Embed Size (px)
Citation preview

Governing Body Meeting to be held on Thursday 5th March 2015 at 1:30pm in the Boardroom,
Nutgrove Villa, Westmorland Road, Huyton, L36 6GA
1. Welcome and Introductions
Dr Andrew Pryce
Chair
2. Apologies for Absence
Dr Andrew Pryce Chair
3. Declarations of Interest
Dr Andrew Pryce Chair
4.
Minutes of the Meeting Held on 5th February 2015 & Matters Arising
Document 33(03)01
Dr Andrew Pryce Chair
STRATEGIC/POLICY ISSUES
5.
The Kings Fund/Nuffield Trust: Risk or reward? The changing role of CCGs in general practice The Governing Body is asked to NOTE the content of the report.
Document 33(03)02
Dianne Johnson Accountable Officer
COMMISSIONING
6. Contracting Progress Update 15/16 The Governing Body is asked to NOTE the content of the report.
Document 33(03)03
Philip Thomas Commissioning Director
FINANCE
7. Finance Report The Governing Body is asked to NOTE the content of the report.
Document 33(03)04
Paul Brickwood Chief Finance Officer
GOVERNANCE
8. Corporate Performance Dashboard
a) Performance Report - Commissioned Services
Document 33(03)05
Philip Thomas
Commissioning Director &
Helen Meredith

PART B Please note that due to the nature of the business Part B of the meeting will
take place without press and public being present.
b) Corporate Services Report The Governing Body is asked to NOTE the content of the report.
Head of Quality & Safety/Lead Nurse
9.
Governing Body Assurance Framework Q3 The Governing Body is asked to NOTE the content of the report.
Document 33(03)06
Dawn Boyer Head of Corporate Services
10.
Risk Management Strategy The Governing Body is asked to APPROVE the Risk Management Strategy and DELEGATE authority to the Accountable Officer to approve changes to the risk management templates as required.
Document 33(03)07
Dawn Boyer Head of Corporate Services
COMMITTEE REPORTING
11. Clinical Quality Committee Key Issues The Governing Body is asked to NOTE the content of the update.
Document 33(03)08
Helen Meredith Head of Quality & Safety/Lead
Nurse
MINUTES TO RECEIVE
12. Clinical Quality Committee – December 2014
Document 33(03)09
13.
Finance & Performance Committee – January 2015
Document 33(03)10
14.
Health & Wellbeing Board – December 2014
Document 33(03)11
DATE AND TIME OF NEXT MEETING:
Thursday 2nd April 2015 at 1:30pm Boardroom, Nutgrove Villa
1
Document 33(03)01
NOTES OF THE GOVERNING BODY MEETING held on Thursday 5th February 2015
in the Boardroom, Nutgrove Villa
Present Apology MEMBERS
Dr Andrew Pryce (Chair) Chair Dianne Johnson Accountable Officer Paul Brickwood Chief Finance Officer Dr Ronnie Thong Clinical Lead – Planned Care & Engagement Dr Aftab Hossain Clinical Lead - Prescribing Dr Peter Ayegba Clinical Lead - Mental Health Dr Pervez Sadiq Clinical Lead - Women & Children Dr Paul Conway Clinical Lead - Quality and Safety Dr David Stokoe Clinical Lead - Primary Care Quality Dr Faisal Maassarani Clinical Lead – Strategy & Planning Dr Simon Perritt Clinical Lead – Unplanned Care Dr Robin Macmillan Secondary Care Doctor Peter Murphy Registered Nurse Susan Bramley Lay Member – Audit & Governance Dilys Quinlan Lay Member – Quality & Safety Ruth Austen-Vincent Lay Member – Patient & Public Involvement
IN ATTENDANCE Andrew Thomas Governance Director Helen Meredith Head of Quality & Safety/Lead Nurse Matthew Ashton Assistant Executive Director (Public Health &
Wellbeing), Knowsley Council
Paul Coogan Healthwatch Knowsley Philip Thomas Commissioning Director Present: Andrea Kelly Personal Assistant
1 Welcome and Apologies for Absence: Action
Dr Pryce welcomed everyone to the meeting. Apologies have been received from Dr Faisal Maassarani and Dr Robin Macmillan. Dr Pryce introduced and welcomed Peter Murphy who has joined the Governing Body in the Registered Nurse role. Peter is currently employed as the Deputy Director of Nursing, Governance and Quality at Salford Royal Foundation Trust. Dr Pryce also informed the Governing Body that Helen Meredith has been formally appointed as the Head of Quality & Safety/Lead Nurse within the CCG, having been undertaking the
2
role on an interim basis since October 2014.
2 Declaration of Interest:
There were no declarations of interest made.
3 Minutes of the Meeting Held on 4th December 2014 & Matters Arising:
The minutes of the meeting held on the 4th December 2014 were agreed as accurate. Matters Arising: St Helens & Knowsley Hospitals Trust A&E Waiting Times Andrew Thomas explained that the Trust was achieving the A&E Waiting Times targets in October 2014 on a year to date basis, but on a month-by-month basis had failed the specific target for October 2014. Primary Care Quality Premium Dianne Johnson informed the Governing Body that the first meeting of the Neighbourhub Groups will now take place within March 2015, not February 2015 as previously stated. Communication & Engagement Plan Ruth Austen-Vincent asked for an update as to when the refreshed Communication & Engagement Plan will be ready. Andrew explained the plan has been delayed and the target of Quarter 3 for completion of the plan has been missed. The aim now is to have this plan completed during Quarter 4, and noted that additional communications support has been brought in from North West Commissioning Support Unit to assist with this process. Ruth noted the importance of having a good consultation as part of the development of the plan. Andrew agreed and confirmed that this would form part of the process. Cancer Waiting Times Philip Thomas informed the Governing Body that the information requested around Cancer Waiting Times is available and will be circulated in a briefing format after the meeting. IAPT Philip introduced this item and the accompanying action plan. He explained that 5 Boroughs Partnership NHS Foundation Trust has developed the action plan to ensure that the IAPT service achieves its performance targets. He advised that the key targets

3
covered in the plan are:
• Waiting times (local target) • DNAs (local target) • Prevalence rates (national target) • Recovery rates (national target)
Philip explained that the Trust currently reports weekly to the CCG on progress against the plan, and there is a meeting in the calendar for Monday 9th February 2015 to discuss progress made on the quality of data received from the service. Su Bramley commented that the plan itself is quite difficult to read. Philip acknowledged the importance of having a clear plan of actions to be taken by the Trust, and to have details of the progress made recorded in the one plan. Dr Ayegba has asked the IAPT team for a clearer plan to be created which can be timescale monitored. He confirmed that monthly meetings are taking place and feedback from these meetings will come to a future Governing Body meeting. Paul Coogan referred to Action 1.3 of the plan, which states that administration staff contact clients who have been waiting more than 4 weeks to ascertain whether they wish to remain on the list. Dr Ayegba confirmed that these calls are about reducing the number of appointments that are not kept, not about the therapy itself, therefore it is appropriate for the administration staff to make these calls. Paul Coogan asked if there is any more detailed understanding as to the reasons for the numbers of appointments where a patient does not attend. Dr Ayegba confirmed that work needs to be undertaken to fully understand why the rates are so high. This work will be brought back to the Governing Body to provide a further update. Action – Philip and Dr Ayegba to provide a further update of progress against the action plan at a future Governing Body meeting. Ruth Austen-Vincent informed the Governing Body that Healthwatch is seeking views on the service from patients who are currently within the IAPT service. She also explained that contact will be made with the Engagement Forum to gain a further understanding of patient experience within the IAPT service. Governance Structure for the Primary Care Quality Premium Dianne explained that the first Neighbourhub Assurance Meetings will be taking place in March and dates will be sent out to those involved shortly.
PT/PA
4
Paul Coogan asked if a meeting could be arranged between Healthwatch and the CCG to discuss resource implications in terms of Healthwatch’s involvement in these Assurance Meetings. Dianne confirmed she was happy for this to be arranged, and stressed the importance of having independent scrutiny at these meetings. Action – Andrew Thomas and Paul Coogan to meet and discuss the resource implications of Healthwatch’s involvement in the Neighbourhub Assurance Meetings. Ruth advised that the Primary Care Quality Premium will need to be included within the Communication & Engagement Plan.
AT/PCoo
4 Primary Care Co-Commissioning:
Dianne Johnson introduced this item and the accompanying briefing report which seeks to inform the Governing Body of the options available to the CCG regarding the levels of involvement in the commissioning of primary care medical services, and the decision made by the Clinical Membership Group. Dianne explained that NHS England has recently published guidance in relation to the co-commissioning of primary care medical service from April 2015. NHS England has requested that CCG’s indicated their preferred options for this co-commissioning from the three models:
• Model A: Greater CCG involvement in influencing commissioning decisions made by NHS England area teams.
• Model B: Joint commissioning arrangement, whereby CCGs and area teams make decisions together.
• Model C: Delegated commissioning arrangements, whereby CCGs carry out defined functions on behalf of NHS England and area teams hold CCGs to account for how effectively they carry out these functions.
Dianne explained that joint commissioning arrangements are already employed within the CCG, to support the re-specification and procurement of the Alternative Primary Medical Services (APMS) contracts. Dianne detailed the aims of co-commissioning, which are to achieve greater integration of health and care services, to raise standards of quality within general practice and to tackle health inequalities. Dianne explained that there are a number of duties within primary care medical services that will remain with NHS England regardless of which Model is chosen. These are:
5
• Individual GP Performance Management • Administration of payments and list management • Setting the terms of GMS, PMS and APMS contracts.
Dianne listed the primary care functions that will be included in delegated arrangements:
• GMS, PMS and APMS contracts • Newly designed enhanced services • Design of local incentive schemes • Ability to establish new GP practices • Approving practice mergers • Making discretionary payments
Dianne explained that there will be no increase in running cost allowance in 2015/16 associated with these new responsibilities, so the CCG will have to ensure that its resources are employed effectively. A review of the CCG’s current staff structure will take place. Dianne explained that following a unanimous vote at the Clinical Membership Group meeting on the 9th December 2014, an application for delegated commissioning arrangements was submitted to NHS England. Dianne confirmed that more information is needed before a final decision can be brought back to the Governing Body for consideration. Dianne noted that the CCG does currently have a range of employed staff with experience in primary care contracting, finance and commissioning. In order to ensure good governance, Dianne advised that a Primary Care Commissioning Committee will be established. This Committee will be held in public, chaired by a Lay Member and will have a majority membership of Lay Members and Executive Directors. Dianne noted that GP’s will be in the minority membership to manage potential conflict of interests, but will play a key role within this Committee. The CCG has recently been informed that the submission has been approved by the regional moderation panel, and is awaiting the outcome of national moderation. Paul Coogan confirmed that Healthwatch would be happy to be involved in the Primary Care Commissioning Committee. Dilys Quinlan asked whether the discretionary payments could involve over-performance. Paul Brickwood explained that these payments would generally be made where national rules and regulations stipulate they need to be. These payments relate to national GMA contracts, and some elements of PMS contract.

6
The Governing Body noted the content of the report.
5 Mandate to NHS England for 2015-16:
Andrew Thomas introduced this briefing paper which seeks to inform the Governing Body of the Mandate from the Government to NHS England for 2015/16 and to identify key implications for the CCG. Andrew explained that the Mandate to NHS England 2015/16 retains the objectives which have previously been set out, but sets out additional responsibilities for NHS England relating to innovation and the broader role of the NHS in society. Andrew advised that the Mandate also highlights two specific areas for focus which are around access and waiting times for mental health services and the implementation of the Better Care Fund. Ruth Austen-Vincent noted the partnership arrangement implications, and stated a need to build this into the Communications & Engagement Plan. The Governing Body noted the content of the report.
6 Planning & Contracting 2015-16:
Philip Thomas introduced this item and the accompanying briefing report. The report sets out the requirements for the NHS planning and contracting round for 2015/16 and outlines how the CCG plans to manage the associated tasks. Philip informed the Governing Body that the guidance released in December 2014 requires the CCG to review and refresh its 2015/16 operational plans according to a national timetable. Philip also noted that alongside this review and refresh of the plans, the CCG needs to renegotiate its one year contracts. Philip explained that these two areas will be worked on together to ensure the national requirements are included within contracts. He explained there are clear actions in place, with timescales in relation to the development and agreements of healthcare contracts for 2015/16. These actions will be monitored and managed by a Task & Finish Group which will run until the end of March 2015. Philip advised that the above actions will enable to the CCG to give NHS England a weekly update on progress. He noted however, that the CCG is still waiting for the NHS Standard Contract to be published which will inform some of the further detail. Paul Brickwood highlighted that the issuing of national tariffs has been delayed as the consultation process is not yet completed.

7
He noted there is a real issue here as this may have an impact on contract agreements being agreed prior to year end. The Governing Body noted the content of the report.
7 Community COPD Service Contract Extension:
Dr Conway introduced this report which seeks the Governing Body’s approval for a three month extension to the contract with Liverpool Heart & Chest Hospital NHS Foundation Trust for the delivery of the Community COPD Service. Dr Conway explained that a new community respiratory disease clinical model has been developed, building on the success of the COPD service, and that a detailed service specification is currently in development prior to the commencement of procurement. Dr Conway noted that in the programme plan, the contract for the Community Respiratory Disease Service is due to be awarded in June 2015 and the contract for the current Community COPD service expires on the 31st July 2015, which only allows a maximum of 45 working days to mobilise the new service. Dr Conway explained that if a new provider is awarded the contract, there are risks associated with a maximum 45 day mobilisation period and as such the Governing Body is requested to approve an extension to the current contract to mitigate these risks. Dr Conway confirmed that the total cost of a three month extension is £362,325. Su Bramley asked whether the tender documentation will allow for flexibility. Dr Conway explained that it does, and it is of key importance that patient care is not affected by any changes. Dianne Johnson assured the Governing Body that legal advice has been sought on the contract extension. The Governing Body noted the content of the report and APPROVED a 3 month contract extension to the current Community COPD Service contract.
PT
8 Procurement of Community Respiratory Disease Service:
Dr Conway introduced this item and the accompanying report which seeks the approval from the Governing Body to delegated approval of the service specification for the Community Respiratory Disease Service. Dr Conway informed the Governing Body that there is a lot of action required over a short time scale to complete the procurement of the new Community Respiratory Service prior to the expiry of the contract for the current service.

8
He noted that the specification needs to be signed off and agreed prior to Thursday 12th February 2015, which did not allow enough time for the paperwork to be ready for circulation to this Governing Body meeting. Dr Conway confirmed the proposal of a delegated group to approval the service specification which would include the Accountable Officer, the CCG Chair, Clinical Lead for Quality & Safety, Lay Members for Quality & Safety, Patient & Public Involvement and Audit & Governance and the Chief Finance officer. Ruth Austen-Vincent wished it to be noted and recognised that this service specification has been built on sound engagement with the public and hard to reach groups. Ruth also commented that it is important to ensure patient and public representation in the procurement process. Dr Conway confirmed that there is public representation involved in the process. The Governing Body noted the content of the report and APPROVED delegated decision making arrangements in respect of the service specification for the Community Respiratory Service.
9 NHS 111 Service Procurement:
Dr Perritt introduced this item and the report to ask the Governing Body to approve delegated decision making arrangements in respect of the re-procurement of the NHS 111 Service. Dr Perritt recapped on the background to this procurement and noted that the Governing Body approved via delegated decision making arrangements, a business case for the new NHS 111 Service in October 2014. Dr Perritt advised that procurement is well underway with the interview process taking place on 10th February 2015. He explained that following this interview process, recommendations will be sent to CCG’s on 13th February 2015 with a decision required by the 27th February 2015 which falls between Governing Body meetings. Ruth Austen-Vincent noted that the delegated decision group in October did have a detailed discussion about public involvement in this process and raised it as an issue. She advised that as a result there is now public representation in this process. Dr Pryce asked when the proposed go-live date is for the new service. Dr Perritt advised it is likely to be towards the end of 2015. Dr Pryce informed the Governing Body that Dr Perritt is heading

9
up the clinical input into the NHS 111 Service procurement across the North West. The Governing Body noted the content of the report and APPROVED delegated decision making arrangements in respect of the re-procurement of the NHS 111 Service.
10 Information Governance Strategy & Policies:
Andrew Thomas introduced this item and the accompanying documents which seeks approval of the updated Information Governance (IG) Strategy and supporting IG & IT policies. Andrew explained that the CCG’s IG Strategy and supporting IG and IT Policies are a key component of the organisation’s information governance arrangements. He confirmed that they provide evidence for the annual IG Toolkit submission. Andrew asked the Governing Body to delegate authority to the Accountable Officer to approve the network and information security risk policy. He explained that this policy was not ready to be circulated for this meeting but has since been received and is ready for consideration. Andrew explained that the Governing Body is also being asked to approve a six month extension to the registration authority policy. He explained that this policy outlines the processes by which access to key NHS systems are managed. There have been national delays so there is a requirement to extend the policy pending these delays being resolved. The Governing Body is also asked to approve that the cycle for a full review of the strategy and policies are increased from annually to three year. Andrew explained that this is to reduce workload as in practice; the policies and strategy do not require a review that often. Dr Pryce commented that it is very important that the strategy and polices are correct, and that they are revisited regularly. The Governing Body noted the content of the report and APPROVED:
• the delegation of authority to the Accountable Officer to approve the network and information security risk policy;
• the information governance strategy and policies; • a six month extension to the registration authority
policy; • the cycle for a full review of the strategy and policies
be increased from annually to every three years.
AT/DJ
11 Conflict of Interest Policy:
Andrew Thomas introduced this item and the accompanying
10
report which seeks the approval to an updated CCG Conflicts of Interest Policy. He explained that the proposed changes are as a result of recently published guidance from NHS England and the CCG’s applications for delegated commissioning of primary care medical services. Andrew noted that the main changes to the policy are:
• A new section setting our arrangements for management conflicts and potential conflicts when designing service requirements, as recommended by MIAA;
• Additions to sections incorporating a new procurement template and the requirement to maintain a register of procurement decision taken;
• Additions to incorporate the requirements of primary care co-commissioning
Dianne Johnson explained that the guidance details a need to publish the register of procurement decisions online, alongside the declarations of interest. Dianne noted this is good practice in showing the openness and transparency of the CCG. The Governing Body noted the content of the report and APPROVED the new Conflicts of Interest Policy.
12 Corporate Performance Dashboard:
Andrew Thomas introduced this item and the accompanying presentation which presents the Governing Body with an overview of performance and outcomes in key areas of the local healthcare system, as well as reporting on the financial position and human resources performance indicators. NHS Constitution Standards Cancer Philip Thomas noted there are performance issues in relation to cancer treatment waiting times. He advised that despite this, performance is improving with six of the nine targets now being achieved. He explained that patient choice and complex cases are the reasons for the 62 day breaches. Dilys Quinlan asked why the target was not being achieved for cancer waiting times ‘referrals from an NHS screening service’. Philip agreed to find out this information for Dilys. Andrew Thomas suggested that some months the numbers are really low, which could be the reason for the changes. Action – Philip Thomas to share the reasons for the target not being achieved in relation to cancer waiting times ‘referrals from an NHS screening service’.
PT

11
Ambulance Response Times Philip also drew the Governing Body’s attention to the ambulance response times. He advised that performance against the targets has decreased during this reporting period. Philip explained that as a way of addressing these persistent performance issues the CCG held a multi-agency workshop in January 2015 to understand usage and hotspots and look at ways of addressing this demand. Su Bramley asked whether there is a link between A&E waiting times and ambulance performance. Philip advised that numbers of admissions are part of the whole picture around performance; he noted that ambulance can be queuing if there is no space within A&E. Philip commented that the overall demand for ambulance services has increased; he noted that this demand is slowly starting to reduce and this was identified at the recent workshop. He noted the need for overall system improvement to enable the ambulance performance to improve. Dr Ayegba suggested that some work needs to be done to understand what percentage of ambulance requests are clinically appropriate and with this we could look to educate the public on the best place to call for assistance. Dr Perritt advised that North West Ambulance Services (NWAS) and commissioners are looking closely at this. NWAS examine the nature of all the calls they receive and are also developing alternative pathways for non-emergencies. He also noted that NWAS have found low numbers of inappropriate calls. Matthew Ashton explained that NWAS and Public Health have looked at this issue over the years to determine how best to educate the public. He noted that there is a need to look at what available data on a more Knowsley specific level. Everyone Counts Outcome Measures Health Care Acquired Infections Andrew Thomas noted that there were no new cases of MRSA in November, and fewer Cdiff cases than in recent months. He advised that early January data suggests that new cases are trailing off and the CCG may achieve its trajectory. Stroke Andrew commented that stroke performance has improved after a poor performance in the first quarter. Peter Murphy asked whether overall mortality from stroke data

12
could be included in this dashboard as it would be particularly useful. Helen Meredith explained this is being looked at and is included in the Quality & Safety Workplan. Emergency Admissions Andrew advised the Governing Body that emergency admissions figures are above the plan with a significant increase at Aintree Hospital due to changes in recording. Paul Brickwood explained that until recently, Aintree Hospital did not include patients in its Clinical Decision Unit as a formal admission; this has now changed and is recorded as an admission which has impacted on the figures. Paul advised that a contract query has been raised by South Sefton CCG as a result of this change as there is a financial impact. Paul Coogan asked if the dashboard could include a definition of emergency readmissions and can identify some of the reasons behind these. Andrew Thomas agreed, and explained that feedback from Systems Resilience Groups (SRG’s) are that there are no Knowsley specific discharge issues coming through. Ruth Austen-Vincent asked what constitutes a follow-up in relation to Mental Health Care Programme Approach (CPA). Philip agreed to find this information out. Action – Philip to define what constitutes a follow-up in relation to Mental Health Care Programme Approach (CPA). Dianne Johnson referred to the emergency admissions data and the table showing a comparison between last year’s data and year to date. She noted an improvement in the figures and suggested this data shows the impact of the new services the CCG has commissioned. Andrew commented that the overall position is stable and efforts are improving these figures Finance Paul Brickwood explained that the CCG remains on track to deliver a 1% surplus in 2014/15. He advised that the CCG has used some of its reserves to mitigate areas of overspend as planned. Paul advised that the CCG has received additional funding for winter resilience, mental health investment and payment for quality premiums earned in 2013/14. Paul reported a slight overspend in primary care which is due to changes in national prescribing, but noted this has been offset by an underspend within the home oxygen service. Paul also noted that there is overspend at St Helens & Knowsley Hospitals, Aintree University Hospital, the Royal Liverpool

13
Hospital and Liverpool Women’s Hospital. He explained that reserves have been utilised to mitigate this position. The CCG enters into pooled budgets arrangement with Knowsley MBC under a Section 75 agreement, and Paul advised that all budgets are forecast to be in line with plans aside from the disability pool which reports a forecast surplus at year end. Paul explained this is due to growth in this area being lower than originally anticipated which has resulted in a saving in this area, and the CCG will receive a share of the underspend. Paul referred to the System Resilience Funding for 2014/15 and the table summarising how funding will be spent to deliver the improved outcomes. The CCG received a total of £1.44m, with £111,000 specifically allocated for mental health schemes. Dr Hossain asked whether the increase in spending at Aintree University Hospital is due to the change in coding as previously discussed. Paul confirmed that it is, and a contract query is in place regarding this. Ruth Austen-Vincent asked for some more information about the underspend in the disability pooled budget. Paul explained that the Council administers this particular budget, and the expectation was that 2012/13 and 2013/14 growth would continue but this has proven not to be the case. Ruth asked whether this has been discussed at the Learning Disability Partnership Board and the Physical and Sensory Impairment Partnership Board. Action – Determine whether the disability pooled budget underspend has been discussed at Partnership Board’s. Su Bramley commented that she was surprised that spend had not increased in this area and questioned as to whether there is enough resource to administer this budget. It was agreed to look into this further and bring to a future meeting. Action – Determine if there is enough resource to administer the Disability Pooled Budget and whether this has any impact on the underspend. Dr Conway noted that the primary care budget is showing as green, but advised there are a lot of practices undertaking cost effective prescribing and there is a risk these practices will not feel the benefits of being on track. Dr Ayegba agreed and commented that not all practices are maximising efficiencies. Dilys Quinlan informed the Governing Body that the Medicines Management Workplan has been agreed and is going to the Quality & Safety Committee for noting. The plan encompasses a lot of initiatives to work with partners to improve quality,
PT
PT

14
effectiveness and efficiency. Human Resources Andrew noted that the sickness levels for November were well below the national averages for the NHS and have remained that way to date. Andrew advised that there are a number of staff who were behind on their mandatory training, but there has been a large push for completion which should be reflected in future figures. The Governing Body noted the content of the report.
13 Equality & Diversity Update:
Andrew Thomas introduced this item and briefing report which seeks to update the Governing Body on key activities and progress against the Knowsley Equality Objectives Plan. Andrew noted that this report also seeks approval to the refreshed plan for 2015/16 and the refreshed Equality & Diversity Strategy for 2015-17. Andrew explained that the plan and strategy have been refreshed in line with the CCG’s commissioning priorities, statutory requirements and recent case law. Andrew discussed the key additions to the revised plan which include:
• The new NHS England ‘Accessible Information Standard’ which is about ensuring that NHS service providers give people information in the format which best suits their needs.
• The new Department of Health Workforce Race Standard’ which ensures that employees from black and minority ethnic background have equal access to career opportunities and receive fair treatment in the workplace.
• Equality analysis against key commissioning priorities and embedding this process into the CCG’s programme management process.
Ruth Austen-Vincent welcomed the work around accessible information and offered the support of the Engagement Forum to support this work. Ruth commented that the workforce race standard is very important and asked if standards around disability, particularly around mental health, can be added to this work to ensure it fits the needs of the local population. The Governing Body noted the content of the report and

15
APPROVED the revised Equality Objective Plan for 2015/16 and the updated Equality & Diversity Strategy for 2015-17.
14. Quality & Safety Committee Key Issues & Minutes:
Dianne Johnson reviewed some of the key issues highlighted at the December meeting of the Quality & Safety Committee. She noted that the Medicines Management Workplan has been approved at an earlier meeting today and wanted to acknowledge and thank those involved in the production of the plan. Helen Meredith also reviewed some of the key issues of the December meeting, in particular the ‘Lessons Learnt’ event which was around sharing, learning and bringing together organisation to discuss the perspectives of families of victims of mental health homicides. Dr Pryce noted that the Governing Body needs to be assured of the actions being taken around Child Sexual Exploitation. Matthew Ashton advised this is a key priority for the Children’s Safeguarding Board and there is a lot of work ongoing in this area. Helen informed the Governing Body that the Health Care Acquired Infections sub-group is now established and met yesterday. The Governing Body noted the content of the Key Issues document and received the minutes of the Committee held on the 7th November 2014.
15. Finance & Performance Committee Key Issues & Minutes:
The Governing Body noted the content of the Key Issues document and received the minutes of the Committee held on the 13th November 2014.
16. Audit Committee Key Issues & Minutes:
Su Bramley noted that in the December meeting the Audit Committee received the Governing Body Assurance Framework and felt confident that all areas have been covered and addressed, and were pleased with the level of assurance the Committee could get from this document. The Governing Body noted the content of the Key Issues document and received the minutes of the Committee held on the 19th September 2014.
17. Committee(s) in Common Key Issues & Minutes:
Dianne Johnson explained that the January meeting focused on the Terms of Reference and confirmed she had fed back the

16
comments made by the Governing Body at the last meeting. Dianne confirmed it is explicitly clear that the Governing Body’s of each CCG will make decisions and not the Committee(s) in Common. The Governing Body noted the content of the Key Issues document and received the minutes of the Committee held on the 5th November 2014.
18. Health & Wellbeing Board – Nov 2014
The Governing Body received the minutes of the Health & Wellbeing Board held on the 5th November 2014. Peter Murphy asked whether the CCG had been involved in the Pharmaceutical Needs Assessment (PNA). Helen confirmed that the CCG had been involved. Ruth noted the PNA had a good response and Knowsley had the highest rate in the North West, she passed her thanks onto Healthwatch for their input into this.
19. Details of the next meeting:
Thursday 5th March the Boardroom, Nutgrove Villa Westmorland Road, Huyton
L36 6GA 1:30pm
The Chair opened the meeting to a Question and Answer Session from the public: Q. I have heard that the contract for the visual impairment services is coming to an end soon and is combining with the hearing services contract. Is this correct? Will this joint service have enough specialist staff? A. Philip Thomas – This service is commissioned through the pooled budget arrangements. I will find this out for you and provide feedback. Q. Some people struggle to afford adaptations for their homes that they may need. Will extra care homes help? A. Dr Pryce – This will be looked into as part of the pooled budget management process. Q. I have heard that the disabled facilities grant is transferring from the Council budget to the CCG’s. Will it be ringfenced?

17
A. Philip Thomas – The money for the Better Care Fund includes the disabled facilities grant and will form part of the pooled budget. Within the submissions the CCG has confirmed this money is ringfenced. Paul Brickwood – The Better Care Fund resource will however stay with the Council. Dianne Johnson – We are working on robust governance arrangements for the Better Care Fund to be open and transparent. This will be looked at in further detail and will come back to a future Governing Body meeting. Comment- The i-Van is a fantastic service. I am aware that the Knowsley Director of Public Health in on board will keeping this service when other Merseyside areas have decided to decommission. You have got it right. I attended national pathology week in the Royal and there was a Type 2 diabetic screening service there. Services like this are very good. Perhaps the i-Van could be used for similar services in the community. A. Matthew Ashton – There are competing priorities within the borough. The i-Van is a priority for Knowsley, there are some issues still to be resolved but we are looking to continue this service for 20 days a month within Knowsley. There is information on board around types, signs and symptoms of cancer with a nurse present who can make referrals if needed. Q. I have concerns about the moving of the surgery from Westvale to Tower Hill. This is an elderly parish and it will be difficult for people to access Tower Hill if they do not own a car. We were invited to the new surgery to ask questions about the move, but when we arrived it was just a tour and we did not have the opportunity to ask any questions. A. Dianne Johnson – I can appreciate your feelings about this. At the moment, NHS England has indicated they are happy with the proposal pending consultation with the public. Jacqui Robinson and colleagues at the North West Commissioning Support Unit are currently leading the consultation and I would like to encourage everyone to feed into this process. If you feel you have not had adequate opportunity to ask questions then I can ask for a session to be held to allow this to happen. Q. I have received feedback from Kirkby mental health patients who do not feel they can feed into these types of forums. I am currently in conversation with Paul Mavers at Healthwatch to look to address these concerns. A. Ruth Austen-Vincent – The North West Commissioning Support Unit needs to address this. Dianne Johnson – Please contact Jacqui Robinson at the North West Commissioning Support Unit with these concerns. I will ask Andrew Thomas to raise this for the CCG. Q. I feel I need to further understand the Primary Care Commissioning Committee. It seems concerning that GP’s will not form the majority of this Committee. A. Dianne Johnson – This is an opportunity for the CCG, we do not know the extent of this at the moment. GP’s have agreed and voted for the Primary Care Commissioning Committee to be a Committee of the Governing Body. We need to ensure there is robust governance in place as there is the potential for conflicts of interest. The CCG has yet to sign up to this, we have only expressed an interest so far. Dr Stokoe – This issue here is around conflicts of interest, and ensuring the CCG

18
is open and transparent. I do not share any concerns around the Primary Care Commissioning Committee. Dianne Johnson – Decisions will be made jointly by all members of the Committee. Q. I am concerned by the changing of the definition of admissions by Aintree. Is there anything we can do? A. Paul Brickwood – There is a contract query in place, we are hoping for renegotiations and a settlement that will suit all parties. Q. Who is involved with the National Tariff consultations? Can the public be involved? A. Paul Brickwood – No, the consultation is for provider organisations to have their say regarding the proposals from Monitor. If enough organisations challenge, then Monitor are asked to review and re-consult. At the moment we do not know the prices. Q. How can the CCG be achieving its targets if the provider is not? A. Paul Brickwood – As an example, there are two sorts of urgent attendances.. A&E and Walk in Centres. Urgent attendances will be calculated for Knowsley patients using both A&E and Walk in Centre’s so Knowsley can meet its target overall, but the individual A&E targets can be failing. Dianne Johnson – We do work well with partners to look at a whole system approach. We are achieving targets for Knowsley patients at present but some individual provider targets are failing and we are working hard to support improvements. It can also be vice-versa, the CCG could be failing its target when the provider is meeting it. Comment - The i-Van nurses are fantastic and we should not let this service go. A. Dianne Johnson – Matt has confirmed that the service will continue in Knowsley. Q. Does delegated commissioning mean that doctors can be doing minor surgery in practices? A. Dianne Johnson – Many practices do this already however, this is not the reason for delegated commissioning. Q. Can you definite GMS, PMS and APMS? A. Dianne Johnson – Yes, we will confirm what these mean for you. Q. Why can’t the two care homes who are failing be closed down? A. Dianne Johnson – We don’t have the authority to do this as Knowsley council hold these contracts.
Document 33(03)02
Report to Knowsley Clinical Commissioning Group Governing Body Date of meeting: 5th March 2015
Report title: Kings Fund and Nuffield Trust Research Report: Risk or Reward? The Changing Role of CCGs in General Practice
Report presented by: Dianne Johnson, Accountable Officer
Purpose of the report: The purpose of the report is to share the findings of the recent research programme conducted by the Kings Fund and Nuffield Trust
Recommendations:
Action / Decision required
The Governing Body is recommended to:
Note the contents of the report
Delegated Powers:
For decision reports only
N/A
Commissioning Values Which area(s) does this support? Please insert ‘x’ that apply
1. Patient centred
2. Safe
3. High quality X
4. Cost effective
5. Outcome focused
6. Closer to home
7. Affordable
[one page only]
Page 1 of 62
GOVERNING BODY
KINGS FUND AND NUFFIELD TRUST RESEARCH REPORT: RISK OR REWARD? THE CHANGING ROLE OF CCGS IN GENERAL PRACTICE
Executive Summary The report provides an overview of the Kings Fund and Nuffield Trust second report in their research programme: Risk or Reward? The Changing role of CCGs in General Practice. The report sets out two research areas; GP involvement in CCGs; and CCG involvement in Primary Care development. Although the report shows that CCGs have broadly maintained levels of engagement from their GP members it also highlights that the sustainability of clinical involvement in commissioning is at risk.
The Governing Body is recommended to note the contents of the report.
Page 2 of 62

1. Purpose of the report
1.1 The purpose of the report is to share the findings of the recent research programme conducted by the Kings Fund and Nuffield Trust: Risk or Reward? The Changing role of CCGs in General Practice (Appendix 1).
2. Recommendations
2.1 The Governing Body is recommended to note the content of the research report.
3. Background 3.1 In August 2012 the shadow Governing Body approved the CCGs involvement in a 3 year
research study undertaken by the Kings Fund and Nuffield Trust. The focus of the research was to understand how CCGs are developing, with particular interest in the relationship between CCGs and member practices. Knowsley is one of six CCGs involved in the research, who all have differing demographics and all remain anonymous.
3.2 The first year’s findings were presented to the Governing Body in September 2013 in a
report entitled Kings Fund and Nuffield Trust Clinical Commissioning Groups; Supporting Improvement in General Practice?
3.3 The findings of the second report are derived from a survey (n: 279), 70 interviews,
observations (18 meetings) and reviews of board papers across the six participating CCGs. 4. Key Issues 4.1 The report sets out two research areas; GP involvement in CCGs; and CCG involvement in
Primary Care development. 4.2 GP Involvement in CCGs
4.2.1 The research found that CCGs had broadly maintained levels of engagement from
their GP members. 4.2.2 Similarly to the research findings in 2013, the survey in 2014 shows there remains a
disparity between leaders’ (those with a formal role) and members’ (those with no formal role) sense of ownership. The report highlights that if this disparity continues over time there is a risk of CCGs losing connection with their members and repeating the pattern of diminishing clinical involvement of previous commissioning formations. However, the highest level of ownership was reported in the two smallest CCGs of the six who participated in the study.
4.2.3 The report raises challenges to sustaining GP involvement owing to pressures on
GP time and capacity, opportunity for leadership development, inefficient internal governance structures, limited lead in times to respond to requests from NHS England, and complex external structures.
Page 3 of 62

4.2.4 Recruitment and retention of GPs is highlighted as a potential problem as less than half of GP leaders reported that they had the support, time and resources to undertake their role effectively.
4.2.5 Over the next few years original governing body member’s term of office will come
to an end. To mitigate the risk of all clinical leaders leaving the organisation at the same time, two out of the six CCGs have staggered the terms of office of its governing body members. The report also highlights that there is potential for there to be competition for leaders from the developing GP provider organisations, e.g. GP federations. This could mean there will be multiple local organisations attempting to draw leaders from a fairly small pool of GPs who are interested in a leadership role. The report highlights the need for succession planning and opportunities for leadership development.
4.3 CCG Involvement in Primary Care Development
4.3.1 The second area of research considers the CCGs involvement in Primary Care development.
4.3.2 It was found that CCG leaders and members agreed that their CCG had a
legitimate role in developing Primary Care. This is a change from more cautious views held a year earlier. However, few members felt that it was appropriate to performance manage GPs. This implies that CCGs may face difficulties maintaining good relationships with members if they take on new contract management responsibilities as part of co-commissioning Primary Care.
4.3.3 The report raises three potential challenges for CCGs moving towards co-
commissioning or delegated commissioning of Primary Care. Firstly, it is suggested that CCGs should understand and be clear about the roles and responsibilities of NHS England and the CCG. Clarity is needed so that there is no ambiguity about accountability and support.
4.3.4 The second potential challenge raised in the report is the management of conflicts
of interest, especially as CCGs move to increase the amount of community based care. The report highlights the need to strike a balance between GPs making a useful contribution and managing a potential conflict.
4.3.5 The final challenge raised in relation to co-commissioning Primary Care is the
relationships within the CCG. Although the research suggests that CCGs are having a positive impact on relationships between practices, the report highlights that increasing the amount of contracting with GPs could affect this in the near future, and therefore the ability to sustain clinical commissioning.
5. Implications for the CCG
5.1 The research found that there is disparity between the sense of ownership that GP members have and GP leaders. This implies that the CCG should continue to engage and be led by the membership of the CCG.
5.2 It was found that recruitment and retention of GP leaders could impact on sustaining clinical
engagement. Although the CCG has staggered the terms of office for Governing Body
Page 4 of 62

Clinical Leads, the report suggests that the CCG should continue with succession planning and provide opportunities for leadership development.
5.3 The CCG has expressed an interest in having delegated commissioning responsibility for
commissioning Primary Care. If this is approved, the report suggests the CCG should work hard to maintain the positive relationships within the CCG and manage potential conflicts of interest.
6. Actions being taken by the CCG 6.1 The CCG participates in an annual 360 Stakeholder Survey administered by Ipsos MORI, in
which a representative from each member practice is invited to complete. The research provides the CCG with feedback on how the membership feels they can influence the CCG, are engaged with the CCG and are informed by the CCG. The CCG will continue to engage the membership through the Clinical Membership Group, Protected Time Events and through supporting Primary Care quality.
6.2 Succession planning is done by providing opportunities for clinicians to get involved in the
CCG i.e. procurement of services and highlighted opportunities to participate in Clinical Reference Groups. As detailed in the CCGs constitution, all GPs are invited to express an interest in becoming a Governing Body Clinical Lead.
6.3 The CCG has expressed an interest in having delegated commissioning responsibility for
Primary Care. In order to manage potential conflicts of interest, the CCG will establish a committee of the Governing Body in which four GPs will be non-voting members. This means that they will provide a valued contribution however cannot vote on decisions in which they will benefit.
6.4 The CCG will continue to participate in the King’s Fund and Nuffield Trust research
programme.
7. Summary 7.1 The report provides an overview of the Kings Fund and Nuffield Trust second report in their
research programme: Risk or Reward? The Changing role of CCGs in General Practice. The report sets out two research areas; GP involvement in CCGs; and CCG involvement in Primary Care development. Although the report shows that CCGs have broadly maintained levels of engagement from their GP members it also highlights that the sustainability of clinical involvement in commissioning is at risk. The CCG will continue to build strong relationships with its membership as it moves towards co-commissioning Primary Care, while also managing potential conflicts of interest.
Managerial Lead – Dianne Johnson, Accountable Officer
Signatory details: Angela Watson, Programme Office Manager, [email protected] 0151 244 4169
Background Documents: None
Appendices:
Page 5 of 62

Appendix 1: Risk or Reward? The Changing Role of CCGs in General Practice, Kings Fund and Nuffield Trust
Page 6 of 62
Risk or reward? The changing role of CCGs in general practice
Research reportHolly Holder, Ruth Robertson, Shilpa Ross, Laura Bennett, Jeni Gosling and Natasha Curry
January 2015
Page 7 of 62

About this reportAs clinical commissioning groups (CCGs) settle into their central role in the reformed NHS, the full scale of the challenges they face is becoming clear. This report, part of a joint project by the Nuffield Trust and The King’s Fund, aims to understand the development of CCGs, and to support them by spreading good practice and learning. It tracks the development of six CCGs, selected to broadly represent CCGs across England. The report, which is based on a survey, interviews, observations and reviews of board papers, considers two research questions: how CCGs are functioning as membership organisations and how they are supporting the development of primary care in their local area.
AcknowledgementsFirst and foremost we would like to express our gratitude for the ongoing time and effort our case study CCGs have put into this project. Thank you for sharing your experiences with us and we look forward to continuing to work with you.
Thanks are also due to our external expert advisory group members Kath Checkland and Nick Mays for their support and guidance, and to John Richards who was kind enough to review this report for us. We are also grateful for the ongoing support of our colleagues Candace Imison, Judith Smith, Rebecca Rosen and Richard Murray.
Find out more at: www.nuffieldtrust.org.uk/publications/risk-or-reward-CCGs
Page 8 of 62

Contents
List of boxes, tables and figures 3
Executive summary 4
Key findings 4
Considerations for CCGs and NHS England 6
1. Introduction 7
The changing role of CCGs in primary care 8
The health and social care context 10
Report structure 11
2. About this research 12
Approach 12
Site profiles 12
3. GPs’ involvement in CCGs 14
Key findings 14
Overall levels of GP engagement 15
Variations in perceptions of the CCG 17
Challenges to sustaining GPs’ engagement and influence in CCGs 20
Future challenges 25
4. CCGs’ involvement in primary care development 28
Key points 28
Mechanisms for driving primary care improvements 31
CCGs’ impact on primary care 33
Considerations for primary care development and ‘co-commissioning’ 35
5. Discussion 40
Page 9 of 62

2
6. Conclusion: balancing the risks and rewards of CCGs’ expanding role in primary care development 44
Appendix 1: Research methodology 45
Documentary analysis 45
Interviews 46
Observations 46
Survey of member practices 46
Appendix 2: Case study site details 48
References 50
Page 10 of 62
3
List of boxes, tables and figures
Boxes
Box 1.1: Description of commissioning and CCGs 9
Box 1.2: Optional additional co-commissioning responsibilities 10
Box 4.1: Examples of conflicts of interest and how they were managed 38
Tables
Table 2.1: Case study site characteristics 13
Table 3.1: Changes to the management services procured from commissioning support units (CSUs) in 2014/15 26
Table A1: Interview type, 2014 46
Table A2: Survey respondents by role 47
Figures
Figure 3.1: How engaged do you feel with the work of the CCG? 2013 and 2014 16
Figure 3.2: Levels of ownership and influence over the CCG, 2014 17
Figure 3.3: Change in the proportion of GPs highly engaged in the work of their CCG by role, 2013 and 2014 17
Figure 3.4: Levels of influence and ownership by role within the CCG, 2014 19
Figure 3.5: ‘The CCG is owned by its members and feels like “our organisation” ’: percentage of all respondents agreeing or strongly agreeing, by site, 2014 19
Figure 3.6: Experience of GPs with a formal role, 2014 21
Figure 3.7: Example of partnership working arrangements 24
Figure 3.8: Influence over GPs’ work by organisation, 2014 25
Figure 4.1: CCGs’ role in influencing GPs’ clinical practice, 2013 and 2014 30
Figure 4.2: Use of mechanisms within CCGs, 2014 31
Figure 4.3: Perceived impact of CCG on patient experience, 2014 34
Page 11 of 62

4 Risk or reward? The changing role of CCGs in general practice
Executive summary
A central component of the NHS reforms that were implemented in England in 2013 was the introduction of 211 general practitioner (GP)-led clinical commissioning groups (CCGs), which have responsibility for over two thirds of the NHS commissioning budget.
While the main commissioning responsibility of CCGs has been to purchase acute and community services on behalf of their populations, they also have an important role in promoting quality improvement in primary care. This role has been carried out in conjunction with NHS England, which has overall responsibility for the commissioning of primary care services.
Over the last year there has been a clear policy direction from NHS England regarding the commissioning of primary care: from April 2015, CCGs will have the option to apply for joint or delegated responsibility for some primary care commissioning activities currently undertaken by NHS England area teams, as part of the co-commissioning policy. However, the future policy landscape for commissioning remains fluid, with the 2015 General Election approaching and the implications of the Five Year Forward View pointing to yet more change to commissioning roles and responsibilities (NHS England and others, 2014). CCGs’ expanding remit in primary care development provides them with an opportunity to strengthen their peer-led improvement activities, but also brings with it certain risks; issues that are explored in this report.
This is the second report1 from a joint research study by the Nuffield Trust and The King’s Fund that tracks the development of six CCGs selected to broadly represent CCGs across England. The research for this report was conducted between January and March 2014, and included a GP survey (with 279 responses), 70 interviews with both GP leaders and GP members of CCGs, and a review of board papers. The analysis explores the involvement of CCGs in primary care from two main perspectives: how they are functioning as membership organisations; and how they are supporting the development of primary care in their areas.
Key findingsIn our case study sites we found that the sustainability of clinical involvement in commissioning was at risk due to waning levels of GP leader engagement in CCGs, potential problems in the recruitment and retention of leaders, and significant pressures on GPs’ time and capacity. Specifically we found that:
• CCGshadbroadlymaintainedlevelsofengagementfromtheirGPmembers(according to participants in our survey).
1 The first report was published in 2013: Naylor and others (2013).
Page 12 of 62

5 Risk or reward? The changing role of CCGs in general practice
• However,theinitialenthusiasmamongsomeGPleadershadstartedtowane,aslessthan half reported that they had the support, time and resources to undertake their role effectively.
• Overthenextfewyears,CCGscouldfaceachallengeinretainingtheirGPleaders,as many reach the end of their initial terms of office and new, potentially more attractive leadership posts arise in GP provider organisations.
• Weobservedthatthecomplexexternalenvironment,tightdeadlinesfromNHSEngland and, at times, inefficient internal governance structures meant that engaging and applying the member voice in decision-making was sometimes difficult. Some of the CCGs had begun to review their governance structures to ensure that GP time was used to best effect.
Our research suggests that the benefits provided by the shift towards CCGs co-commissioning primary care could be compromised by potential conflicts of interest, reductions in running cost budgets and strained relationships with fellow GPs and NHS England. Our fieldwork was carried out before the details of the co-commissioning policy were announced, but the analysis offers a number of insights that should be considered. Specifically we found that:
• CCGleadersandmemberswhotookpartinthisresearchagreedthattheirCCGhad a legitimate role in local efforts to develop primary care; a change from the more cautious views held a year earlier.
• However,fewmembersfeltthatitwasappropriateforCCGstoperformance-manage GPs. This implies that CCGs may face difficulties maintaining good relationships with GP members if they take on new contract management responsibilities as part of co-commissioning.
• CCGleadersquestionedwhethertheyhadsufficientresourcesortimetocarryouttheir expanding role (these views were expressed even before the co-commissioning policy was announced).
• Inourresearch,althoughthemajorityofintervieweesfeltconflictswerebeingdealtwith adequately, we found examples of decisions where there was the potential for, or the perception of, a conflict having occurred. Conflicts of interest will arise more frequently as CCGs take on an extended role in primary care commissioning.
• Aswasfoundinthefirstyearofourresearch,someGPsremainedunclearaboutwhen they were accountable to their CCG or to NHS England. The distinction risks becoming even more confusing as co-commissioning redefines the boundaries once again.
Page 13 of 62

6 Risk or reward? The changing role of CCGs in general practice
Considerations for CCGs and NHS England This report outlines four key areas of work that CCGs and NHS England must focus on in order to ensure that the current model of commissioning is sustainable and maximises the benefits of new co-commissioning arrangements:
1 Sustain the enthusiasm of clinical leaders – To sustain clinical involvement, CCGs and NHS England must invest in a clear primary care leadership strategy that supports current clinical leaders and trains a future cadre.
2 Maintain the strength of the GP membership voice – As CCGs evolve, and commissioning responsibilities develop, CCGs need to explore ways to ensure that the membership voice remains strong in the decision-making process. CCGs will need to demonstrate how GP involvement is impacting their decisions, and maintain a peer-to-peer, supportive relationship rather than focusing excessively on contract compliance and performance management.
3 Manage conflicts of interest – In order to maintain buy-in from members, external organisations and the public as they take on additional commissioning responsibilities, CCGs need to ensure that they are able to demonstrate transparency in their governance processes and should develop the role of lay and other non-GP members of governing bodies.
4 Be clear about the relationship with NHS England – NHS England and CCGs will need to work closely with one another to ensure that the distinction between their roles is understood by GP members. NHS England needs to ensure that CCGs have adequate additional resources to support their expanded role in primary care development.
5. Ensure that CCGs have adequate funding to take on new functions – Management budgets will be reduced from April 2015 at the same time that some CCGs will take on additional commissioning responsibilities. Without adequate resources, some CCGs may struggle to fulfil their new roles effectively.
Page 14 of 62

7 Risk or reward? The changing role of CCGs in general practice
1. Introduction
Since their inception, the main focus of clinical commissioning groups (CCGs) has been on commissioning secondary and community services for their local populations. However, CCGs also have an important role in supporting improvement in primary care, and this role is now set to grow significantly (see Box 1.1 on page 9 for a description of commissioning and CCGs).
In the Five Year Forward View, the six major organisations that oversee the NHS outlined their vision for the health service in 2020 (NHS England and others, 2014). At its core are new, more integrated organisational provider models that all depend to some extent on re-shaping primary care. Through their primary care co-commissioning policy, detailed below, NHS England has indicated that CCGs will play a central role in supporting that change (NHS England and NHS Clinical Commissioners, 2014).
In this second report from a joint Nuffield Trust and King’s Fund programme of research that tracks the progress and activities of six CCGs (chosen to be representative of CCGs across England), we detail the findings from a GP survey, interviews and observations in the CCGs, and desk research that was conducted in spring 2014 to explore three research questions:
1. How involved are GPs in the activities of the CCG, and what relationships are being built between them and CCG leaders?
2. How are CCGs discharging their responsibility to support quality improvement in general practice, and how well placed will they be to do so?
3. What structures and processes are CCGs developing in order to facilitate the above?
In our first report (Naylor and others, 2013) we argued that clinical commissioners had an important window of opportunity to help bring about improvements in general practice, and found that some CCGs were taking positive early steps. In this second report, we describe the progress made over the year since CCGs took on their full legal powers. As the majority of CCGs ready themselves to take on greater responsibilities in primary care, our findings on how they have involved their GP members in decision-making and the approaches they have taken to primary care development provide us with an understanding of the potential of their new role, and some of the possible risks and challenges.
Page 15 of 62

8 Risk or reward? The changing role of CCGs in general practice
The changing role of CCGs in primary care Current roleAlthough the core function of CCGs is commissioning acute and community care, legislation conferred on them a legal duty to support quality improvement in primary care. Core primary care commissioning responsibilities are held by NHS England area teams, who agree and manage GP contracts and commission other primary care services. The distinction is already blurred with some CCGs contracting GPs to deliver some services. And, this is set to expand significantly for interested CCGs. In our first report we explained how CCGs and area teams had some separate and some overlapping responsibilities in primary care that were still being clarified (Naylor and others, 2013).
Future roleIn May 2014, NHS England announced that CCGs would be invited to ‘co-commission’ primary care (NHS England, 2014a). This policy gives CCGs the option to take on a variety of additional responsibilities from April 2015, choosing from three levels:
1. Greater involvement in primary care decision-making: closer collaboration with NHS England area teams.
2. Joint commissioning arrangements: functions exercised by a new joint committee (between the CCG and NHS England area team), with the option to pool funding for investment in primary care.
3. Delegated commissioning arrangements: functions exercised by new CCG primary care commissioning committees, chaired by a lay person and with a majority of lay and CCG executive members. (See Box 1.2 on page 10 for a more detailed explanation; NHS England and NHS Clinical Commissioners, 2014)
Initially, these responsibilities will be limited to general practice but NHS England is also developing plans to give CCGs more responsibility for commissioning specialised services.
It has been announced that CCGs will not receive additional resources to fund these new responsibilities; alongside facing a ten per cent cut in their running cost budgets in 2015/16 (NHS England, 2014b); and should agree local arrangements for sharing staff resources with area teams where appropriate (NHS England and NHS Clinical Commissioners, 2014). Area teams are themselves undergoing a process of restructuring and will be merged from 27 to 14 larger regional offices in order to reduce costs by 15 per cent (Calkin, 2014). There may of course be some CCGs who choose to remain as they currently operate and not undertake any additional commissioning responsibilities.
Page 16 of 62

9 Risk or reward? The changing role of CCGs in general practice
Box 1.1: Description of commissioning and CCGs
What is commissioning?Commissioning is the process of deciding which services to purchase to best suit the needs of a given population. Clinical commissioning refers to a process by which clinicians are given a primary role in this activity. See Naylor and others (2013) for a review of previous attempts at clinical commissioning.
What are CCGs?CCGs are clinically led NHS organisations created by the Health and Social Care Act 2012. They replaced primary care trusts as the statutory bodies responsible for planning and commissioning the majority of NHS health services (excluding primary and some specialised care) in April 2013. CCGs were intended to put responsibility for the design of local health services into the hands of local GPs. This is based on the logic that through their daily interactions with patients, GPs gain an in-depth understanding of their practice population, which makes them best placed to design health services that meet local patients’ needs. There are currently 211 CCGs in England, covering registered populations of between 70,000 and 900,000.
CCGs are membership organisations, meaning that the decisions made should reflect the views of those involved. However, unlike other membership organisations, all GP practices in England must belong to a CCG. Each practice nominates a representative – usually a GP, but in some cases a practice manager or other colleague – to represent them at a members’ forum. Each CCG is led by a governing body which consists of a mixture of general practice representatives, members of the CCG executive team, other clinicians and lay representatives.
CCGs are distinct from the previous incarnations of clinical commissioning GP fundholding in the 1990s (HM Government, 1990) and practice-based commissioning in the 2000s (Department of Health, 2001) in two main ways: first, joining a CCG is a mandatory requirement for GPs and second, the CCG is intended to operate on a membership model whereby the organisation is led by GPs and represents all GPs in its catchment.
Page 17 of 62

10 Risk or reward? The changing role of CCGs in general practice
Box 1.2: Optional additional co-commissioning responsibilities
The health and social care context During this second year of our research, the NHS has continued to strain under severe financial pressure: at the end of 2013/14, around a quarter of NHS trusts and foundation trusts were in deficit, as were one in ten CCGs (National Audit Office, 2014a). In general practice, although patient satisfaction has remained high, the workforce has been under pressure due to a shortage of GPs and diminishing resources (Dayan and others, 2014; and the British Medical Association survey 20141 which reports increased workloads and low levels of morale). General practices have been increasingly seeking to join together in informal networks or more formal federations
1 Note: This survey (British Medical Association, 2014) was carried out by the trade union and professional body for doctors. The survey is carried out quarterly. This iteration took place between 4 and 24 February 2014 and was completed by 420 GPs (response rate of just over 50 per cent).
CCG responsibilities 2014/15• Legaldutytopromotequalityimprovementinprimarycare.
• Delegatedresponsibilityfordesignoflocalenhancedservices(LES)(thatpayGPsfor additional services on top of their core contract).
• CommissioningofGPout-of-hoursservices.
CCG optional additional joint or delegated co-commissioning responsibilities in 2015/16• Generalpracticecommissioning:revieworrenewexistingGPcontracts,award
new ones including ability to design Personal Medical Services (PMS) and Alternative Provider Medical Services (APMS) contracts, establish new practices in an area and approve practice mergers.*
• Generalpracticecontractperformancemanagement.*
• Generalpracticebudgetmanagement.
• Complaintsmanagement.
• Designandimplementationoflocalincentiveschemes(e.g.newlocalincentivesto replace Quality and Outcomes Framework (QOF) payments, LES and directly enhanced services (DES)).
• Makingdecisionsondiscretionarypaymentssuchasreturner/retainerschemesforGPs seeking to return to general practice after a break.
*CCGs who choose the first ‘greater involvement’ level of co-commissioning can be involved in discussions about these areas but will have no decision-making role.
Primary care responsibilities retained by NHS England• Dental,eyehealthandcommunitypharmacycommissioning(althoughCCGs
can be involved in discussions).
• PerformancemanagementofindividualGPs:medicalperformers’list,appraisaland revalidation.
(NHS England and NHS Clinical Commissioners, 2014)
Page 18 of 62

11 Risk or reward? The changing role of CCGs in general practice
in the anticipation that by operating at scale they will be well placed to provide coordinated, multi-disciplinary care of the kind required to respond to the changing needs of the population (Smith and others, 2013).
While health care budgets have been protected from real-terms cuts, adult social care budgets have decreased by 12 per cent in real terms since 2010 through five consecutive years of spending cuts (Association of Directors of Adult Social Services, 2014). To address this imbalance and promote more integrated models of care, the government created the Better Care Fund to shift resources from hospitals to the community by pooling at least £3.8 billion of funding (£5.3 billion based on current plans) into a joint health and social care budget in 2015/16 (National Audit Office, 2014b). At least £1.9 billion of this pooled budget must come from existing CCG allocations.
This context is an important consideration for our research questions. First, it may be more difficult to engage GPs in commissioning while they experience so much pressure from their provider responsibilities. Second, the financial context and the drive to keep patients out of hospital means that the success of CCGs in leading or supporting change is even more critical.
Report structureFollowing a brief outline of our methodology and case study CCGs, this report explores how engagement of GP members and leaders has developed throughout the year, and the current and future challenges facing CCGs. The report then goes on to detail CCGs’ expanding role in supporting quality improvements in primary care, and the opportunities and complexities that have arisen as a result. The report concludes with an analysis of what this evidence tells us about upcoming policy challenges for CCGs as they face a year in which budgets will continue to be constrained and, for some, their role will be expanded to primary care.
Findings from the first year of this research were published in 2013 (Naylor and others, 2013) and a more detailed summary of the survey findings discussed in this report was published in 2014 (Robertson and others, 2014).
Page 19 of 62
12 Risk or reward? The changing role of CCGs in general practice
2. About this research
ApproachOur project set out to follow the development of CCGs in six case study sites over three years, from 2012 to 2015, to understand how CCGs are operating with their GP members and the influence they have over primary care provision. A report was published at the end of the first year, based on research conducted between October 2012 and March 2013, before CCGs took on full statutory responsibilities (Naylor and others, 2013). This report details the second year of research, which was conducted almost one year after CCGs took on statutory responsibilities, in early 2014. Further research is due to be conducted this year, 2015.
The six case study sites were selected at random in 2012, using a stratified approach to ensure that we included CCGs of various sizes and from all four regions of NHS England. We ensured that the sites represented a wide range in terms of level of deprivation, and included both urban and rural areas. The sites have been anonymised in this report.
The six case study sites in year one all continued to take part in year two and we collected information through largely the same methods as in year one:
• documentaryanalysisofdocumentsrelatingtotheCCG,particularlyboardpapers
• semi-structuredinterviewswith70keyindividuals–thosewithandthosewithoutaformal role in the CCG
• observationsof18meetings,themajorityofwhichwereCCGgoverningbodyandmember engagement meetings
• anonlinesurveyofmemberpracticeswith279responses,primarilyfromGPswithout a formal role in the CCG (an approximate response rate of 28 per cent).
See Appendix 1 for a detailed report on the research methods used and Appendix 2 for characteristics of the case study sites. In both the interviews and the survey, particular efforts were made to reach GPs who had no formal role within the CCG.
Site profilesCCGs across England are highly diverse in terms of population size and profile, and our case study sites reflect this diversity. Table 2.1 provides a summary of their characteristics (approximate values are given to protect anonymity).
Page 20 of 62

13 Risk or reward? The changing role of CCGs in general practice
Table 2.1: Case study site characteristics
Site Population (thousands)
Number of practices
Approximate budget
(millions)
Deprivation Location
A 200–300 20–30 £200 Medium to low Mainly ruralB 500+ 60–70 £600 Low Mixed urban/
ruralC 100–200 30–40 £200 Very high UrbanD 300–400 40–50 £400 High UrbanE 100–200 10–20 £200 High UrbanF 200–300 30–40 £300 Low Rural
Note: Population/budget data for 2014/15 were taken from: www.england.nhs.uk/wp-content/uploads/2013/12/ccg-allocation-big-table-v2.pdf
Appendix 2 provides further detail about the historical context and demographic profiles of our case study sites.
Page 21 of 62

14 Risk or reward? The changing role of CCGs in general practice
3. GPs’ involvement in CCGs
Key findings• Duringtheirfirstyearasfullyestablishedcommissioningorganisations,our
survey of GPs found that the CCGs in this study had broadly maintained levels of engagement from their GP members, despite the financial and demand pressures on general practice.
• However,thereisevidencethattheinitialenthusiasmamongsomeoftheGPleaderswho are most closely involved with the work of their CCG has started to wane.
• CCGsinthisstudywerenotalwaysgettingmaximumvalueoutoftheinvolvementof clinicians in commissioning. Some had begun to review their governance structures in an attempt to ensure that valuable GP time is used to best effect.
• CCGsfacedchallengesininvolvingmembersindecision-makingwhileoperatingin a complex external environment that often required them to work at scale with neighbouring CCGs and other health and social care organisations, and to respond to central requests from NHS England.
• AllCCGsinthisstudymovedsomeexternallycommissionedsupportservices in-house in 2014/15, or were considering doing so, giving them more control over the service provided. As running cost budgets reduce in 2015/16, they could find it challenging to achieve efficiency savings in their internal operations without the economies of scale available to commissioning support units (CSUs).
• Thesustainabilityofclinicalinvolvementinthecurrentmodelisatriskunlessresources are invested to support clinicians currently in leadership positions to fulfil these new roles that are very different from their day-to-day clinical work, develop emerging leaders and undertake succession planning.
In this chapter we consider the extent to which this new form of commissioning is enabling clinicians to design local health services and any challenges that are being faced. We asked our participants about their levels of ‘engagement’; understood as their level of interest, enthusiasm, involvement and support for the CCG (although in the survey, terms were not defined). In order to understand the impact of this engagement, we also asked participants whether they felt that decisions taken by the governing body reflected their views, and if they felt as though they ‘owned’ and felt able to influence the CCG. Taken together, these findings give us an indication of the perceived impact of GPs’ engagement and their functioning as membership organisations.
In the first year of our research, we found that GPs were optimistic about what the new commissioning system could achieve, and there was a strong commitment from CCG leaders to making the new arrangements work (Naylor and others, 2013).
Page 22 of 62

15 Risk or reward? The changing role of CCGs in general practice
Engagement among GPs was highly variable, with GP leaders being more positive than GP members. However, engagement was generally better than under the previous commissioning arrangements. Our first report suggested that work was needed to ensure that this enthusiasm would continue, particularly given the pressurised environment GPs are operating within. In the second year of our research, we revisited these issues in order to understand what developments had occurred, looking specifically at the extent to which CCGs have the relationships and structures in place to ensure that the views of their GP member practices feed into their decision-making processes, and how and why leaders’ enthusiasm for commissioning has changed over time.
Where this chapter presents survey results, the term ‘leaders’ refers to those who have a formal role in the CCG (clinical and non-clinical governing body members, locality leads and practice representatives) and ‘members’ refers to those who do not have a formal role in the CCG. As outlined in Appendix 1, a small proportion of survey respondents were practice managers and non-clinical governing body members. However, for ease of reading, survey respondents will be referred to as ‘GPs’ from this point onwards.
CCGs have largely sustained levels of GP engagement during their first year as fully established commissioning organisations
Overall levels of GP engagement “… we [CCGs] live or die by GP engagement. If there’s no GP engagement we’re sort of pointless organisations really, and the mantra is to avoid becoming a PCT [primary care trust] because clearly what we want to avoid is just sort of hide-bound, remote organisations – that we just need to maintain that membership feel.” (Chief finance officer)
Our research indicates that CCGs have largely sustained levels of GP engagement during their first year as fully established commissioning organisations. In January 2014, 71 per cent of GPs reported being at least somewhat engaged in the work of their CCG (Figure 3.1). This was similar to the level of overall engagement reported in February 2013 (73 per cent) (Naylor and others, 2013) and remains much higher than previous commissioning models. During practice-based commissioning, over half of GPs felt ‘not at all’ or ‘not very engaged’ (Wood and Curry, 2009), and if engagement is understood to be comparable with signing up to the scheme, GP fundholding covered only 50 per cent of the population after successive waves of enrolment (Glennerster, 1994).
Page 23 of 62

16 Risk or reward? The changing role of CCGs in general practice
GPs were more positive about the level of influence they had over the CCG than in previous commissioning arrangements
A national survey of more than 5,000 GP practices conducted for NHS England at a similar time to ours (spring 2014) also found that the vast majority of GPs felt they were engaged at least a fair amount with their CCG (82 per cent). The research, conducted by Ipsos MORI, showed that engagement had declined slightly since the previous round of their survey was fielded two years earlier, during the CCG authorisation process (87 per cent; Ipsos MORI, 2014).
Analysis of the impact of this engagement revealed a mixed picture. Over half of GPs who responded to the survey (54 per cent) felt well informed about what the CCG was trying to achieve; and 46 per cent felt that decisions made by the CCG reflected the views of themselves and their colleagues (see Figure 3.2). These figures remain largely unchanged from the previous year and echo findings discussed on pages 22 to 23 about the functioning of some of the internal governance structures.
Despite this varied picture, when asked to reflect on current and past commissioning arrangements, GPs were more positive about the level of influence they had over the CCG than in previous commissioning arrangements. Forty per cent of GPs who responded to our survey reported that they could influence the work of their CCG, compared with just 13 per cent who felt they could influence the work of their primary care trust (PCT) in the past.
Perc
enta
ge o
f all
resp
onde
nts
Completely disengaged
Moderately disengaged
Somewhat engaged
Moderately engaged
Highly engaged
Notes: Respondents who skipped the question were excluded from the distribution. Per cent highly engaged with work of CCG down from 19 per cent (2013) to 12 per cent (2014), p<=0.05. Per cent highly/moderately/somewhat engaged 73 per cent (2013) and 71 per cent (2014); di�erence not signi�cant at p<=0.05.
100
90
80
70
60
0
10
20
30
40
2013(n=208)
2014(n=265)
50
Figure 3.1: How engaged do you feel with the work of the CCG? 2013 and 2014
Page 24 of 62
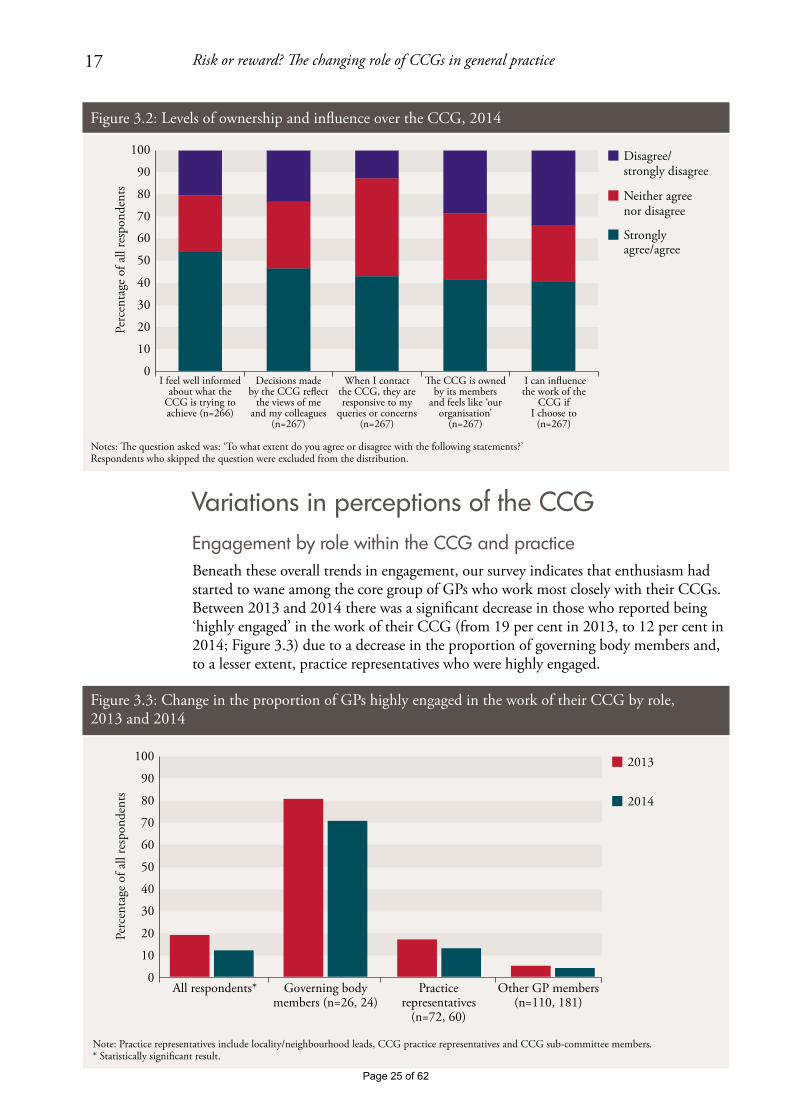
17 Risk or reward? The changing role of CCGs in general practice
Variations in perceptions of the CCGEngagement by role within the CCG and practice Beneath these overall trends in engagement, our survey indicates that enthusiasm had started to wane among the core group of GPs who work most closely with their CCGs. Between 2013 and 2014 there was a significant decrease in those who reported being ‘highly engaged’ in the work of their CCG (from 19 per cent in 2013, to 12 per cent in 2014; Figure 3.3) due to a decrease in the proportion of governing body members and, to a lesser extent, practice representatives who were highly engaged.
Perc
enta
ge o
f all
resp
onde
nts
Notes: �e question asked was: ‘To what extent do you agree or disagree with the following statements?’Respondents who skipped the question were excluded from the distribution.
100
90
80
70
60
0
10
20
30
40
I feel well informed about what the
CCG is trying to achieve (n=266)
Decisions made by the CCG re�ect
the views of me and my colleagues
(n=267)
When I contact the CCG, they are responsive to my
queries or concerns (n=267)
�e CCG is owned by its members
and feels like ‘our organisation’
(n=267)
I can in�uence the work of the
CCG if I choose to
(n=267)
50
Disagree/strongly disagree
Neither agree nor disagree
Strongly agree/agree
Figure 3.2: Levels of ownership and influence over the CCG, 2014Pe
rcen
tage
of a
ll re
spon
dent
s
2013
2014
Note: Practice representatives include locality/neighbourhood leads, CCG practice representatives and CCG sub-committee members. * Statistically signi�cant result.
100
90
80
70
60
0
10
20
30
40
All respondents* Governing body members (n=26, 24)
Practice representatives
(n=72, 60)
Other GP members (n=110, 181)
50
Figure 3.3: Change in the proportion of GPs highly engaged in the work of their CCG by role, 2013 and 2014
Page 25 of 62

18 Risk or reward? The changing role of CCGs in general practice
It was suggested by some that this drop-off in engagement among CCG leaders over time may be because of the pressures in general practice and GPs feeling more committed to protecting their own practice, perhaps at the expense of time spent on CCG-related work. From page 20 we discuss the factors identified in our research that might explain this trend.
“… people have become far more protectionalist about their own provider role… and some of the altruism is lost… I think we’ve got another year window of opportunity to make some big changes… in my view we’re being too slow.” (Governing body member)
Attitudes towards engagement also varied according to respondents’ role in the practice. Practice managers1 who responded to the survey expressed levels of engagement that were higher than those GPs without a formal role in the CCG. In 2014, 85 per cent of practice managers reported being at least somewhat engaged; compared with 71 per cent of GP principals and 59 per cent of salaried GPs. In all of our CCGs, practice managers were able to attend CCG meetings either as representatives of their practices or out of interest. Two CCGs in particular actively encouraged practice managers to attend and contribute to CCG meetings or forums, and in one a practice manager sat on the governing body in a non-voting capacity. One CCG leader described practice managers as “probably the most stable part of the system in many respects” and they “represent the business and can think about the mechanisms by which they can influence the working lives [of GPs]” (GP governing body member).
there remains a disparity between leaders’ and members’ sense of ownership of the CCG
Ownership and influence by role within the CCGLooking at the impact of GPs’ involvement in the CCG, similar to in 2013, the survey in 2014 showed that there remains a disparity between leaders’ and members’ sense of ownership of the CCG, with the former more likely to report ownership of, and engagement with, their CCG (Figure 3.4). As we reported last year, if this disparity continues over time, there is a risk of CCGs losing their connection with their members and repeating the pattern of diminishing clinical involvement of previous commissioning formations.
1 Although our survey was aimed at GPs, a small number of practice managers also responded (n=47 in 2013 and n=28 in 2014; see Appendix 1 for a full breakdown of respondents by type).
Page 26 of 62

19 Risk or reward? The changing role of CCGs in general practice
Variations by size of CCGOne major factor affecting the degree to which GPs felt a sense of ownership over the CCG was the size of their CCG, with the highest levels of ownership reported in the smallest two CCGs (Figure 3.5).
Perc
enta
ge
Note: Site A n=49, site B n=63, site C n=47, site D n=39, site E n=30, site F n=39.
>>> Increasing CCG population size >>>(scale removed to preserve site anonymity)
100
90
80
70
60
0
10
20
30
40
50Site ECCG
ESite CCCG
Site ACCG
Site FCCG
Site DCCG
Site BCCG
Figure 3.5: ‘The CCG is owned by its members and feels like “our organisation” ’: percentage of all respondents agreeing or strongly agreeing, by site, 2014
Perc
enta
ge o
f all
resp
onde
nts
‘I can in�uence the work of the CCG if I choose to.’ Percentage who agree or strongly agree
‘�e CCG is owned by its members and feels like “our organisation’’.’ Percentage who agree or strongly agree
Note: Practice representatives include locality/neighbourhood leaders and sub-committee members.
100
90
80
70
60
0
10
20
30
40
Governing body members (n=24)
Practice representatives (n=60)
Members without a formal role (n=183)
50
Figure 3.4: Levels of influence and ownership by role within the CCG, 2014
Page 27 of 62

20 Risk or reward? The changing role of CCGs in general practice
Some larger CCGs have locality structures in place below their governing body that cover smaller areas, and are often based on pre-existing groupings such as practice-based commissioning clusters or local authority boundaries. These arrangements work in different ways across the country, but in site B in this study, the locality groups are highly developed and hold devolved decision-making power and budgetary responsibility. The greater sense of ownership that can be generated in these smaller groupings may explain why the level of ownership reported in CCG B is higher than in two of the smaller CCGs in the study (Figure 3.5). As one GP locality chair commented:
“… I think GP practices work more effectively if people know each other and are caring for the same group of patients.” (GP locality chair)
Challenges to sustaining GPs’ engagement and influence in CCGsIn this section we consider a number of issues that relate to the organisation and function of the CCG that may be barriers to engagement for GP leaders and practice representatives. These difficulties and frustrations go some way to explaining the declining enthusiasm reported by this group in our survey. Our research has identified these challenges as:
• pressureonGPs’timeandcapacity
• leadershipdevelopment
• internalgovernancestructures
• respondingtorequestsfromNHSEngland
• externalstructures:operatinginacomplexsystem.
Pressure on GPs’ time and capacityThere is a growing recognition that general practice is coming under increased pressure, fuelled by a real-terms decrease in funding in 2013/14, and difficulties recruiting and retaining GPs, who recently reported their lowest levels of job satisfaction for a decade (Dayan and others, 2014). Within this context it is unsurprising that a lack of time and capacity in primary care were the most commonly cited barriers to engagement with clinical commissioning during interviews in both 2013 and 2014. In the second year of our research, GPs told us they had very little or no spare capacity to take an active interest in their CCGs. GPs in four of our case study CCGs reported that engagement in their CCG’s activities came at a cost to patient care and to themselves. Some GP interviewees who had taken on formal roles in the CCG also reported difficulties in finding the time to complete training courses.
This was also reflected in survey responses from GP governing body members and member representatives, less than 40 per cent of whom reported they had the time necessary to undertake their CCG role (Figure 3.6). This is unsurprising given the findings of other research that the time commitment required for CCG work ranged up to 24 hours a week for one clinical chair (Checkland and others, 2014).
Page 28 of 62

21 Risk or reward? The changing role of CCGs in general practice
Leadership developmentFor GPs, particularly those on the governing body, their work with the CCG is very different from their day-to-day clinical practice, and our research suggests that some are struggling with their new commissioning role. Thirty-five per cent of the governing body members and practice representatives who responded to our survey felt that they had received the training and development that they needed to fulfil their role (Figure 3.6). Forty-six per cent believed they had the support necessary to make robust, evidence-based decisions.
GP interviewees highlighted a number of challenges in moving from wearing their ‘practice hat’ to their ‘corporate hat’. For example, GP leads in two sites described the difficulty in getting to grips with the size of the CCG compared with their own practice, and the challenge of considering the whole CCG, not just their own patients. Others commented on an unexpected need to learn about, and deal with, organisational politics, particularly when consulting the membership on potentially difficult decisions, as this governing body member explains:
“I think one of the things I hadn’t taken account of is how much this was to do with people and politics with a small p… So I think what I hadn’t realised was just how much it would be about making sure that you have healthy, balanced relationships, not colluding, and the whole healthy challenge thing is quite tricky, and all of those things have been new.” (GP governing body member)
GP leaders on governing bodies also described a learning curve on which they had to learn new skills to interpret financial information and work to understand the extent of their accountabilities for the decisions made by the CCG.
100
90
80
70
60
0
10
20
30
40
50
I have the support needed to make robust, evidence-
based decisions(n=79)
I have received the training and development necessary
for my role in the CCG(n=79)
I have the time necessary to ful�l my formal role in
the CCG(n=77)
Disagree/strongly disagree
Neither agree nor disagree
Strongly agree/agree
Perc
enta
ge o
f res
pond
ents
who
ha
ve a
form
al ro
le in
the
CC
G
Notes: �e question asked was ‘You told us you have a formal role in the CCG. To what extent do you agree or disagree with the following statements?’. Base: respondents who reported they were a member of the CCG governing body, practice representative, locality/neighbourhood lead or sub-committee member. Respondents who skipped the question were excluded from the distribution.
Figure 3.6: Experience of GPs with a formal role, 2014
Page 29 of 62

22 Risk or reward? The changing role of CCGs in general practice
In addition to the need for support and training to take on these new roles, an accountable officer from the executive team at one of the CCGs acknowledged that there were challenges around building GP confidence:
“But initially, actually they were quite nervous of it, so although you think of these GPs as leaders, actually they are not naturally. Because they’ve run their own, in the scheme of things, tiny businesses, but actually these are big organisations. And by the time that you’re looking at spend around urgent care, you’re talking about many millions of pounds. So it was quite nerve-wracking. And also, the whole issue about being accountable for the decision, again, is fairly new to them.” (Accountable officer)
Developing the skills and confidence of GP leaders was a work in progress for our CCGs that will require continued focus if they are to sustain clinical involvement in their operations.
Internal governance structures In addition to training GPs for leadership roles, it is important that CCGs are structured in a way that allows them to use GPs’ time effectively and maximise the value gained from the time clinicians put into the commissioning process. Our interviews and observations revealed issues with the functioning of governing bodies and member councils that meant they were not always maximising the value of clinical involvement (see Box 1.1 on page 9 for an outline of the internal structure of CCGs).
Governing bodiesThe governing body meetings observed by the research team were generally procedural in nature, with agendas that focused on updates from other meetings and performance reports. GPs and governing body members interviewed in five of our sites reported that it sometimes felt like their meetings were rubber-stamping decisions which had been discussed and agreed by the executive:
“As to the actual governing body decisions a lot of decisions have been discussed at executive level so the managers are all fully up to speed and sometimes the GPs are… the first time they hear about it is in the paper, so… also some of the board GPs are more involved than others, so the managers often will feel that they’ve got clinical buy-in because a couple of people have been consulted.” (Locality chair)
The breadth of governing body agendas and the length of meeting papers (for example, in March 2014 the average length of meeting papers across our case study CCGs was 282 pages, with one CCG reaching 560 pages) meant that during our observations of meetings there was little time for discussion of strategy and commissioning plans. In recognition of this, some of our CCGs were making changes to their governance structures to try to maximise clinical involvement. One of the CCGs involved in this research had set up a governance committee to take many of the day-to-day procedural items away from the governing body. Another had established four programme boards to oversee its four main areas of commissioned activity, which were each chaired by a GP.
Page 30 of 62
23 Risk or reward? The changing role of CCGs in general practice
Member councilsAlthough CCG constitutions describe member councils as forums for representatives to feed the views from their GP practice into the CCG decision-making process, and approve particular plans and strategies, they were described by interviewees as being mainly for one-way information-giving and not being an effective mechanism for influencing the CCG:
“It ends up being a meeting with 30 to 40 people in the room, including, they always tend to bring in support staff to sit round in the back and that size of meeting is never, ever going to be terribly effective. So I mean, the intent without a doubt is practice engagement. The effect is a feeling that we can’t really influence anything.” (GP practice representative)
Nine GP interviewees spread across all of our sites said they did not believe their CCG was being transparent and meaningfully including everyone in their decision-making. GP interviewees who felt they had influenced decisions reported that they had done so through informal contacts. They were positive about being able to approach GPs on their governing body informally – clinician to clinician – with queries or concerns, and they felt listened to; not all GPs felt this was possible within PCTs in the past. Generally, members reported good relationships with GPs on the governing body who were well known, respected and approachable. In a small number of cases, however, members felt that leaders were ‘out of touch’ with the realities of working under the current pressures of the primary care system and did not represent their views.
Responding to requests from NHS EnglandCCG leaders in three sites reported that demands from NHS England with tight deadlines often left them with little time to institute a proper consultation process, either with members of their CCG or other stakeholders. In particular, they highlighted requests for strategy and planning documents to tight timescales. For example, on 20 December 2013, CCGs had been asked to submit five-year strategic plans and two-year operational plans to NHS England by 14 February 2014. This timescale meant that in one CCG, the governing body did not sign off the strategic plan before it was sent to NHS England. We observed a lay member challenging the chair on their lack of involvement in the process during a governing body meeting. The lay member was told the document was formulaic and not the route through which governing body members should influence CCG strategy.
External structures: operating in a complex system CCGs operate in a complex and varied local environment, in which they form partnerships with a range of other organisations including neighbouring CCGs and local authorities. The extent of these joint working arrangements varies across the country, partly driven by the size of each CCG (there is a ten-fold difference between the population covered by the smallest compared with the largest CCGs in England) and other factors such as whether CCG boundaries are co-terminus with the local authority.
Joint arrangements enable CCGs to make efficiency savings through the shared use of resources, and help local organisations produce coordinated strategies and have greater influence over providers. However, these processes also lengthen the decision-making process and require extra meetings with external partners that are an additional call on
Page 31 of 62
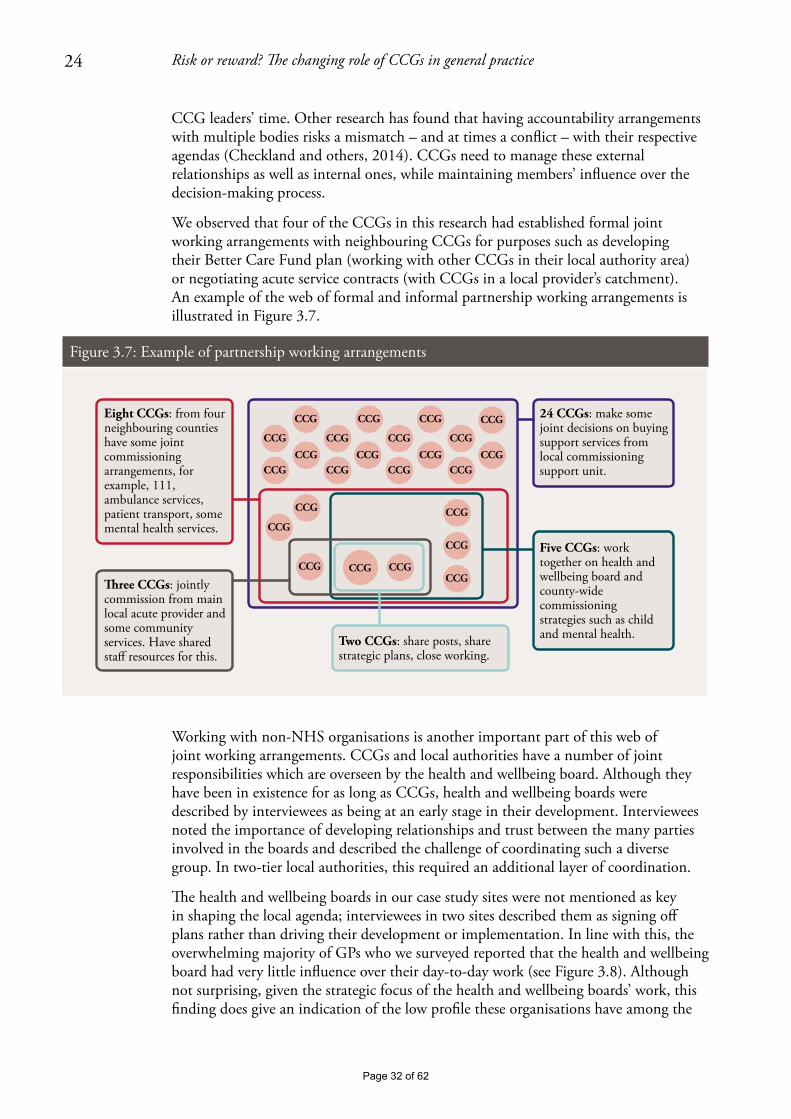
24 Risk or reward? The changing role of CCGs in general practice
CCG leaders’ time. Other research has found that having accountability arrangements with multiple bodies risks a mismatch – and at times a conflict – with their respective agendas (Checkland and others, 2014). CCGs need to manage these external relationships as well as internal ones, while maintaining members’ influence over the decision-making process.
We observed that four of the CCGs in this research had established formal joint working arrangements with neighbouring CCGs for purposes such as developing their Better Care Fund plan (working with other CCGs in their local authority area) or negotiating acute service contracts (with CCGs in a local provider’s catchment). An example of the web of formal and informal partnership working arrangements is illustrated in Figure 3.7.
Working with non-NHS organisations is another important part of this web of joint working arrangements. CCGs and local authorities have a number of joint responsibilities which are overseen by the health and wellbeing board. Although they have been in existence for as long as CCGs, health and wellbeing boards were described by interviewees as being at an early stage in their development. Interviewees noted the importance of developing relationships and trust between the many parties involved in the boards and described the challenge of coordinating such a diverse group. In two-tier local authorities, this required an additional layer of coordination.
The health and wellbeing boards in our case study sites were not mentioned as key in shaping the local agenda; interviewees in two sites described them as signing off plans rather than driving their development or implementation. In line with this, the overwhelming majority of GPs who we surveyed reported that the health and wellbeing board had very little influence over their day-to-day work (see Figure 3.8). Although not surprising, given the strategic focus of the health and wellbeing boards’ work, this finding does give an indication of the low profile these organisations have among the
CCG CCG
CCG
CCG
CCGCCG
CCG
CCG
CCG
CCG
CCG
CCG
CCGCCG
CCG
CCG
CCG
CCG
CCG
CCG
CCG
CCG
CCG
CCG
Two CCGs: share posts, share strategic plans, close working.
�ree CCGs: jointly commission from main local acute provider and some community services. Have shared sta� resources for this.
Five CCGs: work together on health and wellbeing board and county-wide commissioning strategies such as child and mental health.
24 CCGs: make some joint decisions on buying support services from local commissioning support unit.
Eight CCGs: from four neighbouring counties have some joint commissioning arrangements, for example, 111, ambulance services, patient transport, some mental health services.
Figure 3.7: Example of partnership working arrangements
Page 32 of 62
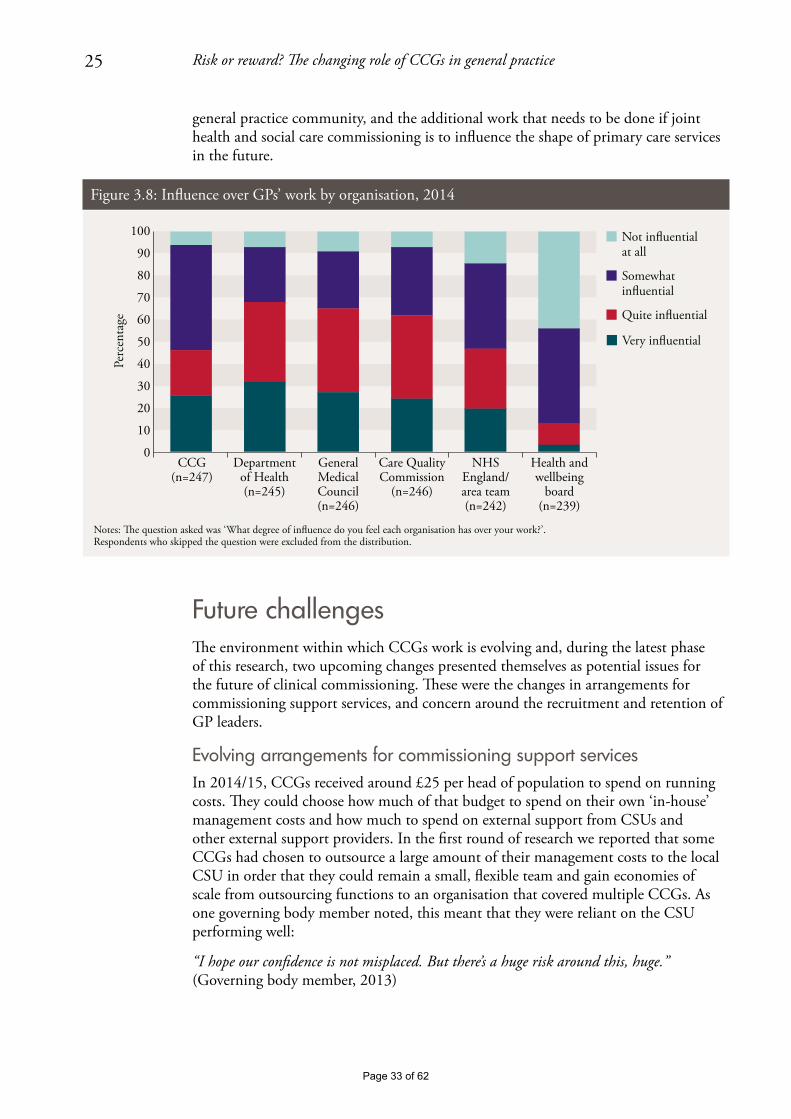
25 Risk or reward? The changing role of CCGs in general practice
general practice community, and the additional work that needs to be done if joint health and social care commissioning is to influence the shape of primary care services in the future.
Future challengesThe environment within which CCGs work is evolving and, during the latest phase of this research, two upcoming changes presented themselves as potential issues for the future of clinical commissioning. These were the changes in arrangements for commissioning support services, and concern around the recruitment and retention of GP leaders.
Evolving arrangements for commissioning support servicesIn 2014/15, CCGs received around £25 per head of population to spend on running costs. They could choose how much of that budget to spend on their own ‘in-house’ management costs and how much to spend on external support from CSUs and other external support providers. In the first round of research we reported that some CCGs had chosen to outsource a large amount of their management costs to the local CSU in order that they could remain a small, flexible team and gain economies of scale from outsourcing functions to an organisation that covered multiple CCGs. As one governing body member noted, this meant that they were reliant on the CSU performing well:
“I hope our confidence is not misplaced. But there’s a huge risk around this, huge.” (Governing body member, 2013)
Notes: �e question asked was ‘What degree of inuence do you feel each organisation has over your work?’. Respondents who skipped the question were excluded from the distribution.
CCG(n=247)
Department of Health (n=245)
General Medical Council(n=246)
Care Quality Commission
(n=246)
NHS England/area team(n=242)
Health and wellbeing
board(n=239)
Not inuentialat all
Somewhat inuential
Quite inuential
Very inuential
Perc
enta
ge
100
90
80
70
60
0
10
20
30
40
50
Figure 3.8: Influence over GPs’ work by organisation, 2014
Page 33 of 62

26 Risk or reward? The changing role of CCGs in general practice
For 2014/15, all of our case study sites had decided to bring at least some services in house, or were considering doing so. Table 3.1 shows the services provided by CSUs to CCGs and the areas where services have been brought in house, or where there were plans to do so. For some this was occurring only at the margins, while for others there was a large shift of services in house.
Table 3.1: Changes to the management services procured from commissioning support units (CSUs) in 2014/15
Key• CSU provides at least some services in this area
← all or part of this service has been moved in house
←? considering moving all or part of this service in house
* all or part of this service moved from CSU to an alternative provider
CCG A CCG B CCG C CCG D CCG E CCG F2013/14 CSU spend per head of population
£7 £12.50 £10 £9 £10 £17
2014/15 CSU spend per head of population
£6 £3 £7 £7 £10 £16.50
Business intelligence • ← • • ←? •Support for redesign ← • •Communications and patient and public engagement
← ← •
Procurement and market management (agreeing contracts)
* ← • • •
Provider management (monitoring contracts)
• • • • ←
Business support/back office ← ← • ← • ←
Note: Service groupings taken from NHS England (2013).
Although there were positive comments about particular services and individuals from the support units, all sites reported some dissatisfaction and there was a common complaint about CSUs being unresponsive. Many highlighted national data-sharing issues that affected the quality of the business intelligence service that the CSUs were able to provide (although there was recognition that this was a national issue and that a workaround had been found). This clinical chair talks about the difficulties that led to CSU services moving in house:
“It just wasn’t up to standards, we weren’t getting any of the information we needed, we weren’t getting the response we needed. I think we had serious concerns about the leadership of the CSU and the senior leadership within it and the ability of staff to deliver the work that we needed. So... and I made that decision [to move most CSU services in house] actually pretty quickly in the middle of... or the beginning of last year.” (GP chair)
Moving services in house raises both risks and opportunities for CCGs. In many cases, it involves bringing CSU staff into the CCG, which takes them closer to the staffing structure of their predecessor PCT. This could be beneficial as it gives the organisation more control over the quality of their support services. However, it also moves away
Page 34 of 62
27 Risk or reward? The changing role of CCGs in general practice
from the leaner, GP-led organisation originally envisaged. One of the reasons for outsourcing functions to external providers was their ability to achieve economies of scale by providing services to a number of CCGs at once. As CCG running cost budgets are reduced in 2015/16 (NHS England, 2014b), and the structure of the commissioning support market continues to change (Welikala, 2015), we can expect to see further changes in the mix of in-house and outsourced commissioning support. CCGs will be challenged to find savings in the services they provide internally without the efficiencies available to CSUs by operating at scale.
Succession planning for GP leadersSuccession planning is a key issue for CCGs which, over the next few years, will see their original governing body members come to the end of their terms of office, often with few new or emerging leaders developing to take over from them. This echoes previous forms of commissioning where research indicated that it was often the ‘usual suspects’ taking on central roles, with the majority of the GP community not interested in commissioning roles (Curry and others, 2008).
CCGs spoke about the need to encourage more GPs to take on leadership roles and to give younger or newer members leadership training
The length of tenure for governing body members is set by each CCG, and in our case study sites GP leaders will reach the end of their terms in 2016 or 2017 (although they are able to stand again). Other researchers have noted that this creates an inbuilt discontinuity of the senior leadership (Checkland and others, 2014) and as international examples suggest, stability in leadership can be a key factor in establishing a successful health care organisation (for example medical groups in the United States, which spent time and resources identifying and developing new leaders; Thorlby and others, 2011). Two of our CCGs had mitigated against the risk of all leaders leaving the organisation at the same time by staggering the terms of their governing body members.
A CCG leader from an area seeking to develop a strong GP provider federation highlighted the potential for there to be competition for leaders from the developing GP provider organisations, as was seen in Corby recently where the CCG chair announced he was stepping down in order to lead a local primary care provider (Health Service Journal, 2014). This will mean two local organisations attempting to draw leaders from a fairly small pool of GPs who are interested in, or feel able to undertake, leadership roles.
Several interviewees across four CCGs spoke about the need to encourage more GPs to take on leadership roles and to give younger or newer members leadership training. In three of the CCGs, GPs were encouraged to take on small pieces of work or small areas of responsibility, in the hope that they could be nurtured into taking on leadership positions as these became vacant. One CCG offered a developmental role on the CCG governing body for less experienced GPs. Continuing and building on these efforts will be essential if CCGs are to sustain strong clinical leadership in the future.
Page 35 of 62
28 Risk or reward? The changing role of CCGs in general practice
4. CCGs’ involvement in primary care development
Key points• CCGleadersandmembersinthisresearchagreedthattheirCCGhadalegitimate
role in local efforts to develop primary care; a change from more cautious views held a year earlier.
• However,fewmembersfeltthatitwasappropriateforCCGstoperformance-manage GPs. This implies that CCGs may face difficulties maintaining good relationships with members if they take on new contract management responsibilities as part of co-commissioning.
• CCGleadersquestionedwhethertheyhadsufficientresourcesortimetocarry out their expanding role. These concerns were raised even before the details of the co-commissioning policy were announced.
• ConflictsofinterestwillarisemorefrequentlyasCCGstakeonanextendedroleinprimary care commissioning. In our research, although the majority of interviewees felt conflicts were being dealt with adequately, we found examples of decisions where there was the potential for, or the perception of, a conflict having occurred.
• Aswasfoundinthefirstyearofourresearch,someGPsremainedunclearaboutwhen they were accountable to their CCG or NHS England. The distinction risks becoming even more confusing as co-commissioning redefines the boundaries once again.
• ThefuturechallengeforCCGswillbetoensurethattheysustainapeer-to-peer,supportive relationship, rather than focusing excessively on contract compliance and performance management. Some of this is within CCGs’ control (that is, what mechanisms they use to implement their new responsibilities), but some of it may depend on the resources and time available to CCGs to maintain these relationships.
Our interest in primary care development included:
• theactivitiestheCCGshadinstigatedtomonitororimprovethequalityofexistingservices
• commissioningdecisionsthatmeantcontractingwithGPpractices
• CCGs’involvementwithanyrestructuringofprimarycare.
In the months preceding the authorisation of CCGs, when we undertook our first year of research, we found that the approaches taken to develop primary care varied significantly. For some, GP leadership and influencing one another’s clinical practice
Page 36 of 62

29 Risk or reward? The changing role of CCGs in general practice
were already commonplace, but others were wary of undertaking this role. The reasons for this caution were numerous:
• notwantingtobeseentobe‘policing’colleagues
• aconcernoverresources
• divertingattentionfromCCGs’primarypurpose
• theimpactonGPengagement
• resistancetodoingajobthatwasseenbysomeasNHSEngland’sandwantingtowait and see how the relationship with NHS England developed.
We reported that the largest factor in determining the CCG’s approach was the local area context that the CCG had inherited and what activities the PCT had established. For example, while all of the case study CCGs shared comparative data and used financial incentives, the extent of this work varied. Some CCG leaders strongly opposed the idea that their responsibilities would be considerably extended into primary care development.
The proportion of GPs who felt that the CCG has a legitimate role in influencing their clinical work has increased
Our latest phase of research suggests that there may have been a shift in opinion and there was widespread acceptance among CCG leaders that primary care was within their remit. Many of those who signalled a note of caution in year one of our research had invested more of the CCG’s time and resources into primary care quality. The following quotes are from the same CCG chair in 2013 and then in 2014:
“[It’s] fairly clear that [CCGs] will not have a role in policing or monitoring practices, and if they try to thrust that upon us I would resist that quite strongly… as far as I’m concerned that role sits squarely with the local area team.” (Chair, 2013)
“… I think there has been a bit of a sea change there, yes. I think 12 months ago I would have said absolutely not, I’m not interested in performance, it’s not my bag, but it’s increasingly clear that NHS England are not going to take that on either so someone has got to do it and I think it is going to probably fall in our laps, yes.” (Chair, 2014)
Additional evidence for this change in attitudes can be drawn from our survey. The proportion of GPs who felt that the CCG has a legitimate role in influencing their clinical work has increased over the last year, as illustrated in Figure 4.1. The increase was significant for prescribing, referrals and the quality of care provided, with 85 per cent now agreeing that the CCG should try to influence their prescribing patterns.
Page 37 of 62
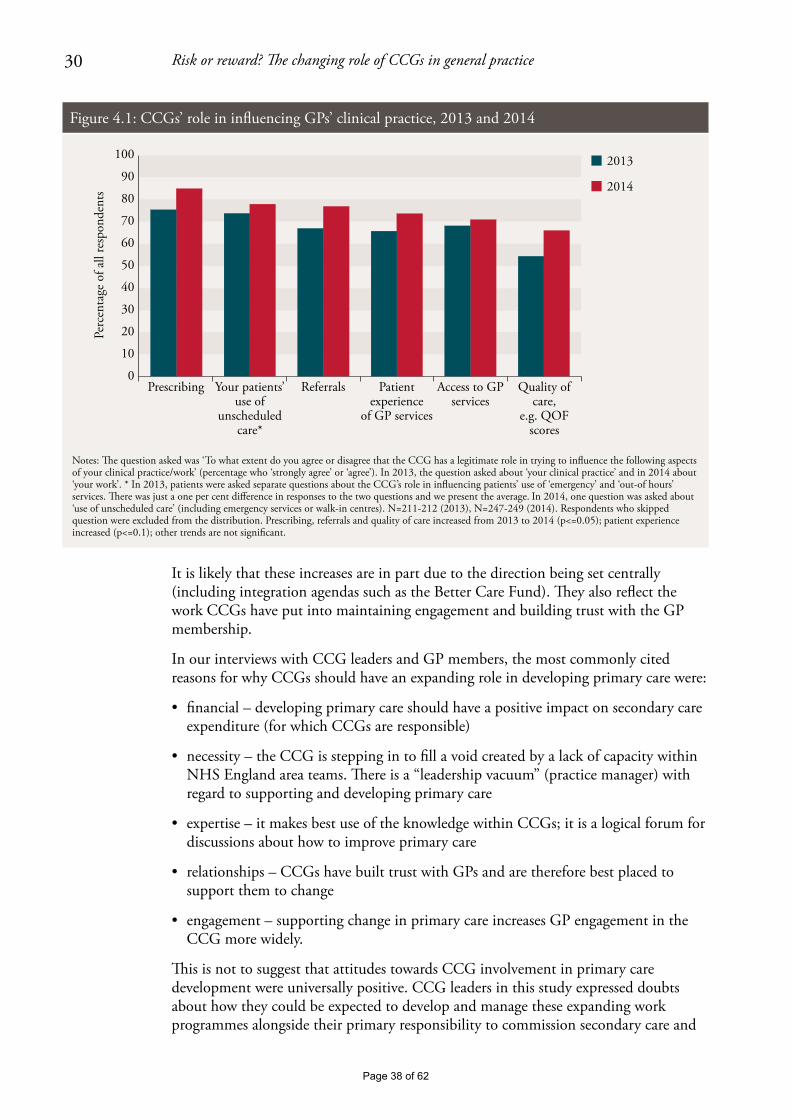
30 Risk or reward? The changing role of CCGs in general practice
It is likely that these increases are in part due to the direction being set centrally (including integration agendas such as the Better Care Fund). They also reflect the work CCGs have put into maintaining engagement and building trust with the GP membership.
In our interviews with CCG leaders and GP members, the most commonly cited reasons for why CCGs should have an expanding role in developing primary care were:
• financial–developingprimarycareshouldhaveapositiveimpactonsecondarycareexpenditure (for which CCGs are responsible)
• necessity–theCCGissteppingintofillavoidcreatedbyalackofcapacitywithinNHS England area teams. There is a “leadership vacuum” (practice manager) with regard to supporting and developing primary care
• expertise–itmakesbestuseoftheknowledgewithinCCGs;itisalogicalforumfordiscussions about how to improve primary care
• relationships–CCGshavebuilttrustwithGPsandarethereforebestplacedtosupport them to change
• engagement–supportingchangeinprimarycareincreasesGPengagementintheCCG more widely.
This is not to suggest that attitudes towards CCG involvement in primary care development were universally positive. CCG leaders in this study expressed doubts about how they could be expected to develop and manage these expanding work programmes alongside their primary responsibility to commission secondary care and
Perc
enta
ge o
f all
resp
onde
nts
Notes: �e question asked was ‘To what extent do you agree or disagree that the CCG has a legitimate role in trying to influence the following aspects of your clinical practice/work’ (percentage who ‘strongly agree’ or ‘agree’). In 2013, the question asked about ‘your clinical practice’ and in 2014 about ‘your work’. * In 2013, patients were asked separate questions about the CCG’s role in influencing patients’ use of ‘emergency’ and ‘out-of hours’ services. �ere was just a one per cent difference in responses to the two questions and we present the average. In 2014, one question was asked about ‘use of unscheduled care’ (including emergency services or walk-in centres). N=211-212 (2013), N=247-249 (2014). Respondents who skipped question were excluded from the distribution. Prescribing, referrals and quality of care increased from 2013 to 2014 (p<=0.05); patient experience increased (p<=0.1); other trends are not significant.
Prescribing Your patients’ use of
unscheduled care*
Referrals Patient experience
of GP services
Access to GP services
Quality of care,
e.g. QOF scores
2013
2014
100
90
80
70
60
0
10
20
30
40
50
Figure 4.1: CCGs’ role in influencing GPs’ clinical practice, 2013 and 2014
Page 38 of 62

31 Risk or reward? The changing role of CCGs in general practice
other services, without extra resources. This and other governance issues are discussed later in this chapter.
Mechanisms for driving primary care improvementsThere are a number of mechanisms available to CCGs to support quality improvement in general practice. These range from education or peer support through to the provision of financial incentives. In this round of research we explored how GPs had reacted to their use and their perceptions of the mechanisms’ impact (outlined in Figure 4.2). Similar to last year, training and education was particularly favoured by GPs as a way of supporting quality improvement; a mechanism which approximately two thirds had used and the vast majority felt was beneficial. As with last year, the use of sanctions for under-performance was least favoured.
All of our CCGs reviewed performance data – of the CCG as a whole and of individual practices. The data – examples are given below – were routinely reviewed at governing body meetings, as well as at certain committee meetings, and in some CCGs at a more local level where GPs were brought together to reflect on one another’s performance and share ideas on how to improve. Two thirds of GPs who responded to our survey felt that sharing comparative data was an appropriate role for CCGs, and of those who had used this mechanism, half felt it had driven improvements.
The majority of the sites shared practice-level performance data with GPs that identified practices within the group. A few interviewees suggested that this appealed to GPs’ “competitive side” and helped to stimulate change. Similarly, peer-pressure in practice-based commissioning was found to be the most effective method of influencing GP referral behaviour (Curry and others, 2008).
Perc
enta
ge o
f all
resp
onde
nts
% who agree that CCGs should use this mechanism
% who have used,or who havebeen a�ected by,this mechanism
% who have usedthis mechanismwho felt it led toimprovements
Note: See Robertson others (2014) for full questions asked. Governing body members have been excluded from the analysis. Only those who said they had been a�ected by the mechanisms were asked to comment on whether they had led to improvements.
100
90
80
70
60
0
10
20
30
40
GP training/education
Comparative data
Financial incentives
Performance objectives
Sanctions forunder-
performance
50
Figure 4.2: Use of mechanisms within CCGs, 2014
Page 39 of 62
32 Risk or reward? The changing role of CCGs in general practice
“Yes, I think, it does drive up a standard because you, kind of, think ‘oh we’re not as good as them… we really need to do something about that’…” (GP, without a formal role in the CCG)
Commonly reviewed indicators included:
• practice-leveldatawithfinancialimplicationsfortheCCG:outpatientreferrals,accident and emergency (A&E) attendances, non-elective activity, prescribing costs, certain care pathways (some CCGs standardised the results to reflect individual practice patient populations)
• practice-leveldatawithaquality/publichealthfocus:certainQOFindicators,EveryOne Counts1 and the GP patient survey.
There are differences of approach in terms of how CCGs are using performance data. In a few CCGs, colour coding was used to illustrate whether a practice’s performance was improving or deteriorating, and one CCG had developed a complex ranking system where scores were assigned to each of the indicators so that practices could be given a final composite score. GPs in these practices had been sharing named practice data for many years and so the CCG had simply built on an existing scheme set up by the previous PCT.
In contrast, in one of our CCGs the governing body had only recently started regularly distributing CCG-level performance data to practices and still did not share named, practice-level data because of a concern about monitoring practices too heavily and risking disengagement. In this CCG, practice-level data were reviewed by the executive, but no action was taken where outliers existed. More recently, the CCG has expressed its intention to extend its work in this area.
As our survey showed, GPs had mixed reactions as to whether or not reviewing comparative data led to improvements (Figure 4.2), and this view was also expressed in our interviews. One GP noted that it was possible to go from “hero to villain” from one month to the next, and as one CCG leader commented, the numbers only show a partial story and many outliers can be understood once an explanation is given. A small number of GPs from different CCGs reported that they continued to have reservations about how far they wanted to be evaluating the performance of their colleagues:
“… as member practices I don’t think we can really go and criticise our peers or our colleagues because it’s not really our place to do so and it’s probably very easy to criticise us as well in return.” (GP practice representative)
With respect to financial mechanisms, all of our CCGs used community-based services contracts2 to support improvements in primary care. Contracts covered a wide range of uses, from commissioning GPs to provide clinical services in the community such as phlebotomy, to commissioning new services such as additional GP cover in nursing homes. In some cases, GPs were being reimbursed using these financial mechanisms for their engagement with CCG activities (such as meeting attendance), which may have contributed to the sustained levels of engagement shown in our survey. Financial
1 For more information, see www.england.nhs.uk/everyonecounts/
2 For more information about the different primary care contracts, see www.bma.org.uk/practical-support-at-work/commissioning/nhs-standard-contract-faqsPage 40 of 62

33 Risk or reward? The changing role of CCGs in general practice
incentives were perceived by the majority of GPs who had received them to be effective in bringing about improvements.
Addressing under-performanceAt the governing body level, the majority of the CCGs in this research used comparative practice data as a way of identifying practices that were outliers in terms of their performance, for example for referral or prescribing rates. The intention is then that CCGs could instigate a process of providing peer support (for example through joining up highly performing practices with those that are outliers) or practice visits by CCG leaders to identify how improvements could be made. In one CCG, if this process does not work, it has a policy by which the under-performing practice would be asked to explain itself to the members’ council (this had not been used to date). None of the CCGs had set performance objectives for practices (unless they were used to monitor specific financial incentives). Some CCG leaders were reluctant to be seen to be setting performance targets out of concern that it would be taking GPs back to the days of PCTs and disengage the membership:
“I’m loath to use those kinds of words [performance management] because they [the membership] will roll their eyes and say, ‘here we go, it’s all over again’. So it’s a really fine line we have to tread.” (Chair)
As NHS England holds GP contracts, the ways in which CCGs can currently address under-performance beyond these peer support methods remain limited. The ultimate sanction the CCG has is to expel a practice from the group. Last year, our research indicated considerable scepticism about whether this was a realistic option and, to date, this mechanism has not been used anywhere in England (Naylor and others, 2013). A similar issue emerged under practice-based commissioning, where PCTs acknowledged that they were unlikely to sanction against under-performing groups unless it was an extreme case (Curry and others, 2008). However, CCGs’ influence on performance may be set to change as some take on contract management responsibilities for some GP services as part of co-commissioning arrangements with NHS England.
CCGs’ impact on primary care In addition to understanding how attitudes to CCGs’ involvement in primary care development have changed in their first year, and the activities undertaken, we were also able to explore the perceived impact on GPs and their patients.
Similar to the previous year in which the survey was conducted, the majority of survey respondents felt that the CCG had made no impact on patient experience of GP services or the quality of care provided in primary care (61 and 58 per cent respectively; see Figure 4.3). However, what Figure 4.3 masks is that, similarly to last year, there is variation between survey respondents, with CCG leaders more likely to report a positive impact compared with the membership. For example, just under 50 per cent of CCG leaders felt that there was a positive impact on patients’ use of unscheduled care, compared with around 20 per cent for the rest of the membership.
Page 41 of 62
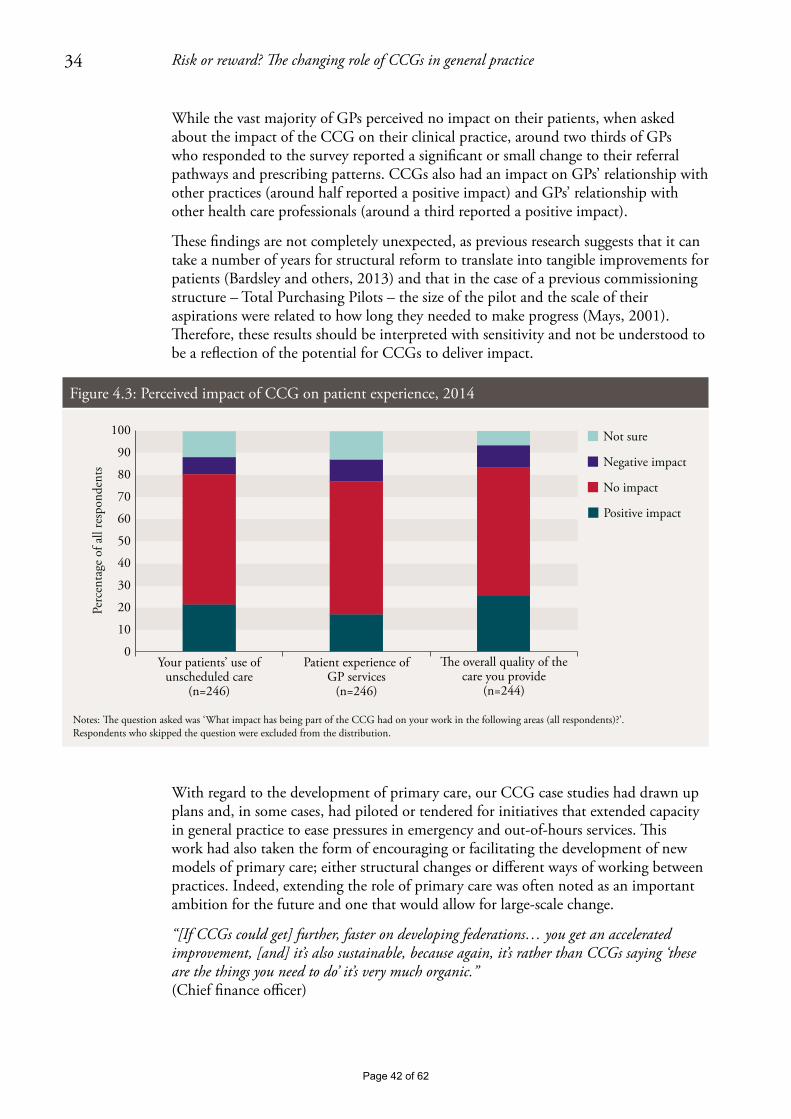
34 Risk or reward? The changing role of CCGs in general practice
While the vast majority of GPs perceived no impact on their patients, when asked about the impact of the CCG on their clinical practice, around two thirds of GPs who responded to the survey reported a significant or small change to their referral pathways and prescribing patterns. CCGs also had an impact on GPs’ relationship with other practices (around half reported a positive impact) and GPs’ relationship with other health care professionals (around a third reported a positive impact).
These findings are not completely unexpected, as previous research suggests that it can take a number of years for structural reform to translate into tangible improvements for patients (Bardsley and others, 2013) and that in the case of a previous commissioning structure – Total Purchasing Pilots – the size of the pilot and the scale of their aspirations were related to how long they needed to make progress (Mays, 2001). Therefore, these results should be interpreted with sensitivity and not be understood to be a reflection of the potential for CCGs to deliver impact.
With regard to the development of primary care, our CCG case studies had drawn up plans and, in some cases, had piloted or tendered for initiatives that extended capacity in general practice to ease pressures in emergency and out-of-hours services. This work had also taken the form of encouraging or facilitating the development of new models of primary care; either structural changes or different ways of working between practices. Indeed, extending the role of primary care was often noted as an important ambition for the future and one that would allow for large-scale change.
“[If CCGs could get] further, faster on developing federations… you get an accelerated improvement, [and] it’s also sustainable, because again, it’s rather than CCGs saying ‘these are the things you need to do’ it’s very much organic.” (Chief finance officer)
Perc
enta
ge o
f all
resp
onde
nts
Notes: �e question asked was ‘What impact has being part of the CCG had on your work in the following areas (all respondents)?’.Respondents who skipped the question were excluded from the distribution.
Your patients’ use of unscheduled care
(n=246)
Patient experience of GP services
(n=246)
Not sure
Negative impact
No impact
Positive impact
�e overall quality of the care you provide
(n=244)
100
90
80
70
60
0
10
20
30
40
50
Figure 4.3: Perceived impact of CCG on patient experience, 2014
Page 42 of 62

35 Risk or reward? The changing role of CCGs in general practice
Many of the CCGs had developed plans for future primary care development (and in a couple of cases the CCG had written strategy documents), detailing how they were planning to support, improve or shape primary care. Within those plans, some of the ideas included:
• improvingcareforspecificgroupssuchaspeoplewithlong-termconditionsandend-of-life care
• addressingpolicyprioritiessuchasintegratedcare,seven-dayworkingandmovingcare into the community – five of the six CCGs in this research had set up access to GPs in A&E and/or walk-in centres
• developmentofnewgeneralpracticegroups:developmentoflocalaccountablecareorganisations; scaling up primary care; strengthening joint working across practices.
The Better Care Fund and the Prime Minister’s Challenge Fund1 were both mentioned as opportunities for CCGs to lead this change. However, some concerns were raised about the Better Care Fund. While some saw this as a way to drive forward the integration agenda, others were concerned about the financial impact of putting CCG resources into social care.
Considerations for primary care development and ‘co-commissioning’Our research indicates that as well as being an opportunity, moving towards co-commissioning presents three challenges for CCGs in the near future. The first relates to the clarity of the relationship between CCGs and NHS England area teams, the second is about how CCGs deal with conflicts of interest and the third relates to relationships within CCG. See Box 1.2 on page 10 for an outline of the co-commissioning proposals.
CCGs and NHS England area teams – roles and responsibilitiesUnderstanding the division between NHS England area teams and CCGs in their responsibilities to support quality improvements in primary care remained a challenge for GP leaders and members alike during the first year of CCG operation. While a certain amount of clarity has been found as a result of the organisations having invested time in building relationships with one another, some concerns remain. It is doubtful that re-defining current arrangements as a result of co-commissioning will improve this situation, at least in the short term.
“… what has been really pretty obvious over the last year is nobody really knowing who owns primary care.” (Practice manager)
In the first round of our research it was unclear how the area teams would interact with practices on quality issues, either directly or working collaboratively with the CCG. The previous interviews with CCG and area team leaders led us to anticipate that the two organisations would work collaboratively on a continuum of support
1 For more information about the Prime Minister’s Challenge Fund, see www.england.nhs.uk/ourwork/qual-clin-lead/calltoaction/pm-ext-access/
Page 43 of 62
36 Risk or reward? The changing role of CCGs in general practice
and intervention, with area teams becoming increasingly involved with the increasing severity of the concern (see Naylor and others, 2013, p. 33, Figure 7). In this year’s research we found that some sites had developed along these lines and had established, for example, joint committee meetings with area teams that tracked the quality of primary care. However, in other sites, the area team had developed separate relationships with practices, using a distinct set of metrics by which to assess performance and directly contacting those who they perceive as under-performing practices. This led to some confusion for GPs and frustration for CCG leaders.
“[NHS England is] in listening mode… They’re expecting us to shape and I presume if we’re heading off in the wrong direction… then we would have heard long before now. It’s very much free rein.” (Chief financial officer)
An ongoing concern was the lack of capacity in area teams and the impact that was having on their relationship with CCGs, as mentioned by the majority of interviewees. The lack of involvement by area teams in some CCGs had been interpreted as an opportunity to design their own approaches to supporting quality in primary care. For example, the area team was often described as having an overseeing role, using the CCG to decide on ideas and priorities (working with the membership) that get signed off by the area team. It is these freedoms that meant, for the majority of CCG leaders, the idea of becoming more involved in primary care development was a natural progression or recognition of work they were already doing.
However, one GP leader described communicating with the area team as “frustrating” and that they came across as “aloof” as a result of their poor communication. Others commented that this distance led the CCG to expect contact from the area team only when they were concerned about something the CCG was doing:
“We don’t work in partnership, we work on the basis: no contact is good.” (Director of strategy)
If this relationship is replicated in other areas, it raises questions about the ease with which these organisations will be able to jointly commission services – where CCGs have expressed an interest in sharing the commissioning function under co-commissioning proposals – or about how much relationship-building will need to go into making it operate effectively. Additionally, from a member GP perspective, the further intertwining of CCGs and NHS England area teams in areas where co-commissioning is introduced could lead to further ambiguity about accountability and support.
Conflicts of interest Managing conflicts of interest is important for demonstrating transparency between leaders and their members, and other external organisations, and for ensuring that CCGs feel able to take decisions that drive change in primary care. The forthcoming introduction of co-commissioning combined with the ongoing ambition to increase the amount of community-based care (as reiterated in the Five Year Forward View: NHS England and others, 2014), means that CCGs will face an increasing number of decisions that may raise conflicts of interest.
Page 44 of 62

37 Risk or reward? The changing role of CCGs in general practice
CCGs in this study were aware of potential conflicts of interest as a result of their involvement in primary care development
Conflicts of interest for CCGs arise at different levels: deciding which providers to use (particularly where this might lead to a change in the proportion of the budget spent on primary rather than secondary care) and deciding what type of services to tender. All six CCGs in this study were aware of potential conflicts of interest as a result of their involvement in primary care development, but CCG leaders were confident that they were dealing with these adequately. Any concern they did express centred on mitigating the possibility of an outside perception that a conflict had occurred. Some unresolved or potential conflicts identified by interviewees included:
• winterpressuresmoneybeingspentonservicesfromacompanyownedbytherelative of a governing body member
• initiativesbeingpilotedbythelocalGPproviderorganisationtoshowproofof concept but potentially giving that organisation an advantage in any future procurement process
• businesscasesbeingwrittenthatwereclearlytargetedataspecificgroupofGPs.
There was little acknowledgement of the potential for an inappropriate decision to be made because of conflicted decision-makers. A common approach was for conflicted GPs to leave the room or to use non-clinicians such as lay members of the governing body or staff from the CSU to provide external scrutiny and ensure probity of decision-making. However, this does limit the useful contribution GP leaders could be making, as outlined by one governing body member below, and represents only a mitigation of a core conflict of interest, rather than its removal:
“I realise that conflict of interest is a problem but, you know, GPs are there for a reason, because GPs know how GPs work…” (GP governing body member)
Box 4.1 gives examples of conflicts of interest in two case study sites and how they were managed.
Page 45 of 62
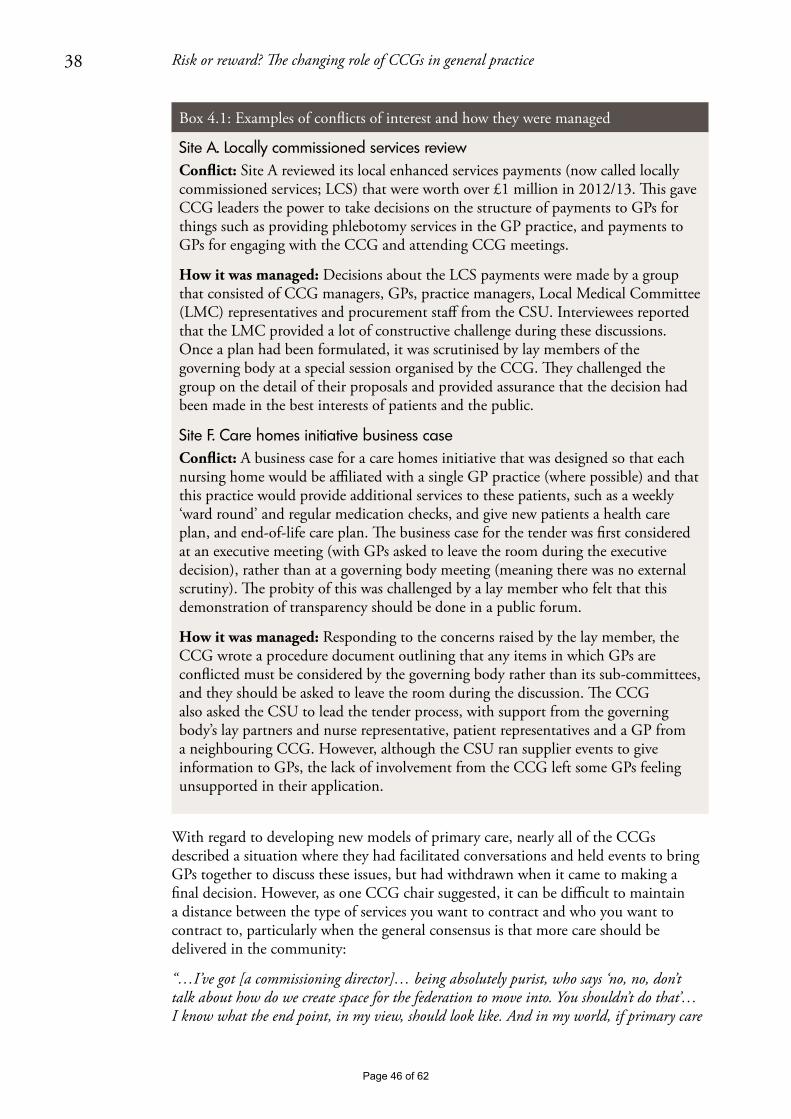
38 Risk or reward? The changing role of CCGs in general practice
Box 4.1: Examples of conflicts of interest and how they were managed
With regard to developing new models of primary care, nearly all of the CCGs described a situation where they had facilitated conversations and held events to bring GPs together to discuss these issues, but had withdrawn when it came to making a final decision. However, as one CCG chair suggested, it can be difficult to maintain a distance between the type of services you want to contract and who you want to contract to, particularly when the general consensus is that more care should be delivered in the community:
“…I’ve got [a commissioning director]… being absolutely purist, who says ‘no, no, don’t talk about how do we create space for the federation to move into. You shouldn’t do that’… I know what the end point, in my view, should look like. And in my world, if primary care
Site A. Locally commissioned services review Conflict: Site A reviewed its local enhanced services payments (now called locally commissioned services; LCS) that were worth over £1 million in 2012/13. This gave CCG leaders the power to take decisions on the structure of payments to GPs for things such as providing phlebotomy services in the GP practice, and payments to GPs for engaging with the CCG and attending CCG meetings.
How it was managed: Decisions about the LCS payments were made by a group that consisted of CCG managers, GPs, practice managers, Local Medical Committee (LMC) representatives and procurement staff from the CSU. Interviewees reported that the LMC provided a lot of constructive challenge during these discussions. Once a plan had been formulated, it was scrutinised by lay members of the governing body at a special session organised by the CCG. They challenged the group on the detail of their proposals and provided assurance that the decision had been made in the best interests of patients and the public.
Site F. Care homes initiative business caseConflict: A business case for a care homes initiative that was designed so that each nursing home would be affiliated with a single GP practice (where possible) and that this practice would provide additional services to these patients, such as a weekly ‘ward round’ and regular medication checks, and give new patients a health care plan, and end-of-life care plan. The business case for the tender was first considered at an executive meeting (with GPs asked to leave the room during the executive decision), rather than at a governing body meeting (meaning there was no external scrutiny). The probity of this was challenged by a lay member who felt that this demonstration of transparency should be done in a public forum.
How it was managed: Responding to the concerns raised by the lay member, the CCG wrote a procedure document outlining that any items in which GPs are conflicted must be considered by the governing body rather than its sub-committees, and they should be asked to leave the room during the discussion. The CCG also asked the CSU to lead the tender process, with support from the governing body’s lay partners and nurse representative, patient representatives and a GP from a neighbouring CCG. However, although the CSU ran supplier events to give information to GPs, the lack of involvement from the CCG left some GPs feeling unsupported in their application.
Page 46 of 62
39 Risk or reward? The changing role of CCGs in general practice
isn’t the bedrock of what we do out of hospital, then we’ve got a problem… So, I’m jumping to the conclusion that groups of practices federated together will definitely be delivering better primary and community care in the future. And [the commissioning director] says ‘no, no you mustn’t do that, you’re the commissioner, you haven’t got to worry about who the provider turns out to be’.” (Chair)
However, maintaining separation of roles in order to avoid conflicts of interest could mean that finding GP leaders to drive change in primary care is difficult if the ‘usual suspects’ have already signed up to being part of the CCG and are therefore unable to participate (and vice versa, as mentioned previously, particularly without adequate succession planning). This may become particularly evident if, as suggested earlier, actively engaged GPs could begin to focus their efforts on developing their own businesses in new models of general practice, rather than continue their interest in commissioning.
Research conducted on practice-based commissioning found that concern over conflicts of interest was a barrier to their progress (Curry and others, 2008); something that CCGs must avoid if they are to drive change in primary care. This is an important issue that is currently being considered by NHS England as part of co-commissioning plans. It has recently announced that CCGs that undertake joint or delegated commissioning responsibilities need to establish a decision-making committee, chaired by a lay partner and with a lay and executive member majority (NHS England, 2014c).
Relationships within CCGsThe closer monitoring of GPs’ clinical practice and the way in which tenders for primary care services are being handled have also begun to cause slight tensions within CCGs. This has shown itself in the relationships between CCG leaders and their members where, for example, members in one CCG felt unsupported during a tendering process, leading to criticisms of the leadership. It was also suggested by one interviewee that relationships between GPs could be affected if CCGs asked practices to compete for a sizeable contract, or if the contract was designed to encourage a large number of patients to migrate between practices. Although our latest survey results suggest that the CCG has had a positive impact on relationships between practices, increasing the amount of contracting with GPs could affect this in the near future.
Page 47 of 62
40 Risk or reward? The changing role of CCGs in general practice
5. Discussion
As the pressures on the NHS and social care have continued to intensify over the last few years, a consensus between policy-makers, commissioners and GPs has emerged that puts primary care at the centre of changes needed to improve the quality of care and meet patient needs (British Medical Association, 2013; Department of Health and NHS England, 2014; Smith and others, 2013). It is clear that CCGs are well placed to lead this change: they have existing links with their GP membership, they have expertise about local primary care services and, for some, they are filling a leadership role that is currently absent.
In comparison to previous attempts to involve clinicians in commissioning, the CCGs in this research appeared to have been relatively successful in securing the support of local GPs, to date. Although the majority felt that CCGs were yet to have a positive impact on patient experience and quality of care, most viewed them as more effective than PCTs. As we found in the first year of our research, there remains an appetite to make the new arrangements a success and this positive start should be harnessed by CCGs as they work with their membership to lead change in primary care.
Extending CCG responsibilities in primary care as proposed under the co-commissioning plans could bring CCGs closer to their members, give them increased levers by which to direct service change in primary care, strengthen the peer-led quality improvement activities the CCG conducts, and control the budget for a larger proportion of their health economy, among other opportunities. However, in this financially difficult period, and depending on how CCGs implement their new role, co-commissioning and other ways in which CCGs are supporting primary care also have the potential to cause disengagement among clinical leaders and their membership if not adequately resourced and supported by GPs. Research on previous commissioning arrangements suggests similar issues: forecast by the findings of this study and research on previous commissioning arrangements: ‘History has shown that while GP commissioners start with a strong desire to be nimble clinically focused organisations, they are usually rushed by policy-makers into becoming larger statutory bodies with wide ranging responsibilities and are then deemed bureaucratic and distant from local professionals’ (Smith and Mays, 2012).
Our research indicated that few GPs felt performance management or the use of sanctions for under-performance were legitimate roles for CCGs. However, these may be necessary tools for CCGs that start managing primary care services. As articulated by the Royal College of General Practitioners and NHS Clinical Commissioners (2014), there are risks and opportunities in all of the co-commissioning options being offered. Those CCGs that undertake further co-commissioning arrangements could risk losing the membership ‘ethos’, but gaining the opportunity to influence the support given to primary care (Royal College of General Practitioners and NHS Clinical Commissioners, 2014). Those CCGs that do not apply for changes to their responsibilities may benefit from having continuity in their relationship with the membership, but would be without additional levers to influence NHS England commissioning.
Page 48 of 62

41 Risk or reward? The changing role of CCGs in general practice
Additionally, the introduction of this expanded remit for interested CCGs comes in a difficult external environment, where budgetary restrictions on the NHS and social care are already putting commissioners and providers under pressure. We outline below the five key areas of work that CCGs must focus on in order to ensure that the current model of commissioning is sustainable and maximises the benefit of new co-commissioning arrangements.
1. Sustain the involvement of clinical leadersEnthusiasm appeared to be waning among many of the clinical leaders who first established CCGs, and only a limited pool of interested GPs was emerging to replace them. One reason for this was the difficulty GP leaders face in balancing their day-to-day clinical work with their role within the CCG, which will not come as a surprise to those who were involved in previous forms of commissioning and understand that it is a ‘labour-intensive and time-consuming’ process (Shaw and others, 2014). GP leaders in this research also reported a lack of the training and development necessary to fulfil their role in the CCG, echoing the views of GPs in practice-based commissioning where only 20 per cent of GP leaders felt they had all the necessary skills (Wood and Curry, 2009). Over the next few years there will be increasing demands on GP leaders’ time from across the health system, and balancing this with any additional commissioning responsibilities will undoubtedly challenge GP leaders further. Providing clinicians with the resources, time and support to understand and deliver their commissioning role is essential. International evidence reflects similar findings here: in New Zealand’s primary care organisations, retaining and nurturing clinical leadership and influence was seen as the single most critical success factor in their development (Smith and Mays, 2007). Evidence from the United States points clearly to the need for heavy investment in leadership, management and training in order to create effective clinical commissioning organisations (Casalino, 2011).
Our survey suggests high levels of engagement in the work of the CCG among practice managers. CCGs should harness the interest of this group, as well as practice nurses and other primary care staff, to broaden the pool of individuals with a deep knowledge of local health services on whom they can draw. As has been highlighted in other parts of the health system, the key will be not only to support the top tier of current leaders, but also to cultivate the depth and breadth of leadership talent across the primary care workforce (West and others, 2014).
Many GP leaders on governing bodies will also reach the end of their terms of office during 2016 and 2017, making succession planning essential to secure the future sustainability of CCGs. We observed positive signs of some CCGs providing training for a broader group of younger clinicians. However, elsewhere it has been reported that many CCGs have stated in their constitutions that GP leaders can only serve for a finite period of time, creating an inevitable instability in their leadership (Checkland and others, 2012). Research with NHS providers suggests that strategic instability and lower staff morale can be caused by board-level vacancies, but that this risk can be negated by having strategies that develop future leaders (Janjua, 2014). This concern should be coupled with the fact that emerging GP provider federations and networks need strong clinical leadership to drive forward change in primary care (Addicott and Ham, 2014) and a role with provider groups may be more attractive to many GPs than roles in the CCG, as they are more closely linked to their day-to-day clinical work.
Page 49 of 62

42 Risk or reward? The changing role of CCGs in general practice
2. Maintain the strength of the membership voiceAs CCG running cost budgets are cut in 2015/16 and local health economies seek to produce the significant savings required by the slowdown in NHS funding growth, commissioners and providers will need to consider what size and configuration of local health and social care organisations are needed to meet that challenge. CCGs are already operating within a complex external environment that requires them to work flexibly in partnerships with a range of other organisations. This collaboration is an important tool for the development of coordinated local strategies and the creation of efficiencies through the joint use of resources. However, CCGs need to ensure that the membership voice remains strong in the decision-making process – something which existing structures do not always seem to deliver – and be able to demonstrate the impact GP involvement is having on their work. They should also ensure that new co-commissioning arrangements do not result in an excessive focus on contract compliance and performance management at the expense of maintaining a peer-to-peer, supportive relationship.
Although only one CCG merger has been approved since CCGs were formally launched in April 2013, it is possible that more may come over the next year. Where mergers take place, our research about engagement within large CCGs points to the importance of developing locality structures that allow for a more distributed model of leadership and a focus on local priorities.
3. Manage conflicts of interest A further challenge for CCGs is around the inherent conflicts of interest that arise from giving budgetary powers directly to groups of clinicians who are involved in provision as well as commissioning. Forthcoming changes mean that the frequency with which CCGs will be asked to make decisions on areas in which they have a vested interest will increase, further blurring the purchaser–provider split. In order to maintain buy-in from their members and external organisations, CCGs need to ensure that they are able to demonstrate transparency in their governance processes. Equally, support will need to be given to CCGs in order to avoid a situation where concern around conflicts of interest leads to inaction and an unwillingness to take bold decisions (as was the case with practice-based commissioning; Curry and others, 2008).
Members of the CCG board who are not GPs have a key role to play in ensuring that conflicts are adequately managed. In some of our sites, CCGs were starting to use their lay members to scrutinise their decision-making processes, and external bodies such as the CSU to run procurement exercises. A broad range of non-GP commissioners should be given more weight both within governing body meetings, and outside. Where co-commissioning is undertaken by CCGs, this suggestion will be reflected in the new decision-making bodies outlined by NHS England (NHS England, 2014c), and lay partner involvement should be strengthened following the national programme of training recently announced (NHS England and NHS Clinical Commissioners, 2014).
4. Be clear about the relationship with NHS England As some CCGs take on additional responsibilities from NHS England, the relationship between them will necessarily change. This is important to consider for two reasons. First, some GPs were already confused about the distinction between the organisations,
Page 50 of 62

43 Risk or reward? The changing role of CCGs in general practice
and the forthcoming arrangements are likely to exacerbate this in the short term. Second, a few of our case study sites told us about capacity issues in the areas teams and how their contact was limited; something which could potentially become more difficult as the area teams are reorganised and their number reduced. CCGs that are given additional commissioning responsibilities under the co-commissioning policy will be able to agree local arrangements for sharing staff with NHS England. However, the risk remains that these resources prove to be inadequate and co-commissioning proves too challenging for GP leaders already feeling the strain of existing commissioning responsibilities.
5. Ensure that CCGs have adequate funding to take on new functionsCCGs have been offered the ability to take on additional commissioning responsibilities at the same time as their running cost budgets are being reduced by ten per cent. Although CCGs that are given these additional responsibilities under the co-commissioning policy will be able to agree local arrangements for sharing staff with NHS England, the risk remains that these resources prove to be inadequate and some CCGs may struggle to fulfil their new roles effectively.
Page 51 of 62

44 Risk or reward? The changing role of CCGs in general practice
6. Conclusion: balancing the risks and rewards of CCGs’ expanding role in primary care development
Our evidence shows that during the first year as fully established commissioning organisations, CCGs took positive first steps in engaging GPs and promoting improvements to the organisation and quality of general practice. However, as the slowdown in NHS funding growth continues, CCGs’ responsibilities expand and CCGs seek to operate within reduced management budgets, the challenges they have faced so far will be intensified.
CCGs’ success at co-commissioning primary care will depend on the extent to which they are able to maintain their peer-to-peer support focus and therefore whether they can mobilise the primary care workforce to develop and deliver new models of care. As their role in improving or developing primary care progresses, CCGs may struggle to find the capacity to take on new commissioning responsibilities in addition to their current commissioning work, and GP leaders will need to balance new roles with the pressure of their day-to-day clinical practice. CCGs also risk being challenged about conflicts of interest – or allowing them to stall innovation – and alienating their members as they seek to address under-performance.
Additionally, if the NHS moves closer to the Five Year Forward View’s vision of a more integrated future system with larger hospital or community-based multi-specialty practices and accountable care organisations (NHS England and others, 2014), the role of CCGs will need to evolve. New larger providers may take on some of the CCGs’ responsibilities for coordinating local provision and planning services for their local populations’ health needs.
Without structures that encourage innovative and critical input from clinicians, CCGs will not be able to achieve one of their original principles: that commissioning led by clinicians will lead to more appropriate decision-making, better outcomes for patients and more effective use of resources (Department of Health, 2011). As CCGs take on extended roles over the next year, they will need to ensure that they mitigate the risks outlined in this report. If they are able to achieve this, CCGs will be better equipped to use their strength as membership organisations to move beyond small-scale progress and deliver real change at scale for patients.
Page 52 of 62
45 Risk or reward? The changing role of CCGs in general practice
Appendix 1: Research methodology
The six case study sites were selected at random in 2012, using a stratified approach to ensure that we included CCGs of various sizes and from all four regions of NHS England. We ensured that the sites represented a wide range in terms of level of deprivation, and included both urban and rural areas.
The CCGs that took part in the research in year one all continued to take part in year two, and we collected information through largely the same methods as in year one:
• documentaryanalysisofkeydocumentsrelatingtotheCCG,particularlyboardpapers
• semi-structuredinterviewswith70keyindividuals–thosewithandthosewithoutaformal role in the CCG
• observationsof18meetings,primarilyCCGgoverningbodyandmemberengagement meetings
• anonlinesurveyofmemberpracticeswith279responses,primarilyfromGPswithout a formal role in the CCG.
This second phase of research was conducted in early 2014. See Naylor and others (2013) for details of the first phase of research.
Documentary analysisContent analysis of governing body board papers and minutes was carried out for each of the case study sites. Papers were selected to cover a period of ten to 12 months between January 2013 and March 2014, depending on availability of papers for each site at the time of analysis.
Analysis focused on content relating to primary care, in particular:
• performancemetricsusedforgeneralpractice
• GPmemberengagement
• relationshipwithNHSEnglandrelatedtoGPcontractmanagement
• primarycareinitiativesandstrategy.
Documentary analysis notes were then coded thematically.
Page 53 of 62

46 Risk or reward? The changing role of CCGs in general practice
InterviewsSemi-structured interviews were carried out with a total of 70 individuals in year two (Table A1). As in year one, these included:
• CCGleaders(clinicalandnon-clinical),includingthechairandaccountableofficerof each site, and practice representatives
• GPmembersandpracticemanagers
• seniormanagersfromNHSEnglandareateamsandCSUs
• representativesoflocalmedicalcommittees.
Year two also included interviews with representatives of local authorities.
The interviews covered:
• engagementwiththeCCG
• theroleoftheCCGinprimarycaredevelopment
• theimpactoftheCCGonclinicalrelationships.
Interview transcripts were coded thematically using qualitative data analysis software.
Table A1: Interview type, 2014
Role Type NumberCCG leaders Clinical 12
Non-clinical 21CCG members With a formal role in CCG 5
No formal role in CCG 12Area team 6Commissioning support unit 6Local medical committee 2Local authority 6Total 70
ObservationsWe conducted observations of governing body, member council and locality meetings in each of the six sites (18 in total). Observation notes were coded thematically using qualitative data analysis software, alongside the interview transcripts.
Survey of member practicesIn each site, all local GPs were invited to complete an online survey. As in year one, the survey was distributed directly to all member practices by email and CCG intranet systems. Practice managers and other personnel were also permitted to complete this survey. Where possible, questions remained the same as those asked in year one, in order to allow comparisons to be made over time.
Page 54 of 62

47 Risk or reward? The changing role of CCGs in general practice
A total of 279 responses were received in year two across the six case study sites. More than three quarters of the responses received were from GPs, with the remainder being mainly from practice managers. This has provided an approximate response rate of 28 per cent, based on the number of all GPs across the case study sites. As in year one, respondents were asked questions on the following issues:
• theirlevelsofengagementwiththeworkoftheCCG
• theroleoftheCCGinsupportingimprovementingeneralpractice
• authorityandaccountabilitywithintheCCG
• theimpactofCCGsonprofessionalrelationships,clinicalpracticeandpatients.
The survey in year two was conducted between January and February 2014 – approximately one year since the first year’s survey was conducted. A full summary of survey results, including comparisons over year one and two, is available (Robertson and others, 2014).
Table A2: Survey respondents by role
Role 2013 2014n % n %
GP principal 149 64 198 71Salaried GP 16 7 34 12Practice manager 47 20 28 10Other/skipped 20 9 19 7Total 232 279
Page 55 of 62

48 Risk or reward? The changing role of CCGs in general practice
Appendix 2: Case study site details
Site A Site A is a mid-sized CCG serving a mixed population that is largely affluent but with some significant pockets of deprivation. The population is older than the national average and has high rates of dementia.
The CCG was formed out of two practice-based commissioning groups. It does not have a formal locality structure, but does divide members into local groupings for the purposes of undertaking peer review and other activities.
The CCG has a partnership agreement with neighbouring CCGs and a number of board-level posts are held jointly. The main secondary care providers are located outside the CCG boundaries, making the CCG a minority commissioner in most cases.
Site BSite B is the largest CCG in our research. Overall, deprivation is low, although the population profile varies significantly across the site.
The CCG has a strong history of GP commissioning and has a locality structure with groupings based largely on former practice-based commissioning groups. More powers are delegated to locality level than in our other sites – each locality is allocated an annual commissioning budget by the governing body, and localities have a delegated budget to invest in improving local patient care. Members report a stronger sense of identity with the locality than the CCG governing body as a whole.
The CCG partners with neighbouring CCGs for commissioning of acute and community services.
Site CSite C is a small, urban CCG with the highest level of deprivation of our case study sites. It has a relatively young population. Mortality rates from cancer and cardiovascular and respiratory diseases are very high, and measures of quality of life for people with long-term conditions are among the poorest in the country.
The CCG was formed on the basis of previous practice-based commissioning groups. It was originally conceived as two separate CCGs, but concerns around sustainability led to a merger. It is beginning to develop locality working and encouraging joint working. It has a relatively large number of small and single-handed practices. The CCG shares a senior post with two other CCGs, and collaborates with neighbouring CCGs through a regional network. The CCG is coterminous with the local authority.
Page 56 of 62

49 Risk or reward? The changing role of CCGs in general practice
Site DSite D is a mid-sized CCG. It operates in an urban environment serving a young, deprived population with high levels of mental health and substance abuse problems.
The CCG was formed out of a single practice-based commissioning group and operates with a number of localities that pre-date the CCG. It has close relationships with neighbouring CCGs and local authorities, including joint strategy and performance committees. However, there are no formal alliances.
Site ESite E is the smallest CCG of our case studies and serves a deprived urban population with high mortality rates, particularly from conditions related to smoking and alcohol.
The CCG consists of a highly cohesive group of practices with a strong local identity and history of collaborative working. The CCG does not have a formal locality structure, but meets with practices in small locality groups as a mechanism for engagement and peer review.
Since its inception, the CCG has worked closely with two neighbouring CCGs as part of an alliance. The alliance has an overarching management team with shared posts and some shared committees.
Site FSite F covers a mid-sized population that is spread over a wide and largely rural area. It is one of the least deprived CCGs in England and has a population that is significantly older than the national average.
There is a long history of GP commissioning and collaboration in the area. The CCG is part of a formal alliance with two neighbouring CCGs, through which an integrated commissioning plan has been jointly developed.
Page 57 of 62

50 Risk or reward? The changing role of CCGs in general practice
References
Addicott R and Ham C (2014) Commissioning and Funding General Practice: Making the case for family care networks. The King’s Fund.
Association of Directors of Adult Social Services (2014) ADASS Budget Survey Report 2014: Final. Available at: www.adass.org.uk/adass-budget-survey-2014/
Bardsley M, Steventon A, Smith J and Dixon J (2013) Evaluating Integrated and Community-based Care: How do we know what works? Nuffield Trust.
British Medical Association (2013) Collaborative GP Alliances and Federations: Guidance for GPs.
British Medical Association (2014) BMA Quarterly Tracker Survey: An extract of responses from GPs.
Calkin S (2014) ‘NHS England restructure: new “sub region” directors appointed’, Health Service Journal, 28 November.
Casalino L (2011) GP Commissioning in the NHS in England: Ten suggestions from the United States. Nuffield Trust.
Checkland K, Coleman A, Perkins N, McDermott I, Petsoulas C, Wright M, Glasby E and Peckham S (2014) Exploring the Ongoing Development and Impact of Clinical Commissioning Groups. Policy Research Unit in Commissioning and the Healthcare System.
Checkland K, Coleman A, Segar J, McDermott I, Miller R, Wallace A, Petsoulas C, Peckham S and Harrison S (2012) Exploring the Early Workings of Emerging Clinical Commissioning Groups: Final report. Policy Research Unit in Commissioning and the Healthcare System.
Curry N, Godwin N, Naylor C and Robertson R (2008) Practice-based Commissioning: Reinvigorate, replace or abandon? The King’s Fund.
Dayan M, Aroras S, Rosen R and Curry N (2014) Is General Practice in Crisis? Nuffield Trust.
Department of Health (2001) Shifting the Balance of Power Within the NHS.
Department of Health (2011) Government Response to the NHS Future Forum Report. Available at: www.gov.uk/government/uploads/system/uploads/attachment_data/file/216361/dh_127719.pdf
Department of Health and NHS England (2014) Transforming Primary Care: Safe, proactive, personalised care for those who need it most. Department of Health.
Glennerster H (1994) Implementing GP Fundholding: Wild card or winning hand? Buckingham five year plan. Open University Press.
Health Service Journal (2014) ‘CCG chair steps down to lead GP “super-practice”’, Health Service Journal, 12 December.
HM Government (1990) National Health Service and Community Care Act 1990.
Ipsos MORI (2014) CCG 360 Degree Stakeholder Survey. Available at: www.england.nhs.uk/wp-content/uploads/2014/10/ccg-360-survey.pdf
Janjua A (2014) Leadership Vacancies in the NHS: What can be done about them? The King’s Fund.
Mays N (2001) The Purchasing of Health Care by Primary Care Organizations: An evaluation and guide to future policy. Open University Press.
National Audit Office (2014a) The Financial Sustainability of NHS Bodies.
National Audit Office (2014b) Planning for the Better Care Fund.
Naylor C, Curry N, Holder H, Ross S, Marshall L and Tait E (2013) Clinical Commissioning Groups: Supporting improvements in general practice? The King’s Fund.
NHS England (2013) Towards Commissioning Excellence: Developing a strategy for commissioning support services. Available at: www.england.nhs.uk/wp-content/uploads/2013/06/towa-commis-exc.pdf
Page 58 of 62
51 Risk or reward? The changing role of CCGs in general practice
NHS England (2014a) Co-commissioning of primary care services. A letter to CCGs and Area Teams, 9 May. Available at: www.hsj.co.uk/Journals/2014/05/12/o/u/q/2014-05-09-CCG-co-commissioning-letter.pdf
NHS England (2014b) CCG Running Costs Allowances 2014/15 & 2015/16. A letter to CCGs and Area Teams, 31 January 2014. Available at: www.england.nhs.uk/wp-content/uploads/2014/02/run-cost-allow-lett.pdf
NHS England (2014c) Managing Conflicts of Interest: Statutory guidance for CCGs. Available at: www.england.nhs.uk/wp-content/uploads/2014/12/man-confl-int-guid-1214.pdf
NHS England and NHS Clinical Commissioners (2014) Next Steps Towards Primary Care Co-commissioning. NHS England.
NHS England, Public Health England, Care Quality Commission, Trust Development Authority, Monitor and Health Education England (2014) Five Year Forward View. NHS England.
Robertson R, Holder H, Bennett L, Ross S and Gosling J (2014) Clinical Commissioning Groups – One Year On: Member engagement and primary care development. Slide pack. Available at: www.nuffieldtrust.org.uk/talks/slideshows/holly-holder-clinical-commissioning-groups-one-year
Royal College of General Practitioners and NHS Clinical Commissioners (2014) The Risks and Opportunities for CCGs When Co-commissioning Primary Care: Things to consider when making your decision.
Shaw S, Smith J, Porter A, Rosen R and Mays M (2014) ‘The work of commissioning: a multisite case study of healthcare commissioning’, BMJ Open, 3, e003341.
Smith J and Mays N (2007) ‘Primary care organisations in New Zealand and England: tipping the balance of the health system in favour of primary care?’, International Journal of Health Planning and Management, 22, 3–19.
Smith, J and Mays, N (2012) ‘GP led commissioning: time for a cool appraisal’, BMJ, 344, e980.
Smith J, Holder H, Edwards N, Maybin J, Parker H, Rosen R and Walsh N (2013) Securing the Future of General Practice: New models of primary care. Nuffield Trust.
Thorlby R, Rosen R and Smith J (2011) GP Commissioning: Insights from medical groups in the United States. Nuffield Trust.
Welikala J (2015) ‘Three southern CSUs to formally merge’, Health Service Journal, 6 January.
West M, Steward K, Eckert R and Pasmore B (2014) Developing Collective Leadership for Health Care. The King’s Fund.
Wood J and Curry N (2009) PBC two years on: Moving forward and making a difference? The King’s Fund.
Page 59 of 62
52 Risk or reward? The changing role of CCGs in general practice
About the authorsHolly Holder is a Fellow in Health Policy at the Nuffield Trust. She is trained in a variety of research methods and specialises in qualitative research. Her current projects at the Trust include evaluating integrated care systems, tracing the evolution of clinical commissioning groups, and comparative analysis of international health and social care systems. Prior to joining the Trust in October 2011, Holly worked for the Centre for Analysis of Social Exclusion at the London School of Economics.
Ruth Robertson returned to The King’s Fund as a Health Policy Fellow in September 2013, after three years spent researching health insurance coverage issues at the Commonwealth Fund in New York. Ruth also worked at The King’s Fund from 2006 to 2010, completing national evaluations of two of Labour’s major health system reforms: practice-based commissioning and patient choice policy. She was previously an analyst at the Healthcare Commission (the predecessor to the Care Quality Commission).
Shilpa Ross is a Senior Researcher in Health Policy at The King’s Fund. She has more than ten years’ experience in carrying out qualitative social research. Current projects include the emerging lessons from clinical commissioning groups, an evaluation of the change process within an integrated care programme and an evaluation of the implementation of Schwartz Rounds in England.
Laura Bennett is a Researcher at The King’s Fund. Her interests include health inequalities, commissioning and the provision of care outside acute hospitals. Current projects include the emerging lessons from clinical commissioning groups, evaluating the implementation of Schwartz Rounds in England and exploring how quality is managed in community health services.
Jeni Gosling has been a Lecturer in Health Management at the London School of Hygiene and Tropical Medicine since 2007. Previously she worked as a Practice Manager in various general practices in London and the Midlands. Her research interests focus on current reforms to the NHS, particularly primary care and general practice, and the impact of management in health services.
Natasha Curry joined the Nuffield Trust in 2011 as a Senior Fellow in Health Policy. Her research interests include clinical commissioning, primary care provider models, integrated care, international health systems and NHS reform. In her previous role at The King’s Fund, Natasha published widely on a number of subjects, including practice-based commissioning, the management of long-term conditions and approaches to clinical and service integration.
Page 60 of 62
53 Risk or reward? The changing role of CCGs in general practice
About The King’s FundThe King’s Fund is an independent charity working to improve health and health care in England. We help to shape policy and practice through research and analysis; develop individuals, teams and organisations; promote understanding of the health and social care system; and bring people together to learn, share knowledge and debate. Our vision is that the best possible care is available to all.
About the Nuffield TrustThe Nuffield Trust is an authoritative and independent source of evidence-based research and policy analysis for improving health care in the UK. Our vision is to help provide the objective research and analysis that boosts the quality of health policy and practice, and ultimately improves the health and health care of people in the UK.
Page 61 of 62

For more information about the Nuffield Trust and The King’s Fund, including details of the latest research and analysis, please visit www.nuffieldtrust.org.uk and www.kingsfund.org.uk
Download further copies of this report from www.nuffieldtrust.org.uk/publications or www.kingsfund.org.uk/publications
Subscribe to our newsletter: www.nuffieldtrust.org.uk/newsletter
Twitter.com/NuffieldTrust Twitter.com/TheKingsFund
Nuffield Trust 59 New Cavendish Street London W1G 7LPTelephone: 020 7631 8450 Email: [email protected]
www.nuffieldtrust.org.uk
The King’s Fund11–13 Cavendish Square London W1G 0ANTelephone: 020 7307 2568Email: [email protected]
www.kingsfund.org.uk
Published by the Nuffield Trust and The King’s Fund.© Nuffield Trust and The King’s Fund 2015. Not to be reproduced without permission.
ISBN: 1-978-905030-91-0
Page 62 of 62
Document 33(03)03
Report to Knowsley Clinical Commissioning Group Governing Body Date of meeting: 5th March 2015
Report title: Contracting Progress Update 15/16
Report presented by: Philip Thomas, Commissioning Director
Purpose of the report: To update the Governing Body on progress with the 2015/16 planning and contracting round.
Recommendations:
Action / Decision required
The Governing Body is recommended to:
Note the report
Delegated Powers:
For decision reports only
N/A
Justification for Part B agenda (if applicable)
N/A
Commissioning Values Which area(s) does this support? Please insert ‘x’ that apply
1. Patient centred x
2. Safe x
3. High quality x
4. Cost effective x
5. Outcome focused x
6. Closer to home x
7. Affordable x
[one page only]
Page 1 of 10

GOVERNING BODY
2015/16 PLANNING AND CONTRACTING PROGRESS UPDATE
Executive Summary Each year the NHS issues national planning guidance to providers and commissioners to inform planning and contracting at a local level. Guidance for 2015/16 was issued on the 23rd December 2014, and requires the CCG to review and refresh its 2015/16 operational plans according to a national timetable. The CCG holds a number of one year contracts with a range of acute, mental health and community providers of NHS services. Each year these contracts need to be reviewed and renegotiated.
This report summarises progress to date on the planning and contracting process and the accompanying guidance. In particular, progress on some elements of planning and contracting is reliant upon the publication of national guidance, and temporary approaches are being adopted in the interim.
The Governing Body is asked to note the contents of the report and progress to date in agreeing new contracts for 2015/16 and preparing its 2015/16 plans.
Page 2 of 10

1. Purpose of the briefing 1.1 The purpose of this report is to update the Governing Body on the progress of the
organisation against the NHS planning and contracting timetable for 2015/16. 2. Background 2.1 Last year, CCGs were required to develop two year operational plans, which included
2015/16, and also an outline 5 year plan. The planning guidance for 2015/16 was issued on the 23rd December 2014, and requires CCGs to review and refresh the 2015/16 operational plans.
2.2 The CCG holds a number of annual contracts with a range of acute, mental health and community providers of NHS services. In parallel with the planning process, each year these contracts need to be reviewed and renegotiated. Total contracted services which are subject to this annual negotiation process amount to approx. £163 million.
2.3 Knowsley CCG has significant contractual relationships with a number of provider organisations across Merseyside. Four main providers, however, are recognised as “key” Providers for Knowsley CCG in that the CCG contributes >5% towards the overall level of Provider income. These are:
a) St Helens & Knowsley Hospitals NHS Trust b) Aintree University Hospitals NHS Foundation Trust c) 5 Boroughs Partnership NHS Foundation Trust d) Liverpool Women’s Hospital NHS Foundation Trust
Together these four “key” providers account for 85% (£138m) of the value for contracts subject to this annual renegotiation process.
2.4 Knowsley also holds contracts of a significant value with Royal Liverpool & Broadgreen Hospitals NHS Trust, Alder Hey Children’s Hospital NHS Foundation Trust and Merseycare. However, due to the volume of Specialised Service delivered by these providers, the CCG is not deemed to be a key stakeholder in these Providers.
2.5 The CCG also contracts with NWAS which is co-ordinated by Blackpool CCG on behalf of the CCGs in the Northwest and is, therefore, a minor associate to the contract.
2.6 The CCG purchases contract management services from the North West Commissioning Support Unit who are contracted to support the CCG in all aspects of contract negotiation, contract management and contract monitoring.
3. Key Issues 3.1 Business Rules - 2015/16 NHS Standard Contract and Tariff
3.1.1 Whilst draft guidance and standard contracts were published on 19 December 2014 and 23
December 2014, respectively, final versions are yet to be received. Additionally, the national tariff consultation saw providers reject the proposals. Commissioners and providers are
Page 3 of 10
proceeding with their negotiations based upon the draft guidance and contract. The CCG is undertaking its financial planning based upon the consultation tariffs. Once final the guidance, contract and tariff arrangements have been published the CCG will need to review its plans to ensure they reflect the guidance and contract requirements and are affordable.
3.1.2 This has implications for another key aspect of the business rules, namely that this year’s guidance calls for close alignment between provider and commissioner plans as follows:
We expect greater consistency between the activity and financial trajectories set out in commissioner and provider plans. The extent to which the trajectories are both realistic and sufficiently aligned will be tested through a joined-up process to ensure that all partners have a shared understanding of how local services will be transformed.
3.1.3 In the absence of an agreed methodology for pricing the activity purchased by
commissioners in contracts, securing agreements and ensuring this alignment will remain challenging.
3.2 Planning
3.2.1 The CCG is required to complete the templates issued alongside the guidance according to the following high level timetable: 13th January 2015 Submission of initial headline plan data 13th February 2015 Checkpoint for progress with planning measures and trajectories 27th February 2015 Submission of full draft plans 27th Feb – 30th March 2015
Assurance of draft plans
By 31st March 2015 Plans to be approved by Governing Body 10th April 2015 Submission of full final plans
3.2.2 The initial submission on the 13th January was made on time and consisted of a high level finance and activity plan. The national deadline for the submission of accompanying performance trajectories for NHS Constitution standards and other key outcomes such as Improving Access to Psychological Therapies (IAPT) was extended to the 28th January, and this submission deadline was met. The next phase is for feedback to CCGs ahead of submission of final plans by 27th February 2015.
3.2.3 The main issue that remains to be resolved as at the time of writing is to review the level of ambition against the Better Care Fund measures, in the light of most current assumptions. Although BCF planning guidance sets an indicative figure for an overall reduction of 3.5% in non-elective admissions, each local area can set its own level of ambition, taking into account local circumstances. As part of the refresh of plans, CCGs are expected to review this ambition in light of the current operational circumstances, taking into account the broad range of planning factors, including: (i) actual performance in the year to date, particularly through the winter; (ii) the likely outturn for 2014/15; and (iii) progress with contract negotiations with providers. These factors require further work before an informed position can be reached and agreed.
Page 4 of 10

3.3 Contracting Update 3.3.1 The high level contracting timetable is as follows:
By 1 Nov 2014 NHS England and CCG Commissioning Intentions provided to
Trusts By 23 Dec 2014 Publication of Final 2015/16 Planning Guidance, including
provisional tariff assumptions, to be followed by: • Standard Contract for 15/16 • Revised Contract Dispute Resolution procedure
Jan 2015 Publication of revised National Tariff1 Jan – 11 Mar 2015 Contract negotiations – including voluntary mediation From 29 Jan 2015 Weekly contract tracker to be submitted each Thursday (CCGs,
NHS England, NHS Trusts) 20 February National Contract stocktake – to check the status of contracts 11 Mar 2015 Contracts signed post-mediation (CCGs, NHS England, NHS
Trusts and Foundation Trusts) 12 Mar – 23 Mar 2015
Contract arbitration (CCGs, NHS England, NHS Trusts)
By 25 Mar 2015 Arbitration outcomes notified to commissioners and providers (CCGs, NHS England, NHS Trusts)
3.3.2 Finance and Activity Plans Through the planning process, progress is being made to determine CCG activity plans with each provider. Providers are developing their own activity plans. These plans will be the subject of negotiation between the CCG and providers as part of the negotiation process. As indicated above, the national tariff proposals have been rejected by providers. In accordance with national guidance, the CCG is undertaking its financial planning using the consultation tariffs. Once national tariffs have been agreed the CCG will review those financial plans to ensure reflect those tariffs and remain affordable.
3.3.3 Reporting and Information Requirements Considerable work has been undertaken in respect of the 5 Boroughs Partnership NHS Foundation Trust (5BP), for which the CCG is co-ordinating commissioner, and where the reporting and information requirements require improvement due to gaps in what is required and reported. Once agreed, compliance with these reporting requirements will be closely monitored and any issues escalated through formal contract management arrangements as necessary.
3.3.4 Commissioning and Provider Intentions The CCG’s draft 2015/16 Commissioning Intentions have been made available to providers. Following the commissioning plan and priorities discussions held with CMG on 10 February 2015, these will be reviewed to ensure they reflect the CCG’s agreed set of priorities for next year.
3.3.5 Quality and CQUIN
Whilst final guidance is awaited, which will set out a number of national CQUIN requirements, members of the Quality and Safety Team are actively engaged in work developing quality schedules and CQUINs for local contracts. As with other aspects of the contracting work, following publication of the final guidance and contract, these schedules and schemes will be reviewed to ensure compliance with that guidance and contract.
Page 5 of 10
4. Actions being taken by the CCG 4.1 The Planning and Contracting Task and Finish Group meets fortnightly to review progress
against the project plan, communicate CCG decisions on contracting negotiation issues, and identify risks or issues.
4.2 The CCG chairs the Contract Negotiation Meetings for the 5BP contract, with those negotiations making good progress to finalise finance and activity plans, information and quality schedules and CQUIN schemes.
4.3 The CCG also attends the contract negotiation meetings for St Helens and Knowsley Teaching Hospitals NHS Trust and Aintree University Hospital NHS Foundation Trust with NWCSU attending others in their capacity as our contracting resource.
4.4 NHSE have established a contract negotiation tracking process, which requires the CCG to submit weekly status reports on negotiations for any contracts where it spends in excess of £5m. NWCSU complete this on behalf of the CCG, liaising with co-ordinating commissioners to obtain status reports, with the CCG signing-off this return prior to submission.
5. Summary 5.1 The CCG is fully engaged in the planning and contracting process to submit the required
planning outputs and agree NHS contracts for 2015/16 and will continue to work closely with co-ordinating commissioners throughout the contract negotiation process to ensure Commissioning Intentions, Service Development and Improvement Plans and CQUIN schemes included in contracts accurately reflect the CCG’s commissioning plans.
5.2 The CCG will also continue to work with partners to ensure that planning and delivery of
contracting for NHS providers is supported in a flexible, timely and commissioner focussed manner.
Management Leads:
Philip Thomas – Commissioning Director Andrew Thomas – Governance Director
Signatory details: Philip Thomas [email protected] 0151 244 4149 Andrew Thomas [email protected] 0151 244 3109
Background Documents:
Appendices:
Appendix 1: NHS Knowsley CCG: Contracts subject to contract negotiation process 2015/16
Appendix 2: Collaborative Commissioning partners for 2015/16 contract round
Appendix 3: Contract Tracker
Page 6 of 10
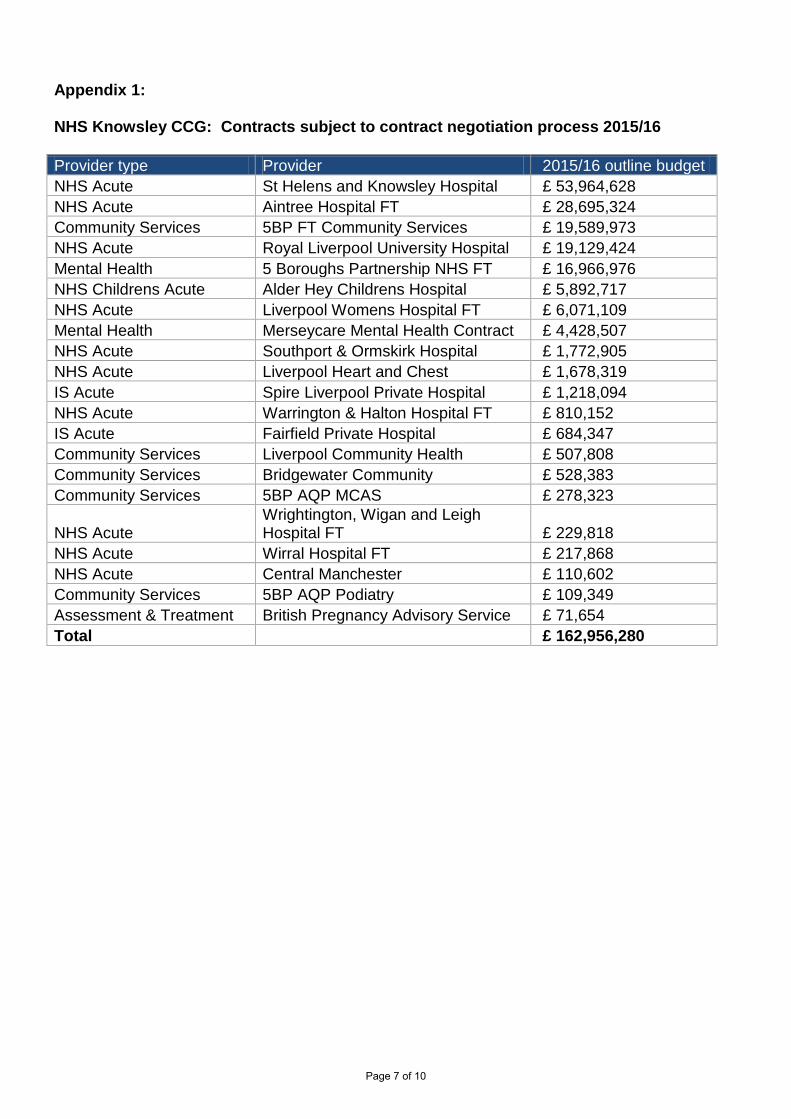
Appendix 1: NHS Knowsley CCG: Contracts subject to contract negotiation process 2015/16
Provider type Provider 2015/16 outline budget NHS Acute St Helens and Knowsley Hospital £ 53,964,628 NHS Acute Aintree Hospital FT £ 28,695,324 Community Services 5BP FT Community Services £ 19,589,973 NHS Acute Royal Liverpool University Hospital £ 19,129,424 Mental Health 5 Boroughs Partnership NHS FT £ 16,966,976 NHS Childrens Acute Alder Hey Childrens Hospital £ 5,892,717 NHS Acute Liverpool Womens Hospital FT £ 6,071,109 Mental Health Merseycare Mental Health Contract £ 4,428,507 NHS Acute Southport & Ormskirk Hospital £ 1,772,905 NHS Acute Liverpool Heart and Chest £ 1,678,319 IS Acute Spire Liverpool Private Hospital £ 1,218,094 NHS Acute Warrington & Halton Hospital FT £ 810,152 IS Acute Fairfield Private Hospital £ 684,347 Community Services Liverpool Community Health £ 507,808 Community Services Bridgewater Community £ 528,383 Community Services 5BP AQP MCAS £ 278,323
NHS Acute Wrightington, Wigan and Leigh Hospital FT £ 229,818
NHS Acute Wirral Hospital FT £ 217,868 NHS Acute Central Manchester £ 110,602 Community Services 5BP AQP Podiatry £ 109,349 Assessment & Treatment British Pregnancy Advisory Service £ 71,654 Total £ 162,956,280
Page 7 of 10
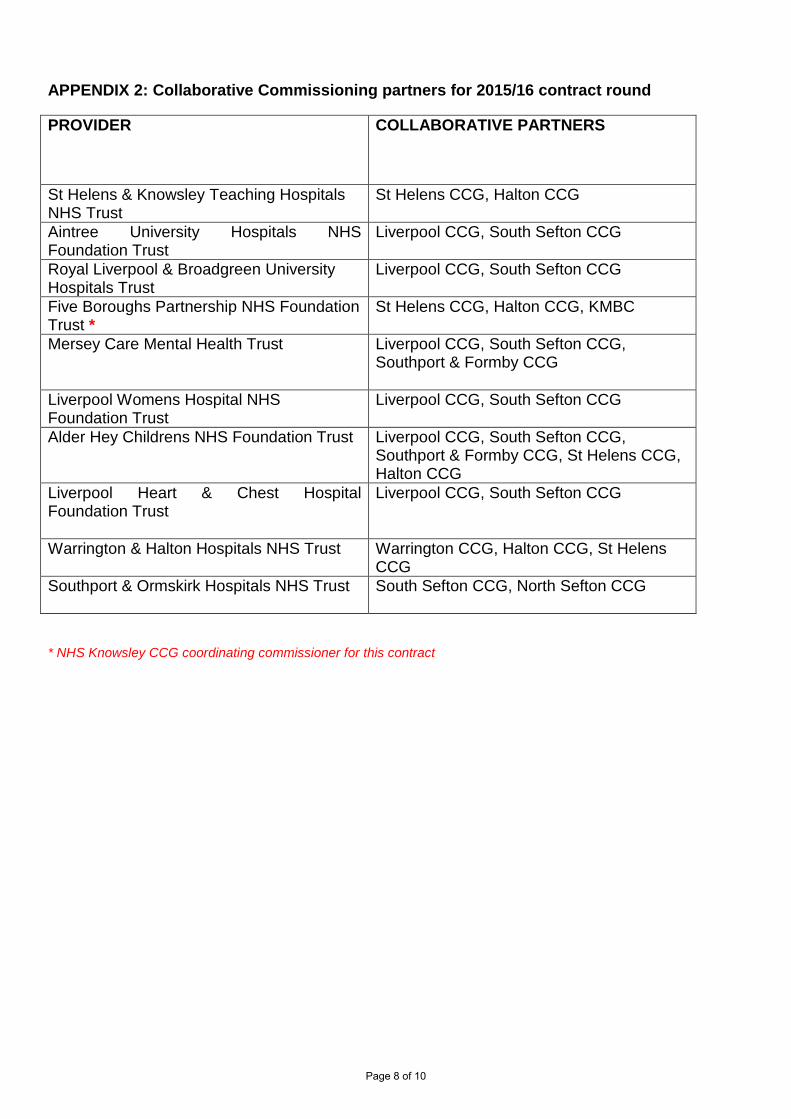
APPENDIX 2: Collaborative Commissioning partners for 2015/16 contract round
PROVIDER COLLABORATIVE PARTNERS
St Helens & Knowsley Teaching Hospitals NHS Trust
St Helens CCG, Halton CCG
Aintree University Hospitals NHS Foundation Trust
Liverpool CCG, South Sefton CCG
Royal Liverpool & Broadgreen University Hospitals Trust
Liverpool CCG, South Sefton CCG
Five Boroughs Partnership NHS Foundation Trust *
St Helens CCG, Halton CCG, KMBC
Mersey Care Mental Health Trust Liverpool CCG, South Sefton CCG, Southport & Formby CCG
Liverpool Womens Hospital NHS Foundation Trust
Liverpool CCG, South Sefton CCG
Alder Hey Childrens NHS Foundation Trust
Liverpool CCG, South Sefton CCG, Southport & Formby CCG, St Helens CCG, Halton CCG
Liverpool Heart & Chest Hospital Foundation Trust
Liverpool CCG, South Sefton CCG
Warrington & Halton Hospitals NHS Trust
Warrington CCG, Halton CCG, St Helens CCG
Southport & Ormskirk Hospitals NHS Trust
South Sefton CCG, North Sefton CCG
* NHS Knowsley CCG coordinating commissioner for this contract
Page 8 of 10
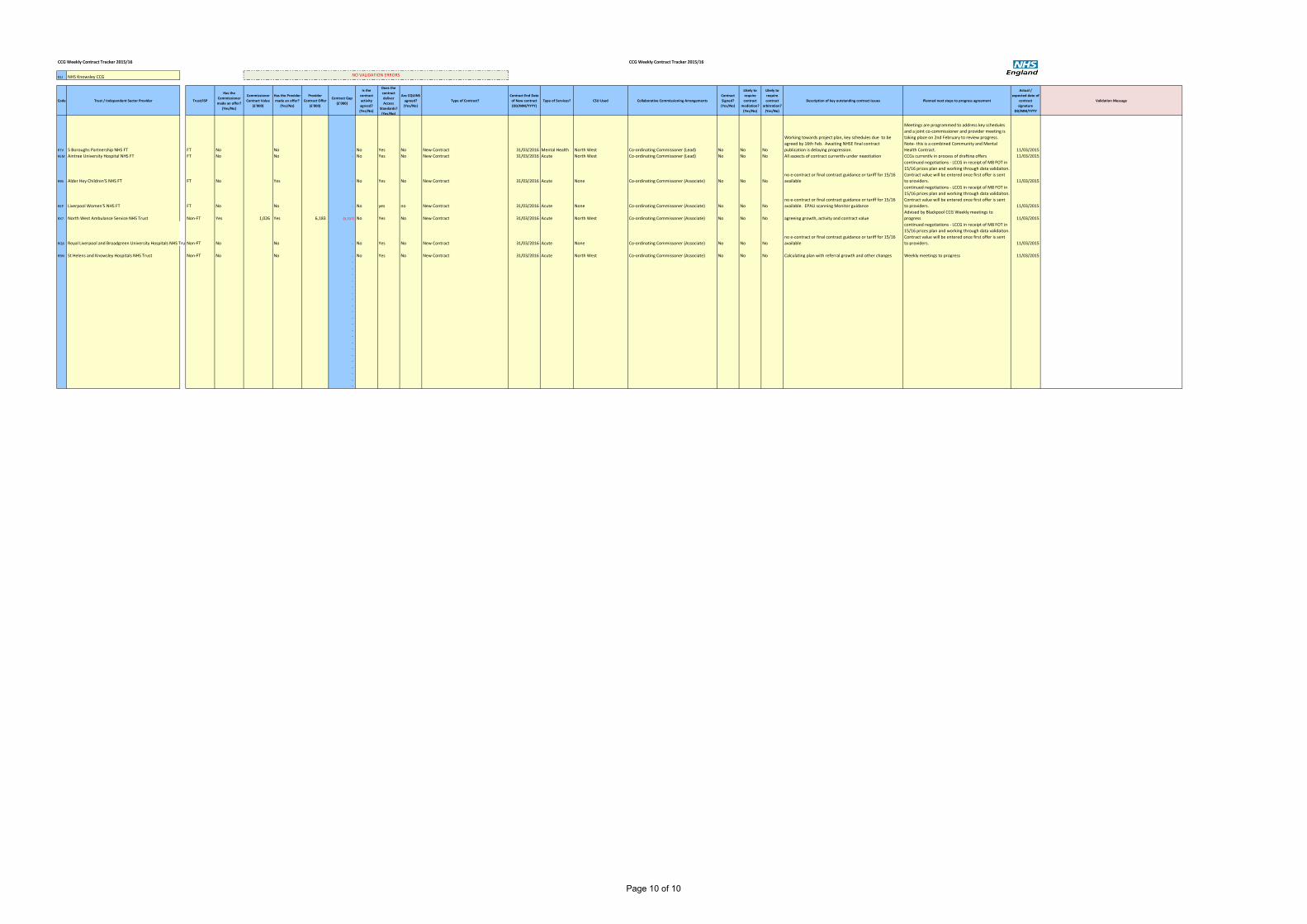
CCG Weekly Contract Tracker 2015/16 CCG Weekly Contract Tracker 2015/16
code CCG
01J NHS Knowsley CCG
Code Trust / Independent Sector Provider Trust/ISP
Has the
Commissioner
made an offer?
(Yes/No)
Commissioner
Contract Value
(£'000)
Has the Provider
made an offer?
(Yes/No)
Provider
Contract Offer
(£'000)
Contract Gap
(£'000)
Is the
contract
activity
agreed?
(Yes/No)
Does the
contract
deliver
Access
Standards?
(Yes/No)
Are CQUINS
agreed?
(Yes/No)
Type of Contract?
Contract End Date
of New contract
(DD/MM/YYYY)
Type of Services? CSU Used Collaborative Commissioning Arrangements
Contract
Signed?
(Yes/No)
Likely to
require
contract
mediation?
(Yes/No)
Likely to
require
contract
arbitration?
(Yes/No)
Description of key outstanding contract issues Planned next steps to progress agreement
Actual /
expected date of
contract
signature
DD/MM/YYYY
Validation Message
Subcode
RTV 5 Boroughs Partnership NHS FT FT No No - No Yes No New Contract 31/03/2016 Mental Health North West Co-ordinating Commissoner (Lead) No No No
Working towards project plan, key schedules due to be
agreed by 16th Feb. Awaiting NHSE final contract
publication is delaying progression.
Meetings are programmed to address key schedules
and a joint co-commissioner and provider meeting is
taking place on 2nd February to review progress.
Note- this is a combined Community and Mental
Health Contract. 11/03/2015 CCG_1000
REM Aintree University Hospital NHS FT FT No No - No Yes No New Contract 31/03/2016 Acute North West Co-ordinating Commissoner (Lead) No No No All aspects of contract currently under negotiation CCGs currently in process of drafting offers 11/03/2015 CCG_1001
RBS Alder Hey Children'S NHS FT FT No Yes - No Yes No New Contract 31/03/2016 Acute None Co-ordinating Commissoner (Associate) No No No
no e-contract or final contract guidance or tariff for 15/16
available
continued negotiations - LCCG in receipt of M8 FOT in
15/16 prices plan and working through data validaiton.
Contract value will be entered once first offer is sent
to providers. 11/03/2015 CCG_1002
REP Liverpool Women'S NHS FT FT No No - No yes no New Contract 31/03/2016 Acute None Co-ordinating Commissoner (Associate) No No No
no e-contract or final contract guidance or tariff for 15/16
available. EPAU scanning Monitor guidance
continued negotiations - LCCG in receipt of M8 FOT in
15/16 prices plan and working through data validaiton.
Contract value will be entered once first offer is sent
to providers. 11/03/2015 CCG_1003
RX7 North West Ambulance Service NHS Trust Non-FT Yes 1,026 Yes 6,183 (5,157) No Yes No New Contract 31/03/2016 Acute North West Co-ordinating Commissoner (Associate) No No No agreeing growth, activity and contract value
Advised by Blackpool CCG Weekly meetings to
progress 11/03/2015 CCG_1004
RQ6 Royal Liverpool and Broadgreen University Hospitals NHS TrustNon-FT No No - No Yes No New Contract 31/03/2016 Acute None Co-ordinating Commissoner (Associate) No No No
no e-contract or final contract guidance or tariff for 15/16
available
continued negotiations - LCCG in receipt of M8 FOT in
15/16 prices plan and working through data validaiton.
Contract value will be entered once first offer is sent
to providers. 11/03/2015 CCG_1005
RBN St Helens and Knowsley Hospitals NHS Trust Non-FT No No - No Yes No New Contract 31/03/2016 Acute North West Co-ordinating Commissoner (Associate) No No No Calculating plan with referral growth and other changes Weekly meetings to progress 11/03/2015 CCG_1006
- CCG_1007
- CCG_1008
- CCG_1009
- CCG_1010
- CCG_1011
- CCG_1012
- CCG_1013
- CCG_1014
- CCG_1015
- CCG_1016
- CCG_1017
- CCG_1018
- CCG_1019
- CCG_1020
- CCG_1021
- CCG_1022
- CCG_1023
- CCG_1024
- CCG_1025
- CCG_1026
- CCG_1027
NO VALIDATION ERRORS
Page 10 of 10

Document 33(02)04
Report to Knowsley Clinical Commissioning Group
Governing Body
Date of meeting: 5th March 2015
Report title: Financial Performance to Month 10
Report presented by: Paul Brickwood, Chief Finance Officer
Purpose of the report: This report summarises the financial performance to month 10 and identifies the key financial risks to delivery of the CCGs financial targets in respect of Programme and Running Costs.
Recommendations:
Action / Decision required
The Governing Body is recommended to:
Note the financial position to month 10.
Delegated Powers:
For decision reports only
Not applicable
Commissioning Values Which area(s) does this support? Please insert ‘x’ that apply
1. Patient centred
2. Safe
3. High quality
4. Cost effective x
5. Outcome focused
6. Closer to home
7. Affordable x
Page 1 of 12

GOVERNING BODY
FINANCIAL PERFORMANCE TO MONTH 10
Executive Summary The purpose of this report is to update the Governing Body on the financial position of the CCG to 31st January 2015, month 10.
In summary the CCG continues to report that it remains on track to deliver a 1% surplus at year end. The report identifies a number of operational budget variances, notably Acute Contracts and Prescribing which can be offset by under-spends elsewhere within the budget or met from available reserves. The forecast position is becoming increasingly more reliable as the year progresses. Recent agreements reached with key acute providers means the risk to overall delivery of the planned surplus is reduced significantly.
Page 2 of 12
1. Purpose of the report
1.1 The purpose of this report is to update the Governing Body on the financial position of the CCG to 31st January 2015, month 10.
2. Recommendations
2.1 The Governing Body is recommended to:
a) Note that subject to the latest forecasting information, the CCG remains on track to deliver a 1% surplus of £2.5 million as set out in its financial plans.
b) Acknowledge the reduction in risk associated with delivering key financial duties due to the improved reliability in forecast expenditure.
3. Background
3.1 This report is consistent with financial information submitted to NHSE for month 10 and covers the following key areas:
a) Financial Performance of Programme and Running Cost Budgets b) Reserves Position c) QIPP Performance d) Financial Risks e) Glossary of Terms
3.2 In determining the year to date and forecast out-turn position the CCG has used the latest
available financial information. For acute commissioning, month 9 data has been extrapolated to produce a forecast outturn position. Prescribing is based upon month 8 information supplied by the PPA.
4. Evidence and Consultation
4.1 The CCG has a statutory duty to ensure expenditure in a financial year does not exceed the allocated budget for both programme and running costs.
4.2 Any underspend against the running costs allowance can be used to offset financial pressures within programme spend. The CCG is not permitted to use its programme allocation to cover running cost expenditure but expenditure on clinical and quality development can be recorded as programme spend.
4.3 NHSE carries out a quarterly assurance process to ensure as a statutory organisation, Knowsley
CCG delivers the best possible services and outcomes for patients within its financial allocation. At each of the quarterly meetings to date the CCG has received assurance from NHSE that the CCG is managing its finances effectively and achieving its key financial duties.
4.4 The CCG is required to submit a monthly report to NHSE summarising the financial performance,
key risks and QIPP delivery. This report is consistent with the Non ISFE report submitted to NHSE at month 10 which will inform discussions with NHSE at the Q4 assurance meeting.
5. Proposals
5.1 There are no specific proposals requiring a decision in this report.
Page 3 of 12

6. Impact on Services to the Population
6.1 There is no direct impact on services to the population as a result of the proposals and recommendations outlined in this report. Through effective management of resources the CCG can assure the Knowsley population, NHSE and the Department of Health that it is sustainable and able to continue commissioning the best possible services and outcomes.
7. Resource Implications
7.1 Appendix 1 summarises financial performance in relation to both programme and running costs and is referenced throughout this section of the report in summarising the financial position.
7.2 NHSE requires that the CCG plans to deliver a 1% surplus (£2.5m) for 2014-15, and at
month 10 the CCG has reported that it remains on track to deliver this by year end. A total surplus of £2.1m is reported to month 10, which is line with the year to date target.
7.3 Mental Health budgets report a forecast surplus of £75k at month 10. There are no significant
issues to report which would affect the forecast out-turn position currently.
7.4 In month 9, the CCG received £111k strategic resilience funding from NHSE to invest in mental health services. Plans have been developed and submitted to NHS England which detail the schemes funded through utilisation of these non-recurrent funds. In order to provide assurance regarding implementation and delivery monthly reporting systems have been established to monitor key performance indicators linked to expected outcomes.
7.5 Acute Commissioning reports a deficit of £253k on acute commissioning to month 10 which
is forecast to £933km at year end. The most significant over-performance is within acute contracts (£709k), which is being partially offset by under-performance of £466k on acute children’s commissioning at Alder Hey.
7.6 The table below shows the year to date contract position with acute providers.
Acute Provider
Current Contract
Value £000
Contract Plan YTD
£000
Contract Actual
YTD £000
Under - /Over +
Performance YTD £000
Funded From
Activity Reserves
£000
Reported Performance
YTD £000
Aintree 29,028 24,140 25,392 1,252 917 335 Central Manchester 111 92 99 7 0 7 Liverpool Heart & Chest 1,648 1,373 1,327 -46 0 -46 Liverpool Woman's 6,071 5,063 5,493 430 50 380 Royal Liverpool Broadgreen 19,129 15,941 16,002 61 9 51 Southport & Ormskirk 1,773 1,477 1,254 -223 0 -223 St Helens & Knowsley 54,616 45,514 47,419 1,905 1,689 216 Warrington & Halton 810 675 180 -495 0 -495 Wirral 218 182 116 -66 0 -66 Wrightington & Wigan & Leigh 230 192 132 -60 0 -60 Fairfield 684 570 873 303 0 303 Oakvale 150 125 125 0 0 0 Spire 1,218 1,015 1,063 48 0 48 Non Contract Activity 81 68 327 259 0 259 Sub Total Acute 115,768 96,427 99,802 3,375 2,666 709
Page 4 of 12

Commissioning
Alder Hey 6,142 5,119 4,652 -467 0 -467
7.7 The table illustrates that in total, acute contracts are over-performing by £3.3m to month 10, which is an improvement in the comparable year to date position reported at month 8 (£3.1m). The CCG has allocated £2.6m of earmarked activity reserves to the highest over-performing contracts, bringing the overall position reported in the ledger down to £709k. Children’s Commissioning at Alder Hey continues to report under-performance against plan.
7.8 Over-performance of £1.2m is reported against the AUH due to a significant number of
emergency admissions above planned levels (actual 4,179 vs. plan 3,332). There remains a degree of uncertainty regarding the Trust’s initial proposal to block urgent care activity at month 6; therefore the financial position currently assumes the contract price will be paid under full PBR rules until a final agreement is reached. At the Aintree Collaborative Commissioning Forum (CCF) in January, co-commissioners agreed to withdraw the activity query notice issued in respect of urgent care. Instead an external review of the urgent care pathway will be commissioned to determine the impact of recent pathway changes. This will be used to inform the contracting process for 2015-16 and the recommendations will be reported via the formal contract management process.
7.9 The escalated negotiations with StHK have now concluded and an agreement has been
reached on the financial position for 2014-15. Over-performance of £1.68m will now be fixed mitigating the risk of further in year over-performance. Challenges totalling £2.6m were accepted by the provider which equated to £474k for Knowsley CCG.
7.10 Primary Care budgets report a year to date deficit of £196k to month 10, with the Prescribing over-spend (£346k) being offset by an under-spend on the Home Oxygen contract (£220k). Prescribing information used to forecast the year end out-turn is based on November data reported by the PPA. The prescribing profiles used for the forecast take in to account seasonal variation such as the anticipated increase in prescribing over the winter making the forecast reasonably reliable at this stage in the financial year.
7.11 Continuing Care reports a surplus of £347k to month 10, with a forecast under-spend of
£543k anticipated at year-end. The most significant contribution to this is an under-spend on the Pooled Budgets with the local authority (£301k). The latest forecast on the Disability Pool suggests demand growth in this area of expenditure has been lower than budgeted for which has resulted in a fortuitous under spend.
7.12 During 2014-15 the CCG had to contribute £951k to a national risk pool for Continuing
Healthcare Restitution cases which pre-date April 2013. Based on forecast expenditure Knowsley was due to get £592k of this money returned but with the instruction that the money could not be spent but had to be used to increase the 1% target underspend (or for some other CCGs reduce an overspend). It was agreed with NHSE, that rather than increase the Knowsley surplus to above 1% instead it would be used to allow St Helens CCG to get to a 1% surplus, retaining the resource within the local health economy.
7.13 Running Costs report a minor underspend of £9k to month 10 which includes the final agreed
SLA value with NWCSU plus increased expenditure on interim staff. Forecast expenditure includes an estimated £95k for potential stranded costs payable to CSU but it remains uncertain at this point if this will be required.
Page 5 of 12

8. Reserves
8.1 Appendix 2 summarises the recurrent and non-recurrent reserves position to month 10. The CCG currently holds £3.8 million in programme reserves which is net of the remaining QIPP savings to be achieved of £338K. A further £288k is held in the running costs reserve which will be used to manage the CSU stranded cost risk and any additional staffing costs. In total 55% of reserves (£2.1m) are committed for specific commissioning schemes, with the remaining £1.7m uncommitted relating to contingencies for generic activity and cost growth.
8.2 As the forecast on acute contracts and Prescribing becomes more reliable the requirement
for contingencies to offset this risk reduced. Therefore, the CCG remains confident that based on forecast expenditure there is sufficient reserves available to cover operational budget pressures and planned investments for the year at Month 10.
9. QIPP Performance
9.1 A separate QIPP report will be presented to the Governing Body outlining performance to date. Appendix 3 summarises QIPP performance to month 10 and demonstrates that year to date QIPP have been delivered in line with plan.
9.2 It should be noted that the majority of savings have been achieved through the utilisation of slippage from reserves since the savings from specialist community service contracts have not delivered to expected levels in year.
10. Human Resources
10.1 There are no Human Resource implications in this report for consideration. 11. Technology
11.1 There are no Technology implications in this report for consideration. 12. Physical Assets
12.1 There are no Physical Asset implications in this report for consideration. 13. Risk Assessment
13.1 Included at Appendix 4 is a summary of the key risks shared with NHSE at month 10. Financial risks associated with delivery of the planned surplus are deemed to be manageable from within CCG resources at this stage in the year.
13.2 Over-performance on acute contracts remains the key risk, but this has reduced significantly
due to an agreement being reached with StHK in full and final settlement of the 2014-15 position. It is highly likely that the CCGs will reach an agreement with Aintree regarding NEL activity in the coming weeks which will further reduce the risk associated with over-performance on acute contracts. There will continue to be a degree of risk until the final out-turn is known or agreed on a settlement basis with providers.
13.3 Their remains a small risk that the costs associated with premises costs recharged by NHS
Property Services (NHSPS) and Community Health Partnership (CHP) to the CCG will be higher than budget as audits to confirm the utilisation of space in NHS buildings is finalised.
Page 6 of 12

A thorough analysis of costs has been carried out in partnership with NHSPS and CHP and the residual financial risk has been assessed at less than £100k.
13.4 There is also a risk the position may worsen beyond the latest forecast in respect of
prescribing although typically the prescribing forecast becomes more reliable as the year progresses and at month 8 it is unlikely to move significantly.
14. Summary
14.1 In summary the CCG continues to report that it remains on track to deliver a 1% surplus at year end.
14.2 The report identifies a number of operational budget variances, most notably Acute Contracts
and Prescribing which will be offset by under-spends elsewhere within the budget or met from available reserves.
14.3 The forecast position is becoming increasingly more reliable as the year progresses.
Agreements reached with key acute providers means the risk to overall delivery of the planned surplus is reduced significantly.
Managerial Lead – Paul Brickwood
Signatory details: Clare Barrow, Head of Finance & Contracts [email protected], 0151 443 3361
Background Documents:
None.
Appendices:
Appendix 1 - Financial Performance of Programme and Running Cost Budgets
Appendix 2 - Reserves
Appendix 3 – QIPP
Appendix 4 – Financial Risk Appendix 5 – Glossary of Terms
Page 7 of 12

Appendix 1 Annual Budget £000
Bud YtD £000
Act YtD £000
Var YtD £000
FORECAST VARIANCE
£000
541001 MENTAL HEALTH CONTRACTS 21,909 18,257 18,284 27 20
541006 CHILD AND ADOLESCENT MENTAL HEALTH 0 -0 0 0 0
541031 MENTAL HEALTH SERVICES - ADULTS 2,116 1,742 1,699 -43 -100
541061 MENTAL HEALTH SERVICES - SPECIALIST SERVICES 100 85 90 6 4
541066 MENTAL HEALTH - WINTER RESILIANCE 111 0 0 0 0
24,237 20,084 20,073 -10 -75
541071 ACUTE COMMISSIONING 117,956 99,093 99,802 709 1,488
541076 ACUTE CHILDRENS SERVICES 6,142 5,119 4,652 -466 -568
541086 AMBULANCE SERVICES 5,586 4,655 4,656 1 4
541091 CLINICAL ASSESSMENT AND TREATMENT CENTRES 861 720 736 17 11
541106 HIGH COST DRUGS 174 145 119 -26 -24
541116 NCAS/OATS 1,130 942 961 19 23
131,849 110,672 110,925 253 933
541141 CENTRAL DRUGS 893 744 702 -43 -71
541146 COMMISSIONING SCHEMES 151 126 108 -18 -11
541151 LOCAL ENHANCED SERVICES 1,848 1,714 1,807 93 -14
541156 MEDICINES MANAGEMENT - CLINICAL 388 324 360 36 48
541161 OUT OF HOURS 724 606 606 0 0
541176 PRIMARY CARE IT 576 431 431 0 -0
541166 OXYGEN 510 424 204 -220 -234
541171 PRESCRIBING 30,499 25,412 25,758 346 341
35,589 29,781 29,976 196 57
541182 CHC ADULT FULLY FUNDED 11,270 9,550 9,417 -133 -301
541191 FUNDED NURSING CARE 1,531 1,276 1,189 -87 -101
541186 CONTINUING HEALTHCARE ASSESSMENT & SUPPORT 184 153 177 24 35
541187 CHC CHILDREN 1,304 1,087 935 -152 -176
14,289 12,066 11,719 -347 -543
541231 LONG TERM CONDITIONS 3,888 3,240 3,241 1 30
541211 COMMUNITY SERVICES 23,080 19,242 19,242 -0 0
541216 CARERS 85 71 71 0 2
541221 HOSPICES 1,103 933 926 -7 -38
541226 INTERMEDIATE CARE 623 517 545 27 78
28,780 24,003 24,024 21 72
541131 WINTER RESILIENCE 1,330 1,121 1,121 0 0
541256 COMMISSIONING - NON ACUTE 0 0 -19 -19 0
541276 NON RECURRENT PROGRAMMES 124 124 124 0 0
541291 PROGRAMME PROJECTS 377 236 238 2 115
541296 REABLEMENT 1,015 846 846 0 0
541301 RECHARGES NHS PROPERTY SERVICES LTD 4,511 3,671 3,671 0 0
541308 SAFEGUARDING 407 339 256 -83 -98
541309 NHS 111 246 205 193 -12 0
99999 I+E SET-UP DEFAULT 2,511 2,092 0 -2,092 -2,511
10,521 8,634 6,431 -2,203 -2,495
541261 COMMISSIONING RESERVE 1,694 0 0 0 -262
541281 NON RECURRENT RESERVE 2,117 0 0 0 -199
3,811 0 0 0 -4610
Programme Costs Grand Total 249,077 205,239 203,148 -2,091 -2,511
Running Costs 3,681 2,840 2,830 -9 -0
GRAND TOTAL 252,758 208,079 205,978 -2,101 -2,511
Other
Reserves
Mental Health
Acute Commissioning
Primary Care
Continuing Care
Community Health
Page 8 of 12

Appendix 2
COMMISSIONING RESERVE
Balance 2014/15
Committed
2014/15 Uncommitted
2014/15 Comments Activity Reserves:Growth 833 833RTT 58 58CEOV 0Readmissions Credit 0Maternity Pathway 0BPT 0PICU 149 149PLCP 0GP IT 0Kirkby WIC 0Mental Health Investment 0A&E Liaison 0HOC-AR 0CHC/FNC 0Primary Care £5 per head >75s 805 805GP Capacity 0Winter Resilience 0Claire House 0SEND 0AQP 0Kirkby LIFT 33 33Specialist Commissioning 0Community Nursing Redesign 0Premises Cost Pressures 0QIPP: 0CVD - Demand Management -61 -61 QIPP Target to be deliveredCOPD Demenand Management -19 -19 QIPP Target to be deliveredDiabetes - Demand Management -64 -64 QIPP Target to be deliveredLocal Priorities - ACS -58 -58 QIPP Target to be deliveredLocal Priorities - BCF -137 -137 QIPP Target to be deliveredPrimary Care Workforce Data captur 3 3Property Contigency 150 150Quality Premium 0Total 1,694 805 889
NON RECURRENT RESERVE
Balance 2014/15
Committed
2014/15 Uncommitted
2014/15 Comments 0.5% Contingency 176 176Willowbrook clinical hospice IT system 15 151% Transformational Winter Plans 187 187Community Equipment Store (CIL) 350 350Cancer Early Detection 0GP IT 240 240Primary Care Quality 07 Day Working 348 300 48Nursing Home Quality Improvements 400 400BCF Establishment 378 378 ContingencyMental Health Winter 23 23
1% Headroom
CHC Restitution 0AQUA 0
Total 2,117 1,328 789
Page 9 of 12

Appendix 3Risks & Opportunities
Risks
Potential Risk Value
Mth09Full Risk
Value£m
Probability of risk being
realised%
Potential Risk Value
£m
Proportion of Total
%
CCGsAcute SLAs 1.00 4.00 20.00% 0.80 52.29%Community SLAs 0.05 0.25 15.00% 0.04 2.45%Mental Health SLAs 0.10 0.20 30.00% 0.06 3.92%Continuing Care SLAs 0.15 0.25 25.00% 0.06 4.08%QIPP Under-Delivery 0.12 0.60 20.00% 0.12 7.84%Performance Issues 0.15 0.50 30.00% 0.15 9.80%Primary Care 0.05 0.10 50.00% 0.05 3.27%Prescribing 0.20 1.00 15.00% 0.15 9.80%Running Costs 0.00 0.00 0.00%Other Risks 0.10 0.50 20.00% 0.10 6.54%
TOTAL RISKS 1.92 7.40 1.53 100.00%Please enter the probability of succe
Mitigations
Expected Mitigation
Value Mth09
Full Mitigation
Value£m
Probability of success
of mitigating
action%
Expected Mitigation
Value£m
Proportion of Total
%
Uncommitted Funds (Excl 2% Headroom)Contingency Held 0.28 0.18 100.00% 0.18 9.74%Contract Reserves 0.70 0.94 90.00% 0.84 46.63%Investments Uncommitted 0.00 0.00 0.00%Uncommitted Funds Sub-To 0.98 1.11 1.02 56.38%Actions to ImplementFurther QIPP Extensions 0.00 0.00 0.00%Non-Recurrent Measures 0.40 0.61 100.00% 0.61 33.99%Delay/ Reduce Investment P 0.29 0.29 60.00% 0.17 9.63%Other Mitigations 0.24 0.00 0.00%Mitigations relying on pote 0.00 0.00 0.00 0.00%Actions to Implement Sub- 0.93 0.90 0.79 43.62%
TOTAL MITIGATION 1.91 2.02 1.81 100.00%
NET RISK / HEADROOM (0.01) 0.28
BEST CASE IMPACT 0.98 1.11 1.02
WORST CASE IMPACT (0.94) (6.29) (0.51)
Page 10 of 12

Appendix 4
QIPP Plan Summary TotalBalance funded from Reserves
CCG Transformational Schemes
QIPP Savings
£000 Investments
£000Net QIPP Plan £000 YTD Plan YTD Actual YTD Variance YTD Actual
Health Economy Wide QIPP:Price Efficiency Acute (5,050) (5,050) (4,208) (4,208) 0Price Efficiency Mental Health (932) (932) (777) (777) 0Price Efficiency Community (1,090) (1,090) (908) (908) 0Price Efficiency Prescribing (1,640) (1,640) (1,367) (1,367) 0TOTAL Health Economy Wide (8,712) 0 (8,712) (7,260) (7,260) 0 0Acute Services:COPD Demand Management (113) (113) (94) 23 117 (94)CVD - Demand Management (363) (363) (303) (198) 105 (303)Diabetes - Demand Management (384) (384) (320) (136) 184 (320)QIPP - ACS Diverts (348) (348) (290) (40) 250 (290)QIPP - BCF (821) (821) (684) (143) 541 (684)
(2,028) (2,028) (1,690) (493) 1,197 (1,690)
TOTAL QIPP (10,740) 0 (10,740) (8,950) (7,753) 1,197 (1,690)
Reserves Used to cover Acute Services QIPP: Mental Health Investments - Unutilised 122 AQUA - Excess Budget 13 Alternative Futures Contract Saving 87 A&E liaison - Excess Budget 1 Kirkby LIFT - Unutilised Reserve 386 Community Nursing Redesign - Unutilised Reserve 450 Contingency 356 Activity Reserves 275 TOTAL 1,690
Recurrent Plan Recurrent to Month 10
Page 11 of 12

Appendix Glossary
5BPFT 5 Boroughs Partnership Foundation Trust AHCH Alder Hey Childrens Hospital Foundation NHS Trust AQP Any Qualified Provider – DH initiative to increase patient choice by allowing all providers who meet the necessary standards to offer a specified service. BCF Better Care Fund – a joint fund with the Local Authority intended to provide better integrated care for vulnerable people in the community – helping to reduce
emergency hospital admissions. CCG Clinical Commissioning Group – made up of GP Practice Members responsible for commissioning most hospital and community services and GP prescribing
budgets. CHC Continuing Health Care – payments made by the NHS for ongoing support post hospital discharge where the patients medical condition meets certain criteria. CMCSU Cheshire and Mersey Commissioning Support Unit – it will provide certain back office support functions to CCGs across the area. COPD Chronic Obstructive Pulmonary Disease – a respiratory disease with high incidence reflecting high smoking levels. CQUINS Contract Quality Incentive Scheme – payment to providers conditional on delivery of specific quality metrics. CSR Comprehensive Spending Review – process by which the Government sets it spending plans for the next normally 3 years. DH Department of Health HRG Health Resource Groups – codification of hospital procedures and activities against which national tariffs are paid by CCGs to hospitals under PbR. IAPT Improving Access to Psychological Therapies – DH initiative to set up these services to help people with low level mental health problems and potentially
preventing more serious mental illness from developing. IR Identification Rules – software algorithm used to determine specialist from non-specialist HRG activity. JSNA Joint Strategic Needs Assessment – A document jointly produced by CCGs and Local Authorities to assess their population’s health and social care needs. LHCH Liverpool Heart & Chest NHS Foundation Trust LWH Liverpool Womens NHS Foundation Trust MCAS Musculoskeletal Assessment Service – physiotherapy triage for orthopaedic problems. MFF Market Forces Factor – an addition to national tariffs which reflects unavoidable cost differences between different areas. Each NHS Trust has its own MFF
calculated using a formula which takes account of local variances on pay and estates costs like rates. NHSE NHS England (formally the NHS Commissioning Board) which manages the NHS, holding CCGs to account as well as commissioning primary care services
(e.g. dentists and GPs) and specialised services. The local branch of NHSE is now called Cheshire & Merseyside Sub-Regional Team. PbR Payment by Results is a system by which acute hospitals get paid for patient activity on a cost per case basis from a national price list (tariff) depending on
what is done. PPA Prescription Pricing Authority – reimburses pharmacists for GP prescriptions. QIPP Quality Innovation Productivity Prevention - DH initiative to ensure that NHS will improve care and do more given the anticipated reduction in NHS funding. RLBUH Royal Liverpool and Broadgreen University Hospital NHS Trust s75 or s256 Section 75 NHS Act 2006 – legislation which allows NHS bodies to enter into partnerships with local authorities and set up joint “pooled” budgets with which
to deliver health improvement. StH&K Knowsley and Knowsley Hospitals NHS Trust SUS Secondary User Service – name of the national computer system which counts the PbR activity TDA Trust Development Agency – national body set up to oversee NHS Trust preparation to become an NHS Foundation Trust. WHHFT Warrington and Halton Hospitals Foundation Trust
Page 12 of 12
Document 33(03)05
Report to Knowsley Clinical Commissioning Group Governing Body Date of meeting: 5th March 2015
Report title: Corporate Performance Report
Report presented by: Philip Thomas, Commissioning Director & Helen Meredith, Head of Quality & Safety/Lead Nurse
Purpose of the report: The purpose of this report is to brief the Governing Body on key performance and quality issues in respect of services commissioned by the CCG.
Recommendations:
Action / Decision required
The Governing Body is recommended to:
Note the contents of the report
Delegated Powers:
For decision reports only
N/A
Justification for Part B agenda (if applicable)
N/A
Commissioning Values Which area(s) does this support? Please insert ‘x’ that apply
1. Patient centred x
2. Safe x
3. High quality x
4. Cost effective x
5. Outcome focused x
6. Closer to home
7. Affordable
[one page only]
Page 1 of 22
GOVERNING BODY
CORPORATE PERFORMANCE REPORT
Executive Summary The CCG is responsible for monitoring and assuring itself of the quality and performance of services which it commissions on behalf of the people of Knowsley, and where necessary to address these issues through the contractual arrangements that are in place for said services.
Key performance headlines can be summarised as follows:
NHS Constitution Standards – The majority of NHS Constitution Standards are being met for Knowsley. Within this, there are a number of areas where performance issues are to be noted, in particular waiting times for diagnostic tests, A&E waiting times, cancer treatment waiting times and ambulance response times.
Everyone Counts Indicators – Performance issues are noted in relation to Mixed Sex Accommodation breaches, healthcare acquired infections (HCAI), and targets for Improving Access to Psychological Therapies (IAPT).
Activity Measures – the CCG is seeing higher than planned levels of activity in both inpatient and outpatient settings, but set against this, A&E activity is less than anticipated. Reported emergency admissions rates are up on the same period last year, but with the caveat that there have been changes in recording of activity, such that overall underlying emergency admission rate is broadly comparable to last year.
Corporate Key Performance Indicators (KPIs) – Sickness absence remains better than average for NHS organisations, and significant progress has been made with statutory and mandatory training compliance.
Page 2 of 22

1. Purpose of the briefing 1.1 The purpose of this report is to brief the Governing Body on key performance and quality
issues in respect of services commissioned by the CCG. 2. Background 2.1 The CCG is responsible for monitoring and assuring itself of the quality and performance of
services which it commissions on behalf of the people of Knowsley, and where necessary to address these issues through the contractual arrangements that are in place for said services.
2.2 The CCG monitors its performance via a range of key performance and outcome indicators, which can broadly be defined as follows:
a) NHS Constitution Standards – The NHS Constitution sets out a range of pledges that the NHS is committed to achieve in order to provide comprehensive high quality services. These are monitored at a CCG level in terms of how well the local healthcare system delivers certain access and waiting time standards, such as referral to treatment waiting times for consultant led services, and A&E waiting times.
b) Everyone Counts Indicators – The planning guidance for the current financial year also set out a number of additional measures including targets to minimise healthcare acquired infections (HCAI), and targets for Improving Access to Psychological Therapies (IAPT) and patient experience indicators such as the Friends and Family test (FFT).
c) Activity Measures – the CCG sets indicative plans for the levels of hospital activity that it expects over the course of the year, and also monitors trends on emergency admissions and readmissions.
d) NHS Outcomes Framework – this framework supports the NHS Mandate, which is the document through which the government provides direction and ambitions for the NHS each year. These outcomes are predominantly published on an annual basis, and updates on this are brought to the Governing Body periodically. The latest update on these outcomes was reported at December 2014 Governing Body.
e) Corporate Key Performance Indicators (KPIs) – Additionally the CCG monitors a range of corporate indicators relating to workforce such as sickness absence and training and compliance with other statutory requirements such as the Freedom of Information Act.
2.3 This briefing addresses current performance against each of these areas by exception.
3. Key Issues 3.1 NHS Constitution Standards
The majority of NHS Constitution Standards are being met for Knowsley. Within this, there are a number of areas where performance issues are to be noted:
3.1.1 Diagnostic Test Waiting Times: In December, the target for 99% of patients to wait no more than 6 weeks for diagnostic tests was breached. Performance for December was 98.9%. This poor performance can be attributed to increasing pressure on urgent care and
Page 3 of 22
additional activity undertaken to deliver improved referral to treatment (RTT) performance which resulted in increased waits for diagnostic elements of pathway. There were 27 breaches of the standard in December, primarily within echocardiography and endoscopy although it is noted that the vast majority of patients waiting more than 6 weeks were seen within the 6-7 week wait bands. The CCG remains on target to achieve the required standard for 2015/16 with year to date performance at 99.6%. Monthly performance at all providers is expected to be recovered to required standard by end of February 2015.
3.1.2 A&E Waiting Times: Whilst the national standard is being met overall for Knowsley registered patients in the year to date (95.99%), for the month of December the standard was not achieved for Knowsley patients, with achievement against the standard at 93.5%. On a provider basis for December AUH was at 86.87%), St Helens & Knowsley was at 91.4% and The Royal Liverpool & Broadgreen University Hospitals was at 88.76%. The CCG continues to engage on performance through the System Resilience Group (SRG) and contract meetings and has put in place a range of measures over the winter period to improve access to primary care so that people are less likely to make unnecessary visits to A&E. The CCG is also working closely with Local Authority colleagues to facilitate safe and timely discharge from hospital – improving flow and releasing capacity.
3.1.3 Cancer Waiting Times: The CCG achieved 5 of the 9 cancer targets and the majority of year to date positions continue to improve. Patient choice and clinical complexity are the main contributor to the breaches of the 62 day wait target. For example, in December there were 8 breaches out of 27 cases 2 of which were patient choice, 3 were due to clinical complexity and the other 3 were due to intra-provider referral delays. The CCG also failed the 31 day standard for subsequent cancer treatments (radiotherapy, target of 94%) with 90% but are achieving year to date with 97.8% For December there were 2 breaches out of a total of 20 patients one of which was patient choice the other was due to clinical complexity. The CCG is working with providers and the CSU to ensure that Root Cause Analysis of all 62 day breaches is undertaken with oversight of key actions via the CCG’s own Serious Incident review group. The CCG, along with partner CCG’s and providers from across Cheshire and Merseyside, attended a single item Quality Surveillance Group meeting in relation to 62 day cancer breaches on 17 February 2015. The agreed action arising from this meeting is that the Merseyside & Cheshire Strategic Clinical Network for Cancer will establish a project group to review and develop pathways of care in line with best practice with a view to reducing variation in access to diagnostics which has been identified as a crucial component in achieving the 62 day standard.
3.1.4 Ambulance Response Times: Performance against all Category A emergency response
times deteriorated in December 2014, with the in month figures for December below the mandated standard for both the Red 1 and Red 2 8 minute standard, and the 19 minute standard. For the most urgent type of calls (Cat A Red 1 8 minutes), only 57.1% of calls were within the standard, the lowest performance year to date. Activity as reported by North West Ambulance Service (NWAS) for December 2014 was 9.3% up on the same period in 2013, with NWAS reporting unprecedented levels of activity overall across the region. A particular issue for NWAS is pressures in A&E departments resulting in ambulances turnaround being delayed. The CCG held a multi-agency workshop on 14 Jan 2015 to examine NWAS performance and system issues affecting that performance. The CCG is now co-ordinating the development and implementation of actions intended to reduce NWAS activity and release capacity through improved turnaround times.
Page 4 of 22
3.2 Everyone Counts Indicators
3.2.1 Mixed Sex Accommodation Breaches: there were two breaches in December at STHK, bringing the year to date total breaches up to five.
3.2.2 Stroke Care: the proportion of stroke patients spending at least 90% of their time on a
stroke unit has been maintained at or above the required standard since September 2014, and significant improvement has been observed at STHK. Year to date performance for the CCG is still short of the 80% standard, at 79.6% but is forecast to achieve the required standard for 2014/15 should current levels of performance be maintained during quarter 4.
3.2.3 Healthcare Acquired Infections: No further cases of MRSA Methicillin-resistant
staphylococcus aureus (MRSA) were reported in December. There have been 5 cases year to date in Knowsley, 2 were community acquired and 3 acute hospital acquired. Clostridium difficile (C diff) performance as at December shows 44 cases against a year to date maximum threshold of 42. The majority of C diff cases are community acquired. Post Infection Reviews (PIR) and Root Cause Analysis (RCA) are being undertaken and followed up through the CCGs quality function. The CCG is engaged with the Mid Mersey HCAI Collaborative Group which reports to providers and commissioners on the development, implementation and monitoring of all areas of HCAI prevention, screening and management. Additionally, a newly formed Health Care Acquired Infections Collaborative has been set up as a sub group of the Clinical Quality Committee and has responsibility for overseeing the implementation of the revised action plan for C difficile and incorporating these into a broader HCAI work plan for the group. The group will meet monthly and is chaired by the Clinical Lead for Primary Care Quality.
3.2.4 Improving Access to Psychological Therapies (IAPT): IAPT services continue to be a national NHS priority for service delivery with prescribed national targets and close scrutiny from NHSE. The CCG is closely monitoring performance at 5 Boroughs Partnership (5BP). The Trust submitted a recovery plan on 10 December 2014, setting out actions to improve performance which addresses: waiting times; DNAs (local targets); recovery rate and prevalence rates (national targets). Highlight reports for the recovery plan are being submitted on a weekly basis and performance management meetings are taking place monthly. Whilst the standard was still not achieved in the third quarter of 2014/15, with 3.58% prevalence against a target of 3.75% for the quarter, this was nonetheless a significant improvement on performance in the first half of the year. 5BP have given an undertaking to the CCG that the improvement actions detailed in the recovery plan will ensure that the Quarter 4 target (3.75%) will be achieved. January performance figures show that 5BP is on track to achieve the national prevalence rate target but not the national recovery rate target by end of this financial year. As the delivery of these and other local targets are reliant on 5BPs ability to recruit, train and supervise IAPT practitioners the CCG has requested a workforce plan from 5BP showing how they will improve and sustain performance into next year.
3.3 Activity Measures 3.3.1 Monthly Activity Return (MAR)
As at December 2014 for all first outpatient attendances (General & Acute specialties, G&A) the CCG is over the year to date plan of 37,276 by 3,853 attendances (10% over plan) with December monthly activity being over plan by 554 attendances. This is 15% over the in-month plan and significantly above plan.
Page 5 of 22

The total number of non-elective episodes (G&A) at December 2014 the CCG is over the plan of 15,726 by 1137 admissions (7% over plan). December in month activity is over plan by 133 attendances. This is 8% over the in-month plan. For the total number of elective episodes, day case at December 2014 the CCG is over the plan of 13,541 by 691 admissions (5% over plan). December in month activity is over plan by 106 attendances. This is 8% over the in-month plan. In relation to A&E activity it is notable that despite the pressures and performance issues referred to above in section 3.1.2, the level of activity for both Type 1 (the more acute) A&E attendances and for all types is lower than was planned for in 2015/16. This indicates that A&E pressures are not driven by increased demand from Knowsley patients, and suggests that measures to manage demand that are being taken by the CCG and across Knowsley are effective.
3.3.2 Emergency admissions
At the end of December the cumulative total for the CCG emergency admissions (composite) is 3380 compared to 3143 for the same period 2013/14. In December there were 338 emergency admissions compared to the 412 reported in November. Further analysis of the emergency admissions shows clearly that the 14/15 increase is predominantly because of an increase at Aintree – the provider breakdown table shows Aintree accounts for about a third of all emergency admissions and emergency admissions have increased 26% compared to last year. The CCG position has increased by 237 admissions since last year, while AUH has seen an increase of 261 for the same period primarily due to changes in recording of activity as reported at previous Governing Body meeting. The implication of this is that the underlying rate of emergency admissions is similar to in 2013/14.
3.3.3 Readmissions
At the end of December the cumulative rate for emergency admissions within 30 days of discharge is 16.58% which is a marginal increase on the same point 13/14. In December 2014 there were 295 readmissions of the 2116 eligible patients; the figure is less than the 371 readmissions in November. Splitting down emergency readmission by provider shows that this reflects the readmission rates at St Helens & Knowsley and Aintree, which are both above 18%.
3.4 Corporate Performance Measures
3.4.1 Workforce Overview: At the end of December 2014 there were 46 (headcount) CCG employees (51 if including lay members) and a whole time equivalent of 43.2. There was one vacancy within the governance directorate relating to the post of Head of Quality & Safety/Lead Nurse which has now been filled. Within the commissioning directorate, the Head of Contracting remains vacant and within Primary Care Support there is a vacancy for a Senior Clinical Pharmacist, which is currently covered on an interim basis.
3.4.2 Sickness Absence: The sickness absence rate for December was 1.07%, which was a
0.06% decrease on the previous month. The rolling sickness absence rate was 3.27%, which remains below the national average.
Page 6 of 22

3.4.3 Statutory and Mandatory Training Compliance: There has been significant improvement in compliance against all areas of the statutory and mandatory training framework, with all modules above the 85% national standard. Managers are issued with reports on the completion of training by their line managed staff to ensure that this is followed up, and staff reminders are sent out as annual certification expires. There will continue to be a focus in the final quarter on information governance training to ensure that the IG toolkit requirements are met.
3.4.4 Freedom of Information Act Compliance (FOI): As at the time of completion of this
report, 168 FOI requests have been received, of which 16 are currently open and within the 20 day response time standard. Year to date there has only been one breach against the 20 day response time standard.
4. Summary 4.1 In summary, overall performance is robust in most areas in relation to the commissioned
services accessed by the people Knowsley, but within this there are key areas where performance is below the required standard, and CCG action is on-going to address these areas.
Managerial Lead – Andrew Thomas, Governance Director & Philip Thomas, Commissioning Director
Signatory details: Andrew Thomas, [email protected], 0151 244 3109
Background Documents:
None.
Appendices:
Appendix 1 – Corporate Performance Dashboard
Page 7 of 22

Corporate Performance Dashboard
Governing Body
Thursday 5th March
Appendix 1
Page 8 of 22

NHS CONSTITUTION STANDARDS
Section 1
2 Page 9 of 22
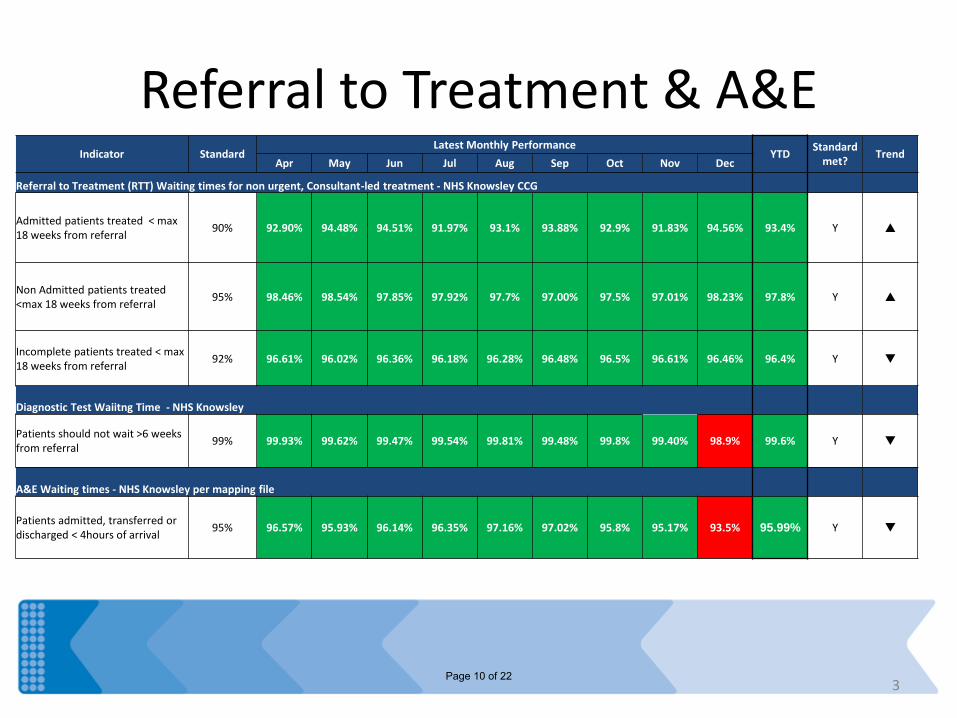
Referral to Treatment & A&E
3
Indicator Standard Latest Monthly Performance
YTD Standard
met? Trend
Apr May Jun Jul Aug Sep Oct Nov Dec
Referral to Treatment (RTT) Waiting times for non urgent, Consultant-led treatment - NHS Knowsley CCG
Admitted patients treated < max 18 weeks from referral
90% 92.90% 94.48% 94.51% 91.97% 93.1% 93.88% 92.9% 91.83% 94.56% 93.4% Y p
Non Admitted patients treated <max 18 weeks from referral
95% 98.46% 98.54% 97.85% 97.92% 97.7% 97.00% 97.5% 97.01% 98.23% 97.8% Y p
Incomplete patients treated < max 18 weeks from referral
92% 96.61% 96.02% 96.36% 96.18% 96.28% 96.48% 96.5% 96.61% 96.46% 96.4% Y q
Diagnostic Test Waiitng Time - NHS Knowsley
Patients should not wait >6 weeks from referral
99% 99.93% 99.62% 99.47% 99.54% 99.81% 99.48% 99.8% 99.40% 98.9% 99.6% Y q
A&E Waiting times - NHS Knowsley per mapping file
Patients admitted, transferred or discharged < 4hours of arrival
95% 96.57% 95.93% 96.14% 96.35% 97.16% 97.02% 95.8% 95.17% 93.5% 95.99% Y q
Page 10 of 22

Cancer Treatment Waiting Times
4
Indicator Standard Latest Monthly Performance
YTD Standard
met? Trend
Apr May Jun Jul Aug Sep Oct Nov Dec
Cancer Waiting Times - maximum 2 week (14days) waits for first outpatient appointment for all patients referred urgently - NHS Knowsley
Patients referred by a GP with suspected cancer 93%
93.7% 94.6% 96.5% 93.5% 92.3% 91.3% 92.4% 93.7% 95.0% 93.5% Y p
Breast symptom patients ( where cancer not initially suspected) 93%
93.4% 94.2% 95.7% 94.2% 94.4% 91.9% 97.8% 95.4% 94.8% 94.8% Y q
Cancer Waiting Times - maximum 1 month (31 days) waits from diagnosis to first or subsequent treatment - NHS Knowsley
From diagnosis to first definitive treatment, all cancers 96%
98.6% 98.4% 97.4% 97.7% 96.3% 97.7% 100.0% 96.9% 100.0% 98.1% Y p
Subsequent treatments where that treatment is surgery 94%
94.1% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 92.3% 100.0% 98.1% Y p
Subsequent treatments where treatment is an anti-cancer drug 98%
100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% Y tu
Subsequent treatments where treatment is radiotherapy 94%
100.0% 100.0% 96.3% 96.5% 100.0% 100.0% 100.0% 94.1% 90.0% 97.8% Y q
Cancer Waiting Times - maximum 2 month (62 days) waits from referral to first definitive treatment for all cancers - NHS Knowsley
For urgent GP referrals for cancer 85% 88.9% 82.7% 83.3% 78.5% 79.2% 96.0% 86.8% 80.0% 70.4% 82.9% N q
For referrals from an NHS screening service
90% 100.0% 83.3% 100.0% 60.0% 66.7% 100.0% 100.0% 100.0% 100.0% 84.6% N tu
Folowing Consultant decision to upgrade patient priority
85% 50.0% 100.0% 0.0% 100.0% 83.3% 75.0% 100.0% 100.0% 100.0% 84.4% N tu
Page 11 of 22

Ambulance Response Times
5
Indicator Organisation Standard Latest Monthly Performance
YTD Standard
met? Trend
Apr May Jun Jul Aug Sep Oct Nov Dec
Category A Ambulance Calls - NWAS provider Level and NHS Knowsley
Cat A emergency responses arriving <8 minutes (Red1)
NWAS
75%
75.7% 73.4% 71.5% 68.5% 72.7% 71.5% 71.3% 68.0% 59.0% 69.8% N q
CCG 72.7% 71.4% 73.0% 78.2% 81.6% 80.0% 74.4% 64.2% 57.1% 71.1% N q
Cat A emergency responses arriving <8 minutes (Red2)
NWAS
75%
75.3% 74.7% 73.2% 69.2% 72.1% 73.3% 73.6% 69.6% 58.5% 70.7% N q
CCG 78.2% 81.2% 74.3% 73.9% 74.3% 74.3% 73.1% 71.7% 62.9% 73.5% N q
Cat A ambulance arriving at scene within 19 minutes
NWAS
95%
96.2% 95.6% 95.4% 94.2% 95.3% 95.1% 93.6% 93.1% 87.7% 93.8% N q
CCG 96.8% 96.0% 97.5% 95.3% 97.8% 95.8% 95.3% 94.4% 91.9% 95.5% Y q
Page 12 of 22

EVERYONE COUNTS
Section 2
6 Page 13 of 22

7
Supporting Measures Indicator Standard
Latest Monthly Performance YTD
Standard met?
Trend Apr May Jun Jul Aug Sep Oct Nov Dec
Everyone Counts - Annex B Supporting Measures
Mixed Sex Accommodation (MSA) breaches: NHS Knowsley
Minimise breaches 0 0 0 0 1 0 1 1 0 2 5 N p
Mental Health Care Programme approach (CPA) - NHS Knowsley
The % of adults on CPA, followed up <7days of discharge
95% 96.1% 100.0% 97.1% 100.0% 100.0% 100.0% 100.0% Y tu
Everyone Counts - Annex C Measures
Stroke
% of stroke patients spending at least 90% of their time on a stroke unit
80% 76.9% 50.0% 72.0% 87.5% 76.2% 94.0% 94.0% 80.0% 87.9% 79.6% N p
% high risk TIA patients assessed and treated within 24hrs
60% 75.0% 100.0% 100.0% 100.0% n/a 100.0% 100.0% 100.0% 100.0% 97.7% Y tu
Page 14 of 22
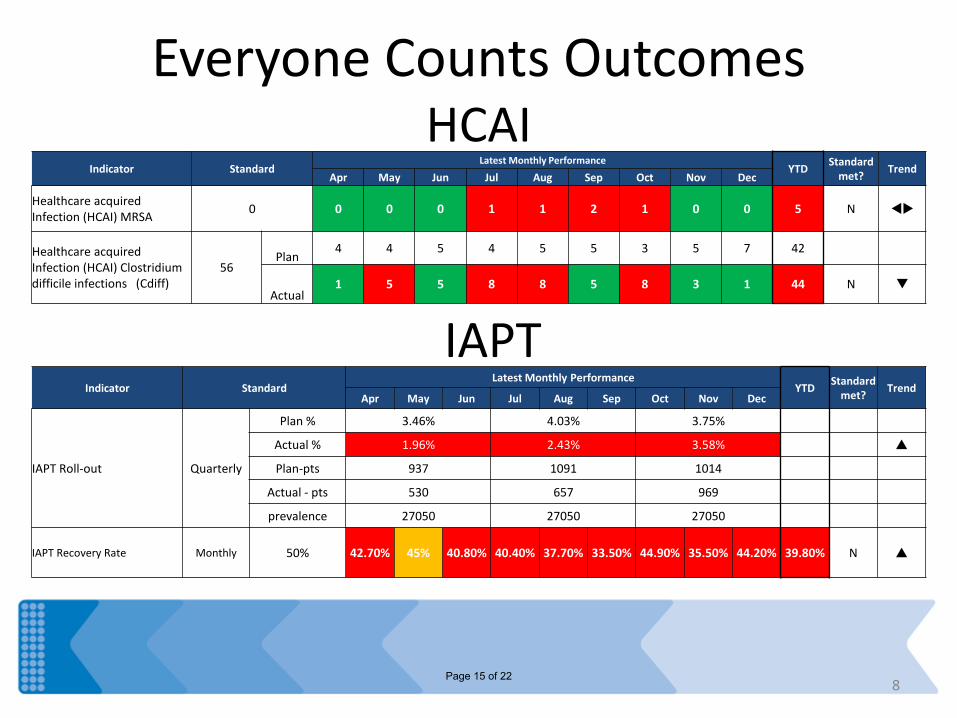
Everyone Counts Outcomes HCAI
8
Indicator Standard Latest Monthly Performance
YTD Standard
met? Trend
Apr May Jun Jul Aug Sep Oct Nov Dec
Healthcare acquired Infection (HCAI) MRSA
0 0 0 0 1 1 2 1 0 0 5 N tu
Healthcare acquired Infection (HCAI) Clostridium difficile infections (Cdiff)
56 Plan
4 4 5 4 5 5 3 5 7 42
Actual 1 5 5 8 8 5 8 3 1 44 N q
IAPT Indicator Standard
Latest Monthly Performance YTD
Standard met?
Trend Apr May Jun Jul Aug Sep Oct Nov Dec
IAPT Roll-out Quarterly
Plan % 3.46% 4.03% 3.75%
Actual % 1.96% 2.43% 3.58% p
Plan-pts 937 1091 1014
Actual - pts 530 657 969
prevalence 27050 27050 27050
IAPT Recovery Rate Monthly 50% 42.70% 45% 40.80% 40.40% 37.70% 33.50% 44.90% 35.50% 44.20% 39.80% N p
Page 15 of 22

Friends & Family Test Response rates (target 15%)
9
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
Provider Inpatients Responses (Avg from main providers)
0.0%
10.0%
20.0%
30.0%
40.0%
Provider AED Responses (Avg from main providers)
Inpatients Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Average
Aintree University Foundation Trust Hospitals REM 43.5% 45.4% 39.9% 50.0% 39.9% 41.5% 38.5% 39.4% 38.1% 41.8%
Liverpool Womens Foundation Trust Hospitals REP 25.7% 19.5% 26.3% 28.0% 56.9% 39.2% 43.0% 59.5% 43.2% 37.9%
Royal Liverpool and Broadgreen University Hospitals RQ6 24.3% 16.1% 33.8% 26.4% 27.6% 28.0% 25.8% 24.9% 24.1% 25.7%
St Helens & Knowsley Hospitals trust RBN 33.8% 30.6% 36.8% 40.4% 33.9% 28.8% 26.5% 25.1% 26.7% 31.4%
31.8% 27.9% 34.2% 36.2% 39.6% 34.4% 33.5% 37.2% 33.0% 34.2%
Accident & Emergency Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Average
Aintree University Foundation Trust Hospitals REM 23.5% 25.0% 24.2% 24.1% 22.2% 22.6% 23.7% 22.1% 22.9% 23.4%
Liverpool Womens Foundation Trust Hospitals REP 25.8% 27.4% 24.4% 47.4% 39.2% 29.4% 40.1% 31.2% 35.6% 33.4%
Royal Liverpool and Broadgreen University Hospitals RQ6 10.6% 5.0% 36.3% 22.5% 23.4% 17.8% 16.5% 16.2% 14.7% 18.1% St Helens & Knowsley Hospitals trust RBN 9.4% 14.8% 26.8% 27.8% 24.4% 17.1% 19.2% 11.0% 5.1% 17.3%
17.3% 18.0% 27.9% 30.4% 27.3% 21.7% 24.9% 20.1% 19.6% 23.0%
Page 16 of 22

Activity
10
G R
Below previous years activity
Over previous years activity
2014-15 YTD
Emergency Readmissions within 30 days (%)*
13-14 16.32%
Actual 16.58%
Composite measure on Emergency Admissions*
13-14 3143
Actual 3380
Emergency admissions for ACS conditions
13-14 1323
Actual 1392
Emergency admissions for Asthma, Diabetes and Epilepsy
<19's
13-14 113
Actual 127
Emergency admissions for Acute conditions not usually requiring hospital admission
13-14 1651
Actual 1902
Emergency Admission for children with LRTI
13-14 133
Actual 97
Planned activity variance Emergency admissions
*Further analysis of this on following page
2014-15 YTD Variance
Inpatient
Total G&A Elective FFCE's Plan 16645
Actual 17292 3.89%
Number of Non-Elective FFCE's
Plan 15726
Actual 16863 7.23%
A&E
Type 1 A&E Attendances Plan 46519
Actual 45232 -2.77%
All A&E Attendances Plan 95848
Actual 83292 -13.10%
Outpatient
Total Number of first referrals made
Plan 42724
Actual 45010 5.35%
First Outpatient attendances following GP referral
Plan 23684
Actual 23424 -1.10%
Number of First Outpatient Attendances ( all referral sources)
Plan 37276
Actual 41129 10.34%
Page 17 of 22

11
Emergency admissions & readmissions
YTD Difference as a %
Composite measure on Emergency Admissions 3380 237 7.01%
Baseline - 13/14 3143
Provider breakdown
Whiston - 14/15 1904 -2 -0.11% 13/14 1906
Aintree - 14/15 982 261 26.58%
13/14 721
RLBUH - 14/15 208 -11 -5.29% 13/14 219
Alder Hey - 14/15 124 -53 -42.74%
13/14 177
Other - 14/15 162 42 25.93% 13/14 120
YTD
Emergency Readmissions within 30 days (%)
16.58%
% - 13/14 16.32%
Provider breakdown
Whiston % - 14/15 18.43%
Aintree % - 14/15 20.74%
RLBUH % - 14/15 9.30%
Alder Hey % - 14/15 12.24%
Other % - 14/15 10.63%
Page 18 of 22
HUMAN RESOURCES
Section 3
12 Page 19 of 22

Human Resources Workforce Overview – Dec 14 Sickness Absence - Dec 14
13
0.2%
1.1%
4.5% 4.6%
3.5%
1.9%
5.85%
5.24%
4.31%
3.49%
2.4%
1.1% 1%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
Dec-13 Feb-14 Apr-14 Jun-14 Aug-14 Oct-14 Dec-14
Total Sick Days/Total WTE Days in month NHS Average CCG Average
4
8
9
10
15
4.0
7.6
8.8 8.8
14.0
0 0 0 0 0 0
2
4
6
8
10
12
14
16
Exe
cuti
ve/S
ecr
eta
riat
Go
vern
ance
Clin
ical
Co
mm
issi
on
ing
Pri
mar
y C
are
Fin
ance
Te
am
Staff Employment
No of Employees WTE Fixed term vacancies
Page 20 of 22

Human Resources Mandatory Training – Feb 2014 Update
14
• At the end of December 2014 there were 50 (headcount) CCG employees/ as a whole time equivalent of 43.79. There is one vacancy within the Governance Directorate relating to the post of Head of Quality & Safety/Lead Nurse (currently covered on an interim basis), one as a Head of Contracting within Commissioning, and a Senior Clinical Pharmacist within Primary Care Support (also currently covered on an interim basis).
• The sickness absence rate for December was 1.07%, which was a 0.06% decrease on the previous month. The rolling sickness absence rate was 3.27%, which was a small increase of 0.09% over the previous period. These figures remain below the national average. (Reports on mandatory training indicate improvements across all areas since this was previously reported, and compliance above the 85% national target. Managers are issued with reports on the completion of training by their line managed staff to ensure that this is followed up, and staff reminders are sent out as annual certification expires. There will continue to be a focus in the final quarter on information governance training to ensure that the IG toolkit requirements are met. 48
49
45
45
45
47
49
51
3
2
6
6
6
4
2
0
0 10 20 30 40 50
Counter Fraud
Equality & Diversity
Fire Safety
Health & Safety Awareness
Infection Control
Information Governance
Safeguarding Adults - Level 1
Safeguarding Children Level 1
Completed
ToComplete
Page 21 of 22

Governance – FOI compliance
15
15 16 16
10 10
20 21
14 16
10
3
4
12
1
0
10
20
Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15
Knowsley CCG - Breached Vs Closed on Time Apr 14 - Nov 14
Breached Open Closed on Time
Page 22 of 22

Document 33(03)06
Report to Knowsley Clinical Commissioning Group Governing Body Date of meeting: 5th March 2015
Report title: Governing Body Assurance Framework
Report presented by: Dawn Boyer, Head of Corporate Services
Purpose of the report: To present the Quarter 3 review of the 2014/15 Governing Body Assurance Framework for review.
Recommendations:
Action / Decision required
The Governing Body is recommended to review the quarter 3 Governing Body Assurance Framework summary appended to this report and note the progress and key actions being taken to address gaps in controls and assurance.
Delegated Powers: For decision reports only
Constitution – Appendix D 7.03
Justification for Part B agenda N/A
Commissioning Values Which area(s) does this support? Please insert ‘x’ that apply
1. Patient centred X
2. Safe X
3. High quality X
4. Cost effective X
5. Outcome focused X
6. Closer to home
7. Affordable X
Page 1 of 11

GOVERNING BODY
GOVERNING BODY ASSURANCE FRAMEWORK
Executive Summary The Governing Body Assurance Framework identifies and quantifies the principal risks to the delivery of the organisation’s goals, the key controls and provides assurance that those controls are operating effectively, or identifies corrective action where required. The report includes both the national and local assurance frameworks and presents the quarter 1 position in respect of the national framework and the quarter 3 position in respect of the local framework for review by the Governing Body. NHS England has confirmed an outcome of assured for quarter 1 in respect of the national CCG assurance framework. Domain 3 (Are CCG plans delivering better outcomes for patients) is the only domain which is assured with support. This is consistent across Merseyside due to the challenges commissioners are currently facing and the risk within the system. At the time of writing the report while the quarter 2 meeting had been held formal feedback from NHS England had yet to be received. The Governing Body Assurance Framework is framed around the CCG’s 3 goals and 9 key objectives. The report identifies 5 high risk areas with the associated controls and assurance ratings. In one case assurance is currently limited, in respect of gaps or delays in the availability and quality of data, information and intelligence. This is a priority for action in the current quarter including appraising alternative options for business intelligence service provision.
Page 2 of 11

1. Purpose of the report 1.1 The purpose of the report is to present the quarterly review of the Governing Body
Assurance Framework for review. 2. Recommendations 2.1 The Governing Body is recommended to review the quarter 3 Governing Body
Assurance Framework summary appended to this report and note the progress and key actions being taken to address gaps in controls and assurance.
3. Background 3.1 The CCG’s Risk Management Strategy sets out the process for identifying,
analysing, evaluating, treating, monitoring and reviewing risks. Key to this is: a) The Governing Body Assurance Framework which identifies and quantifies the
principal risks to the delivery of the organisation’s goals, the key controls and provides assurance that those controls are operating effectively, or identifies corrective action where required.
b) The Corporate Risk Register which provides a summary of the principal risks facing the organisation, together with the actions needed and being taken to reduce these risks to an acceptable level.
3.2 The goals and objectives around which the 2014/15 Governing Body Assurance
Framework has been developed were approved by the Governing Body at its meeting in August.
3.3 The CCG has engaged PwC to undertake work to support the development of the
CCG’s risk management arrangements and this includes 3 phases as follows:
a) Phase 1 – Strategic approach to risk management; b) Phase 2 – Embedding risk management c) Phase 3 – Skills transfer
3.4 Phase 1 is completed and has included two Governing Body Development Sessions focussing on the CCG’s current and aspirational risk maturity and on developing risk appetite. The outputs from this phase include an updated risk management strategy incorporating risk appetite statements which appears elsewhere on this agenda for approval.
4. Governing Body Assurance Framework 4.1 The Governing Body Assurance Framework is structured around the CCG’s key
goals and objectives. These have been reviewed and updated for 2014/15 to reflect the CCG’s strategic plans and feedback from Merseyside Internal Audit Agency (MIAA) arising from their review of and opinion on the 2013/14 Assurance Framework. These still broadly align with the domains in the NHS England CCG Assurance Framework.
4.2 The National CCG Assurance Framework is the mechanism by which NHS England
assures itself that CCGs are delivering the full range of outcomes and standards, both national and local, for its population. This is achieved through quarterly
Page 3 of 11
checkpoint assessments based on a range of performance indicators. The outcome of this is an assessment of assured, assured with support, or not assured intervention required against each of the 6 domains based on the level of risk associated with the CCGs current plans and progress.
4.3 The Local Governing Body Assurance Framework focuses on the local plans and
priorities for the current year to maintain and improve delivery against the outcomes and standards, and is the mechanism by which the Governing Body assures itself that risks to the achievement of these are being appropriately managed. It does this by identifying the principal risks to the achievement of these objectives, the risk rating, key controls, and what assurances are planned or in place to demonstrate that the key controls are effective. Where a gap in either control or assurance is identified this, together with the corrective action and responsible person, is also included.
4.4 An overall assurance rating of significant, reasonable or limited assurance is
provided for each risk, based on the number and strength of key positive assurances which are actually in place. Where this is significant or reasonable this provides assurance to the Governing Body that the risks are being effectively managed. Where the assurance rating is limited this indicates that further attention and action is required. As the year progresses and corrective action is completed the governing body can expect the levels of assurance to increase.
4.5 The outcome of the first quarter National CCG Assurance Framework checkpoint
conversation for 2014/15 indicated that the CCG is assured for quarter 1. Domain 3 (Are CCG plans delivering better outcomes for patients) is the only domain which is assured with support. This is consistent across Merseyside due to the challenges commissioners are currently facing and the risk within the system. The second quarter National CCG Assurance Framework checkpoint conversation for 2014/15 has taken place but the outcome has yet to be confirmed in writing.
Appendix A demonstrates how the national domains map across to the goals in the local assurance framework. This indicates that the Governing Body can take reasonable assurance that the risks to the achievement of local plans and priorities, aimed at maintaining and improving performance in each domain, are being appropriately managed.
4.6 A Governing Body assurance rating summary for quarter 3 is provided at Appendix
B. This is supported by a detailed assurance framework, which sets out the key controls, planned and actual assurances, gaps and proposed corrective action. It is the role of the Audit Committee to scrutinise this detailed Assurance Framework and provide assurance to the Governing Body through submission of minutes and key issues. An Audit Committee meeting is planned for later this month.
4.7 The most significant risks identified to the achievement of the CCG’s objectives are:
a) Failure to manage demand results in failure to meet key constitutional rights e.g.
accident and emergency, referral to treatment, which may result in patient harm and reputational risk. This risk is rated as high, but the assurance rating indicates that the Governing Body can take reasonable assurance that this is being effectively managed, through the CCG’s membership of system resilience groups, the winter plan and contract monitoring processes.
Page 4 of 11

b) Failure to manage the complex provider landscape may affect quality and performance. This risk is rated as high, but the assurance rating indicates that the Governing Body can take reasonable assurance that this is being effectively managed, through Quality Boards and Quality Surveillance Groups, clinical leadership, collaborative and lead commissioning arrangements, and commissioning support and safeguarding services.
c) Uncertainty over future NHS funding or other policy prevents the CCG from delivering local commissioning plans and still achieving financial targets. This risk is rated as high, but the assurance rating indicates that the Governing Body can take reasonable assurance that this is being effectively managed, through the CCG’s 5 year financial strategy.
d) Ineffective governance of services commissioned by the CCG will lead to patient harm, reputational damage or financial loss. This risk is rated as high, but the assurance rating indicates that the Governing Body can take reasonable assurance that this is being effectively managed, through its Clinical Quality and Safety and Finance and Performance Committees and membership of local safeguarding boards.
e) Gaps or delays in availability and quality of data, information and intelligence
reduce effective performance management. This risk is rated as high and the assurance rating is currently limited due to issues in the Commissioning Support Business Intelligence function including delays and omissions reporting key performance issues e.g. cancer waits and failing to deliver a holistic view of the performance of commissioned services combining performance information with intelligence from contract management and quality and safety activities. Additional in house capacity has been recruited to maintain business continuity. However it has been identified that the CCG doesn’t have sufficient in house capacity to undertake a review and specification of data, information and intelligence required and therefore external support is being sought to complete this complex task. A robust service specification will provide a baseline against which both in house and external commissioning options can be appraised.
4.8 The assurance rating for the remaining risks is either reasonable or significant. 4.9 The current status for key actions identified within the assurance framework is as
follows:
Action Identified Status Further develop the communication and engagement plan in support of the CCG’s commissioning priorities
In progress
Annual review of effectiveness of Governing Body and Audit Committee
Planned
Submission and audit of information governance toolkit In progress Complete Annual Governance Statement In progress Secure interim capacity and complete specification for business intelligence service provision
In progress
Fully implement PDR In progress
Page 5 of 11

5. Resource Implications 5.1 Financial
There are no financial implications as a direct result of the proposals in this report. 5.2 Human
There are no additional human resources implications. 5.3 Information Technology
There are no additional information technology implications. 5.4 Physical Assets
There are no additional physical asset implications.
6. Risk Assessment 6.1 The Assurance Framework identifies and quantifies the principal risks to the CCG
and delivery of the goals and strategic objectives for 2014/15. The most significant risks are highlighted in the report above.
7. Impact of population groups
(Including children, vulnerable adults, black and minority ethnic groups, disabled people, men, women and transsexuals)
7.1 The Governing Body assurance framework is a key element of the Risk
Management Strategy, supporting the CCG’s arrangements for quality, safety and safeguarding, and the achievement of its goals and objectives, benefitting the local population through improved health outcomes.
8. Communication Issues 8.1 Risk management training has been provided to key staff with responsibility for
assessing and managing risks in the CCG team. The CCG’s Senior Management Team reviews the risk register monthly and assurance framework quarterly. All projects are required to have risk registers which are reviewed on a monthly basis. The Risk Management Strategy, Risk Registers, guidance and assessment forms will be published on the CCG Intranet. Copies of the strategy and risk registers are also available to members of the public on the website or upon application by post or email.
9. Legal Issues 9.1 The Governing Body assurance framework supports delivery of the key objective in
the Risk Management Strategy to ensure that the CCG complies with statutory and regulatory requirements in respect of risk management and health and safety.
Page 6 of 11

10. Conclusion 10.1 The report presents the quarter 3 review of the assurance framework for review by
the Governing Body.
Managerial Lead – Andrew Thomas, Governance Director
Signatory details: Dawn Boyer, [email protected], 0151 244 4127
Background Documents:
None
Appendices:
A – Mapping CCG Assurance Framework and Governing Body Assurance Framework B – Assurance rating summary quarter 3
Page 7 of 11

Appendix A Mapping CCG Assurance Framework and Governing Body Assurance Framework NATIONAL CCG ASSURANCE FRAMEWORK LOCAL GOVERNING BODY ASSURANCE FRAMEWORK QUARTER 1 ASSESSMENT QUARTER 3 SUMMARY
Domain 1 Are patients receiving clinically commissioned,
high quality services?
Goal 1
Commission high quality services to meet the
needs of patients and the requirements of the NHS
Constitution
Reasonable
Domain 2 Are patient and the public actively involved?
Domain 3
Are CCG plans delivering better outcomes for patients?
Domain 4
Does the CCG have robust governance arrangements?
Domain 6
Does the CCG have strong and robust leadership?
Goal 2
Ensure effective and efficient governance of
the CCG
Goal 3
Continue to develop the CCG to be the best it can
be
Reasonable
Reasonable
Domain 5
Are CCGs working in partnership with others?
Page 8 of 11

Assurance Framework 2014/15 Assurance Rating Summary Quarter 3
Key: ▼ L – Assurance rating reduced from previous Quarter N/A – Not applicable – assurance not expected ► M – Maintained assurance rating from previous Quarter ▲ H - Higher assurance rating than previous Quarter Blank – No comparable rating
Risk No Risk Description
Risk Rating (L & C) Accountable Lead
Assurance Rating
Q1
Assurance Rating
Q2
Assurance Rating
Q3
Assurance Rating
Q4
Assurance Rating Key
Unique Identifie
r
Strategic risk transposed from Assurance Framework document
Risk rating based on
agreed risk matrix
Identified lead on behalf of the CCG who is referred to
as the ‘Risk Owner’ on the Assurance
Framework document
These columns will state either ‘Limited’ ‘Reasonable’ or ‘Significant’ assurance has been awarded dependent on the weight of assurance provided
This column will have ▼or ►or ▲ inserted here to demonstrate any changes since last review
GOAL 1: To commission high quality services to meet the needs of the patients and the requirements of the NHS Constitution Key Objective 1: Improve health outcomes for local people including vulnerable groups
1.1 Activity increases resulting in cost pressures and performance failures
2x4 = 8 Philip Thomas Reasonable Reasonable Reasonable
►
1.2 Commissioning intentions not delivered 3x3 = 9 Philip Thomas Reasonable Reasonable Reasonable ►
1.3 Commissioning intentions do not deliver improved outcomes
2x3 = 6 Philip Thomas Reasonable Reasonable Reasonable ►
1.4 Knowsley priorities not reflected in collaborative commissioning 2x2 = 4 Philip Thomas Reasonable Reasonable Reasonable ►
1.5
Commission services from providers who are unable to deliver specified contract performance and outcomes resulting in no improvement to or deteriorating health outcomes
2x3 = 6 Philip Thomas Reasonable Reasonable Reasonable ►
1.6 Commissioned services fail to address inequalities in health outcomes 2x3 = 6 Philip Thomas Reasonable Reasonable ►
Key Objective 2: Ensure patients rights under the NHS Constitution
2.1 Failure to manage demand results in failure to meet key constitutional rights e.g. A&E, RTT which may result in patient harm and reputational risk
3x4 = 12 Philip Thomas Reasonable Reasonable Reasonable
►
Page 9 of 11

Assurance Framework 2014/15 Assurance Rating Summary Quarter 3
Key: ▼ L – Assurance rating reduced from previous Quarter N/A – Not applicable – assurance not expected ► M – Maintained assurance rating from previous Quarter ▲ H - Higher assurance rating than previous Quarter Blank – No comparable rating
Key Objective 3: Ensure local people get good quality care
3.1 Failure to manage complex provider landscape may affect quality and performance 3x4 = 12 Philip Thomas Reasonable Reasonable Reasonable ►
3.2 Lack of stakeholder engagement results in services that deliver poor patient experience and outcomes 3x3 = 9 Philip Thomas Reasonable Reasonable Reasonable ►
GOAL 2: Ensure effective and efficient governance of the CCG
Key Objective 4: Achieve key financial duties
4.1 Non-delivery of financial duties targets due to inadequate financial management within the CCG
1x5 = 5 Paul Brickwood Significant Significant Significant ►
4.2
Failure to achieve financial targets due to increased demand cost pressures (PbR, CHC, prescribing) or failure to manage budgets robustly
2x4 = 8 Paul Brickwood Reasonable Reasonable Reasonable ►
4.3
Uncertainty over future NHS funding or other policy prevents CCG delivering local commissioning plans and still achieve financial targets
3x4 = 12 Paul Brickwood Reasonable Reasonable Reasonable ►
Key Objective 5: Governance systems meet statutory requirements and good practice requirements
5.1 Ineffective governance of CCG will lead to inability to meet statutory requirements, reputational damage or financial loss
2x4 = 8 Andrew Thomas Significant Significant Significant ►
5.2 Ineffective governance of services commissioned by the CCG will lead to patient harm, reputational damage or financial loss
2x5 = 10 Andrew Thomas Reasonable Reasonable Reasonable ►
Key Objective 6: Performance management is proactive and leads to continuous improvement
6.1 Gaps or delays in availability and quality of data, information and intelligence reduce effective performance management
4x3 = 12 Andrew Thomas Limited Limited Limited ►
Page 10 of 11

Assurance Framework 2014/15 Assurance Rating Summary Quarter 3
Key: ▼ L – Assurance rating reduced from previous Quarter N/A – Not applicable – assurance not expected ► M – Maintained assurance rating from previous Quarter ▲ H - Higher assurance rating than previous Quarter Blank – No comparable rating
6.2 Actions taken to address performance issues are insufficient or not adequate to achieve improvement 3x3 = 9 Andrew Thomas Reasonable Reasonable Reasonable ►
GOAL 3: Continue to develop the CCG to be the best it can be Key Objective 7: Review, refresh and implement the organisational development plan
7.1 Organisational Development Plan fails to keep pace with our ambition and aspiration for the CCG and the local population
4x2 = 8 Dianne Johnson Reasonable Reasonable Reasonable ►
Key Objective 8:Ensure there is sufficient capacity and capability within the organisation
8.1 Insufficient capability and capacity leads to inability to deliver statutory functions and / or commissioning plan
3x3 = 9 Dianne Johnson Significant Significant Significant ►
8.2 Commissioning Support delivery failures leads to inability to deliver statutory functions and / or commissioning plan
3x3 = 9 Dianne Johnson Reasonable Reasonable Reasonable ►
Key Objective 9: Embed the Programme Management Office (PMO) approach throughout the organisation
9.1 Failure to fully embed PMO approach across the whole organisation leads to ineffective / inefficient use of resources and failure to deliver key priorities
3x3 = 9 Dianne Johnson Limited Reasonable Reasonable ►
Page 11 of 11

Document 33(03)07
Report to Knowsley Clinical Commissioning Group Governing Body Date of meeting: 5th March 2015
Report title: Risk Management Strategy
Report presented by: Dawn Boyer, Head of Corporate Services
Purpose of the report: To seek the Governing Body’s approval to the updated Clinical Commissioning Group (CCG) Risk Management Strategy appended to this report
Recommendations:
Action / Decision required
The Governing Body is recommended to:
• Approve the CCG Risk Management Strategy 2015 – 2017 appended to this report;
• Delegate authority to the Accountable Officer to approve changes to the risk management templates appended to the strategy following further development activity as described in the report.
Delegated Powers:
For decision reports only
Justification for Part B agenda (if applicable)
N/A
Commissioning Values Which area(s) does this support? Please insert ‘x’ that apply
1. Patient centred
2. Safe X
3. High quality X
4. Cost effective X
5. Outcome focused
6. Closer to home
7. Affordable
[one page only]
Page 1 of 41

GOVERNING BODY
RISK MANAGEMENT STRATEGY
Executive Summary The report presents an updated Risk Management Strategy 2015/16 – 2017/18 for review and approval by the Governing Body. This has been revised to reflect feedback following a review by PwC, including risk appetite statements developed with the Governing Body, management structure changes, and updates to the risk matrix and risk register format. The report also sets out further development work underway, in respect of the risk management tools used by the CCG which may result in future changes to the templates appended to the strategy. The Governing Body’s views are also sought on an alternative presentation format, to aid user navigation and effective presentation on the intranet.
Page 2 of 41

1. Purpose of the report 1.1 The purpose of the report is to seek the Governing Body’s approval to the updated Clinical
Commissioning Group (CCG) Risk Management Strategy appended to this report. 2. Recommendations 2.1 The Governing Body is recommended to:
2.1.1 Approve the CCG Risk Management Strategy 2015/16 – 2017/18 appended to this report;
2.1.2 Delegate authority to the Accountable Officer to approve changes to the risk management templates appended to the strategy following further development activity as described in the report.
3. Background 3.1 Effective risk management supports the CCG to deliver on its ambition for a healthier,
happier population with a better quality of life, a reduction in health inequalities and improved access to health care when required as close as possible to the patient.
3.2 Risks are inherent in all of the functions that the CCG undertakes and in all of the services that it commissions others to undertake on its behalf. An appropriate and robust risk management framework is an essential requirement for any effective and well governed organisation. The CCG assurance process domains include a requirement that CCG’s have robust governance arrangements. These include an effective risk management strategy.
3.3 The CCG’s Risk Management Strategy was approved by the Shadow Governing Body in
September 2012. It has subsequently been reviewed as part of the development work in respect of the CCG’s risk management arrangements currently being undertaken with PwC.
4. Evidence and Consultation 4.1 The PwC review of the CCG’s current Risk Management Strategy concluded that ‘Our
review of the 2012-2014 Risk Management Strategy found that the document does contain many of the sections and much of the content we would expect to see in such a document. However, there are some areas that could be improved, including:
3.1.1 The CCG’s risk appetite is not articulated within the document; 3.1.2 There is no consideration of cumulative risk; 3.1.3 The Assurance Framework and Corporate Risk Register contain different risks but
should be consistent; and 3.1.4 The manner in which the document is presented offers scope for improvement. A
more engaging format will contribute to greater awareness, buy in and embedding of governance risk and controls.’
4.2 PwC recommended that:
3.2.1 The CCG’s risk appetite should be clearly articulated in the Risk Management Strategy;
3.2.2 Cumulative risk should be considered, incorporated into the risk appetite and reported on a regular basis to the Governing Body;
Page 3 of 41
3.2.3 The Assurance Framework and Corporate Risk register should be aligned so there is clear line of sight between strategic and operational risks; and
3.2.4 The revised strategy document should be represented in a more visual and engaging format – allowing user navigation and effective presentation on the intranet.
4.3 There are also a number of further updates required to reflect changes in the CCG’s
management structure, the senior management team review of the risk matrix and risk register format, and amendments to the Audit Committee terms of reference.
4.4 A facilitated Governing Body Development Session was held in September to discuss risk
appetite and develop risk appetite statements for the CCG’s key risk areas to provide a framework against which the CCG can consider strategic options, inform future control efforts and to take an appropriate level of risk in the achievement of its objectives. This was followed up with individual telephone conversations with PwC to clarify understanding and if possible seek consensus where there were variations in the risk appetite. The resulting statements have been incorporated into the Risk Management Strategy at section 5.
4.5 The next stage of the development activity includes a review of all existing risk registers and
assurance framework collateral, in order to improve the framework for effective risk identification, assessment and prioritisation and process for assessing and reporting cumulative risk and linking the assurance framework and risk register. This will be the subject of a further Governing Body development session. A high level action plan is attached at appendix B.
4.6 A more visual and engaging format for presentation of the risk management strategy has
been developed, allowing user navigation and effective presentation on the intranet, and can be found at http://nww.knowsleyccg.nhs.uk/?id=3642. It is intended that this will be used alongside and complement the more formal Risk Management Strategy document.
5. Proposals 5.1 It is proposed that the updated Risk Management Strategy for 2015/16 – 2017/18 attached
as appendix A is approved by the Governing Body. 5.2 As indicated above work is continuing to develop and improve the risk management
framework. Initial proposals from this work will be presented in a further workshop with the Governing Body for consultation, discussion and development. It is anticipated that this will result in changes to the process described in section 7 and the templates at appendices 5 and 6 of the Risk Management Strategy. Approval is sought to delegate authority to the Accountable Officer to approve these changes following this development activity.
5.3 The final stage of the development work will be effective skills transfer to drive the
implementation of the framework and to equip CCG staff with the confidence and skills to perform their roles and behaviours.
6. Impact on Services to the Population
6.1 The risk management strategy will ensure that the CCG has effective arrangements for oversight of quality and safety processes, and arrangements for safeguarding children and vulnerable adults. Effective risk management will support the CCG to achieve its goals and objectives benefitting the local population through improved health outcomes.
Page 4 of 41

7. Resource Implications 7.1 Financial
The cost of external support to develop the CCG’s risk management arrangements is £25,000 and this is funded from the CCG’s running cost allowance in 2014/15 and 2015/16.
7.2 Human Resources
A required outcome of the development work is an increase in the knowledge and skills of the Governing Body and staff team in order to further embed risk management into the CCG.
7.3 Technology
The proposals include a more visually engaging and easily navigable version of the Risk Management Strategy. This will be presented via the CCG’s Intranet and has no further technology implications.
7.4 Physical Assets
There are no physical asset implications arising from the proposals in this report. 8. Risk Assessment 8.1 There are no significant risks to the CCG in accepting the recommendations in this report,
which will result in an improved Risk Management Strategy.
8.2 If the updated strategy is not accepted, then the CCG will not have a current Risk Management Strategy, and there is a risk that this will be highlighted in the year end audit opinion.
9. Summary
9.1 The report presents an updated CCG Risk Management Strategy for review and approval by the Governing Body. It also highlights the further development activity commissioned to support the development and improvement of the CCG’s risk management arrangements.
Andrew Thomas – Governance Director
Signatory details: Dawn Boyer, [email protected], 0151 244 4127
Background Documents: None. Appendices: Appendix A – Risk Management Strategy 2015 – 2017 Appendix B – Risk management action plan
Page 5 of 41
Appendix A
Risk Management Strategy
2015/16 – 2017/18
Page 6 of 41
Version Control:
Version History: Version Number Reviewing Committee / Officer Date 0.1 Initial draft by Head of Corporate Services for review by
Accountable Officer and Chief Finance Officer 10 July 2012
0.2 Updated to reflect feedback from Accountable Officer and Chief Finance Officer
14 August 2012
1.0 Approved by Shadow Governing Body 12 September 2012 1.1 Reviewed and updated by Head of Corporate Services to
reflect changes in management structure, changes to risk matrix and Audit Committee terms of reference, and initial risk appetite statements. For review by Governance Director.
26 November 2014
1.2 Updated by PwC to reflect final risk appetite statements 2 February 2015 1.3 Amended by Head of Corporate Services to reflect further
planned developments for review by Governance Director. 12 February 2015
1.4 Updated to reflect feedback prior to submission for review by Accountable Officer
18 February 2015
1.5 Updated to reflect feedback from Accountable Officer prior to review and approval by Governing Body
20 February 2015
Page 7 of 41

Contents
1 Introduction 2 Statement of Intent 3 Definitions 4 Strategic Objectives 5 Risk Appetite 6 Accountability and Organisational Structure 7 Systems and Processes for Managing Risk 8 Risk Management Training 9 Monitoring the Effectiveness of the Strategy 10 Communication 11 Strategy Review Arrangements Appendices: 1. CCG Governance Structure 2. CCG Audit Committee Terms of Reference 3. Risk Matrix 4. Identification of Risk & Escalation Process 5. Governing Body Assurance Framework 6. Corporate Risk Register
Page 8 of 41

1. INTRODUCTION 1.1 Effective risk management supports NHS Knowsley Clinical Commissioning
Group (the CCG) to deliver on its ambition for a healthier, happier population with a better quality of life, a reduction in health inequalities and improved access to health care when required as close as possible to the patient.
1.2 Risks are inherent in all of the functions that the CCG undertakes and in all of
the services that it commissions others to undertake on its behalf. Unmanaged risk can impact upon patients and the wider population, the achievement of CCG objectives and its reputation, and its financial and other assets.
1.3 The CCG’s initial Risk Management Strategy 2012 – 14 set out the CCG’s
intentions and arrangements for the effective evaluation and management of its risks. It provides a sound foundation and framework for the continuous identification, assessment, management and monitoring of all risks.
1.4 The CCG has reviewed and updated the strategy for 2015/16 – 2017/18,
drawing on external expertise to ensure that it reflects current good practice in NHS, other public and private sectors. This work will continue through the life of the strategy with further development of the risk management tools used in order to provide a comprehensive integrated view of risks, and to further embed risk management into strategic and operational processes.
2. STATEMENT OF INTENT 2.1 The CCG is committed to establishing an organisational culture that ensures
risk management is an integral part of everything it does. Risk management will be embedded into all management systems and corporate planning as well as the setting of strategy and objectives.
2.2 The risk appetite statements agreed by the Governing Body will be used as a
framework against which to consider strategic options, inform future control efforts, and to take an appropriate level of risk in achievement of the CCG’s objectives.
2.3 The CCG regards the Risk Management Strategy as an important tool in
helping to ensure it achieves its objective of improving health outcomes for the borough and to commission high quality safe services.
2.4 The CCG recognises that a robust risk management system is a key
component of the organisation’s system of internal control and serves to provide assurance to key stakeholders of its capability to deliver its objectives.
Page 9 of 41
3. DEFINITIONS 3.1 Hazard is the potential to cause harm; Risk on the other hand is the likelihood
of harm (in defined circumstances, and usually qualified by some statement of the severity of the harm).
3.2 Risk Assessment is the process where:
• Hazards are identified • Risks associated with each hazard are analysed / evaluated • Appropriate ways to eliminate or control the hazard are identified
3.3 Risk Appetite is the extent to which the organisation is willing to tolerate risk in
order to achieve its objectives. 3.4 The Risk Management System is the culture, processes and structure that are
directed towards effective management of potential opportunities and threats to the organisation achieving its objectives.
3.5 The Risk Register is a record of the organisation’s identified risks, with details
of their assessment (risk score) and how the risk is being managed. 3.6 The Assurance Framework identifies the risks to the strategic objectives of
the organisation and provides assurance that those risks are being managed effectively.
4. STRATEGIC OBJECTIVES 4.1 The CCG’s risk management objectives are to: 4.1.1 Embed key risk management systems and processes
• Establish clearly defined responsibilities for risk management and lines of accountability throughout the organisation
• Provide a robust Governing Body Assurance Framework • Maintain a Corporate Risk Register • Embed operational and project risk registers across all areas of the
organisation • Embed a systematic process for the identification, analysis, evaluation,
treatment and monitoring of risks across all areas of the organisation • Maintain a systematic and consistent approach to learning lessons and
promoting continuous improvement • As far as reasonably practicable, minimise costs associated with risk
Page 10 of 41
4.1.2 Embed risk management into commissioning process
• Ensure that all risks associated with the way the organisation commissions and procures services are identified, assessed, minimised and wherever practicable, eliminated
• Ensure that the design and specification of new services and service re-design actively considers potential risks, including clinical, safeguarding and financial risks, and seeks to minimise or eliminate them
• Embed systematic processes for considering incidents in commissioned services, which compromise the safety and welfare of patients, children and vulnerable adults, and reflecting learning in current and future commissioning activity
• Promote active stakeholder involvement in risk management with particular reference to key partnerships
4.1.3 Ensure that the CCG is ‘risk aware’ and the members of the governing
body and staff are appropriately trained and skilled in risk management
• Raise awareness of risks and their management through a programme of communication and training
• Foster an environment whereby all governing body members and staff understand that risk management is their responsibility
4.1.4 Ensure statutory and regulatory compliance
• Satisfy all mandatory and statutory duties and undertakings • Satisfy the requirements of the Annual Governance Statement • Achieving and improving performance against all internally and externally
regulated risk management activities • Ensure the health and safety of all those who work for or visit the CCG
offices
5. RISK APPETITE 5.1 The Governing Body has determined the risk appetite for each of the CCG’s
strategic risk areas based on the following risk appetite definitions:
• Averse – Avoidance of risk and uncertainty is key • Minimal – Preference is for ultra-low risk options, as little risk as
reasonably possible • Open – Willing to consider all possible options and choose • Hungry – Eager to be innovative and to choose options offering
potentially higher rewards despite greater inherent risk 5.2 The Governing Body has agreed the following risk appetite statements in
respect of each of the CCG’s strategic risk areas:
Page 11 of 41

5.2.1 Quality – No primary risk appetite defined – joint between minimal and open
Appetite to take decisions with potential to expose the organisation to additional scrutiny or interest on commissioning new services where the benefit and innovation justifies it. On existing commissioned services, tolerance for risk taking limited to those decisions where there is no chance of any significant detriment to quality. Senior management aims to minimise the chance of patient harm and the associated damage to the reputation of the NHS.
5.2.2 Transformation – Primary risk appetite defined as open
Constantly reviewing assumptions and business case to drive greater value and outcomes using test and learn approach whilst mitigating policy intent and objective based outcomes. Additional development / innovation used routinely to enable further benefits realisation, value, or enhanced outcomes.
5.2.3 Engagement – Primary risk appetite defined as hungry Consistently developing new ways to improve patient engagement and service
delivery, and prepared to accept short to medium term impacts to achieve longer term objectives
5.2.4 Financial Management – Primary risk appetite defined as open
Prepared to invest for return and minimise the possibility of failing to deliver financial targets by managing the risks to a tolerable level.
5.2.5 Governance and Decision Making – Primary risk appetite defined as open
Innovation supported, with demonstration of commensurate improvements or benefits. Encourage challenge at all levels to drive continuous improvement. The organisation will act independently and proactively manage potential conflicts of interests.
5.2.6 Capacity and Capability – Primary risk appetite defined as open
Prepared to consider options which may have longer term benefits at the expense of short term gains in capacity and capability.
5.3 These risk appetite statements will be reviewed annually by the Governing
Body to ensure their continued accuracy and relevance to the organisational challenges and strategic goals.
Page 12 of 41

6. ACCOUNTABILITY AND ORGANISATIONAL STRUCTURE 6.1 Organisational Structure 6.1.1 The CCG Membership, Governing Body, Committees and senior team are
committed to ensure that risk management is integral to the organisation’s strategic and operational planning, processes and systems.
6.1.2 The CCG has effective governance arrangements capable of taking
responsibility and accountability for quality, finance and performance and:
• Is designed to fit the organisational and reporting arrangements • Will enable maximum probity transparency and accountability within
proportionate and defensible processes • Is robust enough to withstand challenge whilst being flexible enough to
enable local ownership from the clinical community • It not overly bureaucratic but sufficient to safeguard those involved in the
processes • Has been developed on existing sound practices and aligned to NHS
approaches and guidance on good governance 6.1.3 The CCG Governing Body is responsible for ensuring delivery of the
organisation’s aims and objectives and the structures in place to reflect the organisation’s roles and responsibilities. The structure including Governing Body Committees consider each individual aspect of governance at an adequate level of detail but also brings them all together to give the organisation appropriate assurance. The CCG governance structure is attached at appendix 1.
6.1.4 Specific accountabilities, roles and responsibilities for risk management are set
out below and provide a structure that supports the integrated approach to risk and governance.
6.2 The CCG Governing Body 6.2.1 The Governing Body is responsible for determining the CCG’s risk appetite in
relation to the achievement of its strategic goals, which will inform strategic decisions and control efforts.
6.2.2 The Governing Body is committed to providing the resources and support
systems necessary to support the Risk Management Strategy. It has a duty to assure itself that the organisation has properly identified the risks it faces and that it has processes in place to mitigate those risks and the impact they have on the organisation and its stakeholders.
6.2.3 The Governing Body discharges this duty as follows:
• Identifies risks to the achievement of its strategic goals
Page 13 of 41

• Determines the organisation’s level of risk appetite in relation to the strategic risks
• Monitors the risks to the achievement of the CCG’s strategic goals via the CCG Assurance Framework
• Ensures that there is a structure in place for the effective management of risk throughout the CCG
• Receives regular updates and reports from the Audit Committee identifying significant risks and progress on mitigating actions
• Demonstrates leadership, active involvement and support for risk management
6.3 The CCG Audit Committee 6.3.1 The Audit Committee is a committee of the CCG Governing Body responsible
for establishing and maintaining effective systems of integrated governance, risk management and internal control that support the CCG’s overall objectives. The Audit Committee has delegated authority to approve the CCG’s risk management arrangements.
6.3.2 The Audit Committee discharges this duty as follows:
• Approves and reviews the CCG risk management strategy • Approves the policy, procedures and guidelines to support the delivery of
the CCG risk management strategy • Reviews the Annual Governance Statement prior to endorsement by the
CCG • Ensures that the Assurance Framework and Corporate Risk Register are
reviewed and updated on behalf of the Governing Body • Critically reviews the organisation’s financial reporting and internal control
principles • Requests and reviews reports and positive assurances from senior
managers on the arrangements for risk management • Ensures that appropriate relationships exist with both internal and external
audit • Reviews the Internal Audit work programme, ensuring that this is
consistent with the needs of the CCG as identified in the Assurance Framework
• Reviews the findings in relation to risk management systems of significant assurance functions both internal and external
• Monitors responsiveness to findings and recommendations of internal audits, external audit and other assurance functions
• Provides regular updates and reports to the CCG Governing Body identifying significant risks and progress on mitigating actions
• Aligns its work programme with that of the CCG Quality and Safety Committee in respect of clinical and safeguarding risks
6.3.3 The terms of reference of the CCG Audit Committee are attached at appendix
2.
Page 14 of 41

6.4 Responsibilities of other CCG Committees and Sub Committees 6.4.1 All committees and sub-committees of the CCG are responsible for:
• Providing assurance on key controls where this is identified as a requirement in the Assurance Framework
• Ensuring that risks associated with their areas of responsibility are identified, reflected on the risk register, and effectively managed
In addition committees and sub-committees have responsibilities for specific areas of risk management.
6.4.2 The Quality & Safety Committee is responsible for:
• Overseeing quality and safety processes across all commissioned services
• Overseeing arrangements for safeguarding children and vulnerable adults across all commissioned services
• Assuring the Governing Body that quality and patient safety and safeguarding activity is coordinated and transparent and subject to a coherent and systematic review
6.4.3 The Finance & Performance Committee is responsible for:
• Monitoring delivery of QIPP programmes, including key risks, and agreeing corrective action if required
• Monitoring delivery of the CCG commissioning plan, including key risks, and agreeing corrective action if required
• Monitoring delivery of the CCG financial duties, including key risks and make recommendations or agree actions within the framework of the scheme of reservation and delegation contained within the constitution
• Monitoring financial and operational performance across all commissioned services, assessing potential shortfalls and risks, and recommending actions to address them
6.4.4 The Medicines Management Sub-Committee is responsible for:
• Providing assurance to the Governing Body that safe, effective and good governance procedures are in place and are subject to review
• Oversee the management of quality issues and financial risk in prescribing and associated clinical activity
• Develop procedures for safe and secure handling of medicines and local action on safe use of medicines and NICE guidance
Page 15 of 41
6.5 The Accountable Officer 6.5.1 The Accountable Officer has overall accountability for the management of risk
and discharges this duty as follows:
• Continually promotes risk management and demonstrates leadership, involvement and support.
• Ensures an appropriate committee structure is in place, with regular reports to the Governing Body.
• Ensures that senior officers of the CCG are appointed with managerial responsibility for risk management.
• Ensures the development of appropriate Policies, Procedures and Guidelines for the CCG in relation to risk management
• Identifies risks to the achievement of the CCG’s strategic goals • Monitors these via the CCG Assurance Framework and Corporate Risk
Register 6.6 Lay Member – Audit and Governance Lead 6.6.1 The lay member is the governance lead on the CCG Governing Body with
responsibility for oversight of the risk management strategy and systems and discharges this duty as follows:
• Chairs the CCG Audit Committee • Is accountable to the CCG Governing Body for the work of the CCG Audit
Committee • Through the work of the Audit Committee, confirms that appropriate and
effective risk management systems are in place • Promotes risk management processes with all CCG member practices,
ensuring that practices continuously improve quality of primary care and report risks to the CCG for assessment and mitigation.
6.7 Governance Director 6.7.1 The Governance Director has managerial leadership for risk management and
discharges this duty as follows:
• Prepares the risk management strategy for review and approval by the CCG Audit Committee
• Leads the preparation and regular updating of the Assurance Framework and Corporate Risk Register for review by the CCG Audit Committee
• Arranges the development of the policy, procedures and guidelines to support the delivery of the CCG risk management strategy for review and approval by the CCG Audit Committee
• Supports the Chair of the CCG Audit Committee in forward planning and programming activity in respect of risk management and ensuring that committee members are aware of best practice, national guidance and other relevant documents and have access to independent advice as appropriate
Page 16 of 41

• Responds to requests from the CCG Audit Committee for reports and positive assurance on risk management arrangements
• Identifies the training needs of CCG governing body, committee and sub-committee members and staff and ensures these are met
• Other responsibilities of senior officers as set out below 6.8 Executive Directors 6.8.1 Executive Directors should incorporate risk management within all aspects of
their work and are responsible for directing the implementation of the CCG Risk Management Strategy by:
• Contributing to the preparation and updating of the Assurance Framework
and Corporate Risk Register • Demonstrating personal involvement and support for the promotion of risk
management • Ensuring that staff accountable to them understand and pursue risk
management in their areas of responsibility. • Setting personal objectives for risk management and monitoring their
achievement • Ensuring risks are identified and managed and mitigating actions
implemented in functions for which they are accountable. • Ensuring action plans for risks relating to their respective areas are
prepared and reviewed on a regular basis. • Ensuring a risk register is established and maintained that relates to their
area of responsibility and to involve staff in this process to promote ownership of the risks identified.
• Ensuring risks are escalated where they are of a strategic nature. 6.8.2 All governing body members and senior officers are responsible for compliance
with the Risk Management Strategy and must ensure that:
• Staff undertake mandatory and statutory training • Risk assessments are undertaken and recommended actions are
implemented • The reporting of adverse incidents within their work area is undertaken,
together with action to prevent or minimise reoccurrence • They take action to protect themselves and others from risks
6.9 All Staff 6.9.1 All CCG staff are responsible for being aware of and complying with the Risk
Management Strategy and will assist the risk management process by:
• Being aware that they have a duty under legislation to take reasonable care of their own safety and the safety of others who may be affected by
Page 17 of 41
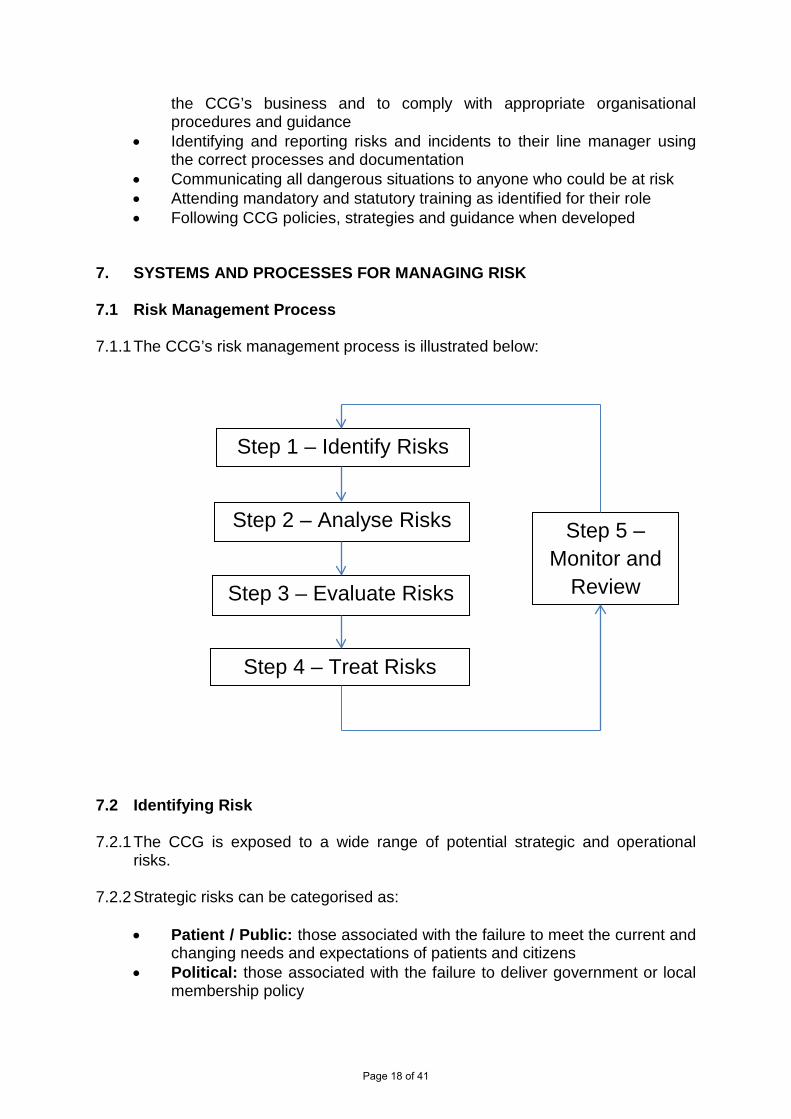
the CCG’s business and to comply with appropriate organisational procedures and guidance
• Identifying and reporting risks and incidents to their line manager using the correct processes and documentation
• Communicating all dangerous situations to anyone who could be at risk • Attending mandatory and statutory training as identified for their role • Following CCG policies, strategies and guidance when developed
7. SYSTEMS AND PROCESSES FOR MANAGING RISK 7.1 Risk Management Process 7.1.1 The CCG’s risk management process is illustrated below: 7.2 Identifying Risk 7.2.1 The CCG is exposed to a wide range of potential strategic and operational
risks. 7.2.2 Strategic risks can be categorised as:
• Patient / Public: those associated with the failure to meet the current and changing needs and expectations of patients and citizens
• Political: those associated with the failure to deliver government or local membership policy
Step 1 – Identify Risks
Step 2 – Analyse Risks
Step 3 – Evaluate Risks
Step 4 – Treat Risks
Step 5 – Monitor and
Review
Page 18 of 41

• Economic: those affecting the ability of the CCG to meet its financial targets
• Market: those affecting the ability of the CCG to secure appropriate cost and quality of provision to deliver its commissioning priorities
• Legislative: those associated with current or potential changes in national or European law
• Social: those relating to the effects of changes in demographic, residential or socio-economic trends
• Technological: those associated with the capacity of the CCG to deal with the pace or scale of technological change or effectively harness technology to deliver its objectives
• Environmental: those relating to the environmental consequences of progressing the CCG’s strategic objectives
7.2.3 Operational risks can be categorised as:
• Clinical: those related to the delivery of effective care and treatment • Contractual: those related to the failure of providers to deliver services • Business: those affecting the delivery of the CCG’s operational business
plans • Health and Safety: those related to accident prevention and securing the
safety and welfare of patients, staff and visitors • Financial: those associated with financial management • Workforce and recruitment: those related to the ability to attract,
develop and retain required capacity and skills • Legal liability: those related to possible breaches of legislation • Estate and technological: those related to reliance on buildings and
operational equipment 7.2.4 The CCG identifies risks from a range of external and internal sources. 7.2.5 External identification of risks occurs via various pathways and agencies,
including external assessments and inspections:
• NHS England • National reports and guidance • NHS litigation authority • Health and Safety Executive • External audit • Merseyside Internal Audit Agency • Care Quality Commission inspections • Ombudsmen reports • Partner agencies • Commissioned providers • Coroner reports • Media and publications • National Patient Safety Agency alerts • Medicines and Healthcare products Regulatory Agency
Page 19 of 41
• Central Alerting System (CAS) from Department of Health 7.2.6 Internal identification of risks occurs via various internal processes and
monitoring arrangements including:
• Strategic and operational planning • Programme and project management • Risk assessment • CCG Committees and sub committees • CCG Membership • Staff members • Staff survey • Patient Participation Groups • Patient satisfaction surveys • Serious untoward incidents • Incidents and complaints monitoring • Claims • Health and Safety, Fire and Environmental audits • Training needs analysis
7.2.7 The identification of risks is the responsibility of all CCG members and staff and
will be done proactively, via regular planning and management activities and reactively, in response to inspections, alerts, incidents and complaints.
7.3 Analysing Risk 7.3.1 Once a risk is identified it will be analysed to determine how the risk may occur,
and the sort of effects it may have. The major controls will be identified, formal and informal, which help to prevent or mitigate the risk, and their effectiveness (adequate, inadequate, or uncertain) will be assessed.
7.4 Assess / Evaluate Risk 7.4.1 The risk assessment will reflect both the likelihood and any consequences of
the risk in terms of:
• Safety - risks should be assessed based on the level of harm likely to be caused and the numbers of people potentially affected.
• Finance - risks should be assessed based on the likely financial loss or cost to the CCG and the impact on the achievement of the key financial duties.
• Reputation - risks should be assessed based on the impact on internal and external stakeholders, in particular the CCG membership, patients and local population and key regulatory bodies such as NHS England, and on the extent and duration of adverse coverage, punitive action or loss of confidence.
Page 20 of 41

7.4.2 Risks will be graded using the CCG’s risk matrix attached at appendix 3 and risk assessment form attached at appendix 4. The level of risk is assessed by judging the likelihood of the residual risk occurring and consequences for the CCG should the event occur. This assessment results in an overall score ranging from 1 to 25 and a risk level of low, moderate, high, or extreme.
7.4.3 In assessing risk it is important to match the consequence to the likelihood, e.g.
trips and falls may happen periodically but serious injury or death while possible is very unlikely. Scoring this risk should be based on the most common consequence from a fall not the extreme worse case which might occur.
7.4.4 In assessing risk it is also important to assess the risk from the point of view of
the CCG as an organisation. Thus whilst there may be a considerable risk to a patient crossing a busy road to get to a CCG Commissioned clinic this would not be a CCG risk as it cannot be held responsible for road safety.
7.5 Treat Risk 7.5.1 Controls should be sufficient to ensure that risks to the delivery of strategic
objectives of the organisation are not compromised. Where controls are insufficient and could impact on the ability to deliver key objectives then escalation of the risk should take place. The risk identification and escalation process is illustrated in appendix 5.
7.5.2 The treatment of risks and responsibility for their management will depend upon
the risk level assessed and the CCG’s risk appetite in relation to that objective area:
• EXTREME RISKS (Scoring 15-25) are unacceptable and require
immediate intervention. They should be escalated immediately to a member of the senior management team who will determine the appropriate response, potentially including suspending activities unless the suspension could trigger an even higher risk to the CCG. All such risks should be reported immediately to the Governance Director.
• HIGH RISKS (Scoring 10-12) should be managed appropriately by the relevant senior manager and reported to the Governance Director.
• MODERATE RISKS (Scoring 4-9) should be managed appropriately by the relevant service and reported to the Governance Director.
• LOW RISKS (Scoring 1-3) are low priority and will be managed appropriately by the relevant service and included on the service or project risk register.
7.5.3 Possible responses to risks are:
• Transfer – commonly through insuring against the risk • Avoid – requiring a review of the objectives threatened by the risk and
may require the suspension or abandonment of certain services or activities at least until risk reduction measures are taken
Page 21 of 41

• Reduce – taking action to reduce the likelihood or consequence of the event thereby reducing the level of risk to an acceptable level
• Accept – do nothing but keep it under review for any changes and if resources permit consider actions to reduce it
7.5.4 Responsibility for determining the most appropriate options will depend upon
the risk level, as indicated above. Expert advice will be sought as required from within the organisation, and from external sources such as the CCG legal advisors, Care Quality Commission, Health & Safety Executive, NHS Litigation Authority, Counter Fraud & Security Management Service, Internal or External Auditors or by sharing best practice and learning from other organisations.
7.6 Monitoring and Review 7.6.1 In order to ensure risks are identified and quantified at all levels two key risk
documents have been developed. The Assurance Framework and Corporate Risk Register will provide assurance that the principal risks to the strategic objectives of the organisation have been identified and are being managed effectively. The Audit Committee has delegated responsibility on behalf of the Governing Body to monitor and scrutinise these documents before presenting them to the Governing body.
7.6.2 These risk management tools are being reviewed to ensure that they align with
the CCG’s risk appetite statements, highlight cumulative risks, and present a comprehensive integrated view of the risk environment.
Assurance Framework
7.6.2 The Governing Body Assurance Framework identifies and quantifies strategic
risks within the organisation. The Framework is the means by which the Governing Body monitors and controls the risks which may impact on the organisation’s capacity to achieve its objectives. The Assurance Framework format is attached as appendix 6.
7.6.3 Each principal risk is scored based on the likelihood and consequence of the
risk resulting in failure to achieve the strategic target. The governing body, through the Audit Committee, will review the Assurance Framework.
7.6.4 The responsibility for managing, monitoring and reviewing strategic risks is
delegated as follows:
• A risk owner, who will be a member of the senior management team, assigned to each strategic risk has overall responsibility for the risk, for ensuring actions are implemented, and for ongoing monitoring.
• The Senior Management Team will review the strategic risks quarterly and may amend scores and assurance ratings as a result of completed actions for approval by the Audit Committee.
• The CCG Audit Committee will review assurance ratings and progress and hold risk owners accountable for delivering identified corrective action
Page 22 of 41
• Update reports on significant and high risks are presented to each Audit Committee together with an indication of any new or emerging issues which may need to be considered.
Corporate Risk Register
7.6.5 The purpose of the Corporate Risk Register is to provide the Executive
Management Team and responsible Committees with a summary of the principal risks facing the organisation, with a summary of the actions needed and being taken to reduce these risks to an acceptable level. The information contained in the Corporate Risk Register should be sufficient to allow the Executive Management Team and responsible Committees to be involved in prioritising and managing major risks.
7.6.6 The Corporate Risk Register supports the Assurance Framework by providing a
means of identifying operational risks which impact on the CCG’s ability to provide assurance against strategic risks. The Corporate Risk Register format is attached as appendix 7.
7.6.7 The governing body, through its Committees, will review the Corporate Risk
Register. 7.6.8 The Executive Management Team will identify those risks which require
escalation to the Corporate Risk Register due to insufficient controls or where the risk threatens the strategic objectives of the organisation.
7.6.9 The corporate risk register will be reviewed monthly by the Executive
Management Team and reported to the responsible Committees. 7.6.10 Operational and project risk registers will be reviewed monthly by the relevant
service or project management team. 7.6.11 Individual risk owners are responsible for compliance with the risk
management strategy in order to ensure that remedial action is taken where key risks are identified within their area of responsibility. This will include monitoring risks, ensuring that actions are taken to manage and reduce risks as required, and updating the relevant risk register.
8. RISK MANAGEMENT TRAINING 8.1 Training and development, including regular updates, will be required to
support the successful and ongoing implementation of the risk management strategy. This will be reflected in the CCG Organisational Development Plan and in individual learning and development plans.
Page 23 of 41

9. MONITORING THE EFFECTIVENESS OF THE STRATEGY 9.1 The Audit Committee will monitor compliance with the Risk Management
Strategy through the papers received throughout the year. The Committee may commission internal audits or seek further assurance and action from officers in areas where there may be a lack of compliance.
10. COMMUNICATION 10.1 This strategy will be communicated via public CCG Governing Body meetings. 10.2 This document will be made available to all employees via the CCG intranet. A
programme of risk management training for all levels of staff will be developed to support implementation and communication.
11. STRATEGY REVIEW ARRANGEMENTS 11.1 This strategy will be reviewed every three years by the Audit Committee.
Page 24 of 41

Appendix 1 – CCG Governance Structure
Clinical Membership Group
Chair: GP Elected by Membership
Commissioning Group Governing Body
Chair: Clinical Leader
Clinical Quality & Safety Committee
Chair: Governing Body Registered Nurse
Audit Committee
Chair: Lay Member – Audit & Governance
HR & Remuneration Committee
Chair: Lay Member - PPI
Finance & Performance Committee
Lay Member – Audit & Governance
Medicine Management Sub-Committee
Lay Member – Quality & Safety
Primary Care Commissioning
Committee
Lay Member – Audit & Governance
Page 25 of 41

Appendix 2
Audit Committee
Terms of Reference
1. Introduction
1.1 The Audit Committee (the Committee) is established in accordance with Knowsley Clinical Commissioning Group’s (the CCG) constitution, standing orders and scheme of delegation. These terms of reference set out the membership, role, responsibilities and reporting arrangements of the Committee and shall have effect as if incorporated into the CCG’s constitution and standing orders.
2. Membership a) Chair of the Committee – Lay Member Audit and Governance Lead b) Lay Member/Clinical Advisor c) CMG Representative (not on Governing Body)
A vice chair will be chosen from these members.
In attendance
a) Internal Audit Representative b) External Audit Representative c) Counter Fraud Representative d) Chief Finance Officer e) Governance Director
2.1 Other senior staff may be invited to attend, particularly when the Committee is
discussing areas of risk or operation that are the responsibility of that officer. Representatives from NHS Protect may be invited to attend meetings.
2.2 At least once a year the Committee should meet privately with the external and internal auditors. Regardless of attendance, external audit, internal audit, local counter fraud and security management (NHS Protect) providers will have full and unrestricted rights of access to the Audit Committee.
2.3 The CCG Chair and Accountable Officer will be invited to attend one meeting each year in order to form a view on, and understanding of, the committee’s operations.
3. Role and Responsibilities
3.1 The Audit Committee is responsible for establishing and maintaining effective systems of integrated governance, risk management and internal control that support the CCG’s overall objectives.
3.2 The duties of the Audit Committee will be driven by the priorities of the CCG, as identified by the CCG, and the associated risks. The key duties of the Committee are:
Page 26 of 41

3.3 Integrated governance, risk management and internal control
3.3.1 The Committee shall review the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the CCG’s activities that support the achievement of the CCG’s objectives.
3.3.2 It’s work will align to that of the Clinical Quality Committee which the CCG has established to seek assurance that robust clinical quality is in place and that other risks are mitigated
3.3.3 The Committee shall approve the detailed financial policies and procedures.
3.3.4 In particular the Audit Committee will review the adequacy and effectiveness of:
a) All risk and control related disclosure statements (in particular the Annual Governance Statement), together with any appropriate independent assurances, prior to endorsement by the CCG.
b) The underlying assurance processes that indicate the degree of achievement of CCG objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements.
c) The policies for ensuring compliance with relevant regulatory, legal and code of conduct requirements and r elated reporting and s elf- certification.
d) The policies and procedures for all work related to fraud and corruption as set out in Secretary of State Directions and as required by the NHS Counter Fraud and Security Management Service.
e) In carrying out this work the Committee will utilise the work of internal audit, external audit and other assurance functions, but will not be limited to these sources. It will also seek reports and assurances from officers and Governing Body members as appropriate, concentrating on the over-arching systems of integrated governance, risk management and internal control, together with indicators of their effectiveness.
f) This above will be evidenced through the Committee’s use of an effective assurance framework to guide it’s work and that of the audit and assurance functions that report to it.
3.4 Internal Audit
3.4.1 The Committee shall ensure that there is an effective internal audit function that meets mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Audit Committee, Accountable Officer and CCG. This will be achieved by: a) Consideration of the provision of the internal audit service, the cost of the
audit and any questions of resignation and dismissal b) Review and approval of the internal audit strategy, operational plan and
more detailed programme of work, ensuring that this is consistent
Page 27 of 41
with the audit needs of the organisation as identified in the assurance framework
c) Considering the major findings of internal audit work (and management’s response), and ensuring co-ordination between the internal and external auditors to optimise audit resources
d) Ensuring that the internal audit function is adequately resourced and has appropriate standing within the CCG
e) An annual review of the effectiveness of internal audit f) Selection of the Internal Auditors
3.5 External Audit
3.5.1The Committee shall review the work and f indings of the external auditors and consider the implications and management’s responses to their work. This will be achieved by:
a) Consideration of the performance of the external auditors, as far as the rules governing the appointment permit.
b) Discussion and ag reement with the external auditors, before the audit commences, of the nature and scope of the audit as set out in the annual plan, and ensuring co-ordination, as appropriate, with other external auditors in the local health economy.
c) Discussion with the external auditors of their local evaluation of audit risks and assessment of the CCG and associated impact on the audit fee.
d) Review of all external audit reports, including the report to those charged with governance, agreement of the annual audit letter before submission to the CCG and any work undertaken outside the annual audit plan, together with the appropriateness of management responses.
e) Selection of external auditors once freedom to appoint is given to the CCG. 3.5.2 The Committee shall, when able, select the External Auditors.
3.6 Other Assurance Functions
a) The Audit Committee will monitor compliance with the Information
Governance Strategy and management framework and provide assurance to the Governing Body.
b) The Audit Committee shall review the findings of other significant assurance functions, both internal and external and consider the implications for the governance of the CCG.
c) These will include, but will not be limited to, any reviews by the Department of Health arm’s length bodies or regulators/inspectors (for example, the Care Quality Commission, NHS Litigation Authority, etc.) and professional bodies with responsibility for the performance of staff or functions (for example, Royal Colleges, accreditation bodies, etc.)
Page 28 of 41
3.7 Counter Fraud
a) The Audit Committee shall approve the counter fraud and security management arrangements and shall review the outcomes of counter fraud work. It shall also approve the counter fraud work programme.
3.8 Management a) The Audit Committee shall request and review reports and positive
assurances from senior staff on the overall arrangements for governance, risk management and internal control.
b) The Committee may also request specific reports from individual functions within the CCG as they may be appropriate to the overall arrangements.
3.9 Financial Reporting a) The Audit Committee shall monitor the integrity of the financial
statements of the CCG and any formal announcements relating to the CCG’s financial performance.
b) The Committee shall ensure that the systems for financial reporting to the CCG, including those of budgetary control, are subject to review as to completeness and accuracy of the information provided to the CCG.
c) The Audit Committee shall approve annual accounts and financial statements before submission to the CCG Annual General Meeting, focusing particularly on:
i. The wording in the Governance Statement and other disclosures relevant to the terms of reference of the committee;
ii. Changes in, and compliance with, accounting policies, practices and estimation techniques;
iii. Unadjusted misstatements in the financial statements; iv. Significant judgements in preparing of the financial statements; v. Significant adjustments resulting from the audit; vi. Letter of representation; and vii. Qualitative aspects of financial reporting.
4. Accountability and Reporting
4.1 The Audit Committee will be ac countable to the Knowsley Clinical Commissioning
Group Governing Body. The Committee will provide the Governing Body with an a nnual report of its work and the assurances that have been received.
4.2 The Audit Committee has the ability to establish sub committees and or short term task and finish groups, to support the discharge of the committee duties.
4.3 The ratified minutes of Audit Committee will be submitted to the Governing Body. Exception reports will also be submitted at the request of the Governing Body.
4.4 The Audit Committee will oversee the work of the Finance and
Page 29 of 41

Performance Committee.
5. Administration
5.1 The Committee will be supported by the Governance Director who will take lead managerial responsibility for forward planning and programme management, ensuring that Committee members are aware of best practice, national guidance and other relevant documents and have access to independent advice as appropriate
5.2 Appropriate administrative support will be provided to support the Chair in the preparation and circulation of the agenda, conduct of the Committee’s business, and i n taking minutes and producing reports on the work of the Committee as required.
6. Quorum
6.1 The Committee will be regarded as quorate if the following are present: a) The Chair (or Vice Chair) of the Committee b) Two other members of the committee
7. Voting
7.1 Wherever a vote is required, it will be on the basis of one member one vote.
8. Frequency and notice of meetings
8.1 The Audit Committee shall meet on at least 4 occasions during the financial year.
Additional meetings may be called by the Chair of the Committee as and when required.
8.2 Members shall be notified at least 10 days in advance that a meeting is due to take place. Exceptionally, the Chair may call an urgent meeting with less notice but not normally on less than 2 working days’ notice.
8.3 Agendas and reports shall be distributed to members 5 working days in advance of the meeting date, except in the case of urgent meetings above where supporting papers will be provided when it is called.
9. Conduct
9.1 All members are required to make open and honest declarations of interest at the commencement of each meeting or to notify the Committee Chair of any actual, potential or perceived conflict in advance of the meeting.
9.2 All members are required to uphold the Nolan Principles and all other relevant NHS Code of Conduct requirements.
9.3 The Committee will: a) Comply with the CCG’s principles of good governance b) Operate in accordance with the CCG’s scheme of reservation and delegation c) Comply with the CCG’s standing orders d) Operate in accordance with these terms of reference
Page 30 of 41
e) Comply with all relevant statutory and regulatory requirements
10. Date and Review
10.1 These Terms of Reference were approved by the Knowsley CCG Governing Body on 21st March 2013.
Version No. 2
Review dates 1st June 2015
Page 31 of 41

Q2. What is the likely consequence for the organisation if it does happen? Level Descriptor Description 5 Catastrophic Safety – Multiple deaths due to fault of CCG.
Finance – Significant financial loss above 1% of CCG budget Reputation – Potential disestablishment by NHSE, litigation, sustained adverse national media, significant adverse public reaction (prolonged high profile campaign including e.g. demonstrations, petitions), membership loses confidence in the CCG
4 Major Safety – Individual death/permanent injury/disability due to fault of CCG Finance – Major financial loss of 0.5-1% of CCG budget Reputation – Criticism or intervention by NHSE, litigation, adverse national media, adverse public reaction (e.g. petition, demonstrations, disruption to meetings), significant membership dissatisfaction
3 Moderate Safety – Moderate injury or illness, requiring medical treatment e.g. fractures due to fault of CCG. Finance – Moderate financial loss less than 0.5% of CCG budget Reputation – Reduced rating from NHSE or other external bodies, litigation, adverse local media coverage, patient complaints & dissatisfaction, membership complaints & dissatisfaction
2 Minor Safety – Minor injury or illness requiring first aid treatment e.g. cuts, bruises due to fault of CCG Finance – Minor financial loss less than 0.2% of CCG budget Reputation – Some criticism and slight possibility of complaint or litigation but minimum impact on organisation
1 Negligible Safety – None or insignificant injury due to fault of CCG Finance – No financial loss or very minor loss Reputation – No impact or loss of external reputation
Q1. What is the likelihood of event happening?
Level Descriptor Description
5 Almost Certain The event is almost certain to occur. Missing the target is almost a certainty.
4 Likely The event will occur in most circumstances. High probability of missing target.
3 Possible The event may well occur at some time. As likely to miss target as to achieve it.
2 Unlikely The event could occur at some time. Small probability of missing target.
1 Rare The event could occur only in exceptional circumstances. No likelihood of missing target.
Appendix 3 RISK MATRIX
Page 32 of 41
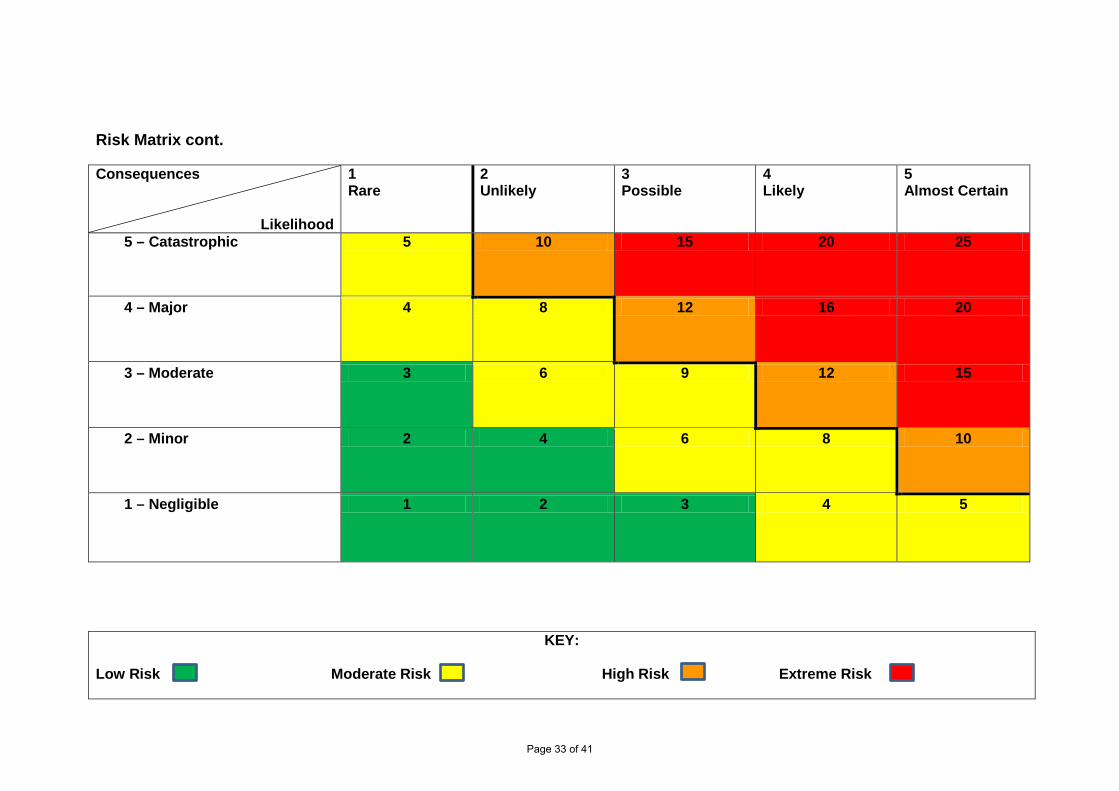
Risk Matrix cont.
Consequences
Likelihood
1 Rare
2 Unlikely
3 Possible
4 Likely
5 Almost Certain
5 – Catastrophic 5 10 15 20 25
4 – Major 4 8 12 16 20
3 – Moderate 3 6 9 12 15
2 – Minor 2 4 6 8 10
1 – Negligible 1 2 3 4 5
KEY:
Low Risk Moderate Risk High Risk Extreme Risk
Page 33 of 41

Appendix 4
Identification of Risk & Escalation Process
CCG Governing Body
Via risk/issue log; Practice Manager meeting item;
practice visits etc.
Identification of risk
Member Practices
Assurance Framework Corporate Risk Register
Executive Management Team Meeting
Executive Director
Teams
Audit Committee
Page 34 of 41
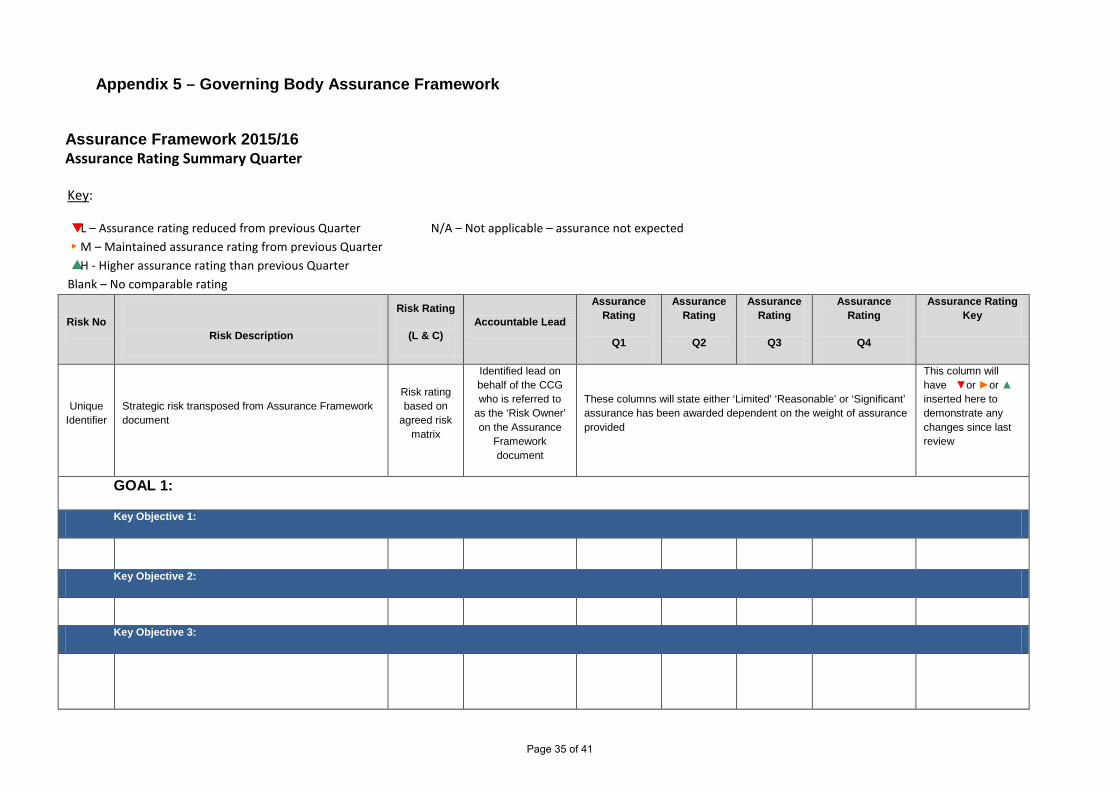
Appendix 5 – Governing Body Assurance Framework
Assurance Framework 2015/16 Assurance Rating Summary Quarter
Key:
▼ L – Assurance rating reduced from previous Quarter N/A – Not applicable – assurance not expected ► M – Maintained assurance rating from previous Quarter ▲ H - Higher assurance rating than previous Quarter Blank – No comparable rating
Risk No
Risk Description
Risk Rating
(L & C) Accountable Lead
Assurance Rating
Q1
Assurance Rating
Q2
Assurance Rating
Q3
Assurance Rating
Q4
Assurance Rating Key
Unique Identifier
Strategic risk transposed from Assurance Framework document
Risk rating based on
agreed risk matrix
Identified lead on behalf of the CCG who is referred to
as the ‘Risk Owner’ on the Assurance
Framework document
These columns will state either ‘Limited’ ‘Reasonable’ or ‘Significant’ assurance has been awarded dependent on the weight of assurance provided
This column will have ▼or ►or ▲ inserted here to demonstrate any changes since last review
GOAL 1:
Key Objective 1:
Key Objective 2:
Key Objective 3:
Page 35 of 41

Risk No
Risk Description
Risk Rating
(L & C) Accountable Lead
Assurance Rating
Q1
Assurance Rating
Q2
Assurance Rating
Q3
Assurance Rating
Q4
Assurance Rating Key
Unique Identifier
Strategic risk transposed from Assurance Framework document
Risk rating based on
agreed risk matrix
Identified lead on behalf of the CCG who is referred to
as the ‘Risk Owner’ on the Assurance
Framework document
These columns will state either ‘Limited’ ‘Reasonable’ or ‘Significant’ assurance has been awarded dependent on the weight of assurance provided
This column will have ▼or ►or ▲ inserted here to demonstrate any changes since last review
GOAL 2:
Key Objective 4:
Key Objective 5:
Key Objective 6:
GOAL 3:
Key Objective 7:
Key Objective 8:
Key Objective 9:
Page 36 of 41
Principal risks Risk owner
Risk status LxC=R
Key controls Assurances on Controls Key Positive Assurance (**External/ Independent)
Gaps in Control (GIC) or Gaps in Assurance (GIA)
Corrective Action Responsibility Target Date
Progress Reports Q1 Q2 Q3 Q4
Assurance rating
Goal 1:
Key Objective 1:
Responsible Committee:
2 x 4 = 8
Assurance Framework 2015/17
Page 37 of 41

Appendix 6 – Corporate Risk Register
NHS Knowsley CCG - CORPORATE RISK REGISTER 2014/15 ▼ Risk reduced
► Risk unchangedRESPONSIBLE OWNER: SENIOR MANAGEMENT TEAM ▲ Risk increased
ID Risk Description Committee Risk Owner
L C Initial Risk Rating
Current Identified Controls in Place L2 C2 Current Risk Rating
Additional controls required L3 C3 Target Risk Rating
Comments & progress in implementing additional controls
Change since last update
Page 38 of 41
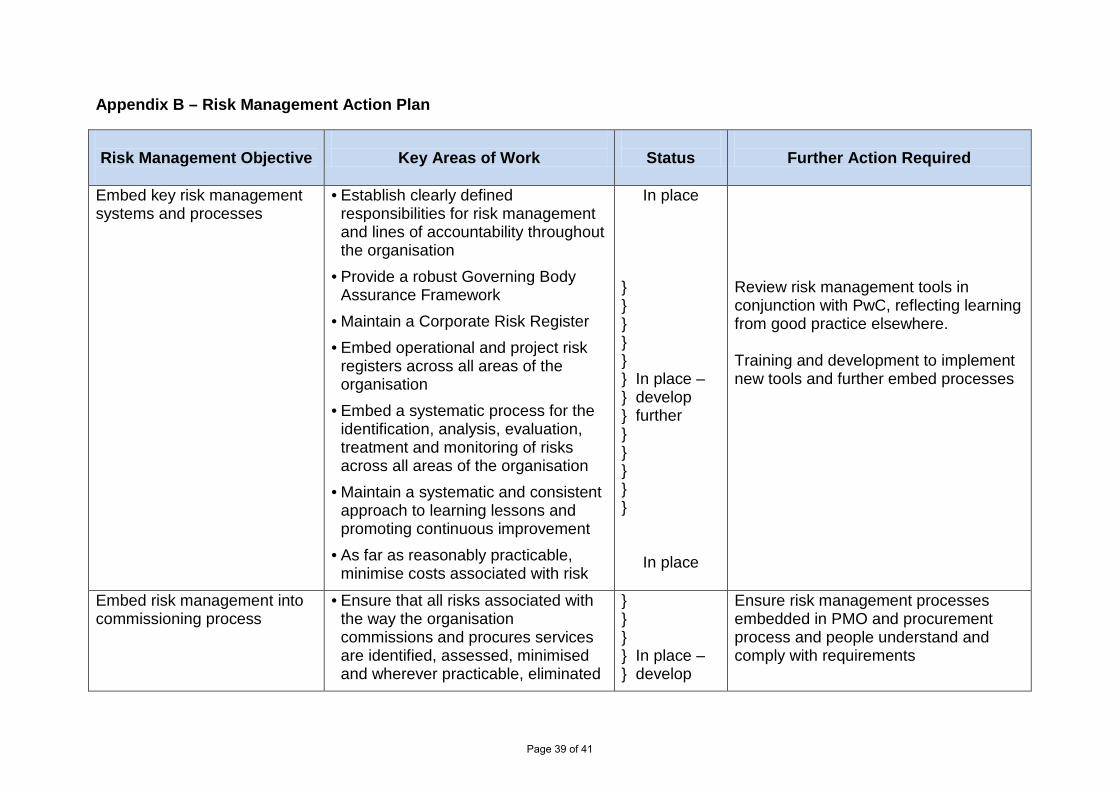
Appendix B – Risk Management Action Plan
Risk Management Objective
Key Areas of Work
Status
Further Action Required
Embed key risk management systems and processes
• Establish clearly defined responsibilities for risk management and lines of accountability throughout the organisation
• Provide a robust Governing Body Assurance Framework
• Maintain a Corporate Risk Register • Embed operational and project risk
registers across all areas of the organisation
• Embed a systematic process for the identification, analysis, evaluation, treatment and monitoring of risks across all areas of the organisation
• Maintain a systematic and consistent approach to learning lessons and promoting continuous improvement
• As far as reasonably practicable, minimise costs associated with risk
In place
} } } } } } In place – } develop } further } } } } }
In place
Review risk management tools in conjunction with PwC, reflecting learning from good practice elsewhere. Training and development to implement new tools and further embed processes
Embed risk management into commissioning process
• Ensure that all risks associated with the way the organisation commissions and procures services are identified, assessed, minimised and wherever practicable, eliminated
} } } } In place – } develop
Ensure risk management processes embedded in PMO and procurement process and people understand and comply with requirements
Page 39 of 41

• Ensure that the design and specification of new services and service re-design actively considers potential risks, including clinical, safeguarding and financial risks, and seeks to minimise or eliminate them
• Embed systematic processes for considering incidents in commissioned services, which compromise the safety and welfare of patients, children and vulnerable adults, and reflecting learning in current and future commissioning activity
• Promote active stakeholder involvement in risk management with particular reference to key partnerships
} further } } } }
In place – develop further
In place – develop further
Review of all open incidents to ensure learning reflected in current and future commissioning activity Build on existing examples of partnership risk management
Ensure that the CCG is ‘risk aware’ and the members of the governing body and staff are appropriately trained and skilled in risk management
• Raise awareness of risks and their management through a programme of communication and training
• Foster an environment whereby all governing body members and staff understand that risk management is their responsibility
} } In place – } develop } further } } }
Further Governing Body development session for discussion and development of assurance framework Skills transfer and staff development sessions
Ensure statutory and regulatory compliance
• Satisfy all mandatory and statutory duties and undertakings
• Satisfy the requirements of the
In place
In place
Page 40 of 41

Annual Governance Statement • Achieving and improving
performance against all internally and externally regulated risk management activities
• Ensure the health and safety of all those who work for or visit the CCG offices
In place – develop further
In place
Completion of development activity commissioned from PwC aims to further develop and improve risk management arrangements
Page 41 of 41

Document 33(03)08
Clinical Quality Committee
KEY ISSUES
Key Issues February 2015
5 PATIENT STORY
Paul Coogan shared with the committee a patient story from 5BPFT Physical Health Community Services.
6 PROPOSED WORK PLAN AND REVISED MEETING SCHEDULE Proposed Work Plan The organisation is currently reviewing all work plans across the CCGs governance structure and a new work plan for the Clinical Quality Committee is introduced to support the proposed revised meeting schedule Revised Meeting Schedule The name of the committee is to change to Clinical Quality Committee (CQC). It was agreed to meet bi-monthly. Agenda a 6 monthly review.
7 ASSURANCE FRAMEWORK AND RISK REGISTER The report presented the strategic and operational risks which are the responsibility of the Quality and Safety Committee for review. Given that only two months have elapsed since the last meeting, further reviews of the risk register and the assurance framework, currently underway; have yet to be completed, so the information is as presented at December.
8 SAFEGUARDING (ADULTS AND CHILDREN) Helen Smith provided an update in relation to children and adult safeguarding. The Safeguarding Service has provided feedback to the Trusts via the CQPG process throughout December 2014 and January 2015. Care Home Update A Core group to support both care homes has been established. This is led by the Interim Head of Safeguarding KMBC. An initial meeting has taken place with subsequent meetings to follow at three weekly intervals. The purpose of the meetings is to monitor and test the robustness of the standards and policies that are in place. Domestic Homicide – A report has gone to the Implementation Group for comment. Safeguarding Strategy All agreed more discussion was required to reflect on the content, if there are any issues and reflect response to OFSTED inspection.
9 LEARNING DISABILITIES UPDATE Helen Meredith Helen outlined the local plans that have been developed in the health sub group of the Knowsley Learning Disability Partnership Board. 10 MERSEYSIDE QUALITY SURVEILLANCE GROUP KEY ISSUES Helen Meredith
Helen stated that a review of QSG Effectiveness was carried out and following guidance from the National Quality Board the Terms of reference have been reviewed. 11 ACUTE SERVICES QUALITY REPORT & QUALITY DASHBOARD Dr Conway
Dr Conway explained that this briefing is based on information received from North West Commissioning Support Unit (NWCSU) who provide support to the CCG in monitoring the
Page 1 of 3

performance of acute care providers against the quality indicators within the NHS contract. Performance of key performance indicators and CQUINs are monitored through the provider CQPGs and were underperformance is reported; recovery action plans are agreed with providers and monitored closely. 12 MENTAL HEALTH QUALITY REPORT Dr Ayegba
This briefing is based on information received from North West Commissioning Support Unit (NWCSU) who provide support to the CCG in monitoring the performance of mental health care providers against the quality indicators within the NHS contract. Performance of key performance indicators and CQUINs are monitored through the provider CQPGs and were underperformance is reported; recovery action plans are agreed with providers and monitored closely 13 NHS SCREENING PROGRAMMES IN MERSEYSIDE Sarah McNulty
Dr Sarah McNulty updated the Quality and Safety Committee on NHS Screening Programmes in Merseyside: Annual Report 2013/2014. A fall in performance across three Cancer Screening Programmes was noted, accompanied by wide variation or uptake at practice level. 14 CQUIN SCHEMES
Although agreed there are five areas of high priorities which will undoubtedly improve outcomes for patients, discussions were on-going in terms of ensuring that data collection requirements were robust but not onerous for Trusts. 15 MEDICINES MANAGEMENT QUARTERLY UPDATE REPORT
Terms of Reference – Require further review and will be brought back to the next meeting. To be progressed against the work plan. Interface (Shared Care) – A policy to set out the position to be adopted is currently being reviewed. Rheumatology Shared Care Agreement – Following an incident relating to an incorrect RSCA posted on the pan Mersey Area Prescribing Committee Website the correct information will be circulated to GPs. Medicines Management Work Plan – Will be a regular item on the agenda and overseen by the Quality Committee. Community Pharmacy Audit - An audit was completed over the last six months to identify adherence by local, pharmacies to agreed practice principles. 16 MEDICINES MANAGEMENT WORK PLAN 2014-16 Dr Hossain
The purpose of the briefing describes in detail the key components of the 2014-2016 Medicines Management Work Plan. The plan has a significant thread throughout of increasing prescribing safety, increasing efficiency and reducing medicines waste. 17 HEALTH CARE ACQUIRED INFECTION (HCAI) ISSUES
The draft terms of reference for the HCAI Network which was requested at the December 2014 Quality Committee were reviewed. The committee held their first meeting on Tuesday 3 February 2015 (monthly thereafter). 18 PRIMARY CARE QUALITY NETWORK QUARTERLY QUALITY
REPORT
Dr Stokoe updated the Quality and Safety Committee on progress relating to Primary Care Quality Improvement, through the work of the Primary Care Support function and the CCG’s Primary Care Quality Network. The report included:
Page 2 of 3
CQC regulation and inspection of GP practices Prime Minister’s Challenge Fund Knowsley CCG has put in a bid and is awaiting the outcome. Personal Medical Services (PMS) Review The funding will remain in Knowsley at the discretion of the CCG over the next 4 years. Primary Care budget is an issue and we will need to manage it carefully. Diabetic Footcare Pathway Through work carried out by the Merseyside Diabetes Network and the Diabetes CRG has resulted in the development of a best practice footcare pathway. This has recently been approved by the PCQN and is due to be formally launched in March 2015. DXS Best Pathway During 2014 clinicians have been exploring the options available to enhance and support GPs during consultation in order to promote improved referrals, promote best practice, enhance patient support and effectively rationalise practice back office resources by reducing duplication of certain tasks Balanced Scorecard A visit to NHS Bolton CCG is being arranged to review their Balanced Scorecard and to assess the viability of developing something similar for Knowsley. The outcome from the visit will be shared with the PCQN.
NEXT MEETING To be confirmed.
Page 3 of 3

Document 33(03)09
Clinical Quality & Safety Committee Notes of Meeting: Friday 5th December 2014 1.30pm
Nutgrove Villa, Boardroom Present Apology
MEMBERS Dr Robin Macmillan Chair of the Committee - Secondary Care Doctor Dilys Quinlan Lay Member, Quality & Safety Ruth Austen-Vincent Lay Member, Patient and Public Involvement Dr Paul Conway Clinical Lead for Quality & Safety Ann Dunne Designated Nurse Safeguarding Children Dianne Johnson Accountable Officer, Knowsley CCG Sarah McNulty Public Health Consultant, Knowsley MBC Helen Smith Head of Safeguarding for Adults Dr David Stokoe Clinical Lead for Primary Care Quality Debra Lawson Head of Commissioning, KMBC Helen Meredith Interim Head of Quality & Safety/Lead Nurse
IN ATTENDANCE Jane Calveley Healthwatch Knowsley Paul Mavers Healthwatch Knowsley Paul Coogan Healthwatch Knowsley Philip Thomas Commissioning Director Andrew Thomas Governance Director Alistair MacFarlane Programme Manager, Knowsley CCG Janet Cummins Advance Care Facilitator, 5BPFT Dr Paul Barry End of Life Clinical Lead, Knowsley CCG Tom Fairclough Senior Programme Manager Ann Shone Note Taker ACTION
1 WELCOME & INTRODUCTIONS & APOLOGIES FOR ABSENCE Chair
Dianne Johnson acted as Chair in the absence of Dr Macmillan. The Chair welcomed all present to the meeting and round-the-table introductions took place. Apologies for absence were received from Dr Macmillan, Philip Thomas, Debra Lawson, Paul Mavers, Paul Coogan, Dr Stokoe, Jane Calveley.
2 DECLARATIONS OF INTEREST All
Individuals will declare any interest that they may have, in relation to
Page 1 of 9

a decision to be made in the exercise of the commissioning functions of Knowsley Clinical Commissioning Group, in writing to the governing body, as soon as they are aware of it and in any event no later than 28 days after becoming aware There were no declarations of interest raised during the meeting.
3 MINUTES AND MATTERS ARISING
The minutes of the last meeting dated 7th November 2014 were accepted as an accurate record.
4 MATTERS ARISING AND REVIEW OF ACTION LOG All
Matters Arising There were no matters arising. Review of Action Log Action: Helen Meredith to review the action log in order to close off outstanding actions before the next meeting.
Helen (M)
5 END OF LIFE – CARE AND COMMUNICATION RECORD
Dr Barry introduced the Care and Communication Record. Dr Paula Powell, Community Consultant for Palliative Care has developed, with support from the Advance Care Planning Team, a Care and Communication Record, to assist clinicians in meeting their responsibilities and helping give patients and families a voice in the planning of their treatment and care at End of Life. This document puts the person at the centre; focuses on the wishes and preferences of the person and those who are important to them; encourages a shared approach to care from all those involved; is a useful guide for health and social care professionals when planning and delivering care.
Janet Cummins explained that the Care and Communication Record is divided into sections and colour coded to guide its use. Where a doctor is in agreement that the person’s care should be supported by this Care and Communication Record they may document relevant conversations and their medical assessment in the blue headed sections. Nurses are asked to complete the green headed sections which relate to the assessment, agreed plan of care and daily care and review. The purple sections relate to the person and communication. This may be completed by the person (where they are able or wish to) or those who are important to them. Where they wish it these sections
Page 2 of 9

can be completed with the support of a health professional. Health and social care staff and person/carers may use the daily communication sheet to share information about the on-going care of the person. For health and professionals there is an Aide-memoire to act as a guide when planning and delivering care for a person and those who are important to them. At the back of the document there is a prescribing guidance (this is general guidance, the person may require different medication that is individual to their needs). It is proposed the Care and Communication record be supported by Knowsley CCG, this support is primarily related to the launch, awareness and education necessary to ensure the document is used effectively and appropriately. The launch and training would aim to include, patient and patient representative groups (e.g. Healthwatch), Community Nursing, GPs and Primary Care, Care Homes, Domiciliary Care Staff and Acute staff.
The majority of the training and support would be provided by the Integrated Advance Care Planning Service, although this is limited by the capacity of this service to provide training across such a wide and diverse group of staff, the ability of providers to release staff for training opportunities may also be a barrier. Such an approach also necessitates the utilisation of the CCG’s communication channels. There is a need for Primary Care to access support training and awareness opportunities to promote the record, as well as to relevant provider organisations who may utilise the document. Such opportunities might include the use of a Protected Time event or GP forums. To provide assurance in relation to the use of the document it is strongly advised that it will need to be audited and evaluated a role which has previously been undertaken for Knowsley by the Advance Care Planning Team in relation to other similar EOL tools. Dr Conway asked how is DNACPR and the pathway are going to be captured. Janet advised that this can be found within the document. Dr Conway also asked how people will be monitored to ensure they complete the document. Dr Barry responded it will be audited. Helen (M) asked how patients and carers had been consulted. Janet replied that an aide-memoire had been taken to health forums. Dilys Quinlan said it was an excellent document but there is a need for people to write clearly in the notes. Dr Barry explained that we have to do this and do it better and it all comes down to the communication skills courses we should all go on. Ruth Austen-Vincent said Healthwatch are holding a public event around domiciliary training and how that is going to fit with the way of working.
Page 3 of 9

Ruth reminded the group that there was a need for conversations with Learning Disability Groups and this was recognised as a specific piece of work that needs to happen. Dianne stated that with regard to the launch event we must continue to raise awareness of the new way of working. Dianne thanked the committee for being supportive of this work. We now need to put into practice the training needed and be very clear what the resource requirements are. The timescale to implement is February/March next year. Action: Update paper to be scheduled for April 2015 on actions completed.
Dr Stokoe
6 PATIENT STORY
Item deferred to next meeting.
7 PRIMARY CARE – MEDICINES MANAGEMENT WORK PLAN
Andy explained that due to a number of changes within the Medicines Management team, it has been decided that this is an appropriate time to review the medicines management function and so an independent review will take place in the new year. This will ensure we can look at best practice and different models of providing practice level support before determining which option will best suit the organisation going forward.
In order to ensure the CCG has sufficient Medicines Management cover during this review period Dr Hossain and Jo O’Brien have carried out a mini procurement, with the result that with effect from 01/12/2014 there will be additional support. Mark Pilling will be supporting Graham Pimblett and working on delivery of key aspects of the Medicines Management work plan.
It is proposed that a delegated sub-group of the Quality & Safety Committee be set up to take forward the work of assuring the committee that the Medicines Management work plan is robust, and also providing assurance to the Finance & Performance Committee that the financial risk is properly addressed. It is also proposed that this group comprise Dr Aftab Hossain, Dianne Johnson, Dilys Quinlan, Su Bramley, Andrew Thomas, Jo O’Brien. The committee is requested to delegate authority to Dianne Johnson, supported by the aforementioned sub-group, to approve the plan. Action: To be brought back to Clinical Quality & Safety Committee in February 2015.
Dr Hossain
Page 4 of 9
Helen (M) felt practice nurses and non-medical staff need to be included in the sub-group. Dianne stated that HCAI also needs to link in with this work. Helen (S) said that there needs to be consideration around the number of Medicines Management safeguarding alerts.
8 MENTAL HEALTH SERVICES
Alistair MacFarlane explained that this briefing is based on information received from North West Commissioning Support Unit (NWCSU) who provide support to the CCG in monitoring the performance of providers against the quality indicators within the NHS contract. Clinical Quality and Performance Group (CQPG) meetings with commissioned Providers continue to oversee performance of quality.
The concerns highlighted within this report continue to be monitored by CQPG and where necessary are reported into contract meetings for relevant contractual action.
Staff Sickness levels at Five Boroughs and Mersey Care and performance against First Episode Psychosis are areas of concern. The implementation of Friends and Family Test for mental health services will commence from January 2015 but both Providers appear to be prepared. The 5 Boroughs Quality and Assurance Task and Finish Group will continue to work with the Trust to receive and review evidence to provide full assurance against the key areas of concern identified by the Single Item Quality Surveillance Group.
Performance of key performance indicators and CQUINs are monitored through the provider CQPGs and where under-performance is reported; recovery action plans are agreed with providers and monitored closely. Dianne suggested that numbers are displayed as percentages. Action: Dr Ayegba to request both numeric and percentages are included in future reports. Dianne said it is good to see the providers’ trends and themes.
Dr Ayegba
9 SAFETY – LESSONS LEARNT
Andy introduced a paper in relation to a Lessons Learnt event he attended hosted by NHS England on 10th September 2014. This paper has already been to PART B of November’s Clinical Quality & Safety Committee. There were 3 relevant sessions within the event.
1. Perspectives from hundredfamilies.org, which supports families of victims of mental health homicides.
Page 5 of 9

2. An overview of the National Confidential Enquiry (NCI) into
mental health homicides by the Centre for Mental Health and Risk at the University of Manchester.
3. Perspectives on communication and engagement with perpetrators, their families and the families of victims.
The Hundredfamilies website provides practical information for families affected by mental health homicides in Britain. The website also provides evidence-based analysis, resources and information for mental health professionals. A key theme of the presentation was a challenge to providers and commissioners that the families of victims are generally poorly served by the processes in place within the NHS. Often families feel powerless and have no control, and find it difficult to access information. It was observed that many investigations took an inordinately long period of time to be competed and reported. The average is 51 months with a range from 19-110 months. The victim’s family are often not involved. A Hundred families research into 108 reports showed that 40% of families had no involvement, 30% were just presented the final report, and only 30% were involved at an early stage. Additionally there is a strong sense that the appropriate lessons are not being learnt and shared, with a common theme being a failure by Trusts to learn from serious untoward incidents, as evidenced by a large degree of commonality between investigation findings. A 2010 report on independent investigations stated that ‘care planning, risk assessment, communication, information sharing and working with families and carers are all basic procedures which should form the bedrock of a well-functioning mental health service and they should no longer be appearing in recommendations with such frequency’. Of all homicides in the UK (approximately 11,000 in the UK from 1996-2012) 10% are committed by people in contact with mental health services. Primary diagnosis in patient homicide includes, drug and alcohol dependence, and schizophrenia. Overall there is a downward trend, with fewer mental health homicides each year than a decade ago. It is hypothesised that this is due to better care and multi-agency working, and possibly increased use of Community Treatment Orders, in essence protecting the public through treatment of perpetrator. Helen (S) explained NHSE had queried some of the information on the website. Ruth responded that it is an important issue being raised and even if information is not accurate it should not become the focus of the conversations. The most important point is that this work is valued and taken forward.
10 ACUTE SERVICES
Dr Conway explained that this is the latest information received from North West Commissioning Support Unit (NWCSU) who
Page 6 of 9

provide support to the CCG in monitoring the performance of acute care providers against the quality indicators within the NHS contract. Each of the issues and concerns are managed through Clinical Quality & Performance Group. Dr Conway asked the committee if they had any questions. Dilys Quinlan referred to the National CQUIN on Dementia and asked what is involved. Dr Conway advised it included identifying patients and referring them to appropriate services - (Fair, find, assess investigate and refer). Also there is a need to have a clinical lead and appropriate training along with carers support. Sarah McNulty referred to page 9 Pneumonia AQ and asked what the issue is in relation to smoking cessation. Dr Conway stated it was a data collection issue not a problem with requests. Ruth referred to the Friends and Family Trust (FFT) and said it did not explain the new target. Dr Conway advised the target is number of patients completing the FFT not the quality of returns completed. Mortality at Aintree - Dr Conway explained the Trust had provided an update to the CQPG and Aintree Collaborative Commissioning Forum had written to the Trust and more work is underway. Dilys asked what the outcome of the cancelled referral was for the patient. Dr Conway to find out and feedback. Action: Dr Conway to find out and feedback to the committee.
Dr Conway
11 SAFEGUARDING ADULTS AND CHILDRENS REPORT
Helen (S) provided an update in relation to children and adult safeguarding. The Quality and Safety Committee has previously received a report at the November committee meeting in relation to two BUPA owned care homes; Hillside Care Centre and Arncliffe Court. Both Care Homes have in place a suspension on new placements and are under a multi- agency management review process led by Knowsley local authority. A professionals meeting immediately followed by a management review meeting to discuss both care homes has been held in November. BUPA representatives were invited to attend the management review meeting. Similar quality and safeguarding concerns have been raised within both care homes. Monitoring visits to both homes continue to take place. Professionals visiting the homes report a measure of improvement in some areas but this was not agreed to be either of any consistency or sustainable. In addition the meeting was made
Page 7 of 9

aware that Arncliffe Court had received a warning notice from CQC. The care home has a right to respond to the notice and the CQC report is not publically available and therefore was not further discussed within the meeting. Helen said staff are very good but they are not supported by management. The management are doing a lot of strategic work and this is not translating down to staff in the home. Helen stated that a core group is to set-up 3-weekly meetings with the first meeting held on 18th December 2014 to give a focus for everybody involved to keep homes on track. Dianne asked how the Core Group is going to report into the CCG. Helen to find out and make Dianne aware. Action: Helen (S) to find out and feedback to Dianne Johnson. Child Sexual Exploitation (CSE): Knowsley Safeguarding Children Board has commissioned an Independent review of the CSE arrangements across the Borough which the CCG are supporting. It is essential that organisations understand the CSE profile of the borough as this will have a significant impact on the commissioning of any new services or redesign of current services. There will need to be particular regard to mental health and therapeutic service provision. Safeguarding Children training: the CCG are currently 94.1% compliant with the mandatory level 1 training. Dianne mentioned there are other forms of CHILD EXPLOITATION which are sometimes related.
H(S)
12 HEALTH CARE ACQUIRED INFECTION (HCAI)
The action plan is to be implemented through sub group. Action: Helen (M) tasked with leading and establishing a sub group.
Helen (M)
13 GOVERNANCE
Andy shared with the committee an extract of the Governing Body Assurance Framework and Risk Register relevant to the Clinical Quality & Safety Committee and asked the committee to review the risks, including assessments and risk levels and current and planned controls and consider whether there are any further risks in relation to the work of the committee which has not been captured. Action: To review the Risk in relation to the Engagement Plan and amend timescales accordingly.
AT
Page 8 of 9
14 EMERGENCY PLANNING RESPONSE AND RESILIENCE (EPRR) ASSURANCE
Andy stated that the report contains the submission to NHSE England of Knowsley CCG’s statement of assurance around EPRR. The submission provides notification of full compliance with the relevant standards and identifies a series of development actions which the CCG intends to take forward to ensure the CCG remains compliant with the relevant standards and requirements. Andy explained to the group that appropriate training and awareness for on-call officers and CCG staff is in place and will be provided as required on an on-going basis to ensure the Accountable Officer can meet the statutory guidance requirements and thereby provide the Governing Body with appropriate assurance of statutory compliance. There are only 4 areas of actions outstanding (shown below) which will be taken during the course of next year.
1. Assessment and update to the risk reduction objectives 2. Additional Training Needs Analysis and schedule additional
training 3. Further Training Needs analysis to be carried out. Joint
Emergency Services Interoperability (on-call) 4. On call personal are required to keep details of training in a
Personal Development Plan (PDP). Sarah said in readiness to respond to emergency situations it would be beneficial to be issued with lessons learnt from previous simulation events. Action: Dianne to circulate Lessons Learnt.
DJ
15 ANY OTHER BUSINESS
Dilys informed the committee that a BBC investigation has found errors in the CQC GP Intelligence Monitoring data methodology which was launched last month on the website and the CQC have been forced to apologise. Action: Dr Stokoe to provide further information on how this may have impacted on Knowsley CCG member practices recently reviewed by the CQC.
Dr Stokoe
DATE & TIME OF NEXT MEETING
Friday, 6th February 2015, 1.30 pm Boardroom, 1st Floor, Nutgrove Villa, Westmorland Road, Huyton. L36 6GA
Page 9 of 9

Document 33(03)10
NOTES OF THE FINANCE & PERFORMANCE COMMITTEE held on Thursday, 8th January 2015 in the Boardroom, Nutgrove Villa
Present Apology
MEMBERS Su Bramley F&P Committee Chair/Lay Member –
Audit & Governance
Dianne Johnson Accountable Officer Dr Ronnie Thong GP/Clinical Lead – Planned Care &
Patient Engagement
Dr Simon Perritt GP/Clinical Lead – Unplanned Care Paul Brickwood Chief Finance Officer Clare Barrow Head of Finance & Contracts Richard Holford Head of Public Health Strategy and
Intelligence
Philip Thomas Commissioning Director
IN ATTENDANCE Dr Andrew Pryce CCG Chair Andrew Thomas Governance Director Julie Moss Director of Integrated Services, KMBC Helen Davies North West CSU Mervyn Kennedy North West CSU Joanne Serridge Finance Manager, Knowsley MBC Sally Hobbs Interim Head of Service Transformation,
Knowsley MBC
Mark Pilling Interim Medicines Management Team Leader
Lorraine Frodsham Note Taker Action 1. Apologies for Absence Apologies for absence were received from Su Bramley, Dr Pryce
and Paul Brickwood. Dianne Johnson informed that she would be Chairing the meeting in Su Bramley’s absence. Introductions were made around the table.
2. Declarations of Interest Mark Pilling declared an interest as he is a Director of a
Medicines Management service and Mervyn Kennedy declared an interest with regard to his work for other CCGs.
3. Minutes of the Meeting Held on 13th November 2014
Page 1 of 11
The minutes of the meeting held on13th November 2014 were accepted as a true and accurate record.
4. Review of Action Log Workplan on Prescribing Overspend – Dianne Johnson
informed that the Quality & Safety Committee delegated decision making around the workplan to a sub-group of that Committee. The Chair of this Committee is also a member of the sub-group. This item to be removed from the log. Detail Regarding Triage Sessions – Helen Davies said that investigations had revealed that some triage sessions had been incorrectly recorded as being converted into procedures but she hoped that changes in data quality will resolve this issue. This item to be removed from the log. Terms of Reference – Dianne Johnsons said that the typos identified had now been corrected. She also informed that she had spoken to Dr Pryce and clarified that he was not a formal member of the Committee but as Chair of the CCG he was free to attend and participate in any CCG Committee meeting. He would, therefore, not be added to the membership of the F&P Committee. This item to be removed from the log. Commissioning Plan Template – Philip Thomas said that he would discuss this under the later agenda item on this issue. This item to be removed from the log. 5BPFT Report on MH Bed Usage – Clare Barrow informed that she had received this report yesterday and she would now share this with the appropriate people. Philip Thomas said he’d had a conversation with John Heritage from 5BPFT about the wider work around beds both in and out of Borough. This item to be removed from the log. StHK Dermatology HRGs – Helen Davies said she was currently working on the Month 8 contract performance report and would ensure that this was included in that report. This item to be removed from the log. Finance & Performance Committee Risks Report - Andy Thomas informed that the amendments suggested to the format of the report were in hand and the quarter 3 refresh will incorporate these changes. This item to be removed from the log. Other Payments to Council – This information had only been received this morning so this was tabled at the meeting. There were some queries regarding the information and Philip Thomas and Clare Barrow will look into these further and report back to the next meeting. This item to remain on the log.
Page 2 of 11

5. Commissioning Plan Progress Update Philip Thomas presented this report to provide the Committee
with an update on progress made to implement the CCG’s commissioning intentions. He explained that originally the plan was for 2014/15 but this may now be extended to 2014/16. As requested at the last meeting, the previous and current RAG ratings were now shown. Regarding interdependencies, Philip Thomas said work was taking place to look at how the Programme Management Office could be used to draw these out and think about how they are reflected in the outcomes going forward. Regarding Intermediate Care, this was currently showing a red RAG rating and Philip Thomas explained that this was due to the fact that a number of schemes were not yet up and running relating to additional GP hours at two further locations: Halewood and Whiston. Regarding the Primary Care IM&T Plan there was an issue regarding telephone lines capacity and this had been flagged up with the Health Informatics Service (HIS). Dr Perritt queried whether they had been pushed on what the issue was as he felt this was a relatively simple matter which should have been resolved by now. Philip Thomas said that a response from HIS had not been forthcoming despite a number of requests being made. Consideration was now being given as to whether to escalate this. Dr Thong commented that he thought the format of the report very good, however, Dianne Johnson pointed out a number of typos which Philip Thomas agreed to correct. Dianne Johnson said that with regard to the Risk/Issues column, she thought it needed to be clearer that they are mitigating risks. Philip Thomas and Andy Thomas agreed to look at this. Clare Barrow thought it would also be beneficial to identify any financial plans for each of the schemes and Philip Thomas agreed to add this. Action : Typos to be corrected and amendments/additions as discussed to be actioned. The Finance & Performance Committee noted the progress made against key programmes within the commissioning plan.
PT/AT
6. Finance Report – Month 8 Clare Barrow reported an overall surplus in relation to both
Page 3 of 11

programme and running costs of £1.7 million at month 8 and she said that the CCG was still on track to achieve the 1% surplus. She also informed that the risk around achieving this surplus had reduced from month 7 to month 8. NEL over-performance at Aintree continues to be a significant contributor to the over-performance on Acute contracts and South Sefton CCG, as co-ordinating commissioner, has raised a contract query with the Trust regarding this. A response has been received from the Trust which includes a proposal to block NEL over-performance at month 6 which would result in a reduction of approximately £800,000 for Knowsley. Commissioners have agreed to accept this block offer. The main over-performance at StHK relates to planned care, and in particular outpatient attendance and outpatient procedures. The Trust is still in the position of ‘escalated negotiations’ and Paul Brickwood is working with Damien Finn (Trust DoF) to agree the outturn position. Once this is done the year end settlement can be agreed. Primary Care budgets reported a year to date deficit of £104,000 to month 8, with the prescribing overspend (£316,000) being partially offset by an underspend on the Home Oxygen contract (£192,000). PPA information to month 6 was used to forecast the prescribing position but the month 7 report has now been received which includes the anticipated Category M price increase and this suggests a deterioration in the forecast outturn of approximately £400,000. The CCG remains within the running cost allocation and reports a year to date underspend of £263,000 to month 8. The CCG has reached an affordable agreement with the CSU regarding the SLA value for 2014-2015 which totals £1.0 million. However, the CCG awaits a detailed financial schedule regarding stranded costs but it is not expected that this will vary significantly from the estimate previously provided. The CCG has set a financial QIPP target of £9.69 million in 2014/15 which is net of investments of £1.05 million. The CCG has utilised slippage from reserves to meet the year to date gap in expected savings. The Finance & Performance Committee noted the content of this report.
7. Contract Performance – Month 7 Helen Davies said that the CCG was achieving 100% in relation
to the Mental Health CPA target of patients being visited within 7 days of discharge. IAPT performance is improving and a
Page 4 of 11

recovery plan is in place. However, the prevalence rate and waiting times remain an issue. Philip Thomas advised that the IAPT performance for 2014/15 would be based upon quarter 4 performance, with the provider confident it would achieve the required performance in quarter 4. Regarding community contracts, COPD/CVD/Diabetes are all performing well. However, the diabetes contract query will remain open until Aintree has sufficiently demonstrated that it can meet the information requirements of the contract. The Knowsley CVD model has been positively received at the national British Association for Cardiac Prevention and Rehabilitation Conference and the service is already achieving Year 5 targets in virtually all KPIs. The COPD contract has achieved a 13.3% reduction in COPD emergency respiratory bed days between years 2 and 3 for the cohort of patients registered for the service. There has also been a 29.5% reduction in admissions for the same cohort over the same period. Dianne Johnson said that in the earlier finance report it was stated that the CCG was not meeting its QIPP target in relation to CVD/COPD and she queried how this was possible given the reductions mentioned. Clare Barrow thought this may be due to a cohort of patients not known to the service being admitted. Helen Davies said that Aintree had been challenged on the fact that diabetes patients were being discharged to secondary care services as opposed to community services. Assurance had been received from the Trust that this will be reviewed and that a reduction will be seen in the numbers being discharged to secondary care services. Dianne Johnson queried whether other Trusts were referring into their own secondary care services. Helen Davies agreed to look into this and report on this in the month 8 report. Two contract queries remain open in relation to the 5BPFT contract. All outstanding reviews have now been completed and CHC assessments are now part of the District Nursing workload. There is still some concern around Mental Health and elderly patients being picked up but things have improved significantly. The Walk-In Centre contract query can now be closed and Helen Davies will produce a formal letter for Dianne Johnson to sign. Regarding complaints relating to the Podiatry Service, Kath McEvoy is to meet with the Service Manager to investigate these further. Andy Thomas said that in terms of the IAPT recovery plan, the percentage of people entering treatment and recovery rates were still not at the level the CCG would expect. He said the
Page 5 of 11

recovery plan needed to be looked at and where this will be by year end. Helen Davies agreed to include this in the month 8 report. Dr Thong said that patients who are being discharged from Merseycare are now supposed to self-refer to the IAPT Service and he queried how we can keep track of the numbers. He also felt that it was not appropriate for patients with severe issues/problems to self-refer. Dr Perritt said there was a higher take-up if patients self-refer as they can pick a time which suits them and that it would be the responsibility of the provider to count the numbers attending irrespective of the route of the referral. Sally Hobbs queried how the recovery rate was measured and Andy Thomas said that when people enter the service there is certain criteria which have to be met for them to go into the service. The recovery is based on the response to a set of questions asked at the start and end of treatment. Dr Thong queried whether there was any measure regarding patients coming back into the system. Dianne Johnson said work was being undertaken on the various measures and a report was to go to the Governing Body on this issue. Mervyn Kennedy said that in relation to Acute performance, at month 7, the CCG is showing a significant overspend on several Trusts totalling £2,571,000. The largest over-performance is at StHK Trust and Aintree, and to a lesser extent Liverpool Women’s, Fairfield and the Royal. As mentioned previously StHK Trust are still involved in the escalated negotiations process. Regarding the Warrington over-performance issue, as discussed at the last meeting there seems to be some correlation between under- performance at Fairfield and StHK Trust particularly around T&O. It seems that this relates to referral patterns changing with patients wanting to be treated closer to home and quicker. Clare Barrow said that critical care was significantly underspent at Warrington and Warrington CCG, as co-ordinating commissioner, has been asked for more information with regard to this but it maybe that the plan needs adjusting. A snapshot of performance against the main KPIs was provided in the report and Mervyn Kennedy briefly went through these. Detailed information on all of these areas was contained within the report. Action : Investigation to be undertaken to see if Trusts are referring into their own secondary care services. To be reported in the month 8 report. Action : Letter to be produced relating to closure of the Walk-In Centre contract query for Dianne Johnson to sign. Action : Detail regarding the IAPT recovery plan and position
HD
HD
HD
Page 6 of 11

at year end to be included in the month 8 report.
The Finance & Performance Committee noted the content of
this report.
8. Contract Negotiations Philip Thomas explained that the CCG holds a number of one
year contracts with a range of acute, mental health and community providers of NHS services. Each year these contracts need to be reviewed and re-negotiated. Details of the providers and current values for contracts subject to the renegotiation process were provided in the report as well as key negotiation issues and the approach being adopted by the CCG to agree new contracts for 2015/16 and progress to date. Andy Thomas asked how confident the CCG was that it would be able to keep to the deadlines contained in the guidance received in terms of sign-off of contracts etc. Clare Barrow said traditionally the sign off of the major contracts such as with Aintree and StHK Trusts had been delayed and not met the deadline but it was hoped to avoid that this year. Normally sign off is delayed due to the financial plans not being agreed and so it was hoped to have these discussions earlier on in the process to avoid any problems in sign off. Mervyn Kennedy said he had attended a meeting this morning where the level of sustained growth going into 2015/16 was discussed and he thought this would be very challenging. The Finance & Performance Committee noted the content of this report.
9. Programme Budgeting 2013/14 Clare Barrow presented this report to the Committee for
information. She explained that the programme budgeting data return is an analysis of commissioning expenditure by healthcare condition. There are currently 23 programme budgeting categories based on the World Health Organisation International Classification of Disease and that many of the categories contain sub-categories. The report contained a table which provided an analysis of net expenditure for Knowsley CCG’s population across the 23 categories which totals nearly £246 million. The top three areas of expenditure for Knowsley CCG are Other £57.5 million, Mental Health Disorders £30.2 million and Problems of the Gastro Intestinal System £17.8 million. Examples of spend classified as Other are Acute expenditure, community expenditure, emergency
Page 7 of 11

transport, non-NHS healthcare, prescribing, clinical supplies and services, premises and primary care LES. As 2013/14 was the first year that Programme Budgeting data was collected there was no previous year’s information to carry out benchmarking. However, the report contained a comparison between Mid Mersey CCGs which showed that both St.Helens CCG and Halton CCG have the same top 3 categories of net expenditure. A further comparison has been carried out locally of Merseyside CCGs and this was also included in the report. Benchmarking information across CCGs nationally is still being compiled by NHS England, but hopefully should be received by the end of January. Once these results are available they will be assessed to see if Knowsley CCG is an outlier in any of the categories. Andy Thomas queried whether spend –v- outcomes would be included in future reports. Clare Barrow said that the Shared Finance Team produce this report and she would ask them if they had been advised whether this would be reported in the future. Action : Clarify what information is to be included in future reports. The Finance & Performance Committee noted the content of this report.
CB
10. Prescribing Budget Update Mark Pilling presented this report to update the Committee on the
prescribing budget position at month 6. He explained that the Knowsley CCG prescribing budget for 2014/15 is £30,525,708 and that the current forecast position for the GP Practice prescribing budget is an underspend of £117,000. However, the budget position of the commissioned services (e.g. CVD/COPD) is currently forecasting an overspend of £280,000 primarily as a result of 5BP non-medical prescribing and expenditure by the South Knowsley Community Drugs Team. This equates to a total forecast overspend of £163,000. Mark Pilling said the Medicines Management Team continue to work with Practices to establish cost efficiency areas and supporting implementation but he felt there was perhaps a need to focus the work of the team in future to perhaps Practices with a significant overspend position. He said that the savings delivered by the Medicines Management Team this year will be in total of £500,000. Scriptswitch is a ‘prescribing decision support’ software tool that all Practices can access and it ensures that the most cost effective, evidence based products are identified, allowing prescribers to make prescription changes at the point of
Page 8 of 11

prescribing. However, a delay in Scriptswitch being reactivated following Practice migration to EMIS web has resulted in lower than expected cost savings. Savings are still expected to be around £100,000 this year from use of this system. The CCG also has in place a Primary Care Quality Premium that incorporates a prescribing component to support high quality and safe prescribing. Discussion took place on the possibility of targeting the Medicines Management Team resources to Practices where prescribing costs are higher than average so that the return/savings achieved will be greater. At this point Dr Thong and Dr Perritt declared an interest. Dr Perritt said he could see the wisdom in targeting particular Practices but unfortunately some GPs income is tied to prescribing quality so if they do not receive the support they need this may lay the CCG open to criticism. Dr Thong commented that a lot of the EatPMC Practices seemed to be spending large amounts. Mark Pilling advised that currently the Medicines Management Team have no input into these Practices. Dr Perritt said that there seemed to be massive variations in over and underspends with one Practice having an overspend of almost twice their budget. Mark Pilling thought there might be an anomaly in prescriber codes which was the cause of the overspend at that particular Practice. Philip Thomas asked for clarification about the purpose of the Medicines Management Team. Mark Pilling said it was to provide advice and support to Practices to ensure that the quality of prescribing is at its best and follows good practice. The team also promote and educate good practice and benchmark variation from good practice. They also provide a hands-on resource for cost savings opportunities. Dianne Johnson said that this whole issue needs to be looked at in more detail and a decision made on the way forward. The workplan that is being produced will highlight a lot of the issues discussed and where it is obvious that waste and overspends can be reduced. The Finance & Performance Committee noted the prescribing budget position and the actions undertaken to manage prescribing.
11. Better Care Fund Update Philip Thomas presented this report to advise the Committee that
confirmation has been received that the BCF plan has been approved following the latest submission on 28th November 2014. The letter from NHS England confirming this was attached to the
Page 9 of 11
report and this letter also advised of the standard conditions which apply to all BCF plans. Dianne Johnson wished to record her thanks to everyone involved in producing this plan as there had been a lot of hard work done on this. Andy Thomas said there was an expectation that all CCGs would look at their targets to see whether or not these were realistic. The Finance & Performance Committee noted the ‘approved’ status of the Better Care Fund Plan.
12. Section 256 Report Julie Moss presented this report which detailed the proposed
allocation of NHS Transfer Funding for Social Care 2014/15 (including Better Care Fund implementation funding). The report also provided details on how these resources will be allocated in order to maximise impact across the Borough. This will be an agenda item at the Health & Wellbeing Board on 29th January 2015 when it will be formally agreed and then submitted to NHS England to agree the transfer of money. Dianne Johnson said the CCG needs to gain assurance about the health outcomes this money will provide, i.e. reduced admissions etc. Philip Thomas said that the scorecard showed a downward trend in terms of some performance and action needs to be taken to improve this or maintain performance. He said that at the Pooled Budget Governance Group the scorecard had been reviewed and a suggestion made that further work was required to make sure that a performance analysis was produced. He said that as we move forward we need to link the money with the outcomes in its entirety and trends need to be plotted. A type on page 2 of Appendix 2 (Memorandum of Agreement) was pointed out (2013/14 should be 2014/15). This will be corrected. Dianne Johnson said that Su Bramley has asked her to raise an issue on her behalf in her absence. She would like to know how the LA and CCG get to a position where we can equally be fully assured around what this money is actually delivering. She felt that reporting should include all pooled budgets, other spend and the BCF so that we can get a feel of the difference these schemes are making to the population of Knowsley. Discussion then took place on the role of the Pooled Budget Governance Group. Dianne Johnson commented that traditionally the Pooled Budget Governance Group mainly focused on finance but it now needs to do more than this and include activity outcomes, quality
Page 10 of 11
and safety issues as well as finance. She felt that the membership of this group should be looked at again to ensure that these areas were covered, and the group may want to involve independent scrutiny also. From April 2015 this group will also need to report into the CCG’s Governing Body. It was agreed to raise this issue at the Pooled Budget Governance Group on 12th January 2015. Action : Typo on Appendix 2 to be amended. Action : Membership and role of Pooled Budget Governance Group to be discussed at the meeting on 12th January 2015. The Finance & Performance Committee noted the content of this report.
JM
PT
13. Items for Receipt There were no items for the Committee to receive. However, it
was agreed that future meetings would receive the minutes of the main Contract Review Boards. Action : Receipt of these minutes to be added the agenda format.
LF
14. Any Other Business Andy Thomas asked if the Committee felt that the Risk Register
and BAF were capturing everything they should. Dianne Johnson said she felt that Pooled Budgets should be included. Action : Pooled Budgets to be added to the Risk Register and BAF.
AT
15. Date and Time of Next Meeting 25th February 2015 at 1.00 p.m. in the Boardroom, Nutgrove Villa.
Page 11 of 11

1
Health and Wellbeing Board
Minutes of the meeting of the Full Board held on Thursday, 11 December 2014 in the Council Chamber, Municipal
Buildings, Huyton
Present:
Knowsley Metropolitan Borough Council – Elected Members Councillor Michael Murphy, Cabinet Member for Health & Social Care (Chairperson) Councillor Ron J Round, Leader of the Council Knowsley Metropolitan Borough Council - Officers Matthew Ashton, Assistant Executive Director (Public Health & Wellbeing) Julie Moss, Assistant Executive Director (Adult Social Care Knowsley Clinical Commissioning Group Dr Andrew Pryce, Chair of Knowsley CCG (Vice-Chairperson) Dianne Johnson, Accountable Officer Dr Ronnie Thong, Clinical Lead for Strategy and Planning Ruth Austen-Vincent, Lay Member for Public and Patient Involvement Healthwatch Knowsley Mary Spreadbury, Chair of Healthwatch Knowsley Engagement Forum Vicki Hornby NHS England Anthony Leo, Director of Commissioning, NHS England
In attendance:
Knowsley Metropolitan Borough Council – Supporting Officers Richard Holford, Head of Public Health Strategy and Intelligence Trudy Bedford, Scrutiny and Partnerships Officer

2
Knowsley Clinical Commissioning Group Alex Robertson, Interim Programme Manager, Respiratory Care 5 Boroughs Partnership NHS Foundation Trust Steve Hull, Assistant Director of Nursing and Safeguarding Healthwatch Knowsley Jane Calveley, Research & Policy Officer
Apologies:
Knowsley Metropolitan Borough Council – Elected Members Councillor Gary See, Cabinet Member for Children and Family Services Knowsley Metropolitan Borough Council - Officers Paul Boyce, Executive Director (Children) Knowsley Metropolitan Borough Council - Supporting Officers Mark Butterworth, Assistant Chief Executive
35. DECLARATION OF INTERESTS
What was this
item about?
This was a standard item to enable Members of the Board to declare
any interest they may have in terms of business on the agenda for
the meeting.
What was
agreed?
There were no declarations of interest submitted by Board Members.
36. MINUTES OF THE FORMAL MEETING - 12 NOVEMBER 2014
What was this
item about?
The minutes of the formal meeting held on 12 November 2014 were
reported back for consideration.
What was
discussed?
A Board Member sought clarity on Minute 31 – Pharmaceutical
Needs Assessment, and the request made at the previous meeting of
the Board for accessible versions of the PNA consultation document
to be circulated to disabled groups had not yet been received.
The Board was informed that the Physical Disabilities Board could
consider the PNA consultation document at a future meeting. To
enable this to take place the consultation period could be extended
beyond the current deadline of 6 January 2015.
Furthermore, the PNA consultation document would be adapted into
an accessible format and circulated to those groups who had not yet
been able to consider the consultation document. The Board was

3
also reassured that all future consultation exercises arranged by
NHS England (Merseyside) would be available in accessible formats.
In relation to Minute 29 – Grow Well: 5 – 19 year olds, it was reported
that the Board’s end of year review for the Board would include a
summary and update on the key actions arising from the discussions
relating to the life course themed sessions.
What was
agreed?
It was AGREED that:-
(i) The minutes of the Board meeting held on 12 November 2014
were received as a correct record and signed by the
Chairman; and
(ii) A summary report be brought to the Board’s last meeting of
this municipal year which outlines the key actions arising from
the life course discussions.
37. PRIORITY AREA UPDATE - RESPIRATORY DISEASE/SMOKING
What was this
item about?
The Board considered a report which set out the progress to date on
the Board’s Joint Health and Wellbeing Strategy key priority area of
respiratory disease/smoking, in particular highlighting the progress
made in relation to:-
• Increase the proportion of four week quitters staying smoke free
for 12 months;
• Reduce smoking in pregnancy; and
• Reduce respiratory hospital admissions, including childhood
asthma.
In this regard Alex Robertson, Interim Programme Manager –
Respiratory Care, Knowsley CCG, reported on the actions taken
since the Board considered this priority at its meeting on 27 March
2014. It was reported that the Borough continued to face significant
challenges relating to respiratory care, which included:
• The eight highest mortality rate due to respiratory conditions out of
326 local areas from 2010-2012;
• The widening of the gap between Knowsley and England’s
premature mortality rate;
• Increasing A&E attendance for childhood asthma; and
• Improving uptake of the influenza vaccine.
In 2013/14, Knowsley spent approximately £5,693,386 on emergency
admissions for adults due to respiratory conditions with the top two

4
reasons being pneumonia and COPD. This accounted for 10% of all
emergency admissions for the year.
The contract for the current COPD service, which was provided by
Liverpool Heart and Chest Hospital NHS Foundation Trust, expired
on 31 July 2015. Given the current demand being placed on the
service and the continued increase in cost of the disease group it
was felt appropriate to consider how the future clinical model for adult
respiratory care could be developed to support a healthier population
and improve quality of life.
Consequently, the CCG would be developing a new Respiratory
Care clinical model which intended to build on the successes of the
current COPD model, to include a broader range of respiratory
conditions. Furthermore, the CCG would be looking for providers to
demonstrate how they would work closely with the third sector, local
authority and other services to assist the patient.
Further updates where also provided on the following key issues:-
• Paediatric Asthma;
• Knowsley Pharmacy Inhaler Technique Project;
• Influenza Vaccination and Excess Winter Deaths;
• Smoking in Pregnancy; and
• Tobacco Control Plan.
What was
discussed?
Clarity was sought on whether the proposed changes to the COPD
service would see a fragmentation of the provision.
The Board was informed that the main driver for the proposed
changes to the COPD service was focused on delivering quality and
seeking improvements across the treatment of all respiratory
illnesses in the Borough.
A Board Member reflected on a particular positive impact of the
current COPD scheme which was the engagement of service users.
Would this successful approach be incorporated into the new
service?
The Board was advised that engagement with a number of service
user groups had been undertaken with initial feedback demonstrating
a positive response to the proposals. Furthermore, the expansion of
the COPD service sought to make it more accessible to patients with
a focus on prevention and providing support to family members.
A Board Member reflected that the COPD proposals were an
excellent example of partnership working and welcomed the
5
systematic approach as detailed in the report. Clarity was sought on
whether the service could link in with broader council activities, such
as parks, green spaces and leisure facilities, which would support the
preventative aspect of the service.
The Activity for Life programme was acknowledged as contributing
towards supporting patients in making positive improvements to their
lifestyle. Therefore, providers would be encouraged to deliver such a
service as part of the new programme. Discussions were also taking
place with the Healthy Homes Scheme to identify how this Scheme
could work closely with the new Respiratory Care service.
A Board Member sought clarity on whether telehealth would be
incorporated into the specifications of the tender?
The Board was informed that telehealth was a very innovative and
flexible service which would form an integral part of the service.
What was
agreed?
It was AGREED that:-
(i) The contents of the report be noted; and
(ii) The actions that had been taken to date and the plans for
further service developments be endorsed.
38. LIVE WELL : WORKING AGE
What was this
item about?
The Board considered a report which sought to inform Members of
the following:-
• Highlighted the key health and wellbeing issues which existed for
the working age population, who were aged between 18 to 65;
and
• Outlined how effective the health and wellbeing system was in
addressing emerging risk factors and identify what improvements
were required.
This was the third themed Health and Wellbeing Board session which
considered each stage of the life course. In this regard the Board
received a verbal presentation which covered the following key
areas:-
• Summarised the wider challenges which impacted upon the health
and wellbeing outcomes for adults in the Borough;
• Identified the four key health and wellbeing illnesses which

6
contributed towards premature deaths in the Borough, which
were:-
• Heart disease and strokes (CVD);
• Cancer;
• Respiratory disease; and
• Mental health and wellbeing.
• Summarised the key services and programmes which were in place to address the four key health and wellbeing illnesses. Highlighting how the services and programmes focused on prevention, early diagnosis, intervention, identification and managing conditions; and
• Highlighted the need to respond to the premature mortality action
plan developed by NHS England to identify local progress and
areas for development.
What was
discussed?
Members of the Borough raised the following questions and
comments:-
• There were broader issues such as welfare reform and poverty
which impacted upon the health of residents. Clarity was sought
on whether the impact of broader social issues had been
considered when looking to identify appropriate treatments?
The Board was informed that the Council’s scrutiny function was
undertaking a scrutiny review which was considering the impact of
welfare reform on residents. It was reported that consultation
relating to this scrutiny review was currently ongoing and would be
circulated to the Engagement Forum.
It was further reported that the remit of this Board was limited to
issues relating to health and wellbeing. However, the remit of the
Knowsley Strategic Board was much broader and had a greater
strategic focus across the Borough. As the Engagement Network
supported both Board’s it was important that they were kept
informed of the Board’s workplans. In terms of social prescribing
this currently took place however, it was recognised that further
work in this area was required. Patients should be encouraged to
explore the range of resources, including access to leisure
services and green space.
• Clarity was sought on how housing landlords could be influenced
to address fuel poverty?
The Board was informed that this was a complex area due to the
differences in housing tenure. First Ark had recently sought to

7
address fuel poverty which should have a bearing on their
residents. However, it was proving difficult to make the same
progress with private sector landlords. The development of the
Community Healthy Homes programme sought to address this by
engaging with tenants to improve the warmth of their home. A
team of advocates from across a range of partners, such as the
Fire Service, First Ark and the Council, would be involved in this
process and it was hoped that this would ensure a broad range of
tenants could benefit from the programme.
• Clarity was sought on the figures detailed in the presentation
relating to the main causes of death in Knowsley during 2012. In
particular did the figures take account of whether the deceased
had learning difficulties? Furthermore, many of the practises had
signed up to the Royal College Cancer Unit and results would be
available soon.
The Board was informed that currently the data relating to deaths
did not reflect whether an individual had learning disabilities.
However, consideration would be given to exploring the possibility
of applying the national figures identified in the report to local
intelligence.
• It was acknowledged that the issues being discussed where wide
ranging and a variety of partners would be trying to bring
improvements to resident’s health. Clarity was sought on whether
a mapping exercise could be undertaken to demonstrate the
different strategic discussions that were taking place across the
various boards.
The Board was informed that a request would be taken to the
Knowsley Implementation Group to determine whether they would
be able to progress this issue further.
• Clarity was sought on the increasing rates of breast cancer and
what processes where in place to address this?
The Board was informed that there had been an increase in the
numbers of patients being diagnosed with breast cancer. This
could be due to a variety of reasons but primary indicators
suggest that it could be related to an increase in more people
undertaking screening or being diagnosed too late.
What was
agreed?
It was AGREED that:-
(i) the health and wellbeing outcomes and challenges during
adulthood be noted;

8
(ii) the health and wellbeing system be acknowledged for the
effectiveness in addressing the needs of adults; and
(iii) the Knowsley Implementation Group be asked to undertake a
mapping exercise of strategic discussions across the various
Boards in Knowsley.
39. SUICIDE AUDIT - JANUARY 2007 TO MARCH 2012
What was this
item about?
The Board considered a report from the 5 Boroughs Partnership
which highlighted the work currently being undertaken in relation to
suicide prevention in the Borough.
In this regard Steve Hull, Assistant Director of Nursing and
Safeguarding, provided a presentation to Board Members which
reported on the Suicide Audit which had taken place between
January 2007 – December 2012.
The presentation highlighted the following:-
• Provided background to suicide rates and the associated factors
which could indicate an increased risk of suicide;
• Summarised the methodology used in the development of the
suicide audit, which involved the forensic examination of 84 sets
of clinical notes, serious untoward incident reports, trust
electronic clinical systems and data received from the National
Confidential Inquiry;
• Reported on the suicide rates by gender and age along with a
summary of patient diagnoses. The diagnoses included the
duration of illness, previous suicide attempts and self harm,
marital status, employment status, family history, length of time a
patient had contact with mental health services and method of
death;
• Summarised the risk factors associated with suicide for males
and females; and
• Identified the key findings from the suicide audit and the
recommendations for future service provision.
What was
discussed?
Board Members raised the following questions and comments in
relation to the presentation received:-
• Clarity was sought on how timely the therapy services where
provided to patients?
The Board was informed that this information could be circulated
separately. The suicide audit had provided an insight into how

9
organisations communicated with each other. This highlighted
that further work around developing communications between
partners was required.
• It was reported that local evidence suggested that there was a
recurring theme highlighting that mental health conditions were
not treated by a psychologist at an early stage. Which made it
difficult to advocate for those residents who were dealing with a
mental health illness.
• Clarity was sought on whether the suicide audit had identified
whether there were any seasonal variations which impacted
upon suicide rates.
The Board was informed that from the evidence gathered there
had been no correlation between seasons and suicide rates.
• The statistics relating to employment status at the time of death
highlighted that there was a clear correlation between
unemployment and suicide. This demonstrated the importance
of securing and providing employment opportunities for
residents, which was something all partners should be working
towards.
• A representative explained that there were issues with access to
therapies and work was ongoing with the Five Boroughs NHS
Trust in an attempt to address this matter. A CCG workshop
would be held in the New Year which would explore this issue
further and efforts would be made to ensure the appropriate
representation was involved in this workshop, in particular both 5
Boroughs NHS Trust and Merseycare.
• A representative acknowledged the importance of ensuring
Merseycare where included in discussions regarding mental
health provision as they also provided mental health services in
the Borough.
• Consideration should be given to building resilience and skills to
equip young people.
• Gaining employment was a barrier for many disabled people.
Recent research undertaken by the Sure Trust identified that the
employment gap for disabled people was significantly higher in
the Liverpool City Region.
• A recent report published by MIND highlighted that people with
mental health issues required specific employment support.
10
Therefore consideration should be given to providing appropriate
support to people with mental health issues when they were
returning to the working environment.
What was
agreed?
It was AGREED that:-
(i) the findings of the Suicide Audit 2007 – 2012 as attached at
Appendix One to the report now submitted be noted;
(ii) the Suicide Reduction Strategy and the associated one year
actions be noted; and
(iii) the 5 Boroughs Partnership and Merseycare Trust be engaged
in discussions relating to the Suicide Audit to ensure a robust
response to providing support to residents in the Borough.
40. PARTNERSHIP UPDATES
What was this
item about?
The Board considered a report which provided an update on the
activities and key areas for development being undertaken to support
partnerships across Knowsley.
In this regard the Board’s attention was drawn to Appendix A of the
report now submitted which provided a summary of key partnership
activity, which included:-
• Child sexual exploitation;
• Knowsley Engagement Network;
• Local Advisory Groups;
• Provider and Wider Stakeholder Forum;
• Joint Intelligence reports, including the Joint Strategic Needs
Assessment;
• Children Safeguarding Board; and
• Adults Safeguarding Board.
What was
agreed?
It was AGREED that the Board was satisfied with the partnership
updates and the actions being undertaken and progress being made
to support the delivery of the Joint Health and Wellbeing Strategy.
41. CHRISTMAS AND NEW YEAR
At this was the last meeting of the Board, prior to the Festive Season, the Chairperson extended her best wishes to both Board Members and officers for a Merry Christmas and a Happy New Year.

11
Minutes 35 to 41 be received as a correct record on the 29th day of January 2015.
......................................................... Chairperson of the Board
(The meeting closed at 2.55pm)





























