Embed Size (px)
Citation preview

Annals of the Rheumatic Diseases, 1987; 46, 787-792
Case report
Gold colitis induced by auranofin treatment ofrheumatoid arthritis: case report and review ofthe literatureH E LANGER, G HARTMANN, G HEINEMANN, AND K RICHTER
From the Department of Internal Medicine, Division of Rheumatology, Hannover Medical School, FRG
SUMMARY A case of ulcerative colitis occurred during treatment of rheumatoid arthritis with thenew oral gold preparation auranofin after a cumulative dose of 2160 mg. A barium enemashowed loss of mucosal pattern and a rectal biopsy disclosed deep erosions, mucosalinflammation, and crypt abscesses. Precipitates of gold were seen in the periglandular stroma. Onelectron microscopy the gold deposits seemed to be identical to granules described in goldnephropathy. As the extrapolated serum gold level was within the normal range at the onset ofthe complication, the morphological findings suggested a local toxicity of the drug. The patientrecovered within 14 days of withdrawal of auranofin and the start of therapy with sulphasalazineand steroids. A review of the published work shows that the previously reported mortality in goldcolitis of 40% has decreased in recent years. The causes of this decrease may be both the earlierdiagnosis of gold colitis and the improved intensive care of its severe complications.
Key words: ulcerative colitis, gold therapy-complications.
Gold salts are effective as slow acting antirheumaticdrugs in rheumatoid arthritis, but treatment must beinterrupted in 14-53% of the patients because ofside effects. 1-3 Drug colitis is known as a rare, butfrequently fatal, complication of gold therapy.4Since its introduction in 19765 the new oral goldcompound auranofin has proved its efficacy inrheumatoid arthritis. 8 Side effects seem to befewer and less severe than those seen with theintramuscular gold preparations.4 Two cases of goldcolitis, however, have been observed during treat-ment with auranofin.9 "() We report a further caseand discuss some aetiological, immunogenetic, andtherapeutic aspects of this complication.
Case report
HISTORYA 47 year old man had suffered from erosiverheumatoid arthritis since 1979. He had also
Accepted for publication 6 May 1987.Correspondence to Dr H E Langer, Abt fur Krankheiten dcrBewegungsorgane und des Stoffwechsels. Medizinische HochschuleHannover, Konstanty-Gutschow-Strassc 8, D 3000, Hannover 61,Federal Republic of Germany.
suffered intermittently from a duodenal ulcer forabout 20 years. Otherwise he was well. In particularhe did not have any indication of inflammatorybowel disease. Treatment of the rheumatoid arth-ritis with chloroquine was stopped after two yearsbecause of inefficacy. Subsequent gold therapy withaurothiopolypeptide was tolerated for two yearswithout complications but then had to be stoppedafter a total dose of 1200 mg because of dermatitisand eosinophilia in the peripheral blood (8%).Treatment was changed to the oral gold preparationauranofin with 3 mg twice daily for nine months, andlater 3 mg three times a day, without side effects. Healso took 300 mg ranitidine twice daily and 100 mgdiclofenac intramuscularly every second day. After11 months and a total dose of 2160 mg auranofin thepatient suddenly developed mucous and bloodydiarrhoea with six to seven stools a day, accom-panied by abdominal pain and tenesmus.
CLINICAL EXAMINATIONExamination showed the typical joint deformities ofrheumatoid arthritis. The abdomen was tender onpalpation in the left lower quadrant. Otherwise nopathological findings were detectable.
787
copyright. on M
ay 4, 2022 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.46.10.787 on 1 O
ctober 1987. Dow
nloaded from

788 Langer, Hartmann, Heinemann, Richter
.Qq5,% '.' "; 4_,_-
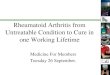
Fig. 2 Dense inflammatory infiltrate throughout thestromal layer ofthe rectal mucous membrane after therapywith auranofin three times a day. So called 'crypt abscesses'and ulcerative lesions as seen in ulcerative colitis.
Fig. 1 Barium enema one week after the onset ofbloody diarrhoea in gold colitis. Loss ofmucosal patternwith irregular gut contours and absent haustration inthe descending and transverse colon.
DIAGNOSTIC FINDINGSLaboratory investigations showed an eosinophilia of9% in the peripheral blood but were otherwisenormal. Rectosigmoidoscopy was performed afterone week and showed intensive reddening andoedema of the mucosa with shallow ulceration andpurulent deposits. A barium enema (Fig. 1) showedabsent haustration in the descending and transversecolon with irregular gut contours. Histology of arectal biopsy specimen showed erosions of themucosa, a dense inflammatory infiltration of thelamina propria with polymorphonuclear neutrophilgranulocytes, eosinophils, lymphocytes, plasmacells, and histiocytes (Fig. 2), and numerous cryptalabscesses (Fig. 3). Staining for gold showed punc-tate black precipitates immediately under the baseof the glands and in the periglandular stroma (Fig.4). Similar changes could not be observed incontrols from five other patients with chronicinflammatory bowel disease. Electron microscopicinvestigation showed a number of phagocytotic cellswithin the mucosal stroma containing numerouslysosomal osmiophilic cytoplasmic structures (Fig.5). Some inclusions were surrounded by a thinmembrane, others lacked membranes and displayed
.. -- . -- ~ . I._P
Fig. 3 Rectal mucous layer after therapy with 3 mgauranofin three times a day. Severe lymphocytic, histiocytic,andpolymorphonuclear leucocyte infiltration.Numerous so called crypt abscesses. Loss ofgoblet cells.Glandular epithelium activated by inflammation.
copyright. on M
ay 4, 2022 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.46.10.787 on 1 O
ctober 1987. Dow
nloaded from

Fig. 4 Rectal mucous layerw 4 ;..in auranofin induced colitis.
, Isolated and complex depositst
# > i z_S ^k *of dark precipitations in
3 macrophages within the*;S*%4?*.^interstitial tissue. Demonstration>t4*61Fie 'F> of gold according to
Borchardt-Michaelis.
an indistinct periphery (Fig. 6). They measuredfrom 10 nm to 32 nm in size and occurred at thebottom of the mucosal layer together with leuco-cytes and other non-specific inflammatory cells.These deposits seemed to be identical to granulesdescribed in gold nephropathy. The cells corres- eponded with those demonstrated histochemically i.(Fig. 4). We presume that these alterations areprecipitations of metallic gold in the colonic mucosa 1-due to the auranofin therapy. Serum gold levelswere measured seven and eight weeks after the x. * 4onset of symptoms and were 135 mg/ml and 130mg/ml respectively. If a half life of two to three tweeks is assumed,6 the serum gold level was withinthe therapeutic range at the onset of the complication.The HLA type was A2, A23, B27, Bw62, Cw2, *Cw3, Dr4. _
HLA-B27 positive tomography of thesacroiliac joints was undertaken and showed normalrJoints. t;
THERAPY ANDCOURSE4*Therapy with auranofin was stopped and treatment .was begun with 1-5 g sulphasalazine four times a day t. vand 50 mg prednisone once daily. All symptomsdisappeared after 14 days. A control rectosigmoid- moscopy was performed after four weeks and showednormal findings. Steroids were reduced slowly andthen withdrawn. In the follow up period of one year ii. " '*the patient showed no evidence of a relapse.
Fig. 5 Macrophagic interstitial cell in the rectDiscussion membrane in gold colitis. Numerous lysosomc
granular structures in the cytoplasma. LocatioIt cannot be proved definitely that the observed as that shown in Fig. 3. Electron microscopy %colitis was due to auranofin, but the absence of out after initialformolfixation and conventionsymptoms of colitis in the past and the rapid technique.
Gold colitis 789
tal mucousal and)n is the samewas carriedzalparaffin
wF'II*,I
. t-I*l
copyright. on M
ay 4, 2022 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.46.10.787 on 1 O
ctober 1987. Dow
nloaded from

790 Langer, Hartmann, Heinemann, Richter
:s.A .-;is ;} 3r w . ih i
.4W, r7.N P,. _,.;X_
-]
b. ts
i *'>zb Zt* M., @,^s__ wv _s a_Ir- >
Fig. 6 Part ofan interstitial macrophage with granulesand Iysosomes partially surrounded by a thin membrane.Compare this with the histochemically demonstrateddeposits in Fig. 3 and the electron photomicrograph inFig. 4. Electron microscopy was carried out after initialformol fixation and conventional paraffin technique.
response after withdrawal of the drug make otherexplanations improbable. Furthermore, the patienthad not taken other drugs known to cause colitis. 13Twenty eight cases of gold induced colitis have beenreported, including two cases due to auranofin"'-35(Tables 1 and 2).The pathogenesis of the complication is unknown.
The normal serum gold level in the patient makesoverdosing of auranofin as the cause of colitisunlikely. It is known that the efficacy and toxicityof gold therapy are not related to serum goldlevels,3638 suggesting that local mechanisms mayplay a part. The histological demonstration ofstainable gold in the colonic mucosa furthersupports the possibility of local toxicity of the dru .Up to 95% of auranofin is excreted in the faeces,-9resulting in a constant contact of the substance withthe colonic mucosa. Diarrhoea frequently occurs inauranofin therapy,41 41 probably caused bya reversible defect in intestinal permeability.2Analogously to mechanisms for gold neph-ritis" r 4 it is suggested that in predisposedindividuals the constant exposure of the colonic
Eo:I0Z
Cz
C) CC
> >>Q > > > > >
c c
_ _
Q-u_
c) C)
Cu
70
2 Q
E
7j) E E E E 1E E E 5 EG
_0ov o t O t S w
C C. ~CuCu,5 C@ : O 0w
c) V0c.< ctUc---- t tctc V
Cu
*_~ O_ c 000c0O E0o Co °..0_0.0.0X0.0X0o0.0
-, S r- m r m z mz ,tz = ) r- kr, r
t k r-.otN^££oo
IM .0X~~~~~~000 OCOCC 0CUCDESnWn=C oCl Q>QY (C
"Jut
io-
W%.V:
copyright. on M
ay 4, 2022 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.46.10.787 on 1 O
ctober 1987. Dow
nloaded from

Gold colitis 791
OOCO50 0~C C O O
M4 0 C4 X e2 C4 w 4 M P! M W P! X
Ct
0n 0
O _
_ =
-J_ ~.0_)*
E E E E C mW =a EC E=
EE lao C o : o0.,,.vXc
n
X
QQQQQ Qc QQ QQ c'0
X "' Et U° 't: 0°=3°._EcEci OXOE :X
_ _6
000 oN oo 000= 0= oo 0 "m0 u m mr- r-£ m " "It
oo o c X o oo ooC000000 00
X
X 3 ,0 .C E °
epithelia to the excreted gold may lead to a changein their antigenicity with formation of antibodiesagainst the mucosa and development of ulcerativecolitis. Unfortunately investigations of immunecomplexes were not performed in the rectal biopsyof our patient.The complication was not associated with
HLA-Dr3, the incidence of which is increased inpatients with adverse reactions to gold, in particularproteinuria.45 7
Diagnosis may be made by rectosigmoidoscopywith rectal biopsy or by barium enema. A review ofthe published work shows that the former methodsseem to be most effective in diagnosing gold colitis.In the reported cases rectal biopsies were per-formed 15 times and led to the diagnosis in allcases, 9 20-24 26-29 32-34 while rectosigmoidoscopyshowed the typical picture of ulcerative colitis inseven9 20) 23 25 26 32 34 and slight alterations infive21 22 27 29 33 of 16 cases. The biopsy specimenswere normal in four patients.24 28 31 Barium enemawas negative in six22-24 28 29 31 and positive in fivepatients.') 20 26
After withdrawal of the drug and introduction ofsulphasalazine and steroids the symptoms dis-appeared within two weeks. Other authors havetried several therapeutic regimens, including steroids,British Antilewisite (BAL), sodium cromoglycate,total parenteral nutrition, and colectomy with mixedresults (Table 1). In our view the treatment ofchoice is sulphasalazine as this drug is also effectivein rheumatoid arthritis. Some patients remittedspontaneously without further therapy after with-drawal of gold. " 25 33 Because of lethal infectiouscomplications due to severe protein losses under thelonglasting diarrhoea with hypogammaglobuli-naemia and an additional steroid therapy21 22steroids should be used cautiously.
Stein and Urowitz23 in a review article on druginduced colitis'3 quote a mortality from. gold colitisof 40%. The analysis of reported cases shows,however, that among 14 patients since 1980 nonehave died of this complication (Table 2). Theimproved prognosis may be a result of earlierdiagnosis and improved supportive therapy, par-ticularly total parenteral nutrition. All patientsreceiving auranofin recovered, though one patientdeveloped toxic megacolon.9 Despite the improvedoutcome in recent years gold colitis should beregarded as a potentially lethal complication.Consequently, diarrhoea during gold therapy shouldalways be taken seriously and early investigation byrectosigmoidoscopy with rectal biopsy should beundertaken in all suspicious cases.We are grateful to Dr P Cullen for help in the correction of themanuscript.
OC._
c
Ic)_
r_ci
11_:cc
..0
E_ouc)cO0X
0
11_
o
.C_)
o0Z
L.
'ON
o
0.
CO4
H.0eu
copyright. on M
ay 4, 2022 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.46.10.787 on 1 O
ctober 1987. Dow
nloaded from

792 Langer, Hartmcann, Heinemann, Richter
References
I The Research Subcomilmittee of the Empirc RheumatisimCouncil. Gold thcraipy in rhcumatoid 'arthritis: rcport of amlulilticcntrc controlled triil. Annii Rheiumii Dio 1960: 19: 95-119.
2 Thc Coopcrating Clinics Committee of the Amiecrican Rhcu-mratism Association. A controlled trial of gold salt therapy inrhcumatoid airthritis. Ariritir Rlieiion 1973: 16: 353-8.
3 Grindulis K A. McConkc B. Outcome of aittcmpts to treatrhcumatoid arthritis with gold. pcnicillanminc. sulphaisalazinc. ordiapsonc. Annii Rlheioni 1)is 1984: 43: 398-401.
4 Gottlicb N L. Gold compounids in the rhcumiaultic discascs. In:Kclcv W N. Harris E D. Ruddy S. Slcdgc C B. cds. TextbookoJ rhiemnatology. Philadelphia: Saundcrs. 1981: 796-814.
5Finkelstcin A E. Walz D T. Batista V. Mizraiji M. Roisman F.Mishcr A. Auranofin-necw oral gold compound tor trcatmcntof rhcumatoid arthritis. Atini Rheutm Dio 1976: 35: 251-7.
6 Bcrgibf F, Bergl6f K. Walz D T. Aurainofin: an oral chrvso-thcraipcutic agcnt for the treatmcnt of rheumiatoid arthritis. JRl/eo,natol 1978: 5: 68-74.
7 Schittcnkirchncr M. Kaik B. Mucllcr-Fassbendcr H. Rau R.Zcidlcr 11. Aurainofin aind sodium aiurothiomalitc in thetrcitment of rhetimltoid arthritis, a double-blind. comparative.multiccntcr study. J Rhetonatol ISuippil 1982: 9: 184-9.
8 Wird J R, Williams 1I J. Eggcr M J et tit. Comparison ofauranofin. gold sodiumii thiomalatc, and plaiccbo in the treat-mcnt of rheumatoid airthritis. Artiritis Rlieioni 1983:, 26: 13)3-15.
9 Jarncr D. Niciscn A M. Auiranofin (SK+F 39162) induccdcntcrocolitis in rhcumiaiitoid airthritis. S'(icnld J Rheinatol 1(93X12: 254-6.
1ff Goebcl K M. Storck U. Kohl F V. llausmann L. KlinischcrEffckt und uncrwtinschtc Arzncimittclwirktingen von Auranofinbci rhcumatoidcr Arthritis. 1oitiere Medizini 1985: 12: 39-45.
11 Silbcrberg D S. Kidd E D. Shmitka T K. Ulan R A. Goldnephropathy. A clinical and pathologic study. Arthritis Rlteliol1971): 13: 812-25.
12 Kaitz A. Little A H. Gold nephropathv. An iimmunopathologicstudy. Archives of Ptatholog 1973: 96: 133-6.
13 Fortson W C. Tcdcsco FJ. Diug-induccd colitis: a rexiscs. AiniJGastroenterol 1984: 79: 878-83.
14 Goldhammcr S. Eimi Fall son todlicher Solganolxergiftung. MedlKlit,ik 1935: 31: 645-7.
15 Pcrry M W. Gold injections aind colitis. JAMA 1939: 113: 965.16 Anderson N L. Palmer W L. The danger of gold salt thcraipv.
Report of a fatal case. JAMA 194ff: 115: 1627-30.17 Kandraic M. Pav J. Pcchova 1. Successful steroid therapy of
scvcre enteritis ciaiused by gold therapy. Cas Lek Cesk 1961:100: 361-7.
18 Kaplinsky N. Pras M. Ulccraitite colitis with gold treatment in
rheumatoid arthritis (Ficbrcw). Harefiali 1971: 80: 406-7.19 Roe M. Scars A D. Arndt J H. Gold reaction panenteritis.
Radiology 1972: 104: 59-6ff.2ff Kaplinsky N. Pras M, Frankl 0. Scverc enterocolitis com-
plicating chrysotherapy. An7ni Rhelon Dis 1973: 32: 574-7.21 Gerster J C, De Kalbermatten A. De Peyer R. Toussaint M,
Carrel J. Reactions toxiques aux scis d'or avec enterocolitegrave chez un homme atteint d'une polyarthrite rhumatoide.Schweiz Med Wochenschr 1976; 106: 160)6-8.
22 Siegman-Igra Y, Yaron M, Siletzki M. Schujman E. Gilat T.Colitis and death following gold therapy. Rheutnatol Rehabil1976: 15: 245-7.
23 Stein H B. Urowitz M B. Gold-induced enterocolitis. Casereport and literature review. J Rheuinatol 1976; 3: 21-6.
24 Sekolnik B R. Katz L A, Kozower M. Life-threatening entero-colitis after gold salt therapy. J Clitn Gastroettterol 1979; 1:145-8.
25 Szpak M W, Johnson R C. Brady C E. Boswell R N. Gold (Au)induced enterocolitis [Abstract]. Gastroenterology 1979; 76:1257.
26 Fam A G. Paton T W. Shamess J. Lewis A J. Fulminant colitiscomplicating gold therapy. J Rheuimatol 198ff: 7: 479-85.
27 Huston G J. Gold colitis. therapy and confirmaition of ilmucosaIrecovery bv mcisurciiemnt of ectal potential diffcrciice.PostgroalMed J 198ff: 56: 875-6.
28 Mairtin D M. Goldmnan J A. Gilliamii J. Naisrallah M. Gold-induced cosinophilic cnterocolitis: rcsponsc to oral cromolvinsodium. Ga.sroentterologs' 1981: 80: 1567-7(1.
29 Eaves R. Hansky J Waillis P. Gold induccd entcrocolitis: CaIscreport aind a revicw of the literature. A lsi NZ J Med 1982; 12:617-2ff.
3ff Sukenik S. Ilirsch M. Yanat-Inbar 1. Kraxwicc Freunld B.lHorowitz Y. Entcrocolitis complicating chrvsothcrapv. Casereport and rev icx of the literaturc. Isx J Med Sci 1982: 18:10)40-3.
31 Nagler J, Pagct S A. Nonexudativc diiarrhca after gold salttherapy: case report and review ot the literaturc. Aml JGastroentterol 1983: 78: 12-14.
32 Reinhart W H1. Kiappcier M. Halter F. Sexere pscudomemii-branous and ulccratixve colitis during goid thecrap. EndoscopY1983; 15: 70-2.
33 White R F. Maijor C A C. Gold colitis. M/cd 1 Ainsi 1983; 1:174-5.
34 Schmidt 11, Rcimann J F. Schmid A. ci a!. (old-Kolitis. DrschMed Wocheitsclir 1984; 109: 1583-5.
35 Jackson C W. Habonbi N Y. Whorwell P J, Schofield P F. Goldinduced enterocolitis. Gut 1986; 27: 452-6.
36 Maiscarenhas B R. Grandai J L. Freybcrg R Ii. Gold metia-holism in patients with rheumatoid arthritis treated with goldcompounds-reinvcstigaited. A tl1rirtis Rlieion7 1972: 15:391-41)2.
37 Gottlicb N L. Smith P M. Smnith E M. Phiarimiacodvnamics of'57Au and "5Au labelled aurothiomalatc in blood: correlatiionwith course of rheumatoid arthritis, gold toxicity and goldexcretion. A rthriti.s Rlelste 1974: 17: 171-81.
38 Dahl S L. Coleman M L. Williams I 1. (ito. Lack of corrclationbetwcn blood gold concentrationis and cliciai.l rcsponsc in
patients with definitc or classic rheumatoid arthritis receixingaurainofin or gold sodium thiomalatc. Atri/titis R/lieliti 1985: 28:1211 -8.
39 Gottlieb N L. Comparative pharmacokinetics of parenteral andoral gold compounds. J Rheumnatol [Suppli 1982; 9: 99-10f.
4ff van Riel P L C M, Gribnan F W J. van de Pritte L B A,Tap S H. Loose stools during auranofin treatment: clinical studyand some pathogenetic possibilities. J R/teumnatol 1983; 10:222-6.
41 Bandilla K. Gross D, Gross W, et al. Oral gold therapy withauranofin. J Rheumnatol jSuppl/: 1982: 9: 154-9.
42 Behrens R. Devereaux M. Hazleman B. Szaz K. Calvin J.Nealc G. Investigation of auranofin-induccd diairhoca. Git1986: 27: 59-65.
43 Watanabe 1. Whitticr C. Moore J, Cuppage F E. Gold nephro-pathy. Ultrastructural. fluorescence. and microanalytic studicsof two paticnts. Arch Pathol Lab Med 1976; 100: 632-5.
44 Viol G W. Minielly J A. Bistricki T. Gold nephropathy. Tissucanalysis by x ray fluorcscent spectroscopy. Arcli Pathol La/Med 1977; 101: 635-40).
45 Wooley P H. Griffin J, Panayi G S. Batchclor J R. Welsh K I.Gibson T J. HLA-Dr antigens and toxic reaction to auro-
thiomalate and D-penicillamine in patients with rheumatoidarthritis. N Engl J Med 1980; 303: 3()12.
46 Perrier P, Raffoux C, Thomas P, et al. HILA antigens and toxicreactions to sodium aurothiopropanol sulphonate and D-
penicillamine in patients with rheumatoid arthritis. Anti RmeuonDis 1985; 44: 621-4.
47 Hakala M, van Assendelft A H W, Ilonen J. Jalava S.Tiilikainen A. Association of different HLA antigens withvarious toxic effects of gold salts in rheumatoid arthritis. AnnRheum Dis 1986: 45: 177-82..
copyright. on M
ay 4, 2022 by guest. Protected by
http://ard.bmj.com
/A
nn Rheum
Dis: first published as 10.1136/ard.46.10.787 on 1 O
ctober 1987. Dow
nloaded from