Embed Size (px)
Citation preview

GP INFORMATION EVENING – MAY 11TH 2017
Dr Nicola YuenClinical Director Obstetrics and Gynaecology / Deputy Chief Medical Officer

Introduction
Dr Nicola Yuen – Clinical Director of O&G
Dr Shobie Shobanan – Staff Specialist O&G
Dr Kishor Singh – Staff Specialist O&G
Dr Sarah Van Der Wal – Staff Specialist O&G

O&G Department at Bendigo Health
New hospital opened in January 2017
Department restructured in late 2016 and implementation of new structure in February 2017

O&G Department Restructure
The process of reviewing the structure considered:
• Identifying service gaps and reviewing the appropriateness and configuration of services
• Best practice in models of care
• Maintaining and improving patient access to care
• Flexibility of clinical systems to respond quickly to changing environments
• Improving consistency and quality of care, safety and clinical governance
• Workforce planning, ensuring the right clinical teams in the right place at the right time
• Strengthening partnerships with our regional hospitals and referring GPs including driving shared care and education

Staffing – Senior Medical Staff O&G
• Director of O&G (0.5FTE)
• 3 full time staff specialists – at least 2 are working M-F 0730-1730; 1 is rostered to birth suite with no other responsibilities
• 5 VMOs providing sessional support for clinic and theatre as well as after hours cover

Staffing - Junior Medical Staff - O&G
• Senior Registrar
• 2 accredited RANZCOG trainee Registrars
• 3 unaccredited Registrars (12 month positions)
• 2 Advanced Diploma GP Registrars (12 month positions)
• 1 Senior RMO (6 month position)
• 3 HMOs ( 3 month position)

What does this mean for the GPs?
More staff available to answer calls!
Birth Suite Reg 54546018 (24 hrs / 7 days)
Assessment Reg 54547205
Monday – Friday 0730-1730 – Birth Suite Consultant; Birth Suite Registrar; Assessment / EPAS Registrar
After hours – 24 hour in hospital Registrar cover (including weekends); Consultant

Models of Care
• A range of models of care will need to be available to reflect clinical needs, safety factors and woman’s choice, and reflect the complexity of care required.
• The aim is to provide responsive and integrated models of care.
• The models will aim to ensure continuity of care for the woman whilst reducing a fragmented approach to care.

Obstetric Clinics
Each week
• 4 Booking in Clinics
• 3 Obstetric Clinics (high risk)
• 1 multidisciplinary Diabetes in Pregnancy Clinic
• 4 Midwives Clinics (low risk)
• Assessment Centre 0900-1700 Mon-Fri

Shared Care
• Process currently being reviewed to bring in line with other maternity hospitals
• Process of accreditation
• E-credential system
• Access to ongoing education from Bendigo Hospital

Documentation for Shared Care
• Medical Registration
• Medical Indemnity Insurance
• Practice Accreditation certificate
• Evidence of postgraduate qualifications
• Referees
• Signed agreement of care
Ongoing accreditation as SMCA
Triennial (as per CPD triennium with RACGP / ACCRM)
Under development
Will require evidence of ongoing CPD relevant to Obstetrics

Gynae Clinics
Each week
• 3 General Gynae clinics
• 2-3 Colposcopy sessions
• 1 Gyn Assessment clinic (post-op reviews; urgent reviews etc)
• 1 Family Planning clinic
• 1 Choices clinic
• EPAS Mon-Fri 0900-1700

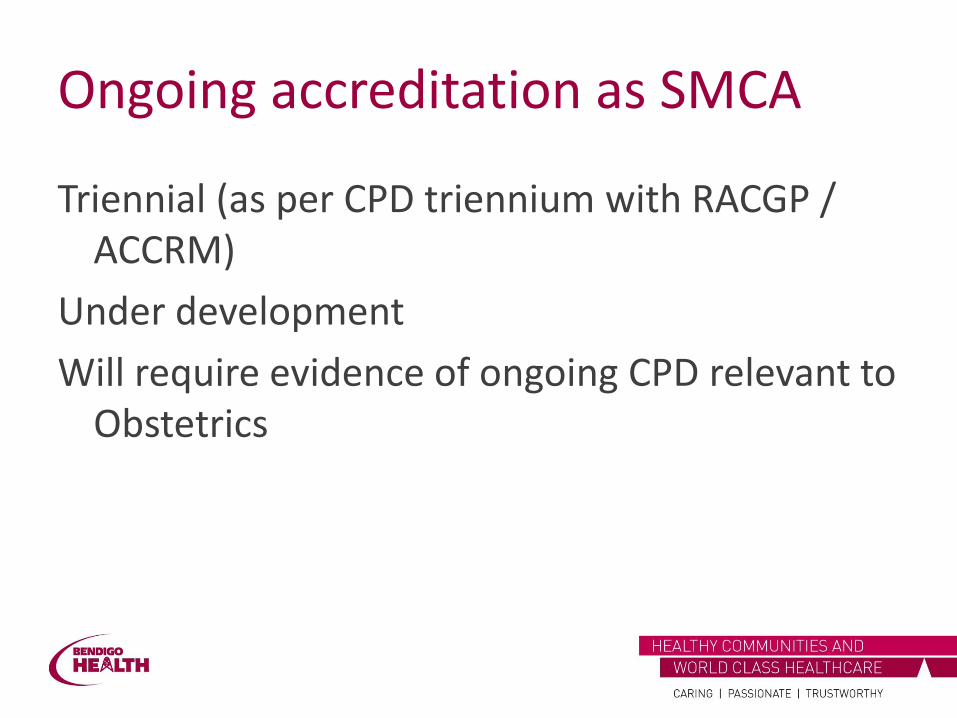
Referrals into the O&G Unit

Obstetric referrals
Booking in appointment with MW at 15-18 weeks unless otherwise indicated
Triaged after booking by Consultant O&G to either low or high risk care and plan for care made
Schedule of visits followed for high or low risk care
All patients seen at 34-36 weeks by O&G Consultant or accredited Registrar
Gynae referrals
Women’s Clinics Referral Triaging Guidelines for Gynae, Colposcopy, Pap, Surgical, TOP and FPC
Requires workup investigations to be accompany referral
• Urgent – refer to ED
• Cat 1 – receive and attend apt within 30 days
• Cat 2 – receive and attend apt 30-90 days
• Cat 3 – receive and attend apt within 365 days

Gynae triage guidelines
Cat 1 – Immediate
Conditions requiring immediate assessment and management in ED – These referrals will not be accepted by Women’s Clinics – results and referrals midwife will phone woman, phone GP and ED and forward referral and investigations to ED.
Excessive blood loss (send to ED)
Severe, debilitating abdominal or pelvic pain (send to ED)
Acute Bartholin’s abscess (send to ED)

Gynae Triage guidelines
CHOICES CLINICS (STOP) AND EPAS REFERRALS
Category 1 – to receive and attend appointment within 30 days (dependent on EDD)
• Surgical termination of Pregnancy: only performed <12/40 at BH
• EPAS: dependent on EDD

Gynae triage guidelines
Urgent – to receive & attend apt within 30 days
Asymptomatic ovarian cyst in women >40 yrs (specified cyst >8cm) Hyperplasia with endometrium > 12mm in all women Malignancy detected on a pap smear – Category 1 Colposcopy Ovarian cyst with pain (>8cm) Peri menopausal bleeding with endometrial lining >12mm Ultrasound report Post-coital bleeding – Category 1 Colposcopy if abnormal pap smear, or abnormal
appearance of cervix PAP results Post-menopausal bleeding pelvic with ultrasound/FBE Prolapse –with urinary retention (consider treating in ED) Severe pelvic pain (consider treating in ED) Unilocular cyst > 50 years of age (>5cm) Pain and Bleeding in Pregnancy – Category 1 EPAS

Unavailable services at Bendigo Hospital
• Medical Termination of Pregnancy - < 8/40 not done at BHCG
Results and referrals midwife will refer to Bendigo Community Health Centre (BCHC) after discussion with woman (phone 54481600, fax 54481699)
• Reversal of tubal ligation – not done at BH. GP notified that referral not accepted
• IVF – advise of local availability and advise GP to refer woman to Monash IVF website

How does this affect GPs?
Guideline provides recommended and mandatory (*) investigations to accompany referral
Abnormal pap smear Pap smear results history * HPV vaccination history If at-risk of STI, high vaginal swab MC&S and STI screen (endocervical swab for chlamydia and gonorrhea PCR, others as indicated)
Pelvic pain Serum b-HCG * Pelvic ultrasound * High vaginal swab MC&S * STI screen (endocervical swab chlamydia and gonorrhea PCR, others as indicated) * Urine MC&S *

Our performance
55%
62% 61%
78%
70%
81%
89%
79%
65%
58%
68%
85%
0
5
10
15
20
25
30
35
40
45
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr 2016 May 2016 Jun 2016 Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017 Mar 2017
Urgent Ref Count Urgent w/in 30 Days

Gynae Elective Surgery Waiting List
0
20
40
60
80
100
120
140
160
180
200
Apr 2016 May 2016 Jun 2016 Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017 Mar 2017

Documentation / communication
• Obstetrics – VMR
• Gynae – letters dictated
Impact of EMR (due for implementation within next 12 months)

Questions??

EARLY PREGNANCY ASSESSMENT
Dr Sarah van der Wal – O+G Staff Specialist

Services offered at Bendigo Health
1. Early Pregnancy Assessment Service
2. Choices Service

Early Pregnancy Assessment Service
• Runs daily
• Both for Initial Assessment and Follow up
• Staffed by Registrar or Senior Resident supervised by Staff Specialist

Scope of Practice of EPAS
• Early Pregnancy Loss
• Pregnancy of Unknown Location
• Early Fetal anomalies

Referrals
• Accept internal and external referrals
• Triaged according to risk
• Information required:
– Last Menstrual Period
– All serum bhCGs performed
– Any US performed
– Any significant Medical/Surgical History

Early Pregnancy Loss
• Miscarriage
– Threatened
– Missed
– Incomplete
– Complete
• Pregnancy of Unknown Location
• Ectopic Pregnancy

Diagnostic Guidelines – Early Pregnancy
• 1st Trimester scans should be performed using ASUM guidelines (2015)
• Gestation sac should usually be visible from 4 weeks and 3 days by TV scan
• Must be eccentrically placed and surrounded by echogenic ring – not intra-cavity fluid (pseudosac)
• Fetal heart visible from 2-6 weeks with a high resolution TV scan, may need to be 3-4mm CRL however


Early Pregnancy – Diagnosis
• bhCG >1200-1500 for TV scanning
• bhCG >3000 for TA scanning

Miscarriage
• Transvaginal Scan:
• MSD (mean Sac Diameter) > 25mm with no visible fetal pole
• CRL >7mm but no fetal heart movements for >30 seconds
• Any doubts – a second scan in 1 week

Miscarriage - Treatment
• Conservative/Expectant –
– Reduced risk (surgical)
– More days of bleeding and greater amount of bleeding
– Approximately 10% of women will require subsequent surgical management
– Efficacy is lower and may take several weeks if intact sac

Miscarriage – Treatment
• 2. Medical
– Misoprostol – 800mc vaginally, 3 hourly, give 2 doses and leave to work for 1-2 weeks (Misoprostol.org), OR 800mcg, 2 doses, 24 hours apart
– Incomplete m/c – 600 mcg
• This Service is not currently offered by Bendigo Health Care Group. If your patient wishes to pursue this you may need to refer elsewhere

Miscarriage Treatment
• 3. Surgical
– Suction Curettage
• General Anaesthetic
• Consider Misoprostol for pre surgical priming (200-400mcg PV or Oral)
• Higher risks – Surgical

Gestational Trophoblastic Disease
• Characteristic US appearance of Complete Mole – Snow storm or Bunch of Grapes.
• More difficult to diagnose Partial Molar pregnancies
• Require Suction Curettage – cannot be treated by medical means
• Follow up via the Women’s Mole Registry


Pregnancy of Unknown Location
• Neither intra-uterine or Extra-uterine
• If bhCG over 1500 and not seen on TV US
• Needs serial 48 hourly bhCG to establish if:
• Early Pregnancy (↑)
• Failing Pregnancy (↓)
• Possible Ectopic (↔)

Ectopic Pregnancy
• Pregnancy located outside the endometrial cavity
• In an unstable patient: treated surgically
• In a stable patient – may consider medical management


Medical Management of Ectopic Pregnancy
• Haemodynamically stable
• NO Intraperitoneal bleeding on the basis of clinical or ultrasound findings
• NO FHR activity on Ultrasound
• Adnexal mass ≤3 cm on Ultrasound
• bhCG ≤ 3000 IU/I
• No pelvic pain
• No contraindications to medical management

Medical Management of Ectopic Pregnancy
• Methotrexate: 50mg/m2
• Requires Normal LFT’s, UEC and FBC prior
• Monitor the above: Day 4, 7, and then weekly with bhCG

Early Fetal Anomalies
• Counselling and referral service
• We refer primarily to the Womens MFM unit
• In the case of a positive FTS – we offer the women NIPT +/- referral

CHOICES
• Fortnightly service for Surgical Termination of Pregnancy
• Requires proof of intrauterine pregnancy (Ultrasound)
• HVS and Chlamydia PCR (endocervical swab)
• Clinic runs on a Monday for the surgical list on a Friday

References
1. ASUM Guidelines for the Performance of First Trimester US May 2015
2. Queensland Clinical Guidelines on Early Pregnancy Loss – Queensland Department of Health July 2015

DYSFUNCTIONAL UTERINE BLEEDING
Dr Kishor SinghStaff Specialist OBGYNBendigo Health

Definition
DUB is defined as any AUB in the absence of pregnancy, infection, neoplasm and systemic disease
Other definitions of DUB:
• AUB without any palpable pelvic pathology
• AUB without any organic pelvic disease
AUB is defined as any variation from the normal menstruation in regard to cyclicity, frequency, volume & duration
Normal Menstruation:
• Cycle: 28 ±7d (5th & 95th centile ~23 to 39.4 d)
• Duration: 2 to 7 days; max 8 days
• Amount of blood loss: 30 to 40 ml; Max 80 ml
• Subjective assessment of MBL is clinically more applicable

Traditional nomenclature of AUB
Menorrhagia = Heavy cyclical periods in terms of duration and/or volume
Metrorrhagia = Irregular periods that includes IMB
Menometrorrhagia = Irregular heavy periods (duration and/or volume)
Oligomenorrhoea = Longer cycle meaning infrequent periods
Oligomenorrhagia = Infrequent heavy periods (duration and/or volume)
Polymenorrhoea = Shorter cycle meaning frequent periods
Polymenorrhagia = Frequent heavy periods (duration and/or volume)

Proposed standardized nomenclature by using descriptive terminology for Abnormal Uterine Bleeding
Heavy menstrual bleeding for MenorrhagiaIntermenstrual bleeding for Metrorrhagia
To discard the term ‘Dysfunctional Uterine Bleeding’
Classified AUB depending on the cause
___________________________________________________________________________________________
For example:
Introduced 9 categories expressed as an acronym PALM-COEIN

AUB-CAUB-OAUB-EAUB-IAUB-N
PALM-COEIN Classification of AUB:
Important shortcomings:
Does not include all the causes
DUB comes as AUB-O or AUB-E
Malignancy is included as AUB-M
Not accepted by all
“Dysfunctional Uterine Bleeding” still exists
10% of gynecological problems
Important cause of anemia
Commonest benign indication for hysterectomy
________________________________________________________________________________________
AUB-PAUB-AAUB-LAUB-M
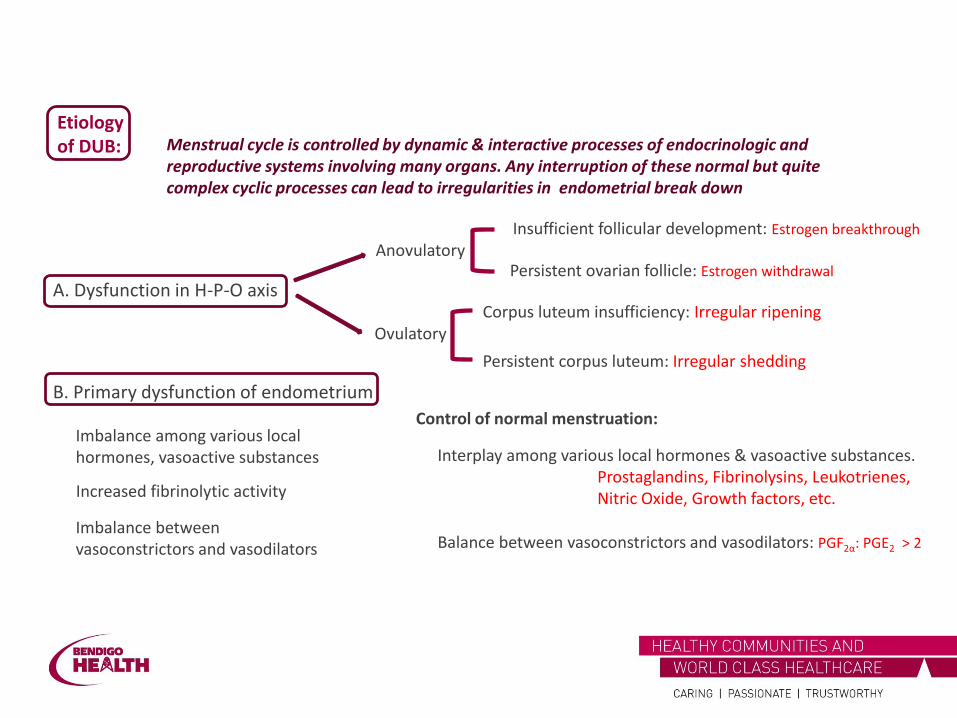
Etiologyof DUB:
A. Dysfunction in H-P-O axis
B. Primary dysfunction of endometrium
Anovulatory
Ovulatory
Insufficient follicular development: Estrogen breakthrough
Persistent ovarian follicle: Estrogen withdrawal
Corpus luteum insufficiency: Irregular ripening
Persistent corpus luteum: Irregular shedding
Imbalance among various local hormones, vasoactive substances
Control of normal menstruation:
Interplay among various local hormones & vasoactive substances.Prostaglandins, Fibrinolysins, Leukotrienes,Nitric Oxide, Growth factors, etc.
Balance between vasoconstrictors and vasodilators: PGF2α: PGE2 > 2
Increased fibrinolytic activity
Menstrual cycle is controlled by dynamic & interactive processes of endocrinologic and reproductive systems involving many organs. Any interruption of these normal but quite complex cyclic processes can lead to irregularities in endometrial break down
Imbalance between vasoconstrictors and vasodilators

Mechanism of menstruation: Progesterone withdrawal
Leakage of lysosomal PG synthetase
PGF2α > PGE2 (2:1) Spiral arteries vasoconstrictionIschaemic necrosis of endometrium
Extravasation of RBCs in the stroma
Converts Arachidonic acid in endometrium to PGF2α and PGE2
PGI2 in endometriumVasodilatation and Inhibition of platelet aggregation Nitric oxide
Menstruation
Primary haemostasis: Platelets plug & fibrin thrombi in the spiral arteries Shed in first 24 hours
Second day: Haemostasis maintained by Spiral artery vasoconstriction & Endothelial swellingRepair process starts by re-epithelization of basal layer
Diffuses into myometrium PG is converted to PGI2
Repair process mediated by Epidermal growth factor and VEGF (its production is stimulated by estrogen & hypoxia)Fibrinolysis: Necessary to deter scarring and obliteration of endometrial cavityPlasminogen activator production is stimulated by estrogen and inhibited by progesterone
More PG Other vasoconstrictors:Endothelin & PAF

Evaluation and Diagnosis:
Aim is to exclude any cause enumerated in the definition
Clinical: History and complete examination
Ultrasound of pelvis
Beta hCG
FBC & Coagulation profile
Endometrial evaluation:
Endometrial biopsy: Pipelle
Hysteroscopy and D&C
Special investigations : as warranted
Irregular ripening
Irregular shedding
Premenstrual:Patchy secretory
Postmenstrual:Patchy proliferative
Investigations:Endometrial histology:
ProliferativeSecretory
Hyperplasia

Factors to be considered:
♦ Age
♦ Amount of bleeding
♦ Infertility
♦ Iron deficiency anaemia
♦ Contraception and future pregnancy
♦ Cost and side effects of therapy; personal & cultural preference
Management:
A. General
B. Medical:
C. Surgical:
▪ Stabilize hemodynamic state
▪ Correction of anemia
▪ Menstrual calendar
▪ NSAIDS
▪ Non-specific hemostatics
▪ Antifibrinolytics
Hormone therapy
▪ Endometrial ablation
▪ Hysterectomy
Non-hormonal
▪ Progestin, OCP, Estrogen ▪ Mirena
Modalities:

Non-hormonal Medical Therapy
Does not interfere with H-P-O axis
Can be combined with other modalities
Reduction of MBL by 25 to 50%
A. NSAIDS: Mefenamic acid, Naproxen, Ibobrufen, etc. & COX-2 inhibitors
– More effective when given about 7 days prior to period in ovulatory DUB
– Can reduce dysmenorrhoea, headache
– Mefenamic acid – additional inhibiting effect on PG receptor binding
B. Antifibrinolytics: Tranexamic acid
– More effective but may produce side-effects
– Non-specific hemostatics: Ethamsylate, Daflon
Cochrane 2013: NSAIDs are more effective than placebo;less effective than tranexamic acid or Mirena; no significant difference in efficacy between other medical treatments

Hormonal Medical Management
Very effective and failure to control with this therapy generally excludes DUB
In an acute bleeding situation, if the bleeding does not abate in 24 h, other diagnostic possibilities (Polyp, pregnancy disturbances & neoplasia) should be excluded
Different medications are used (Progestin, OCP, Estrogen) and the choice
– Is based on physiology of normal menstruation and etiopathogenesis of abnormal bleeding
– Depends on its appropriateness and acceptability to the patient

Hormonal: Progestin Therapy
Logical indications: Anovulation and Corpus luteum insufficiency
High dose followed by a lower standard dose: – Indicated in acute bleeding– Norethisterone 20-30 mg daily till bleeding stops followed by 5mg for 21 days
Second half therapy:
– 10 days from D 16 to 25 (Norethisterone or MPA)– Best suited for endometrial protection in anovulation & corpus luteum
insufficiency
Whole cycle therapy:
– 21 days from Day 5 to Day 25 (Norethisterone or MPA)– Suited for Endometrial hyperplasia– Ovulatory DUB: by correcting local hormone imbalance in endometrium– Also effective in anovulation where estrogen is contraindicated
Hormonal: Oral combined pills
Can correct any menstrual abnormality if there is no contraindications of its use
Can be used in both ovulatory and anovulatory
Very good choice if contraception is desired
Higher dose to arrest the bleeding followed by normal cyclical regime
Estrogen therapy:
– Insufficient endometrium
– Bleeding has been heavy for many days – likely only basalis layer is left
– Endometrial biopsy yields minimal tissue – atrophic
– Not responded to OCP or progestin
– Must be followed by progestin coverage and withdrawal bleed.

Nonsurgical management of heavy menstrual bleeding: a systematic review. Obstet Gynecol. 2013
Compared the effectiveness of nonsurgical treatments for bleeding control, quality of life (QoL) in women with AUB presumed secondary to endometrial dysfunction.
There were 26 articles. All the therapies were effective to some extent. The reduction of
bleeding are:• NSAIDs - 10-52% and Tranexamic acid - 26-54%
• Luteal-phase progestins - 20% increase in bleeding to 67% reduction
• OCPs - 35-69%; Extended cycle oral progestins - 87%; Mirena - 71-95%;
The authors recommended the use of the Mirena over OCPs, luteal-phase progestins, and NSAIDs.
• Could not recommend about QoL

Strategies
A. Puberty or adolescent DUB (Under 20 yrs)
First line: ▪ General supportive▪ NSAIDS, Antifibrinolytics▪ OCP or Progestin
Subsequent: OCP or Progestin
B. Adult DUB (20 to 40-45 years)
♦ To rule out coagulation disorder
♦ Emphasis on desire of child bearing
First line: same as above
Endometrial evaluation (premenstrual):Pelvic ultrasound with/without Hysteroscopy, D&C
Hormone including Mirena: depends on histology
Last option: Surgical
C. Premenopausal (≥45 years)
Acute emergency: Uterine tamponade with balloon,Androgen (Methyl testosterone), Hemostatic D&C
Surgical management threshold is low
♦ Mostly anovulatory
♦ Both ovulatory and anovulatory
♦Mostly anovulatory
♦ To rule out organic disease/malignancy
Similar to Adult type but Endometrial evaluation is mandatory
♦ Immaturity of H-P-O axis

HYSTERECTOMY IN THE 21 ST CENTURY
Dr Shobanan ( Shobie)Consultant Obstetrician & GynaecologistBendigo Health

What is hysterectomy ?
Surgery to remove the uterus
2nd most common type of surgery for women in USA
(LSCS is the most common surgery)
Historical development :
1813 – Vaginal Hysterectomy for prolapse (Germany)
1843 – Abdominal Hysterectomy ( England)
1989 – Laparoscopic Hysterectomy
Demographics of Hysterectomy :
USA – 33 % by age 60 years ( 600,000/year 2011)
UK / Australia – 17 % by age 60 years

Why is hysterectomy performed?
Pelvic support problems ( prolapse)
Abnormal uterine bleeding
Symptomatic fibroids
Endometriosis / chronic pelvic pain
Gynaecological cancer

Are there any alternatives to hysterectomy?
Depending on the cause –
Prolapse – pessary / conservative mx
Abnormal uterine bleeding – mirena / endometrial ablation
Fibroid uterus – conservative / myosure / GnRhanalogues
Endometriosis / chronic pelvic pain – excision of endo/ medical treat
Gynaecological cancer – chemo / radiotherapy

What structures are removed during hysterectomy?
• Total hysterectomy – uterus include cervix
• Total hysterectomy + B/L salphingectomy –uterus & tubes
• Total hysterectomy + B/L salphingo-oophorectomy – uterus / tubes /ovaries
• Supra cervical / sub total hysterectomy – upper uterus removed ( cervix left)
• Radical hysterectomy – total hysterectomy & structures around uterus

How can hysterectomy be performed?
• Vaginal / abdominal / laparoscopic hysterectomy ( LAVH / TLH)
Decision to perform a certain method of hysterectomy depends on several factors:1) Experience / level of comfort with particular surgical
approach2) Patient condition / pathology – very obese /medical
comorbidity/prolapse3) Indication for surgery / available facilities4) Trained staff to work as a team- Laparoscopic
Hysterectomy

Vaginal Hysterectomy

Vaginal Hysterectomy
Uterus removed through vagina/no abdominal incision
Indications / Suitability :
• Uterine prolapse (at least 1st-2nd degree )
• Size of uterus ideally less than 12 wks
• Enough vaginal access / uterine mobility
• No significant abdominal adhesions
• No known adenexal pathology
• Experience of surgeon

Benefits of vaginal hysterectomy
• Least morbidity of all types of hysterectomy
• Morbidity : VH < laparoscopic hysterectomy < abdominal hysterectomy
• Bleeding usually less than abdominal hysterectomy
• Time duration : usually 1 ½ - 2 hrs
• Hospital stay : usually 2-3 days/healing shorter than abdominal – quick recovery
• Ureteric / bladder injury : much safer , as can retract away from uterine artery pedicle

Abdominal Hysterectomy

Abdominal Hysterectomy
Uterus is removed through an incision in lower abdomen Most common hysterectomy in USA – 63%
Benefits :• can do even with significant adhesions• can do for any size uterus / fibroids• available at any centres with gynaecology service• most common option for obese /morbidly obese
and patient with medical • comorbidity / most suitable for large adenexal
pathology and cancer pathology

Abdominal Hysterectomy
Risk and issues : high risk of infection and other complications such as bleeding , blood clots, nerve & tissue damage
Blood loss usually more than vaginal hysterectomy
Time duration : usually 2-3 hrs
Hospital stay : usually 3-4 days
Safety of ureter & bladder : more risk than vaginal hysterectomy
Analgesia & recovery : more analgesia required/more time to recover
Laparoscopic hysterectomy ( LAVH / TLH / Robotic )
Laparoscopic hysterectomy
• Only requires a few small incisions in abdomen-
• Laparoscope inserted through umbilical port – to view pelvic organs
• Other instruments used to perform surgery – via other small incisions
• Uterus removed via vagina ( less than 12-14 wks size ) or removed piece meal by morcellation/bisection if large in size
• Laparoscopic hysterectomy & vaginal hysterectomy –need more skill than abdominal hysterectomy

Laparoscopic Hysterectomy
Increased popularity due to: • ability to produce more haemostasis• can combine other surgeries at the same time -
adhesiolysis, treat endometriosis & adenexalsurgery
• less post operative analgesia, superior cosmetics, minimal bleeding
• Hospital stay 1-2 days, low risk of infection • Return to normal activities much sooner than
other hysterectomies

Laparoscopic Hysterectomy
Risk and other issues :
• Long learning curve
• Risk of urinary track injuries (ureter, bladder) is higher than other hysterectomy methods.
• Surgery time longer compared to other methods:
anaesthesia, positioning, instrument set up,recovery
• Need good team work for best out come – surgeon/ experienced asst/theatre nurses with lap experience/ good anaesthetist

LAVH / TLH
LAVH ( Laparoscopic assisted Vaginal Hysterectomy ) • Slightly less skill needed than for TLH• Upper pedicles (ovarian ligament, infundibula pelvic
ligament, tanserverce cervical ligament) released laparoscopically (with or without bladder dissection/ uterine artery coagulated and cut) – rest is done through vagina
• Uterus removed via vagina and vault closed• LAVH used when uterine pathology with no descent,
but bladder and rectum prolapse present needing vaginal wall repair

LAVH / TLH
Total Laparoscopic Hysterectomy (TLH) :
• Level 5/ 6 Laparoscopic surgical skill needed
• The whole procedure done laparoscopically and uterus released via vagina as a whole/ bisected/ morcellated
• Vault of vagina closed laparoscopically
• Cystoscopy usually done at the end – to make sure ureteric jets visualised and exclude bladder injury
Done at Bendigo Health – when the patient is suitable and for appropriate indication

Da Vinci Surgery - robotic assisted laparoscopic hysterectomy

Da Vinci - surgery
• Very expensive• Very high skill needed• Hysterectomy performed with help of robotic
machine controlled by surgeon• No shown better outcome – comparing TLH
performed without robotic assistanceProven benefit : surgery can be performed when
patient and surgeon living in different countries Eg: Can get the service of the best surgeon from a different country in the future

Overall number of hysterectomies performed has reduced …
This is due to :
• Pap / HPV test / colposcopy – well advanced cervical screening program
• Effective treatment of pre cancerous cervical disease – Laser / LLETZ / cone biopsy
• Publicised concerns that bowel , bladder & sexual function may be affected
• Other less invasive procedures to treat problems of menstruation – Mirena/Endometrial ablation

Thank you