Embed Size (px)
Citation preview

Good Morning and WelcomeThursday, April 23, 2015
Cohort 9 – ICU SCCM Georgia Meeting

Introductions and WelcomeKathy McGowanKathy McGowan, MPH VP, Quality and Safety, GHA
Jan Ratterree, RN, BSN, CIC Infection Prevention/Patient Safety Specialist, GHA
Amy Christie, MD Clinical LeadMedical Center, Navicent Health
Leslie Culpepper, RN Clinical LeadMedical Center, Navicent Health
Will Miles SCCM MD LeadCarolinas Healthcare Charlotte
Diane Byrum SCCM RN LeadSociety of Critical Care
Medicine

Georgia Hospitals
Athens Regional Hospital DeKalb Medical at Hillandale DeKalb Medical at North Decatur Emory Johns Creek Hospital Emory Saint Joseph’s of Atlanta Emory University Hospital Emory University Hospital Midtown Hamilton Medical Center Medical Center, Navicent Health Rockdale Medical Center St. Mary’s Health Care System

17 States

272 Hospitals/392 ICU’s
Arkansas 11Arizona 23Florida 44Illinois 16Kansas 18Kentucky 24Colorado 12Minnesota 15New Jersey 45Oklahoma 15Tennessee 40Texas 13California 2Georgia
35North Carolina 31South Carolina 21Virginia
27392

Introducing the No Preventable Harms Campaign: Creating the safest healthcare system in the world. Starting with catheter-associated urinary tract infection preventionSanjay Saint, et American Journal of Infection Control 43(2015) 254-9

Opportunity for improvementOpportunity for Improvement
• Consider local policies and procedures
• Allow the initiative to be individualized according to site/unit
• One initiative at a time/provide time between initiatives
• Make sure all stakeholders are involved in initial conversation and have input
• Be clear about who should be involved at the local level (e.g., champions and a project manager). Involve all affected staff

State of the CollaborativeState of the Collaborative
Dr. Will Miles

Dr. Amy Christie &
Leslie Culpepper, RN
Georgia Physician and RN Lead
Medical Center, Navicent Health
New Evidence in CAUTINew Evidence in CAUTIPrevention StrategiesPrevention Strategies
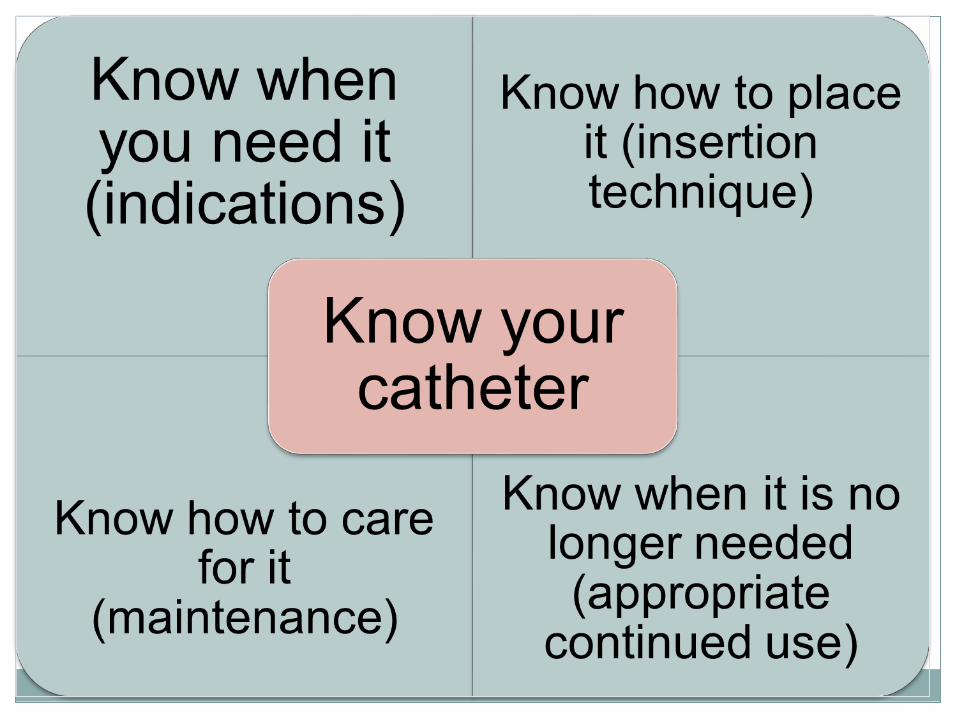

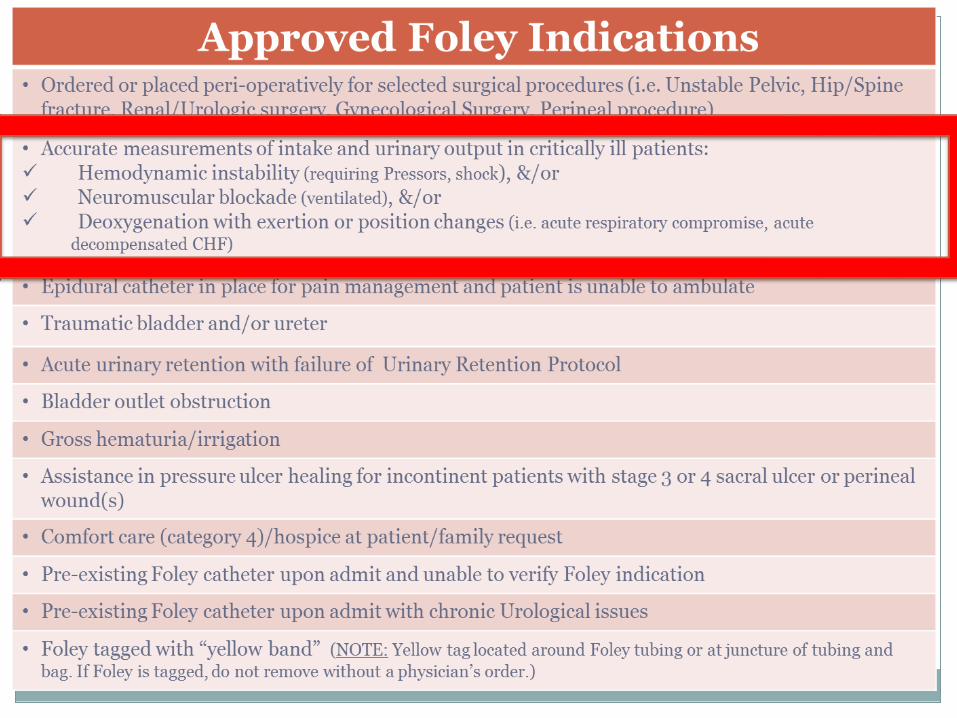
Indications for Placement
• ANA introduced CAUTI Tool in February 2015
• Incorporates CDC best practices
• One page guideline to assess the appropriateness of urinary catheter insertions
• 14 Hospitals participated to test and refine the CAUTI reduction tool and reported positive results



Indications for Placement

Proper Insertion/Alternatives

2-Person Insertion Ideal!
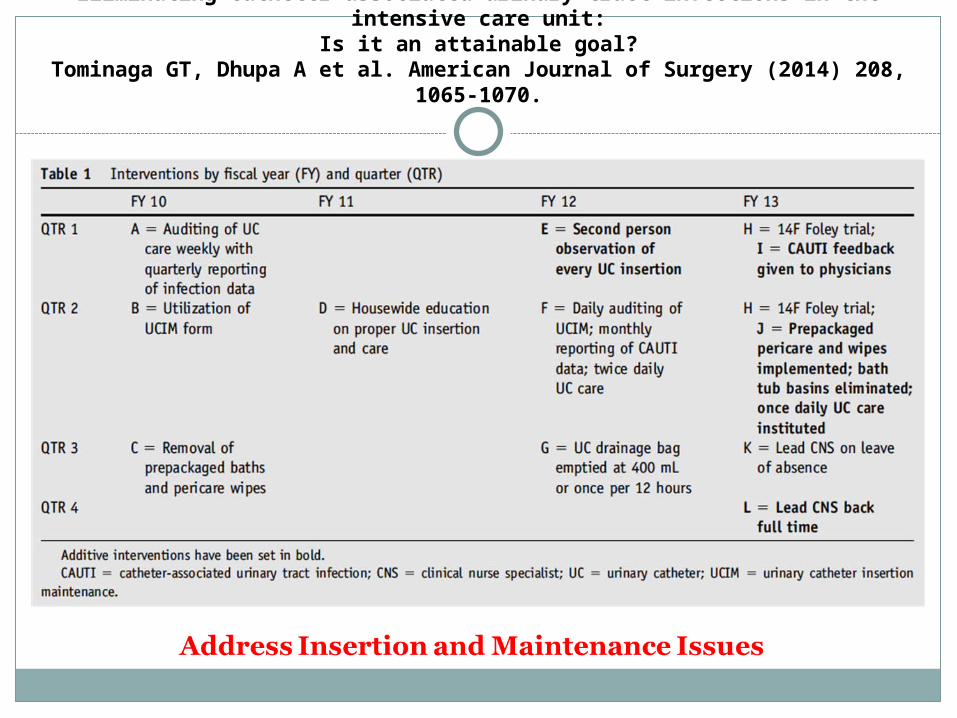
Eliminating catheter-associated urinary tract infections in the intensive care unit:Is it an attainable goal?
Tominaga GT, Dhupa A et al. American Journal of Surgery (2014) 208, 1065-1070.

2 person UC placement, physician notification of CAUTI, reinstitution of pre-packaged bath/peri-care, and implementation of once daily UC care decreased
IR

Appraising the Literature on Bathing Practices and Catheter-Associated Urinary Tract Infections
Urologic Nursing 2015, 35: 11-17. Purpose to evaluate the bathing and cleansing procedures and the
impact of those practices on CAUTI prevention
Meta-analysis: 22 articles included in evaluation
Bath basins increase risk of HAI
Chlorhexidine wipes: CHG no significant difference when compared to sterile water in peri-urethral cleansing prior to catheter insertions
No significant difference in CAUTI reduction when use CHG wipes for cleaning
Plain wipe bathing: Studies have shown a significant reduction in CAUTI
Know When Urinary Catheter is No Longer Needed
Multidisciplinary team education: Finding your champions
I-ACT Training to reduce HAI
Nurse Driven Catheter removal protocol
Identifying and getting buy-in from stakeholders

Interdisciplinary Academy for Coaching and Teaching: Supports the idea of having a hospital based boot camp
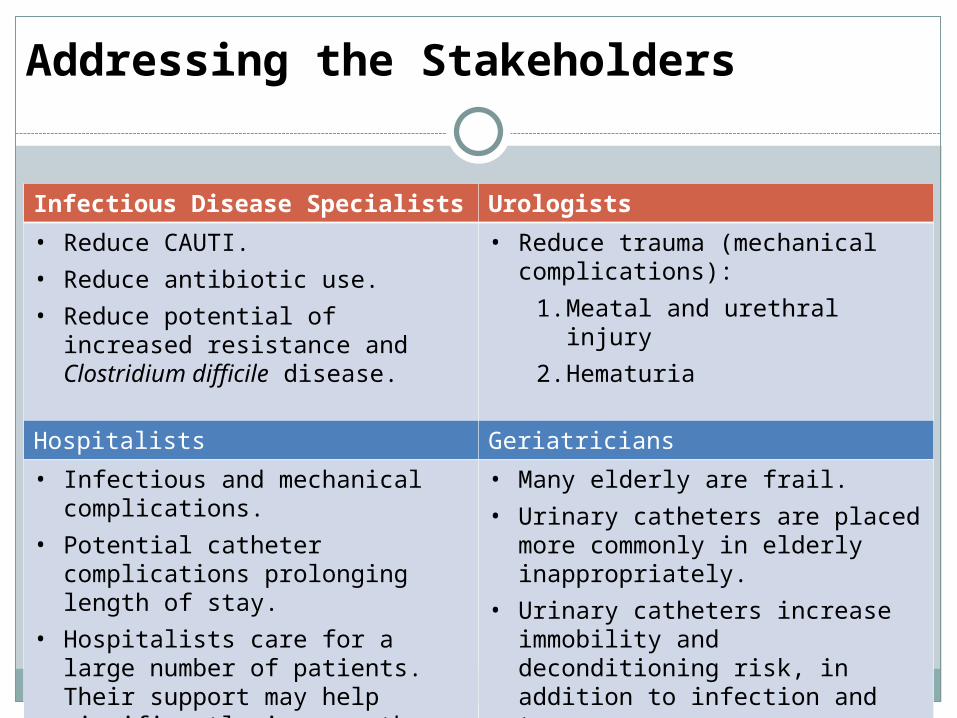
Addressing the Stakeholders
Infectious Disease Specialists Urologists• Reduce CAUTI.• Reduce antibiotic use.• Reduce potential of increased resistance
and Clostridium difficile disease.
• Reduce trauma (mechanical complications):
1. Meatal and urethral injury
2. Hematuria
Hospitalists Geriatricians• Infectious and mechanical complications.• Potential catheter complications
prolonging length of stay.• Hospitalists care for a large number of
patients. Their support may help significantly improve the appropriate use of the urinary catheter.
• Many elderly are frail.• Urinary catheters are placed more
commonly in elderly inappropriately. • Urinary catheters increase immobility
and deconditioning risk, in addition to infection and trauma.
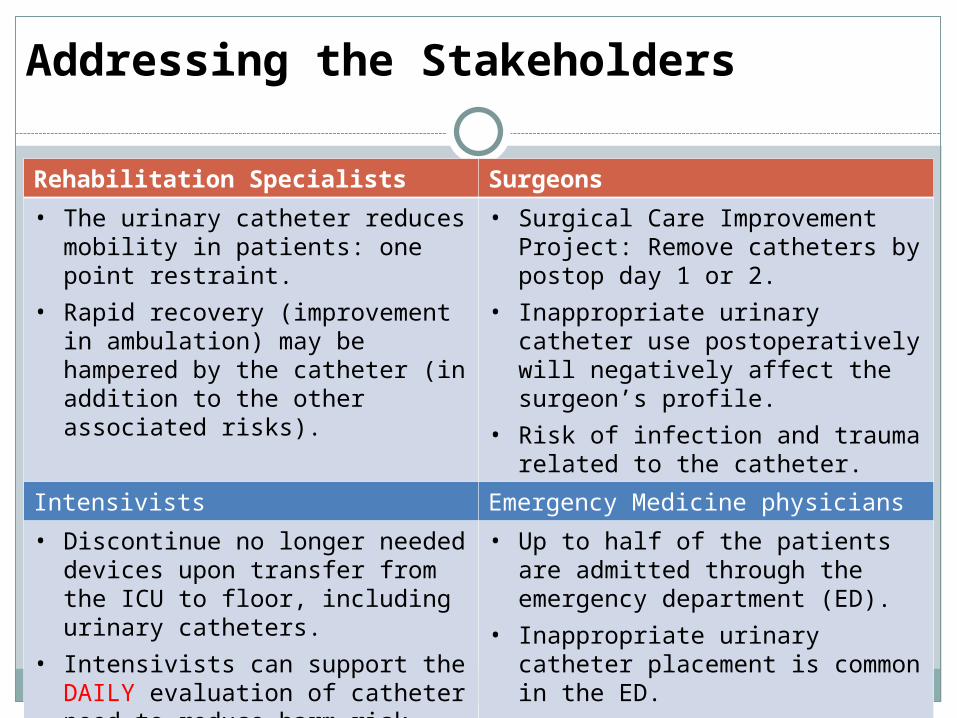
Addressing the Stakeholders
Rehabilitation Specialists Surgeons• The urinary catheter reduces mobility in
patients: one point restraint.• Rapid recovery (improvement in
ambulation) may be hampered by the catheter (in addition to the other associated risks).
• Surgical Care Improvement Project: Remove catheters by postop day 1 or 2.
• Inappropriate urinary catheter use postoperatively will negatively affect the surgeon’s profile.
• Risk of infection and trauma related to the catheter.
Intensivists Emergency Medicine physicians• Discontinue no longer needed devices
upon transfer from the ICU to floor, including urinary catheters.
• Intensivists can support the DAILY evaluation of catheter need to reduce harm risk.
• EARLY MOBILITY?
• Up to half of the patients are admitted through the emergency department (ED).
• Inappropriate urinary catheter placement is common in the ED.
• Promoting appropriate placement of urinary catheters in the ED will reduce inappropriate use hospital-wide.
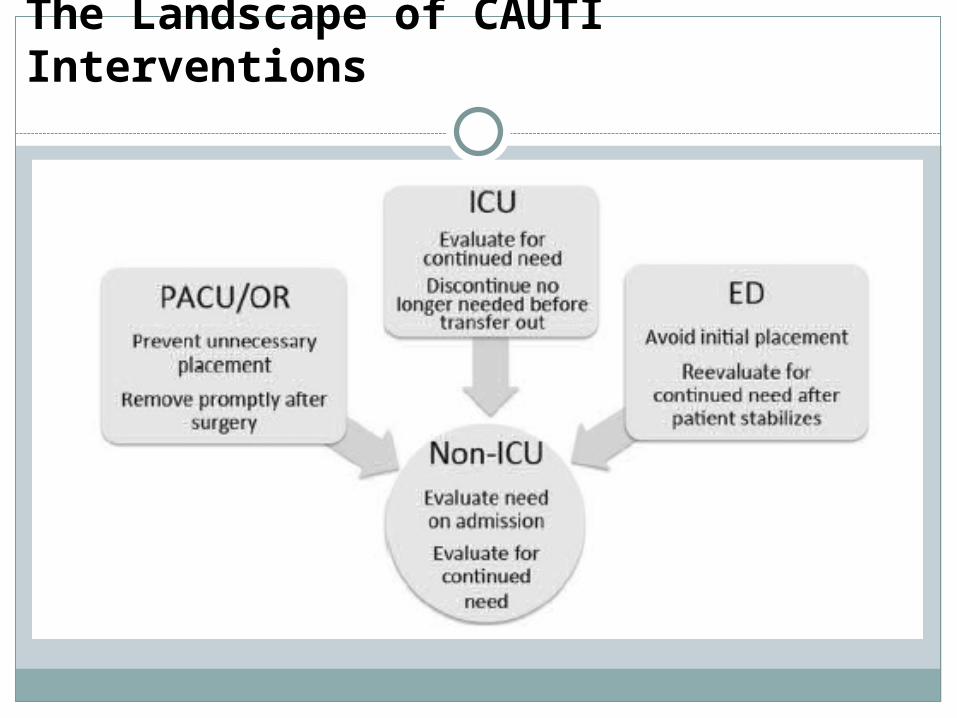
The Landscape of CAUTI Interventions


Introducing the No Preventable Harms Campaign: Creating the safest healthcare system in the world. Starting with catheter-associated urinary tract infection preventionSanjay Saint et al. American Journal of Infection Control 43(2015) 254-9.

Pad Weighing for Reduction of Indwelling Urinary Use and Catheter-Associated Urinary Tract Infection. Beuscher JWOCN 2014, 41: 604-608.
Key for any Catheter Removal Protocol is to offer alternatives to monitor urinary output
Bladder Scanner
In a 7 month period saw a significant reduction in catheter utilization and CAUTI rates

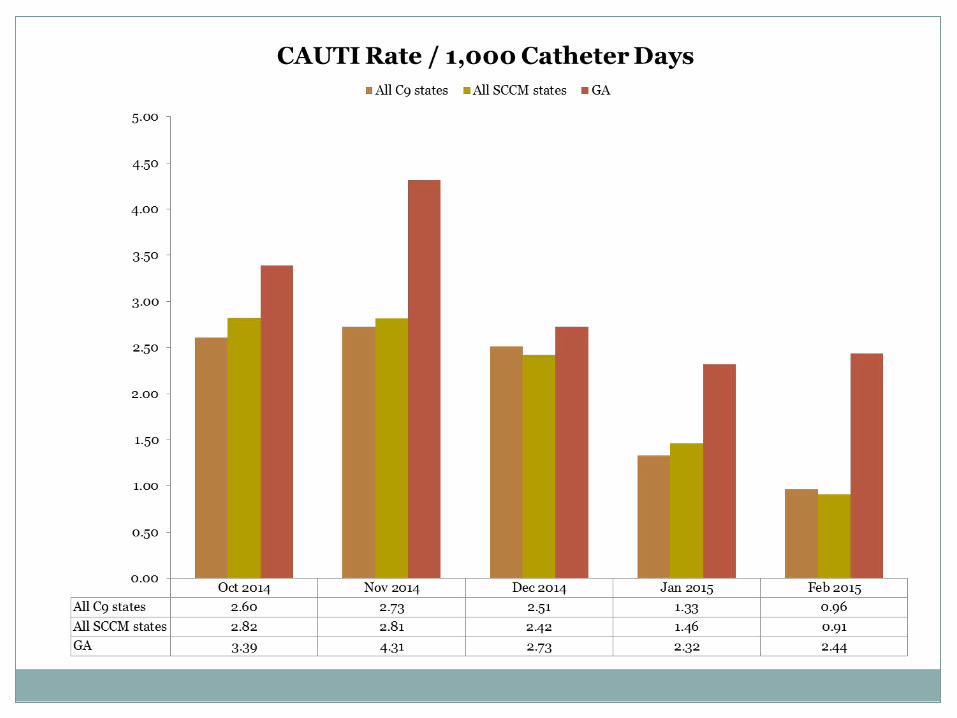
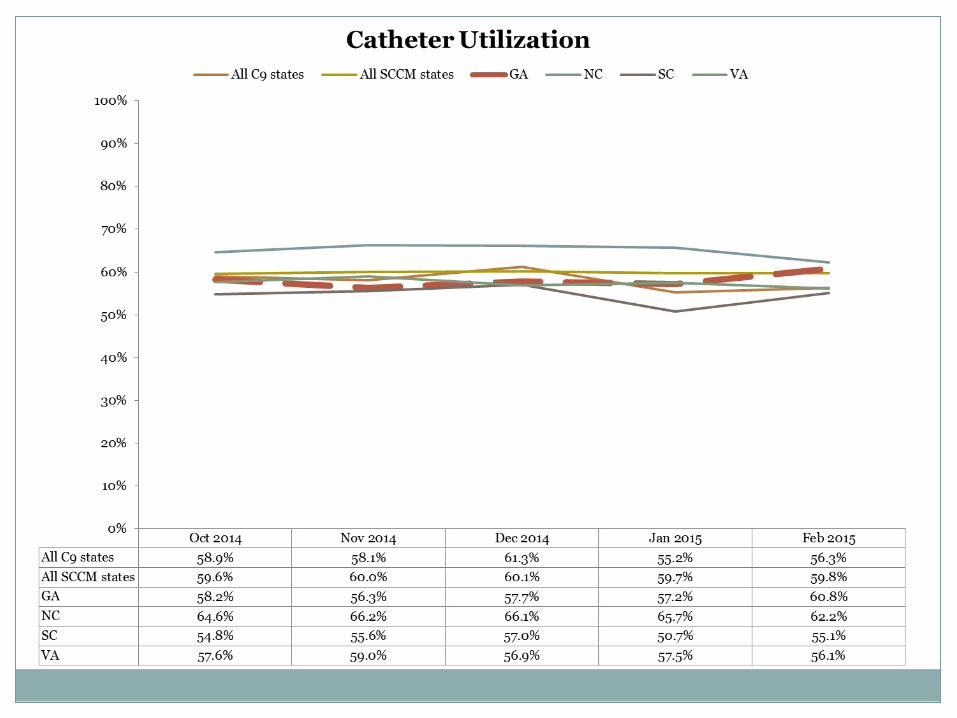
CAUTI QI Project Results
Indwelling Catheter Indwelling Catheter Utilization RateUtilization Rate
CAUTI/1000 catheter CAUTI/1000 catheter daysdays

Interventions are very important along every aspect of catheter lifecycle

Data ReviewData ReviewCAUTI On the CUSP Cohort 9CAUTI On the CUSP Cohort 9
Jan Ratterree RN, BSN, CICInfection Control/Patient Safety Specialist
Georgia Hospital Association







Discussion
What’s working well and what’s getting in our Way?
•Physicians
•Nurses
•Data managers & Improvement professionals
Report Out

Lunch & Culture of Safety Video

Storyboard Rounds – Hospital Teams
Storyboard Rounds
Discuss KEY Lessons and RESULTS Among Teams!

“Take Aways”
Team Lessons from Storyboards!(Facilitators and hospital teams take notes) Highlight key pearls
from Storyboards to support improvement!

Questions of the Day!

Next Steps
Team Planning and Action Plan
Team Huddle and Completion of a WHO, WHAT, and WHEN Plan

Team Report Out
Next Steps Teams will take when they return.
What do sites need to be successful?

Highlights from Culture of Safety Video Highlights from Culture of Safety Video CUSP ToolsCUSP Tools
Diane Byrum, RN





























