation of airborne droplets
Skin contact at the site of a pre-existing lesion
Humans are the only natural host

CORYNEBACTERIUM DIPHTHERIAE
Clinical syndromes
Respiratory diphtheriamalaise, sore throatexudative pharyngitislow-grade feverthick "pseudomembrane”
bacteria, lymphocytes, plasma cells, fibrin, dead cells
may cause airway obstruction

CORYNEBACTERIUM DIPHTHERIAE

CORYNEBACTERIUM DIPHTHERIAE
Clinical syndromes
Cutaneous diphtheriaentry into subcutaneous tissue through breaks in
the skinpapule which evolves into a non-healing ulcer
sometimes covered with a grayish membrane
CORYNEBACTERIUM DIPHTHERIAE
Treatment and control
Early administration of diphtheria antitoxin
Penicillin G or erythromycin to eliminate the organism and terminate toxin production
Active immunization with diphtheria toxoid during childhood (as part of the DPT vaccine) and with booster shots every 10 years
LISTERIA MONOCYTOGENES
Non-spore forming
Facultatively anaerobic small coccobacilli
Causes meningitis and bacteremia
Found in water, soil and the GI tracts of humans and animals

LISTERIA MONOCYTOGENES

LISTERIA MONOCYTOGENES
Human disease restricted to
neonates and the elderly
pregnant women
immunocompromised patientsdefective cell-mediated immunity
LISTERIA MONOCYTOGENES
Pathogenesis
Can grow in macrophages and epithelial cells
Virulent strains produce listeriolysin O, a hemolysin Phospholipase C
Can replicate at 4-8 oC


Growth at 4˚C

LISTERIA MONOCYTOGENES
TransmissionContaminated food
milk, soft cheese, undercooked meat, unwashed raw vegetables, cabbage
From bacteremic mother to fetusThe incidence of disease in AIDS patients is 100-
fold greaterMortality rate (20-30%) higher than most other food-
borne diseases.

LISTERIA MONOCYTOGENES
Clinical syndromesNeonatal diseaseEarly onset disease (granulomatosis infantiseptica)
acquired transplacentally in uterodisseminated abscesses and granulomas in multiple tissues
Late-onset diseaseacquired soon after birthmeningitis or meningoencephalitis
with septicemia

LISTERIA MONOCYTOGENES
Clinical syndromesDisease in adults
mild, influenza-like illness in healthy adultssevere illness in immuno-compromised patients meningitisshould be suspected in organ transplant patients,
patients with cancer, or pregnant women developing meningitis
bacteremiahigh-grade fever and hypotension in acute cases
LISTERIA MONOCYTOGENES
Treatment and control
Penicillin or Ampicillin, either alone or with gentamicin
Trimethoprim-sulfamethoxazole
Avoid raw or partially cooked foods of animal origin, soft cheese or unwashed raw vegetables
ACTINOMYCES

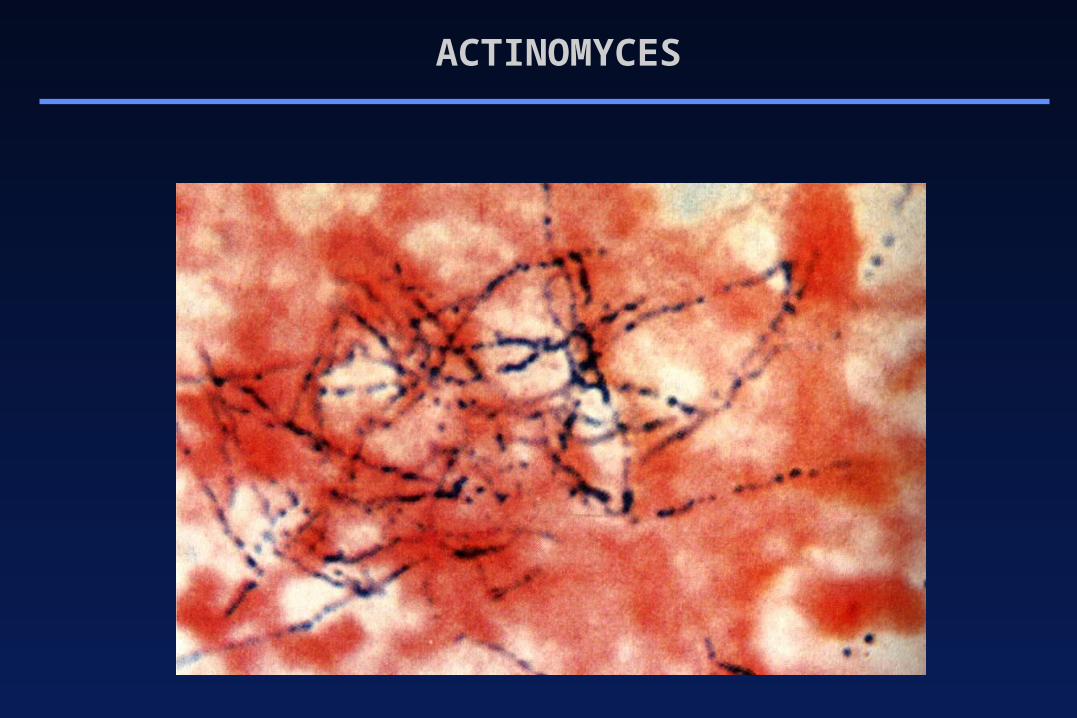
Delicate filamentous forms (hyphae)Actinomyces = "ray fungus" (Gr.)Gram-positive bacilliFacultative anaerobic or strict anaerobic
Form long branching filaments (not acid-fast)
Produce slowly-developing chronic infections
Most human infections are caused by Actinomyces israelii
Actinomyces

Gram stain of Actinomyces in pus
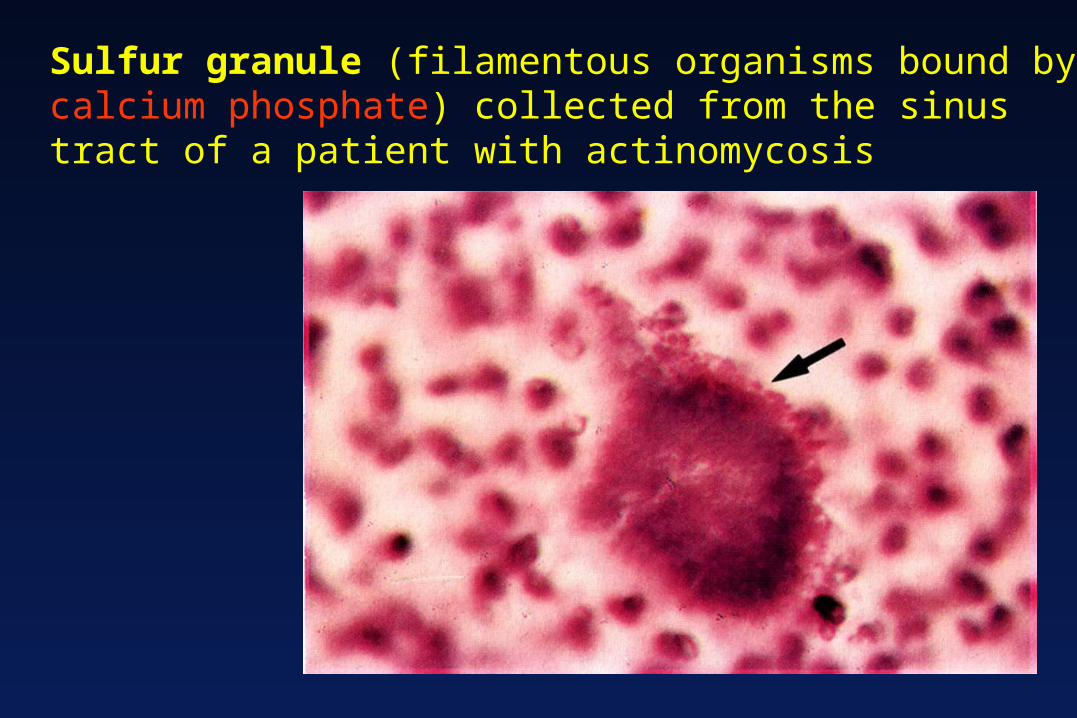
Sulfur granule (filamentous organisms bound by calcium phosphate) collected from the sinus tract of a patient with actinomycosis
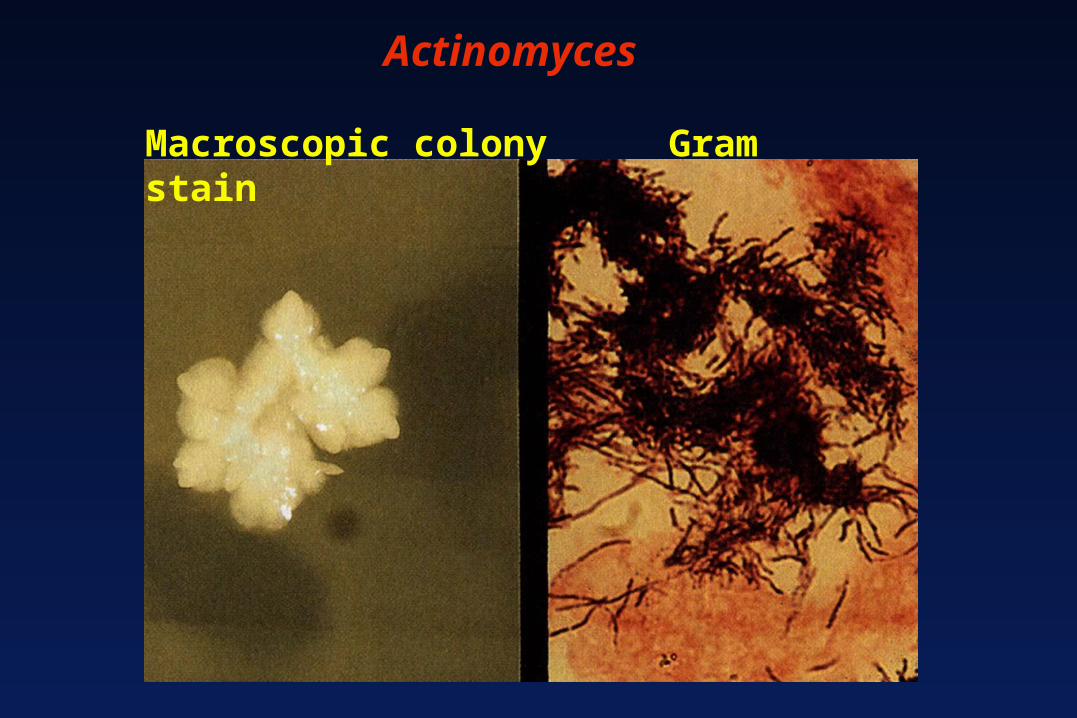
Actinomyces
Macroscopic colony Gram stain
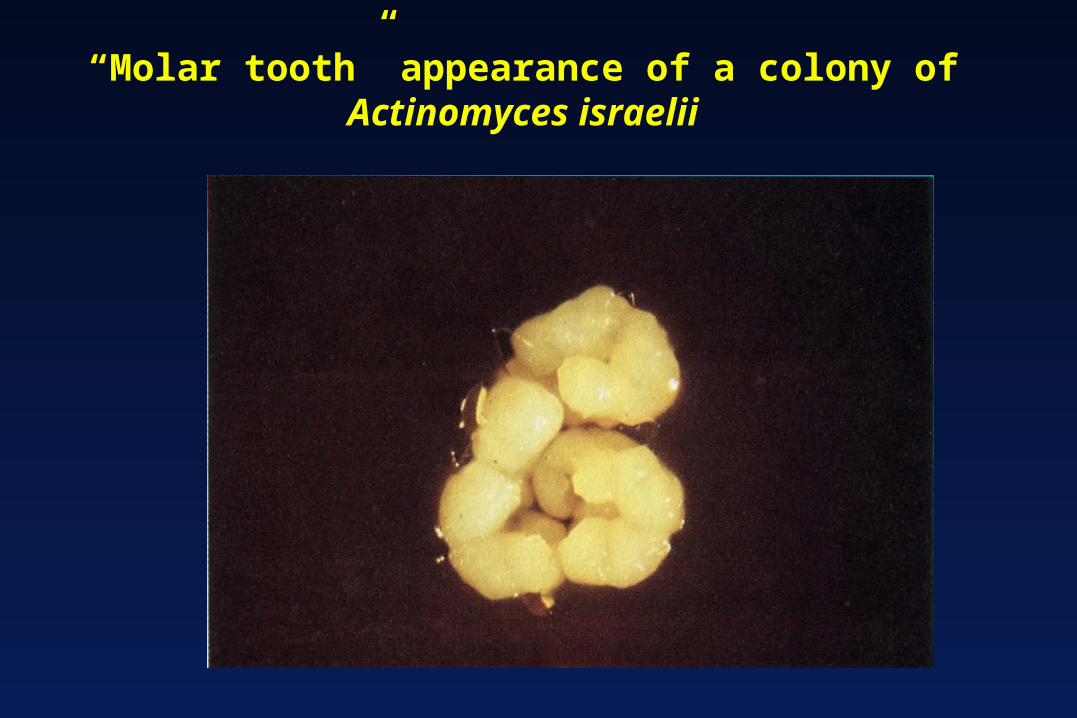
“Molar tooth” appearance of a colony ofActinomyces israelii

Pathogenesis
Cause opportunistic infections ofupper respiratory tractgastrointestinal tractfemale genital tract
when normal mucosal barriers are disrupted
Actinomycosis is characterized by multiple abscesses connected by sinus tracts
Actinomyces
Epidemiology
Endogenous infection
Cervicofacial actinomycosis may occur after dental procedures
The dentist may be the first to diagnose the swelling due to this condition
Thoracic actinomycosis is established via inhalation or via the bloodstream
Actinomyces

Epidemiology
Abdominal infections usually caused by surgery or trauma
Pelvic infections may result from abdominal infections or intrauterine devices
Central nervous system infections spread from other locations
Actinomyces

Actinomyces has colonized the surface of an intrauterine device, leading to the development of
pelvic actinomycosis
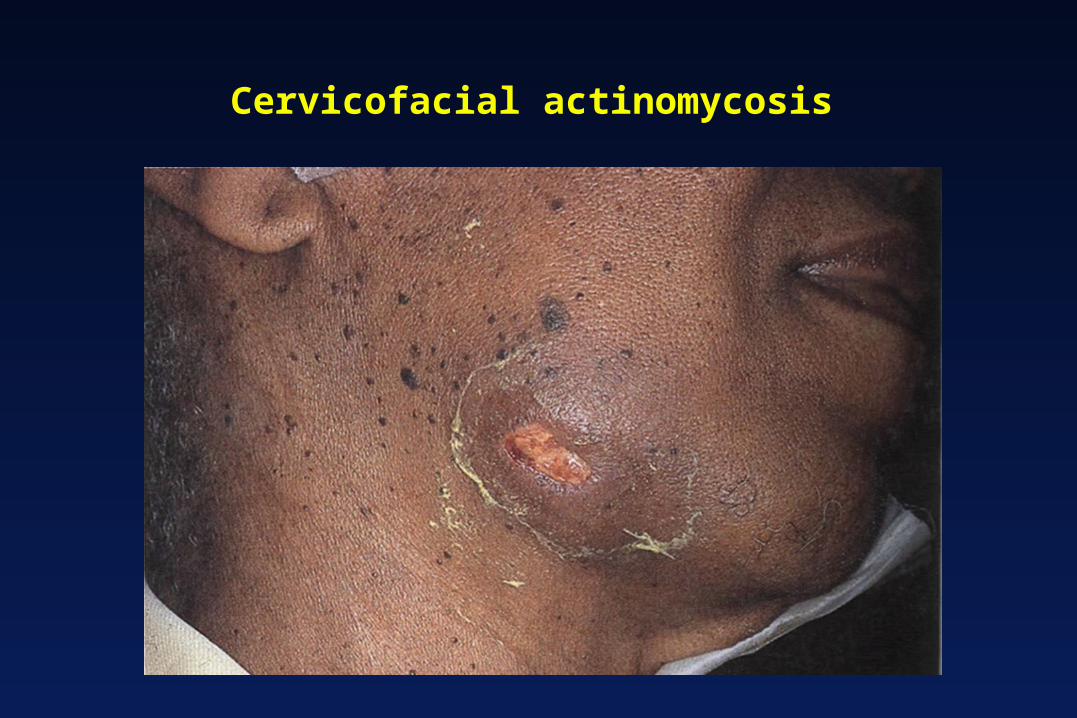
Cervicofacial actinomycosis

Treatment and control
Surgical debridement and long-term administration of penicillin G (or tetracycline, erythromycin or clindamycin)
An undrained focus must be suspected if If infections do not respond to prolonged therapy
Good oral hygiene is necessary for prevention Antibiotic prophylaxis before oral operations
Actinomyces