Embed Size (px)
Citation preview

Governing Body Meeting in Public
Thursday 18th January 2018

[Intentionally left blank]

Governing Body Public Meeting
Thursday 18th January 2018, 9:00am-11:00am
Focolare Centre (Meeting Room 1) – Welwyn Garden City
AGENDA
Item Time Subject Report Action
1. 09:00 WELCOME AND APOLOGIES
FOR ABSENCE Chair Note Verbal
2. DECLARATIONS OF INTERESTS
To receive any new declarations of interest or declarations relating to matters on the Agenda.
To reconfirm current declarations on the Register of Interests are accurate and up-to-date.
Chair Note Enclosed
3. 09:05 MINUTES OF THE LAST MEETING AND MATTERS ARISING
To approve the draft Minutes of:
23rd
November 2017 Governing Body In Public Meeting
12th October 2017 Joint Committee
Chair Approve Enclosed
4. 09:10 ACTION TRACKER
Chair Discuss Enclosed
GOVERNANCE, FINANCE AND PERFORMANCE
5. 09:15 INTEGRATED PERFORMANCE AND QUALITY REPORT Director of
Operations / Director of
Nursing and Quality
Note Enclosed
6. 09:25 CHIEF EXECUTIVES REPORT
Chief Executive Note Enclosed
7. 09:35 GOVERNANCE REPORT
Chief Finance Officer
Approve Enclosed

Item Time Subject Report Action
8. 09:45 FINANCE REPORT
Chief Finance Officer
Note Enclosed
9. 09:55 FINANCIAL OUTLOOK Chief Finance Officer Discuss Enclosed
10. 10:05 EQUALITY AND DIVERSITY ANNUAL REPORT
Director of Workforce
Approve Enclosed
11. 10:15 PUBLIC ENGAGEMENT REPORT
Dr Nicky Williams
Note Enclosed
12. 10:25 ADULT MENTAL HEALTH COMMUNITY SERVICES AND THE HERTFORDSHIRE SUICIDE PREVENTION STRATEGY
Director of Commissioning /
Approve Enclosed
13. 10:35 WORKFORCE REPORT
Director of Workforce
Note Enclosed
14. 10:45 REMUNERATION COMMITTEE TERMS OF REFERENCE
Lay Member for Governance and
Audit / Company Secretary
Approve Enclosed
FOR INFORMATION
15. 10:50 GOVERNANCE & AUDIT COMMITTEE MINUTES
To note the Minutes of the meeting held on:
15th November 2017
Lay Member Governance and
Audit
Note Enclosed
electronically
16. HBL ICT STAKEHOLDER BOARD MINUTES
To note the Minutes of the meeting held on:
18th September 2017
Chief Finance Officer
Note Enclosed
electronically

Item Time Subject Report Action
17. LOCALITY COMMITTEE MINUTES
Minutes of the locality meetings since:
North Hertfordshire – 9 August 2017, 25 October 2017
Upper Lea Valley – 11 October 17
Stevenage – 13 June 2017, 11 July 2017, 12 September 2017, 10 October 2017 and 14 November 2017.
Welwyn and Hatfield – 14th September 2017
Director of Commissioning
Note Enclosed electronically
18. 10:55 QUESTIONS FROM MEMBERS OF THE PUBLIC
To receive any questions from members of the public.
- - -
19. ANY OTHER URGENT BUSINESS
To consider any other matters which, in the opinion of the Chair, should be considered as a matter of urgency.
All Discuss Verbal
20. 11:00 DATE OF NEXT MEETING
22nd
March 2018 09:00am – 11:00am - Public Session 11:00am – 12:00pm - Private Session
Focolare Centre, Meeting Room 1
- -
Resolution to exclude members of the press and public
The Governing Body of the Clinical Commissioning Group resolves that representatives of the press,
and other members of the public, be excluded from the remainder of this meeting having regard to the
confidential nature of the business to be transacted, publicity of which would be prejudicial to the
public interest, in accordance with the Public Bodies (Admissions to Meetings) Act 1960.
Page | 1
Agenda Item No: 2
Date of Meeting: 18th January 2017
Governing Body Meeting in Public
Paper Title: Declarations of Interest
Decision or Approval Discussion Information
Report author: Maryla Hart, Governing Body Administrator
Report signed off by:
Executive Summary: The purpose of this paper is to receive any new declarations of interest or declarations relating to matters on the Agenda, and to reconfirm current declarations on the Register of Interests are accurate and up-to-date.
The following should be recorded in the minutes of the meeting:
Individual declaring the interest. At what point the interest was declared. The nature of the interest. The Chair’s decision and resulting action taken. The point during the meeting at which any individuals retired
from and returned to the meeting - even if an interest has not been declared.
Recommendations
to the members:
To review the Register of Interests of the Governing Body or relevant committee membership, and highlight any potential conflicts, which the Chair needs to manage:
http://www.enhertsccg.nhs.uk/declarations-interest
To declare those interests at the start of the meeting.
To complete a declaration form available from the Company
Secretary. This will be recorded in the Minutes of the meeting.
Conflicts of Interest
involved:
There are none identified.
Page | 2
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.
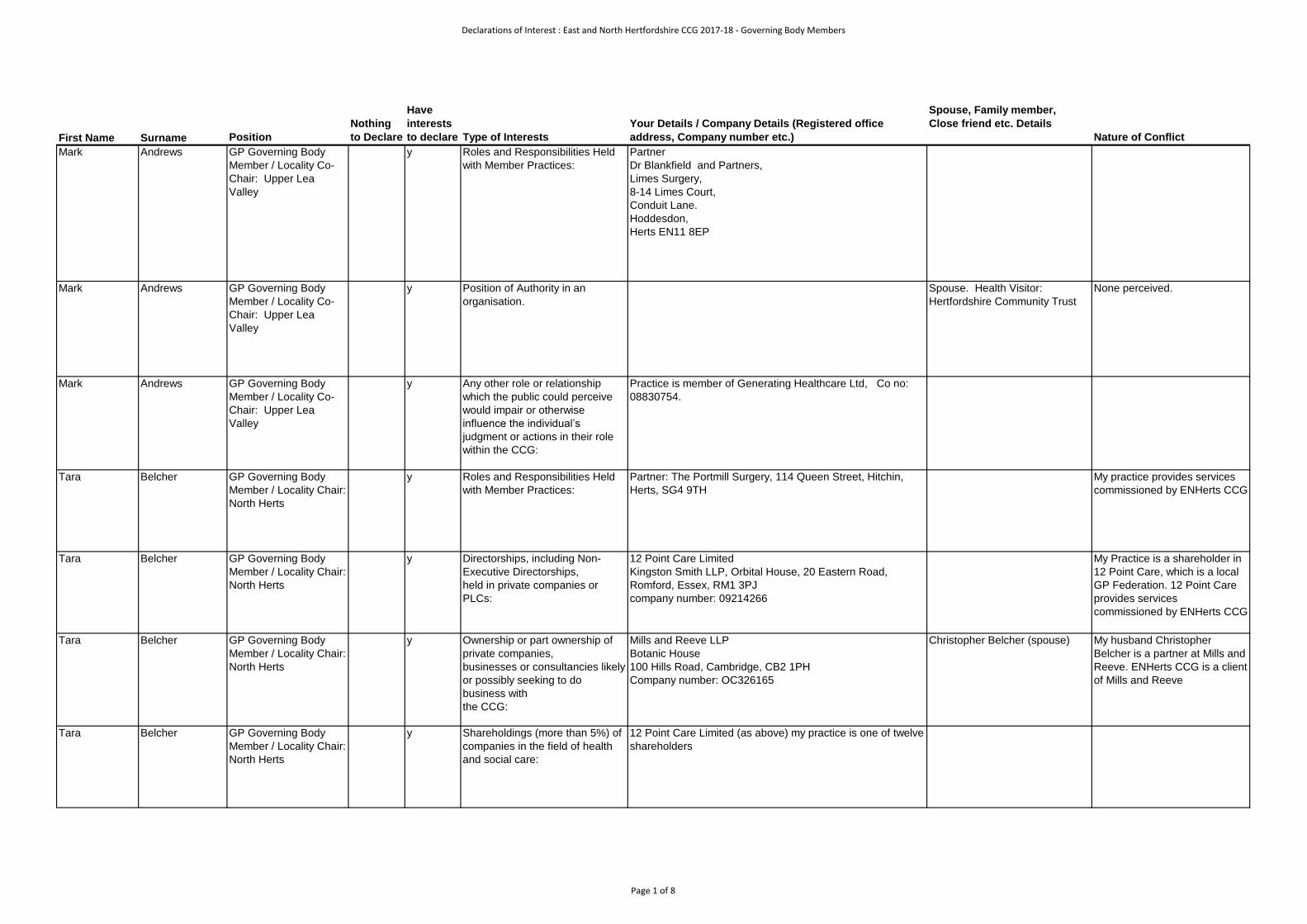
Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
Mark Andrews GP Governing Body
Member / Locality Co-
Chair: Upper Lea
Valley
y Roles and Responsibilities Held
with Member Practices:
Partner
Dr Blankfield and Partners,
Limes Surgery,
8-14 Limes Court,
Conduit Lane.
Hoddesdon,
Herts EN11 8EP
Mark Andrews GP Governing Body
Member / Locality Co-
Chair: Upper Lea
Valley
y Position of Authority in an
organisation.
Spouse. Health Visitor:
Hertfordshire Community Trust
None perceived.
Mark Andrews GP Governing Body
Member / Locality Co-
Chair: Upper Lea
Valley
y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual’s
judgment or actions in their role
within the CCG:
Practice is member of Generating Healthcare Ltd, Co no:
08830754.
Tara Belcher GP Governing Body
Member / Locality Chair:
North Herts
y Roles and Responsibilities Held
with Member Practices:
Partner: The Portmill Surgery, 114 Queen Street, Hitchin,
Herts, SG4 9TH
My practice provides services
commissioned by ENHerts CCG
Tara Belcher GP Governing Body
Member / Locality Chair:
North Herts
y Directorships, including Non-
Executive Directorships,
held in private companies or
PLCs:
12 Point Care Limited
Kingston Smith LLP, Orbital House, 20 Eastern Road,
Romford, Essex, RM1 3PJ
company number: 09214266
My Practice is a shareholder in
12 Point Care, which is a local
GP Federation. 12 Point Care
provides services
commissioned by ENHerts CCG
Tara Belcher GP Governing Body
Member / Locality Chair:
North Herts
y Ownership or part ownership of
private companies,
businesses or consultancies likely
or possibly seeking to do
business with
the CCG:
Mills and Reeve LLP
Botanic House
100 Hills Road, Cambridge, CB2 1PH
Company number: OC326165
Christopher Belcher (spouse) My husband Christopher
Belcher is a partner at Mills and
Reeve. ENHerts CCG is a client
of Mills and Reeve
Tara Belcher GP Governing Body
Member / Locality Chair:
North Herts
y Shareholdings (more than 5%) of
companies in the field of health
and social care:
12 Point Care Limited (as above) my practice is one of twelve
shareholders
Page 1 of 8

Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
Tara Belcher GP Governing Body
Member / Locality Chair:
North Herts
GP Appraiser (Central Midlands Area Team). 06/06/16-
present.
Denise Boardman CCG Programme
Director
y As a registered Occupational Therapist and former member
of the Royal College of Occupational Therapy Professional
Practice Board, I receive “ad hoc” requests to deliver
presentations to specialist sections of the Royal College of
Occupational Therapy. Any requests received are discussed
in 1:1 meetings with my line manager prior acceptance.
Non-Financial Professional
Interests
Non-Financia
Haydar Bolat GP Governing Body
Member / Locality Co-
Chair: Lower Lea Valley
y Roles and Responsibilities within
member practices:
Salary GP, Stanhope Surgery
Stanhope Road
Waltham Cross
EN8 7DJ
employee in a member practice
Haydar Bolat GP Governing Body
Member / Locality Co-
Chair: Lower Lea Valley
y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual’s
judgment or actions in their role
within the CCG:
The Practice is a member of LEA VALLEY HEALTH LTD,
Orbital House, 20 Eastern Road, Romford, Essex, RM1 3PJ
Company number 09114753
Haydar Bolat GP Governing Body
Member / Locality Co-
Chair: Lower Lea Valley
y Directorships, including Non-
Executive Directorships,
held in private companies or
PLCs:
Director of Dr Bolat Ltd
Reg. number: 08683924
3c Government Row
Enfield
EN3 6JN
private limited company (general medical practice activities).
(2011-2017 - inactive locum company).
Harper Brown Director of
Commissioning
y Directorships, including Non-
Executive Directorships,
held in private companies or
PLCs:
/
Ownership or part ownership of
private companies,businesses or
consultancies likely or possibly
seeking to do business with the
CCG:
Harper Brown Consulting Ltd
15 Whiting Street, Bury St Edmunds, Suffolk, IP33 1NX
Company number 08982673
None
Harper Brown Director of
Commissioning
y Position of Authority in an
organisation.
Hononary Senior Lecturer, University of East Anglia, School
of Health Economics, Norwich
None
Dianne Desmulie Lay Member: Public and
Patient Engagement
y Roles and Responsibilities within
member practices:
Member of Hanscombe House Patient Participation Core
Group. I am secretary for the group.
None currently. Potential
conflict re. funding allocations
or issues concerning
performance.
Page 2 of 8

Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
Dianne Desmulie Lay Member: Public and
Patient Engagement
y Directorships, including Non-
Executive Directorships,
held in private companies or
PLCs:
Director of my own company:
Pieve Solutions Ltd
Company No, 5600186. Registered address:
Orchard House, Park Lane, REIGATE, Surrey, RH2 8JX.
I work through this company as a freelance Management
Consultant.
My husband, Robert Pinkham, is
also a director of Pieve Solutions
Lrd and works as a freelance HR
consultant.
None currently.
Dianne Desmulie Lay Member: Public and
Patient Engagement
y Any other connection with a
voluntary or other organisation
contracting for NHS Services.
I am the Volunteer Hub Lead for the Hoddesdon Carers'
Support Hub. This is part of carers in Hertfordshire, a charity
which contracts with Herts County Council and the CCG and
NHS locally. This particular project is funded by the Big
Lottery.
None currently.
Sharn Elton Director of Operations y
Linda Farrant Lay Member:
Governance and Audit
y Position of Authority in an
organisation.
• Non Executive Board Member of OFSTED
-----------------
• Independent Member of Audit and Corporate Governance
Committee of Care Quality Commission wef 27/07/15
• No direct conflict. OFSTED
inspects children’s care
services provided by local
authorities.
------------------
• No direct conflict. CQC
regulates and inspects NHS
providers including GP
practices and and adult social
care with whom CCG
commissions services.
Linda Farrant Lay Member:
Governance and Audit
y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual’s
judgment or actions in their role
within the CCG:
Patient of South Street Surgery. Receive services from GP
Practice in CCG area.
Beverley Flowers Chief Executive /
Accountable Officer
y
Sachin Gupta GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield
y Roles and Responsibilities Held
within member practices
Partner: Garden City Practice, 11 Guessens Road, Welwyn
Garden City, AL8 6QW.
GP Partner since 01/08/2010.
Member Practice of East and
North Herts CCG
Sachin Gupta GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield
y Shareholdings (more than 5%) of
companies in the field of health
and social care:
Director and shareholder in SG Healthcare Limited.
Registration No: 08316300
Address: Bracey's Accountants, Wilbury Way, Hitchin, SG4
0TW.
I do locum GP sessions, Out of Hours and Urgent Care
sessions and GP appraisal work through this company.
Director and shareholder Face and Skin Ltd. Company No:
09964525. Address: Bracey's Accountants, Wilbury Way,
Hitchin, SG4 0TW
I provide non surgical aesthetic procedures through this
company
Wife is co-director. None perceived
None perceived
Page 3 of 8

Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
Sachin Gupta GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield
y Shareholdings (more than 5%) of
companies in the field of health
and social care:
Director and shareholder: Pearl Blossom Ltd; company
number - 10163796 incorporated 05/05/2016
Address: Bracey's Accountants, Wilbury Way, Hitchin, SG4
0TW.
Provider of a residential nursing care home in Lincolnshire.
Director and shareholder Amber Blossom Ltd; Company No:
10673689 incorporated 16/03/2017. Address: Bracey's
Accountants, Wilbury Way, Hitchin, SG4 0TW
Provider of a residential nursing care home in Lincolnshire.
None perceived
None perceived
Gupta Gupta GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield
y Shareholdings (more than 5%) of
companies in the field of health
and social care:
Director Pearl Blossom Group Holding Ltd; company number -
10645623 incorporated 01/03/2017
Address: Bracey's Accountants, Wilbury Way, Hitchin, SG4
0TW.
Manages holdings of Amber Blossom Ltd and Pearl Blossom
Ltd.
None perceived
Sachin Gupta GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield
y Shareholdings (more than 5%) of
companies in the field of health
and social care:
My practice (Garden City Practice) is a shareholder in
Welwyn Hatfield GP Federation - Ephedra Healthcare Ltd,
Suite 3, Middlesex House, Rutherfield Close, Stevenage,
SG1 2EF. Company No: 06560722.
None perceived
Sachin Gupta GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield
y Any connection with a voluntary
or other organisation contracting
for NHS Services
I am a Disciplinary Specific Practitioner (DSP) for NHSE -
PAG (Performance Advisory Group) meetings and PLDP
(Performers List Decision Making) Panel.
None Perceived
Sachin Gupta GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield
y Other specific interests? I am working with Beds & Herts LMC on GPRP - GP
Resilience Programme. I am undertaking practice visits under
this programme.
I am visiting practices outside
ENHCCG
Russell Hall GP Governing Body
Member / Locality Co-
Chair: Stevenage
y Roles and Responsibilities Held
within member practices
Partner Chells Medical Practice, 265 Chells Way, Stevenage,
SG2 0HN
GP Partner. Provider GMS
Services.
[locality representative]
Russell Hall GP Governing Body
Member / Locality Co-
Chair: Stevenage
y Ownership or part ownership of
private companies,businesses or
consultancies likely or possibly
seeking to do business with the
CCG:
Chells Practice is a member of Stevenage Federation, a
private company.
STEVENAGE HEALTH LIMITED
The Health Centre, Stanmore Road, Stevenage,
Hertfordshire, England, SG1 3QA
Company number 08877494
GP Member of Private Provider
Company.
Russell Hall GP Governing Body
Member / Locality Co-
Chair: Stevenage
y Position of Authority in an
organisation.
GP Practice and CCG organisation member as above.
Page 4 of 8

Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
Alison Jackson GP Governing Body
Member / Locality Co-
Chair: Lower Lea
Valley
y Roles and Responsibilities within
member practice
Principle GP Partner at the Maples Health Centre, Vancouver
Road, Turnford, Brokbourne, EN10 6FD.
In a position of influence
[locality representative]
Alison Jackson GP Governing Body
Member / Locality Co-
Chair: Lower Lea
Valley
y Ownership or part ownership of
private companies,
businesses or consultancies likely
or possibly seeking to do
business with the CCG:
The Practice is a member of LEA VALLEY HEALTH LTD,
Orbital House, 20 Eastern Road, Romford, Essex, RM1 3PJ
Company number 09114753
In a position of influence
Rachel Joyce Clinical Advisor y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual's
judegement or actions in their role
within the CCG.
Husband is a consultant working at
East and North Herts NHS Trust and
Private Hospitals.
Sees patients in both NHS and
private Hospitals locally.
Deborah Kearns GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Roles and Responsibilities Held
within member practices
Central Surgery
Bell Street
Sawbridgeworth
CM219AQ
Provider of GMS and Enhanced
Services
Property owner seeking to
improve premises through
Primary Care Transformation
bid.
[locality representative]
Deborah Kearns GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Any connection with a voluntary
or other organisation contracting
for NHS Services
Mantle(Saffron) Ltd Company Number
5752770.
The Priory Thremhall Park, Start Hill, Bishops Stortford,
Hertfordshire, CM22 7WE
Mantle(HB) LLP ref. no OC384165
The Priory Thremhall Park, Start Hill, Bishops Stortford,
Hertfordshire, CM22 7WE
Husband is director. Mantle (Saffron) maintains a
freehold interest in Saffron
Ground in Stevenage, which is
a 4 story office building. 2 floors
are let to the NHS.
Mantle (HB) was the developer
that enabled the initiating
stages of the development of
Central Surgery. This
arrangement predates my role
in the Governing Body. They
have received no professional
fees to date.
Propose to use another 3rd
party developer to deliver the
project and offer open book
financial transparency should
the bid be successful.
Deborah Kearns GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Ownership or part ownership of
private companies,
businesses or consultancies likely
or possibly seeking to do
business with
the CCG:
Practice is a member of federation Stortford Valley Health
Care Ltd
Company number 09489615
Federation planning to bid to
deliver enhanced services.
I am not a director.
Page 5 of 8
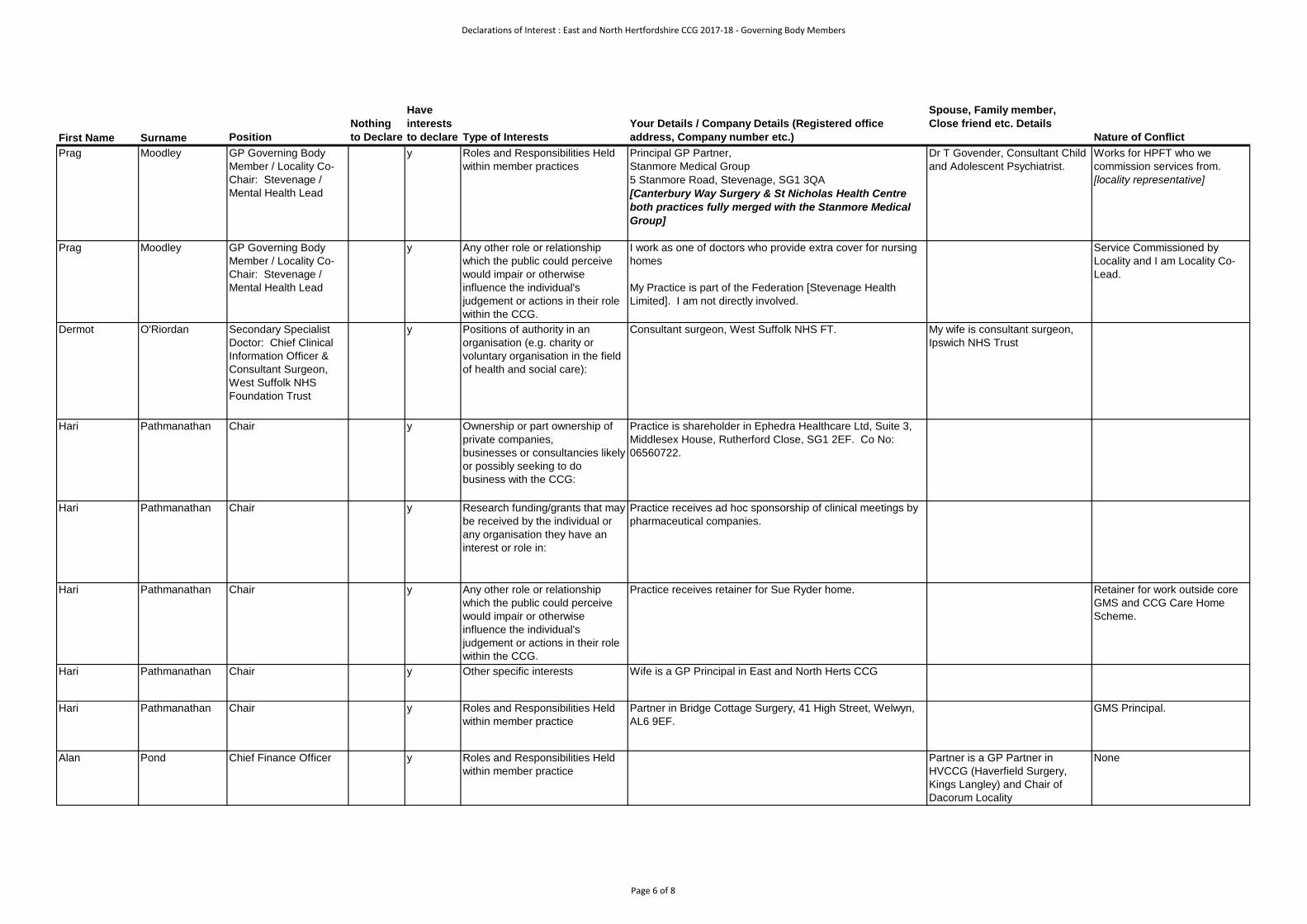
Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
Prag Moodley GP Governing Body
Member / Locality Co-
Chair: Stevenage /
Mental Health Lead
y Roles and Responsibilities Held
within member practices
Principal GP Partner,
Stanmore Medical Group
5 Stanmore Road, Stevenage, SG1 3QA
[Canterbury Way Surgery & St Nicholas Health Centre
both practices fully merged with the Stanmore Medical
Group]
Dr T Govender, Consultant Child
and Adolescent Psychiatrist.
Works for HPFT who we
commission services from.
[locality representative]
Prag Moodley GP Governing Body
Member / Locality Co-
Chair: Stevenage /
Mental Health Lead
y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual's
judgement or actions in their role
within the CCG.
I work as one of doctors who provide extra cover for nursing
homes
My Practice is part of the Federation [Stevenage Health
Limited]. I am not directly involved.
Service Commissioned by
Locality and I am Locality Co-
Lead.
Dermot O'Riordan Secondary Specialist
Doctor: Chief Clinical
Information Officer &
Consultant Surgeon,
West Suffolk NHS
Foundation Trust
y Positions of authority in an
organisation (e.g. charity or
voluntary organisation in the field
of health and social care):
Consultant surgeon, West Suffolk NHS FT. My wife is consultant surgeon,
Ipswich NHS Trust
Hari Pathmanathan Chair y Ownership or part ownership of
private companies,
businesses or consultancies likely
or possibly seeking to do
business with the CCG:
Practice is shareholder in Ephedra Healthcare Ltd, Suite 3,
Middlesex House, Rutherford Close, SG1 2EF. Co No:
06560722.
Hari Pathmanathan Chair y Research funding/grants that may
be received by the individual or
any organisation they have an
interest or role in:
Practice receives ad hoc sponsorship of clinical meetings by
pharmaceutical companies.
Hari Pathmanathan Chair y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual's
judgement or actions in their role
within the CCG.
Practice receives retainer for Sue Ryder home. Retainer for work outside core
GMS and CCG Care Home
Scheme.
Hari Pathmanathan Chair y Other specific interests Wife is a GP Principal in East and North Herts CCG
Hari Pathmanathan Chair y Roles and Responsibilities Held
within member practice
Partner in Bridge Cottage Surgery, 41 High Street, Welwyn,
AL6 9EF.
GMS Principal.
Alan Pond Chief Finance Officer y Roles and Responsibilities Held
within member practice
Partner is a GP Partner in
HVCCG (Haverfield Surgery,
Kings Langley) and Chair of
Dacorum Locality
None
Page 6 of 8
Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
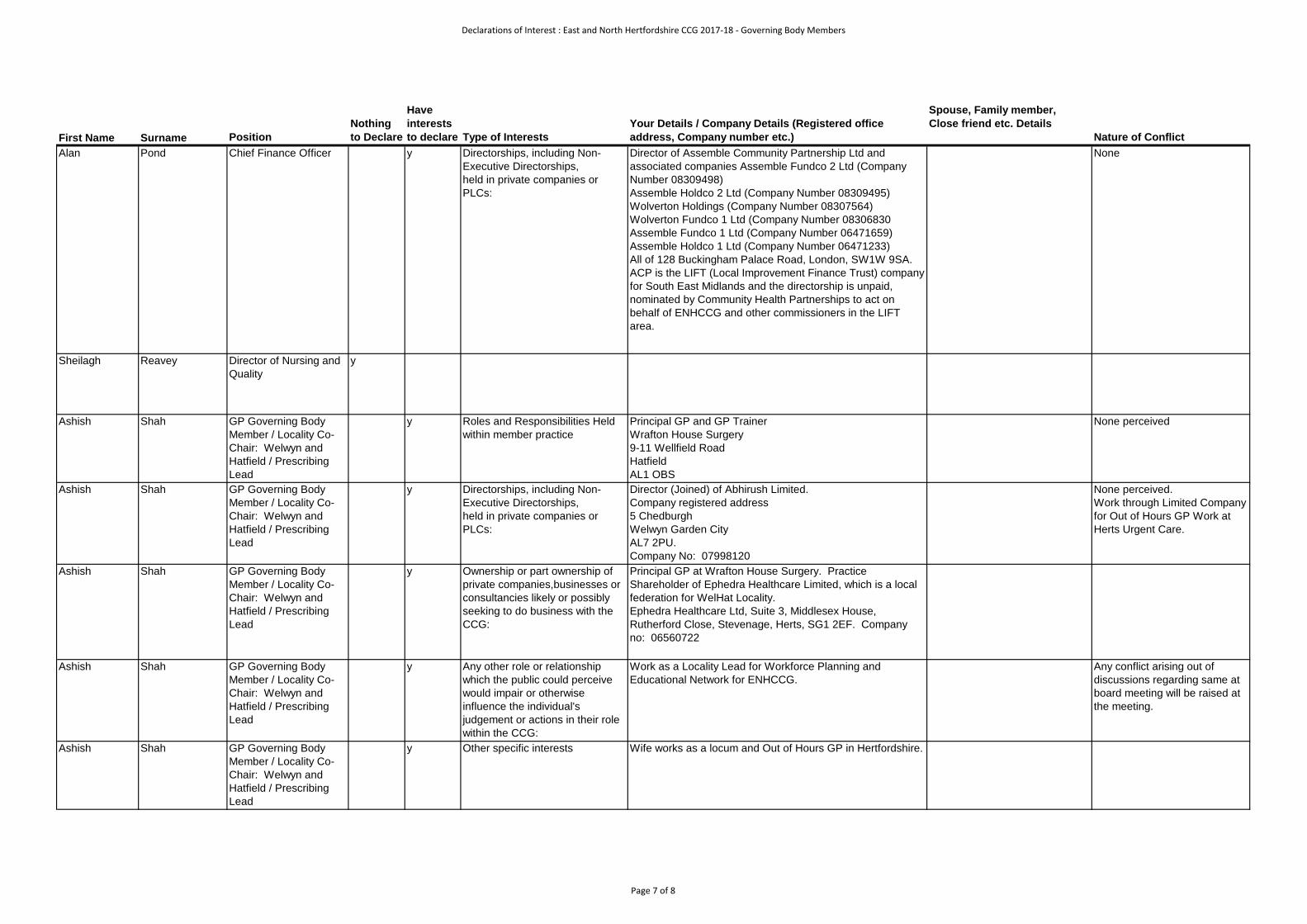
Alan Pond Chief Finance Officer y Directorships, including Non-
Executive Directorships,
held in private companies or
PLCs:
Director of Assemble Community Partnership Ltd and
associated companies Assemble Fundco 2 Ltd (Company
Number 08309498)
Assemble Holdco 2 Ltd (Company Number 08309495)
Wolverton Holdings (Company Number 08307564)
Wolverton Fundco 1 Ltd (Company Number 08306830
Assemble Fundco 1 Ltd (Company Number 06471659)
Assemble Holdco 1 Ltd (Company Number 06471233)
All of 128 Buckingham Palace Road, London, SW1W 9SA.
ACP is the LIFT (Local Improvement Finance Trust) company
for South East Midlands and the directorship is unpaid,
nominated by Community Health Partnerships to act on
behalf of ENHCCG and other commissioners in the LIFT
area.
None
Sheilagh Reavey Director of Nursing and
Quality
y
Ashish Shah GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield / Prescribing
Lead
y Roles and Responsibilities Held
within member practice
Principal GP and GP Trainer
Wrafton House Surgery
9-11 Wellfield Road
Hatfield
AL1 OBS
None perceived
Ashish Shah GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield / Prescribing
Lead
y Directorships, including Non-
Executive Directorships,
held in private companies or
PLCs:
Director (Joined) of Abhirush Limited.
Company registered address
5 Chedburgh
Welwyn Garden City
AL7 2PU.
Company No: 07998120
None perceived.
Work through Limited Company
for Out of Hours GP Work at
Herts Urgent Care.
Ashish Shah GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield / Prescribing
Lead
y Ownership or part ownership of
private companies,businesses or
consultancies likely or possibly
seeking to do business with the
CCG:
Principal GP at Wrafton House Surgery. Practice
Shareholder of Ephedra Healthcare Limited, which is a local
federation for WelHat Locality.
Ephedra Healthcare Ltd, Suite 3, Middlesex House,
Rutherford Close, Stevenage, Herts, SG1 2EF. Company
no: 06560722
Ashish Shah GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield / Prescribing
Lead
y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual's
judgement or actions in their role
within the CCG:
Work as a Locality Lead for Workforce Planning and
Educational Network for ENHCCG.
Any conflict arising out of
discussions regarding same at
board meeting will be raised at
the meeting.
Ashish Shah GP Governing Body
Member / Locality Co-
Chair: Welwyn and
Hatfield / Prescribing
Lead
y Other specific interests Wife works as a locum and Out of Hours GP in Hertfordshire.
Page 7 of 8
Declarations of Interest : East and North Hertfordshire CCG 2017-18 - Governing Body Members
First Name Surname Position
Nothing
to Declare
Have
interests
to declare Type of Interests
Your Details / Company Details (Registered office
address, Company number etc.)
Spouse, Family member,
Close friend etc. Details
Nature of Conflict
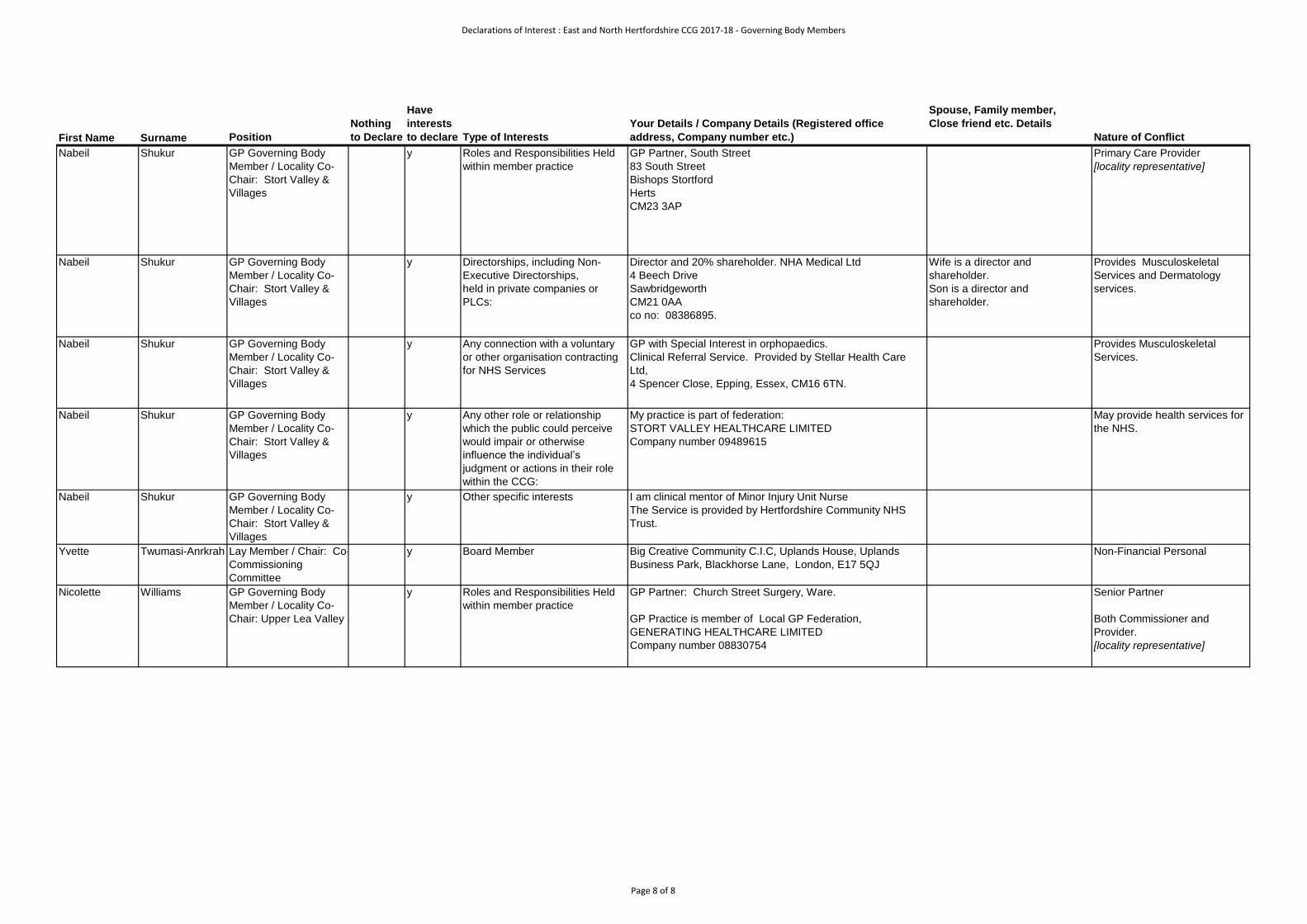
Nabeil Shukur GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Roles and Responsibilities Held
within member practice
GP Partner, South Street
83 South Street
Bishops Stortford
Herts
CM23 3AP
Primary Care Provider
[locality representative]
Nabeil Shukur GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Directorships, including Non-
Executive Directorships,
held in private companies or
PLCs:
Director and 20% shareholder. NHA Medical Ltd
4 Beech Drive
Sawbridgeworth
CM21 0AA
co no: 08386895.
Wife is a director and
shareholder.
Son is a director and
shareholder.
Provides Musculoskeletal
Services and Dermatology
services.
Nabeil Shukur GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Any connection with a voluntary
or other organisation contracting
for NHS Services
GP with Special Interest in orphopaedics.
Clinical Referral Service. Provided by Stellar Health Care
Ltd,
4 Spencer Close, Epping, Essex, CM16 6TN.
Provides Musculoskeletal
Services.
Nabeil Shukur GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Any other role or relationship
which the public could perceive
would impair or otherwise
influence the individual’s
judgment or actions in their role
within the CCG:
My practice is part of federation:
STORT VALLEY HEALTHCARE LIMITED
Company number 09489615
May provide health services for
the NHS.
Nabeil Shukur GP Governing Body
Member / Locality Co-
Chair: Stort Valley &
Villages
y Other specific interests I am clinical mentor of Minor Injury Unit Nurse
The Service is provided by Hertfordshire Community NHS
Trust.
Yvette Twumasi-Anrkrah Lay Member / Chair: Co-
Commissioning
Committee
y Board Member Big Creative Community C.I.C, Uplands House, Uplands
Business Park, Blackhorse Lane, London, E17 5QJ
Non-Financial Personal
Nicolette Williams GP Governing Body
Member / Locality Co-
Chair: Upper Lea Valley
y Roles and Responsibilities Held
within member practice
GP Partner: Church Street Surgery, Ware.
GP Practice is member of Local GP Federation,
GENERATING HEALTHCARE LIMITED
Company number 08830754
Senior Partner
Both Commissioner and
Provider.
[locality representative]
Page 8 of 8

Page | 1
Agenda Item No: 3
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Draft – Governing Body Minutes
Decision or Approval Discussion Information
Report author: Tracey Middleton, Governing Body Clerk
Maryla Hart, Governing Body Administrator
Report signed off by: Jas Dosanjh, Corporate Governance Manager
Executive Summary: To approve the draft Minutes of the meeting held on
23rd November 2017.
Recommendations
to the members:
To approve the Minutes.
Conflicts of Interest
involved:
There are none identified.
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

Page 1 of 10
Governing Body Meeting (Public)
Thursday 23rd November 2017 at 09.00
Focolare Centre, Meeting Room 2, Welwyn Garden City
MINUTES
Present:
Tara Belcher [TB] GP Lead, North Herts.
Harper Brown [HB] Director of Commissioning
Dianne Desmulie [DD] Lay Member, Patient and Public Engagement
Sharn Elton [SE] Director of Operations
Linda Farrant [LF] Lay Member, Governance and Audit
Beverley Flowers [BF] Chief Executive (Accountable Officer)
Sachin Gupta [SG] GP Lead, Welwyn and Hatfield
Russell Hall [RH] GP Lead, Stevenage
Rachel Joyce [RJ] Medical Director
Prag Moodley [PM] GP Lead, Stevenage
Dermot O’Riordan [DO] Secondary Care Specialist
Hari Pathmanathan [HP] Chair
Sheilagh Reavey [SR] Director of Nursing and Quality
Nabeil Shukur [NS] GP Lead, Stort Valley and Villages
Nicky Williams [NW] Deputy Chair
In Attendance:
Sunday Adeniyi [SA] Deputy Chief Finance Officer
Denise Boardman [DB] Programme Director
Gillian Catchpole [GC] Project Manager ENHCCG
Sarah Feal [SF] Company Secretary
Jennifer Kearney [JK] General Manager ENHT
Tracey Middleton [TM] Governing Body Administrator
Gerry Moir [GM] Associate Director for Performance
Charlotte Reynolds [CR] Service Manager Neurological Services, HCT
Michael Taylor [MT] Patient Representative

Page 2 of 10
Item Subject Action by
1. WELCOME AND APOLOGIES FOR ABSENCE
The meeting opened at: 09.00
The Chair welcomed all to the meeting. Apologies were received from:
• Mark Andrews [MA], GP Lead, Upper Lea Valley • Haydar Bolat [HB], GP Lead, Lower Lea Valley • Alan Pond [AP], Chief Finance Officer • Ashish Shah [AS], GP Lead, Welwyn and Hatfield • Yvette Twumasi-Ankrah [YT], Lay Member, Co-Commissioning • Peter Chapman [PC], Patient Representative
Sunday Adeniyi was welcomed to the meeting on behalf of Alan Pond
The Chair declared that the meeting is quorate
2. DECLARATIONS OF INTERESTS
1. The Chair invited the members to reconfirm their current declarations on the Register of Interests and advise of any new declarations.
2. All members confirmed their declarations were accurate and up-to-date.
3. The Chair invited members to declare any declarations relating to matters on the Agenda.
4. The following individuals made declarations in relation to the Agenda:
• Dr Ashish Shah – Item 11 - Prescribing Report - A partner in Wrafton House Surgery, Welwyn & Hatfield locality whose date is included in the locality totals in the report – Apologies received so no Chair action required
• All GP Board Members – Item 11 – Prescribing Report – All GP Board members who have prescribed in the period of the report will have contributed to the data included. GP Board representatives are members of Locality federations which are private companies which may provide CCG – commissioned, services
5. The Chair’s decision was that members can stay for the item as the report is for information purposes
6. All other members confirmed they have no declarations in relation to matters on the Agenda

Page 3 of 10
Item Subject Action by
3. MINUTES OF PREVIOUS MEETING AND MATTERS ARISING
The Minutes of the meeting held on 21.09.17 were approved as an accurate record subject to the following amendments:
• Item 8: Integrated Performance And Quality Report:
1) Point 6 – ‘The Governing body debated the concerns with the balance of quality and operational delivery is having an impact due to capacity and this has been raised with the Quality Committee’
To be replaced with the following text:
‘The Governing Body debated the quality concerns at East and North Herts Trust (ENHT) that the Chair of the Quality Committee raised at the request of the September Quality Committee. Following extensive discussion, it was agreed that the CCG Chief Executive would raise the issues directly with the Chief Executive of the Trust. ACTION: The Chief Executive to raise quality concerns directly with the Chief Executive of ENHT’
2) Point 9 – ‘The Quality Committee reviewed the performance of Herts Urgent Care in depth and it was noted that this was reported previously. The service provision is under discussion and it was noted that the workshop will be the forum for further discussion’
To be replaced with the following text:
‘The Quality Committee had undertaken a Deep Dive into Herts Urgent Care (HUC). Whilst on the whole performance was satisfactory, there was concern at the number of Base 3 closures. It was noted that such closures would be monitored and reported via the Integrated Performance and Quality Report to the Governing Body’
ACTION: The final minutes of the meeting held on 21.09.17 to be updated to reflect amendments.
Matters Arising:
1. None
MH

Page 4 of 10
Item Subject Action by
4. ACTION TRACKER
The contents of the Action Tracker were discussed.
The following actions were agreed to be closed:
2. Item 11: Joint Committee 3. Item 13: Spire Quality Information - will be added to quality report
quarterly 4. Item 15: Amendment to draft minutes
The following updates were provided:
5. Item 9: Locality Committee Annual Report – this will be reviewed at the next workshop
6. Item 12: Transforming Care Review – update in January 7. Item 14: Integrated Performance and Quality Report - update in
January
ACTION: The Action Tracker to be updated to reflect the updates MH
10. STROKE SERVICE CHANGE
An update on the outcomes of the stroke pathway redesign was presented to the Governing Body
1. The Governing Body noted that positive outcomes have been maintained in relation to performance, quality indicators and patient experience throughout the first year of the implementation of the business case. This has been achieved through robust system wide integrated working
2. Clarification was given that this region is one of the few which is compliant
3. Confirmation was given that there is evidence of a direct correlation with performance and when the service changes were made
PM arrived at 09.214. Colleagues agreed that the transformational leadership,
collaboration, systems approach and culture across the structure has been positive
5. Thrombolysis continues to be a challenge and linking with the Ambulance Service and Manchester University which is trialling an app for paramedics which we will be joining
6. The team was acknowledged for the informative presentation and work of the team
7. The learning points to share with different specialisms and the level of sustainability was noted including collaboration. It was agreed that sharing the presentation with the East and North Herts NHS Trust (ENHT) Board would be beneficial

Page 5 of 10
Item Subject Action by
8. The weekend working pattern of consultants was challenged and it was noted that neurologists support the weekend clinics
9. Value for money was challenged and it was noted that this information is benchmarked. The 3 day stay on the unit is an area to regulate and assurance was given that the finances and outputs are monitored
10. ACTION: Feedback from late referrals/attenders data to be broken down to practice level in future and circulated to locality chairs
11. Thanks were extended to GC for her commitment to the CCG during her tenure and wish her well in her retirement
The Governing Body approved the recommendation that the changes implemented across the stroke pathway are integrated into usual business
The Governing Body noted the outcomes from the changes to the stroke pathway
GC, JK, CR left the meeting at 09.50
SE
5. CHIEF EXECUTIVES REPORT
The Chief Executives Report which provided information on the activities being undertaken by the Clinical Commissioning Group was reviewed by the Governing Body.
1. Annual Assessments 2. Commissioning for Quality and Innovation 3. Public Health England’s new “One You” app 4. NHS Continuing Healthcare Operational Performance Targets 5. Transforming Care 6. The “Healthier Future Let’s Talk” consultation programme 7. Nascot Lawn will close in May and the 7 families impacted will be
supported during transition 8. The Public Health Peer Review Report has not been received at
this stage
The Governing Body noted the Chief Executives Report
6. GOVERNANCE REPORT
The Governance Report was reviewed by the Governing Body
1. The Governing Body noted and ratified the decisions made at the Governing Body Workshops
2. The Governing Body noted the report from the Governance and Audit Committee and approved the updated Terms of Reference

Page 6 of 10
Item Subject Action by
3. The Governing Body noted the Strategic Risk Register and Risk Controls Assurance Dashboard
4. The Governing Body approved the Assurance Framework and Corporate Risk Register Proposal
5. The Governing Body noted the Annual Audit Letter from External Audit
6. The Governing Body approved delegated authority to East and North Herts and Herts Valleys Clinical Commissioning Groups Joint Committee to approval proposals for service changes following completion of the “Healthier Future Let’s Talk” consultation programme
7. The Governing Body approved the Committee terms of reference 8. The Governing Body received the Register of Interests and
Register of Gifts and Hospitality 9. The level of “red” areas was clarified 10. RSM will continue as internal Auditors for a further year
The Governing Body approved the Governance Report
7. FINANCE REPORT
The Finance Report for month 4 (2017/18) was reviewed by the Governing Body
1. The Governing Body noted that the CCG financial position as at month 4 is an in-year surplus of £262k which is in addition to the cumulative brought forward plan. The CCG is forecasting to deliver an underspend of £14,498k, to meet the NHS England (NHSE) target control total
2. The Governing Body reviewed the key financial risks and mitigation measures as identified in the report
MT arrived at 09.543. Point 6e was challenged and noted that it is not reflected in the
activity chart. The terminology and use of language will be addressed
4. Elective resource spending was discussed and will be brought to each locality
5. The underspend on staff on page 13 was referred to and it was noted that additional support staff is considered during peak times in line with recruitment challenges
6. The statistics on Page 7 e.g. Accident and Emergency (A&E) statistics refer to East and North Herts NHS Trust activity and the charts refer to CCG activity
7. ACTION: SA to confirm the A&E figures in the month 6 Finance Report
The Governing Body noted the Finance Report
SA/AP

Page 7 of 10
Item Subject Action by
8. INTEGRATED PERFORMANCE AND QUALITY REPORT (IPQR)
The Integrated Performance and Quality Report was reviewed in depth by the Governing Body
1. The Governing Body considered the report which provided an update on the performance and quality of local NHS Trusts in relation to key national performance standards
2. The quality and performance information at CCG level and also at provider level was noted
3. ACTION: An update on e-referrals to be provided at the next Governing Body workshop 07.12.17
4. ACTION: Associate Directorate of Performance (Gerry Moir) to review the data regarding 2016/17 Quality Premium (on page 12 of the report)
5. The nurse assessment and links to psychology pathway were clarified
6. The data and outcomes regarding cancer performance was discussed and disappointment strongly expressed
7. The impact of the winter surges and breaches was considered. Further discussion included: July of this year was the NHS’s busiest month for A&E activity. Reference was made to a quality audit recently undertaken at East and North Herts NHS Trust (ENHT)
8. The good rating in the metrics for mental health was acknowledged
9. Clostridium difficile (C. difficile) data is being rigorously monitored as it is showing a sharp increase in our area. Antibiotic prescribing has been impacted by this and colleagues discussed the changes in antibiotic prescribing in the pathways. The Governing Body agreed that this is an area of concern and it was noted that GP input will be sought in the working party.
10. ACTION: C. difficile to be added as a target for 2018/19 under Antibiotics KPIs rolling 23 month
11. There have been 4 never events reported by ENHT 12. Concerns have been raised with NHS England and the Care
Quality Commission (CQC) and it was noted that the Private Ambulance Service (PAS) was issued a winding up notice by Her Majesty’s Revenue and Customs (HMRC) and East of England Ambulance Service Trust (EEAST) is providing a caretaker service. The CCG is working with the appointed receivers and monitoring the situation. The PAS staff on this area were acknowledged
DO left the meeting at 10.35 – 11.40RJ left the meeting at 10.38 – 10.40
13. Hertfordshire Partnership Foundation Trust (HPFT) is receiving a CQC visit
14. Spire – No areas of concern to bring to the attention of the Governing Body from information provided directly by Spire
RJ
GM
PW
Page 8 of 10
Item Subject Action by
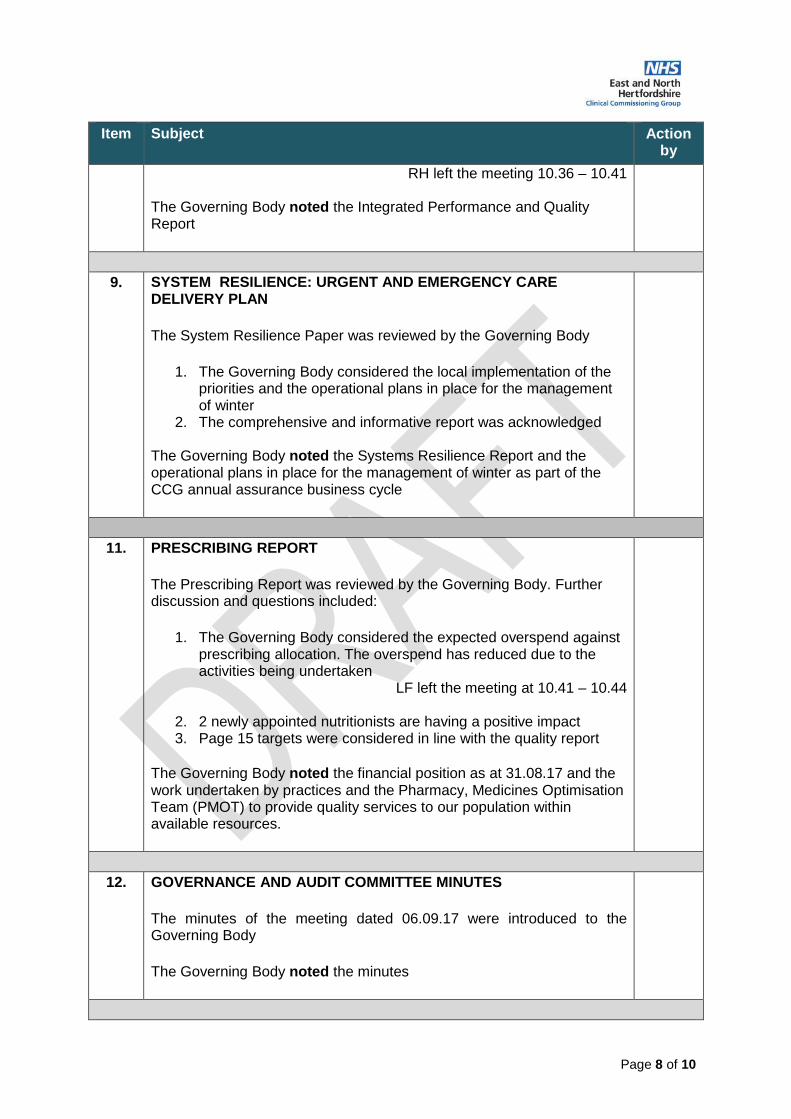
RH left the meeting 10.36 – 10.41
The Governing Body noted the Integrated Performance and Quality Report
9. SYSTEM RESILIENCE: URGENT AND EMERGENCY CARE DELIVERY PLAN
The System Resilience Paper was reviewed by the Governing Body
1. The Governing Body considered the local implementation of the priorities and the operational plans in place for the management of winter
2. The comprehensive and informative report was acknowledged
The Governing Body noted the Systems Resilience Report and the operational plans in place for the management of winter as part of the CCG annual assurance business cycle
11. PRESCRIBING REPORT
The Prescribing Report was reviewed by the Governing Body. Further discussion and questions included:
1. The Governing Body considered the expected overspend against prescribing allocation. The overspend has reduced due to the activities being undertaken
LF left the meeting at 10.41 – 10.44
2. 2 newly appointed nutritionists are having a positive impact 3. Page 15 targets were considered in line with the quality report
The Governing Body noted the financial position as at 31.08.17 and the work undertaken by practices and the Pharmacy, Medicines Optimisation Team (PMOT) to provide quality services to our population within available resources.
12. GOVERNANCE AND AUDIT COMMITTEE MINUTES
The minutes of the meeting dated 06.09.17 were introduced to the Governing Body
The Governing Body noted the minutes

Page 9 of 10
Item Subject Action by
13. HBL ICT STAKEHOLDER BOARD MINUTES
The minutes of the meeting dated 17.07.17 were introduced to the Governing Body
The Governing Body noted the minutes
14. JOINT COMMISSIONING PARTNERSHIP BOARD MINUTES
The minutes of the meeting dated 24.08.17 and 28.09.17 were introduced to the Governing Body
1. Concern was expressed with attendance and it was noted that the Governance arrangements and quorum have been reviewed and amended accordingly
The Governing Body noted the minutes
15. JOINT CO-COMMISSIONING COMMITTEE MINUTES
The minutes of the meeting dated 13.07.17 were introduced to the Governing Body
The Governing Body noted the minutes
16. LOCALITY COMMITTEE MINUTES
The minutes of the following locality meetings were introduced to the Governing Body
• North Hertfordshire dated 10.05.17 and 19.07.17
• Upper Lea Valley dated 12.07.17
• Welwyn and Hatfield dated 20.04.17 and 13.07.17
1. Concern was expressed that the minutes of localities are not being published in a timely fashion
2. ACTION: Locality managers to be contacted and minutes updated on the website
The Governing Body noted the minutes
HP

Page 10 of 10
Item Subject Action by
17. QUESTIONS FROM MEMBERS OF THE PUBLIC
1. There were no questions from the members of public present at the meeting
18. ANY OTHER BUSINESS
18.1 Workforce Survey:
1. A request was made for the business cycle to include monitoring of the staff survey specifically periodic reporting on workforce data e.g. sickness rates, turnover, mandatory training rates. The national survey concludes next month.
2. ACTION: The local workforce results will be brought to the next workshop for discussion
HS
19. DATE OF NEXT MEETING
Thursday 18th January 2018
09:00am – 11:00am - Public Session
11:00am – 12:00pm - Private Session
Focolare Centre, Meeting Room 1
The meeting closed at 10.52

Page | 1
Agenda Item No: 3.1
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Draft Minutes – Joint Committee Meeting
Decision or Approval Discussion Information
Report author: Jas Dosanjh, Corporate Governance Manager
Report signed off by: Hari Pathmanathan, Chair ENHCCG
Nicolas Small, Chair HVCCG
Executive Summary: To approve the draft Minutes of the Joint Committee Meeting held between East and North Herts CCG and Herts Valleys CCG on 12th
October 2017.
Recommendations
to the members:
To approve the Minutes.
Conflicts of Interest
involved:
There are none identified.
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.
Page 1 of 15
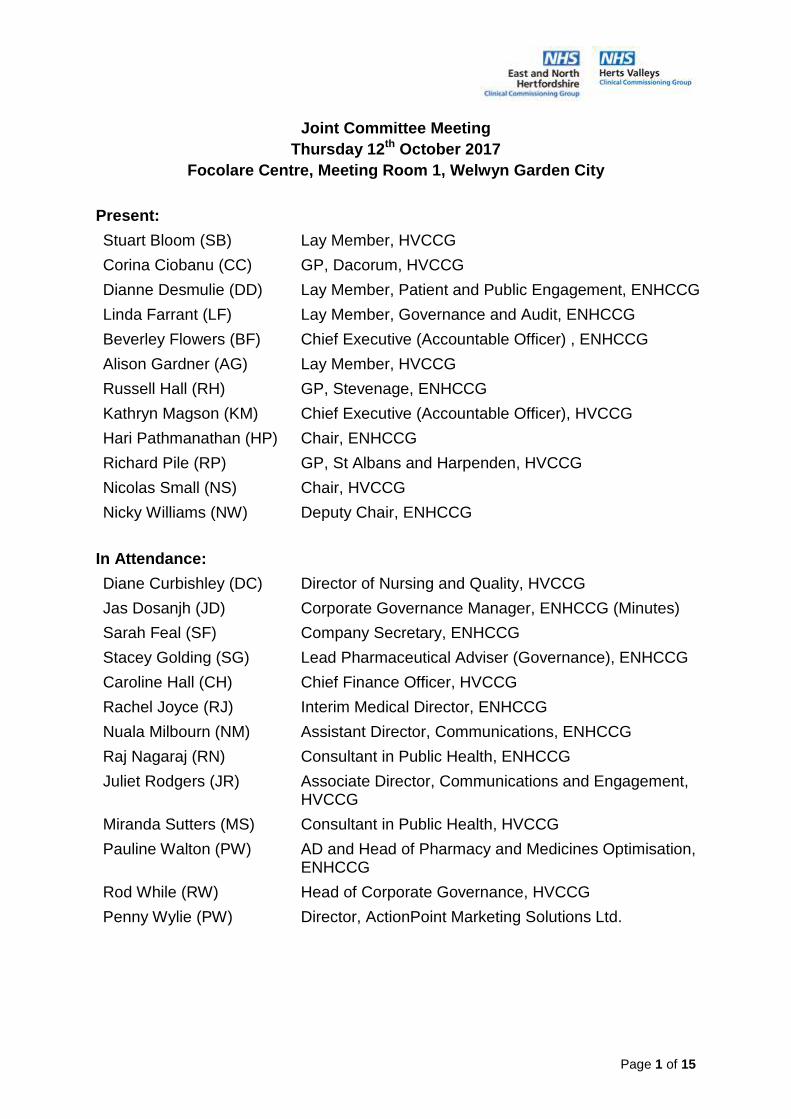
Joint Committee Meeting
Thursday 12th October 2017
Focolare Centre, Meeting Room 1, Welwyn Garden City
Present:
Stuart Bloom (SB) Lay Member, HVCCG
Corina Ciobanu (CC) GP, Dacorum, HVCCG
Dianne Desmulie (DD) Lay Member, Patient and Public Engagement, ENHCCG
Linda Farrant (LF) Lay Member, Governance and Audit, ENHCCG
Beverley Flowers (BF) Chief Executive (Accountable Officer) , ENHCCG
Alison Gardner (AG) Lay Member, HVCCG
Russell Hall (RH) GP, Stevenage, ENHCCG
Kathryn Magson (KM) Chief Executive (Accountable Officer), HVCCG
Hari Pathmanathan (HP) Chair, ENHCCG
Richard Pile (RP) GP, St Albans and Harpenden, HVCCG
Nicolas Small (NS) Chair, HVCCG
Nicky Williams (NW) Deputy Chair, ENHCCG
In Attendance:
Diane Curbishley (DC) Director of Nursing and Quality, HVCCG
Jas Dosanjh (JD) Corporate Governance Manager, ENHCCG (Minutes)
Sarah Feal (SF) Company Secretary, ENHCCG
Stacey Golding (SG) Lead Pharmaceutical Adviser (Governance), ENHCCG
Caroline Hall (CH) Chief Finance Officer, HVCCG
Rachel Joyce (RJ) Interim Medical Director, ENHCCG
Nuala Milbourn (NM) Assistant Director, Communications, ENHCCG
Raj Nagaraj (RN) Consultant in Public Health, ENHCCG
Juliet Rodgers (JR) Associate Director, Communications and Engagement, HVCCG
Miranda Sutters (MS) Consultant in Public Health, HVCCG
Pauline Walton (PW) AD and Head of Pharmacy and Medicines Optimisation, ENHCCG
Rod While (RW) Head of Corporate Governance, HVCCG
Penny Wylie (PW) Director, ActionPoint Marketing Solutions Ltd.
Page 2 of 15
MINUTES
Item Subject Action by
1. WELCOME AND APOLOGIES FOR ABSENCE
The meeting opened at: 14.02
The Chair of Governing Body at East and North Hertfordshire Clinical Commissioning Group (ENHCCG) welcomed all to the meeting, and advised that the meeting will be jointly chaired with the Chair of Board at Herts Valleys Clinical Commissioning Group (HVCCG).
The Chair (ENHCCG) provided an explanation of the format for the meeting and general housekeeping. It was explained that this is a special joint decision-making meeting held in public so that anyone interested (members of the public and journalists) can observe. It is the final stage in a long and considered process which has developed over a number of months, and each individual CCG governing body has discussed the proposals and the members here today are representing the views of their organisations.
The Chair advised that this is not a meeting at which the public can contribute to the debate and the Committee members have reviewed the meeting papers, which include the questionnaire results, public meeting notes and organisational responses. Representatives of the public have been invited to make three minute representations to the joint committee to reflect people’s personal experiences, as the Committee members want to ensure that the patient voice is heard by everyone involved in the decision making process today.
The Chair asked all those around the table to formally introduce themselves and state whether they are a voting member of the Committee (noted as Members on page 1).
No apologies were received.
2. DECLARATIONS OF INTERESTS
The Chair (HVCCG) invited the members to declare any declarations of interest or declarations relating to matters on the Agenda.
No declarations were made.

Page 3 of 15
Item Subject Action by
3. CHIEF EXECUTIVES’ INTRODUCTION
The Chair (HVCCG) invited the Chief Executives from both CCG’s [Beverley Flowers (BF) for ENHCCG and Kathryn Magson (KM)] to provide an explanation of circumstances which led to the consultation process being initiated.
BF and KM explained that:
• Currently this is a difficult time for the NHS due to a number of multi-faceted issues arising from the increasing demands placed on services, i.e. increase in population, but the income available to meet these needs is not growing at the same rate.
• There is a need to review the current provisions and, based on conversations with the public, advice was sought on how to run the consultation process and evaluation.
• Every attempt was made to obtain views from a range of communities, including those from hard to reach groups.
It was highlighted that the financial position of both CCG’s is different from one another and therefore may influence the outcomes of the final decisions taken.
The Chair thanked BF and KM, and introduced Juliet Rodgers (JR) and Nuala Milbourn (NM) who provided an overview of the consultation process, including how it evolved and was carried out.
JR and NM informed the Committee that:
• The consultation was approached jointly by both CCG’s in order to maximise resources and efficiency, to ensure that a common approach would be taken across the county.
• The consultation lasted 10 weeks and each CCG held their own processes for public engagement and feedback led by the Communications Teams.
• The parameters of consultation were clearly set out and the main aim was to reach as many people as possible to obtain views and feedback to inform the decision making process.
• There were 2500 responses and, although this may be a small percentage of the population, when benchmarked we have had a high response rate.

Page 4 of 15
Item Subject Action by
The Chair thanked JR and NM and asked the Committee members to comment on their experience of the consultation process.
The Committee members commented that:
• The public understand the challenges that the NHS is facing and want to get involved; this was demonstrated via the balanced views provided through attendance at planned events, with an increase in involvement from groups who do not usually attend such events.
• Some of the most effective engagement was through the unplanned events/held in locations not typically associated with health, as it allowed for views to be heard from those who don’t usually participate.
• The length of the consultation also provided greater opportunity for more people to get involved and have their views considered.
• The process was rigorous and supported by the CCGs’ Commissioning Prioritisation Framework, with all equality and quality impacts assessed.
Overall, the Committee members were in agreement that the consultation process has been robust and thorough.
4. STATEMENTS FROM INTERESTED PARTIES
The Chair (ENHCCG) invited the representatives of the public to address the Committee. The Committee heard five supporting statements.
The Chair thanked the representatives for sharing their personal experiences via these statements.
5. CONSULTATION – FINDINGS AND FEEDBACK
The Chair (HVCCG) introduced Penny Wylie (PW), Director of ActionPoint Marketing Solutions, and the company that hosted the survey, received both online and written responses and collated the results.

Page 5 of 15
Item Subject Action by
The Committee were advised that the Consultation was effectively broken down into two parts:
a) IVF and fertility services (ENHCCG, HVCCG and West Essex CCG);
• The total in favour of a reduction or stopping IVF was: 54% in ENH, 31% HV and 34% WE, with the majority of responses from those not affected.
• Responses included: - Stopping provisions could lead to mental health issues and
in turn cost the NHS more, - There should be a nationally agreed approach, - There could be an increased cost to the NHS when dealing
with patients who undergo IVF treatment abroad where it is available at a lower cost to private treatment in the UK.
b) Fitness for surgery, gluten-free prescribing, over the counter medicines, female sterilisation (ENHCCG and HVCCG), and vasectomy (HVCCG only);
Fitness for surgery –
• The overall majority were in favour of the proposals that those with a Body Mass Index (BMI); - Of 40+ should reduce weight before surgery: 85% in ENH
and 86% in HV, - Over 30 should reduce weight before surgery: 74% in ENH
and HV.
• In both ENH and HV 86% were in favour that smokers should be required to quit smoking before being referred for non-urgent surgery.
• Responses included: - Being asked to improve health before surgery is not
unreasonable, - Need to take some responsibility for our own health, - Weight loss is difficult for some people due to other health
issues, i.e. mobility.
Gluten-free prescribing –
• The overall majority were in favour of the proposal that gluten-free food should not be available on prescription with the

Page 6 of 15
Item Subject Action by
exception of people with learning disabilities: 76% in ENH and 78% in HV.
• Responses included: - Gluten-free food is widely available in the supermarkets, - It should remain for low income families, - A lot of foods are naturally gluten free already.
RP left the meeting at 15.14
Over the counter medicines –
• The overall majority were in favour of the proposal to limit the prescribing of medicines, products and food items that are available without prescription: 90% in ENH and 89% in HV.
RP re-joined the meeting at 15.16
• Responses included: - A lot of medicines are cheaper over the counter, - Low income families should still be entitled, - Money can be saved; the NHS needs to make cuts
somewhere.
Female sterilisation –
• The majority were in favour of the proposal to stop funding for female sterilisation except in exceptional circumstances: 64% in ENH and 61% in HV.
• Responses included: - Lots of alternative methods are available, - Unwanted pregnancy/children would cost more in long-run, - Should only be funded if there are medical
issues/exceptional circumstances. RN left the meeting at 15.20
Vasectomy –
• This was only considered by HVCCG and 55% were in favour of the proposal to stop funding vasectomy.
• Responses included: - Better/cheaper than consequences of an unwanted
pregnancy, - There are other forms of contraception available.
Page 7 of 15
Item Subject Action by
The Chair thanked PW and the ActionPoint team for the coordination and analysis of the responses.
It was explained that organisational responses to the consultation are including in the meeting papers. It was also explained that a number of detailed questions were raised during the consultation process, both online and postal, in meetings and in organisational submissions. Clinicians from both organisations have provided information in response to these questions and their responses are included in the meeting papers. It was noted that all of this information was provided to Committee members in advance of the meeting.
RN re-joined the meeting at 15.24
There were no questions for PW from the Committee members, and the Chair thanked all those who participated in the consultation to provide their views which will contribute to the outcomes to be reached during this meeting.
The meeting adjourned at 15.30 to 15.42
6. CONSULTATION – ISSUES AND OPTIONS
The Chair (ENHCCG) explained that the Committee will now discuss each proposal in turn, referencing the options and using the questions and responses to inform the discussion.
The Chair reminded the members of the Terms of Reference and that they have delegated authority on behalf of their board / governing body to make the decisions at this meeting and that that those decisions would be binding on the respective governing bodies.
Fitness for surgery
The original consultation proposal was:
o Morbidly obese patients with a BMI over 40 would need to reduce their weight by at least 15% over 9 months or reduce their BMI to less than 40 (whichever is greater) before having non‐urgent surgery;
o Obese patients with a BMI over 30 will not get non‐urgent surgery until they reduce their weight by 10% over 9 months or reduce to less than 30 (whichever is the greater);

Page 8 of 15
Item Subject Action by
o Smokers would be required to quit smoking before being referred for non‐urgent surgery;
There would still be individual exceptional cases where the policy would not apply - where delaying a procedure would cause harm.
The Committee discussed the proposal in relation to the responses:
• It was confirmed that the proposal in relation to routine planned surgery and exceptionality would be applied where the harm of not having surgery is high (i.e. excludes cancer patients, cardiology).
• It was highlighted that many people struggle to lose weight in line with the parameters and that this cohort of patients will require support. It was stated that support will be provided and that it has been found that ill health triggers often motivate people to act in a way to better their health. All agreed that there should be more opportunities at an early stage to highlight health concerns to patients and work with them to address these before they develop.
• It was noted that GPs should have the ability to refer any patient if they felt it was absolutely necessary.
• The use of the BMI calculator as an appropriate indicator of health concerns was queried. It was reported that all evidence and studies of patients in regards to this area have been based on BMI, but it is recognised that this is not the correct tool for all patients, i.e. those with a high muscle mass. Therefore, it will be important that the checks are reviewed correctly by the health professional in relation to the individual patients, and guidance will be provided.
The Chair (ENHCCG) reminded the Committee of the options:
1. Do nothing - retain the current BMI and smoke-free policy on non-urgent surgery;
2. Agree with the proposal with the option of exceptionality on an individual basis.
A vote was taken and counted, the Committee members agreed unanimously with option 2.

Page 9 of 15
Item Subject Action by
Over-the-counter medicines and products on prescription
The original consultation proposal was:
o Limit the prescribing of medicines, products and food items that are available without a prescription from a high‐street pharmacy, registered online pharmacy, supermarket or shop for short-term self-limiting conditions.
Exclusions to this policy would include: - Where there are safeguarding concerns - Patients with long term conditions, for example
osteoarthritis and the need for regular pain relief
The Committee discussed the proposal in relation to the responses:
• It was confirmed that this proposal would only apply to short-term conditions.
• It was queried how this potential change in practice would be implemented by GP’s. It was agreed that our focus would be on significant patient education into the specific medications that are available without a prescription and utilisation of communications via GP surgeries.
• The survey results demonstrated that patients feel this would be a positive change with benefits to be reaped through other avenues, such as freeing up appointment slots in the long-run. Initially appointments may be longer where GP’s attempt to work with patients to educate patients to take responsibility for their own health.
The Chair (ENHCCG) reminded the Committee of the options:
1. Do nothing - continue to prescribe medicines, products and food items readily available over the counter;
2. Agree with the proposal and the above exclusions.
A vote was taken and counted, the Committee members agreed unanimously with option 2.
The prescription of gluten-free foods
The original consultation proposal was:

Page 10 of 15
Item Subject Action by
o No longer provide gluten-free food on prescription with the exception of coeliac patients with learning disabilities or where there are safeguarding concerns.
The Committee discussed the proposal in relation to the responses:
• The quality of gluten-free food in supermarkets was queried. It was advised that there is a lot of choice available in supermarkets, and although some brands are fortified they are not the prime source for tackling deficiencies. There needs to be patient education in relation to other food groups, i.e. dairy, that can be consumed as part of a healthy diet, without over reliance on specific gluten-free produce.
• Clarification was sought regarding what a potential safeguarding concern might entail. It was advised that these would usually involve the welfare of children and concerns that may be raised where the gluten-free requirements of the child diet are not being managed by the primary carer. It was highlighted that GP’s undergo safeguarding training and are therefore equipped to identify any such concerns.
• It was agreed that, if this proposal is to be adopted, a plan will need to be put into place to clarify the process for patients who currently have repeat prescriptions for gluten-free food.
The Chair (HVCCG) reminded the Committee of the options:
1. Do nothing - retain the current CCG policy;
2. Agree with the proposal including the exception of coeliac patients with learning disabilities.
A vote was taken and counted, the Committee members agreed unanimously with option 2.
Female sterilisation
The original consultation proposal was:
o NHS in Hertfordshire would no longer fund female sterilisation except in exceptional circumstances, which would be assessed on a case‐by‐case basis if alternative forms of long‐acting contraception are unsuitable.
The Committee discussed the proposal in relation to the responses:

Page 11 of 15
Item Subject Action by
• Before a decision was made to consult on this area, there was a lot of evidence gathering with regards to alternative long acting safe and effective contraception for women.
• It was acknowledged that feedback received was in relation to the money that could be saved as other cheaper options for contraception are available.
The Chair (HVCCG) reminded the Committee of the options:
1. Do nothing - retain the current CCG policy;
2. Agree with the proposal including the option of exceptionality.
A vote was taken and counted, the Committee members agreed unanimously with option 2.
Vasectomy (HVCCG only)
It was noted that this proposal applies to the HVCCG area only.
The original consultation proposal was:
o HVCCG would no longer fund vasectomy except in exceptional circumstances.
Exclusions to this policy would include: - Where there are safeguarding concerns; - Where there are mental health issues to be taken into
account; - Where the patient is unable to use other forms of
contraception due to the harm they would cause and the only other clinical option is female sterilisation.
The Committee discussed the proposal in relation to the responses:
• It was noted that Herts Valleys CCG has recently adopted an interim policy, after seeking public views, which has stopped routine funding for male sterilisation (vasectomy) but allows funding in the exceptional circumstances (as listed above).
• It was noted that it had been highlighted through feedback that vasectomy is one of the minority contraceptive procedures that men take control of as most other forms of rely on women.

Page 12 of 15
Item Subject Action by
• A third option was proposed based on discussions that had taken place at HVCCG’s commissioning executive committee. This option is to allow access to the service if provided in the community based on agreed criteria. If this policy is adopted by HVCCG then the criteria will be consistent with that of ENHCCG.
The Chair (HVCCG) reminded the Committee of the options:
1. Do nothing - retain current CCG policy;
2. No longer fund vasectomy except in exceptional circumstances;
3. Allow access to the service if provided in the community, based on agreed criteria..
A vote was taken and counted, the Committee members agreed unanimously with option 3.
IVF and specialist fertility services
The original consultation proposal was:
o No longer fund IVF and other specialist fertility treatments, except in exceptional circumstances
The Committee discussed the proposal in relation to the responses:
• It was noted that each CCG has a different starting position with regards to the number of IVF cycles offered under the existing policies; - ENHCCG currently offers up to three cycles, - HVCCG have paused their current policy of offering one
cycle since 16 June 2017.
• The impact that this proposal could have on the mental health of patients who are refused treatment was queried. Assurance was provided that this aspect was investigated in depth prior to commencing the consultation process, however there are very few studies regarding this and a lack of evidence to support any particular views. There is, however, evidence that suggests there are increased rates of depression and other mental health related conditions for those who undergo IVF treatment (regardless of the outcome). However the mental health aspects are not as widely published as the successes.
Page 13 of 15
Item Subject Action by
• It was queried how the work of the Consortium would be affected if the change was to be implemented. It was confirmed that ENHCCG lead the wider range of providers within the Consortium, however it is down to the individual CCG’s to have their own policy in place with regards to the number of IVF cycles to be provided and therefore the decisions made at this meeting will not directly impact the Consortium work that the CCG lead on. It was advised that there are 12 months left for the current Consortium arrangements that are in place.
• The potential issue of ‘postcode lottery’ was raised whereby there may be some social injustice as a result of the proposal being adopted. It was advised that a review has been undertaken of patients seeking IVF and social deprivation, there was no evidence to suggest that there are more applicants from low income backgrounds.
• It was acknowledged that this proposal has received feedback, from those who value NHS funded IVF and specialist fertility treatments, with great strength of emotions and feelings.
• It was advised that spending has been reviewed in depth as part of the Prioritisation Framework and decisions have to be made to widely reduce expenditure. This has been a difficult issue but the decision to consult on this area was not taken lightly, there is a need to weigh up the evidence and how money is spent and both CCG’s are in a different financial position.
• The HVCCG policy has currently been paused for those who were at the end of the eligibility review (have been identified as suitable to receive IVF treatment) to ensure that there was not a sudden influx of demand and an unsustainable backlog whilst the policy was being consulted upon.. It was advised that, if it is agreed to adopt the proposal, those who have had their treatment paused will be provided with treatment in line with the latest policy (one cycle). Patients would be expected to be re-referred by their secondary care clinician by 31 December 2017 (with treatment to be completed within 12 months).
• HVCCG is taking a number of emergency financial measures that reflect the current financial position of the CCG. Should the decision be to stop funding, the policy should be reviewed again in 12 months’ time.
Page 14 of 15
Item Subject Action by
• It was confirmed and noted that ENHCCG is not currently under the same pause as HVCCG and treatment is being provided in line with the current policy (three cycles).
The Chair (ENHCCG) reminded the Committee of the options:
1. Continue to fund the current number of cycles offered (ENHCCG = three, HVCCG = one)
2. Reduce to two cycles (ENHCCG only)
3. Reduce to one cycle (ENHCCG only)
4. Stop funding, except in exceptional circumstances
5. Stop funding altogether
A vote was taken and counted, the Committee members agreed unanimously with:
- option 3 for ENHCCG, - option 4 for HVCCG reflecting the emergency financial
measures that the CCG is taking. The policy would be reviewed in 12 months’ time
The discussions regarding the proposals were drawn to a close as the Committee members unanimously agreed with selected options, within voting conducted in accordance with the delegated authority.
It was agreed that clear plans would be put into place to ensure a smooth implementation of the decisions agreed today.
7. ANY OTHER BUSINESS
No other business was raised for discussion.
8. MEETING CLOSE
The Chairs thanked all members of the public and media in attendance for taking their time to attend this meeting, stating that the views and information gathered during the consultation process have been a very important part of the decision making process and will go on to inform the implementation of the decisions taken.

Page 15 of 15
Item Subject Action by
The Communications Team at both CCG’s were thanked for their hard work and approach to ensure a robust consultation took place.
The meeting closed at: 16.57

Page | 1
Agenda Item No: 4
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Action Tracker
Decision or Approval Discussion Information
Report author: Maryla Hart, Governing Body Administrator
Tracey Middleton, Governing Body Clerk
Report signed off by: Jas Dosanjh, Corporate Governance Manager
Executive Summary: The purpose of this paper is to discuss the Action Tracker.
Recommendations
to the members:
To discuss the Action Tracker.
Conflicts of Interest
involved:
There are none identified.
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

NHS East and North Hertfordshire Clinical Commissioning Group Governing Body Meeting in Public Action Tracker
items for closure in yellow
Item
number
Meeting date Subject Action Responsible
manager
Deadline Past
deadlines
(Since
Revised)
Current position Status
9 23/11/2017 Integrated Performance and Quality Report
An update on e-referrals to be provided at the next Governing Body Workshop 07/12/2017
Medical Director 08/12/2017 24/11/2017 - This item is on the agenda for 07.12.17.
08/12/2017: An update was given at yesterday's
workshop.
To be closed at meeting
on 2018-01-18
12 23/11/2017 Finance Report SA to confirm the A&E figures in the month 6 Finance Report Chief Finance Officer / Deputy Chief Finance
Officer
01/01/2018 01/12/2017: These figures have been ciruclated to the
Governing Body.
To be closed at meeting
on 2018-01-18
14 21/09/2017 Transforming Care Review
Cancer pathway plans to be circulated Chief Executive 02/01/2018 Update not due til January.13/11/2017: ongoing
05/01/2018: Circulated
To be closed at meeting
on 2018-01-18
15 23/11/2017 Integrated Performance and Quality Report
Associate Director of Performance (Gerry Moir) to review the data regarding 2016/17 Quality Premium (on page 12 of the report).
Associate Directorate of Performance
18/01/2018 11/01/2018: Work completed and circulated to the
Governing Body.
To be closed at meeting
on 2018-01-18
16 23/11/2017 Locality Committee Minutes
Locality managers to be contacted and minutes updated on the website
Director of Commissioning
18/01/2018 11/01/2017: Completed and presented to GB
Workshop in Task & Finish Group 2 report
04/01/2018.
To be closed at meeting
on 2018-01-18
17 23/11/2017 AOB: Workforce Survey
The local workforce results will be brought to the next workshop for discussion
Director of Workforce
18/01/2018 12/12/2017: "Workforce Future Operating Model and Funding" on GB Workshop agenda for 4 Jan 18.
18/01/2018: To be discussed today under agenda
item 13.
To be closed at meeting
on 2018-01-18
18 23/11/2017 Integrated Performance and Quality Report
C. difficile to be added as a target for 2018/19 under Antibiotics KPIs rolling 23 month
AD & Head of Pharmacy & Medicines
Optimisation
18/01/2018 11/01/2017: The PMOT suggest that we should
reinstate the 2016/17 antibiotic prescribing
performance indicator for ‘broad spectrum
antibiotics’. This is still monitored by NHSE but is no
longer part of the Quality Premium. The target is still
set at 10%. Whether this is to be an incentivised KPI
under the CFF or just part of the PMOT monthly
monitoring schedule with practices is to be
confirmed.
Ongoing
19 23/11/2017 Stroke Service Change
Feedback from late referrals/attenders data to be broken down to practice level in future and circulated to locality chairs
Director of Operations
18/01/2018 04/01/2018: To be picked up as part of ENHT contract
monitoring.
Ongoing
11/01/2018 1

NHS East and North Hertfordshire Clinical Commissioning Group Governing Body Meeting in Public Action Tracker
items for closure in yellow
Item
number
Meeting date Subject Action Responsible
manager
Deadline Past
deadlines
(Since
Revised)
Current position Status
20 20/07/2017 Locality Committee Annual Report
It was agreed that the work of each locality should be reviewedat a GB workshop
Director of Commissioning
01/03/2018 02/11/2017 13/09/2017: Agreed to include Locality up date at the Governing Body away day event on 02-Nov-1713/11/2017: To be reviewed at the 21st December
workshop.
10/01/2018: This is to be presented at the Governing
Body Workshop on 22nd February 2018.
Ongoing
21 21/09/2017 Integrated Performance and Quality Report
The Chief Executive to raise quality concerns directly with the Chief Executive of ENHT.
Chief Executive 22/03/2018 23/11/2017 23/11/2017: Update in January
05/01/2018: Formal letter sent to ENHT and response
received and circulated. Board to Governing Body in
diary for February 2018. ENHT new Medical Director
and Director of Nursing in post.
Ongoing
11/01/2018 2
Page | 1
Agenda Item No: 5
Date of Meeting: 18 January 2018
Governing Body Meeting in Public
Paper Title: Integrated Performance and Quality Report
Decision or Approval Discussion Information
Report author: Gerry Moir – Associate Director Performance
Cath Slater – Associate Director Quality and Patient Experience
Report signed off by: Sharn Elton – Director of Operations
Sheilagh Reavey – Director of Nursing and Quality
Executive Summary: This Integrated Performance and Quality report provides an update on the performance and quality of local NHS Trusts in relation to key national performance standards. It includes quality and performance information at CCG level and also at provider level (ENHT, PAH, BCF, HCT, EEAST, HPFT, HUC, TPP and Private Providers).
The performance and quality metrics included within the report are published information predominantly for the October position. All metrics have been included with commentary for exceptions where performance standards have not been met.
Recommendations
to the members:
To note
Page | 2
Conflicts of Interest
involved:
None to declare.
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the consequences of a commissioning decision.
Non-Financial Professional Interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career.
Non-Financial Personal Interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit.
Indirect Interests This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision.
Page | 3
1. Executive summary (half page maximum)
This Integrated Performance and Quality report provides an update on the performance and quality of local NHS Trusts in relation to key national performance standards. It includes quality and performance information at CCG level and also at provider level (ENHT, PAH, BCF, HCT, EEAST, HPFT, HUC, TPP and Private Providers).
The performance and quality metrics included within the report are published information predominantly for the October position. All metrics have been included with commentary for exceptions where performance standards have not been met.
2. Background
N/A
3. Issues
N/A
4. Options
N/A
5. Resources implications
N/A
6. Risks/Mitigation Measures
N/A
7. Recommendations
To note
8. Next Steps (including when the decision will be reviewed)
N/A

Integrated Performance and Quality Report
January 2018

Contents |
Description Page Number
Introduction 3
NHS Constitution - CCG Level 6
Provider Profiles 28
ENHT 29
PAH 45
BCF 58
HCT 62
EEAST 72
HPFT 78
HUC 88
TPP 99
Private Providers 100
Glossary 101
2

Introduction|
3
This Integrated Performance and Quality report provides an update on the performance and quality of local NHS Trusts in relation to key national performance standards. It includes quality and performance information at CCG level and also at provider level. The performance and quality metrics included within the report are published information predominantly for the October position. All metrics have been included with commentary for exceptions where performance standards have not been met. A glossary of terms used in this report is provided in the back of this document. In this report the published metrics being reported are for October 2017 unless stated otherwise. Data Sources • Cancer Open Exeter data • Stroke SSNAP • RTT, A&E, Diagnostics, MSA, FFT, DToC and Cancelled Operations UNIFY2 data • Ambulance, DToC , Stroke, HPFT, HUC Trust Reports • HCAI, Safer Staffing, SI’s, Safeguarding, LAC ENHCCG Quality Dashboard Please note: all Trust data is looking at the Trust wide position unless stated as ENHCCG only data.
Key: ‘Increase/ decrease in performance from last period’ denotes the change in performance from the previous period: Improvement/Increased performance/activity compared to prior period; Deterioration/reduced performance/activity compared to prior period; No Change
‘Movement’ denotes increase/decrease in figures from previous period: + Increase in numbers from the previous period - Decrease in numbers from the previous period

Headline Summary
4
Comments ׀ Outlined below is a summary of the key areas of concern and underperformance that the CCG Governing Body need to be aware of. Detailed commentary is provided for each of the areas listed within the report.
CCG
1. Referral to Treatment 2. Diagnostic Waits 3. Cancer Waits 4. Accident & Emergency 5. Ambulance Performance
Slide 16 Slide 17 Slide 18 Slide 20 Slide 21
5. Mental Health 6. Dementia 6. HCAI 7. Safeguarding Adults 8. Safeguarding Children
Slide 22 Slide 24 Slide 25 Slide 26 Slide 27
Acute Trusts
ENHT PAH RFH
1. Stroke 2. Referral to Treatment 3. Cancer Waits 4. Accident & Emergency 5. Ambulance Handovers 6. Cancelled Ops & Outpatients 7. Serious Incidents 8. HCAI 9. Friends and Family 10. Workforce 11. Safer Staffing 12. Other
Slide 31 Slide 33 Slide 34 Slide 36 Slide 37 Slide 38 Slide 39 Slide 40 Slide 41 Slide 42 Slide 43 Slide 44
1. Accident & Emergency 2. Ambulance Handovers 3. Delayed Transfers of Care 4. Serious Incidents 5. HCAI 6. MSA 7. Friends and Family 8. Workforce 9. Safer Staffing 10. Other
Slide 47 Slide 48 Slide 49 Slide 50 Slide 51 Slide 52 Slide 53 Slide 54 Slide 55 Slide 56
1. Summary Cancer waits Diagnostics A&E RTT C.Diff &MRSA Never events Pressure Ulcers Workforce
Slide 59
Other Providers
HCT EEAST HPFT HUC
1. ALOS 2. DToCs 3. EDD 4. Serious Incidents 5. Workforce 6. Safer Staffing 7. PALMS 8. Other
Slide 63 Slide 64 Slide 65 Slide 66 Slide 67 Slide 69 Slide 70 Slide 71
1. AQIs 2. Response Times 3. Turnaround Times
Slide 73 Slide 75 Slide 77
1. Access 2. Safe & Effective 3. CAMHS 4. DToCs 5. Serious Incidents 6. Workforce 7. Other
Slide 80 Slide 81 Slide 82 Slide 83 Slide 84 Slide 85 Slide 87
1. Integrated Urgent Care 2. Serious Incidents 3. Workforce
Slide 90 Slide 97 Slide 98
TPP Slide 99 Private Providers Slide 100
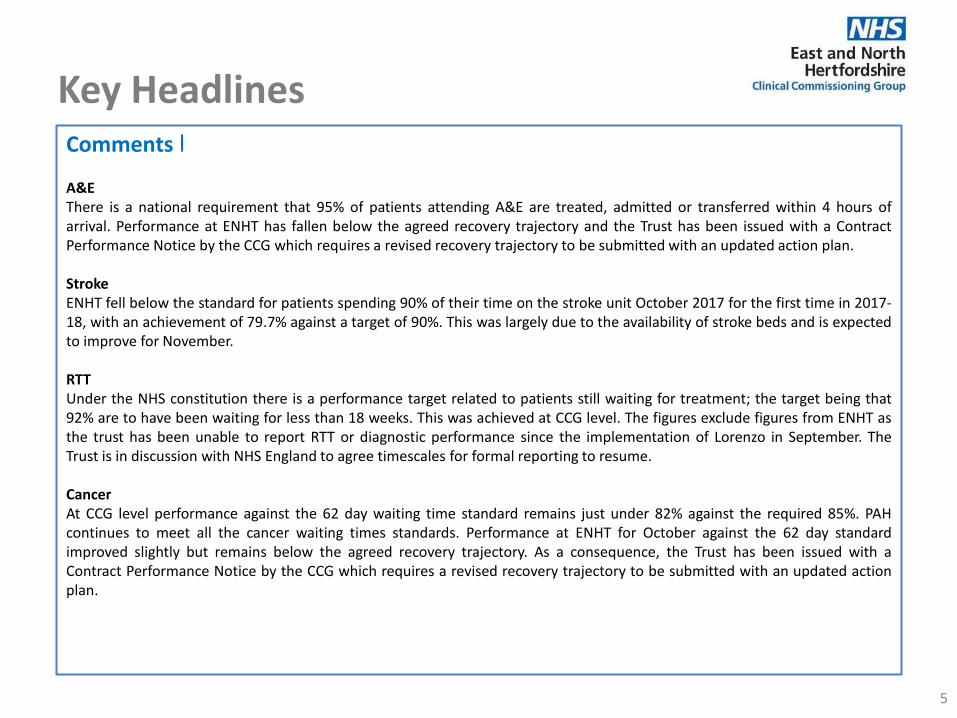
Key Headlines
5
Comments ׀ A&E There is a national requirement that 95% of patients attending A&E are treated, admitted or transferred within 4 hours of arrival. Performance at ENHT has fallen below the agreed recovery trajectory and the Trust has been issued with a Contract Performance Notice by the CCG which requires a revised recovery trajectory to be submitted with an updated action plan. Stroke ENHT fell below the standard for patients spending 90% of their time on the stroke unit October 2017 for the first time in 2017-18, with an achievement of 79.7% against a target of 90%. This was largely due to the availability of stroke beds and is expected to improve for November. RTT Under the NHS constitution there is a performance target related to patients still waiting for treatment; the target being that 92% are to have been waiting for less than 18 weeks. This was achieved at CCG level. The figures exclude figures from ENHT as the trust has been unable to report RTT or diagnostic performance since the implementation of Lorenzo in September. The Trust is in discussion with NHS England to agree timescales for formal reporting to resume. Cancer At CCG level performance against the 62 day waiting time standard remains just under 82% against the required 85%. PAH continues to meet all the cancer waiting times standards. Performance at ENHT for October against the 62 day standard improved slightly but remains below the agreed recovery trajectory. As a consequence, the Trust has been issued with a Contract Performance Notice by the CCG which requires a revised recovery trajectory to be submitted with an updated action plan.
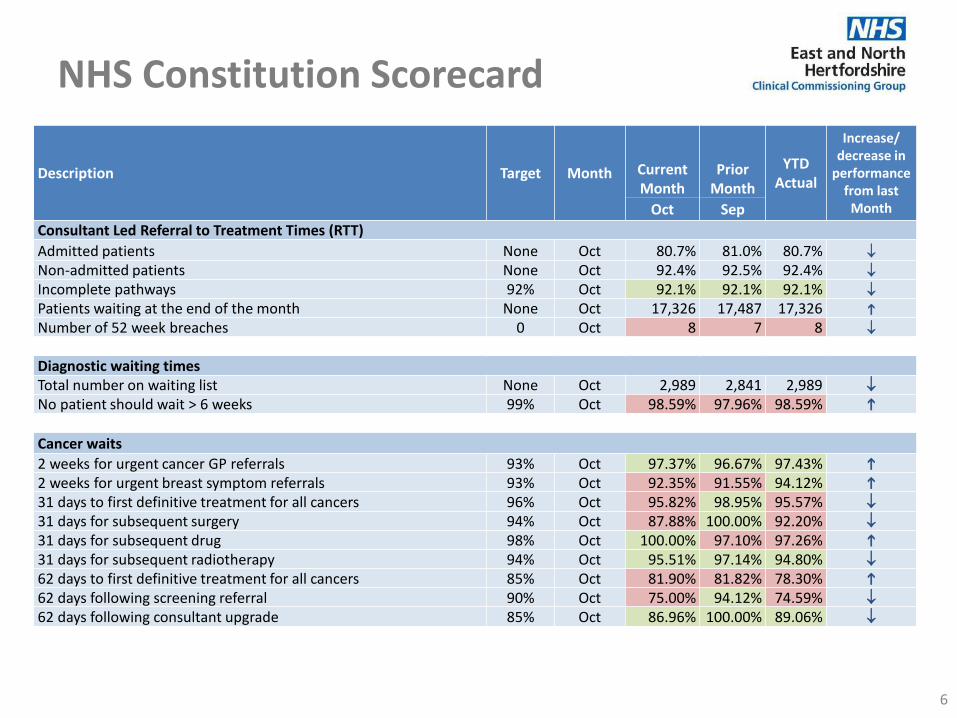
NHS Constitution Scorecard
6
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Consultant Led Referral to Treatment Times (RTT)
Admitted patients None Oct 80.7% 81.0% 80.7%
Non-admitted patients None Oct 92.4% 92.5% 92.4%
Incomplete pathways 92% Oct 92.1% 92.1% 92.1%
Patients waiting at the end of the month None Oct 17,326 17,487 17,326
Number of 52 week breaches 0 Oct 8 7 8
Diagnostic waiting times Total number on waiting list None Oct 2,989 2,841 2,989
No patient should wait > 6 weeks 99% Oct 98.59% 97.96% 98.59%
Cancer waits
2 weeks for urgent cancer GP referrals 93% Oct 97.37% 96.67% 97.43%
2 weeks for urgent breast symptom referrals 93% Oct 92.35% 91.55% 94.12%
31 days to first definitive treatment for all cancers 96% Oct 95.82% 98.95% 95.57%
31 days for subsequent surgery 94% Oct 87.88% 100.00% 92.20%
31 days for subsequent drug 98% Oct 100.00% 97.10% 97.26%
31 days for subsequent radiotherapy 94% Oct 95.51% 97.14% 94.80%
62 days to first definitive treatment for all cancers 85% Oct 81.90% 81.82% 78.30%
62 days following screening referral 90% Oct 75.00% 94.12% 74.59%
62 days following consultant upgrade 85% Oct 86.96% 100.00% 89.06%
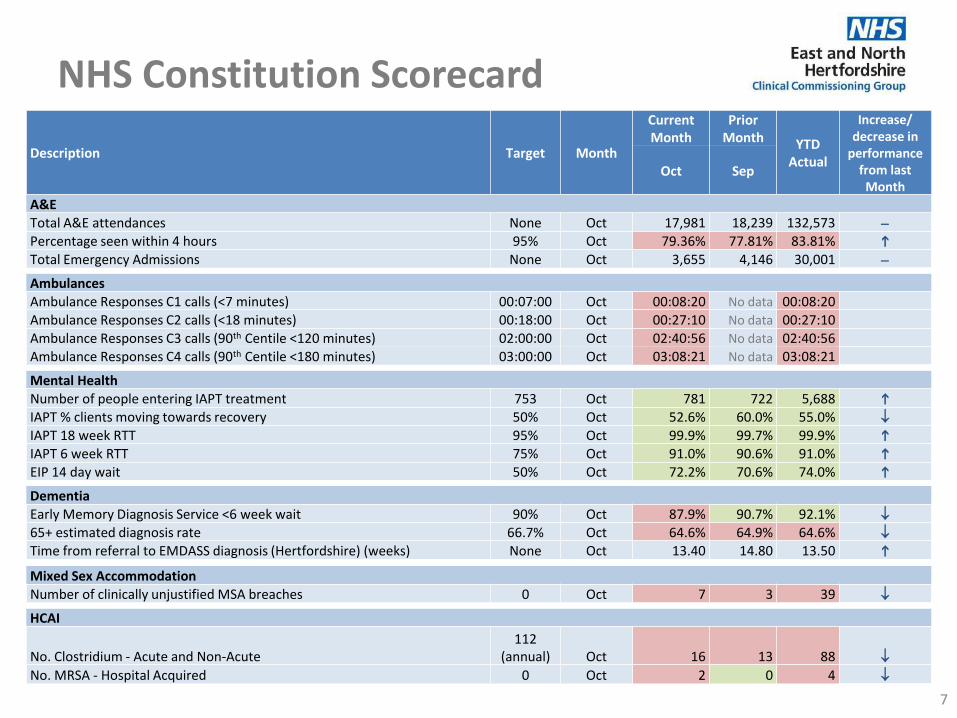
NHS Constitution Scorecard
7
Description Target Month
Current Month
Prior Month YTD
Actual
Increase/ decrease in
performance from last
Month Oct Sep
A&E Total A&E attendances None Oct 17,981 18,239 132,573 -
Percentage seen within 4 hours 95% Oct 79.36% 77.81% 83.81%
Total Emergency Admissions None Oct 3,655 4,146 30,001 -
Ambulances Ambulance Responses C1 calls (<7 minutes) 00:07:00 Oct 00:08:20 No data 00:08:20 Ambulance Responses C2 calls (<18 minutes) 00:18:00 Oct 00:27:10 No data 00:27:10 Ambulance Responses C3 calls (90th Centile <120 minutes) 02:00:00 Oct 02:40:56 No data 02:40:56 Ambulance Responses C4 calls (90th Centile <180 minutes) 03:00:00 Oct 03:08:21 No data 03:08:21
Mental Health Number of people entering IAPT treatment 753 Oct 781 722 5,688
IAPT % clients moving towards recovery 50% Oct 52.6% 60.0% 55.0%
IAPT 18 week RTT 95% Oct 99.9% 99.7% 99.9%
IAPT 6 week RTT 75% Oct 91.0% 90.6% 91.0%
EIP 14 day wait 50% Oct 72.2% 70.6% 74.0%
Dementia Early Memory Diagnosis Service <6 week wait 90% Oct 87.9% 90.7% 92.1%
65+ estimated diagnosis rate 66.7% Oct 64.6% 64.9% 64.6%
Time from referral to EMDASS diagnosis (Hertfordshire) (weeks) None Oct 13.40 14.80 13.50
Mixed Sex Accommodation Number of clinically unjustified MSA breaches 0 Oct 7 3 39
HCAI
No. Clostridium - Acute and Non-Acute 112
(annual) Oct 16 13 88
No. MRSA - Hospital Acquired 0 Oct 2 0 4

ENHCCG | CCG Improvement and Assessment Framework (IAF) Metrics
8
The table below shows the most recent performance against the 51 CCG IAF metrics, some of which are new for 2017/18. The benchmark position from 2016/17, for which ENHCCG was rated as outstanding, has been provided and the table has been formatted to show whether performance has improved or deteriorated since that rating. Of the 41 metrics with updated data available, there has been no change in 16, an improvement in 16, and 8 showing a slightly worsening position, and 1 (A&E 4 hour performance) showing a more significant reduction.
Area Indicator Name Frequency
of
Monitoring
Benchmark
Performance
used for
2016/17
Detailed description Latest
Period of
reporting
Performance
Better/
Worse/
No
change
Better Health
1 Child
obesity
Percentage of children aged 10-11 classified as overweight or
obese Annually 28.90% overweight or obese
2013/14 to
2015/16 29.10%
2
Diabetes
Diabetes patients that have achieved all the NICE-
recommended treatment targets: Three (HbA1c, cholesterol
and blood pressure) for adults and one (HbA1c) for children
Annually 41.7% 91.7% participation in the NDA. 2015/16 41.7%
3 People with diabetes diagnosed less than a year who attend a
structured education course Annually 4.8% 93.3% participation in the NDA. 2014 4.80%
4 Falls Injuries from falls in people aged 65 and over Quarterly 1921 falls per 100,000 population 2016/17 Q4 1966
5
Personalisat
ion and
choice
Personal health budgets Quarterly 18.6 per 100,000 population 2017/18 Q1 21
6 Health
inequalities
Inequality in unplanned hospitalisations for chronic ambulatory
care sensitive conditions
Quarterly
(Rolling 12
months to
latest
quarter)
2476
Rate of emergency admissions for urgent care sensitive
conditions in the most deprived areas of a CCG
compared with the least deprived
2016/17 Q4 2325
7 Anti-
microbial
resistance
Anti-microbial resistance: Appropriate prescribing of antibiotics
in primary care Quarterly 1.2
Total number of prescription items for antibacterial
drugs within the CCG in the previous 12 months 2017 10 1.097
8 Anti-microbial resistance: Appropriate prescribing of broad
spectrum antibiotics in primary care Quarterly 8.60%
Number of prescription items within the CCG in the
previous 12 months (at or below target of 10%) 2017 06 8.70%
9 Carers
Quality of life of carers
207/18: Proportion of carers with a long term condition who
feel supported to manage their condition
Annually 0.81 Average health status (EQ-5DTM) score Not
available Not available
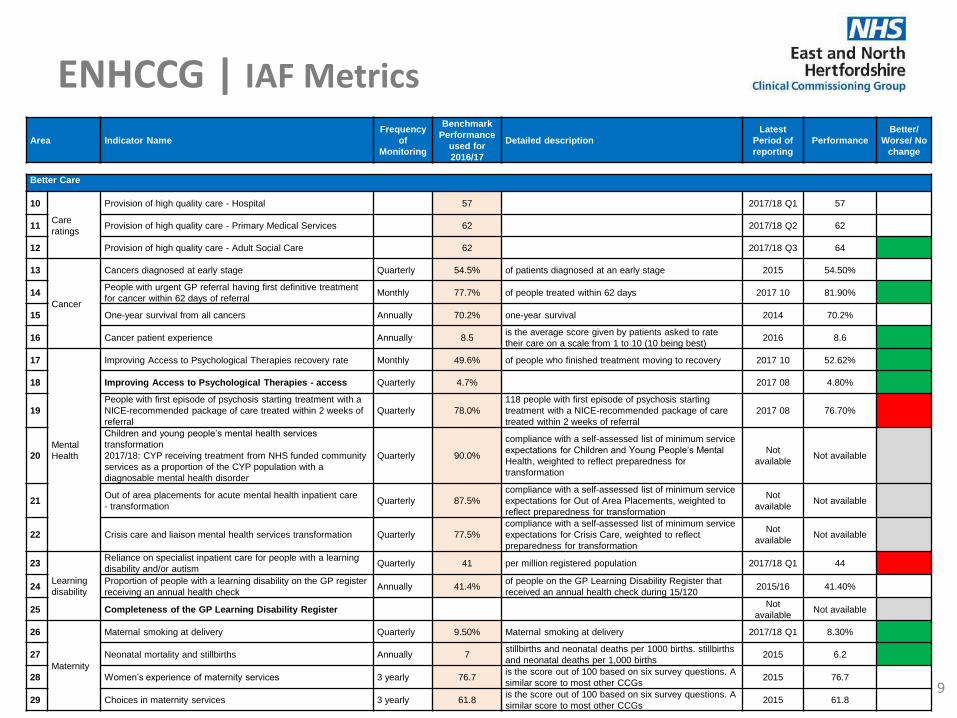
ENHCCG | IAF Metrics
9
Area Indicator Name
Frequency
of
Monitoring
Benchmark
Performance
used for
2016/17
Detailed description
Latest
Period of
reporting
Performance
Better/
Worse/ No
change
Better Care
10
Care
ratings
Provision of high quality care - Hospital 57 2017/18 Q1 57
11 Provision of high quality care - Primary Medical Services 62 2017/18 Q2 62
12 Provision of high quality care - Adult Social Care 62 2017/18 Q3 64
13
Cancer
Cancers diagnosed at early stage Quarterly 54.5% of patients diagnosed at an early stage 2015 54.50%
14 People with urgent GP referral having first definitive treatment
for cancer within 62 days of referral Monthly 77.7% of people treated within 62 days 2017 10 81.90%
15 One-year survival from all cancers Annually 70.2% one-year survival 2014 70.2%
16 Cancer patient experience Annually 8.5 is the average score given by patients asked to rate
their care on a scale from 1 to 10 (10 being best) 2016 8.6
17
Mental
Health
Improving Access to Psychological Therapies recovery rate Monthly 49.6% of people who finished treatment moving to recovery 2017 10 52.62%
18 Improving Access to Psychological Therapies - access Quarterly 4.7% 2017 08 4.80%
19
People with first episode of psychosis starting treatment with a
NICE-recommended package of care treated within 2 weeks of
referral
Quarterly 78.0%
118 people with first episode of psychosis starting
treatment with a NICE-recommended package of care
treated within 2 weeks of referral
2017 08 76.70%
20
Children and young people’s mental health services
transformation
2017/18: CYP receiving treatment from NHS funded community
services as a proportion of the CYP population with a
diagnosable mental health disorder
Quarterly 90.0%
compliance with a self-assessed list of minimum service
expectations for Children and Young People’s Mental
Health, weighted to reflect preparedness for
transformation
Not
available Not available
21 Out of area placements for acute mental health inpatient care
- transformation Quarterly 87.5%
compliance with a self-assessed list of minimum service
expectations for Out of Area Placements, weighted to
reflect preparedness for transformation
Not
available Not available
22 Crisis care and liaison mental health services transformation Quarterly 77.5%
compliance with a self-assessed list of minimum service
expectations for Crisis Care, weighted to reflect
preparedness for transformation
Not
available Not available
23
Learning
disability
Reliance on specialist inpatient care for people with a learning
disability and/or autism Quarterly 41 per million registered population 2017/18 Q1 44
24 Proportion of people with a learning disability on the GP register
receiving an annual health check Annually 41.4%
of people on the GP Learning Disability Register that
received an annual health check during 15/120 2015/16 41.40%
25 Completeness of the GP Learning Disability Register Not
available Not available
26
Maternity
Maternal smoking at delivery Quarterly 9.50% Maternal smoking at delivery 2017/18 Q1 8.30%
27 Neonatal mortality and stillbirths Annually 7 stillbirths and neonatal deaths per 1000 births. stillbirths
and neonatal deaths per 1,000 births 2015 6.2
28 Women’s experience of maternity services 3 yearly 76.7 is the score out of 100 based on six survey questions. A
similar score to most other CCGs 2015 76.7
29 Choices in maternity services 3 yearly 61.8 is the score out of 100 based on six survey questions. A
similar score to most other CCGs 2015 61.8

ENHCCG | IAF Metrics
10
Area Indicator Name Frequency of
Monitoring
Benchmark
Performance
used for
2016/17
Detailed description
Latest
Period of
reporting
Performance
Better/
Worse/
No
change
Better Care
30
Dementia
Estimated diagnosis rate for people with dementia Monthly 65.4% of the estimated number of people with dementia have a
recorded diagnosis 2017 11 64.50%
31 Dementia care planning and post-diagnostic support Quarterly 78.0% of patients with dementia whose care plan has been
reviewed in the preceding 12 months 2015/16 78%
32
Urgent and
emergency
care
Emergency admissions for urgent care sensitive
conditions Quarterly 2259 emergency admissions per 100,000 population 2016/17 Q4 2234
33 Percentage of patients admitted, transferred or
discharged from A&E within 4 hours Monthly 83.70% within 4 hours 2017 10 79.36%
34 Delayed transfers of care attributable to the NHS per
100,000 population Monthly 22.1 delayed transfers per 100,000 population 2017 08 13.3
35 Population use of hospital beds following emergency
admission Quarterly 499.9 days per 1,000 population 2016/17 Q4 499.7
36 End of Life
Care
Percentage of deaths with three or more
emergency admissions in last three months of life
Not
available Not available
37
Primary
medical care
Patient experience of GP services 6 monthly 82.30% of people rating experience as good 2017 81.30%
38 General Practice extended access - percentage of
registered population offered full extended access Bi-annual 1.70% practices in the CCG offering 'full provision'
Not
available Not available
39 Primary care workforce TBC 0.84 full time equivalent per 1000 weighted patients 2017 03 0.88
40 Elective
access
Patients waiting 18 weeks or less from referral to
hospital treatment Monthly 92.60% 18 weeks 2017 10 92.10%
41 7 day
services
Achievement of clinical standards in the delivery of 7
day services 6 Monthly
Not
available Not available
42
NHS
Continuing
Healthcare
People eligible for standard NHS Continuing
Healthcare (eligible per 50,000 population)
2018/18: Percentage of CHC full assessments taking
place in an acute hospital setting
Quarterly 39.30% 2017 08 50.50%
43 Patient
Safety
Evidence that sepsis awareness training amongst
healthcare professionals has been prioritised by
the CCG
Not
available Not available

ENHCCG | IAF Metrics
11
Area Indicator Name
Frequency
of
Monitoring
Benchmark
Performance
used for
2016/17
Detailed description
Latest
Period of
reporting
Performance
Better/
Worse/
No
change
Sustainability
44 Financial
sustainability In-year financial performance Quarterly Green
Assessment of whether CCG is likely to meet
plan 2017/18
Q1 Green
45 Paper-free at
the point of care
Utilisation of the NHS e-referral service to enable
choice at first routine elective referral Monthly 48.60% below target of 80% 2017 10 60.51%
Leadership
46
Probity and
corporate
governance
Probity and corporate governance Quarterly Fully compliant Rating 2017/18
Q1 Fully compliant
47 Workforce
engagement
Staff engagement index Annually 3.82 engagement index on a 1 to 5 scale (5 good) 2016 3.82
48 Progress against workforce race equality standard Annually 0.11 score (higher scores indicate higher differences,
0 indicates equality) 2016 0.11
49 CCGs’ local
relationships
Effectiveness of working relationships in the local
system Annually 61.58
score based on a score based on a 67%
response rate 2016/17 61.58
50
Patient and
community
engagement
Compliance with statutory guidance on patient
and public participation in commissioning health
and care
Not
available Not available
51 Quality of
leadership Quality of CCG leadership Quarterly Green
2017/18
Q1 Green
OVERALL OUTSTANDING
Better 16
Worse 9
No Change 16
Not available 10
Total 51

ENHCCG | Quality Premium 2017/19
12
National /
Local
QP
Domain/AreaDetail
% Value of
QPTarget
2017-18
YTD
2017-18 YTD
£
Early Cancer
Diagnosis
Demonstrate an improvement of 4 percentage points in the proportion of cancers* diagnosed at stages 1
and 2 in the 2017 calendar year compared to the 2016 calendar year. Or; Achieve a proportion of 60%
of cancers* diagnosed at stages 1 and 2 in the 2017 calendar year. *specif ic cancer sites,
morphologies and behaviour - invasive malignancies of breast, prostate, colorectal, lung, bladder, kidney,
ovary, uterus, non-Hodgkin lymphomas, and invasive melanomas of skin.
17% TBC
GP Access
and
Experience
CCGs w ill need to demonstrate in the July 2018 publication of the GP Patient Survey, either:
• 85% of respondents w ith ‘very good or good’ experience; Or
• 3 percentage point increase from July 2017 of respondents w ho said they had a ‘very good’ or ‘good’
experience of making a GP appointment.
17% 69%
Measure 1: CCGs must ensure that in more than 80% of cases w ith a positive NHS CHC Checklist, the
NHS CHC eligibility decision is made by the CCG w ithin 28 days from receipt of the Checklist (or other
notif ication of potential eligibility)
80% or above
92.31% 250,179£
Measure 2: CCGs must ensure that less than 15% of all full NHS CHC assessments take place in an
acute hospital setting.15% or below 46.67% 250,179£
Improved
access to
Children &
Young
People’s MH
services
Required performance is w hichever is the greater of:
At least a 14% increase in the number of individual children and young people aged 0-18 w ith a
diagnosable Mental Health condition starting treatment in NHS funded community services w hen they
need it in 2017/18 based on 2016/17 baseline;
The increase in activity to enable 32% of children and young people aged 0-18 w ith a diagnosable Mental
Health condition starting treatment in NHS funded community services w hen they need it in 2017/18.
17% TBC
3.825%<=0.933% 0.724% 112,580£
3.83% <=13,727 13,657 112,580£
Part C) items per STAR-PU must be equal to or below England 2013/14 mean performance value of
1.161 items per STAR-PU. This threshold w ill remain during 2018/19 (10% of indicator).1.70% <=1.161 1.097 50,036£
LocalBreast Cancer
Screening
The percentage of w omen aged 50-70 w ho w ere screened for breast cancer in the last three years.
CCG to achieve low er of 17/18 England Average or 1% improvement on 16/17 baseline15% TBC
£ 525,375
RTT Incomplete Standard -33%92% or bespoke
trajectory 92.10%* £ -
Maximum 4 hour w aits in A&E Departments -33%95% or bespoke
trajectory 79.36% -£ 175,125
Maximum tw o month (62-day) w ait from urgent GP referral to f irst definitive treatment for cancer -33%85% or bespoke
trajectory81.90% -£ 175,125
Financial
Gatew ay
CCG to manage w ithin its total resource envelope for 2017/18 and not exceed the agreed level of
surplus draw dow n-100%
Loss of all QP if
not met
Quality
Gatew ay
CCG local provider in case of serious quality failure and CCG not considered to be making an
appropriate, proportional response w ith partners to resolve the failure -100%
Loss of all QP if
not met
-£ 350,250
£ 175,125
National
National
Sub total of Gateway performance
Total QP Due
Aw aiting data
Aw aiting data
Aw aiting data
Continuing
Health Care
Bloodstream
Infections
Part A) reduction in the number of gram negative blood stream infections:
- A 10% reduction (or greater) in all E coli BSI reported at CCG level based on 2016 performance data.
(35% of indicator);
- Collection & reporting of a core primary care data set for all E coli BSI in Q2-4 17/18. (10% of indicator).
Part B) reduction of inappropriate antibiotic prescribing for UTI in primary care:
- A 10% reduction (or greater) in the Trimethoprim: Nitrofurantoin prescribing ratio based on CCG
baseline data (June 2015-May 2016) for 2017/18. (22.5% of indicator);
- A 10% reduction (or greater) in the number of trimethoprim items prescribed to patients aged 70 years
or greater on baseline data (June 2015-May 2016) for 2017/18. (22.5% of indicator).
Constitution
Gatew ay
Sub total of QP Indicator performance
TBC
8.5%
8.5%
First data released May
2018
Data released July 2018
5.95%
1.7%

ENHCCG | Quality Premium 2017/19
13
Comments ׀ The Quality Premium (QP) is a reward to CCGs for improvements in the quality of services that they commission and for associated improvements in health outcomes. The total amount payable to CCGs for achievement of the QP is based on £5 per head of population; for ENHCCG, this equates to a potential QP of £2.9M per year. Payment is awarded on the basis of national and local measures being met. Final payment is also dependent on: • The CCG managing within its total resource envelope; failure to do so will result in the loss of any QP payment achieved. • Serious quality failure of a local provider; if the CCG is not considered to be making an appropriate response with partners to resolve
the quality failure this will result in the CCG not achieving any of its payment. • Performance against a set of national constitutional requirements (18 week Referral to Treatment, A&E 4hr Standard and the Cancer
62 Day Wait); failure to meet national targets or agreed bespoke trajectories will result in a reduction to the amount of QP payable (33% per requirement) .
2017/18 Month 7 Performance (see table on next slide for detail): Information is still awaited for metrics worth 74% of the Quality Premium. Of known performance, Pharmacy is currently on track to meet Parts B and C of the Bloodstream Infections Indicator worth £275k of the QP. At Month 7, CHC met the first part of their indicator to ensure that in more than 80% of cases with a positive NHS CHC Checklist, the NHS CHC eligibility decision was made within 28 days from receipt of the Checklist; performance across previous months for this indicator (worth £250k) has been inconsistent however with year to date performance currently below target. CHC are currently not meeting the second part of their indicator which is to ensure that less than 15% of all full NHS CHC assessments take place in an acute hospital setting. Discharge to Assess beds have now gone live which may recover final year performance for the first part of the CHC indicator, however it is unlikely that the second part will recover unless there is a change in methodology for reporting, which has been raised as a national issue. Based on Month 7 known performance (26%), the CCG are currently achieving £525k of QP performance indicators. This is reduced to £175k however with the current failure to achieve constitutional gateways for the A&E 4hr standard and Cancer 62 day wait standard. We are currently shown to be achieving the 18 week referral to treatment gateway, however E&NHT are currently not reporting against this standard. If they were reporting , the QP achievement may be reduced further.
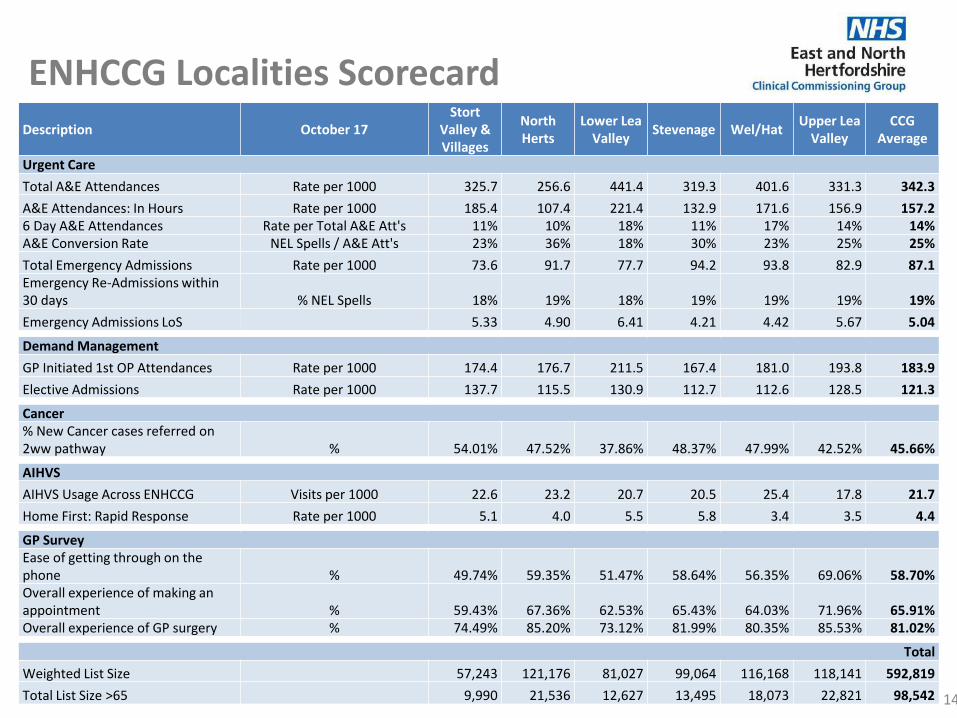
ENHCCG Localities Scorecard
14
Description October 17 Stort
Valley & Villages
North Herts
Lower Lea Valley
Stevenage Wel/Hat Upper Lea
Valley CCG
Average
Urgent Care
Total A&E Attendances Rate per 1000 325.7 256.6 441.4 319.3 401.6 331.3 342.3
A&E Attendances: In Hours Rate per 1000 185.4 107.4 221.4 132.9 171.6 156.9 157.2 6 Day A&E Attendances Rate per Total A&E Att's 11% 10% 18% 11% 17% 14% 14% A&E Conversion Rate NEL Spells / A&E Att's 23% 36% 18% 30% 23% 25% 25%
Total Emergency Admissions Rate per 1000 73.6 91.7 77.7 94.2 93.8 82.9 87.1 Emergency Re-Admissions within 30 days % NEL Spells 18% 19% 18% 19% 19% 19% 19%
Emergency Admissions LoS 5.33 4.90 6.41 4.21 4.42 5.67 5.04
Demand Management
GP Initiated 1st OP Attendances Rate per 1000 174.4 176.7 211.5 167.4 181.0 193.8 183.9
Elective Admissions Rate per 1000 137.7 115.5 130.9 112.7 112.6 128.5 121.3
Cancer % New Cancer cases referred on 2ww pathway % 54.01% 47.52% 37.86% 48.37% 47.99% 42.52% 45.66%
AIHVS
AIHVS Usage Across ENHCCG Visits per 1000 22.6 23.2 20.7 20.5 25.4 17.8 21.7
Home First: Rapid Response Rate per 1000 5.1 4.0 5.5 5.8 3.4 3.5 4.4
GP Survey Ease of getting through on the phone % 49.74% 59.35% 51.47% 58.64% 56.35% 69.06% 58.70% Overall experience of making an appointment % 59.43% 67.36% 62.53% 65.43% 64.03% 71.96% 65.91% Overall experience of GP surgery % 74.49% 85.20% 73.12% 81.99% 80.35% 85.53% 81.02%
Total
Weighted List Size 57,243 121,176 81,027 99,064 116,168 118,141 592,819
Total List Size >65 9,990 21,536 12,627 13,495 18,073 22,821 98,542

ENHCCG | Localities
15
Comments ׀ Activity Shifts since August report: - Aside from some minor changes, the A&E Attendance and Emergency figures are largely unchanged from the previous report;
most notable is a slight increase in the Average Length of Stay. - GP Initiated 1st Outpatient Attendances are higher across all Localities, with the exception of Stort Valley & Villages - The Elective Admission rate shows a small increase across all Localities. - AIHVS utilisation (updated to September) is reduced across all Localities, with the overall rate reduced by 0.5/1,000. - Home First (Rapid Response) utilisation is not significantly different, although the utilisation rate varies between the Localities. - Cancer and GP Survey figures are unchanged.
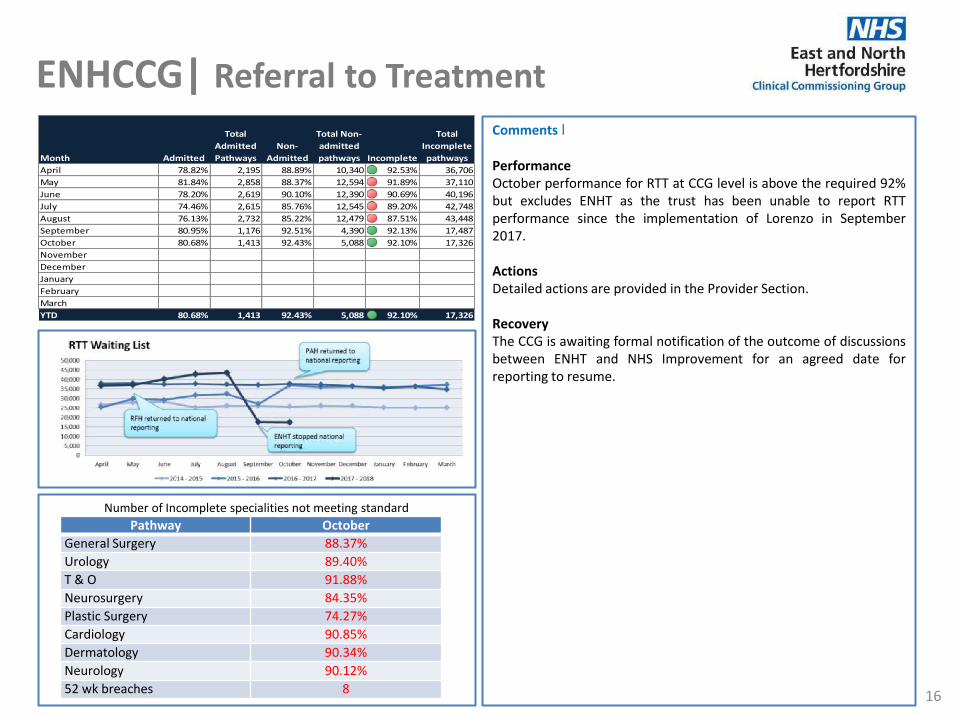
ENHCCG| Referral to Treatment
16
Comments ׀ Performance October performance for RTT at CCG level is above the required 92% but excludes ENHT as the trust has been unable to report RTT performance since the implementation of Lorenzo in September 2017. Actions Detailed actions are provided in the Provider Section. Recovery The CCG is awaiting formal notification of the outcome of discussions between ENHT and NHS Improvement for an agreed date for reporting to resume.
Number of Incomplete specialities not meeting standard
Pathway October
General Surgery 88.37%
Urology 89.40%
T & O 91.88%
Neurosurgery 84.35%
Plastic Surgery 74.27%
Cardiology 90.85%
Dermatology 90.34%
Neurology 90.12%
52 wk breaches 8
Month Admitted
Total
Admitted
Pathways
Non-
Admitted
Total Non-
admitted
pathways Incomplete
Total
Incomplete
pathways
April 78.82% 2,195 88.89% 10,340 92.53% 36,706
May 81.84% 2,858 88.37% 12,594 91.89% 37,110
June 78.20% 2,619 90.10% 12,390 90.69% 40,196
July 74.46% 2,615 85.76% 12,545 89.20% 42,748
August 76.13% 2,732 85.22% 12,479 87.51% 43,448
September 80.95% 1,176 92.51% 4,390 92.13% 17,487
October 80.68% 1,413 92.43% 5,088 92.10% 17,326
November 0.00% 0 0.00% 0 0.00% 0
December 0.00% 0 0.00% 0 0.00% 0
January 0.00% 0 0.00% 0 0.00% 0
February 0.00% 0 0.00% 0 0.00% 0
March 0.00% 0 0.00% 0 0.00% 0
YTD 80.68% 1,413 92.43% 5,088 92.10% 17,326
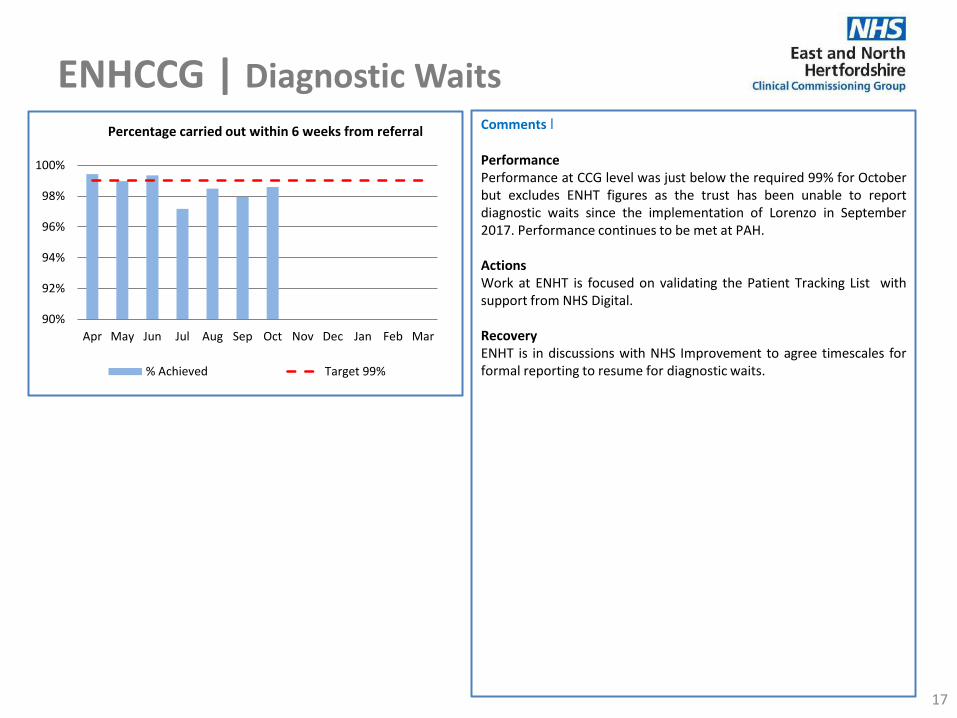
ENHCCG | Diagnostic Waits
17
Comments ׀ Performance Performance at CCG level was just below the required 99% for October but excludes ENHT figures as the trust has been unable to report diagnostic waits since the implementation of Lorenzo in September 2017. Performance continues to be met at PAH. Actions Work at ENHT is focused on validating the Patient Tracking List with support from NHS Digital. Recovery ENHT is in discussions with NHS Improvement to agree timescales for formal reporting to resume for diagnostic waits.
90%
92%
94%
96%
98%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage carried out within 6 weeks from referral
% Achieved Target 99%
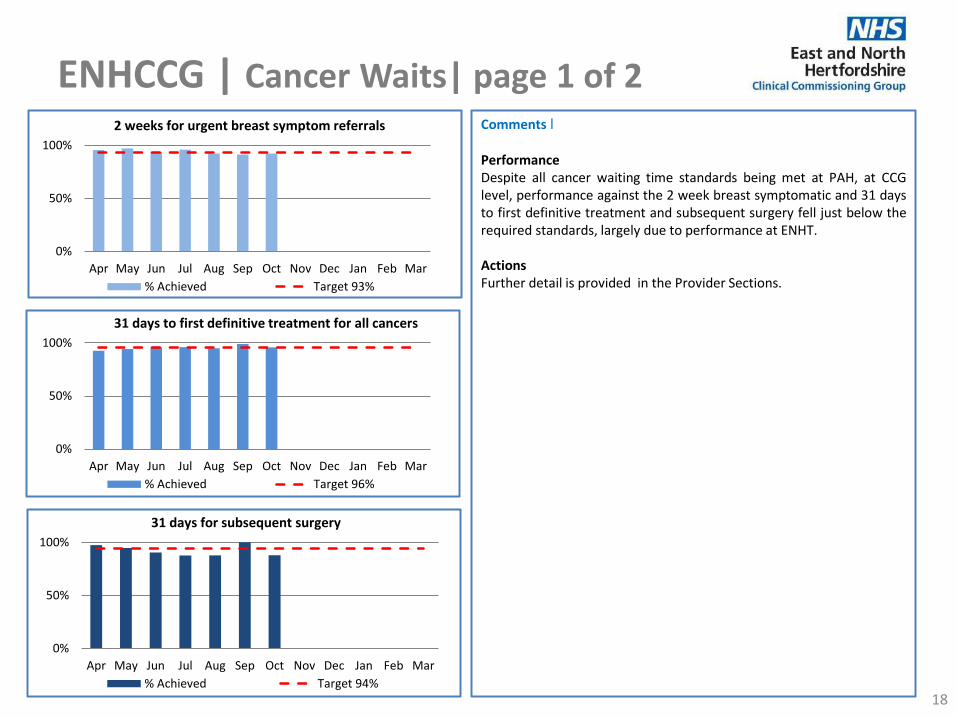
ENHCCG | Cancer Waits| page 1 of 2
18
Comments ׀ Performance Despite all cancer waiting time standards being met at PAH, at CCG level, performance against the 2 week breast symptomatic and 31 days to first definitive treatment and subsequent surgery fell just below the required standards, largely due to performance at ENHT. Actions Further detail is provided in the Provider Sections.
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2 weeks for urgent breast symptom referrals
% Achieved Target 93%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
31 days for subsequent surgery
% Achieved Target 94%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
31 days to first definitive treatment for all cancers
% Achieved Target 96%

ENHCCG | Cancer Waits| page 2 of 2
19
Comments ׀ Performance Performance at CCG level against the 62 day standard to first definitive treatment remains below the required 85%, but has increased month on month since June and is at just under 82% for October. Although all cancer standards are being met at PAH, performance at ENHT remains challenging, particularly in relation to the 62 day standard. Actions The CCG has issued ENHT with a Contract Performance Notice which requires the trust to submit a revised recovery trajectory with an updated action plan to the CCG.
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
62 days to first definitive treatment for all cancers
% Achieved Target 85%
0
10
20
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
100+ Day Cancer Waits ENHCCG Patients
ENHT Other Provider
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
62 days following screening referral
% Achieved Target 90%
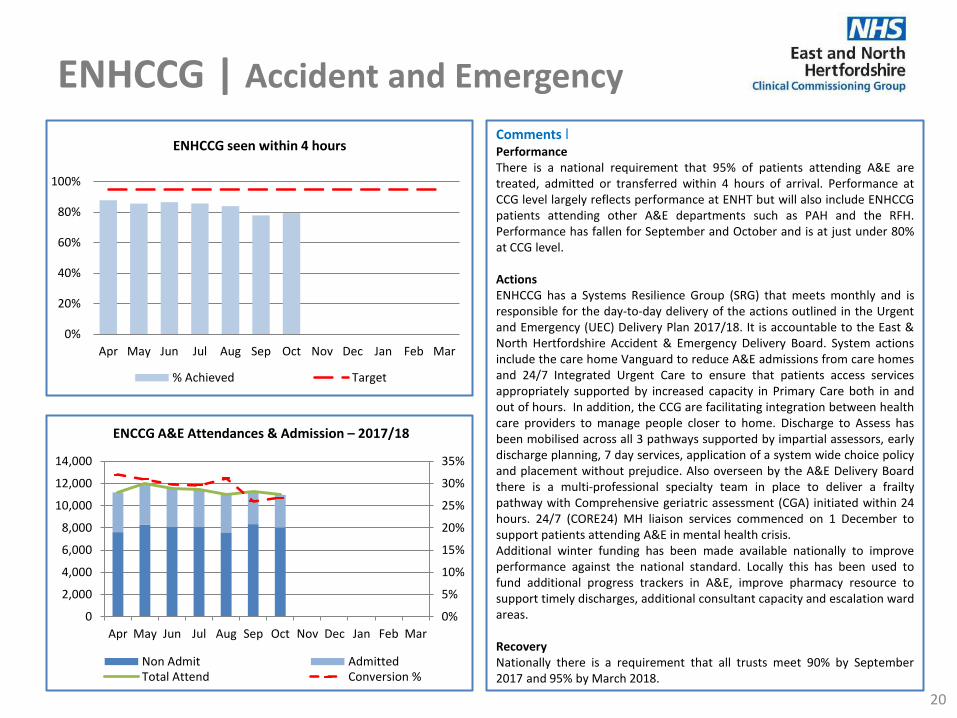
ENHCCG | Accident and Emergency
20
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHCCG seen within 4 hours
% Achieved Target
Comments ׀ Performance There is a national requirement that 95% of patients attending A&E are treated, admitted or transferred within 4 hours of arrival. Performance at CCG level largely reflects performance at ENHT but will also include ENHCCG patients attending other A&E departments such as PAH and the RFH. Performance has fallen for September and October and is at just under 80% at CCG level. Actions ENHCCG has a Systems Resilience Group (SRG) that meets monthly and is responsible for the day-to-day delivery of the actions outlined in the Urgent and Emergency (UEC) Delivery Plan 2017/18. It is accountable to the East & North Hertfordshire Accident & Emergency Delivery Board. System actions include the care home Vanguard to reduce A&E admissions from care homes and 24/7 Integrated Urgent Care to ensure that patients access services appropriately supported by increased capacity in Primary Care both in and out of hours. In addition, the CCG are facilitating integration between health care providers to manage people closer to home. Discharge to Assess has been mobilised across all 3 pathways supported by impartial assessors, early discharge planning, 7 day services, application of a system wide choice policy and placement without prejudice. Also overseen by the A&E Delivery Board there is a multi-professional specialty team in place to deliver a frailty pathway with Comprehensive geriatric assessment (CGA) initiated within 24 hours. 24/7 (CORE24) MH liaison services commenced on 1 December to support patients attending A&E in mental health crisis. Additional winter funding has been made available nationally to improve performance against the national standard. Locally this has been used to fund additional progress trackers in A&E, improve pharmacy resource to support timely discharges, additional consultant capacity and escalation ward areas. Recovery Nationally there is a requirement that all trusts meet 90% by September 2017 and 95% by March 2018.
0%
5%
10%
15%
20%
25%
30%
35%
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENCCG A&E Attendances & Admission – 2017/18
Non Admit AdmittedTotal Attend Conversion %

ENHCCG | Ambulance Performance
21
Comments ׀ Performance New ambulance performance standards came into operation at the end of October to measure ambulance response times. There are 4 new categories of call with associated required average response times: C1 People with life threatening injuries and illness (<7 minutes) C2 Emergency calls (<18 minutes) C3 Urgent calls (<120 minutes) C4 Less urgent calls (<180 minutes) The charts show performance for average response times for EEAST for ENHCCG patients only which are currently not being met. Actions Specific actions are detailed in the provider section under EEAST.
00:00
02:00
04:00
06:00
08:00
10:00
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses C1 calls ENHCCG (<7 minutes)
Av Response Time Av Target < 7 mins
00:0005:0010:0015:0020:0025:0030:00
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses C2 calls ENHCCG (<18 minutes)
Av Response Time Av Target < 18 mins
00:00:0000:45:0001:30:0002:15:0003:00:0003:45:00
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses C3 (<120 mins) and C4 calls (<180 mins) ENHCCG
C3 90th Centile Response Time C4 90th Centile Response Time
C3 Target < 120 mins C4 Target < 180 mins

ENHCCG | Mental Health | page 1 of 2
22
Comments ׀ Performance Performance year to date is above target although the CCG has had 644 more people enter treatment than planned for, but is still expected to reach 17.5% against a target of 16.8%. Encouragingly, this increased access has been met with sustained recovery rates above the 50% target. At this stage of the year, it is highly likely that the CCG will meet and exceed the recovery target. Actions Continued monitoring for deterioration in proxy measures which indicate likely forthcoming slippage in access and recovery: - Referrals - Conversion rate (to entering treatment) - First to second treatment waits - Matched paired scores Recovery None required at this time as targets are being met.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
IAPT % clients moving towards recovery
% Achieved Target 50%
0
200
400
600
800
1,000
1,200
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
People entering IAPT treatment
Number entering through AQP Number entering through HPFT
Combined Target 16.8%

ENHCCG | Mental Health | page 2 of 2
23
Comments ׀ Performance IAPT wait time performance continues to be exceeded against both 6 and 18 week targets despite over projected demand for the service year to date. Actions Continued monitoring of first to second treatment wait times within the service, as well as recovery rates, to ensure the service is operating effectively. Performance Early Intervention Psychosis (EIP) 14 days waits continue to be met. Actions Work is underway with the service to address the increase in demand on this service. Recovery The current increase of referrals and the numbers entering the system for EIP means that the service will have to increase its provision in order to meet the demand and target in 18/19.
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
IAPT 18 week RTT
% Achieved Target 95%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
IAPT 6 week RTT
% Achieved Target 75%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
EIP 14 day wait
% Achieved Target 50%
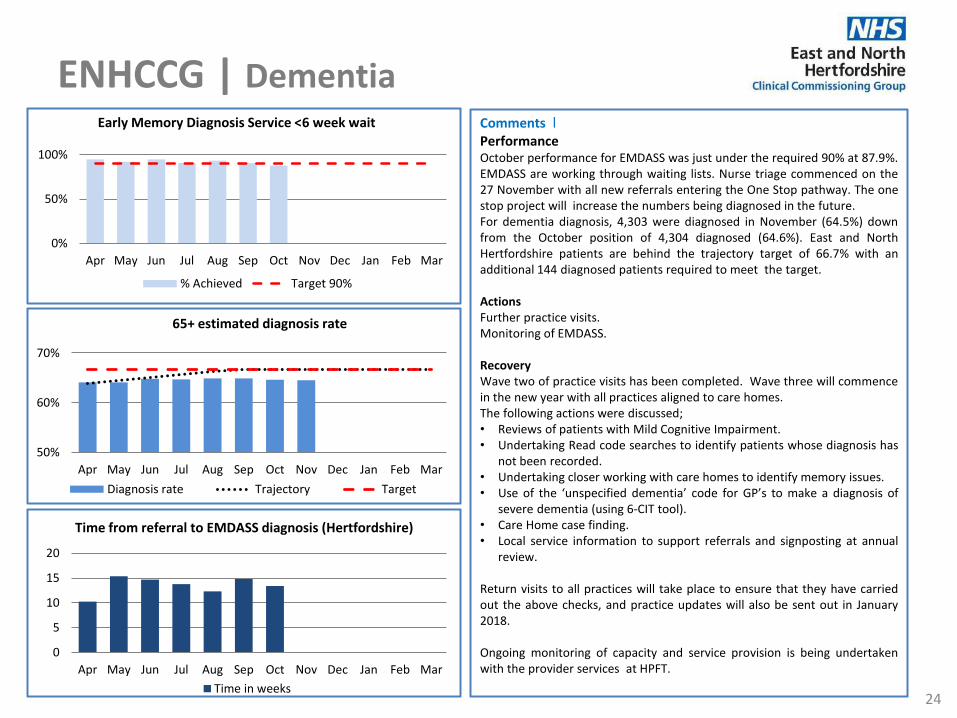
ENHCCG | Dementia
24
Comments ׀ Performance October performance for EMDASS was just under the required 90% at 87.9%. EMDASS are working through waiting lists. Nurse triage commenced on the 27 November with all new referrals entering the One Stop pathway. The one stop project will increase the numbers being diagnosed in the future. For dementia diagnosis, 4,303 were diagnosed in November (64.5%) down from the October position of 4,304 diagnosed (64.6%). East and North Hertfordshire patients are behind the trajectory target of 66.7% with an additional 144 diagnosed patients required to meet the target. Actions Further practice visits. Monitoring of EMDASS. Recovery Wave two of practice visits has been completed. Wave three will commence in the new year with all practices aligned to care homes. The following actions were discussed; • Reviews of patients with Mild Cognitive Impairment. • Undertaking Read code searches to identify patients whose diagnosis has
not been recorded. • Undertaking closer working with care homes to identify memory issues. • Use of the ‘unspecified dementia’ code for GP’s to make a diagnosis of
severe dementia (using 6-CIT tool). • Care Home case finding. • Local service information to support referrals and signposting at annual
review. Return visits to all practices will take place to ensure that they have carried out the above checks, and practice updates will also be sent out in January 2018. Ongoing monitoring of capacity and service provision is being undertaken with the provider services at HPFT.
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Early Memory Diagnosis Service <6 week wait
% Achieved Target 90%
0
5
10
15
20
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Time from referral to EMDASS diagnosis (Hertfordshire)
Time in weeks
50%
60%
70%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
65+ estimated diagnosis rate
Diagnosis rate Trajectory Target

ENHCCG | HCAI
25
population. This slightly below the regional rate of 1.0 and slightly above the national rate of 0.84 per 100,000 population. Post Infection Reviews have been undertaken and an action plan created to address all issues identified within the reviews. These include the fact that routine admission screening had been missed at ENHT. The trust MRSA policy is being reviewed accordingly, and a move to the routine MRSA screening of all acute admissions is planned. Progress against these is being monitored via the Herts IPC Group, and any concerns over lack of progress can be escalated to the QRM if required. Escherichia coli Blood Stream Infection (BSI)
By the end of November 2017, the number of cases reported within the CCG remained above ceiling for that point in the year. The CCG had a rate of 48.11 per 100,000 compared to a regional rate of 47.59 and a national rate of 43.38. As expected 85% of all cases were assigned to the community, and 70% had a recorded primary source of upper or lower urinary tract. An HCAI focus group has been established to review the surveillance data and review progress against the CCG action plan to address E coli BSI. Membership and terms of reference for the Hertfordshire Best Practice UTI Group have been reviewed to fully represent the health economy, and is now Chaired by the CCG and held monthly. A work plan for this group has been developed and includes reductions in catheterised discharged patients from acute care, creation of a catheter formulary, and extension to phase 2 of the care home “To dip or not to dip” educational programme to cover prevention of UTI, hydration, catheter care and recognition of the deteriorating patient.
Comments ׀
Clostridium difficile (CDI) In November 17, the number of C. diff reports declined when compared to previous months. To date during 17/18 the rate of infection per 100,000 population was 16.64 which was slightly below the regional rate of 16.72, but above the national rate of 14.16. Approximately two thirds of cases were apportioned to the community. An HCAI focus group has been established and is meeting monthly to review cases and actions to reduce CDI cases. These include investigation by a pharmacist to establish if individual community cases are linked to antibiotic use within primary care. Presentations regarding antibiotic prescribing and CDI are also planned for the locality Target events in February 18. Trust C diff action plans will also be shared with other Nursing and Quality team members so that actions can also be monitored during Quality Assurance visits. MRSA Blood Stream Infection (BSI) A total of 5 cases have been reported between April and November 2017, against a zero tolerance. This equates to a rate of 0.90 per 100,000
0
20
40
60
80
100
120
Ap
r
May Jun
Jul
Au
g
Sep
Oct
No
v
De
c
Jan
Feb
Mar
ENHCCG C-Diff Cases 2017/18
2016-17cumulative cases
2017-18cumulative cases
2017-18cumulative limit
0
100
200
300
400
Ap
r
May Jun
Jul
Au
g
Sep
Oct
No
v
Dec Jan
Feb
Mar
2016/17Cumulative Cases
2017/18Cumulative Cases
2017/18Cumulative Limit

ENHCCG | Safeguarding Adults
26
Comments ׀ In December the CCG Head of Adult Safeguarding participated in the Domestic Abuse Topic Group led by members of the County Council. Evidence was provided outlining the role the CCG plays in seeking to reduce the levels of domestic abuse and the support to victims through contracts, education, information and assurance processes. Initial feedback concentrates on encouraging the development of champions within each organisation. One GP has already been identified to be a champion. Following the letter from NHSE wanting to understand the progress that NHS organisations have made in reaching compliance with the Prevent Duty, the Head of Adult Safeguarding sought assurance from all four trusts; All organisations are in a position to upload Prevent data onto Unify2 for Q3 early in January 2018. There are systems of assurance from ward to board which includes that board members receive Prevent training
All organisations have in place a clear delivery plan to reach the 85% compliance target for prevent training
All organisations have policies and procedures in place to support staff. The Head of Adult Safeguarding has commissioned an audit of MCA practice within provider organisations similar to the one undertaken in 2014. This audit will take place in March and April 2018 and will include interviews with staff and review of cases. This will provide a picture of the progress made over the last 4 years and the further work that is required. In November the Hertfordshire Safeguarding Adult’s Board held a development session to review the strategic objectives and set the business plan for next year. In December the Head of Adult Safeguarding and Director of Nursing and Quality undertook an adult safeguarding assurance visit to HPFT. Overall we were overall assured regarding the standard of adult safeguarding within the organisation and the significant progress that the organisation has made within the year. A number of recommendations were made and HPFT will provide an action plan that will be monitored in year by the Head of Adult Safeguarding. There were a number of areas of good practice including:
The organisation has introduced a schedule of monthly audits that will be undertaken by operational managers and quality assured by the Local Authority.
Domestic abuse training has been provided to medical staff.
Questions around ‘Feeling safe’ are now asked at admission, on transfer and discharge to provide better oversight of patients’ experiences.
The organisation has developed a daily dashboard to provide operational managers with oversight of all safeguarding concerns raised within their quadrants.
All providers continue to work towards their compliance targets for adult safeguarding and prevent training which are monitored by the Head of Adult Safeguarding through the quarterly dashboards. The main area of concern is regarding Prevent training and ENHT and HPFT have provided action plans outlining how they will meet the NHSE targets for Prevent training.
ENHCCG | Safeguarding Children
27
Comments ׀ • The Designated Office is involved in a number of work streams, in collaboration with partner agencies and the Hertfordshire Safeguarding Children
Board (HSCB). Examples include Safeguarding Supervision and Management Oversight; Scoping of self harm; Preparation for the Joint Targeted Area Inspection (JTAI), Harmful Sexualised Behaviour and development of an Interface between Children and Adult Safeguarding Boards.
• Two Serious Case Reviews (SCRs) have been declared since the previous reporting period. Two SCRs (from investigations in 2014 and 2016) have been published (November 2017 and December 2017). Two further individual cases have been referred for consideration and will now be progressed as multi-agency investigations (as opposed to SCRs). A lead professional, to cover both investigations, has been identified.
• All Section 11 visits to Provider organisations have been completed for 2017. Action plans to improve quality of Safeguarding practice have been formulated where necessary and are monitored by the Designated Office. Recent actioned concerns have been in relation to training compliance, safeguarding supervision and number of children admitted due to self harm/overdose.
• Audit scheduling, for 2017/2018, for Provider services, based on recommendations from Section 11 visits, is complete. • Safeguarding Assurance Tool (SAT) – all key standards in relation to CCG Safeguarding practices reportable to NHS England, are currently rated as Green
as of November 2017. • A fundamental review of the role and functions of Local Safeguarding Children Boards (LSCBs) and an exploration of the child death review process
(Wood Report 2016) has made recommendations for centralisation of SCR information to support a national learning framework and a move of ownership of the arrangements for supporting Child Death Overview Panels from the Department of Education to the Department of Health. A full consultation, regarding progression of future arrangements for CDOP panels, is being led by NHS England and is expected to complete in Spring 2018. The consultation process has highlighted a number of professional concerns including lack of statutory guidance for implementation, lack of governance arrangements, change in roles and responsibilities of Designated Doctors and a shift in how review meetings (first meeting following a child death) are managed. Further information is awaited following conclusion of Consultation process.
• A review of the functions of the Hertfordshire Safeguarding Children Board (HSCB), and it’s relationship with the Adult Board is currently being undertaken by the HSCB chair. A preliminary report is expected in early 2018.
• The CCG Safeguarding Children Training Strategy has been revised, with additional information enclosed regarding Primary Care. Relevant ratification processes will be progressed to enable sign off.
• A Primary Care Dashboard has been developed which will aim to provide the CCG with a single tool to capture key indicators and selected key areas of performance within General Practice. It is envisaged that the information captured will identify areas of good practice as well as highlighting areas where further support or guidance may be required and provide valuable benchmarking and evidence for CQC inspections.
• Looked After Children (LAC) – Completion rates for Initial and Review LAC health assessments are in excess of 80%. Delay in completion of Out of County health assessments continues to be of concern. A clear escalation process involving NHS England and host CCGs is in place to improve the current situation. Quarter 2 figures currently stand at 15% completion within timescale for Initial Health Assessments and 13% for completion of Review Health Assessments.
• Compliance with safeguarding children(SGC) training requires improvement for HPFT who are working to a trajectory to reach compliance by end of March 2018. ENHT SGC training compliance is 86% against the required 90% for level 2, and 33% against 100%for level 4,the latter equates to 2 people. ENHT are working towards achieving compliance by Q3. An ongoing risk for ENHT at this time is a high turnover of staffing within the safeguarding children’s team. Both the Designated Nurse and Doctor have offered additional support during this period of change and will monitor the situation weekly.

PROVIDER PROFILES
28

ENHT |
29
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Stroke 4 hours direct to stroke unit (ASI 2) 90% Oct 71.2% 71.6% 75.7%
90% of time on the stroke unit (IPMR) 80% Oct 79.7% 88.9% 87.1%
Thrombolysed within 3 hours 12% Oct 1.6% 4.8% 6.6%
TIA high risk, not admitted, treated <24 hours (IPMR) 60% Oct 55.6% 51.6% 67.5%
TIA - low risk, treated within 7 days from onset 65% Oct 43.5% 62.1% 55.0%
Consultant Led Referral to Treatment Times (RTT)
Completed - Admitted patients None Oct No data No data
Completed - Non-admitted patients None Oct No data No data
Incomplete pathways 92% Oct No data No data
Patients waiting at the end of the month None Oct No data No data Number of 52 week breaches 0 Oct No data No data
Diagnostic waiting times
Total number on waiting list None Oct No data No data
Patients waiting less than 6 weeks from referral 99% Oct No data No data
Cancer waits
2 weeks for urgent cancer GP referrals 93% Oct 97.11% 97.28% 97.82%
2 weeks for urgent breast symptom referrals 93% Oct 90.06% 91.27% 93.02%
31 days to first definitive treatment for all cancers 96% Oct 91.63% 93.87% 91.22%
31 days for subsequent surgery 94% Oct 74.07% 92.11% 84.88%
31 days for subsequent drug 98% Oct 98.37% 95.52% 95.69%
31 days for subsequent radiotherapy 94% Oct 89.53% 88.48% 89.03%
62 days to first definitive treatment for all cancers 85% Oct 76.77% 73.23% 71.48%
62 days following screening referral 90% Oct 57.89% 94.44% 65.08%
62 days following consultant upgrade 85% Oct 87.50% 66.67% 68.07%

ENHT |
30
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Maternity
Caesarean Section rate (total) 27% Oct 26% 30% 28%
Planned Caesarean Section 11% Oct 13% 14% 13%
Unplanned Caesarean Section 15% Oct 13% 16% 14%
Friends and Family Inpatient Percentage Recommended None Oct 97.0% 97.4% 97.2%
Inpatient Response Rate None Oct 46.0% 39.6% 46.7%
A&E Percentage Recommended None Oct 93.9% 92.2% 93.2%
A&E (Type 1 & 2) Response Rate None Oct 2.0% 1.5% 3.0%
A&E Total A&E attendances None Oct 6,747 No data 74,172 +
Percentage seen within 4 hours 95% Oct 82.16% No data 85.55% Total Emergency Admissions None Oct 1,840 No data 20,096 +
Ambulances Handovers from ambulance to A&E <15mins 100% Oct No data 53.00% 67.50% Number of patients waiting >30 - <60mins None Oct No data 159 477 Number of patients waiting >60mins None Oct No data 40 92
Mixed Sex Accommodation Number of clinically unjustified MSA breaches 0 Oct 0 0 0
VTE VTE Risk Assessments 95% Oct No data No data 97.33%
HCAI
No. Clostridium - Hospital Acquired 11
(annually) Oct 1 2 15
No. MRSA - Hospital Acquired 0 Oct 0 0 1
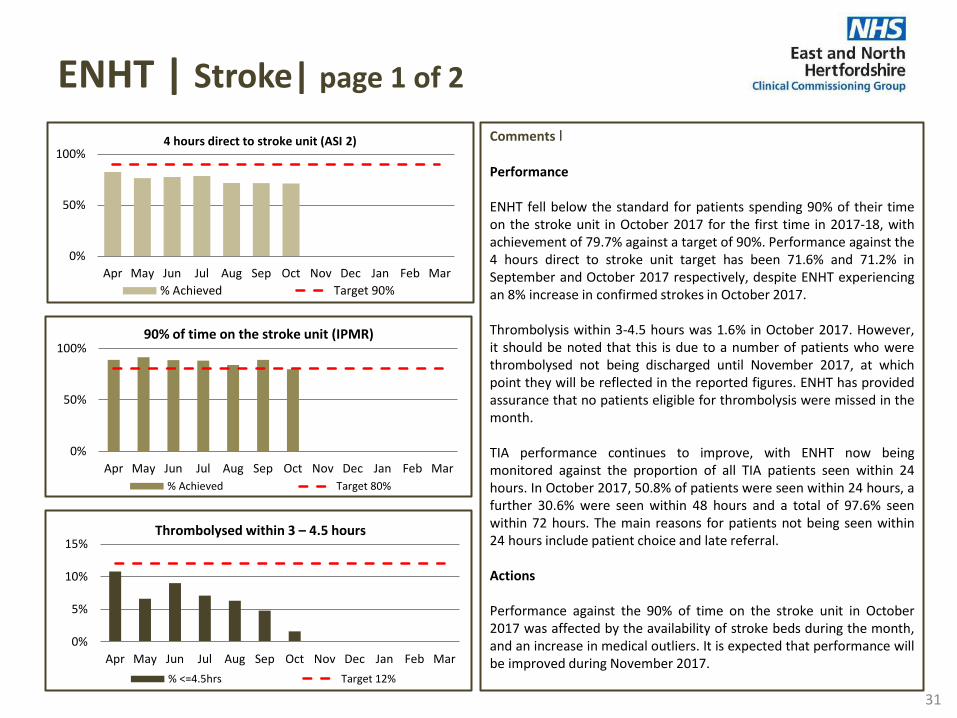
ENHT | Stroke| page 1 of 2
31
Comments ׀ Performance ENHT fell below the standard for patients spending 90% of their time on the stroke unit in October 2017 for the first time in 2017-18, with achievement of 79.7% against a target of 90%. Performance against the 4 hours direct to stroke unit target has been 71.6% and 71.2% in September and October 2017 respectively, despite ENHT experiencing an 8% increase in confirmed strokes in October 2017. Thrombolysis within 3-4.5 hours was 1.6% in October 2017. However, it should be noted that this is due to a number of patients who were thrombolysed not being discharged until November 2017, at which point they will be reflected in the reported figures. ENHT has provided assurance that no patients eligible for thrombolysis were missed in the month. TIA performance continues to improve, with ENHT now being monitored against the proportion of all TIA patients seen within 24 hours. In October 2017, 50.8% of patients were seen within 24 hours, a further 30.6% were seen within 48 hours and a total of 97.6% seen within 72 hours. The main reasons for patients not being seen within 24 hours include patient choice and late referral. Actions Performance against the 90% of time on the stroke unit in October 2017 was affected by the availability of stroke beds during the month, and an increase in medical outliers. It is expected that performance will be improved during November 2017.
0%
5%
10%
15%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Thrombolysed within 3 – 4.5 hours
% <=4.5hrs Target 12%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
90% of time on the stroke unit (IPMR)
% Achieved Target 80%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
4 hours direct to stroke unit (ASI 2)
% Achieved Target 90%

ENHT | Stroke| page 2 of 2
32
Comments ׀ Actions (cont.) Stroke nurses have now completed the appropriate training in order to directly request CT scans and a trial of this process has been undertaken. ENHT are also looking at opportunities to recruit a neurologist to support the Stroke service, which will enable closer links between the Stroke and Neurology Services, and will also further support in-house telemedicine services in 2018. ENHT and HCT are working collaboratively in order to assess the current reduction in the percentage of stroke patients discharged with ESD support. It is believed that recent months have seen a higher acuity of patients, with an increased need for inpatient rehab. Both organisations have been asked to consider what would be needed in order for ESD to flex its current criteria and take higher acuity patients into the service. Moving forward, ENHT will be sharing a breakdown of TIA patients who do not attend within 24 hours by locality and GP practice, in order for the CCG to support actions that encourage the early presentation of these patients at an acute hospital. Recovery TIA response within 24 hours should see a month-on-month improvement. ENHT continues to work towards achievement and sustainment of 80-85% against the 4 hour target.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT TIA - low risk, treated within 7 days from onset
% treated Target 65%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
TIA high risk, not admitted, treated <24 hours (IPMR)
% Achieved Target 60%
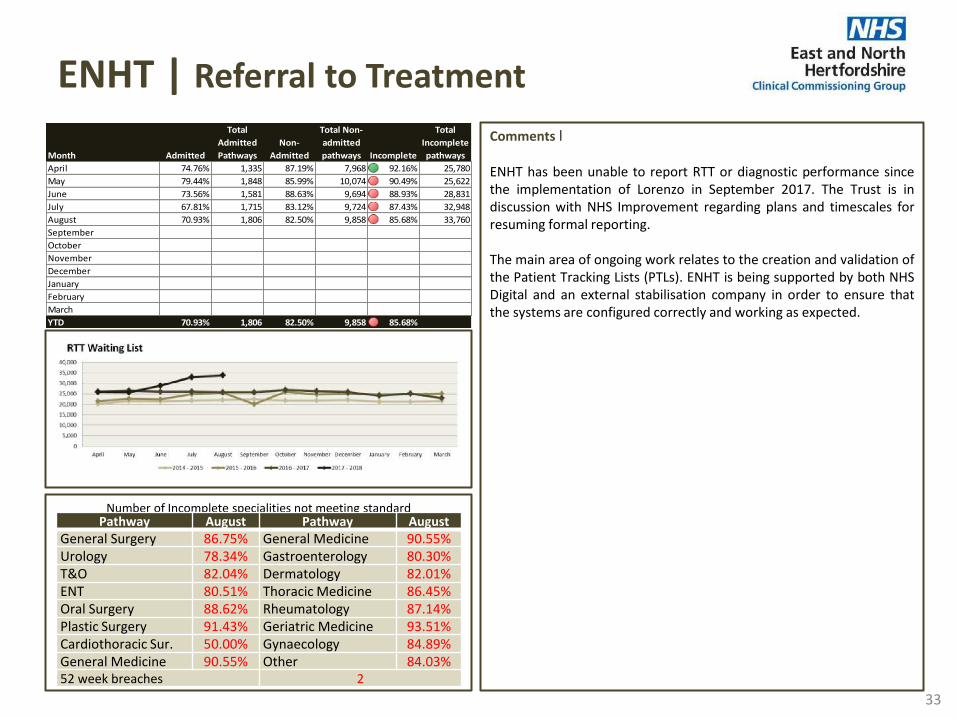
ENHT | Referral to Treatment
33
Comments ׀ ENHT has been unable to report RTT or diagnostic performance since the implementation of Lorenzo in September 2017. The Trust is in discussion with NHS Improvement regarding plans and timescales for resuming formal reporting. The main area of ongoing work relates to the creation and validation of the Patient Tracking Lists (PTLs). ENHT is being supported by both NHS Digital and an external stabilisation company in order to ensure that the systems are configured correctly and working as expected.
Number of Incomplete specialities not meeting standard
Pathway August Pathway August General Surgery 86.75% General Medicine 90.55% Urology 78.34% Gastroenterology 80.30% T&O 82.04% Dermatology 82.01% ENT 80.51% Thoracic Medicine 86.45% Oral Surgery 88.62% Rheumatology 87.14% Plastic Surgery 91.43% Geriatric Medicine 93.51% Cardiothoracic Sur. 50.00% Gynaecology 84.89% General Medicine 90.55% Other 84.03% 52 week breaches 2
Month Admitted
Total
Admitted
Pathways
Non-
Admitted
Total Non-
admitted
pathways Incomplete
Total
Incomplete
pathways
April 74.76% 1,335 87.19% 7,968 92.16% 25,780
May 79.44% 1,848 85.99% 10,074 90.49% 25,622
June 73.56% 1,581 88.63% 9,694 88.93% 28,831
July 67.81% 1,715 83.12% 9,724 87.43% 32,948
August 70.93% 1,806 82.50% 9,858 85.68% 33,760
September 0.00% 0 0.00% 0 0.00% 0
October 0.00% 0 0.00% 0 0.00% 0
November 0.00% 0 0.00% 0 0.00% 0
December 0.00% 0 0.00% 0 0.00% 0
January 0.00% 0 0.00% 0 0.00% 0
February 0.00% 0 0.00% 0 0.00% 0
March 0.00% 0 0.00% 0 0.00% 0
YTD 70.93% 1,806 82.50% 9,858 85.68%
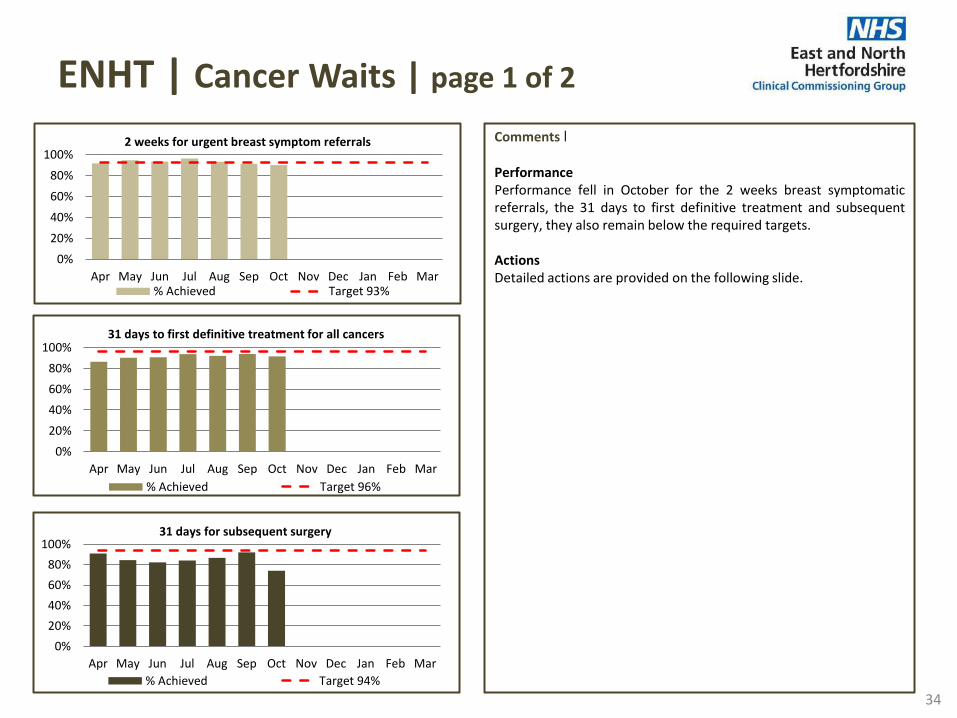
Comments ׀ Performance Performance fell in October for the 2 weeks breast symptomatic referrals, the 31 days to first definitive treatment and subsequent surgery, they also remain below the required targets. Actions Detailed actions are provided on the following slide.
ENHT | Cancer Waits | page 1 of 2
34
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
31 days to first definitive treatment for all cancers
% Achieved Target 96%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
31 days for subsequent surgery
% Achieved Target 94%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
2 weeks for urgent breast symptom referrals
% Achieved Target 93%

Comments ׀ Performance Patients should receive first definitive treatment within 62 days of the referral being received and the national standard for this metric is 85%. The trust has failed to meet the 62 day standard for first definitive treatment since April 2015, although performance in October was 76.8%, increasing to 79.1% following application of the inter trust referral policy which reallocates breaches to trusts referring after day 38 in the pathway. The number of reported 62 day breaches was 23 in October which is the lowest number since April 2017. Performance continues to be below the recovery trajectory as the Trust had expected to be meeting 85% by September. Actions ENHT has been issued with a Contract Performance Notice by the CCG. This requires the trust to submit a revised recovery trajectory to the CCG with an updated action plan. Recovery The trust will need to get formal sign off to the revised recovery trajectory with NHS Improvement, although it is expected that the trust will achieve the required 85% for March 2018.
ENHT | Cancer Waits | page 2 of 2
35
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
62 days following screening referral
% Achieved Target 90%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
31 days for subsequent radiotherapy
% Achieved Target 94%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
62 day for first definitive treatment
% Achieved Post adjustment % 85% Target Trajectory

ENHT | Accident & Emergency
36
Comments ׀ Performance A&E performance in October and November 2017 fell below the agreed recovery trajectory, with achievement of 82.2% and 81.7% against targets of 91.0% and 91.8%. This also marks a deterioration in performance compared to the same time in 2016. Actions ENHT believes that the reported breach numbers are currently overstated whilst Nerve Centre becomes embedded and the staff become used to real time reporting processes. ENHT continues to progress actions in its Patient Flow Improvement Programme, including ensuring streaming of walk in patients is in place, deployment of progress chasers in A&E, and an increase in middle grade and consultant resource. In addition, as part of the plan to manage winter, additional capacity has been put in place, including an additional 16 beds and increased capacity within the Clinical Decision Unit. A senior decision maker has also been placed into the Surgical Assessment Unit. The Discharge Home to Assess Service commenced on 26 November 2017, with the aim of supporting the early discharge of appropriate patients from ENHT so that assessments for ongoing care can be completed within the patients home rather than retaining them in a hospital bed. Recovery A Contract Performance Notice for A&E was issued on 1 December 2017, which requires ENHT to submit a revised recovery trajectory with an updated action plan to the CCG. It is currently expected that the trajectory will achieve the 4 hour standard by March 2018.
0
1000
2000
3000
4000
5000
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep* Oct Nov Dec Jan Feb Mar
A&E patients seen within 4 hours and Breaches
Breaches % Achieved 95% Target Trajectory
* September data not available
0%
5%
10%
15%
20%
25%
30%
35%
40%
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
Apr May Jun Jul Aug Sep* Oct Nov Dec Jan Feb Mar
Emergency attendances and admissions
Type 1 and Other Admissions Non-admissions
Total Attends Conv
* September data not available

ENHT | Ambulance Handovers
37
Comments ׀ Performance ENHT continues to be amongst the best performers regionally in terms of ambulance handovers, with 52.8% of clinical handovers being completed within 15 minutes during September 2017 (compared to a regional average of 38.1%). There has been a reduction in clinical handovers over recent months, however performance remains significantly improved compared to the previous year (performance of 12.9% in September 2016). There were 40 handover delays over 60 minutes in September 2017. During September 2017, there were 167 hours lost to handover at ENHT; a 56.4% reduction compared to September 2016. However, the number of hours lost has increased in recent months, from an average of 60 at the beginning of the year, to 152 in August and September. The introduction of a new electronic clinical patient management system in A&E and implementation of the Ambulance Reporting Programme are the reasons for the decline. Actions Due to the implementation of the Ambulance Response Programme in October 2017, ambulance handover information is not currently available for October or November 2017. ENHT have put in renewed support and oversight to the ambulance pathway since August 2017, which will be focused on further as a result of the improvement programme and the Remedial Action Plan for A&E which include further work on streaming pathways at Lister. Recovery The CCG will continue to closely monitor ambulance handovers to ensure that performance improves over the coming months.
0%
25%
50%
75%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Handovers from ambulance to A&E within 15mins
% <15mins Target
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
20
40
60Handovers delays from ambulance to A&E >60mins
>60mins
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
100
200Handover delays from ambulance to A&E 30-60mins
30-60mins

ENHT | Cancelled Operations & Outpatients
38
Comments ׀ Performance In September and October 2017, the reported information suggests an increase in the number of patients who did not receive a binding date within 28 days following a cancelled appointment. However, it should be noted that these figures are likely to be overstated due to the Lorenzo implementation and that further validation of these figures is required. Cancelled outpatient appointment continue to be higher than the 8% threshold, with 11.0% of appointments cancelled in September 2017, and 10.6% in October 2017. Actions ENHT has stated that as part of the Lorenzo implementation, there has been work undertaken to ensure that the outpatient clinic information held on the system is correct. There are a number of clinics that have been changed in this time, which come through the reported figures as a cancellation but are in fact clinic reconfigurations. A number of actions remain ongoing, including the development of a specialty overview of cancelled appointments, ongoing validation of information held on clinical systems, and transformation work that is aimed at optimising outpatient pathways. Recovery The CCG continues to work closely with ENHT to improve cancellations and waiting times for outpatient appointments. This will continue to be developed on a specialty basis during 2017-18 and 2018-19, and a revised Access and Discharge Meeting will be convened.
0%
5%
10%
15%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Reduction in cancellation of outpatient appointments
% Achieved Target <8%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage treated <28 days of cancellation
% Achieved Target 100%
0
5
10
15
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
No binding date <28 days after cancellation
Number of patients Target = 0

ENHT | Serious Incidents
39
Comments In Q3 ENHT reported 21 SIs across the organisation which is an increase compared to previous quarters. The key themes are diagnostic incidents, treatment delays and sub-optimal care of the deteriorating patient. The Trust has reported 4 Never Events YTD. One relates to wrong site surgery, two relate to retained objects and one relates to a misplaced nasogastric tube.
Infectioncontrol
DiagnosticIncident
Safeguarding adults
MaternityServices
TreatmentDelay
Patient Fall
Suboptimalcare of
deteriorating patient
Surgical/Invasive
ProcedureIncident
MedicationIncident
InformationGovernance
Breach
Self InflictedHarm
MajorIncident
ScreeningIssues
Operation/treatment
givenwithout
validconsent
Q4 1 3 2 1 2 5 1 1 1 0 1 0 0 0
Q1 0 3 0 1 4 1 1 1 0 1 0 1 1 0
Q2 1 2 0 1 0 1 0 1 0 0 0 0 0 0
Q3 0 4 1 1 4 1 5 2 0 2 0 0 0 1
0
1
2
3
4
5
6
Nu
mb
er
E&NHT : Type of Serious Incident Reported 2016/17 -2017/18
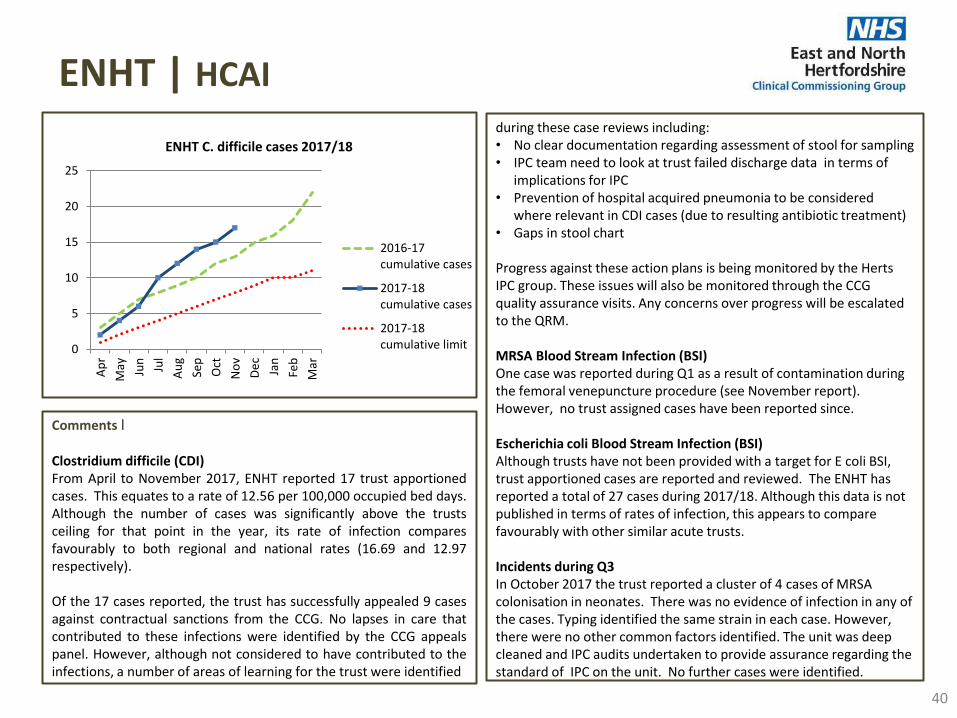
40
ENHT | HCAI during these case reviews including: • No clear documentation regarding assessment of stool for sampling • IPC team need to look at trust failed discharge data in terms of
implications for IPC • Prevention of hospital acquired pneumonia to be considered
where relevant in CDI cases (due to resulting antibiotic treatment) • Gaps in stool chart
Progress against these action plans is being monitored by the Herts IPC group. These issues will also be monitored through the CCG quality assurance visits. Any concerns over progress will be escalated to the QRM. MRSA Blood Stream Infection (BSI) One case was reported during Q1 as a result of contamination during the femoral venepuncture procedure (see November report). However, no trust assigned cases have been reported since. Escherichia coli Blood Stream Infection (BSI) Although trusts have not been provided with a target for E coli BSI, trust apportioned cases are reported and reviewed. The ENHT has reported a total of 27 cases during 2017/18. Although this data is not published in terms of rates of infection, this appears to compare favourably with other similar acute trusts. Incidents during Q3 In October 2017 the trust reported a cluster of 4 cases of MRSA colonisation in neonates. There was no evidence of infection in any of the cases. Typing identified the same strain in each case. However, there were no other common factors identified. The unit was deep cleaned and IPC audits undertaken to provide assurance regarding the standard of IPC on the unit. No further cases were identified.
Comments ׀ Clostridium difficile (CDI) From April to November 2017, ENHT reported 17 trust apportioned cases. This equates to a rate of 12.56 per 100,000 occupied bed days. Although the number of cases was significantly above the trusts ceiling for that point in the year, its rate of infection compares favourably to both regional and national rates (16.69 and 12.97 respectively). Of the 17 cases reported, the trust has successfully appealed 9 cases against contractual sanctions from the CCG. No lapses in care that contributed to these infections were identified by the CCG appeals panel. However, although not considered to have contributed to the infections, a number of areas of learning for the trust were identified
0
5
10
15
20
25
Ap
r
May Jun
Jul
Au
g
Sep
Oct
No
v
De
c
Jan
Feb
Mar
2016-17cumulative cases
2017-18cumulative cases
2017-18cumulative limit
ENHT C. difficile cases 2017/18
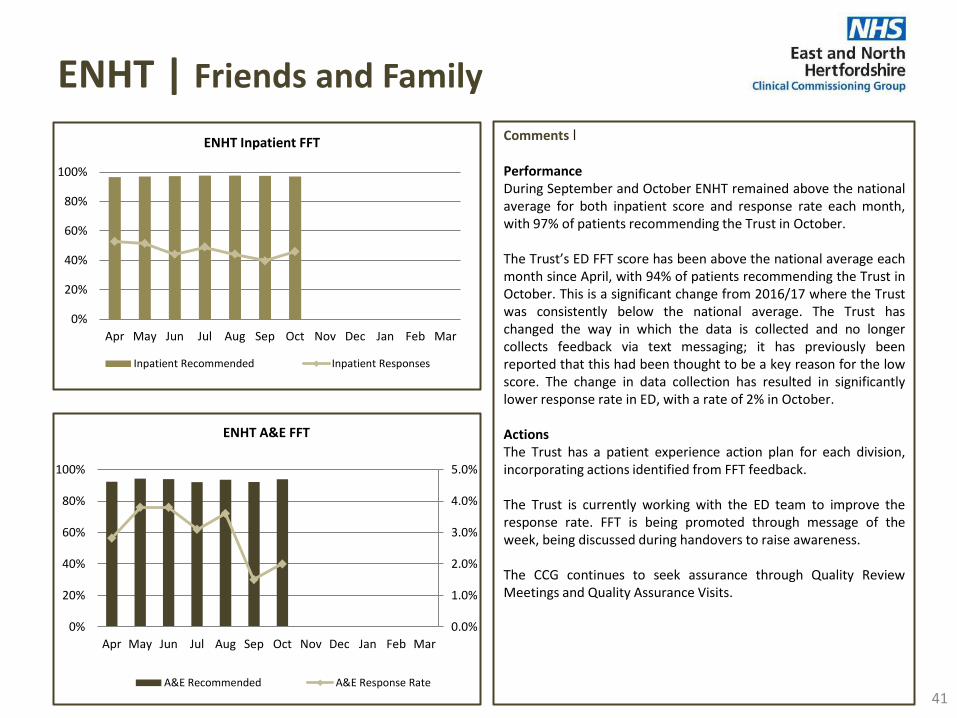
ENHT | Friends and Family
41
Comments ׀ Performance During September and October ENHT remained above the national average for both inpatient score and response rate each month, with 97% of patients recommending the Trust in October. The Trust’s ED FFT score has been above the national average each month since April, with 94% of patients recommending the Trust in October. This is a significant change from 2016/17 where the Trust was consistently below the national average. The Trust has changed the way in which the data is collected and no longer collects feedback via text messaging; it has previously been reported that this had been thought to be a key reason for the low score. The change in data collection has resulted in significantly lower response rate in ED, with a rate of 2% in October. Actions The Trust has a patient experience action plan for each division, incorporating actions identified from FFT feedback. The Trust is currently working with the ED team to improve the response rate. FFT is being promoted through message of the week, being discussed during handovers to raise awareness. The CCG continues to seek assurance through Quality Review Meetings and Quality Assurance Visits.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT Inpatient FFT
Inpatient Recommended Inpatient Responses
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
ENHT A&E FFT
A&E Recommended A&E Response Rate

ENHT | Workforce
42
Comments ׀ Sickness absence The Trust’s annualised sickness absence rate continues to improve, with a rate of 3.39% in September. This is the lowest annualised sickness rate recorded in the Trust since July 2014. The Trust’s aim is to reduce the annualised sickness absence rate to 3.3% by the end of March 2018. Turnover In September, the turnover rate was 12.7% compared to 12.6% in August. The Trust is developing a full retention strategy, with key work streams currently being finalised. A bullying and harassment steering group was launched in September. Vacancy rate There continues to be a number of vacancies at the Trust including ED and ward areas; the vacancy rate has shown a slight improvement with an overall vacancy rate of 8.4% in September. The vacancy rate for band 5 nurses has improved from 17.8% in August to 15.6% in September. The Trust is aiming to reduce the overall vacancy rate to 6%, and the band 5 nursing vacancy rate to 12% by March 2018. Each Division has recruitment plans in place, with bespoke recruitment events planned throughout the year. Work is also being undertaken to enhance the branding of the Trust utilising digital media. Appraisal rate Following initial improvement in the appraisal rate during 2017/18 there has been a decrease during September and October, with a rate of 80.4% in October. The Trust continues to prevent automatic pay progression for staff who have not received an appraisal. A streamlined process has been introduced to record completed appraisals, and Divisions are working on detailed plans to deliver 90% compliance this financial year.
0%
2%
4%
6%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Sickness absence rate
% Achieved Target <3.3%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staff appraised in the last 12 months
% Achieved Target 90%
0%
5%
10%
15%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staff turnover rate
% Achieved Target <10%
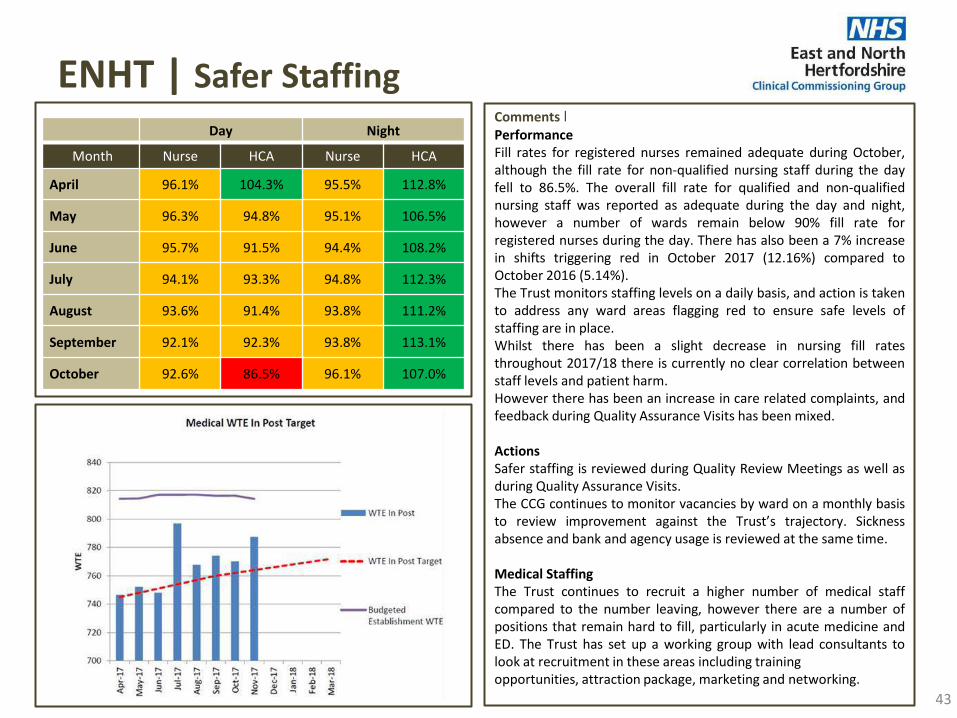
ENHT | Safer Staffing
43
Comments ׀ Performance Fill rates for registered nurses remained adequate during October, although the fill rate for non-qualified nursing staff during the day fell to 86.5%. The overall fill rate for qualified and non-qualified nursing staff was reported as adequate during the day and night, however a number of wards remain below 90% fill rate for registered nurses during the day. There has also been a 7% increase in shifts triggering red in October 2017 (12.16%) compared to October 2016 (5.14%). The Trust monitors staffing levels on a daily basis, and action is taken to address any ward areas flagging red to ensure safe levels of staffing are in place. Whilst there has been a slight decrease in nursing fill rates throughout 2017/18 there is currently no clear correlation between staff levels and patient harm. However there has been an increase in care related complaints, and feedback during Quality Assurance Visits has been mixed. Actions Safer staffing is reviewed during Quality Review Meetings as well as during Quality Assurance Visits. The CCG continues to monitor vacancies by ward on a monthly basis to review improvement against the Trust’s trajectory. Sickness absence and bank and agency usage is reviewed at the same time. Medical Staffing The Trust continues to recruit a higher number of medical staff compared to the number leaving, however there are a number of positions that remain hard to fill, particularly in acute medicine and ED. The Trust has set up a working group with lead consultants to look at recruitment in these areas including training opportunities, attraction package, marketing and networking.
Day Night
Month Nurse HCA Nurse HCA
April 96.1% 104.3% 95.5% 112.8%
May 96.3% 94.8% 95.1% 106.5%
June 95.7% 91.5% 94.4% 108.2%
July 94.1% 93.3% 94.8% 112.3%
August 93.6% 91.4% 93.8% 111.2%
September 92.1% 92.3% 93.8% 113.1%
October 92.6% 86.5% 96.1% 107.0%

ENHT | Other
44
Comments ׀ Mortality (SHMI) The December release of SHMI data (covering the rolling year to June 2017) showed that ENHT had maintained the previous improvements with a SHMI of 102.1. This is well below the upper control limit of 106.6. Following the publication of national guidance regarding learning from deaths progress in relation to the key requirements continues to be monitored through the regular Mortality Review Group. Sepsis During Q2 the Trust continued to perform well in screening and identifying patients with sepsis in ED and inpatient wards, however the Trust struggled to treat patients within the required one hour timeframe. During Q2 95% of patients were appropriately identified in both ED and inpatient areas, however timely treatment with IV antibiotics fell below the required standards (63% in ED and 59% in inpatient areas).The Trust is undertaking a programme of actions to address this poor performance, closely monitored and supported by the CCG. CQC Inspection The Trust has been advised that the CQC will undertake their next unannounced inspection in the spring, and the CQC will be attending key meetings within the Trust over the coming months. The CCG continues to undertake regular Quality Visits to the Trust to seek assurance regarding progress against the CQC development plans.
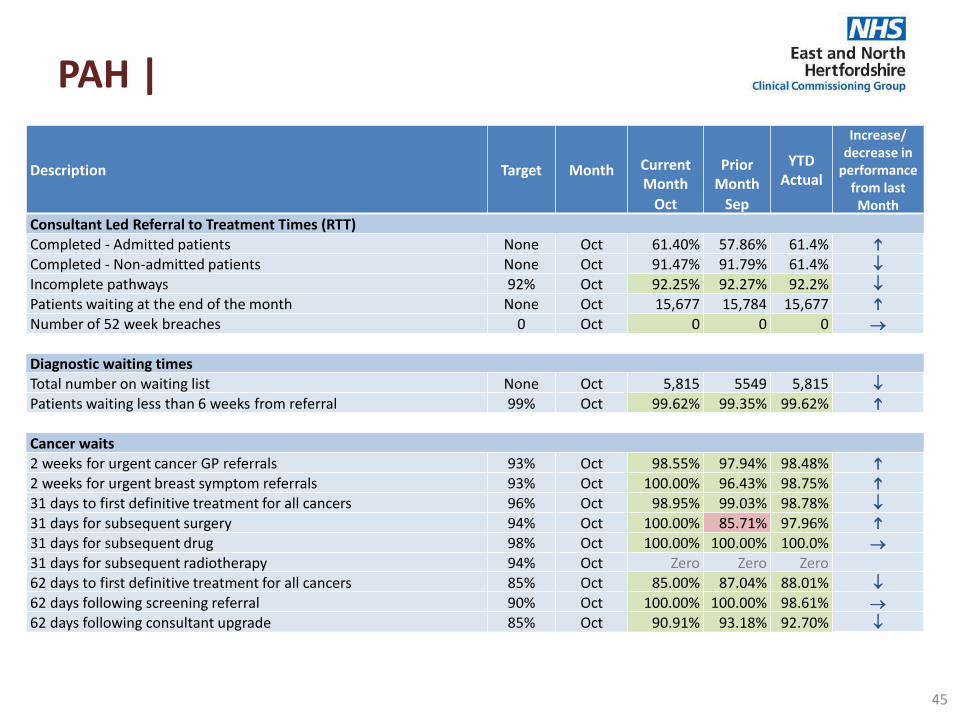
PAH |
45
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Consultant Led Referral to Treatment Times (RTT) Completed - Admitted patients None Oct 61.40% 57.86% 61.4%
Completed - Non-admitted patients None Oct 91.47% 91.79% 61.4%
Incomplete pathways 92% Oct 92.25% 92.27% 92.2%
Patients waiting at the end of the month None Oct 15,677 15,784 15,677
Number of 52 week breaches 0 Oct 0 0 0
Diagnostic waiting times Total number on waiting list None Oct 5,815 5549 5,815
Patients waiting less than 6 weeks from referral 99% Oct 99.62% 99.35% 99.62%
Cancer waits 2 weeks for urgent cancer GP referrals 93% Oct 98.55% 97.94% 98.48%
2 weeks for urgent breast symptom referrals 93% Oct 100.00% 96.43% 98.75%
31 days to first definitive treatment for all cancers 96% Oct 98.95% 99.03% 98.78%
31 days for subsequent surgery 94% Oct 100.00% 85.71% 97.96%
31 days for subsequent drug 98% Oct 100.00% 100.00% 100.0%
31 days for subsequent radiotherapy 94% Oct Zero Zero Zero
62 days to first definitive treatment for all cancers 85% Oct 85.00% 87.04% 88.01%
62 days following screening referral 90% Oct 100.00% 100.00% 98.61%
62 days following consultant upgrade 85% Oct 90.91% 93.18% 92.70%

PAH |
46
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Maternity
Caesarean Section rate (total) 25% Oct 25.1% 27.3% 28.4%
Planned Caesarean Section None Oct 11.9% 12.3% 12.5% Unplanned Caesarean Section None Oct 13.2% 10.8% 15.3%
Friends and Family
Inpatient Percentage Recommended None Oct 98.5% 98.0% 97.6% Inpatient Response Rate None Oct 35.0% 42.6% 38.0%
A&E Percentage Recommended None Oct 97.5% 91.9% 92.8% A&E (Type 1 & 2) Response Rate None Oct 8.9% 22.5% 24.9%
A&E Total A&E attendances None Oct 8,706 8,312 59,387 +
Percentage seen within 4 hours 95% Oct 68.27% 70.32% 74.13%
Total Emergency Admissions None Oct 2,043 1,992 15,947 +
Ambulances Handovers between ambulance and A&E <15mins 100% Oct No data 31.0% 30.7% Number of patients waiting >30 - <60mins None Oct No data 459 2,337 Number of patients waiting >60mins None Oct No data 109 523
Mixed Sex Accommodation Number of clinically unjustified MSA breaches 0 Oct 11 2 37
VTE VTE Risk Assessments 95% Oct 98.47% 98.55% 98.61%
HCAI
No. Clostridium - Hospital Acquired 10
(annually) Oct 0 3 10 No. MRSA - Hospital Acquired 0 Oct 0 0 0

PAH | Accident & Emergency
47
Comments ׀ Performance The ED standard remains the most significantly challenged operational target for PAH, with early figures indicating a further decline in December. Weekly performance reviews with NHSE and NHSI continue with a focus on what support is required during winter. In October and November, ED continued with temporary facilities due to the ED re-configuration, including reduced assessment bed capacity. All assessment areas opened on 4th December 2017. Medical and Nursing staffing levels also continue to be an issue in ED. Actions • Enhanced GP streaming in place; benefit not being fully realised due
to unavailability of CDU during building work. PAH require both areas to be fully functioning to gain full impact. CDU re-opened on 4th December 2017.
• Handover back to re-furbished department completed on 4th December 2017.
• Re-focus the flow through department, internal escalation process being reinforced to all staff.
• Re-launch of the Rapid Assessment and Treatment (RAT) service in new facilities, with dedicated decision maker clinical cover.
Recovery Areas for discussion at NHSE/I meetings include: • 7 day working and senior decision making in ED at weekends. • GP in ED during night time hours. • Medical input and additional doctors on the wards at weekends to
support discharges. The December Local Delivery Board Report reported that the new ED assessment space is starting to show benefits. PAH has been allocated £1.9m from the additional funds announced in the budget to support them achieving 90% by Q4; £1.5m of this money will fund the new assessment beds for the remainder of the financial year.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
A&E seen within 4 hours
% seen Target Trajectory
0%
10%
20%
30%
40%
50%
0
2,000
4,000
6,000
8,000
10,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Emergency attendances & admissions
Admissions Non-admissions Attendances Conv
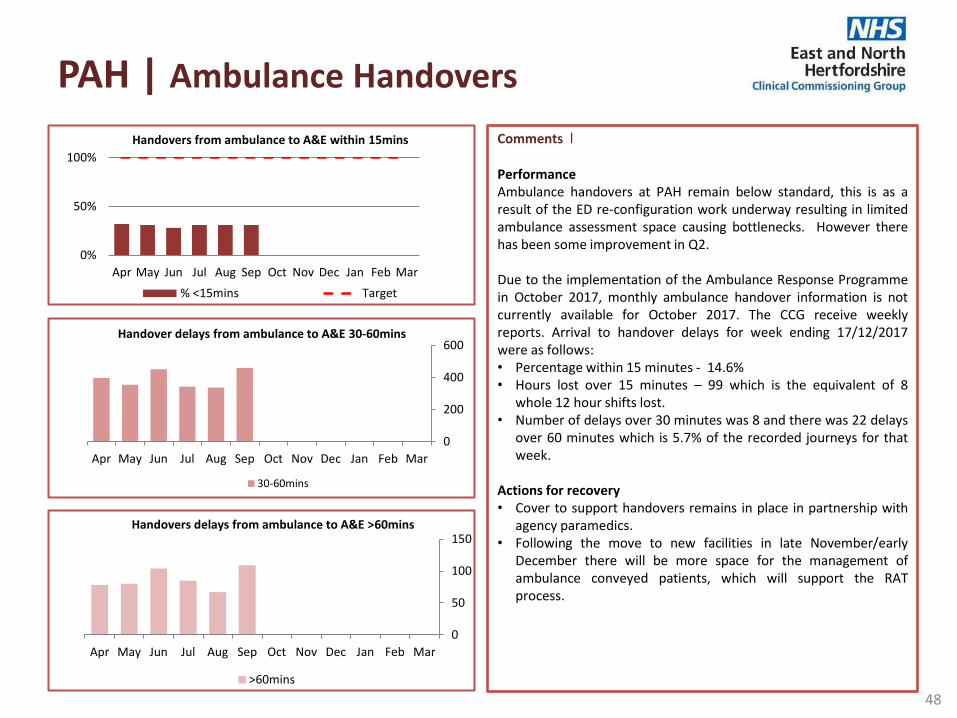
PAH | Ambulance Handovers
48
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
50
100
150Handovers delays from ambulance to A&E >60mins
>60mins
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
0
200
400
600Handover delays from ambulance to A&E 30-60mins
30-60mins
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Handovers from ambulance to A&E within 15mins
% <15mins Target
Comments ׀ Performance Ambulance handovers at PAH remain below standard, this is as a result of the ED re-configuration work underway resulting in limited ambulance assessment space causing bottlenecks. However there has been some improvement in Q2. Due to the implementation of the Ambulance Response Programme in October 2017, monthly ambulance handover information is not currently available for October 2017. The CCG receive weekly reports. Arrival to handover delays for week ending 17/12/2017 were as follows: • Percentage within 15 minutes - 14.6% • Hours lost over 15 minutes – 99 which is the equivalent of 8
whole 12 hour shifts lost. • Number of delays over 30 minutes was 8 and there was 22 delays
over 60 minutes which is 5.7% of the recorded journeys for that week.
Actions for recovery • Cover to support handovers remains in place in partnership with
agency paramedics. • Following the move to new facilities in late November/early
December there will be more space for the management of ambulance conveyed patients, which will support the RAT process.
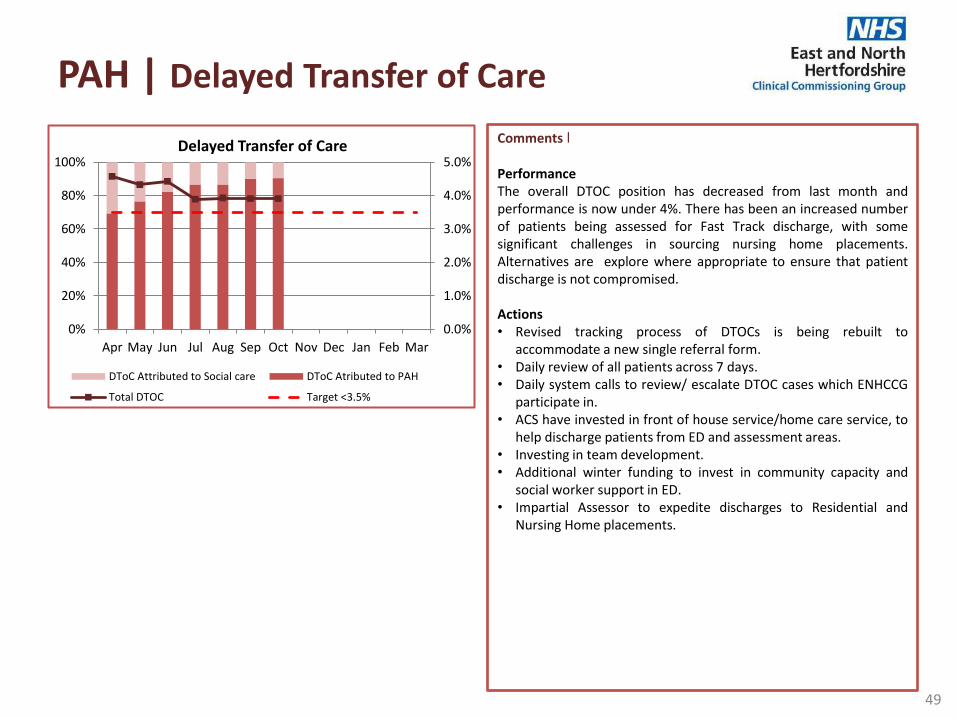
PAH | Delayed Transfer of Care
49
Comments ׀ Performance The overall DTOC position has decreased from last month and performance is now under 4%. There has been an increased number of patients being assessed for Fast Track discharge, with some significant challenges in sourcing nursing home placements. Alternatives are explore where appropriate to ensure that patient discharge is not compromised. Actions • Revised tracking process of DTOCs is being rebuilt to
accommodate a new single referral form. • Daily review of all patients across 7 days. • Daily system calls to review/ escalate DTOC cases which ENHCCG
participate in. • ACS have invested in front of house service/home care service, to
help discharge patients from ED and assessment areas. • Investing in team development. • Additional winter funding to invest in community capacity and
social worker support in ED. • Impartial Assessor to expedite discharges to Residential and
Nursing Home placements.
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Delayed Transfer of Care
DToC Attributed to Social care DToC Atributed to PAH
Total DTOC Target <3.5%
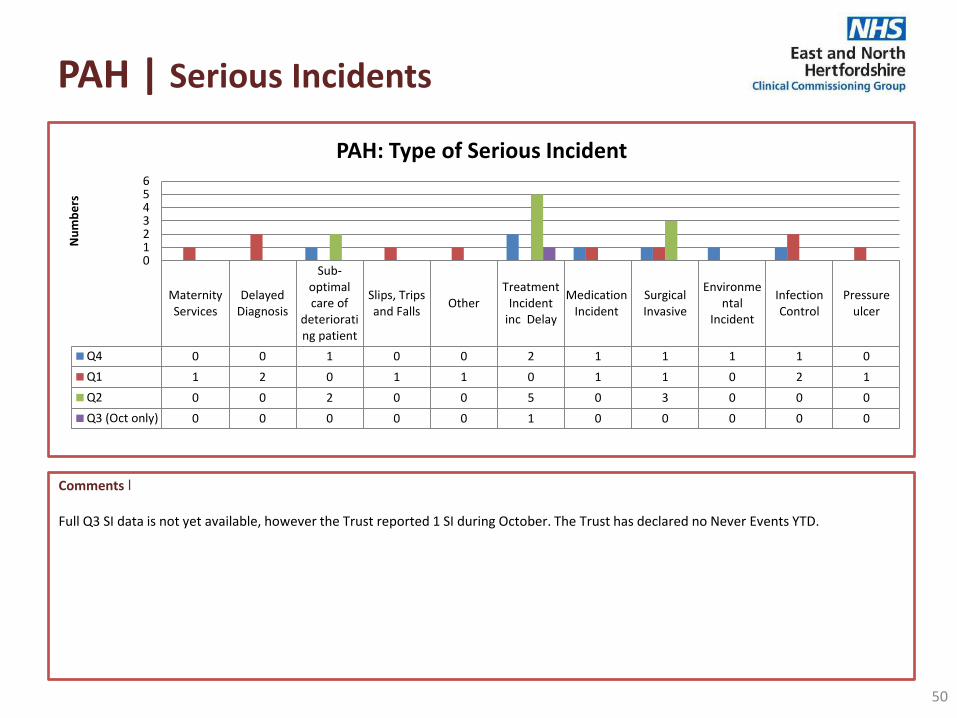
PAH | Serious Incidents
50
Comments ׀ Full Q3 SI data is not yet available, however the Trust reported 1 SI during October. The Trust has declared no Never Events YTD.
MaternityServices
DelayedDiagnosis
Sub-optimalcare of
deteriorating patient
Slips, Tripsand Falls
OtherTreatment
Incidentinc Delay
MedicationIncident
SurgicalInvasive
Environmental
Incident
InfectionControl
Pressureulcer
Q4 0 0 1 0 0 2 1 1 1 1 0
Q1 1 2 0 1 1 0 1 1 0 2 1
Q2 0 0 2 0 0 5 0 3 0 0 0
Q3 (Oct only) 0 0 0 0 0 1 0 0 0 0 0
0123456
Nu
mb
ers
PAH: Type of Serious Incident

PAH | HCAI
51
Comments ׀ Clostridium difficile (CDI) Although significantly above the limit for number of cases at this point in the year, the rate of infection per 100,000 occupied bed days at the end of November was 9.41 which was significantly below regional and national rates at this point (16.69 and 12.97 respectively). Of the 10 cases, 6 were successfully appealed against contractual sanctions as the North Essex HCAI scrutiny panel identified that there were no lapses in care identified that contributed to these infections. Lessons learnt in the review of the remaining cases included delay in isolation or escalation, or delay in sampling. MRSA Blood Stream Infection (BSI) No cases of trust assigned MRSA BSI have been reported during 2017/18.
0
2
4
6
8
10
12
14
16
18
20
Ap
r
May Jun
Jul
Au
g
Sep
Oct
No
v
De
c
Jan
Feb
Mar
PAH C-Diff Cases 2017/18
2016-17cumulativecases
2017-18cumulativecases
2017-18cumulativelimit

PAH | Mixed Sex Accommodation
52
Comments ׀ Performance Delayed transfer of patients from HDU, due to lack of inpatient beds has resulted in a rise in mixed sex accommodation breaches at PAH. During October, 5 of the breaches relate to one individual incident where 4 patients of one gender and 1 patient of the opposite gender were in HDU and the Trust were unable to avoid the breach by moving patients within the department. Actions Matrons are reviewing opportunities to prioritise the order of patients transferred to wards, where a gender breach may be the likely outcome of delay. Escalation processes are in place to alert the site management team of any potential breaches to enable corrective action to be put in place.
0
2
4
6
8
10
12
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of clinically unjustified MSA breaches
No. of breaches

PAH | Friends and Family
53
Comments ׀ Performance The inpatient score and response rate for PAH have been above the national average in September and October, with 98% of patients recommending the Trust in October. The ED FFT score has also been above the national average during September and October with 97% of patients recommending the Trust. However the response rate for ED was below the national average in October. Actions Building work within the ED department is anticipated to have a positive impact on FFT scores over the coming months. ENHCCG accompanies WECCG on Quality Assurance Visits, during which patient feedback is sought.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
PAH Inpatient Survey
Recommended Response Rate
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
PAH A&E Survey
Recommended Response Rate
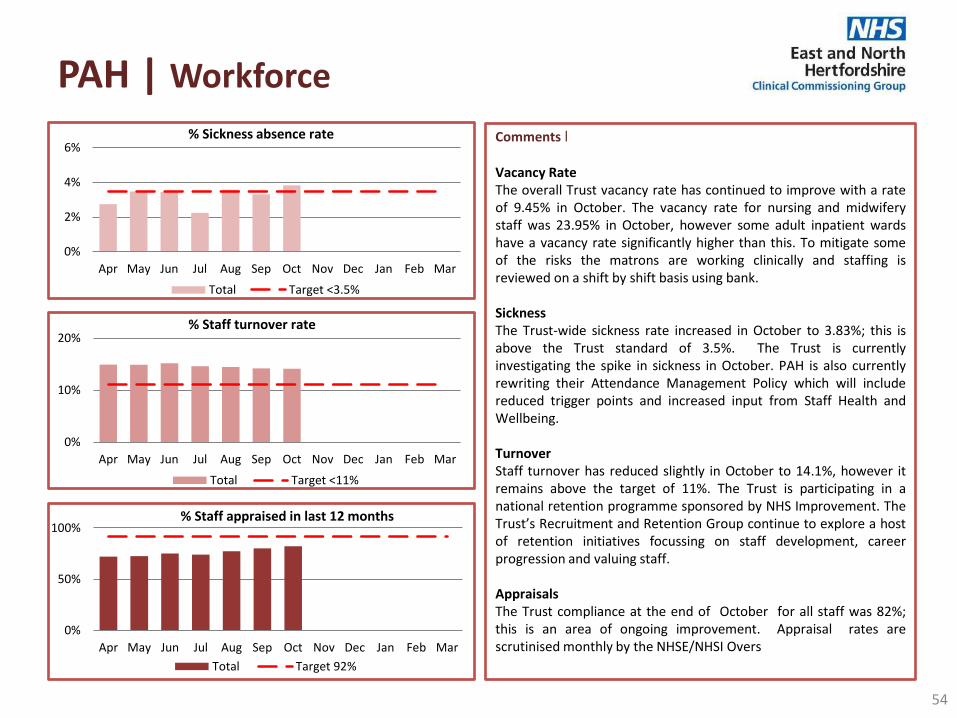
Comments ׀ Vacancy Rate The overall Trust vacancy rate has continued to improve with a rate of 9.45% in October. The vacancy rate for nursing and midwifery staff was 23.95% in October, however some adult inpatient wards have a vacancy rate significantly higher than this. To mitigate some of the risks the matrons are working clinically and staffing is reviewed on a shift by shift basis using bank. Sickness The Trust-wide sickness rate increased in October to 3.83%; this is above the Trust standard of 3.5%. The Trust is currently investigating the spike in sickness in October. PAH is also currently rewriting their Attendance Management Policy which will include reduced trigger points and increased input from Staff Health and Wellbeing. Turnover Staff turnover has reduced slightly in October to 14.1%, however it remains above the target of 11%. The Trust is participating in a national retention programme sponsored by NHS Improvement. The Trust’s Recruitment and Retention Group continue to explore a host of retention initiatives focussing on staff development, career progression and valuing staff. Appraisals The Trust compliance at the end of October for all staff was 82%; this is an area of ongoing improvement. Appraisal rates are scrutinised monthly by the NHSE/NHSI Overs
PAH | Workforce
54
0%
10%
20%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% Staff turnover rate
Total Target <11%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% Staff appraised in last 12 months
Total Target 92%
0%
2%
4%
6%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% Sickness absence rate
Total Target <3.5%
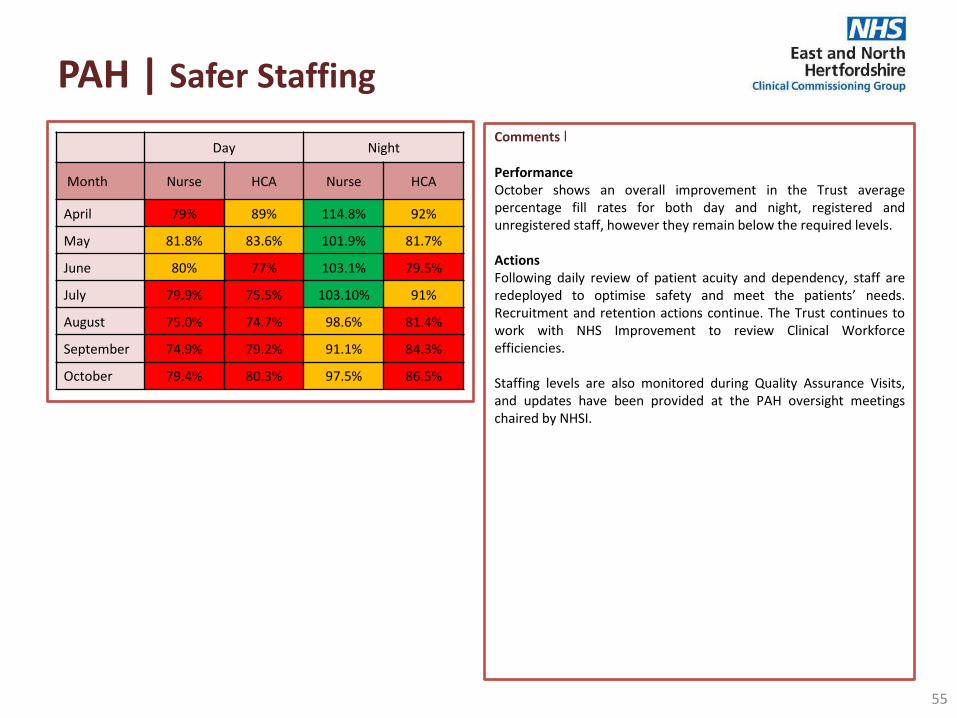
PAH | Safer Staffing
55
Comments ׀ Performance October shows an overall improvement in the Trust average percentage fill rates for both day and night, registered and unregistered staff, however they remain below the required levels. Actions Following daily review of patient acuity and dependency, staff are redeployed to optimise safety and meet the patients’ needs. Recruitment and retention actions continue. The Trust continues to work with NHS Improvement to review Clinical Workforce efficiencies. Staffing levels are also monitored during Quality Assurance Visits, and updates have been provided at the PAH oversight meetings chaired by NHSI.
Day Night
Month Nurse HCA Nurse HCA
April 79% 89% 114.8% 92%
May 81.8% 83.6% 101.9% 81.7%
June 80% 77% 103.1% 79.5%
July 79.9% 75.5% 103.10% 91%
August 75.0% 74.7% 98.6% 81.4%
September 74.9% 79.2% 91.1% 84.3%
October 79.4% 80.3% 97.5% 86.5%
PAH | Other| page 1 of 2
56
Comments ׀ Rheumatology Follow – ups: The trust undertook a review of clinical pathways in outpatients which identified a cohort patients on the rheumatology pathway who have not had follow up reviews by the service since their first appointment. As a result WECCG, ENHCCG and PAH have agreed: • Moratorium on the ratio for 6 months. • Monthly assurance process on the status of the backlog. • Review of Rheumatology pathway to be undertaken. • Harm reviews undertaken of all patients by 31st March. Further discussions are underway with PAH consultants to reach consensus about the clinical audit in relation to advised ratios Oral Surgery & Paediatric Orthopaedic Services PAH wrote to CCGs on 8th November to advise the service for Oral Cancer Surgery patients follow ups at PAH will cease for the next 6/9 months. This service is provided by UCLH as part of a clinical network and the Consultant surgeon is leaving. This activity is commissioned by NHSE and the CCG has asked NHSE to be kept informed of the progress. The Paediatric orthopaedic service is a single handed service and has previously been flagged by PAH as a vulnerable service. Due to the demand PAH had a backlog of 81 referral on e-Referral awaiting an outpatient appointment. As a consequence and for patient safety the service has temporarily ceased accepting new referrals into services and are in the process of producing a business case to recruit an additional consultant. In the interim referrals will go to other local Trusts, the activity numbers into the service at PAH are small and therefore can be absorbed by other providers.
PAH | Other| page 2 of 2
57
Comments ׀ Mortality rates The December release of SHMI data (covering the rolling year to June 2017) showed that PAH has deteriorated further with a SHMI of 108.3. This is the 6th consecutive increase in SHMI for the Trust. The HSMR for August 2016 to July 2017 was 115.5 and statistically “higher than expected”, however it was a slight improvement compared to the previous month. The Trust are working to make improvements in coding, reviewing all pathways, and all outlier alerts. Progress is reviewed through the monthly Contract and Quality Meeting as well as the oversight meeting led by NHS Improvement. CQC Inspection The CQC undertook an announced inspection of PAH services at the beginning of December. Formal feedback following the inspection is awaited.

RFH | Barnet & Chase Farm Hospital
58
Description Target Month
Current Month
Prior Month YTD
Actual
Increase/ decrease in
performance from last
Month Oct Sep
Diagnostic waiting times Percentage carried out within 6 weeks from referral 99% Oct 99.5% 99.8% 99.5%
Cancer waits 2 weeks for urgent cancer GP referrals 93% Oct No data 94.1% 93.7% 2 weeks for urgent breast symptom referrals 93% Oct No data 94.6% 93.8% 31 days to first definitive treatment for all cancers 96% Oct No data 100.0% 99.9% 31 days for subsequent surgery 94% Oct No data 100.0% 100.0% 31 days for subsequent drug 98% Oct No data 100.0% 100.0% 62 days to first definitive treatment for all cancers 85% Oct No data 85.7% 87.5% 62 days following screening referral 90% Oct No data 100.0% 95.5%
Friends and Family Inpatient Percentage Recommended (Chase Farm) None Oct 95.4% 97.8% 94.9%
A&E Percentage Recommended (Barnet) None Oct 80.3% 80.6% 80.2%
A&E ENHCCG patients only Total A&E attendances None Oct 521 528 3656 -
Percentage seen within 4 hours (Trust wide) 95% Oct 88.3% 84.6% 87.7% Total Emergency Admissions None Oct 174 178 1347 -
Ambulances
Number of patients waiting >30 - <60mins None Oct 256 267 1602
Number of patients waiting >60mins None Oct 102 148 610
Mixed Sex Accommodation Number of clinically unjustified MSA breaches 0 Oct 43 33 233
HCAI
No. Clostridium - Hospital Acquired 36
(annual) Oct No data 0 13 No. MRSA - Hospital Acquired 0 Oct No data 0 0

RFH | Summary | page 1 of 3
59
Comments ׀ Cancer 2 week wait The Trust did not achieve the standard of 93% in September, recording 91.9%. Performance has been impacted on by patient and clinician availability over the summer period and the trust has now revised its standard communications with all patients to ensure they are aware they need to make themselves available at short notice for tests and appointments. The standard was expected to be met in October. Cancer 31 day wait diagnosis to treatment- all cancer The combined trust failed the 96% standard achieving 95.6%. This percentage was driven by RFH site where 92.97% was recorded with Barnet achieving 100%. Cancer 31 day wait- subsequent surgery Overall the combined trust achieved 92.14% against the 94% target. However, RFH site recorded 90.91% with Barnet recording 100%. Cancer 62 Days from GP referral For September the combined trust recorded 81.3% against the 85% standard. Barnet achieved 85.7% and the RFH achieved 76.0% which is an improvement on the previous month. The trust are focusing significant resources at recovering this standard and is reporting to NHS Improvement weekly. There are currently pathway redesigns underway in Lower Gastrointestinal, Renal and Lung. The trust has produced cancer recovery plans.

RFH | Summary | page 2 of 3
60
Comments ׀ Diagnostic 6 week wait • For October 17 the combined trust recorded 98.43% which failed the 99% standard. • The CT Radiology modality was non compliant with 56 breaches due to ongoing capacity challenges with cardiac CT. Demand and capacity
work is being undertaken to help address this. • BCF echocardiography and cystoscopy were non compliant. • RFH site recorded 97.2% overall with CT, ECT, colonoscopy and cystoscopy failing the standard. In aggregate, RFH recorded 167 breaches
which is an improvement on last month. • Services are working on improvement plans to recover performance. A&E • A&E performance recovered to 87.04% in October for the combined trust against the 95% standard. Both sites failed with RFH recording
85.3% and Barnet recording 84.5%. • Barnet Hospital has a whole system transformation plan which includes out of hospital capacity and the RFH transformation plan is
complete and awaiting sign off. • The governance and oversight arrangements for winter are being strengthened, the A&E delivery board for both sites will be co-chaired by
RF Group CEO and STP CEO. Winter plans have been agreed with local CCGs and submitted to NHSE. RTT incomplete. • The Trust fell short of the 92% plan achieving 86.86%. The Trust has been improving the management of the patient tracking list (PTL) used
to calculate performance. Further work is required to validate the full position and develop recovery action plans where necessary. ENHCCG has requested details of all patients breaching the standard.
52 week waits • Trust wide 52 week wait breaches total 37 as at the end of October. Details have been requested for the numbers of ENHCCG patients
waiting >52 weeks.

RFH | Summary | page 3 of 3
61
Comments ׀ C. difficile and MRSA blood stream infections At the end of October the Trust had reported a total of 47 cases of C-difficile; 16 of the cases occurred at the Barnet and Chase Farm sites. This is equal to the ceiling for Barnet and Chase Farm sites, and above the ceiling for the Trust as a whole. Through review of the cases no lapses in care have been identified in any of the cases reported at the BCFH sites. Two cases of MRSA have been reported by the RF YTD; neither of the cases occurred at the BCFH sites. Never Events A further Never Event was reported in November relating to wrong site surgery at the Royal Free Hospital site. The Trust has now declared 5 Never Events YTD. One relating to a surgical procedure has occurred at the Barnet site. Pressure ulcers Up to the end of September RF reported 185 grade 2-4 hospital acquired pressure ulcers YTD, 89 of which were at the BCFH sites. There is ongoing bi-monthly training regarding pressure ulcer prevention and management on both sites, and all new staff have pressure ulcer management and prevention included in their nursing induction. The Trust has a Pressure Ulcer Practice and Prevention Initiative in place across all sites, targeting ward areas with the highest prevalence of pressure ulcers. Particular attention is being paid to equipment-related pressure ulcers. Workforce The overall Trust vacancy rate has increased slightly in Q2 compared to Q1 with a rate of 13.21% in September. The turnover rate for RF has remained stable with an overall turnover rate of 15.5% in September; following an increase in Q1 there has been a slight reduction in turnover at the Chase Farm site. The Trust continues to hold monthly open days and 2 assessment centres a month to ensure on-going recruitment.

HCT |
62
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Average Length of Stay Stroke (days) 42 Oct 30.5 27.8 35.8
Stroke rehab pathway (days) 42 Oct 30.2 27.3 32.8
Non-stroke (days) 21 Oct 23.6 28.7 25.7
Non-stroke rehab pathway (days) 21 Oct 19.7 21.8 19.3
Readmission rates within 30 days 1.0% Oct 0.0% 0.0% 0.0%
Early Supported Discharge All new stroke patients discharged from Acute/Community inpatient care into ESD 35% Oct 45.10% 48.94% 53.91%
Percentage of patients assessed and discharged from an acute or inpatient setting within 1 working day of referral 70% Oct 87.00% 96.00% 87.14%
Percentage of patients whose treatment programme started within one working day of discharge from hospital 90% Oct 100.00% 100.00% 88.14%
Consultant Led Referral to Treatment Times (RTT) Completed Non-admitted patients None Oct 89.0% 92.9% 89.0%
Incomplete pathways 92% Oct 96.31% 96.68% 96.31%
Patients waiting at the end of the month None Oct 3,550 3,287 3,550
Number of 52 week breaches 0 Oct 0 0 0
Mixed Sex Accommodation Number of clinically unjustified MSA breaches 0 Oct 0 0 0
HCAI
No. Clostridium - Community Acquired 6
(annual) Oct No data 1 4 No. MRSA - Community Acquired 0 Oct No data 0 0

Comments ׀ Performance The non-stroke ALoS rose sharply in September to 28.7, but has reduced in October to 23.6 against a target of <21. Actions HCT presented to the Contract Review Meeting in November, and noted that the roll out of Red 2 Green (R2G) is starting to improve length of stay and reduce delays in inpatient units. HCT are continuing to support this process, and have recognised that the staff turnover at Herts and Essex Hospital meant that R2G had not properly embedded. The trust has conducted a further roll out/refresh at Herts and Essex to continue to support and improve patient flow and thereby improving performance against the ALoS.
HCT | Average Length of Stay (ALoS)
63
0
5
10
15
20
25
30
35
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Non-stroke (ENHCCG Patients only)
LoS Target <21
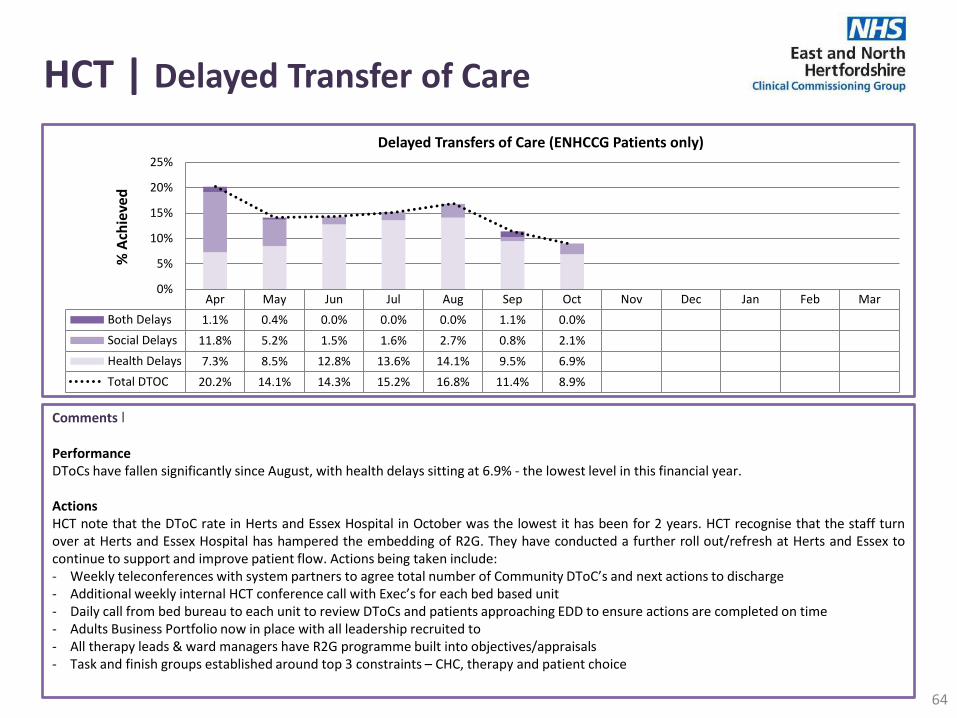
Comments ׀ Performance DToCs have fallen significantly since August, with health delays sitting at 6.9% - the lowest level in this financial year. Actions HCT note that the DToC rate in Herts and Essex Hospital in October was the lowest it has been for 2 years. HCT recognise that the staff turn over at Herts and Essex Hospital has hampered the embedding of R2G. They have conducted a further roll out/refresh at Herts and Essex to continue to support and improve patient flow. Actions being taken include: - Weekly teleconferences with system partners to agree total number of Community DToC’s and next actions to discharge - Additional weekly internal HCT conference call with Exec’s for each bed based unit - Daily call from bed bureau to each unit to review DToCs and patients approaching EDD to ensure actions are completed on time - Adults Business Portfolio now in place with all leadership recruited to - All therapy leads & ward managers have R2G programme built into objectives/appraisals - Task and finish groups established around top 3 constraints – CHC, therapy and patient choice
HCT | Delayed Transfer of Care
64
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Both Delays 1.1% 0.4% 0.0% 0.0% 0.0% 1.1% 0.0%
Social Delays 11.8% 5.2% 1.5% 1.6% 2.7% 0.8% 2.1%
Health Delays 7.3% 8.5% 12.8% 13.6% 14.1% 9.5% 6.9%
Total DTOC 20.2% 14.1% 14.3% 15.2% 16.8% 11.4% 8.9%
0%
5%
10%
15%
20%
25%
% A
chie
ved
Delayed Transfers of Care (ENHCCG Patients only)

Comments ׀ Performance HCT have not met their target of 90% of patients meeting their estimated date of discharge. For October, only 49% of patients were discharged on the date estimated. This is a reduction from previous months. Actions EDD achievement rates are being escalated to the locality managers of each hospital unit, and EDD processes are currently being reviewed by HCT. The embedding of the R2G process will also support EDD achievement.
HCT | Estimated Date of Discharge (EDD)
65
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Estimated Date of Discharge
Achieved

HCT | Serious Incidents
66
Comments ׀ During Q3 HCT reported 7 SIs across the organisation, 2 of which related to ENHCCG patients. HCT has reported no Never Events YTD.
Safeguarding Adults Fracture following a fall IG Breach Pressure ulcer
Q4 0 0 1 0
Q1 0 1 0 0
Q2 0 0 0 1
Q3 0 0 1 1
0
0.2
0.4
0.6
0.8
1
1.2N
um
be
r
HCT (ENHCCG): Type of Serious Incident 2016/17 - 2017/18

HCT | Workforce| page 1 of 2
67
Comments ׀ The Trust’s vacancy rate has fallen in October 2017 to 10.4% against a 10% target. This is in part due to a reduction of 30 wte budgeted establishment in the adult community teams in Herts Valley, which is being implemented through taking out vacancies and reallocating staff across the patch. The remaining vacancies in these services, which had been on hold for this redeployment, can now be recruited to. Recent work to improve recruitment has included distributing 500 posters to Community Centres, libraries, supermarkets etc. across Hertfordshire. Four job fairs have been attended in the last two months and the Trust has also continued to increase its social media presence. ICT staffing is flexed as required to ensure priorities and delivery of safe care. This is monitored at QRM.
Nursing Vacancy Rate by bed base: Apr 17
Nursing Vacancy Rate by Community Team:
October 17 Herts and
Essex QVM Danesbury
Vacancy Rate 32.14% 13.08% 11.47%
October 17 Stevenage Royston Welwyn &
Hatfield North Herts
Vacancy Rate
11.1% 2.4% 17.8% 2.4%
October 17 Lower Lea
Valley Upper Lea
Valley Bishop Stortford
& Stort Valley
Vacancy Rate 9.9% 9.0% 14.1%
HCT Target 8.5% 8.5% 8.5%

HCT | Workforce| page 2 of 2
68
Comments ׀ Staff turnover rates are currently at 14.62% for underlying turnover and 23.16% for total turnover (which includes TUPE transfers out). Under the NHSI Nurse Retention Programme, the Trust’s current priority is a 90 Day Improvement Programme in Herts and Essex Hospital, including running focus groups talking to staff about retention issues. A wider retention workshop for all nurses took place on 4th December and the introduction of a nursing careers clinic is being explored. The stretch target is to reduce nursing turnover from 21.8% to 17% by August 2018. Appraisal rates increased to 89% in October and just 2% under the 90% target. Appraisal rates are increasing as the management cascade to all staff continues. Monitoring and regular training continues.
0%
10%
20%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Vacancy rate
% Vacancy Rate Target <9%
0%
50%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staff appraised in last 12 months
% Appraisal Target 90%
0%
10%
20%
30%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staff turnover rate
% Turnover Target <12%

HCT | Safer Staffing
69
Comments ׀ Herts & Essex hospital continue to have low registered nurse levels due to a vacancy rate of 33.61% of which 4.78 WTE Band 5 vacancies. Long line agency staff continues until vacancies are filled. The additional HCAs on days helped to mitigate for the low RN rates.
Herts and Essex Day
Month Nurse HCA
April 86% 117.1%
May 84.3% 167.3%
June 78.8% 134.0%
July 76.5% 134.2%
August 68.0% 156.7%
September 80.8% 177.7%
October 78.8% 135.2%
QVM Day
Month Nurse HCA
April 86.7% 112.7%
May 91.8% 97.0%
June 95.8% 101.1%
July 83.6% 95.9%
August 84.5% 98.1%
September 93.9% 118.8%
October 95.4% 93.0%
Danesbury Day
Month Nurse HCA
April 103.1% 96.8%
May 97.0% 97.7%
June 93.7% 109.1%
July 91.1% 135.8%
August 89.2% 138.0%
September 92.7% 123.1%
October 92.6% 98.1%
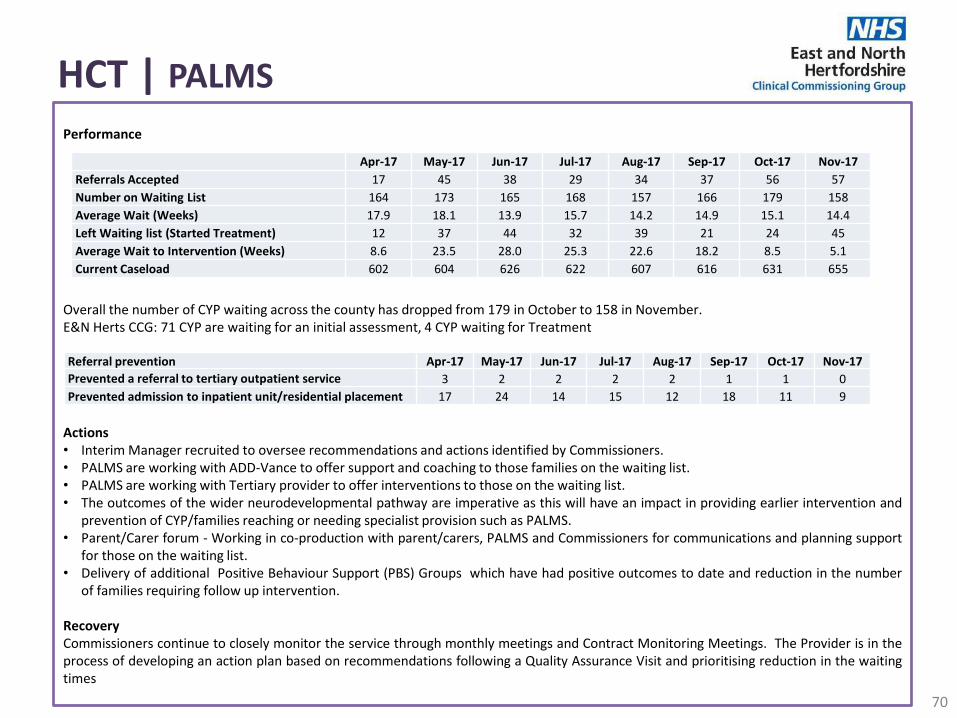
HCT | PALMS
70
Performance Overall the number of CYP waiting across the county has dropped from 179 in October to 158 in November. E&N Herts CCG: 71 CYP are waiting for an initial assessment, 4 CYP waiting for Treatment Actions • Interim Manager recruited to oversee recommendations and actions identified by Commissioners. • PALMS are working with ADD-Vance to offer support and coaching to those families on the waiting list. • PALMS are working with Tertiary provider to offer interventions to those on the waiting list. • The outcomes of the wider neurodevelopmental pathway are imperative as this will have an impact in providing earlier intervention and
prevention of CYP/families reaching or needing specialist provision such as PALMS. • Parent/Carer forum - Working in co-production with parent/carers, PALMS and Commissioners for communications and planning support
for those on the waiting list. • Delivery of additional Positive Behaviour Support (PBS) Groups which have had positive outcomes to date and reduction in the number
of families requiring follow up intervention. Recovery Commissioners continue to closely monitor the service through monthly meetings and Contract Monitoring Meetings. The Provider is in the process of developing an action plan based on recommendations following a Quality Assurance Visit and prioritising reduction in the waiting times
Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17
Referrals Accepted 17 45 38 29 34 37 56 57
Number on Waiting List 164 173 165 168 157 166 179 158
Average Wait (Weeks) 17.9 18.1 13.9 15.7 14.2 14.9 15.1 14.4
Left Waiting list (Started Treatment) 12 37 44 32 39 21 24 45
Average Wait to Intervention (Weeks) 8.6 23.5 28.0 25.3 22.6 18.2 8.5 5.1
Current Caseload 602 604 626 622 607 616 631 655
Referral prevention Apr-17 May-17 Jun-17 Jul-17 Aug-17 Sep-17 Oct-17 Nov-17
Prevented a referral to tertiary outpatient service 3 2 2 2 2 1 1 0
Prevented admission to inpatient unit/residential placement 17 24 14 15 12 18 11 9

HCT | Other
71
Comments ׀ No of avoidable category 3 or 4 pressure ulcers acquired in HCT care There were 2 avoidable HCT acquired category 3 Pressure ulcers reported for October 2017, one from Royston ICT caseload and one from WelHat; one was receiving home carers. Validation of October Pressure ulcers incidents is not complete at the time of reporting. Round 2 of at the base training sessions has commenced with a focus on Pressure ulcer Root Cause Analysis themes and wound assessment CQUIN.
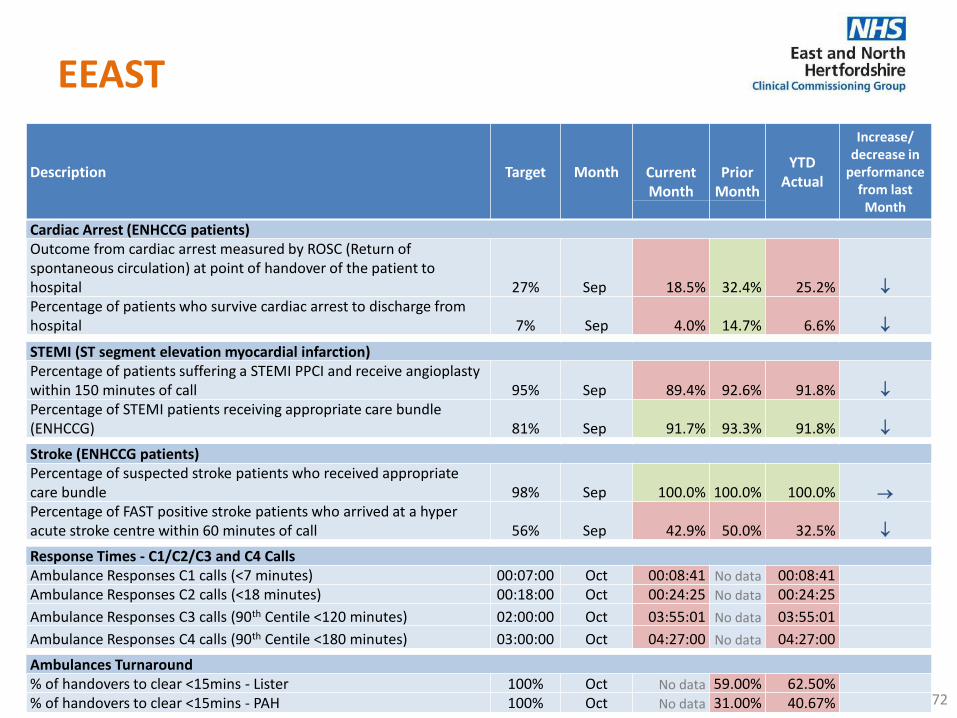
EEAST
72
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Cardiac Arrest (ENHCCG patients) Outcome from cardiac arrest measured by ROSC (Return of spontaneous circulation) at point of handover of the patient to hospital 27% Sep 18.5% 32.4% 25.2%
Percentage of patients who survive cardiac arrest to discharge from hospital 7% Sep 4.0% 14.7% 6.6%
STEMI (ST segment elevation myocardial infarction) Percentage of patients suffering a STEMI PPCI and receive angioplasty within 150 minutes of call 95% Sep 89.4% 92.6% 91.8%
Percentage of STEMI patients receiving appropriate care bundle (ENHCCG) 81% Sep 91.7% 93.3% 91.8%
Stroke (ENHCCG patients) Percentage of suspected stroke patients who received appropriate care bundle 98% Sep 100.0% 100.0% 100.0%
Percentage of FAST positive stroke patients who arrived at a hyper acute stroke centre within 60 minutes of call 56% Sep 42.9% 50.0% 32.5%
Response Times - C1/C2/C3 and C4 Calls Ambulance Responses C1 calls (<7 minutes) 00:07:00 Oct 00:08:41 No data 00:08:41 Ambulance Responses C2 calls (<18 minutes) 00:18:00 Oct 00:24:25 No data 00:24:25
Ambulance Responses C3 calls (90th Centile <120 minutes) 02:00:00 Oct 03:55:01 No data 03:55:01
Ambulance Responses C4 calls (90th Centile <180 minutes) 03:00:00 Oct 04:27:00 No data 04:27:00
Ambulances Turnaround % of handovers to clear <15mins - Lister 100% Oct No data 59.00% 62.50% % of handovers to clear <15mins - PAH 100% Oct No data 31.00% 40.67%

EEAST | AQIs | page 1 of 2
73
Comments ׀ The Trust continues to review the cardiac arrest data closely to better understand any clinical practice that may affect these fluctuations and replicate best practice where possible. Work is ongoing with the air ambulance charities to provide evidence of best practice in order to emulate successes where practicable. Further consultation on the cardiac strategy was sought at the two-day clinical briefing in October from staff and stakeholders.
0%
2%
4%
6%
8%
10%
12%
14%
16%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage of patients who survive cardiac arrest to discharge from hospital
% Achieved Target 7%
0%
10%
20%
30%
40%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Outcome from cardiac arrest measured by ROSC (Return of spontaneous circulation) at point of
handover of the patient to hospital
% Outcome Target 27%
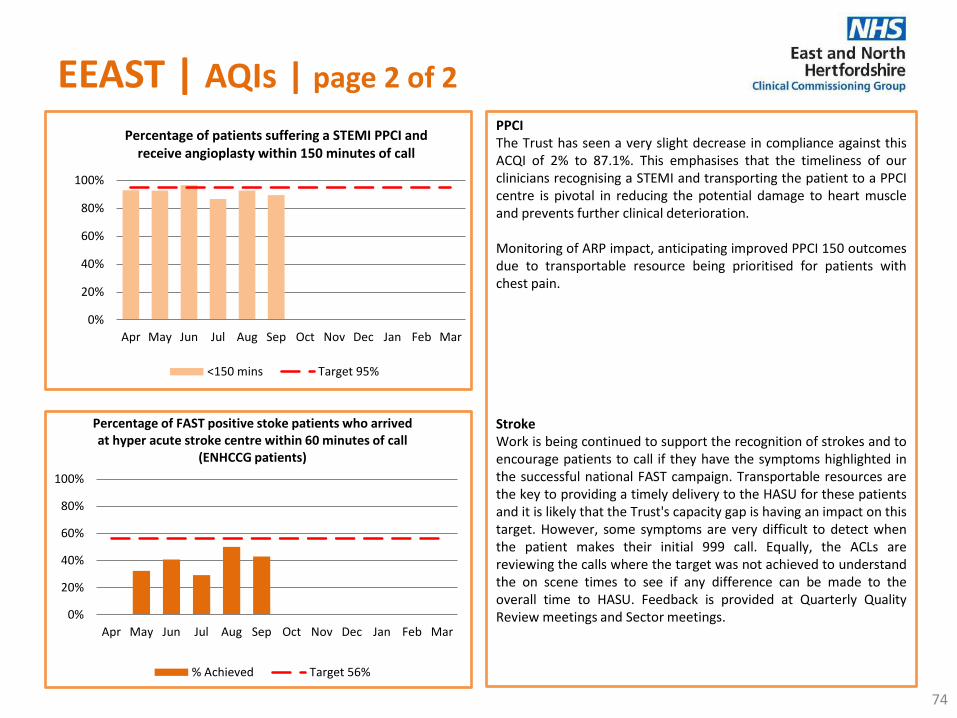
EEAST | AQIs | page 2 of 2
74
PPCI The Trust has seen a very slight decrease in compliance against this ACQI of 2% to 87.1%. This emphasises that the timeliness of our clinicians recognising a STEMI and transporting the patient to a PPCI centre is pivotal in reducing the potential damage to heart muscle and prevents further clinical deterioration. Monitoring of ARP impact, anticipating improved PPCI 150 outcomes due to transportable resource being prioritised for patients with chest pain. Stroke Work is being continued to support the recognition of strokes and to encourage patients to call if they have the symptoms highlighted in the successful national FAST campaign. Transportable resources are the key to providing a timely delivery to the HASU for these patients and it is likely that the Trust's capacity gap is having an impact on this target. However, some symptoms are very difficult to detect when the patient makes their initial 999 call. Equally, the ACLs are reviewing the calls where the target was not achieved to understand the on scene times to see if any difference can be made to the overall time to HASU. Feedback is provided at Quarterly Quality Review meetings and Sector meetings.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage of FAST positive stoke patients who arrived at hyper acute stroke centre within 60 minutes of call
(ENHCCG patients)
% Achieved Target 56%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Percentage of patients suffering a STEMI PPCI and receive angioplasty within 150 minutes of call
<150 mins Target 95%
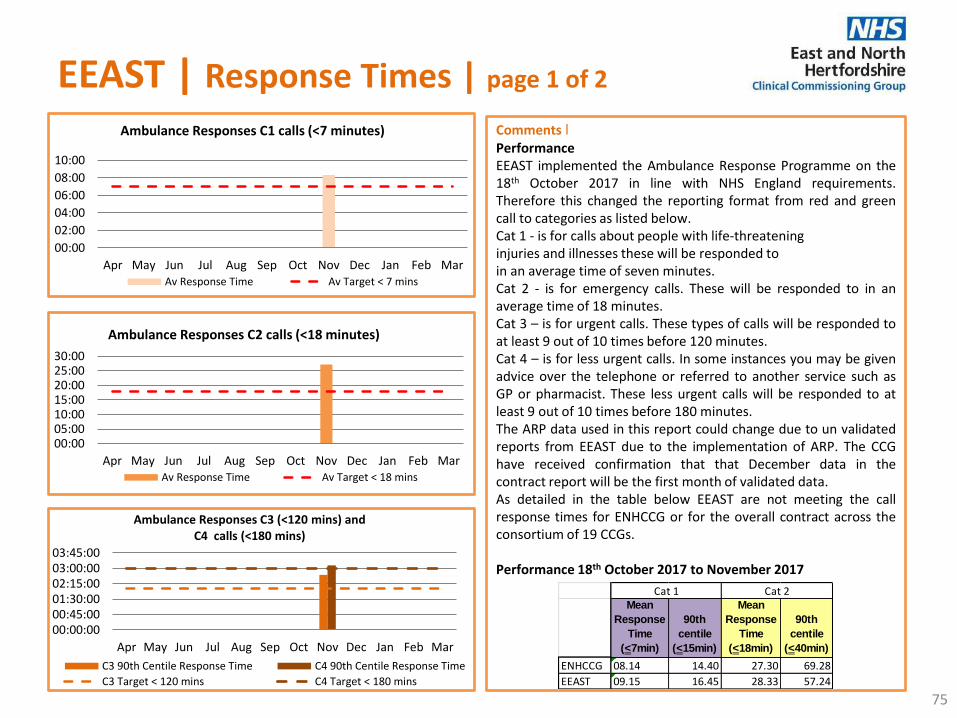
EEAST | Response Times | page 1 of 2
75
Comments ׀ Performance EEAST implemented the Ambulance Response Programme on the 18th October 2017 in line with NHS England requirements. Therefore this changed the reporting format from red and green call to categories as listed below. Cat 1 - is for calls about people with life-threatening injuries and illnesses these will be responded to in an average time of seven minutes. Cat 2 - is for emergency calls. These will be responded to in an average time of 18 minutes. Cat 3 – is for urgent calls. These types of calls will be responded to at least 9 out of 10 times before 120 minutes. Cat 4 – is for less urgent calls. In some instances you may be given advice over the telephone or referred to another service such as GP or pharmacist. These less urgent calls will be responded to at least 9 out of 10 times before 180 minutes. The ARP data used in this report could change due to un validated reports from EEAST due to the implementation of ARP. The CCG have received confirmation that that December data in the contract report will be the first month of validated data. As detailed in the table below EEAST are not meeting the call response times for ENHCCG or for the overall contract across the consortium of 19 CCGs. Performance 18th October 2017 to November 2017
Mean
Response
Time
(<7min)
90th
centile
(<15min)
Mean
Response
Time
(<18min)
90th
centile
(<40min)
ENHCCG 08.14 14.40 27.30 69.28
EEAST 09.15 16.45 28.33 57.24
Cat 1 Cat 2
00:00
02:00
04:00
06:00
08:00
10:00
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses C1 calls (<7 minutes)
Av Response Time Av Target < 7 mins
00:0005:0010:0015:0020:0025:0030:00
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses C2 calls (<18 minutes)
Av Response Time Av Target < 18 mins
00:00:0000:45:0001:30:0002:15:0003:00:0003:45:00
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Responses C3 (<120 mins) and C4 calls (<180 mins)
C3 90th Centile Response Time C4 90th Centile Response Time
C3 Target < 120 mins C4 Target < 180 mins
EEAST | Response Times | page 2 of 2
76
Comments ׀ Performance A predictor tool has been implemented by EEAST which predicts the call category based on the first part of the call conversation with the call operator and caller, C1 predictor tool is currently performing at 57% and Cardiac Arrest C1 predictor continues its positive trend with an outturn of 88%. Conveyance rates for October was 51% of red calls an increase of 2.59% compared to September and 59.21% of green calls a decrease of 3.2%. High vacancy levels have impacted on response times and is being addressed as part of EEAST’s commitment to recruiting more paramedics The vacancy rate for end of November is still high at 18% for ENHCCG and 11% across the Bedfordshire, Hertfordshire and Luton Locality. Another factor impacting on performance is sickness at 8% week ending 10/12/2017 across the consortium. This is 3% above the sickness target of <5%. Actions In order to support delivery of an efficient ambulance service delivering national performance standards, which reflects the ambitions across urgent care, NHS England, NHS Improvement, commissioners and EEAST have agreed, as part of a binding mediation outcome that a jointly commissioned strategic service review is required. It will assess and make practical and implementable recommendations as to the future resourcing required for EEAST in relation to supporting delivery of the Sustainability and Transformation Plan (STP) ambitions, constitutional performance standards and contractual key performance indicators, which are subject to fines and performance management. The work has been commissioned by NHS England and NHS Improvement, with input from EEAST and commissioners who will be joint recipients of the draft and final reports. This work continues and we are expecting the outcome and sign off of the service review by the end of January 2018. Performance is also discussed at the monthly EEAST sector meeting and monthly SLA meeting. CCG’s are also invited to EEAST Operational Performance Improvement and Delivery Group meetings which are held fortnightly and information is provided regarding weekly performance. Recovery Hear and Treat performance is currently delivering 8.9% in November against a target of 9.5%. Private ambulance services are currently being utilised to help with demand.

EEAST | Turnaround Times
77
Comments ׀ Performance ENHT performance for ambulance handovers within 15 minutes handover to clear achievement was 72% for week ending 17/12/2016. There were 8 hour delays over 30 minutes and 1 delay over 60 minutes for week ending 17/12/2016. With regard to PAH, performance for ambulance handovers to clear within 15 minutes for week ending 17/12/2016, achieved 44.7%. There were 8 delays over 30 minutes and 1 delays over 60 minutes within week ending 17/12/2016. ENHCCG continues to commission HALOs working between 10am – 10pm, 7 days a week to facilitate the physical and clinical handover of patients. A Tripartite/Handover Policy is being agreed. Actions Over the last 12 months, ENHT has revised the ambulance handover pathway, including the administrative processes. As a result, ENHT have now significantly improved hours lost over the 15 minute handover time. PAH has recruited agency paramedics to support the queues in ED and a Standard Operating Procedure has been implemented to support the management of the ambulance queue. Recovery The ambulance handover performance and hours lost to handover position will be monitored over the course of the contract 2017-18 to ensure that the improvements continue and are sustained. Ambulance handover performance is also discussed in a number of meetings including the monthly contract meetings with EEAST; EEAST SLA meetings as well as the Operational Performance Group meetings.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Handover to Clear – PAH
<15mins Target 100%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Ambulance Handover to Clear – Lister Hospital
<15mins Target 100%
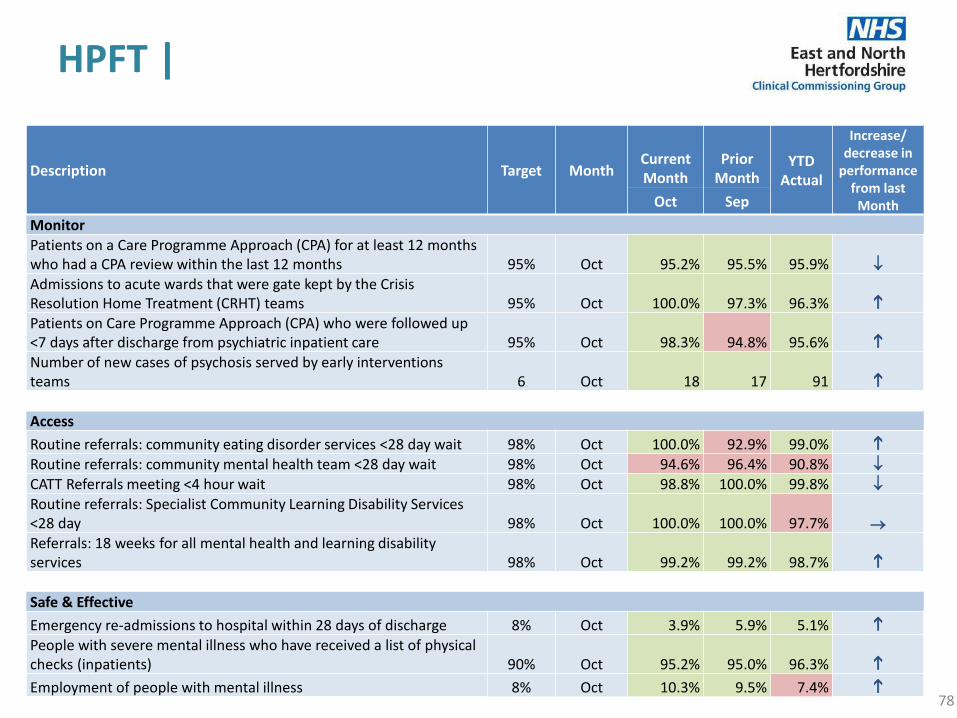
HPFT |
78
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Monitor Patients on a Care Programme Approach (CPA) for at least 12 months who had a CPA review within the last 12 months 95% Oct 95.2% 95.5% 95.9%
Admissions to acute wards that were gate kept by the Crisis Resolution Home Treatment (CRHT) teams 95% Oct 100.0% 97.3% 96.3% Patients on Care Programme Approach (CPA) who were followed up <7 days after discharge from psychiatric inpatient care 95% Oct 98.3% 94.8% 95.6% Number of new cases of psychosis served by early interventions teams 6 Oct 18 17 91 Access
Routine referrals: community eating disorder services <28 day wait 98% Oct 100.0% 92.9% 99.0% Routine referrals: community mental health team <28 day wait 98% Oct 94.6% 96.4% 90.8%
CATT Referrals meeting <4 hour wait 98% Oct 98.8% 100.0% 99.8%
Routine referrals: Specialist Community Learning Disability Services <28 day 98% Oct 100.0% 100.0% 97.7%
Referrals: 18 weeks for all mental health and learning disability services 98% Oct 99.2% 99.2% 98.7%
Safe & Effective
Emergency re-admissions to hospital within 28 days of discharge 8% Oct 3.9% 5.9% 5.1% People with severe mental illness who have received a list of physical checks (inpatients) 90% Oct 95.2% 95.0% 96.3%
Employment of people with mental illness 8% Oct 10.3% 9.5% 7.4%
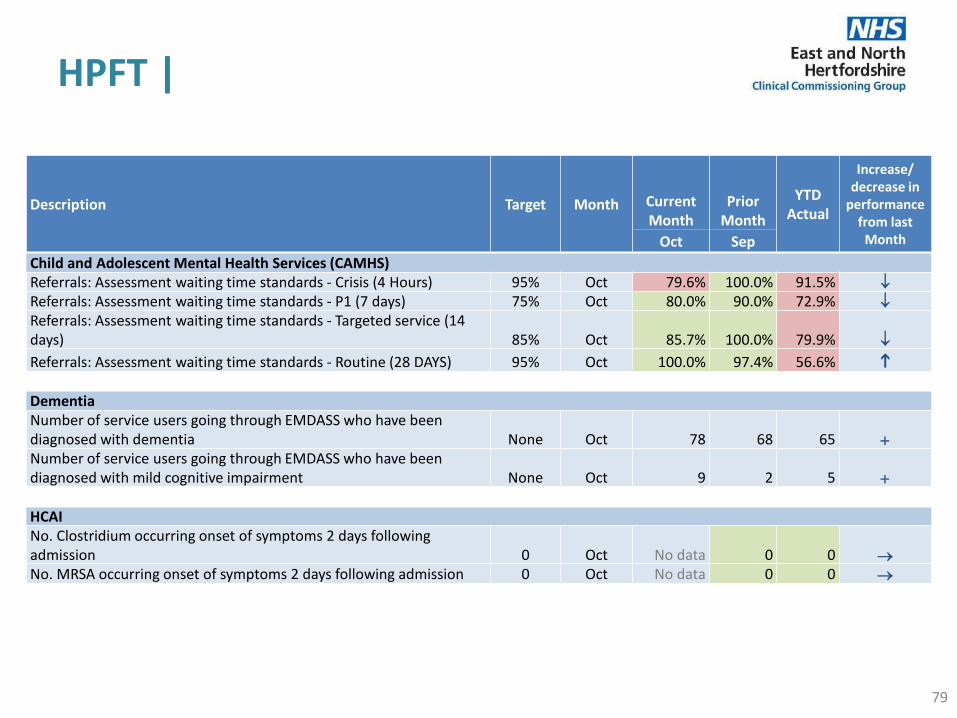
HPFT |
79
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Child and Adolescent Mental Health Services (CAMHS) Referrals: Assessment waiting time standards - Crisis (4 Hours) 95% Oct 79.6% 100.0% 91.5%
Referrals: Assessment waiting time standards - P1 (7 days) 75% Oct 80.0% 90.0% 72.9%
Referrals: Assessment waiting time standards - Targeted service (14 days) 85% Oct 85.7% 100.0% 79.9%
Referrals: Assessment waiting time standards - Routine (28 DAYS) 95% Oct 100.0% 97.4% 56.6% Dementia Number of service users going through EMDASS who have been diagnosed with dementia None Oct 78 68 65 +
Number of service users going through EMDASS who have been diagnosed with mild cognitive impairment None Oct 9 2 5 +
HCAI No. Clostridium occurring onset of symptoms 2 days following admission 0 Oct No data 0 0
No. MRSA occurring onset of symptoms 2 days following admission 0 Oct No data 0 0

HPFT | Access
80
Comments ׀ Performance There were a total of 77 breaches in October of which 7 were in E&SE and 4 in the North. Actions The increase in referrals in the Ware area has challenged East & South East’s ability to achieve the target in November. Work is underway in both North and East & South East with a number of GP practices to ensure that referrals are going to the most appropriate services. Commissioners have agreed HPFT’s proposed new process for managing DNAs, which will be trialled for 3 months and involve stopping the 28 day wait clock after the 1st DNA, as repeat DNAs are impacting on the teams’ ability to meet the 98% target due to the number of breaches. Recovery As of the end of December, there are no patients waiting for initial assessments who are likely to breach, but a number of DNAs still need to be reviewed, which largely relate to October, and could affect the January figures. It is expected that performance will be maintained unless there is an increase in demand.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Routine referrals: community mental health team <28 day wait (ENHCCG)
<28 days Target 98%

HPFT | Safe and Effective
81
Comments ׀ Performance EN CCG achieved 93.81%, 1.19% below the 95% target. Actions East and North SBU are working with those individuals where risk assessments are not completed as part of the supervision process, with clear expectations that these are then to be finalised and are rebooked to sustain performance in future months. Recovery Risk Assessments are expected to be on track by end November. Performance Although HPFT are below the 90% target, they have consistently improved month on month from April 2017. Actions The recording for Adult Social Care Outcomes Framework indicators continues to improve, with the Trust-wide initiative underway. The relatively low percentage in settled accommodation and employment is thought to relate to the fact that those with social care needs were given the initial focus on recording and that these people are likely to have more complex needs and may be more likely not to be in settled accommodation or employment. The overall percentages are expected to increase as the cohort of people who have this recorded widens. Recovery The project plan in process will steadily address this by the end of Q3. .
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Service users with a completed up to date risk assessment
Achieved Target 95%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Settled accommodation for adults with mental health problems
Achieved Target 90%
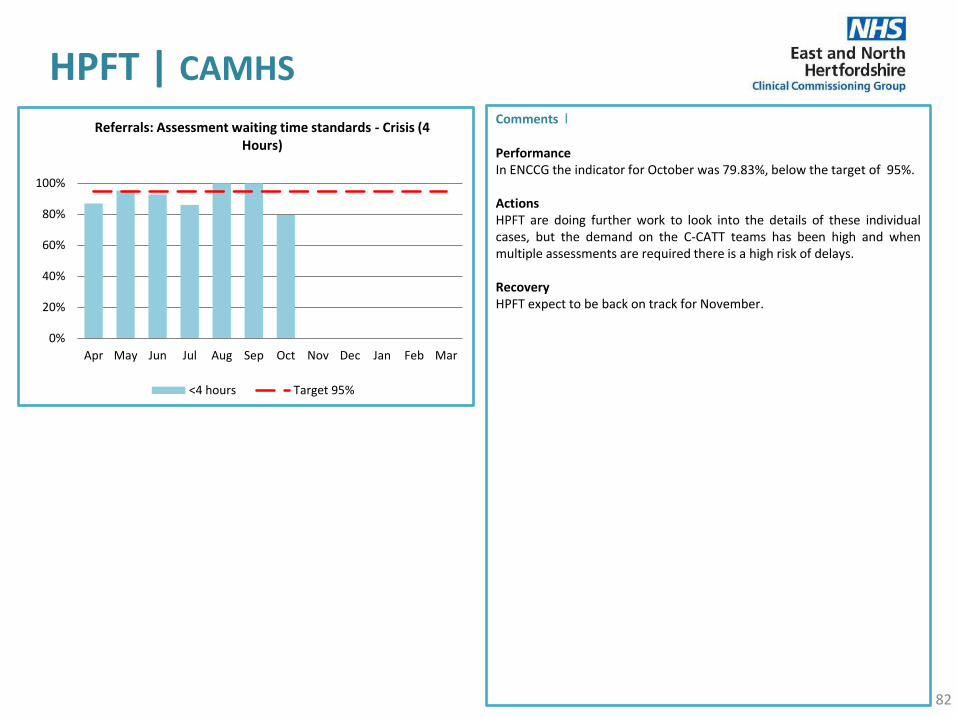
HPFT | CAMHS
82
Comments ׀ Performance In ENCCG the indicator for October was 79.83%, below the target of 95%. Actions HPFT are doing further work to look into the details of these individual cases, but the demand on the C-CATT teams has been high and when multiple assessments are required there is a high risk of delays. Recovery HPFT expect to be back on track for November.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Referrals: Assessment waiting time standards - Crisis (4 Hours)
<4 hours Target 95%

HPFT | Delayed Transfers of Care (DToC)
83
Comments ׀ Performance October DToC performance was above target at 7.32%. However in the preceding months performance had been improving. Actions Over the last quarter (Q2 Jul - Sep) Adult and Older Peoples Services have fully implemented the national Red2Green approach and therefore have a focus on issues causing delay. Across services there is internal scrutiny every week to look at the 5 service users on each ward who have the longest length of stay. This has helped in identifying stranded patients, and themes for reasons for longer stays in the hospital. Across Adult Services and Wren Ward (Functional Frail), HPFT has dedicated discharge facilitators which have started to have a positive effect on lengths of stay and delayed transfers from these units. Adult Community Services (ACS) have been very proactive in addressing issues that cause delays. The longer DToCs in adult services have complex risk profiles and presentations, and are awaiting complex community packages, often accommodation and Tier 4 NHSE funded personality disorder placements. To improve flow through the acute system a number of processes and systems have been implemented and are being embedded to facilitate more effective discharge planning at the point of admission. These include Red2Green, internal professional standards, review of DToC processes, oversight and bed management escalation processes. Recovery The above ongoing work should impact on improvement by the end of Q3.
0%
1%
2%
3%
4%
5%
6%
7%
8%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Delayed Transfers of Care attributable by Trust
% DToC Rate Target
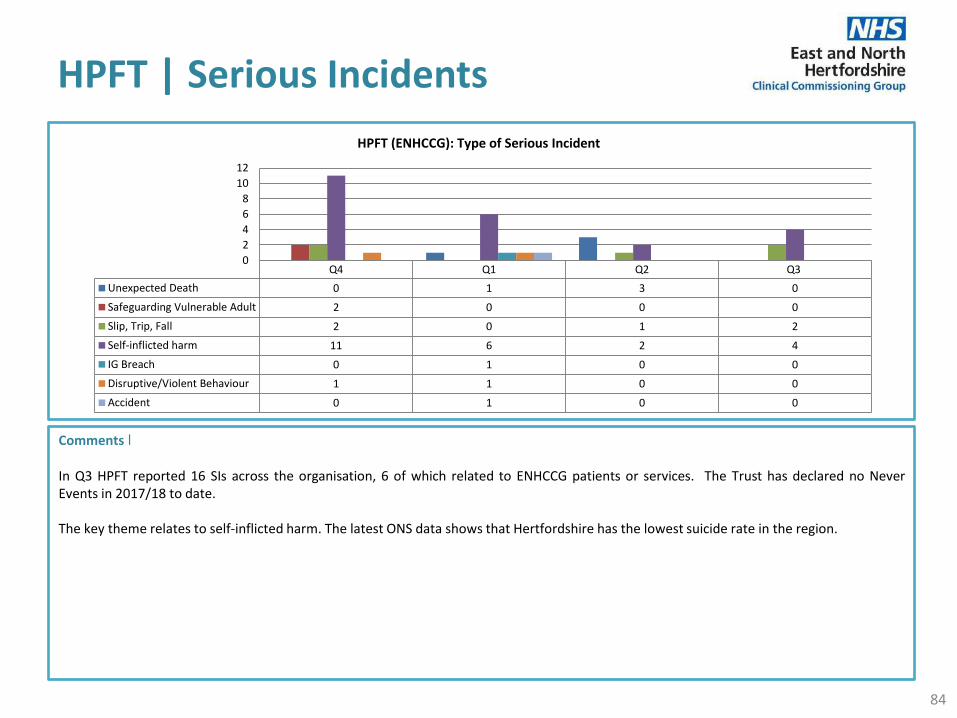
HPFT | Serious Incidents
84
Comments ׀ In Q3 HPFT reported 16 SIs across the organisation, 6 of which related to ENHCCG patients or services. The Trust has declared no Never Events in 2017/18 to date. The key theme relates to self-inflicted harm. The latest ONS data shows that Hertfordshire has the lowest suicide rate in the region.
Q4 Q1 Q2 Q3
Unexpected Death 0 1 3 0
Safeguarding Vulnerable Adult 2 0 0 0
Slip, Trip, Fall 2 0 1 2
Self-inflicted harm 11 6 2 4
IG Breach 0 1 0 0
Disruptive/Violent Behaviour 1 1 0 0
Accident 0 1 0 0
0
2
4
6
8
10
12
HPFT (ENHCCG): Type of Serious Incident
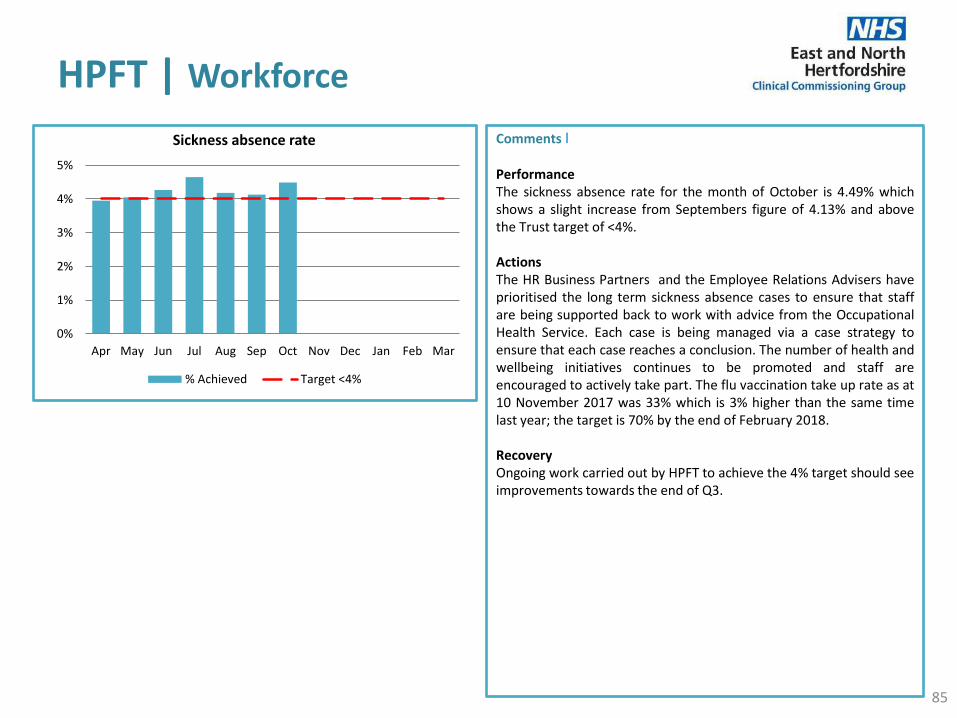
HPFT | Workforce
85
Comments ׀ Performance The sickness absence rate for the month of October is 4.49% which shows a slight increase from Septembers figure of 4.13% and above the Trust target of <4%. Actions The HR Business Partners and the Employee Relations Advisers have prioritised the long term sickness absence cases to ensure that staff are being supported back to work with advice from the Occupational Health Service. Each case is being managed via a case strategy to ensure that each case reaches a conclusion. The number of health and wellbeing initiatives continues to be promoted and staff are encouraged to actively take part. The flu vaccination take up rate as at 10 November 2017 was 33% which is 3% higher than the same time last year; the target is 70% by the end of February 2018. Recovery Ongoing work carried out by HPFT to achieve the 4% target should see improvements towards the end of Q3.
0%
1%
2%
3%
4%
5%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Sickness absence rate
% Achieved Target <4%

HPFT | Workforce
86
Registered Nursing – Inpatient Services
Inpatient Service
Sum of Position
FTE
Sum of Actual FTE
Sum of FTE Variance
% Vacancy
Robin Ward 11.60 4.80 6.80 59%
Albany Lodge 12.80 6.35 6.45 50%
Oak Unit 13.50 7.00 6.50 48%
Swift Ward 17.50 11.00 6.50 37%
Sovereign House
6.00 3.80 2.20 37%
Lambourn Lodge
11.20 7.24 3.96 35%
Seward Lodge 12.00 7.80 4.20 35%
Registered Nursing – Inpatient Services
Strategic Business Unit
Sum of Position
FTE
Sum of Actual FTE
Sum of FTE Variance
% Vacancy
Learning Disability & Forensic
163.11 130.71 32.40 20%
East and North SBU
277.68 218.56 59.12 21%
West SBU 275.08 214.48 60.60 22%
Total 715.87 563.75 152.12 21%
Comments ׀ The Trust continues to have challenges with recruitment with 21% vacancies for Registered Nurses and 17% for Healthcare Assistants. The table to the left sets out the vacancy rates for Registered Nursing workforce for the whole Trust by Strategic Business Unit

HPFT | Other
87
Comments ׀ CQUIN Q2 17/18 Achievement HPFT achieved 77% for Q2 2017, with the opportunity for HPFT to increase this percentage for the CQUIN Improving services for people with mental health needs who present to A&E if sufficient evidence is provided by Q3. This has been signed off for payment with ENCCG Finance and HPFT have acknowledged receiving the formal letter in achieving 77% for Q2 CQUINs 2017/18.

HUC | IUC
88
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep
Home Visits Urgent visits undertaken within 2 hours 95% Oct 87.7% 82.1% 83.2%
Routine visits undertaken within 6 hours 95% Oct 87.8% 84.0% 86.0%
Base face to face consultations following definitive clinical assessment Urgent consultations undertaken within 2 hours 95% Oct 85.0% 91.5% 86.4%
Routine consultations undertaken within 6 hours 95% Oct 94.1% 96.0% 96.5%
NHS 111 % abandoned calls after 30 seconds 5% Oct 1.8% 2.1% 2.7%
Average time to call answer (secs) 60 Oct 32 29 34
% Ambulance dispatches 10% Oct 8.3% 8.9% 7.9%
AiHVS % of calls answered within 60 seconds 95% Oct 93.4% 86.8% 88.8%
Average number daily visits 52 Oct 47 42 44
% Routine visits <6 hours 95% Oct 99.0% 97.8% 96.9%
Visits Passed to the OOH service 0 Oct 4 22 73
Clinican Staffing Percentage 95% Oct 97.0% 97.0% 94.7%
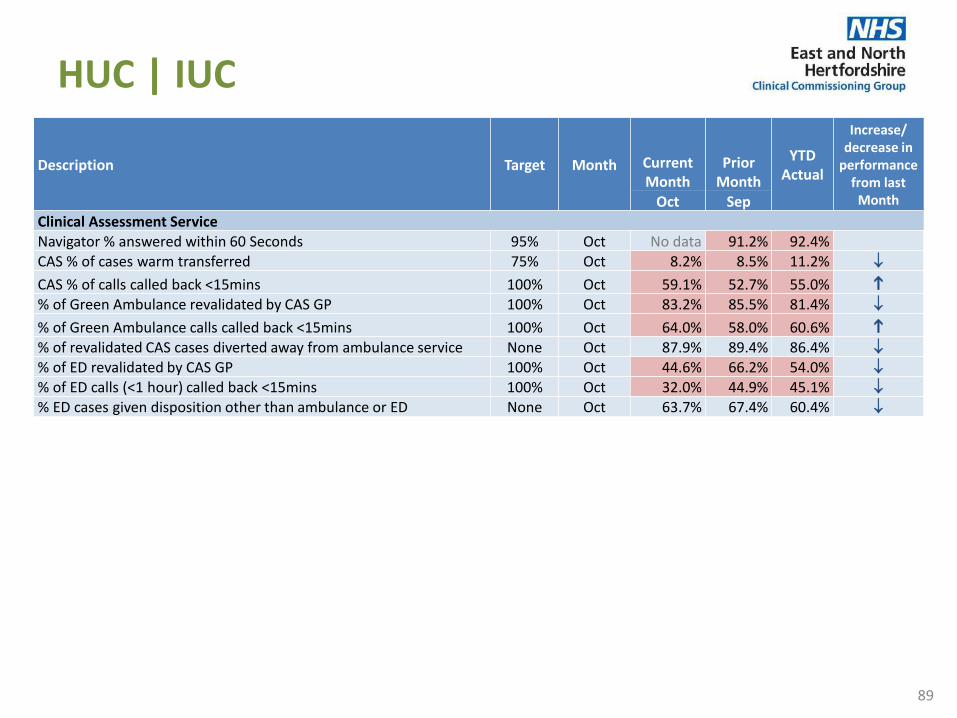
HUC | IUC
89
Description Target Month Current Month
Prior Month
YTD Actual
Increase/ decrease in
performance from last
Month Oct Sep Clinical Assessment Service Navigator % answered within 60 Seconds 95% Oct No data 91.2% 92.4% CAS % of cases warm transferred 75% Oct 8.2% 8.5% 11.2%
CAS % of calls called back <15mins 100% Oct 59.1% 52.7% 55.0% % of Green Ambulance revalidated by CAS GP 100% Oct 83.2% 85.5% 81.4%
% of Green Ambulance calls called back <15mins 100% Oct 64.0% 58.0% 60.6% % of revalidated CAS cases diverted away from ambulance service None Oct 87.9% 89.4% 86.4%
% of ED revalidated by CAS GP 100% Oct 44.6% 66.2% 54.0%
% of ED calls (<1 hour) called back <15mins 100% Oct 32.0% 44.9% 45.1%
% ED cases given disposition other than ambulance or ED None Oct 63.7% 67.4% 60.4%
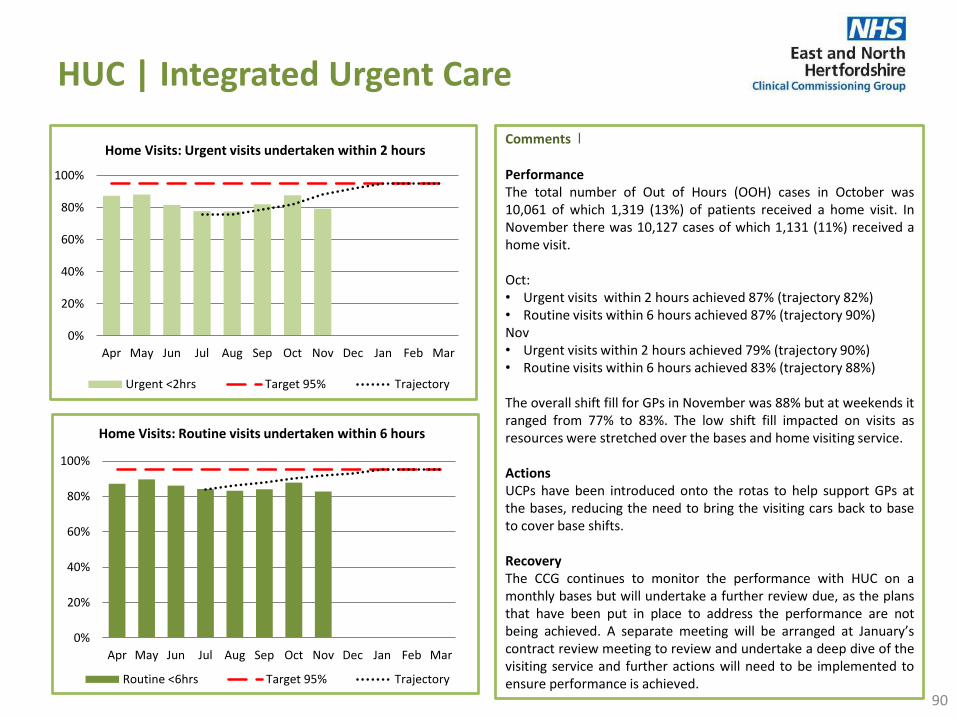
HUC | Integrated Urgent Care
90
Comments ׀ Performance The total number of Out of Hours (OOH) cases in October was 10,061 of which 1,319 (13%) of patients received a home visit. In November there was 10,127 cases of which 1,131 (11%) received a home visit. Oct: • Urgent visits within 2 hours achieved 87% (trajectory 82%) • Routine visits within 6 hours achieved 87% (trajectory 90%) Nov • Urgent visits within 2 hours achieved 79% (trajectory 90%) • Routine visits within 6 hours achieved 83% (trajectory 88%) The overall shift fill for GPs in November was 88% but at weekends it ranged from 77% to 83%. The low shift fill impacted on visits as resources were stretched over the bases and home visiting service. Actions UCPs have been introduced onto the rotas to help support GPs at the bases, reducing the need to bring the visiting cars back to base to cover base shifts. Recovery The CCG continues to monitor the performance with HUC on a monthly bases but will undertake a further review due, as the plans that have been put in place to address the performance are not being achieved. A separate meeting will be arranged at January’s contract review meeting to review and undertake a deep dive of the visiting service and further actions will need to be implemented to ensure performance is achieved.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Home Visits: Urgent visits undertaken within 2 hours
Urgent <2hrs Target 95% Trajectory
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Home Visits: Routine visits undertaken within 6 hours
Routine <6hrs Target 95% Trajectory

HUC | Integrated Urgent Care
91
Comments ׀ Performance Urgent consultations to be seen within 2 hours performed at 87.7% in October and 87.1% in November 2017. The routine consultations of 6 hours has improved and achieved the target in November. As for home visiting, the main impact on performance is a shortage in the shift fill where resource is being stretched to fill the gaps on the rotas. HUC have inducted 5 GPs in November and have had a third UCP start at the beginning of December. Actions HUC are reviewing the visiting capacity against the rota fill to ensure shifts are at the right time and are considering shortening visiting shifts. A consultation is being sent to GPs for feedback on this proposal. HUC continue to train the Senior Clinical Advisors to work within the CAS and to work outside of pathways to support the triage queues. This will help with base staffing fill as GPs will be able to focus on the base/visiting shifts. Recovery As with the home visiting performance, the CCG will continue to monitor the performance with HUC on a monthly bases. A further review will be undertaken as performance has not been achieved over the last few months. A separate meeting will be arranged at Januarys contract review meeting to review and undertake a deep dive of the visiting service and further actions will need to be implemented to ensure performance is achieved.
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Base Face to Face Consultations: urgent consultations undertaken within 2 hours
Urgent <2hrs Target 95%
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Base Face to Face Consultations: Routine consultations undertaken within 6 hours
Routine <6hrs Target 95%

HUC | Integrated Urgent Care
92
Comments ׀ Performance Since the launch of the new CAS models, we have seen GPs have been extremely busy at all times and the 15 minute target for warm transfers has been extremely difficult to achieve. As the service is completely new, the CCG acknowledges that the initial targets that were set locally were going to challenge the service, and there was a risk that the targets would not be achieved. There will be a review of all the IUC KPIs and these will be aligned to the national targets which are to be released in January. Actions The CAS is monitored closely by the CCGs via the contract and quality review meetings. When the national KPIs are launched in January there will be a complete review of all the KPIs to ensure that the service is aligned to the national requirements.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
CAS % of calls called back <15mins
Achieved Target 100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
CAS % of cases warm transferred
Achieved Target 75%

HUC | Integrated Urgent Care
93
Comments ׀ Performance The revalidation of green ambulance calls has undergone a review and there were certain dispositions identified that did not require the input of a GP; the outcome would always result in an ambulance being sent whether the call was revalidated by a GP or other clinicians, so now, these calls are redirected to other clinicians for revalidation. Where cases that should have been sent to the CAS GP for revalidation are identified, these are picked up with the individuals to ensure there is an ongoing feedback for learning purposes. The CAS manager meets with any staff that repeatedly dispatch an ambulance to identify and support any training requirements. Actions The CAS is monitored closely by the CCGs via the contract and quality review meetings. When the national KPIs are launched in January there will be a complete review of all the KPIs to ensure the service is aligned to the national requirements.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% of Green Ambulance revalidated by CAS GP
Achieved Target 100%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% of Green Ambulance calls called back <15mins
Achieved Target 100%

HUC | Integrated Urgent Care
94
Comments ׀ Performance There has been a reduction in the number of ED dispositions for the month of November by 9.5%, and it is felt that this is due to staff becoming more experienced and confident with using pathways and probing techniques improving as more calls are taken. There are a number of CAs that are cautious and lack confidence in making some decisions around sending patients to alternative services other than ED. Ongoing coaching is required for these staff members to help them understand that the patient will be receiving the most appropriate care which can include a home visit, come to centre appointment, attend their own GP surgery or further home management advice. As staff become more confident, with the new processes and service, it is expected that there will be a continuous improvement in the numbers of revalidations.
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% of ED revalidated by CAS GP
Achieved Target 100%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% of ED calls (<1 hour) called back <15mins
Achieved Target 100%

HUC | Integrated Urgent Care
95
Comments ׀ October There were 921 visits with an average of 42 a day and 4 visits were passed into the OOH period. The service reached capacity on one occasion and achieved 97% rota fill for the month; 99.0% of routine visits were carried out within 6 hours. November There were 1,041 visits with an average of 47 per day and one visit passed into the OOH period. The service did not reach capacity; 100% of Routine visits were carried out within 6 hours. The service has entered into the winter period and has now increased capacity to receive 90 visits per day. Call answering did not achieve target and was down on the previous month’s performance. This was due to receiving a influx of calls on the three occasions when target training sessions were being held and calls were being incorrectly diverted to the AiHVS number. Actions AiHVS has seen a decrease in referrals over the past few months which prevents the service on achieving the daily visiting target. The CCG has undertaken a review of the referral criteria and agreed with HUC to the amendments which will see the number of visits increase. HUC have recently started providing the flu service to care homes. This has added additional pressure on AiHVS but will be closely monitored by the CCG against the impact on the wider health system.
0
50
100
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
AiHVS Average number daily visits
No. of Visits Target (60-90)
80%
85%
90%
95%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
AiHVS % of calls answered within 60 seconds
% <60 secs Target 95%
0
20
40
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
AiHVS Visits Passed to the OOH service
No. of Visits Target = 0
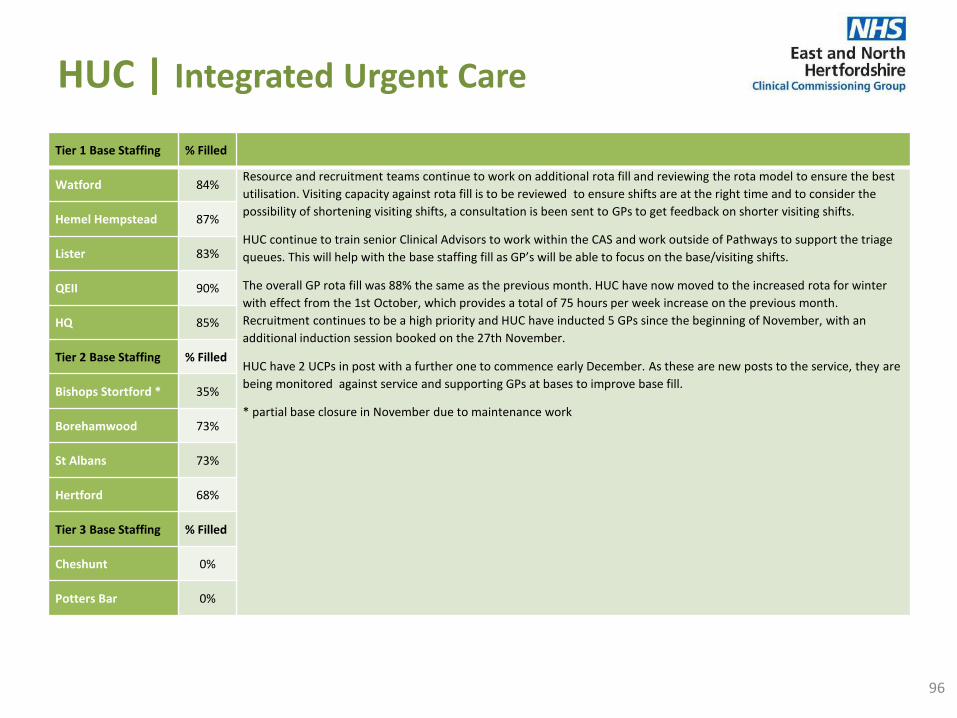
HUC | Integrated Urgent Care
96
Tier 1 Base Staffing % Filled
Watford 84% Resource and recruitment teams continue to work on additional rota fill and reviewing the rota model to ensure the best
utilisation. Visiting capacity against rota fill is to be reviewed to ensure shifts are at the right time and to consider the
possibility of shortening visiting shifts, a consultation is been sent to GPs to get feedback on shorter visiting shifts.
HUC continue to train senior Clinical Advisors to work within the CAS and work outside of Pathways to support the triage
queues. This will help with the base staffing fill as GP’s will be able to focus on the base/visiting shifts.
The overall GP rota fill was 88% the same as the previous month. HUC have now moved to the increased rota for winter
with effect from the 1st October, which provides a total of 75 hours per week increase on the previous month.
Recruitment continues to be a high priority and HUC have inducted 5 GPs since the beginning of November, with an
additional induction session booked on the 27th November.
HUC have 2 UCPs in post with a further one to commence early December. As these are new posts to the service, they are
being monitored against service and supporting GPs at bases to improve base fill.
* partial base closure in November due to maintenance work
Hemel Hempstead 87%
Lister 83%
QEII 90%
HQ 85%
Tier 2 Base Staffing % Filled
Bishops Stortford * 35%
Borehamwood 73%
St Albans 73%
Hertford 68%
Tier 3 Base Staffing % Filled
Cheshunt 0%
Potters Bar 0%
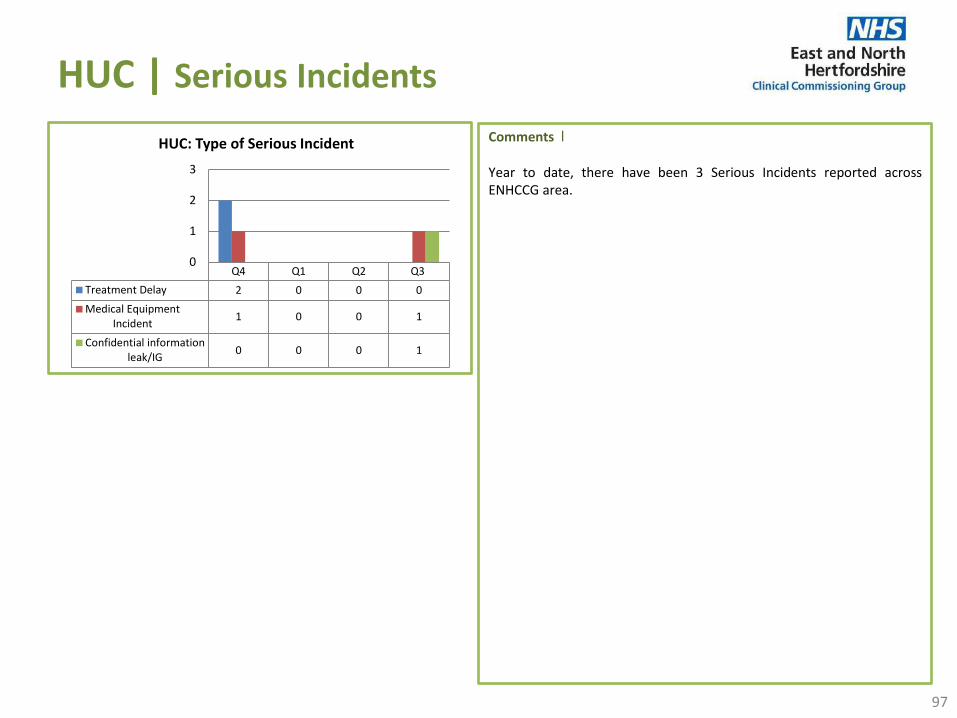
HUC | Serious Incidents
97
Comments ׀ Year to date, there have been 3 Serious Incidents reported across ENHCCG area.
Q4 Q1 Q2 Q3
Treatment Delay 2 0 0 0
Medical EquipmentIncident
1 0 0 1
Confidential informationleak/IG
0 0 0 1
0
1
2
3
HUC: Type of Serious Incident
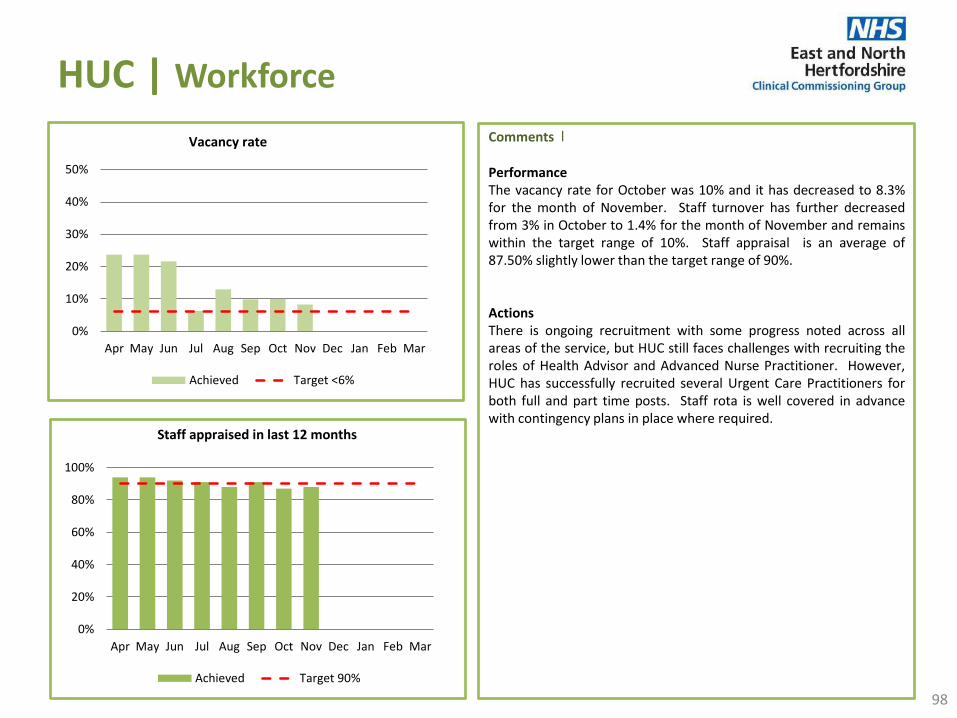
HUC | Workforce
98
Comments ׀ Performance The vacancy rate for October was 10% and it has decreased to 8.3% for the month of November. Staff turnover has further decreased from 3% in October to 1.4% for the month of November and remains within the target range of 10%. Staff appraisal is an average of 87.50% slightly lower than the target range of 90%. Actions There is ongoing recruitment with some progress noted across all areas of the service, but HUC still faces challenges with recruiting the roles of Health Advisor and Advanced Nurse Practitioner. However, HUC has successfully recruited several Urgent Care Practitioners for both full and part time posts. Staff rota is well covered in advance with contingency plans in place where required.
0%
10%
20%
30%
40%
50%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Vacancy rate
Achieved Target <6%
0%
20%
40%
60%
80%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staff appraised in last 12 months
Achieved Target 90%
The Pathology Partnership (TPP)
99
Comments ׀ During Q3 a total of 3 enquiries were received via the GP hotline relating to TPP. This is a decrease compared to Q2. There were no themes in relation to the queries received. Following the organisational change of pathology services in May 2017, the CCG continues to work closely with the provider and host commissioner to monitor the quality of services and ensure practices are kept well informed of any changes. Visits have been undertaken by ENHCCG and C&PCCG Quality Teams to Pathology Services at CUHFT and ENHT to seek assurance regarding the governance processes in place, and assurance that key recommendations from the external review previously undertaken have been implemented. The visits were positive, and it was clear that processes have been strengthened following organisational changes.

Private Providers
100
Comments ׀
Ramsey The RTT incomplete target has been met at CCG level in October 2017, with 99.1% achieved at Pinehill, and 99.7% achieved at Rivers. This means that the required numbers of ENHCCG patients are waiting less than 18 weeks for treatment. This standard has been consistently achieved throughout 2017/18 to date. The diagnostic standard was achieved at CCG level in October 2017 with 100% of ENHCCG patients being seen within 6 weeks for diagnostic tests at both Rivers and Pinehill Hospital. This standard has been consistently achieved throughout 2017/18 to date. Quality An unannounced Quality Assurance visit took place at Pinehill Hospital on 6th December 2017. Good staff engagement with colleagues and patients, positive patient experiences, and good multi-disciplinary working were all noted by ENHCCG. Services Additional Direct Access MRI capacity at Pinehill Hospital came into effect on Monday 3rd July. Referral volumes are increasing, and continues to be monitored by the CCG. Serious Incidents A serious Incident was reported in December bringing the total year to date of 3 SIs reported (April, August and December). There have been no Never events reported YTD.
Spire Harpenden site – July – September 2017 Performance • RTT is 97.1% against the required target of 92%. • Diagnostic Waits is 100% against target of 99%. Bushey site – July – September 2017 Performance • RTT is 100% against the required target of 92%. • Diagnostic Waits is 100% against target of 99%. Any under achievement will be discussed at future contract review meetings. Quality There have been no Never Events reported, Friends and Family score is 99% with 94% as extremely likely to recommended the service, with a 47% response rate (as of September 2017) 2 formal complaints have been received by the service to date (April to September). This contract is hosted by HVCCG.

Glossary
101
Acronyms used in this report
ESD Early Supported Discharge
FAST Facial drooping, Arm weakness, Speech difficulties and Time
FFT Friends & Family Test
GP General Practitioner
HALO Hospital Ambulance Liaison Officer
HASU Hyper Acute Stroke Unit
HCA Health Care Assistant
HCT Hertfordshire Community NHS Trust
HDU High Dependency Unit
HPFT Hertfordshire Partnerships Foundation Trust
HUC Herts Urgent Care
IAPT Increased Access to Psychological Therapies
ICT Integrated Community Teams
IUC Integrated Urgent Care
KPI Key Performance Indicators
LOS Length of Stay
MCA Mental Capacity Act
MRI Magnetic Resonance Imaging
MRSA Methicillin-resistant Staphylococcus Aureus
NHSE NHS England
NHSI NHS Improvement
ONS Office for National Statistics
OOH Out of Hours
PAH Princess Alexandra Hospital NHS Trust
PALMS Positive behaviour service for Autism, Learning disability,
Mental health Service
PBR Payment by Results
PPCI Primary percutaneous coronary intervention
PTL Patient Treatment List
Q1, Q2 etc Quarter 1, Quarter 2 etc
QRM Quality Review Meeting
R2G Red to Green
RAT Rapid Access and Treatment
RFH Royal Free Hospital NHS Trust
Acronyms used in this report
A&E Accident and Emergency
ACL Area clinical Lead
ACQI Ambulance Clinical Quality Indicators
ACS Adult Care Services
AIHVS Acute in Hours Visiting Service
ALOS Average Length of Stay
ARP Ambulance Response Programme
ASCOF Adult Social Care Outcomes Framework
BCF Barnet and Chase Farm Hospital
C&PCCG Cambridge and Peterborough Clinical Commissioning Group
C1 Category 1 Ambulance calls about people with life-
threatening injuries and illnesses.
C2 Category 2 is for emergency calls.
C3 Category 3 is for urgent calls
C4 Category 4 is for less urgent calls.
CAMHS Child and Adolescent Mental Health Services
CAS Clinical Assessment Service
CCATT CAMHS Crisis Assessment Targeted Team
CCG Clinical Commissioning Group
CDI Clostridium Difficile
CDU Clinical Decision Unit
CHC Continuing Health Care
CQC Care Quality Commission
CQUIN Commissioning for Quality and Innovation
CUHFT Cambridge University Hospital Foundation Trust
CYP Children and Young People
DToC Delayed Transfer of Care
ED Emergency Department
EDD Estimated Date of Discharge
EEAST East of England Ambulance Service NHS Trust
EMDASS Early Memory Diagnosis & Support Service
ENHCCG East and North Hertfordshire Clinical Commissioning Group
ENHT East and North Herts NHS Trust
ENT Ears Nose and Throat
Glossary
102
Acronyms used in this report
RN Registered Nurse
RTT Referral To Treatment
SHMI Summary Hospital-level Mortality Indicator
SI Serious Incident
SLA Service Level Agreement
SPQRG Service Performance Quality Review Group
STEMI ST segment elevation myocardial infarction
T&O Trauma and Orthopaedics
TIA Transient Ischemic Attack
UCLH University College London Hospital NHS Foundation Trust
UCP Urgent Care Practitioner
WECCG West Essex Clinical Commissioning Group
WTE Whole Time Equivalent
YTD Year to Date

Page 1 of 4
Agenda Item No: 6
Date of Meeting: 18 January 2018
Governing Body Meeting in Public
Paper Title: Chief Executive’s Report
Decision or Approval Discussion Information
Report author: Jas Dosanjh, Corporate Governance Manager
Report signed off by: Beverley Flowers, Chief Executive
Executive Summary: The purpose of this paper is to provide information on activities being undertaken by the Clinical Commissioning Group.
Recommendations
to the members:
To note the report
Conflicts of Interest
involved:
There are none identified.

Page 2 of 4
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

Page 3 of 4
1. Executive Summary
The purpose of this paper is to provide information on activities being undertaken by the Clinical Commissioning Group.
2. Background
2.1 Terms / Acronyms Used in the Report
CCG Clinical Commissioning Group NHS National Health Service
2.2 Memorandum of Understanding between the East and North Hertfordshire NHS Trust and University College London Hospitals NHS Foundation Trust
East and North Hertfordshire NHS Trust and University College London Hospitals (UCLH) NHS Foundation Trust have agreed to work together to develop a clinical academic partnership between Mount Vernon Cancer Centre and UCLH (Appendix 1).
2.3 Winter Resilience
On 22 November the Chancellor announced additional funding for the NHS in 2017/18. The funding has been allocated in two tranches. Firstly, East and North Herts Trust has been allocated £1,051,000 on a ‘fair shares’ basis to reflect the cost of emergency and urgent elective activity across winter. This will ensure the Acute Trust has the financial resilience to continue to deliver services planned to respond to increased demand over winter. The second tranche of funding (£1,500,000) is for new initiatives to improve A&E performance at East and North Herts Trust over winter to ensure patients are seen and treated within 4 hours. Locally this has been invested in:
• 18 additional Acute Beds to increase ward capacity at the local Acute trust • Additional Out of Hours appointments in the Integrated Urgent Care Service (111 and
Out of Hours services) • Increased carer capacity to support the discharge of patients from hospital • Progress Trackers to support patient flow in the Emergency Department • A Care Home Choice Facilitator to help patient choose their care home of choice • Additional Pharmacy Resource to support out of hours requests for take home
medication • Increased on the day dedicated discharge vehicle capacity over seven days • Increased virtual community bed capacity to support patients to be discharged from
hospital earlier.
These schemes are being implemented across the system. Outcomes are monitored through the local A&E Delivery Board.
2.4 360 degree Stakeholder Survey
The annual CCG 360° Stakeholder Survey is launching on 16 January 2018.
The survey forms a central part of the statutory annual assessment of all CCGs. It is a valuable source of evidence that allows both the CCG and NHS England to monitor how our relationships with stakeholders have continued to develop over the last year and will help inform our continuing organisational and leadership development.

Page 4 of 4
As part of the process, we have identified the key stakeholders we would like to take part in the survey. The relationship we have with our stakeholders is integral to our past and future success and we would therefore like to hear their views. The stakeholders taking part include our GP practices, Chairs and Chief Executives from our providers and neighbouring CCGs, local MPs, Hertfordshire County Council, Healthwatch, patient groups and voluntary organisations.
The results of this research will be anonymous, statistical information only; however due to small numbers in some stakeholder groups it is possible that the CCG will be able to identify individual stakeholders and whether they have taken part or not.
The survey is running from 16 January to 24 February. Once the survey is closed Ipsos Mori will compile their report. It is anticipated that the final report will be submitted to CCGs and NHS England by 31 March 2018.
2.5 STP Leadership
The Hertfordshire and west Essex Sustainability and Transformation Partnership (STP) has appointed Deborah Fielding as the full-time leader to continue the transformation of health and social care services across the area, and Dr Hari Pathmanathan has been appointed as the Joint Clinical Lead.
2.6 Good News
The Department of Health have congratulated the CCG for the improved 18 week referral to treatment performance in September 2017 (Appendix 2).
3. Issues
Not Applicable.
4. Options
Not Applicable.
5. Resources implications
There are none identified.
6. Risks/Mitigation Measures
Not Applicable.
7. Recommendations
The Governing Body is asked to note the report.
8. Next Steps
Not Applicable.

Appendix 1

Appendix 2
Page 1 of 5
Agenda Item No: 7
Date of Meeting: 18 January 2018
Governing Body Meeting in Public
Paper Title: Governance Report
Decision or Approval Discussion Information
Report author: Jas Dosanjh, Corporate Governance Manager
Report signed off by: Alan Pond, Chief Finance Officer
Linda Farrant, Lay Member Governance and Audit (Section 2.4)
Sharn Elton, Director of Operations (Section 2.5)
Executive Summary: This paper seeks the approval of the Governing Body to a number of matters, as required by the CCG’s Constitution, that have been agreed at Governing Body Workshops, including matters approved that require reporting to the Governing Body Meeting in Public for ratification.
This paper provides information on corporate governance activities being undertaken by the Clinical Commissioning Group (CCG).
Recommendations
to the members:
The Governing Body is asked to:
• Note and ratify the decisions made at the Governing Body
Workshops,
• Note the report from the Governance and Audit Committee,
• Note the CCG’s EPRR Core Standards Assurance rating
for 2017/18 as fully compliant.
Conflicts of Interest
involved:
There are none identified.

Page 2 of 5
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

Page 3 of 5
1. Executive Summary
This paper seeks the approval of the Governing Body to a number of matters, as required by the CCG’s Constitution, that have been agreed at Governing Body Workshops, including matters approved that require reporting to the Governing Body Meeting in Public for ratification.
2. Background
2.1 Introduction
This paper provides information on corporate governance activities being undertaken by the Clinical Commissioning Group (CCG).
2.2 Terms / Acronyms Used in the Report
CCG Clinical Commissioning Group NHS National Health Service
2.3 Governing Body Workshops
Summarised below are key discussions and actions agreed from the Governing Body Workshops:
2.3.1 07 December 2017
Ratification of the following policies as a result of the consultation outcome:
- IVF Policy,
- Fitness for Surgery (BMI and smoking) Policy,
- Over the Counter Medicines Policy,
- Gluten-Free Food Policy,
- Female Sterilisation Policy.
2.3.2 21 December 2017
Approval of the next steps for the Extended Access Programme, including sharing of the
service specification with Ephedra and Stevenage Health, amend Fair Processing Notice
for practices, and holding a workshop for Locality Federations.
2.3.3 04 January 2018
Approval of the recommendations from the Hertfordshire Medicines Management
Committee regarding mandatory NICE Technology Appraisal treatments,
Approval of the shared care protocol regarding Adult Mental Health Community Services
and the Hertfordshire Suicide Prevention Strategy.
The Governing Body is asked to note and ratify the decisions made at the Governing Body
Workshops.
Page 4 of 5
2.4 Governance and Audit Committee Meeting
The Minutes of the Governance and Audit Committee meeting of 15 November 2017, as approved at the 10 January 2018 meeting are being submitted to this meeting, as required by the Committee’s Terms of Reference. Items of business considered by the Committee at its January meeting included a review of the following:
Deep-dive into HBL ICT’s Data Security arrangements,
Quality Assurance Report and Minutes from the Quality Committee,
Finance Risks, including system-wide risks, Waivers of Standing Orders and the
Financial Accounts Timetable,
Month 9 Interim Governance Statement,
Progress report from Internal Audit and Interim Head of Internal Audit Opinion,
Progress report from External Audit, Plan and Fees,
IG Forum Six Monthly Report,
Legal Claims annual report and approval of the Claims Handling Policy and Procedure.
The Governing Body is asked to note the report and minutes from the Governance and Audit Committee.
2.5 Emergency Preparedness, Resilience and Response (EPRR)
2.5.1 EPRR Meeting Terms of Reference
The Terms of Reference for the internal EPRR Group were reviewed and approved at the
EPRR meeting that took place on 08 January 2018.
2.5.2 NHS Core Standards Submission 2017/18
The purpose of the national Core Standards process is to assure NHS England that the
CCG is meeting emergency planning duties both contractually and under the Civil
Contingencies Act (2004). Following the assurance meeting and review of the CCG’s
submission, NHS England have confirmed the CCG’s EPRR Core Standards Assurance
rating for 2017/18 as fully compliant (Appendix 1).
The Governing Body is asked to note the CCG’s EPRR Core Standards Assurance rating
for 2017/18 as fully compliant.
2.6 Governing Body Annual Cycle of Business 2017-18 Public and Private
The Annual Cycle of Business was received by the Governing Body in July 2017 and is
available from this link: http://www.enhertsccg.nhs.uk/governing-body-meetings-in-public
3. Issues
Not Applicable.

Page 5 of 5
4. Options
Not Applicable.
5. Resources implications
There are none identified.
6. Risks/Mitigation Measures
Not Applicable.
7. Recommendations
The Governing Body is asked to:
• Note and ratify the decisions made at the Governing Body Workshops,
• Note the report from the Governance and Audit Committee,
• Note the CCG’s EPRR Core Standards Assurance rating for 2017/18 as fully
compliant.
8. Next Steps
Not Applicable.

High quality care for all, now and for future generations
2 January 2018
Dear Sharn,
Re: EPRR Core Standards Assurance Meeting
Thank you for participating in the NHS Core Standards for EPRR Assurance meeting
held on 28th September 2017. The purpose of the assurance meeting was to discuss
your Core Standards submission in an open and facilitative forum, in order to set
priorities moving forward. The Core Standards Panel will then make recommendations to
the Local Health Resilience Partnership (LHRP) and in turn, the Local Resilience Forum
(LRF) in response to your submission.
The purpose of the national Core Standards process is to assure NHS England that you
are fulfilling your organisational, statutory responsibilities. It is a mandatory process by
which the panel seek assurance that you are compliant with each of the core standards
and that you are meeting your emergency planning duties both contractually and under
the Civil Contingencies Act (2004).
Core Standards
The CCG has provided a thorough and evidence-based submission and we are pleased
to acknowledge that you have self-assessed the CCG as fully compliant across all Core
Standards.
Cyber Malware Attack
You stated that lessons had been learned. The ICC was implemented very quickly and
Midlands & East (Central Midlands)
Central Midlands (South Locality)
Charter House
Parkway
Welwyn Garden City
Hertfordshire
AL8 6JL
Email: [email protected]
Tel: 0113 8248900
Sharn Elton
Director of Operations
East & North Herts CCG
Charter House
Parkway
Welwyn Garden City
Appendix 1
High quality care for all, now and for future generations
supported the CCGs coordination of the response. It was evident from the incident that
the IT providers had a lack of understanding of the impact of the incident on patients.
We understand a Hertfordshire wide debrief is to be held.
Governance Deepdive
Your self-assessment explains that the CCG has an internal EPPR meeting which is
chaired by the AEO. It was acknowledged that both attendance and contribution by the
CCG AEO at the LHRP is very good.
Summary
In your EPRR Core Standards self-assessment, you have rated your overall level of
compliance as fully compliant. Following the assurance meeting and review of your
submission, we agree with your EPRR Core Standards Assurance rating of: FULLY
COMPLIANT.
Yours sincerely,
Dominic Cox Prof Jim McManus
LHRP Co-Chair LHRP Co-Chair
Locality Director (South) Director of Public Health
Midlands and East (Central Midlands) Hertfordshire County Council

1
Agenda Item No: 8
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Finance Report Month 8 2017/18
Decision Discussion Information Follow up from last meeting
Report author: Sunday Adeniyi, Deputy Chief Finance Officer
Report signed off by:
Alan Pond, Chief Finance Officer
Executive Summary: This paper provides an update of the finance position as at the end of November 2017.
The CCG financial position as at Month 8 is an in-year surplus of £184k which is in addition to the cumulative brought forward plan. The CCG is forecasting to deliver an underspend of £14,498k, to meet the NHSE target control total.
Recommendations
to the members:
To note the Month 8 position.
Conflicts of Interest
involved:
There are no conflicts of interest
Conflict of Interest Definitions The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the consequences of a commissioning decision.
Non-Financial Professional Interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career.
Non-Financial Personal Interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit.
Indirect Interests This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision.
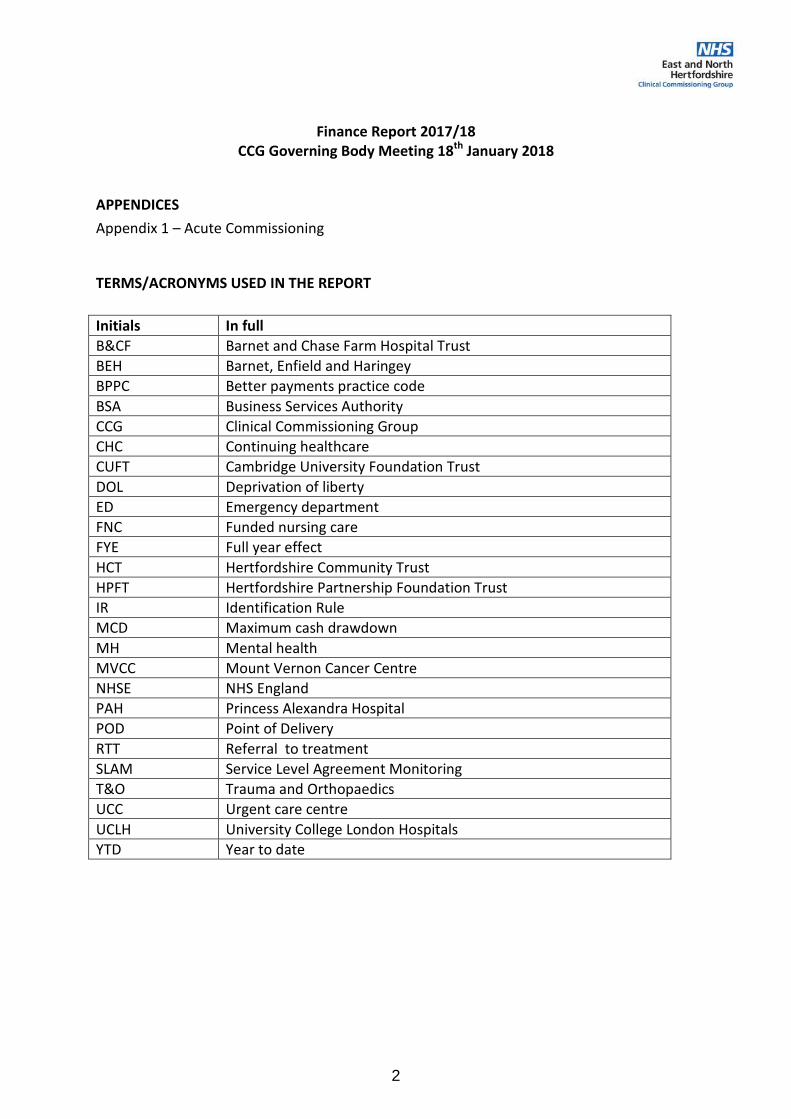
2
Finance Report 2017/18 CCG Governing Body Meeting 18th January 2018
APPENDICES
Appendix 1 – Acute Commissioning
TERMS/ACRONYMS USED IN THE REPORT
Initials In full
B&CF Barnet and Chase Farm Hospital Trust
BEH Barnet, Enfield and Haringey
BPPC Better payments practice code
BSA Business Services Authority
CCG Clinical Commissioning Group
CHC Continuing healthcare
CUFT Cambridge University Foundation Trust
DOL Deprivation of liberty
ED Emergency department
FNC Funded nursing care
FYE Full year effect
HCT Hertfordshire Community Trust
HPFT Hertfordshire Partnership Foundation Trust
IR Identification Rule
MCD Maximum cash drawdown
MH Mental health
MVCC Mount Vernon Cancer Centre
NHSE NHS England
PAH Princess Alexandra Hospital
POD Point of Delivery
RTT Referral to treatment
SLAM Service Level Agreement Monitoring
T&O Trauma and Orthopaedics
UCC Urgent care centre
UCLH University College London Hospitals
YTD Year to date

3
1. EXECUTIVE SUMMARY
The CCG is on line to achieve its planned surplus control total of £14.498m set out in its Financial Plan approved by the Governing Body and NHS England. This control total is the surplus brought forward from the previous year less £200k that the CCG has been allowed to spend of this in 2017/18.
The CCG’s financial position as at Month 8 is an in-year surplus of £184k which is in addition to the cumulative brought forward control total mentioned above.
Running costs for the CCG reported a YTD underspend of £458k and forecast to underspend by £645k on the budget set. The budget set is £1.2m lower than the running cost allocation received with this sum having been effectively transferred internally to fund healthcare services.
The QIPP position is the forecast delivery of £22.3m against a plan of £23.2m resulting in an under delivery of £0.91m – which equates to a delivery yield of 96% for the full year.
The CCG is also delivering the targeted BPPC performance. The target is to pay at least 95% of invoices within 30 days. Actual performance YTD is 99.5% for NHS and 99.1% for Non NHS.
The CCG is currently managing potential financial risks of £1.9m which may impact the delivery of the CCG’s target financial position if crystallised; however these risks are currently mitigated by contingency held by the CCG.
2. KEY PERFORMANCE INDICATORS - Month 8
No Indicator Name Plan Actual Variance YTD Plan Actual Variance Forecast
£'000 £'000
£'000
(UNDER)/
OVER Rating £'000 £'000
£'000
(UNDER)/
OVER Rating
1 Resource Limit vs Spend 489,678 489,678 0 739,853 739,853 0 Our allocation movement this month is £960k
2 Over/Under vs Control total 9,665 9,850 (184) 14,498 14,498 0The CCG is on track and is forecast to deliver
the control total agreed with NHSE
3Running Cost/Admin
(Compared to CCG allocation)8,473 7,207 (1,266) 12,709 10,853 (1,856)
The running cost budget is forecast to
underspend by £645k. The remainder of the
underspend of £1.211m was transferred to
fund programme budget
4 QIPP Performance 12,872 13,800 928 23,230 22,321 (908)The CCG is currently forecasting to deliver
96% of the annual QIPP plan.
5 Contingency Reserve Utilised - - 3,609 2,409 1,200
No contingency reserve has been used to
date, however, in order to deliver our
required position at the year end we have
brought in £1.2m into the forecast.
6National Resilience Reserve
(Available Funds)- - 3,575 3,575 0
BPPC-Number -NHS (%) 95.0% 97.3% 95.0% 95.0%
BPPC-Number -Non-NHS (%) 95.0% 98.5% 95.0% 95.0%
BPPC-Value - NHS (%) 95.0% 99.5% 95.0% 95.0%
BPPC-Value - Non-NHS (%) 95.0% 99.1% 95.0% 95.0%
KEY PERFORMANCE INDICATORS - MONTH 8
Year to Date Full Year Plan
Comment
7

4
3. CCG ALLOCATION & BUDGETS
The CCG allocation as at Month 8 is £739,853k. In Month 8 the CCG received new allocations totalling £46k. The most notable amounts being an additional £600k for Winter Resilience funding and a reduction of £896k for Overseas Visitor Charges.
4. CCG EXPENDITURE OVERVIEW – Month 8
At Month 8 the year to date position is a surplus of £184k against in-year plan; this is in addition to the cumulative brought forward underspend. We are underspent year to date, however, in order to achieve the required financial position at the year end we have brought into the forecast an underspend of £1.2m from the contingency reserve. A summary of the position is shown
below.
Month
£'000
Allocation brought forward 739,807
Winter Resilience Joint commissioning - Primary Care Medical 600
STP funding for MH and Diabetes posts (inc. MH clinical lead post) 71
Children & Young people IAPT Trainee staff support costs 60
Acute hospital urgent and emergency liaison mental health services 105
Acute - 62 Day Wait Tranche 2 Midlands and East 72
Vanguard NCM Q3-4 Local Evaluation funding 34
Charge Exempt Overseas Visitor (CEOV) Adjustment (896)
Total notified allocation 739,853
Description
Annual
budget
£'000
YTD
budget
£'000
YTD
Actual
£'000
YTD
Variance
£'000
(UNDER)/
OVER
FOT
FOT
Variance
£'000
(UNDER)/
OVER
Allocation 739,853 489,678 489,678 0 739,853 -
Budget Heading
Acute Commissioning 406,398 273,021 272,686 (335) 406,414 16
Non Acute Commissioning 193,805 129,165 129,840 675 195,334 1,529
GP Prescribed Drugs 80,316 53,771 54,416 645 81,400 1,084
Other Primary Care 23,645 15,248 14,538 (710) 22,861 (784)
Running Costs 11,498 7,665 7,207 (458) 10,853 (645)
Transformation reserve 3,575 0 0 (0) 3,575 0
Contingency reserve 3,609 0 0 0 2,409 (1,200)
Quality Premium 0 0 0 0 0
0 0
Resilience funding 2,509 1,141 1,141 (0) 2,509 0
Total in year position 725,355 480,012 479,828 (184) 725,355 (0)
TOTAL (UNDER)/OVER SPEND * 14,498 9,665 9,850 (184) 14,498 -
* Required Underspend:
Underspend brought forward from
2015/16 7,743
In-year underspend in 2016/17 6,955
Release of funds to CCG (200)
Control Total 14,498
POSITION AS AT 30TH NOVEMBER 2017

5
4.1 Locality Financial Performance
The locality positions for Month 8 are unvailable at this time. The quality and reliability of the SUS data is being reviewed, there are major concerns especially regarding East and North Herts Trust. Work is currently being undertaken to resolve these problems.
4.2. Programme Budget – Acute Commissioning
4.2.1 Financial Performance
Acute contracts reported a YTD underspend of £335k and is forecast to overspend by £16k (see table below). This reported financial position is based on Month 7 SLAM data. The acute QIPP savings for 2017-18 of £14m is shown separately because budget reductions due to QIPP have not yet been applied at individual provider level, with provider level budgets being based on the currently agreed contract values.
The non-allocation of QIPP by provider means that most providers are showing an underspend against plans, the QIPP needed to be offset against this. Spend in the independent sector continues to overspend, this is being offset by underspends in NHS providers where there has been a reduction in activity greater than the planned QIPP.
A contract update of some of the CCG key acute providers is as follows:
• East and North Hertfordshire NHS Trust
East and North Hertfordshire NHS Trust (ENHT) is showing an under spend of £8.466m against contract. When this underspend is compared against planned YTD QIPP savings of £4.84m, it is
Description
Annual
budget
£'000
YTD
budget
£'000
YTD
Actual
£'000
YTD
Variance
£'000
(UNDER)/
OVER
FOT
£'000
FOT
Variance
£'000
(UNDER)/
OVER
East and North Herts Trust 231,052 154,035 145,569 (8,466) 218,867 (12,185)
Princess Alexandra Hospital 60,197 40,131 38,176 (1,955) 57,438 (2,759)
Royal Free FT 26,814 17,876 17,070 (806) 25,605 (1,209)
Independent Sector 22,678 15,119 18,289 3,170 27,448 4,770
Cambridge University Hospitals 11,555 7,703 7,721 18 11,582 27
Other Acute 68,167 45,445 45,861 416 65,474 (2,693)
Planned Acute QIPP (14,065) (7,287) 7,287 14,065
TOTAL 406,398 273,021 272,686 (335) 406,414 16
COMMISSIONING - ACUTE
POSITION AS AT 30TH NOVEMBER 2017
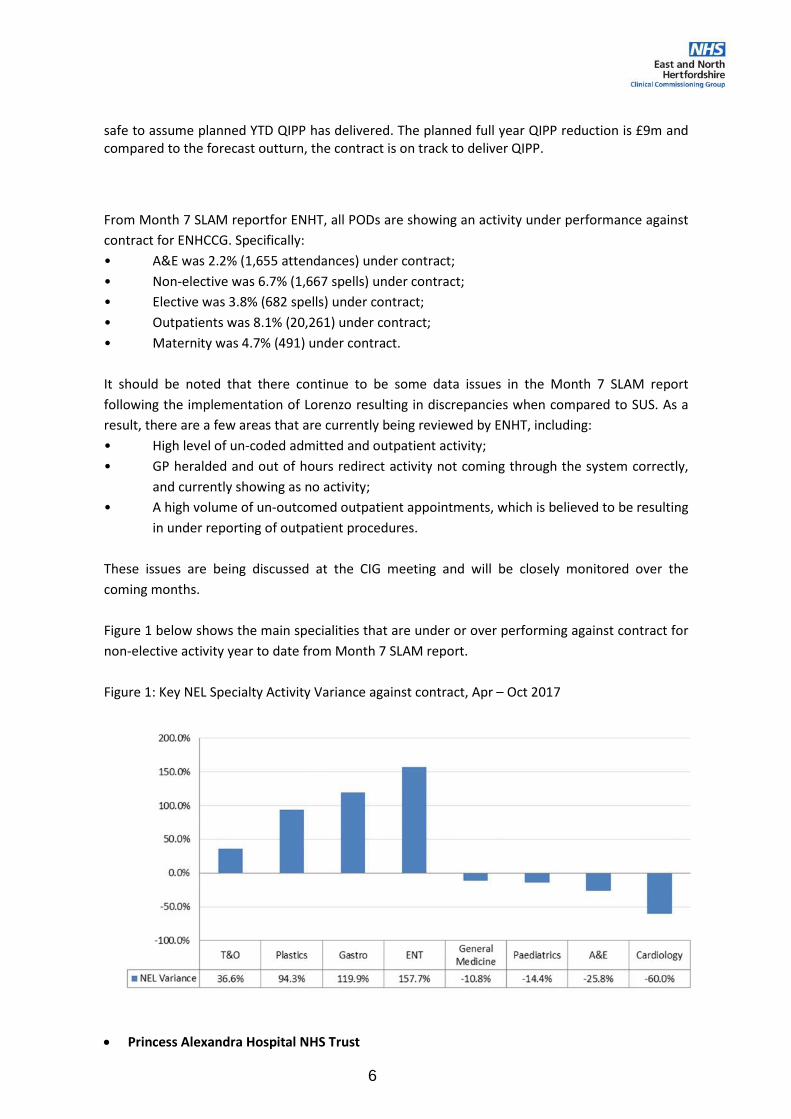
6
safe to assume planned YTD QIPP has delivered. The planned full year QIPP reduction is £9m and compared to the forecast outturn, the contract is on track to deliver QIPP.
From Month 7 SLAM reportfor ENHT, all PODs are showing an activity under performance against
contract for ENHCCG. Specifically:
• A&E was 2.2% (1,655 attendances) under contract;
• Non-elective was 6.7% (1,667 spells) under contract;
• Elective was 3.8% (682 spells) under contract;
• Outpatients was 8.1% (20,261) under contract;
• Maternity was 4.7% (491) under contract.
It should be noted that there continue to be some data issues in the Month 7 SLAM report
following the implementation of Lorenzo resulting in discrepancies when compared to SUS. As a
result, there are a few areas that are currently being reviewed by ENHT, including:
• High level of un-coded admitted and outpatient activity;
• GP heralded and out of hours redirect activity not coming through the system correctly,
and currently showing as no activity;
• A high volume of un-outcomed outpatient appointments, which is believed to be resulting
in under reporting of outpatient procedures.
These issues are being discussed at the CIG meeting and will be closely monitored over the
coming months.
Figure 1 below shows the main specialities that are under or over performing against contract for
non-elective activity year to date from Month 7 SLAM report.
Figure 1: Key NEL Specialty Activity Variance against contract, Apr – Oct 2017
• Princess Alexandra Hospital NHS Trust

7
The CCG’s position (based on the month 7 Flex report from PAH) shows expenditure of £38.2m,
an underspend of £1.96m compared to plan. This position includes reductions of £0.5m in respect
of high cost drug challenges, pass through payments, NHSE activity incorrectly assigned to the
CCG, emergency readmissions credit and penalties for same sex accommodation breaches. It also
includes a £170k adjustment for Maternity Antenatal pathways where PAH have assumed lead
provider status from month 7, however the CCG has not yet commissioned PAH to provide this
service. Work is on-going between the CCG, PAH and ENHT to agree the appropriate pathways
going forward.
From Month 7 SLAM report, the main areas of underperformance are Elective/Daycase activity
which remains £0.7m under contract at M7. This underperformance is partly due to a slow start
in activity in the first quarter of the year, as a result of closing an Orthopaedic ward due to
infection. The ward has since re-opened but is running with 6 beds less than prior to infection
issues. The CCG expects to see elective activity numbers increase to the contracted level during
the remainder of the year, PAH has confirmed they will not be delivering over contract.
Outpatients (First, Follow ups and Procedures) are also underspent by £0.7m, Non Elective activity
is underspent by £0.9m and A&E is under by £50k (488 attendances).
Forecast expenditure of £57.4m is £2.8m below the agreed SLA value. The forecast does not take
account of the new assessment beds opened during November to support flows though ED and
delivery of the 4hr ED target. Work is ongoing to agree how this activity should be counted,
coded and billed. The expectation is that for 2017/18 this capacity will be funded through the new
funds agreed for winter in the Government’s Budget. The forecast also excludes a new counting
and coding challenge recently raised with PAH relating to the increase in numbers of “unwell”
babies which attract an average charge of £900. The value of this for ENHCCG is £158k for
months 2-5, so the potential charge for 2017-18 is £0.4m.
The percentage of activity un-coded at Flex has improved on a monthly basis from 68% at the
start of the year to 30% at month 7, with all activity being coded by Freeze.
• Royal Free NHS Trust
The Trust is reporting a YTD underspend of £806k and forecast underspend of £1.21m compared to contract as at Month 8 however it should be noted that QIPP has yet to be deducted from the contract.
The main areas of underspend are day cases, £374k and £119k for inpatients totalling £493k. Outpatients are under contract by £460k which is broken down into first attendances £198k, Follow up visits £119k and OP procedures under by £211k. Non Elective is under by £301k, an increase if £39k on last month.
The main area of overspend is maternity case mix since the introduction of blood tests on the first appointment which has identified the need for intensive treatment before the patients are coded. Direct access is also over performing by £105k
• Independent Sector

8
Expenditure with contracted independent sector providers (Ramsay, BMI and Spire) is c£3.17m over contract at Month 8. Ramsay’s over-performance is mainly in inpatients; Pinehill and Rivers is significantly overperforming in outpatients.
4.2.2 CCG Activity Performance
The following charts show total CCG activity trend by point of delivery
Total outpatient YTD activity is lower than plan by 6.4% and also below for the same period in previous year. Since September 2017 activity appears to be on the increase although it is still under the CCG plan.
CCG YTD Elective activity is 1.8% below plan and higher than pervious year level by 1.1%. Activity was above plan in September and also in November but falls below plan in all the other months.
Total Outpatient
April May June July Aug Sep Oct Nov Dec Jan Feb Mar Total YTD
2015-16 46,013 42,999 50,719 51,808 44,289 51,837 51,461 50,608 44,453 45,015 42,212 43,216 564,630 389,734
2016-17 42,152 44,097 46,167 42,317 43,807 45,901 44,805 48,507 40,322 46,634 43,168 48,196 536,073 357,753
2017-18 38,272 44,531 45,686 43,549 43,414 40,311 44,992 45,714 346,469 346,469
2017-18 Plan 39,443 46,018 48,208 46,018 48,208 46,018 48,208 48,208 39,443 48,208 43,825 46,015 547,820 370,329
Variance (%) -3.0% -3.2% -5.2% -5.4% -9.9% -12.4% -6.7% -5.2% -6.4%
0
10,000
20,000
30,000
40,000
50,000
60,000
April May June July Aug Sep Oct Nov Dec Jan Feb Mar
Total Outpatient
2015-16
2016-17
2017-18
2017-18 Plan
Elective Activity
April May June July Aug Sep Oct Nov Dec Jan Feb Mar Total YTD
2015-16 4,961 4,898 5,337 5,543 4,581 5,174 5,416 5,303 4,602 5,162 5,259 5,191 61,427 41,213
2016-17 5,325 5,279 5,614 5,474 5,253 5,499 5,719 5,757 4,887 5,627 5,501 6,029 65,964 43,920
2017-18 4,850 5,567 5,549 5,279 5,644 5,852 5,709 5,937 44,387 44,387
2017-18 Plan 4,813 5,616 5,883 5,616 5,883 5,616 5,883 5,883 4,813 5,883 5,348 5,617 66,854 45,193
Variance (%) 0.8% -0.9% -5.7% -6.0% -4.1% 4.2% -3.0% 0.9% -1.8%
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
April May June July Aug Sep Oct Nov Dec Jan Feb Mar
No
of
Ad
mis
sio
ns
Elective Activity
2015-16
2016-17
2017-18
2017-18 Plan

9
YTD A&E activity is above plan by 1.0% and this has been the case all year apart from August and the November where activity is below plan.
YTD Non Elective admissions are above plan by 1.8% and have been all year apart from April. The CCG experienced significant increase in activity of 9.2% in November compared to plan.
A&E Activity
April May June July Aug Sep Oct Nov Dec Jan Feb Mar Total YTD
2015-16 15,008 15,941 16,437 17,740 16,940 16,459 16,976 17,024 16,395 16,714 16,489 18,411 200,534 132,525
2016-17 16,437 18,319 17,560 18,914 17,767 17,859 18,035 17,372 17,173 16,717 15,492 18,295 209,940 142,263
2017-18 17,201 18,364 18,251 18,240 16,979 17,313 17,844 17,155 141,347 141,347
2017-18 Plan 17,199 17,772 17,199 17,772 17,772 17,199 17,772 17,199 17,772 17,772 16,052 17,769 209,249 139,884
Variance (%) 0.0% 3.3% 6.1% 2.6% -4.5% 0.7% 0.4% -0.3% 1.0%
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000
April May June July Aug Sep Oct Nov Dec Jan Feb Mar
No
of
Att
en
dan
ces
A&E Activity
2015-16
2016-17
2017-18
2017-18 Plan
Non - Elective Activity
April May June July Aug Sep Oct Nov Dec Jan Feb Mar Total YTD
2015-16 4,702 4,640 4,626 4,955 4,526 4,386 4,606 4,346 4,575 4,428 4,210 4,529 54,529 36,787
2016-17 4,217 4,465 4,386 4,436 4,195 4,280 4,469 4,635 4,625 4,469 4,073 4,729 52,979 35,083
2017-18 4,233 4,551 4,537 4,398 4,487 4,255 4,263 4,478 35,202 35,202
2017-18 Plan 4,375 4,512 4,375 4,375 4,375 4,238 4,238 4,102 4,238 4,238 3,828 4,241 51,135 34,590
Variance (%) -3.2% 0.9% 3.7% 0.5% 2.6% 0.4% 0.6% 9.2% 1.8%
0
1,000
2,000
3,000
4,000
5,000
6,000
April May June July Aug Sep Oct Nov Dec Jan Feb Mar
No
of
Att
en
da
nce
s
Non-Elective Activity
2015-16
2016-17
2017-18
2017-18 Plan
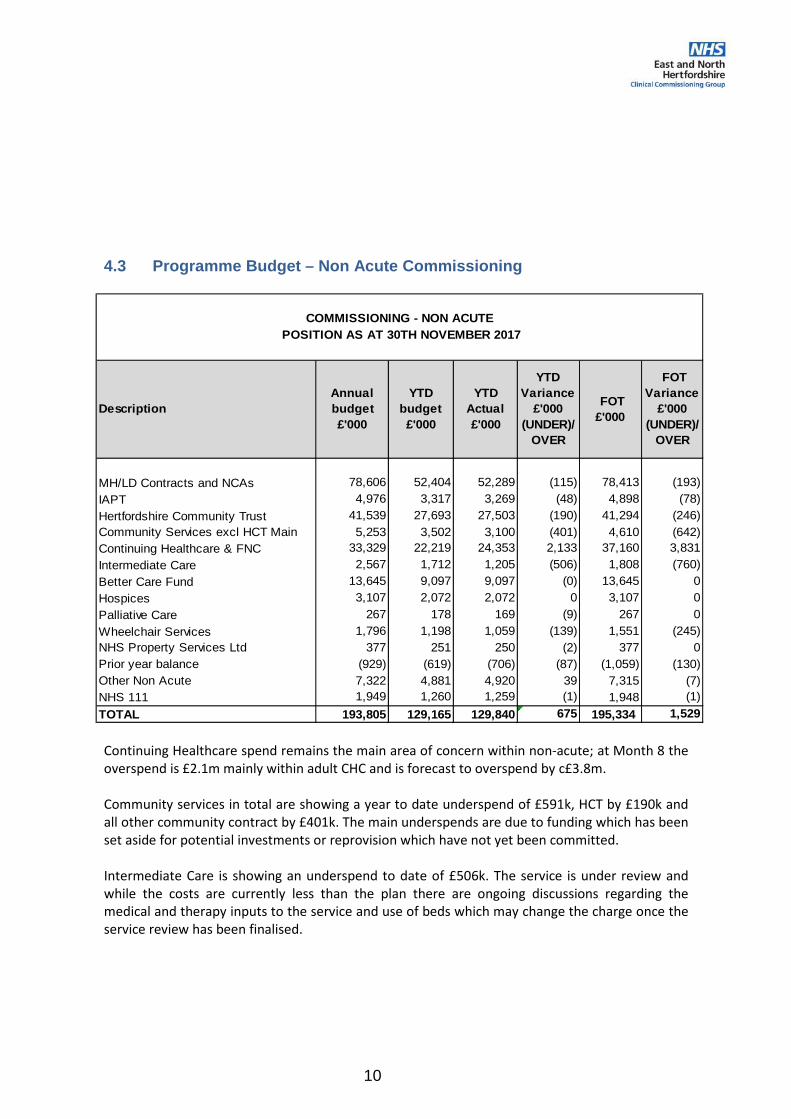
10
4.3 Programme Budget – Non Acute Commissioning
Continuing Healthcare spend remains the main area of concern within non-acute; at Month 8 the overspend is £2.1m mainly within adult CHC and is forecast to overspend by c£3.8m.
Community services in total are showing a year to date underspend of £591k, HCT by £190k and all other community contract by £401k. The main underspends are due to funding which has been set aside for potential investments or reprovision which have not yet been committed.
Intermediate Care is showing an underspend to date of £506k. The service is under review and while the costs are currently less than the plan there are ongoing discussions regarding the medical and therapy inputs to the service and use of beds which may change the charge once the service review has been finalised.
Description
Annual
budget
£'000
YTD
budget
£'000
YTD
Actual
£'000
YTD
Variance
£'000
(UNDER)/
OVER
FOT
£'000
FOT
Variance
£'000
(UNDER)/
OVER
MH/LD Contracts and NCAs 78,606 52,404 52,289 (115) 78,413 (193)
IAPT 4,976 3,317 3,269 (48) 4,898 (78)
Hertfordshire Community Trust 41,539 27,693 27,503 (190) 41,294 (246)
Community Services excl HCT Main 5,253 3,502 3,100 (401) 4,610 (642)
Continuing Healthcare & FNC 33,329 22,219 24,353 2,133 37,160 3,831
Intermediate Care 2,567 1,712 1,205 (506) 1,808 (760)
Better Care Fund 13,645 9,097 9,097 (0) 13,645 0
Hospices 3,107 2,072 2,072 0 3,107 0
Palliative Care 267 178 169 (9) 267 0
Wheelchair Services 1,796 1,198 1,059 (139) 1,551 (245)
NHS Property Services Ltd 377 251 250 (2) 377 0
Prior year balance (929) (619) (706) (87) (1,059) (130)
Other Non Acute 7,322 4,881 4,920 39 7,315 (7)
NHS 111 1,949 1,260 1,259 (1) 1,948 (1)
TOTAL 193,805 129,165 129,840 675 195,334 1,529
COMMISSIONING - NON ACUTE
POSITION AS AT 30TH NOVEMBER 2017

11
4.4 Programme Budget – Primary Care Commissioning
Prescribing costs are based on the April – September BSA drug reports. At Month 8 GP prescribing is £645k overspent with a forecast outturn position of £1084k overspent. The benefit of category M price reduction is not being passed to the CCG which may have effect on QIPP delivery resulting in an overspend on the prescribing budget. Also, CCG is experiencing cost pressure relating to No cheaper stock option (NCSO) drugs. It is noted there has been increase in the number of drugs added to the NCSO list since April 2017. The CCG have already included a YTD cost pressure of £1.4m in this finance report.
£1 per patient The budget is being phased to reflect the pattern of expenditure undertaken by the localities in that during the early part of the financial year plans are evolved and the costs for these are primarily incurred in the second half of the year. The YTD figures are based on actuals with a moderate general accrual of average spend.
Commissioning Framework The annual Budget reflects the 17/18 Components of the CFF at £10.10 per patient population (593k) and the Education & Development Component of 2016/17 which was agreed to be deferred until 2017/18 to reflect more realistic planning and implementation process. The balance carried forward from 16/17 was £929k was reflective of the different levels of spend and stage of implementation amongst localities at 31/03/17
Description
Annual
budget
£'000
YTD
budget
£'000
YTD
Actual
£'000
YTD
Variance
£'000
(UNDER)/
OVER
FOT
£'000
FOT
Variance
£'000
(UNDER)/
OVER
GP Prescribed Drugs 80,316 53,771 54,416 645 81,400 1,084
Central Drugs 2,636 1,765 1,476 (289) 2,206 (430)
Oxygen 834 558 420 (139) 627 (207)
Scriptswitch 196 131 126 (4) 189 (7)
Medicine Management Team 818 545 524 (21) 818 0
Local Enhanced Services 1,759 1,174 994 (180) 1,697 (62)
Primary Care IT 1,928 1,285 1,285 (0) 1,928 0
Out of Hours 5,322 3,480 3,476 (4) 5,317 (4)
Commissioning Framework 6,920 4,589 4,638 49 6,920 0
Acute in hours visiting service 1,647 1,089 1,015 (74) 1,573 (74)
£1 per patient 593 296 282 (14) 593 0
GP Forward View 992 335 301 (34) 992 (0)
TOTAL 103,961 69,019 68,954 (65) 104,260 300
COMMISSIONING - PRIMARY CARE

12
4.5 Corporate Running Costs
The CCG corporate running cost is reporting an underspend YTD of £458k and forecast underspend of £645k against the budget set.
The budget takes into account QIPP savings of £560k and is also £1.2m lower than the allocation actually received. The £1.2m has been added to healthcare budgets.
5. Quality, Innovation, Productivity and Performance (QIPP)
The CCG planned financial savings for 2017-18 is £23.23m and is currently forecast to deliver £22.32m (96%).
The table below shows the overall summary and status of QIPP programmes as at Month 8.
The CCG QIPP plan for 2017-18 is £23.23m out of which £7m can be evidenced to have fully delivered against Better Care Fund, Winter Resilience and Running costs having secured negotiated financial positions which are embedded within their respective budgets. The remaining £16m relates to demand management schemes and optimising the use of medicines.
Budget Actual VarianceAnnual
BudgetForecast Variance
£ £ £ £ £ £
Directors Office 1,169,704 1,064,337 (105,367) 1,754,368 1,605,966 (148,402)
Finance Directorate 3,331,762 3,169,385 (162,377) 4,998,234 4,769,537 (228,697)
Commissioning Directorate 754,585 722,290 (32,295) 1,131,803 1,086,317 (45,485)
Operations Directorate 945,614 919,092 (26,522) 1,418,373 1,381,019 (37,354)
Nursing Directorate 869,473 799,210 (70,262) 1,304,005 1,205,045 (98,960)
Medical Directorate 594,198 533,102 (61,096) 891,218 805,168 (86,050)
Total 7,665,335 7,207,417 (457,918) 11,498,000 10,853,052 (644,948)
Year To Date (£) Full Year (£)
East & North Hertfordshire CCG QIPP Programme 2017/18
Point of DeliveryQIPP Scheme
Description
YTD QIPP
Savings
Target
YTD Actual
QIPP
Achieved
YTD
Variance£ RAG
Annual
Planned
Savings
Forecast
Outturn
Savings
Forecast
Outturn
Variance
£ RAG
£ £ £ £ £ £
Accident & Emergency A&E avoidance schemes £2,220,793 £1,941,669 -£279,124 Amber £3,753,323 £3,321,014 -£432,309 Amber
Outpatient Demand management £1,072,111 £2,983,263 £1,911,152 Green £1,757,000 £4,373,511 £2,616,511 Green
Elective Demand management £1,740,831 £1,370,997 -£369,834 Amber £4,052,608 £2,806,949 -£1,245,659 Amber
Non Elective Demand management £1,498,846 £1,028,085 -£470,761 Green £3,702,603 £2,073,773 -£1,628,830 Red
Medicines Optimisation Prescribing savings £1,352,365 £1,492,166 £139,801 Green £2,444,000 £2,173,505 -£270,495 Amber
Continuing Healthcare Continuing Healthcare £306,667 £336,667 £30,000 Green £500,000 £590,000 £90,000 Green
Better Care Fund Better Care fund review £2,929,441 £2,929,441 £0 Green £4,394,162 £4,394,162 £0 Green
Winter Resilience Efficiency savings £1,110,667 £1,110,667 £0 Green £1,666,000 £1,666,000 £0 Green
Other Programmes e.g. Section 75 budget £266,667 £233,333 -£33,333 Amber £400,000 £362,500 -£37,500 Amber
Running Cost Running costs e.g. Staffing £373,333 £373,333 £0 Green £560,000 £560,000 £0 Green
Total £12,871,721 £13,799,620 £927,899 £23,229,696 £22,321,414 -£908,282

13
There is a risk of £0.9m QIPP under-delivery relating to QIPP schemes not yet agreed within contracts. Some of these schemes are reviewed regularly and the CCG has had to revise the level of expected financial savings due to decisions not to implement changes or where implementation is delayed which means the full year benefit cannot be realised in 2017-18 financial year.
For those QIPPs relating to demand management especially within the acute providers, it is difficult to evidence delivery at individual scheme level. However, a review of 8 months’ activity information from SUS shows a reduction in the level of demand and activity compared to contract which provides some evidence that QIPP schemes are delivering. From the latest activity data received, CCG Elective activity is 1.8% below plan, total Outpatient activity is 6.4% below plan, A&E attendances (excluding follow-ups) are above plan by 1.0% and Non-Elective activity is 1.8% above plan.
The CCG has put in place Governance arrangements for the agreement, approval, monitoring and delivery of QIPP schemes in order to manage this risk. There is the East and North Herts Transformation group which was formed to co-ordinate implementation, delivery and monitoring of identified QIPP/CIP schemes that impacts East and North Herts Trust which is the CCG’s main local provider.
6. KEY FINANCIAL RISKS/MITIGATION MEASURES
The CCG is currently managing potential risks of £1.9m which may impact the delivery of the CCG target financial position if crystallised.
a) QIPP under-delivery – There is a risk of £0.9m QIPP under-delivery relating to QIPP schemes not yet agreed within contracts.
b) Continuing Healthcare Current (CHC) Adult cases CHC expenditure has increased over the past 2 years and is being closely monitored in order to highlight any further pressure on this budget. Risk of further increase in expenditure is estimated at £500k (previously £150k) due to growth (in number and complexities) higher than currently forecast. The CCG is engaging with NHS England who is leading the CHC National Strategic Improvement Programme in a way which ensures better outcomes, better use of resources and financial efficiency.
c) Prescribing costs The recent result of the Community Pharmacy Medicine Margin review has resulted in a reduction in Category M (generic drugs) prices with benefits to accrue to CCGs. However, NHSE have released a policy paper to withhold any windfall savings from CCGs (estimated impact for the CCG c£1m). The impact of this retention means associated prescribing QIPP schemes may not deliver the full benefit for the CCG through reduced medicines expenditure. NHSE has indicated that this benefit will not be lost as a decision to release these savings to CCG will be made later in 2017/18. However, this release is may be dependent on CCGs meeting their individually agreed control totals and will likely me made too late to allow CCGs to invest any of this in 2017/18.
Also, the CCG has reported to NHS England on the risk of additional cost pressure relating to No cheaper stock option (NCSO) drugs which is impacting the prescribing budget. The breakdown of additional NCSO costs over Drug Tariff for April to November is as follows:

14
Cost pressure to September 2017 = £1,403,856 Forecast for October = £ 494,511 Forecast for November = £ 177,873 Total as at November 2017 = £2,076,240 It is noted that there has been increase in the number of drugs added to the NCSO list since April 2017. The CCG have already included the YTD £1.4m cost pressure to September 2017 (FOT £2.8m) in this report. The future risk to the CCG is the volatility around the monthly changes to the NCSO list which currently cannot be determined. The CCG currently assume a forecast broadly in line with current list however this may not be the case hence additional risk of £200k has been recognised. CCG have asked if NHSE will release increase allocation for the net increase in the cost of NCSO drugs to mitigate this risk.
d) Patient Transport Service (PTS) The CCG’s key provider of PTS is subject to a winding up order and liquidation so unable to continue to provide services. In the short term the CCG has had to make transitional arrangements with East of England Ambulance Service and it is likely that a revised contract will be at higher cost. These risks are currently estimated at £250k. This event has also impacted the ongoing procurement of PTS service.
e) System Wide Risks - Financial pressures facing other NHS partners leading to decision to protect their position rather than adopting system-wide position e.g. HCT holding vacancies, ENHT refusing clinical service changes. Loss of engagement with GP Practices could lead to reduction in their gatekeeping function to other NHS funded services.
These risks are currently mitigated by contingency held by the CCG.
7. BALANCE SHEET
7.1 Cash
The table below shows the total amount of cash utilised compared with the amount that would be expected if the annual amount, referred to as maximum cash drawdown (MCD) was spent equally throughout the year. The MCD is calculated as the CCG’s allocation adjusted for non-cash items (depreciation), the planned underspend, and the opening cash bank balance.
Cumulative
year
to Date
£ 000's
Cash Drawn from NHSE 437,200
Drugs recharges 54,087
Home oxygen recharges 422
Total cash drawings 491,710
Cash book position 880
Total cash utilised 492,590
Maximum cash annual drawdown 724,602
Cash Phasing
Equal 1/12ths 483,068
Disproportionate Usage 9,522
( ) indicates less cash drawn than expected)

15
This shows that we have drawn down c£9.5m more than 8/12 of the annual MCD. This is partly attributable to the payment of 16-17 year end creditors and also because the CCG is still paying providers on account based on contract values with the year to date underspends not yet recovered in cash terms.
7.2 Balance sheet as at 30th NOVEMBER 2017
The following table shows the movement in the balance sheet between the end of March 2017 and end of November 2017.
N.B: Debtors figures shown on the balance sheet included VAT adjustments which accounts for the difference In debtors figure shown in section 7.3.
Closing
balance 31
March 2017
Closing
balance
Nov 2017
YTD
movement£'000 £'000 £'000
Non-current Assets
Property, Plant & Equipment 2,855 2,475 (380)
Current Assets
Debtors 1,107 1,259 152
Pre-payments 4,719 16,432 11,713
Cash & Cash Equivalents 298 1 (298)
Total Assets 8,979 20,166 11,187
Current Liabilities
Trade & Other Payables: (46,834) (46,139) 695
Provisions (275) (275) 0
Total Current Liabilities (47,109) (46,414) 695
Total Assets Employed (38,130) (26,248) 11,882
Financed by Taxpayers’ Equity
General Fund 38,130 26,248 (11,882)
of which:
Cash drawings & top-slice (491,710)
Expenditure 479,828
Total Taxpayers’ Equity 38,130 26,248 (11,882)
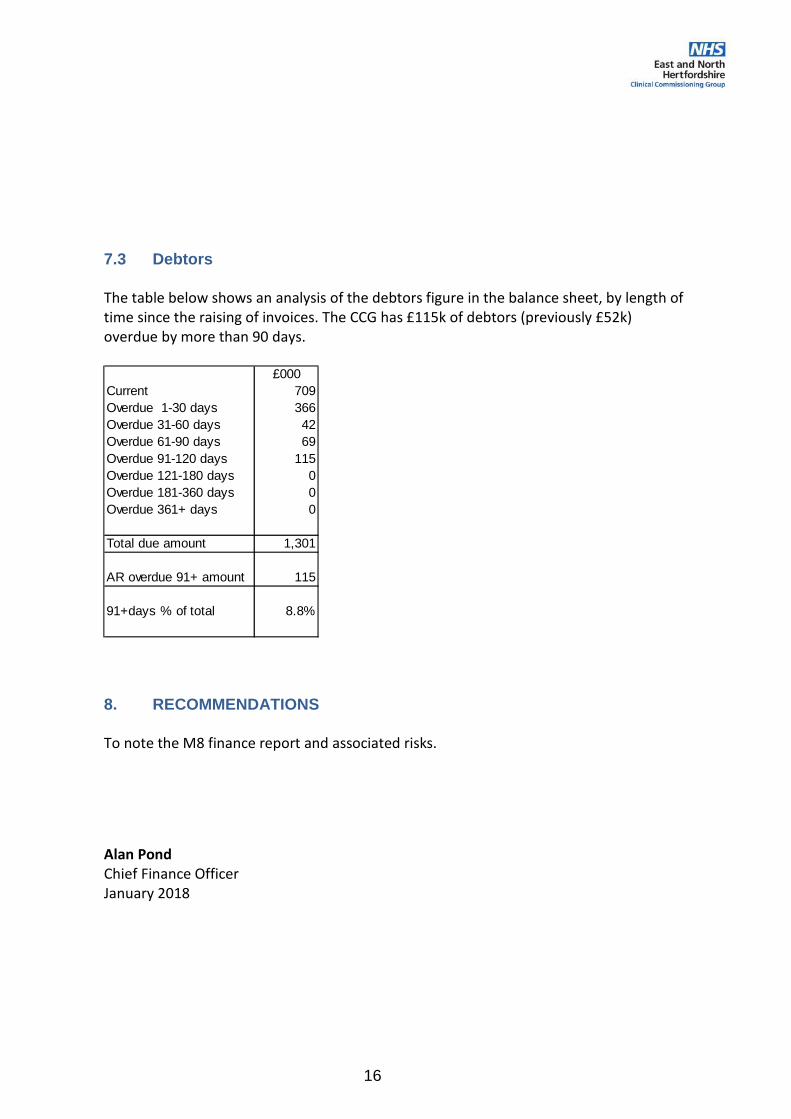
16
7.3 Debtors
The table below shows an analysis of the debtors figure in the balance sheet, by length of time since the raising of invoices. The CCG has £115k of debtors (previously £52k) overdue by more than 90 days.
8. RECOMMENDATIONS
To note the M8 finance report and associated risks.
Alan Pond Chief Finance Officer January 2018
£000
Current 709
Overdue 1-30 days 366
Overdue 31-60 days 42
Overdue 61-90 days 69
Overdue 91-120 days 115
Overdue 121-180 days 0
Overdue 181-360 days 0
Overdue 361+ days 0
Total due amount 1,301
AR overdue 91+ amount 115
91+days % of total 8.8%
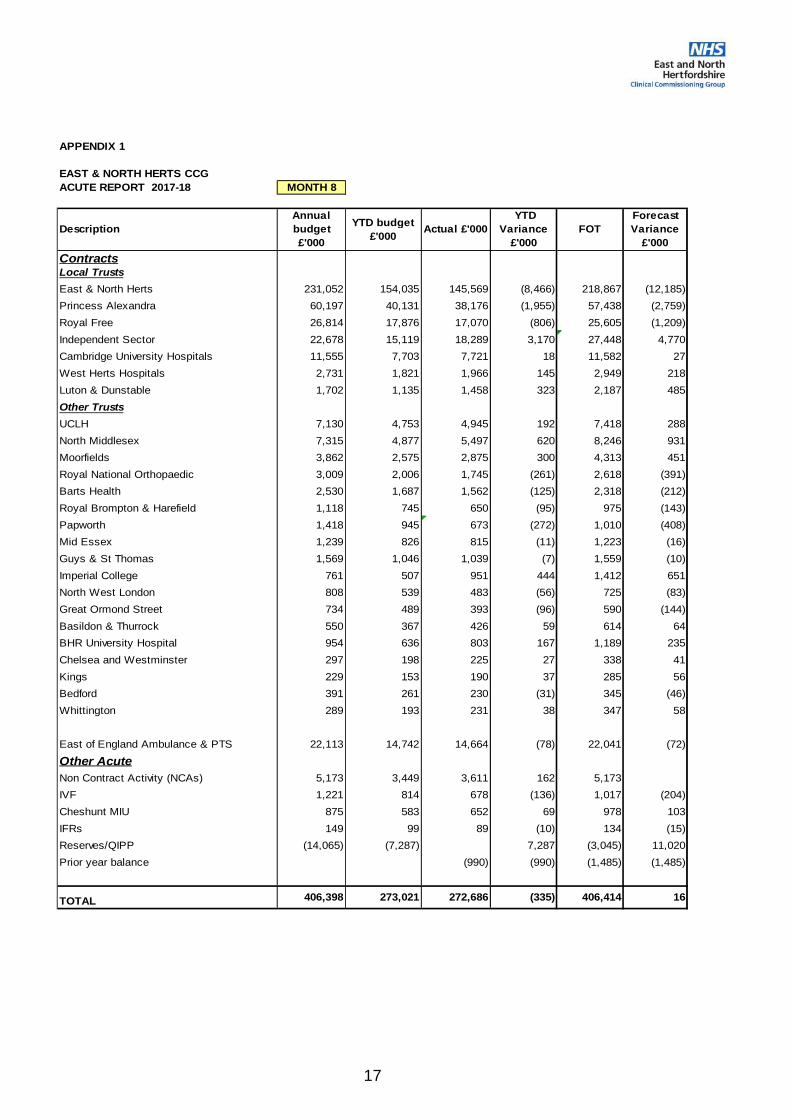
17
APPENDIX 1
EAST & NORTH HERTS CCG
ACUTE REPORT 2017-18 MONTH 8
Description
Annual
budget
£'000
YTD budget
£'000 Actual £'000
YTD
Variance
£'000
FOT
Forecast
Variance
£'000
ContractsLocal Trusts
East & North Herts 231,052 154,035 145,569 (8,466) 218,867 (12,185)
Princess Alexandra 60,197 40,131 38,176 (1,955) 57,438 (2,759)
Royal Free 26,814 17,876 17,070 (806) 25,605 (1,209)
Independent Sector 22,678 15,119 18,289 3,170 27,448 4,770
Cambridge University Hospitals 11,555 7,703 7,721 18 11,582 27
West Herts Hospitals 2,731 1,821 1,966 145 2,949 218
Luton & Dunstable 1,702 1,135 1,458 323 2,187 485
Other Trusts
UCLH 7,130 4,753 4,945 192 7,418 288
North Middlesex 7,315 4,877 5,497 620 8,246 931
Moorfields 3,862 2,575 2,875 300 4,313 451
Royal National Orthopaedic 3,009 2,006 1,745 (261) 2,618 (391)
Barts Health 2,530 1,687 1,562 (125) 2,318 (212)
Royal Brompton & Harefield 1,118 745 650 (95) 975 (143)
Papworth 1,418 945 673 (272) 1,010 (408)
Mid Essex 1,239 826 815 (11) 1,223 (16)
Guys & St Thomas 1,569 1,046 1,039 (7) 1,559 (10)
Imperial College 761 507 951 444 1,412 651
North West London 808 539 483 (56) 725 (83)
Great Ormond Street 734 489 393 (96) 590 (144)
Basildon & Thurrock 550 367 426 59 614 64
BHR University Hospital 954 636 803 167 1,189 235
Chelsea and Westminster 297 198 225 27 338 41
Kings 229 153 190 37 285 56
Bedford 391 261 230 (31) 345 (46)
Whittington 289 193 231 38 347 58
East of England Ambulance & PTS 22,113 14,742 14,664 (78) 22,041 (72)
Other Acute
Non Contract Activity (NCAs) 5,173 3,449 3,611 162 5,173
IVF 1,221 814 678 (136) 1,017 (204)
Cheshunt MIU 875 583 652 69 978 103
IFRs 149 99 89 (10) 134 (15)
Reserves/QIPP (14,065) (7,287) 7,287 (3,045) 11,020
Prior year balance (990) (990) (1,485) (1,485)
TOTAL 406,398 273,021 272,686 (335) 406,414 16

Page | 1
Agenda Item No: 9
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Medium Term Financial Outlook
Decision Discussion Information Follow up from last meeting
Report author: Sunday Adeniyi, Deputy Chief Finance Officer
Report signed off by: Alan Pond, Chief Finance Officer
Purpose of the paper: The paper provides an update regarding financial outlook of the
CCG for 2018/19 to 2020/21.
Recommendations
to the members:
Members are asked to note the financial outlook for 2018/19 to
2020/21 compared to 2017/18
Conflicts of Interest
involved:
none
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the consequences of a commissioning decision.
Non-Financial Professional Interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career.
Non-Financial Personal Interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit.
Indirect Interests This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision.
Page | 2
Governing Body Meeting 18th January 2018
CCG Financial Outlook for 2018/19 to 2020/21
1 Purpose of the Paper
This paper sets out the financial outlook for the next 3 years based on nationally and locally agreed planning assumptions, identifying the scale of the QIPP savings likely to be required each year and compares this to the current year.
2 Appendices
None
3 Terms / Acronyms Used in the Report
Initials In fullCCG Clinical Commissioning Group
CFF Consolidated Funding Framework CNST Clinical Negligence Scheme for Trusts ENHT East and North Hertfordshire Trust HCT Hertfordshire Community Trust HPFT Hertfordshire Partnership Foundation Trust HRG Healthcare Resource Group NEL Non Elective PAH Princess Alexandra Hospital QIPP Quality, Innovation, Productivity and Prevention.RTT Referral to treatment time SDIP Service Development and Improvement Plan
4 Latest Summary Position, as at January 2018
The annual NHS planning and contracting round has been streamlined significantly. The default was for two-year contracts to be agreed in place of those currently negotiated annually, and for there to be a two-year tariff, two-year CQUIN and CCG quality premium schemes. As a result, the CCG already have in place two year contracts for some of the main providers for 2017-18 and 2018-19. This Financial Outlook has updated the 2017-18 financial position and revised the future years to provide assurance of the financial sustainability of the CCG.
In addition Hertfordshire and West Essex STP has been working on STP wide financial planning bringing both the commissioner and providers together to identify the system gap and proffer STP wide solutions. As a result, the STP has issued a common planning guideline and assumptions which underpins this update to the Financial Outlook.

Page | 3
5 Allocations
The CCG published allocation for the planning horizon is as shown in the table below.
The annual growth in CCG allocation is shown in the planning assumptions table below which for 2018-19 is 2.8% or £20.178m. The following specific adjustments have been applied against the programme allocation in each of the planning year.
• A permanent allocation reduction was applied against the CCG baseline in respect of Market Rate adjustments being the net impact of moving NHS property services to market rate.
• In 2017/18 the national tariff for acute services was based on HRG4+. At the time of planning, NHSE were concerned that cost impacts at CCG level could vary widely and calculated what it thought the cost impact of HRG4+ would be. Where costs were expected to increase they allocated further funds and where costs were expected to decrease they took funds away. These calculations were based on 2014/15 activity and for ENHCCG the impact of the move to HRG4+ was seen to be a saving of £3,199k in 2017/18 and £3,251k in 2018/19. The CCG replicated the calculations using four months information from 2016/17 and demonstrated a cost increase of c£2m. NHSE has responded to the representations made by the CCG and as a result the allocation reduction has been amended to £520k in 2017/18 and £529k in 2018/19.
• The calculation of funding transfers between CCGs and specialised commissioning was also applied; the reductions are £5,683k and £5,772k in 2017/18 and 2018/19 respectively. It is assumed that these changes are cost neutral, with equivalent activity being chargeable to NHSE rather than the CCG.
CCG Allocation
2017-18 2018-19 2019-20 2020-21
£'000 £'000 £'000
Total recurrent 696,174 714,925 735,103 756,493
Growth 18,751 20,178 21,390 34,678
Running Cost 12,709 12,709 12,741 12,774
Market Rate Adjustment (466) (466) (466) (466)
Recurrent Allocation 727,168 747,346 768,768 803,479
Non Recurrent - IR remapping (5,683) (5,772) (5,862) (5,954)
Non Recurrent - HRG+remapping (520) (529) (538) (547)
Control total NR drawdown 200 0 0 0
In year NR allocation received @ M8 5,086 146 194 194
In year NR allocation reduction @ M8 (896) (900) (1,000) (1,100)
Non Recurrent Allocation (1,813) (7,056) (7,207) (7,408)
Total Allocation excluding b/f surplus 725,355 740,291 761,561 796,071
Control Total - Surplus 14,498 14,498 14,498 14,498

Page | 4
• Overseas Visitor allocation adjustment – The CCG was charged a Non Recurrent allocation reduction of £896k in respect of overseas visitors in 2017-18 and we have estimated a reduction of £900k for 2018-19 and estimate provided for future years.
• Spring House Non Recurrent allocation – In 2017-18, Spring House allocation has been released to the CCG as Recurrent allocation hence this is now part of the recurrent baseline in future years
• Non Recurrent allocation – All in-year non recurrent allocation and spend has been adjusted except the PMS Premium which for 2018-19 is estimated at £146k (£97k in 2017-18).
5.2 Running Costs Allocation
The running cost allocation growth for 2018-19 is £31k however a separate allocation reduction of 31k means that the running cost stays the same as it was in 2017-18 at £12,709k.
5.3 Control Total
The CCG’s cumulative surplus as at 31 March 2018 is planned to be £14,498k and this will be carried forward in future years as the agreed control total. This means that the CCG is expected to deliver an in-year breakeven financial position in order to ensure this control total is maintained.
5.4 Vanguard
NHS England is bringing the Vanguard programmes in its current pilot state to an end hence the non-recurrent financial allocation of £1.8m received in 2017-18 will not be made available in 2018-19. East and North Herts CCG have evaluated the various programmes and will continue to fund recurrently all of the programmes that have demonstrated net return on investment.
5.5 Primary Care Devolved Commissioning
In 2017-18, the CCG did not have devolved allocation from NHS England for Primary Care Commissioning. However, CCG members have recently voted in favour of devolved commissioning for 2018-19 and onwards. This Financial Outlook has not incorporated any financial flows in respect of devolved commissioning except a £500k estimated provision for additional resources that may be required to managed the new commissioning responsibility.
6. Financial Planning Assumptions
This Financial Outlook has been prepared in line with the planning guidance for the period to
2020/21: “Delivering the Forward View: NHS planning guidance”, published in December
2015, more recent guidance published by NHS England and NHS Improvement in
September 2016, (“NHS Operational Planning and Contracting Guidance 2017-2019”) and
planning assumptions agreed within the Hertfordshire and West Essex STP. The
assumptions are set out in the table below:
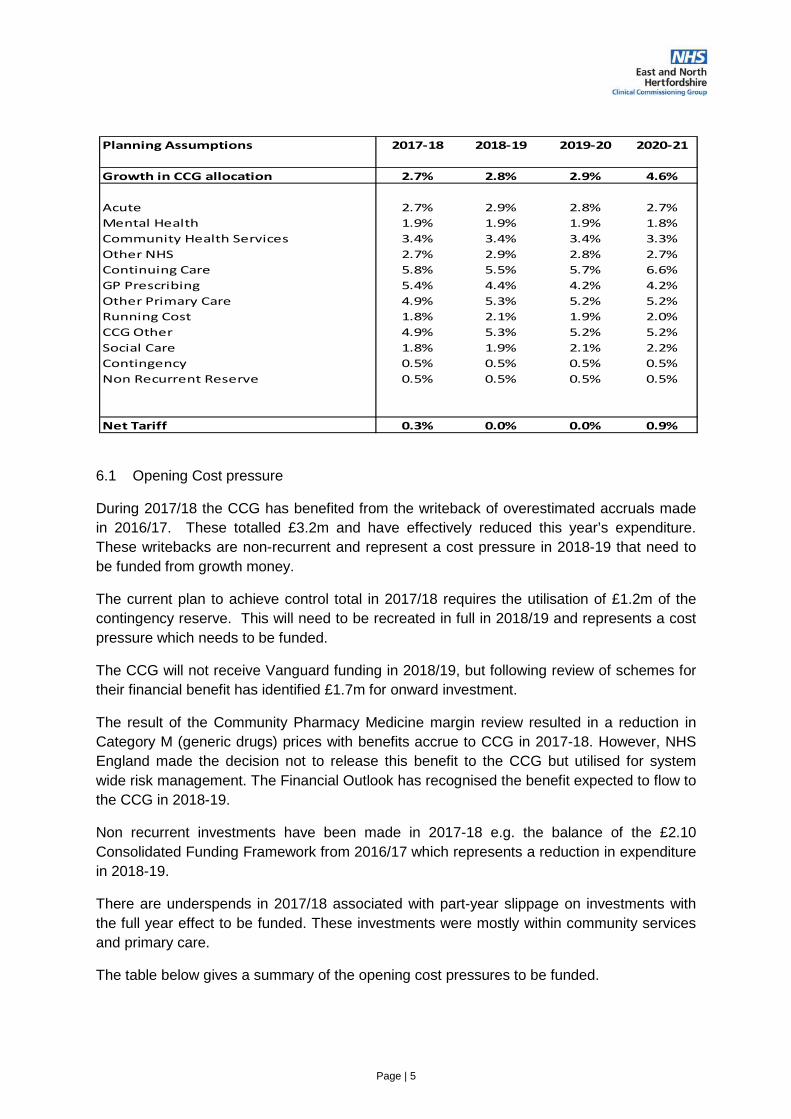
Page | 5
6.1 Opening Cost pressure
During 2017/18 the CCG has benefited from the writeback of overestimated accruals made
in 2016/17. These totalled £3.2m and have effectively reduced this year’s expenditure.
These writebacks are non-recurrent and represent a cost pressure in 2018-19 that need to
be funded from growth money.
The current plan to achieve control total in 2017/18 requires the utilisation of £1.2m of the
contingency reserve. This will need to be recreated in full in 2018/19 and represents a cost
pressure which needs to be funded.
The CCG will not receive Vanguard funding in 2018/19, but following review of schemes for
their financial benefit has identified £1.7m for onward investment.
The result of the Community Pharmacy Medicine margin review resulted in a reduction in
Category M (generic drugs) prices with benefits accrue to CCG in 2017-18. However, NHS
England made the decision not to release this benefit to the CCG but utilised for system
wide risk management. The Financial Outlook has recognised the benefit expected to flow to
the CCG in 2018-19.
Non recurrent investments have been made in 2017-18 e.g. the balance of the £2.10
Consolidated Funding Framework from 2016/17 which represents a reduction in expenditure
in 2018-19.
There are underspends in 2017/18 associated with part-year slippage on investments with
the full year effect to be funded. These investments were mostly within community services
and primary care.
The table below gives a summary of the opening cost pressures to be funded.
Planning Assumptions 2017-18 2018-19 2019-20 2020-21
Growth in CCG allocation 2.7% 2.8% 2.9% 4.6%
Acute 2.7% 2.9% 2.8% 2.7%
Mental Health 1.9% 1.9% 1.9% 1.8%
Community Health Services 3.4% 3.4% 3.4% 3.3%
Other NHS 2.7% 2.9% 2.8% 2.7%
Continuing Care 5.8% 5.5% 5.7% 6.6%
GP Prescribing 5.4% 4.4% 4.2% 4.2%
Other Primary Care 4.9% 5.3% 5.2% 5.2%
Running Cost 1.8% 2.1% 1.9% 2.0%
CCG Other 4.9% 5.3% 5.2% 5.2%
Social Care 1.8% 1.9% 2.1% 2.2%
Contingency 0.5% 0.5% 0.5% 0.5%
Non Recurrent Reserve 0.5% 0.5% 0.5% 0.5%
Net Tariff 0.3% 0.0% 0.0% 0.9%

Page | 6
6.2 Tariff
The draft tariff proposed adopts the design of HRG4+. The advised tariff is a cost inflation of
2.0% (on average across all Trusts including increases for CNST costs) and an efficiency
requirement of 2%, resulting in zero net tariff uplift for 2018-19 onwards until 2020-21 when
the net tariff increase is 0.9%.
6.3 Investments
The CCG Financial Outlook has made provisions for increased demographic and non-
demographic growths of £22.794m in 2018-19. Additional investments were provided in
acute to fund RTT activity, changes in case mix and potential coding and counting changes.
The CCG is planning to increase Mental Health funding in line with increase in allocation to
ensure it meets the Mental Health Parity of Esteem requirements.
The table below gives a summary increased demand/additional investments.
Cost Presure Funded
2017-18 2018-19
Acute Services Prior year benefit 3,008 1,485
Non Acute services prior year 3,614 1,059
CHC Retrospective/prior year benefit (1,066) 650
Contingency Reserve used recurrently 3,580 1,200
Vanguard schemes 1,669
Consolidated Funding Framework (£2.10) (1,107)
Cat M Prescribing benefit (1,200)
Addback of in year underspend 1,717
Total 9,136 5,473
Increased Demand/Additional Investment
2017-18 2018-19
Tariff Changes/inflation 5,608 0
Demographic & Non Demographic change 22,970 22,793
Investments - Acute 0 4,019
Investment - Mental Health 0 760
Investment - Corporate - Devolved Comm. 0 500
Other recurrent investments 3,912 379
Primary Care £1.50 per head year 2 875 0
Investment Costs funded non recurrently 2,900 0
Total 36,265 28,451

Page | 7
The funding position showing the source and use of funds described above is summarised in the table below.
From the above table, the CCG has a financial gap of £13.968m in order to deliver the
agreed control total. This gap will be managed through the development of QIPP schemes.
7 Quality, Innovation, Productivity and Performance (QIPP)
In developing this Financial Outlook, East and North Hertfordshire CCG recognised that the
delivery of the financial challenge is closely intertwined with the delivery of the
Sources and Application of Funds
2017-18 2018-19
Growth 18,751 20,178
Running Cost 71 31
Release of 0.5% transformation 3,575
Control total draw down 200 (200)
Market rate adjustment (425)
Increase in HRG+IR remapping (98)
Estimate increase in overseas visitor (4)
Increase allocation - PMS premium 49
Total 22,172 19,956
Application of Funds
Underlying Position 9,136 5,473
Tariff Changes/inflation 5,608
Demographic & Non Demographic change 22,970 22,793
Investments - Acute 4,019
Investment - Mental Health 760
Investment - Corporate - Devolved Comm. 500
Other recurrent investments 3,912 379
Primary Care £1.50 per head year 2 875
Investment Costs funded non recurrently 2,900
Total 45,401 33,923
Shortfall = savings required (23,230) (13,968)

Page | 8
commissioning challenge. Some of the commissioning challenge being addressed by the
CCG strategic plan includes:
• The challenge in efficient use of financial resources, management resources, sound risk
management and sound governance arrangements
• Inter-practice collaboration working to reduce referrals to secondary services by using
expertise currently residing within general practice, community and voluntary services,
and specialist services commissioned in a community setting
• Working with constituent practices to change clinical and patient activity and health
behaviours to make the best use of available resources.
• Involving patients in commissioning decisions affecting their care
• Working with Community Services, Local authority, Public Health and other sectors, to
identify those at risk of admission to hospital and provide integrated services to cater for
them.
• Continuing the strong performance management of commissioned services to ensure
that the needs of the population that we serve are met
In order to achieve the agreed control total for each year in the planning horizon, the CCG
will need to deliver recurrently the level of QIPP shown in the table below.
The main areas of savings identified from full year effect of previous years QIPP and new
schemes identified are listed below:
• Scaling up of the Early Intervention Vehicle scheme
• Shared Decision making for surgery intervention
• Primary Care variation in outpatient referrals and outcomes
• Circulation – Cardiology
• Biosimilar
• Contract efficiencies e.g. wheelchair service
• Targeted PMOT support to practices and implementation of HMMC guidance
• Anti-coagulation
• Medicines optimisation schemes
QIPP Requirements
2017-18 2018-19 2019-20 2020-21
Acute Services 20,178 11,743
Prescribed drugs 1,982 860
Community Services 500 382
Running Costs 570 250
Primary Care 357
Other transformation programmes 376
QIPP Savings 23,230 13,968 5,532 4,771
Page | 9
8.0 Financial Risks and Opportunities
The Financial Outlook has not included the potential impact of the following risks over the
planning horizon.
• Political Influences – change in general economic outlook may lead Government to seek
further efficiencies from the NHS.
• Policy drive to identify significant unmet healthcare needs
• Significant changes in activity levels resulting in overspend on healthcare contracts
(normal activity growth was provided for in the plan). There is always risk of growth in
Continuing Healthcare and Prescribing thereby leading to unavoidable spend.
• Unavoidable non-recurrent slippage on QIPP schemes
• Unavoidable pressures resulting from national policy that result in significant financial
expenditure
The CCG has in place robust financial framework to enable it respond to these risks should
they materialise.
9 Summarised Financial position
East and North Hertfordshire CCG has a strong underlying financial performance and is
currently forecasting to deliver the planned surplus for 2017/18 of £14.498m. The Financial
Outlook is based on continuing to deliver a target surplus of £14.498m in each of the future
years. Within the Financial Outlook, the CCG has set aside a 0.5% non-recurrent reserve
and a 0.5% contingency reserve to mitigate future financial pressures.
In order to deliver the financial position, the CCG will need to deliver recurrently QIPP
efficiencies of £14m in 2018/19 and a further £5-6m in each of 2019/20 and 2020/21. This
compares to the requirement for £23m in 2017/18.
After building in the savings required to budgets, the overall position is as shown in the table below.

Page | 10
11.0 Recommendations
The Governing Board is asked to:
Note the Financial Outlook for the CCG and the likely future savings that will be required in
order for the CCG to meet its financial control total.
Alan Pond Chief Finance Officer January 2017
2017-18 2018-19 2019-20 2020-21
£'000 £'000 £'000
Total recurrent 696,174 714,925 735,103 756,493
Growth 18,751 20,178 21,390 34,678
Running Cost 12,678 12,709 12,741 12,774
Market Rate Adjustment (466) (466) (466) (466)
Recurrent Allocation 727,137 747,346 768,768 803,479
Non Recurrent - IR remapping (5,683) (5,772) (5,862) (5,954)
Non Recurrent - HRG+remapping (520) (529) (538) (547)
Control total NR drawdown 200 0 0 0
In year NR allocation received @ M8 5,117 146 194 194
In year NR allocation reduction @ M8 (896) (900) (1,000) (1,100)
Non Recurrent Allocation (1,782) (7,056) (7,207) (7,408)
Total Allocation excluding b/f surplus 725,355 740,291 761,561 796,071
Planned Budgets
£'000 £'000 £'000 £'000
Acute Services 406,414 412,027 423,285 440,477
Mental Health Services 83,311 85,109 87,588 92,668
Community Services 54,354 59,280 61,317 64,902
Better Care Fund 13,645 13,904 14,386 14,880
Continuing Care Services 37,160 39,869 42,098 45,251
Prescribing 85,240 86,859 89,609 93,282
Other Primary Care Services 18,989 18,368 17,907 18,593
Other Programme Services 6,865 3,681 3,681 3,681
Running Cost 10,884 12,013 12,246 12,495
Non Recurrent Reserve (0.5%) 3,575 3,642 3,749 3,922
Contingency (0.5%) 2,409 3,706 3,813 3,986
Winter Resilience funding 2,509 1,833 1,884 1,936
Total Spend 725,355 740,291 761,561 796,071
Control Total - Surplus 14,498 14,498 14,498 14,498

Page | 1
Agenda Item No: 10
Date of Meeting: 18 January 2018
Governing Body Meeting in Public
Paper Title: East and North Herts Clinical Commissioning Group (ENHCCG) workforce equality & diversity report.
Decision or Approval Discussion Information
Report author: Paul Curry - Equality and Diversity Lead
Report signed off by:
Louise Thomas
Assistant Director of HR & ODL
Executive Summary:
This is the 2017 East and North Herts Clinical Commissioning Group (ENHCCG) workforce equality & diversity report.
The data presented in this report is produced in order to comply with one of the data publication requirements of the Equality Act 2010, which states that annual workforce data should be published by 21 January each year.
This report considers the findings of the annual workforce data analysis and recommends items for further consideration by the CCG and the Workforce and ODL Shared Service.
Recommendations
to the members:
It is recommended that the contents and findings of the
report are noted.
It is recommended that the CCG and the HR and ODL
Shared Service consider ways of addressing the falling
proportion of BME appointees by looking to identify any
reasons for the change in the level of BME recruitment
and consider career development opportunities within the
CCG for BME staff to support retention. The CCG may
also consider routes to promotion and work life balance for
female employees and the retention of staff aged 20-39.
It is recommended that work is undertaken to reduce the
number of employees not declaring their equalities status
in some categories. This will help to produce better
quality data across all categories of the equalities
monitoring framework.

Page | 2
Conflicts of Interest
involved:
No potential conflicts of interest identified
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.
1. Executive Summary
1.1 This is the 2017 East and North Herts Clinical Commissioning Group (ENHCCG) workforce equality & diversity report.
1.2 The data presented in this report (Appendix A) is produced in order to comply with one of the data publication requirements of the Equality Act 2010, which states that annual workforce data should be published by 21 January each year.
1.3 This report considers the findings of the annual workforce data analysis and makes recommendations for further consideration by the CCG and the Workforce and ODL Shared Service.
2. Background
2.1 ENHCCG has a duty to publish a range of equality and workforce data; some of which is published in the annual report under the equalities section. Other related reports including; Workforce Race Equality Standard report, Gender Pay Gap report and the NHS Equality Delivery System (EDS2) will also be published by April 2018.
2.2 To help meet the requirements of the data publication and target setting requirements of the Equality Act 2010, a Diversity and Equality Strategy and action plan will be produced based on the findings from the different reports.

Page | 3
This will include an overview of equality and diversity, along with the system wide impact of policies and practices.
2.3 The findings will be benchmarked against the local workforce or population data available from Hertfordshire County Council to help provide some useful indicators in comparison with the local population.

Page | 4
3. Data Analysis
3.1 This data refers to the period 1st November 2016 to 31st October 2017. During this period the total number of employees was 308, approximately 7% less than in 2016.
3.2 Overall, the workforce data for ENHCCG is in line with other CCGs (see latest NHS England National Survey 2013)1 and reflects the local working age population. However, a notable exception is the low number of employees with disabilities.
3.3 A few interesting indicators are:
• With the exception of the ‘Marital Status’ category, all other equalities protected characteristics have slightly increased the levels of undeclared data.
• Approximately 36% of employees are not declaring a religion or belief. However, there has been a slight increase in the number of employees declared as Hindu and other religion/belief
• Generally there is a balance between the genders across the pay grades. However, female employees tend to be disproportionally over represented in Bands 2-8a and male employees over represented at Bands 8b- Non AfC. Staff on non-AfC grades refers to very senior managers and those on ad hoc salary grades: this group would include clinical leads
• With the exception of the ‘Marital Status’ category, all other equalities protected characteristics have slightly increased the levels of undeclared data.
• There was an increase in the number of employees under 20 years of age, a decrease in employees aged 20-39 and an increase in all other age groups above this age.
• Female employees are twice as likely to work part-time (35% of female employees compared to 17% of male employees). This is a decrease in female part-time working and an increase in male part-time working over the previous year.
• White employees and female employees were more likely to give “end of fixed term contract” and “work life balance” as reasons for leaving. BME employees were more likely to leave for reasons of “promotion” or “better reward package”.
• Employees within the 20 – 39 age range gave “end of fixed term contract”, “promotion” or “better reward package” as the main reasons for leaving. This could be an indicator of retention issues. For the 40-49 age group the two main reasons for leaving were “promotion” and “work life balance”. For the
1. 1 https://www.england.nhs.uk/wp-content/uploads/2013/12/nationaled_surveys_V8-
2013-12-06.pdf

Page | 5
50-65 age group “end of fixed term contract” and “employee transfer” were the main reasons for leaving.
4. Workforce Race Equality Standard (WRES)
4.1 The NHS Workforce Race Equality Standard (WRES) has been developed as a tool for measuring improvements in the recruitment and employment experience of BME staff. It is an NHS initiative that was developed by the national NHS Equality & Diversity Council in collaboration with NHS staff and independent researchers.
4.2 The aim is to ensure BME staff are treated fairly and their talents valued and developed.
4.3 The WRES CCG Technical Guidance states:
“CCGs are required to have “due regard” to the WRES in respect of their own workforce. It is recognised that the small size of many CCGs means that a literal application and interpretation of the indicators should be approached with caution”. “CCGs should pay due regard to the WRES both as an indication they are complying with their Public Sector Equality Duty and in order to demonstrate that as commissioners they also take the intent of the WRES seriously.”
4.4 From July 2016 CCGs are required to publish an annual WRES report and an action plan. This should include results from the Staff Survey, which give a clearer picture of what it is like to work for the organisation. The staff survey results are likely to be available in February 2018 and a separate WRES report will be produced in March 2018.
4.5 In relation to performance as an employer, a key indicator from the WRES is the relative likelihood of a BME applicant being appointed once shortlisted. In 2017 49 people were appointed to the CCG. In 2017 a White applicant was three times more likely to be appointed once shortlisted than a BME applicant.
4.6 This a change from 2016 when there was no significant difference in the
likelihood of being appointed between White and BME staff; based on 100 staff
appointed in 2016 (twice as many appointees as in 2017).
4.7 There has been a significant change in the proportion of BME appointees in the
last two years. In 2015-16 40% of appointees were from a BME background and
that has dropped to 22% of BME appointees in 2016-17
4.8 This indicates that the change in the relative likelihood of appointment score is
supported by other data.
4.8 Using the same type of comparison we can show that the proportion of
appointments of employees with disabilities has increased from 2% to 6%.
Page | 6
5. Recommendations
5.1 It is recommended that the contents and findings of the report are noted.
5.2 It is recommended that the CCG and the HR and ODL Shared Service consider ways of addressing the falling proportion of BME appointees by looking to identify any reasons for the change in the level of BME recruitment and consider career development opportunities within the CCG for BME staff to support retention. The CCG may also consider routes to promotion and work life balance for female employees and the retention of staff aged 20-39.
5.3 It is recommended that work is undertaken to reduce the number of employees not declaring their equalities status in some categories. This will help to produce better quality data across all categories of the equalities monitoring framework.

Page | 7
APPENDIX A
Workforce Information Analysis – East and North Herts CCG
Equality & Diversity Report 2017
Report Author: Paul Curry
Author Job Title: Equality and Diversity Lead
Supported by: Selina Jassal, Workforce Information Manager
December 2017

Page | 8
Table of Contents
SECTION 1 INTRODUCTION
1.1 Introduction
SECTION 2 ORGANISATIONAL PROFILE
2.1 Gender2.2 Disability2.3 Ethnic Origin2.4 Age2.5 Religion / Belief2.6 Sexual Orientation2.7 Marital Status2.8 Maternity2.9 Leavers
SECTION 3 PAY GRADE COMPARISONS
3.1 Gender
3.2 Ethnicity
3.3 Disability
SECTION 4 RECRUITMENT & SELECTION
4.1 Recruitment & Selection
SECTION 5 TRAINING & DEVELOPMENT
5.1 Training & Development
APPENDIX 1 – Workforce Data Overview
APPENDIX 2 – Leavers Overview
APPENDIX 3 – Leaving Reasons – Protected Characteristics

Page | 9
1.1 Introduction
This report provides East & North Herts Clinical Commissioning Group (ENHCCG) workforce data Equality & Diversity Report.
This is produced in order to comply with some of the data publication requirements of the Equality Act 2010.
Where data is available, comparison has been made between:
• Workforce data from 2015 and 2016
• Local demographics primarily sourced from the 2011 Census.
We refer to this report as the 2017 report as it covers the year from 1 November 2016 - 31 October 2017. The 2016 report covered the period 1 November 2015 – 31 October 2016.
Section 2 outlines the organisational profile as at 31 October 2017.
Section 2 – Organisational Profile
2.1 Gender
Pay Band 2016 2017
Male (%) Female (%) Overall Workforce (%)
Male (%) Female (%) Overall Workforce (%)
Band 2 1.59 - 0.61 - - -
Band 3 0.79 1.96 1.52 0.88 2.56 1.95
Band 4 13.49 14.22 13.94 14.16 13.85 13.96
Band 5 17.46 13.24 14.85 15.04 10.77 12.34
Band 6 19.84 17.16 18.18 16.81 16.41 16.56
Band 7 13.49 20.10 17.58 15.04 21.54 19.16
Band 8a 10.32 11.27 10.91 7.08 11.28 9.74
Band 8b 6.35 7.35 6.97 9.73 7.18 8.12
Band 8c 4.76 4.41 4.55 5.31 4.10 4.55
Band 8d 2.38 3.92 3.33 3.54 4.10 3.90
Band 9 0.79 - 0.30 0.88 - 0.32
Non-AfC 7.14 4.41 5.45 9.73 6.15 7.47
VSM 1.59 1.96 1.82 1.77 2.05 1.95
Table 1 – Gender Pay Comparison
2.2 Disability
Disability Status 2015 Workforce Profile (%)
2016 Workforce Profile (%)
2017 Workforce Profile (%)
Local Demographic (%)
Yes 4.33 3.94 4.22 14.6
No 90.00 89.70 89.29 85.4
Undeclared 5.67 6.36 6.49
Table 2 – Disability Profile Comparison

Page | 10
2.3 Ethnic Origin
Table 3 – Ethnic Origin Comparison
2.4 Age
Table 4 – Age Profile
2.5 Religion / Belief
Religion / Belief 2015 Workforce Profile (%)
2016 Workforce Profile (%)
2017 Workforce Profile (%)
Local Demographic (%)
Atheism 11.00 13.03 12.99 28.61
Christianity 41.33 37.58 36.04 59.48
Hinduism 3.00 3.03 3.57 Not available
Islam 2.67 3.03 2.60 1.70
Other 8.00 6.36 9.09 3.10
Undeclared 32.67 35.15 35.71 7.11
Table 5 – Religion / Belief Comparison
2.6 Sexual Orientation
Sexual Orientation 2015 Workforce Profile (%)
2016 Workforce Profile (%)
2017 Workforce Profile (%)
Local Demographic (%)
LBG 1.00 1.21 0.97 Not available
Heterosexual 72.33 70 69.66 Not available
Undeclared 26.67 28.79 29.55 Not available
Table 6 – Sexual Orientation
Ethnic Origin 2015 Workforce Profile (%)
2016 Workforce Profile (%)
2017 Workforce Profile (%)
Local Demographic (%)
White 75.67 74.24 73.38 83.33
BME 22.33 23.33 20.78 16.67
Other - - 2.60
Undeclared 2.00 2.42 3.25
Age Band 2015 Workforce Profile (%)
2016 Workforce Profile (%)
2017 Workforce Profile (%)
Local Demographic (%)
Under 20 - 0.61 0.65 Not available
20-39 34.67 38.48 31.49 25.34
40-49 30.00 28.79 32.79 15.23
50-65 34.67 31.52 33.77 17.87
65+ 0.67 0.61 1.30 18.81
Undeclared - - - -
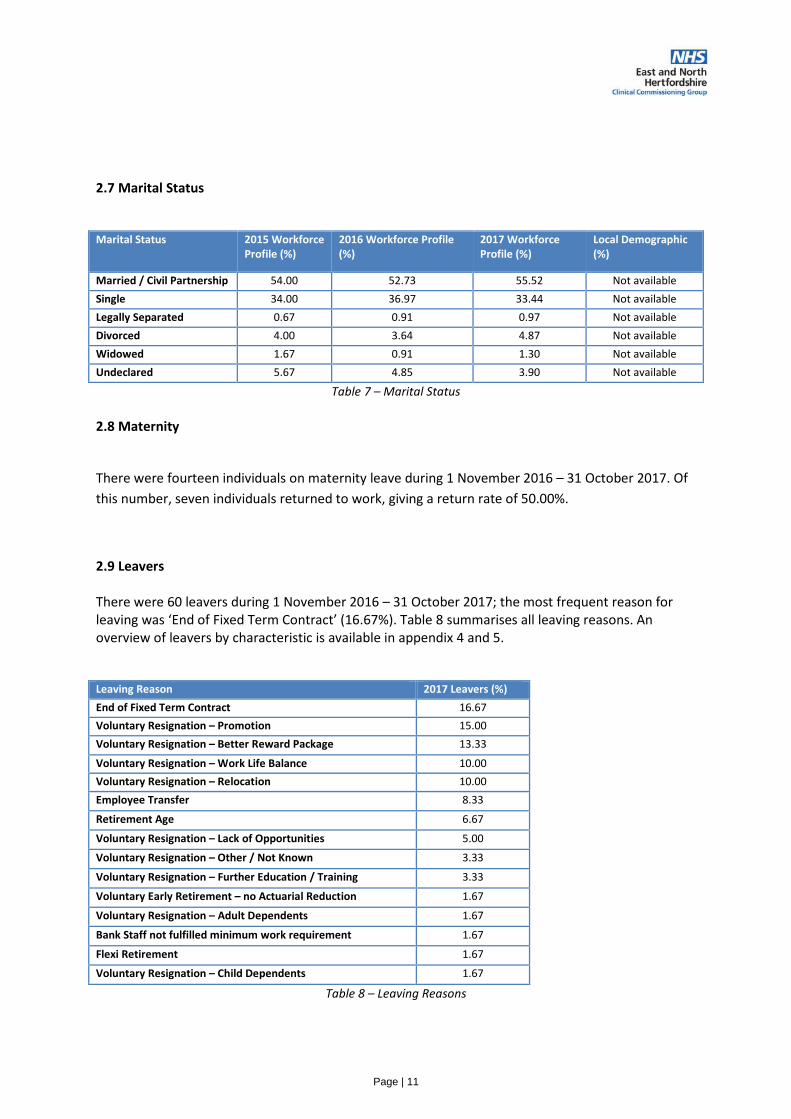
Page | 11
2.7 Marital Status
Marital Status 2015 Workforce Profile (%)
2016 Workforce Profile (%)
2017 Workforce Profile (%)
Local Demographic (%)
Married / Civil Partnership 54.00 52.73 55.52 Not available
Single 34.00 36.97 33.44 Not available
Legally Separated 0.67 0.91 0.97 Not available
Divorced 4.00 3.64 4.87 Not available
Widowed 1.67 0.91 1.30 Not available
Undeclared 5.67 4.85 3.90 Not available
Table 7 – Marital Status
2.8 Maternity
There were fourteen individuals on maternity leave during 1 November 2016 – 31 October 2017. Of
this number, seven individuals returned to work, giving a return rate of 50.00%.
2.9 Leavers
There were 60 leavers during 1 November 2016 – 31 October 2017; the most frequent reason for leaving was ‘End of Fixed Term Contract’ (16.67%). Table 8 summarises all leaving reasons. An overview of leavers by characteristic is available in appendix 4 and 5.
Leaving Reason 2017 Leavers (%)
End of Fixed Term Contract 16.67
Voluntary Resignation – Promotion 15.00
Voluntary Resignation – Better Reward Package 13.33
Voluntary Resignation – Work Life Balance 10.00
Voluntary Resignation – Relocation 10.00
Employee Transfer 8.33
Retirement Age 6.67
Voluntary Resignation – Lack of Opportunities 5.00
Voluntary Resignation – Other / Not Known 3.33
Voluntary Resignation – Further Education / Training 3.33
Voluntary Early Retirement – no Actuarial Reduction 1.67
Voluntary Resignation – Adult Dependents 1.67
Bank Staff not fulfilled minimum work requirement 1.67
Flexi Retirement 1.67
Voluntary Resignation – Child Dependents 1.67
Table 8 – Leaving Reasons
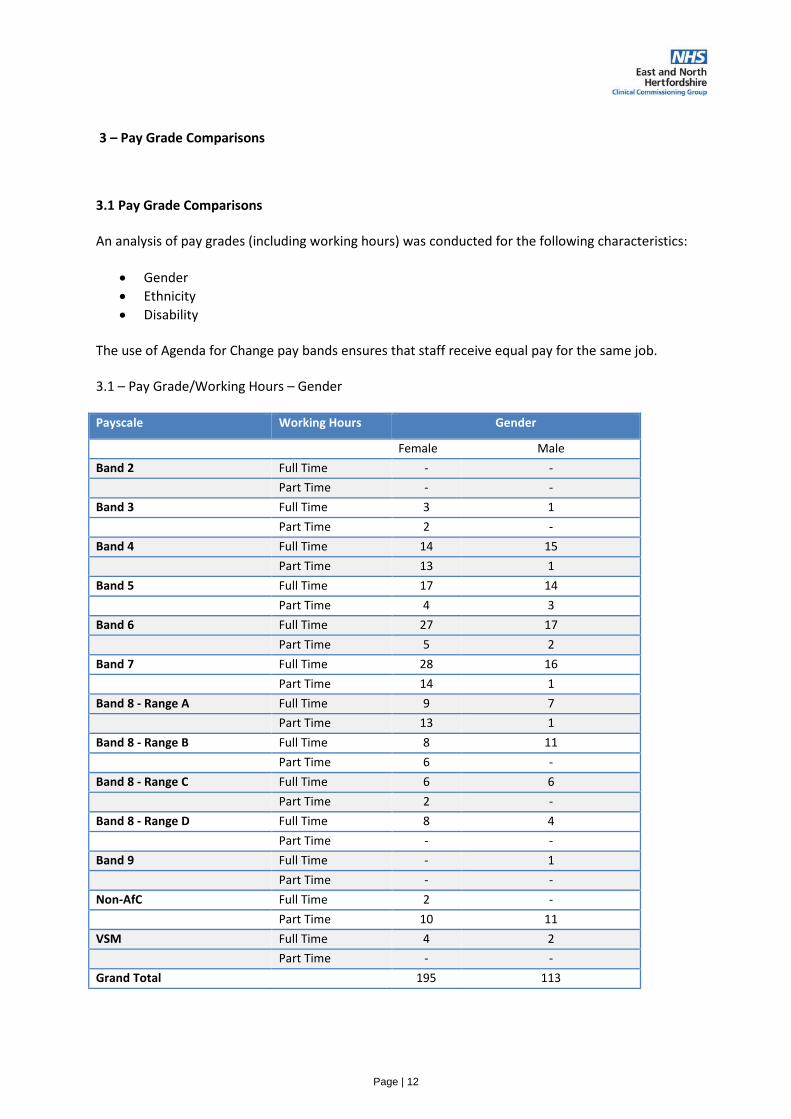
Page | 12
3 – Pay Grade Comparisons
3.1 Pay Grade Comparisons
An analysis of pay grades (including working hours) was conducted for the following characteristics:
• Gender
• Ethnicity
• Disability
The use of Agenda for Change pay bands ensures that staff receive equal pay for the same job.
3.1 – Pay Grade/Working Hours – Gender
Payscale Working Hours Gender
Female Male
Band 2 Full Time - -
Part Time - -
Band 3 Full Time 3 1
Part Time 2 -
Band 4 Full Time 14 15
Part Time 13 1
Band 5 Full Time 17 14
Part Time 4 3
Band 6 Full Time 27 17
Part Time 5 2
Band 7 Full Time 28 16
Part Time 14 1
Band 8 - Range A Full Time 9 7
Part Time 13 1
Band 8 - Range B Full Time 8 11
Part Time 6 -
Band 8 - Range C Full Time 6 6
Part Time 2 -
Band 8 - Range D Full Time 8 4
Part Time - -
Band 9 Full Time - 1
Part Time - -
Non-AfC Full Time 2 -
Part Time 10 11
VSM Full Time 4 2
Part Time - -
Grand Total 195 113

Page | 13
3.2 – Pay Grade/Working Hours – Ethnicity
Payscale Working Hours
BME Undeclared White Other
Band 2 Full Time - - - -
Part Time - - - -
Band 3 Full Time - 1 2 1
Part Time - - 2 -
Band 4 Full Time 7 - 22 -
Part Time 2 - 12 -
Band 5 Full Time 10 1 20 -
Part Time 1 1 5 -
Band 6 Full Time 10 2 32 -
Part Time - - 7 -
Band 7 Full Time 10 2 30 2
Part Time 3 - 12 -
Band 8 - Range A Full Time 3 - 13 -
Part Time 5 - 9 -
Band 8 - Range B Full Time 2 - 16 1
Part Time - - 5 1
Band 8 - Range C Full Time 1 1 10 -
Part Time - - 2 -
Band 8 - Range D Full Time 2 - 10 -
Part Time - - - -
Band 9 Full Time - - 1 -
Non-AfC Full Time 1 - 1 -
Part Time 7 2 9 3
VSM Full Time - - 6 -
Part Time - - - -

Page | 14
3.3 – Pay Grade/Working Hours – Disability
Payscale Working Hours Disability - No Undeclared Disability - Yes
Band 2 Full Time - - -
Part Time - - -
Band 3 Full Time 4 - -
Part Time 2 - -
Band 4 Full Time 29 - -
Part Time 12 2 -
Band 5 Full Time 25 3 3
Part Time 6 1 -
Band 6 Full Time 38 3 3
Part Time 6 - 1
Band 7 Full Time 38 4 2
Part Time 14 1 -
Band 8 - Range A Full Time 14 1 1
Part Time 14 - -
Band 8 - Range B Full Time 19 - -
Part Time 6 - -
Band 8 - Range C Full Time 10 2 -
Part Time 1 - 1
Band 8 - Range D Full Time 11 - 1
Part Time - - -
Band 9 Full Time 1 - -
Part Time - - -
Non-AfC Full Time 2 - -
Part Time 17 3 1
VSM Full Time 6 - -
Part Time - - -

Page | 15
Section 4 Recruitment and Selection 4.1 Recruitment & Selection Overview
Applications Shortlisted Appointed
Gender
Male 406 89 16
Female 454 144 33
Undisclosed 13 2 0
Disability
Yes 34 12 3
No 824 218 41
Undisclosed 15 5 5
Ethnicity
White 299 99 29
BME 531 126 11
Undisclosed 43 10 9
Age Group
Under 20 2 0 2
20-29 years 214 57 9
30-39 years 288 52 11
40-49 years 182 55 16
50-59 years 146 60 7
60-64 years 35 11 2
65+ years 6 0 2
Undisclosed 0 0 0
Religion / Belief
Atheism 73 22 4
Buddhism 7 1 0
Christianity 423 105 18
Hinduism 76 17 2
Islam 102 29 2
Jainism 9 3 0
Judaism 1 0 0
Sikhism 14 1 0
Other 60 19 7
Undisclosed 108 38 16
Sexual Orientation
LGB 17 3 1
Heterosexual 786 214 35
Undisclosed 70 18 13
Marital Status
Married / Civil Partnership 408 102 22
Single 368 99 22
Legally Separated 5 0 -
Divorced 33 13 2
Widowed 10 5 1
Undisclosed 49 16 2

Page | 16
Section 5 – Training and Development
Mandatory Training Participation Rates by Protected Characteristics
Please note: ‘No’ indicates that not all elements of mandatory training have been completed. ‘Yes’
shows that a member of staff has 100% compliance with mandatory training requirements.
Age 19-29 30-39 40-49 50-59 60-69
No 46.42% 46.55% 52.22 52.63% 50.00%
Yes 53.58% 53.45% 47.78% 47.37% 50.00%
Gender Female Male
No 51.09% 68.88%
Yes 48.91% 31.12%
Ethnicity BME Undisclosed White
No 75.86% 44.44% 49.72%
Yes 24.14% 55.56% 50.28%
Disability No Undisclosed Yes
No 50.00% 53.33% 54.54%
Yes 50.00% 46.67% 45.46%
Religion & Belief
Atheism Christianity Hinduism Islam Other Undisclosed
No 55.55% 45.71% 62.50% 62.50% 53.84% 50.56%
Yes 45.55% 54.29% 37.50% 37.50% 46.16% 49.44%
Sexual Orientation
Heterosexual LGB Undisclosed
No 49.48% 25.00% 54.05%
Yes 50.52% 75.00% 45.95%
Marital Status
Divorced Legally Separated
Married/Civil Partnership
Single Undisclosed Widowed
No 25.00% 100.00% 58.21% 41.05% 54.54% 33.33%
Yes 75.00% 41.79% 58.95% 45.46% 66.67

Page | 17
Appendix 1 - Workforce Data Overview
Characteristic 2015Workforce Data (%) 2016 Workforce Data (%) 2017 Workforce Data (%)
Gender
Male 38.00 38.18 36.69
Female 62.00 61.82 63.31
Disability Status
Yes 4.33 3.94 4.22
No 90.00 89.7 89.29
Undeclared 5.67 6.36 6.49
Ethnicity
White 75.67 74.24 73.38
BME 22.33 23.33 20.78
Other - - 2.60
Undeclared 2.00 2.42 3.25
Age Band
Under 20 - 0.61 0.65
20 to 39 34.67 38.48 31.49
40 to 49 30.00 28.79 32.79
50 to 65 34.67 31.52 33.77
65 + 0.67 0.61 1.30
Undeclared - - -
Religion
Atheism 11.00 13.03 12.34
Buddhism 1.33 1.21 0.97
Christianity 41.33 37.58 36.69
Hinduism 3.00 3.03 3.57
Islam 2.67 3.03 27.92
Other 8.00 6.36 7.14
Sikhism 1.00 0.61 0.97
Undeclared 32.67 35.15 7.79
Sexual Orientation
LGB 1.00 1.21 1.30
Heterosexual 72.33 70 69.16
Undeclared 26.67 28.79 29.55
Marital Status
Married / Civil Partnership 54.00 52.73 54.87
Single 34.00 36.97 33.44
Separated 0.67 0.91 0.97
Divorced 4.00 3.64 4.87
Widowed 1.67 0.91 1.30
Undeclared 5.67 4.85 3.90

Page | 18
Appendix 2 – Leavers Overview
Characteristic Leavers (2015) Leavers (2016) Leavers (2017)
Gender
Male 17 27 27
Female 39 36 33
Undeclared - -
Disability
Yes 1 1 3
No 51 55 52
Undeclared 4 7 5
Ethnic Origin
White 35 38 36
BME 21 22 23
Other - - 1
Undeclared - 3 -
Age Band
Under 20 - 1 1
20 to 39 25 29 27
40 to 49 12 16 16
50 to 65 17 16 13
65+ 2 - 3
Undeclared - 1 -
Religion / Belief
Atheism 7 7 7
Christianity 21 21 26
Hinduism 4 4 1
Islam 2 4 4
Other 5 8 6
Undeclared 17 19 16
Sexual Orientation
LGB - 2 1
Heterosexual 40 46 44
Undeclared 16 15 15
Marital Status
Married / Civil Partnership 34 27 25
Single 15 21 30
Legally Separated / Divorced / Widowed 5 6 1
Undeclared 2 9 4

Page | 19
Appendix 3 – Leaving Reasons – Protected Characteristics
Leaving Reason Female (%) Male (%)
End of Fixed Term Contract 15.15 18.52
Voluntary Resignation – Promotion 15.15 14.81
Voluntary Resignation – Better Reward Package 6.06 22.22
Voluntary Resignation – Work Life Balance 12.12 7.41
Voluntary Resignation – Relocation 15.15 3.70
Employee Transfer 9.09 7.41
Retirement Age 9.09 3.70
Voluntary Resignation – Lack of Opportunities 9.09 -
Voluntary Resignation – Other / Not Known 3.03 3.70
Voluntary Resignation – Further Education / Training 3.03 3.70
Voluntary Early Retirement – no Actuarial Reduction - 3.70
Voluntary Resignation – Adult Dependents 3.03 -
Bank Staff not fulfilled minimum work requirement - 3.70
Flexi Retirement - 3.70
Voluntary Resignation – Child Dependents - 3.70
Leaving Reasons – Gender
Leaving Reason White (%) BME (%) Other (%)
End of Fixed Term Contract 19.44 13.04 -
Voluntary Resignation – Promotion 11.11 21.74 -
Voluntary Resignation – Better Reward Package 8.33 21.74 -
Voluntary Resignation – Work Life Balance 13.89 4.35 -
Voluntary Resignation – Relocation 11.11 8.70 -
Employee Transfer 11.11 4.35 -
Retirement Age 11.11 - -
Voluntary Resignation – Lack of Opportunities 2.78 8.70 -
Voluntary Resignation – Other / Not Known - 8.70 -
Voluntary Resignation – Further Education / Training 2.78 4.35 -
Voluntary Early Retirement – no Actuarial Reduction 2.78 - -
Voluntary Resignation – Adult Dependents 2.78 - -
Bank Staff not fulfilled minimum work requirement - 4.35 -
Flexi Retirement - - 100.00
Voluntary Resignation – Child Dependents 2.78 - -
Leaving Reasons – Ethnicity

Page | 20
Leaving Reasons – Religion / Belief
Leaving Reason < 20 Years %
20-39 Years %
40-49 Years %
50-65 Years %
Undeclared %
End of Fixed Term Contract - 18.52 12.50 15.38 -
Voluntary Resignation – Promotion - 18.52 18.75 7.69 -
Voluntary Resignation – Better Reward Package - 18.52 12.50 7.69 -
Voluntary Resignation – Work Life Balance - 7.41 18.75 7.69 -
Voluntary Resignation – Relocation - 14.81 12.50 - -
Employee Transfer - 3.70 6.25 23.08 -
Retirement Age - - - 15.38 -
Voluntary Resignation – Lack of Opportunities - 7.41 6.25 - -
Voluntary Resignation – Other / Not Known - 3.70 6.25 - -
Voluntary Resignation – Further Education / Training
100.00 3.70 - - -
Voluntary Early Retirement – no Actuarial Reduction
- - - 7.69 -
Voluntary Resignation – Adult Dependents - - - 7.69 -
Bank Staff not fulfilled minimum work requirement
- - 6.25 - -
Flexi Retirement - - - 7.69 -
Voluntary Resignation – Child Dependents - 3.70 - - -
Leaving Reasons – Age
Leaving Reason Atheism (%) Christian (%) Hinduism (%)
Islam (%) Other (%) Undisclosed (%)
End of Fixed Term Contract 28.57 11.54 - 25.00 - 25.00
Voluntary Resignation – Promotion
- 15.38 100.00 25.00 16.67 12.50
Voluntary Resignation – Better Reward Package
28.57 19.23 - - - 6.25
Voluntary Resignation – Work Life Balance
14.29 7.69 - - 33.33 6.25
Voluntary Resignation – Relocation
14.29 15.38 - 25.00 - -
Employee Transfer - 11.54 - - 33.33 -
Retirement Age - 11.54 - - - 6.25
Voluntary Resignation – Lack of Opportunities
- - - 25.00 - 12.50
Voluntary Resignation – Other / Not Known
- 3.85 - - - 6.25
Voluntary Resignation – Further Education / Training
- - - - 16.67 6.25
Voluntary Early Retirement – no Actuarial Reduction
- - - - - 6.25
Voluntary Resignation – Adult Dependents
- 3.85 - - - -
Bank Staff not fulfilled minimum work requirement
- - - - - 6.25
Flexi Retirement - - - - - 6.25
Voluntary Resignation – Child Dependents
14.29 - - - - -
Agenda Item No: 11
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Public Engagement Report: Sept 2017 – Jan 2018
Decision Discussion Information Follow up from last meeting
Report author: Mark Edwards, Public Engagement Manager
Report signed off by:
Dianne Desmulie, Lay member for Public Involvement
Dr Nicky Williams, Vice Chair
Purpose of the paper:
To provide the Governing Body with an update of public engagement and involvement activities over the last three months and how these have influenced the commissioning and quality of health services in east and north Hertfordshire, and also inform the Governing Body of the next steps and priorities for the engagement team going forward.
Recommendations
to the members:
To note the activities of the public engagement team, and
support the continued emphasis on recruitment of new
patient and care members via their GP surgeries.
Conflicts of Interest
involved:
None
Conflict of Interest Definitions The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

1. Executive Summary
This report seeks to summarise the principal activities of the public engagement team from September 2017 to January 2018.
The CCG has been involved in a range of public involvement events and activities ranging from listening to patient views on procurement for local services, new GP contracts in Hoddesdon and Welwyn Garden City and commissioning consultations.
Promotional campaigns have focussed on messages for Stay Well this Winter and NHS 111.
Two significant meetings with patient participation group representatives also took place, with presentation from the Chief Executive of the National Association for Patient Participation.
2. Background
Following the retirement of Lynda Dent at the end of the year, who we would like to thank for her years of dedicated service given to the NHS, as well as ongoing discussions with patient members and stakeholders, the CCG is reflecting on its engagement practices and are in the process of coproducing a new strategy and model of engagement. We hope to present this strategy for Governing Body discussion shortly.
Additionally we have sought to develop our reporting ensuring that it more effectively presents the nature of our work going forwards. We hope that this new format will develop over the course of the next year to provide a better sense of the outcomes of our engagement and involvement work.
3. Issues - N/A
4. Options - N/A
5. Resources implications - N/A
6. Risks/Mitigation Measures - N/A
7. Recommendations
To note the activities and forthcoming priorities of the public engagement team.
8. Next Steps - N/A

Key highlights of public involvement projects
1. Procurements – patients have been actively involved and given their views on procurements for community vasectomy and anti-coagulation services, and primary care contracts for The Limes Surgery and Spring House Medical Centre.
2. NHS Let’s Talk – patients have been consulted on and fed back on communication materials explaining the resulting policies from the recent Let’s Talk consultation.
3. We have provided and organisational response and share the consultation on Modernising Radiotherapy Services run by NHS England – this has been extended to the 24th January 2018.
4. We have supported the development of the Integrated Personal Commissioningboard – developing a communications and engagement plan to take forward the project, raise awareness of personal health budgets and involve patients
5. Commissioning Funding Framework (CFF) – four patient members have been recruited to attend the CFF steering group and will continue to input their views over the course of the next few months.
6. Vanguard learning event – the CCG and its partners hosted a successful stakeholder learning event of the better care in care homes vanguard project.
7. The Public Engagement Manager has held meetings with four of the locality patient commissioning groups, along with the wheelchair service user group and met with representatives of the Learning Disability Partnership Board to discuss engagement opportunities with the group.
8. We have created an STP engagement leads project group to look at better ways of joint working and provide assurance that there is public engagement and involvement embedded into the workstreams. We submitted an unsuccessful bid to NHS England for funding to support this work.
Campaigns
1. There has been extensive promotion of the national Stay Well This Wintercampaign from NHS England, using community events, media releases, digital media and through GP practices, partners and patients.
2. The fair processing period for My Care Record as part of the Extended Access to GP Practices in Welwyn and Hatfield.
3. The CCG is supporting the new NHS 111 public information campaign which uses TV and online advertising to promote the wider range of clinicians you can speak to when using NHS 111.
Patient Experience / Quality Improvements
1. Patient members continue to contribute to the cancer steering group on a regular basis and are contributing to a number of key projects.
2. The CCG organised a patient leaders workshop for cancer, looking to develop awareness and education materials for the public to achieve increased awareness of prevention, cancer screening and identifying early signs and symptoms.
3. Additionally two patient stories have been recorded, one looking at cancer and one with a focus on personal health budgets which are yet to be edited.
4. The patient network quality group have met on two occasions and received presentations and fed back on the Hertfordshire Suicide Prevention Strategy and the End of Life Palliative Care Strategy.
Public Involvement &
Engagement report January 2018
Public Engagement events
> Two patient focussed workshops held looking at the development of public engagement in the area with presentations from the Chief Executive of the National Association for Patient Participation were held in November 2017
> The CCG attended four community events (Hatfield Healthfest, Hertford Community Day, Welwyn Hatfield Alliance Conference and the Stevenage Health Summit)
> Integrated Personal Commissioning presented at two voluntary sector conferences
> Promotion of the Let’s Talk consultation at a series of roadshow stalls across east and north Hertfordshire.
> The CCG attended Anglo Hockerill European College and John Henry Newman School to promote career opportunities in the health service along with attendance at three Hertfordshire Head Teachers Forums
Social media engagement
Each day during December, the CCG shared the important work that goes on in the organisation with our followers on Twitter. You can see all of the tweets from the CCG’s ‘advent calendar’ by following this link: https://twitter.com/i/moments/945270290883534849
You said, we did (are doing)
1. We have developed communications materials for the new over-the-counter medication policy following consultation with patient members and stakeholders.
2. Similarly, the end of life and palliative care leaflet has been updated following patient input from the patient network quality group.
3. Following a suggestion from a patient member, we developed a special Stay Well this Winter email bulletin for patients and stakeholders.
4. We are in the process of developing a patient experience questionnaire for patients being treated with cancer and an education and awareness toolkit for cancer.
Next steps
We are in the process of co-producing and completing a new public engagement and involvement strategy for the organisation, which we hope to present to the Governing Body shortly.
Since the end of 2017 the CCG have been engaged with NHS England on an assessment process for our engagement activities. We are currently reviewing the response from NHS England and considering further action. Details of the assessment are due to be made public later in the year.
Twitter - @ENHertsCCG Facebook
Page | 1
Agenda Item No: 12
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Adult Mental Health Community Services and the Hertfordshire Suicide Prevention Strategy
Decision or Approval Discussion Information
Report author: Simon Pattison, Head of Integrated Health and Care Commissioning Team
Report signed off by: Harper Brown, Director of Commissioning
Executive Summary:
This paper provides the Governing Body with updates on a number of mental health related subjects, namely:
- An overview of the Hertfordshire suicide prevention strategy - Details on HPFT’s community mental health services with a
summary of current performance and actions to deliver improvements
- Changes to the Mental Health Act 1983 affecting the process for people who are detained for a mental health assessment
Recommendations
to the members:
It is recommended that Governing Body:
Note the agreed way forward on the Hertfordshire Suicide Prevention Strategy
Note the current performance of HPFT community services and the actions being taken to manage demand
Agree the proposed shared care protocol
Conflicts of Interest
involved:
None
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the consequences of a commissioning decision.
Non-Financial Professional Interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career.
Page | 2
Non-Financial Personal Interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit.
Indirect Interests This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision.
Page | 3
1. Executive summary
This report is a follow up to the report presented to Governing Body in August 2017. This report covers the following areas:
- An overview of the Hertfordshire Suicide Prevention Strategy
- HPFT’s current community mental health services including:
o An outline of mental health community team pressures and current performance
o The new Early Intervention in Psychosis teams
o Details of pilots to explore new models of primary care mental health support
o Details of the shared care physical health check protocol for people with serious mental illness (SMI).
- An overview of the recent changes to Section 135 and 136 of the Mental Health Act 1983.
2. Background
Mental health community services in Hertfordshire are primarily provided by Hertfordshire Partnership University NHS Foundation Trust (HPFT). They are managed by the Integrated Health and Care Commissioning Team (IHCCT) on behalf of East and North Herts CCG, Herts Valleys CCG and Hertfordshire County Council. The current three year contract began in April 2016 and so will run to March 2019. East and North Herts CCG’s contribution to this contract is £69.7million in 2017/18. Between April and September 2017 HPFT had 1,482 people referred to secondary mental health services in East and North Herts.
3. Suicide Prevention Strategy
The Five Year Forward View for Mental Health sets a national ambition of reducing the number of people who die by suicide by 10% compared to the 2016/17 baseline. To support this CCGs are expected to contribute towards the development and delivery of local multi-agency suicide prevention plans, working with local partners. Hertfordshire County Council’s Public Health team have led on the development of a Hertfordshire wide suicide prevention plan. The full plan is available through this link - Hertfordshire’s suicide prevention strategy.
Suicide rates are low in Hertfordshire when measured against local and national comparators, and this trend is broadly stable. 56 deaths were recorded as suicides and open verdicts at Coroner’s inquests in Hertfordshire between April 2015 and March 2016. However, the human cost of death by suicide is extremely high and tends to have an especially heightened and widespread effect for those in the family and beyond. Research in the USA suggests that around 135 people may be affected by each person dying by suicide, and the financial cost is estimated to be around £1.5 million per death. The National Confidential Inquiry into Suicide and Homicide states that 28% of people who died by suicide between 2005 and 2015 were known to mental health services nationally.
The national strategy has seven priority aims:
1. Reduce the risk of suicide in key high risk groups

Page | 4
2. Tailor approaches to improve mental health in specific groups
3. Reduce access to the means of suicide
4. Provide better information and support to those bereaved or affected by suicide
5. Support the media in delivering sensitive approaches to suicide and suicidal behaviour
6. Support research, data collection and monitoring
7. Reducing rates of self-harm as a key indicator of suicide risk.
The 2015/16 Hertfordshire suicide audit, along with the key national areas for action has formed the basis of Hertfordshire’s suicide prevention strategy. This was developed following consultation with over 30 organisations at a multi-agency suicide prevention event in November 2016.
Our vision is to make Hertfordshire a county where no one ever gets to a point where they feel suicide is their only option. This ambition of zero suicides is consistent with the national suicide prevention strategy for England. It forms one of the main aims of this strategy; the other is to improve support for those bereaved or affected by suicide.
This work does not rely on the provision of any extra resource. It is underpinned by the assumption that more can be delivered by improved co-ordination of the many agencies involved, all working to a common aim and plan.
Programme structure for Hertfordshire’s suicide prevention strategy delivery
To deliver the wide range of actions in the suicide prevention action plan, partners across the county work together across a broad range of initiatives. The following programme structure will help co-ordinate this work and monitor and evaluate delivery.
A Suicide Prevention Programme Board, comprised of a small number of sector representatives, meet quarterly to maintain strategic direction, approve the action plan and take any major decisions. Commissioners are represented by Simon Pattison.
A Suicide Prevention Working Group meets once every one or two months and oversees the work of the task and finish groups through structured highlight reports. It escalates major risks and issues to the Suicide Prevention Board. Though it has a core membership, the group is open to interested parties.
The action plan will be delivered by task and finish groups set up around specific actions or delivered through groups already in existence, such as Spot the Signs. These action areas have been drawn from workshop sessions at the November 2016 multi-agency event.

Page | 5
Appendix A details the different groups and the priorities that they are responsible for. Some of the key actions over the next year are:
The launch of ‘Just Talk’ - a mental health campaign for boys and young men in
Hertfordshire. The focus on men and boys recognises that 80% of those who die by
suicide in Hertfordshire are male, and the 20-29 and 40-49 age groups are
particularly high risk. ‘Just Talk’ will launch on 22nd January , the campaign aims to:
o Increase access to mental health services
o Increase recognition of mental health services
o Increase recognition of emotional wellbeing information and support
o Increase reported use of healthy coping strategies by boys
Appendix B provides an overview of the ‘Just Talk’ campaign and Appendices C and
D are examples of some of the campaign literature.
Continuation of the ‘Spot the Signs’ training programme. Over 200 people from 100
different organisations and teams have been on the general Spot the Signs training,
which trains those in the public, private and voluntary sectors to identify when
someone is experiencing suicidal ideation gives them practical tools to help. Spot the
Signs also train GPs in suicide prevention in tailored sessions and 157 GPs from
East and North Herts have now been on training courses. In 2018, the aim is to
reach the GP practices who have yet to undergo training, and to continue to reach
organisations who work with or have staff in high-risk groups for suicide.

Page | 6
A focus on support for bereaved families - the impact of suicide on families is
extremely high, and they as a population are at a greatly increased risk of suicide.
This group will continue work to co-ordinate the support offered by the coroner’s
office, police, the NHS and the voluntary sector, and to identify and address gaps in
provision.
Suicide on the railway accounts for around 5% of all deaths by suicide nationally. Through
the suicide prevention groups we engage with national partners such as British Transport
Police, sharing information on locations that are considered high risk and individual
situations where railway staff have intervened to prevent a suicide attempt. Nationally the
rail industry developed a 9 point plan in 2014/15 which forms the basis of their work to
reduce deaths on the railway. Key actions include:
Identifying ‘at risk’ locations based on incident data with an escalation process for
any location with 3 or more attempts in a 12 month period.
Training for railway staff so they are able to intervene when they are concerned
about someone’s behaviour. Over 15,000 rail industry staff have received training so
far and in 2016/17 there were 48 life-saving interventions by railway staff in
Hertfordshire.
Physical mitigation measures to restrict access to high risk locations.
Promoting help seeking behaviour, for example by the use of ‘Samaritans’ material
on platforms and level crossings.
4. HPFT Adult Community Mental Health Services
This section summarises the main performance issues within adult mental health community services provided by HPFT.
The major adult community related performance measures reported in the contract are shown in Appendix E. Over the last few months the following areas have been the main focus of concern:
The number of routine referrals waiting more than 28 days for a first appointment.
Staffing related metrics – sickness rates, staff with a completed appraisal and mandatory training rates (these metrics include all HPFT staff). These are discussed in the staffing section below.
Routine Referrals Meeting 28 day Wait
Since the start of 2017 HPFT’s Single Point of Access has experienced significant demand pressures. Referrals to HPFT community teams increased by 6% in 2016 compared to. 2015, and are up a further 4% during 2017 compared to the same period in 2016. This led to a drop in performance against the routine referrals target (28 day waiting time target) for both adult and children and young people.
An action plan was developed under four areas to streamline referral processes into SPA and reduce pressures: These were:
i. Technical solutions to SPA, such as introducing a new call handling system.
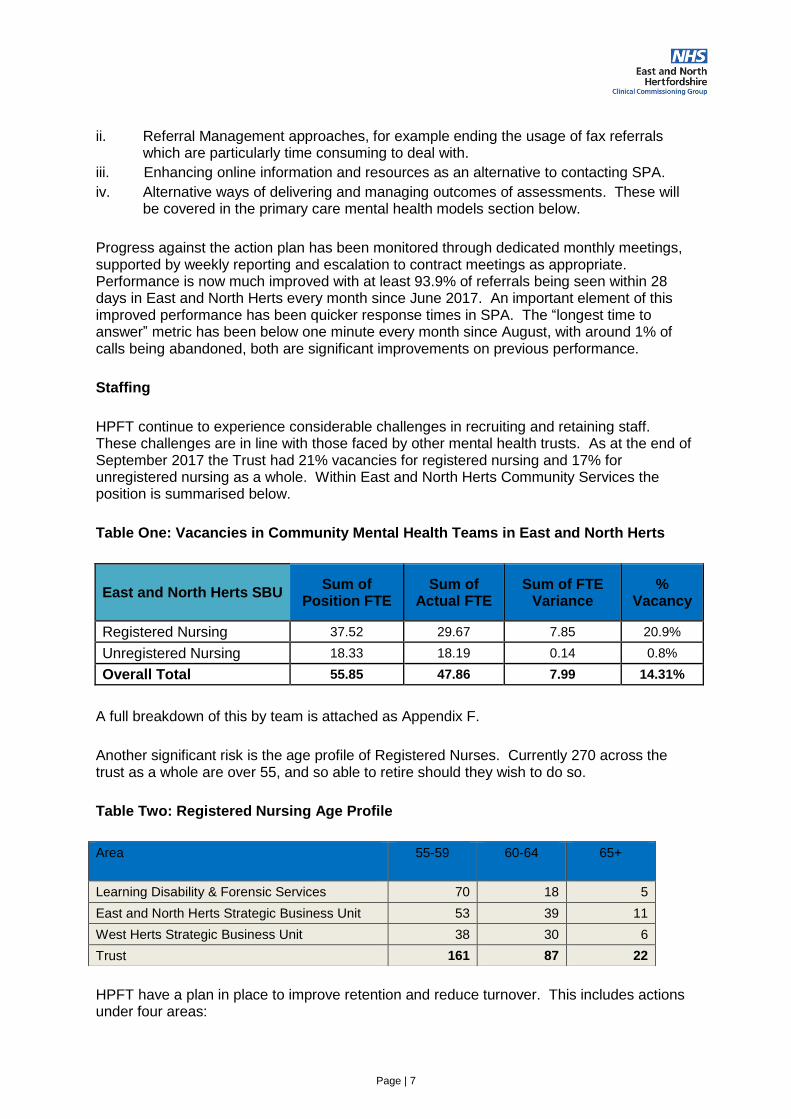
Page | 7
ii. Referral Management approaches, for example ending the usage of fax referrals which are particularly time consuming to deal with.
iii. Enhancing online information and resources as an alternative to contacting SPA.
iv. Alternative ways of delivering and managing outcomes of assessments. These will be covered in the primary care mental health models section below.
Progress against the action plan has been monitored through dedicated monthly meetings, supported by weekly reporting and escalation to contract meetings as appropriate. Performance is now much improved with at least 93.9% of referrals being seen within 28 days in East and North Herts every month since June 2017. An important element of this improved performance has been quicker response times in SPA. The “longest time to answer” metric has been below one minute every month since August, with around 1% of calls being abandoned, both are significant improvements on previous performance.
Staffing
HPFT continue to experience considerable challenges in recruiting and retaining staff. These challenges are in line with those faced by other mental health trusts. As at the end of September 2017 the Trust had 21% vacancies for registered nursing and 17% for unregistered nursing as a whole. Within East and North Herts Community Services the position is summarised below.
Table One: Vacancies in Community Mental Health Teams in East and North Herts
East and North Herts SBU Sum of
Position FTE Sum of
Actual FTE Sum of FTE
Variance %
Vacancy
Registered Nursing 37.52 29.67 7.85 20.9%
Unregistered Nursing 18.33 18.19 0.14 0.8%
Overall Total 55.85 47.86 7.99 14.31%
A full breakdown of this by team is attached as Appendix F.
Another significant risk is the age profile of Registered Nurses. Currently 270 across the trust as a whole are over 55, and so able to retire should they wish to do so.
Table Two: Registered Nursing Age Profile
HPFT have a plan in place to improve retention and reduce turnover. This includes actions under four areas:
Area 55-59 60-64 65+
Learning Disability & Forensic Services 70 18 5
East and North Herts Strategic Business Unit 53 39 11
West Herts Strategic Business Unit 38 30 6
Trust 161 87 22
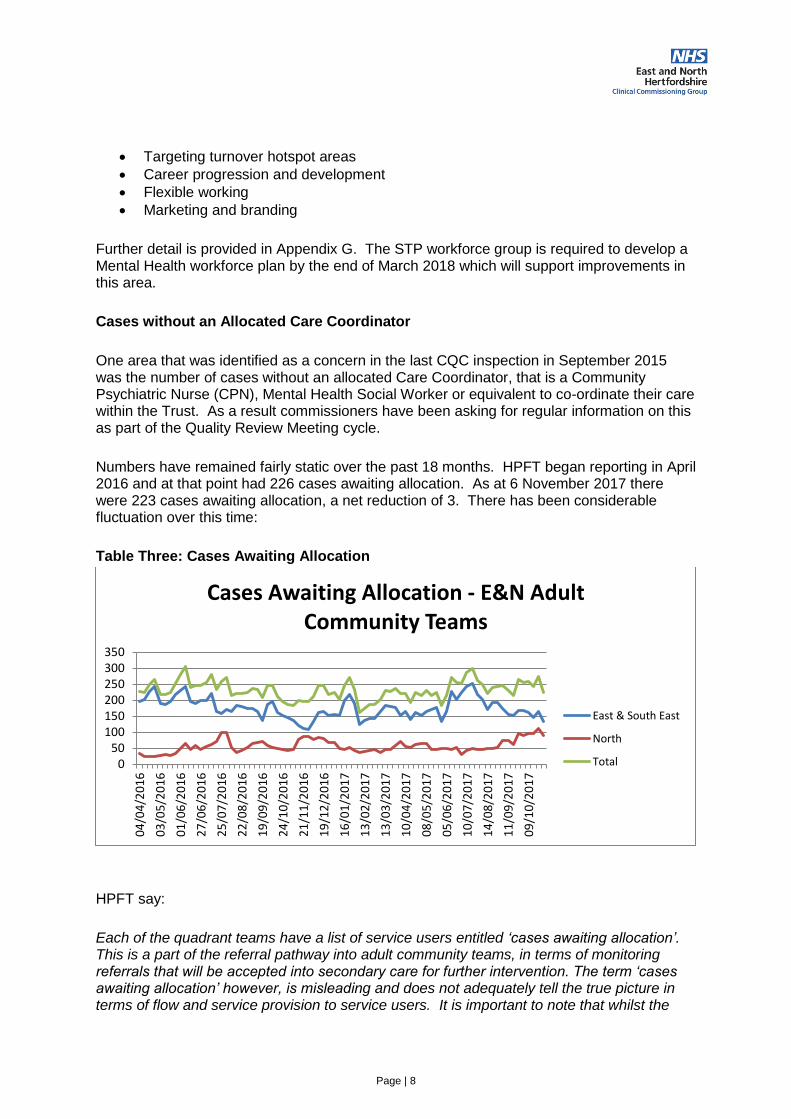
Page | 8
Targeting turnover hotspot areas
Career progression and development
Flexible working
Marketing and branding
Further detail is provided in Appendix G. The STP workforce group is required to develop a Mental Health workforce plan by the end of March 2018 which will support improvements in this area.
Cases without an Allocated Care Coordinator
One area that was identified as a concern in the last CQC inspection in September 2015 was the number of cases without an allocated Care Coordinator, that is a Community Psychiatric Nurse (CPN), Mental Health Social Worker or equivalent to co-ordinate their care within the Trust. As a result commissioners have been asking for regular information on this as part of the Quality Review Meeting cycle.
Numbers have remained fairly static over the past 18 months. HPFT began reporting in April 2016 and at that point had 226 cases awaiting allocation. As at 6 November 2017 there were 223 cases awaiting allocation, a net reduction of 3. There has been considerable fluctuation over this time:
Table Three: Cases Awaiting Allocation
HPFT say:
Each of the quadrant teams have a list of service users entitled ‘cases awaiting allocation’. This is a part of the referral pathway into adult community teams, in terms of monitoring referrals that will be accepted into secondary care for further intervention. The term ‘cases awaiting allocation’ however, is misleading and does not adequately tell the true picture in terms of flow and service provision to service users. It is important to note that whilst the
050
100150200250300350
04
/04
/20
16
03
/05
/20
16
01
/06
/20
16
27
/06
/20
16
25
/07
/20
16
22
/08
/20
16
19
/09
/20
16
24
/10
/20
16
21
/11
/20
16
19
/12
/20
16
16
/01
/20
17
13
/02
/20
17
13
/03
/20
17
10
/04
/20
17
08
/05
/20
17
05
/06
/20
17
10
/07
/20
17
14
/08
/20
17
11
/09
/20
17
09
/10
/20
17
Cases Awaiting Allocation - E&N Adult Community Teams
East & South East
North
Total
Page | 9
numbers remain relatively static, this is not the same group of service users and again reflects the flow into the teams.
Within the tracker there are a number of different categories/reasons why a service user is on the tracker including:
a) Requests from internal referrals (CATT, acute wards).
b) Requests from other internal teams.
c) Cases following initial assessment which may require care co-ordinator allocation, or alternative interventions e.g. Support with housing, social care interventions.
d) Cases that need to be re-allocated to a care co-ordinator following a staff member leaving/long term sick.
The tracker is reviewed on a weekly basis within the teams and the service users have details of how to contact the ‘duty’ worker and Mental Health Helpline. The duty workers will have regular contact with service users on the tracker to monitor their mental state, risks and offer support. Where possible, duty workers will also provide support e.g. completing of forms, signposting to other services.
Requests from internal referrals – CATT (Crisis teams) and acute wards are treated as a priority, as are any other referrals where significant risk is indicated. Some of the cases will ultimately not require care co-ordination, particularly for those cases in category C, a support worker or housing worker may be able to work with the individual in managing their needs. Others may be attending groups and their need for allocation to a care co-ordinator will be reviewed dependent upon their progress.
Primary Care Mental Health Models
As set out above HPFT services are under pressure due to rising demand and difficulties in recruiting staff. Referrals to HPFT community teams increased by 6% in 2016 compared to. 2015, and are up a further 4% during 2017 compared to the same period in 2016. Pressure to ensure timely access to assessment and treatment is compounded by the high number of Did Not Attends (DNAs) for Initial Assessments (IA) with on average 40% of people not attending their first offered appointments for the Adult Community Teams.
One approach being trialled under the STP Mental Health workstream is the development of primary care mental health models. Models of primary mental health care aim to support people better in primary care. Two pilot sites in E&NH will begin in the next three months, based in Stevenage and Hertford. A CPN will be present in a GP practice for the agreed sessions, supported by a social prescribing role, to provide an effective triage, supporting patients to access community resources promptly, where not appropriate for secondary care services. The CPN will also be able to book Initial Assessments where this is deemed appropriate. Urgent, CAMHS, and older peoples referrals will continue to be referred through SPA.
The pilots will be undertaken for six months, and reviewed against performance measures of DNA rates, waiting times, impact upon community mental health team caseload, user / carer feedback, and general practice feedback. Dependent upon the outcome, a business case will be developed for a broader roll out in late 18/19. Localities will be engaged regarding this pilot to help facilitate any broader subsequent roll out.

Page | 10
Early Intervention in Psychosis
Amongst the national mental health performance measures for mental health three have been identified as the key metrics to be reported on at STP level, alongside targets such as the A&E 4 hour waiting time target. These three measures are:
1. The number of people accessing psychological therapies under the IAPT programme.
2. The IAPT recovery rate (i.e. the percentage of people seeing significant improvement in their mental health having been through a course of IAPT treatment).
3. The number of people with a first episode of psychosis starting treatment within two weeks. The national target is that 50% of people start treatment within two weeks.
In 2016/17 and 2017/18 the CCG increased investment in HPFT’s Early Intervention in Psychosis (EIP) service to allow this third target to be met. To deliver this target commissioners agreed a revised service model with HPFT based on standalone First Episode of Psychosis (FEP) teams to concentrate solely on people experiencing their first episode of psychosis. These teams are made up of small mini-teams of three staff managing a caseload between them. These mini-teams include one staff members at each of bands 4, 5 and 6 and is different to the national EIP model which relies entirely on Band 6 CPNs. The national model was considered unrealistic, given the shortage of CPNs both locally and nationally. The local model also gives some resilience in teams, improving continuity if one member of the team leaves.
The two week wait target has been met consistently since it was introduced in April 2016 as set out below:
Table Four: Performance against the two week waiting time target for EIP
The model also includes employment support and access to appropriate therapeutic interventions such as Cognitive Behavioural Therapy for Psychosis (CBTp) and Family Intervention for Psychosis.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
% EIP acceptances accessing services within 14 DaysSource: NHS England Published Figure, except latest month which is HPFT internal figure
Herts Valleys
East and North

Page | 11
Shared care physical health protocol for people with serious mental illness (SMI)
The purpose of developing a shared care protocol for physical health checks is to ensure
that all individuals with SMI have the appropriate physical health checks in the appropriate
setting and that communication across primary and secondary care is outlined to share
information relating to any interventions that occur.
A protocol has been developed based on the Royal College Physical health pathway and
this current draft, Appendix H, has had input so far from: Mental health GP leads for each
CCG, GP members, HPFT Consultants, pharmacy and commissioners.
With CCG agreement the implementation of the shared care protocol is anticipated to be as
soon as possible to meet NHS England target timeframes related to the physical healthcare
CQUIN.
5. Changes to Section 135 and Section 136 of the Mental Health Act
Under sections 135 and 136 of the Mental Health Act 1983 the police, in conjunction with healthcare professionals, can detain someone for a mental health assessment. 808 people were detained for an assessment in Hertfordshire in 2016/17 (records are kept by Hertfordshire Constabulary). The number of people detained has been increasing year on year and has more than doubled from 366 in 2013/14. The Policing and Crime Act 2016 introduced significant changes to this area. These are:
• Section 136 powers may be exercised anywhere other than in a private dwelling; and the definition of a Place of Safety has been extended to include any “suitable place” may be used as a place of safety (providing the occupier or person managing the premises agrees).
• It is unlawful to use a police station as a place of safety for anyone under the age of 18 in any circumstances.
• A police station can only be used as a place of safety for adults in specific circumstances, which are set out in regulations.
• The previous maximum detention period of up to 72 hours will be reduced to 24 hours (unless a doctor certifies that an extension of up to 12 hours is necessary).
• Before exercising a section 136 power police officers must, where practicable, consult a health professional.
• Where a section 135 warrant has been executed, a person may be kept at their home for the purposes of an assessment rather than being removed to another place of safety.
• A new search power will allow police officers to search persons subject to Section 135 or 136 powers for protective purposes.

Page | 12
Since April 2017, Section 136 system partners (Police, HPFT, HCC, EEAST and others) have been working to an implementation plan which outlines a number of actions to prepare for the enactment of the legislation. This has included running the changes in shadow form to monitor adherence to the anticipated changes and timescales as laid out in the legislation.
Data and intelligence from this shadow running has provided the Section 136 system partners with an understanding of where the most significant challenges will be for Hertfordshire. These are:
1. Breach of the 24 hour detention period, due to
Drug and alcohol intoxication
CAMHS social care issues
Availability of Approved Mental Health Professionals (AMHP) out of hours
2. Consultation with a mental health professional before exercising Section 136 powers
Following Regulations being through Parliament, guidelines were published on 31 October 2017, with legislation enforcement from 11 December 2017.
From April 2017 Section 136 system partners have been working to the 24 hour maximum detention period and recording breaches. In 90% of cases the 24 hour period has been adhered to. Figure 1 shows data Jul 2016 – Oct 2017 on the number of detentions which exceeded the 24 hour period (blue line). Breaches were principally due to intoxication and in a small number of cases children needing emergency social care support. For these children, if the (up to 12 hours) extension criteria are not met, there is a risk that short term emergency accommodation might be needed whilst social care packages are put in place.
Figure Five: Total S136 detentions/S136 detentions with duration of over 24 hours (Jul 2016-Oct 2017)
Page | 13
Actions taken to mitigate breaches:
Fully established dedicated Section 136 staff team at HPFT Kingsley Green to ensure Section 136 detentions are triaged and assessed within the maximum time
Focussed piece of work between HPFT and CGL Spectrum to support the top 11 Section 136 frequent attenders, due to alcohol intoxication, being supported within the community through alternative care packages and options should they present for Section 136.
A new purpose build facility, funded through Department of Health Capital funding, for children and young people in Hertfordshire detained under Section 136 to be completed by April 2018, thus adding capacity to Hertfordshire’s Section 136 suites.
In the longer term, HPFT will be undertaking an organisational review and remodelling of community crisis response, which will involve partnership with the voluntary and community sector to sustain and further reduce S136 detentions and ensure people get the right response at the right time.
6. Resources implications
This report does not have any explicit resource implications. As part of the contract negotiations for 2018/19 commissioners are discussing priority areas for investment with HPFT. These are likely to include Early Intervention in Psychosis services.
7. Risks/Mitigation Measures
The HPFT contract is monitored through regular Contract and Quality Review Meetings. Issues are escalated to the Contracts, Performance and Quality and Organisational Performance and Delivery meetings as required.
8. Recommendations
It is recommended that Governing Body:
Note the current performance of HPFT community services and the actions being taken to manage demand.
Agree the proposed shared care protocol.
Note the agreed way forward on the Hertfordshire Suicide Prevention Strategy.

Page | 1
Appendix A: Suicide Prevention Groups
Group name Purpose
Suicide
Prevention
Programme
Board
Comprised of a small number of sector representatives, they meet quarterly to maintain strategic
direction, approve the action plan and take any major decisions.
Suicide
Prevention
Working Group
Meets once every one or two months and oversees the work of the task and finish groups through
structured highlight reports. It escalates major risks and issues to the Suicide Prevention Board.
Though it has a core membership, the group is open to interested parties.
Focus on men
and boys (areas
for action 1 and 2
of the national
action plan)
Design and launch Just Talk campaign, specifically aimed at protecting and improving mental
health of secondary school age boys
Promote the voice and visibility of male role models in Hertfordshire on suicide
Ensure other task and finish groups take into account the high risk for men in their action
plans
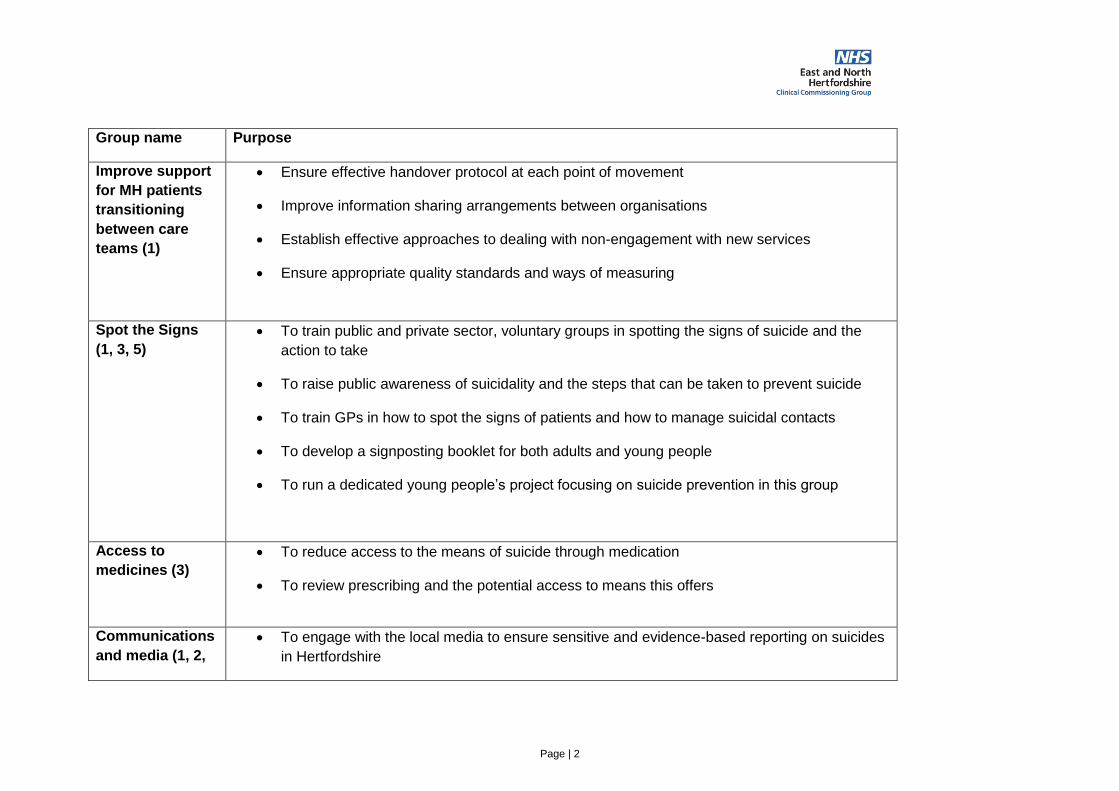
Page | 2
Group name Purpose
Improve support
for MH patients
transitioning
between care
teams (1)
Ensure effective handover protocol at each point of movement
Improve information sharing arrangements between organisations
Establish effective approaches to dealing with non-engagement with new services
Ensure appropriate quality standards and ways of measuring
Spot the Signs
(1, 3, 5)
To train public and private sector, voluntary groups in spotting the signs of suicide and the
action to take
To raise public awareness of suicidality and the steps that can be taken to prevent suicide
To train GPs in how to spot the signs of patients and how to manage suicidal contacts
To develop a signposting booklet for both adults and young people
To run a dedicated young people’s project focusing on suicide prevention in this group
Access to
medicines (3)
To reduce access to the means of suicide through medication
To review prescribing and the potential access to means this offers
Communications
and media (1, 2,
To engage with the local media to ensure sensitive and evidence-based reporting on suicides
in Hertfordshire

Page | 3
Group name Purpose
3, 4, 5, 7)
To promote the activities of the task and finish groups to a wider audience, including
professional stakeholders and the public
To carry out targeted campaigns on specific issues
Signposting and
referral (1, 2, 3, 4,
5, 7)
Improve signposting and referral for people at risk of suicide by non-mental health specialist
professional and voluntary groups
Ensure that the most-used places for signposting and referral, such as HertsHelp, the
Community Directory and 111, are effective in the area of suicide prevention
Monitor and measure efficacy of suicide prevention signposting and referral
Support for
families bereaved
by suicide (4)
Identify current sources of support and any gaps in the county
Develop local support through agencies like police, coroners, mental health services and
voluntary sector
Support for
young people (1,
2, 7)
Oversee work of Spot the Signs Youth project
Develop kite mark quality assurance for mental health work in young people settings
Develop school suicide prevention charter
Research the risk of exposure in suicide prevention delivery in schools

Page | 4
Group name Purpose
Performance
measures and
learning lessons
(6, 7)
Learn lessons from people who die by suicide via: regular suicide audit (consider frequency),
mental health service users, police data, coroner data and other sources
Develop dashboard of suicide prevention performance measures. Monitor and report
regularly. Use to inform what data needs to be collected.
Inform work of wider suicide prevention programme

Page | 1
Appendix B: ‘Just Talk’ Campaign Overview
‘Just Talk’ is a mental health campaign for boys and
young men in Hertfordshire.
Launching W/C 22nd Jan 2018, schools and community
agencies will have access to a range of resources to
promote the campaign. We’ll also be using social media,
sharing young people’s stories, seeing celebrity/big
names engaging with the campaign as role models, and
promoting the stories of ‘normal’ people that young
people can relate to. Professionals and parents will also
be involved in the campaign through events, parent evenings, and communication via
schools.
Why do we need a campaign?
Mental Health in adolescence is a growing issue. 1 in 10 children aged 5-16 have a
clinically significant mental health problem. This figure increases with age.
Prevention and early intervention is vital. Evidence shows that those that receive
support early have better outcomes. However, fear of stigma and discrimination is a
key barrier in accessing mental health support early.
National and local research and service data has demonstrated the need to focus on
mental health in boys, with a number of social and cultural barriers preventing men in
particular from opening up on the topic of mental health.
Importantly, we’re not excluding women. Time to Change found that men won’t
engage with campaigns aimed at women but women still notice campaigns aimed at
men. The campaign
A multi-agency group, chaired by Public Health, is working together to lead the ‘Just
Talk’ campaign to address these issues. Partners include CCGs, schools, health
services, voluntary sector, Watford FC, YC Hertfordshire, and the Time to Change
team.
Extensive local research, working with over 600 secondary school age boys, has
informed the campaign and will provide baseline data to measure impact.
Key messages from the ‘Just Talk’ campaign include:
o We are all affected by mental health, just like physical health
o Talking shows strength not weakness
o Seeking help early means you’re more likely to get better
o There are simple and relevant ways to improve your own mental health (or to
support others to improve their mental health)
o There is support and information available, and it can really help Get involved
Download and use resources from the campaign pages (once live)

Page | 2
Join in with one of the events during the campaign or run your own
Join the conversation on social media using the hashtag #JustTalk
To discuss the campaign further, contact Jen Beer: [email protected]

TalkingshowsstrengthWe all have mental health.We should be able to talk
about it in the same way we
talk about physical health.
For more information visit:healthyyoungmindsinherts.org.uk/justtalk #JUSTTALK
Appendix C
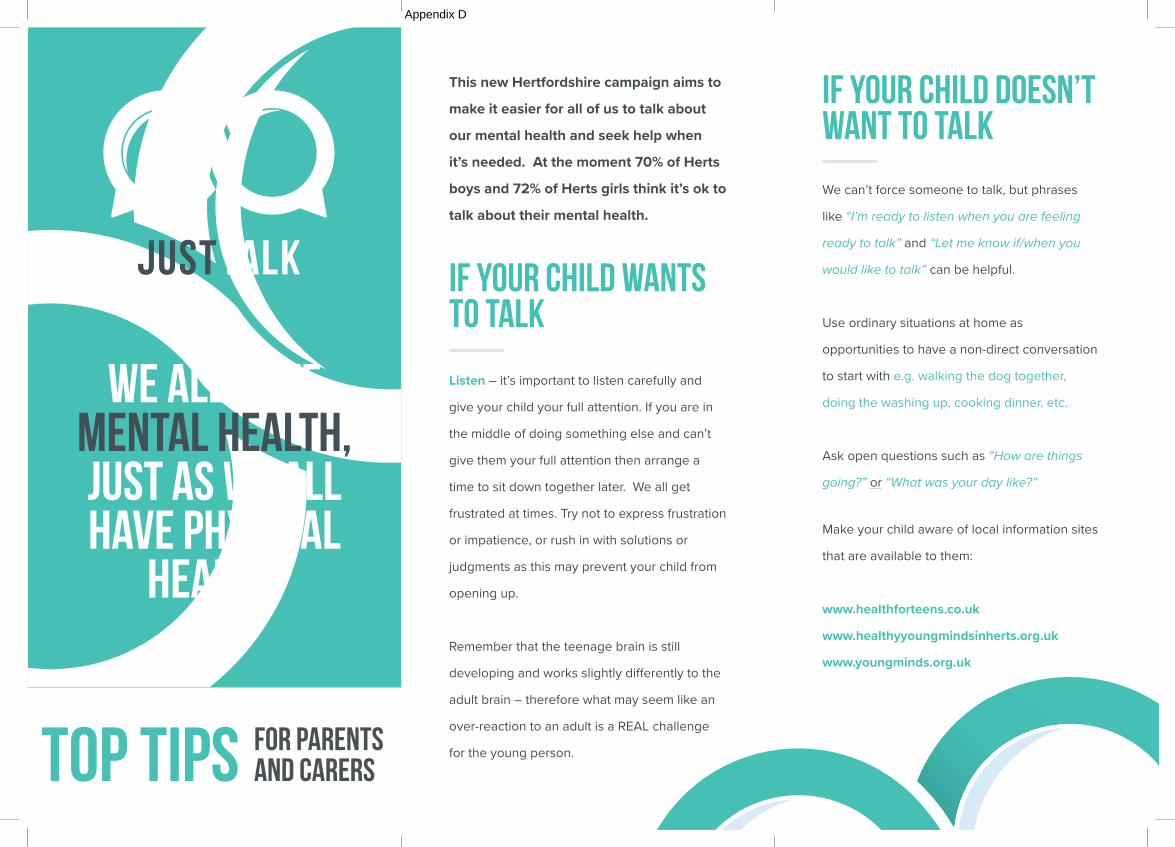
This new Hertfordshire campaign aims to make it easier for all of us to talk about our mental health and seek help when it’s needed. At the moment 70% of Herts boys and 72% of Herts girls think it’s ok to talk about their mental health.
Listen – it’s important to listen carefully and
give your child your full attention. If you are in
the middle of doing something else and can’t
give them your full attention then arrange a
time to sit down together later. We all get
frustrated at times. Try not to express frustration
or impatience, or rush in with solutions or
judgments as this may prevent your child from
opening up.
Remember that the teenage brain is still
developing and works slightly differently to the
adult brain – therefore what may seem like an
over-reaction to an adult is a REAL challenge
for the young person.
If your child wants to talk
TOP TIPS for parentsand carers
We can’t force someone to talk, but phrases
like “I’m ready to listen when you are feeling
ready to talk” and “Let me know if/when you
would like to talk” can be helpful.
Use ordinary situations at home as
opportunities to have a non-direct conversation
to start with e.g. walking the dog together,
doing the washing up, cooking dinner, etc.
Ask open questions such as “How are things
going?” or “What was your day like?”
Make your child aware of local information sites
that are available to them:
www.healthforteens.co.uk
www.healthyyoungmindsinherts.org.uk
www.youngminds.org.uk
If your child Doesn’t want to talk
We all have mental health, just as we all have physical
health.
Appendix D

Think about what language you use – phrases
like ‘Man up’ and ‘Toughen up’ can really make
it difficult for someone to talk about how they’re
feeling for fear of appearing weak. Mental
health problems are not a weakness, and
talking about them should be encouraged as a
sign of strength.
Role model that it’s OK to talk – By admitting
ourselves that sometimes we struggle and
need a little help from others, this shows our
child that it’s OK to reach out.
Signs that a boy is struggling can sometimes be
exhibited differently to girls. Warning signs for
boys may include the following:
Supporting Boys
Irritability, anger, and sensitivity to criticism
Physical pain – if someone is complaining of headaches or backaches with no obvious cause or sign of recovery, it could be a symptom of mental ill health
Reckless or risk taking behaviour – e.g. drinking alcohol or dangerous sports
In a recent Hertfordshire survey, we
discovered that if teenage boys were worried
about their mental health, almost half of them
would seek support from their parent before
anyone else.
However, often boys do worry about talking
to their parents because they don’t want
to burden them or are worried they won’t
understand.
It can help your son know that you are available
to them if you tell them that if they ever want to
talk about anything, you are there.
You could also broaden your knowledge of
mental health by completing the free MindEd
e-learning: www.minded.org.uk/families
Boys most commonly use physical activity and
sports, and technology and video games as
a coping strategy. Girls most commonly use
music or chatting to friends. There are lots of
things that can help boost a young person’s
wellbeing as well as potentially help them to
cope when things go wrong.
Connect: Spend time with family and friends.
Enjoy doing things together and talking to
each other.
Be Active: It keeps you physically healthy, and
makes you feel good.
Keep Learning: Try something new. Try a new
hobby, or learn about something just because it
interests you.
Take Notice: Take a break to see how you feel.
Relax and look around you or listen to music,
take a few deep breaths.
Give: Do something for a friend or relation/
adult, as well as making them feel good, it can
make you feel good too!
Don’t underestimate your role as a parent or carer
Helpful coping strategies

Page | 1
Appendix E: HPFT Community Performance Metrics
Measure CCG Targ
et
April Number
s
May Number
s
June Number
s Apr-17
May-17
Jun-17 Q1 Jul
Numbers
Aug Number
s
Sep Number
s Jul-17
Aug-17
Sep-17 Q2 Oct
Numbers
Oct-17
Percentage of inpatient admissions that have been gate-kept by crisis resolution/ home treatment team
Herts
95% 64/66 80/84 90/94 96.97% 95.24% 95.74
% 95.90
% 91/92 91/92 83/86
98.91%
98.91%
96.51%
97.78%
89/89 100%
ENCCG
95% 27/29 31/34 34/36 93.10% 91.18% 94.44
% 92.93
% 35/36 38/39 36/37
97.22%
97.44%
97.30%
97.32%
33/33 100%
HVCCG
95% 37/38 49/50 56/58 97.37% 98.00% 96.55
% 97.26
% 56/56 53/53 46/49 100% 100%
93.88%
98.10%
56/56 100%
EIP 14 day wait.
Herts
50% 16/20 20/24 14/19 80.00% 83.33% 73.68
% 79.37
% 20/33 23/31 22/34
60.61%
74.19%
64.71%
66.33%
18/28 64.29
%
ENCCG
50% 7/8 10/12 6/8 87.50% 83.33% 75.00
% 82.14
% 8/12 10/16 12/17
66.67%
62.50%
70.59%
66.67%
13/18 72.22
%
HVCCG
50% 9/12 10/12 8/11 75.00% 83.33% 72.73
% 77.14
% 12/21 13/15 10/17
57.14%
86.67%
58.82%
66.04%
5/10 50.00
%
The number of new cases of psychosis served by year to date - Target 150 per year. Cumulative data shown
Herts
150 in
year 20 24 19 20 44 63 33 31 34 96 127 161 28 189
Countywide Target
12 25 37 50 63 75 87
ENCCG
74 8 12 8 8 20 28 12 16 17 40 56 73 18 91
EN Target 6 12 18 25 31 37 43
HVCCG
76 12 12 11 12 24 35 21 15 17 56 71 88 10 98
HV Target 6 13 19 25 32 38 44
Routine referrals to community mental health team meeting
Herts
98% 313/381 383/466 426/454 82.15% 82.19% 93.83
% 86.24
% 440/474 398/457 361/439
92.83%
87.09%
82.23%
87.52%
358/433 82.68
%
ENCCG
98% 174/218 210/264 231/238 79.82% 79.55% 97.06
% 85.42
% 251/267 232/247 239/248
94.01%
93.93%
96.37%
94.75%
209/221 94.57
%
HVC 98% 139/163 173/202 195/216 85.28% 85.64% 90.28 87.26 189/207 166/210 122/191 91.30 79.05 63.87 78.45 149/212 70.28

Page | 2
Measure CCG Targ
et
April Number
s
May Number
s
June Number
s Apr-17
May-17
Jun-17 Q1 Jul
Numbers
Aug Number
s
Sep Number
s Jul-17
Aug-17
Sep-17 Q2 Oct
Numbers
Oct-17
28 day wait CG % % % % % % %
Urgent referrals to community mental health team meeting 24 hour wait
Herts
98% 1/1 1/1 3/3 100% 100% 100% 100% 2/2 1/1 3/3 100% 100% 100% 100% 3/3 100%
ENCCG
98% 0/0 2/2 2/2 Zero 100% 100% 100% 1/1 0/0 3/3 100% zero 100% 100% 3/3 100%
HVCCG
98% 1/1 0/0 1/1 100% Zero 100% 100% 1/1 1/1 0/0 100% 100% zero 100% 0/0 zero
CATT (crisis team) referrals meeting 4 hour wait
Herts
98% 551/551 527/527 640/640 100% 100% 100% 100% 630/630 593/593 536/536 100% 100% 100% 100% 583/590 98.81
%
Rate of referrals meeting maximum 18 week wait time from referral to treatment for all mental health and learning disability services
Herts
98% 1928 1954
2371 2399
2241 2275
98.67% 98.83% 98.51%
98.67%
2293 2320
1945 1973
1812 1830
98.84%
98.58%
99.02%
98.81%
2278 2299
99.09%
ENCCG
98% 982 993
1261 1278
1139 1161
98.89% 98.67% 98.11%
98.54%
1144 1160
958 974
987 995
98.62%
98.36%
99.20%
98.72%
1169 1178
99.24%
HVCCG
98%
946 961
1110 1121
1102 1114
98.44% 99.02%
98.92%
98.81%
1149 1160
987 999
825 835
99.05%
98.80%
98.80%
98.90%
1109 1121
98.93%
The proportion of those on Care Programme Approach (CPA) for at least 12 months who had a CPA review within the last 12
Herts
95% 851/887 815/861 759/788 95.94% 94.66% 96.32
% 96.32
% 710/734 664/706 835/889
96.73%
94.05%
93.93%
93.93%
763/816 93.50
%
ENCCG
95% 416/438 399/417 374/389 94.98% 95.68% 96.14
% 96.14
% 352/362 328/340 407/426
97.24%
96.47%
95.54%
95.54%
375/394 95.18
%
HVCCG
95% 435/449 416/444 385/399 96.88% 93.69% 96.49
% 96.49
% 358/372 336/366 428/463
96.24%
91.80%
92.44%
92.44%
388/422 91.94
%

Page | 3
Measure CCG Targ
et
April Number
s
May Number
s
June Number
s Apr-17
May-17
Jun-17 Q1 Jul
Numbers
Aug Number
s
Sep Number
s Jul-17
Aug-17
Sep-17 Q2 Oct
Numbers
Oct-17
months
The percentage of people under adult mental illness specialties who were followed up within 7 days of discharge from psychiatric in-patient care
Herts
95% 103/105 119/127 148/156 98.10% 93.70% 94.87
% 96.78
% 121/127 120/122 132/138
95.28%
98.36%
95.65%
96.38%
141/144 97.92
%
ENCCG
95% 46/46 52/58 60/63 100.00
% 89.66%
95.24%
96.58%
51/54 56/58 55/58 94.44
% 96.55
% 94.83
% 95.29
% 59/60
98.33%
HVCCG
95% 57/59 67/69 88/93 96.61% 97.10% 94.62
% 96.94
% 70/73 64/64 77/79
95.89%
100% 97.47
% 97.69
% 82/84
97.62%
Rate of service users with a completed up to date risk assessment (inc Learning Disability & Forensic & CAMHS)
Herts
95% 14,210 15,125
15,506 16,432
14,717 15,638 93.95% 94.36%
94.11%
94.11%
14,856 15,628
14,792 15,617
14,634 15,529
95.06%
94.72%
94.24%
94.24%
14,477 15,325
94.47%
ENCCG
95% 7395 7814
8095 8525
7602 8098
94.64% 94.96% 93.88
% 93.88
% 7682 8100
7599 8029
7521 8030
94.84%
94.64%
93.66%
93.66%
7455 7947
93.81%
HVCCG
95% 6815 7311
7411 7907
7115 7540
93.22% 93.73% 94.82
% 94.82
% 7174 7528
7193 7588
7113 7499
95.30%
94.79%
94.85%
94.85%
7022 7378
95.17%
Rate of staff with a current PDP and appraisal
Herts
92% 87.54% 86.94% 86.27
%
86.58%
88.30%
89.26%
90.04
%
Rate of mandatory training completed and up to date
Herts
92% 83.53% 84.93% 84.00
%
83.18%
81.77%
81.50%
81.28
%
Staff Sickness Rate
Herts
<4%
3.96% 4.05% 4.27% 4.09%
4.65% 4.18% 4.13% 4.32% 4.49%

Page | 1
Appendix F: HPFT Community Services - Summary of Fill Rates and Vacancies
Registered Nursing
SBU/TEAM Sum of
Position FTE
Sum of Actual
FTE
Sum of FTE
Variance
% Vacancy
Learning Disability & Forensic SBU
Challenging Behaviour Team 3 1.43 1.57 52
Continuing Care & Placement Team 10.64 7.64 3 28
Criminal Justice & Forensic 1 0 1 100
Criminal Justice Mental Health 2 2 0 0
LD SLDS A&T E/N Team 9 7 2 22
LD SLDS A&T West Team 10.56 9.56 1 9
Total Learning Disability and Forensic 36.2 27.63 8.57 23.67%
East & North Herts SBU
AMH Community Services Centenary & Jubilee 9.88 11.03 -1.15 -12
AMH Community Services Cygnet House 8.6 5 3.6 42
AMH Community Services Holly Lodge 2.4 1 1.4 58
AMH Community Services Saffron Ground 5.8 4.4 1.4 24
AMH Community Services Oxford House 1 1 0 0
AMH Community Services Rosanne House 9.84 7.24 2.6 26
Total East and North Herts SBU 37.52 29.67 7.85 20.92%
West Herts SBU
AMH Community Services NW Herts Dacorum 9.6 8 1.6 17
AMH Community Services NW Herts St Albans 6.2 3.2 3 48
AMH Community Services SW Herts 0.5 1 -0.5 -100
AMH Community Services SW Herts Borehamwood 5 1 4 80
AMH Community Services SW Herts Watford 10.4 7 3.4 33
Total West Herts Strategic Business Unit 31.7 20.2 11.5 36.28%
Overall Total 174.64 127.37 47.27 27.07%

Page | 2
Unregistered Nursing
SBU/TEAM Sum of
Position FTE
Sum of Actual
FTE
Sum of FTE
Variance
% Vacancy
Learning Disability & Forensic SBU
Challenging Behaviour Team 4 3 1 25
Continuing Care & Placement Team 3.79 2.39 1.4 37
LD SLDS A&T E/N Team 4 4 0 0
LD SLDS A&T West Team 3.6 4.6 -1 -28
Total Learning Disability and Forensic 15.39 13.99 1.4 9.10%
East & North Herts SBU
AMH Community Services Centenary & Jubilee 1 5.64 -4.64 -464
AMH Community Services Cygnet House 5.03 5.75 -0.72 -14
AMH Community Services Holly Lodge 2 2 0 0
AMH Community Services Saffron Ground 2.8 2.8 0 0
AMH Community Services Oxford House 2 0 2 100
AMH Community Services Rosanne House 5.5 2 3.5 64
Total East and North Herts SBU 18.33 18.19 0.14 0.76%
West Herts SBU
AMH Community Services NW Herts Dacorum 5 5 0 0
AMH Community Services NW Herts St Albans 4 3 1 25
AMH Community Services SW Herts 3 1 2 67
AMH Community Services SW Herts Borehamwood 2.49 3.49 -1 -40
AMH Community Services SW Herts Watford 6.83 3.96 2.87 42
Total West Herts Strategic Business Unit 21.32 16.45 4.87 22.84%
Overall Total 94.69 83.27 11.42 12.06%
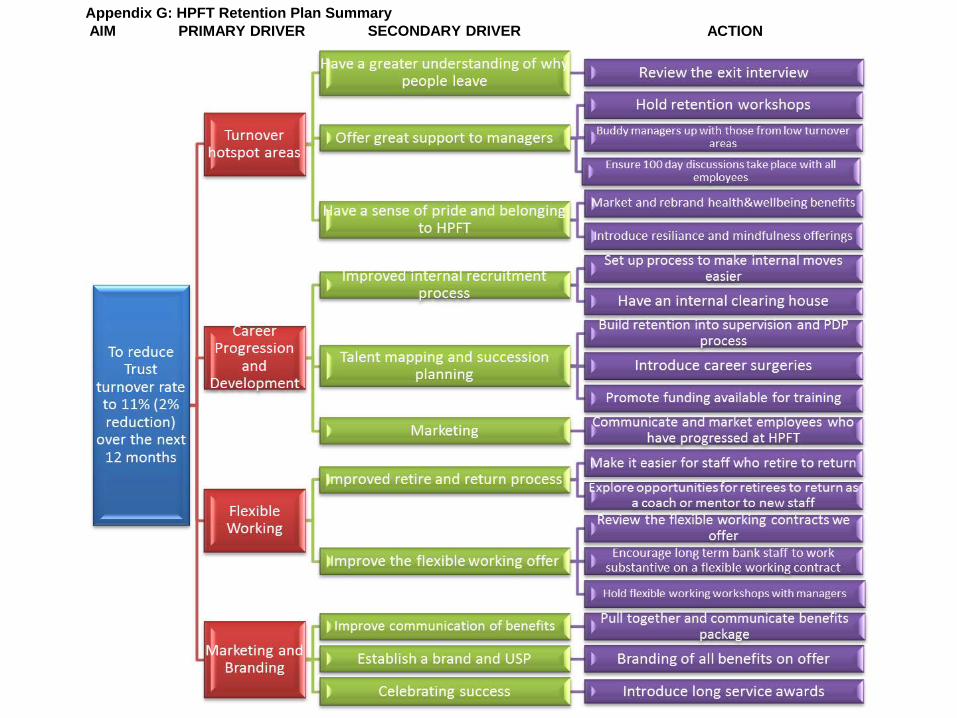
AIM PRIMARY DRIVER SECONDARY DRIVER ACTION
Appendix G: HPFT Retention Plan Summary

1
Appendix H:
SHARED CARE PROTOCOL FOR PHYSICAL HEALTH CHECKS All patients with Serious Mental Illness
Schizophrenia, Bi-polar disorders, or other Psychotic disorders
1. Principles and Scope
• This shared care protocol outlines how the responsibilities for physical health checks are shared between the secondary care specialist and general practitioner (GP).
• Sharing of care assumes effective and responsive communication between the specialist, the GP and the patient.
o The main method of communication between practitioners will be via email or telephone. Moving forward to 18/19 the information will be shared through electronic patient records.
o Communication with the patient will be face to face or over the telephone (with the exception of bookings an appointments which may be by letter or reminder text message).
This document sets out the responsibilities in the delivery of physical health checks for patients with serious mental illness (SMI). It has been developed following guidance from the Royal College of General Practitioners, Royal College of Psychiatrists, Royal College of Nursing and Rethink Mental Illness.1
NICE guidance informing this document CG178 QS80
It has also been cross-referenced to the Hertfordshire Partnership University Foundation Trust Physical Health Policy and co-created through the consultant body and GP membership.
2. Current Guidelines
• There is evidence that people with mental illness are at increased risk of medical disorders, and their life expectancy may be reduced by up to 20 years compared with the general population. People with severe mental illness, especially those with schizophrenia, have increased rates of impaired glucose tolerance, abdominal obesity and other cardiovascular risk factors. Many antipsychotic medications, particularly the atypical antipsychotics, are associated with significant metabolic health risks. These risk factors may be compounded by
1https://www.rcpsych.ac.uk/pdf/NAS%20Integrated%20Physical%20Health%20Pathway%20Dec%2012.pdf

2
increased rates of smoking; lifestyle factors and poor motivation for self-care or change.
• NICE guidelines suggest that people with a diagnosis that puts them at high risk, such as schizophrenia, bipolar disorder, or other psychotic illnesses should have an annual physical examination to include obesity measurement, cardiovascular assessment, smoking and alcohol intake evaluation and relevant blood tests including glucose and cholesterol measurements. People taking medication, such as atypical antipsychotics or lithium, that increases their physical vulnerability should also have the relevant physical investigations
3. Roles and Responsibilities for physical health checks
3.1 Responsibilities of secondary mental health services
The secondary care specialist will:
• Perform baseline physical health monitoring when starting or changing antipsychotic medication. (In acute presentations and based on clinical judgment, the initiation of treatment should not be delayed and the tests carried out as soon as is practical).
• Discuss all available treatment options with the person providing accessible information on the benefits and side effects (useful information at: http://www.choiceandmedication.org/hertfordshire/)
Physical Health checks will include: For anti-psychotics:
i) Family History
ii) Smoking status, Alcohol and illicit substance use status
iii) BMI or other obesity measure (weight and waist circumference), exercise and diet
iv) Blood pressure and pulse
v) Total cholesterol, LDL cholesterol, HDL cholesterol and triglycerides
vi) HbA1c and fasting glucose or random blood glucose*
Vii) Full blood count*
viii) ECG before starting anti-psychotic medication if: (there is family or personal history of CVD, if a physical health check indicates possible risk (e.g. blood pressure monitoring, if they are taking medication known to cause ECG abnormalities or if they are admitted as an inpatient).

3
ix) Liver function tests*
x) Prolactin*
Frequency of review: As a minimum review those prescribed a new antipsychotic at baseline, at least once after 3 months and annually thereafter. Health checks should take place at least annually unless an abnormality of physical health emerges. In these cases, appropriate action should be taken and/or the situation should be reviewed.
During physical health checks the health professional, should also be aware of wider public health issues (for example, dental care, encouraging annual flu jabs)
For patients on lithium medication:
Xi) Lithium Levels
xii) Thyroid function tests
xiii) Kidney function tests (urea and electrolytes)
xiv) Serum calcium levels
xv) Full blood count
(* The following results will be accessible to all clinicians and practitioners via ICE or Pathweb)
• Abnormal results should prompt a medication review by the consultant or psychiatrist, necessary intervention and referral process (as outlined in the Lester 2014 update at appendix 6) Patient information will be arranged. Useful information can be found at: http://www.choiceandmedication.org/hertfordshire/)
• The team psychiatrist will consider the results of the baseline tests when prescribing medication and notify the GP of any tests which are found to be outside of the normal range
• Titration of drug dosage and possible side effects will be monitored until a stable state is achieved.
• NICE guidelines indicate that weight will ideally be checked weekly for the first 6 weeks. In the community, the patient can be encouraged to do this outside of formal reviews and to keep a record to present at the formal reviews.
• All checks should be repeated at 12 weeks (informing the person of their results and sharing results with the GP).
• For patients started on antipsychotics and mood stabilisers, specific tests and additional monitoring is required as outlined above. Mental health services are responsible for monitoring physical health and medication side effects until the
4
person’s condition has stabilised. Responsibility may then transfer to primary care under this shared care protocol. This will be communicated via email to the GPs
• Ahead of a CPA review, a care coordinator will collate all relevant physical health information including information from the patients GP to capture any primary care intervention that has taken place. If an annual health check has not been carried out they should arrange appropriate checks in the appropriate service (which may be either the primary care service or HPFT physical health clinic).
• After the CPA review the updated care plan will be shared with the GP by email, including the physical health diagnosis, any monitoring requirements required and clarity on who will do this
• On discharge from secondary care inpatient services, a discharge notification summary should be emailed to the GP within 48 hours (including any physical health conditions identified since admission) and results of physical health checks conducted during admission
• Send an up to date care plan / CPA review to the GP within 2 weeks of the review
• Inform the GP if clozapine is being prescribed, as secondary care will then be responsible for the annual physical health check. The same will apply to all patients where secondary care continues to provide the regular prescription for any other anti-psychotic including depots
3.2 Responsibilities of the GP
The GP will:
• Be aware of and monitor the increased risk of diabetes, cardiovascular disease, hyperlipidaemia and hyperprolactinaemia in patients who suffer from SMI or are receiving regular anti-psychotics. (Appendix 1)
• Be aware of and monitor the potential complications of lithium toxicity in accordance with national and local guidelines. 2 (Appendix 2)
• Monitor for side effects and refer to psychiatrist for review of medication if necessary. Be aware of Neuroleptic Malignant Syndrome (a rare but potentially fatal side effect), as the individual will need to be referred to A&E immediately. (Appendix 3)
• Carry out physical health monitoring tests at least annually in stabilised patients, using practice case registers to monitor the physical and mental health of people with SMI in primary care.
2 http://www.nrls.npsa.nhs.uk/resources/type/alerts/?entryid45=65426

5
• GP or practice nurse to inform the person of the results and discuss relevant health promotion information. The results should also be shared with the named carer and care coordinator and stored in the electronic patient record
• Share summary record including physical health check results with secondary mental health services on initiation of treatment or admission to an inpatient setting
• Update the GP patient records with the information received from secondary care as part of their treatment and physical health assessments and act on any abnormal results that the GP has been alerted to.
4. In the event of non-attendance
There may be occasions when a person does not attend for their physical health check. In these circumstances:
• If the person is on CPA, then the care coordinator will proactively follow up to encourage attendance and make the relevant notes in the records. This could include supporting with GP appointments and support attendance as required.
• If the person has been discharged to primary care, then the GP will follow their practice policy for non engagement and update the patient records and inform the care coordinator
5. Further information
Additional information is available to secondary care professionals with a smartcard to log into the ‘summary care record’, which provides additional information from the GP systems. To enable the additional information in a patient record, the GP practice is required to take the patients consent (or make a best interest decision) and attach a code on the system to enable this. This process will ease the access of information across primary and secondary care3.
Hertfordshire Partnership University NHS Foundation Trust will regularly undertake a cross check of SMI Patients on CPA and QOF registers to ensure that all individuals at risk have access to appropriate care.
3 https://digital.nhs.uk/summary-care-records/additional-information

6
Appendix 1 - Management of hyperprolactinaemia
Hyperprolactinaemia is probably unavoidable in practice and even when not symptomatic may grossly affect hypothalamic function. It is more common in bipolar disorder and schizophrenia and is linked to longer term clinical consequences such as osteoporosis, hip fractures and possibly breast cancer. Long term use of prolactin elevating drugs should probably be avoided in young women given these risks.
Symptoms of raised prolactin: - Sexual dysfunction, Menstrual disturbances, Galactorrhoea, Gynaecomastia.
Reduced libido and infertility are usually seen with prolactin levels 600-1060Mu/L with galactorrhoea and amenorrhoea occurring when levels exceed 2012Mu/L.
Levels should be taken at baseline, 3 months and annually unless symptoms arise.
Normal prolactin or asymptomatic raised prolactin
Do not increase frequency of routine monitoring unless patient develops symptoms of raised prolactin.
Increased prolactin or symptomatic
1. Check clinical relevance. Consider other causes – pregnancy, lactation, stress, pathological causes e.g. pituitary tumour, hypothyroidism, chronic renal insufficiency, liver disease polycystic ovarian syndrome. 2. If no organic cause found refer back to Consultant Psychiatrist for medication review.
Prolactin Mu/L <550 (male) <600 (female)

7
Appendix 2 - Lithium
Main indications for use – Moderate to severe mania, prophylaxis of bipolar affective disorder & augmentation of an antidepressant.
Mechanism of action – unclear but is thought to influence second messenger pathways.
It is rapidly absorbed from the gastrointestinal tract but has a long distribution phase which is why blood samples should be taken 12 hours post dose in patients who are prescribed a single daily dose of a prolonged –release preparation at bedtime. Most of it is renally excreted so beware of drug interactions – see below. Therapeutic range 0.4 – 1.0mmol/L. Optimal range 0.6 – 0.75mmol/L.
Prescribing & monitoring (for further information refer to lithium guidelines)
Work up e-GFR and TFTs. Full blood count (a lithium may affect white count) ECG recommended in patients who have risk factors for CVD. Baseline measure of weight desirable. Baseline measure of corrected calcium may be helpful as lithium can cause hypercalcaemia
Prescribing Start at 400mg nocte (200mg in the elderly). Plasma levels after 7 days, then 7 days after every dose change until the desired level is reached.
Monitoring Plasma levels every 6 months but more frequent monitoring in the elderly, those prescribed interacting drugs and those with established renal impairment. e-GFR and TFTs every 6 months. Weight/BMI should be monitored. Monitoring of corrected calcium may be helpful as lithium can cause hypercalcaemia
Stopping Reduce slowly over at least 1 month. Avoid incremental reductions in plasma levels of >0.2mmol/L.
https://www.nbt.nhs.uk/sites/default/files/Lithium%20Monitoring%20-%20Statement%20Of%20Good%20Practice.pdf
Adverse effects
Mild GI upset, fine tremor, polyuria and polydipsia. Others – metallic taste, ankle oedema and weight gain. Medium to longer term effects – nephrogenic diabetes insipidus, hypothyroidism & hyperparathyroidism

8
Toxicity
GI – increasing anorexia, nausea and diarrhoea. CNS – muscle weakness, drowsiness, ataxia, coarse tremor and muscle twitching. Above 2mmol/L increased disorientation, seizures, coma and death.
Most risk factors for toxicity involve changes in sodium levels or the way the body handles sodium i.e. loss of sodium results in a rise in plasma levels (dehydration, low salt diets, drug interactions, Addison’s disease.
Drug group Magnitude of effect
Timescale of effect
Additional information
ACE inhibitors Unpredictable Up to 4 fold increases in [Li]
Develops over several weeks
7 fold increased risk of hospitalisation for Lithium toxicity in the elderly. Angiotensin II receptor antagonists may be associated with similar risk
Thiazide diuretics
Unpredictable Up to 4 fold increases in [Li]
Usually apparent in first 10 days
Loop diuretics are safer. Any effect will be apparent in the first month
NSAIDs Unpredictable From 10% to >4 fold increases in [Li]
Variable; few days to several months
NSAIDs are widely used on a prn basis Can be bought without a prescription

9
Appendix 3 - Neuroleptic Malignant Syndrome – a rare, but potentially serious or even fatal, adverse effect of all antipsychotics.
Signs & symptoms (presentation varies considerably) • Fever
• Rigidity
• Diaphoresis
• Confusion
• Fluctuating consciousness
• Fluctuating blood pressure
• Tachycardia
• Raised creatine kinase
• Leukocytosis
• Altered LFTs
This is a medical emergency that requires supportive treatment in general hospital

10
Appendix 4
General points on Antidepressants Most have been associated with hyponatraemia. All patients taking antidepressants should be observed for signs of hyponatraemia, particularly the elderly population.
• Dizziness
• Nausea
• Lethargy
• Confusion
• Cramps
• Seizures
They increase the risk of GI bleeds, again particularly in the elderly.
Administration of 2 serotonergic agents (one not necessarily being an SSRI) can result in Serotonin Syndrome
• Restlessness
• Diaphoresis
• Tremor
• Shivering
• Myoclonus
• Confusion
• Convulsions
• Death
Management is usually within a general hospital setting and constitutes discontinuation of the offending agents and supportive care.

11
Appendix 5 - Scope of the protocol
The scope of this shared care protocol is for patients with the following conditions. NB other patient groups (for example patients with eating disorder present with different physical needs in comparison to other mental health patients.
F10.5 Mental and behavioural disorders due to use of alcohol, Psychotic disorder F11.5 Mental and behavioural disorders due to use of opioids, Psychotic disorder F12.5 Mental and behavioural disorders due to use of cannabinoids, Psychotic disorder F13.5 Mental and behavioural disorders due to use of sedatives or hypnotics, Psychotic disorder F14.5 Mental and behavioural disorders due to use of cocaine, Psychotic disorder F15.5 Mental and behavioural disorders due to use of other stimulants, including caffeine, Psychotic disorder F16.5 Mental and behavioural disorders due to use of hallucinogens, Psychotic disorder F19.5 Mental and behavioural disorders due to multiple drug use and use of other psychoactive substances. Psychotic disorder F20.0 Paranoid schizophrenia F20.1 Hebephrenic schizophrenia F20.2 Catatonic schizophrenia F20.3 Undifferentiated schizophrenia F20.4 Post-schizophrenic depression F20.5 Residual schizophrenia F20.6 Simple schizophrenia F20.8 Other schizophrenia F20.9 Schizophrenia, unspecified F21.X Schizotypal disorder F22.0 Delusional disorder F22.8 Other persistent delusional disorders F22.9 Persistent delusional disorder, unspecified F23.0 Acute polymorphic psychotic disorder without symptoms of schizophrenia F23.1 Acute polymorphic psychotic disorder with symptoms of schizophrenia F23.2 Acute schizophrenia-like psychotic disorder F23.8 Other acute and transient psychotic disorders F23.9 Acute and transient psychotic disorder, unspecified F24.X Induced delusional disorder F25.0 Schizoaffective disorder, manic type F25.1 Schizoaffective disorder, depressive type F25.2 Schizoaffective disorder, mixed type F25.8 Other schizoaffective disorders F25.9 Schizoaffective disorder, unspecified F28.X Other nonorganic psychotic disorders F29.X Unspecified nonorganic psychosis F30.2 Mania with psychotic symptoms F31.2 Bipolar affective disorder, current episode manic with psychotic symptoms F31.5 Bipolar affective disorder, current episode severe depression with psychotic symptoms F32.3 Severe depressive episode with psychotic symptoms F33.3 Recurrent depressive disorder, current episode severe with psychotic symptoms
12
Appendix 6 - Lester tool

13
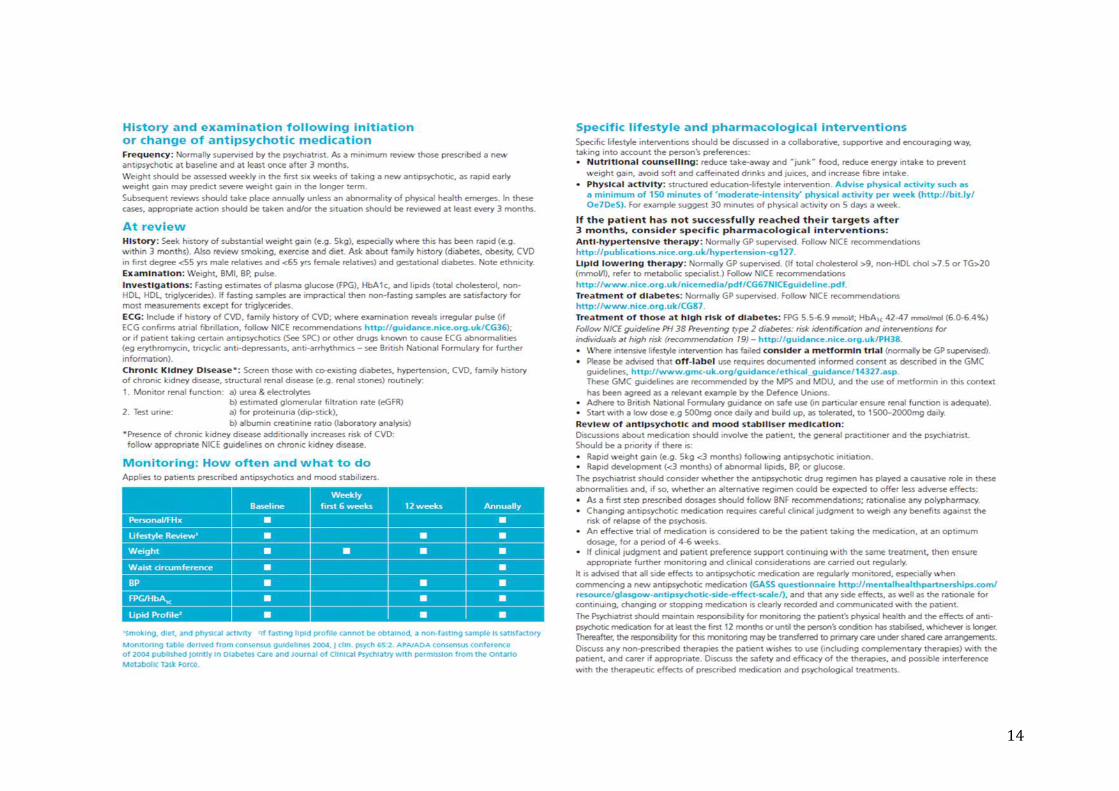
14

15

16
Version Control
Version Date Edits
V4 Oct 29th 2017 Includes edits from: - KD, JB, HP, AZ (HPFT) - AH, EW, MA, PM (CCG)
V5 Nov 1st Additional comments by pharmacy PM confirmed to circulate more widely Next version to consider the appendices and whether the embedded files and physical health check should be appendices
V6 Nov 14th Addition of ICD 10 Codes and scope Feedback from GPs Feedback from MSC HPFT
V7 Final edits AH
V8 Nov 23rd Post GP Leads Meeting
Page | 1
Agenda Item No: 13
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Workforce Report
Decision or Approval Discussion Information
Report author: Wendy Bourne, Senior Human Resources Business Partner
Report signed off by: Louise Thomas AD HR and ODL on behalf of Hein Scheffer, Director of Workforce
Executive Summary: The Quarter 2 workforce report summarises the workforce information run from the Electronic Staff Record (ESR) system from April 2016 to September 2017. The report covers all departments at East and North Herts CCG including HBLICT (Hertfordshire, Bedfordshire and Luton ICT). Information includes staff turnover rates, sickness absence rates and mandatory training compliance.
Appraisal return rates, and basic workforce equality information is stated as a snapshot at the end of September 2017.
The report also details the agency spend by directorate from April 2017 until September 2017.
Recommendations
to the members: The Governing Body is asked to note the Workforce Report for information.

Page | 2
Conflicts of Interest
involved:
No conflicts of interest identified
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the consequences of a commissioning decision.
Non-Financial Professional Interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career.
Non-Financial Personal Interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit.
Indirect Interests This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision.
1. Executive summary
The Quarter 2 workforce report summarises the workforce information run from the Electronic Staff Record (ESR) system and the report covers all departments at ENHCCG including HBLICT (Hertfordshire, Bedfordshire and Luton ICT). Information summarised from April 2016 until September 2017 includes staff turnover rates, sickness absence rates and mandatory training compliance.
Appraisal return rates and basic workforce equality information is stated as a snapshot at the end of September 2017.
The report also details the agency spend by directorate from April 2017 until September 2017.
Page | 3
2. Background
This is the first Workforce Report to be submitted to the Governing Body in this format.
3. Issues
N/A
4. Options
N/A
5. Resources implications
N/A
6. Risks/Mitigation Measures
N/A
7. Recommendations
The Governing Body is asked to review the Workforce Report.
8. Next Steps (including when the decision will be reviewed)
Workforce Report to be presented to the Governing Body twice a year during the business cycle. Quarter 4 as at the end of March 2018 will be presented to the Governing Body in May 2018.

East & North Herts CCG
Workforce ReportQuarter 2: 2017-2018
As at 30 September 2017
This Workforce Report provides an overview on key HR and ODL metrics as at end of Quarter 2 (30 September 2017). Areas covered include sickness absence, employee turnover, establishment, vacancy rates, training and equality monitoring
Table of Contents
Staff Turnover, Absence & Establishment ...................................................................................................................................................................................... 3
Workforce Establishment & Vacancy Rates ............................................................................................................................................................................... 3
Staff Turnover ............................................................................................................................................................................................................................. 3
Agency/Interim Spend ................................................................................................................................................................................................................. 3
Agency Spend by Directorate ....................................................................................................................................................................................................... 3
Sickness Absence ......................................................................................................................................................................................................................... 3
Absence Rate by Directorate ....................................................................................................................................................................................................... 3
ODL Activity & Workforce Equality Information ........................................................................................................................................................................... 4
Mandatory Training ..................................................................................................................................................................................................................... 4
Training Presented ....................................................................................................................................................................................................................... 4
Appraisal Rate .............................................................................................................................................................................................................................. 4
Workforce Profile by Pay Band .................................................................................................................................................................................................... 4
Pay by Age .................................................................................................................................................................................................................................... 4
Gender & Pay ............................................................................................................................................................................................................................... 4
Workforce Equality Information .................................................................................................................................................................................................... 5
Ethnicity & Pay ............................................................................................................................................................................................................................. 5
Starters – Ethnic Origin ................................................................................................................................................................................................................ 5
Age & Gender ............................................................................................................................................................................................................................... 5

Workforce Narrative – Q2 Report................................................................................................................................................................................................... 6
Narrative ...................................................................................................................................................................................................................................... 6
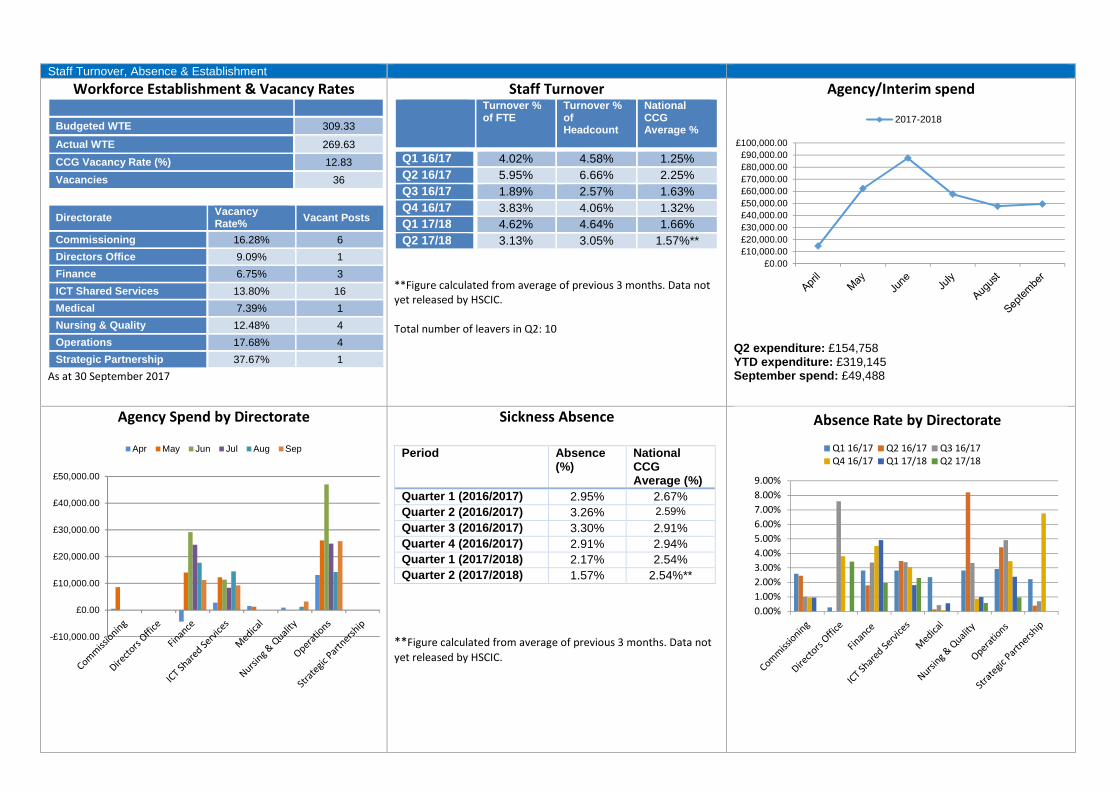
Staff Turnover, Absence & Establishment
Workforce Establishment & Vacancy Rates
Budgeted WTE 309.33
Actual WTE 269.63
CCG Vacancy Rate (%) 12.83
Vacancies 36
Directorate Vacancy Rate%
Vacant Posts
Commissioning 16.28% 6
Directors Office 9.09% 1
Finance 6.75% 3
ICT Shared Services 13.80% 16
Medical 7.39% 1
Nursing & Quality 12.48% 4
Operations 17.68% 4
Strategic Partnership 37.67% 1
As at 30 September 2017
Staff Turnover Turnover % of FTE
Turnover % of Headcount
National CCG Average %
Q1 16/17 4.02% 4.58% 1.25%
Q2 16/17 5.95% 6.66% 2.25%
Q3 16/17 1.89% 2.57% 1.63%
Q4 16/17 3.83% 4.06% 1.32%
Q1 17/18 4.62% 4.64% 1.66%
Q2 17/18 3.13% 3.05% 1.57%**
**Figure calculated from average of previous 3 months. Data not yet released by HSCIC.
Total number of leavers in Q2: 10
Agency/Interim spend
Q2 expenditure: £154,758 YTD expenditure: £319,145 September spend: £49,488
Agency Spend by Directorate Sickness Absence
Period Absence (%)
National CCG Average (%)
Quarter 1 (2016/2017) 2.95% 2.67%
Quarter 2 (2016/2017) 3.26% 2.59%
Quarter 3 (2016/2017) 3.30% 2.91%
Quarter 4 (2016/2017) 2.91% 2.94%
Quarter 1 (2017/2018) 2.17% 2.54%
Quarter 2 (2017/2018) 1.57% 2.54%**
**Figure calculated from average of previous 3 months. Data not
yet released by HSCIC.
£0.00
£10,000.00
£20,000.00
£30,000.00
£40,000.00
£50,000.00
£60,000.00
£70,000.00
£80,000.00
£90,000.00
£100,000.00
2017-2018
-£10,000.00
£0.00
£10,000.00
£20,000.00
£30,000.00
£40,000.00
£50,000.00
Apr May Jun Jul Aug Sep
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
7.00%
8.00%
9.00%
Absence Rate by Directorate
Q1 16/17 Q2 16/17 Q3 16/17Q4 16/17 Q1 17/18 Q2 17/18

ODL Activity & Workforce Equality Information
Overall Compliance Rate: 89.41%
Training Presented
Session Attendees
ENHCCG Induction 9
Mandatory Training Session 17
Interview Skills 6
Performance Management 8
Common Cultures Listening Event 3
Overall Compliance Rate: 79.29%
Acronyms VSM – Very Senior Manager Non AFC – Non Agenda for Change
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Mandatory Training Compliance
2016-2017 2017-2018 IG Compliance 17-18
0
10
20
30
40
50
60
Appraisal Returns
Active Headcount Returns
2 4
4336
5160
3124
14 12 124
60
10
20
30
40
50
60
70
Number of Employees by Pay Band
Workforce Profile by Pay Band
Band 2 Band 3 Band 4 Band 5 Band 6
Band 7 Band 8a Band 8b Band 8c Band 8d
Band 9 Non AFC VSM 0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pay by Age
<20 yrs 20-29 yrs 30-39 yrs
40-49 yrs 50-59 yrs 60-70 yrs
1.75%
0.88%
14.04%
14.04%
16.67%
15.79%
7.02%
8.77%
5.26%
3.51%
0.88%
9.65%
1.75%
0.00%
1.55%
13.92%
10.31%
16.49%
21.65%
11.86%
7.22%
4.12%
4.12%
0.00%
6.70%
2.06%
30% 20% 10% 0% 10% 20%
Band 2
Band 3
Band 4
Band 5
Band 6
Band 7
Band 8a
Band 8b
Band 8c
Band 8d
Band 9
Non AFC
VSM
Gender & Pay
Female Male

Workforce Equality Information
Ethnicity & Pay Pay Band
BME Other Undisclosed White
Band 2 100.00% - - -
Band 3 - 25.00% - 75.00%
Band 4 20.93% - - 79.07%
Band 5 30.56% 2.78% 2.78% 63.89%
Band 6 19.61% - 3.92% 76.47%
Band 7 23.33% 3.33% 3.33% 70.00%
Band 8a 25.81% - - 74.19%
Band 8b 8.33% 8.33% - 83.33%
Band 8c 7.14% - 7.14% 85.71%
Band 8d 16.67% - - 83.33%
Band 9 - - - 100.00%
Non AFC 37.50% 8.33% 8.33% 45.83%
VSM - - - 100.00% 0
1
2
3
4
Band 4 Band 5 Band 7 Non AFC
Starters by Ethnic Origin
A White - British D Mixed - White & Black Caribbean
E Mixed - White & Black African F Mixed - White & Asian
H Asian or Asian British - Indian K Asian or Asian British - Bangladeshi
Undefined Z Not Stated
0.00%
14.04%
26.32%
32.46%
20.18%
7.02%
1.03%
9.28%
20.62%
29.38%
30.93%
8.76%
40% 20% 0% 20% 40%
<20 yrs
20-29 yrs
30-39 yrs
40-49 yrs
50-59 yrs
60-70 yrs
Age & Gender
Female Male
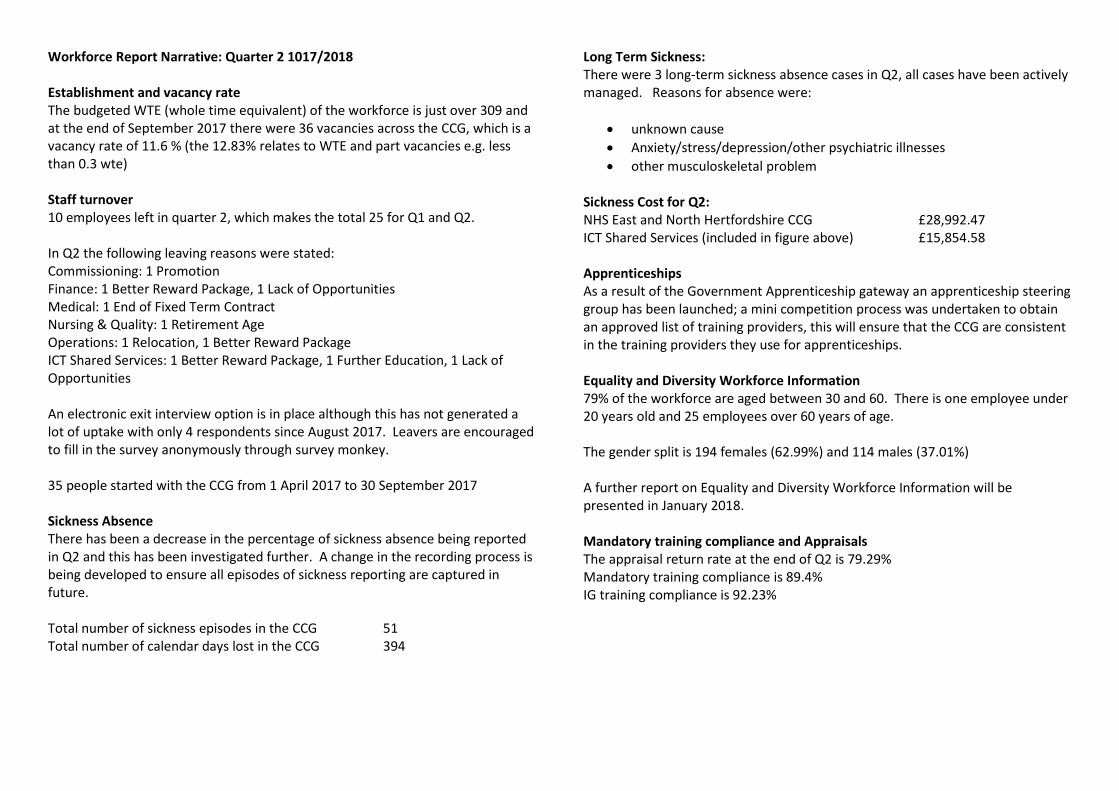
Workforce Report Narrative: Quarter 2 1017/2018
Establishment and vacancy rate The budgeted WTE (whole time equivalent) of the workforce is just over 309 and at the end of September 2017 there were 36 vacancies across the CCG, which is a vacancy rate of 11.6 % (the 12.83% relates to WTE and part vacancies e.g. less than 0.3 wte)
Staff turnover 10 employees left in quarter 2, which makes the total 25 for Q1 and Q2.
In Q2 the following leaving reasons were stated:Commissioning: 1 Promotion Finance: 1 Better Reward Package, 1 Lack of Opportunities Medical: 1 End of Fixed Term Contract Nursing & Quality: 1 Retirement Age Operations: 1 Relocation, 1 Better Reward Package ICT Shared Services: 1 Better Reward Package, 1 Further Education, 1 Lack of Opportunities
An electronic exit interview option is in place although this has not generated a lot of uptake with only 4 respondents since August 2017. Leavers are encouraged to fill in the survey anonymously through survey monkey.
35 people started with the CCG from 1 April 2017 to 30 September 2017
Sickness Absence There has been a decrease in the percentage of sickness absence being reported in Q2 and this has been investigated further. A change in the recording process is being developed to ensure all episodes of sickness reporting are captured in future.
Total number of sickness episodes in the CCG 51 Total number of calendar days lost in the CCG 394
Long Term Sickness: There were 3 long-term sickness absence cases in Q2, all cases have been actively managed. Reasons for absence were:
• unknown cause
• Anxiety/stress/depression/other psychiatric illnesses
• other musculoskeletal problem
Sickness Cost for Q2: NHS East and North Hertfordshire CCG £28,992.47 ICT Shared Services (included in figure above) £15,854.58
Apprenticeships As a result of the Government Apprenticeship gateway an apprenticeship steering group has been launched; a mini competition process was undertaken to obtain an approved list of training providers, this will ensure that the CCG are consistent in the training providers they use for apprenticeships.
Equality and Diversity Workforce Information79% of the workforce are aged between 30 and 60. There is one employee under 20 years old and 25 employees over 60 years of age.
The gender split is 194 females (62.99%) and 114 males (37.01%)
A further report on Equality and Diversity Workforce Information will be presented in January 2018.
Mandatory training compliance and Appraisals The appraisal return rate at the end of Q2 is 79.29% Mandatory training compliance is 89.4% IG training compliance is 92.23%

Page | 1
Agenda Item No: 14
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: Draft – Remuneration Committee Terms of Reference
Decision or Approval Discussion Information
Report author: Sarah Feal, Company Secretary
Report signed off by: Linda Farrant, Lay Member Governance and Audit
Executive Summary: The Terms of Reference for the Remuneration Committee have been reviewed and updated.
The proposed amendments are shown in the document.
Recommendations
to the members:
To approve the Terms of Reference for the Remuneration
Committee
Conflicts of Interest
involved:
There are none perceived.
Page | 2
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

Page | 1
Remuneration Committee
Terms of Reference v3.0
Page | 2
1. Introduction 1.1 The Remuneration Committee (the committee) is established in accordance with
section 6 of NHS East and North Hertfordshire Clinical Commissioning Group’s Constitution, as a committee of the Governing Body.
2. Membership 2.1 The membership of the committee shall include:
Lay Member – Governance and Audit (Chair)
Deputy Chair (Clinical)
Secondary Care Specialist Doctor
2.2 Representatives in attendance The following representatives will usually be in attendance:
Company Secretary
Chief Finance Officer
Chief Executive (Accountable Officer)
Director of Workforce
2.3 No one other than the members of the committee is entitled to be present at committee meetings.
2.4 The committee may invite any person to attend meetings to provide advice and/or expertise as required. Any such person shall not be a member of the committee and shall withdraw upon request.
3. Quorum 3.1 All members of the committee must be present for the quorum to be established.
3.2 No formal business shall be transacted where a quorum is not reached.
4. Frequency of meetings and attendance 4.1 A minimum of one scheduled meeting shall be held per year.
4.2 Members of the committee should make every effort to attend all meetings of the committee. The Secretary to the committee will monitor attendance and will report on this annually. Attendance figures will be published in the Annual Report.
5. Authority 5.1 The committee is authorised by the Governing Body to:
Obtain legal advice, remuneration or other professional advice, including the
appointment of external advisor and/or consultants, related to its functions as it
deems fit at the expense of the Clinical Commissioning Group.
The committee shall recommend appropriate action(s) should be taken by the
Governing Body in allowing the committee to fulfill its terms of reference.

Page | 3
6. Emergency powers 6.1 Where an urgent decision needs to be made in between scheduled meetings,
members of the committee can convene an Extra-ordinary meeting to discuss a particular issue. Quorum rules in paragraph 3 still apply.
6.2 If it is not practicable to meet in person, matters can be dealt with through telephone or the exchange of emails. The exercise of such powers shall be reported and minuted at the next committee meeting.
7. Duties 7.1 The duties of the committee can be categorised as follows:
7.1.1 to have delegated authority to determine the policy regarding contracts of employment, where applicable, and remuneration of the members of the Governing Body and Very Senior Managers;
7.1.2 to have delegated authority to determine the individual remuneration arrangements for members of the Governing Body and Very Senior Managers, taking into account feedback on performance from the Chair or Chief Executive.
7.1.3 to determine remuneration for those referred to above and in doing so the committee shall review and agree:
a. overall market positioning of the remuneration package;
b. individual base salaries and increments (where applicable);
c. any annual and/or long term incentive arrangements and the relevant targets for
performance related schemes.
7.1.4 to consult with the Chief Executive (Accountable Officer) and Chair of the Governing Body in relation to their proposals relating to the remuneration of members of the Governing Body and Very Senior Managers;
7.1.5 to approve any changes to the standard contract of employment for members of the Governing Body and Very Senior Managers, where applicable, including termination arrangements taking into account relevant guidance and current good practice;
7.1.6 to agree terms for the termination of a contract having regard to HM Treasury guidance and current good practice, including any redundancy or exit packages;
7.1.7 to determine remuneration policy and packages with regard to the group’s overarching reward and benefit strategy for staff, the arrangements in the wider health service, guidance from HM Treasury and current good practice;
7.1.8 to have oversight of Off-payroll working through an intermediary (IR35);
7.1.9 to provide a statement in the annual report to include:
a. the remuneration received by members of the Governing Body and Very Senior
Managers;
b. Membership of the Remuneration Committee. This means the names of the
members and the Chair;
Page | 4
c. the number of meetings of the committee and those members who attended
each meeting;
d. the name of any person, including any employee of the clinical commissioning
group, who provided advice and/or services to the committee in the exercise of
their functions. Where such a person is not a member of the Very Senior
Managers: a description of the nature of any other services that person has
provided to the group during the financial year and whether that person was
appointed by the committee must be published; and
e. undertake any other duties as directed and authorised to undertake by the
Governing Body and / or the Council of Members.
8. Reporting arrangements to the Governing Body 8.1 The committee will report to the Governing Body on an annual basis and the following
documents will be presented:
Minutes of the committee’s meetings.
9. Reporting arrangements of other Committees and Groups 9.1 There are none identified.
10. Annual review of the Committee 10.1 The committee will:
Review that these Terms of Reference have been complied with and whether they
remain fit for purpose;
Determine whether its planned activities and responsibilities for the previous year
have been sufficiently discharged; and,
Recommend any changes and / or actions it considers necessary, in respect of the
above.
11. Committee servicing 11.1 The committee shall be supported administratively by the Company Secretary (or other
nominated representative), who’s duties in this respect will include:
Agreement of the Agenda with the Chair and collation of papers;
Providing written notice of meetings to committee members, and the papers, not
less than 5 working days before the meeting;
Taking the minutes and keeping a record of matters arising and issues to be
carried forward;
Producing a single document to track the committee’s agreed actions and report
progress to the committee;
Producing draft minutes for approval within 5 working days of the meeting.
Submit the draft minutes to the Human Resources Department to update staff
records.

Page | 5
Terms of Reference reviewed by: Remuneration Committee
Review Date: 27th November 2017
Governing Body Approval Date: 18th January 2018
Next Review Date: January 2019

Page | 1
Agenda Item No: 15
Date of Meeting: 18 January 2018
Governing Body Meeting in Public
Paper Title: Governance and Audit Committee Minutes
Decision or Approval Discussion Information
Report author:
Report signed off by: Governance and Audit Committee
Executive Summary: Approved minutes of the Governance and Audit Committee attached for the Governing Body to note
Recommendations
to the members:
To note the minutes of the Governance and Audit Committee
Conflicts of Interest
involved:
n/a
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.
1 | P a g e
Governance and Audit Committee
Wednesday 15 November 2017
Charter House, 1st Floor Room MR1.2, Welwyn Garden City
MINUTES
Present:
Dianne Desmulie [DD] Lay Member, Patient and Public Engagement
Linda Farrant [LF] Lay Member, Governance and Audit (Chair)
Nicky Williams [NW] Deputy Chair
In Attendance:
Lisa Clampin [LC] Lead Partner BDO, External Audit
Jas Dosanjh [JD] Corporate Governance Manager (Minutes)
Sarah Feal [SF] Company Secretary
Sheilagh Reavey [SR] Director of Nursing and Quality (item 6)
Chris Rising [CR] Senior Manager RSM, Internal Audit
Alan Pond [AP] Chief Finance Officer

2 | P a g e
Item Subject Action by
1. WELCOME AND APOLOGIES FOR ABSENCE
The Chair welcomed all to the meeting.
Apologies were noted from:
Becci Goodchild [BG], Principal Consultant RSM, Nick Bernstein [NB], Audit Manager BDO, External Audit.
2. DECLARATIONS OF INTERESTS
The Chair invited the committee members to reconfirm their current declarations on the Register of Interests and advise of any new interests. All members confirmed their declarations were accurate and up-to-date.
The Chair invited the committee members to declare any interests relating to matters on the Agenda. All members confirmed they have no declarations in relation to matters on the Agenda.
3. MINUTES OF PREVIOUS MEETING AND MATTERS ARISING
The minutes of the meeting held on 06 September 2017 were approved as an accurate record.
Matters arsing included a discussion regarding the agreed re-appointment of the current internal auditors (RSM) for another year (2018/19), as agreed at the previous meeting.
ACTION: AP to formalise extension of internal audit contract. AP
4. COMMITTEE ACTION TRACKER
The contents of the Action Tracker were discussed and all actions highlighted in yellow were agreed to be closed.
CR advised that the one open action regarding the scheduling of an advisory internal audit of Continuing Healthcare (CHC) is currently being agreed with AP.

3 | P a g e
Item Subject Action by
DD queried whether the CHC audit will also include a review of outcomes. AP confirmed that the audit will be looking at internal processes and value for money. SR advised that the Quality Committee will be receiving a report from CHC and patient feedback can be considered as part of this review.
The Committee noted the updates for the action tracker.
5. FINANCE
5.1 FINANCE RISKS UPDATE REPORT
AP presented the finance risks update report and advised that the CCG is currently managing potential risks of £1.6m which may impact the delivery of the CCG target financial position if crystallised. The risks include QIPP under-delivery, Continuing Healthcare (CHC) growth in number and complexity of activities, prescribing risks and system-wide risks. Financially, these risks are currently mitigated by the contingency reserve held by the CCG.
AP advised that other issues include;
under performance of provider contracts,
savings retained centrally by NHS England (i.e. from the reduction in generic drug prices with benefits that would otherwise accrue to the CCG),
revised contract with new patient transport service provider likely to be at a higher cost (following winding up order and administration of current provider and transitional arrangements in place with East of England Ambulance Service).
The Committee noted the Financial Risks update report.
5.2 WAIVERS OF STANDING ORDERS
The Committee noted that there have been no waivers of standing orders since last reported.

4 | P a g e
Item Subject Action by
6. QUALITY COMMITTEE
6.1 QUALITY ASSURANCE REPORT
SR presented the Quality Assurance Report which provided updates from the Quality Committee meeting held on 14 September 2017. LF highlighted that the main concerns outlined in the report have already been escalated to the Governing Body and they are aware of the actions being taken.
SR provided an overview of the concerns identified from the ongoing review of;
Hertfordshire Partnership Foundation Trust – regular review of workforce and recruitment issues
Hertfordshire Community Trust – regular review of diabetic remedial action plan
Barnet and Chase Farm Hospital (Royal Free Foundation Trust) – regular review of key performance indicators
Princess Alexandra Hospital Trust – continues in special measures, high vacancies and long ED delays, the risk regarding Rheumatology is now on the RCAD
East and North Hertfordshire Trust – concerns regarding cancer target, discharge summaries, sepsis performance, and care issues have not been mitigated with unknown outcomes from the implementation of the new system (Lorenzo). There will be focused report presented for review at the Quality Committee meeting in December 2017
East of England Ambulance Service – ongoing monitoring of performance, handover delays and vacancies
Herts Urgent Care – continued routine monitoring, the risk regarding base closures and workforce has been added to the RCAD
Private Ambulance Services – received a winding up notice from HMRC on 28 September 2017 and went into administration on 2 October 2017; East of England Ambulance Service provided a rescue package and the caretaker services. Issues have been escalated to NHSE and NHSI

5 | P a g e
Item Subject Action by
LF advised that the internal auditors have been asked to carry out a review of the patient transport service contract and provider management, to identify lessons learned. AP commented the other three CCGs want to carry out a similar review and for this to be undertaken jointly reflecting the consortium arrangements.
ACTION: AP and CR to discuss the mechanisms and agree the parameters of the patient transport service internal audit to incorporate all four CCGs.
The following policies have been reviewed and approved: Safeguarding Adults Policy Serious Incident Policy Complaints Policy
The Committee noted the Quality Assurance Report.
6.2 QUALITY COMMITTEE MINUTES
The Committee noted the approved minutes of the Quality Committee meeting held on 15 June 2017.
AP/CR
7. RISK MANAGEMENT
7.1 RISK PROFILE REPORT
JD presented the Risk Profile Report which includes the Strategic Risk Register (SRR) and Risks, Controls and Assurance Dashboard (RCAD) which were reviewed across the CCG between June and August 2017 and signed off at the Executive Team Meeting on 07 November 2017.
Following the review, 7 risks remain on the SRR and there are now 36 risks on RCAD and the key findings identified since the last update in September 2017 were:-
10 risks have been mitigated to a lower risk rating (ID 4.1, 5.24 and Strategic Risk 5),
21 risks remain at the same risk rating (ID 1.32, 1.33, 1.50, 1.54, 3.4, 5.4, 5.8, 5.12, 5.22, 5.25),
1 risk has seen an increase of its risk rating (ID 1.10), 3 risks have been mitigated and closed, 5 new risks have been identified and added.

6 | P a g e
Item Subject Action by
The Committee discussed mitigation for Strategic Risk 3 and whether the STP work streams have reduced the current risk. All agreed that the outcomes of streamlined processes delivered with fewer additional resources are yet to materialise from the collective and joint collaboration approach. It was agreed that the risk should remain at its current risk rating.
The Committee noted the SRR and RCAD and approvedsubmission to the Governing Body.
8. INTERNAL AUDIT PROGRESS REPORT
CR presented the Internal Audit Progress Report which details the results of Internal Audit work undertaken for the year.
The following reports 2017/18 have been finalised by the CCG since the Governance and Audit Committee meeting in September 2017:
Prescribing - Delivery of QIPP Schemes (substantial assurance) – with three low recommendations.
Delivery of the Financial Plan, including QIPP (substantial assurance) – with two low recommendations.
Business Continuity Planning, including HBL ICT (substantial assurance) – with no recommendations or weaknesses.
General Data Protection Regulations Compliance (advisory) – with five general recommendations.
It was noted that the GDPR training session organised by Jennie McCollin was very successful.
LC questioned whether the projected completion date for recommendation 5 was realistic, SF confirmed that there is a GDPR working group that meet monthly to ensure all actions are on track.
ACTION: SF to share GDPR implementation plan with LF. SF
7 | P a g e
Item Subject Action by
Delivery of IAPT (substantial assurance) – with one low recommendation.
LF queried whether the Joint Commissioning Partnership Board administration is as robust as stated within the audit. CR and SF advised that the governance arrangements have been reviewed and this was observed during the audit.
Conflicts of Interest (reasonable assurance) – with two medium and three low recommendations.
CR advised that this is a similar position to other clients, and proactive reviews will tighten up the process. SF confirmed that the new process for obtaining declarations will be rolled out from the end of November 2017 with planned completion by March 2018.
LF thanked CR for completing the audits to plan and acknowledged that the CCG audit leads have contributed to the completion by adhering to the process.
The Committee noted the Internal Audit Progress Report.
9. COUNTER FRAUD PROGRESS REPORT
CR presented the Counter Fraud Progress Report on behalf of BG and advised that a complete fraud risk assessment for the year is currently being completed.
CR questioned whether the Committee would like to review this at the next meeting. The Committee agreed to receive the assessment via email and to bring to the January Committee meeting if there are any issues/concerns which need to be discussed.
ACTION: BG to circulate fraud risk assessment to Committee members for information (if concerns are identified then this is to be added for review at the January Committee meeting).
The Committee noted the Counter Fraud Progress Report.
BG

8 | P a g e
Item Subject Action by
10. EXTERNAL AUDIT UPDATE
LC provided a verbal update and confirmed that an introduction and scoping meeting had taken place with AP and Beverley Flowers.
LC advised that a meeting has been scheduled with the previous External Auditors taking place later this month.
LC confirmed that they are still on track for reporting in line with the agreed timescales.
The Committee noted the External Audit update provided.
11. AUDIT RECOMMENDATIONS TRACKER
The Audit Recommendations Tracker was reviewed by the Committee and progress reviewed.
The actions highlighted in yellow were agreed to be closed as the recommendations have been implemented:
Information Governance (16/17) – IA Ref. 1.4 and 1.8 Conflicts of Interest (16/17) – IA Ref. 1, 4, and 5 Effectiveness of the Case Management System (16/17) – IA
Ref. 1.3 QIPP and Financial Planning (17/18) – IA Ref. 2, 3 and 7 Conflicts of Interest (17/18) – IA Ref. 1.1.1, 1.1.2, 1.1.4 and
1.1.7 Delivery of Improving Access to Psychological Therapies
(17/18) – IA Ref. 1.1.9
The updates for open recommendations were reviewed and noted:
Cyber Security – IA Ref. 3.12 has an implementation date of December 2017
Effectiveness of the Case Management System (16/17) – IA Ref. 1.1, 1.2, 1.5, 1.6 and 1.7 have an implementation date of March 2018
Patient Engagement (16/17) – IA Ref. 1.1, 1.2 and 1.3 have revised implementation dates of August 2018, it was noted this was due to a member of the team retiring soon
Conflicts of Interest (17/18) – IA Ref. 1.6 has an implementation date of March 2018
9 | P a g e
Item Subject Action by
Delivery of the Financial Plan, including QIPP (17/18) – IA Ref 1.1.4 and 1.1.7 have implementation dates of December 2017 and 30 November 2017 respectively
Prescribing, Delivery of QIPP Schemes (17/18) – IA Ref 2, 4 and 5 have implementation dates of 30 November 2017, January 2018 and December 2017 respectively
GDPR Governance Advisory Audit (17/18) – IA Ref. 1, 2, 3, 4 and 5 have implementation dates of March 2018
The Committee noted the progress made with the implementation of recommendations on the tracker.
13. ANY OTHER BUSINESS
13.1 NHS Audit Committee Chairs Forum
LF advised that the main themes from the NHS Audit Committee Chairs Forum were:
challenging financial positions for CCGs and providers, STP progress, the recent cyber-attack.
LF queried whether we have assurance that the CCG is compliant with data security and protection requirements and whether we need to seek assurance from providers that they compliant.
AP advised that the CCG receives assurance from HBL ICT via the work carried out by the HBL ICT Stakeholder Board. In relation to seeking assurance from providers, this is already sought by other bodies/mechanisms (i.e. IG Toolkit submissions) and therefore we would be duplicating processes if we were to seek assurance.
The Committee agreed that an assurance report should be provided regarding the CCG’s compliance with data security requirements and assurance from HBL ICT.
ACTION: AP to advise Phil Turnock that a report is required regarding the HBL ICT data security arrangements and assurance to the Committee via a deep-dive review at the meeting in January 2018.
AP/ PT

10 | P a g e
Item Subject Action by
SF queried whether the CCG required insurance specifically for cyber security.
ACTION: SF to review current insurance arrangements with NHS Resolution to assess whether cyber security claims would be covered by the policy.
The Committee noted the update provided by LF.
13.2 Committee Dates for 2018/19
The Committee discussed the meeting dates scheduled for 2018/19 and all confirmed that they have the dates in their diaries.
LC and AP proposed that the meeting scheduled to take place in May will be too early in terms of reporting the outcomes of the External Audit review and should therefore be rearranged to a later date that month.
It was noted that rescheduling the meeting could impact on the collation of papers for the Governing Body meeting in Public, at which the Annual Report will be signed off. LF and AP advised that the Annual Report will be reviewed in depth by the Governance and Audit Committee in March and therefore any amendments requested by the Committee at the meeting in May would be presented as a summary sheet to the Governing Body with Annual Report.
The Committee agreed that the Governance and Audit Committee meeting scheduled for 09 May 2018 should be rescheduled to 16 May 2018.
ACTION: JD to reschedule the May 2018 Governance and Audit Committee to 16 May 2018 and update invites accordingly.
SF
JD
12. ANNUAL CYCLE OF BUSINESS 2017-18
The Committee reviewed the Annual Cycle of Business.
ACTION: JD to update the Annual Cycle of Business:
add Deep Dive into HBL ICT Data Security to the Committee meeting schedule for January 2018,
JD

11 | P a g e
Item Subject Action by
if required, add Counter Fraud Risk Assessment to the January meeting following confirmation by LF,
review reporting scheduled for the Information Governance items to ensure they reflect the timeline agreed at the previous Committee meeting.
The Committee noted the Annual Cycle of Business for 2017-18.
14. DATE OF NEXT MEETING
Wednesday 10th January 2018: 10:00am – 12:30pm Charter House, 1st Floor MR1.2, Welwyn Garden City

Page | 1
Agenda Item No: 16
Date of Meeting: 18th January 2018
Governing Body Meeting in Public
Paper Title: HBL ICT Stakeholder Board Minutes
Decision or Approval Discussion Information
Report author:
Report signed off by: HBL ICT Stakeholder Board
Executive Summary: Approved minutes of the HBL ICT Stakeholder Board attached for the Governing Body to note
Recommendations
to the members:
To note the minutes of the HBL ICT Stakeholder Board
Conflicts of Interest
involved:
n/a
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

HBL ICT Stakeholder Board Meeting - Minutes
Monday, 18th September 2017 at Charter House, WGC
Present: Alan Pond, CFO E&NH CCG (Chair) Phil Turnock, Director Shared Services HBL ICT Keith Fairbrother, Hd. Technical Services HBL ICT Liz Cox, Deputy CFO Luton CCG Peter Collins, Hd. IM&T Integration & Service Delivery HPFT
1 Apologies
Caroline Hall, CFO HVCCG Trudi Mount, IM&T HVCCG Ben Jay, CFO Beds CCGMalcolm Miller, Deputy CFO Beds CCG Phil Bradley, CFO HCT Billy Aspinall, AD Performance & Information HCT Alan Davies, CFO Luton CCG John Bennett, IM&T HPFT Ronke Akerele, AD HPFT
Welcome: Peter Collins, HPFT
Actions
2 Register any Conflict of Interest - None
3 Minutes from previous meeting & matters arising (document provided)
Minutes from 17/7/17 approved. Actions updated – see Action Log.
4 Finance Report – Period 5 (document provided) AP reported an overall small overspend of £30. Pay underspend relates to current vacancies & savings. Final position satisfactory.
Income - HUC costs 2016/£16K but for current year - £70k. HUC are moving out of Ascot Lane and therefore services required from HBL ICT will change but they will still need to pay if access to our network/firewalls is required at any of their selected sites. Exit cost payable by HUC. PT has presented HUC with a new invoice and schedule which we envisage will be disputed by HUC
PT to discuss with 1) D ArcherHUC & 2) Beds/Luton CCG
5 Service Performance August 2017 (document provided) 5.1 Service Statement - this summarises all service performance documents provided for this meeting. Main KPI is still below target although the volume of ‘aged calls’ are still a concern. Starting a review of stats. classification as not all calls are ‘incidents’ so need to be correctly identified from the outset as this impacts on the service levels. Also bank staff’s accounts are usually set up immediately without having SLA in place; account locked out after 30 days of non use. Use of reset tool started to increase (gradually). PT explained the process: graphs indicate users of SpecOps to reset passwords. ServiceNow monitors number of calls received in total. To avoid duplication, group asked for comparison of 1) staff doing resets themselves. 2) resets via the Service Desk using SpecOps 3) resets via Service Desk using AD. Also capture & analyse what’s happening between Service Desk & self service facility. Identify organisations that are still not encouraging staff to use SpecOps. KF to ascertain breakdown of user usage of SpecOps and analysis against service calls ICT BRMs encouraged by the positive feedback from partners.
Duty Manager – position created 1/8/17 and is going well. New phone system introduced on 17/8/17. Weekend working & extended support hours need to be reviewed if we are to develop technical performance (2
nd line engineers) & recruit the relevant skills.
Extended support is very labour intensive & costly; this is also unpopular with some technical staff, who have moved away & accepted different positions within HBL. The possibility of 3
rd party supplier operating the weekend working put to Steering Group.
This was rejected as group preferred that out of hours working was adjusted to suit.
Risks are going down and overall improved. Infrastructure in a better position than it was - more stable & less outages. Remaining items to be moved: domain controllers moving into DC w/c 18/9/17. Comms Room on 1
st fl Charter House being revamped to house all data
lines, that come into the building.
KF
PT/KF briefly explained the resilience of the DC and the monitoring of component failure.
HPFT stated that overall the service is good.
5.2 HBL KPIs August 2017
5.3 Call Agent’s Stats
5.4 GPIT KPIs June 2017
6 HSCN – N3 Replacement (document provided)
PT stated that BLMK STP (Beds, Luton & Milton Keynes STP) has asked HBL to lead on the procurement side for a number of organisations mainly around Beds, Luton & Milton Keynes as well as anyone in the HBL partnership, Herts & West Herts Hospitals. E&NH Hospitals have not committed to it & unsure how they do their N3 replacement. This will start Nov 2017 once suppliers have been vetted. Bulk of N3 is GP land (£600K), Acute Trust (£150K), HBL (£35K) Rem. (£30K ). Each organisation will have an individual contract with the new N3 supplier – HBL will have no involvement outside of the procurement activity.
West Essex have joined the ‘Essex Coin Collaborative Procurement’. E&NH Trust not yet confirmed their N3 Replacement procurement status.
AP stated that we need to have contracts before procurement in place for those whom HBL will manage. All must to agree to design specification to go forward or opt out before process begins. Main N3 circuit does not cover other subsidiary services i.e. IPT. N3 offers extra BT overlay services bought separately. AP emphasized the key importance of technical design and what organisations want it for – need to be able to get to their applications wherever they are. 4x CCGs to decide where to go with this with their GPs. 2x Herts CCGs do want GPs to be linked up to our network, 2x Beds/Luton CCGs do not want this. Milton Keynes as yet undecided. Possibility that hospices/care homes could join our geographical network footprint area at a later stage.
7 Microsoft Licensing for GPIT (document provided) Prices will increase as from June 2018. Issues with supporting older model (Windows7) especially around Beds – requirement is to go with Windows10. Possible way to reduce MS licencing bill would be to purchase just CALS as we would no longer need the ‘Core’ CALS current connection to the server, exchange & sequel. With NHSmail2, exchange no longer needed. The operating system is the expensive part of the system.
Beds CCG now moved to ITS for overall IT support. Licences for GPs – we can either 1) buy from Microsoft Products & Service Agreement (MPSA) 3 year support or 2) EA subscription based. Either scheme would be capital funded by NHSE. Prices will significantly increase 2018 – from £19 per licence to £40 across the patch. PT proposes that MPSA perpetual licences is the way forward for GPIT as there would be the opportunity to upgrade at a later stage (Year 4 onwards) i.e operating system. Patching will be available while in support. AP stated that over the 4 year period, it is still cost effective to buy the licences up front as long as NHSE has the capital funding to allocate for the purchasing of perpetual licences.
Licences would have to be identified to GP practices and their successors. Ownership of the licence needs to be clear i.e. whom it belongs to. Needs to be protected for the practices so that we can maintain the ownership within the partnership & CCGs. Licences can be purchased as & when required. If capital is not available, it will be a problem as no funds have been set aside at CCG level & could slow down the replacement programme. AP still prefers perpetual licences.
The Board agreed the proposal to purchase of MPSA perpetual licences for GPIT subject to capital funding
Action: recommend perpetual licences & confirm NHSE capital funding PT
8 Technical Developments (documents provided) 8.1 Data Centre(s) KF stated that N3 circuits now in ARC DC. Installing routers for the WAN w/c 18/9/17. Working with Virgin/ANS re: delays in speed of links between the 2 DCs. Should be complete this week and start testing some migrations across & then move services in. Next major piece of work – refit of PABX room, where all data line come into Charter House; start October through to January 2018. Services will have to be taken down to feed new room into DC. Data will flow through ARC while this is being done to avoid service interruption. KF also stated that all data services have been via the new DC for the last few months.
8.2 NHSmail2PT – archive extraction now finalised. Report on large file sizes for HPFT to come. Now waiting for Accenture to come in to action the migration. Plan is to finalise NHSmail by December 2017. KF explained the issue of creating profiles for all 7.5K staff for configuration on MS Outlook . It will be all scripted and automated. 100 users from the 2 providers to pilot the scheme. AP preferred to retain the use of MS Outlook as it’s the way staff is currently working. Any cost comes as part of the current EA. HPFT customers were given Outlook web. PT confirms NHSmail2 should be finished by December 2017.
8.3 Mobile Device ManagementCurrent provider is MobileIron. Future options: 1) MobileIron (MI) 2) AirWatch (AW). HBL prefer AirWatch - although it is more expensive, it is the better option.
- MI Perpetual £208 for 3 year period. - MI Cloud £36.80 for 1 year licence subscription (subject to change year-on-year) - Airwatch Cloud – £41.11 per year for 3 year subscription with no cost for Sophos
MI & AW almost identical in price. Hidden costs – hosting the servers.
NHSmail recommendation is to go with AirWatch – advantage is the single content locker, which would allow access to shared folders on mobile phones. Good benefits & time saving features. EPR also available. KF would want to test features. HBL ICT Steering group’s recommendation is to go with AirWatch; this board to agree. There are 2 separate issues: 1) Mobile device management. Need to agree timing - when to do this, as well as running both systems side by side for a time. Windows phones to stay on MI for old devices @ £9 per month; new phones deployed would be covered by AirWatch. AirWatch is ready to go as a pilot scheme. HCT want to replace all 1500 on their brick phones with Smart phones; HPFT also have 600/700 Windows phones. AirWatch is ready to go as a pilot scheme. Partners can change their old phones to Smart phones & go with AirWatch.
The Board agreed the proposal to migrate to the AirWatch MDM Service.
2) Phone Devices. Need to be clear on phone specification i.e. which phone does the best job re: size of screen, resolution, photo quality, reliability. Needs to be a decent specification. HCT have J5s, HPFT have 50x J5s ready to use. What phones are needed for the future? Do we standardise to 2/3 different models? Also to consider what it will be used for: bigger screen & more memory will be much more expensive; J5 is OK for emails and phone calls @ £150; J3 is the cheapest Android phone. Decisions must be driven by need. KF considers functionality, stability, security of handset important. Apple is a better device. HBL prefer Samsung android which is just as good. HBL can support & manage (upgrades & applications) either one with AirWatch. Androids cover multiple suppliers.
KF to clarify if 932 devices include iPads.
AP stated that AirWatch would be our mobile device manager of choice in the future.
8.4 HBL Technical Customer Journey – document to share with group.
8.5 Replacement of Edge Switches (Capital Investment) verbal Looking at replacing switches at 2 trust sites (HCT/HPFT). Needs to do this now & upgrade infrastructure in order to support services i.e telephony, skype for business, & including replacing Barracuda. KF will put this into site order & take to Steering group to discuss.
PT
KF
KF

May need capital from the 2 providers; HVCCG £940K+. CISCO’s costs currently unknown but this project would go out to tender. Need to invest in more centralised switching.
9 Cyber Security (document provided) 9.1 Monthly Cyber Security ReportKF reported that there had been an influx in SPAM emails arriving in the last few weeks. ICT’s communication seems to function well – staff more vigilant & aware. Still patching the environment. Once DataCentre complete, will look to upgrading the entire server environment to Windows Server 2016 – this will drastically reduce the number of patches needed (this will be a licence cost). Currently we have 280 servers, 80 sequel reducing to 20. As we have more performance now we do not need as many therefore reducing costs.
9.2 Consolidated Risks from Penetration TestingKF – Audit findings – there are not many left open. Server certificate for the wireless – now called NCORP (amended 10/1/18). Once switched on, connection will be to a new SSID (authenticated). Changes going through to finalise. May no longer need to bring this to the Stakeholder Board in future.
10 HBL ICT Risk Register (document provided) PT pointed out that all rated 12 except for Cyber Security at 15 - would always be quite high for the foreseeable future. InterceptX purchased in July 2017 is now deployed. ICT 199 (Microsoft) at risk 12 is mainly cost/prices as future prices currently unknown. However, AP did not think this a high level risk (12) to HBL. Suggested two lists – one for HBL and one for partners to score & manage their own risks, which are likely to be different. PT – discuss with Alex McLaren for risks to be relayed back to partners. HBL to advise on licences, good practice & provide expertise
PT/AML PT
11 A O B
PT raised the subject of ‘attendance of nominated partner members’ at these meetings. Although the meetings are usually represented by a member of each partnership, the level of authority can be sporadic so making it difficult to finalise decisions/quorum. This can be of a concern. PT feels this needs to be addressed & asks members to consider: change date/time of meeting; change the frequency of the meetings i.e. bi monthly, quarterly. All member feedback required.
LC commented that the sheer volume of content /information sent out by ICT is a ‘bit of a struggle’.
ALL
Date of next meeting: 20
th November 2017 2- 4pm Room MR 2.6 Charter House WGC
(Meeting 16th
October 2017 cancelled).

Page | 1
Agenda Item No: 17
Date of Meeting: 18th January 2017
Governing Body Meeting in Public
Paper Title: Locality Commissioning Meeting Minutes
Decision or Approval Discussion Information
Report author:
Report signed off by: Locality Commissioning Meetings
Executive Summary: Approved minutes of the Locality Commissioning Meetings attached for the Governing Body to note
Recommendations
to the members:
To note the approved minutes of the Locality Commissioning Meetings
Conflicts of Interest
involved:
n/a
Conflict of Interest Definitions
The following table describes the sub-classifications of interests:
Type Description
Financial Interests This is where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-Financial
Professional Interests
This is where an individual may obtain a non-financial professional benefit
from the consequences of a commissioning decision, such as increasing
their professional reputation or status or promoting their professional
career.
Non-Financial
Personal Interests
This is where an individual may benefit personally in ways which are not
directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect Interests This is where an individual has a close association with an individual who
has a financial interest, a non-financial professional interest or a non-
financial personal interest in a commissioning decision.

1
MINUTES
Meeting: North Herts Locality Commissioning Meeting
Date: 9th August 2017
Venue: Letchworth Centre for Healthy Living
Attendee Organisation Role/Responsibility Present
Dr Matt Jarvis (MJ) Ashwell Surgery GP Yes
Mark Pilling (MP) Ashwell Surgery Practice Manager Yes
Dr Richard Stanley (RS) The Baldock Surgery GP Yes
Michael Sissens (MS) The Baldock Surgery Practice Manager Apologies
Dr Rob Graham (RG) Birchwood Surgery GP Apologies
Zoe Smith (ZS) Birchwood Surgery Practice Manager Yes
Dr Keith Greenish (KG) Courtenay House GP Yes
Denise Robson (DR) Courtenay House Practice Manager Yes
Dr Adrian Wood (AW) Garden City Surgery GP Yes
Anne Hegarty (AH) Garden City Surgery Practice Manager Apologies
Dr Rob Newby (RNe) Knebworth and Marymead GP Yes
Ken Spooner (KS) Knebworth and Marymead Practice Manager Yes
Dr Mel Lacy (ML) Nevells Road Surgery GP Yes
Gill Wilcox (GW) Nevells Road Surgery Practice Manager Apologies
Dr Alka Chandrayan (AC) Orford Lodge GP Apologies
Nichola Goddard (NG) Orford Lodge Practice Manager Yes
Dr Tara Belcher (TB) Portmill Surgery GP Yes
Melanie Felgate (MF) Portmill Surgery Practice Manager Yes
Dr Fiona Sinclair (FS) Chair Regal Chambers GP Apologies
Dr Victoria Fraser (VF) Regal Chambers GP Yes
Hayley Marshall (HM) Regal Chambers Practice Manager Apologies
Rebecca Bols (RB) Sollershott GP Apologies
Sandie Ince (SI) Sollershott Practice Manager Apologies
Dr Rajpreet Millan (RM) Whitwell Surgery GP Yes
Lorraine Gary (LG) Whitwell Surgery Practice Manager Yes
Dan Rahemtulla (DR) Lloyds Pharmacy Community Pharmacist Apologies
Jennifer Piggott (JP) PCG Representative Patient Rep Yes
Denise Boardman (DB) E&N Herts CCG Programme Director Apologies
Saskia Vercaeren (SV) Prescribing Advisor Prescribing Advisor Yes
Dr Simon Chatfield (SC) Locality Representative Locality LTC Lead Yes
Sue Russell (SR) E&N Herts CCG Prescribing Lead Apologies
Victoria Robinson (VR) E&N Herts CCG Locality Manager Yes
Phil O’Meara (POM) E&N Herts CCG Finance Team Leader Apologies
Carrie Walsh (CW) Regal Chambers Deputy Manager Yes
Dr Jeremy Cox (JC) Orford Lodge GP Apologies
Dr Carole Brooks (CB) Birchwood Surgery GP Yes
Dr Amit Sudarshan (AS) Orford Lodge GP Yes
Renna Bharania (RB) E&N Herts CCG In Practice Pharmacist Yes
Alan Pond (AP) E&N Herts CCG Finance Director Yes

2
1. Introduction and Apologies Apologies noted above. Declarations of interest The Chair invited the Practice Representatives to reconfirm their current declarations on the Register of Interests and ensure the current version is the most up-to-date.
2. Actions and Notes
The minutes of the previous meeting were agreed to be an accurate representation
All previous actions were confirmed to be still ongoing and are being worked on
3. Meeting dates going forward:
Dates agreed for locality meetings till Dec 17. Clinical attendance is expected at locality meetings, target events and the Council of Members events as part of the CFF engagement element.
There are currently Council of Member’s meetings scheduled for September and December, meaning there is a lot happening in those two months
TB suggests cancelling locality meetings for those 2 months, however this leaves quite a big gaps between dates, therefore it was suggested adding a locality meeting into October as well as a target event
AP clarified that the Council of Members meetings are an important way for the Governing Body to keep in touch with practices
All practices were in agreement that the engagement payments paid for attending meetings should be fair across the practices. SC to put proposal to the Harper Brown for approval.
TB clarified that, going forward, locality meetings will be cancelled during months of Council of Members meeting, but the locality will still have meetings during target event months. Locality agreed with this and therefore a locality meeting will be scheduled for the October.
Action: VR to schedule locality meeting for October and cancel September and December meetings.
VR
4. Integrated Care Provider Board
TB queried whether or not the locality wants to change the structure of this meeting as this is the direction for the future of localities.
AP commented that the best starting place would be to identify the locality’s key providers and how they would like to engage with them
Through this, the locality can then decide whether they would like to change how they pay them, as well as look at what staff they should have versus what staff they have
It was suggested that a member of the acute trust should always be included
KG commented that it may be best to include a mediator such as Anna Cason at every meeting, as someone who is a go-between for the locality and providers.
TB suggested that large providers could be invited to the target event, whilst

3
others who the locality would like to speak to but do not have time during the locality meeting, could have a meeting with the GPs leads where they could pose the locality’s questions to the provider. TB suggests that the locality could email queries to VR before each meeting, who could compile and then send to the provider in advance so the provider can prepare to answer the questions.
AW commented that he is worried that the provider board approach could lead to rationing in other areas whilst the locality decide what they do and do not want to focus on
AP commented that it is more a process of prioritising areas which will reduce A&E admissions. In 5 years’ time demand will only increase and capacity issues will get worse. The locality needs to reduce these admissions and think about the future instead of the here and now.
KS believes it should be more about telling Home First to focus on patients the locality want them to focus on, as long as it helps A&E admissions and believes the locality are already doing this
5. Flu
TB presented to the locality the proposed strategy for this year
The aims of the strategy are to reduce patient morbidity and reduce demand on GPs (See Flu Plan for details).
TB suggested taking any issues such as this forward to the practice managers meeting on the 16th of August for discussion.
Comment made that working age 18-64 tend to be more difficult to engage with, as well as housebound
6. Whitwell CQC
Dr Rajpreet Milan presented to all, the plan and changes made at Whitwell as the practice were previously in special measures and have now progressed to good, which is a very impressive achievement.
RM commented that the improvements they have made, and the impact the CQC has had on staff and the practice in general was really positive.
SC commented that the methodology of CQC inspections is changing, although nothing has been confirmed yet
KG queried what had become of the NHSE premise team as they used to help practices through CQC inspections. He queried whether there is a team which helps with this now. AP comments that he does not believe NHSE sees premises inspections as being their responsibility anymore
GPFV
KS reported to the locality that the WelHat Survey has completed and feedback is being compiled which means the locality should get a North Herts one up and running as soon as possible, at least before the end of September.
Locality did not consider the 12 hours admin involved in the extended hours work, and that the costs for EA did not include this.
Query raised as to whether practices could look at additional hours of a

4
morning – AP replied that there is no reason why it couldn’t be considered but no clarity has been provided by NHSE. It would need to be at a service level instead of at hub level.
Workforce Optimisation
KS updated the locality, stating that the presentation on Workflow Optimisation at the STP event, seemed to be a better course, although the procurement from the CCG did not include them as a provider.
SC outlined Regal Chambers previous issue with the 2 potential providers being given, none of which were the one which Regal Chambers wanted. The practice had requested for their proportion of the funds from the CCG to put towards a different provider, however the amount from CCG funds was a lot less than expected.
Action: AP to provide a spreadsheet of what money is available to the locality for what
AP
7. Hot Topics and Any Other Business Accessible Data Standard – NHSE stated on Radio 4 that all practices are able to provide documents in braille and other formats
AP commented that he had not heard of it
Comment made that GMS contract does say that practices should be able to provide it if needed
Action: VR to find out from CCG which provider is delivering this service and how practices go about using it
District Nursing – KS discussed blood tests and care homes, Roebuck nursing home does not have a nurse so blood tests for residents has now become the practice’s responsibility.
Comment was made that this should be the phlebotomy service’s responsibility, and that the issue should be reported to the contracts hotline
It was noted that Homefirst would visit the patient if they were already seeing them, so could the practice possibly refer them to the service
This led into a discussion about how KS would like to be able to hold providers to account regarding these sort of issues. AP explained that it is for that exact reason that the Provider Board has been set up
KS commented that if urgent care is needed, GPs will always try to fit them in, and that care will always fall back to them should a service fail to provide. HCT need to be held to account, and provide the service they have agreed to, because the impact hits practices unfairly.
VF queried whether phlebotomy service should move in-house? However SC commented that it is a brilliant idea, but is not manageable in practice as it requires leadership, and no one is willing to take this on
AP also commented that the services has always traditionally been contracted, but does not have to be that way, and that the service is not considered a priority for HCT as the trust will prioritise where they believe their money is best spent
VF commented that the service is not a priority because community nurses are used to help the trust when they are short staffed
Locality feel like the contract with TPP was forced on them in some ways
AP commented that there is no defined commissioner for phlebotomy or
VR

5
pathology and that the best course of action for the locality is to identify, collate and present the problems with the service to help ascertain whether or not the service is working
Action: KS to write up a side of A4 document on issues and what service we are expecting to be presented to HCT at the provider board meeting
TB suggested inviting providers to the target event, and recommended practices email VR with questions to be presented to providers before the meeting so they can prepare answers
Home First – KG queried that Rapid Response should be just that, the ability to get people to patients quickly
AP commented that the service has become rapid access more than rapid response and that the structure which was set up initially now needs to change. The issue has been discussed at the Governing Body meeting and is being investigated.
AW commented that it is very rare that you need them to attend within the hour
KG commented that the service should be focusing their resources, although AP argued that this unfortunately makes them too rigid and therefore ineffective
KS argued that the Rapid Response contract states 1 hour, and they are judged on that. He argued that the locality should bring them in to a provider board meeting so the locality can help redesign the service that best suits the locality requirements.
EpiPens – VF queried the use of EpiPens and was informed that we are still awaiting a decision on them from GB. SV noted and will feedback as available Workforce – RS updated the locality on the CCG funded associate training course. He encouraged practices to consider their training capacity and let him know if there is anyone who should be included.
SC commented that the best way for practices to recruit is to be a training practice
The course is fully funded and involves 3 days over 3 months. Only medically trained staff can take part and there is no backfill, however the process has been streamlined and is now much easier to apply
Action: RS to provide list of who to contact for what and how best to contact them
KS PM’s SV RS
8. Date and Time of Next Meeting 13th September
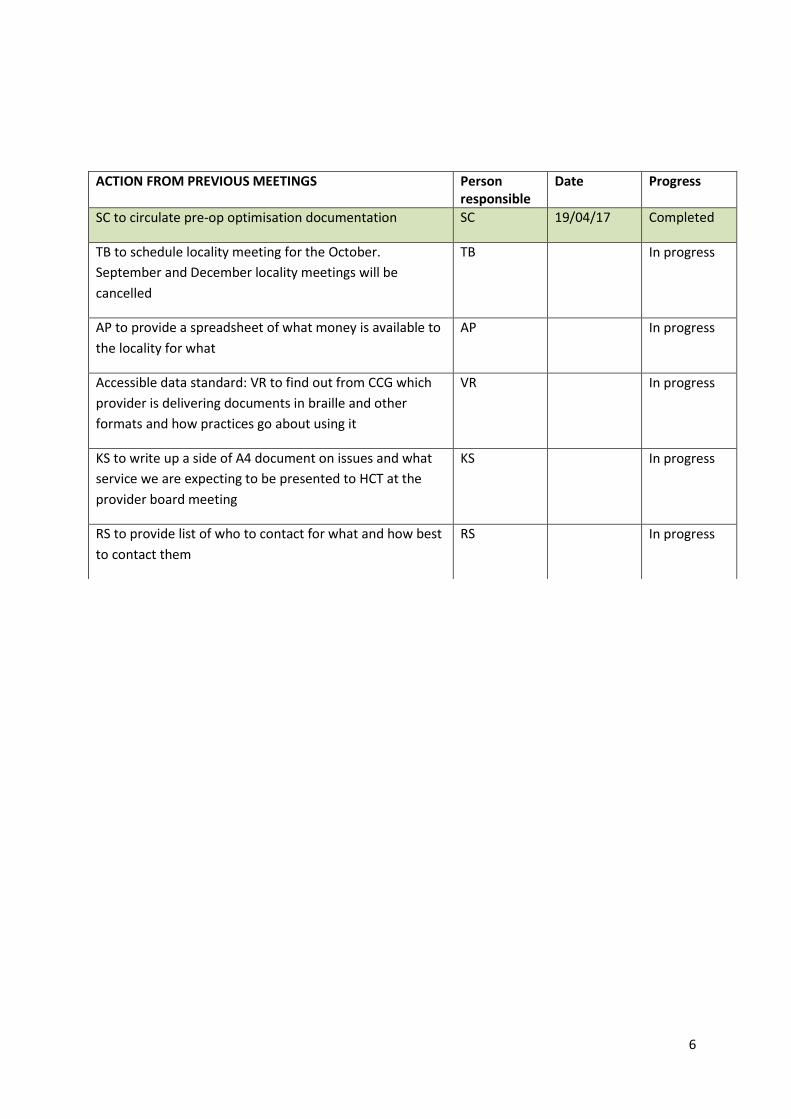
6
ACTION FROM PREVIOUS MEETINGS Person responsible
Date Progress
SC to circulate pre-op optimisation documentation SC 19/04/17 Completed
TB to schedule locality meeting for the October.
September and December locality meetings will be
cancelled
TB In progress
AP to provide a spreadsheet of what money is available to
the locality for what
AP In progress
Accessible data standard: VR to find out from CCG which
provider is delivering documents in braille and other
formats and how practices go about using it
VR In progress
KS to write up a side of A4 document on issues and what
service we are expecting to be presented to HCT at the
provider board meeting
KS In progress
RS to provide list of who to contact for what and how best
to contact them
RS In progress

1
MINUTES
Meeting: North Herts Locality Commissioning Meeting
Date: 25th October 2017
Venue: Letchworth Centre for Healthy Living
Attendee Organisation Role/Responsibility Present
Dr Matt Jarvis (MJ) Ashwell Surgery GP Yes
Mark Pilling (MP) Ashwell Surgery Practice Manager Yes
Dr Richard Stanley (RS) The Baldock Surgery GP Yes
Michael Sissens (MS) The Baldock Surgery Practice Manager Yes
Dr Rob Graham (RG) Birchwood Surgery GP Apologies
Zoe Smith (ZS) Birchwood Surgery Practice Manager Yes
Dr Keith Greenish (KG) Courtenay House GP Yes
Denise Robson (DR) Courtenay House Practice Manager Yes
Dr Adrian Wood (AW) Garden City Surgery GP Apologies
Anne Hegarty (AH) Garden City Surgery Practice Manager Apologies
Dr Rob Newby (RNe) Knebworth and Marymead GP Apologies
Ken Spooner (KS) Knebworth and Marymead Practice Manager Yes
Dr Mel Lacy (ML) Nevells Road Surgery GP Yes
Gill Wilcox (GW) Nevells Road Surgery Practice Manager Apologies
Dr Alka Chandrayan (AC) Orford Lodge GP Apologies
Nichola Goddard (NG) Orford Lodge Practice Manager Yes
Dr Tara Belcher (TB) Portmill Surgery GP Yes
Melanie Felgate (MF) Portmill Surgery Practice Manager Apologies
Dr Fiona Sinclair (FS) Regal Chambers GP Apologies
Dr Victoria Fraser (VF) Regal Chambers GP Yes
Hayley Marshall (HM) Regal Chambers Practice Manager Yes
Sollershott GP Apologies
Sandie Ince (SI) Sollershott Practice Manager Yes
Dr Rajpreet Millan (RM) Whitwell Surgery GP Apologies
Karen Story (KSt) Whitwell Surgery Practice Manager Yes
Jennifer Piggott (JP) PCG Representative Patient Rep Apologies
Saskia Vercaeren (SV) Prescribing Advisor Prescribing Advisor Apologies
Dr Simon Chatfield (SC) Locality GP Lead Locality Chair Yes
Victoria Robinson (VR) E&N Herts CCG Locality Manager Yes
Phil O’Meara (POM) E&N Herts CCG Finance Team Leader Apologies
Carrie Walsh (CW) Regal Chambers Deputy Manager Apologies
Alan Pond (AP) E&N Herts CCG Finance Director Apologies
Dr Jeremy Cox (JC) Orford Lodge GP Yes
Dr Carole Brooks (CB) Birchwood Surgery GP Yes
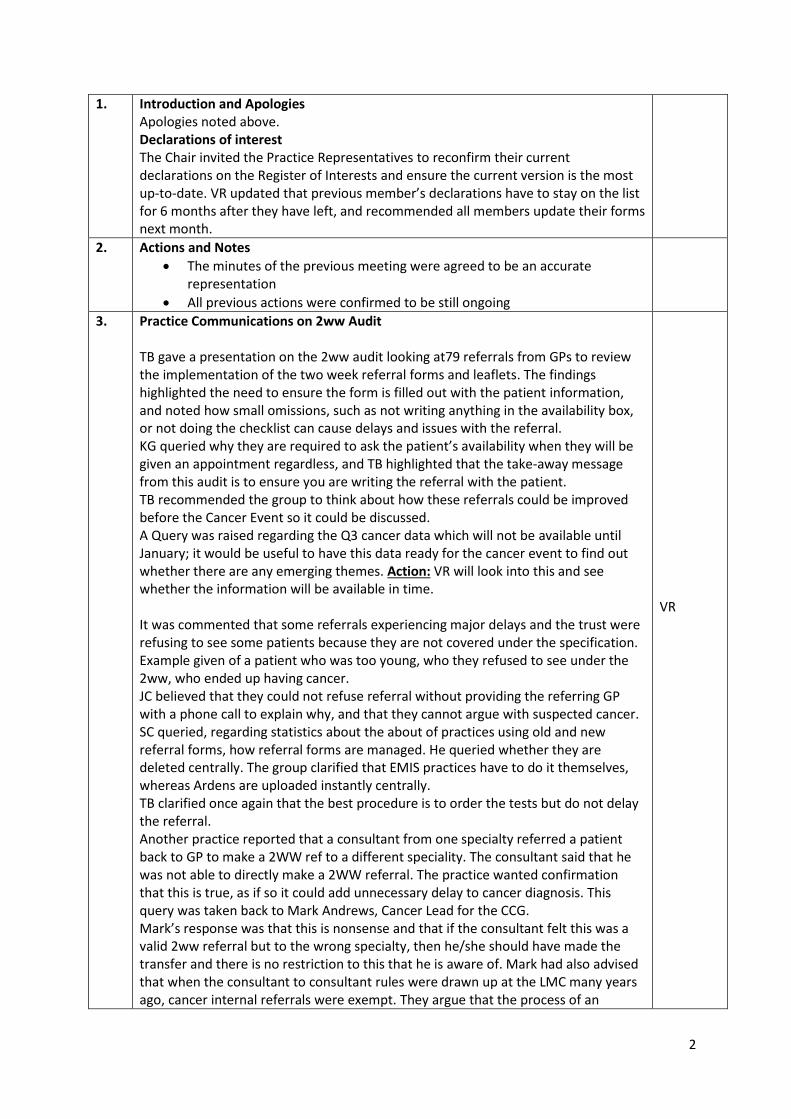
2
1. Introduction and Apologies Apologies noted above. Declarations of interest The Chair invited the Practice Representatives to reconfirm their current declarations on the Register of Interests and ensure the current version is the most up-to-date. VR updated that previous member’s declarations have to stay on the list for 6 months after they have left, and recommended all members update their forms next month.
2. Actions and Notes
The minutes of the previous meeting were agreed to be an accurate representation
All previous actions were confirmed to be still ongoing
3. Practice Communications on 2ww Audit TB gave a presentation on the 2ww audit looking at79 referrals from GPs to review the implementation of the two week referral forms and leaflets. The findings highlighted the need to ensure the form is filled out with the patient information, and noted how small omissions, such as not writing anything in the availability box, or not doing the checklist can cause delays and issues with the referral. KG queried why they are required to ask the patient’s availability when they will be given an appointment regardless, and TB highlighted that the take-away message from this audit is to ensure you are writing the referral with the patient. TB recommended the group to think about how these referrals could be improved before the Cancer Event so it could be discussed. A Query was raised regarding the Q3 cancer data which will not be available until January; it would be useful to have this data ready for the cancer event to find out whether there are any emerging themes. Action: VR will look into this and see whether the information will be available in time.
It was commented that some referrals experiencing major delays and the trust were refusing to see some patients because they are not covered under the specification. Example given of a patient who was too young, who they refused to see under the 2ww, who ended up having cancer. JC believed that they could not refuse referral without providing the referring GP with a phone call to explain why, and that they cannot argue with suspected cancer. SC queried, regarding statistics about the about of practices using old and new referral forms, how referral forms are managed. He queried whether they are deleted centrally. The group clarified that EMIS practices have to do it themselves, whereas Ardens are uploaded instantly centrally. TB clarified once again that the best procedure is to order the tests but do not delay the referral. Another practice reported that a consultant from one specialty referred a patient back to GP to make a 2WW ref to a different speciality. The consultant said that he was not able to directly make a 2WW referral. The practice wanted confirmation that this is true, as if so it could add unnecessary delay to cancer diagnosis. This query was taken back to Mark Andrews, Cancer Lead for the CCG. Mark’s response was that this is nonsense and that if the consultant felt this was a valid 2ww referral but to the wrong specialty, then he/she should have made the transfer and there is no restriction to this that he is aware of. Mark had also advised that when the consultant to consultant rules were drawn up at the LMC many years ago, cancer internal referrals were exempt. They argue that the process of an
VR

3
internal transfer is slower than a new 2ww referral. But he can see no reason why this should be the case if the consultant is responsible in acting and communicating with colleagues immediately. It was recommended that the practice report this to the GP hotline and Mark advised he will raise this at the next cancer board. It was commented made that cancer diagnosis in A&E is still an issue for the locality.
4. Extended Access Planning and Vote VR informed the group that the trajectory for the installation of the IT for extended access has changed, and despite asking to be first North Herts locality are now down for installation in quarter 4 which is 15 months away. The Locality are not expected to deliver the service for the 1st April 2018, but will now be expected to deliver during Q4 after the roll out. SC commented that the current extended hour’s DES will be renewed at the end of this year for 18/19, but will then finish, although that has not been confirmed in writing yet. TB advised that with the DES still in place for 18/19 the practices will not be losing money, so all this change in trajectory has done is provided more time to prepare and organise. TB also advised that it is better to start this service in the summer as it is less busy, and the IT costs will be the same regardless of what time of year the service is started, and it was agreed that starting without the IT in place will make it more difficult for the locality. TB advised that there is £350k available to provide extended access, if the locality does not use the money it will be used to procure the service from another provider. Action: VR will ask about procurement process for extended access SC commented that he is surprised by the number of GPs interested in providing a 7 day service. TB commented that this way of working suits younger GPs, or those with children. KG queried whether these GPs would be able to commit to these times regularly. TB advised that there are a series of questions which need to be answered regarding the service, they are:
1. Why have the locality only just found out about this change of trajectory?
2. Is the DES definitely still going to be available? 3. Will the CCG definitely go to procurement for 18/19 if the locality
decides not to go ahead with this? 4. How are the locality expected to deliver before the IT installation,
and without the necessary systems? 5. If the locality manages to find a way will they be able to start
sooner? 6. What will happen to the money if it is not spent? 7. Are we able to run the service and the DES in parallel?
SC advised that he had previously queried the expected process regarding DES with Dee Boardman, and she had informed it that it is expected to continue but this has not been formally confirmed. KS confirmed that Dee Boardman has agree that early mornings are available should practices be able to justify that they are needed and that the patient survey has shown Saturdays are wanted by patients, but there is no demand for Sundays.
VR

4
KS raised concerns that looking at the distribution of funds, paying GPs £80 per hour makes management and other costs quite tight, he suggested using nurses in the evenings would make it easier and more affordable, but he recommended further investigation into the different options available. KS commented that the easiest way of providing the service would be through 12 Point Care. He recommended that the federation look into this and that the locality give them the ability to do this as they could buy the software on the locality’s behalf, as well as write rotas. KS suggested that the federation would benefit from employing a federation manager to help enable this. TB advised that this could be written into the budget. TB commented that extended access is for routine planned care, although it was queried whether 111 will be added into this. It was queried whether it would be possible to use the appointments to aid phlebotomy services? TB commented that this is a very good idea however queried whether transportation and storage would be difficult outside of regular hours. TB commented that getting a phlebotomist to work a few hours five days a week would be relatively cheap and easy to do, and would also solve the current issues being experienced with the service. TB advised, the current phlebotomy service is not working and the current contract finishes next year, which could possibly provide the locality with the opportunity to put a plan forward. KG raised the concern that every phlebotomy service provider is currently trying to leave the current contract. He queried whether this must mean that the contract is too cheap, and whether the locality could therefore afford to run it. It was noted that the current contract runs on £1.90 per bleed, and is only enough money to cover one HCA. TB advised that the locality’s patients needed to get blood tests from somewhere and that the contract was awarded to TPP. SC commented that there is the option to delay the proposed vote until more information is available, he does not know how profitable the DES scheme is for practices, so if the locality would like to delay until further information regarding the scheme is available then that is a possibility. TB advised that there a currently 3 models which the locality can decide on:
1.Let the CCG procure for the service 2.Agree that the federation 12 Point Care provide the service 3. Practices to provide the service as a collective.
TB advised that there is a possibility that 12 Point Care will not want to do it, but if they could be encouraged to run a service with a HCA and a Phlebotomist then there would be enough margin of profit left to afford a federation manager to help run it. The locality decided to take a vote on the preferred course of action:
1. 0 voted to procure 2. 13 voted for 12 Point Care to provide the service 3. 2 abstained for the reason that they believed there was not
enough information to vote today.
SC advised that he will ask 12 Point Care what the federation’s plans are. TB advised that they will try and find out what is happening to the DES.
5. Locality Transformation Planning and agreement TB asked for feedback on the latest locality transformation plan, after the recent discussions at the additional session at the Target event, and advised that the locality plans still has £40k of funds still available for investment, and queried if anyone else had any ideas to put forward.KG advised that he does not see a future in
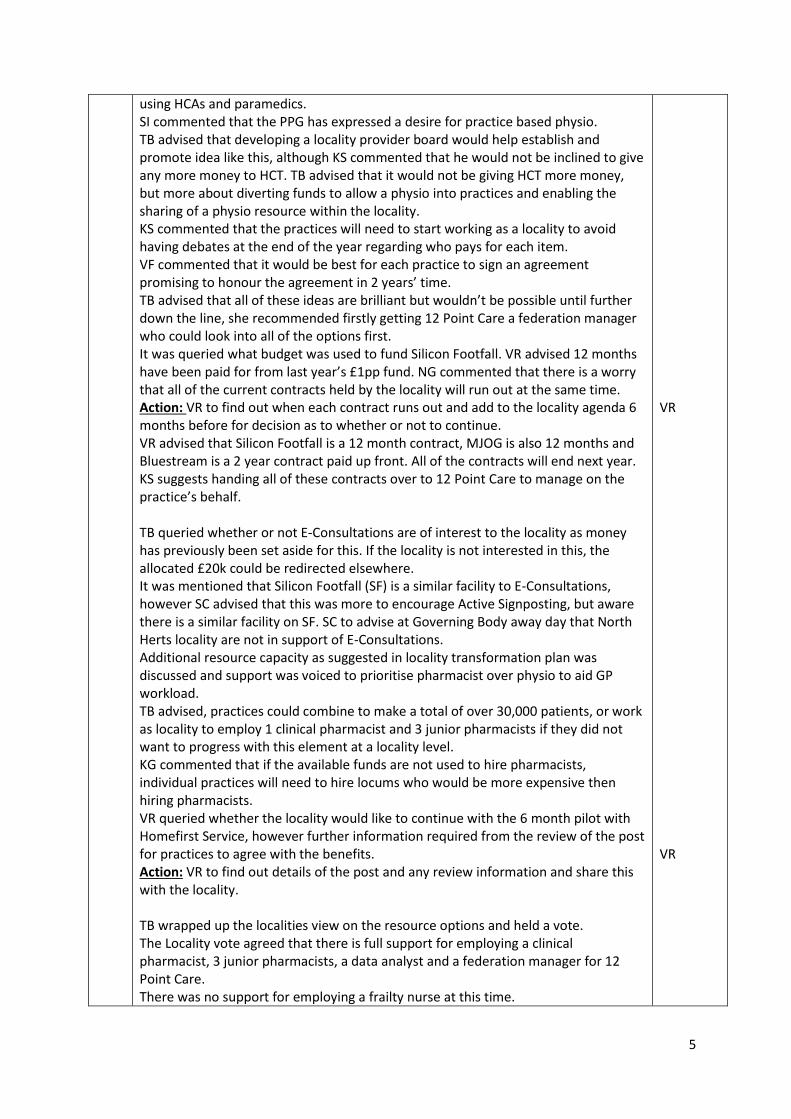
5
using HCAs and paramedics. SI commented that the PPG has expressed a desire for practice based physio. TB advised that developing a locality provider board would help establish and promote idea like this, although KS commented that he would not be inclined to give any more money to HCT. TB advised that it would not be giving HCT more money, but more about diverting funds to allow a physio into practices and enabling the sharing of a physio resource within the locality. KS commented that the practices will need to start working as a locality to avoid having debates at the end of the year regarding who pays for each item. VF commented that it would be best for each practice to sign an agreement promising to honour the agreement in 2 years’ time. TB advised that all of these ideas are brilliant but wouldn’t be possible until further down the line, she recommended firstly getting 12 Point Care a federation manager who could look into all of the options first. It was queried what budget was used to fund Silicon Footfall. VR advised 12 months have been paid for from last year’s £1pp fund. NG commented that there is a worry that all of the current contracts held by the locality will run out at the same time. Action: VR to find out when each contract runs out and add to the locality agenda 6 months before for decision as to whether or not to continue. VR advised that Silicon Footfall is a 12 month contract, MJOG is also 12 months and Bluestream is a 2 year contract paid up front. All of the contracts will end next year. KS suggests handing all of these contracts over to 12 Point Care to manage on the practice’s behalf. TB queried whether or not E-Consultations are of interest to the locality as money has previously been set aside for this. If the locality is not interested in this, the allocated £20k could be redirected elsewhere. It was mentioned that Silicon Footfall (SF) is a similar facility to E-Consultations, however SC advised that this was more to encourage Active Signposting, but aware there is a similar facility on SF. SC to advise at Governing Body away day that North Herts locality are not in support of E-Consultations. Additional resource capacity as suggested in locality transformation plan was discussed and support was voiced to prioritise pharmacist over physio to aid GP workload. TB advised, practices could combine to make a total of over 30,000 patients, or work as locality to employ 1 clinical pharmacist and 3 junior pharmacists if they did not want to progress with this element at a locality level. KG commented that if the available funds are not used to hire pharmacists, individual practices will need to hire locums who would be more expensive then hiring pharmacists. VR queried whether the locality would like to continue with the 6 month pilot with Homefirst Service, however further information required from the review of the post for practices to agree with the benefits. Action: VR to find out details of the post and any review information and share this with the locality. TB wrapped up the localities view on the resource options and held a vote. The Locality vote agreed that there is full support for employing a clinical pharmacist, 3 junior pharmacists, a data analyst and a federation manager for 12 Point Care. There was no support for employing a frailty nurse at this time.
VR VR
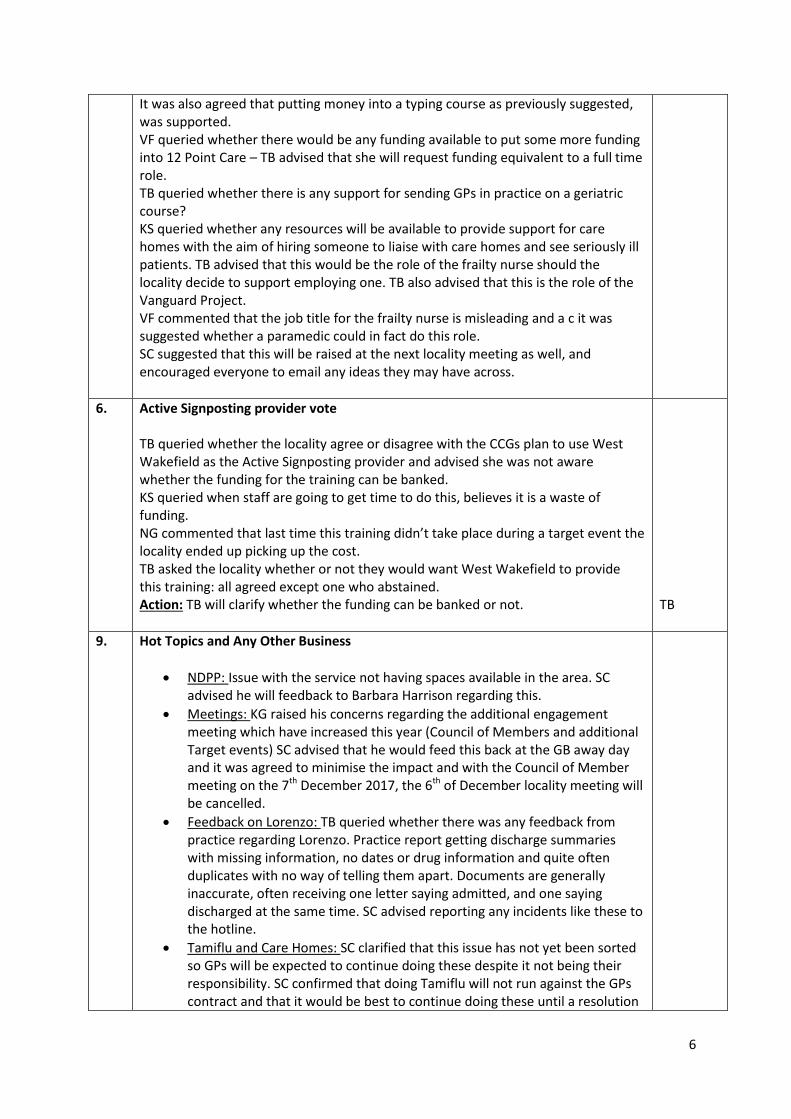
6
It was also agreed that putting money into a typing course as previously suggested, was supported. VF queried whether there would be any funding available to put some more funding into 12 Point Care – TB advised that she will request funding equivalent to a full time role. TB queried whether there is any support for sending GPs in practice on a geriatric course? KS queried whether any resources will be available to provide support for care homes with the aim of hiring someone to liaise with care homes and see seriously ill patients. TB advised that this would be the role of the frailty nurse should the locality decide to support employing one. TB also advised that this is the role of the Vanguard Project. VF commented that the job title for the frailty nurse is misleading and a c it was suggested whether a paramedic could in fact do this role. SC suggested that this will be raised at the next locality meeting as well, and encouraged everyone to email any ideas they may have across.
6. Active Signposting provider vote TB queried whether the locality agree or disagree with the CCGs plan to use West Wakefield as the Active Signposting provider and advised she was not aware whether the funding for the training can be banked. KS queried when staff are going to get time to do this, believes it is a waste of funding. NG commented that last time this training didn’t take place during a target event the locality ended up picking up the cost. TB asked the locality whether or not they would want West Wakefield to provide this training: all agreed except one who abstained. Action: TB will clarify whether the funding can be banked or not.
TB
9. Hot Topics and Any Other Business
NDPP: Issue with the service not having spaces available in the area. SC advised he will feedback to Barbara Harrison regarding this.
Meetings: KG raised his concerns regarding the additional engagement meeting which have increased this year (Council of Members and additional Target events) SC advised that he would feed this back at the GB away day and it was agreed to minimise the impact and with the Council of Member meeting on the 7th December 2017, the 6th of December locality meeting will be cancelled.
Feedback on Lorenzo: TB queried whether there was any feedback from practice regarding Lorenzo. Practice report getting discharge summaries with missing information, no dates or drug information and quite often duplicates with no way of telling them apart. Documents are generally inaccurate, often receiving one letter saying admitted, and one saying discharged at the same time. SC advised reporting any incidents like these to the hotline.
Tamiflu and Care Homes: SC clarified that this issue has not yet been sorted so GPs will be expected to continue doing these despite it not being their responsibility. SC confirmed that doing Tamiflu will not run against the GPs contract and that it would be best to continue doing these until a resolution

7
is found.
MH Lead: SC queried whether there are any volunteers who would like to step forward for the role.
Ambulance: SC queried whether the locality had seen the communications which had been circulated. All confirmed they had.
Delegated Commissioning: SC made the locality aware that this is due shortly and advised that this will be voted on soon, there has not be a recommendation from the GB yet.
De-Commissioning: SC advised that the results have been circulated, that an implementation date will be provided soon. VF commented that there are worries around breaches of GMS contract, which SC assured are being worked on.
10. Date and Time of Next Meeting 8th November

8
ACTION LOG Person responsible
Date Progress
TB to schedule locality meeting for the October. September
and December locality meetings will be cancelled
TB August 17 Completed
AP to provide a spreadsheet of what money is available to
the locality for what
AP September 17 Completed
VR to look into cancer data and when it will be available by VR 8th November 17 In progress
VR to query process and expectation for procurement for
extended access
VR 8th November 17 In progress
VR to find out when each locality contract (MJOG, Silicon
Footfall etc.) runs out and add to the locality agenda 6
months before for decision as to whether or not to continue.
VR 8th November 17 In progress
VR to find out feedback from the Homefirst Co-ordinator
pilot
VR 8th November 17 In progress
TB will clarify whether Active Signposting funding can be
banked or not.
TB 8th November 17 In progress
1 | P a g e
MINUTES
Meeting: Stevenage ICPB and Locality Meeting
Date: Tuesday 13th June 2017 - 12.30 to 2.30pm
Venue: Cromwell Hotel, High Street, Old Town, Stevenage, SG1 3AZ.
Attendee do these Organisation Present
1. Dr Russell Hall (RH) Chair GP Chells Way Surgery Y
2. Dr Prag Moodley (PM) GP Stanmore Medical Group Y
3. David Myers (DM) Chells Way Surgery Y
4. Susan Lincoln (SL) PM Stanmore Medical Group Y
5. Mark Banks (MB) PM King George Surgery Y
6. Dr Rini Saha (RS) GP King George Surgery Y
7. Fiona Lucas (FL) PM Symonds Green Y
8. Dr Masood GP Symonds Green Y
9. Elaine Cook (EC) PM Bedwell Medical Centre Y
10. Allison Seymour (ALS) PM Bedwell Medical Centre Y
11. Sandra Copping (SC) PM Manor House Y
12. Karen Smith (KS) Nurse Manor House Y
13. Manjit Phugura (MP) PM Shephall Health Centre Y
14. Deena Keefe(DK) Locality Manager CCG Y
15. Barbara Harrison Assoc Director For Commissioning ENH CCG Y
16. Michelle Morrissey Team Administrator CCG Y
17. Sabina Tai (ST) HomeFirst & Rapid Response Project Manager Y
18. Sharn Elton (SE) Director Operations and Resilience CCG Y
19. Maxine Davis(MD) Senior Pharmaceutical Advisor ENHCCG Y
20. Della McMurdo (DMM) HPFT Service Mgr community Mental Health Y
21. Julie Hoare (JH) HCT Director of Service Development and Partnerships
Y
22. Yasha Rai (YR) HCT Community Matron Y
23. Jacqui Carrett (JC) Service Manager ICRS Y
24. Dr K Daodu GP Shephall Way Surgery Y
25. Michael Hall Kings Medical Student – Manor House Surgery Y
26. Michael Henderson HPFT Services Lead Y
27. Sean Dale-Molloy HomeFirst/ Rapid Response Y
28. Sunday Adeniyi (SA) ENH CCG Y
29. Daisy Clegg GPST2 Stanmore Y
30. Hannah Wright HCS Team Manager – Stevenage Older People Y
31. M. Asal Jabul GPST1 Y
1. Apologies and Introductions – RH welcomed everyone. Apologies – noted

2 | P a g e
Declarations of Interest – The Chair invited the Practice Representatives to reconfirm their current declarations on the Register of Interests were accurate and up to date. All members confirmed their interests were accurate and up to date carried out by email.
2. Integrated Provider Board EK delivered a presentation and discussion took place around HomeFirst. Explained that referral times are based around trying to see patients within 1-2 weeks, and that they are triaged first. EK personally does 2 sessions per week and will usually see 3-4 patients per session. GPs can refer to her directly. SE commented that a Frailty Assessment unit opened in early May. Locality Plan – ST gave an update, informing the locality that Jayne Dingemans and Dr Bell will be coming to the next ICPB meeting 11th July.
Amendment made 12.09.17
Ardens – EC queried with the project lead if Arden’s could be removed from S1 after the trial
period if not suitable but project manager did not know the answer to this question. SE said the
project lead should be able to inform practices of this information. Bedwell have been to view
the Arden’s software at another practice and was not convinced it was better that what we are
currently using plus Arden’s templates looked ‘very busy’. Bedwell have decided to use their
own templates which are better and much easier for their clinicians to use. EC also raised that
Arden’s is not being fully utilised at the moment so nobody really knows how good or bad its
capabilities are.
EC made further enquires whether it is compulsory to have Arden’s and was informed by Dr RH
it is not compulsory. It was suggested by Dr PM that it might be worth the whole locality using
Arden’s. It was also suggested that perhaps Bedwell’s templates could be used to improve
Arden’s templates.
COPD – Comment made that the pathway is working and that, out of 70 patients 40% have undergone pulmonary rehab. Comment made that care plans will need to be personalised and that locality will need to be clear on this so consistency can be guaranteed. Query as to which care plan should be used, suggested that locality should link in with Emily Byway to find out what is available, with the suggestion of inviting her to the next PM Meeting. SE also commented that they are also looking at the My COPD app to try and assess ease of use. Comment made that process in practice is needed so all are following the same process and a way of telling practices which patients need to be seen. It was queried whether Acute Chest Team could feed this back and inform practices of admission. COPD team identified 68 patients in the locality. JC and team will work with the practices and discuss these individual patients at MDT Meetings for future care planning.
TOR – Revised draft has been circulated, however there is an error – wording currently states that there are 8 Target Events a year. DK will amend and circulate to get sign off.

3 | P a g e
Wound Product Prescribing – Scheme needs setting up with a proposal needing to be put into place. There is no financial saving, but will save time. Ability to split packs in now available. Proposal to be shared to see whether the process could be used. PM outlines that at the moment doctors cannot prescribe 1 dressing and that this will save time. Scheme will be piloted. UTI – Plan to feedback at next ICPB Meeting. Only 4 practices data is available so far Action :
DK to amend TOR and circulate to group for sign off
DK to organise for Emily Byway to attend Practice Managers meeting to discuss Care
Plans.
3. Action notes from previous meeting (9th May 17) – see action log
4. HCT/Rapid Response
Staffing updates provided
Recruitment for 3 x Band 5s underway
Work with care homes underway
Enough referrals going through
Capacity is full
5. Weight Management Service
Locality are apparently not using the service, have been using Slimming World (SW) and Weight Watchers (WW)
To be eligible patient has to have had 1 previous form of intervention
RH outlines that the problem is that we don’t know whether or not they have failed
New flier has been developed, has been sent to practices and is available online
Anyone with key risk score of over 10 is also eligible
Links with SW and WW are being developed allowing them to refer – links not in place at the moment but are being worked on
Service can see 500 people in a year
Has been running one month and has only just had first referral
Referrals from Mental Health are also available (See attached report for further information)
6. Finance and Locality Information Pack (LIP) update (see pack)
SA advised that allocation will not be available until the next meeting
7. Mental Health Update
See newsletter attached
New leaf college now available and is free for those with LTC and Mental Health
GP training is also available
Spectrum are also promising not to turn anyone away, so it should be easier to use HPFT to get further input. The waiting times for this are currently shorter as well.
8. LTC Update
Diabetes audit to be completed by the end of July
CFF issues regarding plans
Next meeting to be held on 29th June, will be looking at CFF and Harper Brown to give input

4 | P a g e
9. Prescribing Update
Repeat prescriptions being targeted – Symonds Green currently have 20% of prescriptions as repeats – this is good and encouraged as it reduces workload
MD also comments that they are formatting a letter and asks for the locality to email her with examples of issues with local pharmacies and prescribing dispensing complaints so these can be submitted
Coeliac and prescribing Gluten Free are also being discussed, with 3 options for the future of the prescribing being put forward. Practices are being asked to vote on which of the 3 options would be their preference via a survey which has been emailed out. Survey needs to be completed by 22nd June.
MD also asked that the locality please send at least one rep to the meeting
RH also commented on the issue with pharmacy calling to ask doctors about difficulties getting some medications and querying what alternatives they could give. He comments that doctors don’t know this information and was wondering whether a list of alternative options could be provided
Another comment regarding doctors having to do dosette boxes as pharmacies are not
Observation made that repeat prescriptions tie in very nicely with EPS.
10. Consolidating Funding Framework (CFF)
Nothing more to add
Query as to what the 35p for education can be used on, DK will get clarification
1) 10.
AOB
Target Event – Next event is on the 20th of September, KS to liaise with DK for target event agenda, PMs to liaise regarding admin training
CFF – EC queried whether or not CFF will continue for 3 years in order to organise engagement and work out who would be most important to put through training. SE explained that is it confirmed but not guaranteed, and that the CCG are unsure whether the STP will affect the CFF. SE recommends working on the basis of yes, it will continue, but is unsure of its future.
Travax – EC queried whether the payment has been stopped as they can no longer access. Clarified that it is still being sorted out
Mental Health(amended 12.09.17) – EC raised when letters are received from the mental health team they only state the item of medication they change. Our GP’s requested all the medication the patient is taking should be listed - not just the item/s they change. GSF Meetings(amended 12.09.17) – EC raised that their GSF meetings are taking much longer due to the added CFF areas of discussion needed to take place with the MDT team. Bedwell’s concern is the main ethos of the GSF meeting will be lost and cancer patient’s discussion will be restricted due to the added time it is taking to talk about the CFF MDT areas.
Vasectomy – Only one clinic is available, EC queried whether more are opening? Answer is no, no others planned
Bereavement – not using fax machine now, communications only being accepted via post from 23rd. RH comments that this is another reason why Trust are needed to attend this meeting. SE recommends that the issue be sent to Laura and Contracts Hotline, comments that HPFT are also getting rid of their fax machine as well, with all referrals now being done via email.
Working with pharmacy – MB purposed meeting on July 6th at 7.15 to meet with Superdrug prescribing lead. He would like to encourage more clinical staff to attend

5 | P a g e
E-Learning – Current agreement has expired, locality agreement from previous meeting to use £1 per patient money to fund one more year. Bedwell and Chells to fund own learning from this fund as well
Dates of Next Meeting: 11th July 2017 @ Cromwell Hotel, High Street Stevenage – 12.30 to 2.30pm
12th Sept 2017 @ Cromwell Hotel, High Street Stevenage – 12.30 to 2.30pm
ACTIONS Person
Responsible
DATE
2) 1
1
1
1. Shephall – phlebotomy service- need a
phlebotomist to work from the surgery for their
patients.
Issue ongoing since Jan 2017. HED was dealing with
the matter with the Contracts team at the CCG and
TPP team.
Need to escalate to Harper Brown to resolve, as
Patients have a petition and are escalating.
DK 09.05.17 – HB to contact practice directly to discuss
2. Minor Injures evaluation report, Locality would like NC and The Executive Team to support what the locality can do next and also they want support in taking next steps, and funding. 21.02.17 – SE to feedback to the CCG and see what funding is available and see if we can go forward on this. 14.03.17 – Minor Injuries is not part of the CFF 2017/18. Need CCG confirmation if the Minor Injury scheme will be supported going forward. Needs to include QIPP and make savings, Locality need to agree to report. 11.04.17 – Locality need to highlight which specific injuries there are opportunities for, and produce a business case to the CCG for a service. This could be a good example of a new locality service.
SE/CCG
Locality to make a
decision.
Ongoing
3. Feedback regarding the phlebotomists and the issue of printing forms on Ice and also coming to the surgery without being able to sign in with their smartcards. DK – emailed the service on 06.04.17 and is chasing the issues. Examples were requested from the team now. Emailed again 17.05.17, chased 06.06.17. Contract team dealing with the issues directly.
DK Contract is changing
from TPP – trying to
find out who will be
taking over
4.Get the GP Hotline Contracts Team to report to the locality, as to what actions are being taken and what has changed due to this. So the locality knows what
DK/Anna
Cason
AC replied that
report will not be

6 | P a g e
has been done by them using the reporting tool. Common themes of issues.
available until
Thursday
Ongoing
5.Diabetes service issues raised by Karen Smith and locality, SE to liaise with the service 11.04.17 – KS has a meeting 12.04.17with the service to discuss Update 09.05.17 - KS spoke to HCT awaiting to meet up with them.
SE Not heard back
from hospital, KS to
email again and CC
SE
Ongoing
6.Transgender – NC/HED to establish commissioning arrangements for issues for continuing support Ravi to email on behalf of the locality regarding the issues. To be forwarded to NHSE
RP Ongoing
8.School Nursing services – MAG will contact and liaise/update the locality.
MAG Completed 09.5.17
AC to contact
HomeFirst/ Rapid
Response if any
further queries
9.NDPP figures for the locality – locality want the figures they need to work from for CFF 2017/2018
DK Ongoing
10.E-Referrals update on the target for the year end – data a few months behind.
DK/JA Ongoing
Jamie still trying to
get data – 1% off at
end of year
11. DK to invite Emily Byway to PM meeting to discuss COPD Care Planning – outcome of meeting to be fed back to locality.
DK Ongoing
12. JC to feedback names of 68 patients identified in the locality who are in need of future care planning
JC Ongoing
13. Representative from the Trust needed at every meeting
JC JC to take back -
Ongoing
14. All practices to create a register of catheters, make sure locality has process in place, include community services
All Ongoing

7 | P a g e
15. DK to change working in TOR around number of Target Events, circulate for agreement
DK Ongoing
16. Practices to complete survey by the 22nd June, choosing which of 3 options for gluten-free prescribing they would prefer
All Ongoing
17. DK to get clarification regarding what the 35p for education can be used for
DK Ongoing

1 | P a g e
MINUTES
Meeting: Stevenage ICPB and Locality Meeting
Date: Tuesday 11th July 2017 - 12.30 to 2.30pm
Venue: Cromwell Hotel, High Street, Old Town, Stevenage, SG1 3AZ.
Attendee do these Organisation Present
1. Dr Russell Hall (RH) Chair GP Chells Way Surgery Y
2. Dr Prag Moodley (PM) GP Stanmore Medical Group Apologies
3. David Myers (DM) Chells Way Surgery Y
4. Susan Lincoln (SL) PM Stanmore Medical Group Y
5. Mark Banks (MB) PM King George Surgery Y
6. Dr Rini Saha (RS) GP King George Surgery Apologies
7. Fiona Lucas (FL) PM Symonds Green Y
8. Dr Masood GP Symonds Green Apologies
9. Elaine Cook (EC) PM Bedwell Medical Centre Apologies
10. Allison Seymour (ALS) PM Bedwell Medical Centre Y
11. Sandra Copping (SC) PM Manor House Apologies
12. Karen Smith (KS) Nurse Manor House Y
13. Manjit Phugura (MP) PM Shephall Health Centre Apologies
14. Deena Keefe(DK) Locality Manager CCG Y
15. Barbara Harrison Assoc Director For Commissioning ENH CCG Y
16. Michelle Morrissey Team Administrator CCG Y
17. Sabina Tai (ST) HomeFirst & Rapid Response Project Manager Apologies
18. Sharn Elton (SE) Director Operations and Resilience CCG Apologies
19. Maxine Davis(MD) Senior Pharmaceutical Advisor ENHCCG Y
20. Della McMurdo (DMM) HPFT Service Mgr community Mental Health Y
21. Julie Hoare (JH) HCT Director of Service Development and Partnerships
Y
22. Yasha Rai (YR) HCT Community Locality Manager Y
23. Jacqui Carrett (JC) Service Manager ICRS Y
24. Dr K Daodu GP Shephall Way Surgery Apologies
25. Michael Henderson HPFT Services Lead Apologies
26. Sean Dale-Molloy HomeFirst/ Rapid Response Y
27. Sunday Adeniyi (SA) ENH CCG Y
28. Beverley Flowers (BF) Chief Executive ENH CCG Y
29. Sonia Sharman Manor House Y
30. Michelle Myers PM Chells Way Surgery Apologies
31. Mary Bishop PM Stanmore Medical Group Y
32. Dr P Raveendran GP Bedwell Medical Centre Y
33. Dr A Cormack GP Shephall Way Surgery Y

2 | P a g e
1. Apologies and Introductions – RH welcomed everyone. Apologies – noted above Declarations of Interest – The Chair invited the Practice Representatives to reconfirm their current declarations on the Register of Interests were accurate and up to date and send their forms back to the CCG, informing them of whether or not there are any changes.
2. Integrated Provider Board – See attached notes
TOR – Revised draft has been circulated with amendment to the number of Target events. RH commented that further adjustment to the number of meetings – should be 7 - will need to be made before being agreed. DK will amend and circulate to get sign off. Action :
DK to amend TOR and circulate to group for sign off
3. Action notes from previous meeting (13th June 17) – see updated action log
4. HCT/Rapid Response
Staffing updates provided
Currently recruited 1 Case Management Nurse, still interviewing for more
5. Prescribing Update – See attached email from MD dated 9.7.17
Main items of discussion at the moment are repeat prescriptions and flu
Currently trying to increase the use of electronic prescriptions
Agreement was made to promote flu ethically and to ensure PharmaOutcomes is used
General issues around communications should hopefully be aided by pharmacies moving to nhs.net
Pharmacies have also agreed to get the patient to either tick and initial next to the item they want, or for the pharmacist to sign to say that they have seen patient in order to stop over order and ordering items not needed
Issues have also been caused by GPs moving surgeries, which has affected baselines, because of this, email will be being sent to practices shortly asking to confirm the names of the GPs in each surgery
KPIs and budget setting will be coming out soon
The next meeting with pharmacy has been organised to take place in 6 month time. It is a very useful meeting, so would encourage more GPs to attend.
6. Finance and Locality Information Pack (LIP) update (see pack)
LIP has been distributed, locality still in deficit
All localities have had an up-lift, figures being finalised and will be circulated by SA soon
Locality allocation:
SA reported that locality allocation has been approved by the CCG exec and is now going to the governing body. The methodology adopted in allocating funds to locality this year used option 3 approved in 2016-17 as a starting baseline. The CCG looked at the weighted population growth in each locality which for Stevenage is 1.35% and these were funded accordingly. The balance of the allocation was distributed equally to all locality (2.11%). For Stevenage the proposed 2017/18 funding is £112,048 (16.67%). CCG

3 | P a g e
finance is currently allocating budgets and monthly locality finance reports will be available for next month.
7. Mental Health Update
See newsletter attached
DMM updated: Looking to assign a senior to each practice – Cassie will be contacting practices individually to organise
8. LTC Update
KS reported that the last LTC meeting was held on the 29th of June, not much was covered but discussions did link in with catheters and UTI
9. GPFV and Access
See Denise Boardman presentation, attached
Extended access builds on extended hours as is being rolled out everywhere
There are 7 core requirements: o Timing of appointments o Capacity o Measurement o Advertising and ease of access o Digital o Inequalities o Access to wider system
Pre-bookable and same day appointments are the preference
Locality to discuss
RH requested PMs to discuss the options and decisions per practice during PM’s meeting and to ensure input from GPs at their practice is obtained before this meeting on the 20/07/17
Deadline given to advise CCG of locality decision – 09/09/17
£3.17 available for scheme
£1.50 transformational money available as enabling money which could be used to assist with setting up service and employing Project Manager
RH suggested all 6 localities coming together for workshop type meeting to discuss what each locality will be offering and how they are approaching this
1) 10.
AOB
AIVHS – New service has started putting notes directly into SystmOne systems such as “Note: GP to prescribe” just dropping documents into records with no tasking, and embedded letters. Comment made that this is worrying and could be missed by practices. BF will take this back to raise with HUC and AIVHS, JH to discuss with HCT
HUC – Directly booking into systems. Practices have not agreed for this to be an option. BF clarifies that process still needs to be agreed, but that it will be mandatory within 3 years
Non-tariff – RP observed variance figures against non-tariff lines on the report. He then asked if non-tariff is “block”, what is responsible for the variance. SA clarified that non-tariff does not necessarily mean “block” because there are activities with local prices reported within non-tariff lines. Any changes in activity compared to plan will result in variance.
Target Event – Next event is on the 20th of September, DK to circulate current agenda to PMs. Agenda needs admin/ PM training items. DK to circulate 2 additional dates for future targets, also suggested that 3 targets needed a year to cover the required topics.
4 | P a g e
CFF – Practices informed to forward any comments regarding Q1 to Barbara Harrison for the CFF Q1 Review.
£2.10 16/17 – Claims still being processed by DK and will advise.
Ardens – AS queried PM’s previous comment suggesting that every practice should be using the same system. Bedwell do not want to use Ardens as they feel that their templates are more user-friendly and capture all the info that is required. RH clarified that if it is templates which are making Bedwell reluctant to change, then they should be aware that templates can be changed on Ardens to reflect their ones. If Bedwell’s templates are better, CCG should amend and use the better ones.
o EoL template should not be used at the moment.
Health Visitors – Query as to whether or not they are around anymore. Clarified that some practices do still see them, whilst others do not.
Dates of Next Meeting: 12th Sept 2017 @ Cromwell Hotel, High Street Stevenage – 12.30 to 2.30pm Target Event – 20th Sept 17 at Stevenage Football Club 10th Oct 17 @ Cromwell Hotel
ACTIONS Person
Responsible
DATE
2) 1
1
1
1. Shephall – phlebotomy service - need a
phlebotomist to work from the surgery for their
patients.
Issue ongoing since Jan 2017. HED was dealing with
the matter with the Contracts team at the CCG and
TPP team.
Need to escalate to Harper Brown to resolve, as
Patients have a petition and are escalating.
DK 09.05.17 – HB to contact practice directly to discuss 11.07.17 – Ongoing, DK to discuss with HB and keep RH in the loop
2. Minor Injures evaluation report, Locality would like NC and The Executive Team to support what the locality can do next and also they want support in taking next steps, and funding. 21.02.17 – SE to feedback to the CCG and see what funding is available and see if we can go forward on this. 14.03.17 – Minor Injuries is not part of the CFF 2017/18. Need CCG confirmation if the Minor Injury scheme will be supported going forward. Needs to include QIPP and make savings, Locality need to agree to report. 11.04.17 – Locality need to highlight which specific injuries there are opportunities for, and produce a business case to the CCG for a service. This could be a good example of a new locality service. 12.09.17 – See email from SE
SE/CCG
BF to liaise with SE
11.07.17
Closed 12.09.7 see
email attached from
SE
3. Feedback regarding the phlebotomists and the issue of printing forms on Ice and also coming to the surgery without being able to sign in with their
DK Ongoing

5 | P a g e
smartcards. DK – emailed the service on 06.04.17 and is chasing the issues. Examples were requested from the team now. Emailed again 17.05.17, chased 06.06.17. Contract team dealing with the issues directly. Contract is changing from TPP – trying to find out who
will be taking over
11.07.17 – Practices requested to email DK with examples to establish whether sickness or annual leave is the problem, then DK will escalate to service with examples and dates
12.09.17 – no
feedback from
practices to DK
between 11.07.17
and 12.09.17
4. Get the GP Hotline Contracts Team to report to the locality, as to what actions are being taken and what has changed due to this. So the locality knows what has been done by them using the reporting tool. Common themes of issues.
Completed Closed - Circulated
with Agenda for
11/07/17
5.Diabetes service - issues raised by Karen Smith and locality, SE to liaise with the service 11.04.17 – KS has a meeting 12.04.17with the service to discuss Update 09.05.17 - KS spoke to HCT awaiting to meet up with them. 11.07.17 – KS reported that templates not being completed by consultants which affects 8 Care Processes and national guidance – feedback to diabetes group, practices to collect examples and issues and let DK know
SE Ongoing
6.Transgender – NC/HED to establish commissioning arrangements for issues for continuing support Ravi to email on behalf of the locality regarding the issues. To be forwarded to NHSE
Completed RP advised to close
this action 11.07.17
8. School Nursing services – MAG will contact and liaise/ update locality
Completed Closed
9.NDPP figures for the locality – locality want the figures they need to work from for CFF 2017/2018 11.07.17 – email has been sent, Fiona is collating, locality need coversion ratio
Completed Closed
10.E-Referrals - update on the target for the year end – data a few months behind. 11.07.17 – Year end target not met by 1%, Jamie Archer to email figures. Meeting being arranged for e-referrals with secretaries – DK to forward more info
DK/JA Ongoing
11. COPD Care Planning - DK to invite Emily Byway to PM meeting to discuss COPD Care Planning – outcome
Completed Closed 20/07/17

6 | P a g e
of meeting to be fed back to locality – Meeting to take place on the 20/07/17 at Chells
12. COPD - JC to feedback names of 68 patients identified in the locality who are in need of future care planning – liaising with practices to discuss
JC Ongoing
13. Acute Trust Rep - Representative from the Trust needed at every meeting 11.07.17 – JC confirmed Jenny Lohan to attend from September
JC Ongoing
14. Catheter Register - All practices to create a register of catheters, make sure locality has process in place, include community services 11.07.17 – Practices still doing searches
All Ongoing
15. TOR - DK to change wording in TOR around number of Target Events to 3 and Locality meetings to 7, circulate for agreement
DK Circulated 12.09.17
16. Gluten-free prescribing - Practices to complete survey by the 22nd June, choosing which of 3 options for gluten-free prescribing they would prefer
Completed Closed
17. CFF Cancer Element - DK to get clarification regarding what the 35p for education can be used for
DK Ongoing, just finalising answer
18. Council of Members - DK to circulate venues and dates for Council of Members meetings
DK Ongoing
19. Documents dropping into patient record - SystmOne practices finding documents, requests and notes dropped into records with no tasking, and embedded letters. Comment made that this is worrying and could be missed by practices. JH to discuss with HCT & AIVHS, BF to address with HUC & CCG colleagues Example from Stanmore to be forwarded to JH 12.09.17 – emails sent after 11.07.17 meeting by BF
JH/BF Ongoing
21. School Nursing services – School nursing not referring to CAHMS, relying on GPs to do the referral. Public Health commission this service, need to work closer with them JH to liaise with service to address the issues and discuss with AMM
JH/AMM Ongoing
22. Target Event – DK to send 20/09/17 agenda to PM’s DK to circulate two additional dates for future targets
DK Ongoing – 2 dates are- 30th Nov 17 and 8th Feb 18

1 | P a g e
MINUTES
Meeting: Stevenage ICPB and Locality Meeting
Date: Tuesday 12th September 2017 - 12.30 to 2.30pm
Venue: Cromwell Hotel, High Street, Old Town, Stevenage, SG1 3AZ.
Attendee do these Organisation Present
1. Dr Russell Hall (RH) Chair GP Chells Way Surgery Y
2. Dr Prag Moodley (PM) GP Stanmore Medical Group Y
3. David Myers (DM) Chells Way Surgery Y
4. Susan Lincoln (SL) PM Stanmore Medical Group Apologies
5. Mark Banks (MB) PM King George Surgery Y
6. Dr Rini Saha (RS) GP King George Surgery Y
7. Fiona Lucas (FL) PM Symonds Green Y
8. Dr Masood GP Symonds Green Y
9. Elaine Cook (EC) PM Bedwell Medical Centre Y
10. Allison Seymour (ALS) PM Bedwell Medical Centre Y
11. Sandra Copping (SC) PM Manor House Y
12. Karen Smith (KS) Nurse Manor House Y
13. Manjit Phugura (MP) PM Shephall Health Centre Y
14. Deena Keefe (DK) Locality Manager CCG Apologies
15. Barbara Harrison Assoc Director For Commissioning ENH CCG Apologies
16. Michelle Morrissey Team Administrator CCG Y
17. Sabina Tai (ST) HomeFirst & Rapid Response Project Manager Apologies
18. Sharn Elton (SE) Director Operations and Resilience CCG Y
19. Maxine Davis(MD) Senior Pharmaceutical Advisor ENHCCG Apologies
20. Della McMurdo (DMM) HPFT Service Mgr community Mental Health Y
21. Julie Hoare (JH) HCT Director of Service Development and Partnerships
Y
22. Yasha Rai (YR) HCT Community Locality Manager Y
23. Jacqui Carrett (JC) Service Manager ICRS Y
24. Dr K Daodu GP Shephall Way Surgery Apologies
25. Michael Henderson HPFT Services Lead Apologies
26. Sean Dale-Molloy HomeFirst/ Rapid Response Apologies
27. Sunday Adeniyi (SA) ENH CCG Y
28. Sonia Sharman Manor House Apologies
29. Michelle Myers PM Chells Way Surgery Y
30. Mary Bishop (MPB) PM Stanmore Medical Group Y
31. Dr P Raveendran (PR) GP Bedwell Medical Centre Apologies
32. Dr A Cormack GP Shephall Way Surgery Apologies
33. Dr Imon Chakraborty GP Stanmore Medical Group Y
34. Dr M Duggan GP Manor House Y
35. Dr L Epstein GP Shephall Way Surgery Y
36. Sarah Bell Medical Director Garden House Hospice Care Y
37. Ken Moore (KM) PPG Representative Y

2 | P a g e
38. Rajeev Kaja (RK) GP Stanmore Medical Group Y
39. Luke Maddocks (LM) King George Surgery Y
40. James Gleed (JG) Assoc Director For Commissioning ENH CCG Y
41. Dr Zaid Ismail (ZI) GP IT Lead – ENH CCG Y
42. Shane Scott (SS) Head of Primary Care ICT – ENH CCG Y
43. Sarah Brennan Business Change Analyst HBLICT Y
1. Apologies and Introductions – PM welcomed everyone. Ken Moore, PPG Representative gave a brief introduction, informing the locality that he is the chair of the PPG at Stanmore and is an ambassador for Healthwatch in Stevenage. Apologies – noted above Declarations of Interest – The Chair invited the Practice Representatives to reconfirm their current declarations on the Register of Interests were accurate and up to date and send their forms back to the CCG, informing them of whether or not there are any changes.
2. Integrated Provider Board – See attached notes and action log.
Feedback on current projects
TOR – Revised draft has been circulated with amendment to the number of meetings, and now agreed as Final.
3. Action notes from previous meeting (11th July 17) – see updated action log All attendees agreed the minutes of 11th July 2017 as an accurate representation.
4. HCT/Rapid Response
Staffing update - 2 x community psychiatric nurses established within the Stevenage team
58% of referrals are stabilised and sent back to GP services
RH mentioned an issue regarding a referral to Rapid Response which they tried to put through at 6pm, it was declined as they did not have anyone available to prescribe, and it looked like the patient may have needed medicines prescribed. RH queried whether or not the service has cover available with someone who can prescribe.
YR agreed that they should have taken it and aimed to put it through the following day, will look into it and make sure it does not happen again
PM suggested looking into a link with Out Of Hours so it would just be a case of just going to them to prescribe, but the care could still be offered.
5. Prescribing Update – Wound products –
JH updated that a paper for Stevenage Locality was submitted to the Board about the availability of having centralised wound products, so nurses wouldn’t have to fill out forms and submit to GPs to prescribe. This has also been fed into the STP to be considered. May not be a cost saving but definitely a time saving process.
Other ideas to save time and costs were also suggested. JH recommended submitting

3 | P a g e
any cost/time saving ideas to the operational group who will look into them.
MPB suggested that the coloured forms should be looked at as that would save a lot of time
Community diabetic nurse requests and changing the diabetics prescription system was also suggested
SE suggested that the locality should start looking at further work streams that may be of interest
PM commented that only one GP attends the operational group and encourages more to attend if they can, as they will be leading on these ideas and their input will be useful.
Prescribing update RS reported:
Prescribing update is on phase 3 switches looking at various other medications. Practices will be provided with a breakdown on how much they have spent and saved
KPIs do look like the locality are not achieving a lot at the moment, but this is mainly down to the following:
o Locality have been encouraged to use Nitro instead of Trimethoprim as this is the switch they are doing the worst on comparatively
o Blood glucose strips: the threshold has gone to 70% which is why the locality are in the red
o Combination inhalers are improving within the locality but the threshold is being increased
KS raised the issue of practices making a clinical decision not to prescribe antibiotics and then patient is seen by OOH who prescribe antibiotics with the same symptoms.
Another point also made about just in case boxes and prescribing regimes. There is currently an Ardens template which provides pre-printed prescription sheets which allows for an increase in medication so the patient doesn’t have to come back into the practice to get changes, which also can cause delays to patients in pain – this can be quite time-consuming for GPs
PM comments that this is a piece of work which Dr Balam could look at as it would save time
LM informed the locality of a template Bedford use for End of Life care which automatically updates when you insert just in case meds details – RP commented that this has already been tried and was not accepted, although RH commented that this system is currently used in Chells Way and that it does work
There is currently an issue in Arden as it does not print it as a yellow form
PM suggests the JH should put this down on the agenda as an area to look at as it would save lots of time
RK confirmed that it is mainly about the controlled drugs and how they want you to sign off on the controlled drugs individually
6. Finance and Locality Information Pack (LIP) update (see pack)
SA informed the locality that the allocation for the year has been circulated, Stevenage allocation for the year is around £112 million
Monthly reports will be sent, but will be running 2 months behind
Latest report available is for Q1 and currently shows an overspend of £208k
When broken down, this overspend is mainly down to prescribing which is around £140k
Acute spend has gone down, but prescribing is an obvious issue for Stevenage locality
EC queried what the value is of the Continuing Health Care money, SA clarified that it is around £5.4m for the year, and that he is still seeking clarification as to how much of that can be controlled by the locality
RH commented that finance have told them previously that it is part of the CCG budget,

4 | P a g e
and that the locality should be aware of these costs even though they have no control over them
Locality would like a further breakdown regarding their overspend and possibly what groups or categories of prescribing in comparison to other localities
MPB queried how the prescribing budget was distributed this year, it was clarified that it was fair shares
SE commented that if the locality are able to see a reduction in A&E admissions over the course of the year then this may in turn put more pressure on areas such as prescribing, so that maybe there should be a way of tracking that throughout the coming year, although RH commented that it is for that reason that they do not look at individual parts of the budget but the budget as a whole
7. Mental Health Update
PM reminded the locality about Learning Disability Health Checks and that the template has now been changed. The new template is available on Ardens and is a national template.
He highlighted that information needs to be sent to the carer prior to the checks due to the carer having a lot of work to do before the health check
PM also mentioned that the data from the last year’s health checks has not been fed back properly as they are being told that they achieved 46% overall, when an internal audit showed this to be closer to 80%, so please make sure practices are sending the data otherwise payment will not be made
PM also mentioned Health Young Minds in Herts which is a new website and a new resource. PM recommends using the website for guidance if you do not know what to do with a patient
A comment was made that the service does refer patients back to GPs however, with one patient spending 45 minutes on the phone to Health Young Minds, only to be told to return to their GP
Another query was also made regarding how the service differs from Kooth, PM clarified that Kooth is on this service as is only a counselling service
PM also commented that the locality should continue with the Dementia work as they have previous done very well and that they should continue to meet their targets
8. LTC Update
IC commented that following on from the UTI update, more guidance regarding what antibiotics to use is now available on the CCG website alongside a video
Herts Valleys are also piloting Social Prescribing and are currently recruiting to help navigate and prescribe the most appropriate route, if it is successful then it could be implemented in Stevenage.
CFF the take home message was mainly to continue what the locality are doing and they should receive payment
KS commented that MyPlan has not been passed, so the locality should continue what they are already doing, and also highlighted that the social prescribing is more to do with prescribing help and care than drugs
Query raised regarding what is the difference between Herts Help and social prescribing, KS confirm that they are the same thing with a different name
9. GPFV and Access
RK clarified that extensive discussions have taken place over the last couple of months at Federation meetings, but after an initial vote practices decided not to provide the service through the federation due to the costings. However, there was a discussion at the

5 | P a g e
practice managers meeting 31.08.17 which has led to the federation being asked to look into this yet again.
The federation will be holding a meeting on the 13.09.17 to discuss and will feed back after this meeting. Locality in agreement that the service should be offered via the federation for all locality patients in order not to procure the service.
PM commented that if the federation says no to doing extended access at the meeting on the 13.09.17 Stanmore Medical Group will go ahead and provide the service, which will be open to any practice who may want to collaborate as they do not want another provider to come into the locality to provide this service on their behalf
Question raised regarding continuance of the existing Extended Hours DES as some practice’s do not believe they have time to provide both. PM clarified that extended hours will continue as it stands for now, but in the future questions might be asked as to how cost effective it is to run both services, he also commented that as a practice they will not be offering both services at the same time.
JG clarified that the DES is expected to continue until the end of April 2018, so it will run alongside the extended access
RH also commented that they are two different services, as extended access is a locality based project for the CCG as a whole, looking at providing 50% this year and 100% next year, whereas the DES is an individual practice decision, so there is a possibility that the federation takes extended access on, and then practices decide whether to participate in the DES on an individual basis.
Alternatively, if Stanmore decide that they are large enough to take that on for the locality then the federation will be able to provide more workforce not less, so practices could decide to do both depending on their individual circumstances
1) Winter Resilience
JG outlined that the CCG is very keen to work with a few localities or a few groups of practices within the locality to look at piloting additional winter schemes at a greater scale than just a single practice and to use a single clinical record, which SystmOne will allow.
SS commented that there are a number of ways in which practices can work together, but that we are looking for some practices to explore the options in more detail, and how to use shared appointments and records
PM queried which practices would be interested in looking at this – all practices confirmed that they would be willing to take part
RP queried why this is being brought up as winter pressure and whether the funding will be coming from there – PM clarified that this is being looked into now so that when extended access is in place the IT issues are already sorted out
JG adds to this that if the IT is not sorted out before extended access then the service will fail
MPB queried how 111 will fit into this picture, JG highlights that there is also an opportunity for one or more practices to pilot direct booking from integrated urgent care. This is a target for the CCG for next year, so it would be beneficial to work with some practices now to establish the technological requirements of how this might work.
King George Surgery was previously involved in something a bit like this with 111, MB comments that if 111 are now on SystmOne they should be able to book straight in without problems
JG queried whether they would then be interested in piloting again now that 111 is using SystmOne, MB replies that it would potentially be an option
LM comments that if the locality had digital dictating then GPs would be able to see patients anywhere and the dictating would go back to their own secretaries to the

6 | P a g e
registered practice – SS comments that the infrastructure behind that idea is quite complex. It could be an option further down the line but could not be seen as a possibility quite yet.
2) 10.
AOB
£1pp 2017/2018 use for training – EC outlined that the locality will pay out the money as agreed in the practice Manager’s meeting on 31.08.17, and now draw a line under the issue. The name of the funding will be changed to Training Budget instead of the e-Learning Budget and this year can be spent on either e-learning or in house training dependant on individual preference as already agreed at the Practice Managers meeting on 31.08.07. Money for 2018/19 will be discussed nearer the time, and the options of E-learning or face to face training, bearing in mind the cost of the package may depend on the numbers. Decision approved at this meeting by all members.
Dr Zaid Ismail – wanted to let locality know that he is happy to help practices with IT for GPFV should they need it, alongside Martina Vogel-Matthews.
Winter Resilience – MPB outlined that SL has submitted a plan, and the idea has been backed by RH, which includes carrying out ward rounds on a Wednesday. The request went through to Jo Burlingham who replied that strong rationale would be needed to support another care home round on a Wednesday in terms of the impact on the out of hours period. The governing body recognised the benefit of carrying out an additional ward round on a Friday afternoon or Monday morning even though it is not directly in the out of hours period (as suggested by the requirements), but suggests that a Wednesday would be difficult to justify. RH explained that the new guidance did not allow funding for this, so to justify funding, they would have to be able to rationalise how it is value for money and will reduce admissions and call outs. RH comments that it would be best to get as much rationale and evidence together, put the plan in, copy SE and RH in and see what the response is. RH will support any evidence SL is able to provide. Need to evidence why and justify the In Hours element and RH suggested that if there is any £1pp money left it could be considered to be used for additional ward rounds.
Flu funding – Stevenage plan tweaked and resubmitted following email from James Gleed/ Harper Brown and comments about the plan.
Inhalers – EC commented that community matrons should be able to prescribe branded inhalers rather than generic
Federation – EC would like to thank the federation for all of their hard work so far for GPFV and Access, and would like everyone to support them every way they can as they have put a lot of work into everything.
Patient rep – PM comments that from the next meeting onwards there will be a standing item of patient feedback, encourages KM to ask any questions he may wish to know. KM queries how many of the practice around the table have a functioning PPG – every practice confirmed that they did.
Shephall Phlebotomy – discussed in action log – discussed at Practice managers meeting 31.08.17 and approved today, all agreed to buy additional clinics for Shephall using the £1pp from 17/18 as the CCG do not have any additional funding and cannot make any changes to the existing contract which is on a block basis until March 2019. TPP Service will be procured in 2019. DK will liaise with Shephall and also the contracts team to start the process, staffing costs etc. DK discussed at PMs meeting at the possibility of locality piloting their own staff carrying out phlebotomy sessions, in readiness for a future service.

7 | P a g e
Dates of Next Meeting: Target Event – 20th Sept 17 at Stevenage Football Club 10th Oct 17 @ Cromwell Hotel 14th Nov 17 @ Cromwell Hotel
12th Dec 17 @ Stevenage Football Club (note Change of venue for this meeting only)
ACTIONS Person
Responsible
DATE
3) 1
1
1
1. Shephall – phlebotomy service - need a
phlebotomist to work from the surgery for their
patients.
Issue ongoing since Jan 2017. HED was dealing with
the matter with the Contracts team at the CCG and
TPP team.
Need to escalate to Harper Brown to resolve, as
Patients have a petition and are escalating.
09.05.17 – HB to contact practice directly to discuss 11.07.17 – Ongoing, DK to discuss with HB and keep RH in the loop 12.09.17 – locality agreed to use £1pp 17/18 to
purchase additional clinics for Shephall.
DK 12.09.17 – Ongoing - £1pp money agreed to be used to ask TPP whether they can provide staffing MP to liaise with Commissioning Team and DK to resolve
2. Minor Injures evaluation report, Locality would like NC and The Executive Team to support what the locality can do next and also they want support in taking next steps, and funding. 21.02.17 – SE to feedback to the CCG and see what funding is available and see if we can go forward on this. 14.03.17 – Minor Injuries is not part of the CFF 2017/18. Need CCG confirmation if the Minor Injury scheme will be supported going forward. Needs to include QIPP and make savings, Locality need to agree to report. 11.04.17 – Locality need to highlight which specific injuries there are opportunities for, and produce a business case to the CCG for a service. This could be a good example of a new locality service. 12.09.17 – See email from SE- closed
SE/CCG
BF to liaise with SE
11.07.17
Closed 12.09.7 see
email attached from
SE
3. Feedback regarding the phlebotomists and the issue of printing forms on Ice and also coming to the surgery without being able to sign in with their smartcards. DK – emailed the service on 06.04.17 and is chasing the issues. Examples were requested from the team now. Emailed again 17.05.17, chased 06.06.17.
DK Ongoing
12.09.17 – no
feedback from
practices to DK
between 11.07.17

8 | P a g e
Contract team dealing with the issues directly. Contract is changing from TPP – trying to find out who
will be taking over
11.07.17 – Practices requested to email DK with examples to establish whether sickness or annual leave is the problem, then DK will escalate to service with examples and dates 12.09.17 – no feedback rec’d to date from practices
and 12.09.17
4. Get the GP Hotline Contracts Team to report to the locality, as to what actions are being taken and what has changed due to this. So the locality knows what has been done by them using the reporting tool. Common themes of issues.
Completed Closed - Circulated
with Agenda for
11/07/17
5.Diabetes service - issues raised by Karen Smith and locality, SE to liaise with the service 11.04.17 – KS has a meeting 12.04.17with the service to discuss Update 09.05.17 - KS spoke to HCT awaiting to meet up with them. 11.07.17 – KS reported that templates not being completed by consultants which affects 8 Care Processes and national guidance – feedback to diabetes group, practices to collect examples and issues and let DK know
SE Ongoing
12.09.17 – No
update, waiting to
hear from secondary
care
6.Transgender – NC/HED to establish commissioning arrangements for issues for continuing support Ravi to email on behalf of the locality regarding the issues. To be forwarded to NHSE
Completed RP advised to close
this action 11.07.17
8. School Nursing services – MAG will contact and liaise/ update locality
Completed Closed
9.NDPP figures for the locality – locality want the figures they need to work from for CFF 2017/2018 11.07.17 – email has been sent, Fiona is collating, locality need coversion ratio
Completed Closed
10.E-Referrals - update on the target for the year end – data a few months behind. 11.07.17 – Year end target not met by 1%, Jamie Archer to email figures. Meeting being arranged for e-referrals with secretaries – DK to forward more info
DK/JA Ongoing – email
from JA dated 30th
June and 28th July
Resent the locality
11. COPD Care Planning - DK to invite Emily Byway to PM meeting to discuss COPD Care Planning – outcome of meeting to be fed back to locality – Meeting to take place on the 20/07/17 at Chells
Completed Closed 20/07/17

9 | P a g e
12. COPD - JC to feedback names of 68 patients identified in the locality who are in need of future care planning – liaising with practices to discuss
JC Closed
13. Acute Trust Rep - Representative from the Trust needed at every meeting 11.07.17 – JC confirmed Jenny Lohan to attend from September
JC Closed
14. Catheter Register - All practices to create a register of catheters, make sure locality has process in place, include community services 11.07.17 – Practices still doing searches
All Closed
15. TOR - DK to change wording in TOR around number of Target Events to 3 and Locality meetings to 7, circulate for agreement
DK Closed
16. Gluten-free prescribing - Practices to complete survey by the 22nd June, choosing which of 3 options for gluten-free prescribing they would prefer
Completed Closed
17. CFF Cancer Element - DK to get clarification regarding what the 35p for education can be used for
DK Ongoing, just finalising answer
18. Council of Members - DK to circulate venues and dates for Council of Members meetings 7
th Dec 17 – Fielder Centre,, Hatfield, 12.30-4.00pm
8th
March 18 – Robertson House, Six Hills Way, Stevenage.
DK Closed.
19. Documents dropping into patient record - SystmOne practices finding documents, requests and notes dropped into records with no tasking, and embedded letters. Comment made that this is worrying and could be missed by practices. JH to discuss with HCT & AIVHS, BF to address with HUC & CCG colleagues Example from Stanmore to be forwarded to JH 12.09.17 – emails sent after 11.07.17 meeting by BF
JH/BF Ongoing 12.09.17 – example need to be sent to JH, this is still happening, predominately blood and bowel services
21. School Nursing services – School nursing not referring to CAHMS, relying on GPs to do the referral. Public Health commission this service, need to work closer with them JH to liaise with service to address the issues and discuss with AMM. JH confirmed that Kay Gilmour has suggested that she comes to the locality meeting and discusses what the service offers and the changes. [email protected])
JH/AMM Ongoing 12.09.17 – service has offered to attend locality or practice mangers meeting, PM will follow up and ask them to attend
22. Target Event – DK to send 20/09/17 agenda to PM’s DK to circulate two additional dates for future targets – 30th Nov 17 and 8th Feb 18
DK Closed
23. ICPB Agenda - JH to look into just in case medication and prescribing changes as an area which could be changed to save time for GPs
JH Ongoing
24. Locality Meeting Agenda – Patient Feedback to be added as a standing item
DK Completed 10.10.17

10 | P a g e

1 | P a g e
MINUTES
Meeting: Stevenage ICPB and Locality Meeting
Date: Tuesday 10th October 2017 - 12.30 to 2.30pm
Venue: Cromwell Hotel, High Street, Old Town, Stevenage, SG1 3AZ.
Attendee do these Organisation Present
1. Dr Russell Hall (RH) Chair GP Chells Way Surgery Y
2. Dr Prag Moodley (PM) GP Stanmore Medical Group Y
3. David Myers (DM) Chells Way Surgery Apologies
4. Susan Lincoln (SL) PM Stanmore Medical Group Apologies
5. Mark Banks (MB) PM King George Surgery Y
6. Dr Rini Saha (RS) GP King George Surgery Y
7. Fiona Lucas (FL) PM Symonds Green Apologies
8. Dr Masood GP Symonds Green Apologies
9. Elaine Cook (EC) PM Bedwell Medical Centre Y
10. Allison Seymour (ALS) PM Bedwell Medical Centre Y
11. Sandra Copping (SC) PM Manor House Y
12. Karen Smith (KS) Nurse Manor House Y
13. Manjit Phugura (MP) PM Shephall Health Centre Y
14. Deena Keefe (DK) Locality Manager CCG Y
15. Barbara Harrison Assoc Director For Commissioning ENH CCG Apologies
16. Michelle Morrissey Team Administrator CCG Y
17. Sabina Tai (ST) HomeFirst & Rapid Response Project Manager Y
18. Sharn Elton (SE) Director Operations and Resilience CCG Apologies
19. Maxine Davis(MD) Senior Pharmaceutical Advisor ENHCCG Apologies
20. Della McMurdo (DMM) HPFT Service Mgr community Mental Health Apologies
21. Julie Hoare (JH) HCT Director of Service Development and Partnerships
Apologies
22. Yasha Rai (YR) HCT Community Locality Manager Y
23. Jacqui Carrett (JC) Service Manager ICRS Y
24. Michael Henderson HPFT Services Lead Y
25. Sean Dale-Molloy HomeFirst/ Rapid Response Apologies
26. Sunday Adeniyi (SA) ENH CCG Y
27. Michelle Myers PM Chells Way Surgery Y
28. Mary Bishop (MPB) PM Stanmore Medical Group Y
29. Dr P Raveendran (PR) GP Bedwell Medical Centre Y
30. Dr A Cormack GP Shephall Way Surgery Apologies
31. Dr Imon Chakraborty (IC) GP Stanmore Medical Group Y
32. Dr M Duggan GP Manor House Y
33. Dr L Epstein GP Shephall Way Surgery Y
34. Dr Sarah Bell Medical Director Garden House Hospice Care Apologies
35. Ken Moore (KM) PPG Representative Y
36. Dr Rajeev Kaja (RK) GP Stanmore Medical Group Y
37. Hannah Wright Stevenage HCT ACS Team Manager Y

2 | P a g e
38. Jenny Lohan (JL) General Manager NHS Trust Y
39. Matthew Charles Age UK Apologies
1.
Apologies and Introductions – RH welcomed everyone. Jenny Lohan, General Manager from the NHS Trust introduced herself. She manages cardiology, respiratory, renal, diabetes and end of life, but also has an input into ED, stroke and frailty. The locality asked her some questions:
ALS queried E-referral issues, JL commented that Lorenzo changeover had caused issues, but once it is up and running and staff are used to it, problem should be addressed.
JL commented that she will take back and check whether Choose and Book was working. Also commented that the biggest impact was from patient DNAs, and that working to reduce DNAs would reduce overall waiting times. Locality raised the issue of not having sufficient appointments to be booked via Choose and Book.
Increase in demand has also affected bookings, and putting on more clinics is the only option, but is not simple as will have to find a clinician to put on these clinics.
PM commented about ensuring all consultants are aware that they are able to give a medical certificate to patient’s, as they often come straight from an appointment to the doctors as the consultant will not give them a certificate. PR commented that he has seen some who were given certificates for longer than 2 weeks. This is a waste of both patient and practice time – many consultants are unaware that they can write these. Any examples of this please also forward to RH, as this is now national guidance.
Query regarding lack of diabetes foot checks was also raised. JL commented that Locality requested that it would be good if the templates were completed as it would help them.
PM suggested that the group email any queries and issues they have for JL to DK, who will forward to JL to take back.
MPB queried patients without an NHS Number being automatically rejected, asked whether a process to ensure not automatically rejected is put into place.
Apologies – noted above Declarations of Interest – The Chair invited the Practice Representatives to reconfirm their current declarations on the Register of Interests were accurate and up to date and send their forms back to the CCG, informing them of whether or not there are any changes.
2. Integrated Provider Board – See attached notes and action log.
Feedback on current projects
Items discussed: o UTI o Discharge Home to Assess o Anxiety Screening Tool o Frailty o EoL

3 | P a g e
3. Action notes from previous meeting (12th September 17) – see updated action log All attendees agreed the minutes of 12th September 2017 as an accurate representation. Correction - Dr Raveendran did attend but did not sign in.
4. HCT/Rapid Response Capacity update:
8 patients on Rapid Response case load
71 patients on Rapid Response case management
Rapid Response case load still has capacity available
YR encouraged more practices to try to make maximum number of referrals where they can
5. Prescribing Update – RS gave update:
NRT -Highlighted that (NRT) Nicotine Replacement products will not be available on FP10 wef 1st of October 2017.Voucher scheme (letter) available on S1. Funding has been removed by Public Health England for this unless request goes through the appropriate channels.
Now only able to get NRT products by going to a No Smoking service who hold a contract with Public Health, letter will then be given to the patient then products available.
However, the service will only able to prescribe 2 weeks’ worth of a single product, unless patient is pregnant.
RS commented that practice’s should not be prescribing these on FP10
Bedwell Medical Centre, Manor House and Stanmore have the highest figures for this
Within the last 4 months around £8,000 would have been spent on nicotine replacement, and continuing to do this through FP10 means this money will come out of the locality prescribing budget.
Housebound - Query raised regarding the best procedure for housebound patients, RS confirmed that in these circumstances use normal referral and state that the patient is housebound, only truly housebound patients should be referred by the clinicians, with the client’s permission and not self-referral, so that it can be confirmed that they are housebound and it is safe to visit.
Transgender shared Care - Further update provided on transgender shared care. All localities have come to the conclusion that they are not comfortable with transgender prescribing as it is very specialist and many of the drugs have side-effects. Consultation has been opened because of this, finishing on the 16th October 2017.
All localities have specified that they would like the initiation and ongoing management of drugs related to gender care to remain with the specialist
Low Priority drugs for NHS Funding - Another consultation has been set up regarding drugs which are low priority for NHS funding, this contains a list of 18 drugs.
RS recommends that everyone shares their view on both consultations for their views.
Heparin - Prescribed from hospital query from KS, RS commented that it is best to remember that the hospital do everything and care of the patients i.e. from Obs and Gynae, except from patients at risk, such as cancer who are on long term Heparin.

4 | P a g e
OTC – Over the Counter (OTC) consultation has gone into the national programme, the CCG will issue guidance once aware, but the current guidance still states that you “should not”, not that you “cannot” prescribe for patients. All colleagues in the CCG should be following the same policy.
The aim now is to change patient behaviour towards this instead, which is where patient representatives can help by delivering this message to patients that the NHS is struggling, so to keep essential services free and available the public will need to pay for certain things where they can.
Issues with cross-charging between Stevenage, Knebworth and Marymead is still causing issues for finance so no update available yet on the target.
6. Finance and Locality Information Pack (LIP) update (see pack)
SA confirmed that there is nothing to add to last month’s report, once the next report is available it will be sent to all and discussed at the next meeting.
7. Mental Health Update
See Newsletter emailed to all.
New referral form for CAMHS is now available and for Mental Health on Ardens
PM warns that some may not be happy with the new form, but it has been developed by mental health leads across the CCGs by looking at the referrals sent to HPFT and the time taken to chase up information, which is wasting their time and resources
PM commented that the form looks long but it is asking for basic information and will reduce the amount of feedback and rejections sent from HPFT
GPs do not have to use this form if they do not want to and the referral will still be accepted, but PM recommends including all of the information stated on the form in the letter, otherwise it will be rejected.
Dementia - PM asked the locality to continue working on dementia diagnosis, as Stevenage locality have been doing well picking up on screening.
8. Children’s Services – School Nursing
See presentation, attached
Provide public health programme for children, service commissioned by the local authority
Websites for teens, parents and carers has been set up, as well as a text service for 11-19 year olds.
Immunisations are still carried out by the service, but is due to go to procurement soon
ALS queried whether the referral forms can be provided in a word or PDF format? It was confirmed that this is not available yet, but is something the team will look into
RP queried how immunisation information gets back to the practice – service clarified that a report in provided weekly and uploaded to SystmOne
Query raised around the confusion with CAMHS and referrals which practices are not made aware of. CAMHS bounced back a referral which was made by school nursing service without informing the doctors. Service confirmed that the GP should have been copied into the referral to CAMHS.
PM commented that locality were not aware that the service could refer direct to
5 | P a g e
CAMHS, service confirmed that if they are working with a child they are expected to do their own referrals.
ALS commented about ADHD referrals and whether or not the service refers using a CAF and doctor input? Service replied that they may not involve the GP unless they have been previous involved with the issue, they also commented that they are under the impression that the ADHD pathway was via a GP, so will try to remind schools of the correct process.
PM queried the process regarding children with mental health issues, service clarified that they do an assessment and then follow whichever pathway meets the child’s needs, but if they could not meet these needs would refer up. PM queried whether this was referral up to tier 1 or 2, service clarified they refer to tier 1.
PM also queried the service’s capacity and waiting times – service confirmed that there are currently no staffing vacancies, but that the service is small. Regarding referrals, they offer appointments within 4 weeks, however can struggle to meet that target sometimes.
3 part-time nurses cover the Stevenage area, with a support team.
Posters provided detailing the websites.
9. LTC Update
Last meeting was held in August, the next one is not due until November 2017.
IC commented that there is still an ongoing issue being discussed via email is LTC section of the CFF and the lack of clarity around how many should fall into the 2 or more LTC category and how to make it more fair
DK confirmed that CCG has agreed: the national figure for patients with LTC is around 6%, so practices should identify patients with 2 or more LTC that are not included in the frailty index and should be looking at approximately 2% of the overall practice population. Out of that 2% the CFF asks that 60% of these identified should have care plans. However, please remember that practices should already be carrying out reviews on all their patients via QOF.
DK is available to assist and clarify if any of the practices need support. IC requested this confirmation by email as he had not seen this guidance.
MB queried whether Ardens is up and running and all of the appropriate templates are now available? PM clarifies that this process is still ongoing and they are going through forms systematically and updating.
10. 10 Patient Participation Group Update
KM has been in contact with the Carers Lead for Stevenage, with a meeting due to be step up with the Carer Champions for November to establish what the champion’s role is and what else they would like to be able to do.
The Stevenage Dementia National Alliance group has been set up with help from the Alzheimer’s Society but are struggling to meet due to the person who was organising the meeting leaving the council.
KM also in the process of trying to set up a meeting with all the chairs of the PPG’s in Stevenage.
KM also attended meeting with North Herts CVS which involved encouraging more people to go to the chemist.
KM will look into funding for EoL project.
KM to be added to the mailing list

6 | P a g e
11. 10.
AOB
Extended Access Update: MB updated that a working group has been set up to look at extended access. The group are currently considering potential locations and key areas, and how to fill the appointments that will be available. The paperwork for the transformation money has been completed, and a meeting has been arranged with Dee Boardman and James Gleed to gain feedback on 12.10.17. Locations - emails have been sent to the owners of possible buildings to see whether they would be available for use.
Cancer 2ww audit: RH recommended that all look at the paperwork which was distributed with the pack regarding referrals and looking at issues such as some practices using old forms. ALS queried the recommendation that a sticker be placed on the report with information regarding the referral, PM commented that they usually say to the patient that if they have not heard in two weeks to phone the secretaries and find out why.
Delegated Commissioning: RH advised that this will be on next month’s agenda and that there will be a vote towards the end of the year where it will be decided whether or not to go delegated. No recommendation has been made by the GB yet.
CDC: RP received a referral from the school nurse to refer to the CDC, but it was declined saying to look at website, RP is not sure how to proceed with this. RH advised trying to send the referral to CDC step 2.
Pine Lodge Hospital Contract - RP asked whether the pathway can be reviewed when it comes up for renewal, as it is not working. RH recommended reporting any issues like that to the contracts hotline as they can address these at the Contract meetings.
Diabetes Visits - Dr Winicour: MB queried whether Dr Winicour will be sending out dates or whether practices need to contact him. DK clarified that there is no requirement in this year’s CFF to do that but practices can if they would like to as it would be advantageous, however an improvement plan does need to be completed for each practice as part of CFF.
Dates of Next Meeting: 14th Nov 17 @ Cromwell Hotel 30th Nov Target Event @ Stevenage Football Club 7th Dec Council of Members @ Fielder Centre, Hatfield. 12th Dec 17 @ Stevenage Football Club (note Change of venue for this meeting only) 8th Feb Target Event @ Stevenage Football Club 8th March Council of Members @ Robertson House, Six Hills Way, Stevenage.
ACTIONS Person
Responsible
DATE
1) 1
1
1
1. Shephall – phlebotomy service - need a
phlebotomist to work from the surgery for their
patients.
Issue ongoing since Jan 2017. HED was dealing with
the matter with the Contracts team at the CCG and
TPP team.
Need to escalate to Harper Brown to resolve, as
DK 12.09.17 – Ongoing - £1pp money agreed to be used to ask TPP whether they can provide staffing MP to liaise with Commissioning Team and DK to resolve
7 | P a g e
Patients have a petition and are escalating.
09.05.17 – HB to contact practice directly to discuss 11.07.17 – Ongoing, DK to discuss with HB and keep RH in the loop 12.09.17 – locality agreed to use £1pp 17/18 to
purchase additional clinics for Shephall.
10.10.17 – now with contracts team to organise, and
liaise with the Trust
3. Feedback regarding the phlebotomists and the issue of printing forms on Ice and also coming to the surgery without being able to sign in with their smartcards. DK – emailed the service on 06.04.17 and is chasing the issues. Examples were requested from the team now. Emailed again 17.05.17, chased 06.06.17. Contract team dealing with the issues directly. Contract is changing from TPP – trying to find out who
will be taking over
11.07.17 – Practices requested to email DK with examples to establish whether sickness or annual leave is the problem, then DK will escalate to service with examples and dates 12.09.17 – no feedback rec’d to date from practices.
DK Closed
5.Diabetes service - issues raised by Karen Smith and locality, SE to liaise with the service 11.04.17 – KS has a meeting 12.04.17with the service to discuss Update 09.05.17 - KS spoke to HCT awaiting to meet up with them. 11.07.17 – KS reported that templates not being completed by consultants which affects 8 Care Processes and national guidance – feedback to diabetes group, practices to collect examples and issues and let DK know. 10.10.17 – JL will take this back and liaise with the team.
SE / JL/ KS Ongoing
12.09.17 – No
update, waiting to
hear from secondary
care
10. E-Referrals - update on the target for the year end – data a few months behind. 11.07.17 – Year end target not met by 1%, Jamie Archer to email figures.
DK/JA Closed

8 | P a g e
Meeting being arranged for e-referrals with secretaries – DK to forward more info 10.1017 – Data released only up until May, Jamie Archer is looking into it. Resent data 06.10.17.
17. CFF Cancer Element - DK to get clarification regarding what the 35p for education can be used for. 10.10.17 – 35p can only be used for education event, locality have decided not to use Hot Topics. DK and KS to liaise re: Target Event 30.11.17
DK Closed
19. Documents dropping into patient record - SystmOne practices finding documents, requests and notes dropped into records with no tasking, and embedded letters. Comment made that this is worrying and could be missed by practices. JH to discuss with HCT & AIVHS, BF to address with HUC & CCG colleagues Example from Stanmore to be forwarded to JH 12.09.17 – emails sent after 11.07.17 meeting by BF If we do not get any examples sent to Julie by the 24th October 2017, we propose to close the action. [email protected]
JH/BF Ongoing 12.09.17 – example need to be sent to JH, this is still happening, predominately blood and bowel services
21. School Nursing services – School nursing not referring to CAHMS, relying on GPs to do the referral. Public Health commission this service, need to work closer with them JH to liaise with service to address the issues and discuss with AMM. JH confirmed that Kay Gilmour has suggested that she comes to the locality meeting and discusses what the service offers and the changes. [email protected])
JH/AMM Closed – attended 10.10.17 ICPB mtg
23. ICPB Agenda - JH to look into just in case medication and prescribing changes as an area which could be changed to save time for GPs. 10.10.17 – all to email JH ideas.
JH Ongoing
24. Locality Meeting Agenda – Patient Feedback to be added as a standing item
DK Completed 10.10.17
25. Outpatient Certification - Still seems to be an ongoing problem despite going through the contracts hotline. Please copy in the GP liaison at ENHT any queries regarding outpatient certification of patients to: Claire Checkley [email protected] Please send any examples. Med Certs - All to ensure that any examples of consultants failing to write out Med Certs are forwarded to RH
All Ongoing
26. Acute Trust – Group to email any queries and issues they have for JL to DK, who will forward to JL to take back.
All Ongoing
1 | P a g e
MINUTES
Meeting: Stevenage ICPB and Locality Meeting
Date: Tuesday 14th November 2017 - 12.30 to 2.30pm
Venue: Cromwell Hotel, High Street, Old Town, Stevenage, SG1 3AZ.
Attendee do these Organisation Present
1. Dr Russell Hall (RH) Chair GP Chells Way Surgery Y
2. Dr Prag Moodley (PM) GP Stanmore Medical Group Y
3. Michelle Myers (MM) Chells Way Surgery Apologies
4. Susan Lincoln (SL) PM Stanmore Medical Group Y
5. Mark Banks (MB) PM King George Surgery Y
6. Dr Rini Saha (RS) GP King George Surgery Y
7. Fiona Lucas (FL) PM Symonds Green Y
8. Dr Masood GP Symonds Green Y
9. Elaine Cook (EC) PM Bedwell Medical Centre Y
10. Allison Seymour (ALS) PM Bedwell Medical Centre Y
11. Sandra Copping (SC) PM Manor House Y
12. Karen Smith (KS) Nurse Manor House Y
13. Manjit Phugura (MP) PM Shephall Health Centre Apologies
14. Deena Keefe (DK) Locality Manager CCG Y
15. Barbara Harrison Assoc Director For Commissioning ENH CCG Apologies
16. Michelle Morrissey Team Administrator CCG Apologies
17. Sabina Tai (ST) HomeFirst & Rapid Response Project Manager Y
18. Sharn Elton (SE) Director Operations and Resilience CCG Y
19. Maxine Davis(MD) Senior Pharmaceutical Advisor ENHCCG Y
20. Della McMurdo (DMM) HPFT Service Mgr community Mental Health Apologies
21. Julie Hoare (JH) HCT Director of Service Development and Partnerships
Apologies
22. Yasha Rai (YR) HCT Community Locality Manager Y
23. Jacqui Carrett (JC) Service Manager ICRS Y
24. Michael Henderson HPFT Services Lead Y
25. Sean Dale-Molloy HomeFirst/ Rapid Response Apologies
26. Daniel Marshall Chief Exec – citizens advice Stevenage Apologies
27. Sunday Adeniyi (SA) ENH CCG Apologies
28. Mary Bishop (MPB) PM Stanmore Medical Group Y
29. Dr P Raveendran (PR) GP Bedwell Medical Centre Y
30. Dr A Cormack GP Shephall Way Surgery Y
31. Dr M Duggan GP Manor House Apologies
32. Dr O Lawson GPSTR Manor House Y
33. Ruksana Parkar Locality Manager Y
34. Claire Checkley Primary Care Customers Relations Coordinator Y
35. Ken Moore (KM) PPG Representative Y
36. Dr Rajeev Kaja (RK) GP Stanmore Medical Group Y
37. Heather Wong Shephall Health Centre – GPST2 Y
2 | P a g e
38. Marian Malak Shephall Health Centre – GPST2 Y
39. Matthew Charles Age UK Y
40. Teresa Sutherill (TS) Chells Way Surgery Y
41. Samantha Law GP Chells Way Surgery Y
42. Chin Okunga (CO) ENHT Y
1.
Apologies and Introductions – Apologies – were noted Declarations of Interest – The Chair invited the Practice Representatives to reconfirm their current declarations on the Register of Interests were accurate and up to date. All members confirmed their interests were accurate and up to date.
2. Integrated Provider Board – ST confirmed her role is changing and would be stepping down. Her role will be covered by MH. Minutes and Action Log for Provider meeting (10.10.17) was discussed. See attached notes and action log.
Items discussed: o EOL Update o UTI Update o COPD update o Winter Locality Plans
3. Action notes from previous meeting (10th October 17) see updated action log below All attendees agreed the minutes of 10th October 2017 as an accurate representation.
4. Prescribing Update – MD updated the group on the following:
Prescribing finance data - this was late due to the cross charging between GPs moving to N Herts. Cross charging is no longer happening but due to the delay in financial data it is still being adjusted for. The locality are forecast an over spend of £129K which is significantly better than initially calculated , it also differs from the data in the locality finance pack. MD to speak to Sunday to ensure he is aware of the newest data and the adjustments that are being made.
KPIs - there is slow movement in the KPI position across the practices , Stevenage is the only locality not achieving the QP / KPI for Nitrofurantoin as a percentage of Nitrofurantoin and Trimethoprim. MD asked GPs to remind all prescribers of the updated guidance.
In addition there is another antibiotic related QIPP A 10% reduction (or greater) in

3 | P a g e
the number of Trimethoprim items prescribed to patients aged 70 years or greater on baseline data (June15-May16) for 2017/18. Until recently we have not been able to measure this target locally but now we have access to epact2 which has demographic data in we can. Unfortunately the CCG are not achieving this target but are moving towards this as trimethoprim prescribing is reducing overall. Audits and epact data have shown that 50% of the trimethoprim prescribing is this age group is for prophylaxis. Guidance on prescribing for recurrent UTIs will be circulated shortly.
https://www.england.nhs.uk/wp-content/uploads/2016/09/annx-b-quality-premium-14-07-17.pdf
Action: Guidance on prescribing for recurrent UTIs will be circulated shortly MD
5. Discharge Home to Assess – DH2A Please see attached presentation shared by RW. RW went to discuss the following:
4 month pilot upto the 31st March2018
There is a national requirement to do this pilot
Budget only enough to support the pilot for this length of time coming from the Better Care Fund.
RW confirmed patients that come out of hospital will be given 2 weeks prescription.
Concerns were raised that this will have an impact on prescribing budgets and primary care.
SE added that this is a short pilot, which will be monitored for consequences. Also the costs will be reattributed from other areas where cost savings can be made in the system.
Team will be working closely with the community team.
Only 3 wards are being focused on for now
6. Finance and Locality Information Pack (LIP) update (see pack) Finance lead sent there apologies. To feedback at next month’s meeting.
7. HCT Rapid Response update
Still to recruit case management nurse
District nurse – 1.5 vacancy
3 banking staff consistently which is back filled by agency
8. Mental Health Update
PM confirmed there is a pilot where patients will be referred to secondary care.
At the moment they are being referred to SPoA with long waiting times and up to 5 hours assessments per patient per referral.
A lot of time is wasted hence targets are not being met and patients not seen quicker.
Solution – is to have a community based clinic in Stevenage.
Patients will be triaged and processed. No referral notes.

4 | P a g e
To be seen within 7 days maximum.
Only cost would be to rent an accommodation
Suicidal cases referred directly to SpoA.
PM added that system 1 access is required from all practices. Practices agreed and felt this was a good idea.
Clinics to take place on Wednesdays
Appointment system required
Premises – Canterbury surgery
Action: PM to send letter of when pilot will start so referrals can start coming in.
9. £1P
£1PP – Care Ward Rounds (Weds)
Phlebotomy Service: DK confirmed this is on standstill. Contracts team and acute services are still in discussion. RH added we may need to use the remaining £1pp to do something as a locality.
It was agreed that Stanmore will look to employ a phlebotomist and share it across the locality, Shephall first.
MB and SL to put a plan together and cost it. They will feedback at the next locality meeting.
Action: Phlebotomy – Employ and share phlebotomist - MB and SL to put a plan together and cost it. To be discussed at PMs meeting and agreed next locality meeting.
10. Lister – Primary Care Customer Relations - Liaison
CC/CO said they are happy for the locality to contact them with any queries or issues they may have with the Lister. The correct route would be to report the issues to the contract hotline who will escalate to the trust and log the issues.
11. LTC Update
Last 2 meetings were cancelled so nothing to report
More information coming from my care plan.
12. 10 Patient Participation Group Update
Letter regarding flu vaccines to be prepared and sent to the local newspaper via PPG.
Special meeting taking place in Manor House – Dementia – 30th November
17th January – Alliance meeting
13. 10.
AOB
Target: RH recommended that sign in for target is done at tea and coffee break to increase attendance
Delegated Commissioning:

5 | P a g e
7th December 2017: Council of Members debate and vote 8th December 2017: Formal notification to NHS England. RH advised that this should be discussed at the target event on 30th November
NDPP: EC confirmed some feedback from their patient from the NDPP programme. The course does not educate on prevention. 22 people started only 5 people left on the course. RH confirmed we need to feed this back to the programme.
Flu Plan: STV Plan not accepted by CCG, however it has been agreed £4,800 is available amongst the practices if the locality meets their targets. More work needs to be done for over 65 LTC group. If individual practices meet their target then they will get their portion of their funds if the locality does not meet its target.
MB added the following:
Resubmitted our plan relating to obtaining funding from the transformation fund (£1.50 per patient). This has been received by the CCG and will reviewed at the next meeting with Denise Boardman and James Gleed - Wednesday 22 November 2017.
Spoken to HCT and the Stevenage Hub regarding to using their facilities for the service. Both have been extremely positive during the discussions.
The Project team are receiving updates from Webinars arranged by NHS England on the
subject of Extended Access. Questions for a patient’s survey have been sent to the Practice Managers for feedback -
Positive responses received so far. The survey will hopefully be published in December or January. This will hopefully be done via the CCG - Mark Edwards.
Dates of Next Meeting:
30th Nov 2017Target Event @ Stevenage Football Club
7th Dec 2017Council of Members @ Fielder Centre, Hatfield.
12th Dec 2018 @ Stevenage Football Club (note Change of venue for this meeting only)
8th Feb 2018 Target Event @ Stevenage Football Club
8th March Council of Members @ Robertson House, Six Hills Way, Stevenage.
ACTIONS Person
Responsible
DATE
1) 1
1
1
1. Shephall – phlebotomy service - need a
phlebotomist to work from the surgery for their
patients.
Issue ongoing since Jan 2017. HED was dealing with
the matter with the Contracts team at the CCG and
TPP team.
Need to escalate to Harper Brown to resolve, as
DK 12.09.17 – Ongoing - £1pp money agreed to be used to ask TPP whether they can provide staffing MP to liaise with Commissioning Team and DK to resolve

6 | P a g e
Patients have a petition and are escalating.
09.05.17 – HB to contact practice directly to discuss 11.07.17 – Ongoing, DK to discuss with HB and keep RH in the loop 12.09.17 – locality agreed to use £1pp 17/18 to
purchase additional clinics for Shephall.
10.10.17 – now with contracts team to organise, and
liaise with the Trust
14.11.17 – Stanmore to employ phlebotomist and
share with locality from £1pp – to be approved
Ongoing
5.Diabetes service - issues raised by Karen Smith and locality, SE to liaise with the service 11.04.17 – KS has a meeting 12.04.17with the service to discuss Update 09.05.17 - KS spoke to HCT awaiting to meet up with them. 11.07.17 – KS reported that templates not being completed by consultants which affects 8 Care Processes and national guidance – feedback to diabetes group, practices to collect examples and issues and let DK know. 10.10.17 – JL will take this back and liaise with the team.
SE / JL/ KS Ongoing
12.09.17 – No
update, waiting to
hear from secondary
care
Practices to send
queries to the
hotline
19. Documents dropping into patient record - SystmOne practices finding documents, requests and notes dropped into records with no tasking, and embedded letters. Comment made that this is worrying and could be missed by practices. JH to discuss with HCT & AIVHS, BF to address with HUC & CCG colleagues Example from Stanmore to be forwarded to JH 12.09.17 – emails sent after 11.07.17 meeting by BF If we do not get any examples sent to Julie by the 24th October 2017, we propose to close the action. [email protected]
JH/BF Closed
23. ICPB Agenda - JH to look into just in case medication and prescribing changes as an area which could be changed to save time for GPs. 10.10.17 – all to email JH ideas.
JH Closed
25. Outpatient Certification - Still seems to be an ongoing problem despite going through the contracts hotline. Please copy in the GP liaison at ENHT any
All Ongoing

7 | P a g e
queries regarding outpatient certification of patients to: Claire Checkley [email protected] Please send any examples. Med Certs - All to ensure that any examples of consultants failing to write out Med Certs are forwarded to RH
26. Acute Trust – Group to email any queries and issues they have for JL to DK, who will forward to JL to take back.
All Closed - no emails recorded
27. Guidance on prescribing for recurrent UTIs will be circulated shortly MD
Ongoing
28. PM to send letter of when mental health pilot will start so referrals can start coming in
Ongoing
29. Phlebotomy – Employ and share phlebotomist - MB and SL to put a plan together and cost it. To be discussed at PMs meeting and agreed next locality meeting.
Ongoing
1
MINUTES
Meeting: Upper Lea Valley Locality Commissioning Meeting
Date: 11 October 2017 at 1 pm
Venue: Priory Hall, Ware Priory, SG12 9AL
PRACTICE/ORGANISATION ROLE ATTENDEES Amwell Street GP Dr Jo Roberts
Buntingford & Puckeridge GP Dr Will Nicholson
Castlegate GP Dr Phil Lancaster
Church Street GP Co- Chair Dr Nicky Williams
Church Street Locality Lead Nurse Lucy Eldon
Dolphin House GP Dr Martyn Davies
Hailey View GP Dr Anna Clark
Hanscombe House GP Dr Hemantha Abeywickrema
& Dr R Shah
The Limes GP Co-Chair Dr Mark Andrews
Amwell Street Practice Manager Julie Tripp
Buntingford & Puckeridge Practice Manager Teresa Davidson
Dolphin House Practice Manager Jill O’Brien
Hailey View Practice Manager Val McCann
Park Lane Practice Manager Dee Gudgeon
Wallace House Practice Manager Rachael Hunt
PCG Chair Charles Ledsam
GHC Federation Manager David Eyre
Director of Commissioning CCG Harper Brown
CCG Finance Manager Alison Saward
Locality Manager CCG Pam Jardine
Administrator CCG Helen Hemmingfield
Welcome & Apologies MA welcomed everyone to the meeting. Apologies were received from Drs Jay Kuruvatti, Jacqui Sheridan and Anna Makepeace, who were attending the NESTA launch and from Dr Dilesh Shah, Karen Cassell and Barbara Harrison.
Declarations of Interest The Chair invited the Practice Representatives to reconfirm that their current declarations on the
Register of Interests (which were sent out with the meeting papers) were accurate and up-to-date. Members present confirmed that their interests were accurate. GHC Federation was reminded that the CCG was still awaiting Declaration of Interest forms for
Federation Directors. No conflicts of interests to agenda items were reported.

2
Action: Declaration of interest forms to be submitted to Governance by Generating Health Care
Federation to include the newly registered Clinical Directors. The Limes to submit changes to the Declaration of Interest Register.
Minutes of Previous Meeting The minutes of the previous meeting were agreed as accurate.
CFF Q2 Submissions An update was sent out on the CFF on the 10th October by BH, AD for Commissioning & Localities.
The CCG have given practices an extension to the 10th November for submission of Q2 outputs. Practices reported that there is still a lack of clarity and uncertainty especially around Long Term
Conditions. It was suggested that this item should come back to next month’s meeting when everyone has read and understood it.
Cancer MA asked Board Members if they had reviewed the ENHT 2ww Audit disseminated by the Cancer
Steering Group and circulated with papers. He stated that Cancer performance is not good across the CCG.
MA informed practices that forms are not being completed correctly with some practices still using the old forms.
Some practices also send letters with no forms. MA asked that if practices are going to send letters, then letters need to have a good amount of
detail, including basic information such as a contact number. MA informed practices of the MDDC Service (Multi Disciplinary Diagnostics Centre) at ENHT. He
requested that details of the MDDC be sent out to all practices including the referral forms and templates. He also requested that this is put onto Ardens.
MA reminded practices of the support offered by Jay Smith of Cancer UK as outlined at Target. Jay Smith has offered help to Practices with their Cancer plans and is available to provide training.
Jay will also analyse cancer data by practice in time for the February’s Target which has been scheduled purely as a cancer training event.
Action: PJ to liaise with Gillian Catchpole, Cancer Programme Manager to circulate details of MDDC service to practices, including referral forms and templates.
Extended Access Teresa Davidson and Rachael Hunt prepared a document for practices to consider the possible options for extended access. This was circulated to the Locality Board with locality papers. Locality staff were also surveyed on their availability. Options proposed were:
(1) Do nothing – CCG to Commission (2) Hub Working: evenings and weekends - Individual practices to cover similar to extended hours
DES for all Hub practices. (3) Option 3: Single Locality hub with Federation or other provider within the locality providing cover
for weekends and evenings
service to current extended hours commitments for all Practices were asked decide which option they would prefer. A lengthy discussion followed and practices were asked to vote on this.
Decision: The majority of practices voted to provide extended access and to task the working group to come up with how this will be delivered.
3
The next steps will be for a survey to be sent out to all patients by practices to determine the level of demand.
GPFV £1.50 allocations NW presented a summary of the various proposals submitted for GPFV funding for the locality for 2017/18. All 6 proposals have been approved. Details of the proposals were circulated with Locality Board papers and practices were asked to contact NW if they required any additional information. A further proposal on Year 2 funding (2018/19) is to be submitted at a later date. PJ to go through the GPFV proposals with Practice Managers and the PM’s meeting which was scheduled for the following week. Silicon Footfall - GPFV A proposal was submitted by the Federation as part of the GPFV submissions to implement Silicon Footfall across the locality. DE reported that most practices have signed up to Silicon Footfall. Contracts have been signed and all looks very good. DE explained it is like an interactive website and said that 3 practices may be late adopters. DE to provide more information at the next Practice Managers meeting. Funding for Clinical Training - GPFV LE provided an update on funding available for various clinical training and stated that some courses will be funded via £2.10 fund whilst training for new types of clinical staff will be funded via £1.50 funds. She asked practices to refer clinical staff that required training to her. LE reminded practices that this window of opportunity is only open until March 2018 as some of the funds had already been carried over from last year and cannot be carried over to the next financial year. LE informed practices that a training catalogue was circulated to all practices in the CCG and that training for nurses was funded and was free to nurses. Rachel Hunt thanked LE for all the training that members of the practice had received. NW informed the Board that training on Active Signposting is currently being worked up for front line staff in practices. She informed practices that the CCG is currently reviewing a number of recommended training providers to deliver the Active Signposting project and that the CCG will write to practices shortly so that they can make the decision. Localities are to collectively nominate their preferred provider as only 1 training provider will be commissioned to provide the training across the CCG.
Provider Board Update
GP into Rapid Response NW informed the Board that Laura Smith has started in her role as the new GP into Rapid
Response Team and was currently on her induction period with the team. NW mentioned that Laura has some good ideas on how to move forward with Rapid Response and will be attending the Locality Board when she has settled in to provide an update to the Board.
NESTA NW informed the Board of the launch of NESTA 100 day challenge which was happening on 11
and 12 October. NW stated that NESTA is an international charitable organisation and has been commissioned by NHS England and was completely free for the locality. NESTA looks to empowering people with small ideas and turn them into improved ways of working, removing blockages, and were currently working with the locality’s integrated teams.
Two area of work were chosen. In Hertford, work is being done with patients over the age of 65 with mental health problems and testing different ways of looking after them.
In Hoddesdon, the team are working on frail and elderly patients who are housebound.

4
Care homes It was reported that Anna Makepeace has been looking into how services can be delivered into
care homes in a slightly different way. Money has been identified from the Council that may be able to help. A couple of care homes in Ware are likely to be chosen.
Vanguard have sent information to all the care homes regarding the procedure that needs to be followed if they are any concerns about a resident. Vanguard are happy to have discussions with GPs with responsibility for residents in care homes.
A discussion was then held about Rapid Response and how stretched they were. It was suggested that if practices had any problems or issues that they email Anna Makepeace or the locality leads.
PCG Update
CL informed the locality that the PCG were scheduled to be at Sainsbury’s on 7 October as part of COPD/Respiratory awareness campaigns. However there was a mix up with the bookings with the result that they were unable to attend.
He informed the locality that this has now been deferred to 13 January 2018.
Governing Body Update MA informed the Board that discussions have been held around QIPP savings. He reported that there has been voting on IVF and the numbers of cycles to be offered. There was also voting on gluten free products and on prescribed over the counter medicines. MA reported that the decisions will be going to public voting at JCC before sign off. West Herts CCG has also been going through the same process and once agreed across the two CCG’s, these decisions will come into effect. Pay Review As part of QIPP, NHS England has informed the CCG they need to implement a prospective pay review of out patient referrals. An audit has been carried out on practices and discussions have been held in the workshop. NHS England has asked practices to review two of the higher activities, which were ENT and gynaecology. Out patient referrals The board were informed that the locality was one of the localities for high outpatient referrals. The new MSK triage service is coming on line and the CCG have been asked to do some training on this. At some point in the next 6 months Orthopaedics will go to a triage service. The model is being currently developed. NW brought to the Board’s attention a couple of topics from the bulletin. These were: stop smoking prescribing has changed completely for nurses and record sharing for children around safeguarding issues. LE reminded practices of the Prescribing Update Forum on smoking which has been scheduled for 21st November 2017. Sponsorship Declarations Rules from NHS England on Conflicts of Interests have changed. This includes declarations for hospitality and sponsorship. Detailed guidance is to be provided from Sarah Feal, CCG Head of Governance on the changes and how these changes impact on the locality and on practices and also what practices need to do to comply with regulations. Action: PJ to get further clarification on sponsorship from Governance.

5
Delegation NW informed the Board that at the Council of Members meeting is to be held on 7th December. Practices will need to vote on whether the CCG should continue as Joint Commissioning with NHSE or to go to Delegated status. NW reminded practices that if their clinical representative is not able to attend on 7 Dec then they should inform the CCG beforehand so that the CCG would have their vote. NW requested that Delegation is put on November’s locality agenda so that the locality can come up with a view point. Action: PJ to put Delegation on November’s Locality Agenda.
GHC Federation
Summer Pressures invoice has been sent to Wakefield and Federation are awaiting payment. Monies will go out to the Practices as soon as the payment has been received.
The Winter Pressures details were sent out week commencing 9th October and should have been received.
GHC reported that they have tendered for The Limes which was currently in procurement. The tender will be submitted by the closing date of 13th October.
GHC also reported that they have signed a deal with a Locum agency and that this has been sent to all practices.
The Federation has put in a bid with NHS England for 5 pharmacists.

6
ACTION LOG
Actions from October 2017 meeting Person
Responsible Date Progress
Park Lane PM to email Locality Manager with further information on issue with call so that it can be brought to HUC’s attention.
Dee Gudgeon/ Pam Jardine
asap HUC were contacted and confirmed that HUC cover was provided to all practices in ULV. They reported that this was an isolated incident for which they apologised and agreed to speak to the call handler. Action closed.
Declaration of interest forms to be submitted to Governance by Generating Health Care Federation to include the newly registered Clinical Directors.
GHC asap Still awaiting Declaration of Interest forms from to be completed with appointment of new directors of GHC Federation with names of practices for which they have responsibility.
The Limes to submit changes to the Declaration of Interest Register
Limes Surgery asap Submitted to Governance by practice. GPs to remain on Register for 6 months after notification. Action closed.
Action: PJ to request that Gillian Catchpole circulate details of MDDC service to practices, including referral forms and templates
PJ=> GC asap MDDC forms circulated by PJ on 23.10.17. Also featured in Bulletin dated 7 Nov 17 Action closed
Sponsorship Declarations: PJ to request further clarification on the changes on sponsorship and hospitality from the Governance
Pam Jardine asap Governing Body to circulate to practices in due course.
Delegation to be put on November’s Agenda.
PJ Nov On Agenda Action closed
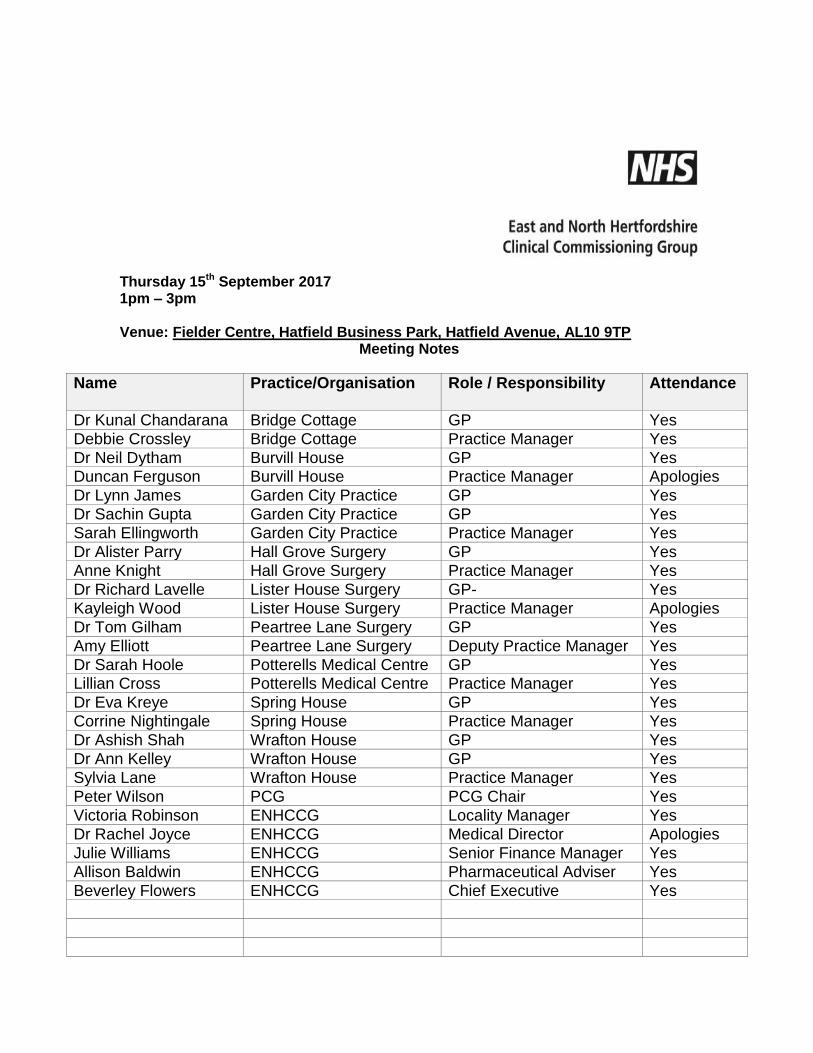
Thursday 15th September 2017 1pm – 3pm Venue: Fielder Centre, Hatfield Business Park, Hatfield Avenue, AL10 9TP
Meeting Notes
Name
Practice/Organisation Role / Responsibility Attendance
Dr Kunal Chandarana Bridge Cottage GP Yes
Debbie Crossley Bridge Cottage Practice Manager Yes
Dr Neil Dytham Burvill House GP Yes Duncan Ferguson Burvill House Practice Manager Apologies
Dr Lynn James Garden City Practice GP Yes
Dr Sachin Gupta Garden City Practice GP Yes
Sarah Ellingworth Garden City Practice Practice Manager Yes
Dr Alister Parry Hall Grove Surgery GP Yes
Anne Knight Hall Grove Surgery Practice Manager Yes
Dr Richard Lavelle Lister House Surgery GP- Yes
Kayleigh Wood Lister House Surgery Practice Manager Apologies
Dr Tom Gilham Peartree Lane Surgery GP Yes
Amy Elliott Peartree Lane Surgery Deputy Practice Manager Yes
Dr Sarah Hoole Potterells Medical Centre GP Yes Lillian Cross Potterells Medical Centre Practice Manager Yes
Dr Eva Kreye Spring House GP Yes
Corrine Nightingale Spring House Practice Manager Yes
Dr Ashish Shah Wrafton House GP Yes
Dr Ann Kelley Wrafton House GP Yes
Sylvia Lane Wrafton House Practice Manager Yes
Peter Wilson PCG PCG Chair Yes
Victoria Robinson ENHCCG Locality Manager Yes
Dr Rachel Joyce ENHCCG Medical Director Apologies
Julie Williams ENHCCG Senior Finance Manager Yes
Allison Baldwin ENHCCG Pharmaceutical Adviser Yes
Beverley Flowers ENHCCG Chief Executive Yes
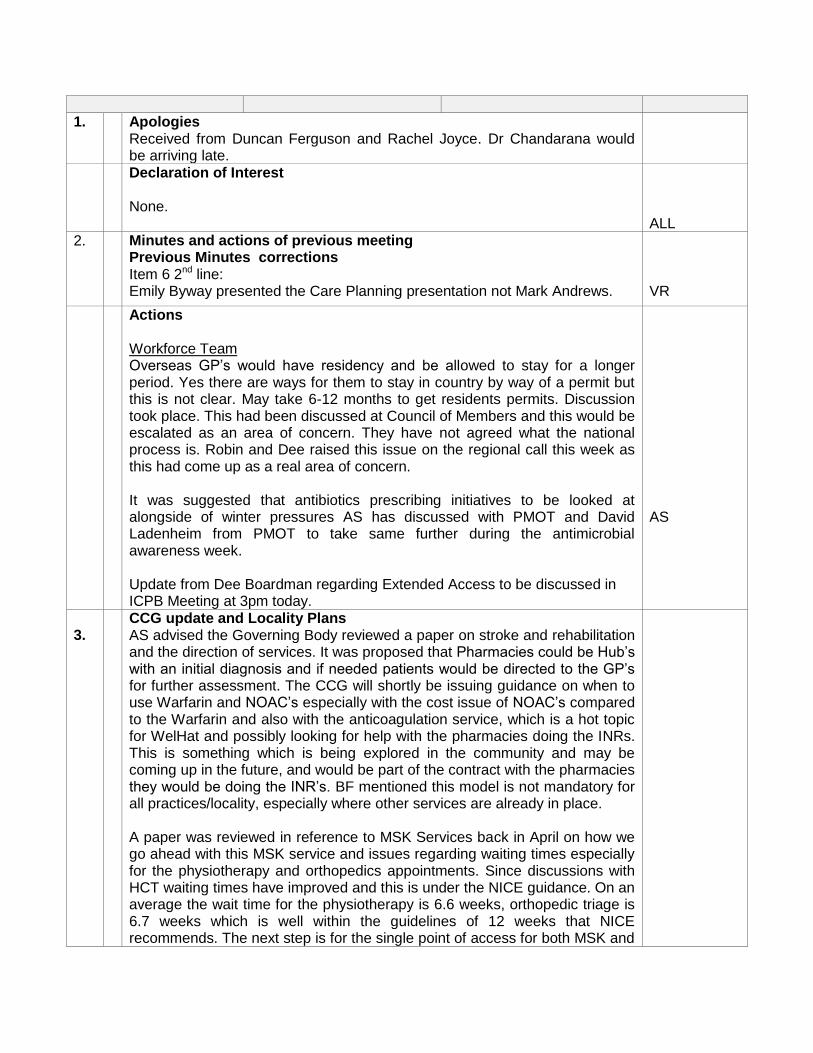
1.
Apologies Received from Duncan Ferguson and Rachel Joyce. Dr Chandarana would be arriving late.
Declaration of Interest None.
ALL
2. Minutes and actions of previous meeting Previous Minutes corrections Item 6 2nd line: Emily Byway presented the Care Planning presentation not Mark Andrews.
VR
Actions Workforce Team Overseas GP’s would have residency and be allowed to stay for a longer period. Yes there are ways for them to stay in country by way of a permit but this is not clear. May take 6-12 months to get residents permits. Discussion took place. This had been discussed at Council of Members and this would be escalated as an area of concern. They have not agreed what the national process is. Robin and Dee raised this issue on the regional call this week as this had come up as a real area of concern. It was suggested that antibiotics prescribing initiatives to be looked at alongside of winter pressures AS has discussed with PMOT and David Ladenheim from PMOT to take same further during the antimicrobial awareness week. Update from Dee Boardman regarding Extended Access to be discussed in ICPB Meeting at 3pm today.
AS
3.
CCG update and Locality Plans AS advised the Governing Body reviewed a paper on stroke and rehabilitation and the direction of services. It was proposed that Pharmacies could be Hub’s with an initial diagnosis and if needed patients would be directed to the GP’s for further assessment. The CCG will shortly be issuing guidance on when to use Warfarin and NOAC’s especially with the cost issue of NOAC’s compared to the Warfarin and also with the anticoagulation service, which is a hot topic for WelHat and possibly looking for help with the pharmacies doing the INRs. This is something which is being explored in the community and may be coming up in the future, and would be part of the contract with the pharmacies they would be doing the INR’s. BF mentioned this model is not mandatory for all practices/locality, especially where other services are already in place. A paper was reviewed in reference to MSK Services back in April on how we go ahead with this MSK service and issues regarding waiting times especially for the physiotherapy and orthopedics appointments. Since discussions with HCT waiting times have improved and this is under the NICE guidance. On an average the wait time for the physiotherapy is 6.6 weeks, orthopedic triage is 6.7 weeks which is well within the guidelines of 12 weeks that NICE recommends. The next step is for the single point of access for both MSK and
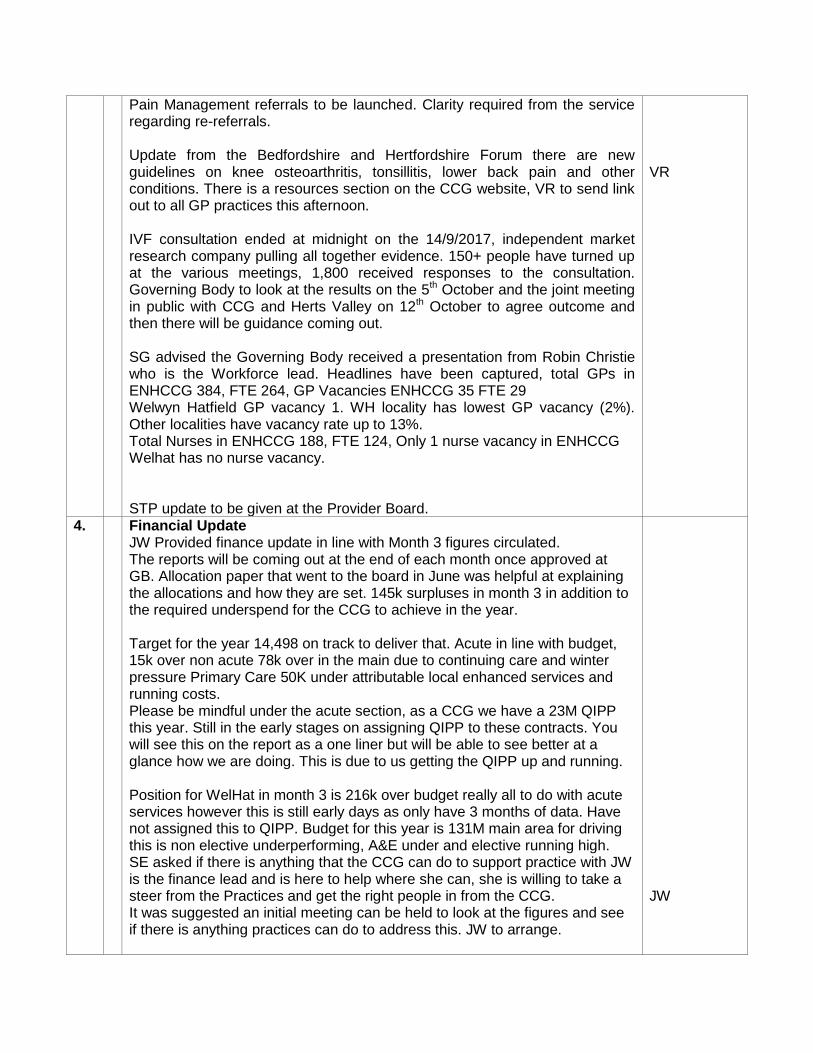
Pain Management referrals to be launched. Clarity required from the service regarding re-referrals. Update from the Bedfordshire and Hertfordshire Forum there are new guidelines on knee osteoarthritis, tonsillitis, lower back pain and other conditions. There is a resources section on the CCG website, VR to send link out to all GP practices this afternoon. IVF consultation ended at midnight on the 14/9/2017, independent market research company pulling all together evidence. 150+ people have turned up at the various meetings, 1,800 received responses to the consultation. Governing Body to look at the results on the 5th October and the joint meeting in public with CCG and Herts Valley on 12th October to agree outcome and then there will be guidance coming out. SG advised the Governing Body received a presentation from Robin Christie who is the Workforce lead. Headlines have been captured, total GPs in ENHCCG 384, FTE 264, GP Vacancies ENHCCG 35 FTE 29 Welwyn Hatfield GP vacancy 1. WH locality has lowest GP vacancy (2%). Other localities have vacancy rate up to 13%. Total Nurses in ENHCCG 188, FTE 124, Only 1 nurse vacancy in ENHCCG Welhat has no nurse vacancy. STP update to be given at the Provider Board.
VR
4. Financial Update JW Provided finance update in line with Month 3 figures circulated. The reports will be coming out at the end of each month once approved at GB. Allocation paper that went to the board in June was helpful at explaining the allocations and how they are set. 145k surpluses in month 3 in addition to the required underspend for the CCG to achieve in the year. Target for the year 14,498 on track to deliver that. Acute in line with budget, 15k over non acute 78k over in the main due to continuing care and winter pressure Primary Care 50K under attributable local enhanced services and running costs. Please be mindful under the acute section, as a CCG we have a 23M QIPP this year. Still in the early stages on assigning QIPP to these contracts. You will see this on the report as a one liner but will be able to see better at a glance how we are doing. This is due to us getting the QIPP up and running. Position for WelHat in month 3 is 216k over budget really all to do with acute services however this is still early days as only have 3 months of data. Have not assigned this to QIPP. Budget for this year is 131M main area for driving this is non elective underperforming, A&E under and elective running high. SE asked if there is anything that the CCG can do to support practice with JW is the finance lead and is here to help where she can, she is willing to take a steer from the Practices and get the right people in from the CCG. It was suggested an initial meeting can be held to look at the figures and see if there is anything practices can do to address this. JW to arrange.
JW

SE pointed out that Stevenage Locality had recruited a data analyst. Is this something Welhat can look into? Might be good to speak to the Locality and whether this is useful and what is coming out of the data. VR to ask Deena Keefe, if lessons learnt and findings could be shared. BF advised as part of the elective activities against other providers across Beds and Herts – 3 CCG’s we are roughly on track with variation under on some elements, and noted that Herts Valley CCG at the beginning of the year were in a deficit they currently have a recovery plan in place to save around 48M. From the acute providers point of view PAH is where is should be West Herts Trust is finding it difficult to deliver its control total. For East and North Herts trust delivering its financial position that because they have done a number of things internally to reduce their costs base, they are increasingly concerned they are behind on elective activity and seeing waiting lists go up. Clarity requested if £2.10 if those monies are unspent will it go into the base line? BF advised this needs to be spent on agreed projects, or a plan will need to be agreed for this to be realigned, within guidelines. BF reiterated the confirmed winter pressures funding available and how this measured up against the amount of GP hours used last year.
5. LTC Update - Dr Sarah Hoole Update received on social prescribing. SH advised, Emily Byway talked about care planning and using the Ardens template at last LTC meeting and advised there is a lot of development work going on. This is a generic template care plan on the Ardens. SH reminded practices there is a 2 year contract for those who have Ardens. Prescribing update – Allison Baldwin AB advised, Looking at finances, it is too early to have an idea the overall performance but the latest figures for month 3 for WelHat shows 1.76% over budget, Compared to a CCG overspend of 0.52% In relation to prescribing element of the CFF, copies of the latest metrics for the Practices handed out to see how practices are performing. 21 out of 45 indicators are in green and practices range from 1-3 of the 5 indicators that are green. AB reminded practices that each indicator achieved is associated with practice payment. Mental health update - From Dr Preenal Shah No update next MH meeting 20th September, so a written report will be circulated after then. Workforce planning and education update – Dr Ashish Shah A paper went to the board of information submitted by practices, AS asked if practices were happy with sharing the Welhat data on what has been said in the paper at the locality. It was agreed that they would be happy to share this at Locality level.
6. PPG update – Peter Wilson Last patient commissioning meeting was on the 2nd August, spent time on the patient consultation and extended access, focusing on the understanding and what they were about so that members could take back to their PPGs. PW advised about the work they have been doing on patients understanding of cancer based on Mark Andrews presentation to a patient group, patients

are not aware/don’t recognise the early symptoms of cancer resulting in a later diagnosis. That group has pulled resources from the NHS and local charities are going to produce some slides for Breast Cancer month which is next month and we hope and anticipate and hope that the CCG will distribute these. Current Information on practice display screens reviewed and agreed which are relevant to WelHat. The topic of Sepsis was also discussed and this came as a shock as it was new information for the patients present, and had also been featured on Panorama this week. There is a keenness to have information prepared for patients. PW also took the opportunity to give his Congratulations to all on the CCGs status graded as outstanding.
7. Any Other Business
Flu Campaign Approval of our flu template - flu campaign for this year – talked about getting MJOG funded at a grop discounted rate for practices, and MJOG are trying to get this set this up from the 1st October. It was agreed that this will be funded from part of flu planning budget and part £2.10, as per the original locality plan. AS and VR to progress with order and set up the 2 practices without the MJOG facility. Flu plan circulated to practices, and welcomed those who would like the opportunity to step up as locality Flu lead to come back to the leads. Also, welcomed practices to forward any ideas of subjects for the next Target event in November. CFF There will be an appeals process at the end of the year that will be led by The Primary Care Steering Group, with members being an exec, some directors and a GP in the room and welcomed Governing Body members. CN advised that Spring House now has a fully functioning access to ICE and thanked VR and the leads for all their help in finally getting this resolved. VR advised that some practices would have received appeals payments notifications yesterday and clarified that the 2 payments financial balance and record sharing. Any problems please ask. Peartree Group announced since their last inspection, they were now overall Good, met with congratulations from all. SE advised practices can do ward rounds on Friday afternoon or at weekend funded from out of hours money.
AS and VR
8. Date and time of next meeting – next locality meeting Thursday 12th October.
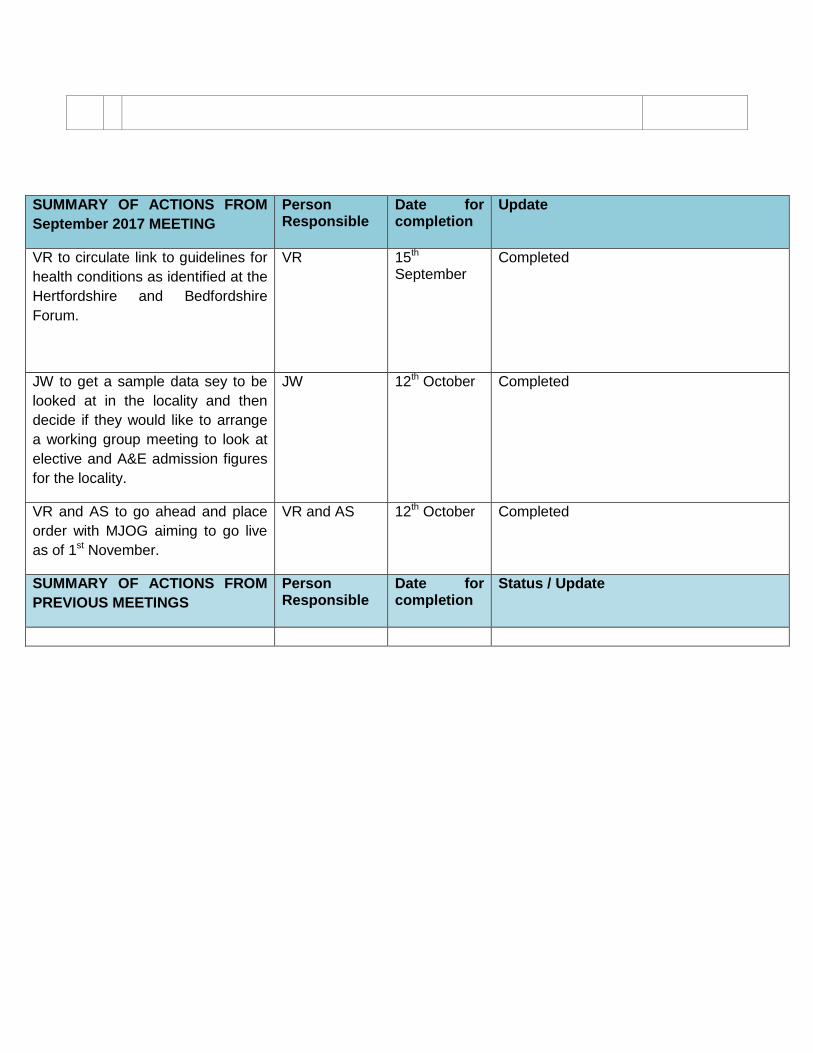
SUMMARY OF ACTIONS FROM
September 2017 MEETING
Person Responsible
Date for completion
Update
VR to circulate link to guidelines for
health conditions as identified at the
Hertfordshire and Bedfordshire
Forum.
VR 15th September
Completed
JW to get a sample data sey to be
looked at in the locality and then
decide if they would like to arrange
a working group meeting to look at
elective and A&E admission figures
for the locality.
JW 12th October Completed
VR and AS to go ahead and place
order with MJOG aiming to go live
as of 1st November.
VR and AS 12th October Completed
SUMMARY OF ACTIONS FROM
PREVIOUS MEETINGS
Person Responsible
Date for completion
Status / Update





























