-
8/11/2019 Graham 2014 Bifosfonato
1/15
-
8/11/2019 Graham 2014 Bifosfonato
2/15
-
8/11/2019 Graham 2014 Bifosfonato
3/15
-
8/11/2019 Graham 2014 Bifosfonato
4/15
tant to know what happens during long-term adminis-
tration. From a clinical point of view, it is reassuring
that
the inhibition of bone resorption reaches a new steady-
state level rather than becoming progressively lower,
even when the compounds are given continuously.27
The level of suppression depends on the administered
dose and has also been observed in humans.28 There
seems to be no progression of the antiresorptive effectwith
time, which suggests that the bisphosphonate bur-
ied in the bone is inactive for at least as long as it
remains
buried there. This also means that within the therapeu-
tic-dosage range, there is little risk of a continuous and
progressive decrease in bone turnover in the long run
that might lead to an increase in bone fragility. An
additional important pharmacologic property of bisphos-
phonates is that the total dose administered is a major
determinant of their effects. This has been well studied
for ibandronate29 and zoledronate.30 In both cases the
same inhibition of bone resorption has been docu-
mented regardless of whether the bisphosphonate wasgiven in
small frequent (eg, daily) doses compared with
larger doses given less frequently. This was the basis for
the development of intermittent-dosing regimens in hu-
mans.
The pronounced selectivity of bisphosphonates for
bone rather than other tissues is the basis for their value
in clinical practice. Their preferential uptake by and
adsorption to mineral surfaces in bone bring them into
close contact with osteoclasts. During bone resorption,
bisphosphonates are probably internalized by endocyto-
sis along with other products of resorption. Many studies
have shown that bisphosphonates can affect osteoclast-mediated
bone resorption in a variety of ways, including
effects on osteoclast recruitment, differentiation, and re-
sorptive activity, and may induce apoptosis.
Because mature, multinucleated osteoclasts are
formed by the fusion of mononuclear precursors of he-
matopoietic origin, bisphosphonates could also inhibit
bone resorption by preventing osteoclast formation, in
addition to affecting mature osteoclasts. In vitro,
bisphosphonates can inhibit dose-dependently the for-
mation of osteoclast-like cells in long-term cultures of
human bone marrow.31 In organ culture, also, some
bisphosphonates can inhibit the generation of mature
osteoclasts, possibly by preventing the fusion of oste-
oclast precursors.32,33
It is likely that bisphosphonates are selectively inter-
nalized by osteoclasts rather than other cell types be-
cause of their accumulation in bone and the endocytic
activity of osteoclasts. During the process of bone resorp-
tion, the subcellular space beneath the osteoclast is acid-
ified by the action of vacuolar-type proton pumps in the
ruffled border of the osteoclast membrane.34 The acidic
pH of this microenvironment causes dissolution of the
hydroxyapatite bone mineral, whereas the breakdown
of the extracellular bone matrix is brought about by the
action of proteolytic enzymes, including cathepsin K.
Because bisphosphonates adsorb to bone mineral, espe-
cially at sites of bone resorption where the mineral is
most exposed,35,36 osteoclasts are the cell type in bone
most likely to be exposed to the highest concentrations
of free, nonmineral-bound bisphosphonate as a result
of the release of the bisphosphonate from bone mineral
in the low-pH environment beneath osteoclasts. It hasbeen
estimated that pharmacologic doses of alendronate
that inhibit bone resorption in vivo could give rise to
local concentrations as high as 1 mM alendronate in the
resorption space beneath an osteoclast, which is much
higher than the concentrations of bisphosphonates re-
quired to affect osteoclast morphology and cause oste-
oclast apoptosis in vitro.37
In contrast to their ability to induce apoptosis in os-
teoclasts, which contributes to the inhibition of resorp-
tive activity, some experimental studies suggest that
bisphosphonates may protect osteocytes and osteoblasts
from apoptosis induced by glucocorticoids.38
Recent ev-idence suggests that the inhibition of osteocyte
apoptosis
by bisphosphonates is mediated through the opening of
connexion 43 hemichannels and activation of extracel-
lular signal-regulated kinases.39 The possibility that
bisphosphonates used clinically may get access to osteo-
cytes differentially depending on their mineral-binding
affinities and inherent structural properties needs to be
studied.
STRUCTURE-ACTIVITY RELATIONSHIPS ANDMECHANISMOF
ACTION
The features of the bisphosphonate molecule necessaryfor
biological activity were well defined in the early
studies. The P-C-P moiety is responsible for the strong
affinity of the bisphosphonates for binding to hydroxy-
apatite and allows for a number of variations in structure
on the basis of substitution in the R1 and R2 positions on
the carbon atom (Fig 1). The ability of the bisphospho-
nates to bind to hydroxyapatite crystals and to prevent
both crystal growth and dissolution was enhanced when
the R1 side chain (attached to the geminal carbon atom
of the P-C-P group) was a hydroxyl group (as in eti-
dronate) rather than a halogen atom such as chlorine (as
in clodronate). The presence of a hydroxyl group at the
R1 position increases the affinity for calcium (and, thus,
bone mineral) because of the ability of bisphosphonates
to chelate calcium ions by tridentate rather than biden-
tate binding.40
The ability of bisphosphonates to inhibit bone resorp-
tion in vitro and in vivo also requires the P-C-P struc-
ture. Monophosphonates (eg, pentane monophospho-
nate) or P-C-C-P or P-N-P compounds are ineffective as
inhibitors of bone resorption. Furthermore, the antire-
sorptive effect cannot be accounted for simply by adsorp-
tion of bisphosphonates to bone mineral and prevention
of hydroxyapatite dissolution. It became clear that
S152 RUSSELLat Pontificia Universidad Catolica de Chile on
August 18, 2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
5/15
bisphosphonates must inhibit bone resorption by cellular
effects on osteoclasts rather than simply by physico-
chemical mechanisms.
After the successful clinical use of clodronate and
etidronate in the 1970s and 1980s, more potent antire-
sorptive bisphosphonates, which had different R2 side
chains but in which R1 was unaltered, were studied. In
particular, bisphosphonates containing a basic primary
amino-nitrogen atom in an alkyl chain (as in pamidr-
onate and alendronate) were found to be 10- to 100-fold
more potent than etidronate and clodronate. Then, in
the 1980s, there was a phase in which synthesis of novel
compounds took place specifically to determine their
possible effects on calcium metabolism, with the result
that compounds highly effective as inhibitors of bone
resorption were identified and studied.
These compounds, especially those that contain a ter-
tiary amino-nitrogen (such as ibandronate41 and olpad-
ronate42), were even more potent at inhibiting bone
resorption. Among this generation of compounds that
were synthesized to optimize their antiresorptive effects,
the most potent antiresorptive bisphosphonates were
those containing a nitrogen atom within a heterocyclic
ring (as in risedronate43 and zoledronate44), which are up
to 10 000-fold more potent than etidronate in some
experimental systems (Fig 2).
The analysis of structure-activity relationships al-
lowed the spatial features of the active pharmacophore
to be defined in considerable detail even before the
molecular mechanism of action was fully elucidated. For
maximal potency, the nitrogen atom in the R2 side chain
must be a critical distance away from the P-C-P group
and in a specific spatial configuration.45 This principle
was used successfully for predicting the features required
in the chemical design of new and more active com-
pounds.
Although the structure of the R2 side chain is the
major determinant of antiresorptive potency, both phos-
phonate groups are also required for the drugs to be
pharmacologically active.
FIGURE 1
The generic structure of pyrophosphate compared with
bisphos-phonates and their functional domains.
FIGURE 2
Structures of the bisphosphonates used in clinical studies
classi-
fied according to their biochemical mode of action.
PEDIATRICS Volume 119, Supplement 2, March 2007 S153at
Pontificia Universidad Catolica de Chile on August 18,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
6/15
In summary, studies of the relationships between
bisphosphonate structure and antiresorptive potency
suggested that the ability of bisphosphonates to inhibit
bone resorption depend on 2 separate properties of the
bisphosphonate molecule. The 2 phosphonate groups,
together with a hydroxyl group at the R1 position,46
impart high affinity for bone mineral and act as a bone
hook, which allows rapid and efficient targeting
ofbisphosphonates to bone mineral surfaces. Once local-
ized within bone, the structure and three-dimensional
conformation of the R2 side chain (as well as the phos-
phonate groups in the molecule) determine the biolog-
ical activity of the molecule and influence the ability of
the drugs to interact with specific molecular targets. Our
understanding of what these molecular targets might be
has become much clearer as a result of recent work.
Over the years there have been many efforts to
explain how bisphosphonates work on cells, especially
via inhibitory effects on enzymes (eg, by direct or in-
direct inhibition of the osteoclast proton-pumpingHATPase,47,48
phosphatases, or lysosomal enzymes49,50).
Because osteoclasts are highly endocytic, bisphospho-
nate present in the resorption space is likely to be inter-
nalized by endocytosis and thereby affect osteoclasts di-
rectly.25 The uptake of bisphosphonates by osteoclasts in
vivo has been confirmed by using radiolabeled51 and
fluorescently labeled alendronate, which was internal-
ized into intracellular vacuoles. After cellular uptake, a
characteristic morphologic feature of bisphosphonate-
treated osteoclasts is the lack of a ruffled border, the
region of invaginated plasma membrane facing the re-
sorption cavity. Bisphosphonates also disrupt the cy-toskeleton
of the osteoclast.52 Early explanations for
these effects invoked the inhibition of protein kinases or
phosphatases that regulate cytoskeletal structure, such
as protein tyrosine phosphatases.5356 However, a more
likely mechanism by which the cytoskeleton may be
affected involves loss of function of small GTPases such
as Rho and Rac.
Since the early 1990s there has been a systematic
effort by our group and others to elucidate the molecular
mechanisms of action of bisphosphonates,5,57,58 and we
have proposed that bisphosphonates can be classified
into at least 2 major groups with different modes of
action (Fig 3). The first group comprises the nonnitro-
gen-containing bisphosphonates that perhaps most
closely resemble pyrophosphate, such as clodronate and
etidronate, and these can be metabolically incorporated
into nonhydrolyzable analogues of adenosine triphos-
phate (ATP) by reversing the reactions of aminoacyl
transfer RNA synthetases.59 The resulting metabolitescontain the
P-C-P moiety in place of the ,-phosphate
groups of ATP, thus resulting in nonhydrolyzable
(AppCp) nucleotides.6063 It is likely that intracellular
accumulation of these metabolites within osteoclasts in-
hibits their function and may cause osteoclast cell death.
The AppCp-type metabolites of bisphosphonates are cy-
totoxic when internalized and cause similar changes in
morphology to those observed in clodronate-treated
cells, possibly by interference with mitochondrial ATP
translocases.64 Overall, this group of bisphosphonates,
therefore, seem to act as prodrugs, being converted to
active metabolites after intracellular uptake by oste-oclasts in
vivo.
In contrast, the second group contains the more po-
tent, nitrogen-containing bisphosphonates such as alen-
dronate, risedronate, and zoledronate. Members of this
group interfere with other metabolic reactions, notably
in the mevalonate biosynthetic pathway, and affect cel-
lular activity and cell survival by interfering with protein
prenylation and, therefore, the signaling functions of
key regulatory proteins. These mechanisms have been
reviewed in detail elsewhere.1 The mevalonate pathway
is a biosynthetic route responsible for the production of
cholesterol, other sterols, and isoprenoid lipids such
asisopentenyl diphosphate (also known as isopentenyl py-
rophosphate), as well as farnesyl diphosphate (FPP) and
geranylgeranyl diphosphate (GGPP). FPP and GGPP are
required for the posttranslational modification (prenyla-
tion) of small GTPases such as Ras, Rab, Rho, and Rac,
which are prenylated at a cysteine residue in character-
istic C-terminal motifs.65 Small GTPases are important
signaling proteins that regulate a variety of cell processes
important for osteoclast function, including cell mor-
phology, cytoskeletal arrangement, membrane ruffling,
trafficking of vesicles, and apoptosis.6669 Prenylation is
FIGURE 3
Two distinct molecular mechanisms of action of bisphospho-
nates (BPs) that both inhibit osteoclasts (see text for
details). GTP
indicates guanosine triphosphate.
S154 RUSSELLat Pontificia Universidad Catolica de Chile on
August 18, 2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
7/15
required for the correct function of these proteins be-
cause the lipid prenyl group serves to anchor the pro-
teins in cell membranes and may also participate in
protein-protein interactions.70
Many observations point to the importance of the
mevalonate pathway for osteoclast function and
strengthen the proposal that the nitrogen-containing
bisphosphonates inhibit osteoclastic bone
resorptionpredominantly by inhibition of this pathway. These
bisphosphonates inhibit the synthesis of mevalonate me-
tabolites including FPP and GGPP, and thereby impair
the prenylation of proteins,71 and cause alteration of
function of small GTPases. There is a strong structure-
activity relationship such that changes to the structure of
the nitrogen-containing R2 side chain or to the phospho-
nate groups, which alter antiresorptive potency, also
influence the ability to inhibit protein prenylation to a
corresponding degree.72 An important verification of the
critical importance of this pathway has come from show-
ing that the addition of intermediates of the mevalonatepathway
(such as FPP and GGPP) could overcome
bisphosphonate-induced apoptosis and other events in
many cell systems. Another prediction was that if inhi-
bition of the mevalonate pathway could account for the
antiresorptive effects of bisphosphonates, then the statin
drugs should also inhibit bone resorption. Statins are
inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A
(HMG-CoA) reductase, one of the first steps in the me-
valonate pathway. They proved to be even more potent
than bisphosphonates at inhibiting osteoclast formation
and bone resorption in vitro,73,74 an effect that could also
be overcome by the addition of geranylgeraniol (whichcan be used
for protein geranylgeranylation) but not
farnesol (which is used for protein farnesylation). Hence,
it seems that although nitrogen-containing bisphospho-
nates can prevent both farnesylation and geranylgera-
nylation of proteins (probably by inhibiting enzymes
required for synthesis of FPP and GGPP), loss of gera-
nylgeranylated proteins in osteoclasts is of greater con-
sequence than loss of farnesylated proteins. This is con-
sistent with the known role of geranylgeranylated
proteins such as Rho, Rac, and Rab in processes that are
fundamental to osteoclast formation and function (eg,
cytoskeletal rearrangement, membrane ruffling, and ve-
sicular trafficking75), and further work has confirmed
this, particularly the importance of Rab proteins.
The comparison between bisphosphonates and statins
is interesting. The statins are widely used as cholesterol-
lowering drugs (they are able to lower cholesterol bio-
synthesis by inhibiting 3-hydroxy-3-methylglutaryl co-
enzyme A reductase). Despite several studies, there is no
substantial evidence that statins have effects on bone
when used clinically, perhaps because they are selec-
tively taken up by the liver rather than bone, which is
the converse of the case for bisphosphonates. Therefore,
this is an excellent example of how drug specificity is
achieved by highly selective tissue targeting.
The exact enzymes of the mevalonate pathway that
are inhibited by individual bisphosphonates have been
partially elucidated. Several enzymes of the pathway use
isoprenoid diphosphates as a substrate (isopentenyl py-
rophosphate isomerase, FPP synthase, GGPP synthase,
squalene synthase) and, thus, are likely to have
similarsubstrate-binding sites. Thus, if nitrogen-containing
bisphosphonates act as substrate analogues of an isopre-
noid diphosphate, it is possible that these bisphospho-
nates will inhibit more than 1 of the enzymes of the
mevalonate pathway. Early studies revealed that incad-
ronate and ibandronate, but not other bisphosphonates,
are inhibitors of squalene synthase, an enzyme in the
mevalonate pathway that is required for cholesterol bio-
synthesis.76,77 Inhibition of squalene synthase, however,
would not lead to inhibition of protein prenylation.
However, it is now clear that farnesyl pyrophosphate
synthase (FPPS) is a major site of action of the
nitrogen-containing bisphosphonates (N-bisphosphonates).78
FPPS catalyzes the successive condensation of isopente-
nyl pyrophosphate with dimethylallyl pyrophosphate
and geranyl pyrophosphate. There is a strong relation-
ship among individual bisphosphonates between inhibi-
tion of bone resorption and inhibition of FPPS, with the
most potent bisphosphonates having IC50 values (con-
centration that inhibits response by 50%) in the nano-
molar range.79 Modeling studies have provided a molec-
ular rationale for bisphosphonate binding to FPPS.80 Our
recent studies using protein crystallography, enzyme ki-
netics, and isothermal titration calorimetry led to thefirst
published high-resolution radiograph structures of
the human enzyme in complexes with risedronate and
zoledronate.81 These agents bind to the dimethylallyl/
geranyl pyrophosphate ligand pocket and induce a con-
formational change. The interactions of the N-bisphos-
phonate cyclic nitrogen with Thr201 and Lys200 suggest
that these inhibitors achieve potency by positioning their
nitrogen in a proposed carbocation82 binding site. This
explains how the nitrogen moiety is so important to the
potency of these bisphosphonates. Kinetic analyses re-
veal that inhibition is competitive with geranyl pyro-
phosphate and is of a slow, tight-binding character,
which indicates that isomerization of an initial enzyme-
inhibitor complex occurs after binding of the N-bisphos-
phonate.
Taken together, these observations clearly indicate
that bisphosphonates can be grouped into 2 classes:
those that can be metabolized into nonhydrolyzable an-
alogues of ATP (the least potent bisphosphonates) and
those that are not metabolized but can inhibit protein
prenylation (the potent, nitrogen-containing bisphos-
phonates). The identification of 2 such classes may help
to explain some of the other pharmacologic differences
between the 2 classes.
PEDIATRICS Volume 119, Supplement 2, March 2007 S155at
Pontificia Universidad Catolica de Chile on August 18,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
8/15
CLINICAL APPLICATIONS OF BISPHOSPHONATES
After it was shown that bisphosphonates inhibited ex-
perimentally induced calcification and bone resorption,
their potential application to clinical disorders was obvi-
ous, but it took many years for them to become well
established.
The earliest clinical applications of bisphosphonates
included use of etidronate as an inhibitor of calcificationin
fibrodysplasia ossificans progressiva (formerly known
as myositis ossificans) and in patients who had under-
gone total hip replacement surgery to prevent subse-
quent heterotopic ossification and improve mobility.83
One of the other early clinical uses of bisphospho-
nates was as agents for bone imaging, bone scanning,
for which they still remain outstandingly useful for de-
tecting bone metastases and other bone lesions. The
application of pyrophosphate and simple bisphospho-
nates as bone-scanning agents depends on their strong
affinity for bone mineral, particularly at sites of in-
creased bone turnover, and their ability to be linked to
a-emitting technetium isotope.84,85
The most impressive clinical application of bisphos-
phonates has been as inhibitors of bone resorption, es-
pecially for diseases in which no effective treatment
existed previously. Thus, bisphosphonates became the
treatment of choice for a variety of bone diseases in
which excessive osteoclast activity is an important
pathologic feature, including Paget disease of bone, met-
astatic and osteolytic bone disease, and hypercalcemia of
malignancy, as well as osteoporosis.
The clinical pharmacology of bisphosphonates is char-
acterized by low intestinal absorption (
1%4%) buthighly selective localization and retention in bone.
Sig-
nificant adverse effects of bisphosphonates are mini-
mal.8688 Although there are more similarities than dif-
ferences between individual compounds and each
bisphosphonate is potentially capable of treating any of
the disorders of bone resorption in which they are used,
in practice different compounds have come to be favored
for the treatment of different diseases. There are cur-
rently at least 10 bisphosphonates (etidronate, clodr-
onate, tiludronate, pamidronate, alendronate, risedr-
onate, zoledronate, and ibandronate and, to a limited
extent, olpadronate and neridronate) that have been
registered for various clinical applications in various
countries. To a major extent, the diseases in which they
are used reflects the history of their clinical development
and the degree of commercial interest in and sponsor-
ship of the relevant clinical trials.
Paget disease was the first clinical disorder in which a
dose-dependent inhibition of bone resorption could be
demonstrated by using bisphosphonates in humans.89,90
Bisphosphonates have become the most important drugs
used in the treatment of Paget disease.91 For many years
pamidronate given by intravenous infusion was used
extensively, 92 but the newer and more potent bisphos-
phonates can produce even more profound suppression
of disease activity than was possible with the bisphos-
phonates available in previous years.93,94 The latest ad-
vance is with zoledronate,95 which, when given as a
single 5-mg infusion, produced a greater and longer-
lasting suppression of excess bone turnover than even
oral risedronate given at 30 mg/day over 2 months,
hitherto one of the most effective treatments.In terms of
commercial success, the use of bisphos-
phonates in oncology has been preeminent. Many can-
cers in humans are associated with hypercalcemia
(raised blood calcium) and/or increased bone destruc-
tion. Bisphosphonates are remarkably effective in the
treatment of bone problems associated with malignan-
cy96 and are now the drugs of choice.9799 Clinical trials
that investigate the benefit of bisphosphonate therapy
use a composite end point defined as a skeletal-related or
bone event, which typically includes pathologic fracture,
spinal cord compression, radiation or surgery to bone,
and hypercalcemia of malignancy. Bisphosphonates sig-nificantly
reduce the incidence of these events in my-
eloma100 and in patients with breast cancer metasta-
ses101,102 and in metastatic prostate cancer,103 lung
cancer,
renal cell carcinoma, and other solid tumors. The goals
of treatment for bone metastases are also to prevent
disease-related skeletal complications, palliate pain, and
maintain quality of life. Zoledronate,104 pamidronate,
clodronate, and ibandronate105,106 have demonstrated ef-
ficacy compared with placebo.
There is the important possibility that the survival of
patients may be prolonged107109 in some groups of pa-
tients. Recently, osteonecrosis of the jaw
110
was identi-fied as a potential complication of high-dose
bisphospho-
nate therapy in malignant diseases.
The other area of outstanding commercial success
with bisphosphonates has been in the therapy of osteo-
porosis, which is a major public health problem.111,112 Up
until the 1990s, there were few treatments for osteopo-
rosis. As a drug class the bisphosphonates have emerged
in the past few years as the leading effective treatments
for postmenopausal and other forms of osteoporosis.
Etidronate was the first of these,113115 followed by alen-
dronate116118 and then risedronate.119,120 All have been
approved as therapies in many countries and can in-
crease bone mass and reduce fracture rates at the spine
by 30% to 50% and at other sites in postmenopausal
women.121 The reduction in fractures may be related not
only to the increase in bone mass arising from the inhi-
bition of bone resorption and reduced activation fre-
quency of bone-remodeling units but also to enhanced
osteon mineralization.122 These bisphosphonates also
prevent bone loss associated with glucocorticosteroid ad-
ministration. 123,124
Among the newer bisphosphonates, ibandronate125
was introduced recently as a once-monthly tablet. In
addition to formulations to be taken by mouth weekly or
S156 RUSSELLat Pontificia Universidad Catolica de Chile on
August 18, 2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
9/15
monthly, new routes of administration are being stud-
ied, especially periodic (eg, 3 monthly) injections with
ibandronate and once-yearly treatment with zoledr-
onate.126 This has the attraction of delivering a defined
dose without the variability associated with oral admin-
istration as well as avoiding potential gastrointestinal
intolerance. If these approaches are accompanied by
greater compliance and convenience, they are likely tobecome
popular methods of treatment.
Other clinical issues under consideration with
bisphosphonates include the choice of therapeutic regi-
men (eg, the use of intermittent dosing rather than
continuous, intravenous versus oral therapy), the opti-
mal duration of therapy, the combination with other
drugs such as teriparatide, and their extended use in
related indications (eg, glucocorticosteroid-associated
osteoporosis, male osteoporosis, childhood osteopenic
disorders, arthritis, and other disorders). Therefore,
there is much that needs to be done to improve the way
in which existing drugs can be used and to introducenew
ones.
In pediatrics, pamidronate has proved remarkably ef-
fective in increasing bone in children with the inherited
brittle-bone disorder, osteogenesis imperfecta.127,128
SOMECURRENT ISSUESWITH BISPHOSPHONATES: BONE
ARCHITECTURE, STRUCTURE, ANDSTRENGTH,ANDONBONE
HEALING ANDFRACTURE REPAIR
Many experimental and clinical studies show that
bisphosphonates conserve bone architecture and
strength.129133 However, there have been concerns about
whether the use of prolonged high doses of bisphospho-nates may
impair bone turnover to such an extent that
bone strength is impaired. High doses in animals are
associated with increased microdamage134,135 and even
fractures.136 It has been suggested that bisphosphonates
might prevent naturally occurring microscopic cracks in
bone from healing. There have been isolated reports of
adynamic bone associated with bisphosphonate usage,137
but long-term use of the bisphosphonates in the therapy
of osteoporosis seems to be safe.138 Case reports of in-
duction of osteopetrosis-like lesions in children who
were treated with excessive doses of pamidronate have
been published.139
A question often asked is whether bisphosphonates
inhibit fracture repair. By reducing bone turnover one
might expect bisphosphonates to interfere with fracturehealing.
However, a recent long-term study in a beagle
dog model that simulated fracture repair has demon-
strated that ibandronate treatment did not adversely
affect normal bone healing.140 Studies of repair processes
after creating drill-hole defects in dogs also showed no
impairment with ibandronate.141
Several other recent studies raised the intriguing pos-
sibility that bisphosphonates may enhance fracture re-
pair and related processes.142 In studies of the osseointe-
gration of metal implants in ovariectomized rats,
treatment with ibandronate resulted in improved os-
seointegration rather than impairment of the healingprocess.143
Potential applications of bisphosphonates in
orthopedics include protection against loosening of pros-
theses,144better integration of biomaterials and implants,
improved healing in distraction osteogenesis,145 and con-
serving bone architecture after osteonecrosis146,147 and in
Perthes disease.148
There are potentially important differences between
clinically useful bisphosphonates regarding their po-
tency and duration of action. Efficacy is closely related to
affinity for bone mineral and ability to inhibit FPP syn-
thase. Recent studies showing that there are marked
differences among bisphosphonates in binding to
hy-droxyapatite149 may explain the variations in retention
and persistence of effect that have been observed in
animal and clinical studies. In the case of zoledronic acid,
in particular, the remarkable magnitude of effect and
prolonged duration of action can be explained in part by
these new observations. In explaining the long duration
of action, it has been proposed that there is continual
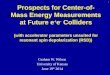
FIGURE 4
Bisphosphonate (BP) uptake and detachment from bone surfac-
es: effect of binding affinity on recirculation of
bisphosphonate
on and off bone surfaces. The differences in mineral-binding
af-
finity may affect distribution into different bone
compartments
and persistence of drug action at bone surfaces. (Adapted
from
Nancollas GH, Tang R, Phipps RJ, et al. Bone.
2006;38:617627.)
PEDIATRICS Volume 119, Supplement 2, March 2007 S157at
Pontificia Universidad Catolica de Chile on August 18,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
10/15
recycling of bisphosphonate off and back onto the bone
surface. This notion is supported by observations that
bisphosphonates can be found in plasma and urine
many months after dosing (Fig 4).
There are numerous examples of bisphosphonates
having effects on cells and tissues outside the skeleton.
The effects on osteoclast precursors, tumor cells, macro-
phages, and,-T cells are examples and in all cases areprobably
explained by sufficient bisphosphonates enter-
ing cells to inhibit the mevalonate pathway. A well-
recognized adverse effect of the nitrogen-containing
bisphosphonates is that they cause an acute-phase re-
sponse in vivo,150,151 which can lead to induction of fever
and flu-like symptoms in patients. These effects are
transient and occur predominantly on first exposure to
the drug, especially with intravenous administration.
The mechanism has been attributed to release of proin-
flammatory cytokines, and the mechanism has been fur-
ther unraveled by showing that it involves selective re-
ceptor-mediated activation of,-T cells, leading to
theirproliferation and activation.152 The bisphosphonate ef-
fect involves the mevalonate pathway in vitro and can
be overcome by using statins.153
Another interesting aspect of these nonskeletal effects
are the observations made on protozoan parasites, the
growth of which can be inhibited by bisphosphonates
acting on FPPS.154,155
In the future, other clinical indications ripe for future
study include the prevention of bone loss and erosions in
rheumatoid arthritis, possible applications in other joint
diseases, the reduction of bone loss associated with peri-
odontal disease, and loosening of joint prostheses.The recent
elucidation of the likely mode of action of
bisphosphonates within cells opens up the possibility of
exploiting the subtle and potentially important differ-
ences between the classes of bisphosphonates and indi-
vidual compounds.
REFERENCES
1. Russell RGG. Bisphosphonates: from bench to bedside. Ann
N Y Acad Sci. 2006;1068:367401
2. Bijvoet O, Fleisch H, Canfield RE, Russell RGG,
eds.Bisphos-
phonates on Bone. Amsterdam, Holland: Elsevier Science; 1995
3. Fleisch H.Bisphosphonates in Bone Disease: From the
Laboratory tothe Patient. 4th ed. San Diego, CA: Academic Press;
2000
4. Green JR. Bisphosphonates: preclinical review.
Oncologist.
2004;9(suppl 4):313
5. Rogers MJ. From molds and macrophages to mevalonate: a
decade of progress in understanding the molecular mode of
action of bisphosphonates. Calcif Tissue Int. 2004;75:451461
6. Fleisch H, Neuman WF. Mechanisms of calcification: role
of
collagen, polyphosphates, and phosphatase. Am J Physiol.
1961;200:1296 1300
7. Fleisch H, Bisaz S. Isolation from urine of pyrophosphate,
a
calcification inhibitor. Am J Physiol. 1962;203:671675
8. Fleisch H, Russell RGG, Straumann F. Effect of
pyrophosphate
on hydroxyapatite and its implications in calcium homeosta-
sis. Nature. 1966;212:901903
9. Russell RG. Excretion of inorganic pyrophosphate in hy-
pophosphatasia.Lancet. 1965;10:461464
10. Schibler D, Russell RGG, Fleisch H. Inhibition by
pyrophos-
phate of aortic calcification induced by vitamin D3
in rats.Clin
Sci. 1968;35:363372
11. Fleisch H, Russell RGG, Bisaz S, Casey PA, Muehlbauer
RC.
The influence of pyrophosphate analogues (diphosphonates)
on the precipitation and dissolution. Calcif Tissue Res.
1968;
(suppl):1010A
12. Francis MD, Russell RGG, Fleisch H. Diphosphonates
inhibit
formation of calcium phosphate crystals in vitro and patho-
logical calcification in vivo. Science. 1969;165:12641266
13. Fleisch H, Russell RGG, Francis MD. Diphosphonates
inhibit
hydroxyapatite dissolution in vitro and bone resorption in
tissue culture in vivo. Science. 1969;165:12621264
14. Jung A, Bisaz S, Fleisch H. The binding of pyrophosphate
and
two diphosphonates by hydroxyapatite crystals. Calcif Tissue
Res.1973;11:269280
15. Fleisch H, Russell RGG, Bisaz S, Muehlbauer RC, Williams
DA. The inhibitory effect of phosphonates on the formation
of
calcium phosphate crystals in vitro and on aortic and kidney
recalcification in vivo. Eur J Clin Invest. 1970;1:1218
16. Schenk R, Merz WA, Muhlbauer R, Russell RGG, Fleisch H.
Effect of ethane-1-hydroxy-1,1-diphosphonate (EHDP)
anddichloromethylene diphosphonate (Cl 2 MDP) on the calcifi-
cation and resorption of cartilage and bone in the tibial
epiph-
ysis and metaphysis of rats. Calcif Tissue
Res.1973;11:196214
17. Fleisch H, Maerki J, Russell RGG. Effect of pyrophosphate
on
dissolution of hydroxyapatite and its possible importance in
calcium homeostasis.Proc Soc Exp Biol Med. 1966;122:317320
18. Russell RGG, Muhlbauer RC, Bisaz S, Williams DA, Fleisch
H.
The influence of pyrophosphate, condensed phosphates,
phosphonates and other phosphate compounds on the disso-
lution of hydroxyapatite in vitro and on bone resorption
induced by parathyroid hormone in tissue culture and in
thyroparathyroidectomised rats. Calcif Tissue Res. 1970;6:
183196
19. Trechsel U, Stutzer A, Fleisch H. Hypercalcemia induced
with an arotinoid in thyroparathyroidectomized rats: a new
model to study bone resorption in vivo. J Clin Invest.
1987;80:
16791686
20. Stutzer A, Fleisch H, Trechsel U. Short- and long-term
effects
of a single dose of bisphosphonates on retinoid-induced bone
resorption in thyroparathyroidectomized rats. Calcif Tissue
Int.
1988;43:294299
21. Schenk R, Eggli P, Fleisch H, Rosini S. Quantitative
morpho-
metric evaluation of the inhibitory activity of new ami-
nobisphosphonates on bone resorption in the rat. Calcif
Tissue
Int. 1986;38:342349
22. Muehlbauer RC, Russell RGG, Williams DA, Fleisch H. The
effects of diphosphonates, polyphosphates, and calcitonin on
immobilisation osteoporosis in rats. Eur J Clin Invest.
1971;
1:33634423. Ferretti JL. Effects of biosphosphonates on bone
biomechan-
ics. Bijvoet O, Fleisch HA, Canfield RE, Russell RGG, eds.
In:
Bisphosphonates on Bone. Amsterdam, Holland: Elsevier
Science; 1995:211229
24. Shinoda H, Adamek G, Felix R, Fleisch H, Schenk R, Hagan
P.
Structure-activity relationships of various bisphosphonates.
Calcif Tissue Int. 1983;35:8799
25. Flanagan AM, Chambers TJ. Dicholormethylenebisphospho-
nate (C12MBP) inhibits bone resorption through injury to
osteoclasts that resorb C12 MBP-coated bone. Bone Miner.
1989;6:3343
26. Smith R, Russell RGG, Bishop M. Disphosphonates and
Pages
disease of bone.Lancet. 1971;1(7706):945947
27. Reitsma PH, Bijvoet OLM, Verlinden-Ooms H, van der Wee-
S158 RUSSELLat Pontificia Universidad Catolica de Chile on
August 18, 2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
11/15
Pals LJA. Kinetic studies of bone and mineral metabolism
during treatment with (3-amino-1-hydroxy-propylidene)-
1,1-bisphosphonate (APD) in rats. Calcif Tissue Int.
1980;32:
145157
28. Garnero P, Shih WJ, Gineyts E, Karpf DB, Delmas PD. Com-
parison of new biochemical markers of bone turnover in late
postmenopausal osteoporotic women in response to alendro-
nate treatment. J Clin Endocrinol Metab. 1994;79:16931700
29. Bauss F, Russell RG. Ibandronate in osteoporosis:
preclinical
data and rationale for intermittent dosing. Osteoporos
Int.2004;
15:423433
30. Gasser JA, Green JR. Long-term protective effect of a single
IV
injection of zoledronic acid on cancellous bone structure
and
cortical bone in ovariectomized rats. Bone. 2002;30(suppl):
41S
31. Hughes DE, MacDonald BR, Russell RG, Gowen M. Inhibition
of osteoclast-like cell formation by bisphosphonates in
long-
term cultures of human bone marrow. J Clin Invest. 1989;83:
19301935
32. Boonekamp PM, van der Wee-Pals LJA, van Wijk-van Len-
nep MLL, Wil Thesing C, Bijvoet OLM. Two modes of action
of bisphosphonates on osteoclastic resorption of mineralized
matrix.Bone Miner. 1986;1:2739
33. Lowik CWGM, van der Pluijm G, van der Wee-Pals LJA, Bloysvan
Teslong-de Groot H, Bijvoet OLM. Migration and pheno-
typic transformation of osteoclast precursors into mature
osteoclasts: the effect of a bisphosphonate. J Bone Miner
Res.
1988;3:185192
34. Suda T, Nakamura I, Jimi E, Takahashi N. Regulation of
osteoclast function. J Bone Miner Res. 1997;12:869 879
35. Masarachia P, Weinreb M, Balena R, Rodan GA. Comparison
of the distribution of 3H-alendronate and 3H-etidronate in
rat
and mouse bones. Bone. 1996;19:281290
36. Azuma Y, Sato H, Oue Y, et al. Alendronate distributed
on
bone surfaces inhibits osteoclastic bone resorption in vitro
and
in experimental hypercalcemia models. Bone. 1995;16:
235245
37. Sato M, Grasser W. Effects of bisphosphonates on isolated
rat
osteoclasts as examined by reflected light microscopy. J
Bone
Miner Res. 1990;5:3140
38. Plotkin LI, Weinstein RS, Parfitt AM, Roberson PK,
Manol-
agas Sc, Bellido T. Prevention of osteocyte and osteoblast
apoptosis by bisphosphonates and calcitonin. J Clin Invest.
1999;104:13631374
39. Plotkin LI, Aguirre JI, Kousteni S, Manolagas SC, Bellido
T.
Bisphosphonates and estrogens inhibit osteocyte apoptosis
via
distinct molecular mechanisms downstream of extracellular
signal-regulated kinase activation. J Biol Chem. 2005;280:
73177325
40. Ebrahimpour A, Francis MD. Bisphosphonate therapy in
acute and chronic bone loss: physical chemical
considerations
in bisphosphonate-related therapies. In: Bijvoet O, Fleisch
HA, Canfield RE, Russell RGG eds. Bisphosphonates on
Bones.Amsterdam, Holland: Elsevier Science; 1995:125136
41. Muehlbauer RC, Bauss F, Schenk R, et al. BM 21.0955, a
potent new bisphosphonate to inhibit bone resorption. J Bone
Miner Res. 1991;6:10031011
42. Papapoulos SE, Hoekman K, Lowik CWGM, Vermeij P, Bij-
voet OLM. Application of an in vitro model and a clinical
protocol in the assessment of the potency of a new bisphos-
phonate.J Bone Miner Res. 1988;4:775781
43. Goa KL, Balfour JA. Risedronate.Drugs Aging.
1998;13:8391;
discussion 92
44. Green JR, Mueller K, Jaeggi KA. Preclinical pharmacology
of
CGP42446, a new, potent, heterocyclic bisphosphonate com-
pound. J Bone Miner Res. 1994;9:745751
45. Ebetino FH, Bayless AV, Amburgey J, Ibbotson KJ,
Dansereau
S, Ebrahimpour A. Elucidation of a pharmacore for the
bisphosphonate mechanism of bone antiresorptive activity.
Phosphorus Sulfur Silicon Relat Elem. 1996;109/110:217220
46. van Beek E, Lowik C, Oue I, Papapoulos S. Dissociation
of
binding and antiresorptive properties of hydroxybisphospho-
nates by substitution of the hydroxyl with an amino group.
J Bone Miner Res. 1996;11:14921497
47. David P, Nguyen H, Barbier A, Baron R. The
bisphosphonate
tiludronate is a potent inhibitor of the osteoclast vacuolar
H()-ATPase.J Bone Miner Res. 1996;11:14981507
48. Carano A, Teitelbaum SA, Konsek JD, Schlesinger PH,
Blair
HC. Bisphosphonates directly inhibit the bone resorption ac-
tivity of isolated avian osteoclasts in vitro. J Clin Invest.
1990;
85:456461
49. Felix R, Russell RGG, Fleisch H. The effect of several
diphos-
phonates on acid phosphohydrolases and other lysosomal
enzymes.Biochim Biophys Acta. 1976;429:429438
50. Lerner UH, Larsson A. Effects of four bisphosphonates on
bone resorption, lysosomal enzyme release, protein
synthesis,
and mitotic activities in mouse calvarial bones in vitro.
Bone.
1987;8:179189
51. Sato M, Grasser W, Endo N, et al. Bisphosphonate action:
alendronate localization in rat bone and effects on
osteoclast
ultrastructure.J Clin Invest. 1991;88:2095210552. Murakami H,
Takahashi N, Sasaki T, et al. A possible mech-
anism of the specific action of bisphosphonates on
osteoclasts:
tiludronate preferentially affects polarized osteoclasts
having
ruffled borders. Bone. 1995;17:137144
53. Schmidt A, Rutledge SJ, Endo N, et al. Alendronate
inhibition
of protein tyrosine phosphatase activity. Proc Natl Acad Sci
U S A. 1995;93:30683073
54. Endo N, Rutledge SJ, Opas EE, Vogel R, Rodan GA, Schmidt
A. Human protein tyrosine phosphatases: alternative splicing
and inhibition by bisphosphonates.J Bone Miner Res. 1996;11:
535543
55. Opas EE, Rutledge SJ, Golub E, et al. Alendronate
inhibition
of protein-tyrosine-phosphatase-meg1. Biochem Pharmacol.
1997;54:721727
56. Murakami H, Takahashi N, Tanaka S, et al. Tiludronate
in-
hibits protein tyrosine phosphatase activity in osteoclasts.
Bone.1997;20:399 404
57. Rogers MJ, Watts DJ, Russell RGG, et al. Inhibitory effects
of
bisphosphonates on growth of amoebae of the cellular slime
mold Dictyostelium discoideum. J Bone Miner Res. 1994;9:
10291039
58. Rogers MJ, Xiong X, Brown RJ, et al. Structure-activity
rela-
tionships of new heterocycle-containing bisphosphonates as
inhibitors of bone resorption and as inhibitors of growth of
Dictyostelium discoideum amoebae. Mol Pharmacol. 1995;47:
398402
59. Rogers MJ, Brown RJ, Hodkin V, Russell RGG, Watts DJ.
Bisphosphonates are incorporated into adenine nucleotides
by human aminoacyl-tRNA synthetase enzymes. Biochem Bio-phys Res
Commun.1996;224:863869
60. Rogers MJ, Ji X, Russell RGG, et al. Incorporation of
bisphos-
phonates into adenine nucleotides by amoebae of the cellular
slime mould Dictyostelium discoideum. Biochem J. 1994;303:
303311
61. Frith JC, Monkkonen J, Blackburn GM, Russell RGG, Rogers
MJ. Clodronate and liposome-encapsulated clodronate are
metabolized to a toxic ATP analog, adenosine 5,-
dichloromethylene triphosphate, by mammalian cells in vitro.
J Bone Miner Res. 1996;12:13581367
62. Frith JC, Monkkonen J, Auriola S, Monkkonen H, Rogers
MJ.
The molecular mechanism of action of the antiresorptive and
anti-inflammatory drug clodronate: evidence for the forma-
tion in vivo of a metabolite that inhibits bone resorption
and
PEDIATRICS Volume 119, Supplement 2, March 2007 S159at
Pontificia Universidad Catolica de Chile on August 18,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
12/15
-
8/11/2019 Graham 2014 Bifosfonato
13/15
101. Pavlakis N, Schmidt R, Stockler M. Bisphosphonates for
breast cancer.Cochrane Database Syst Rev. 2005;(3):CD003474
102. Coleman RE. Bisphosphonates in breast cancer. Ann
Oncol.
2005;16:687695
103. Parker CC. The role of bisphosphonates in the treatment
of
prostate cancer. BJU Int. 2005;95:935938
104. Smith MR. Zoledronic acid to prevent skeletal
complications
in cancer: corroborating the evidence. Cancer Treat Rev.
2005;
31(suppl 3):1925
105. Bell R. Efficacy of ibandronate in metastatic bone
disease:
review of clinical data. Oncologist. 2005;10(suppl 1):8134
106. Body JJ, Diel IJ, Lichinitzer M, et al. Oral ibandronate
reduces
the risk of skeletal complications in breast cancer patients
with metastatic bone disease: results from two randomised,
placebo-controlled phase III studies. Br J Cancer. 2004;90:
11331137
107. McCloskey EV, MacLennan ICM, Drayson M, Chapman C,
Dunn J, Kanis JA. A randomized trial of the effect of clodr-
onate on skeletal morbidity in multiple myeloma. MRC
Working Party on Leukeaemia in Adults. Br J Haematol.1998;
100:317325
108. Berenson JR, Lichtenstein A, Porter L, et al. Efficacy of
pam-
idronate in reducing skeletal events in patients with
advanced
multiple myeloma. N Engl J Med. 1996;334:488493109. Diel IJ,
Solomayer EF, Costa SD, et al. Reduction in new
metastases in breast cancer with adjuvant clodronate treat-
ment.N Engl J Med. 1998;339:357363
110. Maerevoet M, Martin C, Duck L. Osteonecrosis of the jaw
and
bisphosphonates [published correction appears in N Engl
J Med. 2005;353:2728]. N Engl J Med. 2005;353:99102
111. Carmona RH. Bone Health and Osteoporosis: A Report of
the
Surgeon General. Rockville MD: US Department of Health and
Human Services, Office of the Surgeon General; 2004. Avail-
able at: www.hhs.gov/surgeongeneral/library/bonehealth/
content.html. Acessed December 13, 2006
112. Russell RGG. Pathogenesis of osteoporosis. In: Hochberg
MC,
Silman AJ, Smolen SJ, Weinblatt ME, Weisman MH, eds.
Rheumatology. 3rd ed. St Louis, MO: Mosby; 2003:20752147
113. Watts NB, Harris ST, Genant HK, et al. Intermittent
cyclical
etidronate treatment of postmenopausal osteoporosis. N Engl
J Med. 1990;323:7379
114. Storm T, Thamsborg G, Steinriche T, et al. Effect of
intermit-
tent cyclical etidronate therapy on bone mass and fracture
rate in women with postmenopausal osteoporosis. N Engl
J Med. 1990;322:12651271
115. van Staa TP, Abenhain L, Cooper C. Use of cyclical
etidronate
and prevention of non-vertebral fractures. Br J Rheumatol.
1998;37:8794
116. Liberman UA, Weiss SR, Broll J, et al. Effect of oral
alendro-
nate on bone mineral density and the incidence of fractures
in
postmenopausal osteoporosis. The Alendronate Phase III Os-
teoporosis Treatment Study Group. N Engl J Med. 1995;333:
14371443117. Black DM, Cummings SR, Karpf DB, et al. Randomised
trial of
effect of alendronate on risk of fracture in women with ex-
isting vertebral fractures. Fracture Intervention Trial
Research
Group. Lancet. 1996;348:15351541
118. Bone HG, Hosking D, Devogelaer JP, et al. Ten years
expe-
rience with alendronate for osteoporosis in postmenopausal
women. N Engl J Med. 2004;350:11891199
119. Reginster J, Minne HW, Sorenson OH, et al. Randomized
trial
of the effects of risedronate on vertebral fractures in
women
with established postmenopausal osteoporosis. Vertebral Ef-
ficacy With Risedronate Therapy (VERT) Study Group. Osteo-
poros Int.2000;11:8391
120. McClung MR, Geusens P, Miller PD, et al. Effect of
risedr-
onate on the risk of hip fracture in elderly women. Hip
Intervention Program Study Group. N Engl J Med. 2001;344:
333340
121. Boonen S, Laan RF, Barton IP, Watts NB. Effect of
osteopo-
rosis treatments on risk of non-vertebral fractures: review
and
meta-analysis of intention-to-treat studies. Osteoporos Int.
2005;16:12911298
122. Chavassieux PM, Arlot ME, Reda C, Wei L, Yates AJ,
Meunier
PJ. Histomorphometric assessment of the long-term effects of
alendronate on bone quality and remodeling in patients with
osteoporosis.J Clin Invest. 1997;100:14751480
123. Adachi JD, Bensen WG, Brown J, et al. Intermittent
etidr-
onate therapy to prevent corticosteroid-induced
osteoporosis.
N Engl J Med. 1997;337:381387
124. Saag KG, Emkey K, Schnitzer TJ, et al. Alendronate for
the
prevention and treatment of glucocorticoid-induced osteopo-
rosis. Glucocorticoid-Induced Osteoporosis Intervention
Study Group. N Engl J Med. 1998;339:292299
125. Chesnut CH, Skag A, Christiansen C, et al. Effects of
oral
ibandronate administered daily or intermittently on fracture
risk in postmenopausal osteoporosis. J Bone Miner Res. 2004;
19:12411249
126. Reid IR, Brown JP, Burckhardt P, et al. Intravenous
zoledronic acid in postmenopausal women with low bone
mineral density. N Engl J Med. 2002;346:653661127. Glorieux FH,
Bishop NJ, Plotkin H, Chabot G, Lanoue G,
Travers R. Cyclic administration of pamidronate in children
with severe osteogenesis imperfecta.N Engl J Med. 1998;339:
947952
128. Rauch F, Glorieux FH. Osteogenesis imperfecta, current
and
future medical treatment. Am J Med Genet C Semin Med Genet.
2005;139:3137
129. Borah B, Ritman EL, Dufresne TE, et al. The effect of
risedr-
onate on bone mineralization as measured by micro-
computed tomography with synchrotron radiation: correla-
tion to histomorphometric indices of turnover. Bone.2005;37:
19
130. Borah B, Dufresne TE, Chmielewski PA, Gross GJ, Prenger
MC, Phipps RJ. Risedronate preserves trabecular architecture
and increases bone strength in vertebra of ovariectomized
minipigs as measured by three-dimensional microcomputed
tomography.J Bone Miner Res. 2002;17:11391147
131. Borah B, Dufresne TE, Chmielweski PA, Johnson TD,
Chines
A, Manhart MD. Risedronate preserves bone architecture in
postmenopausal women with osteoporosis as measured by
three-dimensional microcomputed tomography. Bone. 2004;
34:736746
132. Lalla S, Hothorn LA, Haag N, Bader R, Bauss F. Lifelong
administration of high doses of ibandronate increases bone
mass and maintains bone quality of lumbar vertebrae in rats.
Osteoporos Int. 1998;8:97103
133. Bauss F, Lalla S, Endele R, Hothorn LA. Effects of
treatment
with ibandronate on bone mass, architecture, biomechanical
properties, and bone concentration of ibandronate in
ovari-ectomized aged rats. J Rheumatol. 2002;29:22002208
134. MashibaT, Mori S, Burr DB, et al. The effects of
suppressed
bone remodeling by bisphosphonates on microdamage accu-
mulation and degree of mineralization in the cortical bone
of
dog rib. J Bone Miner Metab. 2005;23(suppl):3642
135. Mashiba T, Hirano T, Turner CH, Forwood MR, Johnston
CC,
Burr DB. Suppressed bone turnover by bisphosphonates in-
creases microdamage accumulation and reduces some biome-
chanical properties in dog rib. J Bone Miner Res. 2000;15:
613620
136. Flora L, Hassing GS, Cloyd GG, Bevan JA, Parfitt AM,
Villa-
nueva AR. The long-term skeletal effects of EHDP in dogs.
Metab Bone Dis Relat Res.1981;3:389300
137. Odvina CV, Zerwekh JE, Rao DS, Malouf N, Gottschalk FA,
PEDIATRICS Volume 119, Supplement 2, March 2007 S161at
Pontificia Universidad Catolica de Chile on August 18,
2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
14/15
Pak CY. Severely suppressed bone turnover: a potential com-
plication of alendronate therapy. J Clin Endocrinol Metab.
2005;90:12941301
138. Ott SM. Long-term safety of bisphosphonates. J Clin
Endocri-
nol Metab. 2005;90:18971899
139. Whyte MP, Wenkert D, Clements KL, McAlister WH, Mumm
S. Bisphosphonate-induced osteopetrosis.N Engl J Med.2004;
349:457463
140. Monier-Faugere MC, Geng Z, Paschalis EP, et al.
Intermittent
and continuous administration of the bisphosphonate iban-
dronate in ovariohysterectomized beagle dogs: effects on
bone morphometry and mineral properties.J Bone Miner Res.
1999;14:17681778
141. Bauss F, Schenk RK, Hort S, Muller-Beckmann B, Sponer
G.
New model for simulation of fracture repair in full-grown
beagle dogs: model characterization and results from a long-
term study with ibandronate. J Pharmacol Toxicol Methods.
2004;50:2534
142. Little DG, McDonald M, Bransford R, Godfrey CB, Amanat
N.
Manipulation of the anabolic and catabolic responses with
OP-1 and zoledronic acid in a rat critical defect model. J
Bone
Miner Res.2005;20:20442052
143. Kurth AH, Eberhardt C, Muller S, Steinacker M, Schwarz
M,
Bauss F. The bisphosphonate ibandronate improves
implantintegration in osteopenic ovariectomized rats. Bone.
2005;37:
204210
144. Wilkinson JM, Eagleton AC, Stockley I, Peel NF, Hamer
AJ,
Eastell R. Effect of pamidronate on bone turnover and im-
plant migration after total hip arthroplasty: a randomized
trial. J Orthop Res. 2005;23:18
145. Little DG, Smith NC, Williams PR, et al. Zoledronic
acid
prevents osteopenia and increases bone strength in a rabbit
model of distraction osteogenesis. J Bone Miner Res.
2003;18:
13001307
146. Little DG, Peat RA, Mcevoy A, Williams PR, Smith EJ,
Bal-
dock PA. Zoledronic acid treatment results in retention of
femoral head structure after traumatic osteonecrosis in
young
Wistar rats. J Bone Miner Res. 2003;18:20162022
147. Lai KA, Shen WJ, Yang CY, Shao CJ, Hsu JT, Lin RM. The
use
of alendronate to prevent early collapse of the femoral head
in patients with nontraumatic osteonecrosis: a randomized
clinical study. J Bone Joint Surg Am. 2005;87:21552159
148. Little DG, McDonald M, Sharpe IT, Peat R, Williams P,
McE-
voy T. Zoledronic acid improves femoral head sphericity in a
rat model of Perthes disease. J Orthop Res. 2005;23:862868
149. Nancollas GH, Tang R, Phipps RJ, et al. Novel insights
into
actions of bisphosphonates on bone: differences in interac-
tions with hydroxyapatite. Bone. 2006;38:617 627
150. Sauty A, Pecherstorfer M, Zimmeroth I, et al.
Interleukin-6
and tumor necrosis factor alpha levels after bisphosphonates
treatment in vitro and in patients with malignancy. Bone.
1996;18:133139
151. Schweitzer DH, Oostendorp-vande Ruit M, van der Pluijm
G,
Lowik CWGM, Papapoulos SE. Interleukin-6 and the acute
phase response during treatment of patients with Pagets
disease with the nitrogen-containing bisphosphonate dimeth-
ylaminohydroyxpoproylidene bisphosphonate. J Bone Miner
Res. 1995;10:956962
152. Sanders JM, Ghosh S, Chan JM, et al. Quantitative
structure-
activity relationships for gammadelta T cell activation
bybisphosphonates.J Med Chem. 2004;47:375384
153. Thompson K, Rogers MJ. Statins prevent bisphosphonate-
induced gamma, delta T-cell proliferation and activation in
vitro. J Bone Miner Res. 2004;19:278288
154. Gabelli SB, McLellan JS, Montalvetti A, Oldfield E,
Docampo
R, Amzel LM. Structure and mechanism of the farnesyl
diphosphate synthase fromTrypanosoma cruzi: implications for
drug design. Proteins. 2005;62:80 88
155. Szabo CM, Matsumura Y, Fukura S, et al. Inhibition of
gera-
nylgeranyl diphosphate synthase by bisphosphonates and
diphosphates: a potential route to new bone antiresorption
and antiparasitic agents. J Med Chem. 2002;45:21852196
S162 RUSSELLat Pontificia Universidad Catolica de Chile on
August 18, 2014pediatrics.aappublications.orgDownloaded from
http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/http://pediatrics.aappublications.org/
-
8/11/2019 Graham 2014 Bifosfonato
15/15
DOI: 10.1542/peds.2006-2023H2007;119;S150Pediatrics
R. Graham G. RussellBisphosphonates: Mode of Action and
Pharmacology
ServicesUpdated Information &
_2/S150.full.htmlhttp://pediatrics.aappublications.org/content/119/Supplementincluding
high resolution figures, can be found at:
References
_2/S150.full.html#ref-list-1http://pediatrics.aappublications.org/content/119/Supplementfree
at:This article cites 125 articles, 19 of which can be accessed
Citations
_2/S150.full.html#related-urlshttp://pediatrics.aappublications.org/content/119/SupplementThis
article has been cited by 17 HighWire-hosted articles:
Subspecialty Collections
s_subhttp://pediatrics.aappublications.org/cgi/collection/therapeuticTherapeutics
ogy_subhttp://pediatrics.aappublications.org/cgi/collection/pharmacolPharmacologythe
following collection(s):
This article, along with others on similar topics, appears
in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables)
or in its entirety can be found online at:Information about
reproducing this article in parts (figures,
Reprintshttp://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN:
1098-4275.Grove Village, Illinois, 60007. Copyright 2007 by the
American Academy of Pediatrics. Alland trademarked by the American
Academy of Pediatrics, 141 Northwest Point Boulevard,
Elkpublication, it has been published continuously since 1948.
PEDIATRICS is owned, published,PEDIATRICS is the official journal
of the American Academy of Pediatrics. A monthly
http://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.htmlhttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.htmlhttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.htmlhttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.htmlhttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#ref-list-1http://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#ref-list-1http://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#ref-list-1http://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#ref-list-1http://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#related-urlshttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#related-urlshttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#related-urlshttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#related-urlshttp://pediatrics.aappublications.org/cgi/collection/therapeutics_subhttp://pediatrics.aappublications.org/cgi/collection/therapeutics_subhttp://pediatrics.aappublications.org/cgi/collection/therapeutics_subhttp://pediatrics.aappublications.org/cgi/collection/pharmacology_subhttp://pediatrics.aappublications.org/cgi/collection/pharmacology_subhttp://pediatrics.aappublications.org/cgi/collection/pharmacology_subhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/reprints.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtmlhttp://pediatrics.aappublications.org/cgi/collection/therapeutics_subhttp://pediatrics.aappublications.org/cgi/collection/therapeutics_subhttp://pediatrics.aappublications.org/cgi/collection/pharmacology_subhttp://pediatrics.aappublications.org/cgi/collection/pharmacology_subhttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#related-urlshttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#related-urlshttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#ref-list-1http://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html#ref-list-1http://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.htmlhttp://pediatrics.aappublications.org/content/119/Supplement_2/S150.full.html