-
8/18/2019 Good Man 1997
1/7
J. Child Psychol. Psychiat. Vol, 38. No, 5, pp.
581-586,Cambridge University P
© 1997 Association for Child Psychology and PsycPrinted in Great
Britain, All rights rese
0021-9630/97 $15.00 +
The Strengths and Difficulties Questionnaire: A Research
Note
Robert GoodmanInstitute of Psychiatry, London, U.K.
A novel behavioural screening questionnaire, the Strengths and
Difficulties Questionnaire(SDQ), was administered along with Rutter
questionnaires to parents and teachers of 403children drawn from
dental and psychiatric clinics. Scores derived from the SDQ and
Rutterquestionnaires were highly correlated; parent-teacher
correlations for the two sets ofmeasures were comparable or
favoured the SDQ. The two sets of measures did not differ intheir
ability to discriminate between psychiatric and dental clinic
attenders. Thesepreliminary findings suggest that the SDQ functions
as well as the Rutter questionnaireswhile offering the following ad
dition al a dva nta ges: a focus on streng ths as well as
difficulties;better coverage of inattention , peer relationships,
and prosocial behaviour; a shorter format;and a single form
suitable for both parents and teachers, perhaps thereby
increasing
parent-teacher correlations.
Keywords: Questionnaire, child behaviour, psychopathology,
strengths.
Abbreviations: CBCL: Child Behavior Checklist; ROC: Receiver
Operating Characteristic;S D Q : Strengths and Difficulties
Questionnaire.
In t roduct ion
This paper describes a brief behavioural screeningquestionnaire
that provides balanced coverage of childrenand young people's
behaviours, emotions, and relation-ships. The value of this novel
Strengths and DifficultiesQuestionnaire (SD Q) is evaluated against
the benchm arkset by the Rutter parent and teacher questionnaires.
TheSDQ has been designed to meet the needs of
researchers,clinicians, and educationalists.
The Rutter questionnaires are long-established andhighly
respected behavioural screening questionnairesthat have proved
valid and reliable in many contexts(Elander & Rutter, 1996).
Though substantially shorterand therefore quicker to complete than
the Child
Behavior Checklist (CBCL; Achenbach, 1991a), theRutter parent
questionnaire seem no less useful for manypurposes (Berg, Lucas,
& McGuire, 1992; Elander &Rutter, 1995; Fom bonn e, 1989).
Developed three decadesago, the Rutter questionnaires have
generally worn well,though they do show their age in some ways.
Thus allitems are about undesirable traits whereas the recenttrend,
particularly in education, has been to emphasisechildren's
strengths and no t just their deficits. In addition,the range of
behavioural items covered by the Rutterquestionnaires is now
somewhat dated. Thus nail-bitingand thumb-sucking are included
whereas many areasof contemporary interest—including
concentration,
Requests for reprints or sample questi^pnnaires (available
impulsivity-reflectiveness, having friends, being timised, and
acting prosocially—are poorly cov
Finally, whereas one version of the Achenbach qtionnaire is
designed for completion by young pethemselves (Achenbach, 1991b),
there is no equivRutter questionnaire for self-completion.
A previous research note (Goodman, 1994) descan expanded Rutter
parent questionnaire that inporated all of the original Rutter
items as well as additional items, mostly on children's strengths.
inclusion of these additional items did not appeaattenuate the
valuable properties of the original Rquestionnaire as a behaviour
screening instrumthough the extra items presumably did make
questionnaire somewhat more time-consuming to plete. Factor
analyses suggested that among chiof normal intelligence the
expanded questionnairetapping five distinct dimensions; conduct
problemotional symptoms, hyperactivity, peer problemsprosocial
behaviour.
Using these findings as a guide, the SDQ was desto meet the
following specifications; it should fit easone side of pap er; it
should be applicable to childrenyoung people ranging from 4 to 16
years; the version should be completed by parents and teachesimilar
version should be available for self-report;strengths and
difficulties should be well represented
there should be equal num bers of items on each orelevant
dimensions, namely conduct problems, emoal symptoms, hyperactivity,
peer relationships, and
i l b h i Thi i f
-
8/18/2019 Good Man 1997
2/7
S2 R. G OO D M AN
Materials and MethodsamplingQuestionnaires were obtained on 403
children aged 4-16
ears attending one of two London child psychiatric clinics orhe
children's department of a London dental hospital. Thearents of
children attending these clinics were recruited into
he study until a planned total of roughly 150-250 children
hadeen attained for both dental and psychiatric samples. In
theental clinic and one of the psychiatric clinics (Clinic A),aren
ts who had given informed consent were asked to completewo
behavioural screening questionnaires while awaiting theirlinic
appointment. Participating parents were subsequentlysked for
permission for their child's teacher to be approachedn a similar
basis. The other psychiatric clinic (Clinic B)outinely used
questionnaires prior to the first assessment,ending them to all
paren ts and, when permission was obtaine d,o teachers as well. In
this clinic, parents were routinely sentoth behavioural screening
questionnaires and asked if they
would be willing for their answers (and the teacher's answers)
toe used not only for clinical purposes but also for research.
Some of the parents from Clinic B did not completeuestionnaires
themselves but did give permission for teacheruestionnaires to be
used for research. The proportion ofefusals was not systematically
recorded since, as explainedater, the statistical analyses did not
require the samples to beepresentative.
MethodsRespondents were administered a Rutter questionnaire and
a
Strengths and Difficulties Questionnaire (SDQ) in
randomisedrder. Parents were given the Rutter A(2) Questionnaire
andeachers the Rutte r B(2) Que stionna ire; both were scored in
thetandard way to generate scores for total deviance, conduct
problems, emotional symptoms, and hyperactivity (Rutter,1967;
Rutter, Tizard, & Whitmore, 1970; Schachar, Rutter, &Smith,
1981).
The informant-rated version ofthe SDQ was administered toboth
parents and teachers. This version of the SDQ iseproduced in full
in Appendix A for information only. The
SDQ asks about 25 attributes, 10 of which would generally behoug
ht of as strengths, 14 of which would generally be thou ght
of as difficulties, and on e of wh ich— gets on better with ad
ultshan with other children —is neutral. Though no SDQ item
isdentically worded to any Rutter item, five items are
similarly
worded. The initial choice of items was guided by the factor
oadings and frequency distributions that had previously
beenobtained on an expanded Rutter parent questionnaire (Good-man,
1994); items were subsequently modified and amalga-mated on the
basis of a succession of informal trials as well asadvice from
colleagues. The 25 SDQ items are divided between5 scales of 5 items
each, as shown below.
Hyperactivity Scale. Restless, overa ctive, can not stay stillor
long ; Con stantly fidgeting or squirm ing ; Easily
distracted, concentration wanders ; '•'Thinks things out
beforeacting '; an d Sees tasks through to the end, good
attentionpan''.
Emotional Symptoms Scale. Ofte n com plains of head-aches,
stomach -ache or sick nes s ; M an y worries, often seemswo rried ;
Often unhapp y, down-hearted or tearful ;
Nervous or clingy in new situations, easily loses confidence
;and M an y fears, easily sca red .
Conduct Problems Scale. Often has temper tantrums or
Peer Problems Scale. Ra the r solitary, tends to pa lone ; 'Has
at least one good friend ; ''Generally liked bother children ; Pick
ed on or bullied by other ch ild ren ; Gets on better with adults
than with other children .
Prosocial Scale. Considerate of other people's feelin Sh ares
readily with other children (treats, toys, pencils, e Helpful if
someone is hurt, upset or feeling ill ; Kiyounger childre n ; and
Often volunteers to help
(parents, teachers, other children) .Each item can be marked no
t tr ue , som ewha t tru certainly true . For all of the items
except the five pabov e in italics, the item is scored 0 for n ot
tr ue , somewhat tru e , and 2 for certain ly tru e . Fo r the
fiveprinted abo ve in italics, the item is scored 2 for not true 1
f somewh at tru e , and 0 for certainly true . The scoeach of the
five scales is generate d by sum ming t he scores five items that m
ake u p that scale, thereby generating ascore rangin g from 0 to
10. The scores for hypera cemotional symptoms, conduct problems,
and peer procan be summed to generate a total difficulties score
rfrom 0 to 40; the prosocial score is not incorporated reverse
direction in to the to tal difficulties score since the aof
prosocial behaviours is conceptually different fropresence of
psychological difficulties.
The Rutter A(2) and the SDQ were both completed parents of 346
children: 158 dental clinic attenders anpsychiatric clinic
attenders. The R utter B(2) and the SDQboth completed by the
teachers of 185 children: 39 dentaattenders and 146 psychiatric
clinic attenders. Most teacher reports were on psychiatric clinic
attende rs becauparents of children attending Child Psychiatric
Cligenerally agreed to the clinic sending questionnaires to tfor
clinical as well as research purposes; parents of chattending the
dental clinic or Child Psychiatric Clinic Aless likely to give
permission for teacher questionnaires
obtained solely for research purposes.
Statistical AnalysisAs in previous studies comparing the
validity of di
screening questionnaires (e.g. Berg et al, 1992), analyReceiver
Operating Characteristic (ROC) curves were uestablish how well each
questionnaire was able to distbetween high- and low-risk samples,
determining the areathe curve for each questionnaire (Hanley &
M cNeil, 198this purpose, the only underlying assumption is that
crecruited from the two psychiatric clinics were substamore likely
to have psychiatric disorders than children refrom the dental
clinic. There is no assumption that all srecruited from the
psychiatric clinics had psychiatric dinor that all subjects
recruited from the dental clinic wefrom psychiatric disorder.
Equally, there is no assum ptithe psychiatric samp le was
representative of all children b4 and 16 who attend psychiatric
clinics, nor that thesample was representative of all children
attending clinics, let alone of all children aged between 4 an d
16. SROC curves for the SDQ and Rutter questionnairederived from
the same set of patients, the statistical comof the areas under
these ROC curves allowed for thenatu re ofthe d ata (Hanley &
McN eil, 1982). Com parisoparent-teacher correlations of the SDQ
and questionnaires also allowed for the paired nature of thusing
structural equation modelling (EQS, BMDP StaSoftware) and examining
whether constraining the twolations to be the same resulted in a
significantly poo
-
8/18/2019 Good Man 1997
3/7
S T R E N G T H S A N D D I F F I C U LT I E S Q U E S T I O N N
A I R E 58
could securely be generalised to representative
epidemiologicalor clinical samples; such estimates will
subsequently be derivedfrom other studies in progress.
Reported correlations are Pearson product-moment corre-lations,
but the pattern of findings was not changed whenSpearman
correlations were used instead. Intraclasscorrelations—which are
often appro priate for reliabilityestimates—were not used to
measure parent-teacher agreementeven though this agreement could be
construed as an index ofinter-rater reliability. Parents and
teachers make ratings basedon different sources of information,
whereas measures of inter-rater reliability are more appropriately
derived from inde-pendent ratings based on the same source of
information.Furthermore, employing intraclass correlations would
haveinvolved mixing parent- and teacher-derived scores, and
thiswould have been inappropriate since mean scores
differedsystematically between parent and teacher ratings—a
differenceallowed for when interpreting these scores (Rutter, 1967;
Rutteret al., 1970; and see Appendix B).
ResultsAge and Gender
The mean age {SD) ofthe dental sample was 10.8 years(3.1) while
that ofthe psychiatric sample was 9.8 years(3.3), a significant
difference [t (401) = 3 .00, /? < .01]. Asexpected, the propor t
ion of males was higher in thepsychiatric sample (63%, 153/244)
than in the dentalsample (5 3% , 85/159) [cont inu i ty-adjus ted/
(1) = 3.03,p < .05, 1-tailed]. The results reported here are for
th esample as a whole, tho ug h closely similar results wereobta
ined when ROC and corre lational analyses w ererepeated separately
for boys and girls, and separately forchildren aged 4-10 and
11-16.
Sensitivity
0 8
0 6
0.4
0.2
0 0 2 0 4 0 6 0 8
1 1
0.8
0.6
0.4
0 2
Sensitivity
°
I D
1
_:_^ : - . ; - —
ŜDQ
° Rutter
0 0 2 0 . 8.4 0.61-Specif ic i ty
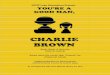
Pigure 2. RO C curves for teacher-rated questionnair
Discriminating between Psychiatric andNonpsychiatric Samples
The ability of the two questionnaires to distinguibetween dental
and psychiatric cases is reflected in thReceiver Operating
Characteristic (ROC) curves sin Figs. 1 and 2 for parent and
teacher reports respectively. The R OC curves for the Rutter
questionare based on total de viance scores, whereas the curves are
based on tota l difficulties score s. The cparable ability of the
two measures to discriminbetween the two samples is evident from
the extent towhich the two curves almost superimpose on one anQua
ntitatively, this comparability can be judged froarea un der each o
fth e curves, which is a measure owell that m easure discriminates
between the two samthe area under the curve would be 1.0 for a
measur
discriminated perfectly, and .5 for a measure that dcriminated
with no better tha n chance accuracy. Forpare nt re ports, the area
un der the curve (95 % confiinterval) was .87 (.83-.91) for the SDQ
as compared.87 (.83-.91) for the R utter A(2) parent
questionnainonsignificant difference (z = .13, = .9). Fo r
teachreports, the corresponding values were .85 (.78-.93the SDQ as
compared with .84 (.76-.93) for the RB(2) teacher question naire— a
nonsignificant diffe(2 = .41 , ; ; = .7).
SDQ-Rutter CorrelationsTable 1 shows the correlations between SD
Q and
R Th l i l
-
8/18/2019 Good Man 1997
4/7
4 R. GOODMAN
Table 1Inter-measure Correlation for Each Type of Rater
Total Deviance/Difficulties scoreConduct Problems scoreEmotional
Symptoms scoreHyperactivity score
SDQ-Rut te r
Parent report
.88
.88
.78
.82
correlation
Teacher reportA^= 185
.92
.91
.87
.90
ble 2er-rater Correlations for Each Type of Measure
tal Deviance/Difficulties scoreonduct Problems scoremotional
Symptoms scoreyperactivity scoreer Problems scoreosocial Behaviour
score
Parent-Teachercorrelation(N =
SDQ.62*.65.41.54.59.37
= 128)
Rutter.52.57.47.55——
* Correlation significantly higher than the com parabletter
correlation (p < .02); all othe r comp arisons non-nificant.
ions can be presented on two SDQ scores—the peeroblems score and
the prosocial behaviou r score—sinceey have no Rutter
counterpart.
rent-Teacher Correlations
Table 2 presents the correlation coefficients betweenacher- and
parent-derived scores when both are usinge SDQ or when both are
using Rutter questionnaires.r comparable scores, the
cross-situation correlations
the SDQ and Rutter measures were generally similar,art from the
higher SDQ correlation for total score ̂ (1) = 5.90, p < .02].
Thou gh the co rrelations were
wer when the analyses were repeated for the dental andychiatric
samples separately, these correlations werenerally comparable for
the SDQ and Rutter measures,art from a higher SDQ co rrelation for
total score in theychiatric sample [x ̂ (1) = 4.05, p <
.05).
Discussion
Given the well-established validity and reliability ofth etter
questionna ires (Elander & Rutte r, 1996), the highrrelation
between the total scores generated by the
used identical items for parents and teachers whereRutter
questionnaires were somewhat differenparents and teachers. The ROC
analyses showed thtwo measures had equivalent predictive
validitjudged by their ability to distinguish between psycand
nonpsychiatric samples. Of course, discrimibetween psychiatric and
dental clinic attendersrelatively easy task, but the high
correlation beSDQ and Rutter scores within each clinic group suthat
the two measures are also likely to be compdiscriminating in more
demanding screening tasksas detecting nonreferred cases of child
mental problems in the community; further empirical swould be
needed to confirm this. Since previous shave shown that CBCL and
Rutter parent questioscores are highly correlated (Berg et al.,
1992; Fom bon1989), and that these two sets of questionnaires
acomparable predictive vahdity (Berg et al., 1992)likely that the
SDQ and CBCL will also be hcorrelated and have comparable validity;
directparisons are currently under way.
The SDQ and Rutter questionnaires can each beto generate
separate scores for conduct probemotional symptoms, and
hyperactivity. For eathese three scores, there was a high
correlation bethe SDQ score and the Rutter score; and
parent-tecorrelations were comparable for the two semeasures.
Despite its brevity, the SDQ also gentwo scores that have no Rutter
counterparts; aproblems score and a prosocial behaviour score.
The performance of the SDQ could potentiallybeen undermined by
three of its design features; incof strengths as well as
difficulties; use of an idequestionnaire for both parents and
teachers; acompact presentation on just one side of
paperequivalence of the SDQ and Rutter scores suggesthese three
features have not had an adverse effectshould encourage researchers
and clinicians whcontemplating incorporating similar features
intoquestionnaires.
Rutter questionnaires are routinely used to catechildren as
likely psychiatric ca se s or no n- caccording to whether their to
tal deviance score is eqor greater than a standard cut-off; 13 on
the Ruparent questionnaire and 9 on the Rutter teachertionnaire
(Rutter, 1967; Rutter et al., 1970). Us
-
8/18/2019 Good Man 1997
5/7
STRENGTHS AND DIFEICULTIES QUESTIONNAIRE 8
ifferent studies simply because those studies havemployed the
same cut-off. Comparability is particularlyikely to be lost when
high- and low-risk samples areontrasted. A worked example may be
helpful. Study Xnvolves 100 children from a high-risk population
with arue rate of psychiatric disorder of 50 %; if the
screening
questionnaire has a sensitivity of 8 and a specificity of .8when
using the standard cut-off, the questionnaire willdentify 40 true
positives and 10 false positives. Study Ynvolves 100 children from
a low-risk population with arue rate of disorder of 10%; even with
the sameensitivity and specificity, the questionnaire will identify
8rue positives and 18 false positives. Despite using the
same questionnaire and the same cut-off, a comparison ofcases
from studies X and Y will primarily be a
comparison of true positives from study X with falsepositives
from study Y.
Given these problems, the best strategy for researchersmay be to
choose cut-offs according to the likely disorderrate in the sample
being studied, and according to the
relative importance for that study of false positives andfalse
negatives. It may also be appropriate to adjust cut-offs for age
and gender. Ongoing clinical and epidemio-logical studies using the
SDQ should provide the basis forcut-offs adjusted for these sample
characteristics. Inaddition, planned trials should establish if the
predictivevalidity of the SDQ can further be improved by
analgorithm that combines SDQ scores with scores from anadditional
and even briefer screening instrument thatelicits the respondent's
view on whether the child hassignificant emotional or behavioural
difficulties, and onthe extent to which these difficulties result
in socialimpairment or distress for the child, or burden for
others.Until these various studies are completed, SDQ users canuse
the provisional cut-off scores shown in Appendix B,which are
derived partly from the samples used for thisstudy and partly from
other ongoing epidemiologicalsurveys using the SDQ . The bo rde
rlin e cut-offs can beused for studies of high-risk samples where
false positivesare not a major conc ern; the ab no rm al cut-offs
can beused for studies of low-risk samples where it is
moreimportant to reduce the rate of false positives.
ConclusionThese initial findings suggest that the SDQ may
function as well as the Rutter questionnaires (and, byinference,
the Achenbach questionnaires) while offering
the following additional advantages: a compact foa focus on
strengths as well as difficulties; better covof inattention, peer
relationships, and prosocial biour ; and a single form suitable for
both parents teachers, perhaps thereby increasing
parent-tecorrelations.
Acknowledgements —I am very grateful for the willin
operation of parents and teachers, and for the invaassistance of
E)r. Hilary Richards and the staff of theLondon clinics that
participated in the study: the Depaof Paediatric Dentistry of
King's Dental Institute, CambChild Guidance Centre, and the
Department of ChilAdolescent Psychiatry, Hounslow.
References
Achen bach, T. M. (1991a). M anual for the Child BehavChecklist
14-18 and 99 Profile. Burlington, VT : U niveof Vermont Department
of Psychiatry.
Achenbach, T. M. (1991b). Manua l for the Youth Self-Reand 1991
Profile. Burlington, vf : University of Ver
Department of Psychiatry.Berg, I., Lucas, C , & McGu ire, R.
(1992). Measurembehaviour difficulties in children using standard
administered to mothers by computer: Reliability aidity. European
Child and Adolescent Psychiatry, 1, 14-2
Elande r, J., & Rutter, M. (1996). Use and developmenRutter
Parents' and Teachers' Scales. International JournalMethods in
Psychiatric Research, 6, 63-78.
Fombonne, E. (1989). The Child Behavior Checklist Rutter
Parental Questionnaire: A comparison betwescreening instruments.
Psychological Medicine, 19, 111-
Goodman, R. (1994). A modified version ofthe Rutterquestionnaire
including items on children's strengresearch note. Journal of Child
Psychology and Psychi35, 1483-1494.
Hanley, J. A., & M cNeil, B. J. (1982). The meaning anthe
area under a receiver operating characteristic curve. Radiology,
143, 29-36.
Hanley, J. A., & McN eil, B. J. (1983). A method of comthe
areas under receiver operating characteristic derived from the same
cases. Radiology, 148, 839-843.
Rutter, M. (1967). A children's behaviour questionncompletion by
teachers: Preliminary findings. JournalChild Psychology and
Psvehiatry, 8, 1-11.
Rutter, M., Tizard. J., & Whitmore, K. (1970). Educathealth
and behaviour. London: Longman.
Schachar, R., Rutter, M., & Smith, A. (1981). The
teristics of situationally and pervasively hyperactive
cImplications for syndrome definition. Journal of Child chology and
Psychiatry, 22, 375-392.
Accepted manuscript received 26 Septembe
-
8/18/2019 Good Man 1997
6/7
86 R. GOODMAN
Appendix A: Strengths and Difficulties Questionnaire
r each item, please mark the box for Not True, Somewhat True or
Certainly True. It would help us if you answered all items asst you
ean even if you are not absolutely certain or the item seems daftl
Please give your answers on the basis of the child'shaviour over
the last six months or this school year.
hilds Name
te of Birth.
gnature
Considerate of other people's feelingsRestless, overactive.
cannot stay still for longOften complains of headaches,
stomach-aches or sicknessShares readily with other children
(treats, toys, pencils etc)Often has temper tantrums or hot
tempersRather solitary, tends to play aloneGenerally obedient,
usually does what adults requestMany worries, often seems
worriedHelpful if someone is hurt, upset or feeling illConstantly
fidgeting or squirmingHas at least one good friendOften fights with
other children or bullies themOften unhappy, down-hearted or
tearfulGenerally liked by other childrenEasily distracted,
concentration wandersNervous or clingy in new situations, easily
loses confidenceKind to younger childrenOften lies or cheatsPicked
on or bullied by other childrenOften volunteers to help others
(parents, teachers, other children)Thinks things out before
actingSteals from home, school or elsewhereGets on better with
adults than with other childrenMany fears, easily scaredSees tasks
through to the end. good attention span
Date
arent/Teacher/Other (please specify:)Thank you very much or your
help
N otTrue
n
n
n
nn
n
SomewhatTrue
n
n
Male/Fem
CertainlyTrue
n
n
nn
Robert Goodman, 1977
Appendix B: Provisional Banding of SDQ Scores
hese bands, which are not adjusted for age or gender, have been
chosen so that roughly 80 of children in the community arermal, 10
are borderline, and 10 are abnormal.
Parent completedTotal Difficulties ScoreEmotional Symptoms
ScoreConduct Problems ScoreHyperactivity ScorePeer Problems
ScoreProsocial Behaviour Score
Teacher completedTotal Difficulties ScoreEmotional Symptoms
ScoreC d P bl S
Normal Borderline Abnormal
0-130-30-20-50-2
6-10
0-110-4
14^1643635
12-155
17-405-104^107-104-100 - 4
l^-*06-10
-
8/18/2019 Good Man 1997
7/7