Embed Size (px)
Citation preview

GP and Primary Care
Update
John Howard, Vijay Nayar & Janet Rutherford
March 2018

Goodbye to….
Dr Cyrus Fernandes – Leaving TPD role in April
Dr Nicholas Foreman - Leaving TPD role in April
Dr Pauline Foreman - Leaving TPD role in April

Welcome to…
Dr Sunil Gupta – AD for Essex (Basildon & Chelmsford)
Dr Krish Radhakrishnan – AD for Essex (Harlow & Southend)
Dr Andrew Wright – AD for Foundation
Dr Samuel Ajetunmobi - TPD Basildon
Dr Janet Malcolm - TPD Cambridge (MAT leave cover post)

HEE….
• New ADs
• M&E Primary Care Programme
• ARCP review
• Review of GP educators by March 2019

PCSE/Performers List
• Capita now solely responsible for PCSE…..
• Application portal progressing!?!
• Pensions – expect problems
• February intake uploaded to NPL
• 2013 Directions to HEE….
• We (still) hope to remove the need for HEE
trainees to be on the NPL from August 2018

Lead Employer
and Contracts….
• New contract appears to be settling….
• StH&K – now taking on Public Health – GP educators…
• Indemnity – central discussions – state backed indemnity..
• In EoE, StH&K will provide from August 2018
• Still seeking solution to apprenticeship levy issue
• OOH – new COGPED guidance in discussion
• New RCGP GP with Extended roles framework

GMC’s General Professional
Capabilities
Curriculum must align by August 2019

Dr Bawa-Garba
• Reflection is our best defence
• Statements from AoMRC, HEE, Defence Societies
• Best guidance letter from Regional Medical Directors

Workforce
• Joint work with NHSE including shared data group
• M&E STP Primary Care Workforce plans
• Specialty training and International GP recruitment
• New support/retention proposals
• GP Nursing – M&E GPN 10 point plan Delivery Board
• PAs
• Clinical Pharmacists
• Medical Assistant Role
• Apprenticeships
• Primary Care Leadership Collaborative
• Preceptorships/Fellowships

Primary Care STP
Workforce Plans
• 71% looking at Primary Care Home with GP at the centre
• Workforce plans are rudimentary – gap with reality
• Capacity and capability at STP level an issue
• Unified capitated budget envisaged in most
• Care provision to units of 30,000-50,000 patients
• Mostly reliant on international recruitment – little creativity
in terms of skill mix
• Regional team is realistic

M&E - GP numbers

2018 ST Recruitment
• 2873 offers made – 200 more applicants appointable
than last year
• 250 on reserve list (london)
• EoE – 331 offers
• We will fill

International GP
Recruitment • Expansion of international recruitment to achieve 5000
target by 2020 – current England aim 3000 GPs
• M&E – aspiration c1,200 international GPs….
• Recruitment agencies – 2 for M&E – select by CV and
then matched to CCG/practices in recruitment exercise in
UK
• HEE commissioning language courses
• Preparatory (observational) phase – HEE education
• HEE will support supervisors
• National discussion and contract – awaiting funding and
timescales

Other elements
• Essex pilot continues
• Learning from Essex…..
• I&R assessments
• Supervised placement in employing practice using
HEE “hub and spoke” model
• April – Norfolk, Waveney and Suffolk
• July - Cambridge and Peterborough
• October – Mid and South Essex

New Retention scheme

GP Nursing 10 Point Plan
• England - £3m this year
• 2017-18 £1m for GPN educational
Leadership
• 2017-18 £1m to map mentors &
Placements
• Support career framework,
Preceptorships, returners etc
• Target increased placements by
15% 2017-18, 20% 2018-19

GP Nursing 10
Point Plan – M&E
• Regional workshop 22nd December
• M&E GPN Conference 21st March, Loughborough
• New GPN leads 0.6(8)WTE in each HEE Local Office
• £23k per STP for 0.2WTE GPN lead nurse – hopefully
will attract matched funding
• c£22k per STP footprint CEPN/TH to increase GP
pre-registration placements
• £50k evaluation of multi-professional preceptorships
at Anglia Ruskin informing HEE nationally

Training hubs (CEPNs)
• Conference 21st March – London
• Nomenclature – CEPN Training Hub
• To be based on STP footprint to feed in to LWAB, but
maintain local network
• M&E programme – 4 months interim funding on STP
footprint for all
• New operating framework
• Post-CCT GP Fellows (q.v.)
• 2019 – 4 Placement pilots

Training Hubs

Postgraduate Medical Placement Fee
Average district general hospital
200 total postgraduate medical posts
50 Trust funded posts
150 national tariff posts
50 undergraduate medical posts
N.B. For ease local tariff posts not included
UG Tariff placement fee total
(£33,286 x 1.2) = £1,997,160
PG Tariff placement fee total
(£12,152 x 1.2) = £2,187,360
Based on MFF of average 1.2
Medical Placement fee total
= £4,184,520

Post CCT GP Fellowships
2017-18 Model: • 19 GP post CCT Fellowships
• 14 PA preceptorships
• 34 GP nurse preceptorships
• £300,200 in total
• GP post CCT - £4,200 + £1,800 = £6,000
• PA preceptor - £3,000 + £1,800 = £4,800
• GP nurse preceptor - £1,700 + £1,800 = £3,500

Post CCT GP Fellowships
2018-19 model:
• M&E programme - Training Hubs/STP joint bids
• Educational and training allowance support : £5k
• 20% (1 day / 2 sessions) salary support for 12 month
programme (to cover the education and training
element only) =£18,963
• Total per Fellowship: £23,963
• 75 across M&E
• Single BMJ advert late March/early April

PAs
• New course payment framework from January 2018 – 510
hours in primary care, £5k programme support and
additional £5k if student contracts to work in GP
• Placements paid at SIFT rate
• Further Primary Care incentives in discussion
• Preceptorship criteria in development
• Physicians Associates Ambassadors appointed – Pauline
Weir, Lauren Rottman

Clinical Pharmacy New pre-registration programme
NHS England Clinical Pharmacist scheme:
• 1500 clinical pharmacists – on track; 3229 practices
• Interim evaluation published
• Surprisingly few problems; patient facing role vs. meds
management; “statement of progress”

Primary Care
Leadership Collaborative
• Now on to 2nd cohort
• Selected as preferred model nationally
• Evaluation positive
• Will continue

Conclusions
• Be optimistic – grasp opportunities
• Things will get more complex
• We need a single primary care
education network and educational
governance
• I believe the values we live by will be
replicated in the next generation
• Use technology…..

Assessment
• Changes in the Gold Guide
• ARCP Development Group
• QA results
• BLS, audit and level 3
safeguarding
• Audio-COTs…….

Gold Guide
• Latest version issued 31.01.2018
• Ability to consider educator reports at
ARCP has been removed
• Usual length of GP extensions changed to
1 year + 6 months
• All panel members need training every 3
years
• ARCP needed prior to an IDT
• More reasons for applying for OOPE

ARCP Development
Group
• A big thank you……………
• Amended panel checklist
• Amended divvy sheets
• Amended panel handbooks
• Various policies agreed eg late
unavailability, COI, TOOT etc
• Local phrases document

QA Results - RCGP
• Reviewed all unsatisfactory and 10% satisfactory outcomes, huge spreadsheet….
• 276 in total
• New indicators
• Record that have reviewed the recommendations of the last panel
• Translate required development points into competencies, rather than list them as actions

QA – main learning
points from satisfactory outcomes
• Mandatory evidence as opposed to
naturally occurring evidence
• Mandatory 5 observed intimate
examinations
• ESRs should be based on eportfolio
evidence only and not on exam results
• And then…..

BLS and the
final ESR
• BLS and AED training in the ST3 year such that it is still in date beyond the trainee’s CCT date
• ALS training if undertaken during GP training and still in date beyond the trainee’s CCT date
• NB ALS training is not a curricular requirement for GP training and so is not eligible for study leave reimbursement
• NB We think BLS may need to be face to face

Audit
• 2 cycle audit or QiA both acceptable
• Trainee needs to have been personally
involved in either of these, although it
might be a group/practice audit
• Could happen at any point during the
training programme
• ES needs to be confident that evidence in
place before ‘ticking’ it off at the final ESR

Level 3
Safeguarding
• Log entry detailing the acquisition of level
3 knowledge eg course, emodules etc
• Certificare and reflections on the above
• At least one more log entry detailing the
practical application of that knowledge eg
case reviews, MDT meeting etc
• Again, the ES needs to be confident that
the evidence is present

A few last things…..
• Form R every year, no matter what
• ATC trainees will now have their ST1 ESR
centrally
• Any breaks in training need to be covered
by an OOP application
• Attending a local ARCP panel is a great
learning opportunity, so do please
volunteer!

Addressing Differential Attainment in Postgraduate Medical Education in the east of England

• Differential attainment is a symptom not a diagnosis
• Causes are complex and multifactorial
• Differential access to the curriculum
• Perceived bias
• Level of support
• Cultural factors
Understanding Differential Attainment

Understanding Differential Attainment
Wider educational & sociocultural
landscape (macro)
Institutional culture & resources (meso)
Individual factors (micro)
Policies
Exam structures
Recruitment
Induction
Support
Assessment
Learning styles
Culture
Language
Interactions

GMC Promoting excellence: standards for medical education and training

Theme 1. Learning environment and culture
• Promoting Cultural competence through Faculty
Development
• Developing Educators who support fairness and diversity in clinical education and training
• Tackling bullying, harassment and discrimination
• Appropriate adherence to the Public Sector Equality Duty

Cultural Competence
Ability to interact with people from different cultures and respond to their health needs
– Individuals and Organisations
Creating a working culture and practices that recognise, respect, value and harness difference for the benefit of the organisation and individuals

•Self-awareness of own culture
•Assumptions
•Stereotypes
•Biases and their impact
Cultural Competence

Theme 2. Educational governance and leadership
• Involve trainees and PPV members in our activities eg faculty board meetings, assessment processes, interviews
• HEE Quality Framework for raising concerns about education and training
• Systems for recruiting, selecting and appointing learners and educators are open, fair and transparent
• Equality, diversity and fairness training for anyone involved in recruitment and selection
• Analysis of E&D to address issues of Differential Attainment

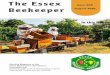
PSU referrals
0
10
20
30
40
50
60
70
80
90
100
Total UK Non-EU EU
total as %
% referred toPSU

Theme 3. Supporting Learners
• All learners have an appropriate induction
– Cultural Induction
• Effective Professional Support Unit
• Learning plans and career advice based on individual needs
• Early warning systems to identify trainees who may face difficulties in training
• Tailored support systems available for all and trainees
• Detailed and constructive feedback for learners

Referral to PSU
Not punitive
Supportive
Confidential
Impartial advice

Performance
Workload Psychological Factors
Life events Sleep Loss
Family Pressure Training and Education
Health Issues Cultural factors

• Psychological support • Occupational Health • LTFT/ OOPC • Placement transfer • Supernumerary placement • Rotations to reduce travel
times • Tackling bullying, harassment
and discrimination
• Exam Support • Communication Skills • Emotional Intelligence
testing • Dyslexia Screening • Careers coaching • Coaching and
Mentorship • Support for Educators
Professional Support Unit

Cultural induction
Support Resilience

Theme 4. Supporting Educators
• Fair recruitment and selection of Educators
• Appropriate induction to their role with regular appraisals and access to professional development
• Faculty of Education and Leadership
• Faculty development to address Cultural Competence and Differential Attainment
• Giving Effective Feedback, Role Modelling, Emotional Intelligence
• Coaching and Mentoring

Theme 5. Developing and implementing curricula and assessments
• Ensure that all learners have equitable access to the curriculum
• Assessments are fair, reliable and valid – ARCP process
• Assessors are appointed using a fair recruitment and selection process
• Encourage and attract a diverse pool of assessors
• Assessors receive training relevant to issues of equality, diversity, fairness and bias
• Detailed and constructive feedback for all candidates
• E&D Analysis of exam and ARCP outcomes

Doctors switching specialty
• Specialty and Associate Specialists (SAS) or Consultant level doctors looking for a career change into general practice
Re-entry doctors
• GP trainees who have passed their Work Place Based Assessment and one of the two required exams (either Applied Knowledge Test (AKT) or Clinical Skills Assessment (CSA))
Top up training
• Overseas trained doctors who are planning on working in the UK but are required to undertake more training to demonstrate equivalence to the CCT via CEGPR route
Targeted GP Training scheme

Thank you
@NHS_HealthEdEng