Embed Size (px)
DESCRIPTION
http://emedicine.medscape.com/article/329958-overview
Citation preview

10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 1/10
Gout and Pseudogout Clinical PresentationAuthor: Bruce M Rothschild, MD; Chief Editor: Herbert S Diamond, MD more...
Updated: Sep 21, 2015
HistoryThe spontaneous onset of excruciating pain, edema, and inflammation in themetatarsalphalangeal joint of the great toe (podagra; see the image below) ishighly suggestive of acute crystalinduced arthritis. Podagra is the initial jointmanifestation in 50% of gout cases; eventually, it is involved in 90% of cases.Podagra is not synonymous with gout, however: it may also be observed in patientswith pseudogout, sarcoidosis, gonococcal arthritis, psoriatic arthritis, and reactivearthritis.
Gout. Acute podagra due to gout in elderly man.
Other than the great toe, the most common sites of gouty arthritis are the instep,ankle, wrist, finger joints, and knee. In early gout, only 1 or 2 joints are usuallyinvolved. Consider the diagnosis in any patient with acute monoarticular arthritis ofany peripheral joint except the glenohumeral joint of the shoulder.
The most common sites of pseudogout arthritis are large joints, such as the knee,wrist, elbow, or ankle. Case reports have documented carpal tunnel syndrome as aninitial presentation of pseudogout. Case reports of calcium pyrophosphate (CPP)crystals forming masses in the spinal ligamentum flavum have been documented.[67] These have led to both singlelevel and multilevel myelopathy.
Although crystalinduced arthritis is most commonly monoarticular, polyarticularacute flares are not rare, and many different joints may be involved simultaneouslyor in rapid succession. Multiple joints in the same limb often are involved, as wheninflammation begins in the great toe and then progresses to involve the midfoot andankle.
Gout attacks begin abruptly and typically reach maximum intensity within 812hours. Affected joints are red, hot, and exquisitely tender; even a bed sheet on theswollen joint is uncomfortable. The onset of symptoms in pseudogout can resembleacute gout or be more insidious and may occur over several days.
Untreated, the first attacks resolve spontaneously in less than 2 weeks. A history ofintermittent inflammatory arthritis, in which the joints return to normal betweenattacks, is typical of crystalline disorders and is characteristic of gouty arthritis earlyin its course.
Gout initially presents as polyarticular arthritis in 10% of patients. Elderly women,particularly women with renal insufficiency who are taking a thiazide diuretic, candevelop polyarticular arthritis as the first manifestation of gout. These attacks mayoccur in coexisting Heberden and Bouchard nodes. Such patients may also developtophi more quickly, occasionally without prior episodes of acute gouty arthritis.[68, 69,70]
The pattern of symptoms in untreated gout changes over time. The attacks canbecome more polyarticular. More proximal and upperextremity joints becomeinvolved. Attacks tend to occur more frequently and last longer.
Eventually, patients may develop chronic polyarticular arthritis, sometimes nearlysymmetrical, that can resemble rheumatoid arthritis. Indeed, chronic polyarticulararthritis that began as an intermittent arthritis should prompt consideration of acrystalline disorder in the differential diagnosis.
Acute flares of gout can result from situations that lead to increased levels of serumuric acid, such as the consumption of beer or liquor, overconsumption of foods withhigh purine content, trauma, dehydration, or the use of medications that elevatelevels of uric acid. Acute flares of gout also can result from situations that lead todecreased levels of serum uric acid, such as the use of radiocontrast dye ormedications that lower the levels of uric acid, including allopurinol and uricosurics.
Patients with gout have as much as 1000 times more uric acid in the body asunaffected individuals do and are almost twice (1.97 times) as likely to developrenal stones as healthy individuals are[71] ; therefore, they may have a history ofrenal colic and hematuria. Indeed, renal stones may precede the onset of gout in

10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 2/10
14% of affected patients. Whereas 52% of these patients may have stonescomposed entirely of uric acid, 20% may develop calcium oxalate or sometimescalcium phosphate stones.[72]
Because gout is frequently present in patients with the metabolic syndrome (eg,insulin resistance or diabetes, hypertension, hypertriglyceridemia, and low levels ofhighdensity lipoproteins) and because the presence of these associated disorderscan lead to coronary artery disease, these problems should be sought and treated inpatients diagnosed with gout.
It is important to ask about a history of peptic ulcer disease, renal disease, or otherconditions that may complicate the use of the medications used to treat gout.
Fever, chills, and malaise do not distinguish cellulitis or septic arthritis from crystalinduced arthritis, because all 3 illnesses can produce these signs and symptoms. Acareful history may uncover risk factors for cellulitis or septic arthritis, such aspossible exposure to gonorrhea, a recent puncture wound over the joint, or systemicsigns of disseminated infection.
Physical ExaminationPatients experiencing an acute attack of gout or pseudogout most often presentwith involvement of a single joint. However, all joints must be examined todetermine whether the patient’s arthritis is monoarticular or polyarticular. Involvedjoints have all the signs of inflammation: swelling, warmth, erythema, andtenderness.
The erythema over the joint may resemble cellulitis; the skin may desquamate asthe attack subsides. The joint capsule becomes quickly swollen, resulting in a lossof range of motion of the involved joint.
Patients may be febrile during an acute gout attack, particularly if it is polyarticular.However, it is important to look for sites of infection that may have seeded the jointand caused an infectious arthritis resembling or coexisting with acute gouty arthritis.
Migratory polyarthritis is a rare presentation. Polyarticular gout commonly involvesthe small joints of the fingers and toes, as well as the knees. An inflammatorysynovial effusion may be present. Uncommonly, acute gout may present as carpaltunnel syndrome.
Posterior interosseous nerve syndrome is a rare compression neuropathy thatmanifests as inability to extend the fingers actively. The syndrome has beenreported in a patient with elbow swelling from an attack of pseudogout; in this case,treatment with intraarticular steroids led to resolution of the nerve palsy.[73]
Patients with established gout may have chronic arthritis. Affected joints evidencetenderness and swelling, with or without redness, warmth, or joint damage.
Tophi
Although gout typically causes joint inflammation, it can also cause inflammation inother synovialbased structures, such as bursae and tendons. Tophi are collectionsof urate crystals in the soft tissues. They tend to develop after about a decade inuntreated patients who develop chronic gouty arthritis. Tophi may develop earlier inolder women, particularly those receiving diuretics.[68, 69, 70]
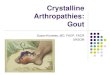
Tophi are classically located along the helix of the ear, but they can be found inmultiple locations, including the fingers, the toes, the prepatellar bursa, and alongthe olecranon, where they can resemble rheumatoid nodules (see the imagesbelow). Rarely, a creamy discharge may be present.[74, 75] The finding of anapparent rheumatoid nodule in a patient with a negative rheumatoid factor assay ora history of drainage from a nodule should prompt consideration of gout in thedifferential diagnosis.[76]
Gout. Tophaceous deposits in ear.
10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 3/10
Gout. Tophaceous deposits on elbow.
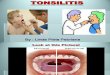
Gout. Chronic tophaceous gout in untreated patient with endstage renal disease.
Eye involvement
The folklore surrounding gout has also involved the eye, and before the 20thcentury, a myriad of common and unusual ocular symptoms were falsely ascribed togout. Medical science has since documented eye involvement as a rare but definiteaspect of gout. All manifestations of gout in the eye are secondary to deposition ofurate crystals within the ocular tissue.[77, 78]
Tophi have been described in the eyelids.[79, 80, 81] Conjunctival nodules containingneedlelike crystals have been described within the interpalpebral areas, sometimesassociated with a mild marginal keratitis. Band keratopathy with refractile, yellowcrystals in the deep corneal epithelial cells and at the level of the Bowmanmembrane are not uncommon.[82]
Blurring of vision from the corneal haze or a foreign body sensation due to epithelialbreakdown may occur. Gout rarely can be associated with anterior uveitis; DukeElder mentions this as a cause of hemorrhagic iritis in his classic Text Book ofOphthalmology. Scleritis and tendinitis have also been described. Besides thecornea, the iris, anterior chamber, lens, and sclera have been found to harbor uratecrystals; on postmortem examination, urate crystals have also been found in tarsalcartilage and in the tendons of extraocular muscles.[77, 78]
ComplicationsComplications of gout include the following:
Severe degenerative arthritisSecondary infectionsUrate or uric acid nephropathyIncreased susceptibility to infectionUrate nephropathyRenal stonesNerve or spinal cord impingement [83, 84]
Fractures in joints with tophaceous gout [85]
Differential Diagnoses
Contributor Information and DisclosuresAuthorBruce M Rothschild, MD Professor of Medicine, Northeast Ohio Medical University; Adjunct Professor,Department of Biomedical Engineering, University of Akron; Research Associate, University of Kansas Museumof Natural History; Research Associate, Carnegie Museum
Bruce M Rothschild, MD is a member of the following medical societies: American Association for theAdvancement of Science, American College of Rheumatology, International Skeletal Society, New YorkAcademy of Sciences, Sigma Xi, Society of Skeletal Radiology
Disclosure: Nothing to disclose.
Coauthor(s)Mark L Francis, MD Professor of Medical Education, Department of Medical Education, Paul L Foster School ofMedicine, Texas Tech University Health Sciences Center
Mark L Francis, MD is a member of the following medical societies: American College of Physicians, Phi BetaKappa
10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 4/10
Disclosure: Nothing to disclose.
Anne V Miller, MD Chief, Rheumatology Division; Assistant Professor of Internal Medicine, Department ofMedicine, Division of Rheumatology, Southern Illinois University School of Medicine
Anne V Miller, MD is a member of the following medical societies: Alpha Omega Alpha, American College ofPhysicians, American College of Rheumatology, International Society for Clinical Densitometry
Disclosure: Nothing to disclose.
Chief EditorHerbert S Diamond, MD Visiting Professor of Medicine, Division of Rheumatology, State University of New YorkDownstate Medical Center; Chairman Emeritus, Department of Internal Medicine, Western Pennsylvania Hospital
Herbert S Diamond, MD is a member of the following medical societies: Alpha Omega Alpha, American Collegeof Physicians, American College of Rheumatology, American Medical Association, Phi Beta Kappa
Disclosure: Nothing to disclose.
AcknowledgementsRichard W Allinson, MD Associate Professor, Department of Ophthalmology, Texas A&M University HealthScience Center; Senior Staff Ophthalmologist, Scott and White Clinic
Richard W Allinson, MD, is a member of the following medical societies: American Academy of Ophthalmology,American Medical Association, and Texas Medical Association
Disclosure: Nothing to disclose.
Lawrence H Brent, MD Associate Professor of Medicine, Jefferson Medical College of Thomas JeffersonUniversity; Chair, Program Director, Department of Medicine, Division of Rheumatology, Albert Einstein MedicalCenter
Lawrence H Brent, MD is a member of the following medical societies: American Association for theAdvancement of Science, American Association of Immunologists, American College of Physicians, andAmerican College of Rheumatology
Disclosure: Abbott Honoraria Speaking and teaching; Centocor Consulting fee Consulting; GenentechGrant/research funds Other; HGS/GSK Honoraria Speaking and teaching; Omnicare Consulting fee Consulting;Pfizer Honoraria Speaking and teaching; Roche Speaking and teaching; Savient Honoraria Speaking andteaching; UCB Honoraria Speaking and teaching
Andrew A Dahl, MD Director of Ophthalmology Teaching, MidHudson Family Practice Institute, The Institutefor Family Health; Assistant Professor of Surgery (Ophthalmology), New York College of Medicine
Andrew A Dahl, MD is a member of the following medical societies: Alpha Omega Alpha, American Academy ofOphthalmology, American College of Surgeons, American Medical Association, American Society of Cataractand Refractive Surgery, and Wilderness Medical Society
Disclosure: Nothing to disclose.
Paul E Di Cesare, MD, FACS Professor and Chair, Department of Orthopedic Sugery, University of California,Davis, School of Medicine
Paul E Di Cesare, MD, FACS is a member of the following medical societies: American Academy of OrthopaedicSurgeons, American College of Surgeons, and Sigma Xi
Disclosure: Stryker Consulting fee Consulting
Steven C Dronen, MD, FAAEM Chair, Department of Emergency Medicine, LeConte Medical Center
Steven C Dronen, MD, FAAEM is a member of the following medical societies: American Academy ofEmergency Medicine and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Gino A Farina, MD, FACEP, FAAEM Associate Professor of Clinical Emergency Medicine, Albert EinsteinCollege of Medicine; Program Director, Department of Emergency Medicine, Long Island Jewish Medical Center
Gino A Farina, MD, FACEP, FAAEM is a member of the following medical societies: American Academy ofEmergency Medicine, American College of Emergency Physicians, and Society for Academic EmergencyMedicine
Disclosure: Nothing to disclose.
Harris Gellman, MD Consulting Surgeon, Broward Hand Center; Voluntary Clinical Professor of OrthopedicSurgery and Plastic Surgery, Departments of Orthopedic Surgery and Surgery, University of Miami, Leonard MMiller School of Medicine
Harris Gellman, MD is a member of the following medical societies: American Academy of Medical Acupuncture,American Academy of Orthopaedic Surgeons, American Orthopaedic Association, American Society for Surgeryof the Hand, and Arkansas Medical Society
Disclosure: Nothing to disclose.
Joseph Kaplan, MD, MS, FACEP Attending Physician, Department of Emergency Medicine, Martin ArmyCommunity Hospital, Fort Benning
Joseph Kaplan, MD, MS, FACEP is a member of the following medical societies: American College ofEmergency Physicians
Disclosure: Nothing to disclose.
Jegan Krishnan, MBBS, FRACS, PhD Professor, Chair, Department of Orthopedic Surgery, Flinders Universityof South Australia; Senior Clinical Director of Orthopedic Surgery, Repatriation General Hospital; PrivatePractice, Orthopaedics SA, Flinders Private Hospital
Jegan Krishnan, MBBS, FRACS, PhD, is a member of the following medical societies: Australian MedicalAssociation, Australian Orthopaedic Association, and Royal Australasian College of Surgeons
10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 5/10
Disclosure: Nothing to disclose.
Edward A Michelson, MD Associate Professor, Program Director, Department of Emergency Medicine,University Hospital Health Systems of Cleveland
Edward A Michelson, MD is a member of the following medical societies: American College of EmergencyPhysicians, National Association of EMS Physicians, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Sriya K M Ranatunga, MD, MPH Associate Professor, Department of Clinical Medicine, Southern IllinoisUniversity School of Medicine
Disclosure: Nothing to disclose.
Hampton Roy Sr, MD Associate Clinical Professor, Department of Ophthalmology, University of Arkansas forMedical Sciences
Hampton Roy Sr, MD is a member of the following medical societies: American Academy of Ophthalmology,American College of Surgeons, and PanAmerican Association of Ophthalmology
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center Collegeof Pharmacy; EditorinChief, Medscape Drug Reference
Disclosure: Medscape Salary Employment
R Christopher Walton, MD Professor, Director of Uveitis and Ocular Inflammatory Disease Service, Departmentof Ophthalmology, Assistant Dean for Graduate Medical Education, University of Tennessee College ofMedicine; Consulting Staff, Regional Medical Center, Memphis Veterans Affairs Medical Center, St JudeChildren's Research Hospital
R Christopher Walton, MD is a member of the following medical societies: American Academy ofOphthalmology, American College of Healthcare Executives, American Uveitis Society, Association for Researchin Vision and Ophthalmology, and Retina Society
Disclosure: Nothing to disclose.
References
1. Choi HK, Atkinson K, Karlson EW, et al. Alcohol intake and risk of incident gout in men: a prospectivestudy. Lancet. 2004 Apr 17. 363(9417):127781. [Medline].
2. Choi HK, Curhan G. Gout: epidemiology and lifestyle choices. Curr Opin Rheumatol. 2005 May. 17(3):3415. [Medline].
3. Currie WJ. The gout patient in general practice. Rheumatol Rehabil. 1978 Nov. 17(4):20517. [Medline].
4. Martinon F, Glimcher LH. Gout: new insights into an old disease. J Clin Invest. 2006 Aug. 116(8):20735.[Medline]. [Full Text].
5. So A. Gout in the spotlight. Arthritis Res Ther. 2008. 10(3):112. [Medline]. [Full Text].
6. DuskinBitan H, Cohen E, Goldberg E, Shochat T, Levi A, Garty M, et al. The degree of asymptomatichyperuricemia and the risk of gout. A retrospective analysis of a large cohort. Clin Rheumatol. 2014 Apr.33(4):54953. [Medline].
7. Edwards NL. Treatmentfailure gout: a moving target. Arthritis Rheum. 2008 Sep. 58(9):258790.[Medline].
8. Bluestone R, Waisman J, Klinenberg JR. The gouty kidney. Semin Arthritis Rheum. 1977 Nov. 7(2):97113. [Medline].
9. Bleyer AJ, Hart TC. Genetic factors associated with gout and hyperuricemia. Adv Chronic Kidney Dis. 2006Apr. 13(2):12430. [Medline].
10. Reginato AM, Mount DB, Yang I, Choi HK. The genetics of hyperuricaemia and gout. Nat Rev Rheumatol.2012 Oct. 8(10):61021. [Medline]. [Full Text].
11. Krishnan E, LessovSchlaggar CN, Krasnow RE, Swan GE. Nature versus nurture in gout: a twin study.Am J Med. 2012 May. 125(5):499504. [Medline].
12. LiuBryan R, Scott P, Sydlaske A, et al. Innate immunity conferred by Tolllike receptors 2 and 4 andmyeloid differentiation factor 88 expression is pivotal to monosodium urate monohydrate crystalinducedinflammation. Arthritis Rheum. 2005 Sep. 52(9):293646. [Medline].
13. Nagase M, Baker DG, Schumacher HR Jr. Immunoglobulin G coating on crystals and ceramics enhancespolymorphonuclear cell superoxide production: correlation with immunoglobulin G adsorbed. J Rheumatol.1989 Jul. 16(7):9716. [Medline].
14. OrtizBravo E, Sieck MS, Schumacher HR Jr. Changes in the proteins coating monosodium urate crystalsduring active and subsiding inflammation. Immunogold studies of synovial fluid from patients with gout andof fluid obtained using the rat subcutaneous air pouch model. Arthritis Rheum. 1993 Sep. 36(9):127485.[Medline].
15. Akahoshi T, Murakami Y, Kitasato H. Recent advances in crystalinduced acute inflammation. Curr OpinRheumatol. 2007 Mar. 19(2):14650. [Medline].
16. Martinon F. Mechanisms of uric acid crystalmediated autoinflammation. Immunol Rev. 2010 Jan.233(1):21832. [Medline].
17. Terkeltaub RA. What stops a gouty attack?. J Rheumatol. 1992 Jan. 19(1):810. [Medline].
18. Yagnik DR, Evans BJ, Florey O, et al. Macrophage release of transforming growth factor beta1 duringresolution of monosodium urate monohydrate crystalinduced inflammation. Arthritis Rheum. 2004 Jul.50(7):227380. [Medline].
19. Lioté F, Ea HK. Recent developments in crystalinduced inflammation pathogenesis and management.
10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 6/10
Curr Rheumatol Rep. 2007 Jun. 9(3):24350. [Medline].
20. Richette P, Bardin T. Gout. Lancet. 2010 Jan 23. 375(9711):31828. [Medline].
21. Singh JA, Reddy SG, Kundukulam J. Risk factors for gout and prevention: a systematic review of theliterature. Curr Opin Rheumatol. 2011 Mar. 23(2):192202. [Medline].
22. McAdamsDemarco MA, Maynard JW, Coresh J, Baer AN. Anemia and the onset of gout in a populationbased cohort of adults: Atherosclerosis Risk in Communities study. Arthritis Res Ther. 2012 Aug 20.14(4):R193. [Medline]. [Full Text].
23. Choi HK, Willett W, Curhan G. Fructoserich beverages and risk of gout in women. JAMA. 2010 Nov 24.304(20):22708. [Medline].
24. Choi HK, Curhan G. Soft drinks, fructose consumption, and the risk of gout in men: prospective cohortstudy. BMJ. 2008 Feb 9. 336(7639):30912. [Medline]. [Full Text].
25. Yang Q, Guo CY, Cupples LA, Levy D, Wilson PW, Fox CS. Genomewide search for genes affectingserum uric acid levels: the Framingham Heart Study. Metabolism. 2005 Nov. 54(11):143541. [Medline].
26. Dehghan A, Köttgen A, Yang Q, Hwang SJ, Kao WL, Rivadeneira F, et al. Association of three geneticloci with uric acid concentration and risk of gout: a genomewide association study. Lancet. 2008 Dec 6.372(9654):195361. [Medline]. [Full Text].
27. Wallace C, Newhouse SJ, Braund P, Zhang F, Tobin M, Falchi M, et al. Genomewide association studyidentifies genes for biomarkers of cardiovascular disease: serum urate and dyslipidemia. Am J Hum Genet.2008 Jan. 82(1):13949. [Medline]. [Full Text].
28. Kolz M, Johnson T, Sanna S, Teumer A, Vitart V, Perola M, et al. Metaanalysis of 28,141 individualsidentifies common variants within five new loci that influence uric acid concentrations. PLoS Genet. 2009Jun. 5(6):e1000504. [Medline]. [Full Text].
29. Merriman TR. Population heterogeneity in the genetic control of serum urate. Semin Nephrol. 2011 Sep.31(5):4205. [Medline].
30. Vitart V, Rudan I, Hayward C, Gray NK, Floyd J, Palmer CN, et al. SLC2A9 is a newly identified uratetransporter influencing serum urate concentration, urate excretion and gout. Nat Genet. 2008 Apr.40(4):43742. [Medline].
31. Campion EW, Glynn RJ, DeLabry LO. Asymptomatic hyperuricemia. Risks and consequences in theNormative Aging Study. Am J Med. 1987 Mar. 82(3):4216. [Medline].
32. Hall AP, Barry PE, Dawber TR, McNamara PM. Epidemiology of gout and hyperuricemia. A longtermpopulation study. Am J Med. 1967 Jan. 42(1):2737. [Medline].
33. Lin HY, Rocher LL, McQuillan MA, Schmaltz S, Palella TD, Fox IH. Cyclosporineinduced hyperuricemiaand gout. N Engl J Med. 1989 Aug 3. 321(5):28792. [Medline].
34. Rho YH, Zhu Y, Zhang Y, Reginato AM, Choi HK. Risk factors for pseudogout in the general population.Rheumatology (Oxford). 2012 Nov. 51(11):20704. [Medline]. [Full Text].
35. Watanabe H, Yamada S, Anayama S, Sato E, Maekawa S, Sugiyama H, et al. Pseudogout attackinduced during etidronate disodium therapy. Mod Rheumatol. 2006. 16(2):1179. [Medline].
36. Taggarshe D, Ng CH, Molokwu C, Singh S. Acute pseudogout following contrast angiography. ClinRheumatol. 2006 Feb. 25(1):1156. [Medline].
37. Ciancio G, Bortoluzzi A, Govoni M. Epidemiology of gout and chondrocalcinosis. Reumatismo. 2012 Jan19. 63(4):20720. [Medline].
38. Zhu Y, Pandya BJ, Choi HK. Prevalence of gout and hyperuricemia in the US general population: TheNational Health and Nutrition Examination Survey 20072008. Arthritis Rheum. 2011 Oct. 63(10):313641.[Medline].
39. Kim KY, Ralph Schumacher H, Hunsche E, Wertheimer AI, Kong SX. A literature review of theepidemiology and treatment of acute gout. Clin Ther. 2003 Jun. 25(6):1593617. [Medline].
40. Terkeltaub RA. Gout: Recent advances and emerging therapies. Rheumatic Disease Clinics Update.2008;3(1):19.:
41. Garg R, Sayles HR, Yu F, Michaud K, Singh J, Saag KG, et al. Goutrelated health care utilization in USemergency departments, 2006 through 2008. Arthritis Care Res (Hoboken). 2013 Apr. 65(4):5717.[Medline].
42. Miao Z, Li C, Chen Y, Zhao S, Wang Y, Wang Z, et al. Dietary and lifestyle changes associated with highprevalence of hyperuricemia and gout in the Shandong coastal cities of Eastern China. J Rheumatol. 2008Sep. 35(9):185964. [Medline].
43. Cea Soriano L, Rothenbacher D, Choi HK, García Rodríguez LA. Contemporary epidemiology of gout inthe UK general population. Arthritis Res Ther. 2011 Mar 3. 13(2):R39. [Medline]. [Full Text].
44. Trifirò G, Morabito P, Cavagna L, Ferrajolo C, Pecchioli S, Simonetti M, et al. Epidemiology of gout andhyperuricaemia in Italy during the years 20052009: a nationwide populationbased study. Ann Rheum Dis.2013 May. 72(5):694700. [Medline].
45. Reed D, Labarthe D, Stallones R. Epidemiologic studies of serum uric acid levels among Micronesians.Arthritis Rheum. 1972 JulAug. 15(4):38190. [Medline].
46. Rose BS. Gout in Maoris. Semin Arthritis Rheum. 1975 Nov. 5(2):12145. [Medline].
47. Choi HK, De Vera MA, Krishnan E. Gout and the risk of type 2 diabetes among men with a highcardiovascular risk profile. Rheumatology (Oxford). 2008 Oct. 47(10):156770. [Medline].
48. OlaniyiLeyimu BY. Consider gout in patients with risk factors, regardless of age. Am Fam Physician. 2008Jul 15. 78(2):176. [Medline].
49. Fravel MA, Ernst ME. Management of gout in the older adult. Am J Geriatr Pharmacother. 2011 Oct.9(5):27185. [Medline].
50. Singh H, Torralba KD. Therapeutic challenges in the management of gout in the elderly. Geriatrics. 2008Jul. 63(7):138, 20. [Medline].
10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 7/10
51. Simmonds HA, McBride MB, Hatfield PJ, Graham R, McCaskey J, Jackson M. Polynesian women are alsoat risk for hyperuricaemia and gout because of a genetic defect in renal urate handling. Br J Rheumatol.1994 Oct. 33(10):9327. [Medline].
52. Hochberg MC, Thomas J, Thomas DJ, Mead L, Levine DM, Klag MJ. Racial differences in the incidence ofgout. The role of hypertension. Arthritis Rheum. 1995 May. 38(5):62832. [Medline].
53. Mody GM, Naidoo PD. Gout in South African blacks. Ann Rheum Dis. 1984 Jun. 43(3):3947. [Medline].[Full Text].
54. Schumacher HR, Taylor W, JosephRidge N, PerezRuiz F, Chen LX, Schlesinger N, et al. Outcomeevaluations in gout. J Rheumatol. 2007 Jun. 34(6):13815. [Medline].
55. Becker MA, MacDonald PA, Hunt BJ, Lademacher C, JosephRidge N. Determinants of the clinicaloutcomes of gout during the first year of uratelowering therapy. Nucleosides Nucleotides Nucleic Acids.2008 Jun. 27(6):58591. [Medline].
56. Yü T, Talbott JH. Changing trends of mortality in gout. Semin Arthritis Rheum. 1980 Aug. 10(1):19.[Medline].
57. Forman JP, Choi H, Curhan GC. Uric acid and insulin sensitivity and risk of incident hypertension. ArchIntern Med. 2009 Jan 26. 169(2):15562. [Medline]. [Full Text].
58. Kim SY, De Vera MA, Choi HK. Gout and mortality. Clin Exp Rheumatol. 2008 SepOct. 26(5 Suppl51):S1159. [Medline].
59. Lottmann K, Chen X, Schädlich PK. Association between gout and allcause as well as cardiovascularmortality: a systematic review. Curr Rheumatol Rep. 2012 Apr. 14(2):195203. [Medline]. [Full Text].
60. Feig DI, Johnson RJ. The role of uric acid in pediatric hypertension. J Ren Nutr. Jan/2007. 17(1):7983.[Medline].
61. Krishnan E, Svendsen K, Neaton JD, et al. Longterm cardiovascular mortality among middleaged menwith gout. Arch Intern Med. 2008 May 26. 168(10):110410. [Medline].
62. Kuo CF, See LC, Luo SF, Ko YS, Lin YS, Hwang JS, et al. Gout: an independent risk factor for allcauseand cardiovascular mortality. Rheumatology (Oxford). 2010 Jan. 49(1):1416. [Medline].
63. Janeczko L. Gout Tied to Higher Risk of Heart Attack and Stroke. Medscape Medical News. Available athttp://www.medscape.com/viewarticle/813367. Accessed: November 4, 2013.
64. Seminog OO, Goldacre MJ. Gout as a risk factor for myocardial infarction and stroke in England: evidencefrom record linkage studies. Rheumatology (Oxford). 2013 Sep 17. [Medline].
65. Barclay L. Gout Linked to Increased Vascular Disease Risk. Medscape Medical News. Available athttp://www.medscape.com/viewarticle/830663?nlid=64464_2224&src=wnl_edit_medp_rheu&spon=27.Accessed: September 8, 2014.
66. Clarson LE, Hider SL, Belcher J, Heneghan C, Roddy E, Mallen CD. Increased risk of vascular diseaseassociated with gout: a retrospective, matched cohort study in the UK Clinical Practice Research Datalink.Ann Rheum Dis. 2014 Aug 27. [Medline].
67. Lin SH, Hsieh ET, Wu TY, Chang CW. Cervical myelopathy induced by pseudogout in ligamentum flavumand retroodontoid mass: a case report. Spinal Cord. 2006 Nov. 44(11):6924. [Medline].
68. Puig JG, Michan AD, Jimenez ML, et al. Female gout. Clinical spectrum and uric acid metabolism. ArchIntern Med. 1991 Apr. 151(4):72632. [Medline].
69. Meyers OL, Monteagudo FS. Gout in females: an analysis of 92 patients. Clin Exp Rheumatol. 1985 AprJun. 3(2):1059. [Medline].
70. Macfarlane DG, Dieppe PA. Diureticinduced gout in elderly women. Br J Rheumatol. 1985 May.24(2):1557. [Medline].
71. Kramer HM, Curhan G. The association between gout and nephrolithiasis: the National Health andNutrition Examination Survey III, 19881994. Am J Kidney Dis. 2002 Jul. 40(1):3742. [Medline].
72. Marchini GS, Sarkissian C, Tian D, Gebreselassie S, Monga M. Gout, stone composition and urinary stonerisk: a matched case comparative study. J Urol. 2013 Apr. 189(4):13349. [Medline].
73. Taniguchi Y, Yoshida M, Tamaki T. Posterior interosseous nerve syndrome due to pseudogout. J HandSurg Br. 1999 Feb. 24(1):1257. [Medline].
74. Dalbeth N, Schauer C, Macdonald P, PerezRuiz F, Schumacher HR, Hamburger S, et al. Methods oftophus assessment in clinical trials of chronic gout: a systematic literature review and pictorial referenceguide. Ann Rheum Dis. 2011 Apr. 70(4):597604. [Medline].
75. Stocker SL, Graham GG, McLachlan AJ, Williams KM, Day RO. Pharmacokinetic and pharmacodynamicinteraction between allopurinol and probenecid in patients with gout. J Rheumatol. 2011 May. 38(5):90410. [Medline].
76. Chehab MR, Goyal J, Schlesinger N. Tophaceous Pustulelike Rash in a Patient with Gout. J Rheumatol.2012 Jan. 39(1):1945. [Medline].
77. Coassin M, Piovanetti O, Stark WJ, Green WR. Urate deposition in the iris and anterior chamber.Ophthalmology. 2006 Mar. 113(3):4625. [Medline].
78. Slansky HH, Kubara T. Intranuclear urate crystals in corneal epithelium. Arch Ophthalmol. 1968 Sep.80(3):33844. [Medline].
79. Bernad B, Narvaez J, DiazTorné C, DiezGarcia M, Valverde J. Clinical image: corneal tophus depositionin gout. Arthritis Rheum. 2006 Mar. 54(3):1025. [Medline].
80. MCWILLIAMS JR. Ocular findings in gout; report of a case of conjunctival tophi. Am J Ophthalmol. 1952Dec. 35(12):177883. [Medline].
81. Morris WR, Fleming JC. Gouty tophus at the lateral canthus. Arch Ophthalmol. 2003 Aug. 121(8):11957.[Medline].
82. Fishman RS, Sunderman FW. Band keratopathy in gout. Arch Ophthalmol. 1966 Mar. 75(3):3679.[Medline].
10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 8/10
83. Julkunen H, Heinonen OP, Pyörälä K. Hyperostosis of the spine in an adult population. Its relation tohyperglycaemia and obesity. Ann Rheum Dis. 1971 Nov. 30(6):60512. [Medline]. [Full Text].
84. KOSKOFF YD, MORRIS LE, LUBIC LG. Paraplegia as a complication of gout. J Am Med Assoc. 1953May 2. 152(1):378. [Medline].
85. Nguyen C, Ea HK, Palazzo E, Lioté F. Tophaceous gout: an unusual cause of multiple fractures. Scand JRheumatol. 2010. 39(1):936. [Medline].
86. Janssens HJ, Fransen J, van de Lisdonk EH, van Riel PL, van Weel C, Janssen M. A diagnostic rule foracute gouty arthritis in primary care without joint fluid analysis. Arch Intern Med. 2010 Jul 12.170(13):11206. [Medline].
87. Barthelemy CR, Nakayama DA, Carrera GF, Lightfoot RW Jr, Wortmann RL. Gouty arthritis: a prospectiveradiographic evaluation of sixty patients. Skeletal Radiol. 1984. 11(1):18. [Medline].
88. Dalbeth N, Clark B, Gregory K, Gamble G, Sheehan T, Doyle A, et al. Mechanisms of bone erosion ingout: a quantitative analysis using plain radiography and computed tomography. Ann Rheum Dis. 2009Aug. 68(8):12905. [Medline].
89. Fodor D, Albu A, Gherman C. Crystalassociated synovitis ultrasonographic feature and clinical correlation.Ortop Traumatol Rehabil. 2008 MarApr. 10(2):99110. [Medline].
90. de Ávila Fernandes E, Kubota ES, Sandim GB, Mitraud SA, Ferrari AJ, Fernandes AR. Ultrasoundfeatures of tophi in chronic tophaceous gout. Skeletal Radiol. 2011 Mar. 40(3):30915. [Medline].
91. Fernandes EA, Lopes MG, Mitraud SA, Ferrari AJ, Fernandes AR. Ultrasound characteristics of goutytophi in the olecranon bursa and evaluation of their reproducibility. Eur J Radiol. 2011 Jan 13. [Medline].
92. Thiele RG, Schlesinger N. Diagnosis of gout by ultrasound. Rheumatology (Oxford). 2007 Jul. 46(7):111621. [Medline].
93. Loffler C, Sattler H, Peters L, Loffler U, Uppenkamp M, Bergner R. Distinguishing gouty arthritis fromcalcium pyrophosphate disease and other arthritides. J Rheumatol. 2015 Mar. 42(3):51320. [Medline].
94. Naredo E, Uson J, JiménezPalop M, Martínez A, Vicente E, Brito E, et al. Ultrasounddetectedmusculoskeletal urate crystal deposition: which joints and what findings should be assessed for diagnosinggout?. Ann Rheum Dis. 2014 Aug. 73(8):15228. [Medline].
95. Pineda C, AmezcuaGuerra LM, Solano C, RodriguezHenríquez P, HernándezDíaz C, Vargas A, et al.Joint and tendon subclinical involvement suggestive of gouty arthritis in asymptomatic hyperuricemia: anultrasound controlled study. Arthritis Res Ther. 2011 Jan 17. 13(1):R4. [Medline]. [Full Text].
96. Ottaviani S, Juge PA, Aubrun A, Palazzo E, Dieudé P. Sensitivity and Reproducibility of Ultrasonographyin Calcium Pyrophosphate Crystal Deposition in Knee Cartilage: A Crosssectional Study. J Rheumatol.2015 Aug. 42 (8):15113. [Medline].
97. De Miguel E, Puig JG, Castillo C, Peiteado D, Torres RJ, MartínMola E. Diagnosis of gout in patients withasymptomatic hyperuricaemia: a pilot ultrasound study. Ann Rheum Dis. 2012 Jan. 71(1):1578. [Medline].
98. Dalbeth N, Clark B, Gregory K, Gamble G, Sheehan T, Doyle A, et al. Mechanisms of bone erosion ingout: a quantitative analysis using plain radiography and computed tomography. Ann Rheum Dis. 2009Aug. 68(8):12905. [Medline].
99. AlArfaj AM, Nicolaou S, Eftekhari A, Munk P, Shojani K, Reid G, et al. Utility of dual energy computedtomography (DECT) i8n tophaceous gout. Ann Rheum Dis. 2008;58:S878.
100. Ward IM, Scott JN, Mansfield LT, Battafarano DF. DualEnergy Computed Tomography DemonstratingDestructive Calcium Pyrophosphate Deposition Disease of the Distal Radioulnar Joint MimickingTophaceous Gout. J Clin Rheumatol. 2015 Sep. 21 (6):3147. [Medline].
101. Shimizu T, Hori H. The prevalence of nephrolithiasis in patients with primary gout: a crosssectional studyusing helical computed tomography. J Rheumatol. 2009 Sep. 36(9):195862. [Medline].
102. Poh YJ, Dalbeth N, Doyle A, McQueen FM. Magnetic Resonance Imaging Bone Edema Is Not a MajorFeature of Gout Unless There Is Concomitant Osteomyelitis: 10year Findings from a HighprevalencePopulation. J Rheumatol. 2011 Nov. 38(11):247581. [Medline].
103. McQueen FM, Doyle A, Reeves Q, Gao A, Tsai A, Gamble GD. Bone erosions in patients with chronicgouty arthropathy are associated with tophi but not bone oedema or synovitis: new insights from a 3 T MRIstudy. Rheumatology (Oxford). 2014 Jan. 53(1):95103. [Medline].
104. Oostveen JC, van de Laar MA. Magnetic resonance imaging in rheumatic disorders of the spine andsacroiliac joints. Semin Arthritis Rheum. 2000 Aug. 30(1):5269. [Medline].
105. [Guideline] Khanna D, Fitzgerald JD, Khanna PP, Bae S, Singh MK, Neogi T, et al. 2012 AmericanCollege of Rheumatology guidelines for management of gout. Part 1: Systematic nonpharmacologic andpharmacologic therapeutic approaches to hyperuricemia. Arthritis Care Res (Hoboken). 2012 Oct.64(10):143146. [Medline].
106. [Guideline] Khanna D, Khanna PP, Fitzgerald JD, Singh MK, Bae S, Neogi T, et al. 2012 AmericanCollege of Rheumatology guidelines for management of gout. Part 2: Therapy and antiinflammatoryprophylaxis of acute gouty arthritis. Arthritis Care Res (Hoboken). 2012 Oct. 64(10):144761. [Medline].
107. Goodman A. UrateLowering Cuts Complications From Gout. Medscape [serial online]. Available athttp://www.medscape.com/viewarticle/814057. Accessed: November 18, 2013.
108. Reber P, Crevoisier X, Noesberger B. Unusual localisation of tophaceous gout. A report of four cases andreview of the literature. Arch Orthop Trauma Surg. 1996. 115(5):2979. [Medline].
109. Schapira D, Stahl S, Izhak OB, BalbirGurman A, Nahir AM. Chronic tophaceous gouty arthritis mimickingrheumatoid arthritis. Semin Arthritis Rheum. 1999 Aug. 29(1):5663. [Medline].
110. Shogan CP, Folio CL. Tophaceous gout and rheumatoid arthritis awareness. J Am Osteopath Assoc. 2008Jul. 108(7):352; author reply 3523. [Medline].
111. Zhang Y, Neogi T, Chen C, Chaisson C, Hunter DJ, Choi H. Lowdose aspirin use and recurrent goutattacks. Ann Rheum Dis. 2014 Feb 1. 73(2):38590. [Medline].
112. Schumacher HR, Berger MF, LiYu J, PerezRuiz F, BurgosVargas R, Li C. Efficacy and tolerability of
10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 9/10
celecoxib in the treatment of acute gouty arthritis: a randomized controlled trial. J Rheumatol. 2012 Sep.39(9):185966. [Medline].
113. Medsafe Pharmacovigilance Team. Colchicine: lower doses for greater safety. Available athttp://www.medsafe.govt.nz/profs/puarticles/colchdose.htm. Accessed: October 3, 2008.
114. Nuki G. Colchicine: its mechanism of action and efficacy in crystalinduced inflammation. Curr RheumatolRep. 2008 Jul. 10(3):21827. [Medline].
115. Zhang W, Doherty M, Bardin T, et al. EULAR evidence based recommendations for gout. Part II:Management. Report of a task force of the EULAR Standing Committee for International Clinical StudiesIncluding Therapeutics (ESCISIT). Ann Rheum Dis. 2006 Oct. 65(10):131224. [Medline].
116. Terkeltaub RA, Furst DE, Bennett K, Kook KA, Crockett RS, Davis MW. High versus low dosing of oralcolchicine for early acute gout flare: Twentyfourhour outcome of the first multicenter, randomized, doubleblind, placebocontrolled, parallelgroup, dosecomparison colchicine study. Arthritis Rheum. 2010 Apr.62(4):10608. [Medline].
117. Terkeltaub RA, Furst DE, Digiacinto JL, Kook KA, Davis MW. Novel evidencebased colchicine dosereduction algorithm to predict and prevent colchicine toxicity in the presence of cytochrome P450 3A4/Pglycoprotein inhibitors. Arthritis Rheum. 2011 Aug. 63(8):222637. [Medline].
118. FDA takes action to stop the marketing of unapproved injectable drugs containing colchicine. US Food andDrug Administration. Available at www.fda.gov/bbs/topics/news/2008/new01791.html. Accessed:September 30, 2008.
119. Roddy E. Hyperuricemia, gout, and lifestyle factors. J Rheumatol. 2008 Sep. 35(9):168991. [Medline].
120. PerezRuiz F, HerreroBeites AM, Carmona L. A twostage approach to the treatment of hyperuricemia ingout: The "Dirty Dish" hypothesis. Arthritis Rheum. 2011 Dec. 63(12):40026. [Medline].
121. Yu T. The efficacy of colchicine prophylaxis in articular gouta reappraisal after 20 years. Semin ArthritisRheum. 1982 Nov. 12(2):25664. [Medline].
122. [Guideline] Wallace SL, Singer JZ, Duncan GJ, et al. Renal function predicts colchicine toxicity: guidelinesfor the prophylactic use of colchicine in gout. J Rheumatol. 1991 Feb. 18(2):2649. [Medline].
123. Markel A. Allopurinolinduced DRESS syndrome. Isr Med Assoc J. 2005 Oct. 7(10):65660. [Medline].
124. Singer JZ, Wallace SL. The allopurinol hypersensitivity syndrome. Unnecessary morbidity and mortality.Arthritis Rheum. 1986 Jan. 29(1):827. [Medline].
125. McAdams DeMarco MA, Maynard JW, Baer AN, Gelber AC, Young JH, Alonso A, et al. Diuretic use,increased serum urate levels, and risk of incident gout in a populationbased study of adults withhypertension: the Atherosclerosis Risk in Communities cohort study. Arthritis Rheum. 2012 Jan. 64(1):1219. [Medline]. [Full Text].
126. Stamp LK, Taylor WJ, Jones PB, Dockerty JL, Drake J, Frampton C, et al. Starting dose is a risk factor forallopurinol hypersensitivity syndrome: a proposed safe starting dose of allopurinol. Arthritis Rheum. 2012Aug. 64(8):252936. [Medline].
127. VázquezMellado J, Morales EM, PachecoTena C, et al. Relation between adverse events associated withallopurinol and renal function in patients with gout. Ann Rheum Dis. 2001 Oct. 60(10):9813. [Medline].
128. Riedel AA, Nelson M, JosephRidge N, Wallace K, MacDonald P, Becker M. Compliance with allopurinoltherapy among managed care enrollees with gout: a retrospective analysis of administrative claims. JRheumatol. 2004 Aug. 31(8):157581. [Medline].
129. Rees F, Jenkins W, Doherty M. Patients with gout adhere to curative treatment if informed appropriately:proofofconcept observational study. Ann Rheum Dis. 2012 Jun 7. [Medline].
130. Hair PI, McCormack PL, Keating GM. Febuxostat. Drugs. 2008. 68(13):186574. [Medline].
131. Schumacher HR Jr, Becker MA, Wortmann RL, Macdonald PA, Hunt B, Streit J, et al. Effects offebuxostat versus allopurinol and placebo in reducing serum urate in subjects with hyperuricemia and gout:a 28week, phase III, randomized, doubleblind, parallelgroup trial. Arthritis Rheum. 2008 Nov 15.59(11):15408. [Medline].
132. Becker MA, Schumacher HR Jr, Wortmann RL, et al. Febuxostat compared with allopurinol in patients withhyperuricemia and gout. N Engl J Med. 2005 Dec 8. 353(23):245061. [Medline].
133. Becker MA, Schumacher HR, Espinoza LR, Wells AF, MacDonald P, Lloyd E, et al. The urateloweringefficacy and safety of febuxostat in the treatment of the hyperuricemia of gout: the CONFIRMS trial.Arthritis Res Ther. 2010. 12(2):R63. [Medline]. [Full Text].
134. Jackson RL, Hunt B, MacDonald PA. The efficacy and safety of febuxostat for urate lowering in goutpatients 65+ years of age. BMC Geriatr. 2012 Mar 21. 12:11. [Medline]. [Full Text].
135. Wells AF, MacDonald PA, Chefo S, Jackson RL. African American patients with gout: efficacy and safetyof febuxostat vs allopurinol. BMC Musculoskelet Disord. 2012 Feb 9. 13:15. [Medline]. [Full Text].
136. Chohan S, Becker MA, MacDonald PA, Chefo S, Jackson RL. Women with gout: efficacy and safety ofuratelowering with febuxostat and allopurinol. Arthritis Care Res (Hoboken). 2012 Feb. 64(2):25661.[Medline].
137. Bieber JD, Terkeltaub RA. Gout: on the brink of novel therapeutic options for an ancient disease. ArthritisRheum. 2004 Aug. 50(8):240014. [Medline].
138. Committee for Medicinal Products for Human Use (CHMP). Summary of opinion1 (initial authorisation):Krystexxa (pegloticase. Available athttp://www.ema.europa.eu/docs/en_GB/document_library/Summary_of_opinion__Initial_authorisation/human/002208/WC500134058.pdf. Accessed: June 14, 2013.
139. Sundy JS, Baraf HS, Yood RA, et al. Efficacy and tolerability of pegloticase for the treatment of chronicgout in patients refractory to conventional treatment: two randomized controlled trials. JAMA. 2011 Aug 17.306(7):71120. [Medline].
140. Huang HY, Appel LJ, Choi MJ, et al. The effects of vitamin C supplementation on serum concentrations ofuric acid: results of a randomized controlled trial. Arthritis Rheum. 2005 Jun. 52(6):18437. [Medline].

10/27/2015 Gout and Pseudogout Clinical Presentation: History, Physical Examination, Complications
http://emedicine.medscape.com/article/329958clinical 10/10
Medscape Reference © 2011 WebMD, LLC
141. So A, De Smedt T, Revaz S, et al. A pilot study of IL1 inhibition by anakinra in acute gout. Arthritis ResTher. 2007. 9(2):R28. [Medline].
142. Lee YH, Lee CH, Lee J. Effect of fenofibrate in combination with urate lowering agents in patients withgout. Korean J Intern Med. 2006 Jun. 21(2):8993. [Medline].
143. So A, De Meulemeester M, Pikhlak A, et al. Canakinumab for the treatment of acute flares in difficulttotreat gouty arthritis: Results of a multicenter, phase II, doseranging study. Arthritis Rheum. 2010 Oct.62(10):306476. [Medline].
144. Lowry F. FDA Panel Says No to Canakinumab for Gout Attacks. Medscape Medical News. Available athttp://www.medscape.com/viewarticle/745076. Accessed: February 9, 2011.
145. Schumacher HR Jr, Becker MA, Lloyd E, MacDonald PA, Lademacher C. Febuxostat in the treatment ofgout: 5yr findings of the FOCUS efficacy and safety study. Rheumatology (Oxford). 2009 Feb. 48(2):18894. [Medline].
146. Sundy JS, Becker MA, Baraf HS, Barkhuizen A, Moreland LW, Huang W, et al. Reduction of plasma uratelevels following treatment with multiple doses of pegloticase (polyethylene glycolconjugated uricase) inpatients with treatmentfailure gout: results of a phase II randomized study. Arthritis Rheum. 2008 Sep.58(9):288291. [Medline].
147. Savient Pharmaceuticals, Inc. Krystexxa Prescribing Information. Available athttp://www.krystexxa.com/hcp/default.aspx.
148. Kelly JC. Gout risk high in those with psoriasis, psoriatic arthritis. Medscape Medical News. March 28,2014. [Full Text].
149. Merola JF, Wu S, Han J, Choi HK, Qureshi AA. Psoriasis, psoriatic arthritis and risk of gout in US men andwomen. Ann Rheum Dis. 2014 Mar 20. [Medline].
150. Wilson ME, Wan SH, Beyder A, Osborn TG, Beckman TJ. Acute polyarticular gout presenting as delirium.J Clin Rheumatol. 2013 Jun. 19(4):2212. [Medline].