Embed Size (px)
DESCRIPTION
Gout July 2010
Citation preview
Gout
Objectives
• To review the etiology and pathophysiology of gout
• To recognize predisposing factors for gout
• To review diagnostic criteria and evaluation for gout
• To know the appropriate treatment for acute and chronic gout
What is Gout?• Marked by recurrent attacks of acute inflammatory
arthritis• Disease of kings or rich man’s disease• Characterized by an abnormal metabolism of uric acid -
hyperuricemia• Overload of uric acid in the body which subsequently
deposited in the tissues of body.• Crystals of uric acid deposited in joint tissues will cause
joint inflammation (arthritis)• Repeated attacks of gouty arthritis can damage the joint
and lead to chronic arthritis.
Signs & Symptoms• Most common site for gout is the small joint at the base of
the big toe (75%). When this happens it is known as podagra.
• Also affect other joints e.g. ankles, knees, wrists, fingers & elbows
• Acute attack is characterized by a rapid onset of pain in the affected joint, followed by warmth, swelling, redness & tenderness
• 1st attack can subside spontaneously after 1 or 2 weeks
• With time, attacks can occur more frequently & may last longer – in the same joint or in another joint
• Collection of uric acid crystals outside joints form tophi which can be seen e.g. in elbows, fingers etc

URATE, HYPERURICEMIA & URATE, HYPERURICEMIA & GOUTGOUT
• Urate: end product of purine metabolismUrate: end product of purine metabolism
• Hyperuricemia: serum urate > urate solubility (> Hyperuricemia: serum urate > urate solubility (> 6.8 mg/dl)6.8 mg/dl)
• Gout: deposition of monosodium urate crystals Gout: deposition of monosodium urate crystals in tissuesin tissues
HYPERURICEMIA & GOUTHYPERURICEMIA & GOUT
• Hyperuricemia caused byHyperuricemia caused by
OverproductionOverproduction
UnderexcretionUnderexcretion
• No Gout w/o crystal depositionNo Gout w/o crystal deposition
Classification of Hyperuricemia• Uric acid overproduction
– Accounts for 10% of hyperuricemia– Defined as 800mg of uric acid excreted– Acquired disorders
• Excessive cell turnover rates such as myleoproliferative disorders, Paget’s disease, hemolytic anemias
– Genetic disorders: derangements in mechanisms that regulate purine neucleotide synthesis.
• Uric acid underexcretion– Accounts for >90% of hyperuricemia– Diminished tubular secretory rate, increased tubular reabsorption,
diminished uric acid filtration• Drugs, other systemic disease that predispose people to renal insufficiency
Pathogenesis of Gouty Inflammation
• Urate crystals stimulate the release of numerous inflammatory mediators in synovial cells and phagocytes
• The influx of neutrophils is an important event for developing acute crystal induced synovitis
• Chronic gouty inflammation associated with cytokine driven synovial proliferation, cartilage loss and bone erosion
Prevalence of Gout• 5x more common in men than in pre-menopausal
women.• In male – onset of gout usually after puberty.• In women – gout usually occurs after menopause.• After age 60 – incidence almost same as men.• If your parents have gout, you have 20% chance of
developing it.• Not all people with elevated serum uric acid will have
gout. Only 10% of people with hyperuricemia develop gout.
• People with long standing hyperuricemia can form tophi (uric acid crystals deposit) in tissue.
GOUT: A Chronic Disease of 4 GOUT: A Chronic Disease of 4 stagesstages
• Asymptomatic hyperuricemiaAsymptomatic hyperuricemia
• Acute Flares of crystallizationAcute Flares of crystallization
• Intervals between flaresIntervals between flares
• Advanced Gout & ComplicationsAdvanced Gout & Complications
ACUTE GOUTY FLARESACUTE GOUTY FLARES
• Abrupt onset of severe joint inflammation, Abrupt onset of severe joint inflammation, often nocturnal;often nocturnal;
Warmth, swelling, erythema, & pain;Warmth, swelling, erythema, & pain;
Possibly feverPossibly fever
• Untreated? Resolves in 3-10 daysUntreated? Resolves in 3-10 days
• 90% 190% 1stst attacks are monoarticular attacks are monoarticular
• 50% are podagra50% are podagra
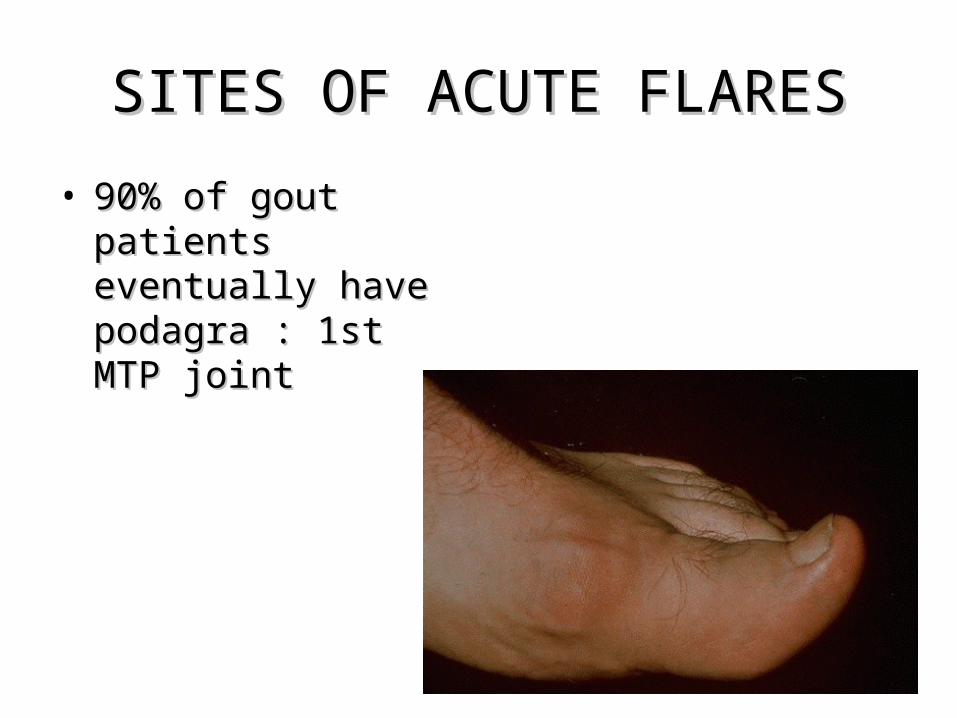
SITES OF ACUTE FLARESSITES OF ACUTE FLARES
• 90% of gout patients 90% of gout patients eventually have eventually have podagra : 1st MTP podagra : 1st MTP jointjoint
INTERVALS SANS FLARESINTERVALS SANS FLARES
• AsymptomaticAsymptomatic
• If untreated, may advanceIf untreated, may advance
• Intervals may shortenIntervals may shorten
• Crystals in asymptomatic jointsCrystals in asymptomatic joints
• Body urate stores increaseBody urate stores increase
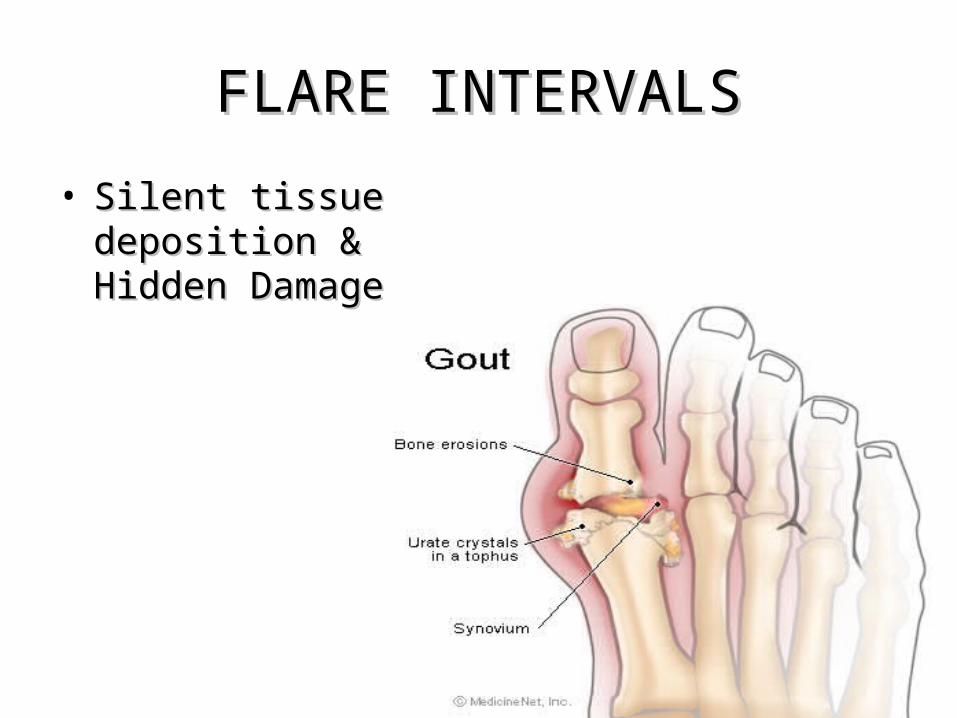
FLARE INTERVALSFLARE INTERVALS
• Silent tissue Silent tissue deposition & Hidden deposition & Hidden DamageDamage
ADVANCED/ CHRONIC GOUTADVANCED/ CHRONIC GOUT
• Chronic ArthritisChronic Arthritis
• X-ray ChangesX-ray Changes
• Tophi DevelopTophi Develop
• Acute Flares continueAcute Flares continue
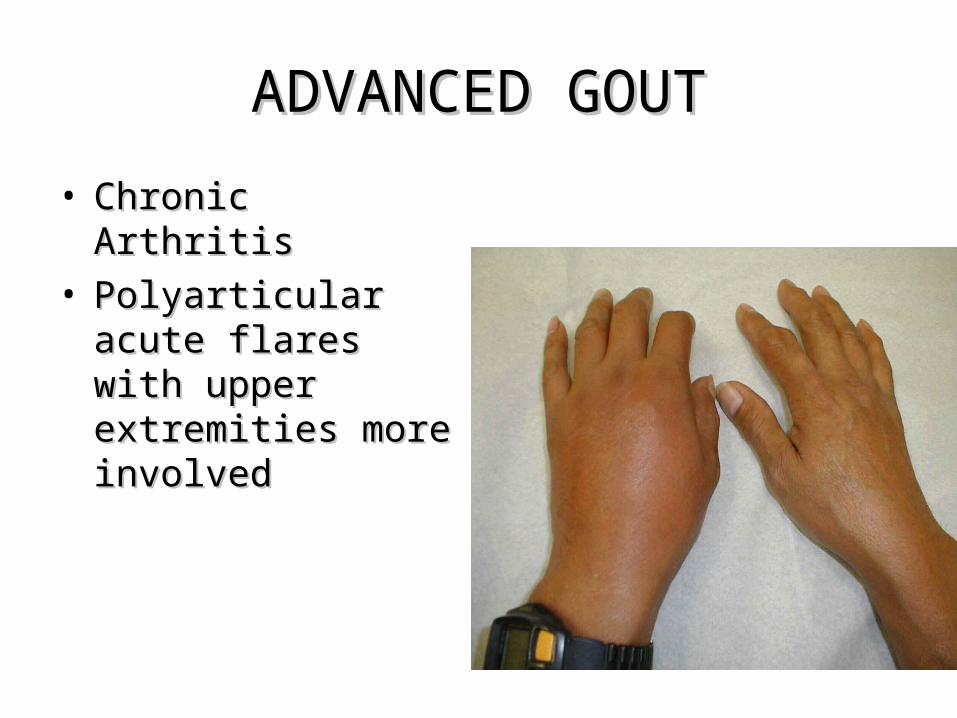
ADVANCED GOUTADVANCED GOUT
• Chronic ArthritisChronic Arthritis• Polyarticular acute Polyarticular acute
flares with upper flares with upper extremities more extremities more involvedinvolved
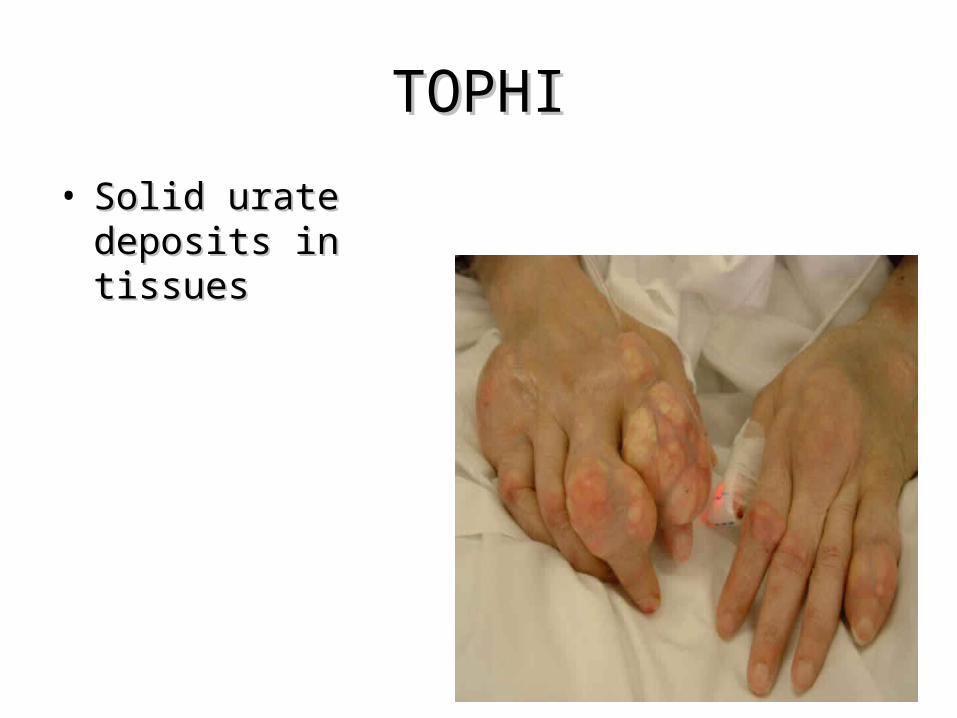
TOPHITOPHI
• Solid urate deposits in Solid urate deposits in tissuestissues
TOPHI RISK FACTORSTOPHI RISK FACTORS
• Long duration of hyperuricemiaLong duration of hyperuricemia
• Higher serum urateHigher serum urate
• Long periods of active, untreated goutLong periods of active, untreated gout
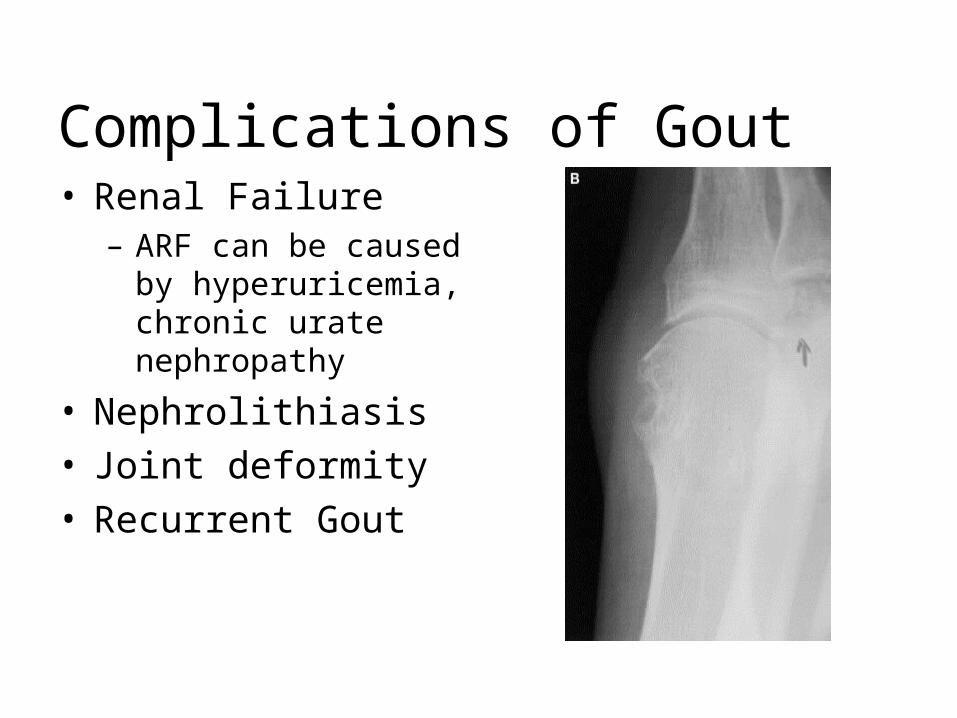
Complications of Gout
• Renal Failure– ARF can be caused by
hyperuricemia, chronic urate nephropathy
• Nephrolithiasis• Joint deformity• Recurrent Gout
GOUT RISK FACTORSGOUT RISK FACTORS
• MaleMale• Postmenopausal femalePostmenopausal female• Advancing ageAdvancing age• HypertensionHypertension• Pharmaceuticals:Pharmaceuticals:
Diuretics, Aspirin, Diuretics, Aspirin, cyclosporine, nicotinic cyclosporine, nicotinic acid, cytotoxicsacid, cytotoxics
• Hereditary – 20% chance Hereditary – 20% chance if parents haveif parents have
• hypothyroidismhypothyroidism
GOUT RISK FACTORSGOUT RISK FACTORS
• Alcohol intakeAlcohol intakeHighest with beerHighest with beerNot increased with wineNot increased with wine
• High BMI (obesity)High BMI (obesity)• Diet high in meat, seafood, internal organs, yeast, oily Diet high in meat, seafood, internal organs, yeast, oily
fishfish• Abnormal kidney functionAbnormal kidney function• Rapid turnover of cells- e.g. psoriasis & tumourRapid turnover of cells- e.g. psoriasis & tumour• Lead poisoningLead poisoning• Starvation & dehydrationStarvation & dehydration
Diagnosis
• Most reliable test is detecting uric acid in joint fluid obtained by joint aspiration(arthrocentesis)
• Bright needle- like uric acid crystals can be seen in the joint fluid under polarized microscope
• Blood test – uric acid levels, kidney function• X-rays – can show joint damage esp in patients
who have multiple episodes of gouty arthritis
Treatment Goals
• Gout can be treated without complications. • Therapeutic goals include
– terminating attacks – providing control of pain and inflammation – preventing future attacks – preventing complications such as renal
stones, tophi, and destructive arthropathy
Non- Pharmacologic Treatments
• Immobilization of Joint• Ice Packs• Abstinence of Alcohol
– Consumption can increase serum urate levels by increasing uric acid production. When used in excess it can be converted to lactic acid which inhibits uric acid excretion in the kidney
• Dietary modification– Low carbohydrates– Increase in protein and unsaturated fats– Decrease in dietary purine-meat and seafood. Dairy
and vegetables do not seem to affect uric acid
Pharmacologic Treatment For Gout
Can be divided into :
1) Acute Gout Treatment
2) Chronic Gout Treatment
Acute Gout treatment
• Agents : A) NSAIDs
B) Corticosteroids
C) Colchicine• Do not start a urate lowering agent(e.g. allopurinol)
during an acute attack• If patient on urate lowering agent, do not stop or adjust
dose
Colchicine
• Must be started in 1st 24 hour• Narrow therapeutic-toxic ratio – GI upset in 80% -
including nausea, diarrhoea,or abdominal cramps• Limited therapeutic use in acute gout• Other S/E – bone marrow suppression,renal failure,
congestive heart failure,death• Adm orally in hourly dose of 0.5mg to 0.6mg until pain &
inflammation resolved or until max dose 0f 6mg/24hr• Or 2mg IV then 0.5mg q6H until cumulative dose of 4mg
over 24 hours
Colchicine - continue
• Not effective late in flare• For healthy adults only• Should not be used by elderly patients or those with
kidney, liver or bone marrow disorders, pregnancy• Erythromycin & H2 blockers ( cimetidine, famotidine &
ranitidine) may intensify GI S/E of colchicine• Long term colchicine therapy may also weaken the
respiratory muscles, esp in renal patients
Non steroidal Anti-inflammatory Drugs
• Used in patient without contraindication – e.g. peptic ulcer, warfarin
• Need max dose/potent NSAIDs
E.g. Indomethacine 50mg tid
Diclofenac 50mg tid
Meloxicam 7.5mg daily
Celecoxib 200mg daily or bd• Continue until pain/inflammation absent for 48 hours
NSAIDs will be covered in Topic 2 – Rheumatoid arthritis
Corticosteroid
• Used when NSAIDs risky or contraindicated e.g. – elderly - renal impairment - liver impairment• Used when NSAIDs ineffective• Mode of adm – i) intra-articular with drainage (risk of sepsis) eg Triamcinolone 10-40mg or Dexamethasone 2-10mg alone or with lignocaine ii) oral prednisolone 40-60mg daily for 3-4 days. Then taper by 5mg every 2-3 days• Improvement seen in 12-24 hours
Urate Lowering Treatment(Chronic Gout Treatment)
• NEVER start a uric acid lowering agent during an acute attack
• Halt crystal formation→cure the disease• Asymptomatic hyperuricemia is not an indication for
treatment• Who to treat? (Indication)
i) tophi or chronic arthritis
ii) failure of colchicine prophylaxis
iii) radiographic changes of gout
iv) multiple joint involvement
v) nephrolithiasis (renal stones)
vi) extremely high levels of serum uric acid (>12mg/dl)
Agents That Reduces Uric Acid Synthesis
Allopurinol (Zyloric ®)
• An inhibitor of xanthine oxidase, an enzyme which converts purine (from DNA breakdown) into uric acid
• Taken orally – start low e.g. 50-100mg daily• ↑by 50-100mg every 2-3 days according to symptoms• Average dose : 300mg daily - lower dose if renal/hepatic insufficiency
- higher dose in non-responders• In divided doses if more than 300mg/day• Prophylactic colchicine until allopurinol dose stable
Allopurinol - continued
• S/E : headache, dyspepsia, diarrhea, rash, drug interactions, acute exacerbation of gout initially
• Rarely – life threatening hypersensitivity• Drug interaction with – coumadin(warfarin) - cyclosporin - azathioprine Allopurinol may prolong half-life of these
drugs & increase toxicity
Agents That Increase Uric Acid Excretion• These are called uricosurics• E.g. of uricosurics include sulfinpyrazone and probenecid• MOA : compete with uric acid for reabsorption in the proximal
tubules, preventing uric acid reabsorption and resulting in uricosuria
• Uricosurics are usually choice for preventing gout in the following patients:
- those less than 60 years old
- those with normal diets 24 hours
- those with normal kidney function
- those who have no risk o kidney stones
- those who excrete less than 700mg of uric acid over
URICOSURICS
PROBENECID ( Benemid )• ROA : oral• Dose :
- 250mg bd for 1 week then followed by 500mg bd
- best taken with food or milk to prevent GI S/E
- drink lots of fluid – prevent formation of kidney stones
- avoid large doses of vit c – ↑risk of kidney stones• S/E : LOA, drowsiness, vomiting, headache, sore gum & frequent
urination
Drug Interactions of Probenecid
• Salicylates & aspirin can ↓ effectiveness of probenecid
• Probenecid can prolong or enhance the action of sulfonylureas - ↑ hypoglycemia
• ↑ half-life of some NSAIDs• ↑ plasma concentration of methotrexate• Prolong ketamine & thiopental anaesthesia
URICOSURICS
Sulfinpyrazone ( Anturan )ROA : oral
Dose : – 100-200mg daily with food or milk
increasing 2-3 week to 600mg daily in 2 divided doses
S/E : GI upset, LOA, drowsiness, blood dyscrasias, kidney stones,
and acute exacerbation of gout initially, hypersensitivity
reactions(rash)
Should not be used for acute gout
Drug Interactions Of Sulfinpyrazone
• May ↑ effects of these drugs
warfarin→↑bleeding
tolbutamide → ↓blood sugar
• May ↓ the effects of these drugs
theophylline →worsening of asthma
verapamil → worsening of heart problem
• May ↑ hepatotoxicity of paracetamol
Gout Prophylaxis
Colchicine (at low dose)• Indication:
- until dose of urate lowering drug optimized
- If pt cannot take a urate lowering drug• Dose:
- 0.6mg qd or occasionally bid
- 0.3mg qd or q2days if renal dx or elderly
SMALLEST DAILY DOSE POSSIBLE
INDIVIDUALISE