Embed Size (px)
Citation preview


ARTHROPODSOF
MEDICAL ImpORTANCEFOURTH EDITION
Physician’s Guide to


CRC PR ESSBoca Raton London New York Washington, D.C.
ARTHROPODSOF
MEDICAL ImpORTANCEFOURTH EDITION
Jerome Goddard, Ph.D.Medical Entomologist
Bureau of Environmental HealthMississippi State Department of Health
andClinical Assistant Professor of Preventive Medicine
School of MedicineThe University of Mississippi Medical Center
Jackson, Mississippi
Physician’s Guide to

About the cover:
L–R, from the top: lone star tick (CDC); stable fly (USDA, ARS); horse fly (JG); millipede (US, FWS);caterpillar (US, FWS); fire ant (MCES);
Culex
mosquito laying eggs (CDC); giant fish-eating spider (JG); kissing bug (CDC).
Senior Editor: John SulzyckiProject Editor: Susan FoxProject Coordinator: Jamie SigalCover Designer: Dawn SniderMarketing Manager: Nadja English
This book contains information obtained from authentic and highly regarded sources. Reprinted material is quoted withpermission, and sources are indicated. A wide variety of references are listed. Reasonable efforts have been made to publishreliable data and information, but the author and the publisher cannot assume responsibility for the validity of all materialsor for the consequences of their use.
Neither this book nor any part may be reproduced or transmitted in any form or by any means, electronic or mechanical,including photocopying, microfilming, and recording, or by any information storage or retrieval system, without priorpermission in writing from the publisher.
The consent of CRC Press LLC does not extend to copying for general distribution, for promotion, for creating new works,or for resale. Specific permission must be obtained in writing from CRC Press LLC for such copying.
Direct all inquiries to CRC Press LLC, 2000 N.W. Corporate Blvd., Boca Raton, Florida 33431.
Trademark Notice:
Product or corporate names may be trademarks or registered trademarks, and are used only foridentification and explanation, without intent to infringe.
Visit the CRC Press Web site at www.crcpress.com
© 2003 by CRC Press LLC
No claim to original U.S. Government worksInternational Standard Book Number 0-8493-1387-2
Library of Congress Card Number 2002031436Printed in the United States of America 1 2 3 4 5 6 7 8 9 0
Printed on acid-free paper
Library of Congress Cataloging-in-Publication Data
Goddard, Jerome.Physician’s guide to arthropods of medical importance / Jerome Goddard.--4th ed.
p. ; cm.Includes bibliographical references and index.ISBN 0-8493-1387-2 (alk. paper)
1. Arthropod vectors. I. Title: Arthropods of medical importance. II. Title.[DNLM: 1. Arthropod Vectors. 2. Parasitic Diseases. 3. Arthropods--pathogenicity. 4.
Bites and Stings--therapy. WC 695 G578p 2002]RA641.A7 G63 2002641.4
′
32—dc21 2002031436
disclaimer page Page 1 Wednesday, November 20, 2002 1:41 PM

FOREWORD
Those who write forewords for books always say they are honored to be asked to doso. I really mean that. Over the last five years, I have gotten to know Dr. JeromeGoddard very well as we have collaborated on a number of research projects of mutualinterest. This book is a product of his exceptional knowledge and experience whichI have noted first hand.
Dr. Goddard has had a unique career in what may be best termed “applied medicalentomology.” For a number of years after completing his graduate education inentomology, he served in the School of Aerospace Medicine, Brooks Air Force Base,San Antonio, Texas. During that time, he taught and consulted and, in doing so,developed a global perspective on the role of arthropods in human diseases. Thatperspective has been preserved in each edition of this book, a text that has been usedby military, public health and other medical providers, both at home and on assign-ment, over the years.
As an allergist-immunologist, I see many patients who seek evaluation for conditionsthought to be related to insect stings or bites. This book is an especially usefulcompendium of the typical and atypical responses to these insects and other arthropodsand the entomology is a great help for those who are distant from college zoologycourses. Patients are greatly relieved to know their health care provider is informed inthis area and are more willing to accept recommendations offered in that context.
The fourth edition continues the previous tradition in that the information providedis practical and presented in a format optimal for use on an as-needed basis. Theaddition of 32 new color photographs and updating of many of the black and whitephotographs is a major plus. In addition, seven new case histories enliven the text.General guidelines to treatment of conditions resulting from exposure to arthropodsand appropriate references to detailed material are also provided.
With globalization of commerce, same-day air travel between continents, andmilitary activity in the most remote parts of the world, there is increasing contact witharthropod species otherwise not commonly encountered. This text has come of age ata time when it is needed most. It will especially be valued by health care providerswho find themselves in unknown territory, both geographically and medically.
Richard D. deShazo, M.D.Professor of Medicine and PediatricsDirector, Division of AllergyChairman, Department of MedicineUniversity of Mississippi Medical Center


PREFACE
Among the scientific disciplines, the relative importance of medical entomologycontinues to increase. Malaria affects hundreds of millions of people annually, anddevelopment of the much-needed malaria vaccine seems as distant as ever. Also,dengue fever inflicts pain and suffering on millions of persons each year, and now isthreatening the southern U.S. There are even “new” or emerging vector-borne diseasesbeing recognized. Lyme disease was unknown 30 years ago. Now it is the mostcommonly reported vector-borne disease in the U.S., with about 17,000 cases reportedeach year. Human cases of tick-borne ehrlichiosis were first described in the U.S. in1986; now at least three different ehrlichial agents have been found affecting humans.
Age-old vector-borne diseases such as epidemic typhus, plague, yellow fever, andrelapsing fever are still around. These agents remain endemic in many parts of theworld, and under the right conditions (e.g., war or disaster), can quickly erupt intoepidemics. Arthropod adaptability, combined with ecological and environmental changeand frequent air travel, ensure that vector-borne diseases will continue to be a problemfor humankind.
For most people living in the industrialized nations, the threat from insects, spiders,or mites lies primarily with stings and bites of various species and reactions, bothallergic and nonallergic, to them. For example, due to the ubiquity of honeybees orfire ants (in many areas), almost every person is occasionally stung. Allergic reactionscan be severe — resulting in death. In addition, for unknown reasons, fire ant invasionsinto nursing homes — resulting in attacks on patients — seem to be increasing in thesouthern United States.
This book was written to provide physicians, other health care providers, and publichealth officials with a reference of these insects, mites, scorpions, and spiders of publichealth importance as well as topics related to these organisms. Voluminous workscould be developed on many of these topics. However, a deliberate effort has beenmade to keep extraneous information to a minimum. Also, as in all areas of science,entomology has controversy over certain points and “facts.” In many cases these factsare constantly changing and being revised. Accordingly, I have chosen to streamlinethe references in this book and to provide views that represent a general consensusof the current status of each subject.
The primary focus of this arrangement is to provide easy, almost instant access toessential information concerning these topics. It is not the intent of this reference to

Figure 1Zoogeographic regions of the world. (From: U.S. DHEW, Public Health Service.)
make entomologists out of the readership. Specialists should be consulted wheneverpossible for definitive identification of an arthropod. Extensive technical jargon hasbeen avoided as much as possible in the “General Description” sections. However, aglossary is included to aid the reader in defining and/or locating descriptive terms andcharacters.
The volume begins with several chapters on the pathologic conditions caused byarthropods and the principles of treating those conditions. These are provided becausea physician may first have to identify the nature of an arthropod-caused problem (sting,bite, blistering, etc.). Chapter 1, Principles of Treatment, includes the rationale behindthe various treatment regimes. This should be helpful because, although specificrecommendations may change through time, the underlying principles of controllingthe immune response will not. When arthropods are mentioned in Part I, there will bea parenthetical reference indicating where in Part III the reader can go for more detailedinformation. Part II consists of a chapter on identification of arthropods and a chapteron common signs and symptoms of vector-borne disease.
The third major part of the book is an alphabetical arrangement of the arthropodsof medical importance with clearly marked subheadings for easy information access.To find a topic or insect section, the reader should look for that name or topicalphabetically. Keep in mind that all flies are grouped together, as are all lice, all mites,etc. A person wishing to find the topic “screwworm fly” would consult the flieschapters. Also, it is important to remember that common names vary with locality. A“blue-tailed darner” may mean one thing to the author and something totally differentto someone else. Often the geographic distributions of the arthropods are given inrelation to zoogeographic region. Figure 1 is provided to reacquaint the reader withthese regions. The Index includes the various pathologic conditions and as many ofthe common names as possible to aid the reader in finding a particular topic or insect.Also, it is important to remember that if a patient brings in to the clinic an insect, mite,or spider associated with a particular health problem, it is prudent to deal with theproblem (with this reference, hopefully) at hand but also to submit the specimen to

a university or health department entomologist for definitive identification. This mightbe important for later follow-up, consultation, or legal matters.
In Physician’s Guide to Arthropods of Medical Importance, 4th Edition, the chaptershave been updated with much of the latest information. In addition, a new chapter hasbeen added on pentastomes because they are classified by many entomologists asarthropods due to their chitinous exoskeleton. The mosquito chapter has been exten-sively rewritten in light of West Nile virus and new classification of the genus Aedes.Lastly, many of the older photographs have been replaced with new, improved ones(or line drawings), and eight pages of color photographs have been added. I am veryexcited about this new edition and wish to extend appreciation to my colleagues forcontinued interest in this book.
Finally, every effort has been made to ensure that the treatment recommendationsherein are current and widely recognized as appropriate. However, it must be emphasizedthat treatment recommendations may change over time and should not be construed tobe the sole specific treatment guidelines for any one case. Physicians should consultappropriate medical literature (Conn’s Current Therapy, for example) and/or drug pack-age inserts for the most up-to-date treatment recommendations.
Jerome Goddard, Ph.D.


ACKNOWLEDGMENTS
1ST EDITION
This book would not have been possible without the help and advice of numerousindividuals. My special thanks are due to two medical entomologists. Chad McHugh,a uniquely insightful civilian U.S. Air Force entomologist (Brooks AFB, TX), mostgenerously read every chapter (sometimes more than once) and offered invaluableadvice and comments. LTC Harold Harlan (an outstanding Army entomologist at theUniformed Services University of the Health Sciences, Bethesda, MD) also read theentire book, giving helpful advice and additional information. Both of these individualswere more than willing to take time out of their busy schedules to work through a quitevoluminous manuscript.
A few physicians with whom I work directly or indirectly reviewed portions of themanuscript and/or offered much-needed comments: Drs. Mary Currier and Tom Brooks(Mississippi Department of Health), and Drs. David Conwill and John Moffitt (Universityof Mississippi Medical Center).
During the formative stages of the manuscript the following individuals reviewedspecific chapters or subject areas: Dr. Hans Klompen (Institute of Arthropodology andParasitology, Georgia Southern University), Dr. Paul Lago (Biology Department, Uni-versity of Mississippi), Dr. Robert Lewis (Department of Biology/Zoology, Iowa StateUniversity), Maj. Tom Lillie (a U.S. Air Force Entomologist), Mr. Tim Lockley (USDA,APHIS, Imported Fire Ant Lab), and Dr. Hal Reed (Biology Department, Oral RobertsUniversity).
Information on specific arthropods and/or photographs were provided by Dr.Virginia Allen (Geisinger Medical Center, Pennsylvania), Mr. Steve Bloemmer (TVA,Land Between the Lakes), Dr. Tom Brooks (University of Mississippi Medical Centerand Mississippi Department of Health), Drs. Richard Brown, Clarence Collison, and BobCombs (Mississippi State University, Entomology Department), Mr. Ian Dick (Environ-mental Health Department, The London Borough of Islington), Ms. Sandra Evans (U.S.Army Environmental Hygiene Agency, Aberdeen Proving Ground), Mr. Harry Fulton(Mississippi Department of Agriculture, Bureau of Plant Industry), LTC Harold Harlan(a U.S. Army Entomologist), Dr. James Jarratt (Mississippi State University, EntomologyDepartment), Dr. Hans Klompen (Institute of Arthropodology and Parasitology, Geor-gia Southern University), Mr. John Kucharski (USDA, Agricultural Research Service), Dr.Paul Lago (Biology Department, University of Mississippi), Maj. Tom Lillie (a U.S. AirForce Entomologist), Mr. Tim Lockley (USDA, APHIS, Fire Ant Lab), Dr. Chad McHugh

(Civilian U.S. Air Force Entomologist), Dr. Hal Reed (Biology Department, Oral RobertsUniversity), Dr. Richard Robbins (Armed Forces Pest Management Board, Defense PestManagement Information Analysis Center), Dr. John Schneider (Mississippi State Uni-versity, Entomology Department), and Ms. Sue Zuhlke (Mississippi Gulf Coast MosquitoControl Commission).
The U.S. Air Force medical entomology facts sheets (from the Epidemiology Divisionof the USAF School of Aerospace Medicine) were instrumental in writing somechapters, as were some written sections and illustrations from the Mississippi Depart-ment of Health publication, The Mosquito Book by Ed Bowles. Les Fortenberry(Mississippi Department of Health) did most of the original art work. Much of Chapter28 (Ticks) was taken from a previous military manual written by the author entitledTicks and Tick-Borne Diseases Affecting Military Personnel. Art work in that publicationwas originally done by Mr. Ray Blancarte (USAF School of Aerospace Medicine), andsome photography was done by Mr. Bobby G. Burnes (also of the USAF School ofAerospace Medicine). The Centers for Disease Control “Key to Arthropods of MedicalImportance,” which is revised and included as a figure in Chapter 8, was originallywritten by H. D. Pratt, C. J. Stojanovich, and K. S. Littig.
My wife, Rosella M. Goddard, did much of the typing and encouraged me duringthe 3 years of manuscript preparation. I owe a great deal of gratitude to her.
2ND EDITION
Chad McHugh (U.S. Air Force Civilian Entomologist), Dr. David Conwill (University ofMississippi Medical Center), and Dr. Mary Currier (Mississippi Department of Health)provided helpful comments.
The following persons provided photographs or permission to use their material: Dr.Mary Armstrong, Ralph Turnbo, and Tom Kilpatrick (all at the Mississippi Departmentof Health), Dr. Alan Causey (University of Mississippi Medical Center), Mike and KathyKhayat (Pascagoula, MS), and Dr. Gary Groff (Pascagoula, MS).
As always, my wife, Rosella, and my sons, Jeremy and Joseph, helped me im-mensely. Many of the sting or bite lesions were photographed from my boys as wespent time in the field collecting specimens.
3RD EDITION
As scientific knowledge continues to expand at an unprecedented rate, it is obviousthat no one person can hope to keep up. Accordingly, I continue to utilize severalscientists/physicians as resource persons. Their help is critical; I could not keep thisbook up-to-date without their help. They are Dr. Chad McHugh (U.S. Air Force CivilianEntomologist), Dr. Hans Klompen (currently at Ohio State University), Drs. DavidConwill and William Lushbaugh (University of Mississippi Medical Center), Dr. Fernandode Castro (Dermatology Associates, Lexington, KY), and Drs. Mary Currier and RisaWebb (Mississippi Department of Health). Phyllis Givens (Jackson, MS) and GeorgeAllen (Jackson, MS) provided photographs or specimens.
Again, my wife, Rosella, and my sons, Jeremy and Joseph, helped me immensely.Fourteen of the pictures in this book are of Jeremy or Joseph, either to illustrate lesionsor to demonstrate a particular activity.

4TH EDITION
Dr. Chad McHugh (U.S. Air Force Civilian Entomologist), Dr. Chris Paddock (CDC), Dr.Mary Currier (Mississippi Department of Health), and Drs. John Moffitt and RicharddeShazo (University of Mississippi Medical Center) provided helpful comments. Dr.deShazo was invaluable in helping me update the allergy sections, and graciouslyallowed me to use a brief portion of his writing in Chapter 1 under “Mechanisms ofAllergic Reactions.”
The following persons provided photographs, specimens, or permission to use theirmaterial: Dr. Mike Brooks (Laurel, MS), Dr. Barry Engber (North Carolina Departmentof Health), Dr. James Jarratt (Mississippi State University), Dr. Richard Russell andStephen Doggett (Westmead Hospital, Westmead, Australia), Sheryl Hand and Dr. SallySlavinski (Mississippi Department of Health). I am especially indebted to James Jarratt,a long-time friend who has helped me through the years photograph specimens andallowed me to use his (much better) photos.


AUTHOR
Jerome Goddard is a medicalentomologist in the Bureau ofEnvironmental Health, MississippiState Department of Health, andalso holds two appointments inthe School of Medicine, The Uni-versity of Mississippi Medical Cen-ter — Clinical Assistant Professorof Preventive Medicine and Assis-tant Professor of Medicine.
He received his bachelor’s andmaster’s degrees in biological sci-ence from the University of Mis-sissippi in 1979 and 1981, and hisPh.D. degree in medical entomol-ogy from Mississippi State Univer-sity in 1984. In December of 1985he was commissioned as an of-ficer in the U.S. Air Force and
served as a medical entomologist in the Epidemiology Division of the USAF School ofAerospace Medicine, Brooks AFB, Texas, for three and a half years. In 1988 he wasnamed Best Academic Instructor in the Residents in Aerospace Medicine Course andCompany Grade Officer of the Year. Since March of 1989 Dr. Goddard has been servingin the capacity of State Medical Entomologist at the Mississippi Department of Health,Jackson, Mississippi, where he designs, implements, and supervises all entomologicalprojects and vector control programs relating to public health throughout the state ofMississippi. In addition, he serves as editor of the health department publication,Mississippi Morbidity Report.
Dr. Goddard has authored or co-authored over 100 scientific publications in the fieldof medical entomology and is the author of Ticks and Tick-borne Diseases AffectingMilitary Personnel, published by the U.S. Air Force, as well as Infectious Diseases andArthropods, published by Humana Press. He was recently featured in Reader’s Digest

and on a series entitled “Living with Bugs” on the Learning Channel. In 2001, Dr.Goddard published a novel about a mosquito-borne disease outbreak entitled, The Wellof Destiny. Dr. Goddard frequently presents seminars and guest lectures nationally andinternationally on “Arthropods and Medicine” and related topics. He is a member ofSigma Xi, the Entomological Society of America, the American Association for theAdvancement of Science, the Mississippi Mosquito and Vector Control Association, andthe Mississippi Entomological Association. His main research interests are the ecologyand epidemiology of tick-borne diseases.

DEDICATIONS
Dr. Paul K. LagoThank you for your love of entomology, maintenance of high academic standards, andacts of patience and kindness. You are truly an entomologist par excellence.
Millard and Betty LothenoreThank you for an example of integrity and unconditional love.
E.J. and ClareneThank you each for a parent’s love and more; for faith, hope, strength, phone calls …Words cannot express my appreciation to you both.
Rosella, my wifeThank you for being a saint; for unswerving support through thick and thin … forloving me.


TABLE OF CONTENTS
PART IPathological Conditions Caused by Arthropods and
Principles of Their Treatment
Chapter 1Principles of Treatment for Arthropod Bites, Stings, and Other Exposure ................. 3
Chapter 2Allergy to Arthropods and Their Venoms .................................................................... 11
Chapter 3Stings ............................................................................................................................... 29
Chapter 4Bites ................................................................................................................................. 39
Chapter 5Dermatitis, Urticaria, and Blistering from Contact with Arthropods .......................... 55
Chapter 6Myiasis (Invasion of Human Tissues by Fly Larvae)................................................... 61
Chapter 7Delusions of Parasitosis (Imaginary Insect or Mite Infestations) ............................... 67
PART IIIdentification of Arthropods and the Diseases They Cause
Chapter 8Identification of Medically Important Arthropods ....................................................... 79
Chapter 9Signs and Symptoms of Arthropod-Borne Diseases .................................................... 99

PART IIIArthropods of Medical Importance
Chapter 10Ants .................................................................................................................................107
Chapter 11Bees ................................................................................................................................115
Chapter 12Blister Beetles ................................................................................................................121
Chapter 13Bugs (The True Bugs) ..................................................................................................125
Chapter 14Caterpillars (Urticating) .................................................................................................137
Chapter 15Centipedes ......................................................................................................................145
Chapter 16Cockroaches ...................................................................................................................149
Chapter 17Earwigs ...........................................................................................................................153
Chapter 18Fleas ................................................................................................................................155
Chapter 19Flies (Biting) ...................................................................................................................163
Chapter 20Flies (Non-Biting) ..........................................................................................................185
Chapter 21Flies Whose Maggots Cause Myiasis in Humans ........................................................195
Chapter 22Lice ..................................................................................................................................215
Chapter 23Millipedes .......................................................................................................................225
Chapter 24Mites ...............................................................................................................................229
Chapter 25Mosquitoes .....................................................................................................................249
Chapter 26Moths (Species Whose Scales or Hairs Cause Irritation) ...........................................291

Chapter 27Pentastomes (Tongue Worms) .....................................................................................297
Chapter 28Scorpions ........................................................................................................................301
Chapter 29Spiders ............................................................................................................................309
Chapter 30Ticks ...............................................................................................................................327
Chapter 31Wasps (Paper Wasps, Hornets, and Yellowjackets) ...................................................387
PART IVPersonal Protection Measures Against Arthropods
Chapter 32Pros and Cons of Repellents ........................................................................................399
Chapter 33Arthropod-Specific Personal Protection Techniques ...................................................407
PART VFurther Reading, Glossary, and Index
Further Reading .............................................................................................................417
Glossary ..........................................................................................................................419
Index ...............................................................................................................................427


PART I
PATHOLOGICALCONDITIONS CAUSEDBY ARTHROPODS AND
PRINCIPLES OF THEIRTREATMENT


3
Principles of Treatment for Arthropod Bites, Stings, and Other Exposure
CHAPTER 1
PRINCIPLES OFTREATMENT FOR
ARTHROPOD BITES,STINGS, AND
OTHER EXPOSURE
TABLE OF CONTENTS
I. Introduction ......................................................................................................... 4
II. Direct Effects of Arthropod Exposure ............................................................... 4
III. Hypersensitivity Reactions to Arthropod Venom or Saliva ............................. 5A. Hypersensitivity Reactions ............................................................................. 5B. Local Hypersensitivity Reactions ................................................................... 7C. Systemic Hypersensitivity Reactions ............................................................. 7D. Late Hypersensitivity Reactions .................................................................... 7E. Delayed Hypersensitivity Reactions .............................................................. 8F. Treatment Principles for Hypersensitivity Reactions ................................... 8
IV. Neurotoxic Venoms ............................................................................................ 9A. Mechanisms of Toxicity ................................................................................. 9B. Treatment Principles for Neurotoxic Venoms ............................................. 9
V. Necrotic Venoms ................................................................................................. 9A. Mechanisms of Toxicity ................................................................................. 9B. Treatment Principles for Necrotic Venoms ................................................ 10
References ....................................................................................................................... 10

4
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
I. INTRODUCTION
Arthropods adversely affect humans in a number of ways. There are direct, nonallergiceffects such as tissue damage due to stings, bites, and vesicating fluid exposure andtissue infestation by the bugs themselves (e.g., myiasis). Additionally, some venomsproduce necrosis in human tissues, while others produce neurological effects. Indirecteffects on human health are disease transmission and allergic reactions to bites andstings, as well as allergic reactions to arthropod skins or emanations.
Since there are different underlying mechanisms that produce the pathologicalreactions associated with arthropods, it is imperative that attending physicians properlycategorize a reaction in order to counteract those ill effects. This chapter is designedto present a brief overview of the underlying principles of treating arthropod exposure,focusing on the different types of pathological conditions produced by arthropods. Noeffort is made to explain in detail the immunological and physiological basis underlyingthese types of pathology; instead, a general overview of the mechanisms involved andways to counteract or control them is given. No mention is made of the immunopatho-logical consequences of arthropod-borne parasite infections.
II. DIRECT EFFECTS OF ARTHROPOD EXPOSURE
Certainly, bees or wasps can sting and produce toxic effects in humans by their venomalone, regardless of hypersensitivity. Venoms in many social wasps and bees containsubstances that produce pain and release histamine (directly, not IgE mediated) (seeChapter 3 for a more detailed discussion). Stings or bites cause some tissue damageand inflammation. Inflammation is a result of at least three events: (1) an increase inblood supply to the affected area; (2) an increase in capillary permeability allowinglarger molecules to cross through the endothelium; (3) leukocytes, mostly neutrophilsand macrophages, migrating into the affected tissues.
It has often been estimated that between 500 and 800 honey bee stings could causehuman death due to toxic effects of the venom alone. One author calculated that 1,500honey bee stings would constitute the median lethal dose for a 75 kg person basedupon extrapolation from the LD50 of bee venom for mice.1 These direct toxic effects(from honey bees or other social Hymenoptera) would include release of histamine,contraction of smooth muscle, increase in capillary permeability, vasodilation with aresulting drop in blood pressure, destruction of normal tissue barriers, destruction ofred blood cells, and pain. Severe cases would probably result in renal failure.1
Treatment strategies would include symptomatic treatment until the venom effects werediminished. Since histamine is a component of bee, wasp, and hornet venoms, andsince melittin (found in honey bee venom) causes histamine to be released from cells,administration of antihistamines would be indicated. In addition, therapeutic agents tocounteract the ill effects of histamine release, e.g., bronchodilators, would also behelpful.
Biting insects produce direct effects on humans as well. Mosquitoes are a nuisancedue to their biting behavior, and they may produce tiny punctate hemorrhages (withor without a halo) or persistent papular lesions.2 Sometimes large wheals with grosssurrounding edema are produced due to sensitization. Black flies, attacking by thethousands, may cause severe annoyance and small itchy papules and/or swelling.2
Ceratopogonid midges also bite in vast numbers causing irritation and numerous

5
Principles of Treatment for Arthropod Bites, Stings, and Other Exposure
minute papular lesions that may persist for several days.2 Other biting insects that affecthuman health directly include bed bugs, kissing bugs, horse and deer flies, stable flies,fleas, and lice. Treatment principles for the direct effects of biting insects generallyinvolve palliative antipruritic lotions or creams and a brief course of systemic corticos-teroids if necessary.2
Some caterpillars possess poison-filled spines that break off in human skin uponhandling or other contact (see Chapters 5 and 14). These spines release venom-likesubstances into the skin upon contact, and pathology similar to a sting may develop.Except in systemic reactions, treatment generally involves topical application of palliatives.2
In addition, the imbedded broken off spines themselves may need to be removed. Thismay be done with clear adhesive tape in a repeated “stripping” action.
Myiasis, the invasion of human tissue by living fly maggots, is also a direct effectof arthropods on human health (see Chapters 6 and 21). Although inflammation andsecondary infection may be involved, the primary treatment is to remove the maggot(s).Most pathology associated with myiasis resolves fairly readily after removal.
Blister beetles contain the vesicating agent, cantharidin, which produces water-filledblisters on human skin a few hours after exposure. Blisters resulting from exposure aregenerally not serious but may require efforts to prevent secondary infection.
III. HYPERSENSITIVITY REACTIONS TO ARTHROPODVENOM OR SALIVA
Sometimes the human immune system produces undesirable results in trying to protectthe body. In a hypersensitive or “allergic” person, a relatively innocuous antigen elicitsan out-of-proportion immune reaction. Thus, the tissue damage resulting from hyper-sensitivity is worse than the damage produced by the salivary secretion, venom, orother antigen itself.
A. Hypersensitivity Reactions
Hypersensitivity reactions fall into two principal categories, reflecting the two majorsubdivisions of the immune system. The first category includes those reactions initiatedby antibody (for instance, immediate hypersensitivity reactions), in which symptomsare manifest almost immediately after exposure to antigen by a sensitized person. Thesecond category includes those reactions initiated by T lymphocytes (delayed hyper-sensitivity), and symptoms are usually not obvious for a number of hours or days.
Some authors break hypersensitivity down into four types: I, II, III, and IV. TypesI to III involve antibody mediated reactions. Type I reactions are IgE-mediatedimmediate hypersensitivity reactions. A systemic reaction to a honey bee sting is a goodexample of type I hypersensitivity. Because the allergen is directly introduced into theblood or tissue, a severe reaction can occur, such as anaphylactic shock. Type IIreactions are antibody-mediated “cytotic” reactions like those occurring with somehemolytic reactions. Type III reactions are mediated by circulating antibody-antigencomplexes and cause clinical syndromes like serum sickness. Type IV reactions aremediated by T lymphocytes and macrophages and occur independent of antibody.
Allergens and specific antibodies produced to allergens do not by themselves causethe pathological symptoms associated with immediate hypersensitivity. Instead, thechemical substances (called mediators) released or activated in the host’s tissues,

6
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
resulting from the antigen–antibody binding in solution or on the cell membranes,cause the characteristic tissue damage associated with hypersensitivity.
In atopic persons, the initial exposure to an allergen stimulates an immunoglobulinE (IgE) response. IgE is a minor component of normal blood serum having aconcentration of approximately 1 µg/ml. IgE levels are generally higher in atopicpersons than in normal subjects of the same age; however, a normal IgE level does notexclude atopy. IgE levels are also elevated in persons with parasitic worm infections,which indicates its beneficial role in humans. IgE-sensitized mast cells in the gutmucosa provide a good defense against the worms attempting to traverse the gut wall.The IgE produced in atopic individuals in response to allergens sensitizes mast cells,which degranulate upon future exposure to allergen.
Mast cells are similar structurally and functionally to basophils. They are found inassociation with mucosal epithelial cells as well as in connective tissue. Mast cellscharacteristically contain approximately 1000 granules, which upon degranulationrelease pharmacological mediators causing the allergic symptoms.
Mechanisms of allergic reactions. Having “allergies” reflects an autosomal dominantpattern of inheritance with incomplete penetrance. This pattern of inheritance showsup as a propensity to respond to allergen exposure by producing high levels ofallergen-specific IgE. Excess production of IgE appears to be controlled by variousimmune response genes located in the major histocompatibility complex (MHC) onchromosome 6.
IgE response is dependent upon prior sensitization to allergen. The allergen mustfirst be internalized by antigen-presenting cells, including macrophages, dendritic cells,activated T lymphocytes, and B lymphocytes. After allergen processing, peptidefragments of the allergen are presented with class II (MHC) molecules of host antigen-presenting cells to CD4+T lymphocytes. These lymphocytes have receptors for theparticular MHC-peptide complex. This interaction results in release of cytokines by theCD4+ cell. T-helper lymphocytes (CD4+) are apparently in two classes: TH1 and TH2.If the CD4+ cells that recognize the allergen are of the TH2 class, a specific group ofmediators is released, including interleukin-4 (IL-4), IL-5, and IL-9. Other cytokines suchas IL-2, IL-3, IL-10, IL-13, and granulocyte-macrophage stimulating factor (GM-CSF), arealso released in the process of antigen recognition but are not specific to the TH2 class.Cytokines such as IL-4, IL-5, and IL-6 are involved in B-cell proliferation and differen-tiation. Activated B lymphocytes (with bound allergen) are stimulated by these cytokinesto multiply and secrete IgM antibody. IL-4, IL-6, IL-10, and IL-13 from TH2 cells promoteB-cell isotype switching to IgE production. Thus, atopy appears to be a result ofpredisposition toward TH2-type responses, resulting in production of large quantitiesof allergen-specific IgE.
IgE antibodies specific for a certain allergen bind to mast cells and basophils. Whenthese “sensitized” cells are re-exposed to the offending allergen, IgE molecules attachedto the surface of mast cells and basophils become cross-linked by allergen, leading toa distortion of the IgE molecules and a subsequent series of enzymatic reactions andcell degranulation which release mediators into the blood stream and local tissues. Themost important pre-formed mediator is histamine, which causes vasodilation, increasedvascular permeability (leading to edema), and mucous secretion (respiratory tract).Other mediators are formed during degranulation such as Prostaglandin D2 (PGD2), thesulfidopeptide leukotrienes LTC4, LTD4, and LTE4 (slow reacting substance of anaphy-

7
Principles of Treatment for Arthropod Bites, Stings, and Other Exposure
laxis), platelet-activating factor (PAF), and bradykinin. PAF is a potent chemotacticfactor, and the sulfidopeptide leukotrienes and bradykinin are vasoactive compounds.Cross-linking of IgE on mast cells also activates phospholipase A2 and releasesarachidonic acid from the A2 position of cell membrane phospholipids. Mast cells thenmetabolize arachidonic acid through the cyclocxygenase pathway to form prostaglan-din and thromboxane mediators or through the lipoxygenase pathway to formleukotrienes.
Once the allergic reaction begins, mast cells amplify it by releasing vasoactive agentsand cytokines such as GM-CSF, tumor necrosis factor α (TNF-α), transforming growthfactor β, IL-1 to IL-6, and IL-13. These cytokines lead to further IgE production, mastcell growth, and eosinophil growth, chemotaxis, and survival. For instance, IL-5, TNF-α, and IL-1 promote eosinophil movement by increasing their expression of adhesionreceptors on endothelium. Then, arriving eosinophils secrete IL-1, which favors TH2 cellproliferation and mast cell growth factor IL-3. Eosinophils release oxygen radicals andproteins which are toxic to affected tissues.
B. Local Hypersensitivity Reactions
Local allergic reactions involve the nose, lung, and occasionally the skin. These areaswhere allergen makes contact with sensitized (IgE “loaded”) tissues are usually the onlyones affected in these reactions. Allergic and perennial rhinitis, as well as asthma, maybe due to arthropods or their emanations. A good example of this is house dust miteallergy (see Chapter 24).
C. Systemic Hypersensitivity Reactions
Systemic allergic reactions are more likely to occur when the allergen reaches theblood or lymph circulations and involve several organ systems. Anaphylaxis is theterm often used to describe the rapid, sometimes lethal sequence of events occurringin certain cases upon subsequent exposure to a particular allergen. Initial signs ofanaphylaxis are often cutaneous, such as generalized pruritus, urticaria, and/orangioedema. If the reaction continues, excessive vasodilation and increased vascularpermeability caused by histamine and the other mediators may lead to irreversibleshock. When angioedema affects the larynx, oropharynx, or tongue, the upper airwaycan become occluded. Pulmonary edema and bronchial constriction may lead torespiratory failure.
D. Late Hypersensitivity Reactions
A cutaneous late phase IgE-mediated response in allergic individuals may appear 2 to48 hours after challenge and is characterized by a second wave of inflammatorymediators and dramatic influx of immune and inflammatory cells to the site of antigenexposure. These reactions, also called large local reactions, are pruritic, painful,erythematous, and edematous, and often peak within 12 hours after stings. The edemafrom large local reactions can, in extreme cases, be severe enough to cause compres-sion of nerves or blood vessels to an extremity.3 Late phase asthma and anaphylaxisoccur via similar mechanisms.

8
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
E. Delayed Hypersensitivity Reactions
An allergic dermatitis, characterized by eczema-like eruptions on the skin, may developin response to insect or mite body parts, saliva, or feces secondary to the immediatereaction. Delayed-type hypersensitivity reactions typically appear over a period ofseveral days, perhaps not maximal until 48 or 72 hours after antigen exposure. This iscell-mediated immunity wherein CD4-positive T lymphocytes react with antigen andrelease lymphokines into tissues. These lymphokines may serve as attractants formonocytes.
F. Treatment Principles for Hypersensitivity Reactions
Antihistamines block most, if not all, of the effects of histamine release. This isaccomplished by competing for histamine at its receptor sites, thus preventing hista-mine from attaching to these receptor sites and producing an effect on body tissues.Oral administration of antihistamines is often recommended for local reactions. Intreating generalized systemic or anaphylactic reactions, epinephrine remains the mostimportant treatment and can be life-saving. Antihistamines such as diphenhydraminehydrochloride are given parenterally.
Localized wheal and flare reactions to mosquito bites may even be prevented by useof oral antihistamines. One study demonstrated that persons who had previously haddramatic cutaneous reactions to mosquito bites, when taking cetirizine (Zyrtec®), hada 40% decrease in the size of the wheal response at 15 minutes and the size of the bitepapule at 24 hours.4
Corticosteroids have an anti-inflammatory effect. They act by various mechanismsincluding vasoconstriction, decreasing membrane permeability, decreasing mitoticactivity of epidermal cells, and lysosomal membrane stabilization within leukocytes andmonocytes. In antigen-dependent T cell activation reactions (delayed hypersensitivity),steroids inhibit antigen-specific lymphocyte activation and proliferation. Also, inhibitionof the influx of inflammatory cells by glucocorticoids leads to inhibition of theappearance of inflammatory mediators during the late phase. Applied topically to theskin, steroids deplete Langerhans cells of CD1 and HLA-DR molecules, blocking theirantigen presenting function.
In certain arthropod-related allergies (including asthma) such as dust mite orcockroach allergies, inhaled steroids, leukotriene antagonists, or cromolyn sodium maysometimes be used. Cromolyn stabilizes mast cells against degranulation, thus prevent-ing release of histamine, leukotrienes, and other pharmacologic mediators. The use ofepinephrine in severe or systemic hypersensitivity reactions acts to suppress (stabilize)mediator release from mast cells and basophils and reverses many of the end organresponses to the pharmacological mediators of anaphylaxis. Thus, there is bronchodilationand relaxation of smooth muscle. The prompt use of epinephrine can often lead tocomplete resolution of the clinical manifestations of anaphylaxis within minutes.5
Other specific interventions may be needed to manage anaphylaxis (see Chapter 2for more detail). These include actions such as supplemental inspired oxygen, endot-racheal intubation, cricothyrotomy, adrenergic stimulants (such as isoproterenol, dopam-ine, norepinephrine, nebulized β2 agonists), glucagon (for β-blocked patients), H1 andH2 antihistamines, and glucocoricoids.5,6 Careful monitoring of each individual case,with particular attention to the intensity and relative progression of the anaphylaxis,

9
Principles of Treatment for Arthropod Bites, Stings, and Other Exposure
should enable the attending physician to decide which of these additional measuresare indicated.
IV. NEUROTOXIC VENOMSA. Mechanisms of Toxicity
Widow spiders and some scorpions produce ill effects in humans by neurotoxicvenoms. Widow spider (Latrodectus spp.) venom is a neuromuscular-damaging proteinthat affects ion transport. It produces sweating, piloerection, muscular spasm, weak-ness, tremor, and sometimes paralysis, stupor, and convulsions. This type of venommay not produce obvious skin lesions but will primarily produce the systemic reactions.
Scorpion venom is also neurotoxic. It contains multiple low-molecular-weight basicproteins (the neurotoxins), mucus (5 to 10%), salts, and various organic compoundssuch as oligopeptides, nucleotides, and amino acids. Unlike most spider and snakevenoms, scorpion venom contains little or no enzymes. The low molecular weightproteins increase permeability through the neuronal sodium channels. These toxinsdirectly affect the neuronal portion of the neuromuscular junction causing depolariza-tion of the nerve and myocyte. They may also increase permeability of neuronal sodiumchannels in the autonomic nervous system. Systemic symptoms of scorpion envenoma-tion include blurred vision, sweating, spreading partial paralysis, muscle twitching,abnormal eye movements, excessive salivation, hypertension, and sometimes convul-sions. Death (if it occurs) is usually a result of respiratory paralysis, peripheral vascularfailure, and/or myocarditis.
B. Treatment Principles for Neurotoxic Venoms
Strategies for treating an arthropod bite or sting that is neurotoxic in nature involvecounteracting the effects of the venom and supportive treatment. Antivenins arecommercially available for many of the widow spider venoms and the venoms of somescorpion species. Muscle relaxants, calcium gluconate and/or antivenin are often usedfor widow spider bites (see Chapter 29). Antivenin is sometimes used in treatingscorpion stings along with anticonvulsants, vasodilators, assisted ventilation, and othersupportive measures as needed (see Chapter 28).
V. NECROTIC VENOMSA. Mechanisms of Toxicity
In contrast to the widow spiders, violin spiders (brown recluse is one of the mostnotable) have venom that is necrotic in activity coupled with hyaluronidase that actsas a spreading factor. Brown recluse spider venom contains a lipase enzyme,sphingomyelinase D, which is significantly different from phospholipase A in bee andwasp venoms. This specific lipase is the primary necrotic agent involved in theformation of the typical lesions (see Chapter 29). It is possible that neutrophilchemotaxis is induced by sphingomyelinase D.7 The subsequent influx of neutrophilsinto the area is critical in the formation of the necrotic lesion.

10
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
B. Treatment Principles for Necrotic Venoms
Treatment of a necrotic arthropod bite (e.g., brown recluse) is controversial becausecontrolled studies are lacking and the severity of the bite is variable.8 Currently, it mayinvolve antibiotic therapy, antivenin (if available), and dapsone, if the patient is notglucose-6-phosphate dehydrogenase deficient7–11 (see Chapter 29). King12 said thatapplication of ice packs may be very important in limiting necrosis since activity of thenecrotic enzyme in brown recluse venom is related to temperature.
REFERENCES1. Camazine, S., Hymenopteran stings: reactions, mechanisms, and medical treatment, Bull.
Entomol. Soc. Am., p. 17, Spring 1988.
2. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 9.
3. Moffitt, J. E. and deShazo, R. D., Allergic and other reactions to insects, in Rich’s ClinicalImmunology Principles and Practice, 2nd ed., Rich R. R., Fleisher, W. T., Kotzin, B. L.,Schroeder, H. W., Jr., Eds., Mosby, New York, 2001, p. 47.3.
4. Reunala, T., Brummer-Korvenkotio, H., Karppinen, A., Coulie, P., and Palosuo, T.,Treatment of mosquito bites with cetirizine, Clin. Exp. Allergy, 23, 72, 1993.
5. Sullivan, T. J., Treatment of reactions to insect stings and bites, in Monograph on InsectAllergy, 2nd ed., Levine, M. I. and Lockey, R. F., Eds., American Academy of AllergyImmunology, Milwaukee, WI, 1986, chap. 7.
6. Wasserman, S. I., Anaphylaxis, in Rich’s Clinical Immunology Principles and Practice, 2nded., Rich R. R., Fleisher, W. T., Kotzin, B. L., Schroeder, H. W., Jr., Eds., Mosby, New York,2001, p. 46.7.
7. King, L. E., Jr., Spider bites, Arch. Dermatol., 123, 41, 1987.
8. Berger, R. S., Spider bites and scorpion stings, in Conn’s Current Therapy, Rakel, R. E.,Ed., W. B. Saunders, Philadelphia, 1992, 1093.
9. Delozier, J. B., Reaves, L., King, L. E., Jr., and Rees, R. S., Brown recluse spider bites ofthe upper extremity, S. Med. J., 81, 181, 1988.
10. Rees, R., Campbell, D., Reiger, E., and King, L. E., Jr., The diagnosis and treatment ofbrown recluse spider bites, Ann. Emer. Med., 16, 945, 1987.
11. Maters, E., Sams, H., and King, L., Jr., Loxoscelism, New. Engl. J. Med., 339, 1944, 1998.
12. King, L. E., Jr., Brown recluse bites: stay cool, J. Am. Med. Assoc., 254, 2895, 1986.

11
Allergy to Arthropods and their Venoms
CHAPTER 2
ALLERGY TOARTHROPODS AND
THEIR VENOMS
TABLE OF CONTENTS
I. Allergy to Stings or Bites ................................................................................. 12A. Introduction and Medical Significance ....................................................... 13
Normal Reaction to Stings or Bites ........................................................ 14Severe Local (or Large Local) Reaction to Stings or Bites .................. 14Systemic Reaction to Stings or Bites ...................................................... 14Cross-Reactivity among Venoms ............................................................ 15
B. Management and Treatment ........................................................................ 15Normal Reaction ...................................................................................... 15Severe Local (or Large Local) Reaction ................................................. 16Systemic Reaction .................................................................................... 16Long-Term Management of Insect Sting Allergy .................................. 18
C. Avoidance of Offending Insects ................................................................. 19
II. Allergy — Irritation Caused by Consuming or Inhaling Insect orMite Parts ........................................................................................................... 21A. Introduction and Medical Significance ....................................................... 21
Reactions via the Respiratory Route ...................................................... 22Reactions via the Digestive Tract ........................................................... 25
B. Management and Treatment ........................................................................ 25House Dust Mites .................................................................................... 25Cockroaches ............................................................................................. 25Food Contamination ................................................................................ 26
References ....................................................................................................................... 26

12
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
CASE HISTORY
ALLERGIC REACTION TO FIRE ANT STING?
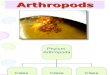
A woman called saying she washaving an allergic reaction to anant sting. From her descriptionof the event and the mound, thespecimen was likely a fire ant.She quickly described her le-sion — small pustule — andhow she had felt since the sting.The sting had happened the daybefore. What to do? Go to thehospital? Before I heard anythingmore about the case, I told herthat if she thought she was hav-ing an allergic reaction to a stingshe should go to the doctor im-mediately. She persisted in tell-ing the story. It seemed obviousthat she was not having an aller-gic reaction. It had happenedthe day before. There was noswelling or systemic effects.Wheal and flare are commoninitial signs of fire ant stings;pustular lesions are normal 24hours later (Figures 1 and 2).
Figure 1Typical fire ant lesions approximately 30 min after sting(reprinted from Lab. Med. 25, 366, 1994, copyright1994 by the American Society of Clinical Pathologists,with permission).
I. ALLERGY TO STINGS OR BITESA. Introduction and Medical Significance
People encounter insects in almost everything they do. Inevitably, thousands of personsare stung or bitten daily. For most people, local pain, swelling, and itching are the onlyeffects, and they gradually abate. For others, life-threatening allergic reactions occur.More people die each year in the U.S. from bee and wasp stings than from snake bites.1
Why? Probably because more people are exposed to stinging insects than to poisonoussnakes; therefore, some individuals become hypersensitive to such stings. Consider fireants. They are so numerous and widespread in the southern U.S. that all persons inthat area are at high risk of being stung. In a 1988 survey, 2,022 physicians in 13southern states reported treating 20,755 patients for reactions to fire ant stings. Theseincluded 13,139 (63%) patients who had local reactions, 395 (2%) who were treated forcellulitis or sepsis, and 413 (2%) who suffered anaphylactic shock.2

13
Allergy to Arthropods and their Venoms
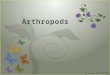
Comment: Fire ants are responsible for thousands of human stings in the southern U.S. eachyear. Whenever their mound is disturbed, they boil out aggressively looking for the intruder.There are generally three types of reactions to stings: normal, large local, and systemic.Large local reactions can occur for several days after a sting, but are characterized byextensive swelling over a large area. For example, if a person is stung on the hand, he orshe may swell past the elbow. A systemic reaction — generalized urticaria, angioedema,anaphylaxis — usually begins 10 to 20 min after the sting. However, very rarely, symptomsmay not start for many hours. In this case (above), the woman may have confused herterminology. Sometimes people trying to describe a bite or sting site use words that havetotally different meanings to a health care provider.
(Adapted from Lab. Med. 25, 366, 1994, © 1994 by the American Society of ClinicalPathologists, with permission.)
Figure 2Pustules resulting from fire ant stings, 24 h after sting (photo courtesy Ralph Turnbo).
Stinging insects in the order Hymenoptera such as bees, wasps, and ants can killpeople in two ways: by the sheer numbers of stings producing toxic effects, and bythe allergic reactions in susceptible individuals. It generally takes 500 or more bee stingsto kill an individual by the toxic effects of the venom alone (see Chapter 1 fordiscussion of direct effects), but as few as one sting may prove fatal for the person withbee sting allergy.
Numerous arthropods can cause allergic reactions in persons by their stings,including various wasps, bees, ants, scorpions, and even caterpillars. However, theones most commonly involved are paper wasps, yellowjackets, honey bees, and fireants (see the sections in Part III for discussions of each of these groups).
In addition to stings, bites from some arthropods may produce allergic reactions,including anaphylaxis and other systemic effects (Figure 1). However, systemic hyper-sensitivity reactions to arthropod bites are much less common (almost rare) than thoseresulting from stings. The groups most often involved in producing systemic effects by

14
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
their bites are the kissing bugs (genus Triatoma), black flies, horse flies, and deer flies.3
Mosquitoes, to a lesser extent, are involved, with several reports in the literature of largelocal reactions, urticaria, angioedema, headache, dizziness, lethargy, and even asthma.3a
Tick bites may sometimes cause extensive swelling and rash. Ticks reported to do soare the hard ticks, Ixodes holocyclus and Amblyomma triguttatum, and the soft tick,Ornithodoros gurneyi. Arthropod saliva from biting insects contains anticoagulants,enzymes, agglutinins, and mucopolysaccharides. Presumably, these components ofsaliva serve as sensitizing allergens.
Normal reaction to stings or bites. A normal reaction to one or a few stings involvesonly the immediate area of the sting and appears within 2 to 3 min. Usually, it consistsof redness, itching, swelling, pain, and formation of a wheal at the site. The reactionusually abates within 2 h or so. If a person is stung by numerous hymenopterans, theacute toxic reaction (nonallergic) resulting from large amounts of venom can be severe.Murray4 describes a man who was stung over 2,000 times by bees and exhibited signsof histamine overdosage — severe headache, vomiting, diarrhea, and shock.
Severe local (or large local) reaction to stings or bites. Large local reactions arecharacterized by painful, pruritic swelling of at least 5 cm in diameter (but stillcontiguous with the sting site), and may involve an entire extremity. Large localreactions usually peak within 48 h and last as long as 7 days. Most patients with largelocal reactions have detectable venom-specific IgE antibodies. Large local reactionshave not been shown to increase the risk for anaphylaxis upon subsequent stings.Venom immunotherapy has been shown to be effective for preventing large localreactions to some hymenopterans, but is rarely required.
Systemic reaction to stings or bites. Systemic allergic reactions produce symptomsin areas other than the sting site. Thus, the allergic person may have both the local pain,
Figure 1Hypersensitivity reaction to numerous mosquito bites (photo courtesy Dr. Elton Hansens,with permission.)

15
Allergy to Arthropods and their Venoms
wheal, and itching from the sting, as well as generalized pruritus, urticaria, angioedema,respiratory difficulty, syncope, stridor, gastrointestinal distress, and hypotension (Table1). Systemic reactions usually begin with widespread cutaneous symptoms such asangioedema or urticaria. These skin manifestations may be the extent of the systemicreaction, or there may be progression to a generalized pruritus, widespread edema, andupper respiratory distress. In severe reactions, shock begins to develop with a rapidpulse and low blood pressure. The victim may feel a constriction in his throat and chest,and breathing continues to become difficult. Sometimes, a severe allergic reactionresults in anaphylactic shock and death within 10 or 15 min, although 20 to 30 min ismore common. In a study of 641 deaths from Hymenoptera stings in the U.S.,respiratory conditions accounted for 53% of the deaths.5 Autopsies revealed character-istic laryngeal, epiglottal, and pulmonary edema, along with both serous and mucoidsecretions.
Cross-reactivity among venoms. There seems to be a consensus that considerablecross-reactivity occurs among the vespid venoms (yellowjacket, paper wasp, andhornet), meaning that a person sensitized to one vespid venom could have a seriousreaction to a sting from other members of the group.6 Limited studies have indicatedcross-reactivity between honey bee and bumble bee venoms. Generally, however,honey bee allergic individuals do not exhibit cross-reactivity to vespid venoms (note:there are exceptions — some individual patients have shown cross-reactivity betweenhoney bee and yellowjacket venoms6). Immunologic cross-reactivity among fire antvenoms and some vespid venoms has been demonstrated but there is no evidence ofcross-reactivity in the clinical setting.
B. Management and Treatment
Normal reaction. Treatment for a normal or mild local reaction involves the use ofice packs and/or pain relievers to minimize pain and washing the wound to lessen thechances of secondary infection. Oral antihistamines may help counteract the effects ofhistamine (IgE mediated or not) in the affected tissues resulting from certain venomcomponents. Alexander7 recommended calamine products (Caladryl® is often used inthe U.S.).
The use of meat tenderizer containing the enzyme papain is of no therapeutic value.8
The theory behind the use of papain is valid because in vitro incubation of papain andvenom leads to destruction of the venom activity. However, in a laboratory experiment
Table 1Signs and Symptoms of Anaphylaxis
General Apprehension, uneasiness, weaknessCutaneous Erythema, pruritus, urticaria, angioedemaGastrointestinal Abdominal cramps, vomiting, diarrheaGenitourinary Urinary or fecal incontinence, uterine crampsRespiratory Chest tightness, cough, dyspnea, stridor, wheezingCardiovascular Dizziness, lightheadedness, syncope, hypotension
From Monograph on Insect Allergy, Second Edition, Levine, M. I. and Lockey, R. F.,Eds., American Academy of Allergy and Immunology, 1986. With permission.

16
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
with mice, there was no marked inhibition of lesion development in mice receivingpapain or Adolph’s® meat tenderizer by intradermal injection or topical application.9
Severe local (or large local) reaction. In the case of a large local reaction charac-terized by considerable swelling and tenderness around the sting site, rest and elevationof the affected limb may be needed. The patient should avoid exercise since it mayexacerbate the swelling. If the sting site is on or near the throat, nose, or eye area, orif there is widespread swelling, patients should definitely seek medical care. Treatmentinvolves analgesics, topical high potency steroids, oral antihistamines to relieve itching,and systemic steroids (such as prednisone) if swelling is severe.10 Superimposedinfections such as cellulitis or septicemia, unusual with hymenoptera envenomation,require aggressive treatment that may include hospitalization, incision, and systemicantibiotics.11 If the offending arthropod is a biting fly such as a mosquito, cutaneousreactions may even be prevented by use of high potency topical or oral antihistamines.One study demonstrated that persons who had previously had dramatic cutaneousreactions to mosquito bites, when taking cetirizine (Zyrtec®), had a 40% decrease in thesize of the wheal response at 15 min and the size of the bite papule at 24 h.12
Systemic reaction. Persons who experience a generalized allergic reaction (evenmild) may be at risk of a severe reaction and possible death upon the next sting (days,weeks, or months later). In the event of a systemic reaction, the most important aspectof care is for that person to get to an emergency facility for immediate treatment. If theindividual has an epinephrine kit, it should be used. An ice pack on the sting site maydelay absorption of venom, and removal of a honeybee stinger may also reduce venomabsorption. However, people should be reminded that these measures should not delayseeking emergency treatment in any way.
Physicians often do several things to treat a severe allergic reaction. There may besome minor differences in procedures used (depending upon the reference consulted),but the immediate goal is the same — maintain an adequate airway and support theblood pressure. The American Academy of Allergy and Immunology published stepsfor the management of anaphylaxis (Table 2).13 The following is a modification (seeWasserman14) of suggestions made by Stafford et al.15 for treatment of severe reactionsto fire ant stings, which is fairly typical for the management of similar reactions to allHymenoptera stings:
An immediate subcutaneous injection of 0.3 to 0.5 ml of a 1:1,000 solution ofepinephrine (preferably intramuscularly in the lateral thigh) should be administered,and repeated, with blood pressure monitoring, at ten minute intervals if necessary.Intravenous epinephrine may be administered at a rate of 2 µg/min for treatmentof severe shock or cardiac arrest, but bolus administration should be avoided. Theairway must be established and maintained by using endotracheal intubation orcricothyrotomy, if necessary. Intravenous fluids should be given to replenish de-pleted intravascular volume in the treatment of anaphylactic shock. Norepinephrine,H1 and H2 blocking agents may be required. Systemic corticosteroids and both typesof antihistamines may prevent recurrent or biphasic anaphylaxis. Glucagon isappropriate for patients on beta blockers.
Administration of oxygen (see Table 2) may be needed to minimize development ofhypoxia, which by itself may contribute to vascular collapse and cerebral edema. Also,wheezing that is refractory to repeated doses of epinephrine can be treated with

17
Allergy to Arthropods and their Venoms
Table 2Management of Anaphylaxis
General therapeutic measuresAssessmentEpinephrine (intramuscularly in the lateral thigh)Glucagon if on beta blockers
Specific interventionsAirway obstruction
Upper airway obstructionSupplemental inspired oxygenExtension of the neckOropharyngeal airwayEndotracheal intubationCricothyrotomy
Lower airway obstructionSupplemental inspired oxygenInhaled beta agonistsConventional treatment for status asthmaticus
HypotensionPeripheral vascular defects
Trendelenberg positionIntravenous isotonic sodium chlorideVasopressors if required (dopamine, intravenous
epinephrine, norepinephrine)Diphenhydramine plus cimetidine
Cardiac dysfunctionConventional therapy of dysrhythmiasDiphenhydramine plus cimetidine
Suppression of persistent or recurrent reactionsDirect observation for at least 12 h after anaphylaxisSystemic glucocorticoids
Formulate plan to minimize future reactions
Educate in insect avoidance techniques
Medic-Alert® tag
Self-injectable epinephrine
Venom immunotherapy
Adapted from Monograph on Insect Allergy, Second Edition, Levine,M. I. and Lockey, R. F., Eds., American Academy of Allergy andImmunology, 1986. With permission. Modified with informationin Yates et al.10

18
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
continuously nebulized beta agonists such as albuterol.16 However, the administrationof epinephrine is the most important element of treatment. It acts to suppress mediatorrelease from mast cells and basophils and reverses many of the end organ responsesto mediators of anaphylaxis. Complete resolution of the clinical manifestations ofanaphylaxis often occurs within minutes. The critical and immediate use of epinephrineis why some people who are allergic to bee or wasp stings carry sting kits containingsyringes loaded with the drug. At least two preloaded syringes are available (Ana-Kit,®
Miles Labs, Spokane, WA, and Epi-Pen,® Center Labs, Port Washington, NY) in bothadult and pediatric versions. In case of a sting, the allergic person can give himself aninjection that may very well save his life. Alexander7 recommends that one or two closeand reliable relatives of the allergic person should also be carefully instructed in thecorrect use of the kit, and especially the administration of epinephrine.
It is important to note that just because an individual uses the epinephrine injectionin case of a sting does not mean he should avoid prompt medical treatment. It is stillvital to get to a hospital or physician as quickly as possible. The sting kits or loadedsyringes are meant only to stave off fulminating symptoms long enough for the victimto get to a hospital. This is especially important in light of the fact that sometimes thereis a second phase of anaphylaxis 4 to 10 h after the initial reaction.17
Insect sting kits and/or auto injector syringes must be prescribed by a physician. Anyperson who has suffered even mild symptoms of an allergic reaction should becounseled to obtain a kit and keep it available wherever there is a chance of beingstung.
It might also be a good idea for all insect-allergic persons to wear a Medic-Alert®
(Medic-Alert Foundation, Turlock, CA) tag or card to alert medical personnel of theirallergy in case they lose consciousness.
Long-term management of insect sting allergy. Sting-allergic patients and theirphysicians should also think of long-term management of the problem. There is alwaysthe possibility of being stung again. Immunotherapy is a procedure used by allergiststo increase the allergic person’s tolerance to insect venom. The process works bystimulating serum venom-specific IgG and decreasing titers of serum venom-specificIgE. It is accomplished by numerous injections of venom from offending insects (orfrom extracts from whole bodies in the case of fire ants). Initially, the injections are veryweak. The dosages are gradually increased over time until the patient can tolerateapproximately the same amount of venom as in a sting. Then, the patient is kept ona maintenance dose to keep up that tolerance. Generally, however, 3 to 5 years oftreatment is sufficient.18 Graft19 has shown that immunotherapy is highly effective andsafe for prevention of future systemic reactions to Hymenoptera stings. In a study20 of65 patients on a maintenance dose of fire ant whole body extract, only 1 (2%) patientof 47 who were subsequently stung by fire ants had an anaphylactic reaction.Physicians deciding whether or not to initiate venom immunotherapy base theirdecision upon clinical history and results of venom skin tests and venom-specificradioallergosorbent tests (RASTs) (see also Table 3). Adults with a history of systemicreaction and a positive venom skin test or RAST should receive immunotherapy.21 Forsome persons, it may seem too expensive and inconvenient to go through withimmunotherapy, but it is a way for persons with insect allergy to lead a relativelynormal life.

19
Allergy to Arthropods and their Venoms
C. Avoidance of Offending Insects
Here are some ways for both allergic and nonallergic individuals to avoid stinginginsects.
1. Each year, have someone eliminate bee, wasp, and fire ant nests around thehome — preferably early in the summer before the nests get large. Pest controloperators will usually do this for a fee. If the homeowner wishes to accomplishnest elimination, he or she should wait until night or a very cool morning tominimize the threat of stings (persons who are insect sting allergic should notattempt this). If nest elimination is accomplished at night, a flashlight shouldnot be used unless a red filter is used. Bees and wasps will zero in on the beam.
2. Wear light or khaki-colored clothing when outside during warm weather.These colors are less attractive than dark colors. Be careful to avoid bright-colored floral patterned clothes.
3. While driving a car during the warm weather months, car windows should beclosed and the air conditioning used.
4. Do not go barefoot during the warm weather months. Bees are often foundfeeding on flowers at ground level, and fire ants have numerous feeding trails(even long distances from their mounds).
Table 3Selection of Patients for Venom Immunotherapy
Sting Reaction ST/RASTa Venom Immunotherapy
Systemic, non-life-threatening (child) immediate, + or – Nogeneralized, confined to skin (urticaria,angioedema, erythema, pruritus)
Systemic, life-threatening (child) immediate, + Yesgeneralized, may involve cutaneous symptoms,but also has respiratory (laryngeal edema orbronchospasm) or cardiovascular symptoms(hypotension/shock)
Systemic (adult) + Yes
Systemic – No
Large local + or – No>2 in. in diameter>24 h in duration
Normal + or – No<2 in. in diameter<24 h in duration
From Monograph on Insect Allergy, Second Edition, Levine, M. I. and Lockey, R. F., Eds., American Academyof Allergy and Immunology, 1986. With permission.a Venom skin test or venom-specific radioallergosorbent test.

20
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
5. Wear long pants and long sleeves when working outdoors.6. Wear gloves when gardening. A lot of people are stung on the hand while
picking vegetables.7. Avoid the use of scented sprays, perfumes, shampoos, suntan lotions, and
soaps when working outdoors.8. Avoid clover patches, gardens full of blossoms, blossoming trees, fields of
goldenrod, and other areas with concentrations of bees, wasps, or ants.9. Be cautious around rotting fruit, garbage cans, and littered picnic areas,
especially in the late summer and early fall. Yellowjackets often feed in thoseareas.
10. Avoid drinking sodas or eating popsicles, ice-cream cones, watermelons, andother sweets outdoors. This may attract bees and yellowjackets.
11. If you see a bee or wasp nest, or encounter a nest before the insects becomeagitated, retreat slowly. Do not panic. However, once the nest is disturbed, itis best to run immediately even though the hymenopterans are attracted tomovement.
OFTEN ASKED QUESTION
MY DOCTOR SAID I WAS ALLERGIC TO KISSING BUGS.HOW CAN THAT BE SINCE THEY DON’T STING?
Most people are aware that you can become sensitized to venoms from many differentstinging insects, leading to allergic reactions ranging from mild to severe (includinganaphylactic shock). However, there is confusion when it comes to allergic reactions tobites. Arthropod bites may produce allergic reactions as well, though rare, presumably aresult of hypersensitivity to salivary components secreted during the biting process. Arthro-pod saliva contains anticoagulants, enzymes, agglutinins, and mucopolysaccharides whichmay serve as sensitizing allergens. Reactions have occurred following bites by manydifferent types of arthropod but most commonly from bites by Triatoma (kissing bugs), horseand deer flies, and mosquitoes.
Triatoma allergy. Kissing bugs — so named because of the nasty habit of taking abloodmeal from the face — belong to the insect family Reduviidae (hence the sometimesused moniker “reduvid bugs”), but specifically, the subfamily Triatominae. Within thissubfamily, some (not all) species fall under the genus Triatoma — triatomines may also bein other genera. There are at least 10 Triatoma species found in the United States, but onlyabout six of these are likely to be encountered.1,2 Allergic reactions have been reportedfrom bites by five species (T. protracta, T. gerstaeckeri, T. sanguisuga, T. rubida, and T.rubrofasciata.3), although in the U.S., T. protracta is the species most often reported inallergic reactions.4,5 Kissing bug bites may be painless, leaving a small punctum withoutsurrounding erythema, or cause delayed local reactions appearing like cellulitis. Anaphy-lactic reactions include itchy, burning sensations, respiratory difficulty, and other typicalsymptoms of anaphylaxis.2
Triatoma bugs feed on vertebrate hosts such as bats, other small and medium-sizedmammals, birds, and humans. Accordingly, the pests are often found in association withtheir host nest or habitation — caves, bird nests, rodent burrows, human houses, etc. For

21
Allergy to Arthropods and their Venoms
II. ALLERGY — IRRITATION CAUSED BY CONSUMING ORINHALING INSECT OR MITE PARTS
A. Introduction and Medical Significance
Several insect or mite species (or their body parts) may cause irritation and/or allergicreactions when inhaled and, less commonly, when ingested. House dust mites,Dermatophagoides farinae (and D. pteronyssinus), several species of mayflies andcaddisflies, some nonbiting chironomid midges, and cockroach body parts or feces arethe major inhalant offenders. As these arthropods die, their decaying cast skins becomepart of the environmental dust. In addition, insect emanations such as scales, antennae,feces, and saliva are suspected as being sources of sensitizing antigens. Compoundingthe problem, the average child spends 95% of his or her time indoors, providing plentyof time for sensitization. As for the digestive route, cockroach vomit, feces, and piecesof body parts or shed skins contaminating food are most often the cause of insectallergy via ingestion.
example, T. protracta is found in woodrat nests. Bugs periodically fly away from the nestsof their hosts (nocturnal cyclical flights) and may be attracted to lights at dwellings,subsequently gain entrance, and try to feed. Some species are able to colonize houses; theyseem especially prolific in sub-standard structures with many cracks and crevices, mudwalls, thatch roofs, etc.
Protection from Triatoma bites. Personal protection measures from kissing bugs involveavoidance (if possible) — such as not sleeping in adobe or thatched-roof huts in endemicareas — and exclusion methods such as putting up bed nets.6 Domestic or peri-domestickissing bug species (Mexico, Central and South America) may be controlled by properconstruction of houses, sensible selection of building materials, sealing of cracks andcrevices, and precision targeting of insecticides within the home. In the U.S., preventionof bug entry into homes may involve outdoor light management (i.e., lights placed awayfrom the house, shining back toward it, instead of lights on the house), and efforts to findand seal entry points around the home.
REFERENCES
1. Schofield, C. J. and Dolling, W. R., Bedbugs and kissing-bugs, in Medical Insects andArachnids, Lane, R.P. and Crosskey, R.W., Eds., Chapman and Hall, London, 1993, pp.483-516.
2. Rohr, A. S., Marshall, N.A., and Saxon, A., Successful immunotherapy for Triatomaprotracta induced anaphylaxis, J. Allergy Clin. Immunol., 73, 369-375, 1984.
3. Ryckman, R. E., Host reactions to bug bites: a literature review and annotated bibliog-raphy, Calif. Vector Views, 26, 1-23, 1979.
4. Marshall, N., Liebhaber, M., Dyer, Z., and Saxon, A., The prevalence of allergicsensitization to Triatoma protracta in a southern California community, J. Med. Entomol.,23, 117-124, 1986.
5. Marshall, N.A. and Street, D.H., Allergy to Triatoma protracta I. Etiology, antigenpreparation, diagnosis, and immunotherapy, J. Med. Entomol., 19, 248-252, 1982.
6. Goddard, J., Kissing bugs and Chagas’ disease, Infect. Med., 16, 172-175, 1999.

22
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Reactions via the respiratory route. Until the mid-1960s physicians simply diag-nosed certain people as being allergic to house dust. Subsequently, Dutch researchersmade the first link between house dust allergy and house dust mites22,23 (see alsoChapter 24). The mites commonly infest homes throughout much of the world andfeed on shed human skin scales, mold, pollen, feathers, and animal dander. They arebarely visible to the naked eye and live most commonly in mattresses and otherfurniture where people spend a lot of time. The mites are not poisonous and do notbite or sting, but they contain powerful allergens in their excreta, exoskeleton, andscales. For the hypersensitive individual living in an infested home, this can meanperennial rhinitis, urticaria, eczema, and asthma, often severe. House dust mites canalso be triggers for atopic dermatitis.24
Recent evidence indicates that early and prolonged exposure to inhaled allergens(such as dust mites and cockroaches) plays an important role in the development ofboth bronchial hyperreactivity and acute attacks of asthma. Accordingly, bronchialprovocation with house dust mite or cockroach allergen can increase nonspecific
Figure 3Magnified view of hairs from dermestid beetle.Left: hastisetae (175×); right: spicisetae (400×).(From: USAF Medical Service Digest, courtesyMaj. Tom Lillie.)
Figure 2Insect larvae often collectivelytermed “maggots”: fly larva (A), flealarva (B), mealworm larva (C),moth larva (D), and weevil larva(E). (From U.S. DHEW, PHS, CDC,pictorial keys.)

23
Allergy to Arthropods and their Venoms
Figure 4Warehouse beetle larvae (Coleoptera: Dermestidae). Left:dorsal view; right: ventral view. (From: USAF MedicalService Digest, courtesy Maj. Tom Lillie.)
reactivity for days or weeks. So, the root cause of asthma onset is sometimes the resultof exposure to house dust mites or cockroaches. Asthma-related health problems aremost severe among children in inner-city areas. It has been hypothesized that cock-roach-infested housing is at least partly to blame. In one study of 476 asthmatic inner-city children, 50.2% of the childrens’ bedrooms had high levels of cockroach allergenin dust.25 That study also found that children who were both allergic to cockroachallergen and exposed to high levels of this allergen had 0.37 hospitalizations a year,as compared with 0.11 for other children.25
Mayflies and caddisflies are delicate flies that spend most of their lives underwateras immatures. They emerge as adults in the spring and summer in tremendousnumbers, are active for a few days, and then die. They do not bite or sting, but bodyparticles from mass emergence of these insects have been well documented as causingallergies.
Nonbiting midges in the family Chironomidae have also been implicated as causesof insect inhalant allergy. A greater prevalence of asthma has been demonstrated inAfrican populations seasonally exposed to the “green nimitti” midge, Cladotanytarsus

24
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
CASE HISTORY
BUGS IN PEANUT BRITTLE
A woman brought in a peanut brittle bar purchased at a grocery store, and upon eating it,said she observed bugs in it. She claimed that she immediately threw up and was very ill.She asked that I identify the specimens and document the event for her lawyer. The fooditem was examined and found to contain larvae and adults of the Indian meal moth, acommon food pest (Figure 1). I wrote a letter detailing the product brought in (lot numberand other package details), and species identification of the insect and its habits. I alsomade statements to the effect that the insects in question would not cause immediatenausea, and that I could not verify that the food product was infested at time of purchase.
Comment: When people bring in opened food products claiming that the product wasinfested with bugs upon purchase, medical personnel should not say or write things thatconfirm the allegation. Actual physical illness is usually not the issue — these cases almostalways result in lawsuits. Medical personnel generally have no objective information abouthow long the product had been at the client’s home, or how it had been treated,intentionally or otherwise.
(Adapted from Lab. Med. 25, 371, 1994, © 1994 by the American Society of ClinicalPathologists, with permission.)
Figure 1Adults and larval Indian meal moths removed from peanut brittle (reprinted from Lab.Med. 25, 366, 1994, copyright 1994 by the American Society of Clinical Pathologists, withpermission).

25
Allergy to Arthropods and their Venoms
lewisi.26,27 Kagen et al.28 implicated Chironomus plumosus as a cause of respiratoryallergy in Wisconsin.
In areas heavily infested with cockroaches, constant exposure to house dustcontaminated with cockroach allergens is unavoidable. Accordingly, many peoplebecome sensitized and develop cockroach allergy. In a study in Thailand, 53.7% of 458allergic patients reacted positively to cutaneous tests to cockroach body parts.29 In astudy in New York City the figure was even higher; over 70% of almost 600 allergicpatients routinely visiting seven hospitals reacted positively to cockroach antigen.30
Reactions via the digestive tract. Adult beetles and larval flies, moths, or beetles,as well as their cast skins, often contaminate food and may be responsible for irritationand/or allergic responses through ingestion. Physicians are often confronted withparents worried about their children who have inadvertently eaten a “maggot” in theircereal, candy bar, or other food product. These “maggots” may be moth, beetle, or flylarvae (Figure 2), and generally cause no problems upon ingestion. However, somebeetle larvae (primarily the family Dermestidae) found in stored food products possessminute barbed hairs (Hastisetae) and slender elongate hairs (Spicisetae) that apparentlycan cause enteric problems31 (Figures 3 and 4). The symptoms experienced afteringesting dermestid larvae have been attributed to mechanical action of the hastisetaeand spicisetae resulting in tissue damage or irritation in the alimentary tract. Clinicalsymptoms include diarrhea, abdominal pain, and perianal itch.32,33
Cockroaches seem to be most often involved in allergic responses. Allergens arepresent in cockroach feces, which can be inadvertently ingested in heavily infestedareas. Other allergens are present in cockroach vomit, which can be introduced intofoodstuffs.
B. Management and Treatment
House dust mites. Management of house dust mite allergy may be achieved byimmunotherapy, as well as encasing mattresses with plastic, keeping mattresses free ofdust, using a synthetic pillow, keeping airborne dust levels low, use of tile or woodfloors instead of carpet, and efficient and frequent housecleaning. For vacuuming,double-thickness filters or HEPA filters are needed for maximum results. The house-cleaning tasks are best accomplished by a nonallergic person or family member. Sincethe mites require a relative humidity of 60% to flourish, humidity control — byincreasing ventilation or using a dehumidifier — will limit mite numbers in a house.Recent studies have demonstrated the effectiveness of benzyl benzoate and/or tannicacid for the treatment of mites in carpets. However, results are equivocal and tannicacid may cause color changes in carpets. Further, even with the use of acaricides,airborne allergen loads may not be reduced below sensitization levels. One thing thatdoes seem to show promise is the combined use of heat and steam treatment of homefurnishings. One study showed that a single treatment of home furnishings reducedmite allergen load to below the risk level for sensitization and improved the asthmaticpatients’ BHR by fourfold.34
Cockroaches. Cockroach inhalant allergy may be managed by symptomatic therapy,immunotherapy with cockroach extracts, and intense sanitation and pest controlmeasures to reduce roach populations. Again, killing cockroaches may not eliminateantigen from the dwelling. The shelf life of cockroach allergen is several years. It isbetter to live in a dwelling that has never had a cockroach infestation. Treatment ofother insect inhalant allergy also includes avoidance and symptomatic therapy. Where

26
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
avoidance is impossible or impractical because of residential or occupational exposure,antihistamines, inhaled steroids, beta-2 agonists, or cromolyn sodium may be indicated.
Food Contamination. To prevent allergic reactions resulting from ingesting insectparts or fluids, sanitation is the answer. Food preparation areas should be thoroughlycleaned and sanitized prior to cooking, even if the areas “look” clean. Cockroaches mayhave contaminated these surfaces during the night. Leftovers should be properlycovered and/or refrigerated to prevent cockroach feeding. Cereal, nuts, candy, flour,and corn meal should be examined before consumption for evidence of insectinfestation such as small beetles or weevils. Staples such as flour, meal, and cereals canbe placed in tight-fitting plastic containers to prevent insect infestation.
Both insect inhalant and sting allergy, like any other allergy, can usually beeffectively managed and treated. By avoiding the offending types or species involved,practicing good sanitation (in the case of inhalant or ingestant allergies), and applyingappropriate immunotherapy or antihistamine therapy, allergic persons should be ableto conduct their lives in a relatively normal manner.
REFERENCES1. Parrish, H. M., Analysis of 460 fatalities from venomous animals in the U.S., Am. J. Med.
Sci., 245, 129, 1963.
2. Stafford, C. T., Hutto, L. S., Rhoades, R. B., Thompson, W. O., and Impson, L. K., Importedfire ants as a health hazard, S. Med. J., 82, 1515, 1989.
3. Hoffman, D. R., Allergic reactions to biting insects, in Monograph on Insect Allergy, 2nded., Levine, M. I. and Lockey, R. F., Eds., American Academy of Allergy Immunology,Milwaukee, WI, 1986, chap 14.
3a. Gluck, J. C., Asthma from mosquito bites: a case report, Ann. Allergy, 56, 492, 1986.
4. Murray, J. A., A case of multiple bee stings, Cent. Afr. J. Med., 10, 249, 1964.
5. Levine, M. I. and Nall, T. M., Pathologic findings in Hymenoptera deaths, in Monographon Insect Allergy, 2nd ed., Levine, M. I. and Lockey, R. F., Eds., American Academy ofAllergy Immunology, Milwaukee, WI, 1986, chap 4.
6. Richman, P. G. and Baer, H., Hymenoptera venoms: composition, immunology,standardization, stability, in Monograph on Insect Allergy, 2nd ed., Levine, M. I. andLockey, R. F., Eds., American Academy of Allergy Immunology, Milwaukee, WI, 1986,chap 2.
7. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 10.
8. Ross, E. V. Jr., Badame, A. J., and Dale, S. E., Meat tenderizer in the acute treatment ofimported fire ant stings, J. Am. Acad. Dermatol., 16, 1189, 1987.
9. Agostinucci, W., Cardoni, A. A., and Rosenberg, P., Effect of papain on bee venomtoxicity, Toxicon, 19, 851, 1981.
10. Yates, A. B., Moffitt, J. E., and deShazo, R. D., Anaphylaxis to arthropod bites and stings,Immunol. Allerg. Clin. North America, 21, 635, 2001.
11. Frazier, C. A., Anaphylactic response to insect stings, Compr. Ther., 2, 67, 1976.
12. Reunala, T., Brummer-Korvenkotio, H., Karppinen, A., Coulie, P., and Palosuo, T.,Treatment of mosquito bites with cetirizine, Clin. Exp. Allergy, 23, 72, 1993.
13. Levine, M. I. and Lockey, R. F., Eds., Monograph on Insect Allergy, 2nd Edition, AmericanAcademy of Allergy Immunology, Milwaukee, WI, 1986.
14. Wasserman, S. I., Anaphylaxis, in Rich’s Clinical Immunology Principles and Practice, 2nded., Rich, R. R., Fleisher, W. T., Kotzin, B. L., Schroeder, H. W., Jr., Eds., Mosby, New York,2001, p. 46.7.

27
Allergy to Arthropods and their Venoms
15. Stafford, C. T., Hoffman, D. R., and Rhoades, R. B., Allergy to imported fire ants, S. Med.J., 82, 1520, 1989.
16. Kemp, S. F. and deShazo, R. D., Anaphylaxis and anaphylactoid reactins, in Allergens andAllergen Immunotherapy, 2nd ed., Lockey, R. F. and Bukantz, S. C., Eds., Marcel Dekker,New York, p. 544.
17. Sullivan, T. J., Treatment of reactions to insect stings and bites, in Monograph on InsectAllergy, 2nd ed., Levine, M. I. and Lockey, R. F., Eds., American Academy of AllergyImmunology, Milwaukee, WI, 1986, chap 7.
18. Reisman, R. E., Insect stings, N. Engl. J. Med., 331, 527, 1994.
19. Graft, D. F., Venom immunotherapy for stinging insect allergy, Clin. Rev. Allergy, 5, 149,1987.
20. Hylander, R. D., Ortiz, A. A., Freeman, T. M., and Martin, M. E., Imported fire antimmunotherapy: effectiveness of whole body extracts, J. Allergy Clin. Immunol., 83, 232,1989.
21. Graft, D. F. and Schuberth, K. C., Indications for venom immunotherapy, in Monographon Insect Allergy, 2nd ed., Levine, M. I. and Lockey, R. F., Eds., American Academy ofAllergy Immunology, Milwaukee, WI, 1986, chap 8.
22. Spieksma, F. Th. M., The house dust mite, Dermatophagoides pteronyssinus, producer ofhouse dust allergin, Thesis, University of Leiden, Netherlands, 1967, 65.
23. Spieksma, F. Th. M. and Spieksma-Boezeman M. I. A., The mite fauna of house dust, withparticular reference to the house dust mite, Dermatophagoides pteronyssinus, Acarologia,9, 226, 1967.
24. Cameron, M.M., Can house dust mite triggered atopic dermatitis be alleviated usingacaricides? Br. J. Dermatol., 137, 1, 1997.
25. Rosenstreich, D.L., Eggleston, P., Kattan, M., Baker, D., Slavin, R.G., Gergen, P., Mitchell,H., McNiff-Mortimer, K., Lynn, H., Ownby, D., and Malveaux, F., The role of cockroachallergy and exposure to cockroach allergen in causing morbidity among inner-citychildren with asthma, New Engl. J. Med., 336, 1356, 1997.
26. Gad El Rab, M. O. and Kay, A. B., Widespread immunoglobulin E-mediated hypersensitivityin the Sudan to the “green nimitti” midge, Cladotanytarsus lewisi, J. Allergy Clin.Immunol., 66, 190, 1980.
27. Kay, A. B., MacLean, C. M., Wilkinson, A. H., and Gad El Rab, M. O., The prevalence ofasthma and rhinitis in a Sudanese community seasonally exposed to a potent airborneallergen, the “green nimitti” midge, Cladotanytarsus lewisi, J. Allergy Clin. Immunol., 71,345, 1983.
28. Kagen, S. L., Yunginger, J. W., and Johnson, R., Lake fly allergy: incidence of chironomidsensitivity in an atopic population, J. Allergy Clin. Immunol., 73, 187, 1984.
29. Choovivathanavanich, P., Insect allergy: antigenicity of cockroach and its excrement, J.Med. Assoc. Thailand, 57, 237, 1974.
30. Cornwell, P. B., The Cockroach, Vol. 1., Hutchinson and Co., London, 1968, chap. 13.
31. Lillie, T. H. and Pratt, G. K., The hazards of ingesting beetle larvae, USAF Med. Service Dig.,31, 32, 1980.
32. Okumura, G. T., A report of canthariasis and allergy caused by Trogoderma (Coleoptera:Dermestidae), Calif. Vector Views, 14, 19, 1967.
33. Jupp, W. W., A carpet beetle larva from the digestive tract of a woman, J. Parasitol., 42,172, 1956.
34. Htut, T., Higenbotta, T. W., Gill, G. W., Darwin, R., Anderson, P. B., and Syed, N.,Eradication of house dust mite from the homes of atopic asthmatic subjects: a double blindstudy, J. Aller. Clin. Immunol., 107, 55, 2001.


29
Stings
CHAPTER 3
STINGS
TABLE OF CONTENTS
I. Introduction and Medical Significance ............................................................ 29
II. Pathology Produced by Arthropod Stings ...................................................... 30
III. Stinging Behavior .............................................................................................. 31
IV. Morphology of the Sting Apparatus ................................................................ 31
V. Venom Components and Activity ................................................................... 35
References ....................................................................................................................... 38
I. INTRODUCTION AND MEDICAL SIGNIFICANCE
As discussed in the first chapter, stings by venomous arthropods can produce directeffects in humans by the toxic action of the venom alone or indirect effects due toallergic reactions (Table 1). Direct toxic effects are very rare but may include cerebralinfarction, neuropathies (even optic), and seizures.1-3 In addition, secondary infectionmay arise from stings, especially if the lesion is scratched (Figure 1). The direct effectsof a sting can be mild such as pain, itching, wheal, flare, etc., or can be serious whennumerous stings are received and the large amount of venom injected produces toxiceffects. Small children are at a higher risk for developing severe toxicity due to theirsmaller body weight. One account of a toxic reaction in a child from massive hornetstings described clinical features such as coma, respiratory failure, coagulopathy, renalfailure, and liver dysfunction.4 But for most individuals, the risk of a severe reactionresulting from either a toxic or allergic mechanism is quite low. Lightning claims morelives annually in the U.S. than stinging arthropods,5 and adverse reactions to penicillinkill seven times as many.6
Many arthropods can sting, but several groups are notorious offenders. Parrish7
analyzed fatalities due to venomous animals in the U.S. from 1950 to 1959 and found

30
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
that 229 of 460 recorded deaths were due to the stings of yellowjackets, other wasps,ants, and bees. Honey bees, being essentially ubiquitous, accounted for a large portionof those numbers. In other countries, combined with these hymenopterans, scorpionscause significant mortality. One reference8 lists 20,352 deaths from scorpion stings inMexico alone during the periods 1940–49 and 1957–58. In Brazil, there are more than5,000 reported stings and 48 deaths from scorpions each year.9
II. PATHOLOGY PRODUCED BY ARTHROPOD STINGS
Alexander10 described a typical hymenopteran sting (excluding ants) as a central whitespot marking the actual sting site surrounded by an erythematous halo. The entire
Figure 1Secondary infection of fire ant sting lesion due to scratching.
Table 1Various Reactions to Insect Stings
Reactions Response Comments
Normal Local pain, itching, swelling Generally subsides in 2 hLarge local Extensive swelling Subsides in several daysAnaphylaxis Live-threatening shock, Immediate medical attention required
difficulty breathingToxic reactions Headache, vomiting, Nonallergic, caused by direct effect of
diarrhea, shock many stingsUnusual syndromes Serum sickness May result from multiple stings or sting
Vasculitis in/near a nerveNeuritisReversible renal diseases

31
Stings
lesion generally is a few square centimeters in area. He also reported an initial rapiddermal edema with neutrophil and lymphocyte infiltration. Plasma cells, eosinophils,and histiocytes appear later. Lesions produced by fire ant stings are characterized bya central wheal with surrounding erythema, followed by the development of a vesicle,and finally a pustule10 (see Color Figures 3-1 through 3-4). According to Caro et al.11
the pustules are thin-roofed, contain polymorphonuclear cells and lymphocytes after24 h, and eosinophils, plasma cells, polymorphonuclear cells, and lymphocytes after72 h. Of course, the histopathology of arthropod stings varies with the insect andwhether or not the victim has pre-exsting antibody to an insect venom. Most large localreactions reflect the presence of IgE antibody. deShazo et al.12 described such reactionsin detail in studies of fire ant stings. While the typical wheal and flare reactions followedby a sterile pustule were composed of a non-specific cellular infiltrate, the erythema-tous, indurated and pruritic large local reactions occurring in individuals with venom-specific IgE consisted of an eosinophil rich mixed cellular infiltrate with denselypolymerized fibrin. The fibrin gel structure is manifested by the edematous, induratedquality of these lesions which take 3 to 5 days to resolve.
III. STINGING BEHAVIOR
Most stinging wasps and some bees are solitary or subsocial insects, and they use theirstings primarily for subduing prey. This “offensive” use of stinging and venom by thesespecies rarely leads to human envenomization, except in a few cases of inadvertent ordeliberate handling of the specimens. These venoms generally only cause slight andtemporary pain to humans.
The social wasps, bees, and ants are a different story. They use the sting primarily asa defensive weapon, and their venom causes intense pain in vertebrates. Workers (sterile,female insects) of all these groups instinctively defend their nest. Figure 2 illustrates howquickly fire ants attack their victims. Encountering a single bee, wasp, or ant out foragingfor food is generally not dangerous and will not usually result in a sting. However,walking too near a nest will elicit rapid defensive stinging behavior by numerous guardbees, wasps, or ants. In yellowjackets, the numerical response is in proportion to theextent of the disturbance and the defensive flight is brief (1.5 to 5 min) and usuallyconfined to a radius of about 7 m around the nest.10
IV. MORPHOLOGY OF THE STING APPARATUS
In all stinging wasps, bees, and ants the stinger is a modified ovipositor, or egg-layingdevice, that may no longer function in egg laying. Accordingly, in the highly socialHymenoptera only a queen or other reproductive caste member lays eggs; the workersgather food, conduct other tasks, and can sting intruders.
A typical ovipositor (nonstinging) consists of three pairs of elongate structures, calledvalves, which can insert the eggs into plant tissues, soil, etc. One pair of the valvesmakes up a sheath and is not a piercing structure, whereas the other two pairs forma hollow shaft that can pierce substrate in order for the eggs to pass down through.Two accessory glands within the body of the female inject secretions through theovipositor to coat the eggs with a gluelike substance.

32
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
(B)
(A)
Figure 2How fast fire ants attack doll posed against tree. (A) 0 seconds; (B) 10 seconds.

33
Stings
Figure 2 (continued)How fast fire ants attack doll posed against tree. (C) 30 seconds.
(C)
For the stinging configuration, the ovipositor has several modifications to enable astinging function (Figures 3 and 4). The genital opening from which the eggs pass isanterior to the sting apparatus, which is flexed up out of the way during egg laying.Also, the accessory glands have been modified. One now functions as a venom glandand the other (the Dufour’s gland) is important in production of pheromones. Thevenom gland leads to a venom reservoir or poison sac, which may contain up to 0.1ml of venom in some of the larger hymenopterans.
The stinger itself is well adapted for piercing the skin of vertebrates. In the case ofyellowjackets there are two lancets and a median stylet that can be extended and thrustinto a victim’s skin (Figure 5). Penetration is not a matter of a single stroke, but insteadby alternate forward strokes of the lancets, sliding along the shaft of the stylet. The tipsof the lancets are slightly barbed (and actually recurved like a fishhook in the case ofhoney bees) so that they are essentially sawing their way through the victim’s flesh.Contraction of the venom sac muscles injects venom through the channel formed bythe lancets and shaft. The greatly barbed tip of the lancets in honey bees prevents thestinger from being withdrawn from vertebrate skin, thus the entire sting apparatus istorn out as the bee flies away. Other hymenopterans, on the other hand, can stingrepeatedly.

34
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 4Microscopic view of end of wasp abdomen showing sting apparatus.
Figure 3Cut away view of yellowjacket sting apparatus (from USDA Agri. Handbk. No. 552).

35
Stings
V. VENOM COMPONENTS AND ACTIVITY
Table 2 lists some of the active constituents of vespid wasp, honey bee, and fire antvenoms, adapted from Schmidt.13 Table 3 shows the common names of these allergensbased upon World Health Organization nomenclature. Venoms are highly complexmixtures of pharmacologically and/or biologically active agents. Since some venomsare similar, there may be cross-reactivity reactions in humans, but not always. Hista-mine is the most predominant low molecular weight component. Serotonin, dopamine,noradrenalin, and acetylcholine are also present. The amount of serotonin seems to bedirectly related to the painfulness of the sting. Melittin is a protein polypeptide toxinthat is a primary constituent of honey bee venom. It is a direct agent of hemolysis.Apamin is one of the smallest polypeptides known (molecular weight 2038). It is aneurotoxin and its interaction with the spinal cord is well established. MCD (mast-celldegranulating) peptide, as a mastocytolytic agent, is very effective in releasing hista-
Figure 5Lateral views of yellowjacket worker sting apparatus, retracted and extended during maximumthrust (from USDA Agri. Handbk. No. 552).

36
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Table 2Protein Composition of Selected Hymenoptera Venomsa
Honey bees Vespid wasps Fire Ants
EnzymesPhospholipase A1 - + +b
Phospholipase A2 10-12% -Phospholipase B 1% + +Hyaluronidase 1-2% + -Acid phosphatase 15 - +Alkaline Phosphatase + -Lipase - +Esterase + +Protease - + -
PeptidesHemolysins Melittin 40% +Mastolytic peptides MCD peptide 2% MastoparansNeurotoxins Apamin 3% +Antigen 5 - + +Kinins - +Group specific allergens + + +
aSymbols: + = present; - = absent; no symbol = not investigated.bSpecificity unknownAdapted from Schmidt, J.O., Clin. Exp. Allergy, 24, 511, 1994.
Table 3World Health Organization Nomenclature for SomeCommon Fire Ant, Vespid Wasp, and Bee Allergens
Arthropod Allergen Common Name
Fire ants Sol i I PhospholipaseSol i II —Sol i III Antigen 5 groupSol i IV —
Vespid wasps Dol m I Phospholipase A1
Dol m II HyaluronidaseDol m III Acid phosphataseDol m V Antigen 5
Honey bees Api m I Phospholipase A2
Api m II HyaluronidaseApi m III MelittinApi m IV Acid phosphatase
Adapted in part from Moffitt, J. E. and deShazo, R. D., Allergic and other reactions to insects,in Rich’s Clinical Immunology Principles and Practice, 2nd ed., Rich, R. R., Fleisher, W. T.,Kotzin, B. L., and Schroeder, H. W., Jr., Eds., Mosby, New York, 2001, p. 47.6.

37
Stings
mine. Interestingly, MCD peptide only comprises approximately 2% of bee venom butcan produce effects equal to that of melittin, comprising as much as 50% of bee venom.Kinins take an intermediary position between biogenic amines and high molecularweight compounds. The relative importance of kinins in envenomization is yet to beclarified. Phospholipase A is an enzyme that can attack structural phospholipidsresulting in damage to biological membranes, mitochondria, and other cellular constitu-ents. There are two types of phospholipase — A1 and A2 (see Table 3 for current namesfor these allergens). Phospholipase A2 is present in honey bee venom, whereas vespid(wasps, yellowjackets, and hornets) venoms contain phospholipase A1. Hyaluronidaseis a spreading factor that opens the way for other venom components to move throughhost tissues. It works by hydrolyzing hyaluronic acid, which resists the spread ofharmful substances through epithelial and connective tissue.
As for which of these venom components serve as allergens, honey bee allergens arephospholipase A2, hyaluronidase, acid phosphatase, and melittin. Allergens contained invespid venoms are phospholipase A1, hyaluronidase, and a protein called antigen 5.14
Imported fire ants (IFA) possess a venom of an alkaloid nature, which is apparentlythe first venom of animal origin recognized to be of this type. IFA venom exhibitspotent necrotoxic activity. About 95% of their venom consists of water insoluble 6-n-alkyl, or alkenyl, 2-methyl piperidines, which do not produce allergic reactions inpeople but are responsible for pain and pustule formation (Figure 6). The other portionof fire ant venom is an aqueous solution of proteins, peptides, and other smallmolecules that produces the allergic response in hypersensitive individuals. Of theproteins found, four allergens have been isolated (from Solenopsis invicta) — Sol i I,Sol i II, Sol i III, and Sol i IV.15,16 Some patients react to every combination of the four
Figure 6Pustules resulting from fire ant stings.

38
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
allergens.13 Sol i II, III, and IV are not immunologically related to bee or wasp venomproteins, so there is no cross-reactivity with bee or wasp venoms. However, peoplesensitized to other Hymenoptera venoms do show in vitro sensitivity to Sol i I. Theclinical interpretation of this finding is unclear. This may explain how someone livingoutside an IFA area could have a systemic reaction to their first fire ant sting uponentering a geographic area containing IFAs.
Harvester ant venom is approximately 70% proteins, including phospholipase A2 andB, hyaluronidase, lipase, acid phosphatase, esterases, and others. In the harvester antspecies, Pogonomyrmex badius, high levels of lipase have been found.
Scorpion venom is primarily neurotoxic, containing multiple low molecular weightbasic proteins (the neurotoxins), mucus (5 to 10%), salts, and various organic com-pounds such as oligopeptides, nucleotides, and amino acids. It contains little or noenzymes. Toxicity from scorpion stings is a result of direct or indirect action upon thehost nervous system.
REFERENCES1. Day, J. M., Death due to cerebral infarction after wasp stings, Archiv. Neurol., 7, 184, 1962.
2. Fox, R. W., Lockey, R. F., and Bukantz, S. C., Neurologic sequelae following the importedfire ant sting, J. Aller. Clin. Microbiol., 70, 120, 1982.
3. Maltzman, J. S., Lee, A. G., and Miller, N. R., Optic neuropathy occurring after bee andwasp sting, Opthalmology, 107, 193, 2000.
4. Watemberg, N., Weizman, Z., Shahak, E., Aviram, M., and Moar, E., Fatal multiple organfailure following massive horet stings, Clin. Toxicol., 33, 471, 1995.
5. Camazine, S., Hymenopteran stings: reactions, mechanisms, and medical treatment, Bull.Entomol. Soc. Am., p. 17, Spring 1988.
6. Idsøe, O., Guthe, T., Wilcox, R. R., and De Weck, A. L., Nature and extent of penicillinside-reactions, with particular reference to fatalities from anaphylactic shock, Bull.W.H.O., 38, 159, 1968.
7. Parrish, H. M., Analysis of 460 fatalities from venomous animals in the U.S., Am. J. Med.Sci., 245, 129, 1963.
8. Mazzotti, L. and Bravo-Becherelle, M. A., Scorpionism in the Mexican republic, inVenomous and Poisonous Animals and Noxious Plants in the Pacific Region, Keegan,H. L. and MacFarlane, W. V., Eds., Pergamon Press, Oxford, 1963, 119.
9. Warrell, D.A., Venomous bites and stings in the tropical world, Med. J. Austr., 159, 773,1993.
10. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 10.
11. Caro, M. R., Derbes, V. J., and Jung, R., Skin responses to the sting of the imported fireant (Solenopsis saevissima), Arch. Dermatol., 75, 475, 1957.
12. deShazo, R. D., Griffing, C., Kwan, T. H., Banks, W. A., and Dvorak, H. F., Dermalhypersensitivity reactions to imported fire ants, J. Allergy Clin. Immunol., 74, 841, 1984.
13. Schmidt, J.O., Let’s not forget the crawling Hymenoptera, Clin. Exp. Allergy, 24, 511, 1994.
14. Reisman, R. E., Insect stings, N. Engl. J. Med., 331, 523, 1994.
15. Hoffman, D. R., Dove, D. E., and Jacobson, R. S., Allergens in Hymenoptera venom. XX.Isolation of four allergens from imported fire ant venom, J. Allergy Clin. Immunol., 82,818, 1988.
16. deShazo, R. D., Butcher, B. T., and Banks, W. A., Reactions to stings of the imported fireant, New Eng. J. Med., 323, 462, 1990.

39
Bites
CHAPTER 4
BITES
TABLE OF CONTENTS
I. Introduction ....................................................................................................... 39
II. Mouthpart Types ............................................................................................... 40
III. Pathology of Insect Bites ................................................................................. 44
IV. Clues to Recognizing Insect Bites ................................................................... 46A. Diagnosis ....................................................................................................... 46B. Characteristics of Lesions............................................................................. 46
True Bugs ..................................................................................................... 46Lice ................................................................................................................ 46Fleas .............................................................................................................. 47Mosquitoes and Biting Midges .................................................................... 47Horse and Deer Flies ................................................................................. 47Black Flies .................................................................................................... 48Sand Flies ...................................................................................................... 48Spiders and Centipedes ............................................................................... 48Ticks .............................................................................................................. 49Mites .............................................................................................................. 49
C. Number of Lesions and Location on the Body ......................................... 51
References ....................................................................................................................... 54
I. INTRODUCTION
Bites by arthropods can be as medically significant as stings, especially for thehypersensitive individual. In this chapter I have lumped all bites together for discussion.However, the term “bite” probably should be restricted in meaning to describepurposeful biting by species for either catching prey or blood feeding, and not to

40
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
accidental or inadvertent biting by plant-feeding species. Phytophagous or predaceousinsect species may “bite” in self defense, piercing the skin with the proboscis, but theinjury is actually a stab wound and not a true bite.
The method of obtaining blood differs among blood-feeding arthropods. Somespecies such as bed bugs, kissing bugs, and fleas, obtain blood directly from venulesor small veins — a method termed solenophagy. Others, such as ticks, horse and deerflies, black flies, and tsetse flies, obtain blood by lacerating blood vessels and feedingfrom the pool of blood thus formed — a method termed telmophagy. The method ofblood feeding likely plays a significant role in whether a species is able to acquire andtransmit pathogenic microorganisms.
II. MOUTHPART TYPES
Insect mouthparts, at least in the medically important species, can be generally dividedinto three broad categories: (1) biting and chewing (Figure 1a), (2) sponging (Figure1b), and (3) piercing–sucking (Figure 1c). Within these categories there are numerousadaptations and/or specializations among the various insect orders. The biting andchewing mouthpart types, such as those in food pest insects, and sponging mouthparttypes, found in the filth fly groups, are of little significance regarding human bites, butpiercing–sucking mouthparts, and especially the bloodsucking types, are of consider-able importance. Insect piercing–sucking mouthparts vary primarily in the number andarrangement of the stylets, which are needle-like blades, and the shape and positionof the lower lip of insect mouthparts, the labium. Often, what is termed the proboscisof an insect with piercing–sucking mouthparts is an ensheathment of the labrum,stylets, and labium. These mouthparts are arranged in such a way that they form twotubes. One tube is usually narrow, being a hollow pathway along the hypopharynx,and the other is wider, formed from the relative positions of the mandibles or maxillae.Upon biting, saliva enters the wound via the narrow tube, and blood returns throughthe wider tube by action of the cibarial or pharyngeal pump.
The true bugs (order Hemiptera), such as bed bugs, kissing bugs, and assassin bugs,have the labium formed into a three- or four-segmented cylindrical proboscis (Figure2). There are four stylets formed from the mandibles and maxillae. In some cases, asin bed bug feeding, the labium folds up above the skin surface, allowing the fascicle(the stylets linked together in a complete unit) to penetrate the skin for feeding.
Sucking lice (order Phthiraptera, suborder Anoplura) do not have an elongatedproboscis, but they do have piercing mouthparts that contain several recurved hooksthat serve to anchor the mouthparts during feeding. There are no palps. Three styletsmake up the fascicle in anoplurans; they are pushed into host tissues by muscularaction in the act of biting. Two of the stylets represent the mandible and maxilla, andthe other forms the tube functioning as a salivary duct. Salivary secretions are releasedinto the wound, and the pharyngeal pump begins to draw blood into the digestive tractvia the food duct.
Fleas (order Siphonaptera) have a pair of stylets composed of maxillary laciniae thatpierce host skin. There is also an unpaired stylet formed from the epipharynx. All threeof these structures form the fascicle. The laciniae are bladelike and produce the wound.Blood is then pumped into the pharynx by pharyngeal and cibarial pumps.
Not all flies have piercing–sucking mouthparts, but of those that do, there isconsiderable variation. Mosquitoes have six stylets (two mandibles, two maxillae, the

41
Bites
hypopharynx, and labrum-epipharynx) ensheathed in an elongated, cylindrical labium.This combined structure forms the prominent proboscis of mosquitoes (Figures 3a, 3b,and 4). Upon biting, only the fascicle is inserted into the host’s skin; the labium foldsup above the skin surface (Figure 3c).
Although relatively short, sandfly mouthparts are efficient organs of penetration.1
The labrum is broad and tapering to a point which bears a number of small spinyprojections. Only the female has mandibles which take the form of blades bearing
Figure 1Chewing (A), sponging (B), and piercing–sucking (C) mouthparts (from: U.S. DHHS CDC Publ.No. 83:8297).

42
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 3Mosquito mouthparts (A), cross-section of fascicle (B), and mouthparts position upon biting (C)(from: U.S. Navy Laboratory Guide to Medical Entomology).
Figure 2True bugs (order Hemiptera) often have a three- or four-segmented cylindrical proboscis.

43
Bites
numerous small serrations. The maxillary stylets, formed by the galeae, are also blade-like and bear numerous fine denticles on their inner margins and a few additional teethnear the end on their outer margins. The labium is elongated and channeled to carrythe stylet and hypopharanx. It has a pair of soft labellar lobes distally. At the sides ofthe proboscis are the two maxillary palps which are longer than the proboscis itself.
Horse flies, deer flies, black flies, and biting midges basically have the same typeof mouthparts — scissorlike (Figure 5). Most of the stylets are much flattened comparedto those of mosquitoes. In addition, the mandibles are flattened and move in atransverse manner. Upon feeding, the mandibles move in a scissorlike fashion and themaxillae are thrust in and out of the wound causing pooled blood in the host’s tissues.A more specific description of horse fly mouthparts is provided by Snow.1 The horsefly labrum is relatively soft with a blunt tip and is not used for penetration. However,the mandibles are large and blade-like, and these and the styliform maxillary galeaeare the piercing organs. Once these mouthparts have made a wound and fluids areflowing out of it, the labium, which does not enter the wound itself but kinks up onthe skin’s surface, draws up blood by means of pseudotracheae on the labellar lobes.
Stable flies have a hardened, conspicuous proboscis (primarily the labium) that canclearly be seen held out in front of the head. The proboscis has the small labella atits tip composed of everted rasping teeth. With a hard thrust, aided by twisting of thelabella, the anterior end of the labium is inserted into the host’s skin. The hardenedlong proboscis enables stable flies to inflict painful bites even through socks, sleeves,and other tight fitting clothing.
Some noninsect arthropods such as spiders, mites, and ticks have piercing–suckingmouthparts, albeit the structures are derived from different morphologic features thanthose of insect mouth parts. Mites and ticks (subclass Acari, sometimes also called
Figure 4Microscopic view of mosquito proboscis.

44
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
acarines) have a feeding structure, or gnathosoma, that is headlike and may bemistaken for a true head. The gnathosoma, consisting of mouthparts and palps, isarranged to form a tubular structure for obtaining food and passing it into the digestivetract. The cutting and/or piercing mouthpart structures of acarines are the chelicerae.Chelicerae may be used for tearing, as in the case of scabies mites, or piercing, as inthe case of chiggers. In ticks there is also an anchoring hypostome, which is a veryprominent structure and bears teeth on its ventral surface.
III. PATHOLOGY OF INSECT BITES
Arthropod bites basically consist of punctures made by the mouthparts of bloodsuckinginsects; the actual mechanical injury to human skin is generally minimal. However, inthe case of horse flies, there may be more tissue damage due to their “slashing–lapping”feeding method and their large size. By far, most lesions on human skin are producedby host immune reactions to the offending arthropod salivary secretions or venom.2
Arthropod saliva is injected while feeding to lubricate the mouthparts upon insertion,increase blood flow to the bite site, inhibit coagulation of host blood, anesthetize thebite site, suppress the host’s immune and inflammatory responses, and/or aid indigestion. Upon repeated exposure to a particular arthropod salivary secretions,humans may become allergic to its bites. After becoming sensitized, it is not unusualto have large local reactions to bites by that particular arthropod.
Arthropod bites are often characterized by urticarial wheals, papules, vesicles, andless commonly, blisters. After a few days or even weeks secondary infection, discol-oration, scarring, papules, or nodules may persist at the bite site.2 Figure 6 showssecondary infection resulting from scratching a mosquito bite. Complicating the picturefurther is the development of late cutaneous allergic responses in some atopicindividuals. Diagnosis may be especially difficult in the case of biopsies of papules ornodules. Biopsies usually reveal a dense infiltrate of a mixture of inflammatory cellssuch as lymphocytes, plasma cells, histiocytes, giant cells, neutrophils, and eosinophils.
Figure 5Horse fly mandibles are large and blade-like.

45
Bites
Figure 6Secondary infection resulting from mosquito bites.
Lesions containing a majority of lymphocytes could be mistaken for a lymphomatousinfiltrate. If the infiltrate is predominantly perivascular and extending throughout thedepths of the dermis, the lesion might be confused with a lupus erythematosus.Eosinophils are commonly seen in papules or nodules resulting from arthropod bites.There may be a dense infiltration of neutrophils, resembling an abscess. Occasionallyremains of arthropod mouthparts are present within the lesion, and there may be agranulomatous inflammation in and around these mouthparts. Scabies mites occur inthe stratum corneum and can usually be seen upon microscopic examination. Newlesions from scabies such as papules or vesicles are covered by normal keratin, whereasolder lesions have a heaped-up parakeratotic surface.3 There may also be a perivascularinfiltrate of lymphocytes, histiocytes, and eosinophils.3
Histopathologic studies of late cutaneous allergic responses have revealed mixedcellular infiltrates, including lymphocytes, polymorphonuclear leukocytes, and somepartially degranulated basophils. A prominent feature of late cutaneous allergic reac-tions has been fibrin deposition interspersed between collagen bundles in the dermisand subcutaneous tissues.
Infectious complications. Secondary infection with common bacterial pathogenscan occur in any lesion in which the integrity of the dermis is disrupted, whether bynecrosis or excoriation.4 Infection may result in cellulitis, impetigo, ecthyma, folliculitis,furunculosis, and other manifestations. Three findings may be helpful in making thediagnosis of secondary bacterial infection:4

46
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
• Increasing erythema, edema, or tenderness beyond the anticipated pattern ofresponse of an individual lesion suggests infection.
• Regional lymphadenopathy can be a useful sign of infection, but it may alsobe present in response to the primary lesion without infection.
• Lymphangitis is the most reliable sign and suggests streptococcal involvement.
IV. CLUES TO RECOGNIZING INSECT BITESA. Diagnosis
If a patient recalls no insect or arachnid exposure, arthropod bites may pose frequentdifficulty in diagnosis. However, bites should be considred in the differential diagnosisof any patient complaining of itching. Diagnosis of insect bites depends upon (1)maintaining a proper index of suspicion in this direction (especially during the summermonths), (2) a familiarity of the insect fauna in one’s area, and (3) obtaining a goodhistory.5 It is very important to find out what the patient has been doing lately, e.g.,hiking, fishing, gardening, cleaning out a shed, etc. However, even history can bemisleading in that patients may present a lesion that they think is an insect bite, whenin reality the correct diagnosis is something like urticaria, folliculitis, or delusions ofparasitosis. Physicians need to be careful not to diagnose “insect bites” based uponlesions alone and should call upon entomologists to examine samples. Other clues thatmight be helpful in diagnosing insect bites include number of lesions and location onthe body (see Section C below).
B. Characteristics of Lesions
True bugs. Members of the Hemiptera produce variable lesions upon biting. Bed bugbites are multiple and often linear in distribution. They are characterized by welts,inflammation, and often purpuric spots. Alexander3 reported that red blotches progress-ing to form large urticarial wheals are frequent reactions to Cimex bites and that bullouslesions are not uncommon. Assassin bugs (including wheel bugs) inflict a bite that isimmediately and intensely painful. There may be a small red spot or vesicle at the bitesite and considerable swelling; numbness may also occur. The kissing bugs generallyhave a painless bite, but they may produce four distinct reactions depending uponsensitivity: (1) a papule with a central punctum, (2) small vesicles grouped around thebite site with swelling and little redness, (3) large urticarial lesion with a centralpunctum and surrounding edema, or (4) hemorrhagic nodular-to-bullous lesions.
Lice. Pubic lice bites produce intense pruritus and discoloration of the skin (bluishgrey maculae) if the infestation is long standing. Other than that, individual lesions areusually not discernable.3 Head lice bites may be pustular in appearance. Secondaryinfection such as impetigo contagiosa on the scalp, head, or neck may indicate headlice infestation.3 The direct effect of body lice feeding is intense irritation, probably dueto proteins in their saliva. This leads to widespread excoriation. The usual clinicalpresentation for body lice is pyoderma in covered areas. Uninfected bites present assmall papules or puncta on an erythematous base.6 In most clinical settings, the patientmay already be undressed when the physician gets to see him, and only the ulcerations,infections, and excoriations are present — the acutal lice are found in the seams of thepatient’s clothing.6 In general, primary sensitization to body lice is attained 3 to 8months after the original infestation. From that point on, feeding by the lice will cause

47
Bites
intense itching. Secondary sensitization may develop some 12 to 18 months after theinitial infestation, resulting in a systemic reaction to louse bites characterized by afeeling of malaise and pessimistic frame of mind. The body lice infested personbecomes apathetic if left alone and irritable if roused (this is the origin of the term“feeling lousy”). In addition, the skin of people who continually harbor body licebecomes hardened and darkly pigmented, a condition known as vagabond’s syndrome.
Fleas. Flea bites often occur in irregular groups of several to a dozen or more. Thetypical flea bite on a human consists of a central spot surrounded by an erythematousring. There is usually little swelling, but the center may be elevated into a papule,vesicle, or bulla.3 Papular urticaria is seen in persons with chronic exposure to fleabites. The lesions appear in crops and all stages can be seen simultaneously — freshwheals, persistent papules, vesicles, scratch marks, exudation, encrustation, and oftensecondary infection.3
Mosquitoes and biting midges. Mosquitoes and biting midges (Ceratopogonidae)cause itching and welts by their bites. In many individuals the typical wheal and flarereaction is evident approximately 30 min after the bite (Figure 7 and Color Figure 4-5).The size and extent of the lesions are largely a result of the species of insect involved,the sensitivity status of the individual, and age of the individual. Delayed, small butpruritic papules are common after mosquito bites. These generally appear several hoursafter the bite and usually last 1 to 3 days, but occasionally persist for weeks. Duringthe spring and summer months, children who play outdoors often exhibit numerousmosquito bite lesions of varying ages (Figure 8).
Horse and deer flies. Female horse and deer flies (family Tabanidae) have broad,scissor-like mouthparts that can slash a deep painful wound in their host’s skin. Bites
Figure 7Wheal and flare on shoulder blade caused by mosquito bite 30 min earlier.

48
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
by tabanids often become secondarily infected, leading to cellulitis.3 However, in theabsence of allergy or secondary infection, there is generally no reddening or swelling.
Black flies. Black flies often produce reddened, itching papules. Subsequently,multiple nodules may develop. It is not uncommon for the whole affected area to swellmarkedly.3 The arms, legs, and face are common sites of attack, but a favorite site isthe posterior cervical region, particularly at the base of the hair. In the case of blackfly-transmitted onchocerciasis, the condition is extremely pruritic, and widespreadpapules and lichenification occur, particularly around the shoulders and upper armsand buttocks and thighs. Microfilariae invade the dermis and destroy the elastic tissueso that the skin may hang in folds, especially in the groin area.
Sand flies. Sand fly bites may produce itching papules, vesicles, wheals, and acondition closely resembling papular urticaria. Additionally, sand flies may transmit theparasite responsible for cutaneous leishmaniasis. In those cases, exposed skin areas arethe most commonly bitten, resulting in papules and nodules that break down, ulcerate,and crust. There is usually healing within a year, but with considerable scarring.
Spiders and centipedes. Widow spiders differ from violin spiders in regard toreactions to their bites. In the case of widow spiders there is often a pin prick sensationinitially. Two red puncture marks may be present at the bite site, and there may be adeveloping dull, numbing pain around the site that builds to a peak 1 to 3 h after thebite. Centipedes may also produce two puncture wounds at the bite site, but there isusually redness and swelling present, with immediate intense pain. Violin spider bitesare rarely, if ever, accompanied by pain initially. However, within 2 to 8 h there is mildto severe pain at the site, erythema, blanching, itchiness, and vesiculation.
Figure 8Lesions of varying ages due to mosquito bites.

49
Bites
Ticks. Ticks will attach to human skin and remain attached for several days. Theactual penetration is usually not painful, except in the case of some of the species withvery long mouthparts. However, inflammation or even hypersensitivity reactions mayoccur after a few days of tick attachment (Figures 9 and 10 and Color Figures 4-6 and4-7). After tick removal, a reddened nodule may persist at the bite site for weeks oreven months.
Mites. Chigger bites usually lead to an intensely itchy dermatitis composed ofpustules and wheals (Figure 11 and Color Figure 4-8). Lesions occur within 3 to 6 hafter exposure to chigger-infested areas. Alexander3 states that an edematous whealwith a tiny central vesicle may persist for 8 to 15 days.
Bites by the straw itch mite produce itching a few hours after attack. Often, smallurticarial papules with a tiny central vesicle (0.5 mm diameter) mark the site of skinpuncture.3 Other human-biting mites such as the tropical rat mite produce immediatesharp itching pain upon biting and cause small urticated papules.
Figure 9Hypersensitivity reaction resulting from tick bite — presumably a reaction to tick saliva. Tick bitewas in center of lesion.

50
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 10Seed tick bites around ankle, 4 days post-attachment (photo courtesy Tom Kilpatrick).

51
Bites
Figure 11Chigger bites around ankle.
Scabies mites have an affinity for the wrists and the areas between the fingers(although they certainly occur in other areas). Accordingly, scabies is often character-ized by rashlike lesions that typically occur in tracks in the webbing between the fingersor on the wrists. Alexander3 described the burrow as a greyish line resembling a pencilmark, about 5 mm long on average. Sometimes, however, scabies lesions may besingular (papules or vesicles) or even bullous. (Note: rashes may occur over much ofthe body as a result of scabies infestation, but the rash may not correspond to thelocation of mite burrows.)
Cheyletiella mites (such as C. parasitivorax, C. yasguri, C. blakei, and C. furmani)produce scattered or localized urticae, papules, or 2 to 6 mm papulo-vesicles in theareas of skin where direct contact with an infested pet occurs — the flexor sides ofarms, breasts, and abdomen.7
C. Number of Lesions and Location on the Body
The number of lesions on a patient and location on the body may also provide cluesto the diagnosis of arthropod bites. Tables 1 and 2 provide information on arthropodbite possibilities based upon these two factors. In addition to the number of lesions andtheir location, the distribution or pattern of the bites may be diagnostic (Table 3).Residual effects of arthropod bites that occurred days or weeks earlier may also beclassified (Table 4).

52
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Table 1Clues to Biting Arthropods Based upon Location ofLesions on the Body
Location of Lesions Possible Arthropod(s)
Predominantly on left side of body Imaginary “bugs” (see Chap. 7)(if right-handed) or right side ofbody (if left-handed)
Legs or feet FleasMosquitoesSpidersChiggersCentipedes
Trunk ChiggersBed bugsScabiesTicksBody licePubic liceSpidersCheyletiella mites
Genitalsa ScabiesChiggers
Arms or hands MosquitoesBlack fliesMitesBiting midgesSpidersFleasCheyletiella mitesCentipedesSand fliesWheel bugs
Head, neck, or face MosquitoesBlack fliesBiting midgesSand fliesHead liceKissing bugs
a The presence of crusted, pruritic papules on the penis and buttocks is highlyindicative of scabies.

53
Bites
Table 2Clues to Biting Arthropods Basedupon Number of Lesions on the Body
Number of Lesions Possible Arthropod(s)
Single TickSpiderCentipedeWheel bugKissing bug
Few FleasMosquitoesStable fliesHorse and deer fliesKissing bugsSand flies
Multiple MosquitoesBlack fliesBiting midges (Culicoides)FleasLiceChiggersSeed ticksMitesBed bugsScabies
Table 3Diagnostic Patterns of Arthropod Bitesa
Pattern of Bite Lesions Possible Arthropod(s)
Scattered MosquitoesHorse and deer fliesBlack fliesBiting midgesHead and body lice
Grouped FleasPubic liceChiggersScabies
Linear Bed bugsChiggers
a Adapted in part from Frazier.8

54
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Table 4Cutaneous Sequelae Resulting from Arthropod Bitesa
PossibleSequelae Location on Body Arthropod(s)
Single nodule Scalp or trunk TickMultiple nodules Legs or ankles Black flyPurpuric spots Trunk Bed bugBluish spots Pubic and perianal area Pubic liceHyperpigmentation Waistline and genitals ChiggerHyperpigmentation Trunk Body lice
a Adapted in part from Frazier.8
REFERENCES1. Snow, K.R., Insects and Disease, John Wiley & Sons, New York, 1974, chaps. 4, 5.
2. Frazier, C. A., Diagnosis of bites and stings, Cutis, 4, 845, 1968.
3. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, 251.
4. Kemp, E.D., Bites and stings of the arthropod kind, Postgrad. Med., 103, 88, 1998.
5. Allington, H.V. and Allington, R.R., Insect bites, JAMA, 155, 240, 1954.
6. Elgart, M.L. Pediculosis, Dermatol. Clinics, 8, 219, 1990.
7. van Bronswijk, J. E. M. H. and de Kreek, E. J., Cheyletiella of dog, cat, and domesticatedrabbit, a review, J. Med. Entomol., 13, 315, 1976.
8. Frazier, C. A., Jr., Insect Allergy, Warren Green, St. Louis, 1969, chap. 9.

55
Dermatitis, Urticaria, and Blistering from Contact with Arthropods
CHAPTER 5
DERMATITIS, URTICARIA,AND BLISTERING
FROM CONTACT WITHARTHROPODS
TABLE OF CONTENTS
I. Blistering from Exposure to Blister Beetles ................................................... 56A. Medical Significance ..................................................................................... 56B. Contributing Factors/Species ....................................................................... 57C. Management/Treatment ............................................................................... 57
II. Dermatitis and Urticaria from Exposure to Larval Lepidopterans ................ 57A. Medical Significance ..................................................................................... 57B. Contributing Factors/Species ....................................................................... 58C. Management/Treatment ............................................................................... 59
III. Inhalent Irritation or Contact Dermatitis from Moth Hairs or Scales ........... 59A. Medical Significance ..................................................................................... 59B. Contributing Factors/Species ....................................................................... 59C. Management/Treatment ............................................................................... 60
References ....................................................................................................................... 60

56
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
I. BLISTERING FROM EXPOSURE TO BLISTER BEETLESA. Medical Significance
Most beetles are harmless and can be handled by humans with no ill effects. However,blister beetles, primarily species in the families Meloidae and Staphylinidae, possessvesicating chemical substances in their body fluids (see also Chapter 12). The blisteringfluid in meloids is cantharidin, but may be a somewhat different compound instaphylinids. When the meloid beetles sense danger, they exude cantharidin by fillingtheir breathing tubes with air, closing their breathing pores, and building up body fluidpressure until fluid is pushed out through one or more leg joints. This secretion or“venom” readily penetrates human skin and produces fluid-filled blisters in a few hours(Figure 1).
The blisters that result from exposure to live blister beetles or their dried pulverizedbody parts are generally few and self-limiting. Alexander1 states that generally there isno pain or itch associated with the blisters as long as they do not rupture. Extensiveblister beetle exposure may irritate the kidneys due to the penetrating activity of
Figure 1Blister on arm resulting from blister beetle exposure (photocourtesy Ralph Turnbo).

57
Dermatitis, Urticaria, and Blistering from Contact with Arthropods
cantharidin.2 If ingested, the substance can cause nausea, diarrhea, and vomiting;horses have died from ingesting numerous striped blister beetles.3
Frazier and Brown2 reported that a good indication of blister beetle attack is that theblisters are all in the same stage of development and there is no accompanying rasharound them. In addition, there may be a line or track of blisters where the beetlecrawled over the skin. Alexander1 reported that areas commonly affected are the face,neck, chest, thighs, and calves, and the buttocks in children.
B. Contributing Factors/Species
Blister beetle dermatoses are seasonal, with most cases reported in the late summer asthe beetles emerge and feed in gardens and field crops. Three common blister beetlesin the U.S. are the ashgray and striped blister beetles in the central and southeasternU.S. and oil beetles (several species) in the southwestern U.S. Contact with the beetlesmay occur intentionally, such as in the case of a child picking one up, or accidentally,such as the beetle crawling on an unsuspecting victim sitting on the ground, workingin the garden, etc. In southern Texas in late summer the author has observed hundredsof black oil beetles crawling over the ground in a random, solitary fashion, presumablylooking for food.
C. Management/Treatment
Blisters resulting from blister beetle exposure are generally not serious, and reabsorp-tion usually occurs in a few days if the blisters are unruptured. If blisters are rupturedthe skin may flake, and there may be a mild reddening of the area before clearing ina week or so.2 For treatment, exposed areas should be washed, antibiotic ointmentsapplied to prevent secondary infection, and the areas bandaged for protection until theblisters reabsorb.
II. DERMATITIS AND URTICARIA FROM EXPOSURE TOLARVAL LEPIDOPTERANS
A. Medical Significance
Caterpillars of many species can produce mild to severe dermatitis, urticaria, nodularconjunctivitis, pain, headache, and even convulsions (rare) via tiny hairs that irritate orinject a venom (Figure 2) (see also Chapter 14). According to Alexander,1 visible lesionsare usually preceded by a burning itch. The itch is often followed by the appearanceof 2 to 5 mm tiny, rose-red maculopapules or papules. Keegan4 has given an accountof the direct injury produced by caterpillars and moths, and Alexander1 provides anindepth discussion of human reactions to Lepidoptera. In the scientific literature,distinction is usually made between direct contact with urticating caterpillars (erucism)and contact with scales or hairs of adult butterflies or moths (lepidopterism) (see nextsection).
Relatively speaking, only a few lepidopterous species are involved in erucism.However, urticating caterpillars can become numerous, resulting in a significant healthhazard. In the 1920s the San Antonio schools had to be closed due to a large emergenceof puss caterpillars and the resulting numerous stings among the school-age children.5

58
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
The caterpillars were so numerous on posts, walls, and bushes that virtually anyoutdoor activity resulted in a sting.
Even a few urticating caterpillars can be a serious problem if a person has an eyelesion or exhibits acute systemic symptoms when exposed. The puss caterpillar isespecially dangerous, sometimes causing cardiovascular and neurologic manifestations.Frazier and Brown2 report a case in which a young woman stepped barefoot on a pusscaterpillar. Within minutes she experienced symptoms of shock with respiratorydistress; upon arrival at the hospital she had hypotension and brachycardia. She wassuccessfully treated for shock and pain but reported numbness in the foot and leg forseveral days. Eye lesions may be relatively benign when single pointed hairs are foundon the palpebral conjunctiva (they can generally be removed by an opthamologist), orthey can be extremely serious with loss of vision in the case of numerous deeplyembedded hairs or spines that progressively penetrate deeper and deeper due to eyemovement and barbs on the hairs.1
B. Contributing Factors/Species
Both mechanical irritation and injection of venom by the caterpillar spines or hairscontribute to the urticarial response in humans. Many of the hairs, setae, or spinesof the offending species are hollow and connected to venom glands. Upon exposure,these structures may be broken, allowing venom to either be injected into the skinor to ooze out onto abraded skin. In addition, in a study of gypsy moth caterpillars,whole first instar larvae contained an average of 17.3 ng of histamine, and the hairlikesetae of the fifth instar larvae contained 80 ng of histamine per organism.6 Accord-ingly, histamine release, as well as a hypersensitivity reaction, likely play a role inurticaria and dermatitis associated with these caterpillars. Four common species ofLepidoptera that have caterpillars that can sting upon exposure to human skin arethe saddleback caterpillar, the IO moth caterpillar, the brown tail moth caterpillar,and the puss caterpillar. Although not true “stinging” caterpillars, the gypsy moth
Figure 2Many caterpillars with thick or prominant spines can cause a sting similar to that ofwasps.

59
Dermatitis, Urticaria, and Blistering from Contact with Arthropods
caterpillar and related groups have been known to cause a dermatitis on human skinupon exposure. Detailed discussions of the biologies of these species are providedin Chapter 14.
C. Management/Treatment
Treatment mainly involves personal protection and/or avoidance of the offendingspecies. Embedded spines or hairs can sometimes be removed by “stripping” the lesionwith cellophane tape. Acute urticarial lesions may respond satisfactorily to topicalcorticosteroid lotions and creams (desoximetasone gel has been frequently used),which reduce the intensity of the inflammatory reaction. Oral antihistamines mayrelieve itching and burning sensations. Systemic administration of corticosteroids hasalso been used for itching and pain. Pain relievers may also be needed, especially inthe case of puss caterpillar stings. Systemic reactions require close monitoring andaggressive treatment (see Chapter 2).
III. INHALANT IRRITATION OR CONTACT DERMATITISFROM MOTH HAIRS OR SCALES
A. Medical Significance
The term “lepidopterism” refers to urticaria and irritation caused by adult moths andtheir hairs or scales (see Chapter 26 for further discussion of the species involved).Reports of particularly severe lepidopterism have come from the South Americancountries of Peru, Brazil, Venezuela, and Argentina. In that area, female moths in thegenus Hylesia have barbed urticating setae, which are broken off and become airborneas the moths flutter around lights. This results in urticating rashes and upper respiratoryirritation. In the U.S., the tussock moths and their relatives (family Lymantriidae) causerashes, upper respiratory irritation, and eye irritation to forest workers in the PacificNorthwest.7
B. Contributing Factors/Species
In most cases of lepidopterism, huge outbreaks of offending moth species lead toenvironmental air becoming laden with broken hairs or scales. In the U.S., the Douglasfir tussock moth, Orgyia pseudotsugata, female covers her egg masses with froth andbody hairs. These hairs, along with other hairs from the tips of the female abdomen,become airborne and cause irritation to humans in and near infested forests. Outbreaksof the Douglas fir tussock moth appear to develop almost explosively, and then subsideabruptly after a year or two. During an outbreak, there are literally billions ofcaterpillars crawling on the ground, trees, brush, and buildings. Accordingly, airbornelevels of the offending hairs are quite high. A related species, the white-marked tussockmoth (O. leucostigma), occurs throughout most of North America and may be involvedin cases of lepidopterism, especially in the East. Rothschild et al.8 also lists moths inthe genera Epanaphe, Anaphe, Gazalina, and Epicoma (family Notodontidae) as beingcauses of occasional lepidopterism.

60
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
C. Management/Treatment
Treatment mainly involves personal protection and/or avoidance of the offendingspecies. During the season of Hylesia moth emergence (South America), it may helpto turn off outdoor lights. In affected areas of the U.S., air conditioning and frequentchanges of filters may help reduce airborne levels of spines or hairs. Sensitive personsshould avoid walking in forests heavily infested with tussock or gypsy moths. Physi-cians should be aware that cases diagnosed as simple conjunctivitis or keratoconjunc-tivitis occurring in areas with extreme moth infestation (tussock moths in the PacificNorthwest and gypsy moths in the East) may be due to contact with airborne mothhairs.
Acute urticarial lesions may respond satisfactorily to topical corticosteroid lotionsand creams (desoximetasone gel has been frequently used), which reduce the intensityof the inflammatory reaction. Oral antihistamines may relieve itching and burningsensations. In more serious cases, oral prednisone may be indicated. Rosen9 saidsystemic administration of corticosteroids in the form of intramuscular triamcinoloneacetonide has been remarkably effective in relieving severe itching due to gypsy mothdermatitis.
REFERENCES1. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 7.
2. Frazier, C. A. and Brown, F. K., Insects and Allergy and What To Do About Them,University of Oklahoma Press, Norman, OK, 1980, chap. 19.
3. Bahme, A. J., Cantharides toxicosis in the equine, Southwest. Vet., 21, 147, 1968.
4. Keegan, H. L., Some medical problems from direct injury by arthropods, Int. Pathol., 10,35, 1969.
5. Foot, N. C., Pathology of the dermatitis caused by Megalopyge opercularis, a Texascaterpillar, J. Exp. Med., 35, 737, 1922.
6. Shama, S. K., Etkind, P. H., Odell, T. M., Canada, A. T., and Soter, N. A., Gypsy mothcaterpillar dermatitis, N. Engl. J. Med., 306, 1300, 1982.
7. Perlman, F., Press, E., Googins, G. A., Malley, A., and Poarea, H., Tussockosis: reactionsto Douglas fir tussock moth, Ann. Allerg., 36, 302, 1976.
8. Rothschild, M., Reichstein, T., Von Euw, J., Alpin, R., and Harman, R. R. M., ToxicLepidoptera, Toxicon, 8, 293, 1970.
9. Rosen, T., Caterpillar dermatitis, Dermatol. Clin., 8, 245, 1990.

61
Myiasis (Invasion of Human Tissues by Fly Larvae)
CHAPTER 6
MYIASIS (INVASION OFHUMAN TISSUES BY
FLY LARVAE)
TABLE OF CONTENTS
I. Introduction and Medical Significance ............................................................ 61A. Accidental Myiasis ........................................................................................ 62B. Facultative Myiasis ........................................................................................ 63C. Obligate Myiasis ........................................................................................... 63
II. Contributing Factors ......................................................................................... 63A. Accidental Myiasis ........................................................................................ 63B. Facultative Myiasis ........................................................................................ 63C. Obligate Myiasis ........................................................................................... 64
III. Prevention, Management, and Treatment ....................................................... 64A. Prevention ..................................................................................................... 64B. Management/Treatment ............................................................................... 64
References ....................................................................................................................... 65
I. INTRODUCTION AND MEDICAL SIGNIFICANCE
The condition of fly maggots infesting the organs and tissues of people or animals isreferred to as myiasis. Specific cases of myiasis are clinically defined by the affectedareas(s) involved. For example, there may be traumatic (wound), gastric, rectal,auricular, and urogenital myiasis, among others. Myiasis can be accidental, when flylarvae occasionally find their way into the human body, or facultative, when fly larvae

62
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
enter living tissue opportunistically after feeding on decaying tissue in neglected,malodorous wounds. Myiasis can also be obligate in which the fly larvae must spendpart of their developmental stages in living tissue. Obligate myiasis is the most seriousform of the condition from a pathogenic standpoint and constitutes true parasitism.
Fly larvae are not capable of reproduction and, therefore, myiasis under normalcircumstances should not be considered contagious from patient to patient. Transmis-sion of myiasis occurs only via an adult female fly. See Chapter 21 for discussions ofthe most common species involved and their biologies.
A. Accidental Myiasis
Accidental enteric myiasis (sometimes referred to as pseudomyiasis) is mostly a benignevent, but the larvae could possibly survive temporarily, causing stomach pains, nausea,or vomiting. Numerous fly species in the families Muscidae, Calliphoridae, andSarcophagidae may produce accidental enteric myiasis. Some notorious offenders are: thecheese skipper, Piophilia casei, the black soldier fly, Hermetia illucens, and the rat-tailedmaggot, Eristalis tenax. Other instances of accidental myiasis occur when fly larvae enterthe urinary passages or other body openings. Flies in the genera Musca, Muscina,Fannia, Megaselia, and Sarcophaga have often been implicated in such cases.
CASE HISTORY
HUMAN PARASITES OR MAGGOTS?
A woman sent me approximately 20 worm-like specimens collected from inside her toiletand on the floor around the toilet. “How are these things getting there?” she asked. “Doesthis mean we excreted these worms/parasites?” Upon examination, the specimens wereidentified as soldier fly larvae, Hermetia illucians, common pests inhabiting decaying orputrefying organic matter (Color Figure 21-18). This species has been reported as a causeof intestinal myiasis, but — as in this case — it is difficult to tell if the maggots were excretedinto the toilet or were deposited as eggs by the adult fly in the toilet area due to decayingwood and build-up of organic matter at the toilet/floor interface. I recommended that thewoman have the toilet taken up, thoroughly cleaned, and a new wax seal installed. Shecalled back saying her husband found many more specimens under the toilet where theflange meets the sewer pipe and even in the wax seal itself.
Comment: More than likely, this was a case of mistaken identity — maggots feeding in andaround a toilet confused as parasites coming from inside the people using the toilet. Veryfrequently toilets leak a little around the connection to the sewer, allowing water andorganic debris to accumulate — perfect conditions for soldier fly larvae.

63
Myiasis (Invasion of Human Tissues by Fly Larvae)
B. Facultative Myiasis
Facultative myiasis may result in considerable pain and tissue damage as fly larvae leavenecrotic tissues and invade healthy tissues. Numerous species of Muscidae, Calli-phoridae, and Sarcophagidae have been implicated in facultative myiasis. In the U.S.,the calliphorid Phaenicia sericata has been reported causing facultative myiasis onseveral occasions.1,2 Another calliphorid, Chrysomya rufifacies, has been recentlyintroduced into the U.S.3 from the Australasian region and is also known to be regularlyinvolved in facultative myiasis. Other muscoid fly species which may be involved inthis type of myiasis include: Calliphora vicina, Phormia regina, Cochliomyia macellaria,and Sarcophaga haemorrhoidalis.
C. Obligate Myiasis
Several fly species must develop in the living tissues of a host. This is termed obligatemyiasis and is caused by species affecting sheep, cattle, horses, and many wild animals.In people, obligate myiasis is primarily due to the screwworm flies (Old and New World)and the human bot fly (Color Figure 6-9). Obligate myiasis is rarely fatal in the case ofthe human bot fly of Central and South America, but it has led to considerable pathologyand death in the case of screwworm flies. Screwworm flies use livestock as primary hosts,but they do attack humans. If, for example, a female screwworm fly oviposits just insidethe nostril of a sleeping human, hundreds of developing maggots may migrate through-out the turbinal mucous membranes, sinuses, and other tissues. Surgically, it would beextremely difficult to remove all the larvae. Fortunately, due to the sterile male releaseprogram, screwworm flies have been virtually eliminated from the U.S. and Mexico.
II. CONTRIBUTING FACTORSA. Accidental Myiasis
Accidental enteric myiasis generally occurs from ingesting fly eggs or young maggotson uncooked foods or previously cooked foods that have been subsequently infested.Cured meats, dried fruits, cheese, and smoked fish are the most commonly infestedfoods. Other cases of accidental myiasis may occur from the use of contaminatedcatheters, douching syringes or other invasive medical equipment, or sleeping with thebody exposed.
B. Facultative Myiasis
Several fly species lay eggs on dead animals or rotting flesh. Accordingly, the flies maymistakenly oviposit in a foul-smelling wound of a living animal. The developingmaggots subsequently invade healthy tissue. Facultative myiasis most often is initiatedwhen flies oviposit in necrotic, hemorrhaging, or pus-filled lesions. Wounds withwatery alkaline discharges (pH 7.1 to 7.5) have been reported to be especially attractiveto blow flies. Facultative myiasis frequently occurs in helpless semi-invalids who havepoor (if any) medical care. Often, in the case of the very elderly, their eyesight is soweak that victims do not detect the myiasis. In clinical settings, facultative myiasis ismost likely to occur in incapacitated patients who have recently had major surgery orthose having large or multiple uncovered or partially covered festering wounds.However, not all human cases of facultative myiasis occur in or near a wound. In the

64
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
U.S., larvae of the blow fly, P. sericata, have been reported from the ears and nose ofhealthy patients with no other signs of trauma in those areas.4
C. Obligate Myiasis
Obligate myiasis is essentially a zoonosis; humans are not the ordinary host but maybecome infested. Human infestation by the human bot fly is very often via a mosquitobite — the eggs are attached to mosquitoes and other biting flies (see section in PartIII for more details); however, human screwworm fly myiasis is a result of direct egglaying onto a person, most often in or near a wound or natural orifice. Egg-layingactivity of screwworm flies occurs during daytime.
III. PREVENTION, MANAGEMENT, AND TREATMENTA. Prevention
Prevention and good sanitation can avert much of the accidental and facultative myiasisoccurring in the industrialized world. Exposed foodstuffs should not be unattended forany length of time to prevent flies from ovipositing therein. Covering, and preferablyrefrigerating leftovers should be done immediately after meals. Washing fruits andvegetables prior to consumption should help remove developing maggots, althoughvisual examination should also be accomplished during slicing or preparing theseitems. Other forms of accidental myiasis may be prevented by protecting invasivemedical equipment from flies and avoiding sleeping nude, especially during daytime.To prevent facultative myiasis, extra care should be taken to keep wounds clean anddressed, especially on elderly or helpless individuals. Daily or weekly visits by a homehealth nurse can go a long way to prevent facultative myiasis in patients who stay athome. In institutions containing invalids or otherwise helpless patients, every effortshould be made to control entry of flies into the facility. This might involve such thingsas keeping doors and windows screened and in good repair, thoroughly sealing allcracks and crevices, installing air curtains over doors used for loading and unloadingsupplies, and installing UV electrocuter (or the new electronic types) fly traps in areasaccessible to the flies but inaccessible to patients. Prevention of obligate myiasisinvolves avoiding sleeping outdoors during daytime in screwworm-infested areas andusing insect repellents in Central and South America to prevent bites by bot fly egg-bearing mosquitoes.
B. Management/Treatment
Treatment of accidental enteric myiasis is probably not necessary (although there maybe rare instances of clinical symptoms), since in most cases there is no developmentof the fly larvae within the highly acidic stomach environment and other parts of thedigestive tract. They are killed and merely carried through the digestive tract in apassive manner. Treatment of other forms of accidental myiasis as well as facultativeor obligate myiasis involves removal of the larvae. Alexander5 recommends debride-ment with irrigation. Others suggested surgical exploration and removal of larvae underlocal anesthesia.4 Care should be taken not to burst the maggots upon removal. Humanbot fly larvae have been successfully removed using “bacon therapy”, a treatmentmethod involving covering the punctum (breathing hole in the patient’s skin) with raw

65
Myiasis (Invasion of Human Tissues by Fly Larvae)
meat or pork.6 In a few hours the larvae migrate into the meat and are then easilyextracted (see Chapter 21 for more discussion). Maggot infestation of the nose, eyes,ears, and other areas may require surgery if larvae cannot be removed via naturalorifices. Since blow flies and other myiasis-causing flies lay eggs in batches, there couldbe tens or even hundreds of maggots in a wound.
REFERENCES1. Greenberg, B., Two cases of human myiasis caused by Phaenicia sericata in Chicago area
hospitals, J. Med. Entomol., 21, 615, 1984.
2. Merritt, R. W., A severe case of human cutaneous myiasis caused by Phaenicia sericata,Calif. Vector Views, 16, 24, 1969.
3. Richard, R. D. and Ahrens, E. H., New distribution record for the recently introducedblowfly Chrysomya rufifacies in North America, Southwest. Entomol., 8, 216, 1983.
4. Anderson, J. F. and Magnarelli, L. A., Hospital-acquired myiasis, Asepsis, 6, 15, 1984.
5. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 8.
6. Brewer, T.F., Wilson, M.E., Gonzalez, E., and Felsenstein, D., Bacon therapy andfuruncular myiasis, J. Amer. Med. Assoc., 270, 2087, 1993.


67
Delusions of Parasitosis (Imaginary Insect or Mite Infestations)
CHAPTER 7
DELUSIONS OFPARASITOSIS
(IMAGINARY INSECT ORMITE INFESTATIONS)
TABLE OF CONTENTS
I. Introduction ....................................................................................................... 67
II. Actual Arthropod Causes of Dermatitis .......................................................... 68
III. Delusions of Parasitosis .................................................................................... 69
IV. Workplace Infestations ..................................................................................... 74
References ....................................................................................................................... 74
I. INTRODUCTION
Some people have delusions of parasitosis (DOP) in which they think they are infestedwith arthropod parasites. The condition is not uncommon. Any public health orextension service entomologist who has worked with the public has encountered thisproblem in one form or another. Schrut and Waldron1 reported seeing over 100 casesin 5 years. Alexander2 and Slaughter et al.2a have provided excellent overviews of thissubject. Before discussing this phenomenon, some clarifying definitions are in order.
Entomophobia. Entomophobia is often erroneously used as a catchall term toexplain abnormal reactions in some people to insects or mites. This word has beenloosely used to include several distinct psychic phenomena such as abnormal fear of

68
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
insects or arachnids, delusions of parasitic mite infestations, and “computer mite,”“paper mite,” or “cable mite” caused dermatitis in the workplace. More precisely,however, entomophobia is a terrible fear or dread of insects, mites, or spiders. It maybe characterized by hysterical reactions at the sight of the feared arthropods.Entomophobia may be related to, but is distinctly different from, delusions of parasi-tosis and computer or cable mite dermatitis.
Delusions of Parasitosis. DOP is an emotional disorder in which the patient isconvinced that tiny, almost invisible insects or mites are present on/in his body. Someresearchers prefer to label the disorder “pyschogenic parasitosis” bcause not all patientsare delusional in the classic sense.2b In most cases, DOP is a monosymptomatichypochondriacal psychosis in which there are no other thought disorders and thedelusions are not a result of another psychiatric illness. However, DOP cases can beassociated with paranoia/schizophrenia, which can quite possibly endanger the healthcare provider. The author has encountered such patients who subsequently began tothink that health department officials (including the entomologist!) were “out to gethim”. The mental and emotional stress from DOP may be severe, leading to destructivebehaviors such as quitting jobs, burning furniture, abandonig homes, using pesticidesdangerously and repeatedly, etc.
Workplace infestations. Sometimes there is an imaginary insect or mite infestationat the workplace. Workers may complain of “cable mites,” “paper mites,” or “computermites” biting them and producing lesions. Strictly speaking, this situation may not beDOP in that often there is a real substance in the work environment causing theproblem (fiberglass or other insulation, chemicals, paper or cardboard splinters, etc.).
Prior to categorizing persons into any of these three groups, it is imperative that athorough entomological inspection be made at the residence or workplace. This shouldbe done with an objective and open mind because of the possibility of there being areal insect or mite problem. A pest control operator (exterminator) could do this, buta university, health department, or extension entomologist would be better since theygenerally have had more entomological training. Provided below is a brief overviewof the insect or mite species that could be the cause of a real infestation (please referto each of these sections in Part III for further details).
II. ACTUAL ARTHROPOD CAUSES OF DERMATITIS
There are two human-specific mites: the human scabies mite, Sarcoptes scabei, and thehuman follicle mite, Demodex folliculorum. The human scabies mite burrows beneaththe outer layer of skin, leaving crusted papules and/or a sinuous red trail along the skinfor a few centimeters. The infestation causes itching and commonly occurs in thewebbing between the fingers and on the wrists and elbows. Skin scrapings of affectedareas will usually contain the mites. The human follicle mite occurs in the majority ofhumans in hair follicles around the nose and eyelids, but generally causes no pathologyor discomfort. Physicians should be aware of the follicle mite so that, when detectedduring a skin scraping, the mites will not be inadvertently reported as the cause of themysterious biting.
There are a few other mite species (not host specific for humans) that will readilybite people. Usually, these are only opportunistic infestations that are self-limiting. Theydo not take up residence and reproduce on or in the skin. The tropical fowl mite,Ornithonyssus bursa (a parasite of sparrows), the northern fowl mite, O. sylviarum (a

69
Delusions of Parasitosis (Imaginary Insect or Mite Infestations)
parasite of chickens), and the tropical rat mite, O. bacoti (a parasite of rats) willaggressively bite people, causing pain and itching. In a lot of cases of “mysterious” miteinfestation a rat or bird nest can be found some place in the dwelling, and the patientis being bitten by one of these mite species. These mites can be seen (about 1 mm long)and are often captured while biting or crawling on the skin.
Other mites such as the grocer’s itch mite, Glycyphagus domesticus, the spiny ratmite, Laelaps echidnina, the straw itch mite, Pyemotes tritici, the baker’s mite, Acarussiro, and the dried fruit mite, Carpoglyphus lactis, may occasionally be involved in casesof dermatitis. However, these cases are usually limited to those persons with occupa-tions bringing them into prolonged, close association with these products. Again, noneof these species can live on or in human skin.
Body and head lice, Pediculus humanus corporis and P. humanus capitis, can causediscomfort and itching. Pubic lice, Pthirus pubis, live on humans in the pubic andperianal regions. However, lice are large enough to see, and thus are usually foundduring a physical exam.
If a patient is elderly or has poor eyesight, fleas may be the cause of their mysteriousbites in the home. Slowly pulling a white towel or part of a sheet around in the patient’shouse should yield several fleas if the house is infested. Incidentally, homeowner fleaproblems seem to have increased in the last decade or so.
Bed bugs also could be the cause of mysterious bites. Usually, bed bugs are aproblem only where primitive and unsanitary conditions exist; however, they mayoccasionally be introduced into affluent homes, hotels, and institutions. One sign ofbed bug infestation is the presence of small specks of blood on bedding or skin. Uponexamination of the premises, bed bugs can be found (they are plenty big enough tosee) beneath loosened wallpaper, in the seams of bedding, or in cracks in the furniture.They are similar in size and appearance to immature cockroaches.
Again it must be emphasized that cases of imaginary insect or mite infestations mustbe carefully investigated to rule out actual arthropod causes. Scrapings of skin lesionsshould be taken for examination for scabies mites. A competent entomologist shouldexamine the patient’s workplace and/or residence for evidence of insects or mites.Careful attention should be given to rat- or bird-infested dwellings, since they mayharbor parasitic mites. If repeated collection attempts, skin scrapings, and/or insecti-cidal treatments are unsuccessful, and if the patient exhibits symptoms consistent withdelusions of parasitosis, then a diagnosis of DOP should be strongly considered.
III. DELUSIONS OF PARASITOSIS
I usually encounter about 5 to 10 cases of DOP each year (Table 1 is a partial listingof delusory parasitosis cases and workplace infestations I have investigated). Thedisorder shows patterns of typical behavior.3
Sometimes an initial and real insect infestation precedes and triggers the delusion.In a majority of cases the victim is an elderly white female, and the “bugs” may appearand disappear while they are being watched; they enter the skin and reappear andinvade the hair, nose, and ears (in one case I was investigating, while I was there thewoman cried out loudly saying that one of the mites had suddenly run up her nose).Oddly, DOP patients often claim that the bugs are in their rectum or vagina, onlycoming out at night. The patients claim that the “bugs” are able to survive repeatedinsecticidal sprays and the use of medicated shampoos and lotions. Frequently there

70
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
is a history of numerous visits to medical doctors and dermatologists. Lesions may bepresent, although neurotic excoriation may be the cause.4 The physician or entomolo-gist is often presented with tissue paper, small bags, or other containers with thepresumed pests (Figure 1). However, these usually contain dust, specks of dirt, driedblood, pieces of skin (Figure 2), and occasionally common (nonharmful) householdinsects or their body parts. Alexander2 said that presentation of such “evidence,”together with the intensity of the patient’s belief, is almost pathognomonic of thedisorder. Out of desperation the victims may move out of their home, only to reportlater that the “bugs” have followed them there too. An affected person may be sopositive of his infestation and give such a detailed description that other familymembers may agree with the patient. They may even be “infected” themselves; thus,the delusion has been transferred. Sometimes affected persons become excessivelypreoccupied with cleanliness and spend all available money on cleaners, soaps,disinfectants, insecticides, etc. in order to thoroughly clean, scrub, and sterilize theirhome.
The following are some excerpts from letters received in my office from patientsapparently suffering from DOP.
Table 1Breakdown of Selected Imaginary Insect or Mite Infestations Reportedto the Mississippi State Department of Health, 1989–95
EntityCase No. Affected Age Sex Race Complaint
1. Individual ~60 M B “Parasites in rectum and penis; come outat night to bite”
2. Individual Elderly F W “Mites on the skin”3. Individual 40 M B “Bugs going in and out of skin”4. Individual ~60 F W “Bugs in my rectum”5. Individual 65 F W “Bugs biting like fire; making life
miserable”6. Individual 70 F W “Longstanding mite infestation on skin”7. Individual 33 M W “Mite infestation; appears as white smoke
or flakes”8. Individual Elderly F W “Being taken over by bugs”9. Individual 75 F W “Must be ticks and fleas in my house”
10. Individual 50 M W “Mysterious bug bites for years”11. Individual ~60 F B “Tiny bugs gliding over my body”12. Individual ~60 F W “Tiny insects in my ear for 9 mos”13. Individual ~60 F W “Tiny mites biting and making life
miserable”14. Workplace 25–55 F W “Paper mites in medical records”15. Workplace 18–50 F W, B “Mites in boxes and shipping crates”16. Workplace 21–48 F W, B “Paper and computer mites in medical
records”17. Workplace 21–50 F W, B “Paper and computer mites in medical
records

71
Delusions of Parasitosis (Imaginary Insect or Mite Infestations)
Figure 1Example of samples sent in to the Mississippi Department of Health for possible “insect infestation.”
Figure 2Pieces of skin from a sample sent in by a DOP patient.

72
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Patient 1: Elderly Female
The attached package of specimens were (sic) taken from objects in my house whenthey could be seen — the beds, bathtub, and from myself when I could both seeand feel them. I picked them up with a Lysol solution cloth or paper towel . . . Myhouse has been sprayed and fumigated many times . . . I have been told that if Ihave mites, I could not see them . . . Please let me know how to capture somethingso small, and mites which cannot be seen. These are making life miserable for me. . . Is there a possibility that my trouble could be some type of fly larva?
Patient 2: Elderly Female
I couldn’t get everything in the (other) containers into this one, and left those thathad fallen to the bottom, here. In transferring from 3 containers to this one I’m suresome specimens were left clinging. This is a three day accumulation. There weredefinitely [her underline] 6–8 live, jumpy specimens. Thank you! I hope you willinspect everything, even scraping the sidewalls (of the container), and top and thosethat are almost invisible to the naked eye.
These two accounts are quite typical of cases I have investigated. From reading thesetwo letters it seems that affected patients obsessively feel there are mites, invisible to
CASE HISTORY
“MITES” IN A WOMAN’S EAR
A 60-year-old white female came to my office after she had been to a family practitionerand three dermatologists to no avail with the problem of “tiny insects living on her skin,but especially inside the ears.” Upon being seen, she presented samples she had collected— several coffee cups, small pill bottles, and vials, all containing skin scrapings, ear wax,and/or dried blood. During interview she stated that the problem began 9 months earlieras an infestation on the skin but, due to repeated pesticide treatments (on her skin), was nowin her ears. She also revealed that she regularly forced Kwell® (1% lindane) into her earsvia a syringe. Other extreme measures to rid her and her house of the “bugs” includedintensive scrubbing of floors and walls, and “rubbing her skin raw.”
Careful examination of the patient and the samples she had brought revealed no evidenceof insect or mite infestation. Previous examinations by dermatologists had ruled out scabies.Based upon the characteristic presentation of “imaginary bugs” in this case, results of theinterview and exam, and history of numerous visits to various physicians, a tentativediagnosis of delusions of parasitosis (DOP) was made. The patient was referred back to herfamily physician with instructions to have him contact the author for further discussion.
Comment. DOP is more common than one might think. During 3 years, 14 cases werereported to the Mississippi Department of Health. Certainly, many more cases never getreported to a state public health agency.
(Adapted from J. Agromed. 2, 53, 1995, copyright 1995, the Haworth Medical Press,Binghamton, NY, with permission.)

73
Delusions of Parasitosis (Imaginary Insect or Mite Infestations)
Figure 3An interdisciplinary approach to treatment of DOP (From: Infections in Medicine, 15, 169, 1998).
the naked eye, that readily infest humans. It may be a fear of the unknown, that thereare invisible insects or mites that nobody knows much about (even “doctors”)contributing to this delusion. Thus, whenever these patients feel a tingling sensationor have an itchy place on their skin, they are afraid and later become convinced thatmites are on or under their skin.
On the other hand, there may be internal physiological causes of the pruritus,mistakenly believed to be arthropod-produced, such as diabetes, icterus, atopic derma-titis, and lymphoblastomas. At times, the mental disturbance of pellagra takes the formof delusion of parasitosis and disappears with appropriate therapy.4 Hinkle4a listed 50common prescription drugs and their side effects including parathesias, itching,urticaria, and rash. One case of DOP was clearly attributed to cocaine abuse.4b
After ruling out actual arthropod causes (see previous section) and underlyingmedical conditions, physicians may wish to refer the patient to a psychiatrist. But mostDOP patients will not see a psychiatrist. Instead, they will seek out another physician,thus starting the whole process over. An interdisciplinary approach, mainly involvingfamily practice physicians, dermatologists, psychiatrists, and entomologists (Figure 3),is needed to help DOP patients. Family practice physicians or general practitioners areusually the first providers who see DOP patients. Physicians need to be careful not todiagnose “insect bites” based upon lesions alone and should call upon entomologiststo examine samples. Entomologists need to understand the medical complexity ofdelusions — that there are intensive worries, true delusions, and a whole host ofabnormal personality traits associated with DOP — and avoid any hint of medicalevaluation of the patient. Treatment strategies — including the antipsychotic drugpimozide — have been proposed.5-8 Many dermatologists report good success in

74
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
treating DOP patients with pimozide; however, the drug has several adverse effects andshould only be used with careful supervision.
IV. WORKPLACE INFESTATIONS
Computer, paper, or cable mite dermatitis in a workplace may not be strictly a delusionof parasitosis. Often, these people are actually experiencing a prickling, tingling, orcreeping sensation caused by a real substance in their environment (rock wool orfiberglass insulation, paper fragments, dust, and other debris).9 This problem isexacerbated by mass hysteria (“Every time I come to work here I get bitten by tinymites!”). Imaginary mite infestations in the workplace typically involve females whowork with old, dusty records or elaborate electronic equipment. I have seen this severaltimes in hospital medical records offices. Contributing factors include inadvertentconfirmation by physicians, bites from fleas or mosquitoes at home being scratched atwork, and unscrupulous pest control operators willing to spray for computer or cablemites in the absence of a real pest.
Dealing with an imaginary workplace infestation is difficult. First of all, a competentpest control operator should inspect the premises, looking for possible causes of themysterious biting. He or she should set glue boards (sticky traps) in affected areas andcheck them at regular intervals. If there is an actual arthropod pest in sufficient numbersto bite employees, they will likely be captured on the monitoring devices. If no actualinsect or mite infestation can be identified in the affected area, then environmentalfactors such as carpets, paper splinters and particles, static electricity, ventilationsystems, and indoor air pollutants must be considered. Sometimes hiring an “outside”cleaning crew to thoroughly clean the area will eliminate the supposed infestaiton. Ifproblems continue, an industrial hygienist should be consulted for inspection for thesetype of irritants.
REFERENCES1. Schrut, A. H. and Waldron, W. G., Psychiatric and entomological aspects of delusionary
parasitosis, J. Am. Med. Assoc., 186, 213, 1963.
2. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 25.
2a. Slaughter, J. R., Zanol, K., Rezvani, H., and Flax, J. F., Psychogenic parasitosis, a case seriesand literature review, Psychosomatics, 39, 491, 1998.
2b. Zanol, K., Slaughter, J., and Hall, R., An approach to the treatment of psychogenicparasitosis, Inter. J. Dermatol., 37, 56, 1998.
3. Goddard, J., Analysis of 11 cases of delusions of parasitosis reported to the MississippiDepartment of Health, S. Med. J., 88, 837, 1995.
4. Obermayer, M. E., Dynamics and management of self-induced eruptions, Calif. Med., 94,61, 1961.
4a. Hinkle, N., Delusory parasitosis, American Entomol., 46, 17, 2000.
4b. Elpern, D.J., Cocaine abuse and delusions of parasitosis, Cutis, 42, 273, 1988.
5. Gould, W. M. and Gragg T. M., Delusions of parasitosis — an approach to the problem,Arch. Dermatol., 112, 1745, 1976.
6. Koblenzer, C. S., Psychocutaneous Disease, Grune and Stratton, Orlando, FL, 1987, pp.116–120.

75
Delusions of Parasitosis (Imaginary Insect or Mite Infestations)
7. Torch, E. M. and Bishop, E. R. Jr., Delusions of parasitosis — psychotherapeuticengagement, Am. J. Psychother., 35, 101, 1981.
8. Driscoll, M.S., Rothe, M.J., Grant-Kels, J.M., and Hale, M.S., Delusional parasitosis: adermatologic, psychiatric, and pharmacologic approach, J. Am. Acad. Dermatol., 29, 1023,1993.
9. Possick, P. A., Gellin, G. A., and Key, M. M., Fibrous glass dermatitis, Am. Ind. Hyg. Assoc.J., p. 12, Jan–Feb, 1970.


PART II
IDENTIFICATION OFARTHROPODS AND THE
DISEASES THEY CAUSE


79
Identification of Medically Important Arthropods
CHAPTER 8
IDENTIFICATION OFMEDICALLY IMPORTANT
ARTHROPODS
TABLE OF CONTENTS
I. Principles of Identification and Naming ......................................................... 79
II. Brief Review of Arthropod Morphology ......................................................... 80A. Introduction .................................................................................................. 80B. Characteristics of Insects ............................................................................. 81C. Characteristics of Spiders ............................................................................. 82D. Characteristics of Mites and Ticks .............................................................. 85E. Characteristics of Scorpions......................................................................... 85F. Characteristics of Centipedes and Millipedes ............................................ 85
III. Identification Keys ............................................................................................ 87
IV. Other Clues to Identifying an Offending Arthropod ..................................... 97
I. PRINCIPLES OF IDENTIFICATION AND NAMING
Precise identification of an offending arthropod is extremely important in medicalsettings and may have far-reaching implications. For example, a person bitten by anonpoisonous spider does not need the expensive and intense treatments that a personbitten by a poisonous spider needs. Also, treatment recommendations for pubic licediffer radically from those for nymphal ticks in the pubic region (yet the two are oftenconfused). Obviously, accurate identification is crucial from the outset.
Entomologists have their own jargon and terminology, as do all specialties. How-ever, this terminology can be deciphered once the reader understands the basis for

80
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
arthropod naming. Generally, arthropods aregrouped into classes, orders, families, gen-era, and species according to shared com-mon morphological structures. Specimenswith eight legs and two body regions areplaced in one category, specimens with sixlegs and three body regions are placed inanother, etc. Making things easier, many timesthe names assigned to these categories aredescriptive of the arthropods in that cat-egory. For example, insects with two wingsare in the order Diptera, meaning two wings(other common insect orders are provided inTable 1). Species names may further describethe arthropod — Buggus erythrocephalawould mean having a red head, the termmelanogaster would mean dark or black belly,the name Calliphora vomitoria or C.cadaverina for a blowfly would give thereader some idea of what kind of thingsthese flies are attracted to or breed in. However, not all names given to arthropods aredescriptive of the organism; some memorialize a specialist in that field. Buggus parkeri,bacoti, kochi, blakei, walkeri, or smithi would be named after Drs. Parker, Bacot, Koch,Blake, Walker, or Smith, respectively. The first person to describe a new species (andpublish the name) becomes the author of that scientific name and that person’s nameis often cited with the arthropod, e.g., Phlebotomus diabolicus Hall. If subsequently thespecies is moved to another genus through some kind of taxonomic revision, theauthor’s name is retained but in parenthesis — Lutzomyia diabolica (Hall). If twospecies are subsequently determined to be the same species (things like this happenfrequently), the oldest described species — first published one — becomes the officialname. The other name is then considered a synonym and goes away. Governing allthis is the standard code of rules of nomenclature that has been laid down by theInternational Commission on Zoological Nomenclature.
II. BRIEF REVIEW OF ARTHROPOD MORPHOLOGYA. Introduction
There is tremendous variety among the arthropods, but identification of the majorgroups is not difficult if one is familiar with their general morphology. In fact, it is rarelynecessary to use a microscope to separate the classes of Arthropoda (insects, spiders,scorpions, etc.). Table 2 presents a summary of the key characteristics of these classes.On the other hand, more specific identification of specimens beyond the “class” canbe difficult without aid of proper literature and, perhaps, special training. Identificationto the species level often must be done by specialists who conduct taxonomic researchwith that particular group. For outside help with identifications, try a local universityentomology department (usually at the land grant universities), a military base (theArmy and Navy employ over 100 professional entomologists), or the entomologydepartment of the Smithsonian Institution.
Table 1Names of Some CommonInsect Orders
Insect Order Common Names
Ephemeroptera MayfliesOdonata Dragonflies, damselfliesOrthoptera Grasshoppers, cricketsBlattaria CockroachesIsoptera TermitesPhthiraptera LiceHemiptera BugsColeoptera BeetlesSiphonaptera FleasDiptera FliesLepidoptera Butterflies, mothsHymenoptera Ants, wasps, bees

81
Identification of Medically Important Arthropods
Table 2Key Characteristics of Adults of Selected Arthropod Groups
Arthropod Group Key Characteristics
Insects • Six legs• Three body regions — head, thorax, abdomen• Some with wings
Spiders • Eight legs• Two body regions — cephalothorax, abdomen
Mites and Ticks • Eight legs (as adults)• One globose or disk-shaped body region• No true head, mouthparts only
Scorpions • Eight legs• Broad, flat body region and posterior tail with sting
Centipedes • Numerous legs, “hundred leggers”• One pair of legs per body segment• Often dorsoventrally flattened
Millipedes • Numerous legs, “thousand leggers”• Two pair of legs per body segment• Often cylindrical
B. Characteristics of Insects (Class Hexapoda)
Like all arthropods, insects possess a segmented body and jointed appendages. Beyondthat, however, there is tremendous variation: long legs, short legs; four wings, twowings, no wings; biting mouthparts, sucking mouthparts; soft bodies, hard bodies; etc.Compounding identification problems, immature forms of most insects look nothinglike the adults. Despite the diversity, adults can at once be recognized as insects byhaving three pairs of walking legs and three body regions, or tagmata: head, thorax(bearing legs, and wings if present), and abdomen (Figure 1). No other arthropods havewings. However, some insect groups may have never had wings, or have lost themthrough adaptation. In particular, several medically important species are wingless (lice,fleas).
Identification of immature insects presents entirely different problems. In those insectsthat have simple metamorphosis (grasshoppers, lice, true bugs), the immatures (callednymphs) look like the adults, get larger at each molt, and develop wings (if present)during later molts (Figure 2). Identifying nymphs as insects and placing them in theirproper orders is generally not a problem. However, in those groups with completemetamorphosis (beetles, flies, bees and wasps, moths and butterflies, fleas, etc.), theimmature stage, or larva, looks nothing like the adult (Figure 3). Often, the larva is worm-like. The three body regions are never as distinct as they are in adults, but generally thethree pairs of walking legs are evident, although they are often extremely short. Fly larvae(maggots) lack walking legs and, although some (such as mosquitoes) have three bodyregions, others (such as houseflies, blowflies, etc.) have no differentiated areas (Figure4A). Caterpillars and similar larvae often appear to have legs on some abdominalsegments (Figure 4D). Close examination of these abdominal “legs” (prolegs) reveals thatthey are unsegmented fleshy projections, with or without a series of small hooks

82
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 2Head lice life cycle — example of simple metamorphosis (from: U.S. DHHS, CDC, Publ. No. 83-8297).
(crochets) on the plantar surface, and structurally quite unlike the three pairs ofsegmented walking legs on the first three body segments behind the head.
C. Characteristics of Spiders (Class Arachnida, Order Aràneae)
A spider has two body regions — an anterior cephalothorax and posterior abdomenconnected by a waist-like pedicel (Figure 5). The former bears head and thorax
Figure 1Insect with body regions labeled (A), and several representative insects (B) (from: U.S. DHEW,PHS, CDC, Pictorial Keyes).

83
Identification of Medically Important Arthropods
Figure 3House fly life cycle — example of complete metamorphosis (from: U.S. DHHS, CDC, Publ. No. 83-8297).
Figure 4Various types of insect larvae: fly (A), flea (B), beetle (C), moth (D), and another kind of beetle(E) (from: U.S. DHEW, PHS, CDC, Pictorial Keys).

84
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 5Various spiders: top, tarantula; middle, brown recluse; bottom, black widow dorsal view (from:U.S. DHEW, PHS, CDC, Pictorial Keys).
structures, including four pairs of walking legs, generally eight simple eyes on theanterior dorsal surface, and mouthparts. The mouthparts, called chelicerae, are gener-ally fang-like and are used to inject poison into prey, all spiders being predaceous.Located between the chelicerae and the first pair of walking legs are a pair of shortleg-like structures called pedipalpi that are used to hold and manipulate prey. Pedipalpimay be modified into copulatory organs in males. The abdomen is usually unsegmentedand bears spinnerets for web production at the posterior end. Immatures look the sameas adults, except smaller.
Harvestmen, or daddy longlegs (order Opiliònes), have many characteristics incommon with true spiders; however, they differ in that the abdomen is segmented andis broadly joined to the cephalothorax (not petiolate). Most species have extremelylong, slender legs.

85
Identification of Medically Important Arthropods
D. Characteristics of Mites and Ticks (Class Arachnida, Subclass Acari)
These small arachnids characteristically have only one apparent body region (cepha-lothorax and abdomen fused), the overall appearance being globose or disk-shaped inmost instances (Figure 6). This general appearance quickly separates the Acari fromother arthropods. The body may be segmented or unsegmented with eight walking legspresent in adults. Larvae, the stage just out of eggs, have only six (rarely, fewer) legs,but their single body region readily separates them from insects. They attain their fourthpair of legs at the first molt, and hereafter are called nymphs until they become adults.As in spiders, immature ticks and mites are generally similar in appearance to adults.In general, ticks are considerably larger than mites. Adult ticks are generally pea-sized;mites are about the size of a grain of sand (often even smaller).
E. Characteristics of Scorpions (Class Arachnida, Order Scorpiònes)
The body of a scorpion is easily separable into an anterior broad, flat area and aposterior “tail” with a terminal sting (Figure 7). Although these outward divisions donot correspond with actual lines of tagmatization, they do provide an appearancesufficient to distinguish these arthropods from most others. Like spiders, the mouthpartsare chelicerae and the first elongate appendages are pedipalpi. The pedipalpi aremodified into pinchers and are used in prey capture and manipulation. Four pairs ofwalking legs are present. Immatures are similar to adults in general body form.
F. Characteristics of Centipedes and Millipedes (Classes Chilopodaand Diplopoda)
Centipedes and millipedes bear little resemblance to the other arthropods previouslydiscussed. They have hardened, elongated “worm-like” bodies with distinct heads andmany pairs of walking legs. Centipedes — often commonly called “hundred leggers”— are swift-moving predatory organisms with one pair of long legs on each bodysegment behind the head (Figure 8). Millipedes (“thousand leggers”), on the otherhand, are slow-moving omnivores or scavengers that have two pairs of short legs on
Figure 6Tick (A) and mite (B) (from: U.S. DHEW, PHS, CDC, Pictorial Keys).

86
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 8Centipedes (A, B) and millipede (C) (from: U.S. DHEW, PHS, CDC, Pictorial Keys).
Figure 7Typical scorpion (from: U.S. DHEW, PHS, CDC, Pictorial Keys).

87
Identification of Medically Important Arthropods
each body segment (after the first three segments which only have one pair each)(Figure 8). Immatures are similar to the adults.
III. IDENTIFICATION KEYS
The identification of a particular arthropod to place it in its correct class, order, family,genus, or species is achieved by finding the answers to a paired series of questions setout in the form of keys. Most keys are dichotomous, giving the reader two choices ineach couplet, and the reader is then referred to another couplet depending upon theanswer. This flow chart of sorts continues until an identification is reached. Some keyshave good pictures and illustrations to aid in the identification while others have nothingbut written descriptions. For example, a key couplet might refer the reader to look atthe wing of an insect and compare it to a line drawing of several variations of wings(see Figure 9 for an example). The chart that follows is an updated and revised Centersfor Disease Control (CDC) pictorial key to the arthropods of medical importance. Thischart is provided to enable the non-entomologist reader to identify an arthropod inquestion to major group or family level. In addition to this chart, morphologicalcharacteristics and helpful identification hints for each of the arthropod groups discussedin this book are provided in each of the respective chapters dealing with those groups.
Figure 9Example of how identification keys work. A specimen is compared to line drawings. Note how thewing veins of the fly in the hand match those in the line drawing.

88
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
KEY TO SOME COMMON CLASSES AND ORDERS OFARTHROPODS OF MEDICAL IMPORTANCE
Three or four pairs of legssee Set 2
Five or more pairs of legssee Set 22
2
1
Three pairs of legs, with antennae
Class Insecta(Insects)
see Set 3
Four pairs of legs, without antennae
Class Arachnida(Scorpions, Spiders, Ticks, etc.)
see Set 20
3
Wings present, well developedsee Set 4
Wings absent or rudimentarysee Set 12

89
Identification of Medically Important Arthropods
KEY TO SOME COMMON CLASSES AND ORDERS OFARTHROPODS OF MEDICAL IMPORTANCE (continued)
4
One pair of wings
Order Dipterasee Set 5
Two pairs of wingssee Set 6
5
Wings with scales
MosquitoesWings without scales
Other flies
6
Sucking mouthparts, consisting of anelongated proboscis
see Set 7
Biting/chewing mouthpartssee Set 8

90
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
7
Wings usually totally covered with scales,proboscis coiled up under head
Order Lepidoptera(Butterflies and Moths)
Wings not covered with scales,proboscis directed backward between
front legs when not in use
Order Hemiptera(True Bugs and Kissing Bugs)
8
9
Both pairs of wings membranous andsimilar in structure, although they
may differ in sizesee Set 9
Front pair of wings leathery orshell-like, serving as covers for the
membranous hind wingssee Set 10
Hind wings much smaller than front wings
Order Hymenoptera(Bees, Wasps, Hornets, and Ants)
Both pairs of wings similar in size
Order Isoptera(Termites)
KEY TO SOME COMMON CLASSES AND ORDERS OFARTHROPODS OF MEDICAL IMPORTANCE (continued)

91
Identification of Medically Important Arthropods
KEY TO SOME COMMON CLASSES AND ORDERS OFARTHROPODS OF MEDICAL IMPORTANCE (continued)
10
Front wings somewhat hardenedwithout distinct veins, meeting ina straight line down the middle
see Set 11
Front wings leathery or paperlikewith a network of veins, usually
overlapping at the middle
Order Orthoptera(Cockroaches, Crickets,
Grasshoppers)(Note: Cockroaches now placed
in order Blatteria)
11
Abdomen with prominent forceps,wings shorter than abdomen
Order Dermaptera(Earwigs)
Abdomen without forceps,wings typically covering abdomen
Order Coleoptera(Beetles)
12
Abdomen with three elongate, tail-likeappendages at tip, body usually
covered with scales
Order Thysanura(Silverfish and Fire Brats)
Abdomen without three longtail-like appendages at tip,
body not covered with scalessee Set 13

92
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
13Abdomen without narrow waist
see Set 14
14Abdomen with prominent pair of forceps
Order Dermaptera(Earwigs)
Abdomen without forcepssee Set 15
Abdomen with narrow waist
Order Hymenoptera(Ants)
15
Body strongly flattened from side toside, antennae small, fitting into
grooves in side of head
Order Siphonaptera(Fleas)
Body not strongly flattened from side toside, antennae projecting from side
of head, not fitting into groovessee Set 16
KEY TO SOME COMMON CLASSES AND ORDERS OFARTHROPODS OF MEDICAL IMPORTANCE (continued)

93
Identification of Medically Important Arthropods
KEY TO SOME COMMON CLASSES AND ORDERS OFARTHROPODS OF MEDICAL IMPORTANCE (continued)
17
Pronotum covering head
Order Blatteria(Cockroaches)
Pronotum not covering head
Order Isoptera(Termites)
18
Mouthparts consisting of tubular jointedbeak, tarsi three- to five-segmented
Order Hemiptera(Bedbugs)
Mouthparts retracted into heador of the chewing type, tarsi
one- or two-segmentedsee Set 19
16
Antenna with nine or more segmentssee Set 17
Antenna with three to five segmentssee Set 18

94
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
19
Mouthparts retracted into head, adaptedfor sucking blood, external
parasites of mammals
Order Phthiraptera(Sucking Lice)
Mouthparts of the chewing type,external parasites of birds
and mammals
Order Phthiraptera(Chewing Lice)
20
Body oval, consisting of asingle saclike region
Subclass Acari(Ticks or Mites)
Body divided into two distinctregions, a combined head-thorax
and an abdomensee Set 21
21
Abdomen joined to head-thorax(cephalothorax) by a slender waist,
abdomen with segmentationindistinct or absent, stinger absent
Order Araneae(Spiders)
Abdomen broadly joined tocephalothorax, abdomen distinctlysegmented, ending with a stinger
Order Scorpiones(Scorpions)

95
Identification of Medically Important Arthropods
KEY TO SOME COMMON CLASSES AND ORDERS OFARTHROPODS OF MEDICAL IMPORTANCE (continued)
22
Five to nine pairs of legs in somespecies, swimmerets in others, one or two
pairs of antennae present, principallyaquatic organisms
Subphylum Crustacea(Crabs, Crayfish, Shrimp
and Copepods)
23Ten or more pairs of legs, swimmeretsabsent, one pair of antennae present,terrestrial organisms, body segments
each with only one pair of legs
Class Chilopoda(Centipedes)
Ten or more pairs of legs, swimmeretsabsent, one pair of antennae present,terrestrial organisms, body segments
each with two pairs of legs
Class Diplopoda(Millipedes)

96
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Table 3Some Questions that May be Helpful in Determining the OffendingArthropod or Other Causes of Unexplained Dermatitisa,b
Question to Ask Patient Possible Cause
Preliminary General Questions
Where do you work?/Nature of work? Occupational exposure to arthropods or irritating fibers, e.g., fiberglass
At work do you sit/stand directly under AC Fiberglass or other fibers hitting them vents, fans, etc.Any curtains or carpets installed or cleaned? Fibers from such items can cause irritationWhat time of year did lesions occur? Spring and summer — arthropods likely
Patient Remembers Seeing/Removing the Biting/Stinging Bug
Was it “worm-like”? Centipede, caterpillarWas it firmly attached? Tick, pubic liceDid it jump greatly? FleaWas it “beetle-like”? Blister beetleWas it very tiny (head of a pin or smaller)? Mite, immature tickDid it fly off? Biting fly, mosquito, bee, wasp, hornet
Patient Did Not See/Remove Arthropod
What time of day did these lesions occur? If night — mosquitoes, if outdoors or unscreened house; bed bugs also possible (indoors)
Where were you when these lesions occurred? Outdoors — biting flies, mosquitoes, fire ants, chiggers;Indoors — fleas, mites, bed bugs
Do you own pets (especially ones which go Fleas, ticks, cheyletiellid mites outside)?Did you go hiking, fishing, or hunting prior to Ticks, chiggers, biting flies, mosquitoes, etc. lesion development?Did you work in the yard or garden prior to Biting flies, mosquitoes, fire ants, chiggers, lesion development? etc.Did you go berry picking, flower digging, or Chiggers, ticks, mosquitoes, biting flies, fire do some other activity prior to lesion ants development?Were you cleaning out an attic, garage, or Spiders, scorpions shed prior to lesion development?Are there bats or bird nests in your attic or Mites, soft ticks under the eaves of your windows?
a Not exhaustive.b Intended as a guide only.

97
Identification of Medically Important Arthropods
IV. OTHER CLUES TO IDENTIFYING AN OFFENDINGARTHROPOD
When a patient with a lesion supposedly caused by an arthropod comes to a clinic,efforts should be made to identify that organism or at least make an educated guess.Sometimes, pertinent questions about the patient’s activities just prior to lesion devel-opment are helpful in making this determination. Table 3 is a listing of such questionsand the corresponding arthropods. This table is by no means exhaustive and is offeredas a guide only. Certainly, in tropical and subtropical areas the list of possible offendingarthropods is almost endless.


99
Principles of Treatment for Arthropod Bites, Stings, and Other Exposure
CHAPTER 9
SIGNS AND SYMPTOMSOF ARTHROPOD-BORNE
DISEASES
TABLE OF CONTENTS
I. Introduction ....................................................................................................... 99
II. Common Signs and Symptoms ........................................................................ 99
I. INTRODUCTION
The human body may react in various ways to disease pathogens and/or introducedforeign substances such as arthropod venom or saliva. One might think, therefore, thata careful listing of signs and symptoms of arthropod-caused problems would be usefulto the practicing clinician in making diagnoses. Unfortunately, these reactions are rarelyspecific for one particular pathogen or offending arthropod. However, the presence ofcertain signs and symptoms may alert physicians to diagnostic possibilities. Furtherconfirmation may be aided by specific laboratory findings. The following is analphabetical listing of common signs and symptoms of arthropod-borne diseases. Byno means should it be considered as a complete differential diagnosis of any of thesymptoms discussed.
II. COMMON SIGNS AND SYMPTOMS
Acute abdomen. Rigid, board-like abdomen, accompanied by intense pain, is oftena sign of a black widow spider bite. It is caused in this case by the neurotoxic effectsof the venom.

100
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Adenopathy. There may be generalized adenopathy in the early stages of Africantrypanosomiasis — the glands of the posterior cervical triangle being most conspicu-ously affected (Winterbottom’s sign). Also, generalized adenopathy may be seen in theacute stage of Chagas’ disease.
Anaphylaxis. Anaphylactic shock is often a result of arthropod stings (less com-monly, bites), hypersensitivity to arthropod venom or saliva being the cause in thiscase.
Anemia. Anemia may be seen in cases of malaria, babesiosis, and trypanosomiasis.Anemia can be especially severe in falciparum malaria. In addition, systemic reactionsto brown recluse spider bites (systemic loxoscelism) may result in hemolytic anemia.
Asthma, bronchial. Cockroaches and house dust mites are important causes ofnasal allergies and asthma, especially in children. Recently, there has been increasedawareness that asthma in urban-dwelling children may be due to (or at least exacer-bated by) cockroaches.
Axillary pain, acute. Venoms from arthropod stings may be transported to axillarylymph nodes and cause transient intense pain. This is especially true for some of thestinging caterpillars.
Blister. A blister may occur at arthropod bite sites. Blistering may also occur as aresult from blister beetles contacting human skin.
Bulls-eye rash. See Erythema Migrans.Chagoma. Indurated, erythematous lesion on the body (often head or neck)
caused by Trypanosoma cruzi infection (Chagas’ disease). May persist for 2 to 3months.
Chyluria. Presence of chyle (lymphatic fluid) in the urine. Often seen in lymphaticfilariasis. Urine may be milky white and even contain microfilariae.
Coma. Sudden coma in a person returning from a malarious area suggests cerebralmalaria. Also, African trypanosomiasis (sleeping sickness) may lead to coma after a longperiod of increasingly severe symptoms of meningoencephalitis. Rocky Mountainspotted fever and other rickettsial infections may lead to coma.
Conjunctivitis. Chronic conjunctivitis may occur in onchocerciasis and Chagas’disease.
Dermatitis. Several arthropods may directly or indirectly cause dermatitis. Chiggersand other mites may attack the skin, causing a maculopapular rash. Scabies mites mayburrow under the skin’s surface making itchy trails or papules. Lice may give rise tohypersensitivity reactions with itchy papules. Chigoe fleas burrow in the skin (espe-cially on the feet), causing local irritation and itching. Macules or erythematous nodulesmay result as a secondary cutaneous manifestation of leishmaniasis.
Diarrhea. Leishmaniasis (specifically kala-azar) may lead to mucosal ulcerationand diarrhea. In falciparum malaria, plugging of mucosal capillaries with parasitized redblood cells may lead to watery diarrhea.
Edema. Edema may result from arthropod bites or stings. Large (but still contigu-ous) areas or edema from bites or stings are known as large local reactions. Loiasis (anematode worm transmitted by deer flies) may cause unilateral circumorbital edemaas the adult worm passes across the eyeball or lid. Passage of the worm is brief, butinflammatory changes in the eye may last for days. Loiasis may also lead to temporaryappearance of large swellings on the limbs, known as Calabar swellings at the siteswhere migrating adult worms occur. Unilateral edema of the eyelid, called Romaña’ssign, may occur in Chagas’ disease. African trypanosomiasis (sleeping sickness) mayresult in edema of the hips, legs, hands, and face.

101
Principles of Treatment for Arthropod Bites, Stings, and Other Exposure
Elephantiasis. Hypertrophy and thickening of tissues, leading to an “elephant leg”appearance, may result from lymphatic filariasis. Tissues affected may include a limb,the scrotum, and the vulva.
Encephalitis. Inflammation of the brain may result from infectin with any numberof mosquito-borne viruses such as St. Louis, eastern equine, West Nile, and LaCrosseencephalitis viruses.
Eosinophilia. Helminth worms often provoke eosinophilia. Atopic diseases such asrhinitis, asthma, and hay fever also are characterized by eosinophilia.
Eosinophilic cerebrospinal fluid pleocytosis. Cerebrospinal fluid eosinophilic pleo-cytosis can be caused by a number of infectious diseases (including rickettsial and viralinfections), but is primarily associated with parasitic infections.
Epididymitis. Epididymitis, often associated with orchitis, may be an early compli-cation of lymphatic filariaisis.
Erythema migrans. Cutaneous lesion that may follow bites of ticks infected withthe causative agent of Lyme disease, Borrelia burgdorferi. Typically the lesion consistsof an annular erythema with a central clearing surrounded by a red migrating border.Although EM does not always occur, it is virtually pathognomonic for Lyme disease.
Eschar. A round (generally 5 to 15 mm) spot of necrosis may be indicative ofboutonneuse fever (a spotted fever group illness) or scrub typhus. The eschar developsat the site of tick or chigger bite.
Excoriation. Lesions produced by excoriation may be a sign of imaginary insect ormite infestations (delusions of parasitosis).
Fever. Fever may accompany many arthropod-borne diseases, including the rick-ettsioses, dengue, yellow fever, plague, the encephalitides, and others. In some casesthere are cyclical peaks of fever, such as in relapsing fever (tick-borne) or malaria.Falciparum malaria is notorious for causing extremely high fever (107° or higher).Filariasis may be marked by fever, especially early in the course of infection.
Hematemesis. Coffee-ground color or black vomit is a sign of yellow fever.Hemoglobinuria. Falciparum malaria is the cause of “blackwater fever”. Sometimes
systemic reactions to brown recluse spider bites lead to hemoglobinuria.Hives. See Urticaria.Hydrocele. Hydrocele is often a result of lymphatic filariasis, developing as a
sequel to repeated attacks of orchitis.Hyponatremia. Sometimes hyponatremia, or low blood sodium level, is a labora-
tory finding in Rocky Mountain spotted fever.Itch. Intense itching, especially at night, is a sign of scabies infestation. Itch is also
a common result of various insect bites or stings.Kerititis. Inflammation of the cornea is sometimes a result of ocular migration of
Onchocerca volvulus microfilariae. The condition may lead to blindness.Leukocytosis. Leukocytosis may occur in systemic loxoscelism. Systemic loxoscelism
is a rare complication of brown recluse spider bites.Leukopenia. Leukopenia is a prominent sign of ehrlichiosis. It may also occur
(3000 to 6000 per mm3) with a relative monocytosis during the afebrile periods ofmalaria.
Lymphadenitis. Inflammation of one or more lymph nodes may be a sign oflymphatic filariasis — especially the femoral, inguinal, axillary, or epitrochlear nodes.
Lymphangitis. Lymphangitis may be an early symptom of lymphatic filariasis. Thelimbs, breast, or scrotum may be involved.
Lymphocytosis. Lymphocytosis is generally seen in Chagas’ disease.

102
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Maggots. The presence of fly larvae in human tissues is termed myiasis. Variousblowflies, botflies, and other muscoid flies are usually involved.
Meningoencephalitis. Meningoencephalitis may be caused by trypanosomes in thecases of African trypanosomiasis (sleeping sickness) or Chagas’ disease (althoughgenerally milder). Also, falciparum malaria infection may be cerebral, with increasingheadache and drowsiness over several days, or even sudden onset of coma.
Myocarditis. Chagas’ disease often leads to myocardial infection. African trypano-somiasis may also cause myocarditis to a lesser extent.
Necrosis. Cell death caused by progressive enzymatic degradation may result fromspider envenomization, especially the brown recluse, Loxosceles reclusa.
Neuritis. Neuritis may be caused by bee, ant, or wasp venom. Occasionally stingsto an extremity result in weakness, numbness, tingling, and prickling sensations fordays or weeks. Neuritis may also result from infection with the Lyme disease spirochete.
Nodules, subcutaneous. Tick bites may ultimately result in nodules. Fly larvae inthe skin (myiasis) may also present as nodules. Notorious offenders are the humanbotfly larva, Dermatobia hominis, the Tumbu fly, Cordylobia anthropophaga, androdent botfly larvae, Cuterebra spp.
Onchocercoma. Coiled masses of adult Onchocerca volvulus worms beneath theskin enclosed by fibrous tissues may occur in patients living in tropical countriesendemic for ochocerciasis.
Orchitis. Orchitis may result from lymphatic filariasis; repeated attacks may leadto hydrocele.
Paralysis. Ascending flaccid paralysis may result from tick attachment. The paraly-sis is believed to be caused by a salivary toxin injected as the tick feeds.
Proteinuria. Proteinuria, with hyaline and granular casts in the urine, is commonin falciparum malaria.
Puncta. A small, point-like pierce mark may mark the bite or sting site of anarthropod. Paired puncta may indicate spider bite or centipede bite.
Rash. Rash may accompany many arthropod-borne diseases such as Rocky Moun-tain spotted fever, ehrlichiosis, murine typhus, and African trypanosomiasis. The rashmay appear to be ring-like, and expanding in the case of Lyme disease (see ErythemaMigrans). An allergic urticarial rash may be seen in the case of bites or stings.
Rhinitis, allergic. Intermittent or continuous rhinitis may be due to exposure tohouse dust mites or cockroaches.
Romaña's Sign. Early in the course of Chagas’ disease there may be unilateralpalpebral edema, involving both the upper and lower eyelids. This generally occurswhen a kissing bug (the vector of the Chagas’ organsism) bites near the eye.
Shock. Shock may occur from arthropod stings (rarely bites) as a result ofhypersensitivity reactions to venom or saliva. Shock may also accompany falciparummalaria.
Splenomegaly. Splenomegaly may result from lymphoid hyperplasia in both Afri-can and American trypanosomiasis. It may also occur in visceral leishmaniasis (kala-azar).
Swelling. See Edema.Tachycardia. Both African and American trypanosomiasis may produce tachycar-
dia. In Chagas' disease tachycardia may persist into the chronic stage where it may beassociated with heart block.

103
Principles of Treatment for Arthropod Bites, Stings, and Other Exposure
Thrombocytopenia. Although not specific for any one disease, thrombocytopenia— low platelet count — may occur as a result of infection with Rocky Mountain spottedfever organisms.
Ulcers, cutaneous. A shallow ulcer (slow to heal) may be a sign of cutaneousleishmaniasis. In the New World, cutaneous leishmaniasis lesions are most often foundon the ear. Also, a firm, tender, raised lesion up to 2 cm or more in diameter may occurat the site of infection in African trypanosomiasis.
Urticaria. Urticaria may result from an allergic or generalized systemic reaction toarthropod venom or (more rarely) saliva.
Winterbottom’s Sign. In the early stages of African trypanosomiasis, patients mayexhibit posterior cervical lymphadenitis.


PART III
ARTHROPODS OFMEDICAL IMPORTANCE


107
Ants
CHAPTER 10
ANTS
TABLE OF CONTENTS
I. Ants in General ................................................................................................108
II. Fire Ants ...........................................................................................................108A. General and Medical Importance ..............................................................108B. General Description ....................................................................................109C. Geographic Distribution .............................................................................109D. Biology/Behavior .........................................................................................110E. Treatment of Stings .....................................................................................110
III. Harvester Ants ..................................................................................................110A. General and Medical Importance ..............................................................110B. General Description ....................................................................................111C. Geographic Distribution .............................................................................111D. Biology/Behavior .........................................................................................111E. Treatment of Stings .....................................................................................111
IV. Velvet Ants .......................................................................................................113A. General and Medical Importance ..............................................................113B. General Description ....................................................................................113C. Geographic Distribution .............................................................................114D. Biology/Behavior .........................................................................................114E. Treatment of Stings .....................................................................................114
References ......................................................................................................................114

108
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
I. ANTS IN GENERAL
Ants (family Formicidae) are very successful organisms occurring in tremendousnumbers worldwide in terrestrial habitats. They are eusocial insects containing threecastes: queens, males, and workers. Their highly developed social structure makesthem an interesting and much studied group. All ant species may bite (if they arephysically large enough), and some species sting (Color Figure 10-10). In addition,some species emit a foul-smelling substance when handled. The imported fire ants,harvester ants, and velvet ants (not actually ants) are discussed in this chapter. Manyother species may be of public health importance; a few of them are listed in Table 1.
II. FIRE ANTSA. General and Medical Importance
There are some native fire ants in the U.S., but the imported ones, Solenopsis invictaand S. richteri, are the worst pests. Imported fire ants (IFAs) sting aggressively andinject a necrotizing venom consisting primarily of alkaloidal compounds, which theyuse to paralyze or kill their prey. The ants characteristically boil out of their moundsin great numbers at the slightest disturbance (Color Figure 10-11). Worker IFAs attachto the skin of their victim with their mandibles and lower the tip of their abdomento inject the stinger forcefully (Figure 1); therefore, IFAs both bite and sting, but theirstings cause the subsequent burning sensation and wheal. Alexander1 said thecharacteristic symptom of IFA sting is a burning itch. Within 24 h, a pustule developswhich may persist for a week or longer.2 Individuals have sustained up to 10,000
Table 1Some Ants that are Known to Sting People
Scientific Name Common Name Where Occurs
Solenopsis invicta Red imported fire ant (IFA) S. America, Southern U.S.S. richteri Black IFA S. America, Southern U.S.S. xyloni Southern fire ant California to South Carolina down
into parts of FloridaS. geminata Fire ant Texas to South Carolina down to
S. AmericaPogonomyrmex barbatus Red harvester ant Western U.S.P. californicus California harvester ant Western U.S.P. occidentalis Western harvester ant Western U.S.P. badius Eastern U.S.Myrmica rubra U.K.M. ruginodes U.K.Paraponera clavata Viente-cuatro hora hormiga BrazilMonomorium bicolor AfricaMyrmecia gulosa Red bulldog ant AustraliaM. pyriformis Bulldog ant AustraliaM. forficata Australia

109
Ants
Figure 3U.S. Department of Agriculture imported fireant quarantines, generally representing thedistribution of the ants in the U.S. (from: USDA,APHIS, updated January 2002).
IMPORTEDFIRE ANTS
ImportancePainful stings; allergic RXNS
DistributionMuch of southern U.S.; native to South
America
LesionImmediate — erythema and central
wheal, later — pustules
Disease TransmissionNone
Key ReferenceLofgren et al., Ann. Rev. Entomol., 20, 1,
1975
TreatmentPain relievers, antipruritic lotions for
local RXNS; systemic RXNS mayrequire antihistamines, epinephrine,and/or other measures
Figure 2Imported fire ant (from: “Mississippi’s Health,”Summer 1990 issue).
stings without systemic toxic or immunologicreactions.3 However, hypersensitivity to IFAvenom may result in severe allergic reactionsfrom just a few stings (see Chapter 2).
B. General Description
All ants have the first, and sometimes second,segment of the abdomen node-like. Adult workerfire ants (Figure 2) have two nodes, are ap-proximately 4 to 6 mm long, and are reddishbrown (red form, most widely distributed) orbrownish black (black form). Outdoors, fireants are best recognized by the appearance oftheir mounds, which are elevated earthenmounds 8 to 90 cm high surrounded by rela-tively undisturbed vegetation.
C. Geographic Distribution
Both IFA species were accidentally introducedinto the U.S. (in the Mobile area) in the timeperiod of 1918 to 1940. The red form, S. invicta,was brought in from Brazil, and the black form,S. richteri, came from Uruguay. The ants mayhave originally been imported in infested nurs-ery stock or dirt used for ship ballast. Throughsubsequent unintentional dissemination bypeople and through dispersal by flooding andmating flights, the red form has spread rapidly,and its range now extends from the southernAtlantic coast westward into central Texas. Atleast 250 million acres in the U.S. are currentlyinfested. The black form currently occurs only
Figure 1Fire ants bite in order to gain leverage for theact of stinging (from: USDA Yearbook ofAgriculture, 1952).

110
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
in northeastern Mississippi, northwestern Alabama, and a small portion of southernTennessee. States currently reporting IFA infestations are Virginia, North Carolina,South Carolina, Georgia, Florida, Alabama, Mississippi, Arkansas, Louisiana, Oklahoma,Tennessee, and Texas (Figure 3). Recently, fire ants have been reported in New Mexico,Arizona, and California.
D. Biology/Behavior
An IFA colony is usually started by a single fertilized queen with an initial burrow; thefirst eggs are laid from 24 to 48 h after completion of the burrow. Normal developmentfrom egg to worker takes approximately 24 to 30 days depending upon temperatureand available soil moisture. These first workers open the nest and begin to deepen thetunnel. After about 60 days a few minor workers appear, and at about 5 months a fewmajor workers can be found. The nest is further excavated and the characteristic moundbegins to form during the 5-month period after initial colony formation. After 1 year,individuals in the nest may number 10,000 or more, and the colony typically increasesfrom about 30,000 workers after 1 to 11/2 years to around 60,000 workers after 2 to21/2 years. Major workers are 3 to 5 mm long and live 90 to 180 days; queens are abit larger, live 2 to 5 years, and can lay 1,500 eggs a day. A colony is considered tobe mature after 3 years and may contain as many as 200,000 workers or more in someareas. A single mature colony can produce 4,500 potential new queens during a year.Some heavily infested areas may contain 50 to 400 or more mature colonies per acre.Reproduction in the red IFA may occur throughout the year but peaks from late Maythrough August. During nuptial flights, newly inseminated queens select a landing sitesuitable for colony formation, and burrow excavation is begun shortly thereafter.
Fire ants are omnivorous in their feeding habits but prefer insects, spiders, othersmall arthropods, and earthworms over plant feeding. In heavily infested areas, wherefood is in short supply, fire ants will eat the germ plasm of newly germinated seeds,girdle the stems of small seedlings, and consume hatchling vertebrates. Foragingtunnels 15 to 25 m long are used by workers to collect food for the colony. Thesetunnels are excavated just below the soil surface and extend outward from the moundin all directions. Foraging workers travel through these tunnels, emerge from anopening, and search for a food source. Once a food source is located, the foragingworker returns to the tunnel laying a trail of pheromone for other worker ants to follow.
E. Treatment of Stings
Fire ant stings are usually treated in a manner similar to wasp or bee stings. However,the pustules characteristically produced by IFA stings may need to be covered withbandages to avoid excoriation. Ice packs, antibiotic ointments, or hydrocortisonecreams are often used for local reactions, and epinephrine, antihistamines, and othersupportive measures are indicated for more serious, systemic reactions (see Chapter 2).
III. HARVESTER ANTSA. General and Medical Importance
Harvester ants, Pogonomyrmex spp., are dangerous ant species that readily sting peopleand animals (Figure 4). The reaction to their stings is not always localized; it may spread

111
Ants
HARVESTER ANTS
ImportancePainful stings; possible allergic RXNS
DistributionIn U.S., most species western
LesionVariable
Disease TransmissionNone
Key ReferenceCreighton, W. S., Harvard Bull. Mus.
Compar. Zool., Vol. 104, 585 pp.1950
TreatmentLocal RXNS — wash wound; pain
relievers; systemic RXNS may requireantihistamines, epinephrine, and/orother measures
Figure 4Worker harvester ant.
along the lymph vessels, producing intense painin the lymph nodes in the axilla or groin longafter the original sting pain subsides. Althoughrelatively uncommon, systemic hypersensitivereactions may result from harvester ant stings.
B. General Description
Harvester ants are red to dark brown ants 2 to3 times larger than fire ants; they have largewide heads (Figure 5). Several species charac-teristically have many small, parallel ridges onthe head. In addition, a good way to distinguishbetween harvester ants and fire ants is by theshape and size of their mounds (Figure 6).Harvester ant mounds are usually flat or slightlyelevated and are surrounded by an area of novegetation 1 to 3 m or more in diameter. Fire antmounds are distinctly elevated and composedof excavated dirt.
C. Geographic Distribution
There is only one harvester ant species east ofthe Mississippi River, Pogonomyrmex badius,which is distributed throughout the southeast-ern states. In the western U.S. approximately 20species occur. Three of the notorious offendersare the red harvester ant (P. barbatus), theCalifornia harvester ant (P. californicus), andthe western harvester ant (P. occidentalis).
D. Biology/Behavior
These ants are diurnal soil-inhabiting insectsthat build their nests in open areas. They feedon seeds and store them in honeycomb-likechambers within their nests. Harvester ants clearout a large vegetation-free, crater-like area onthe ground surface and have one or more holesleading down into the nest. Like other ants,their colonies consist of at least one reproduc-tive queen, several males, and many non-reproductive female workers. The workers arethe ones that sting to defend the nest.
E. Treatment of Stings
Local first aid for harvester ant stings consists of

112
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 5Microscopic view of harvester ant. Notice large head and mandibles.
Figure 6AHarvester ant mound; actually, a “cleared out” area with a centralized entrance (photocourtesy Dr. Chad P. McHugh, Brooks AFB, Texas).

113
Ants
Figure 6BFire ant mound.
washing the site with soap and water and applying ice packs. Unlike most ant species(and similar to the honey bee), the sting may be torn off in the wound uponenvenomization by P. californicus.4 Allergic reactions may require administration ofepinephrine, antihistamines, and other supportive treatment (see Chapter 2).
IV. VELVET ANTSA. General and Medical Importance
Velvet ants (also sometimes called woolly ants, cow killers, mule killers, or mutillidwasps) are actually wingless female wasps in the family Mutillidae: they only resemblehuge ants (Figure 7). The wingless females have a long stinger and can inflict a painfulsting. They are sometimes a problem to barefoot bathers on sandy beaches.
B. General Description
Velvet ants do not have a node on the petiole, which is characteristic of the true ants.Also, females (the ones confused with ants) are generally larger than true ants. Bothmale and female velvet ants are covered with a bright red, orange, black, or yellowpubescence. There are several species, but the more commonly encountered ones arefrom 0.75 to 2.5 cm in length.

114
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
C. Geographic Distribution
Members of this wasp family are widely distrib-uted, but most U.S. species occur in the south-ern and western areas of the country. Onenorthern species, Dasymutilla occidentalis, iscommon on the sandy beaches of Lake Erie inthe summer, causing much distress to barefootbeachgoers.5
D. Biology/Behavior
These “ants” are solitary, diurnal wasps that areoften associated with dry, sandy environments.Male mutillids are winged, females are wing-less. Their larvae are parasites of bees and otherwasps. Females run about in the open searchingfor a suitable place to lay their eggs.
E. Treatment of Stings
Being solitary wasps (not actually ants), stingsby numerous velvet “ants” are rare. Disinfectionof the sting site, application of ice packs, and/or administration of analgesics are often indi-cated for normal or local sting reactions. In theevent of an allergic reaction, epinephrine, anti-histamines, and other supportive measures maybe needed.
REFERENCES1. Alexander, J. O., Arthropods and Human Skin,
Springer-Verlag, Berlin, 1984, chap. 10.
2. Favorite, F., Imported fire ant, Pub. HealthRep., 73, 445, 1958.
3. Diaz, J. D., Lockey, R. F., Stablein, J. J., andMines, H. K., Multiple stings by imported fireants without systemic effects, S. Med. J., 82,775, 1989.
4. Ebeling, W., Urban Entomology, University ofCalifornia, Division of Agricultural Science,Los Angeles, 1978, 351.
5. Frazier, C. A., Insect Allergy: Allergic Reactionsto Bites of Insects and Other Arthropods, WarrenH. Green Inc., St. Louis, 1969, 45.
Figure 7Female velvet ant (from: U.S. DHEW, PHS, CDC,Pictorial Keys).
VELVET ANTS
ImportancePainful stings
DistributionIn U.S., most species occur in South
and West
LesionVariable
Disease TransmissionNone
Key ReferenceMickel, C. E., Bull. U.S. Nat. Mus., No.
143, 1928
TreatmentLocal — ice packs; pain relievers
systemic — may requireantihistamines, epinephrine, and/orother measures

115
Bees
CHAPTER 11
BEES
TABLE OF CONTENTS
I. Honey bees ......................................................................................................116A. General and Medical Importance ..............................................................116B. General Description ....................................................................................116C. Geographic Distribution .............................................................................116D. Biology/Behavior .........................................................................................116E. Treatment of Stings .....................................................................................117
II. Africanized or “Killer” Bees ............................................................................117A. General and Medical Importance ..............................................................117B. General Description ....................................................................................118C. Geographic Distribution .............................................................................118D. Biology/Behavior .........................................................................................118E. Treatment of Stings .....................................................................................118
III. Bumble bees ....................................................................................................118A. General and Medical Importance ..............................................................118B. General Description ....................................................................................119C. Geographic Distribution .............................................................................119D. Biology/Behavior .........................................................................................119E. Treatment of Stings .....................................................................................119
References ......................................................................................................................120

116
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
HONEY BEES
Figure 1Worker honey bee (from: “Mississippi’s Health,”Summer 1990 issue, with permission).
I. HONEY BEESA. General and Medical Importance
Honey bees, Apis mellifera, are commonly en-countered insects and account for numerousstings (and even death due to allergy) in the U.S.each year.1 The problem lies not with their ag-gressiveness, but with their ubiquity. They arevirtually everywhere outdoors during the warmmonths — in backyard clovers, window sill flow-ers, garden vegetables blooms, waste receptaclesareas, etc. Unlike most other Hymenoptera, thehoney bee worker has a barbed stinger and cansting only once. To escape, the bee must leaveits entire stinging apparatus attached to the skinof its victim. Making matters worse, during sting-ing events honey bees release alarm pheromonesassociated with the sting gland, causing otherbees in the vicinity of a pheromone-markedvictim to attack and inflict multiple stings.
B. General Description
Honey bees are the familiar yellow-orange andblack-striped bees with two membranous wingsthat are commonly seen on flowers in the springand summer (Figure 1). They have featheredhairs (when observed under magnification) andno spurs on their hind tibia. Worker honey beesare approximately 15 to 20 mm long, and dronesare slightly larger and more robust. There are“races” of honey bees in the U.S.; the goldItalians and the black or gray Caucasian racesmake up the majority of bees found in thiscountry. A close relative, the Africanized or“killer” bee, has recently been introduced intothe U.S. (see Section II).
C. Geographic Distribution
Honey bees are not native to several continents(including North America, north of Mexico), butthey have been introduced virtually worldwidefor pollination and honey production.
D. Biology/Behavior
A. mellifera is a highly social insect. The colonyconsists of an egg-laying queen, drones to fertil-
ImportancePainful stings; allergic RXNS
DistributionAlmost worldwide
LesionLocal swelling; central white spot with
erythematous halo
Disease TransmissionNone
Key ReferenceMichener, C. D., Ann. Rev. Entomol., 14,
299, 1969
TreatmentLocal RXNS — ice packs; pain relievers
systemic RXNS — may requireantihistamines, epinephrine, and/orother measures

117
Bees
AFRICANIZEDHONEY BEES
Figure 2Africanized honey bee worker (left) andEuropean honey bee worker (right) (photocourtesy John Kucharski and the USDAAgricultural Research Service).
ImportanceHighly aggressive; painful stings; allergic
RXNS
DistributionSouth and Central America, Mexico,
South Texas (but increasing in U.S.)
LesionSame as honey bee sting
Disease TransmissionNone
Key ReferenceWinston, M. L., Ann. Rev. Entomol., 37,
173, 1992
TreatmentLocal RXNS — ice packs; pain relievers
numerous stings (nonallergic RXNS)— treat for histamine overdosagesystemic RXNS — may requireantihistamine, epinephrine, and/orother measures.
ize the queen, and workers to gather food andcare for the young. Most honey bee colonies areman-made and -maintained; however, wild colo-nies exist, mostly from escaped swarms, and theyare usually found in hollow trees. Cells in ahoney bee nest are in vertical combs, two celllayers thick. The colonies are perennial, with thequeen and workers overwintering in the hive.Normally, there is only one queen per colony,and queens may live several years. When a newone is produced, it may be killed by the oldqueen, or one of the two queens may leave witha swarm of workers to build a new nest.
E. Treatment of Stings
Local treatment of honey bee stings consists ofremoving the stinger, disinfecting the sting site,and applying ice packs to slow the spread ofvenom. The stinger should be removed as quicklyas possible. Conventional advice in the scien-tific literature has emphasized that the stingshould be scraped off, never pinched. But arecent study1a has shown that the method ofremoval is irrelevant, and even slight delays inremoval caused by concerns about the correctprocedure are likely to increase the dose ofvenom received. Other than stinger removal,Alexander2 said that nonallergic local reactionsseldom require treatment. In the case of a se-vere or large local reaction, oral antihistaminesand topical applications of corticosteroid creamsmay help, as well as rest and elevation of theaffected arm or leg.
Allergic (systemic) reactions to bee stings canbe life-threatening events and may require ad-ministration of epinephrine, antihistamines, andother supportive treatment (see Chapter 2).
II. AFRICANIZED OR“KILLER” BEES
A. General and Medical Importance
The Africanized honey bee (AHB) is a strain ofhoney bee that was brought to South Americafrom Africa to improve honey production. In1956, 26 swarms of the AHB escaped fromexperimental colonies near Sao Paulo, Brazil

118
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
and have subsequently multiplied and spread throughout much of South and CentralAmerica.3 They are now in parts of the southern U.S. Winston4 presents a detailed up-to-date review of the status of the AHB.
The AHB looks almost identical to our domesticated strains of European honey bees(Figure 2), but it is more likely to attack with little provocation, stay angry for a longertime, and exhibit massive stinging behavior in colony defense. Although there are somedifferences in the venom of AHB vs. European bees, AHB stings are not more toxicthan those of domestic bees. However, death of humans and domestic or wild animalscan result from toxic effects of multiple stings (400 to 1,000 stings) or from anaphylacticshock from an allergic reaction to very few stings (see Chapter 2).
As the AHB makes its way further into the U.S., numbers of sting-related deaths willlikely increase. In Venezuela in 1978 (before AHB) there were 12 deaths attributed tohoney bee stings. In 1988 (after AHB) there were 100 bee-sting-related deaths.5 Anincrease in mortality of this magnitude may be avoided in the U.S. by better beekeepingpractices and prompt medical management of stinging events.
B. General Description
AHBs look identical to the common honey bee (Figure 2). Only a specialist can tellthem apart.
C. Geographic Distribution
Africanized bees are native to Africa. Since their accidental introduction in 1956, theyhave colonized most of South America, Central America, and Mexico. They are nowreported from the southern one half of Texas, parts of New Mexico, Arizona, andCalifornia. Their spread into other southern U.S. states is likely.
D. Biology/Behavior
Most biological aspects of AHBs are similar to that of domestic honey bees (seepreceding section); however, the mating habits of AHBs are such that Africanizedqueens tend to mate almost always with Africanized drones. They also reproduce ata high reproductive rate and swarm frequently. AHB colonies have more guard beesthan European bee colonies; up to 50% of the bees in an AHB colony may be guardbees that respond to a disturbance.
E. Treatment of Stings
Since the venoms are similar, AHB stings can be treated in the same manner as domestichoney bee stings. One note may be added — in the case of tens or hundreds of stings,extensive histamine release may result from venom action and not necessarily due froman allergic reaction. Accordingly, physicians may need to treat for histamine overdosage.
III. BUMBLE BEESA. General and Medical Importance
There are several species of bumble bees in the genera Bombus, Megabombus, andPyrobombus. Bumble bees, like other stinging Hymenoptera, will attack and sting when

119
Bees
BUMBLE BEES
Figure 3Bumble bee worker (from: North Carolina Agr.Exp. Sta. Tech. Bull. No. 152).
their nest is disturbed. A significant number ofstinging incidents occur yearly, and some indi-viduals experience allergic reactions. However,bumble bees are neither as aggressive nor asabundant as honey bees, and therefore gener-ally are not as dangerous.6
B. General Description
Bumble bees have feathered hairs on their bodyand have spurs on their hind tibia. They arerobust bees, usually 20 mm or more in length,having black and yellow pubescence on theirabdomen (Figure 3). They are often confusedwith carpenter bees, which are similar in sizeand appearance, except carpenter bees have nopubescence on the abdomen. Carpenter beesrarely sting and are often seen forming galleriesin wooden structures such as barns, sheds,stables, etc.
C. Geographic Distribution
Bumble bees occur throughout the U.S. andover much of the world.
D. Biology/Behavior
Most bumble bees are diurnal plant feeders thatnest in the ground, usually in loose fibroushabitats such as mouse nests, insulation, orgrass clippings. The colonies are annual, withonly fertilized queens overwintering. Thesequeens start new nests in the spring and thecolony builds to between 100 and 500 bees bylate summer. The opening to their nests mayappear moundlike from materials excavated bythe bees. Bumble bee nest openings that re-semble fire ant mounds have been seen.
E. Treatment of Stings
Local treatment of bumble bee stings involvesice packs and/or pain relievers and washing tolessen the chances of secondary infection. Inthe case of a severe or large local reaction, oralantihistamines and topical applications of corti-costeroid creams may help, as well as rest andelevation of the affected arm or leg.
ImportancePainful stings; allergic reactions
DistributionAlmost worldwide
LesionSimilar to other wasps and bees; central
white spot and erythematous halo
Disease TransmissionNone
Key ReferenceMitchell, T. B., North Carolina Agri.
Exp. Sta. Tech. Bull. No. 152, 1962
TreatmentLocal RXNS — ice packs; pain relievers
systemic RXNS — may requireantihistamines, epinephrine, and/orother measures

120
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
For allergic (systemic) reactions, administration of epinephrine, antihistamines, andother supportive treatment may also be required (see Chapter 2).
REFERENCES1. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,
Macmillan, New York, 1979, chap. 17.
1a. Visscher, P.K., Vetter, R.S., and Camazine, S., Removing bee stings, Lancet, 348, 301, 1996.
2. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 10.
3. Michener, C. D., The Brazilian honey bee — possible problem for the future, Clin.Toxicol., 6, 125, 1973.
4. Winston, M. L., The biology and management of Africanized honey bees, Ann. Rev.Entomol., 37, 173, 1992.
5. Gomez-Rodriguez, R., Manejo de la Abeja Africanizada, Direccion General DesarrolloGanadero, Caracas, Venezuela, 1986.
6. Biery, T. L., Venomous Arthropod Handbook, USAF pamphlet #161–43, Brooks AFB, TX,1977, 18.

121
Blister Beetles
CHAPTER 12
BLISTER BEETLES
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................121
II. General Description .........................................................................................121
III. Geographic Distribution ..................................................................................122
IV. Biology/Behavior .............................................................................................122
V. Treatment of Exposed Areas ..........................................................................123
References ......................................................................................................................123
I. GENERAL AND MEDICAL IMPORTANCE
Blister beetles are plant-feeding insects that contain a blistering agent in their bodyfluids. Most are in the family Meloidae, although some are in the Staphylinidae family.The agent in meloid beetles, cantharidin, has the formula C10H12O4 and penetrates theskin, readily producing blisters in a few hours1 (also see Chapter 5). The blistering agentin staphylinids may be somewhat different chemically from cantharidin. In any event,handling the live beetles or contact with their pulverized bodies may cause blistering.Lehman et al.2 reported tingling and burning prior to blister formation, but other reportsindicated an almost symptomless course except for the blisters.3 Dermatoses fromblister beetle contact are seasonal, with most cases in the U.S. occurring in July, August,and September. Alexander4 said that workers harvesting the potato crop, as well aschildren running around barefoot, are particularly vulnerable to attack.
II. GENERAL DESCRIPTION
Blister beetles are elongate, soft-bodied specimens that have the pronotum (sectionbetween head and wings, viewed from above) narrower than the head or wings (Figure1). Two of the common blister beetle species are both potato beetles, one with orange

122
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
and black longitudinal stripes (Figure 2A) and one black with gray wing margins(Figure 2B). Members of the genus Meloe are called “oil beetles” because they exudean oily substance from their legs when disturbed. Oil beetles are approximately 20 to25 mm long and black, with no hind wings, giving the appearance that their wings aretoo short (Figure 2C).
III. GEOGRAPHIC DISTRIBUTION
The ash-gray (Epicauta fabricii) and striped blister beetles (E. vittata) are common inthe central and southeastern areas of the U.S. Oil beetles and other large, roundedspecies are common in the southwestern U.S. from Texas to southern California. Manyother blister beetle species are common in the western U.S. In Europe, three importantblister beetles are Paederus limnophilus, P. gemellus, and Lytta vesicatoria, the “Spanishfly” of Southern Europe.
IV. BIOLOGY/BEHAVIOR
Blister beetles have a very unusual biology. Larvae of the meloid beetles feed on theeggs of grasshoppers and in the nests of solitary bees. After several larval stages, theypupate and later emerge as adult beetles. Adults are plant feeders that may emerge inlarge numbers and appear in gardens and field crops quite suddenly.
Figure 1Typical blister beetle. (Redrawn from a figure originally by Dr. Carl Mohr, Berkeley, CA.)

123
Blister Beetles
V. TREATMENT OF EXPOSEDAREAS
Blisters from exposure to the beetles are gener-ally not serious and will be reabsorbed in a fewdays if unruptured. Even if the blisters areruptured, there is normally complete clearing in7 to 10 days. Affected areas should be washedwith soap and water and bandaged until theblisters reabsorb. Antibiotic ointments or creamsmay help prevent secondary infection. Largeblisters, and those occurring on the feet wherethey will be rubbed, may need to be drained,treated with antiseptics, and bandaged.5 If thebeetles or beetle products are ingested, thecantharidin may cause nausea, diarrhea, vomit-ing, and abdominal cramps.
REFERENCES1. Harwood, R. F. and James, M. T., Entomology
in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, chap. 17.
2. Lehman, C. F., Pipkin, J. L., and Ressmann, A. C.,Blister beetle dermatitis, Arch. Dermatol., 71, 36,1955.
3. Giglioli, M. E. C., Some observations on blisterbeetles, family Meloidae, in Gambia, WestAfrica, Trans. R. Soc. Trop. Med. Hyg., 59, 657,1965.
4. Alexander, J. O., Arthropods and Human Skin,Springer-Verlag, Berlin, 1984, chap. 7.
5. Frazier, C. A. and Brown, F. K., Insects andAllergy and What To Do About Them, Universityof Oklahoma Press, Norman, OK, 1980, chap.19.
BLISTER BEETLES
Figure 2Blister beetles: the striped blister beetle (A), ash-gray blister beetle (B), and oil beetle (C) (adaptedin part from: U.S. DHEW, PHS, CDC, PictorialKeys).
ImportanceContact may produce blisters on skin
DistributionMany areas of world, including U.S.
LesionGenerally painless, large blisters
Disease TransmissionNone
Key ReferenceLehman et al., Arch. Dermatol., 71,
36–38, 1955
TreatmentGenerally not serious; topical antibiotics
and bandaging to prevent secondaryinfection


125
Bugs (The True Bugs)
CHAPTER 13
BUGS (THE TRUE BUGS)
TABLE OF CONTENTS
I. Bed Bugs ..........................................................................................................126A. General and Medical Importance ..............................................................126B. General Description ....................................................................................126C. Geographic Distribution .............................................................................128D. Biology/Behavior .........................................................................................128E. Treatment of Infestation/Bites ....................................................................128
II. Conenose Bugs (Assassin and Kissing Bugs) ................................................129A. General and Medical Importance ..............................................................129B. General Description ....................................................................................130C. Geographic Distribution .............................................................................131D. Biology/Behavior .........................................................................................131E. Treatment of Infestation/Bites ....................................................................132
III. Wheel Bugs ......................................................................................................134A. General and Medical Importance ..............................................................134B. General Description ....................................................................................134C. Geographic Distribution .............................................................................134D. Biology/Behavior .........................................................................................134E. Treatment of Bites .......................................................................................134
References ......................................................................................................................135

126
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
I. BED BUGSA. General and Medical Importance
The common bed bug, Cimex lectularius, (Fig-ure 1) has been an associate of humans forthousands of years. The blood-sucking parasitesare common in Third World countries, espe-cially in areas of extreme poverty. Bed bugs hadnearly disappeared in developing countries untilrecently, where, in the last 5 to 10 years, theyhave been making a progressively rapid come-back. The author increasingly receives reportsof the parasites inside U.S. hotel rooms. Onerecent report of an infested house in GreatBritain contained a description of literally thou-sands of the bugs under and within the bed andin the mattress seams1 (Figure 2). According tothe authors, the area where the bed was againstthe wall was black with a layer of bed bugexcrement, cast skins, and eggs several millime-ters thick.1 Bed bugs have been found naturallyinfected with >20 disease organisms such asthose causing anthrax, plague, hepatitis, andtyphus. However, bed bugs have never beenproven to biologically transmit even one humanpathogen. Their principal medical importance isthe itching and inflammation associated withtheir bites. Occasionally hemorrhagic bullae resultfrom bed bug bites.
B. General Description
Adult bed bugs are approximately 5 mm long,oval shaped, and flattened (Figures 1 and 3).They somewhat resemble unfed ticks or smallcockroaches. Adults are reddish-brown (chest-nut) in color; the immatures resemble adults butare yellowish-white. Bed bugs have a pyramid-shaped head with prominent compound eyes,slender antennae, and a long proboscis tuckedbackward underneath the head and thorax. Theprothorax (dorsal side, first thoracic segment)bears rounded, winglike lateral horns on eachside. Hind wings on bed bugs are absent entirely;the forewings are represented by two small pads.
BED BUGS
Figure 1Adult bed bug, Cimex lectularius (from: USDHEW, PHS, CDC, Pictorial Keys).
ImportanceNuisance and irritation from bites
DistributionWorldwide
LesionLinear grouping of red blotches,
urticarial wheals; sometimes bullouslesions
Disease TransmissionNone
Key ReferencesUsinger, R. L., Thomas Say Found.
(Entomol. Soc. Amer.), Vol 7, 1966
Ryckman et al., Bull. Soc. Vector Ecol.,6, 93, 1981.
TreatmentAntiseptic or antibiotic creams or
lotions; antihistamines for urticarialRXNS; eliminate infestation in home

127
Bugs (The True Bugs)
CASE HISTORY
BED BUGS IN HOTEL ROOM
A physician called asking questions about a strange insect infestation she had encounteredin a hotel (one of the major chain hotels) in Denver, Colorado during a medical conference.She said that about 11:00 P.M. while reading in bed a small “cockroach-like bug” crawledon her arm. Blood came out when she smashed it. Later, after going to sleep, she wasawakened by another one on her arm — it also was full of blood. She captured a few andbrought them back for identification. I told her by phone that the bugs were likely bed bugs,but asked to see the specimens. Upon receiving the specimens 2 days later, they wereconfirmed as Cimex lectularius.
Comment. Even though bed bugs are not as common as they used to be, they still may beencountered from time to time, even in affluent settings. A traveler may bring in some ofthe bugs in his or her suitcases or belongings, and soon the bugs take up residence in cracksand crevices, behind baseboards, or under mattresses. Any cockroach-like insects comingout from the mattress or environs to bite are highly suspect (cockroaches have chewingmouthparts and NEVER suck human blood). Get another room — better yet, get anotherhotel!
Figure 2Numerous bed bugs congregating on the underside of a mattress (photo courtesy Mr. IanDick and The London Borough of Islington, Environmental Health Department).

128
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
C. Geographic Distribution
The common bed bug is cosmopolitan, occurring in temperate regions worldwide.Another bed bug species, C. hemipterous, is also widespread but is mostly found in thetropics. Several other bed bug species occur on bats, but they do not bite people.
D. Biology/Behavior
Bed bugs possess stink glands and emit an odor. Homes heavily infested with the bugshave this distinct odor. Bed bugs feed at night, hiding in crevices during the day. Hidingplaces include seams in mattresses, crevices in box springs, and spaces under baseboardsor loose wall paper.
There are five nymphal stages that must be passed before development to adults.Once an adult, the life span is 6 to 12 months. Each nymphal stage must take a bloodmeal in order to complete development and molt to the next stage (Color Figure 13-12).The bugs take about 5 to 10 min to obtain a full blood meal. Bed bugs can survivelong periods of time without feeding, and when their preferred human hosts are absentthey may take a blood meal from any warm-blooded animal.
E. Treatment of Infestation/Bites
Bed bugs have piercing–sucking mouthparts typical of the insect order Hemiptera.Accordingly, bites from the bugs often produce welts and local inflammation, probablydue to allergic reactions to saliva injected via the mouthparts during feeding (seeChapter 2). On the other hand, for many people the bite is nearly undectectable. Bedbug bites are generally self-limiting and require little specific treatment other thanantiseptic or antibiotic creams or lotions to prevent infection. Antihistamines may be
Figure 3Bed bug feeding beside the author’s wedding ring, showing relative size.

129
Bugs (The True Bugs)
needed for urticarial reactions. In addition, efforts should be made to eliminate thesource of the bites. Insecticide treatments for bed bugs are effective but should beconducted carefully, since people have prolonged, close contact with the treated areas— beds, couches, etc. where bed bugs live.
II. CONENOSE BUGS (ASSASSIN AND KISSING BUGS)A. General and Medical Importance
Many members of the family Reduviidae have an elongate (cone-shaped) head, andhence the name “conenose bugs.” Most reduviids “assassinate” or kill other insects.Some of the assassin bugs occasionally bite people, producing very painful lesions(Color Figure 13-13). A common offender is Melanolestes picipes. There is a report oftwo of these bugs biting an 8-year-old, causing intense pain for hours, swelling at thebite site for days, and later, ulcers.1a A relatively small but important group of reduviidsin the subfamily Triatominae feeds exclusively on vertebrate blood. Notorious membersof this group are frequently in the genus Triatoma, but not all (see Figure 4 for aclassification scheme of this group). Triatomines are called “kissing bugs” because theirblood meals are occasionally taken from the area around the human lips. Other sites
Figure 4Partial classification scheme for insect family Reduviidae.

130
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
of human attack, in order of frequency, are the hands, arms, feet, head, and trunk.Kissing bugs are not able to feed through clothing. Very often, their bites are painless.However, subsequent reactions to their bites range from a single papule to gianturticarial lesions — sometimes with dizziness and nausea — depending on the degreeof allergic sensitivity.
Kissing bugs may transmit the agent of Chagas’ disease, or American trypanosomia-sis, one of the most important arthropod-borne diseases in tropical America. Chagas’disease is a zoonosis (originally a parasite of wild animals) mostly occuring in Mexicoand Central and South America (Figure 5), but a few indigenous cases have beenreported in Texas, Tennessee, and California.2,3,3a Serological evidence has identified T.cruzi as far north as Oklahoma.3b At present, some 16 to 18 million people areestimated to be infected, with 90 to 100 million people at risk.4 Chagas’ disease has bothacute and chronic forms, but is perhaps best well known for its chronic sequelaeincluding myocardial damage with cardiac dilation, arrhythmias and major conductionabnormalities, and digestive tract involvement such as megaesophagus and megacolon.
B. General Description
Assassin bugs are often black or brown in color. They have elongate heads with theportion behind the eyes narrowed and “necklike” (Figure 6A). The beak is short andthree-segmented, and its tip fits into a groove in the ventor of the thorax. In non-triatomines the beak is thick and curved. The abdomen is often widened in the middle,exposing the lateral margins of the segments beyond the wings. Kissing bugs are similarin appearance to many assassin bugs, except they have orange and black markingswhere the abdomen extends laterally past the folded wings (Figure 6B and 7), and athin, straight proboscis. In addition, the dorsal portion of the first segment of the thoraxconsists of a conspicuous triangular-shaped pronotum. Most adult kissing bugs are 1to 3 cm long and are good fliers.
Figure 5Approximate geographic distribution of Chagas’ disease.

131
Bugs (The True Bugs)
KISSING BUGS
Figure 6Adult assassin bug (A) and kissing bug (B)(from: U.S. DHEW, PHS, CDC Pictorial Keys).
ImportanceBlood feeding on humans — often at
night anaphylaxis has been reportedfrom bites
DistributionMost medically important species occur
in the Americas
LesionVariable — papular, nodular, or bullous
Disease TransmissionChagas’ disease
Key ReferenceLent, H. and Wygodzinsky, P., Bull. Am.
Mus. Nat. Hist. 163 (Art. 3), 123, 1979
TreatmentLocal RXNS — antihistamines, Caladryl®
systemic RXNS: antihistamines,epinephrine, and other supportivemeasures as needed
C. Geographic Distribution
Numerous species of assassin bugs occur es-sentially worldwide. The wheel bug belongs tothis group (see Section III). Reduvius senilis,the tan assassin bug, is found in the desertareas of the southwestern U.S. and Mexico. R.personatus occurs throughout the U.S. andsouthern Europe. Melanolestes picipes is widelydistributed in the United States.
There are several species of kissing bugs thatwill attack humans, and many reduviid bugs arecapable of transmitting Trypanosoma cruzi, thecausative agent of Chagas’ disease. However,only a few species are efficient vectors. The fourprincipal vectors of Chagas’ disease in Centraland South America are Panstrongylus megistus,Rhodnius prolixus, Triatoma infestans, and T.dimidiata. The most important vector in Mexicois T. barberi. In the southwestern U.S., T.gerstaeckeri (Figure 8A) and T. protracta (Fig-ure 8B) are important kissing bug species, andT. sanguisuga (Figure 8C) occurs throughoutmuch of the U.S. Figure 9 shows the U.S. distri-bution of five common kissing bugs.
D. Biology/Behavior
Assassin bugs are predaceous on other insectsand are often found lying in wait for their preyon various plants or flowers. They, along withthe kissing bugs, undergo simple metamorpho-sis; the developing nymphs look very much likeadults, except smaller.
Kissing bugs are nocturnal insects that areable to fly to their hosts with speed and agility.Both sexes bite and they take their blood mealsat night, hiding in any available crack or crevicebetween feedings (about 36 h). Triatoma, as agroup, normally feed on a wide variety of smallmammals, but will readily feed on humans.Infection rates with Trypanosoma cruzi, thecausative agent of Chagas’ disease, may be ashigh as 80 to 100% in some adult triatomine bugpopulations.5,6 Human kissing bug bites are es-pecially common occurrences in poor, under-developed areas with dilapidated or poorlyconstructed huts or shacks. Infection is not bythe salivary secretions associated with the bite

132
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 7Kissing bug showing abdomen extending laterally past foldedwings.
but by fecal contamination of the bite site; however, other routes of transmission maybe overlooked. In some communities in Mexico, for example, people believe that bugfeces can cure warts or that the bugs have aphrodisiac powers.5 In addition, Mexicanchildren often play with triatomine bugs collected in their houses, and in Jaliscoreduviid bugs are eaten with hot sauce by the Huichol Indians.5
E. Treatment of Infestation/Bites
Treatment for conenose bug bites involves washing the wound with soap and water.Itching lesions may be relieved with topical palliatives such as Caladryl® and/or oralantihistamines. Mild systemic reactions may require oral or i.m. antihistamines. Anaphy-lactic shock is rare, but has been reported. In that case, shock should be treated withepinephrine, antihistamines, and other supportive measures (see Chapter 2). Follow-up for possible development of Chagas’ disease may be needed for patients withkissing bug bites in endemic areas.
Figure 8Adult Triatoma gerstaeckeri (A), T. protracta (B), and T. sanguisuga (C) (from: U.S. DHEW, PHS,CDC Pictorial Keys).

133
Bugs (The True Bugs)
Figure 9Approximate U.S. distributions for five commonly encountered kissing bugs.

134
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
WHEEL BUGS
Figure 10Adult wheel bug (from: U.S. DHEW, PHS, CDC,Pictorial Keys).
ImportancePainful bite
DistributionU.S.
LesionSwollen, inflammed, and indurated at
bite site
Disease TransmissionNone
Key ReferenceHall, M. C., Arch. Intern. Med., 33, 513,
1924
TreatmentNone may be needed, oral analgesics,
Caladryl®, topical corticosteroids mayhelp
III. WHEEL BUGSA. General and Medical Importance
The wheel bug, Arilus cristatus, is also in thefamily of true bugs called Reduviidae. Theybite humans only in self-defense. However,the bite is characterized by immediate, intensepain.7,8 Inflammation may become chronic, pro-ducing lesions at the bite site resembling pap-illomas.
B. General Description
Wheel bugs are gray and approximately 3 cmlong (Figure 10). The insects, as their nameimplies, have a cogwheel-like crest on the dor-sal side of their prothorax (Figure 11). Thisgives the appearance of a half wheel on theirupper body. They also have a small, narrowhead and long, piercing–sucking mouthpartstucked under their head and prothorax.
C. Geographic Distribution
The wheel bug is common from New Mexicothrough the southern and eastern U.S.
D. Biology/Behavior
These insects attack and eat soft-bodied insects.They inject a salivary fluid into their prey viatheir long beak. Being true bugs (Hemiptera),wheel bugs develop by simple metamorphosis,meaning that immatures are called nymphs andare almost identical to the adults.
E. Treatment of Bites
Bites of the wheel bug, although painful, areusually localized and self-limiting. Specific treat-ment measures are probably not necessary.

135
Bugs (The True Bugs)
REFERENCES1. King, F., Dick, I., and Evans, P., Bed bugs in Britain, Parasitol. Today, 5, 100, 1989.
1a. Eads, R. B., An additional report of a reduviid bug attacking man, J. Parasitol., 36, 87. 1950.
2. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, chap. 7.
3. Schiffler, R. J., Mansur, P., Navin, T. R., and Limpakarnjanarat, K., Indigenous Chagasdisease in California, J. Am. Med. Assoc., 251, 2983, 1984.
3a. Herwaldt, B. L., Grijalva, M. J., Newsome, A. L., McHee, C. R., Powell, M. R., Nemec, D.G., Steurer, F. J., and Eberhard, M. L., Use of PCR to diagnose the fifth reportd U.S. caseof autothonous transmission of Trypanosoma cruzi in Tennesse, 1998, J. Infect. Dis., 181,395, 2000.
3b. Bradley, K. K., Bergman, D. K., Woods, J. P., Crutcher, J. M., and Kirchoff, L. V.,Prevalence of American trypanosomiasis among dogs in Oklahoma, J. Amer. Vet. Med.Assoc., 217, 1853, 2000.
4. Schofield, C.J. and Dolling, W.R., Bedbugs and kissing bugs, in Medical Insects andArachnids, Lane, R.P. and Crosskey, R.W., Eds., Chapman and Hall, London, 1993, chap.14.
5. Schettino, P. M. S., Arteaga, I. H., and Berrueta, T. U., Chagas disease in Mexico, Parasitol.Today, 4, 348, 1988.
6. DeShazo, T., A survey of Trypanosoma cruzi infection in Triatoma spp. collected inTexas, J. Bacteriol., 46, 219, 1943.
7. Biery, T. L., Venomous Arthropod Handbook, USAF pamphlet #161–43, Brooks AFB, TX,1977, 13.
8. Hall, M. C., Lesions due to the bite of the wheel bug Arilus cristatus, Arch. Intern. Med.,33, 513, 1924.
Figure 11Wheel bug, showing cogwheel-like crest on upper side.


137
Caterpillars (Urticating )
CHAPTER 14
CATERPILLARS(URTICATING)
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................137
II. General Description .........................................................................................138
III. Geographic Distribution ..................................................................................138
IV. Biology/Behavior .............................................................................................141
V. Treatment of Stings ..........................................................................................142
References ......................................................................................................................143
I. GENERAL AND MEDICAL IMPORTANCE
Several moth and butterfly families have species whose caterpillars possess urticatinghairs or spines that secrete a poison when exposed to human skin1,2 (see also Chapter5). Urtication by larval lepidopterans is often termed eurcism. Most of the time exposureto urticating caterpillars is accidental or incidental, but in some cases there is delibratecontact (e.g., children playing with caterpillars). In many species there is a severeburning sensation immediately following the sting. This may be followed by swelling,numbness, urticaria, and intense stabbing pain that radiates to a nearby axillary oringuinal region; lymphadenitis may also be present. Usually the effects of these toxichairs are limited to burning and inflammation of the skin, but they may progress tosystemic reactions such as headache, nausea, vomiting, paralysis, and shock andconvulsions (rare).2 Days later, the lesion may show a pattern similar to that of thespines of the offending specimen (Figures 1 and 2). Other caterpillars, such as gypsymoth larvae, are not “stinging caterpillars,” but their hairs may cause dermatitis,

138
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
ImportancePoison hairs or spines cause stings or
irritation
DistributionMany species involved worldwide
LesionVariable — papular eruption, erythema,
local swelling
Disease TransmissionNone
Key ReferencesHenwood, B. P. and MacDonald, D. M.,
Clin. Exp. Dermatol., 8, 77, 1983
Rosen, T., Dermatologic Clinics, 8, 245,1990.
TreatmentLocal RXNS — topical products such as
Caladryl®, corticosteroids, and painrelievers; systemic RXNS — mayrequire antihistamines, epinephrine,and other supportive measures
Note: Eye lesions may be particularlyserious and should be seen by aspecialist
URTICATING CATERPILLARS
Saddleback Caterpillar, Sibine stimulea
especially in sensitive persons. Alexander3 pre-sented an excellent review of the urticatingcaterpillars with detailed discussion of the na-ture of their venoms and hair/spine structure.
II. GENERAL DESCRIPTION
Five common urticating caterpillars will bediscussed in this section — many others occur(Table 1). Automeris io caterpillars are larvaeof the IO moth. Full-grown caterpillars areabout 5 to 8 cm long, pale green, with lateralstripes of red or maroon over white runningthe length of the body (Figure 3A). The brown-tail moth larva, Euproctis chrysorrhoea, is amostly black caterpillar with brown hairs anda row of white tufts on each of its sides. Thepuss caterpillar, Megalopyge opercularis, alsosometimes called the opossum bug, asp, Italianasp, or el perrito, is about 3 cm long, tan todark brown in color, and completely covereddorsolaterally with hair that causes it to re-semble small tufts of cotton (Figure 3B). Theyreally do not look like caterpillars. Intermingledamong all those fine hairs on the back areclusters of venomous spines. Sibine stimulea,the saddleback caterpillar, is 2 to 3 cm long,has a brown sluglike body, and is coveredmid-dorsally with markings that resemble abrown or purplish saddle sitting on a greenand white saddle blanket (Figure 3C). Gypsymoth larvae, Lymantria dispar, are approxi-mately 3 to 5 cm long and gray to brown incolor with yellow stripes (Figure 3D). Theyalso may appear to have red or blue spotsalong the sides and top of the body. As in theother members of the family Lymantriidae,gypsy moth larvae have long tufts of hair alongthe body.
III. GEOGRAPHICDISTRIBUTION
The IO moth is found in the Nearctic region; itis quite common throughout the eastern U.S.Brown-tail moth caterpillars are bothersome pests

139
Caterpillars (Urticating )
Figure 1Skin lesion from exposure to stinging caterpillar, 2 days post-sting.
Figure 2Caterpillar responsible for sting lesion depicted in Figure 1.
in Europe and eastern portions of the U.S. where they have been accidentallyintroduced. The saddleback caterpillar is found in many parts of the world. In the U.S.it is generally distributed southeast of a diagonal line drawn from Massachusetts to themiddle of Texas. Puss caterpillars are primarily found in the southern U.S. andsouthward into Central and South America. They seem to be especially a problem inTexas. Gypsy moths occur in Europe and the eastern U.S.

140
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
CASE HISTORY
On 30 September 1994 the author was collecting insects at the Copiah County GameManagement Area in central Mississippi when his son inadvertently brushed his rightforearm against a puss caterpillar. Several of the caterpillars had been seen on a fallen logand some bushes just prior to the sting incident. The offending specimen was collected,identifed, and photographed at the site (Figure 1). Within 5 min the patient experienced
intense, throbbing pain at the sting site. Anerythematous spot approximately 4 cm in diam-eter developed (Figure 2), containing a few raisedpapule-like structures, presumably where the poi-sonous hairs or setae contacted the skin. After 20min the patient was complaining of severe pain inthe right axilla. The patient was photographedduring the time of this axillary pain (Figure 3 —actual arm positions, photo not contrived). Noother symptoms developed and the pain subsidedwithin 45 min. The erythematous spot resolved in24 h.
Comment: Many moth families have species whoselarvae possess stinging or urticating spines or hairs.One of the most troublesome of these is the pusscaterpillar, Megalopyge opercularis, a member of
the flannel moth family. The puss caterpillar is widely distributed in the southern U.S.extending down into Mexico; members of the species feed on a variety of deciduous treesand shrubs. Interestingly, its appearance is not what one might expect for a caterpillar.Instead of being worm-like, or worm-like with prominent spines, the puss caterpillar isshaped like a teardrop and looks like a tuft of cotton or fur. It may vary in color from lightyellow to gray or reddish-brown. Stings from the puss caterpillar may cause immediate
Figure 1Puss caterpillar (reprinted from: Amer.Fam. Phys. 52, 86, July, 1995, copyright1995 by the American Academy of FamilyPhysicians, with permission).
Figure 2Puss caterpillar sting site — 15 minutes after sting (reprinted from: Amer. Fam. Phys. 52,86, July, 1995, copyright 1995 by the American Academy of Family Physicians, withpermission).

141
Caterpillars (Urticating )
intense local burning pain (often referred to as “shooting” pain), headache, nausea,vomiting, lymphadenopathy, lymphadenitis, and sometimes shock and respiratory distress.Stings can be especially severe in children.
From reports in entomological and medical literature, this case was fairly typical, exceptperhaps for the lack of local swelling. Certainly, a person with hypersensitivity to the venomcould react in a much more profound manner, possibly leading to shock and respiratorydistress. But even in the absence of an allergic reaction, puss caterpillar stings can lead totemporary severe pain and partial immobilization.
(Adapted from Amer. Fam. Phys. 52, 86, Copyright 1995, the American Academy of FamilyPhysicians. With permission.)
Figure 3Axillary pain caused by puss caterpillar sting — actual arm positions, photo not contrived.
IV. BIOLOGY/BEHAVIOR
IO moth larvae feed on the leaves of a variety of plants, including corn and willow.In most areas they produce only one annual generation, but in the southernmost areasof their distribution there may be a second generation. Therefore, depending on thearea of the country, larval stages can be found anytime from spring to fall. The brown-tail moth is a serious pest of forest and shade trees, as well as many varieties of fruittrees. Caterpillars of this species are most active between April and July.
The saddleback caterpillar may be found feeding on the leaves of a variety of trees,shrubs, and other plants from May to November. The puss caterpillar also feeds on theleaves of a wide range of trees and shrubs. In the southern area of its range, it mayhave two generations per year. The first generation develops in the spring and earlysummer, while the second generation develops in the fall. They seem to be especiallyabundant from September to November. Every few years there are “outbreaks” of pusscaterpillars that lead to numerous stings, especially among children. They are com-

142
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
monly found on the exterior walls of houses, sheds, gates, and fences; thus, risk ofhuman contact is high.
The gypsy moth was introduced into the eastern U.S. in the 1860s and has sincebecome widely distributed throughout New England (and is now spreading south-ward), where it causes widespread damage to forest trees. Eggs are laid on tree trunksin July and August in masses covered with froth and body hairs from the female. Eggsoverwinter and the tiny first-stage larvae emerge the following spring, usually in lateApril or early May. The females can fly but weakly. Dispersal of the gypsy mothinfestation is primarily by young larvae on silken threads traveling tree to tree or limbto limb by “ballooning” in the wind.
V. TREATMENT OF STINGS
Without additional or ongoing contact with the offending caterpillar, lesions resolve atvarying times depending upon the species involved. Generally, saddleback and IOcaterpillar dermatitis subsides within 2 to 8 h; gypsy moth dermatitis within 48 h; andbrown-tail moth and puss caterpillar disease (various systemic manifestations) within7 to 10 days.4
Local treatment of urticating caterpillar stings consists of careful repeated strippingof the sting site with adhesive or cellophane tape to remove the spines (if the offendingspecies was stout-spined), application of ice packs, and oral administration of antihis-tamines to help relieve itching and burning sensation. Acute urticarial lesions may befurther relieved by application of topical corticosteroids, which help reduce the
Table 1Some Species of Lepidoptera Whose Larvae are Known to Sting orCause Dermatitis
Species Condition Where Occurs
Megalopyge opercularis Sting Southern U.S., Central and South America
Several other Megalopyge spp. Sting South AmericaSibine stimulea Sting Neotropical, NearcticAutomeris io Sting NearcticSeveral other Automeris spp. Sting South AmericaHemileuca spp. Sting Nearctic, South AmericaEuproctis chrysorrhoea Sting Nearctic, PalearcticE. similis Sting Nearctic, PalearcticE. edwardsii Sting AustraliaE. flava Sting OrientalThaumetopoea wilkinsonii Sting Palearctic, AfrotropicalT. pityocampa Sting Palearctic, AfrotropicalOrchrogaster contraria Sting AustraliaSeveral Hylesia spp. Sting & dermatitis ArgentinaLymantria dispar Dermatitis Europe, Eastern U.S.Orgyia pseudotsugata Dermatitis Northwestern U.S.O. leucostigma Dermatitis Nearctic

143
Caterpillars (Urticating )
Figure 3Some caterpillars that sting (A–C) or cause dermatitis (D): IO moth larva (A), pusscaterpillar (B), saddleback caterpillar (C), and gypsy moth larva (D) (adaptedfrom: U.S. DHEW, PHS, CDC, Pictorial Keys).
intensity of the inflammatory reaction. Allen et al.5 reported good results withdesoximetasone gel applied twice daily to the affected areas. Rosen4 said systemicadministration of corticosteroids in the form of intramuscular triamcinolone acetonidehas been remarkably effective in relieving both severe itching due to gypsy mothdermatitis and pain due to puss caterpillar dermatitis.
For severe pain associated with the puss caterpillar or IO moth larvae, physicianssometimes administer meperidine HCl, morphine, or codeine3; aspirin is reportedly noteffective. Systemic hypersensitivity reactions such as hypotension or bronchospasm areusually treated with epinephrine, antihistamines, and other supportive measures (alsosee Chapter 2). Eye lesions (especially those resulting from forceful contact withcaterpillars) may be very serious and should be seen by a specialist.3
REFERENCES1. Maschwitz, U. W. and Kloft, W., Morphology and function of the venom apparatus of
insects — bees, wasps, ants, and caterpillars, in Venomous Animals and their Venoms,Vol. 3, Bücherl, W. and Buckley, E., Eds., Academic Press, New York, 1971, 38.
2. Keegan, H. L., Some medical problems from direct injury by arthropods, Int. Pathol., 10,35, 1969.
3. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 12.
4. Rosen, T., Caterpillar dermatitis, Dermatol. Clin., 8, 245, 1990.
5. Allen, V. T., Miller, O. F. III, and Tyler, W. B., Gypsy moth caterpillar dermatitis —revisited, J. Am. Acad. Dermatol., 24, 979, 1991.


145
Centipedes
CHAPTER 15
CENTIPEDES
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................145
II. General Description .........................................................................................146
III. Geographic Distribution ..................................................................................146
IV. Biology/Behavior .............................................................................................146
V. Treatment of Bites ...........................................................................................148
References ......................................................................................................................148
I. GENERAL AND MEDICAL IMPORTANCE
Centipedes are long, multisegmented arthropods that characteristically have one pairof legs per body segment (millipedes have two pairs per segment). They are agile, fast-moving creatures that can inflict a painful bite.1 In fact, some of the larger species canproduce extreme pain. The venom is a cytolysin-based compound. Most humancentipede bites result when a centipede is stepped on, picked up, or otherwise contactsthe body. Centipede bites are rarely fatal to humans, but deaths have been reported.Members of the genus Scolopendra, which occur in North America, can be 20 to 25cm long and produce bites with intense burning pain lasting 1 to 5 h. The bite ischaracterized by two puncture wounds at the site of attack, often red and swollen.Other symptoms may include anxiety, vomiting, irregular pulse, dizziness, and head-ache.2 Secondary infections can occur, and superficial necrosis at the bite site maypersist for several days. In addition to their bites, large species (such as in the genusScolopendra) have claws that can make tiny punctures if they crawl on human skin.

146
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
CENTIPEDES
ImportancePainful bites
DistributionNumerous species worldwide
LesionOften two hemorrhagic punctures
Disease TransmissionNone
Key ReferenceKeegan, H. L., Inter. Pathol., 10, 35,
1969
TreatmentAnalgesics; antibiotics; possibly tetanus
prophylaxis
Figure 1Centipedes: Scutigera coleoptrata (A) andScolopendra heros (B) (from: U.S. DHEW, PHS,CDC, Pictorial Keyes).
II. GENERAL DESCRIPTION
Centipedes are dorsoventrally flattened, have adistinct head, relatively long antennae, alongwith the one pair of legs per body segment(Figure 1). The first body segment bears a pairof claws that contain ducts for the expulsion ofa paralyzing venom contained in a gland at thebase of the claw. The number of body seg-ments, and thus number of legs, is variabledepending on the species, but it usually rangesfrom 15 to over 100 pairs. Many species are 3to 8 cm long, whereas some tropical speciesmay reach 45 cm. The common house centi-pede, Scutigera coleoptrata, is approximately 4cm long and has long antennae and fragile legs.From above, the relative lengths of the legs giveit an oval appearance.
III. GEOGRAPHICDISTRIBUTION
Centipede species in the northern U.S. are smalland generally harmless to man, but larger spe-cies in the southern U.S. and tropics can inflicta painful bite. The common house centipede, S.coleoptrata, occurs throughout southern Europeand the eastern parts of the U.S. and Canada.Scolopendra polymorpha occurs in the south-western U.S., and S. heros occurs in southernCalifornia. S. cingulata is a common speciesaround the Mediterranean and in the Near East.In Asia, S. morsitans is very large and can inflictsevere bites.
IV. BIOLOGY/BEHAVIOR
Centipedes lay their eggs in moist soil or veg-etation. Development is slow, with about 10instars. Adult centipedes may live 3 to 5 years.They usually hide during the day under rocks,boards, and bark, or in cracks, crevices, closets,etc. At night, they emerge to hunt for prey suchas insects and other small arthropods. The largerspecies may feed on small vertebrates. Thiscarnivorous habit brings centipedes into close

147
Centipedes
CASE HISTORYPAINFUL CENTIPEDE BITE
On July 10, a man in Jackson, Mississippi was awakened during the night by a sharp,needle-like bite on his knee. Looking around in bed, he found the offending specimen —a centipede, which he collected for identification (Figure 1). A red and swollen lesion ofa few centimeters in diameter appeared on his knee, followed by headache and dizzinesswhich lasted approximately 20 min. The patient self-medicated with Chlortrimeton (4 mg)and all symptoms were completely resolved by morning. No further complications oc-curred.
Comment: Centipede bites are usually not life threatening. The arthropods do not actuallybite with their mouthparts, but instead with sharpened claws on their modified first pair oflegs with which they hold their prey. They have a poison gland situated in the basalsegment of the modified legs and inject venom through the claws. Clinical features ofcentipede bites vary with locality and species, but generally are immediately painful, withsome swelling and local tenderness for a few hours. More severe reactions rarely occur, andmay include anxiety, vomiting, irregular pulse, dizziness, and headache. This particularcentipede was identified as Hemiscolopendra punctiventris, a member of the orderScolopendromorpha. This group is principally tropical; in the U.S. they occur mainly in thesouthern states.
Figure 1Centipede that bit patient.

148
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
contact with people as they frequently enter tents and buildings in search of prey. Theyinject venom through a pair of powerful claws on the first body segment. The clawsare connected to poison glands located in the body trunk.
V. TREATMENT OF BITES
Most centipede bites are uncomplicated and self-limiting.3 Pain from bites usuallysubsides in 8 to 36 h. Treatment recommendations include washing the bite site withsoap and water, applying ice or cool wet dressings, and taking analgesics for pain.Alexander4 said that established inflammatory lesions require appropriate antibiotics.
REFERENCES1. Remington, C. L., The bite and habits of a giant centipede (Scolopendra subspinipes) in
the Philippine Islands, Am. J. Trop. Med., 30, 453, 1950.
2. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, 459.
3. Keegan, H. L., Some medical problems from direct injury by arthropods, Int. Pathol., 10,35, 1969.
4. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 24.

149
Cockroaches
CHAPTER 16
COCKROACHES
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................149
II. General Description .........................................................................................150
III. Geographic Distribution ..................................................................................150
IV. Biology/Behavior .............................................................................................151
V. Treatment of Infestation ..................................................................................151
References ......................................................................................................................152
I. GENERAL AND MEDICAL IMPORTANCE
Cockroaches are among the most important residential, commercial, institutional, andindustrial pests today. Several of the approximately 3,500 species in the world havebecome adapted to living in human habitations (Table 1). These are sometimes referredto as “domestic” or “domiciliary” species and will breed in homes, institutions, orindustry, sharing with people their food, water, shelter, and warmth (Figure 1). Beingindoors, they can remain active throughout the year. They consume any human oranimal food or beverage, as well as dead animal and plant materials, leather, glue, hair,wallpaper, fabrics, and the starch in bookbindings.
Cockroaches adversely affect human health in several ways: they sometimes bitefeebly, especially gnawing the fingernails of sleeping children; they may enter humanear canals, they contaminate food, imparting an unpleasant odor and taste; and theymay transmit disease organisms mechanically on their body parts (Color Figure 16-14).In addition, cockroach excrement and cast skins contain a number of allergens to whichsensitive people may exhibit allergic responses (Color Figure 16-15) (also see Chapter2). Asthma-related health problems are most severe among children in inner-city areas.

150
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Table 1Some Cockroach Species Found in Close Association with Humans
Species Common Name Where Occurs
Blattella germanica German cockroach CosmopolitanB. asahinae Asian cockroach Far East, FloridaBlatta orientalis Oriental cockroach CosmopolitanPeriplaneta americana American cockroach CosmopolitanP. fuliginosa Smoky brown cockroach Central and Southern U.S.P. brunnea Brown cockroach Tropics, parts of U.S.P. australasiae Australian cockroach Tropics, neotropicsSupella longipalpa Brown banded cockroach Tropics, subtropics, parts of temperate
zone
It has been hypothesized that cockroach-infested housing is at least partly to blame.In one study of 476 asthmatic inner-city children, 50.2% of the childrens’ bedrooms hadhigh levels of cockroach allergen in dust.1 That study also found that children who wereboth allergic to cockroach allergen and exposed to high levels of this allergen had 0.37hospitalizations a year, as compared with 0.11 for other children.1
Opinions differ regarding the role of cockroaches in disease transmission. Somehealth officials see no association between cockroaches and disease and think thatcockroaches are merely nuisance pests. However, many human disease-causing organ-isms have been found on the legs, other body parts, or fecal pellets of cockroaches.2
Several researchers have obtained data indicating that the insects may be mostcommonly implicated in the transmission of Salmonella.3
II. GENERAL DESCRIPTION
Cockroaches are dorsoventrally flattened, fast-running, nocturnal insects that seekwarm, moist, secluded areas. They have prominent, multisegmented filiform antennae,cerci on the abdomen, and two pairs of wings. Many species can fly, but the domesticU.S. species rarely do so; however, the newly imported Asian cockroach in the Floridaarea both flies frequently and comes to lights.4 Adult German and brown bandedcockroaches are approximately 15 mm long, whereas the American and Orientalcockroaches are 30 to 50 mm long (Figure 2). Some tropical species are even longer.Immature cockroaches look similar to adults (except they have no wings) and someof the first nymphal instars are so small as to be confused with ants.
III. GEOGRAPHIC DISTRIBUTION
The German, Oriental, and American cockroaches are cosmopolitan in distribution. TheGerman cockroach is probably the most important overall pest in human habitationsworldwide. The American cockroach is an especially severe pest in the tropics andsubtropics. Brown banded cockroaches are a pest in the tropics and subtropics, andthey are increasing as a pest in the temperate zone. They probably now infest the entireU.S.

151
Cockroaches
IV. BIOLOGY/BEHAVIOR
Cockroaches belong to the insect order Blattaria(formerly they were in the Orthoptera) and areclosely related to crickets and grasshoppers.They develop by gradual metamorphosis inwhich the nymphs, when hatched, look similarto the adults, albeit smaller. Some cockroachspecies live outside and feed on vegetation andother organic matter. However, species that livein buildings are mostly scavengers, feeding ona wide variety of foods including starches, sweets,grease, meat products, glue, hair, and book-bindings. Cockroaches usually choose to live inprotected areas that provide a warm and humidenvironment. American and Oriental cockroachesgather in large groups in protected areas suchas wall voids or around steam pipes. The Ger-man cockroach spends most of its time hidingin cracks and crevices in dark, warm, and hu-mid areas close to food and water. Brownbanded cockroaches are generally found onceilings, high on walls, behind picture frames,or in electric appliances (if someone says cock-roaches are living inside their telephone orradio, the brown banded species is probablythe culprit). These roaches do not require asclose an association with moisture as Germancockroaches do.
V. TREATMENT OF INFESTATION
Disease transmission or allergic reactions due tocockroaches are best prevented by controllingcockroaches in the residential, institutional, andindustrial environment. The best approach tocockroach control involves good sanitation,protecting against new entry, and a combina-tion of least toxic pesticidal applications (baits,dusts, sticky traps, and residuals). In recentyears, several cockroach bait products havebeen marketed which are extremely effective inreducing roach populations. In some cases withproper use of baits, traditional pesticide spray-ing is no longer needed for cockroach control.
COCKROACHES
Figure 1Adult American cockroach; large commonlyencountered specimens.
ImportanceContamination of food; cockroach
allergy
DistributionNumerous species worldwide
Disease TransmissionMechanical transmission of various
bacteria and possibly viruses
Key ReferencesRoth, L. M. and Willis, E. R.,
Smithsonian Misc. Coll. Vol. 134 No.10, 1957
Benson, G. P. and Zungoli, P.A.,Cockroach chapter in MallisHandbook of Pest Control, Hedges,S. A., Ed., GIE Media, Cleveland, OH
TreatmentAvoidance and control; possibly
immunotherapy for allergy

152
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
REFERENCES1. Rosenstreich, D.L., Eggleston, P., Kattan, M., Baker, D., Slavin, R.G., Gergen, P., Mitchell,
H., McNiff-Mortimer, K., Lynn, H., Ownby, D., and Malveaux, F., The role of cockroachallergy and exposure to cockroach allergen in causing morbidity among inner-citychildren with asthma, New Engl. J. Med., 336, 1356, 1997.
2. Roth, L. M. and Willis, E. R., The medical and veterinary importance of cockroaches,Smithsonian Miscellaneous Collection, Vol. 134 (#10), 1957.
3. Rueger, M. E. and Olson, T. A., Cockroaches as vectors of food poisoning and foodinfection organisms, J. Med. Entomol., 6, 185, 1969.
4. Brenner, R. J., Koehler, P. G., and Patterson, R. S., The Asian cockroach, Pest Manag., 5,17, 1986.
Figure 2Five common adult cockroaches (L–R): American, smoky brown, Oriental, German, Brown-banded.

153
Earwigs
CHAPTER 17
EARWIGS
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................153
II. General Description .........................................................................................153
III. Geographic Distribution ..................................................................................154
IV. Biology/Behavior .............................................................................................154
References ......................................................................................................................154
I. GENERAL AND MEDICAL IMPORTANCE
Earwigs are relatively harmless insects that are occasionally seen inside homes. Theyare included in this reference because of an old wives’ tale that these insects enterhuman ears causing much torment (hence the name “earwig”). Earwigs do not enterhuman ears, or even bite, but some of the larger species may pinch human skin withtheir abdominal cerci.1
II. GENERAL DESCRIPTION
Earwigs are elongate, slender, flattened insects that are dark-colored and have forceps-like cerci (abdominal pincers). They are generally 4 to 20 mm long, and many specieshave short, stubby wings (Figure 1). Earwigs have chewing mouthparts and thread-likeantennae. Nymphs resemble the adults with differences in abdominal segments andforcep structure. Earwigs may be mistaken for rove beetles (family Staphylinidae).

154
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
III. GEOGRAPHICDISTRIBUTION
Numerous species of earwigs occur worldwide.The European earwig, Forficula auricularia,and the ringlegged earwig, Euborellia annulipes,are cosmopolitan and commonly encountered.Other pest species include the striped earwig,Labidura riparia, and the seaside earwig,Anisolabis maritima.
IV. BIOLOGY/BEHAVIOR
Earwigs are mostly nocturnal feeders, feedingon dead and decaying vegetable matter. A fewspecies will feed on living plants, and some arepredaceous. They may be destructive to gardenvegetables, flowers, stored grains, and green-house plants. During the day, earwigs hide incracks and crevices, under bark, or in piles ofdebris. It is not unusual to find them in privatewater well buildings and well casings. Accord-ingly, they can enter the system occasionallyand even come out of a faucet. Earwigs lay theireggs in burrows in the ground or among debris,and the female tends them until hatching. Thisdisplay of maternal care is rare among insects.Earwigs undergo simple metamorphosis andhave as many as six nymphal stages. In someareas, they invade homes by the thousandslooking for food and, like cockroaches, becomevery real pests. For further information the readeris referred to Ebeling,2 who discusses earwigspecies and their biology in detail.
REFERENCES1. Bishopp, F. C., Injury to man by earwigs,
Proc. Entomol. Soc. Wash., 63, 114, 1961.
2. Ebeling, W., Urban Entomology, University ofCalifornia, Division of Agricultural Science,Los Angeles, 1978, 560.
EARWIGS
Figure 1Adult earwig (from: U.S. DHEW, PHS, CDC,Pictorial Keys).
ImportanceHarmless — but often mistakenly
believed to invade human ears
DistributionWorldwide
LesionNone
Disease TransmissionNone
Key ReferenceHoffman, K. M., Proc. Entomol. Soc.
Washington, 89, 1, 1987
TreatmentNone needed

155
Fleas
CHAPTER 18
FLEAS
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................155A. Cat and Dog Fleas, Ctenocephalides felis and C. canis ........................ 157B. Oriental Rat Flea, Xenopsylla cheopis .................................................... 157C. Human Flea, Pulex irritans ................................................................... 158D. Chigoe Flea, Tunga penetrans .............................................................. 158E. Northern Rat Flea, Nosopsyllus fasciatus ............................................... 158F. Sticktight Flea, Echidnophaga gallinacea.............................................. 158G. “Sand Fleas” .................................................................................................159
II. General Description .........................................................................................159
III. Geographic Distribution ..................................................................................159
IV. Biology/Behavior .............................................................................................160
V. Treatment of Bites/Infestation ........................................................................161
References ......................................................................................................................161
I. GENERAL AND MEDICAL IMPORTANCE
Fleas are small, laterally flattened, wingless insects that are of great importance asvectors of disease in many parts of the world.1,2 Historically, public health workers havebeen most concerned with fleas that carry the agents of bubonic plague and flea-bornetyphus from rats to people and fleas that transmit plague among wild rodents andsecondarily to humans. However, in many minds (especially the lay public), theinsidious attacks by fleas on people and domestic animals causing irritation, blood loss,and severe discomfort are equal in importance to the disease threat. Included here arediscussions of a few of the more common species, comments as to their medicalimportance, and notes on their biologies.

156
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
FLEAS
Adult Cat Flea, Ctenocephalides felis
The skin reaction to flea bites is of the de-layed type. Feingold and Benjamini3 describedthe process. The flea bite lesion initially is apunctate hemorrhagic area representing the siteof probing by the insect. Lesions may occur inclusters as the flea explores the skin surface,frequently stopping and probing. There is usu-ally formation of a wheal around each probesite with the wheal reaching its peak in 5 to 30min. Pruritus is almost always present. In mostcases there is a transition to an indurated papu-lar lesion within 12 to 24 h. In sensitized indi-viduals the delayed reaction appears in 12 to 24h, persisting for a week or more. The delayedpapular reaction with its intense itching is oftenthe reason people come to a clinic.
Plague. Plague, a zoonotic disease causedby the bacterium, Yersinia pestis, has been as-sociated with humans since recorded history.Few diseases can compare to the devastatingeffects of plague on human civilization. Forexample, in the 14th century 25 million peopledied of plague in Europe. To this day, there arestill hundreds of cases occurring annually overmuch of the world (Figure 1). Sylvatic plague,sometimes also called campestral plague, is ever-present in endemic areas, circulating amongrock and ground squirrels, deer mice, voles,chipmunks, and others. Transmission from wildrodents to humans is rare. Y. pestis inflicts dam-age on the host animal by an endotoxin presenton its surface. Hematogenous dissemination ofthe bacteria to other organs and tissues maycause intravascular coagulation and endotoxicshock, producing dark discoloration in the ex-tremities (thus, the name “black death”). Threeclinical forms of plague are recognized: bu-bonic, septicemic, and pneumonic. The septice-mic and pneumonic forms are usually second-ary to the bubonic form, and the bubonic formis the most common in the Americas. Pneu-monic plague is the most dangerous because ofits spread by aerosols (coughing).
There are several methods by which fleastransmit plague. Probably the most importantmethod of infection occurs when fleas ingestplague bacilli along with host (rodent) blood.
ImportanceBiting; annoyance; papular urticaria;
vectors of disease
DistributionNumerous species worldwide
LesionVariable depending upon species; in
U.S., most lesions irregular, very itchyred wheals; may be papular,vesicular, or bullous
Disease TransmissionPlague; murine typhus; intermediate
hosts of dog tapeworm
Key ReferenceLewis, R.E., Flea chapter in Medical
Insects and Arachnids, edited byLane and Crosskey, Chapman andHall Co., 1993.
TreatmentTopical corticosteroids; antibiotics if
secondary infection; tungiasis(tropics) may require excision of theembeded fleas

157
Fleas
Figure 1Status of plague in the world.
In the flea stomach, tremendous multiplication of the bacteria takes place (flea fecesthen also become infected). In some species — especially Xenopsylla — furthermultiplication of the bacteria occurs in the proventriculus, resulting in the fleabecoming “blocked”. When blocked fleas try to feed, there is regurgitation of bloodmeal products from previous feedings. Blocked fleas become increasingly starved andrepeatedly bite in order to get a blood meal. Also, as mentioned, flea feces can beinfective, especially when rubbed into abrasions (such as bite wounds) in the skin.Plague bacilli can remain infective in flea feces for as long as 3 years.3a
A. Cat and Dog Fleas, Ctenocephalides felis and C. canis
Cat fleas are the fleas most often encountered by people in the U.S. (the dog flea isrelatively rare in North America). Contrary to their name designation, dog fleas mayfeed on cats and cat fleas feed on dogs. In fact, in many areas the predominant fleaspecies infesting dogs is the cat flea. Both species are mainly just pest species.However, the fleas are intermediate hosts of the dog tapeworm, Diphylidium caninum,and their bites may produce papular urticaria. Children sometimes become infected viaclose contact with a flea-infested dog.
B. Oriental Rat Flea, Xenopsylla cheopis
This medically important flea is an ectoparasite of Norway rats and roof rats. It is theprimary vector of the agent of plague, Yersinia pestis, (see previous section) and isinvolved in the transmission of murine (endemic) typhus organisms, Rickettsia typhi,from rat to rat and from rats to people. Murine typhus is one of the most widelydistributed arthropod-borne infections, endemic in many coastal areas and portsthroughout the world. Almost all cases in the U.S. are concentrated in central and south-central Texas and in Los Angeles and Orange Counties in California.

158
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
C. Human Flea, Pulex irritans
This flea occasionally becomes abundant on farms, especially in abandoned pig pens.Feingold and Benjamini3 said this flea was one of two primary species involved in fleabite allergic reactions in the San Francisco area.
D. Chigoe Flea, Tunga penetrans
This flea, also sometimes called the jigger, nigua, chica, pico, pique, or suthi, burrowsinto the skin of people in tropical and subtropical regions.4 In most cases the favoritepoints of attachment are between the toes and under the toe nails. Unlike most fleaspecies, which spend only a small proportion of their lives on a host animal, T.penetrans remains embedded in the skin. The female remains embedded throughoutblood engorgement and egg development, which leads to great enlargement of the fleabody. Enlarging female fleas on human feet cause intense itching and inflammation andmay produce swellings and ulceration. Secondary infection is common.
E. Northern Rat Flea, Nosopsyllus fasciatus
The northern rat flea spends most of its adult life on Norway rats and roof rats. Thisflea is also involved in the transmission of murine typhus organisms among rats andto humans.
F. Sticktight Flea, Echidnophaga gallinacea
This flea (Figure 2) is primarily a pest of poultry, but humans are often attacked. Asin the case with the chigoe flea, E. gallinacea attaches firmly to its host and engorgeswith blood. It may remain embedded in the integument of the host for some time.Chickens frequently have dark flea-covered patches around the eyes, comb, or wattles.
Figure 2Sticktight flea (from: USDA Bull. No. 248, 1948).

159
Fleas
G. “Sand Fleas”
The lay public uses the term “sand fleas” so much that it is included in this section.In the northern U.S. what people call sand fleas are usually cat or dog fleas found invacant lots and associated with stray cats or dogs. In the western U.S., cat fleas orhuman fleas associated with deer, ground squirrels, stray cats and dogs, or prairie dogsare sometimes termed “sand fleas.” Cat and dog fleas, and occasionally sticktight fleas,are called sand fleas in the South. In addition, tiny crustaceans in the order Amphipodaoccurring abundantly in seaweed along coastal beaches are also called sand fleas orbeach fleas.
II. GENERAL DESCRIPTION
Adult fleas have laterally compressed bodies, are between 2 to 6 mm long, and areusually brown or reddish-brown with stout spines on their head and thorax (Figure 3).They have a short, clublike antenna over each eye. Each segment of their three-segmented thorax bears a pair of powerful legs terminating in two curved claws. Thechigoe flea is actually quite easily identified since it is so small (1 mm) and has a greatlyshortened thorax. Figure 4 is a depiction of the heads of the species discussed here.Most fleas move quickly on skin or in hair and can jump 30 cm or more. They arereadily recognized by their jumping behavior when disturbed.
III. GEOGRAPHIC DISTRIBUTION
Most of the 2,000 or so species of fleas are seldom seen or encountered, being foundonly on some small rodents, bats, or birds, often within a restricted range. Below are
Figure 3Adult cat flea, Ctenocephalides felis, with parts labeled (from: U.S. DHEW, PHS,CDC, Pictorial Keys).

160
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
the distributions of the seven species discussed here:
• Cat and Dog Fleas — Worldwide in and around homes with pets. In certainregions one species may occur to the exclusion of the other.
• Oriental Rat Flea — Worldwide wherever Rattus rattus is found.• Human Flea — Nearly cosmopolitan although there may be large geographic
areas apparently free of this species. This seems to be especially true in areasuninhabited by people.
• Chigoe Flea — Tropical and subtropical regions of North and South America,the West Indies, and Africa. After a 40-year absence, this species has recentlyreappeared in Mexico.5 There is one record of the chigoe flea in the U.S.(Texas).6
• Northern Rat Flea — Widespread over Europe and North America and lesscommonly in other parts of the world.
• Sticktight Flea — Widely distributed in the warmer countries of the world,including Australia.
IV. BIOLOGY/BEHAVIOR
Adult fleas have piercing–sucking mouthparts and feed exclusively on blood. The hostsof fleas are domesticated and wild animals, especially wild rodents. If hosts areavailable, fleas may feed several times daily, but in the absence of hosts, adults mayfast for months, especially at low-to-moderate temperatures. Some of the above-mentioned species have specialized life cycles, but in general, the life cycle of mostfleas ranges from 30 to 75 days and involves complete metamorphosis.
Since cat fleas are a notable pest and seemingly ubiquitous, their life cycle ispresented here. Adult female fleas begin laying eggs 1 to 4 days after starting periodicblood feeding. Blood meals are commonly obtained from cats, dogs, and people, butother medium-sized mammals may be affected as well. Females lay 10 to 20 eggs dailyand may produce several hundred eggs in their lifetime. Eggs are normally deposited
Figure 4Flea heads: Ctenocephalides felis (A),Ctenocephalides canis (B), Xenopsyllacheopis (C), Pulex irritans (D), Tungapenetrans (E), Nosopsyllus fasciatus (F),and Echidnophaga gallinacea (G)(redrawn from: U.S. DHEW, PHS, CDCPictorial Keys and USDA Misc. Publ. No.500).

161
Fleas
in nest litter, bedding, carpets, etc. Warm, moist conditions are especially favorable foregg production. Eggs quickly hatch into spiny, yellowish-white larvae. Flea larvae havechewing mouthparts and feed on host-associated debris including food particles, deadskin, and feathers. Blood defecated by adult fleas also serves as an important sourceof nutrition for the larvae. Larvae pass through three instars prior to pupating. Flealarvae are very sensitive to moisture and will quickly die if continuously exposed toless than 60 to 70% relative humidity. Pupating flea larvae spin a loose silken cocooninterwoven with debris. If environmental conditions are unfavorable, or if hosts are notavailable, developing adult fleas may remain inactive within the cocoon for extendedperiods. Adult emergence from the cocoon may be triggered by vibrations resultingfrom host movements.
V. TREATMENT OF BITES/INFESTATION
The chigoe or burrowing flea, T. penetrans, may need to be removed surgically.Alexander4 said that within the first 48 h of attachment, a sterile needle may be usedto accomplish this. During maturation of the eggs, curettage of the contained flea andcautery of the hollow are sufficient.4 For a mature flea, Alexander recommended totalexcision of the flea under local anesthesia.4
Most other fleas bite but do not remain attached or embedded. Dog or cat flea bitesproduce reddening, papules, and itching, but generally require no specialized medicaltreatment. Oral antihistamines may help relieve the itching, and corticosteroids can aidin resolution of the lesions. Scratching of flea bites may produce secondary infectionand should be avoided. An antiseptic or antibiotic ointment may be indicated. Ofprimary concern, however, is to eliminate the source of flea infestation. This mayinvolve sanitation, insecticidal treatment of pets, and spraying of both indoor andoutdoor premises.
REFERENCES1. Bibikova, V. A., Contemporary views on the interrelationships between fleas and the
pathogens of human and animal diseases, Ann. Rev. Entomol., 22, 1, 1977.
2. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, chap. 14.
3. Feingold, B. F. and Benjamini, E., Allergy to flea bites, Ann. Allergy, 19, 1275, 1961.
3a. Service, M. W., Medical Entomology for Students, Chapman and Hall, New York, 1996,chap. 11.
4. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 11.
5. Ibanez-Bernal, S. and Velasco-Castrejon, O., New records of human tungiasis in Mexico,J. Med. Entomol., 33, 988.
6. Ewing, H.E. and Fox, I., The fleas of North America, U.S.D.A. Misc. Publ. 500, 1943, 28.


163
Flies (Biting)
CHAPTER 19
FLIES (BITING)
TABLE OF CONTENTS
I. Black Flies ........................................................................................................164A. General and Medical Importance ..............................................................164B. General Description ....................................................................................164C. Geographic Distribution .............................................................................164D. Biology/Behavior .........................................................................................165E. Treatment of Bites .......................................................................................165
II. Deer Flies .........................................................................................................166A. General and Medical Importance ..............................................................166B. General Description ....................................................................................166C. Geographic Distribution .............................................................................166D. Biology/Behavior .........................................................................................167E. Treatment of Bites .......................................................................................167
III. Horse Flies .......................................................................................................168A. General and Medical Importance ..............................................................168B. General Description ....................................................................................168C. Geographic Distribution .............................................................................168D. Biology/Behavior .........................................................................................168E. Treatment of Bites .......................................................................................169
IV. Midges (Biting Midges, Biting Gnats) ............................................................169A. General and Medical Importance ..............................................................169B. General Description ....................................................................................169C. Geographic Distribution .............................................................................169D. Biology/Behavior .........................................................................................170E. Treatment of Infestation .............................................................................170
V. Sand Flies .........................................................................................................171A. General and Medical Importance ..............................................................171B. General Description ....................................................................................176

164
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
C. Geographic Distribution .............................................................................176D. Biology/Behavior .........................................................................................177E. Treatment of Bites .......................................................................................177
VI. Stable Flies .......................................................................................................178A. General and Medical Importance ..............................................................178B. General Description ....................................................................................178C. Geographic Distribution .............................................................................178D. Biology/Behavior .........................................................................................179E. Treatment of Bites .......................................................................................180
VII. Tsetse Flies .......................................................................................................180A. General and Medical Importance ..............................................................180B. General Description ....................................................................................182C. Geographic Distribution .............................................................................182D. Biology/Behavior .........................................................................................182E. Treatment of Bites .......................................................................................183
References ......................................................................................................................183
I. BLACK FLIESA. General and Medical Importance
Black flies (also called buffalo gnats, turkey gnats, and Kolumbtz flies) are small,humpbacked flies that are important as vectors of disease and as nuisance pests.1,2 Inthe tropics, black flies are vectors of the parasite, Onchocerca volvulus, which causesa chronic nonfatal disease with fibrous nodules in subcutaneous tissues and sometimesvisual disturbances and blindness (river blindness). Onchocerciasis infects approxi-mately 18 million people in Africa and Latin America.3 In the temperate region blackflies are notorious pests, often occurring in tremendous swarms and biting viciously.The bites may be painless at first, but bleed profusely. Systemic reactions to black flybites have been reported consisting of itching, burning, papular lesions accompaniedby fever, leukocytosis, and lymphadenitis. Death can result from anaphylactic shock,suffocation, and/or toxemia.
B. General Description
Black flies vary in size from about 2 to 5 mm and are thus smaller than mosquitoes.They are black, humpbacked flies with broad wings and stout bodies (Figure 1). Blackflies have short legs and large compound eyes. Their antennae are short (although in9 to 12 segments) and bare.
C. Geographic Distribution
There are numerous important species of black flies: Prosimuliim mixtum is a seriouspest of people and animals in much of the U.S. as well as Cnephia pecuarum in theMississippi Valley. Simuliim vittatum and S. venustum seriously annoy livestock,fishermen, and campers in U.S. In the Balkans region (former Yugoslavia), there have

165
Flies (Biting)
BLACK FLIES
Figure 1Typical adult black fly (from: Miss. State Dept.Health Publ. “The Mosquito Book,” by E. Bowles).
been severe outbreaks of S. colombaschense(the infamous golubatz fly) and S. erythro-cephalum. Other notorious pests in Europe in-clude S. equinum, S. ornatum, and S. reptans.In Africa, members of the S. damnosum and S.neavei complexes are important vectors ofonchocerciasis. In Central and South America,vectors of onchocerciasis are S. ochraceum andS. metallicum.
D. Biology/Behavior
The larvae of black flies are aquatic and developin shallow, fast-flowing streams, mainly in up-land regions. The filter-feeding larvae have acirclet of numerous radiating rows of tiny hookslocated on the tip of the abdomen. These hooksare used for attaching to silk, which the larvaesecrete onto solid substrates. Larvae also pro-duce silk for construction of the pupal cocoon.There are usually 6 to 9 larval instars. The den-sities of larvae can be tremendously high, and insome areas they can cover the entire substrate atthe head of stream riffles. Life cycle length variesfrom 1 year to as little as 2 weeks depending onthe species and geographic location. Males formsmall mating swarms during prenuptial behavior,and mating occurs in the air. Eggs are usually laidin groups of 150 to 600 in or near a water source.Adult black flies are most prevalent during latespring and early summer when they may bepresent in large swarms. They are usually en-countered near streams or lake outlets, but dueto migration, may be dispersed and found tens ofmiles from the original water source. Black fliesbite in the daytime, mostly in early morning andnear evening.
E. Treatment of Bites
Black fly bites may be itchy and slow healing.Antiseptic and soothing lotions as well as cor-ticosteroids may relieve pain and itching andhelp lesions resolve. Systemic reactions charac-terized by hives, wheezing, fever, leukocytosis,and/or widespread urticaria require intensiveevaluation and treatment. If the reaction is mild,oral antihistamine therapy may suffice, but se-vere reactions involving shock will probably
ImportanceFierce biters; possible systemic RXNS
DistributionNumerous species worldwide
LesionVariable — often small itching papules,
sometimes erythematous wheals andswelling
Disease TransmissionOnchocerciasis
Key ReferencesGudgel, E. F. and Grauer, F. H., Arch.
Dermatol. Syphiol., 70, 609, 1954
Crosskey, R. W., John Wiley, Chichester(U.K.), 1990
TreatmentPalliative creams and/or corticosteroids;
oral antihistamines may relieveitching; systemic RXNS may requiretreatment for shock

166
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
ImportanceAnnoyance; painful bites
DistributionNumerous species worldwide
LesionDeep and painful singular lesions,
sometimes leading to cellulitis
Disease TransmissionTularemia; loiasis (Africa)
Key ReferencesStone, A., USDA Misc Publ #305, 1938
Foil, L. D., Parasitol. Today, 5, 88, 1989
TreatmentSystemic antibiotics if cellulitis; allergic
RXNS may require antihistamines andepinephrine; otherwise soothingointments, lotions
DEER FLIES
Figure 2Adult deer fly, Chrysops discalis (from: U.S.DHHS (CDC) Publ. No. 83–8297).
require epinephrine (see Chapter 2). Personsbitten by black flies in Africa and Latin Americamay need follow-up for possible developmentof onchocerciasis.
II. DEER FLIESA. General and Medical Importance
Deer flies belong to the family Tabanidae (thesame one as horse flies) but are usually muchsmaller. Deer flies are extremely annoying topeople in the outdoors during summer months,often circling persistantly around the head. Likehorse flies, deer flies have scissorlike mouth-parts and can inflict painful bites. Deer fly bitesoften become secondarily infected; in hyper-sensitive individuals they have been known toproduce systemic reactions characterized bygeneralized urticaria and wheezing. In the U.S.,the deer fly Chrysops discalis mechanically trans-mits tularemia organisms from rabbits to peopleby its bites.4,5 In the African equatorial rainforest, deer flies (particularly C. silacea and C.dimidiata) transmit the filarial parasite Loa loa.Loiasis affects an estimated 2 to 13 millionindividuals and is characterized by Calabarswellings (localized nonpitting edema mainlyon the wrists or ankles, 5 to 20 cm in diameter,lasting from a few hours to a few days), gener-alized pruritus, arthralgia, fatigue, hypereosino-philia, and sometimes serious CNS involvement.6
The pathognomonic symptom of loiasis, sub-conjunctival migration, is actually uncommon.
B. General Description
Deer flies (about 8 to 15 mm long) are abouthalf as large as horse flies (Figure 2). They havewings with dark markings and have apical spurson their hind tibiae (Figure 3). Many deer flyspecies are gray or yellow-gray in color withvarious arrangements of spots on the abdomen.
C. Geographic Distribution
Numerous deer fly species occur almost world-wide. In the U.S., C. discalis occurs sparsely inthe East but more so in the Southwest. Chrysops

167
Flies (Biting)
Figure 3Deer fly.
atlanticus is a troublesome pest in the eastern U.S., and C. noctifer is one of the mostcommon western species. Chrysops silacea and C. dimidiata occur in Africa.
D. Biology/Behavior
Deer flies breed in moist or semiaquatic sites such as margins of ponds, damp earth,or other sites containing various amounts of mud and water. The worm-like carnivorouslarvae spend their life in these wet, muddy habitats and then migrate to drier areas ofsoil to pupate. After the pupal stage, the adult flies emerge. The entire life cycle maytake 2 years or more to complete in temperate regions. Females seek a blood meal,whereas males feed on flower and vegetable juices. In the temperate zones, deer fliesare active in the late spring and summer months, mostly in the early morning and lateafternoon. Members of the genus Chrysops live in areas having a mixture of forest andopen land and feed on various members of the deer family. However, they willaggressively pursue and bite people. Interestingly, in Africa, studies have shown thatthe presence of wood fires in local villages is attractive to C. silacea.7 Most bloodsuck-ing insects are repelled by the smoke of a wood fire.
E. Treatment of Bites
Except for secondary infections, which require an appropriate antibiotic, deer fly bitesare generally few and self-limiting. Antiseptic and soothing lotions may relieve pain and

168
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
HORSE FLIES
ImportanceAnnoyance; painful bites; possible
systemic RXNS
DistributionNumerous species worldwide
LesionDeep and painful singular lesions
sometimes leading to cellulitis
Disease TransmissionNone
Key ReferencesStone, A., USDA Misc Publ #305, 1938
Foil, L. D., Parasitol. Today, 5, 88, 1989
TreatmentSystemic antibiotics if cellulitis; allergic
RXNS may require antihistamines andepinephrine; otherwise soothingointments, lotions
Figure 4Adult horse fly (from: USDA Yearbook ofAgriculture, 1952).
itching. Allergic reactions characterized by hives,wheezing, and/or widespread urticaria requireintensive evaluation and treatment. If the reac-tion is mild, oral antihistamine therapy may suf-fice, but severe reactions involving shock willprobably require epinephrine (see Chapter 2).
Follow-up may be prudent for persons bittenby deerflies in the southwestern U.S. (tularemia)or the African equatorial rain forest (L. loa filari-asis).
III. HORSE FLIESA. General and Medical Importance
Horse flies (also family Tabanidae) are large,robust bloodsucking flies that are notoriouspests of horses, cattle, deer, and other mam-mals.1 Several species of horse flies will alsoattack people. Horse fly bites have been knownto produce systemic reactions in humans char-acterized by generalized urticaria and wheez-ing.
B. General Description
Horse flies look like giant robust house flies.They are often 20 to 25 mm long and have largeprominent eyes (Figure 4). The antennae haveonly three sections. Their proboscis projectsforward, and the female’s mouthparts arebladelike for a slashing/lapping feeding method.
C. Geographic Distribution
Horse flies are distributed worldwide. Mostpeople-biting species are in the genera Ta-banus, Hybomitra, and Haematopota. Some ofthe notorious pest species include Tabanusatratus (the large black horse fly), T. lineola,and T. similis (the familiar striped horse flies) inthe eastern U.S., and T. punctifer and Atylotusincisuralis in the West.
D. Biology/Behavior
Horse fly biology is very similar to that of deerflies. Basically, they breed in moist or semi-

169
Flies (Biting)
aquatic sites such as pond margins, damp earth, or rotten logs. The grublike larvaespend their life in wet mud, dirt, or shallow water and then pupate in drier patchesof soil. Larval development may take a year or more. After a pupal stage, the adult fliesemerge. Females seek a blood meal, whereas males feed on nectar from flowers andother vegetable juices. In the temperate region, horseflies are active only in the warmermonths of the year.
E. Treatment of Bites
Horse fly bites are generally few and self-limiting. If secondary infection/cellulitisdevelops, appropriate systemic antibiotics are indicated. Antiseptic and soothing lotionsmay relieve pain and itching. Allergic reactions characterized by hives, wheezing, and/or widespread urticaria require intensive evaluation and treatment. If the reaction ismild, oral antihistamine therapy may suffice, but severe reactions involving shock willprobably require epinephrine (see Chapter 2).
IV. MIDGES (BITING MIDGES, BITING GNATS)A. General and Medical Importance
The biting midges are very tiny slender gnats in the family Ceratopogonidae; they aresometimes called “punkies,” “no-see-ums,” “gnats,” or “flying teeth” (see Color Figure19-16). In the Caribbean region and Australia they are referred to as “sand flies” (notto be confused with psychodid sand flies, see Section V of this chapter). Adult bitingmidges are vicious and persistent biters, and some persons have strong reactions totheir bites. Their small size allows them to pass through ordinary screen wire used tocover windows and doors. These tiny insects are generally not involved in thetransmission of disease agents to humans. However, in Africa and South Americacertain species may be able to transmit filariae, protozoa, and viruses (particularly Shuniand Oropouche viruses in the Simbu group of arboviruses).
B. General Description
Biting midges are typically gray in color (although some species may be yellowish),extremely small, 0.6 to 1.5 mm, and delicate (Figure 5) with narrow wings that have fewveins and no scales. The wings may be clear or hairy, sometimes distinctly spotted (withpigment, not scales as in mosquitoes), and folded scissorlike over the abdomen at rest.The eyes on each side of the head are black and the proboscis protrudes forward anddownward. Biting midges somewhat resemble other small species of nonbiting gnats inthe family Chironomidae, but they are not as large and mosquito-like as chironomids.Swarms of biting midges are small and inconspicuous. People attacked by this midge willoften comment when outdoors, “Something is biting me but I can’t see what it is.”
C. Geographic Distribution
There are numerous species of Ceratopogonidae inhabiting much of the world intemperate and tropical areas: Culicoides furens is a vicious biter occurring in saltmarshes along the Atlantic and Gulf Coasts, from Massachusetts to Brazil, and alongthe Pacific Coast, from Mexico to Ecuador. In California, Leptoconops torrens and L.

170
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
BITING MIDGES
Adult Biting Midge, Culicoides furens
ImportanceAnnoyance from biting
DistributionNumerous species occurring worldwide
LesionMinute papular lesions with
erythematous halo, wheals may occurin sensitized persons
Disease TransmissionGenerally none
Key ReferencesKwan, W. H. and Morrison, F. O., Ann.
Soc. Entomol. Quebec, 19, 127, 1974
Downes, J. A., Memoirs Entomol. Soc.Canada, 104, 1, 1978
TreatmentAntipruritic lotions or creams
carteri are very bothersome. C. pulicaris is aserious pest of farm workers in Europe, andForcipomyia (Lasiohelea) taiwana is a severepest in Taiwan and Japan. In the Near andMiddle East, Central Asia, Africa, and SouthernEurope, L. kerteszi is an avid biter of people. Itsbites may become vesicular, resulting in anopen lesion that may exude moisture for aweek or more. Austroconops macmillani is avicious biter in western Australia, and L.spinosifrons is a beach pest in East Africa, Mada-gascar, India, Sri Lanka, and the Malay Archi-pelago.
D. Biology/Behavior
Only female ceratopogonids bite people; themales feed on the nectar of flowers. Femalesfeed by the way of small cutting teeth on theelongated mandibles in their proboscis whichthey use to make a small cut in the skin. Achemical is present in the saliva to preventblood clotting. Some of the cut capillaries bleedand form a tiny pool of blood that is thensucked up. Larval stages develop in highly or-ganic detritus overlaying the bottom of shallowareas of water or in water-saturated soil high inorganic material. They especially seem to befound in salt marshes. The larvae look more likeworms than maggots (Figure 5). Female bitingmidges lay their eggs on the water or on avariety of objects overhanging larval habitats.Most species are active only in the warmermonths of the year, but some may be activeyear round. Lillie et al.8 found that adultCulicoides host-seeking activity was greatest nearsunrise and sunset, during the night when themoon was full, and during the afternoon hoursin winter and early spring. They usually do notbite during the midday, except when the sky isheavily overcast and the winds are calm.
E. Treatment of Infestation
Alexander9 said that simple antipruritics (oilycalamine lotion or hydrocortisone with addedanti-infective agents) are all that is needed forbiting midge bites. Probably the best course ofaction for those affected by biting midges is a

171
Flies (Biting)
Figure 5Life stages and life cycle of Culicoides furens (photo courtesyFlorida Medical Entomology Laboratory, IFAS, Univ. Florida).
combination of avoidance and personal protection measures. Use of finer mesh screenwire can prevent entry of these flies into dwellings. Repellents containing DEET andlong-sleeved shirts and long pants can provide relief to those persons outside ininfested areas. DEET has been shown to be very effective in repelling Culicoides.10
The bath oil, Avon Skin-So-Soft®, is sometimes used as a repellent, and controlledstudies indicate that the product provides some protection from Culicoides midges.10
However, product effectiveness is not because it repels midges, but because theoiliness traps the midges on the skin surface.
V. SAND FLIES
A. General and Medical Importance
Sand flies are tiny bloodsucking flies in the family Psychodidae that transmit thecausative agents of bartonellosis (Carrión’s disease), sand fly fever, and leishmaniasis.Sand fly fever, a viral disease, occurs in those parts of southern Europe, the Mediter-ranean, the Near and Middle East, Asia, and Central and South America where thePhlebotomus vectors exist. Bartonellosis caused by the bacillus, Bartonella bacilliformis,occurs in the mountain valleys of Peru, Ecuador, and southwest Colombia. Leishma-niasis occurs in tropical and subtropical areas over much of the world (Figure 6). Therehas been a recent resurgence of leishmaniasis. It is now found in 88 countries and isincreasingly being reported in non-endemic areas. Contributing factors to the increasein leishmaniasis include human settlement in zoonotic foci and urbanization up to theedge of forests. In many cases, the sylvatic cycles have now become peridomestic. Thelife cycle of Leishmania donovani is shown in Figure 7 to illustrate the involvementof sand flies in parasite life cycles.
Clinically, leishmaniasis manifests itself in four main forms: (1) cutaneous, (2)mucocutaneous, (3) diffuse cutaneous, and (4) visceral. The cutaneous form mayappear as small and self-limited ulcers that are slow to heal. When there is destruction

172
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
CASE HISTORYPAINFUL HORSE FLY BITE
On June 20 a woman in Jackson, Mississippi was awakened during the night by a painfulinsect bite on her right arm. Looking around, she noticed a large horse fly on the ceilingabove the bed. Earlier that evening the horse fly had gotten inside the house and she andher husband had unsuccessfully tried to find/remove it. Apparently, the horse fly laterfound the victim sleeping and attempted to take a blood meal. Within 8 hours the bite sitewas a 5-cm erythematous indurated plaque, hot to the touch (Figure 1). Other than apersistent itch for a few days, no further complications arose.
Comment. Horse flies are robust flies known for biting horses, cows, and other largemammals. Some species are almost 2 inches long. They do not have tube-like mouthpartsfor piercing-sucking, but instead, have a complex arrangement of blade-like mandibles andstyliform maxillary galeae which cut/slash wounds in their hosts’ skin (Figure 2). Horse fliesthen draw up the blood by means of pseudotracheae on labellar lobes. Blood uptake isquite inefficient, with blood often seen dripping from the wound.
The lesion described (above) was warm on palpation due to inflammation and vasculardilatation. Various immune cells attracted to the site (or formed) as part of the immunereaction release histamine which causes blood vessels to dilate. Induration of a lesion likethis is not only from the influx of cells but histamine also causes fluid to be leaked fromthe small skin blood vessels making the area feel hard and raised. Other than possiblesecondary infection, no human diseases are known to be caused by horse flies.
Figure 1Lesion resulting from horse fly bite, 8 h post bite.

173
Flies (Biting)
of nasal and oral mucosa, the disease is labeled mucocutaneous leishmaniasis (Figure8). Sometimes there are widespread cutaneous papules or nodules all over the body— a condition termed diffuse cutaneous leishmaniasis. Finally, the condition in whichthe parasites invade cells of the spleen, bone marrow, and liver — causing widespreadvisceral involvement — is termed visceral leishmaniasis. The only human sand-fly-transmitted disease in the U.S. is probably the few cases of cutaneous leishmaniasisdiagnosed each year in south Texas.11-13
For a long time, the above-mentioned Old World and New World disease forms werecorrelated with various Leishmania species and geographic regions to make a well-defined classification. As is the case in many paradigms in science, this classificationis turning out to be not so clear cut. There is apparently a whole spectrum of disease— from cutaneous to visceral — depending upon many factors such as species ofLeishmania, numbers of parasites (parasite burden), and the predominant host immuneresponse. The idea that a few Leishmania species each cause a distinct and separateclinical syndrome is no longer valid. For example, a visceral species, L. chagasi, hasalso been isolated from patients with cutaneous leishmaniasis in several CentralAmerican countries. However, the particular parasite species and geographic locationmay still serve as useful epidemiologic “labels” for the study of the disease complexand generalized statements can be made. For example, L. donovani and L. infantumgenerally cause visceral leishmaniasis in the Old World, while L. tropica and L. majorcause cutaneous lesions. In the New World, visceral disease is mainly caused by L.chagasi, cutaneous lesions by L. mexicana and related species, and mucocutaneouslesions by L. braziliensis. Further, by sorting out which species do not cause humandisease in a given area, researchers are more able to focus their studies on the ecologyand behavior of those that do.
Figure 2Diagrammatic representation of horse fly mouthparts.

174
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 6Approximate world-wide distribution of leishmaniasis.

175
Flies (Biting)
Figure 7Life cycle of Leishmania donovani (reprinted with permission of Macmillian PublishingCompany from ESSENTIALS OF MEDICAL PARASITOLOGY by Thomas J. Brooks, Jr., Copyright(c) 1963 Thomas J. Brooks, Jr.).

176
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
B. General Description
Sand flies are tiny (about 3 mm long), golden, brownish, or gray long-legged flies(Figure 9). The females have long, piercing mouthparts adapted for blood sucking. Adistinctive feature of these flies is the way they hold their wings V-shaped at rest. Theyhave long, multisegmented antennae and hairs (not scales) covering much of the bodyand wing margins.
C. Geographic Distribution
Members of the sand fly genera Phlebotomus and Sergentomyia occur in the Old World,and Lutzomyia, Brumptomyia, and Warileya occur in the tropics and subtropics of theNew World. P. argentipes is the chief vector of visceral leishmaniasis in many areas ofthe Old World; P. langeroni has recently been incriminated. Lutzomyia longipalpis isa major vector in the New World. Old World sand fly vectors of dermal leishmaniasisinclude P. caucasicus, P. papatasi, P. longipes, and P. pedifer. New World vectors ofthe malady include L. olmeca, L. trapidoi, L. ylephiletrix, L. verrucarum, L. peruensis,and others. Sand fly fever vectors are primarily P. papatasi and P. sergenti. Bartonellosisis transmitted by L. verrucarum.
Since P. papatasi is the most important and widespread vector of zoonotic cutaneousleishmaniasis caused by Leishmania major in the Old World, its distribution is givenin Figure 10.
Figure 8Mucocutaneous leishmaniasis (photo courtesy Armed Forces Institute of Pathology, negativenumber 74-8873-1).

177
Flies (Biting)
SAND FLIES
Figure 9Adult sand fly (from: Miss. State Dept. HealthPubl. “The Mosquito Book,” by E. Bowles).
Figure 10Approximate geographic distribution ofPhlebotomus papatasi.
ImportanceVectors of several important diseases
DistributionNumerous species almost worldwide
LesionSometimes red papules and/or urticarial
wheals
Disease TransmissionLeishmaniasis, bartonellosis, sand fly
fever
Key ReferenceYoung, D. G. and Perkins, P. V., J. Am.
Mosq. Contr. Assoc., 44, (2), Part 2(Supplement), 1984
TreatmentExcept for hypersensitivity RXNS,
palliative antipruritic lotions orcreams
Lutzomyia anthophora or L. diabolica,which generally occur in south and centralTexas as well as in parts of Mexico, are thoughtto be the vectors of human cases of cutaneousleishmaniasis in Texas.
D. Biology/Behavior
Female sand flies are blood feeders; males arenot, but will suck moisture from availablesources. Despite their medical importance, muchof what is known about sand flies is speculativeor based on limited field observations. Sandflies are usually found in microhabitats withinlarger biological communities. Examples of thesemicrohabitats are caves, cavities, tree holes,burrows, pit latrines, animal enclosures, andother buildings. Breeding is believed to takeplace in these areas, and feeding on hostsoccurs there or in the close vicinity. Sand fliesin the genus Brumptomyia feed on armadillos,whereas Lutzomyia spp. feed on both mam-mals and reptiles. Members of the genusSergentomyia feed on reptiles and amphibians.Phlebotomus spp. are exclusively mammal feed-ers. Sand flies are generally active at night whenthere is little or no wind, but a few species mayfeed during the day if disturbed or under cloudyor shaded conditions. They normally rest dur-ing the day in their microhabitats. Sand flydevelopment is relatively slow, taking up toseveral months to complete the life cycle.
P. papatasi, the primary vector of leishma-niasis in the Middle East region, is a nocturnal,desert species flying from sunset through dark.It enters dwellings from animal burrows up to50 m away. Its activity diminishes rapidly whenrelative humidity falls below 65%, temperaturerises above 80°F, or wind velocity exceeds 5mi/h.
E. Treatment of Bites
Sand flies are relatively uncommon, thus theirbites are generally few and self-limiting. Sooth-ing and antiseptic lotions may relieve itchingand prevent secondary infection. Follow-up ofpatients with sand fly bites or persons withexposure to areas endemic with the several

178
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
STABLE FLIES
ImportanceNuisance biting
DistributionMost of world
LesionSmall evanescent papules
Disease TransmissionNone
Key ReferenceZumpt, F., Gustave Fischer Verlag
Publishing Co., Berlin, 1973
TreatmentExcept for hypersensitivity RXNS (rare)
or secondary infection, soothing and/or antiseptic lotions or creamssufficient
Adult Stable Fly, Stomoxys calcitrans
sand-fly-transmitted diseases is needed to diag-nose and treat these maladies. In the case ofleishmaniasis, diagnosis is delayed by physi-cians unfamiliar with the clinical features andvarious forms of the disease. Cutaneous leish-maniasis is often initially described as a “boil” or“ulcer that fails to heal.” In addition, cutaneousleishmaniasis needs to be differentiated fromother skin lesions such as those resulting fromleprosy, tuberculosis cutis, sporotrichosis, histo-plasmosis (Histoplasma duboisii), molluscumcontagiosum, and cutaneous sarcoidosis.
VI. STABLE FLIESA. General and Medical Importance
The stable fly, Stomoxys calcitrans, is a signifi-cant medical and veterinary pest.14 People whosay “a house fly bit me” are usually mistakenlyreferring to the stable fly. The flies (sometimesalso called dog flies) are fierce biters of people,pets, and livestock, and are a major pest insome seacoast areas, impeding development.Because of their bloodsucking habits, the flieshave been suspected of transmitting a numberof human diseases by mechanical action, butproof is lacking.
B. General Description
Stable flies are 5 to 6 mm long, have a dull graythorax with four dark longitudinal stripes, andhave a dull gray abdomen with dark spots(Figure 11). They look very similar to house-flies, but they are slightly larger and have a rigidproboscis projecting forward in a bayonetlikefashion (Figure 12). In contrast, house flies havesponging mouthparts that project downward.
C. Geographic Distribution
The stable fly occurs throughout most of theworld. There is a related species, S. nigra, thatoccurs throughout Africa and attacks horses,donkeys, cattle, and people.

179
Flies (Biting)
Figure 11Stable fly life cycle (from: Alabama Coop. Ext. Ser.).
Figure 12House fly (A) and stable fly (B) mouthpart comparison (from: U.S. DHHS (CDC) Publ. No. 83–8297).
D. Biology/Behavior
Both male and female stable flies are vicious biters, both taking bloodmeals. It onlytakes 3 to 4 min for them to engorge to full capacity. The female lays her eggs in plantwaste, cut grass, old hay stacks, piles of fermenting seaweed, or manure (if there issufficient straw or hay mixed in it). Larval development takes 8 to 30 days dependingupon temperature. The larvae (maggots) look almost identical to those of house flies.Stable flies may overwinter as pupae, but normal pupal development takes about 1 to

180
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
3 weeks. Overall, under optimum conditions,the total time for development of stable fliesfrom eggs to adults is about 35 days. Adultsremain alive for a month or two. They bitepeople and animals during the day.
E. Treatment of Bites
Stable fly bites are generally few and self-limit-ing. Antiseptic and soothing lotions may relievepain and itching. Allergic reactions character-ized by hives, wheezing, and/or widespreadurticaria are rare but require intensive evalua-tion and treatment.
VII. TSETSE FLIESA. General and Medical Importance
There are over 20 species of flies in the genusGlossina which are called tsetse flies. Most ofthe species are vectors of trypanosomes of peopleand animals (Figure 13); however at least sixspecies are of primary importance as vectors ofAfrican trypanosomiasis, caused by subspeciesof the protozoan, Trypanosoma brucei (ColorFigure 19-17). The disease is called sleepingsickness because there is often a steady pro-gression of meningoencephalitis, with increaseof apathy, fatigability, confusion, and somno-lence. The patient may gradually become moreand more difficult to arouse and finally be-comes comatose. The disease is re-emergingand the WHO estimates that 350,000 to 500,000cases of African trypanosomiasis occur eachyear. Countries affected the most include theDemocratic Republic of Congo, Angola, andSudan. Making matters worse, there is risingresistance to melarsoprol, the only widely avail-able drug for CNS involvement in African trypa-nosomiasis. Nash15 and Willet16 provided verygood reviews of the complicated African trypa-nosomiasis problem. Briefly, the chief vectors ofTrypanosoma brucei gambiense, the cause ofthe Gambian form of sleeping sickness, areGlossina palpalis, G. fuscipes, and G. tachinoides.Cases of Gambian sleeping sickness occur inwestern and central Africa and are usually more
TSETSE FLIES
Adult Tsetse Fly
ImportanceVectors of sleeping sickness
DistributionTropical Africa
LesionSmall punctate hemorrhages unless
sensitive to saliva (in that case —itchy wheals)
Disease TransmissionAfrican trypanosomiasis
Key ReferenceWillet, K. C., Ann. Rev. Entomol., 8,
197, 1963
TreatmentSoothing and/or antiseptic lotions or
creams

181
Flies (Biting)
Figure 13Life cycle of Trypanosoma rhodesiense and gambiense(reprinted with permission of Macmillian Publishing Companyfrom ESSENTIALS OF MEDICAL PARASITOLOGY by Thomas J.Brooks, Jr., Copyright (c) 1963 Thomas J. Brooks, Jr.).

182
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 14Side view of tsetse fly head (from: U.S. Navy Laboratory Guide to Medical Entomology).
chronic. In eastern Africa, the Rhodesian (or eastern) form, which is virulent and rapidlyprogressive, is caused by T. brucei rhodesiense. The primary vectors of the Rhodesianform are G. morsitans, G. swynnertoni, and G. pallidipes. The eastern form is commonlycontracted by travelers on game safaris or eco-vacations. Other than the possibility forsleeping sickness transmission, the bites of tsetse flies are of minor consequence.However, some individuals become sensitized to the saliva, and subsequent bitesproduce welts.
B. General Description
Tsetse flies are 7 to 13 mm long and yellow, brown, or black. They fold their wingsscissorlike over their back at rest, and this, along with other body features, makes themappear wasplike or honey beelike. The arista arising from the short, three-jointedantennae has rays that are branched bilaterally (Figure 14). Tsetse flies have a long,slender proboscis that is held out in front of the fly at rest. The discal cell (first M) lookslike a meat cleaver or hatchet (Figure 15).
C. Geographic Distribution
Tsetse flies are generally confined to tropical Africa between 15° N and 20° S latitude.Glossina morsitans is a bush species found in wooded areas and brush country ineastern Africa. In western and central Africa, where members of the G. palpalis groupare the principal vectors, the flies are predominantly found near the specializedvegetation lining the banks of streams, rivers, and lakes.
D. Biology/Behavior
Tsetse flies feed on a wide variety of mammals and a few reptiles; people are not theirpreferred hosts. Both sexes feed on blood and bite during the day. Tsetse flies have alife span of about 3 months (less for males), and females give birth to full-grown larvae

183
Flies (Biting)
Figure 15Adult tsetse fly (from: USDA Yearbook of Agriculture, 1952).
on dry and loose soil in places like thickets and sandy beaches. The larvae burrow a fewcentimeters into the substrate and pupate. The pupal stage lasts 2 weeks to a month, afterwhich the adult fly emerges to continue the life cycle.
E. Treatment of Bites
Tsetse fly bites are generally self-limiting. Antiseptic and soothing lotions may relievepain and itching. Persons sensitive to tsetse fly bites may require antihistamine and/or other treatment to control the immune response. Persons bitten in endemic areasfor sleeping sickness should be followed-up for development of the disease. There aretreatment strategies (quite complex) for African sleeping sickness. For information,contact the Parasitic Disease Drug Service, Centers for Disease Control and Prevention,U.S. Public Health Service, Atlanta, Georgia, telephone 404-639-3670.
REFERENCES1. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,
Macmillan, New York, 1979, chap. 9.
2. Nelson, G. S., Onchocerciasis, Adv. Parasitol., 8, 173, 1970.
3. 3rd Rep. WHO Expert Committee on Onchocerciasis, WHO Tech. Rep. Ser. No. 752,World Health Organization, Geneva, 1987.
4. Hopla, C. E., The ecology of tularemia, Adv. Vet. Sci. Parasitol., 18, 25, 1974.
5. McDowell, J. W., Scott, H. G., and Stojanovich, C. J., Tularemia, U.S.P.H.S. (CDC) TrainingGuide, United States Public Health Service, Washington, DC, 1964.
6. Pinder, M., Loa loa — a neglected filaria, Parasitol. Today, 4, 279, 1988.
7. Caubere, P. and Noireau, F., Effect of attraction factors on sampling of Chrysops silaceaand C. dimidiata, vectors of Loa loa filariasis, J. Med. Entomol., 28, 263, 1991.

184
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
8. Lillie, T. H., Kline, D. L., and Hall, D. W., Diel and seasonal activity of Culicoides spp.near Yankeetown Florida, monitored with a vehicle-mounted insect trap, J. Med. Entomol.,24, 503, 1987.
9. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 9.
10. Schreck, C. E. and Kline, D. L., Repellency determinations of four commercial productsagainst six species of ceratopogonid biting midges, J. Am. Mosq. Contr. Assoc., 41, 7, 1981.
11. Furner, B. B., Cutaneous leishmaniasis in Texas: report of a case and review of theliterature, J. Am. Acad. Dermatol., 23, 368, 1990.
12. Grimaldi, G. Jr., Tesh, R. B., and McMahon-Pratt, G., A review of the geographicdistribution and epidemiology of leishmaniasis in the New World, Am. J. Trop. Med. Hyg.,41, 687, 1989.
13. McHugh, C. P., Grogl, M., and Kerr, S. F., Isolation of Leishmania mexicana from Neotomamicropus collected in Texas, J. Parasitol., 76, 741, 1990.
14. Newson, H. D., Arthropod problems in recreational areas, Ann. Rev. Entomol., 22, 333,1977.
15. Nash, T. A. M., A review of the African trypanosomiasis problem, Trop. Dis. Bull., 57, 973,1960.
16. Willet, K. C., African trypanosomiasis, Ann. Rev. Entomol., 8, 197, 1963.

185
Flies (Nonbiting)
CHAPTER 20
FLIES (NONBITING)
TABLE OF CONTENTS
I. House and Other Filth Flies ...........................................................................186A. General and Medical Importance ..............................................................186B. General Description ....................................................................................186C. Geographic Distribution .............................................................................188D. Biology/Behavior .........................................................................................188E. Treatment of Infestation .............................................................................189
II. Eye Gnats .........................................................................................................190A. General and Medical Importance ..............................................................190B. General Description ....................................................................................190C. Geographic Distribution .............................................................................190D. Biology/Behavior .........................................................................................190E. Treatment of Infestation .............................................................................190
III. Nonbiting Midges .............................................................................................191A. General and Medical Importance ..............................................................191B. General Description ....................................................................................191C. Geographic Distribution .............................................................................191D. Biology/Behavior .........................................................................................192E. Treatment .....................................................................................................192
References ......................................................................................................................193

186
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
FILTH FLIES
Adult House Fly, Musca domestica
ImportanceNuisance; contamination; myiasis
DistributionNumerous species worldwide
LesionNon-biting, no lesion
Disease TransmissionSeveral agents mechanically
Key ReferenceB. Greenberg’s Two Vol. Set on Flies and
Disease, Princeton University Press,1971
I. HOUSE AND OTHER FILTHFLIES
A. General and Medical Importance
The term “filth flies” refers to members of thefamilies Muscidae, Sarcophagidae, and Calli-phoridae, which are domestic nonbiting fliescommonly seen in/around human dwellings.Although other species or groups could beconsidered “filth flies,” this topic will be re-stricted to those fly families (above) represent-ing the house flies, flesh flies, and blow flies.These flies do not bite, but are medically impor-tant in the mechanical transmission of diseaseagents from feces or dead animals to foodstuffsor food preparation areas. Throughout the world,these flies serve as carriers of organisms causingdiseases such as typhoid, diarrhea, bacillaryamoebic dysentery, cholera, giardiasis, pinworm,and tapeworm. They may spread these agentsvia their mouthparts, body hairs, or sticky padsof their feet, as well as through their vomitus orfeces.1 The egglaying habits of these insectsmay also lead to another human malady, myia-sis, which is the infestation of people by themaggots of flies (see Chapter 6).
B. General Description
House flies are about 5 to 8 mm long, with adull gray thorax and abdomen (not shiny). Thethorax has four longitudinal dark stripes (Figure1). Mature house fly larvae are 10 to 13 mm longand usually creamy white in color (Figure 2).Overall, the larvae have a conical shape withtwo dark-colored mouth hooks at the narrowend and two oval spiracular plates at the broadposterior end. The three sinuous slits in thespiracular plate are diagnostic features for thisspecies (Figure 1).
Flesh flies look like house flies but are gen-erally larger (11 to 13 mm long); they have threedark longitudinal stripes on their thorax, a check-erboard pattern of gray on the abdomen, andsometimes a reddish-brown tip on the abdomen(Figure 3). The larvae of flesh flies are similar tothose of house flies, except they have straightspiracular slits and often an incomplete ringaround the spiracular plate (Figure 3).

187
Flies (Nonbiting)
Figure 1Adult (left) and larval (right) house fly (from: U.S. DHHS (CDC) Publ. No. 83–8297).
Figure 2House fly larva (maggot), showing relative size.
Figure 3Adult (left) and larval (right) flesh fly (redrawn from: USDA, ARS, Agri. Hndbk No. 655, Feb.1991).

188
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Blow flies (also known as green or bluebottle flies) are about the same size as fleshflies, although some of the bluebottle flies (genus Calliphora) are larger and morerobust (Figure 4). Blow flies, with the exception of the cluster fly, are metallic bronze,green, black, purplish, or blue colored. They are the commonly encountered “greenflies” seen on flowers, dead animals, and feces, or occasionally indoors. Blow flymaggots resemble both house fly and flesh fly maggots but have straight spiracular slitsand most often a complete sclerotized ring around the spiracular plate (Figure 4).
C. Geographic Distribution
House flies, Musca domestica, occur worldwide in association with human dwellings.There are numerous blow fly species occurring over most regions of the world.Phaenicia sericata is a very common blow fly that is cosmopolitan in distribution.Calliphora vicina is one of the most common bluebottle species in Europe and NorthAmerica. Various species of flesh flies also occur worldwide. One of the most commonis Sarcophaga haemorrhoidalis, which is virtually worldwide in distribution andcommon in the U.S.
D. Biology/Behavior
Like all Diptera, these flies exhibit a complete life cycle, having egg, larva, pupa, andadult stages (Figure 5). All three filth fly groups discussed in this section have similarbiologies. Females lay their eggs, singly or in clusters, on or adjacent to an appropriatemedium for larval development. However, flesh fly females deposit living larvae ratherthan eggs. One to a few days later the eggs hatch and the first-stage larvae emerge and
Figure 4Adult (left) and larval (right) blow fly (from: U.S. Navy Laboratory Guide to Medical Entomology).

189
Flies (Nonbiting)
enter the food source where they feed and develop. Since the outer skin of a larva isnonliving and cannot grow, this skin (exoskeleton) must be periodically shed as thelarva grows. Molting occurs three times in these filth fly families. Eventually, larvalgrowth is completed and a pupa is formed inside the last larval skin. The larval growthperiod ranges from 2 days to 3 weeks depending upon temperature, and the pupalstage takes a similar length of time. The entire house fly life cycle can occur in 8 to10 days under summer conditions. Emerging adults are active, moving from oneattractant to another throughout most of the daylight hours. House flies are stronglyattracted to feces, decaying organic material, and foodstuffs. Garbage and pet feces arealmost always the important breeding sources of house fly problems in urban settings.Flesh flies breed in decaying meat or animal excretia. Most blow flies lay their eggs onanimal carcasses, and the developing maggots quickly dispose of the carrion. However,some blow fly species breed in dog manure or decaying organic matter. The entireblow fly life cycle requires 9 to 25 days or more.
E. Treatment of Infestation
Filth flies are best controlled by a combination of good sanitation, mechanicalexclusion, ultraviolet light traps, and chemical control (when necessary). Good sani-tation includes emptying and steam-cleaning dumpsters on a regular schedule andotherwise eliminating breeding sites. Mechanical exclusion methods include air curtainsand properly fitted doors and screens. Ultraviolet light traps (some electrocute the flies,others stun them and trap them on glue boards) work well indoors, and the newermodels are quite safe. Insecticidal treatments are best performed by competent pestcontrol operators.
Figure 5Life cycle of the house fly (from: U.S. DHHS (CDC) Publ. No. 83–8297).

190
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
ImportanceMechanical disease transmission
DistributionNumerous species almost worldwide
LesionNonbiting; sometimes cause minute
scratch lesions on eyeball
Disease TransmissionYaws and pinkeye
Key ReferenceB. Greenberg’s Two Vol. Set on Flies and
Disease, Princeton University Press,1971
EYE GNATS
Figure 6Typical eye gnat (from: U.S. DHHS (CDC) Publ.No. 83–8297).
II. EYE GNATSA. General and Medical Importance
Members of the fly family Chloropidae are vari-ously known as eye gnats, grass flies, eye flies,and fruit flies (although other flies are the truefruit flies). Members of the genus Hippelates aretroublesome pests that are strongly attracted tothe eyes of humans and other animals wherethey feed on the fluids of the eye surface andtear canal. Other species are attracted to serousdischarges from sores, as well as excrement.They do not bite but they do have spongingmouthparts that are “spined”; these spines maycause eye irritation.2 The lesions (minutescratches on the eyeball) that result from thesespines are thought to be entry points for diseaseagents such as that of pinkeye and yaws.
B. General Description
These flies are small, bare flies about 2 mm longthat are often shiny black (Figure 6). Most Hip-pelates eye gnats have a large, black, curvedspur on the hind tibia. Their antennae are shortwith bare aristae. The gnats are frequently seenon dogs around the eyes and anal–genital area.
C. Geographic Distribution
This is a large and widespread group composedof hundreds of species; numerous species occuralmost worldwide.
D. Biology/Behavior
Eye gnats are common in agricultural areas,meadows, and other places where there is con-siderable grass. Larvae of most species feed ingrass stems, decaying vegetation, and excre-ment. Hippelates larvae can be found feedingon decaying organic matter or roots of plants inthe soil. Eggs hatch in about 3 days, the larvalstage lasts about 2 weeks, and the pupal stagefollows — adults emerge a few days later.
E. Treatment of Infestation
Since eye gnats do not actually bite, treatmentinvolves only the incidental diseases transmit-

191
Flies (Nonbiting)
NONBITINGMIDGES
Adult Nonbiting Midges, Chironomidae
ImportanceMassive emergences; airborne body
parts induce hypersensitive RXNS insome people
DistributionNumerous species almost worldwide
Disease TransmissionNone
Key ReferenceGrodhaus, G., Calif. Vector Views, 22,
71, 1975
TreatmentSensitive persons can avoid infested
areas in spring and summer; stayindoors during emergences; weardust masks when outdoors, seeallergist for treatment
ted, e.g., pinkeye and yaws. Avoidance of thegnats is important. Most insect repellents workreasonably well in minimizing their nuisancepresence around humans (although it should beemphasized that repellents should not be sprayedon or near the eyes).
III. NONBITING MIDGESA. General and Medical Importance
Nonbiting midges (Chironomidae) are oftenconfused with mosquitoes, but they are innocu-ous insects except during times when they areunusually abundant. They do not bite, butmassive emergences may produce traffic haz-ards, bother livestock, and cover residences.3,4
Sometimes it is difficult to keep swarms out ofthe eyes or to avoid inhaling them.
B. General Description
Midges are delicate insects, approximately thesame size as mosquitoes, but they have a shortproboscis that is not adapted for piercing (Fig-ure 7). They have six-segmented antennae (pos-sibly more, but no less), and in the males theantennae are plumose. Chironomids often havetiny hairs on the wing veins and on the mem-brane of the wing itself. Adult specimens arevariously colored (usually brown or gray) andrange in size from barely visible to mosquito-sized. Chironomids hold their wings roof-likeover the abdomen at rest. They form hugeswarms near water.
Chironomid larvae are wormlike, having ahardened shell-like head capsule. Mature larvaehave 12 body segments and prolegs on theirfirst and last body segments. Some chironomidlarvae are red and are frequently called “blood-worms.”
C. Geographic Distribution
Numerous species of chironomids occur world-wide. Three notorious pest species includeTanytarsus lewisi in northeastern Africa,Glyptotendipes paripes in the southeastern U.S.,and Chironomus decorus in the northeasternU.S.

192
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
D. Biology/Behavior
Midges are extremely abundant around standing water (especially freshwaterponds, lakes, and reservoirs), since the larvae are aquatic. The life stages ofchironomids include the egg, four larval instars, pupa, and adult. Depending uponthe species and time of year, development from egg to adult is 1 month to 2 years.The larva is the only feeding stage; larval food items are varied depending uponspecies, and include such items as small particulate organic matter, plants, or evenother insects or tiny crustaceans. The larvae generally inhabit the bottom sedimentsin water sources. Most adult midges rest during daytime and fly at night. They areattracted to light in great numbers and sometimes huge swarms hover in the air,producing a humming sound.
E. Treatment
Persons sensitive to airborne chironomid body parts or emanations can sometimesmove away from the source of the chironomid midges, e.g., a large freshwaterreservoir. Efficient air conditioning can help keep the indoor environment free ofallergen. Sensitive persons may also gain protection from the offending particles bywearing a dust or particle mask when outdoors during chironomid emergences. Inaddition, sensitive persons should consult an allergist for treatment.
Figure 7Adult female (A), male (B), and larval (C) nonbiting midge (Chironomidae).

193
Flies (Nonbiting)
REFERENCES1. Frazier, C. A. and Brown, F. K., Insects and Allergy and What To Do About Them,
University of Oklahoma Press, Norman, OK, 1980, 107.
2. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, 251.
3. Bay, E. C., Anderson, L. D., and Sugarman, J., The abatement of a chironomid nuisanceon the highways at Lancaster, California, Calif. Vector Views, 12, 29, 1965.
4. Beck, E. C. and Beck, W. M. Jr., The Chironomidae of Florida. II. The nuisance species,Fla. Entomol., 52, 1, 1969.


195
Flies (Which May Cause Myiasis)
CHAPTER 21
FLIES (WHICH MAYCAUSE MYIASIS)
TABLE OF CONTENTS
I. Human Bot Flies ..............................................................................................196A. General and Medical Importance ..............................................................196B. General Description ....................................................................................197C. Geographic Distribution .............................................................................197D. Biology/Behavior .........................................................................................197E. Treatment of Infestation .............................................................................197
II. Screwworm Flies ..............................................................................................198A. General and Medical Importance ..............................................................198B. General Description ....................................................................................199C. Geographic Distribution .............................................................................199D. Biology/Behavior .........................................................................................199E. Treatment .....................................................................................................200
III. Congo Floor Maggot ........................................................................................200A. General and Medical Importance ..............................................................200B. General Description ....................................................................................201C. Geographic Distribution .............................................................................201D. Biology/Behavior .........................................................................................201E. Treatment of Bites .......................................................................................201
IV. Tumbu or Mango Fly ......................................................................................202A. General and Medical Importance ..............................................................202B. General Description ....................................................................................202C. Geographic Distribution .............................................................................202D. Biology/Behavior .........................................................................................202E. Treatment of Infestation .............................................................................204
V. Sarcophagid Flies (Wohlfahrtia spp.) ............................................................204A. General and Medical Importance ..............................................................204

196
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
B. General Description ....................................................................................204C. Geographic Distribution .............................................................................205D. Biology/Behavior .........................................................................................205E. Treatment .....................................................................................................205
VI. Other Flies Which May Occasionally Cause Myiasis ....................................206A. General and Medical Importance ..............................................................206B. General Description ....................................................................................210C. Geographic Distribution .............................................................................213D. Biology/Behavior .........................................................................................213E. Treatment of Infestation .............................................................................213
References ......................................................................................................................214
I. HUMAN BOT FLIESA. General and Medical Importance
Some fly larvae develop in living flesh (also see Chapter 6); the human bot fly is oneof them. This fly, Dermatobia hominis (Figure 1), is a parasite of humans, cattle, swine,cats, dogs, horses, sheep, other mammals, and a few birds in Mexico and Central andSouth America.1,2 The larvae (Figure 2) burrow in the host’s tissues, feeding andeventually emerging to drop to the ground and pupate. In people, the larvae have beenrecovered from the head, arms, back, abdomen, buttocks, thighs, and axilla. Humaninfestation is often characterized by painful, discharging cutaneous swellings on thebody. The condition is rarely fatal but can be in very young children (<5 years old);the larvae infesting the scalp penetrate the incompletely ossified skull and enter thebrain.3 Although the parasite does not occur in the U.S., cases are occasionally seenin travelers to endemic areas. One such case was reported from Ohio in which a localphysician submitted a second-stage larva to the Ohio Department of Health foridentification.4 The larva had been removed from a patient who had recently returnedfrom Brazil. The Mississippi Department of Health has recently been involved in twocases in people returning from Belize.
Figure 1Human bot fly: first-stage larva (A), second-stage larva (B), third-stage larva (C), and adult (D)(from: USDA Misc. Publ. No. 631, 1947).

197
Flies (Which May Cause Myiasis)
HUMAN BOT FLY
Human Bot Fly, Dermatobia hominis
ImportanceLarvae cause myiasis in humans
DistributionMexico, Central and South America
LesionSuperficial, painful swelling with central
opening
Disease TransmissionNone
Key ReferenceSancho, E., Parasitol. Today, 4, 242,
1988
TreatmentExcision of larvae; bacon therapy. JAMA
270, 2087, 1993.
B. General Description
Dermatobia hominis resembles a bluebottle fly(a large bluish member of the family Calli-phoridae), is approximately 15 mm long, has ayellowish or brown head and legs, and has aplumose arista (a bristle-like branch off of theantennae).
C. Geographic Distribution
Dermatobia hominis does not occur in the U.S.but is common in parts of Mexico and Centraland South America. Sancho5 reports its distribu-tion from the northern provinces of Mexico(Taumalipas, bordering southern Texas) to thenorthern Argentine provinces of Misiones, TresRios, Corrientes, and Formosa — roughly be-tween latitudes 25°N and 32°S. Vacationers mayacquire this parasite in tropical America andreturn home before completion of maggot de-velopment.
D. Biology/Behavior
Human bot flies have a unique and almostunbelievable life cycle. The adult flies catchvarious bloodsucking flies (such as mosquitoes)and attach eggs to their sides with a quick-drying glue. These carrier flies later feed onhumans (or other hosts) at which time thenewly hatched bot fly larvae penetrate the hostskin. The larvae feed inside a subdermal cavityof the host for 5 to 10 weeks. For respiration,they maintain a hole open to the external air.When mature, the larvae emerge, drop to thesoil, and pupate. Interestingly, the fully fedlarvae leave their hosts during the night or earlymorning, never during the afternoon, presum-ably to avoid desiccation.5 After a month or so,the adult flies emerge to mate and begin the lifecycle over.
E. Treatment of Infestation
Alexander6 said attempts to express D. hominislarvae by pressure on or around the lesion arefruitless and painful. The recommended thera-peutic procedure for all forms of myiais is direct

198
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
removal of the maggots and treatment to prevent/control secondary infection. Second-ary infection may result if the larva is ruptured or killed within its cavity and notremoved. A traditional Central American remedy is occlusion of the punctum (breathinghole in the skin) with raw meat or pork, a treatment sometimes called “bacon therapy”.Apparently, the larva will almost always migrate into the applied piece of meat. AnAmerican group modified this approach and was able to successfully extract 10 larvaeafter 3 hours of bacon therapy.6a
II. SCREWWORM FLIESA. General and Medical Importance
Two important species of screwworm flies that feed in living tissues are Chrysomyabezziana, the Old World screwworm, and Cochliomyia hominivorax, the New Worldscrewworm. Larvae of these calliphorid flies are obligate parasites of living flesh(humans and domestic and wild mammals), feeding during their entire larval periodinside a host. Screwworm infestation causes damage to tissues that is compounded bytwo factors: (1) screwworms may travel through living tissues and not just remainsubdermal like the Tumbu fly or others, and (2) eggs are laid in batches of 100 to 400resulting in multiple infestation within the host.
Female flies most often oviposit on or near a wound; however, human infestationshave resulted from the flies ovipositing just inside the nostril while a person sleeps inthe daytime, especially if there is a nasal discharge. Upon hatching, the larvae beginfeeding, causing extensive destruction of tissue and a bloody discharge. Tissues aroundthe lesion become swollen and pockets may be eaten out beneath the skin. Infestedpersons may die from tissue destruction. Human cases are uncommon but do occurin areas where screwworm infestations occur in livestock. In 1935 there were 55
Figure 2Human bot fly third-stage larva.

199
Flies (Which May Cause Myiasis)
SCREWWORMFLIES
Adult Old World Screwworm Fly,Chrysomya bezziana
ImportanceHuman myiasis — sometimes fatal
DistributionCentral and South America; Oriental and
Afrotropical regions; part of S. Pacificregion
LesionPocketlike sinuses in tissues
Disease TransmissionGenerally none
Key ReferenceJames, M. T., USDA Misc Publ #631,
1947
TreatmentRemoval of larvae by irrigation or
surgical means
reported cases during a large outbreak in live-stock in Texas.7 Since the New World screw-worm fly has been eradicated from the U.S.,human cases are rare and due entirely to for-eign travel. An imported case of traumatic screw-worm myiasis was reported in a soldier woundedduring military action in Panama.8 Cases ofmyiasis caused from the Old World screwwormfly are common in the Orient but relatively rarein Africa.9
B. General Description
Adult Chrysomya bezziana are green to blue andhave the base of the stem vein (radius) ciliateabove, but they have at most only two narrowlongitudinal thoracic stripes (Figure 3A). Theyare approximately 8 to 12 mm long. Full grownC. bezziana larvae have the usual 12 segmentswith belts of dark spines encircling them (Figure3B). Adult C. hominivorax are bluish-green,medium-sized flies with a yellowish-orange faceand three dark stripes on the thorax (Figure 3C).The base of the stem vein (radius) bears a rowof bristle-like hairs on the dorsal side. Full-grownlarvae are about 2 cm long, appear pinkish incolor, and have prominent rings of spines aroundthe body (Figure 3D).
C. Geographic Distribution
The distribution of the New World screwwormonce extended from the U.S. to southern Brazil,but it now has been limited to South and CentralAmerica due to an eradication program involvingthe sterile male release technique. The Old Worldscrewworm occurs in the Afrotropical and Orien-tal regions extending south into Indonesia, thePhilippines, and New Guinea (but not Australia).
D. Biology/Behavior
Females of both screwworm species are attractedto wounds in mammals and lay eggs at the edgeof the wounds. Eggs are deposited in batches of150 to 500 and hatch approximately 15 h later.The larvae feed while embedded in living tissue;sometimes, however, the peritremes (the plate

200
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
surrounding the breathing tubes) are visible. The larvae emerge from the host asprepupae 4 to 7 days later and fall to the ground where they pupate for a week or more.The entire life cycle from egg to egg takes about 24 days under optimum conditions.Adult screwworm flies are active all year round but only fly during daylight.
E. Treatment
Treatment of screwworm fly myiasis involves removal of the larvae. This may be donein several ways, but often there is surgical exploration and removal of the larvae underlocal anesthesia.10 Alexander6 advocated irrigation with chloroform or ether under localor general anesthesia. Infestation of the nose, eyes, ears, and other areas may requiresurgery if larvae cannot be removed via natural orifices. Since screwworm flies lay eggsin batches, there could be tens or even hundreds of maggots in a wound.
III. CONGO FLOOR MAGGOTA. General and Medical Importance
The Congo floor maggot, Auchmeromyia senegalensis (=luteola), is a blow fly. Itslarvae suck human blood while their hosts are sleeping on the floor in huts or otherdilapidated infested dwellings. While this blood feeding behavior may not actually bemyiasis in the strictest sense, this species will be discussed in this section. Congo floormaggots are not known to transmit disease agents. The bite of the larva is generally
Figure 3Screwworm flies: Adult female Chrysomya bezziana (A), larval C. bezziana (B), adult femaleCochliomyia hominivorax (C), and larval C. hominivorax (D) (from: USDA Misc. Publ. No. 631,1947).

201
Flies (Which May Cause Myiasis)
CONGO FLOORMAGGOT
ImportanceNocturnal blood feeding maggots;
nuisance
DistributionSub-Sahara Africa; Cape Verde Islands
LesionGenerally trivial pin prick lesions
Disease TransmissionNone
Key ReferenceJames, M. T., USDA Misc Publ #631,
1947
TreatmentGenerally none needed
Figure 5Auchmeromyia senegalensis, abdomen of maleshowing exceptionally long second segment (A);larval stage (B) (from: USDA Misc. Publ. No.631, 1947).
Figure 4Auchmeromyia senegalensis.
felt as a pin prick, but sensitive persons mayexperience pain, swelling, and irritation.
B. General Description
Adult A. senegalensis are 8 to 13 mm long,yellow-brown flies. They are similar in appear-ance to the Tumbu fly (next section) but havethe second visible abdominal segment longerthan the third (Figures 4 and 5). Males of theCongo floor maggot fly have widely separatedeyes. Full-grown larvae are up to 18 mm long.
C. Geographic Distribution
The Congo floor maggot is an African calli-phorid occurring throughout Africa south ofthe Sahara Desert and in the Cape VerdeIslands.
D. Biology/Behavior
Congo floor maggot larvae occur in the earthenfloor of huts or other similar dry soil situations.They feed periodically at night by suckingblood from individuals sleeping on the ground.The larvae take about 20 min to feed on theirhost then drop to the ground. They may feeddaily if given the opportunity. Larvae go throughthree stages, which may include 6 to 20 bloodfeedings. They eventually pupate in the soilfor about 2 weeks, after which the adultsemerge. The entire life cycle is approximately10 weeks under optimal conditions, and de-velopment continues year round with no dia-pause. The adults feed on feces, fallen fruit,and other fermenting materials. The adultsmate and then the female lays her eggs in dry,dusty, or sandy soil, often in a hut. This fly hasalso been reported to be associated with war-thogs, aardvarks, and hyenas.
E. Treatment of Bites
Blood feedings by the Congo floor maggot aregenerally not serious but may cause consider-able discomfort. Since the maggots cannotclimb vertically, avoidance is possible by sleep-ing in beds at least 10 cm off the ground.

202
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
TUMBU FLY
ImportanceFuruncular type of myiasis
DistributionTropical Africa
LesionRed or shiny nodules on skin; lesion
very similar to that caused byDermatobia hominis
Disease TransmissionNone
Key ReferenceJames, M. T., USDA Misc Publ #631,
1947
TreatmentDirect removal of larvae
Figure 6Cordylobia anthropophaga adult female.
IV. TUMBU OR MANGO FLYA. General and Medical Importance
The Tumbu fly, Cordylobia anthropophaga, is ablow fly (family Calliphoridae) whose larvaecan burrow into human subcutaneous tissuesproducing a furuncular type of myiasis (see alsoChapter 6). The lesion resembles a boil andoften has a serous exudate. The first symptomis a slight itching, which occurs in the first dayor two of the infestation. In a few days a reddishpapule develops, and then the typical boil-likelesion develops. With multiple infections thelymph glands may become enlarged and fevermay be present.11 Children are most commonlyaffected, and lesions usually occur on areas ofthe body normally covered with clothing sincethe adult flies tend to oviposit on soiled cloth-ing. In an imported case seen in Maine, lesionsappearing as boils approximately 25 mm in diam-eter contained second-stage Tumbu fly larvae.11
B. General Description
The adult Tumbu fly is similar in appearance tothe adult of the Congo floor maggot as well asother flies in related genera. Accordingly, it isdifficult to identify precisely. The body of bothsexes is yellow-brown and about 6 to 12 mmlong (Figure 6). The second and third visibleabdominal segments are of equal length. Malesof this species have eyes nearly contiguous (Congofloor maggot males have eyes widely separated).Full-grown larvae are 13 to 15 mm long.
C. Geographic Distribution
Tumbu flies occur in the Afrotropical region.
D. Biology/Behavior
Tumbu flies cause cutaneous myiasis in severalmammalian hosts, including humans. Dogs arethe most common domestic hosts, and severalspecies of wild rats are the preferred field hosts.The adult flies feed on plant juices, rotting plantor animal matter, and feces. They are mostactive in the early morning (7:00 to 9:00) andlate afternoon (4:00 to 6:00). Adult flies lay theireggs in shady areas of sand contaminated with

203
Flies (Which May Cause Myiasis)
CASE HISTORY
MAGGOT IN URINARY TRACT
A large regional hospital sent in a fly maggot supposedly recovered from a urine sample(Figure 1). Lab personnel apparently did not think such an event was possible. “Was it reallya maggot?” they asked. “What should we do?” “Are there more in the urinary tract?” Uponexamination, the maggot was identified as a syrphid fly larva. Although not usually involvedin urinary myiasis, the species was from a group of flies known to occasionally cause otherforms of myiasis in people. Accordingly, the case was considered urinary tract myiasis andthe physicians acted accordingly.
Comment: The maggots are generally expelled in cases of accidental urinary myiasis bynoninvasive species. Therefore, specific treatment may not be needed.
(Adapted from Lab. Med. 25, 369, 1994, Copyright 1994, by the American Society ofClinical Pathologists. With permission.)
Figure 1Syrphid fly larva recovered from urine sample; suspected case of accidental urinary myiasis.
excrement or sometimes on soiled clothing. Improperly washed diapers placed in theshade to dry are a common oviposition site. The flies do not oviposit directly on theskin or hairs of a host. Eggs hatch and the larvae remain buried in the dirt or sand untila host approaches. In the presence of a host the larvae actively search for and get onthe host. Penetration of the skin is rapid and ordinarily unnoticeable. The larvadevelops in the subcutaneous tissues for about 10 days. As the larva develops the lesionbegins to look boil-like and a clear fluid, occasionally stained with blood or larval feces,may ooze from the boil. Larvae (now prepupae) then exit the lesion and pupate in theground. About 10 to 14 days later the adults emerge, mate, and begin laying new batchesof eggs. The adult female only lives 2 to 3 weeks. People are most commonlyparasitized during the rainy season, but fly development continues year round.

204
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
WOHLFAHRTIAFLIES
Figure 8Adult female Wohlfahrtia magnifica (A) and W.vigil (B) (from: USDA Misc. Publ. No. 631, 1947).
ImportanceW. magnifica — myiasis similar to
screwworm fly; W. vigil — furuncularmyiasis
DistributionW. magnifica — southern Palearctic; W.
vigil — northern U.S. and Canada
LesionW. magnifica — deep lesions in the
nose or in existing wounds; W. vigil— papule- or pustule-looking lesionscontaining larvae
Disease TransmissionNone
Key ReferenceJames, M. T., USDA Misc Publ #631,
1947
TreatmentRemoval of the larvae by expression,
direct picking, and/or by irrigation
Figure 7Comparison of Wohlfahrtia (A)and Sarcophaga (B) abdomens.
E. Treatment of Infestation
As in other types of myiasis, the only knowntherapeutic procedure, other than applying lo-cal palliatives, is direct removal of the maggots(surgically if necessary) and treatment to pre-vent/control secondary infection. Service11a saysa standard method for Tumbu larvae removal isto cover the small hole in the swelling withmedicinal liquid paraffin. This prevents the larvafrom breathing through its posterior spiraclesand forces it to wriggle a little further out of theswelling to protrude the spiracles. In doing so,it lubricates the pocket (in the skin) and thelarva can then be extracted by gently pressingaround the swelling.
V. SARCOPHAGID FLIES(WOHLFAHRTIA SPP.)A. General and Medical Importance
Two important sarcophagid flies that causemyiasis are Wohlfahrtia magnifica and W. vigil.Wohlfahrtia magnifica larvae produce trau-matic myiasis throughout their host’s tissues —much like a screwworm fly. Human fatalitiesresulting from this species have been reported.2
Wohlfahrtia vigil larvae are not as invasive;they are usually limited to dermal tissues pro-ducing a furuncular or boil-like lesion.2
B. General Description
The Wohlfahrtia spp. look very similar to fleshfly adults (Sarcophaga), but instead of the check-erboard pattern on their abdomen they haveclearly defined spots (Figure 7). The abdomenof W. vigil is almost entirely black (Figure 8B).

205
Flies (Which May Cause Myiasis)
C. Geographic Distribution
Wohlfahrtia magnifica occurs in the southern Palearctic region. Wohlfahrtia vigiloccurs in northern North America, primarily Canada and the northern U.S.
D. Biology/Behavior
Wohlfahrtia magnifica is an obligatory parasite in the wounds and natural orifices ofwarm-blooded animals, including humans. It never develops in carrion or rottingmaterials. Females of both W. magnifica and W. vigil are larviparous, i.e., the adult flydeposits living larvae on potential hosts. Both tiny skin lesions (tick bite, scratch, etc.)and mucous membranes of natural orifices are used as entry points by the larvae. Thedeveloping larvae feed for 5 to 7 days within a host, after which they emerge, fall tothe ground, and pupate. W. vigil is also an obligatory parasite, but it rarely penetratesdeeper than dermal tissues. Dogs, cats, rodents, rabbits, mink, foxes, and humans arehosts of this pest. The larvae form a boil-like swelling under the skin with a circularopening through which the larva can be partially seen. After maturing, the larvaeemerge, drop to the ground, and pupate. Multiple lesions are common on patientsinfested with W. vigil, with the average number being 12 to 14.2
E. Treatment
Wohlfahrtia vigil infestations are relatively easy to treat, because the larvae are easily seenand removed. Unlike other forms of furuncular myiasis, expression seems easy anduncomplicated.6 Wohlfahrtia magnifica infestations are much more serious, since theyoften involve numerous, voraciously feeding larvae within the nose or in existing wounds.Irrigation and/or possible surgical exploration to remove the larvae will be needed.
VI. OTHER FLIES WHICH MAY OCCASIONALLYCAUSE MYIASIS
A. General and Medical Importance
Larvae of flies in the genus Cuterebra, often found in squirrels (called “wolves”) andrabbits may rarely parasitize humans, forming a warblelike dermal tumor.25, 26 In a casethe author recently consulted on (See Case History), a 3-year-old boy had two Cuterebralarvae — on his side and neck — forming boil-like lesions. Several health care providersexamined the boy and either diagnosed the lesions as boils or larval migrans (from doghookworm) since there were short migration trails visible in the skin. To everyone’ssurprise, one physician finally recognized the myiasis and expressed a larva from the necklesion.
Other flies may occasionally cause myiasis in humans (Figures 9 to 11) (see Chapter6). This behavior is termed facultative myiasis (see Color Figure 21-18). In some of thesecases the larvae enter living tissues after feeding in neglected, malodorous wounds. Inother cases, ports of entry include natural orifices such as the ears, urinary opening,or anus. Table 1 provides a list of some species occasionally involved in facultativemyiasis and notes on their biologies. Sometimes these fly larvae can be identified bylooking at the shape and pattern of the posterior spiracles (Figures 12 and 13).

206
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
CASE HISTORY
ANIMAL BOT FLY LARVA IN CHILD
A 3-year-old boy complained of being “stung” on his side and neck (approximately 3 cmunder the lower jaw bone) while watching television early one morning. His mother saidthat within 5 min, typical sting-like “welts” occurred at the places the child pointed out.Within a day or so, a line of vesicles extended away from the lesions — presumably wherethe larvae were migrating in the skin. The lesion on his side extended upward in a sinuousfashion about 10 cm, ending in a small papule. No further development occurred at the sidelesion (apparently the developing larva died). The larva on his neck migrated about 4 cmlaterally and began to enlarge. After about 14 days the dermal tumor was inflammed andcontained an opening in the center about 3 mm in diameter, apparently through which thelarva obtained air. The child cried often and complained of severe pain. Despite numeroustrips to physicians, the myiasis was not diagnosed until almost 4 weeks after the initial“stinging incident.” An ER physician expressed the larva, which was ultimately forwardedto the Health Department for identification. Upon examination, the specimen (Figure 1)appeared to be a second-stage larva of a fly in the genus Cuterebra (the rabbit and rodentbot flies). Figure 2 is a drawing of the posterior spiracular slits of the specimen.
Figure 1Cuterebra fly larva removed from neck of 3-year-old child.

207
Flies (Which May Cause Myiasis)
Comment: These fly larvae commonly infest squirrels, chipmunks, other wild rodents, andrabbits. Occasionally, they also infest dogs and cats. Human infestations are extremely rare.Although most reports in the scientific literature say that the eggs or larvae are not depositeddirectly on the hosts (being laid instead in pathways, dens, etc. of the hosts), there isevidence of direct deposition in this case. Physicians should carefully examine boils orother skin lesions for fly larvae, especially if the lesion is refractory to standard treatments.
Figure 2Drawing of posterior spiracles from Cuterebralarva infesting child.
Figure 9Several representative blow flies. Theyare usually shiny blue or green incolor.

208
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Tab
le 1
Som
e F
ly S
pec
ies
No
t O
rdin
aril
y C
ausi
ng
My
iasi
s b
ut
May
Op
po
rtu
nis
tica
lly
be
Fo
un
d i
n L
ivin
g T
issu
es/H
ost
s
Type
of
Fly
Myi
asis
Fly
Spec
ies
Dis
trib
utio
nC
omm
ents
Ref
eren
ce
Uri
nary
Fann
ia c
anic
ular
isC
osm
opol
itan
Bre
eds
in a
nim
al f
eces
or
deca
ying
veg
etab
le m
atte
rJa
mes
2
F. s
cala
risC
osm
opol
itan
Foun
d ou
tdoo
rs m
ore
than
F.
cani
cula
ris;
also
kno
wn
asJa
mes
2
th
e la
trin
e fly
Mus
ca d
omes
tica
Cos
mop
olita
nB
reed
s in
ani
mal
fec
es,
garb
age,
etc
.M
usci
na s
tabu
lans
Cos
mop
olita
nB
reed
s in
ani
mal
fec
es a
nd d
ecay
ing
vege
tabl
e m
atte
rTe
icho
myz
a fu
sca
Nea
rly
cosm
opol
itan
Bre
eds
in e
xcre
men
t, se
wer
s, a
nd d
rain
sM
egas
elia
sca
laris
Nea
rly
cosm
opol
itan
Sing
h an
d R
ana12
Cut
aneo
usPh
aeni
cia
seric
ata
Cos
mop
olita
nV
ery
com
mon
sap
roph
agus
flie
s at
trac
ted
to f
resh
car
rion
And
erso
n an
d or
tra
umat
ic
Mag
nare
lli,10
G
reen
berg
,13 a
nd
Mer
ritt14
P. c
uprin
aaN
earc
ticB
reed
s in
gar
bage
and
dog
fec
esPh
orm
ia r
egin
aH
olar
ctic
One
of
the
mos
t nu
mer
ous
flies
in
the
sout
hern
U.S
.H
all15
and
Hal
l an
d
Tow
nsen
d16
Coc
hlio
myi
a m
acel
laria
Nea
rctic
and
Ver
y ab
unda
nt c
arri
on b
reed
erA
lexa
nder
6
ne
otro
pica
l re
gion
s

209
Flies (Which May Cause Myiasis)
Cal
lipho
ra v
icin
aH
olar
ctic
Act
ive
mos
tly i
n th
e co
ol-w
eath
er m
onth
s of
the
yea
rA
lexa
nder
6
Sarc
opha
gaN
earl
y co
smop
olita
nB
reed
s in
car
rion
and
exc
rem
ent
Jam
es2
ha
emor
rhoi
dalis
Chr
ysom
ya r
ufifa
cies
Ori
enta
l an
d
neot
ropi
cal
Her
met
ia il
luce
nsN
earl
y co
smop
olita
nA
dult
know
n as
bla
ck s
oldi
er f
lyA
dler
and
B
ranc
ato24
Cut
ereb
ra s
pp.
New
Wor
ldR
oden
t bo
tsR
ice
and
Dou
glas
25
Rec
tal
Eris
talis
ten
axC
osm
opol
itan;
mos
tLa
rvae
cal
led
rat
taile
d m
aggo
ts
com
mon
in
hola
rtic
F. s
cala
risC
osm
opol
itan
F. c
anic
ular
isC
osm
opol
itan
Mus
ca d
omes
tica
Cos
mop
olita
nG
odda
rd17
Mus
cina
sta
bula
nsC
osm
opol
itan
Aur
alPh
aeni
cia
seric
ata
Cos
mop
olita
nD
avie
s18 a
nd
Kel
ler
and
Kel
ler19
P. c
uprin
aaN
earc
ticG
odda
rd20
Sarc
opha
ga c
itelli
vora
Phor
mia
reg
ina
Hol
arct
icD
amsk
y et
al.21
aO
nly
mea
nin
g th
e N
earc
tic
form
her
e (=
P.
pal
lesc
ens
of S
ha
nn
on).

210
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 10Drone fly, Eristalis tenax, adult and larva; often reported as a cause of accidental or facultativemyiasis. (From: USDA, ARS, Agri. Hndbk. No 655, Feb. 1991.)
Figure 11Fly larvae frequently involved in urinary (facultative)myiasis. (From: USDA, ARS, Agri. Hndbk. No. 655, Feb.1991.)

211
Flies (Which May Cause Myiasis)
Figure 12Posterior spiracles of various fly larvae occasionally involved in myiasis: Mature muscoid fly larva(A), rear view of fly larva (B), Musca domestica (C), Musca sorbens (D), Musca crassirostris (E),Wohlfahrtia vigil (F), Muscina stabulans (G), Cynomyopsis cadaverina (H), Phaenicia cae-ruleiviridis (I), Phaenicia sericata (J), Chrysomya chloropyga (K), Chrysomya albiceps (L),Sarcophaga crassipalpis (M), Note: D, E, K, and L occur in the Old World only (adapted in partfrom: USDA Misc. Publ. No 631, 1947).
One of the most commonly implicated fly groups is the Calliphoridae (blow flies).Several species of blow flies, and especially Phaenicia sericata and Phormia regina,have been reported as causes of facultative myiasis in humans. The discussion belowwill be limited to those two species.
B. General Description
Phaenicia sericata is a typical-looking blow fly — shiny green or coppery green (Figure14A). Phormia regina, also called the black blow fly, is more slender and is olive-

212
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 13Posterior end of fly larva removed from the ear of a 4-month-old child. Note size and shapeof spiracular slits (photo courtesy Dr. Alan Causey, University of Mississippi Medical Center,Jackson, MS).
Figure 14Adult (A) and larval (B) Phaenicia sericata; adult (C) and larval (D) Phormia regina(from U.S. DHHS (CDC) Publ. No. 83–8297 and USDA Misc. Publ. No. 631, 1947).

213
Flies (Which May Cause Myiasis)
colored or nearly black (Figure 14C). The pubescence surrounding the anterior spiracleof P. regina is orange.
C. Geographic Distribution
Phaenicia sericata is nearly cosmopolitan in distribution and is probably the mostabundant species of Phaenicia in North America. Phormia regina is holarctic indistribution. Goddard and Lago23 found P. regina to be the most common blow fly inMississippi, with specimens encountered throughout the year (peak numbers occurringin April and September).
D. Biology/Behavior
The general life history of blow flies is included in the preceding section on nonbitingfilth flies. Other specific comments on these two species are presented here. Phaeniciasericata is a species that is quick to appear at fresh carrion, although it is also attractedto a wide range of decaying substances. In many cases, facultative myiasis cases seemto be the result of P. sericata being attracted to festering and malodorous wounds withsubsequent invasion of healthy human tissue. Phormia regina is very commonthroughout the U.S. during the warmer months (April to September). It also is abundantnear a wide variety of decaying substances, especially carrion.
E. Treatment of Infestation
Therapeutic measures for blow fly myiasis include removal of the maggots, surgicallyif necessary, and treatment for secondary bacterial and/or fungal infections should theyoccur.
CASE HISTORY
TRAUMATIC MYIASIS
On February 17, 2000 a physician from a local hospital submitted a vial of insect larvaefor identificaiton. The tiny, worm-like specimens had been removed from a middle-agewoman found lying in the woods with a large open wound in her scalp. Upon microscopicexamination, the larvae were found to be second stage blow fly (insect family Calli-phoridae) larvae.
Comment: This was a classic case of traumatic myiasis. It is not unusual for blow flies tolay eggs in wounds of people or animals, especially when the wound is neglected ormalodorous. In nature, these flies oviposit on dead and rotting carcasses, so one can seehow they might occasionally choose a festering wound on a livng animal. However, thisis still “accidental” or “opportunistic” myiasis and not purposeful, obligate myiasis.

214
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
REFERENCES1. Guimarães, J. H. and Papavero, N., A tentative annotated bibliography of Dermatobia
hominis, Arq. Zool., 14, 223, 1966.
2. James, M. T., The flies that cause myiasis in man, USDA Misc. Publ. No. 631, U.S.Department of Agriculture, Washington, D.C., 1947.
3. Rossi, M. A. and Zucoloto, S., Fatal cerebral myiasis by the tropical warble fly, Dermatobiahominis, Am. J. Trop. Med. Hyg., 22, 267, 1973.
4. Anon., Ohio Vector News, 10, March 1991.
5. Sancho, E., Dermatobia, the neotropical warble fly, Parasitol. Today, 4, 242, 1988.
6. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 8.
6a. Brewer, T.F., Wilson, M.E., Gonzales, E., and Felsenstein, D., Bacon therapy and furuncularmyiasis, J. Amer. Med. Assoc., 270, 2087, 1993.
7. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, chap. 13.
8. Mehr, Z., Powers, N. R., and Konkol, K. A., Myiasis in a wounded soldier returning fromPanama, J. Med. Entomol., 28, 553, 1991.
9. Zumpt, F., Myiasis in Man and Animals In The Old World, Butterworths, London, 1965, 118.
10. Anderson, J. F. and Magnarelli, L. A., Hospital-acquired myiasis, Asepsis, 6, 15, 1984.
11. Rice, P. L. and Gleason, N., Two cases of myiasis in the U.S. by the African Tumbu fly,Cordylobia anthropophaga, Am. J. Trop. Med. Hyg., 21, 62, 1972.
11a. Service, M. W., Medical Entomology for Students, Chapman and Hall, London, 1996,p. 161.
12. Singh, T. S. and Rana, D., Urogenital myiasis caused by Megaselia scalaris: a case report,J. Med. Entomol., 26, 228, 1989.
13. Greenberg, B., Two cases of human myiasis caused by Phaenicia sericata in Chicago areahospitals, J. Med. Entomol., 21, 615, 1984.
14. Merritt, R. W., A severe case of human cutaneous myiasis caused by Phaenicia sericata,Calif. Vector Views, 16, 24, 1969.
15. Hall, D. G., The Blowflies of North America, Thomas Say Foundation, EntomologicalSociety of America, Lanham, MD, 1948, 168.
16. Hall, R. D. and Townsend, L. H., Jr., The blowflies of Virginia, Virginia Polytechnic Instituteand State University, Research Bulletin No. 123, 1977.
17. Goddard, J., Unpublished data, 1989.
18. Davies, D. M., Human aural myiasis: a case in Ontario, Canada and a partial review, J.Parasitol., 62, 124, 1976.
19. Keller, A. P., Jr. and Keller, A. P., III., Myiasis of the middle ear, Laryngoscope, 80, 646,1970.
20. Goddard, J., Unpublished data, 1987.
21. Damsky, L. J., Baur, H., and Reeber, E., Human myiasis by the black blowfly, Minn. Med.,59, 303, 1976.
23. Goddard, J. and Lago, P. K., An annotated list of the Calliphoridae of Mississippi, J. Ga.Entomol. Soc., 18, 481, 1983.
24. Adler, A. I. and Brancato, F. P., Human furuncular myiasis caused by Hermetia illucens,J. Med. Entomol., 32, 745, 1995.
25. Rice, P. L. and Douglas, G. W., Myiasis in man by Cuterebra, Ann. Entomol. Soc. Am., 65,514, 1972.
26. Goddard, J., Human infestation with rodent botfly larvae: a new route of entry? S. Med.J., 90, 254, 1997.

215
Lice
CHAPTER 22
LICE
TABLE OF CONTENTS
I. Body Lice .........................................................................................................216A. General and Medical Importance ..............................................................216B. General Description ....................................................................................216C. Geographic Distribution .............................................................................217D. Biology/Behavior .........................................................................................217E. Treatment of Infestation .............................................................................217
II. Head Lice .........................................................................................................217A. General and Medical Importance ..............................................................217B. General Description ....................................................................................218C. Geographic Distribution .............................................................................218D. Biology/Behavior .........................................................................................218E. Treatment of Infestation .............................................................................220
III. Pubic or Crab Lice ...........................................................................................221A. General and Medical Importance ..............................................................221B. General Description ....................................................................................221C. Geographic Distribution .............................................................................222D. Biology/Behavior .........................................................................................222E. Treatment of Infestation .............................................................................222
References ......................................................................................................................223

216
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
BODY LICE
ImportanceIrritation; disease transmission
DistributionEssentially worldwide
LesionRed papules, 3 to 4 mm in diameter;
purpuric halo may be present
Disease TransmissionEpidemic typhus; trench fever; epidemic
relapsing fever
Key ReferencesNuttall G. H. F., Parasitol, 10, 80, 1917
Witkowski, J. A. and Parish, L. C.,Infect. Med., 14, 287, 1997.
TreatmentTreatment of all clothing and bedding
of infested individuals; pediculicidalshampoos and lotions
Figure 1Adult body louse (from: U.S. DHEW, PHS, CDC,Pictorial Keys).
I. BODY LICEA. General and Medical Importance
The body louse, Pediculus humanus corporis, isa blood-feeding ectoparasite of humans. Bodyand head lice look almost identical, but headlice remain more or less on the scalp and bodylice on the body or in clothing. Body lice arerelatively rare among affluent members of in-dustrial nations, yet they can become severeunder crowded and unsanitary conditions suchas war or natural disasters. Body lice may trans-mit the agent of epidemic typhus, Rickettsiaprowazeki, and there have been devastatingepidemics of the disease in the past. Typhus isstill endemic in poorly developed countrieswhere people live in filthy, crowded conditions.Besides louseborne typhus, body lice transmitthe agents of trench fever and epidemic relaps-ing fever. Trench fever is still widespread inparts of Europe, Asia, Africa, Mexico, and Cen-tral and South America, but mainly in an asymp-tomatic form. Epidemic relapsing fever occursprimarily in Africa; there were 4,972 cases with29 deaths reported worldwide in 1971.1 Asidefrom the possibility of disease transmission,body lice may cause severe skin irritation. Theusual clinical presentation is pyoderma in cov-ered areas. Characteristically, some swelling andred papules develop at each bite site. There areintermittent episodes of mild to severe itchassociated with the bites. Compounding this,some individuals become sensitized to antigensinjected during louse biting, leading to general-ized allergic reactions. Subsequent excoriationof the skin by the infested individual may leadto impetigo or eczema. Alexander2 noted thatlong-standing infestations may lead to a brown-ish-bronze pigmentation of the skin, especiallyin the groin, axilla, and upper thigh regions.
B. General Description
Body lice are tiny (2 to 4 mm long), elongate,soft-bodied, light-colored, wingless insects (Fig-ure 1). They are dorsoventrally flattened, withan angular ovoid head and a nine-segmentedabdomen. The eggs are small (about 1 mm),

217
Lice
oval, white or cream-colored objects with a distinct cap on one end. The head bearsa pair of simple lateral eyes and a pair of short five-segmented antennae. Body lice areusually about 15 to 20% larger than head lice. They have modified claws enabling themto grasp tightly to hair shafts or clothing while they feed via piercing–suckingmouthparts. Body lice eggs are primarily laid in clothing.
C. Geographic Distribution
Body lice occur essentially worldwide.
D. Biology/Behavior
The body louse lives primarily on the clothing of infested individuals and moves toadjacent body areas to feed. The eggs are attached to fibers of clothing with a stronggluelike substance; they seem to be especially located along the seams inside ofunderwear or other places where clothing contacts the body. Eggs hatch in 5 to 11 days,depending on the temperature, and the young (called nymphs) begin feeding. Devel-oping nymphs feed and molt several times before reaching the adult stage. The egg-to-adult cycle is about 3 to 5 weeks long. Body lice can survive in clothing even if itis habitually removed at night, but usually will die if the clothing is not worn for severaldays. They seem to especially prefer wool clothing.
E. Treatment of Infestation
Since body lice infest both the patient and his clothing, control strategies involvefrequently changing clothing, washing infested garments in very hot water or havingthem dry cleaned, and using pediculicidal lotions or shampoos. The primary elementof control is to ensure that all clothing and bedding of infested persons is sanitized/treated. Clothing and bedding can also be disinfected by spraying a pyrethrin prepa-ration such as A200® spray, R&C spray, or RID® spray. When mass treatments areindicated (such as in a war or natural disaster), insecticide dusts are applied to the bodyand clothing. The U.S. military has mass delousing equipment that is compact andmodern, utilizing a miniature air compressor and small “air paint brush” nozzles to treataffected individuals and their clothing.
II. HEAD LICEA. General and Medical Importance
The head louse, P. humanus capitis, looks and behaves somewhat similar to the bodylouse, but is confined to the scalp. Head lice have been pests of humans throughoutthe ages, as evidenced by the discovery of ancient hair combs dating back to the firstcentury B.C. containing the remains of lice and their eggs. Head lice generally pose nosignificant health threat to infested persons, although heavily infested persons oftenhave occipital and cervical adenopathy and occasionally a generalized morbilliformeruption. The primary negative effects of lice infestation are embarrassment and socialsanctioning.

218
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
HEAD LICE
ImportanceIrritation; itching; secondary infection
DistributionEssentially worldwide
LesionItchy scalp, often secondarily infected as
lesions of impetigo contagiosa
Disease TransmissionNone
Key ReferencesNuttall, G. H. F., Parasitol, 10, 80, 1917
Witkowski, J. A. and Parish, L. C.,Infect. Med., 14, 287, 1997
TreatmentPediculicidal shampoos
Figure 2Adult head louse (from: U.S. DHEW, PHS, CDC,Pictorial Keys).
B. General Description
Head lice are tiny (1 to 3 mm long), elongate,soft-bodied, light-colored, wingless insects (Fig-ure 2). They are dorsoventrally flattened, withan angular ovoid head and a nine-segmentedabdomen (Figure 3). The head bears a pair ofsimple lateral eyes and a pair of short five-segmented antennae. Head lice possess spe-cially modified claws that enable them to grasptightly to hair shafts while they feed throughspecially modified piercing–sucking mouthparts.Head lice look almost identical to body lice.However, they vary distinctly in behavior; headlice occur chiefly on the head, whereas bodylice occur on the body and clothing. Head liceeggs (nits) are about 1 mm long, oval objectswith a distinct cap on one end. They are whiteto cream-colored when viable and firmly at-tached to the hair. Under examination with thenaked eye, they can be confused with dandruff,globules of hair oil or hairspray, and othersubstances, but they are easily identified undermoderate magnification.
C. Geographic Distribution
Head lice occur on humans essentially world-wide.
D. Biology/Behavior
Head lice live on the skin among the hairs onthe patient’s head. Nits are laid on the shaft ofthe hair, near the base, and attached with astrong gluelike substance, most commonly be-hind the ears and at the nape of the neck(Figure 4). As long as adult lice remain on thescalp, they can live for about a month. Becausethey require the warmth and blood meals af-forded by the scalp, it is generally reported thatlice can survive only about 24 h if removed. Butin one study involving hundreds of head liceremoved from children, none survived longerthan 15 h; most died between 6 to 15 h.4 Liceeggs hatch after 5 to 10 days, and the young(called nymphs) begin feeding immediately. Eachfeeding lasts several minutes. As the lice de-velop they feed frequently, both day and night,

219
Lice
Figure 3Microscopic view of head louse. Note strongclaws suited for holding hair shafts.
Figure 4Head lice life cycle (from: U.S. DHEW, PHS, CDC, PictorialKeys).

220
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
particularly when the patient is quiescent. In as little as 18 to 20 days they maturethrough three molts, mate, and the females are ready to lay eggs to start the nextgeneration. The egg-to-adult cycle averages 3 weeks.
E. Treatment of Infestation
Management of head lice infestations requires three general steps5: (1) delousinginfested individuals through application of pediculicidal shampoos or cream rinses,with retreatment as necessary; (2) removing nits from the hair as thoroughly as possible;and (3) delousing personal items (clothes, hats, combs, pillows, etc.).
An important principle of head lice management is to treat all infested members ofa family concurrently. If an infested school-aged child is the only family membertreated, he or she may be quickly reinfested by a sibling or parent who is alsounknowingly infested. Individuals with lice should be treated with one of the approvedpediculicidal shampoos or cream rinses. There are several over-the-counter shampoos(RID®, A200®, R&C Shampoo®, and others) containing pyrethrins that are generallyeffective. However, because these products are not sufficiently ovicidal, successfulmanagement may require one or two repeat applications at 7 to 10 day intervals to killnewly hatching lice. There is one over-the-counter product containing the syntheticpyrethroid, permethrin, that is ovicidal (Nix®), which is applied as a creme rinse aftershampooing. Because Nix® has significant ovicidal activity in addition to its pediculi-cidal effect, a single treatment may sometimes be sufficient for total eradication of liceand viable eggs.5 However, many state health departments still recommend a secondtreatment 7 to 10 days later — even with Nix®. Another product, KWELL® (containinglindane, an organochlorine), is available by prescription as a shampoo. However,inappropriate use of lindane, such as frequent, repeated applications or ingestion, canresult in neurotoxicity. Brandenburg et al.6 have shown that single treatments with thesynthetic pyrethroids are more effective than treatments with lindane. Recently, theFDA re-approved malathion (Ovide® lotion) as a prescription drug for the treatmentof head lice infestation. Any of these products — even lindane — are quite safe whenused as directed. No matter which product they choose, patients should be instructedto follow the precautions and instructions on the product label.
Concerning the removal of nits, it is advisable to remove as many as possible fortwo reasons. First, reducing the number of viable ova in the hair reduces the chanceof persistent infestation and treatment failure. Second, removal of nits lessens concernabout continued infestation and risk of spread to others, thus allowing resumption ofnormal daily routine and/or school. Removal of all nits is probably impossible. For thisreason, persons should be instructed to use the specially designed combs providedwith the pediculicides and to follow the product instructions. Combing out nits is moresuccessful if the hair is damp.
Finally, efforts should be made to delouse personal belongings of infested individu-als. Washable clothing, hats, bedding, and other personal items should be washedproperly and dried in a clothes drier for at least 20 to 30 min. Nonwashable clothesshould be dry cleaned. Other personal items such as combs and brushes should bethoroughly washed in one of the pediculicidal products or soaked in hot water (130°F or more) for 5 to 10 min. Upholstery exposed to potential infestation should bevacuumed thoroughly. Use of certain appropriately labeled pyrethrum aerosols onfurniture, carpeting, and other places where lice are suspected may kill a stray louse

221
Lice
or two, but since the lice do not willingly leave their host and do not survive long offthe host, these treatments would serve primarily as a psychological adjunct to othertreatments and generally are not recommended.
Lice Resistant to Pediculicides. During recent years, there has been an increase inreports of head lice treatment failures. These failures are most often the result ofreinfestation or lack of adherence to already established treatment protocols. However,there does appear to be some development of resistance in certain lice populations toconventional agents such as permethrin, pyrethrins, and organochlorine insecticides.7,8,8a
A study of field-collected lice from Buenos Aires showed definite resistance topermethrin.8 However, it is unlikely that any particular population of lice is resistantto all pediculicides. The various lice treatment products have different active ingredi-ents in various classes of insecticide — for example, KWELL® has lindane (chlorinatedhydrocarbon); Ovide® has malathion (organophosphate); NIX® has permethrin (syn-thetic pyrethroid); A200®, R&C®, and RID® have pyrethrins (botanical). Patients withsuspected populations of resistant head lice should switch and be treated with aproduct containing a different class of active ingredient, again paying careful attentionto label directions. It has been suggested that ivermectin could be effective in treatingresistant head lice.9,10 Ivermectin is an antiparasitic drug discovered in the early 1970sthat is a derivative of avermectin B1, a compound produced by Streptomyces avemitilis.It is a systemic parasiticide/acaricide, killing the pests as they feed on their host.Ivermectin already has approval in the U.S. for treatment of onchocerciasis andstrongyloidiasis. Treatment with oral ivermectin for resistant head lice seems to be apromising approach, but additional data are needed to demonstrate the safety of thisapproach.9
III. PUBIC OR CRAB LICEA. General and Medical Importance
Since the 1960s widespread sexual freedom, particularly among young unmarriedindividuals, has contributed significantly to the growing incidence of pubic liceinfestation.11 The condition is known as “pediculosis pubis” or “pthiriasis” and is causedby Pthirus pubis. The lice occur almost exclusively in the pubic or perianal areas, rarelyon eyelashes, eyebrows, or other coarse-haired areas. They feed on human bloodthrough piercing–sucking mouthparts. Often, louse bites produce discrete, round, slaty-gray or bluish spots (maculae caeruleae).11 The bites may also cause intense itching dueto the host’s reaction to proteins in the louse saliva. Secondary infections may occurif the infestation is not treated. Excoriation of the skin from extensive scratching maylead to inflammation of the skin and lymph glands due to bacterial infection. Ifinfestation occurs in the eyelashes, there may be blepharitis, an inflammation of theeyelids. Pubic lice are not known to transmit disease organisms. However, pediculosispubis frequently coexists with other venereal diseases, particularly gonorrhea andtrichomonas. One study indicated that one third of patients with pubic lice may haveother sexually transmitted diseases.12
B. General Description
Adult pubic lice are dark gray to brown in color. They are called “crab lice” becauseof their crablike shape. They are distinctly flattened, oval, and much wider than bodyor head lice (Figure 5). As with head and body lice, the head bears a pair of simple

222
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
PUBIC LICE
Figure 5Adult pubic louse (from: U.S. DHEW, PHS, CDC,Pictorial Keys).
ImportanceItching; irritation; secondary infection
DistributionEssentially worldwide
LesionVariable — sometimes bluish spots
Disease TransmissionNone
Key ReferencesNuttall, G. H. F., Parasitol, 10, 383, 1917
Witkowski, J. A. and Parish, L. C.,Infect. Med., 14, 287, 1997
TreatmentPediculicidal shampoos
lateral eyes and a pair of short five-segmentedantennae. They are 1.5 to 2.0 mm long and havetheir second and third legs enlarged containinga modified claw with a thumblike projection,which aids them in grasping hair shafts (Figure6). The individual egg or “nit” is dark brown incolor, opalescent, and smaller than that of thebody louse.
C. Geographic Distribution
Pubic lice occur on humans virtually world-wide.
D. Biology/Behavior
Pubic lice require human blood to survive. Theyare only found on humans and do not infestrooms, carpets, beds, pets, etc. If lice happen tobe forced off their host, they will die within 24to 48 h. Fisher and Morton11 report that this timeis <20 h. Female pubic lice deposit their eggs(nits) mainly on the coarse hairs of the pubicarea and rarely on hairs of the chest, armpits,eyebrows, eyelashes, and mustache. In veryrare cases, they have been found in the scalp.They lay approximately 30 eggs during their 3to 4 week life span. There are three nymphalmolts. Nymphs look almost identical to adults,only smaller.
Pubic lice do not fly, jump, or even crawlvery much. They often spend their entire lifefeeding in the same area where the eggs weredeposited. Pubic lice are transmitted from per-son to person most often by sexual contact,although it is possible (though rare) for trans-mission to occur via toilet seats, clothing, orbedding.
E. Treatment of Infestation
Since pubic lice infestations are usually trans-mitted through sexual contact, it is important tohave the sexual contacts of the infested personexamined and treated if needed. Likewise, sincesome family members all sleep in the same bed,if one member of a family has an infestation, allfamily members should be examined and theinfested ones treated. As with head and body

223
Lice
Figure 6Microscopic view of immature pubic louse holding hair shaft.
lice control products, some are sold over-the-counter and some are by prescription.KWELL® (lindane) shampoo, applied for 5 min in the shower, is quite effective fortreatment of infestations in the pubic, perianal, chest, or underarm areas. Also effectiveare KWELL® lotion (applied for 12 h), synergized pyrethrins (over-the-counter productssuch as RID®, A200®, and R&C®), and permethrin (NIX®). Treatment is usually repeatedin 1 week. Treatments should closely follow directions on the box, bottle, or packageinsert. For pubic louse infestations of the eyebrows or eyelashes, mechanical removalof nits is used; twice daily applications of petrolatum for 7 to 10 days, or possiblyanticholinesterase eye ointments, yellow oxide of mercury, or fluorescein are alsoused.13 At the same time of treatment, infested persons should wash all their under-clothes and bedding in hot water for 20 min or more, and dry them on the hottestsetting. Because of the limited survivability of pubic lice off their hosts, insecticidalsprays, fogs, etc. in the patient’s home, work, or school are not necessary.
REFERENCES1. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,
Macmillan, New York, 1979, chap. 8.
2. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 5.
3. Witkowski, J.A. and Parish, L.C., What’s new in the management of lice, Infect. Med., 14,287, 1997.
4. Meinking, T.L., Taplin, D., Kalter, D.C., and Eberle, M.W., Comparative efficacy oftreatments for pediculosis capitis infestations, Arch. Dermatol., 122, 267, 1986.

224
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
5. Baumgartner, E. T., Head lice and their management, Miss. Morb. Rep., 8, 1, 1989.
6. Brandenburg, K., Deinard, A. S., DiNapoli, J., Englender, S. J., Orthoefer, J., andWagner, D., One percent permethrin cream rinse vs 1% lindane shampoo in treatingpediculosis capitis, Am. J. Dis. Child., 140, 894, 1986.
7. Downs, A. M. R., Stafford, K. A., Harvey, I., and Coles, G. C., Evidence for doubleresistance to permethrin and malathion in head lice, Br. J. Dermatol., 141, 508, 1999.
8. Bailey, A. M. and Prociv, P., Persistent head lice following multiple treatments: evidencefor insecticide resistance in Pediculus humanus capitus, Austr. J. Dermatol., 41, 250, 2000.
8a. Picollo, M. I., Vassena, C. V., Casadio, A. A., Massimo, J., and Zebra, E. N., Laboratorystudies of susceptiblity and resistance to insecticides in Pediculus capitis, J. Med. Entomol.,35, 814, 1998.
9. Estrada, B., Head lice: what about ivermectin? Infect. Med., 15, 823, 1998.
10. Burkhart, K.M. and Burkhart, C.G., Ivermectin is available for use against lice, Infect. Med.,14, 689 (letter), 1997.
11. Fisher, I. and Morton, R.S., Pthirus pubis infestation, Br. J. Vener. Dis., 46, 326, 1970.
12. Chapel, T. A., Katta, T., and Kuszmar, T., Pediculosis pubis in clinic for treatment ofsexually transmitted disease, Sex. Trans. Dis., 6, 257, 1979.
13. Buntin, D. M., Rosen, T., Lesher, J. L., Jr., Plotnick, H., Brademas, M. E., and Berger, T. G.,Sexually transmitted diseases: viruses and ectoparasites, J. Am. Acad. Dermatol., 25, 527,1991.

225
Millipedes
CHAPTER 23
MILLIPEDES
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................225
II. General Description .........................................................................................225
III. Geographic Distribution ..................................................................................226
IV. Biology/Behavior .............................................................................................226
V. Treatment ..........................................................................................................227
References ......................................................................................................................227
I. GENERAL AND MEDICAL IMPORTANCE
Millipedes, sometimes called “thousand leggers,” are elongate, wormlike arthropodsthat are commonly found in soft, decomposing plant matter.1 They do not bite or stingbut some species secrete (and in some cases forcefully discharge) defensive body fluidscontaining quinones such as toluquinone and p-benzoquinones and/or hydrogencyanide that may discolor and burn human skin. Alexander2 said that affected skinbecomes yellowish-brown in color, turning to a dark mahogany brown within 24 h. Themahogany discoloration is attributed to oxidation of quinones on contact with the skin.3
There may be blistering in a day or two, exfoliating to expose a raw surface.4 Radford5
provided an excellent review of millipede burns in people.
II. GENERAL DESCRIPTION
Millipedes are somewhat similar to centipedes except they have two pairs of legs onmost body segments and are generally rounded instead of flattened (Figure 1). In

226
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
MILLIPEDES
Figure 1Millipede (from: U.S. DHEW, PHS, CDC, PictorialKeys).
ImportanceSome species cause burns on skin
DistributionNumerous species worldwide
LesionYellow to brown discoloration; blisters
Disease TransmissionNone
Key ReferenceRadford, A. J., Trop. Geogr. Med. 27,
279, 1975
TreatmentSkin — wash thoroughly to remove
fluids, apply antiseptics; eye —immediate, thorough washing, consultan opthamologist for treatmentguidelines
addition, the mouthparts point downward, ratherthan forward as is the case with centipedes.Millipedes have one pair of antennae. Manyspecies of millipedes are cylindrical (althoughsome are flat) with a hardened, burnished me-tallic look. Some of the tropical species canattain a length of 30 cm.2
III. GEOGRAPHICDISTRIBUTION
There are numerous species of millipedes world-wide. A genus commonly encountered in leaflitter in North America is Narceus which con-tains several species. Rhinochrichus latespargorfound in Haiti, Spirostreptus spp. found in Indo-nesia, and Orthoporus spp. found in Mexico arereported to cause human burns.
IV. BIOLOGY/BEHAVIOR
Millipedes are commonly found under rocks, insoil, and in leaf litter. They are mostly nocturnalin habit and may be active year round; how-ever, millipedes are more commonly encoun-tered during the wet season. When uncovered,they coil up into a tight spiral (Figure 2). Someof the more slender, agile species are attractedto light and may congregate on front porches,patios, or sidewalks of homes. Female milli-pedes lay their eggs in the soil. Upon hatching,immature millipedes have few body segmentsand three pairs of legs; additional legs are addedwith each molt. They go through 2 to 7 instarsbefore reaching the adult stage. Depending uponspecies, millipedes live from 1 to 7 years. Con-cerning the poisonous secretions, for the major-ity of millipede species the secretions ooze outand form droplets around the foramina, but afew species (from genera Spirobolida,Spirostreptus, and Rhinocrichus) can squirt theirsecretions for some distance.5

227
Millipedes
V. TREATMENT
Exposed skin should be washed with copious amounts of water as soon as possible.Alexander2 and Radford4 recommended using the solvents ether or alcohol to helpremove the noxious fluids. Antiseptics may need to be applied.4 Antibiotics areindicated if secondary infection is suspected.2 Eye exposure requires thorough irriga-tion with warm water as soon as possible. An opthamologist should be consulted forcurrent treatment recommendations.
REFERENCES1. Borror, D. J., Triplehorn, C. A., and Johnson, N. F., An Introduction to the Study of Insects,
6th ed., Saunders College Publishing, Philadelphia, 1989, 138.
2. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, 385.
3. Shpall, S. and Frieden, I., Mahogany discoloration of the skin due to the defensivesecretion of a millipede, Pediatr. Dermatol., 8, 25, 1991.
4. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, 460.
5. Radford, A. J., Millipede burns in man, Trop. Geogr. Med., 27, 279, 1975.
Figure 2Millipede coiled up in tight spiral.


229
Mites
CHAPTER 24
MITES
TABLE OF CONTENTS
I. Chigger Mites ...................................................................................................230A. General and Medical Importance ..............................................................230B. General Description ....................................................................................230C. Geographic Distribution .............................................................................231D. Biology/Behavior .........................................................................................231E. Treatment of Bites .......................................................................................231
II. House Dust Mites ............................................................................................232A. General and Medical Importance ..............................................................232B. General Description ....................................................................................232C. Geographic Distribution .............................................................................232D. Biology/Behavior .........................................................................................232E. Treatment of Infestation .............................................................................233
III. Imaginary Mites ................................................................................................233A. Introduction .................................................................................................233B. Treatment .....................................................................................................234
IV. Human Biting Mites .........................................................................................234A. General and Medical Importance ..............................................................234B. Mite Biology and Discussion of Species ...................................................234
Generalized Mite Life Cycle .......................................................................234Discussion of Species .................................................................................235
Order Mesostigmata ................................................................................235Tropical Rat Mite ................................................................................235Tropical Fowl Mite .............................................................................235Northern Fowl Mite ...........................................................................236Spiny Rat Mite ....................................................................................236Chicken Mite ......................................................................................236House Mouse Mite .............................................................................236

230
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Order Prostigmata ...................................................................................238Straw Itch Mite ...................................................................................238Clover Mite .........................................................................................238Cheyletiellid Mite ...............................................................................239
Order Astigmata ......................................................................................239Grain and Flour Mites .......................................................................239
C. Treatment of Infestation/Bites ....................................................................241
V. Scabies Mites (Human Itch or Mange Mites) ................................................241A. General and Medical Importance ..............................................................241B. General Description ....................................................................................242C. Geographic Distribution .............................................................................242D. Biology/Behavior .........................................................................................242E. Treatment of Infestation .............................................................................243F. Management of Scabies in Nursing Homes ..............................................244
VI. Follicle Mites ....................................................................................................245A. Introduction .................................................................................................245B. Discussion of Species .................................................................................246
References ......................................................................................................................246
I. CHIGGER MITESA. General and Medical Importance
Larvae of mites in the family Trombiculidae, sometimes called “chiggers,” “harvestmites,” or “red bugs,” are medically important pests around the world. Over 3000species of chigger mites occur in the world, but only about 20 species cause dermatitisor transmit diseases such as the agent of scrub typhus. Larval chiggers crawl up onblades of grass or leaves and subsequently get on passing vertebrate hosts. On humans,they generally crawl to and attach where clothing fits snugly or where flesh is tender,such as ankles, groin, or waistline. Chiggers then pierce the skin with their mouthparts,inject saliva into the wound (which dissolves tissue), and then suck up this semi-digested material. Feeding generally lasts a few days. Most U.S. pest chiggers produceitching within 3 to 6 h, followed by dermatitis consisting of macules and wheals. Atapproximately 10 to 16 h, red, dome-shaped papules appear, and itching increases inseverity over the next 20 to 30 h.1 Not all medically important chiggers produce thefamiliar itch reactions; those serving as vectors of scrub typhus (central, eastern, andsoutheastern Asia) are not associated with itching or skin reactions.2
B. General Description
Adult chigger mites are oval shaped (approximately 1 mm long) with a bright red,velvety appearance. But it is the larval stage that attacks vertebrate hosts; adults do notbite. Accordingly, it is the larval stage or accompanying lesion that is ordinarilycollected/seen in a clinical setting. Chigger larvae are very tiny (0.2 mm long), roundmites with numerous setae (Figure 1). The mites may be red, yellow, or orange in colorand have a single dorsal plate (scutum) bearing two sensillae and 4 to 6 setae.

231
Mites
CHIGGERS
Figure 1Chigger mite, Leptotrombidium akamushi, dorsal(left) and ventral (right) views. (From: USDA,ARS, Agri. Hndbk #655, Feb. 1991.)
ImportanceIrritation; intense itching; disease
transmission in the Far East
DistributionNumerous species worldwide
LesionVariable — often a red, dome-shaped
papule
Disease TransmissionNone in U.S.; scrub typhus in central,
eastern, and southeastern Asia
Key ReferenceJenkins, D. W., Am. J. Hyg. 48, 22, 1948
TreatmentAntipruritics and/or topical
corticosteroids
C. Geographic Distribution
Chigger species are mostly tropical and sub-tropical, although they occur from Alaska toNew Zealand and from sea level to over 16,000feet in altitude. Some particularly common pestchiggers are Eutrombicula alfreddugesi in theU.S. and parts of Central and South America,Neotrombicula autumnalis in Europe, and E.sarcina in Asia and Australia. Chiggers in thegenus Leptotrombidium transmit the agent ofscrub typhus in Japan, Southeast Asia, and partsof Australia.
D. Biology/Behavior
Chigger mites are found in moist microenviron-ments within grassy, weedy, or wooded areas,especially forest edges and wild blackberrypatches (at least in the southern U.S.). Adultchiggers are predaceous. The female lays eggssingly on soil or litter, and the eggs hatch inabout 1 week. After hatching, the life cycleincludes six stages: (1) the inactive prelarva(deutovum or maturing larva), (2) the parasiticlarval stage, (3) quiescent protonymph/firstnymphal stage (nymphochrysalis), (4) preda-ceous deutonymph/second nymphal stage, (5)quiescent tritonymph/third nymphal stage(imagochrysalis), and (6) the free-living adultstage. The entire life cycle from egg to adultmay be completed in about 60 days. In thenorthern U.S. the mites are active from aboutMay through September, but in the South theymay be active essentially year round. The para-sitic larvae normally feed on rodents, insecti-vores, and ground-frequenting birds, but giventhe chance some species will avidly feed onpeople. Larval chigger mites inject saliva thatdissolves host cellular tissue. The mites theningest this mixture of lymph, dissolved bodytissues, and stray blood cells. They do not “suckblood” in the sense that other ectoparasites do.
E. Treatment of Bites
After exposure to infested outdoor areas, hotsoapy baths or showers will help remove anychiggers, attached or unattached. Antiseptic,

232
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
HOUSE DUSTMITES
ImportanceAllergies
DistributionAlmost worldwide
LesionGenerally none — nonbiting
Disease TransmissionNone
Key Referencevan Bronswijk, J. E. M. H., J. Allergy 47,
31, 1971
TreatmentDust and dust mite control; standard
treatment for allergies
Figure 2Adult female house dust mite, Dermato-phagoides farinae. (From: USDA, ARS, Agri.Hndbk #655, Feb. 1991.)
hydrocortisone, and/or anesthetic (benzocaine)solutions or ointments are often used as treat-ments to minimize itching and reduce chancesof secondary infection.
II. HOUSE DUST MITESA. General and Medical Importance
Mites in the genus Dermatophagoides are com-monly found in houses worldwide and havebeen associated with house dust allergy. Sincethe mid 1960s, considerable research on housedust allergy has revealed that both D.pteronyssinus and D. farinae possess powerfulallergens in the mites themselves, as well as intheir secretions and excretia. The fecal pelletsare especially allergenic. Although dust mitesare harmless in that they do not sting or bite, aconsiderable amount of allergic rhinitis, asthma,and childhood eczema is attributable to theirpresence in the human environment.3 Some stud-ies have investigated the link between housedust mite allergens and atopic dermatitis.4
B. General Description
Adult house dust mites are white to light tan incolor and about 0.5 mm long (Figure 2). Theircuticle has numerous fine striations. The miteshave plump bodies (not flattened), well-devel-oped chelicerae, and suckers at the ends oftheir tarsi.
C. Geographic Distribution
Contrary to its common name, the Europeanhouse dust mite, D. pteronyssinus, actually iswidespread throughout the world. It was thefirst species recognized as having a significantrelationship with house dust allergy.5 The Ameri-can house dust mite is D. farinae, and it is alsoa cosmopolitan inhabitant of houses.
D. Biology/Behavior
House dust mites are associated with furniture(especially mattresses, sofas, and recliner chairs)

233
Mites
and debris in household carpets. They are generally more numerous in mattresses andbedrooms than other areas of a house. In a study in Hawaii,6 dust samples taken fromcarpets always had more mites than dust from noncarpeted floors. Old carpets notcared for properly contained more dust mites than new ones or those often cleaned.The preferred food source of the mites is believed to be shed human skin scales,although they will eat mold, fugal spores, pollen grains, feathers, and animal dander.The mites are most abundant in warm homes with high humidities. Laboratorypopulations exhibit maximum growth at 25°C and about 75% relative humidity and onlysurvive 10 days or less at 40 or 50% relative humidity (RH).7,8 High mite levels occurduring periods of high RH, and these levels become low when RH drops below thecritical level for extended periods. Both D. pteronyssinus and D. farinae have fivedevelopmental stages: egg, larva, protonymph, tritonymph, and adult. The life cycle iscompleted in about 1 month, and adults may live 2 months or so at optimumtemperatures. Cultures of house dust mites are maintained in beds on a year-roundbasis, and seasonal fluctuations occur.3
E. Treatment of Infestation
House dust mite allergy is managed by immunotherapy using mite extracts and byefforts to minimize the level of dust mites in the patient’s home. Since long-fiberedcarpets are difficult to clean, tile, wood, or other “hard” floor covering may be neededin those homes. Vacuuming should be done regularly, especially in the bedroom(although the allergic person probably should not be the one vacuuming). Double-thickness filters or HEPA filters are needed for maximum results. The mattresses shouldbe vacuumed intensely. Studies have demonstrated that after mattresses were vacuum-cleaned, there was as much as an eightfold reduction in the number of mites thatbecame airborne during bedmaking.9,10 In addition, synthetic pillows and plasticmattress covers should be used and there should be a yearly replacement of mattresses.Sheets and blankets should be cleaned with hot water on a regular basis. Efforts shouldalso be made to reduce household humidity levels, since high humidity favors mitegrowth and reproduction. Although results have been somewhat equivocal, somestudies have demonstrated the effectiveness of benzyl benzoate for carpet treatmentsto reduce mite allergen levels.11,12 However, reducing the number of mites does notalways lower allergen levels right away.
III. IMAGINARY MITESA. Introduction
Patients claiming to be infested with mites (that subsequently cannot be seen, collected,or controlled) may be suffering from delusions of parasitosis (DOP) (see Chapter 7). Thisemotional disorder is covered more thoroughly in Part I of this book, but basicallyinvolves the unwarranted belief that tiny, almost invisible insects or mites are present onthe body. Characteristically, the patient presents to the clinic with pieces of tissue paperor small bags or cups containing the presumed mites or insects. However, these usuallyonly contain dust, specks of dirt, dried blood, pieces of skin, and occasionally common(nonharmful) household insects or their body parts. Skin lesions may be present, but self-induced causes are possible. The majority of such patients are elderly females.1

234
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
B. Treatment
Cases of imaginary insect or mite infestations must be carefully investigated to rule outactual arthropod causes. Skin scrapings of lesions should be examined for scabiesmites. A competent entomologist should examine the patient’s workplace and/orresidence. Careful attention should be given to rat- or bird-infested dwellings since theymay harbor parasitic mites. If repeated collection attempts and/or insecticidal treat-ments are unsuccessful, and if the patient exhibits symptoms consistent with DOP, thenDOP should be strongly considered as the cause of the problem. After ruling out actualarthropod causes and any underlying medical conditions, physicians often refer thepatient to a psychiatrist.
IV. HUMAN BITING MITESA. General and Medical Importance
There are actually only two human-associated parasitic mites, the scabies mite and thehair follicle mite (see the following sections on these two mites). However, many otherspecies of mites are important to public health, such as chiggers and house dust mites,which were covered previously. This section includes a hodgepodge of the remainingmite species that may be involved in human bites or cases of dermatitis (clover mitesare included — they do not bite, but often invade homes en masse). Most mitesmentioned here are important only as causes of itch or dermatitis, but the house mousemite, Liponyssoides (formerly Allodermanyssus) sanguineus, is a vector of rickettsialpoxin Massachusetts, Connecticut, New York, Pennsylvania, and Ohio.13
B. Mite Biology and Discussion of Species
Generalized mite life cycle. It is difficult to describe a “typical” mite life cycle andaccompanying life stages since there is tremendous variation among the various orders;however, most mites generally display the following life cycle. Adult females lay eggs
Figure 3Female rat mite with parts labeled (from:U.S. DHHS (CDC) Publ. No. 83–8297).

235
Mites
that hatch into larvae, pass through one to threenymphal stages, and finally become adults. Thelarvae have only three pairs of legs — nymphsand adults have four pairs. The first nymphalstage is called a protonymph, the second iscalled a deutonymph, and the third nymphalstage, if present, is called a tritonymph. In somemite orders, one of the nymphal stages is anonfeeding phoretic stage for passive transport(in the fur of animals, in bird feathers, oninsects, etc.). Figure 3 is provided to familiarizethe reader with some of the more prominentmorphological characters of mites.
Discussion of species
Order Mesostigmata
Tropical rat mite. Ornithonyssus bacoti is fairlyeasy to recognize. Females have scissorlike che-licerae, narrow, tapering dorsal and genitoventralplates, and an egg-shaped anal plate (Figure 4).In addition, the protonymphal stage and adultfemales suck blood, and become tremendouslydistended after feeding. They look like tinyengorged ticks.
The tropical rat mite is an ectoparasite of rats.The adult mites produce a nonfeeding larvalstage, a bloodsucking protonymphal stage, anda nonfeeding deutonymphal stage. A completegeneration of this species usually takes about 2weeks. Females can live unfed 10 days or moreafter rats have been trapped out of a building.Tropical rat mites bite people, readily produc-ing a papulovesicular dermatitis with accompa-nying urticaria.
The tropical rat mite is widely distributed onall continents in association with rats.
Tropical fowl mite. Ornithonyssus bursa issimilar in appearance to the tropical rat mite,but has a wider dorsal plate (Figure 5).
The biology of the tropical fowl mite is simi-lar to that of the tropical rat mite, except it isfound on domestic and wild birds. It may befound on rodents, but rarely. This species isfound on poultry, but it is also a significantparasite of the English sparrow.
Tropical fowl mites are distributed over mostof the world but are more commonly seen intropical and subtropical areas.
BITING MITES
ImportancePainful bites; itching; irritation
DistributionNumerous species worldwide
LesionVariable — erythema, bright red
papules of varying sizes
Disease TransmissionGenerally none; possibly rickettsialpox
Key ReferenceSections on “Biting Mites” in Alexander,
Arthropods and Skin, Springer-Verlag,Berlin, 1984
TreatmentGenerally palliative treatment only;
eliminate source of exposure
Figure 4Adult tropical rat mite, Ornithonyssus bacoti(from: USDA, ARS, Agri. Hndbk. #655, Feb.1991).

236
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Northern fowl mite. Ornithonyssussylviarum also is similar in appearance to thetropical rat mite but has a much shorter sternalplate (Figure 6). This plate has only four setae;the setae on the dorsal plate are quite short. Thenorthern fowl mite is a pest of domestic fowl,pigeons, sparrows, and starlings. The speciesoverwinters in bird nests or cracks and crevicesof buildings. Unlike the chicken mite, D. gallinae,the northern fowl mite spends its entire life onthe host. In poultry houses the mites are usuallyonly found on the birds, but they have beenfound on eggs and cage litter. Northern fowlmites cannot survive more than a month or so inthe absence of their poultry hosts. The northernfowl mite occurs in temperate regions worldwide.
Spiny rat mite. Laelaps echidnina is easilyrecognized by its large genitoventral plate, witha concaved posterior margin into which theanal plate fits (Figure 7). Spiny rat mites areectoparasites of the Norway rat and roof rat.This species is probably the most prevalent mitespecies occurring on rats in the U.S., particularlyin the central and northern regions of the coun-try. The spiny rat mite is found worldwide.
Chicken mite. Dermanyssus gallinae haslarge dorsal and anal plates, a short sternalplate, and needlelike chelicerae (Figure 8).
The chicken mite, also known as the “redmite of poultry,” is commonly found on domes-tic fowl, pigeons, English sparrows, starlings,and other birds. This mite is one of the mostcommon species causing human dermatitis inpoultry houses, farms, ranches, and marketswhere chickens are traded or sold. Poultryworkers are often bitten on the backs of thehands and on the forearms. D. gallinae is noc-turnal; during the day the mites hide in cracksand crevices in chicken houses or buildingswhere infested birds nest. Eggs are deposited inthese hiding places. The chicken mite occursworldwide.
House mouse mite. Liponyssoides san-guineus looks similar to the chicken mite (D.gallinae). Females of the house mouse mite canbe distinguished from most other mites by thepresence of two dorsal shields, a large anteriorplate, and a small posterior plate bearing onepair of setae (Figure 9).
Figure 5Adult tropical fowl mite (redrawn inpart from: U.S. DHEW, PHS, CDC,Pictorial Keys).
Figure 7Adult spiny rat mite (from: U.S. DHHS(CDC) Publ. No. 83–8297).
Figure 6Adult northern fowl mite.

237
Mites
The house mouse mite is primarily an ectoparasite of mice, but has been collectedfrom rats and other rodents. The protonymphs, deutonymphs, and adults all suckblood. The life cycle from egg to adult takes about 18 to 23 days.
CASE HISTORY
MYSTERIOUS MITES INFESTING A WORKPLACE
In early October in central Mississippi, a group of women working in a relatively new four-story building complained of seeing numerous tiny, almost invisible mites crawling aroundon their desks and office cubicles. As far as was known, the mites were not biting theworkers. The affected office suite consisted of approximately twelve, 10 × 10 cubicles, eachcontaining a desk, a filing cabinet, and a few personal items. The partitions (making up thecubicles) were padded on each side with a carpet-like covering and stood 6 feet high. Ahard plastic rim topped each partition. Careful inspection of the affected area revealedthousands of tiny tan to yellow colored mites, mostly seen walking along the upper edgesof the partitions. Specimens were collected, examined microscopically, and identified asspider mites, family Tetranychidae. Upon further investigation at the office suite, a desk inone of the cubicles was found to have a potted plant on it which was heavily infested withspider mites and in contact with the partition. Mites were seen climbing the partition fromthat point.
Comment: Tetranychids (spider mites) are plant feeders which may reach up to 0.8 mmin length and vary in color from yellowish to greenish, orangish, reddish, or red. Somespecies are red only in winter. Spider mites receive their name from their ability to spin afine web over the leaves of the plant upon which they feed. At times, the entire plant maybe covered with this webbing. Potted plants are the source of a variety of insect and miteinfestations in workplaces. In fact, a competent pest control technician will often ask to seeindoor plants first when investigating a bug problem in a work setting.
Figure 8Adult chicken mite Dermanyssusgallinae. (From: USDA, ARS, Agri.Hndbk. #655, Feb. 1991.)
Figure 9Adult house mouse mite Liponyssoidessanguineus. (From: USDA, ARS, Agri.Hndbk. #655, Feb. 1991.)

238
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
The house mouse mite occurs in northern Africa, Asia, Europe, and the U.S.(primarily the northeast).
Order Prostigmata
Straw itch mite. Pyemotes tritici is an elongate species that has the first and secondpairs of legs widely separated from the third and fourth pairs (Figure 10A). Also, thismite has a club-shaped hair between the base of the first and second pairs of legs. Themale is so small that it is almost invisible to the naked eye. Females with eggs maybecome enormously swollen (about 1 mm) with their abdomen resembling a tiny pearl(Figure 10B).
Straw itch mites are parasites of several insect species, but will bite people readily.Human bites occur when humans come into contact with infested straw, hay, grasses,beans, peas, grains, and other materials. Accordingly, agricultural workers, personswho process or handle grain, or those who sleep on straw mattresses are most proneto infestation. Alexander1 said that severe human infestations may occur with upwardsof 10,000 lesions on an individual. Attacks are more frequent during the hot weathermonths. This mite has a curious life cycle. As the female feeds, the opisthosomabecomes enormously distended (Figure 10B). Also, all of the nymphal stages occurwithin the egg so that after hatching, active young occur in the body of the gravidfemale. Each adult female may produce 200 to 300 young. Males mate with emergingyoung females at or near the genital opening of the mother.
Straw itch mites occur in most areas of the world.Clover mite. Clover mites in the Bryobia praetiosa complex are tiny reddish-brown
mites about 0.8 mm long. They have extremely long first pairs of legs and wedge-shaped body hairs (Figure 11).
Clover mites are commonly found on herbaceous plants such as ivy, grass, andclover, as well as some deciduous trees (especially fruit trees). They tend to developmost where there is abundant and actively growing vegetation. This may present aproblem when homeowners plant shrubs or ivy immediately next to their houses. Themites will invade homes in great numbers, especially in the fall, as the weather startsto get cold. Quite often they swarm by the thousands over outer walls of buildings and
Figure 11Adult clover mite (from: U.S. DHHS (CDC)Publ. No. 83–8297).
Figure 10Adult straw itch mite (A) and gravid adultfemale (B) (from: U.S. Navy LaboratoryGuide to Medical Entomology).

239
Mites
make their way indoors around doors, windows, or cracks. They do not bite people,but often cause alarm.
Clover mites are cosmopolitan in distribution.Cheyletiellid mite. Cheyletiella yasguri, C. blakei, and C. parasitivorax have fused
cheliceral bases further fused with the subcapitulum forming a capsular gnathosoma(Figure 12). This makes it look like they are wearing a helmet. They have free andhighly developed palpi with strong curved claws that look like an extra pair of legsnear the mouthparts.
The Cheyletiellidae are parasites of birds and various species of small mammals. TheCheyletiella spp. mentioned in this section are obligate parasites of small or medium-sized mammals (including pet dogs, cats, and pet rabbits), living on the keratin layerof the epidermis; they do not burrow. These mites may cause a mangelike conditionon pets and a transient itching dermatitis on humans who handle these pets. In mostcases the patient complains of itching and has papules or papulovesicles (2 to 6 mmdiameter) on the flexor side of the arms, on the breasts, or on the abdomen. Mites arerarely found in scrapings of the lesions, since the mites have usually left the personby the time medical advice is sought. Cheyletiella eggs are attached to hairs on the host(pet dog, cat, etc.) about 2 to 3 mm above the host’s skin. These mites cannot survivemore than 48 h off their hosts.
In a review of the Cheyletiella,14 specimens were reported from small pets in the U.S.,South America, Western Europe, Australia, New Zealand, and few widely scatteredspots in Africa, India, and Japan.
Order Astigmata
Grain and flour mites. There are several species of grain and flour mites that cancause grocer’s itch, copra itch, and other lay-named itches. They are tiny mites (0.5 mmor less) that are pale gray or yellowish-white, and they have the first and second pairsof legs widely separated from the third and fourth pairs (Figures 13 to 15). Also, theyhave conspicuous long hairs (Figure 16).
Mites causing grocer’s itch, copra itch, vanillism, wheat pollard itch, and dried fruitdermatitis are basically scavengers on a wide variety of organic matter including flour,meal, grains, dried fruits, vanilla pods, meats, and other similar products. These tiny
Figure 12Adult cheyletiellid mite.
Figure 13Adult grain mite (from: U.S. DHHS (CDC)Publ. No. 83–8297).

240
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
mites have brief developmental times and can multiply into the billions in a storedproduct in a very short period of time. They do not suck blood, but they will penetratethe superficial epidermis, producing a temporary pruritus.
Grain and flour mites occur worldwide wherever people have shipped foodproducts.
Figure 16Microscopic view of grain mite, Acarus siro.
Figure 14Adult ham mite (from: U.S. DHHS (CDC) Publ.No. 83–8297).
Figure 15Adult cheese mite (from: U.S. DHHS (CDC) Publ.No. 83–8297).

241
Mites
C. Treatment of Infestation/Bites
Human infestations with the above-mentioned mite species are mostly transitory andthe reaction is variable. Sensitive people may develop dermatitis. These mite specieswill not take up permanent residence on human skin and thus perpetuate theinfestation. Accordingly, treatment primarily involves alleviation of the symptoms, andavoidance and/or eradication of the mites from the pet, home, or workplace. Acuteurticarial lesions may respond satisfactorily to topical corticosteroid lotions and creams,which reduce the intensity of the inflammatory reaction. Oral antihistamines mayrelieve itching and burning sensations.
V. SCABIES MITES (HUMAN ITCH OR MANGE MITES)A. General and Medical Importance
Scabies, caused by Sarcoptes scabei, is probably the most important disease caused bymites with at least 300 million cases annually.15 It occurs worldwide, affecting all racesand socioeconomic classes in all climates.1 The tiny mites burrow under the skin, leavingsmall open sores and linear burrows that contain the mites and their eggs. When a personis infested with scabies mites for the first time, there is little pathology for about a month,until sensitization develops. When that happens, there is severe itching, especially at nightand frequently over much of the body. Large patches of erythema or rash may occur onthe body. The patient’s tissues apparently become sensitized to various proteins liberatedby the mites. Interestingly, the generalized rash may not correspond to the sites wherethe mites are burrowing. The burrows are usually located on the hands, wrists, andelbows, especially in the webbing between the fingers and the folds of the wrists.16,17
Alexander1 said that burrows are sometimes few in number and difficult to find. Genitallesions are common in scabies. The presence of crusted, excoriated, pruritic papules onthe penis or buttocks is virtually pathognomonic.18 In many cases severe itching causesthe patient to scratch himself vigorously, leading to secondary infections such asimpetigo, eczema, pustules, and boils.
The author has encountered scabies problems frequently in nursing homes. In theelderly, reactions to the mite are often not inflammatory — as seen in younger people— and are muted. Accordingly, scabies is often missed by the attending health careprovider. Bedridden patients with scabies complain of intense itching. Mites may befound on the back of such patients (unusual).
People who cannot scratch themselves and the immunocompromised (e.g., AIDSpatients) may develop more serious scabies infestations. In this case, millions of mitesmay inhabit thick crusts over the skin — a condition called Norwegian scabies orcrusted scabies. Alexander1 says there are two principal components of the eruption,localized horny plaques and a more diffuse erythematosquamous appearance. He alsosays that patients with Norwegian scabies are frequently inmates of long-stay institu-tions, and when presented to the dermatologist appear to be suffering from chronicexfoliative eczema.
It should be noted here that animal forms of scabies (such as canine or equine) arealso caused by “races” of S. scabei, but these mites cannot propagate in human skin.Canine scabies can be temporarily transferred to humans from dogs, causing itchingand papular or vesicular lesions primarily on the waist, chest, or forearms. However,treatment or removal of the infested dog will result in a gradual resolution of this typeof scabies.1

242
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 17Microscopic view of scabies mite removed from human skin.
B. General Description
Sarcoptes scabei are very tiny (0.2 to 0.4 mm long), oval, saclike, eyeless mites (Figure17). Their legs are rudimentary; the anterior two pairs have bell-shaped suckers on thetips of them. The body is covered with striations and has several stout blunt spines anda few long setae (Figure 18). Scabies mite mouthparts are composed of toothedchelicerae and one-segmented palps fused to the central hypostome. Nymphs lookalmost identical to the adults, except smaller.
C. Geographic Distribution
Human scabies mites occur worldwide. There are several scabies mites that occur ondomestic animals (dogs, cats, horses, and camels) worldwide also. These “races” of S.scabei are virtually indistinguishable from the human form, but do not producesustained infestations on people.
D. Biology/Behavior
Scabies is transmitted by close, human-to-human contact with infested individuals.there is some evidence that fomites may be important sources of infestation or re-infestation.19 Touching or shaking the hands of infested persons is a major mode oftransmission. The practice of several family members sleeping in one bed contributesto its spread, as does sexual activity. In addition, institutionalized children (day care)and elderly (nursing homes) seem to be contributing to an increase in the incidenceof scabies.
A female mite infests a new host by burrowing beneath the outer layer of skin andlaying her eggs in the tunnels that she excavates. A six-legged larval stage emerges fromeach egg and molts to the first nymphal stage in 2 or 3 days. Nymphal and adult stages

243
Mites
CASE HISTORY
SCABIES IN AN INSTITUTION FORTHE MENTALLY HANDICAPPED
On August 10, 1999, the medical director at a local institution for the mildly retarded calledsaying that several of his patients were obviously scratching themselves — even to the pointof bleeding. He was wondering what different types of arthropod pests might be respon-sible. On August 13, I visited the institution and found approximately 12 male patientscomplaining of intense itching. Most had obvious rashes on the arms and trunks. One manhad numerous, self-inflicted, deep fingernail scratch marks on his body which wereunbandaged and bleeding. I told the medical director that scabies was likely the cause ofthe itching, but skin scrapings, performed by a dermatologist, would be needed forconfirmation. Later I interviewed maintenance staff asking questions about the layout of thebuilding, history of pest (such as rat or bird) problems, and bird nesting (or lack thereof) inthe attic. Nothing out of the ordinary was noted. I then took dust samples — alcohol swipesof furniture, bedding, etc. — from affected patient’s rooms. Back at the lab, dust sampleswere examined microscopically for the presence of human biting mites. A sample from onepatient’s bed contained dust, debris, pieces of excoriated skin, and a scabies mite, Sarcop-tes scabei, thus confirming scabies infestation. Patients were subsequently treated withscabicidal lotions and the infestation eliminated.
Comment: Investigation of this event revealed several interesting features. The patientswere itching so severely that they were scratching themselves to the point of bleeding.Perhaps this was due to their altered mental status or lowered immune status. Second, theinfestation was so great that scabies mites could be found in the bed. Most scabiesinfestations involve only a few mites; finding them is a difficult task. Except in cases ofNorwegian (also called “crusted”) scabies, it is extremely rare to find the mites on furniture,bedding, and the like.
have eight legs. Larvae and nymphs are often found in short burrows or in hair follicles.After a few days the nymphs molt to the next nymphal stage. After the second nymphalstage adults are formed. The entire life cycle takes 10 to 17 days. The mites apparentlyeat human skin, although the immatures may feed on hair follicle secretions.
Survival of scabies mites off-host is probably a few days — more likely hours. Studieshave shown that the mites may survive 1 to 5 days at room conditions, but may havea difficult time infesting a host after being off the host (presumably due to the mite’sweakened condition).19
E. Treatment of Infestation
First of all, scabies should be confirmed by isolating the mites in a skin scraping, sinceother forms of dermatitis may resemble scabies infestation. Scrapings should be madeat the burrows, especially on the hands between the fingers and the folds of the wrists.Some dermatologists may choose to scrape burrows located on the feet.1 To do thescraping, mineral oil is placed on a sterile scapel blade and allowed to flow ontosuspected lesions. By gentle scraping with the blade, the tops of burrows or papulesare removed. The oil and scraped material is then transferred to a glass slide and acoverslip applied. Diagnosis can be made either by finding mites, ova, or fecal pellets.

244
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
SCABIES MITES
Figure 18Human scabies mite.
ImportanceIntense itch; secondary infection
DistributionWorldwide
LesionBurrows and papules where mites are
located; generalized rash may occurin other areas
Disease TransmissionNone
Key ReferencesScabies section in Alexander, Arthropods
and Skin, Springer-Verlag, Berlin,1984
Mellenby, K., Classey Ltd. Publishers,Hampton, Middlesex, U.K., 1972
TreatmentScabicides (cream or lotion) per label
instructions
Alternatively, mites can be extracted from aburrow by gently pricking open the burrowwith a needle and working toward the endwhere the tiny mites usually are. A hand lensmay be useful for this task.
Once a scabies infestation is confirmed, treat-ment can be initiated. Since the mites cannotlive very long off of a human host, insecticidetreatments of bedding, furniture, rooms, etc. isunnecessary. It is recommended, however, thatupon initiation of treatment, the patient’s bedcovers, pillow cases, and undergarments beremoved and washed on the hot wash cycle. Ifthe patient is a chile, toys, stuffed animals, etc.should be removed from human contact for aweek or so.
There have been several products used forscabies treatment in the past, such as sulfurointment, benzyl benzoate, lindane, crotamiton,and thiabendazole. The most widely used in theU.S. today are lindane (Kwell®), permethrin(Elimite®), and crotamiton (Eurax®). There havebeen reports of lindane-resistant scabies, espe-cially in cases of immigrants or recent travelersto Central and South America or Asia.20 Regard-less of the product used, package instructionsshould be followed carefully. For most scabicides,the product is applied to the entire body, exceptthe head (see package insert; sometimes thehead is treated), and left on for 14 to 48 hdepending upon instructions. After that, a cleans-ing bath may be taken. A second treatment maybe called for in the instructions. Itching maypersist for weeks or more after treatment anddoes not necessarily indicate treatment failure.The post-treatment itch/rash is often treatedwith cortisone cream. Some physicians pre-scribe oral antipruritic agents (antihistamines orhydroxyzine) simultaneously with the applica-tion of scabicides.
F. Management of Scabies in NursingHomes
Since scabies control in institutions can bedifficult and frustrating, a brief outline of acontrol strategy is offered here. First of all, thediagnosis should be confirmed. Frequently, sca-bies control measures are implemented with

245
Mites
only weak evidence of infestation, e.g., “Lookssorta’ like a scabies rash to me.” However,implementing a large-scale control effort onthe suspicion that an outbreak is occurring inthe nursing home is medically and administra-tively unsound. The active ingredients in scabi-cidal creams or lotions are pesticides. A der-matologist should be consulted to perform skinscrapings on affected patients. Once the infes-tation is confirmed, treatment with one of thescabicidal products can be initiated. Both pa-tients and employees with direct, close contactwith affected patients should be treated. Ifcases reappear, aggressive treatment strategiesmay have to be used such as simultaneouslytreating all patients and employees in the nurs-ing home (and possibly even family membersof employees).21,22 Consultation with state orlocal health department epidemiology person-nel is often helpful as well. There have beenstudies showing the effectiveness of a single,oral dose of ivermectin for treatment of humanscabies;23 however, this anti-helminthic drug isnot yet approved for scabies and additionalcontrolled studies are needed.
VI. FOLLICLE MITESA. Introduction
Although there are numerous species ofDemodex (family Demodecidae) infesting wildand domestic animals, only two species of themites are specific human-associated mites andare called follicle mites. The minute, wormlikemites live exclusively in hair follicles or seba-ceous glands. They have no proven detrimentaleffect on humans, although some authors haveattributed various pathological conditions of theskin to Demodex. Alexander1 provides a goodreview of this issue. He concludes, “It should beemphasized that, in general, Demodex is a harm-less saprophyte. It is only exceptionally that itappears to exercise a pathogenic influence, as,for example, when excessive amounts of cos-metics prepare the ground for its proliferationor when it escapes into the dermis.” Variousestimates of the incidence of human Demodexinfestation range from about 25 to 100%, and
FOLLICLE MITES
ImportanceLives in human skin but mostly harmless
DistributionWorldwide
LesionGenerally none
Disease TransmissionNone
Key ReferenceDesch, C. and Nutting, W. B.,
J. Parasitol., 58, 169–177, 1972
TreatmentGenerally none needed
Figure 19Hair follicle mite (from: U.S. DHHS (CDC) Publ.No. 83–8297).

246
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
clinicians should be aware of mite appearance, since they may be seen during skinscraping examination.
B. Discussion of Species
Demodex folliculorum lives in the hair follicles and D. brevis in the sebaceous glands.Both species are similar in appearance (with the exception that D. brevis is a shortenedform) and are elongated, wormlike mites with only rudimentary legs (Figure 19). Theyare approximately 0.1 to 0.4 mm long and have transverse striations over much of thebody. These mites most commonly occur on the forehead, malar areas of the cheeks,nose and nasolabial fold, but they can occur anywhere on the face, around the ears,and occasionally elsewhere.1 Most people acquire Demodex mites early in life fromhousehold contacts — primarily maternal.
REFERENCES1. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, 357.
2. Traub, R. and Wisseman, C. L., The ecology of chigger-borne rickettsiosis (scrub typhus),J. Med. Entomol., 11, 237, 1974.
3. Wharton, G. W., House dust mites, J. Med. Entomol., 12, 577, 1976.
4. Cameron, M.M., Can house dust mite-triggered atopic dermatitis be alleviated usingacaricides?, Br. J. Dermatol., 137, 1, 1997.
5. Voorhorst, R., Spieksma-Boezeman, M. I. A., and Spieksma, F. Th. M., Is a mite(Dermatophagoides sp.) the producer of the house dust allergen? Allergy Asthma., 10, 329,1964.
6. Sharp, J. L. and Haramoto, F. H., Dermato-phagoides pteronyssinus and other Acarina inhouse dust in Hawaii, Proc. Hawaii. Entomol. Soc., 20, 583, 1970.
7. Murton, J. J. and Madden, J. L., Observations on the biology, behavior and ecology of thehouse dust mite, Dermatophagoides ptero-nyssinus in Tasmania, J. Aust. Entomol. Soc., 16,281, 1977.
8. Arlian, L. G., Dehydration and survival of the European house dust mite, Dermatophagoidespteronyssinus, J. Med. Entomol., 12, 437, 1975.
9. van Bronswijk, J. E. M. H. and Sinha, R. N., Pyroglyphid mites and house dust allergy,J. Allergy, 47, 31 1971.
10. van Bronswijk, J. E. M. H., Schoonen, J. M. C. P., and Berlie, M. A. F., On the abundanceof Dermatophagoides pteronyssinus in house dust, Res. Popul. Ecol., 13, 67, 1971.
11. Chang, J.H., Becker, A., Ferguson, A., Manfreda, J., Simons, E., Chan, H., Noertjojo, K. andChan-Yeung, M., Effect of application of benzyl benzoate on house dust mite allergenlevels, Ann. Allergy Asthma Immunol., 77, 187, 1996.
12. Huss, R.W., Huss, K., Squire, E.N. Jr., Carpenter, G.B., Smith, L.J., Salata, K. and Hershey,J., Mite allergen control with acaricide fails, J. Allergy Clin. Immunol., 94, 27, 1994.
13. Huebner, R. J., Jellison, W. L., and Pomerantz, C., Rickettsialpox — a newly recognizedrickettsial disease. IV. Isolation of a rickettsia, apparently identical with the causative agentof rickettsialpox, from Allodermanyssus sanguineus, a rodent mite, Pub. Health Rep., 61,1677, 1946.
14. van Bronswijk, J. E. M. H. and de Kreek, E. J., Cheyletiella of dog, cat, and domesticatedrabbit, a review, J. Med. Entomol., 13, 315, 1976.

247
Mites
15. Service, M. W., Medical Entomology for Students, Chapman and Hall, London, 1996, p.248.
16. Bartley, W. C. and Mellanby, K., The parasitology of human scabies (women andchildren), Parasitology, 35, 207, 1944.
17. Johnson, C. G. and Mellanby, K., The parasitology of human scabies, Parasitology, 34, 285,1942.
18. Buntin, D. M., Rosen, T., Lesher, J. L., Jr., Plotnick, H., Brademas, M. E., and Berger, T. G.,Sexually transmitted diseases: viruses and ectoparasites, J. Am. Acad. Dermatol., 25, 527,1991.
19. Arlian, L. G., Biology, host relations, and epidemiology of Sarcoptes scabei, Ann. Rev.Entomol., 34, 139, 1989.
20. Purvis, R. S. and Tyring, S. K., An outbreak of lindane-resistant scabies treated successfullywith permethrin 5% cream, J. Am. Acad. Dermatol., 25, 1015, 1991.
21. Juranek, D. D., Currier, R. W., and Millikan, L. E., Scabies control in institutions, inCutaneous Infestations and Insect Bites, Orkin, M. and Maibach, H. I., Eds., MarcelDekker, New York, 1985, chap. 18.
22. Paules, S. J., Levisohn, D., and Heffron, W., Persistent scabies in nursing home patients,J. Fam. Prac., 37, 82, 1993.
23. Meinking, T. L., Taplin, D., Hermida, J. L., Pardo, R., Kerdel, F. A., The treatment of scabieswith ivermectin, New Eng. J. Med., 333, 26, 1995.


249
Mosquitoes
CHAPTER 25
MOSQUITOES
TABLE OF CONTENTS
I. General and Medical Significance ..................................................................250A. Malaria ..........................................................................................................250B. Yellow Fever ...............................................................................................253C. Dengue Fever ..............................................................................................253D. Lymphatic Filariasis .....................................................................................254E. Other Human-Infesting Filarial Worms .....................................................255F. Encephalitides ..............................................................................................258
Eastern Equine Encephalitis ...................................................................258St. Louis Encephalitis .............................................................................258West Nile Encephalitis ...........................................................................258Western Equine Encephalitis .................................................................260LaCrosse Encephalitis .............................................................................260Other California Group Encephalitis .....................................................262Venezuelan Equine Encephalitis ...........................................................262Japanese Encephalitis .............................................................................262
G. Other arboviral diseases .............................................................................262Rift Valley Fever .....................................................................................262Ross River Disease .................................................................................262
II. Basic Biology/Ecology .....................................................................................263
III. General Description of Mosquitoes ................................................................265
IV. Discussion of Some Common U.S. Species...................................................268
V. Discussion of Some Major Pest Species in Other Areas ofthe World .........................................................................................................279
References ......................................................................................................................289

250
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
I. GENERAL AND MEDICALSIGNIFICANCE
Mosquitoes are by far the most important of thebloodsucking arthropods worldwide, causingannoyance and disease to humans, other mam-mals, and birds. Swarms of salt marsh mosqui-toes torment people living on seacoasts through-out the world. In those areas, it is not unusualto experience a mosquito landing rate of over200 mosquitoes per minute. Inland, rice fieldsand wetlands produce tremendous mosquitoproblems each year. Discarded automobile tires,ditches, bird baths, and paint cans are excellentmosquito breeding grounds in urban areas. Inmany cases normal outdoor work and otheractivities are often interfered with by swarms ofmosquitoes.
About 3,000 species of mosquitoes have beendescribed worldwide. Relatively few of themare significant vectors of human diseases; how-ever, the mosquito-transmitted disease problemworldwide is quite severe. Table 1 details bio-logical data on medically important mosquitoesin the U.S. Below is a brief description of someof the major mosquito-transmitted diseases.
A. Malaria
Malaria remains prevalent in several large areasof the world (especially so in Africa), resultingin staggering case numbers and millions ofdeaths (Figure 1). In 1986 there were an esti-mated 489 million cases of the disease world-wide and 2.3 million deaths.1 To make mattersworse, mosquito vectors of malaria are becom-ing resistant to many of the pesticides beingused to control them, and the malaria parasitesthemselves are becoming resistant to the pro-phylactic drugs used to prevent the disease.
Malaria in humans is caused by any one offour species of protozoans in the genus Plasmo-dium (P. vivax, P. malariae, P. ovale, and P.falciparum). The life cycle is quite complicatedand fraught with technical terms (Figure 2).Malaria parasites are acquired and transmittedto humans by bites from Anopheles mosquitoesonly. However, not every species of Anophelesis a vector; less than half of the 200 or so known
MOSQUITOES
Adult Mosquito (USDA, ARS, Agri.Hndbk. No. 182, 1961)
ImportanceAnnoyance and disease transmission
DistributionNumerous species worldwide
LesionPunctate hemorrhages, papular lesions,
or large wheals with edema
Disease Transmission#1 arthropod vector of disease agents —
malaria, dengue, encephalitis, etc.
Key ReferencesCarpenter, S. J. and Lacasse, W. J.,
University of California Press,Berkeley, 1955
Darsic, R. F. and Ward, R. A., Amer.Mosq. Control Assoc. (Book), Fresno,CA, 1981
TreatmentGenerally, palliative creams or lotions;
topical corticosteroids and antibioticcreams or ointments may be needed;oral antihistamines may be effectivein reducing symptoms of mosquitobites

251
Mosquitoes
OFTEN ASKED QUESTION
WHY CAN’T MOSQUITOES TRANSMIT THE AIDS VIRUS?
Because human immunodeficiency virus (HIV) is a blood-borne pathogen, concerns havebeen raised about the possible transmission of HIV by blood-feeding arthropods. Labora-tory studies and epidemiologic surveys indicate that this possibility is extremely remote. Forbiological transmission, the virus must avoid digestion in the gut of the insect, recognizereceptors on and penetrate the gut, replicate in insect tissue, recognize and penetrate theinsect salivary glands, and escape into the lumen of the salivary duct. In one study by Webband colleagues, the virus persisted for 8 days in bedbugs.1 Another study by Humphrey-Smith and colleagues2 showed the virus to persist for 10 days in ticks artificially fed mealswith high levels of virus (≥105 tissue culture infective doses per milliliter (TCID/ml), butthere was no evidence of viral replication. Intra-abdominal inoculation of bedbugs andintrathoracic inoculation of mosquitoes was used to bypass any gut barriers, but again thevirus failed to multiply.1 Likewise, in vitro culture of HIV with a number of arthropod celllines indicated that HIV was incapable of replicating in these systems. Thus, biologicaltransmission of HIV seems extremely improbable.
Mechanical transmission would most likely occur if the arthropod were interrupted whilefeeding, and then quickly resumed feeding on a susceptible host. Transmission of HIVwould be a function of the viremia in the infected host and the virus remaining on themouthparts or regurgitated into the feeding wound. The blood meal residue on bedbugmouthparts was estimated to be 7 × 10–5 ml, but 50 bedbugs, interrupted while feeding onblood containing 1.3 × 105 TCID/ml HIV, failed to contaminate the uninfected blood onwhich they finished feeding or the mouse skin membrane through which they refed.1
Within minutes of being fed blood with 5 × 104 TCID of HIV, stable flies regurgitated 0.2µl of fluid containing an estimated 10 TCID.3 The minimum infective dose for humanscontaminated in this manner is unknown, but under conditions such as those in sometropical countries where there are large populations of biting insects and a high prevalenceof HIV infection, transfer might be theoretically possible, if highly unlikely. In thesecountries, however, other modes of transmission are overwhelmingly important, and,although of fatal importance to the extremely rare individual who might contract HIVthrough an arthropod bite, arthropods are of no significance to the ecology of the virus.
An epidemiologic survey of Belle Glade, a south Florida community believed to have anumber of HIV infections in individuals with no risk factors, provided no evidence of HIVtransmission by insects.4 Interviews with surviving patients with the infections revealed thatall but a few had engaged in the traditional risk behavior (e.g., drug use and unprotectedsex). A serosurvey for exposure to mosquito-borne viruses demonstrated no significantassociation between mosquito contact and HIV status. Nor were repellent use, timeoutdoors, or other factors associated with exposure to mosquitoes related to risk of HIVinfection. A serosurvey for HIV antibodies detected no positive individuals between 2 and10 years of age or 60 and older. No clusters of cases occurred in houses without other riskfactors. There was thus no evidence of insect-borne HIV transmission.
REFERENCES1. Webb, P. A., Happ, C. M., Maupin, G. O., Johnson, B. J. B., Ou, C.-H., and Monath,
T. P., Potential for insect transmission of HIV: experimental exposure of Cimexhemipterous and Toxorhynchites amboinensis to human immunodeficiency virus, J.Infect. Dis., 60, 970, 1989.

252
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
2. Humphrey-Smith, I., Donker, G., Turzo, A., Chastel, C., and Schmidt-Mayerova, H.,Evaluation of mechanical transmission of HIV by the African soft tick, Ornithodorosmoubata, AIDS, 7, 341, 1993.
3. Brandner, G., Kloft, W. I., Schlager-Vollmer, Platten, E., and Neumann-Opitz, P.,Preservation of HIV infectivity during uptake and regurgitation by the stable fly,Stomoxys calcitrans, L. AIDS-Forschung., 5, 253, 1992.
4. Castro, K. G., Lieb, S., Jaffe, H. W., et al., Transmission of HIV in Belle Glade,Florida: lessons for other communities in the United States, Science, 239, 193, 1988.
(Adapted from: McHugh, C. P., Lab. Med., 25, 436, 1994, Copyright 1994, by the AmericanSociety of Clinical Pathologists. With permission.)
Table 1Biological Data on Medically Important Mosquitoes in the U.S.a
Larval Biting Flight DiseaseMosquito Species Habitat(s)b Timec Ranged Agente
(mi)
Aedes aegypti AC C, D <0.5 DG, YFA. albopictus AC, TH D <0.5 DG, YF, (CE), (WNV)Ochlerotatus dorsalis SM, LM D 10–20 (WEE)O. melanimon IP, FW D 1–2 WEE, CEO. mitchellae GP, FW D .5–1 (EEE)O. nigromaculis IP, FW D 1–2 (WEE), (CE)O. sollicitans SM C 5–10 EEEO. taeniorhynchus SM C, N 5–10 VEE, (CE)O. triseriatus TH, AC D .5–1 CEO. trivittatus GP, WP, FW C, N .5–1 CEA. vexans FW, GP, IP C, N 1–5 CE, (EEE)Anopheles crucians SM, FS, LM C 1–2 (M), (VEE), (EEE)A. freeborni RF, DD C 1–2 M, (WEE), (SLE)A. quadrimaculatus FW, GP, LM C .5–1 MCoquillettidia perturbans FS, GP, LM C, N 1–2 EEE, (VEE)Culex nigripalpus GP, FW, DD C .5–1 SLE, (WNV)C. pipiens/quinquefasciatus AC, SCB, GRP C, N <0.5 SLE, WNV, (WEE), (VEE)C. restuans WP, GRP, DD C, N 1–2 WNV, (EEE), (WEE)C. salinarius GP, LM, FS C, N 1–5 WNV, (EEE)C. tarsalis IP, RF, GRP C, N 1–2 WEE, SLECuliseta inornata GRP, DD C, N 1–2 (WEE), (CE)C. melanura FS, WP C, N .5–1 EEEMansonia titillans FS, GP, LM C, N 1–5 (VEE)Psorophora columbiae IP, RF, GRP C, N 1–5 VEEP. discolor IP, RF, GRP C, N 1–5 VEE
a Adapted from U.S. Air Force Mosquito Surveillance Data.b AC = artificial containers; DD = drainage ditches; FS = freshwater swamps; FW = flood waters; GP =
grassland pools; GRP = ground pools; IP = irrigated pastures; LM = lake margins; RF = rice fields; SCB = sewercatch basins; SM = salt marshes; TH = tree holes; WP = woodland pools.
c C = crepuscular (dusk and dawn); D = day; N = night.d Values given are estimates of normal flight ranges. For some species, seasonal migratory flights may be 10
times these values.e Parentheses indicate secondary or suspected vectors, otherwise, primary vectors. CE = California group
encephalitis; DG = dengue; EEE = Eastern equine encephalitis; M = malaria; SLE = St. Louis encephalitis; VEE= Venezuelan equine encephalitis; WEE = Western equine encephalitis; WNV = West Nile virus; YF = yellowfever.

253
Mosquitoes
species are considered vectors. Falciparum malaria is the worst of the four species andis often fatal in infants and young children. Most malaria occurring in the U.S. each yearis a result of people having relapses from former cases or from cases recently acquiredin foreign countries where malaria is endemic (introduced malaria). During 1988, therewere 1,023 malaria cases reported in the U.S. — 991 of them were introduced cases.2
B. Yellow fever
Yellow fever (YF), is probably the most lethal of all the arboviruses and has had adevastating effect on human social development. The causative agent, a flavivirus,occurs in Africa and South and Central America, and is maintained in a sylvatic formamong monkeys by forest or scrub mosquitoes. An urban form of the disease occurswhen humans become infected and transmission occurs from person to person byAedes aegypti. Mild cases may be characterized by fever, headache, generalized achesand pains, and nausea. Persons with severe YF may exhibit high fever, headache,dizziness, muscular pain, jaundice, hemorrhagic symptoms, and profuse vomiting ofbrown or black material. There is often collapse and death. Even though there is aneffective vaccine, the WHO estimates that 200,000 people are infected with YF everyyear, resulting in 30,000 deaths.3,4 Many large epidemics have occurred in the past,especially during the time of exploration of the New World. For example, 20,000 of27,000 British troops were killed by YF during an expedition to conquer Mexico in1741.
C. Dengue fever
Dengue fever, caused by a virus in the family Togaviridae, is responsible for wide-spread morbidity (breakbone fever) and some mortality (dengue hemorrhagic fever,DHF) in much of the tropics and subtropics each year (Figure 3). There are four closelyrelated, but antigenically distinct, virus serotypes (DEN-1, DEN-2, DEN-3, and DEN-4).DHF (sometimes called Dengue Shock Syndrome in its most severe form) is ahemorrhagic complication occuring mostly in children, and is thought to be a result ofsequential infection by more than one dengue serotype and/or variations in viral
Figure 1Approximate worldwide distribution of malaria (from: Florida Dept. Health andRehabilitative Services).

254
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Fig
ure
2Li
fe c
ycle
of
ma
lari
a.
(Fro
m:
U.S
. N
avy
“G
uid
e to
Ma
lari
a P
reve
nti
on a
nd
Con
trol
”.)

255
Mosquitoes
virulence. Most dengue infections result in relatively mild illness characterized by fever,headache, myalgia, rash, nausea, and vomiting. However, DHF is often severe and ischaracterized by petechiae, purpura, mild gum bleeding, nosebleeds, gastrointestinalbleeding, and dengue shock syndrome. The case fatality rate of DHF in most countriesis about 5%, with most deaths occurring among children. In one recent study of DHFin the Cook Islands, deaths occurred in patients 14 to 22 years old and were due toacute upper gastrointestinal bleeding.5 The virus is transmitted between humans by A.aegypti and A. albopictus. Dengue fever seems to be increasing in prevalence andgeographic distribution, especially in southeast Asia, India, the Caribbean, and Centraland South America. As many as 100 million cases of dengue occur annually, and severalhundred thousand cases of DHF.6
D. Lymphatic filariasis
Lymphatic filariasis (Figure 4) is an important human disease occurring in much of theworld. Malayan filariasis, caused by Brugia malayi, is mostly confined to southeast Asia,and the Bancroftian form, Wucheria bancrofti, is prevalent over much of the tropicalworld. The World Health Organization estimated that 250 million cases of Bancroftian orBrugian filariasis occurred worldwide in 1974.7 There was at one time a small endemiccenter of human filariasis near Charleston, S.C. that has apparently disappeared. How-ever, we still have an efficient vector in the U.S., Culex quinquefasciatus, that couldtransmit the filarial worms should an introduction occur. Bancroftian filariasis is aninteresting disease in that there is no other known vertebrate host of the worms. It istransmitted solely by mosquitoes, and there is no multiplication of the parasite in themosquito vector.8 In addition, the adult worms may live up to 10 years in humans.8
Figure 3Worldwide distribution of dengue, 1993 (from: U.S. DHHS, PHS, CDC, MMWR, 43, No. SS-2, July22, 1994).

256
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 4Life cycle of Wuchereria bancrofti (reprinted with permission of Macmillian PublishingCompany from ESSENTIALS OF MEDICAL PARASITOLOGY by Thomas J. Brooks, Jr. Copyright(c) 1963 Thomas J. Brooks, Jr.).
E. Other human-infesting filarial worms
Numerous filarial worms are transmitted to humans and other mammals by mosquitoesand black flies. Examples include the causative agents of Bancroftian and Malayanfilariasis (discussed above), loiasis, onchocerciasis, and dirofilariasis (dog heartworm).

257
Mosquitoes
CASE HISTORY
FATAL CASE OF MOSQUITO-TRANSMITTED ENCEPHALITIS
An 11-year-old Native American from an Indian community developed a fever of 103˚F anddiarrhea on the 31st of July. Gastroenteritis was reportedly “going around” in the commu-nity at the time. He was taken to a local emergency room and given symptomatic treatment.He was somewhat better until the night prior to admission when he developed a headache,stomachache, and decreased appetite. He went to bed early, which was unusual for him.The next morning he went with his family to a scheduled ophthalmologic exam and sleptmost of the 1 h drive. He was drowsy and nauseated on arrival at the clinic, then “turnedpale” and began grand mal seizure activity. He was taken to the emergency room, loadedwith Dilantin and transferred to the admitting hospital. On admission, he was responsivebut lethargic. His admission temperature was 102.2˚F. His admission laboratory showed awhite blood cell count of 19,500 with 59% neutrophils, 19% band forms, and 16%lymphocytes. The hematocrit was 34.4% and the serum glucose with 184 mg per 100 ml.Spinal fluid showed a white blood cell count of 980, with 91% neutrophils, no organismsseen on gram stain, negative latex agglutination, a protein of 68, and a glucose of 105 mgper 100 ml. Additional blood, spinal fluid, and stool cultures were obtained. The patientwas placed on Claforan and Dilantin. He remained febrile up to 105˚F, but became moreresponsive and was ambulatory by the second day after admission. At approximately 2P.M., the 5th of August, the patient experienced another seizure with eye deviation to theright and head turning to the right. CT showed enhancement of the cisterna, but only mildincreased intracranial pressure. Respirations became irregular and the patient was elec-tively intubated and hyperventilated. He was started on Streptomycin, PZA, and INH forpossible TB, and Acyclovir for possible CNS herpes. His condition deteriorated over thenext 24 hours until he showed no evidence of brain stem function. A lumbar puncture wasperformed for viral studies as none of his previous cultures were growing. He was taken offthe ventilator the evening of August 6th. At autopsy the patient’s meninges were relativelyclear, but cerebral edema was present. Confirmation of infection with eastern equineencephalitis (EEE) virus was made by the CDC (Ft. Collins); two separate serum samplesindicated a fourfold rise in HI antibody to EEE virus and ELISA tests indicated presence ofspecific IgM.
Comment: Investigation of this EEE case revealed several interesting features. The patientlived in a house without window screens. This likely led to increased exposure to mosqui-toes (and thus, biting) — a risk factor for any mosquito-borne disease. An environmentalsurvey of the Indian community revealed numerous prime Coquillettidia perturbans (thesuspected mosquito vector in this case) breeding sites. In addition, C. perturbans werecollected by CDC light traps in the community at the time of the survey. No other knownvectors of EEE virus were collected. Finally, mosquito trapping a year later (same month aspatient’s infection) at the Indian community revealed that this species was the predominantspecies in the area.
(Adapted from J. Agromed. 2, 53, 1995, Copyright 1995, the Hayworth Press, Binghamton,NY. With permission.)
Other filarial worms may or may not cause symptomatic disease and are less wellknown (and thus have no common name), such as Mansonella ozzardi, M. streptocerca,M. perstans, Dirofilaria tenuis, D. ursi, D. repens, and others. Beaver and Orihel9
reported 39 such cases that were caused by Dirofilaria immitis (dog heartworm), otherDirofilaria sp., Dipetalonema sp., and Brugia sp.

258
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
The dog heartworm, Dirofilaria immitis, occurs mainly in the tropics and subtropicsbut also extends into southern Europe and North America. This worm infects severalcanid species, sometimes cats, and, rarely, humans. Numerous mosquito species arecapable of transmitting dog heartworm, especially those in the genera Aedes, Ochlerotatus,Anopheles, and Culex. Mosquitoes pick up the microfilariae with their blood meal whenfeeding on infected dogs. In endemic areas, a fairly high infection rate may occur inlocal mosquitoes.
Undoubtedly, thousands of people in the U.S. are bitten each year by mosquitoesinfected with D. immitis. Fortunately, humans are accidental hosts, and the larvaeusually die. However, they may occasionally be found as a subadult worm in the lung(seen as a coin lesion on x-ray exam).10 The incidence of dog heartworm in humansmay well be decreasing in the U.S. because of widespread — and fairly consistent —treatment of domestic dogs for heartworm. The closely related D. tenuis is commonlyfound in the subcutaneous tissues of raccoons (again, mosquito-transmitted) and mayaccidentally infest humans as nodules in subcutaneous tissues.
F. Encephalitides
In temperate North America, the worst mosquito-borne diseases are probably theencephalitides. Certainly not all cases of encephalitis are mosquito-caused (enterovi-ruses and other agents are often involved), but mosquito-borne encephalitis haspotential to become a serious cause of morbidity and mortality covering widespreadgeographic areas each year.
Eastern equine encephalitis. Eastern equine encephalitis (EEE) is generally the mostvirulent, being severe and frequently fatal (mortality rate 30 to 60%). Fortunately, largeand widespread outbreaks are not common; between 1961 and 1985 only 99 humancases were reported.11 EEE occurs in late summer and early fall in the central andnorthcentral U.S., parts of Canada, southward along the coastal margins of the easternU.S. and the Gulf of Mexico, and sparsely throughout Central and South America. Theecology of EEE is poorly understood. The virus circulates in wild bird populations, butthe exact mechanism of spread to humans is largely speculative. The mosquitoesOchlerotatus sollicitans, Coquillettidia perturbans, and possibly A. vexans may beinvolved.
St. Louis encephalitis. St. Louis encephalitis (SLE) produces lower mortality ratesthan EEE (3 to 20%), but it occurs occasionally in large epidemics in much of the U.S.Like EEE, most cases occur in late summer (Figure 5). In 1933 there were 1,095 casesin St. Louis with more than 200 deaths.12 From 1975 to 1976 there were over 2,000 casesreported from 30 states, primarily in the Mississippi valley.12 SLE is a bird virus that istransmitted by C. tarsalis (western and southwestern U.S.), C. quinquefasciatus (centralU.S.), and C. nigripalpus (Southeastern U.S.) (Figure 6).
West Nile encephalitis. West Nile virus (WNV) was identified for the first time inthe Western Hemisphere in New York in 1999. By the end of the year, the virus hadcaused encephalitis in 62 people and numerous horses in and around New York City,resulting in 7 human and 10 equine deaths.13 The virus continued to spread insubsequent years, and now evidence of WNV has been found in at least 43 states andthe District of Columbia. WNV will likely eventually occur throughout the United Statesand down into Central and South America. As far as severity of the disease, WNV isno more dangerous than SLE (one of our “native” encephalitis viruses). Like SLE, WNVis more dangerous to older patients. Interestingly, of the first five patients in New York

259
Mosquitoes
Figure 5Case numbers of California serogroup (CE) encephalitis, eastern equineencephalitis (EEE), and St. Louis encephalitis (SLE), showing appearanceof cases in mid-to-late summer (from: U.S. DHHS, Publ. No. [CDC] 93–8017).

260
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
City admitted to hospitals, four had severe muscle weakness and respiratory difficulty,a finding atypical for encephalitis.14 Also, GI complaints such as nausea, vomiting, ordiarrhea occurred in 4 of 5 patients.14 Much is yet unknown about the ecology of WNVin the United States, but we do know the virus causes a bird disease, and is transmittedby mosquitoes. The house sparrow has been found to be one of the best amplifyinghosts in nature, producing highest viremias for the longest period of time. Although thevirus has been isolated from many mosquito species, the main vectors are believed tobe Culex pipiens, Cx. quinquefasciatus, Cx. salinarius, and possibly Ochlerotatusjaponicus.
Western equine encephalitis. Western equine encephalitis (WEE), occurring in thewestern and central U.S., parts of Canada, and parts of South America, has occurredin several large outbreaks. There were large epidemics in the north central U.S. in 1941and in the central valley of California in 1952. The 1941 outbreak involved 3,000 cases.During 1964–1997, there were 639 human WEE cases reported to the CDC, for anational average of 19 cases per year.15 WEE is generally less severe than EEE and SLE,with a mortality rate of only 2 to 5%. Cases appear in early to midsummer, and areprimarily due to bites by infected Culex tarsalis mosquitoes.
LaCrosse encephalitis. LaCrosse encephalitis (LAC) has historically affected chil-dren in the midwestern states of Ohio, Indiana, Minnesota, and Wisconsin. However,it is increasingly being diagnosed in the southern states. The mortality rate of LAC isgeneraly less than 1%, but seizures (even status epilepticus) and cerebral herniationmay result from LAC infection. In fact, most LAC patients present with seizures. Thenational average for LAC is 73 per year.15 Cases occur in July, August, and September.LAC is a bunyavirus that is transmitted to humans by Ochlerotatus triseriatus. Interest-
Figure 6Life cycle of St. Louis encephalitis.

261
Mosquitoes
CASE HISTORY
SEIZURES ASSOCIATED WITH LACROSSE ENCEPHALITIS
In late June of 1999, a six-month-old, previously healthy infant was brought to an emer-gency department (ED) with a several-hour history of fever up to 101.6°F. He was experi-encing a focal seizure characterized by uncontrollable blinking of the left eye, twitchingof the left side of the mouth, and random tongue movement. In the ED, seizures continuedintermittently in spite of the administration of diazepam and lorazepam. The infant wasstarted on phenytoin and admitted to the hospital. Examination of CSF upon admissionshowed 294 white blood cells (47% polymorphonuclear leukocytes, 41% histiocytes, 12%lymphocytes), and 3 red blood cells. Protein and glucose were within normal limits.Admission CT scan was read as normal. The infant was started on acyclovir because of thepossibility of herpes encephalitis, and cefotaxime and vancomycin were also initiated tocover possible bacterial infection. The patient then became seizure-free. He was taken offintravenous phenytoin and started on oral phenobarbital. Focal seizures, which progressedto generalized tonic clonic seizures, recurred on the fourth hospital day, at which time hehad a therapeutic level of phenobarbital. After a repeat CT scan, which was read as withinnormal limits, the child was transferred to another hospital. On admission, the infant wasnoted to have continuous seizure-like movements of the chin and face. A repeat lumbarpuncture revealed 307 white blood cells (33% polymorphonuclear leukocytes, 29% lym-phocytes, and 38% histiocytes), 812 red blood cells, a protein of 104 mg/dl and a glucoseof 74 mg/dl. He was continued on acyclovir, cefotaxime, and vancomycin. The patient wasintubated secondary to excessive secretions and to avoid respiratory compromise. He wasagain treated with lorazepam and restarted on phenytoin. Seizure activity ended. Thepatient continued to be intermittently febrile. He was extubated on the sixth continuoushospital day. Herpes PCR results from admission samples were negative. In addition,admission blood, urine, and CSF cultures were negative, and on the ninth hospital day,cefotaxime and vancomycin were discontinued. Patient’s maximum temperature on thatday was 100.1°F, and he was becoming more alert and playful. The patient subsequentlybecame and remained afebrile and without seizure activity, so he was transferred back tothe original hospital on the twelfth hospital day for completion of 21 days of intravenousacyclovir. On Day 21 he was discharged home on oral phenytoin. He had some residualleft-sided weakness requiring several weeks of physical therapy. A sample of CSF was sentto a reference laboratory for testing for antibodies to various encephalitis agents includingherpes and arboviruses. Results showed an indirect fluorescent antibody titer of 1:8 toLaCrosse (LAC) virus. Serum was sent to CDC for confirmation, which showed the presenceof IgM antibody to LaCrosse virus.
Comment: Differentiation of LAC infection must be made from other encephalitides (post-vaccinal or post-infection), tick-borne encephalitis (not common in the U.S.), rabies,nonparalytic polio, mumps meningoencephalitis, aseptic meningitis from enteroviruses,herpes encephalitis, various bacterial, mycoplasmal, protozoal, leptospiral, and mycoticmeningitides or encephalitides, and others. Any cases of encephalitis in late summer shouldbe suspect. Specific identification is usually made (with the help of the Centers for DiseaseControl in Ft. Collins) by finding specific IgM antibody in acute serum or CSF, or antibodyrises (usually HI test) between early and late serum samples. Serological identification ofthe particular virus is complicated because of cross-reactivity with heterologous viruses ofthe same group. For example, IgM antibody from patients with LAC virus infection has thehighest titers to LAC virus itself, but also reacts to a lesser extent with Snowshoe Hare virusand to a still lesser extent with Jamestown Canyon virus (two other viruses within theCalifornia serogroup).

262
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
ingly, the virus may be transferred from adult female O. triseriatus to her offspringthrough ovarial contamination. Some amplification of the virus takes place in naturethrough an O. triseriatus, wild vertebrate cycle.
Other California group encephalitis. Although LAC (above) encephalitis is prob-ably the most notorious, several other California group encephalitis viruses exist. NorthAmerican forms include California encephalitis (CE), Jamestown Canyon (JC), JerrySlough (JS), Keystone (KEY), San Angelo (SA), Trivittatus (TVT), and others. Viruses inthe California serogroup are primarily pathogens of rodents and lagomorphs. They aretransmitted to people by several species of mosquitoes, but especially the tree-hole,floodwater, and snow pool mosquitoes in the genera Ochlerotatus and Aedes spp.California group encephalitis viruses generally produce only mild illness in humans(mortality rates 1% or so).
Venezuelan equine encephalitis. Venezuelan equine encephalitis (VEE) is relativelymild in humans and rarely affects the central nervous system, but it will be included hereas an encephalitid. VEE is endemic in Mexico and Central and South America; epidemicsoccasionally reach the southern U.S. Cases generally appear during the rainy season.Although the mortality rate is generally <1%, significant morbidity is produced by thisvirus. In an outbreak in Venezuela from 1962 to 1964, there were more than 23,000reported human cases with 156 deaths.16 In 1971, an outbreak of VEE in Mexico extendedinto Texas resulting in 84 human cases.17 There was a more recent outbreak in Colombiaand Venezuela during the summer of 1995 with 75,000 to 100,000 human cases.18
Japanese encephalitis. Japanese encephalitis (JE) does not occur in the U.S., butit is the principal cause of epidemic viral encephalitis in the world, with approximately45,000 clinical cases occurring annually.19 JE epidemics have, at times, been widespreadand severe. In 1924 there were 6,125 cases with 3,797 deaths.20 Historically, JE has beenfocused in the northern areas of countries in southeast Asia, East Asia, and midsouthernAsia, especially China and Vietnam. Recently there has been a steady westwardextension of reported epidemic activity into northern India, Nepal, and Sri Lanka, anda southern movement into Australia. JE is highly virulent. Approximately 25% of thecases are rapidly fatal, 50% lead to neuropsychiatric sequelae, and only 25% fullyrecover.19 In temperate zones JE has a summer–fall distribution, but in the tropics noseasonal peak is apparent. There are several mosquito vectors of JE, but probably themost important is Culex tritaeniorhynchus, a rice-field-breeding species.
G. Other arboviral diseases
Rift Valley fever. Rift Valley fever (RVF), occurring throughout sub-Saharan Africa andEgypt, is a Phlebovirus in the family Bunyaviridae. It causes abortions in sheep, cows,and goats, and heavy mortality of lambs and calves. In humans, it may result in fever,myalgias, encephalitis, hemorrhage, or retinitis. Permanent visual impairment has beenreported.16 Huge epidemics occasionally occur; in 1950 to 1951, there were anestimated 100,000 sheep and cattle cases and at least 20,000 human cases.16 Outbreakscontinue: in 1998 there were 27,500 human cases and 170 deaths from RVF in Kenya.21
Although RVF may be acquired by handling infective material of animal origin duringnecropsy or butchering, it is also transmitted by mosquitoes, especially Ochlerotatus/Aedes mosquitoes.
Ross River virus disease. Ross River (RR) disease, also called epidemic polyarthritis,occurs throughout most of Australia and occasionally New Guinea and some PacificIslands such as Fiji, Tonga, and the Cook Islands. It causes fever, headache, fatigue,

263
Mosquitoes
rash, and — most notably — arthritis in the wrist, knees, ankles, and small joints ofthe extremities. The disease is not fatal, but may be debilitating with symptomsoccurring for weeks or months. RR disease is the most common arboviral disease inAustralia with >5000 cases annually. During 1997, there were 6683 cases reported.22
Peak incidence of RR occurs from January through March, when the mosquito vectorsare most abundant. Serological studies and laboratory research have indicated that mostlikely kangaroos and wallabies are natural hosts for RR virus. There are severalmosquito vectors of RR virus in Australia, but particularly Culex annulirostris inlandand Ochlerotatus vigilax and O. camptorhynchus in northern and southern coastalareas, respectively.
II. BASIC BIOLOGY/ECOLOGY
Mosquitoes undergo complete metamorphosis, having egg, larval, pupal, and adult stages(Figure 7). Larvae are commonly referred to as wigglers and pupae as tumblers. Larvaeand pupae of mosquitoes are always found in water. The water source may be anythingfrom water in discarded automobile tires to water in the axils of plants, to pools, puddles,swamps, and lakes. Mosquito species differ in their breeding habits, biting behavior, flightrange, etc. However, a generalized description of their life cycle is presented here andwill serve as a useful basis for understanding mosquito biology and ecology. Most larvaein the subfamily Culicinae hang down just under the water surface by a breathing tube(siphon), whereas anopheline larvae lie horizontally just beneath the water surfacesupported by small notched organs of the thorax and clusters of float hairs along theabdomen. They have no prominent siphon. Mosquito larvae feed on suspended particlesin the water as well as microorganisms. They undergo four molts (each successively
Figure 7Mosquito life stages.

264
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
larger), the last of which results in the pupal stage. With optimum food and temperatureconditions, the time required for larval development can be as short as 7 days.
Mosquito pupae are quite active and will “tumble” toward the bottom of their watersource upon disturbance. Pupae do not feed. They give rise to adult mosquitoes in 2to 4 days. This process begins with the splitting of the pupal skin along the back. Theemerging adult must dry its wings and separate and groom its head appendages beforeit can fly away (Figure 8). This is a critical stage in the survival of mosquitoes. If thereis too much wind or wave action, the emerging adult will fall over while leaving itsskin, becoming trapped on the water surface to soon die.
Adult mosquitoes of both sexes obtain nourishment for basic metabolism and flightby feeding on nectar. In addition, females of most species obtain a blood meal frombirds or mammals for egg development. Breeding sites selected for egg laying differby species, but generally mosquitoes can be divided into three major breeding groups:permanent water breeders, floodwater breeders, and artificial container/tree holebreeders. Anopheles and many Culex mosquitoes select permanent water bodies, suchas swamps, ponds, lakes, and ditches that do not usually dry up. Floodwater mosqui-toes lay eggs on the ground in low areas subject to flooding. During heavy rains, watercollecting in these low areas covers the eggs, which hatch from within minutes up toa few hours. Salt marsh mosquitoes (Ochlerotatus sollicitans), inland floodwatermosquitoes (A. vexans), and dark rice field mosquitoes (Psorophora columbiae) areincluded in this group. Artificial container/tree hole breeders are represented by yellowfever mosquitoes (A. aegypti), Asian tiger mosquitoes (Aedes albopictus), tree holemosquitoes (O. triseriatus), and others. However, several species of Anopheles andCulex may also occasionally oviposit in these areas. Some of these container-breedingspecies lay eggs on the walls of a container just above the water line. The eggs areflooded when rains raise the water level. Other species oviposit directly on the watersurface.
Figure 8Adult mosquito emerging from pupal stage. (From: Miss. Dept. Health Publ. “The Mosquito Book”,E. Bowles.)

265
Mosquitoes
Female Anopheles mosquitoes generally lay eggs on the surface of the water at night.Each batch usually contains 100 to 150 eggs. The Anopheles egg is cigar shaped, about1 mm long, and bears a pair of air-filled floats on the sides. Under favorable conditions,hatching occurs within 1 or 2 days.
Aedes and Ochlerotatus mosquitoes lay their eggs on moist ground around the edgeof the water or, as previously mentioned, on the inside walls of artificial containers justabove the water line. Aedes and Ochlerotatus eggs will die if they become too dry whenfirst laid. However, after the embryo in the egg develops, the eggs can withstand dryconditions for long periods of time. This trait has allowed Aedes and Ochlerotatusmosquitoes to use temporary water bodies for breeding, such as artificial containers,periodically flooded salt marshes or fields, tree holes, and storm water pools. Also,Aedes mosquitoes have inadvertently been carried to many parts of the world as dryeggs in tires, water cans, or other suitable containers. The Asian tiger mosquito (A.albopictus) was introduced into the U.S. in the 1980s in shipments of used truck tirecasings imported from Taiwan and Japan. Once these tires were stacked outside andbegan to collect rainwater, the eggs hatched.
Psorophora mosquitoes also lay dry-resistant eggs. These mosquitoes are often a majorproblem species in rice fields. Eggs are laid on the soil and hatch once the field is irrigated.
Culex mosquitoes lay batches of eggs that are attached together to form little floatingrafts. Upon close inspection of a suitable breeding site, these egg rafts can often be seenfloating on the surface of the water.
In tropical areas, mosquito breeding may continue year round, but in temperateclimates many species undergo a diapause in which the adults enter a dormant statesimilar to hibernation. In preparation for this, females become reluctant to feed, ceaseovarian development, and develop fat body. They may seek a protected place to passthe approaching winter. Some species, instead of passing the winter as hibernatingadults, produce dormant eggs that can survive the harsh effects of winter.
Mosquitoes vary in their biting patterns as well. Most species are diurnal in activity,biting mainly in the early evening. However, some species, especially A. aegypti andA. albopictus, bite in broad daylight (although there may be a peak of biting very earlyand late in the day). Others, such as the salt marsh species and many members of thegenus Psorophora do not ordinarily bite during the day but will attack if disturbed (suchas walking through high grass harboring resting adults).
III. GENERAL DESCRIPTION OF MOSQUITOES
Adult mosquitoes can be distinguished from other flies by several characteristics (Figure9 is provided to familiarize the reader with these characteristics) (see also Color Figure25-19). They have long, 15-segmented antennae, a long proboscis for bloodsucking,and scales on the wing fringes and wing veins. Scale patterns on the “back” (scutum)of mosquitoes can sometimes be used to identify the species (Figure 10). The mosquitohead is rounded, bearing large compound eyes that almost meet. Males can usually beseparated from females by their bushy antennae (Figures 11C,D). Female Anophelesmosquitoes have palpi as long as the proboscis (Figure 11B); other groups do not havethis characteristic. Larval mosquitos, commonly called “wiggle tails” or “wigglers,” arewhite to dark gray in color and possess no legs or wings. They bear simple or branchedtufted hairs along the body, anal gills, antennae, and chewing mouthparts. Culicinelarvae have a prominent siphon tube for respiration at the water surface. Anopheline

266
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 9Adult mosquito with parts labeled (from: U.S. DHEW, PHS, CDC, Pictorial Keys).

267
Mosquitoes
Figure 10Examples of thoracic markings of mosquitoes (not necessarily drawn to scale): (a) Aedes aegypti,(b) Ochlerotatus infirmatus, (c) O. atlanticus, (d) O. thibaulti, (e) O. trivittatus, (f) O. triseriatus,(g) Psorophora varipes, (h) P. ciliata, (i) Orthopodomyia signifera, (j) Uranotaenia sapphirina,(k) Culex restuans. (From: USDA, ARS, Agri. Hndbk. No. 173, 1960.)

268
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
species do not, and thus must lie horizontally just beneath the water surface. Pupalmosquitoes, often called “tumblers,” also occur in water. They are comma-shaped, withtwo prominent respiratory trumpets on the thorax and a set of paddles on the lastabdominal segment.
IV. DISCUSSION OF SOME COMMON U.S. SPECIES*
Yellow Fever MosquitoAedes aegypti (Linnaeus)
Medical Importance: Known vector of yellow fever and dengue fever
Distribution: Cosmotropical in distribution, occurring worldwide within the 20°Cisotherms (Figure 12)
Figure 11Mosquito head and appendages: Aedes female (A), Anopheles female (B), Aedes male (C), andAnopheles male (D) (from: USDA, ARS, Tech. Bull. No. 1447).
* The descriptions for each mosquito species are only general comments about their macroscopic appearance.Mosquito identification to the species level is quite difficult, utilizing a number of microscopic character-istics. Specific identifications should be performed by specialists at institutions that routinely handle suchrequests (universities, extension services, state health departments, the military, etc.).

269
Mosquitoes
Figure 12Approximate geographic distribution of Aedes aegypti.
Description: Typical Aedes mosquito with a pointed abdomen (at tip) and black andwhite rings on the legs. Small black species with a silver-white lyre-shaped figure onthe upper sides of its thorax (Figure 13); also silver-white bands on the hind tarsi andabdomen
Remarks: Breeds in shaded artificial containers around buildings such as tires, cans,jars, flower pots, and gutters; usually bites during the morning or late afternoon; readilyenters houses and prefers human blood meals, biting principally around the ankles orback of the neck; flight range from 100 feet to 100 yards; in many places where A.albopictus has been introduced, this species has virtually disappeared, apparently beingdisplaced
Figure 13Adult Aedes aegypti.

270
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 15Adult Aedes albopictus.
Asian Tiger MosquitoAedes albopictus (Skuse)
Medical Importance: Aggressive, daytime biting mos-quito often found associated with piles of used automo-bile tires; vector of the agents of yellow fever and denguefever; has been found naturally infected with LaCrosseencephalitis virus
Distribution: Widely distributed in the Oriental re-gion, the Hawaiian Islands, and parts of the eastern U.S.,where it was accidentally introduced in 1986 (Figure 14);recently reported from the African continent (Nigeria)
Description: Very similar in appearance to A. aegypti witha black body and silver-white markings (Figure 15); majordifference between the two: A. albopictus has a single, silver-white stripe down the center of the dorsum of the thorax(instead of the lyre-shaped marking)
Remarks: Breeds in artificial containers such as cans, gutters, jars, tires, flower pots,etc., seems especially fond of discarded tires; aggressive mosquito, often landing andbiting immediately; flight range is generally less than a quarter mile
Figure 14Approximate geographic distribution of Aedes albopictus.

271
Mosquitoes
The Salt Marsh MosquitoOchlerotatus sollicitans (Walker)
(Note: Reinert23 recently reclassified many Aedesspecies as genus Ochlerotatus)
Medical Importance: Fierce biter; can often dis-courage coastal development (in Louisiana, one of themost important pest species in coastal parishes13);known vector of the agent of EEE
Distribution: Nearctic region along the easterncoastal and inland saline areas (Figure 16)
Description: Bronze-brown species with goldenyellow markings (Figure 17); whitish-yellow bands onupper side of abdomen with yellowish stripe downcenter; short palps with small white tips, banded legs,and dark proboscis with a single band in the middle
Remarks: Breeds primarily in salt marshes floodedby tides or rain; breeds throughout the year, althoughdevelopmental time is longer in winter; aggressive
biter that feeds at night (however, adults rest on vegetation during the day and willreadily bite when disturbed); flight range is between 5 and 10 miles
Figure 16Approximate geographic distribution of Ochlerotatus sollicitans.
Figure 17Adult Ochlerotatus sollicitans.

272
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
The Inland Floodwater MosquitoAedes vexans (Meigen)
Medical Importance: Bothersome pest and pos-sibly vector of EEE virus
Distribution: Holarctic and Oriental regions, Pa-cific Islands, Transvaal region, Mexico, and parts ofCentral America (Figure 18)
Description: Typical Aedes mosquito with apointed abdomen (at tip) and black and white ringson the legs. Medium-sized brown to golden brownmosquito with light gray or white markings shapedlike wide “B’s” on the dorsum of the middle seg-ments of abdomen (Figure 19); hind tarsi with nar-row white rings on all segments and short and darkpalps with a few white scales at the tip
Remarks: Breeds in any temporary body of freshwater in both wooded and openareas; many broods produced each year from May through September when breedingareas are flooded by rains; vicious biter, active mainly at dusk and just after dark; flightrange is 5 to 10 miles
Figure 18Approximate geographic distribution of Aedes vexans.
Figure 19Adult Aedes vexans.

273
Mosquitoes
Figure 21Adult Anopheles quadrimaculatus.
Figure 20Approximate geographic distribution of Anopheles quadrimaculatus.
Malaria MosquitoAnopheles quadrimaculatus Say
Medical Importance: One of many Anophelesmosquitoes that can transmit the agent of malaria tohumans; principal vector in the eastern half of U.S.(in early 20th century when malaria was commonin U.S.)
Distribution: Central and eastern U.S., southernCanada, and Mexico (Figure 20)
Description: Actually five sibling species (namedA, B, C1, C2, D) which all look alike, but differ inbehavior and ecology; medium to large dark brownmosquitoes with palps as long as the proboscis,dark unbanded legs, and wings marked by fourdark spots (Figure 21); long maxillary palps in bothsexes (typical characteristics of all Anopheles mos-
quitoes); feed with their proboscis, head, and body in an almost straight line (manyspecies feed almost perpendicular to skin surface of host) — it looks like they arestanding on their heads when they bite [Figure 22] (also characteristic of all Anophelesmosquitoes)
Remarks: Breed in permanent freshwater sites such as ponds, pools, swamps, andrice fields containing emergent or floating vegetation (as most Anopheles mosqui-toes); breeding may be continuous throughout year, especially if mild winters;however, peak populations usually during July or August (decline rapidly duringSeptember and October); adults rest during the day in cool, dark, damp areas andcome out to feed at night; adults usually fly no more than 4 miles from their breeding area

274
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Culex nigripalpus Theobald
Medical Importance: Major vector of SLEvirus in the southeastern U.S. (in 1990, centraland southern counties of Florida experiencedoutbreak of 212 cases with 10 deaths25)
Distribution: Southern U.S., Antilles,Mexico, Central America, Trinidad, Ecuador,Colombia, Venezuela, the Guianas, Brazil, andParaguay (Figure 23)
Description: Typical Culex mosquito witha blunt abdomen (at tip) and hardly anystriking features; adults medium-sized darkmosquitoes with rounded abdomen, unbandeddorsally (Figure 24); white patches may bepresent laterally; difficult to distinguish fromother small Culex mosquitoes.
Figure 23Approximate geographic distribution of Culex nigripalpus.
Figure 24Adult Culex nigripalpus.
Figure 22Feeding positions of mosquitoes: Anopheles (A) Culex (B)(from: USDA, ARS, Agri. Hndbk. No. 173).

275
Mosquitoes
Figure 25Approximate geographic distribution of Culex quinquefasciatus (including C. pipiens).
Figure 26Adult Culex quinquefasciatus.
Remarks: Active in spring, summer, and autumn, but generally most abundant inautumn; breeds in shallow rainwater pools and semipermanent ponds
Southern House MosquitoCulex quinquefasciatus Say
Medical Importance: One of the major vectors of SLE virus (numerous outbreaksof SLE associated with this species); primary vector of WNV in southern states; highlyanthropophilic species in many parts of the tropical and subtropical world where it isalso a major vector of lymphatic filariasis
Distribution: C. pipiens complex, which includes C. quinquefasciatus, cosmotropicalin distribution (Figure 25); in North America this group is represented by three mainmembers: the northern house mosquito, C. pipiens, occurs in areas above 39° N.latitude; the southern house mosquito, C. quinquefasciatus, occurs at latitudes less than36° N. latitude; between 36° and 39° N. latitudes, C. pipiens and C. quinquefasciatus,
as well as hybrids between the two, are encountered
Description: Typical Culex mosquito with a bluntabdomen (at tip) and hardly any striking features;medium-sized brown mosquito with a few whitebands on upper side of the abdominal segments(Figure 26); bands widest in middle of dorsum andnarrow laterally; legs and proboscis dark andunbanded; difficult to distinguish from other Culexmosquitoes
Remarks: Breeds in ditches, storm sewer catchbasins, cesspools, and polluted water (also breeds inartificial containers around homes such as cans, jars,and tires); readily enters homes producing the famil-iar “singing” sound around persons at night; flightrange variable, but may be as far as 1100 m in asingle night

276
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 27Approximate geographic distribution of Culex salinarius.
Figure 28Adult Culex salinarius.
Culex salinarius Coquillett
Medical Importance: Often occurs in extremely high numbers and thus a nuisancepest; secondary vector of SLE, WNV, and EEE viruses
Distribution: U.S. and Canada east of Rocky Mountains, as well as Bermuda andparts of Mexico (Figure 27); especially com-mon along the Atlantic and Gulf Coasts
Description: Typical Culex mosquito (“LBC”little brown Culex) with a blunt abdomen (attip) and hardly any striking features; brownspecies has both proboscis and hind tarsi en-tirely dark (no white bands) (Figure 28); dorsalabdominal segments have dingy and ofteninconspicuous basal bands of yellowish orbrownish scales; bands usually irregular andnarrow
Remarks: Breeds in ditches, pools, artificialcontainers, and often salty water, such as thatin salt marshes; found breeding year round inGulf coastal states; feeds readily on people,mostly outdoors, but occasionally inside build-ings; feeding heaviest at dusk and first hoursof darkness; flight range 1 mile or more

277
Mosquitoes
Encephalitis MosquitoCulex tarsalis Coquillett
Medical Importance: Abundant and widespread species; main vector of WEE virus;also transmits SLE virus in western and southwestern U.S.; probably the most ubiqui-tous commonly encountered mosquitoes in California
Distribution: Most of U.S., parts of south-western Canada, and Mexico (Figure 29)
Description: Medium-sized mosquito, darkbrown to black in color, having white bandson the legs and abdomen (Figure 30); broadwhite band in middle of proboscis; ventor ofabdomen is white with a black chevron oneach segment
Remarks: Primarily a rural species thatbreeds in both polluted and clear water inground pools, grassy ditches, and artificialcontainers; in arid and semiarid regions, fre-quently found in canals and ditches associ-ated with irrigation; domestic and wild birdspreferred food source, but people readilyattacked; most active soon after dusk; activeprimarily in summer, but may remain activeall winter in southern parts of range
Figure 29Approximate geographic distribution of Culex tarsalis.
Figure 30Adult Culex tarsalis.

278
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 31Approximate geographic distribution of Psorophora columbiae.
Figure 32Adult Psorophora columbiae.
Dark Rice Field MosquitoPsorophora columbiae (Dyar and Knab)
Medical Importance: Although occasionally involved as secondary vector of severalencephalitides, primary adverse effect on people is nuisance biting; vicious biter andthus severe nuisance pest
Distribution: Much of the southeastern U.S. as farnorth as New York state and west to southern SouthDakota, south to Texas and northern Mexico (Figure31); records from Arizona and New Mexico may beclosely related species in the Ps. confinnis complex.
Description: Large mosquito dark brown to black(Figure 32); white bands on the legs and yellow bandon otherwise dark proboscis; first segment of hindtarsus is brown with a white ring in the middle; lightand dark scales give much of the body and wings a“salt and pepper” effect
Remarks: Breeds in open, temporary pools of fresh-water such as ditches, rice fields, and low floodedareas; eggs deposited on moist soil subject to floodingeither by rain or irrigation; several broods producedin active season (April to October); bites aggressivelyduring day or night and can fly 6 to 8 miles

279
Mosquitoes
V. DISCUSSION OF SOME MAJOR PEST SPECIES IN OTHERAREAS OF THE WORLD
Anopheles albimanus Weidemann
Medical Importance: One of the most important vectors of malaria in Mexico,Central and South America, and Caribbean
Distribution: Extreme southern U.S. (Texasand Florida), Mexico, Central America, SouthAmerica (probably only Colombia, Venezuela,and Ecuador), Antilles, and Caribbean (Figure33)
Description: All Anopheles females havelong maxillary palps and wings often spotted;A. albimanus is small dark species (Figure34) with pale hind legs unlike many otherrelated Anopheles species; black proboscisand white terminal segment of palpi
Remarks: Hot, humid climates; most abun-dant during the wet season where they breedin sunny pools, pits, puddles, ponds, marshes,lagoons, and artificial containers, especiallythose water sources containing floating orgrassy vegetation; females feed on people anddomestic animals, both indoors and outdoors;usually rest outdoors after feeding
Figure 33Approximate geographic distribution of Anopheles albimanus.
Figure 34Adult Anopheles albimanus.

280
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 36Adult Anopheles darlingi.
Anopheles darlingi Root
Medical Importance: One of major contributors to endemic malaria in extremesouthern Mexico and Central and SouthAmerica; adults feed readily on people andoften collect in large numbers inside houses
Distribution: Mexico through CentralAmerica southward into Argentina and Chile(Figure 35)
Description: Last three segments of the hindtarsi entirely white (Figure 36); long, slender,black proboscis; white terminal segment ofpalpi; light spot at the cross vein on the frontwing margin smaller than the preceding darkspot
Remarks: Breeds in shaded areas of fresh-water marshes, swamps, lagoons, rice fields,lakes and ponds, and the edges of streams,especially those with vegetation; feeds onhumans indoors and rests indoors after feed-ing
Figure 35Approximate geographic distribution of Anopheles darlingi.

281
Mosquitoes
Anopheles gambiae Giles(Consists of Several Species in a Complex)
Medical Importance: Most efficient malaria transmitter in Africa (including allmembers of the complex); highly anthropophilic (blood meal analyses have indicatedthat more than 50% of fed females contain human blood)
Distribution: At least six members of the complex and their distributions in Africaare presented below (Figure 37):
1. A. arabiensis: tropical Africa, southwest Arabia, the Cape Verde Islands,Zanzibar, Pemba, Madagascar, and Mauritius
2. A. gambiae: tropical Africa, Bioko, Zanzibar, Pemba, and Madagascar3. A. melas: coastal West Africa4. A. merus: brackish water habitats in East and South Africa
5. A. quadriannulatus: Ethiopia, SouthAfrica, Swaziland, Zambia, Zanzibar, and Zim-babwe6. A. bwambae: Uganda
Description: Members of complex gener-ally look like the one depicted in Figure 38;precise identification of members of speciescomplex done by genetic methods, comparingenzyme and chromosome characteristics
Remarks: Each member of complex mayexhibit different behaviors, but larvae of A.gambiae and A. arabiensis (formerly species Aand B of the complex) occur in all types ofwater-containing depressions close to humanhabitations including pools, puddles, hoofprints, borrow pits, and even rice fields; espe-cially abundant during rainy season; femaleshave average flight range of about 1 mile
Figure 37Approximate geographic distribution of the Anopheles gambiae complex.
Figure 38Adult Anopheles gambiae.

282
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 39Approximate geographic distribution of the Anopheles leucosphyrus group.
Figure 40Anopheles balabacensis, a memberof the A. leucosphyrus group.
The Anopheles leucosphyrus Group
Medical Importance: Group of Anopheles mosquitoes (containing about 20 closelyrelated species); contains several main vectors of malaria in Southeast Asia
Distribution: Distributions of three of the main malaria vectors in the group aregiven below (Figure 39):
1. A. balabacensis: mainland of Southeast Asia, southern islands of Philippines,Sabah, Kalimantan (Borneo), and Java
2. A. dirus: mainland of Southeast Asia3. A. leucosphyrus: Malaysia, Kalimantan (Borneo), and Sumatra
Description: Members of group have numerous spotswithin the wings and on the legs (Figure 40); conspicu-ously white joints where the tibia and tarsus meet oneach hind leg
Remarks: Breed in shaded freshwater pools in andamong rocks, in hoof prints, vehicle ruts, and the like;many are forest species that bite man and animalsoutdoors; fed females generally rest outdoors (in thecase of A. balabacensis, the females rest on forestvegetation during the day, congregate around humandwellings at sundown, remain quiescent on vegetationfor some time after dark, then enter the dwellings tofeed on sleeping persons)

283
Mosquitoes
The Anopheles minimus Complex
Medical Importance: Important vectors of malaria in tropical Africa, the Indiansubcontinent, and Southeast Asia.
Distribution: The distributions of three members of the A. minimus complex aregiven below (Figure 41):
1. A. flavirostris: most of Indonesia and the Philippines2. A. funestus: most of tropical Africa3. A. minimus: Burma, Bangladesh, India, Cambodia, Laos, Malaysia, Thailand,
Vietnam, and Taiwan
Figure 41Approximate geographic distribution of the Anopheles minimus complex.
Figure 42Adult Anopheles minimus.
Description: Small, dark specimens havingnarrow white bands on the female palps (Fig-ure 42). A. minimus has a totally dark probos-cis
Remarks: A. flavirostris bites indoors butrests outdoors afterward; both A. flavirostrisand A. minimus breed in grassy edges ofsmall foothill streams, springs, irrigation ditches,or seepages; they both prefer shaded areas; A.funestus is an extremely important vector ofmalaria in tropical Africa (second only to A.gambiae); larvae of A. funestus prefer marshes,swamps, and edges of streams; feed indoorsand outdoors, but rest outdoors after feeding

284
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 43Approximate distribution of Anopheles pseudopunctipennis.
Figure 44Adult Anopheles pseudopunctipennis.
Anopheles pseudopunctipennis Theobald
Medical Importance: Important vector of malaria in Mexico, Central America, andparts of South America; primary vector of a large malaria outbreak in Oaxaca, Mexicoduring 1998
Distribution: Southern U.S. southward toArgentina, and Antilles (Figure 43)
Description: Females are large gray mos-quitoes with black legs (Figure 44); two nar-row white bands and a white tip on thepalps; totally dark proboscis; entirely blackhind tarsus; two light spots on the front wingmargin
Remarks: Highland species occurring mostabundantly during the dry season; heavyrains during the wet season flush the larvaeout of their breeding sites, which includeshallow, quiet, or slow-moving water such asdrying stream beds; adults enter houses andbite people readily

285
Mosquitoes
Anopheles stephensi Liston
Medical Importance: Widely distributed urban vector of malaria
Distribution: Afghanistan, Bangladesh, Burma, China, India, Indochina, Iraq, Nepal,Oman, Pakistan, Saudi Arabia, and United Arab Emirates (Figure 45); one of the most
abundant species in the Persian Gulf region
Description: Females have numerous whitespots on both the legs and wings (Figure 46);hind tarsal segments have narrow white bandapically (last segment is dark); females havewhite-tipped palps and one dark spot on thefront margin of the wing proximal to theoutermost spot; abdomen is almost totallycovered with scales
Remarks: Breeds in man-made habitats suchas wells, cisterns, gutters, pools, and manyother peridomestic water sources; accordingly,malaria transmitted usually localized and lim-ited to urban centers; adults bite people bothindoors and outdoors and rest mainly indoorsafter feeding; flight range usually does notexceed 1/2 mile
Figure 45Approximate geographic distribution of Anopheles stephensi.
Figure 46Adult Anopheles stephensi.

286
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 48Adult Culex tritaeniorhynchus.
Figure 47Approximate geographic distribution of Culex tritaeniorhynchus.
Culex tritaeniorhynchus Giles
Medical Importance: Vector of JE virus in Far East; also most important nuisancemosquito during July and August in Japan
Distribution: Saudi Arabia, Borneo, Celebes, China, India, Iran, Iraq, Japan, Okinawa,Israel, Lebanon, Syria, Turkey, Java, Sumatra, Philippines, Sri Lanka, Madagascar, Egypt,Gold Coast, Nigeria, Cameroon, Sudan, Zaire,Kenya, Tanzania, Angola, Namibia, Uganda,Zanzibar, Mozambique, and Ivory Coast (Fig-ure 47); especially abundant in Korea, Japan,and eastward through central China
Description: Very small mosquito (aver-age size is 3 mm, the Japanese forms may belarger), dark reddish-brown in color with abanded proboscis (Figure 48)
Remarks: Breeds in freshwater collectionssuch as natural and artificial water impound-ments, ground pools, and drainage and irri-gation ditches; readily bites people; also feedson horses, cows, pigs, and other animals

287
Mosquitoes
Culex annulitostris Skuse
Medical Importance: Most medically important mosquito in Australia; main vectorof the flaviviruses Murray Valley encephalitis and Kunjin (a subtype of West Nile virus),and the main inland vector of the alphaviruses Ross River and Barmah Forest
Distribution: Southern and western Australasian region (including the entire Austra-lian mainland), Indonesia, Philippines (Figure 49)
Description: Medium sized, brown mos-quito; similar to U.S. species, Culex tarsalis,tarsi banded, scutum dark, proboscis withcomplete white ring in middle (Figure 50);may be difficult to distinguish from other,closely related, Australian species
Remarks: Active mid-spring to late fall;breeds in freshwater areas such as naturaland artificial water impoundments, groundpools, and drainage and irrigation ditches;does not breed in artificial containers; readilybites people; also feeds on other mammalsand birds
Figure 49Approximate geographic distribution of Culex annulirostris.
Figure 50Adult Culex annulirostris.

288
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Mansonia annulifera (Theobald)
Medical Importance: Probably most important vector of Wuchereria malayi (lym-phatic filariasis) in Orient, Philippines, and New Guinea; significant nuisance, beingstrongly anthropophilic
Distribution: Borneo, Burma, Celebes, India, Indochina, Java, New Guinea, Philip-pines, Sumatra, and Thailand (Figure 51)
Description: Similar to other Manso-nia mosquitoes (except lighter) with legs,palps, wings, and body covered with amixture of brown and pale (white orcreamy) scales giving them a dusty ap-pearance; pale species ranging in colorfrom yellow to light brown; mottled wingswith very broad and asymmetrical scalesand banded legs (Figure 52); very promi-nent silvery-white scales on midlobe ofscutellum
Remarks: Most commonly found inponds, pools, backwaters, swamps, andmarshes that contain the aquatic plantsPistia spp. and Eichhornia spp; larvaeobtain oxygen by puncturing the under-water stems of aquatic plants (like othermembers of genus)
Figure 51Approximate geographic distribution of Mansonia annulifera.
Figure 52Adult Mansonia annulifera.

289
Mosquitoes
REFERENCES1. Sturcher, D., How much malaria is there worldwide?, Parasitol. Today, 5, 39, 1989.
2. Morris, C. D., Baker, R. H., and Nayer, J. K., Human malaria. Florida Medical EntomologyLaboratory (IFAS) Fact sheet, July, 1990.
3. WHO, Yellow fever, WHO/EPI/GEN/98.11, Geneva, 1998, 6.
4. WHO, Yellow fever technical consensus meeting, WHO/EPI/GEN/98.08, Geneva, 1998,3.
5. CDC, San Juan Laboratories, Dengue Surveillance Summary, 62:1, 1991.
6. Gubler, D. J., Epidemic dengue and dengue hemorrhagic fever: a global public healthproblem in the 21st century, in Emerging Infections, Vol. 1, Scheld, W. M., Armstrong, D.,and Hughes, J. M., Eds., ASM Press, Washington, D.C., 1998, 3.
7. WHO Expert Committee on Filariasis, Third Report, Tech. Rep. Ser. No. 542, World HealthOrganization, Geneva, 1974.
8. Laurence, B. R., The global distribution of bancroftian filariasis, Parasitol. Today, 5, 260,1989.
9. Beaver, P. C. and Orihel, T. C., Human infection with filariae of animals in the UnitedStates, Am. J. Trop. Med. Hyg., 14, 1010, 1965.
10. Thomas, J.G., Sundman, D., Greene, J.N., Coppola, D., Lu, L., Robinson, L.A., and Sandin,R.L., A lung nodule: malignancy or the dog heartworm?, Infect. Med., 15, 105, 1998.
11. Morris, C. D., Eastern equine encephalomyelitis, in The Arboviruses: Epidemiology andEcology, Vol. 3, Monath T. P., Ed., CRC Press, Boca Raton, FL, 1988, chap. 24.
12. Chamberlain, R. W., History of St. Louis encephalitis, in St. Louis Encephalitis, Monath,T. P., Ed., American Public Health Association, Washington, D.C., 1980, 7.
13. CDC, Outbreak of West Nile-like viral encephalitis: New York, CDCMMWR, 48, 845, 1999.
14. Asnis, D. W., Conetta, R., Teixeira, A., et al., The West Nile virus outbreak of 1999 in NewYork: the Flushing Hospital experience, Clin. Infect. Dis., 30, 413, 2000.
15. CDC Data, Epidemiology and Ecology Section, Arbovirus Diseases Branch, Division ofVector-Borne Infectious Diseases, CDC, Ft. Collins, Colorado, 1998.
16. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, 212.
17. Anon., Venezuelan equine encephalomyelitis, a national emergency, USDA, APHIS-81-1,U. S. Department of Agriculture, Washington, D.C., 1972.
18. Weaver, S. C., Salas, R., Rico-Hesse, R., Ludwig, G. V., Oberste, M. S., Boshell, J., Tesh,R. B., Re-emergence of epidemic Venezuelan equine encephalomyelitis in South America,The Lancet, 348, 436, 1996.
19. Burke, D. S. and Leake, C. J., Japanese encephalitis, in The Arboviruses: Epidemiology andEcology, Vol. 3, Monath T. P., Ed., CRC Press, Boca Raton FL, 1988, chap. 28.
20. Rappleye, W. C., Epidemic encephalitis, etiology, epidemiology, treatment, Third Report,Matheson Commission, Columbia University Press, New York, 1939.
21. Woods, C. W., Karpati, A. M., Grein, T., McCarthy, N., Gaturuku, P., Muchiri, E., Dunster,L., Henerson, A., Khan, A. S., Swanepoel, R., Bonmarin, I., Martin, L., Mann, p., Smoak,B. L., Ryan, M., Ksizek, T. G., Arthur, R. R., Ndikuyeze, A., Agata, N. N., and Peters, C.J., An outbreak of Rift Valley fever in northwestern Kenya, Emerg. Inf. Dis., 8, 138, 2002.
22. New South Wales Department of Health, Ross River virus, NSW Dept. Health, PublicHealth Unit, Fact Sheet, Sydney, Australia, p. 1, 2002.
23. Reinert, J. F., New classification for the composite genus Aedes, elevation of subgenusOchlerotatus to generic rank, reclassification of the other subgenera, and notes on certainsubgenera and species, J. Amer. Mosq. Contr. Assoc., 16, 175, 2000.

290
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
24. Chapman, H. C. and Johnson, E. B., The mosquitoes of Louisiana, La. Mosq. Contr. Assoc.Tech. Bull. No. 1 (Revised), 1986.
25. Anon., St. Louis encephalitis outbreak in central Florida — 1990, Florida Epigram, 1, 1,1991.

291
Moths (Species Whose Scales or Hairs Cause Irritation)
CHAPTER 26
MOTHS (SPECIES WHOSESCALES OR HAIRS
CAUSE IRRITATION)
TABLE OF CONTENTS
I. Introduction and Medical Importance ...........................................................291
II. General Description of Some Species Involved ...........................................292
III. Geographic Distribution ..................................................................................293
IV. Biology/Behavior .............................................................................................294
V. Treatment ..........................................................................................................294
References ......................................................................................................................294
I. INTRODUCTION AND MEDICAL IMPORTANCE
As discussed in Chapter 14, several species of Lepidoptera have larvae, commonlycalled urticating caterpillars, that possess stinging hairs or spines and can inflict apainful sting upon exposure to human skin (erucism). Some moth species as adultsbear scales and/or hairs, which may detach, become airborne, and cause urticaria andirritation in humans (see Chapter 5). Irritation from adult moths is called lepidopterism.Several moth species in the families Notodontidae, Saturniidae, and Lymantriidae havebeen reported as causes of lepidopterism. The dermatitis may present as localized,widespread, or generalized erythematous macules that rapidly evolve into urticarialwheals.2 Wheals are often, but not always, replaced by small infiltrated papules orpapulovesicles. Lepidopterism is especially severe in South America during certain

292
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
LEPIDOPTERISM
Douglas Fir Tussock Moth, Orgyiapseudotsugata
ImportanceUrticaria; irritation; respiratory problems
from airborne moth hairs or scales
DistributionSeveral species worldwide, especially
those in genus Hylesia in SouthAmerica
LesionVariable — often itchy papules or
maculopapules
Disease TransmissionNone
Key ReferenceRosen, Dermatol. Clinics, 8, 245, 1990
TreatmentAntihistamines, topical corticosteroids,
and/or calamine products; occasionaloral steroids may be indicated
times of the year due to moths in the genusHylesia.1 Severe problems have occurred else-where. DeLong3 reported an epidemic of 500,000cases of caterpillar dermatitis in and aroundShanghai, China, which was associated with anunexpected population explosion of yellow-tailmoths in surrounding rural areas and appropri-ate climatic conditions conducive to wind-blownspread of the disease.
In the U.S., the tussock moths and theirrelatives in the family Lymantriidae may causeirritation. The female Douglas fir tussock moth,Orgyia pseudotsugata, covers her egg masseswith froth and body hairs. These hairs, alongwith other airborne hairs from the tips of thefemale abdomens, cause rashes, upper respira-tory irritation, and eye irritation to forest workersin the Pacific Northwest.4 A related species, thewhite marked tussock moth, O. leucostigma,occurs throughout most of North America andmay also be involved in cases of lepidopterism,especially in the East. In addition, airborne gypsymoth hairs, silken threads, and shed skins havebeen reported to cause a pruritic cutaneous re-action in sensitive individuals.
II. GENERAL DESCRIPTION OFSOME SPECIES INVOLVED
Moths in the genus Hylesia are about 20 mmlong and have a wing span of about 40 mm.Alexander5 states that the northern species(Mexico, Central America) are a golden color,while those from Peru and Argentina have darkbrown or black stripes on the body. The wingsand body are covered with numerous scalesand long hairs.
Tussock moths and their relatives are me-dium-size moths whose larvae are quite hairy.Female Douglas fir tussock moths are wingless.Males are brownish-gray with a wingspan ofabout 25 mm (Figure 1A). The mature caterpil-lars are about 30 mm long and are gray tobrown in color, with a black head (Figure 1B).They bear two, long dark tufts or pencils of hairsimilar to horns right behind the head; a similar

293
Moths (Species Whose Scales or Hairs Cause Irritation)
but longer pencil is on the posterior. Four dense, buff-colored tussocks are locatedforward along the middle of the back.
The white marked tussock moth is larger than the Douglas fir tussock moth. Femalesare wingless; males are gray and have lighter hind wings with a wingspan of about 30mm. The mature caterpillars are about 35 mm long and are light brown with yellowand black stripes. In contrast to the Douglas fir tussock moth, O. leucostigma caterpil-lars have a bright red head. Again, there are tufts of white hair on the dorsal side ofthe first four abdominal segments.
The gypsy moth female has a wingspread of approximately 50 mm, is winged (incontrast to the tussock moths mentioned above), and has white and black markings(Figure 1C). The males are a little smaller than females and are gray. Mature gypsy mothcaterpillars, like other members of the Lymantriidae, have long tufts of hair along thebody (Figure 1D). They are approximately 30 to 50 mm long, gray in color, and haveyellow stripes running lengthwise down the body. They may also appear to have redor blue spots along the sides and top of the body.
III. GEOGRAPHIC DISTRIBUTION
Hylesia moths occur from Mexico to Argentina.5 The Douglas fir tussock moth is aserious pest in western North America. Some of the worst outbreaks have occurred inBritish Columbia, Idaho, Washington, Oregon, Nevada, California, Arizona, and NewMexico. The white marked tussock moth occurs throughout most of North America.Gypsy moths occur in Europe and in the eastern U.S.
Figure 1Some irritating moths: Douglas fir tussock moth male (A) (females are wingless), Douglas firtussock moth larva (B), gypsy moth female (C), and gypsy moth larva (D) (taken in part fromUSDA Agri. Hndbk. No. 536).

294
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
IV. BIOLOGY/BEHAVIOR
Female Hylesia moths have barbed or spiny urticating setae that are called fleshettes.Fleshettes may break off and become airborne as large numbers of the moths emergeand gather around lights in towns or cities.1 Hylesia moths lay their eggs in clusters onthe branches of trees, and the female coats the eggs with urticating spines. The life cycleis about 3 months long.
Tussock moths and their relatives are serious defoliators of forest, shade, andoccasionally fruit trees. The Douglas fir tussock moth feeds primarily on fir trees.Usually the first indication of attack appears in late spring. Larvae from newly hatchedeggs feed on the foliage of the current year, causing it to turn brown. The small larvaeare inconspicuous, but by mid-July they are larger and more colorful. To feed indifferent areas of the tree, they lower themselves through the tree canopies by silkenthreads. By wind action this often spreads them to nearby uninfested trees. By Augustthe larvae stop feeding and drop to the ground, crawling everywhere looking for aplace to pupate. Female moths do not fly. Eggs are laid on tree trunks or branches,usually near the cocoon from which the female emerged.6 Tussock moths overwinterin the egg stage.
Gypsy moths lay eggs on tree trunks in July and August in masses covered with frothand body hairs from the female. Eggs overwinter and the tiny first stage larvae emergethe following spring, usually in late April or early May.7 The females can fly, but onlyweakly. Dispersal of gypsy moth infestation is primarily by young larvae on silkenthreads traveling tree to tree or limb to limb by “ballooning” in the wind.
V. TREATMENT
Treatment mainly involves personal protection and/or avoidance of the offendingspecies. During season of Hylesia (South America) moth emergence, it may help to turnoff outdoor lights. In affected areas of the U.S., air conditioning and frequent changesof filters may help reduce airborne levels of scales or hairs. Sensitive persons shouldavoid walking in forests heavily infested with tussock moths.
Acute urticarial lesions may respond satisfactorily to topical corticosteroid lotionsand creams (desoximetasone gel has been frequently used), which reduce the intensityof the inflammatory reaction. Oral antihistamines may relieve itching and burningsensations. In more serious cases, oral steroids may be indicated. Rosen2 said systemicadministration of corticosteroids in the form of intramuscular triamcinolone acetonidehas been remarkably effective in relieving severe itching due to gypsy moth dermatitis.
REFERENCES1. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,
Macmillan, New York, 1979, chap. 17.
2. Rosen, T., Caterpillar dermatitis, Dermatol. Clin., 8, 245, 1990.
3. DeLong, S., Mulberry tussock moth dermatitis, J. Epidemiol. Comm. Health, 35, 1, 1981.
4. Perlman, F., Press, E., Googins, G. A., Malley, A., and Poarea, H., Tussockosis: reactionsto Douglas fir tussock moth, Ann. Allergy, 36, 302, 1976.
5. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 12.

295
Moths (Species Whose Scales or Hairs Cause Irritation)
6. Borror, D. J., Triplehorn, C. A., and Johnson, N. F., An Introduction to the Study of Insects,6th ed., Saunders College Publishing, Philadelphia, 1989, 654.
7. Nichols, J. O., The gypsy moth in Pennsylvania — its history and eradication, PennsylvaniaDept. Agri. Misc. Bull. No. 4404, 1962, 13.


297
Pentastomes (Tongue Worms)
CHAPTER 27
PENTASTOMES(TONGUE WORMS)
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................297
II. General Description .........................................................................................298
III. Geographic Distribution ..................................................................................298
IV. Biology/Behavior .............................................................................................298
V. Treatment ..........................................................................................................299
References ......................................................................................................................299
I. GENERAL AND MEDICAL IMPORTANCE
Pentastomes (Phylum Pentastomida), sometimes also classified as members of theArthropoda because of their chitinous exoskeleton, are worm-like parasites foundmainly in the respiratory tracts of carnivorous mammals, reptiles, and birds.1 Pentastomiasis(human parasitism by pentastomes) may occur in the viscera, where nymphs developin the liver, spleen, lungs, and other organs, or in the nasopharyngeal area, includingthe nasal passages, larynx, or Eustachian tubes. Fortunately, human pentastomiasis ismostly asymptomatic and only found by radiography, surgery, or autopsy. Occasion-ally, human infestations may cause discomfort in the throat, paroxysmal coughing, andsneezing.

298
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
II. GENERAL DESCRIPTION OF SOME SPECIES INVOLVED
Pentastome worms vary in color and shape, depending upon the species, but aregenerally colorless to yellow, ringed organisms with no apparent legs or body regions.The body may be cylindrical or flattened. Females may be up to 130 mm long and 10mm wide; males are smaller, being up to 30 mm long. On either side of the mouth aretwo pairs of hollow, fanglike hooks which can be retracted into grooves like the clawsof a cat.
III. GEOGRAPHIC DISTRIBUTION
Two species of pentastomes account for 99% of the infections in humans.2 The tongueworm, Linguatula serrata (Figure 1), which occurs worldwide, is often found in thenasal passages and frontal sinuses of several host animals, but especially dogs.Armillifer armillatus (Figure 2) ordinarily inhabits the respiratory tract of certain snakesin central Africa.
IV. BIOLOGY/BEHAVIOR
The life cycle of Linguatula serrata is provided here as a fairly typical example ofpentastomid biology. Adults are often found in the nasal passages and frontal sinusesof canines and felines. Eggs are produced and pass out of their host in nasal discharges
Figure 1The tongue worm, Linguatula serrata.
Figure 2Armillifer armillatus, a common pentastome found in snakes.

299
Pentastomes (Tongue Worms)
that are deposited in water or on vegetation. An intermediate host (example: rabbit orsheep) swallows contaminated water or vegetation and the eggs hatch into primarylarvae which penetrate the intestinal wall and become lodged in the liver, lungs, ormesenteric nodes. The larvae then pass through two molts resulting in a pupa-likestage. Up to seven more molts may occur before the nymphal stage develops(sometimes called an infective larva). The nymphs then migrate to the abdominal orpleural cavity of the intermediate host where they become encysted. When a definitivehost (dog or cat) eats the intermediate host, the nymphs escape rapidly and migrateanteriorly, subsequently clinging to the lining within the host’s mouth. From this pointthey migrate to the nasal cavities where they develop into adults. The adult stage maysurvive for up to 2 years.
V. TREATMENT
Treatment of pentostomiasis is usually not necessary, but in symptomatic cases surgicalremoval of the parasites may be needed.3
REFERENCES1. Markell, E. K., Voge, M., and John, D. T., Medical Parasitology, 7th Ed., W. B. Saunders,
Philadelphia, 1998, 359.
2. Binford, C. H. and Conner, D. H., Pathology of Tropical and Extraordinary Diseases, Vol.2, Armed Forces Institute of Pathology, Washington, 1976, 38.
3. Hobmaier, A. and Hobmaier M., On the life cycle of Linguatula rhinaria, Am. J. Trop. Med.20, 199, 1940.


301
Scorpions
CHAPTER 28
SCORPIONS
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................301
II. General Description .........................................................................................302
III. Geographic Distribution ..................................................................................304
IV. Biology/Behavior .............................................................................................304
V. Treatment of Stings ..........................................................................................307
References ......................................................................................................................308
I. GENERAL AND MEDICAL IMPORTANCE
Scorpions are eight-legged arthropods that can inflict a painful sting (Color Figure 28-20). There are about 1,400 species occurring on all major land masses except Antarctica.Some species are more dangerous than others, depending upon their type of venom;size and appearance do not determine the medical importance of a scorpion. Forexample, scorpions in the genera Pandinus and Heterometrus (Old World) andHadrurus (New World) are huge and menacing, but they constitute no serious healthhazard. Most species (Centruroides vittatus is a common offender in the southwesternU.S., Figure 1A) can elicit local effects by their stings in a manner similar to that of beesand wasps. There is immediate sharp pain at the site of venom injection and oftenmoderate local edema (which may be discolored). Dr. Scott Stockwell at the WalterReed Biosystematics Unit compares the sting to hitting your thumb with a hammer.Regional lymph node enlargement, local itching, paresthesia, fever, and occasionallynausea and vomiting may also occur.1 Signs and symptoms in a person stung by ascorpion with this type of venom usually subside in a few hours; however, it must be

302
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
SCORPIONS
Centruroides vittatus, a commonscorpion species.
noted that a person with insect sting allergycould have a systemic reaction from this type ofvenom.
The other, more deadly, scorpion speciesare in the family Buthidae and have a venomthat is more neurologic and hemolytic in activ-ity. Systemic effects from such stings includedrowsiness, abdominal cramps, blurred vision,spreading partial paralysis, muscle twitching,abnormal eye movements, profuse salivation,perspiration, priapism, hypertension, tachy-cardia, and convulsions.2–4 Extreme restless-ness, resembling seizure, is a frequent present-ing sign in children.5 In fact, very small childrenmay flail, writhe, and display roving eye move-ments. Death is probably due to respiratoryparalysis, peripheral vascular failure, and/ormyocarditis, and it may occur at any intervalbetween 1.5 to 42 h.1 Four cases of scorpionsting in the southwestern U.S. by our onlydangerous species, C. exilicauda (formerlycalled C. sculpturatus), caused severe clinicalmanifestations including respiratory failure,metabolic acidosis, and severe multiorgan sys-tem disease.6 Other than the sting of C.exilicauda in Arizona and surrounding areas,scorpion stings in the U.S. are not usually life-threatening (barring allergic reaction), but scor-pions constitute a severe problem in otherareas of the world, such as northern Africa andCentral and South America. For example, thenumber of scorpion stings in Morocco is esti-mated to be 40,000 per year.4
II. GENERAL DESCRIPTION
Scorpions are crablike in appearance, withpincers attached to their two front appendages(Figure 2). Their five-segmented “tail” termi-nates in a bulbous structure with a prominentcurved stinger (Figure 3). Adult scorpions varyin size from 2 to 10 cm, depending upon thespecies. Most American species are yellowish-brown or brown in color. C. exilicauda, thedangerous U.S. species, is yellow to yellowish-brown in color and is relatively small (usually6 cm maximum) (Figure 1B). It is a slenderspecies with very narrow and elongate tail
ImportancePainful sting; some species deadly
DistributionOnly one dangerous species in the U.S.;
numerous species in other areas
LesionVariable — sometimes local swelling
and discoloration
Disease TransmissionNone
Key ReferencePolis, G. A., Stanford University Press,
1990
TreatmentIce packs; anticonvulsants; vasodilators;
sometime antivenin serum for deadlyspecies

303
Scorpions
Figure 1Centruroides vittatus (A), avery common species in thesouthwestern U.S. andCentruroides exilicauda (B),a dangerous U.S. species(reprinted with permission ofUniversity Press of Mississippifrom SCORPIONS OFMEDICAL IMPORTANCE byHugh L. Keegan, Copyright (c)1980 University Press ofMississippi).
Figure 2Typical scorpion in a stinging position (U.S. Army Photo Courtesy of LTC H. J. Harlan, 74thMed. Det.).

304
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
segments. Immatures have a diagnostic small spine or tubercle at the base of thestinger (Figure 4). A variant form of C. exilicauda may also occur with two irregularblack stripes down its back. At one time people thought this striped version of C.exilicauda was another species named C. gertschi.
III. GEOGRAPHIC DISTRIBUTION
Table 1 lists some of the dangerous scorpions worldwide and their distributions. About90 species occur in the U.S. and all but four of these naturally occur west of theMississippi River. The most commonly encountered species in the southwestern U.S.is the common striped scorpion, C. vittatus, whose sting is as painful as a wasp or beesting. The species is especially common in Texas and is responsible for numerousnonfatal stings each year. The only dangerous scorpion (other than via allergic reaction)in the U.S., C. exilicauda, occurs primarily in Arizona, but also in southeasternCalifornia, Nevada, southern Utah, and southwestern New Mexico. In Mexico, thisspecies has been found in Baja, California at Puerto Punta Penasco, Sonora.
Figure 4Side view of Centruroides exilicauda stinger showingdiagnostic small spine or tubercle. This structure is lessobvious in adults.
Figure 3Close-up of stinger of Pandinus imperator.

305
Scorpions
Table 1Geographic Distribution of SomeDangerously Venomous Scorpionsa
Region Country Species
Old World Algeria Buthus occitanusAndroctonus australis
Egypt A. australisA. amoreuxiLeiurus quinquestriatus
Iraq Hemiscorpion lepturusA. crassicauda
Israel L. quinquestriatusA. crassicaudaA. bicolor
Jordan B. occitanusMorocco A. mauritanicus
A. australisA. amoreuxiB. occitanus
South Africa Parabuthus triradulatusP. transvaalensisP. villosus
Sudan B. minaxTurkey A. crassicauda
L. quinquestriatusMesobuthus gibbosus
New World Argentina Tityus bahiensisBrazil T. bahiensis
T. serrulatusGuyana T. cambridgeiMexico Centruroides noxius
C. suffussusC. infamatusC. elegansC. limpidus
Trinidad T. trinitatisU. S. C. exilicaudaVenezuela T. trinitatis
C. gracilis
a From Keegan, H. L., Scorpions of Medical Importance, Univer-sity of Mississippi Press, Jackson, MS, 1980, chap. 3. Withpermission.

306
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Androctonus australis, the fat-tailed scorpion (Figure 5A), is a highly venomous,very aggressive scorpion found in North Africa in Egypt, Algeria, Tunisia, and Libya.Subspecies of A. australis may occur in the Middle East. The fat-tailed scorpion isresponsible for 80% of all reported scorpion stings in Algeria; about one third of themare fatal.7 Buthus occitanus (Figure 5B) is a widely distributed, dangerous scorpioncomposed of several subspecies; it is found in southern France, Spain, Italy, Greece,several Mediterranean islands, Israel, Jordan, and northern Africa. The dangerouslyvenomous scorpion, Leiurus quinquestriatus, is found in Turkey southward throughSyria, Lebanon, Jordan, Israel, and down into northern Africa. In the Middle East,Prionurus (=Androctonus) crassicauda is responsible for many serious stinging inci-dents annually. Tityus serrulatus and T. bahiensis are probably the most dangerousspecies in Brazil. In South Africa, Parabuthus triradulatus, P. transvaalensis, and P.villosus are dangerous.
IV. BIOLOGY/BEHAVIOR
Female scorpions have pouches in which the young develop for a time period, beforebeing born alive. Subsequently, they climb onto the mother’s back and remain thereuntil molting about 2 weeks later. After this molt, the young scorpions scatter to livesolitary lives, molting 6 or 7 more times before reaching maturity.
Figure 5Androctonus australis (A), and Buthus occitanus (B) (reprinted withpermission of University Press of Mississippi from SCORPIONS OF MEDICALIMPORTANCE by Hugh L. Keegan, Copyright (c) 1980 University Press ofMississippi).

307
Scorpions
Scorpions are nocturnal feeders, feeding mostly on insects and spiders, althoughthere are examples of the larger species being seen feeding on lizards, snakes, andother small vertebrates. They seize prey with their claws and paralyze it by their sting.During the day scorpions remain concealed and are only encountered when peopledisturb them. Some of the most dangerous species are known as bark scorpionsbecause they are often found under loose bark and in the crevices between the basesof palm tree leaves. They do not burrow but hide under boards, bricks, and otherrubbish. Ground scorpions, on the other hand, burrow into loose sand or gravel andare capable of hibernating without food or water for up to 7 months.
Around homes, scorpions are usually found under the houses and in attics. Theyenter attics by climbing between wall partitions. However, they will abandon attics assoon as the temperature gets too high, migrating downward into the walls, and if anopening is available, into the house itself. They favor attics with air conditioning ductsthat provide cool temperatures and a place to hide.
Because they will seek water, they are often found in bathrooms, kitchens, orlaundry rooms at night. It is not uncommon to find them in bathtubs or sinks, whichthey entered seeking water and then were unable to climb back out.
The amount of venom injected with a sting varies with the size of scorpion.Whittemore and Keegan8 found that electrically stimulated specimens of a large speciesfrom the Middle East yielded an average of 0.48 mg, whereas the average yield froma small, but highly dangerous species of Centruroides from Mexico was only 0.075 mg.
V. TREATMENT OF STINGS
Many species of scorpions are innocuous and produce stings that are followed by sharppain or a burning sensation and a wheal, which usually disappears with no compli-cations. The venom of dangerous species is quite neurotoxic. Death is due tocardiovascular failure or paralysis of the respiratory muscles within a few hours.
After a sting by a dangerous species, it is important for patients to stay calm in orderto minimize absorption of venom into the body. A pressure dressing over the sting sitemay be helpful, as well as application of ice packs. In adults, symptoms may be self-limited with resolution occurring in several hours. Children are at greatest risk of severereactions.5,9 In many countries administration of a potent antivenin within a couple ofhours of the sting may be needed for treatment of severe envenomization.1,9 Antiveninsare commercially available for many (but not all) of the dangerous scorpions world-wide. There is some controversy concerning antivenin use; the best course may be toevaluate and administer antivenin only as needed. In the U.S. an antivenin forCentruroides exilicauda envenomization is produced from goat serum at Arizona StateUniversity and is approved by the Arizona Board of Pharmacy for use within the stateof Arizona.10 But there was a 58% rate of serum sickness in one study.9 Since theantivenin is not an FDA approved product and cannot be used across state lines, itsapplication is limited.10
Scorpion sting therapy may include mechanical ventilation to improve oxygenationand administration of CNS depressants such as midazolam (a benzodiazepine) andvasodilators such as selective α1 blockers and calcium channel blockers.4,10 Others haveused intravenous propralonol HCL.11 Patients treated with midazolam should becarefully monitored for underventilation or apnea which can lead to hypoxia/cardiacarrest.

308
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
REFERENCES1. Keegan, H. L., Scorpions of Medical Importance, University of Mississippi Press, Jackson,
MS, 1980, chap. 3.
2. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, chap. 17.
3. Bücherl, W. and Buckley, E., Eds., Venomous Animals and their Venoms, Vol. III.,Venomous Invertebrates, Academic Press, New York, 1971.
4. Ghalim, N., El-Hafney, B., Sebti, F., Heikel, J., Lazar, N., Moustanir, R., and Benslimane,A., Scorpion envenomation and serotherapy in Morocco, Am. J. Trop. Med. Hyg., 62, 277,2000.
5. Polis, G. A., The Biology of Scorpions, Stanford Univ. Press, Stanford, CA, 1990, chap. 10.
6. Berg, R. A. and Tarantino, M. D., Envenomization by the scorpion Centruroides exilicauda(C. sculpturatus): severe and unusual manifestations, Pediatrics, 87, 930, 1991.
7. Nichol, J., Bites and Stings — The World of Venomous Animals, Facts on File, Inc., NewYork, 1989, 58.
8. Whittemore, F. W. and Keegan, H. L., Medically important scorpions in the Pacific area,in Venomous and Poisonous Animals and Noxious Plants of the Pacific Region, Keegan,H. L. and MacFarlane, W. V., Eds., Pergamon Press, Oxford, 1963, 107–110.
9. Bond, G.R., Antivenin administration for Centruroides scorpion sting: risk and benefits,Ann. Emerg. Med., 21, 788, 1992.
10. Gilby, R., Williams, M., Walter, F.G., McNally, J., and Conroy, C., Continuous intravenousmidazolam infusion for Centruroides exilicauda envenomation, oral presentation, NorthAmerican Congress of Clinical Toxicology, Orlando, FL, Sept. 1998.
11. Rachesky, I. J., Banner, W. Jr., Dansky, J., and Tong, T., Treatments for Centruroidesexilicauda envenomation, Am. J. Dis. Child., 138, 1136, 1984.

309
Spiders
CHAPTER 29
SPIDERS
TABLE OF CONTENTS
I. Spiders in General ...........................................................................................310A. Medical Importance ....................................................................................310B. Treatment of Bites .......................................................................................310
II. Brown Recluse and Other Violin Spiders ......................................................310A. General and Medical Importance ..............................................................310B. General Description ....................................................................................312C. Geographic Distribution .............................................................................312D. Biology/Behavior .........................................................................................312E. Treatment of Bites .......................................................................................313
III. Black Widow and Other Widow Spiders ......................................................314A. General and Medical Importance ..............................................................314B. General Description ....................................................................................317C. Geographic Distribution .............................................................................317D. Biology/Behavior .........................................................................................318E. Treatment of Bites .......................................................................................321
IV. Hobo Spiders ...................................................................................................321A. General and Medical Importance ..............................................................321B. General Description ....................................................................................322C. Geographic Distribution .............................................................................322D. Biology/Behavior .........................................................................................322E. Treatment of Bites .......................................................................................322
V. Funnel Web Spiders ........................................................................................322A. General and Medical Importance ..............................................................322B. General Description ....................................................................................323C. Geographic Distribution .............................................................................323D. Biology/Behavior .........................................................................................323E. Treatment of Bites .......................................................................................323

310
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
VI. Tarantula Spiders .............................................................................................324A. General and Medical Importance ..............................................................324B. General Description ....................................................................................324C. Geographic Distribution .............................................................................324D. Biology/Behavior .........................................................................................324E. Treatment of Bites .......................................................................................325
References ......................................................................................................................325
I. SPIDERS IN GENERALA. Medical Importance
There are more than 30,000 named species of spiders ranging in size (including legs)from a few millimeters to more than 17 cm (7 in.). Even some non-tarantulas are verylarge (Figure 1). All spiders with the exception of the family Uloboridae are venomousand use their venom to immobilize or kill prey; however, the chelicerae of manyspecies are too short to penetrate human skin. Of the remaining species (that can inflicthuman bites), the widow spiders (Latrodectus spp.), the violin spiders (Loxoscelesspp.), and hobo spiders (Tegenaria agrestis) are significant causes of local or systemiceffects from envenomization in the U.S. In Australia, the Sydney funnel web spider(Atrax robustis) and related species can cause serious illness and death. In SouthAmerica, the Brazilian Huntsman, Phoneutria fera, is a threat to humans, and AranhaArmedeira, Phoneutria nigriventer, has extremely potent venom.
It is important to note that at least 50 other species have been implicated in biteson humans. Bites from these species, although painful, are not likely to be dangerous.An account given by Carpenter et al.1 illustrates this point. A 15-year-old boy was bittenby a plectreurid spider, Plectreurys tristis, in Kern County, California. Initially the biteproduced pain, edema, and slight pallor at the site of the wound. The initial symptomspersisted for 15 to 30 min, and subsequently the patient reported vague, diffusenumbness near the site. All symptoms resolved within 2 h. Since not all spider bitesare life-threatening or lead to necrotic lesions, it is important for the patient to bringin to the clinic the offending spider for identification. This might help physicians avoidexpensive treatments used for spider bites from dangerous species. In addition to thedirect effects of spider venom, spider bites may produce secondary infections andallergic reactions (apparently rare in the U.S.).
B. Treatment of Bites
The treatment for most spider bites involves washing the bite site, applying coldcompresses, avoiding exercise, and treating with tetanus prophylaxis (if indicated),analgesics for pain, and antibiotics if secondary infection is suspected.2 Additionalmeasures are needed for bites by dangerous species such as hobo, widow, brownrecluse, and funnel web spiders (see discussions below).
II. BROWN RECLUSE AND OTHER VIOLIN SPIDERSA. General and Medical Importance
Violin spiders have a venom that produces necrotic cutaneous lesions (Color Figures29-21 through 29-23). The brown recluse spider, Loxosceles reclusa, is probably the

311
Spiders
most important of the violin spiders in the U.S. However, several other species occurin the Southwest (L. rufescens, L. deserta, L. arizonica) and Northeast that can producenecrotic lesions. L. laeta is a notorious violin spider in South America.
Every year, the brown recluse spider (also called the “fiddleback spider”) is respon-sible for numerous cases of envenomization. The bite is usually localized, but mayproduce considerable necrosis resulting in an unsightly scar.3,4 Research on brown reclusevenom has indicated that it produces necrotic and hemolytic effects, but not neurologic.Brown recluse venom contains several fractions, but the primary dermonecrotic compo-nent appears to contain the phospholipase enzyme, sphingomyelinase D, which acts ontissues by activation of platelet aggregation, thrombosis, and massive neutrophil infiltra-tion.2,5 The bite is usually painless until 3 to 8 hours later when it may become red,swollen, and tender. One study reported that the clinical signs of brown recluse biteobserved when the patients were first seen in a clinical setting included erythema,cellulitis, rash, and/or blister.6 Later, a black scab may develop, and eventually, an areaaround the site may decay and slough away, producing a large ulcer from 1 to 25 cmin diameter. Finally, the edges of the wound thicken and become raised while the centralarea is filled by scar tissue. Healing may require months, and the end result is often asunken scar (Figure 2). A helpful distinguishing sign of a brown recluse bite is thetendency of the lesion to extend downward in a gravitationally dependent manner. Thedirection of the lesion is dependent on the victim’s position while the vessel damage wasproduced. Asymmetrical lesions (especially the “flowing downhill” type) are rare fromother arthropod bites.
Systemic reactions — called systemic loxoscelism — characterized by hematuria,anemia, fever, rash, nausea, vomiting, coma, and cyanosis have sometimes beenreported from brown recluse bites. Systemic signs and symptoms are rare and, if they
Figure 1Huge fish-eating spider collected in Mississippi — not a tarantula. (Photo courtesy Sheryl Handand Dr. Sally Slavinski.)

312
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
occur, usually begin two to three days followingenvenomization in contrast to the local cutaneouslesion which is evident by 12 to 24 h.7 Hemolysis,always heralded by rash and fever, has been re-ported occurring as early as 24 h and as late as 3days after the bite.7 It usually continues for 72 h.There was a recent report of shock in a 13-year-oldgirl which began 9 h after being bitten by a violinspider.8
B. General Description
The adult brown recluse is a medium-sized spiderwith a 20 to 40 mm legspan and a color range fromtan to dark brown (Figure 3 and Color Figure29-24). The most distinguishing characteristics aresix eyes arranged in a semicircle of three pairs ontop of the head and a violin-shaped marking (baseforward) extending from the area of the eyes to thebeginning of the abdomen.
C. Geographic Distribution
Although its distribution may be more widespread,the brown recluse spider is most commonly found in the southcentral United States(Figure 4). L. deserta, L. rufescens, L. arizonica, and L. devia are closely related speciesoccurring mostly in the southwestern U.S. that may also cause necrotic arachnidism(Figure 4). In South America, there is a close relative to the brown recluse, L. laeta, thatcauses a severe necrotic lesion sometimes referred to as “gangrenous spot.” L. laeta hasbeen introduced into the U.S. and is established in Los Angeles County, California andpossibly at Harvard University (Cambridge, Massachusetts).
D. Biology/Behavior
The brown recluse is nocturnal in its feeding habits and most frequently found insidehouses in bathrooms, bedrooms, cellars, attics, the folds of clothing, cardboard boxes, andstorage areas, and also outdoors under rocks and rubble. Homes that are infested mayeasily contain hundreds of specimens. However, the spiders are not aggressive but willbite if pressure is placed on them. At night, they may crawl into garments and bite peopleattempting to dress the next morning. Common sites are under the arms or on the lowerparts of the abdomen. Brown recluse spiders are very resilient, being active in temperaturesranging from 40°F to 110°F, and they may live as long as 2 years.
Figure 2Sunken scar resulting from brown recluse bite; 4 monthspost bite. (From: Mississippi Cooperative Extension ServicePubl. No. 2154.)

313
Spiders
VIOLIN SPIDERS
Figure 3Brown recluse spider (USDA photo).
ImportanceSeveral closely related species cause
necrotic lesions; possibly hemolyticanemia
DistributionU.S., South America, Parts of Africa and
Australia
LesionVariable through time — papule with
erythema, large central zone ofpallor, mottling, then blackening ofcentral zone, ulceration
Disease TransmissionNone
Key ReferenceRees, et al., Ann. Emer. Med., 16, 945,
1987
TreatmentControversial — may include ice packs,
antibiotics, dapsone, and antivenin
E. Treatment of Bites
Persons bitten by a spider should make an effortto collect the spider and bring it in to a clinic foridentification. Positive identification of the spiderby an expert can be helpful, because bites ofmost spiders are temporarily painful but notdangerous. In the case of the brown recluse,prompt medical treatment may be needed toprevent severe reactions.
A specific antidote (antivenin) has shownsuccess in patients prior to development of thenecrotic lesion,9 but currently it is not widelyavailable. Also, some brown recluse bites areunremarkable, not leading to necrosis. There-fore, treatment is quite controversial. Some stud-ies have indicated that application of ice iseffective (the necrotic enzyme, sphingomyelinaseD, increases in activity as temperature increases— so keep it low). There have been reports ofsuccessful treatment by early, total excision ofthe bite site followed by split thickness skingrafting; however, more recent evidence arguesagainst wound excision.6 Rees et al.9 reportedgood success with the leukocyte inhibitor dap-sone, which eliminated the need for surgery inmany brown recluse bites (Figure 5). Othershave also advocated dapsone.10–12 Theoreticalevidence supports its use — histological exami-nation of bites in animals shows evidence ofextensive neutrophil infiltration at the site ofultimate necrosis. Dapsone is contraindicated inpersons with glucose-6-phosphate dehydroge-nase (G6PD) deficiency due to potential mas-sive hemolysis, and may produce side effects(even in non-G6PD patients) that could be con-fused with the systemic effects of brown reclusespider bite: malaise, nausea, and hemolysis.Further, there is some evidence that dapsone isineffective. A randomized, blinded, controlledstudy of venom effects in rabbits failed to showany benefit from the use of the drug.13 How-ever, studies in rabbits may not be comparableto humans, and dapsone is still probably themost suitable treatment.14

314
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
III. BLACK WIDOW AND OTHER WIDOW SPIDERSA. General and Medical Importance
Several species of widow spiders occur worldwide, but Latrodectus mactans is the onemost generally associated with the name “black widow spider.” It is also sometimesreferred to as the hourglass, shoe button, or po-ko-moo spider. The black widow spiderinjects a potent neurotoxin upon biting. Initially, the bite itself produces a mild burning/stinging pain; but more than half of the patients in one study did not know they hadbeen bitten.15 The venom exerts a specific effect on the central nervous system, causingdepletion of acetylcholine at motor nerve endings and provoking the release ofcatecholamines at adrenergic nerve endings. Unlike the skin necrosis or systemichemolysis associated with bites from the brown recluse spider, black widows producepain in the regional lymph nodes, usually in the axilla or inguinal area, piloerection,increased blood pressure and white blood cell count, and profuse sweating and nausea.The bite site may appear as a bluish-red spot with a white areola and sometimes aurticarial rash. Significant envenomization may be accompanied by systemic symptomsof weakness, tremor, severe myalgia, muscular spasm, a rigid boardlike abdomen, andtightness in the chest. Bites on the torso are more likely to cause muscle cramps inthe abdomen. Paralysis, stupor, and convulsions may occur in severe cases, and rarelydeath. The painful, rigid abdomen may be mistaken for appendicitis. Latrodectismcan also be misdiagnosed as an alimentary toxic infection, acute psychosis, tabiccrisis, pneumonia, tetanus, meningitis, acute renal failure, and various exanthematic
Figure 4Approximate geographic distributions of spiders causing necrotic arachnidism in the U.S. andCanada. (From: CDC, MMWR, 45, 1 1996.)

315
Spiders
A
B
Figure 5Brown recluse spider bite lesion development — treated with dapsone. Lesion at 3 days post-bite(A), 8 days (B), 12 days (C), 15 days (D), and 27 days (E).

316
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
C
D
Figure 5Continued.
diseases.15 Wingo16 reported that the mortality rate from black widow bites is <1%;Alexander17 said it is 4 to 6%. Other, related widow spiders are perhaps moredangerous. The redback spider, Latrodectus mactans hasselti, ubiquitous in Australia,can occasionally cause death in humans, and its bite is the commonest envenomizationrequiring antivenom in Australia, with at least 250 cases per year receiving antivenom.18
At least 17 deaths had been reported from bites by this species prior to developmentof antivenom.19

317
Spiders
Males and immature spiders also bite but usually produce milder symptoms. Somereferences indicate that the males are harmless due to the lesser amount of venominjected because of their smaller size and proportionately shorter chelicerae.
B. General Description
Mature female black widow spiders are shiny black with a leg span of 30 to 40 mm(Figure 6 and Color Figure 29-25). On the underside of the abdomen is a characteristicred or orange hourglass shaped marking. There is considerable variation among speciesand even subspecies (see Figure 6). Males are considerably smaller than females,averaging 16 to 20 mm in leg span, and have red and white marks on the dorsal sideof the abdomen. Immature widow spiders (spiderlings) are tan to grayish in color withvery little or no black. They have orange and white marking on their abdomens thatresemble “racing stripes.”
C. Geographic Distribution
Five species of widow spiders occur in America north of Mexico. Three (L. mactans,L. variolus, and L. hesperus) are similar in appearance. The black widow spider, L.mactans, is widely distributed in the U.S., occurring from southern New England toFlorida west to California and Oregon; it is more common in the southern part of therange. The northern black widow spider, L. variolus, occurs in the New England areaand adjacent Canada south to Florida and west to eastern Texas, Oklahoma, andKansas; it is more common in the northern part of this range. The western black widow,L. hesperus, is found in western Texas, Oklahoma, and Kansas north to the adjacentCanadian provinces and west to the Pacific Coast states. The brown widow spider, L.
E
Figure 5Continued.

318
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
geometricus, has been reported from southernFlorida and the coast of southern California; thered widow spider, L. bishopi, is limited to south-ern Florida.
Dangerous widow spiders in other parts ofthe world include L. geometricus (already men-tioned occurring in Florida and southern Cali-fornia), occuring worldwide in the tropics andsubtropics; the black widow subspecies L.mactans tredecimquttatus, in southern Europe;L. mactans hasselti, a problem in Australia andIndia; Latrodectus mactans cinctus, a danger-ous widow spider in South Africa; and L. mactansmenavodi, one of medical significance on theisland of Madagascar. The redback spider, L.mactans hasselti, is now established in Japan(probably imported from Australia).20
D. Biology/Behavior
Widow spiders are found in various habitats inthe wild, in protected places such as crawlspaces under buildings, in water meter hous-ings, holes in dirt embankments, piles of rocks,boards, bricks, or fire wood, and dense plantgrowth such as grain and cotton fields.
Inside buildings, they avoid strong light andfavor dark corners behind or underneath appli-ances or furniture that is seldom moved, ingarage corners, deep closets, damp cabinets,etc. With the advent of indoor plumbing, themost frequent site of encounter in previousdecades, the outdoor privy, has become lesscommon. Widow spiders will establish a webwherever conditions seem favorable, and if thereis a suitable food source, they may establish along-term infestation.
Widow spiders are active primarily duringthe warm months of the year. Few adults sur-vive cold winter weather, except indoors inheated places, but immature spiders may over-winter in large numbers. Mating takes place inthe spring. Contrary to popular belief, whichgave rise to the name black widow spider, themale is seldom killed and eaten by the female.If the female is well fed, the male usually leavesafter mating and may mate again with otherfemales. If the female is not well fed, she mayconsume the male for nutrients to produce the
WIDOW SPIDERS
Female Black Widow Spider, Latro-dectus mactans
ImportanceNeurotoxic venom
DistributionSeveral species almost worldwide
LesionMinimal — two puncta
Disease TransmissionNone
Key ReferenceMaretic, Z., Toxicon, 21, 457, 1983
TreatmentIce packs; muscle relaxants; sometimes
antivenin, calcium gluconate

319
Spiders
CASE HISTORY
UNKNOWN SPIDER BITE
An out-of-town ER physician called one night about a possible black widow (BW) spiderbite in a young boy. The family had killed the spider and brought it in with the boy. Byreport, it somewhat resembled a black widow. The site of the bite was unremarkable,except for two small puncta. At the time of the call, the boy was not exhibiting anysignificant pain, nausea, sweating, or other symptoms usually associated with BW bites.The physician asked for identification advice and possible suggestions on what course ofaction to take.
Based upon the description given over the telephone, the spider seemed to be an aberrantBW, a male BW, or possibly a closely related species, Latrodectus variolus. What seemedto be confusing the physician was the presence of several bright red hash marks on thedorsal side of the spider’s abdomen (not present on a “normal” BW) in addition to the redhourglass-shaped marking on its underside. The physician was informed that in all likeli-hood the specimen was a BW and the case should be treated as such (based upondevelopment of symptoms in that particular patient).
Comment: There are at least five species of “widow” spider in the U.S. Physicians shouldbe aware that not all widow spiders fit the typical black widow appearance (Figure 1). Somespecimens have red markings on the dorsal side of the body (in addition to the redhourglass-shaped mark on the underside of the abdomen). In addition, in some species, thehourglass marking is “broken” and not complete.
(Adapted in part from J. Agromed., 2, 53, 1995, Copyright 1995, the Hayworth Press,Binghamton, NY. With permission.)
Figure 1Typical female black widow underside showing red hourglass marking (Photo courtesyDr. James Jarratt, Mississippi Cooperative Extension Service).

320
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
eggs he fertilized, thus contributing to the success of the species. The female lays 250to 750 eggs at a time and spins a spherical sac of strong silk around them.
The young hatch in 2 to 4 weeks. After emerging from the egg sac they spin a strandof silk that enables them to be carried by the wind, dispersing them into thesurrounding area. Male black widow spiders molt 4 to 7 times and females molt 7 to9 times during a period of several weeks to several months, depending on thetemperature, food availability, and other factors. More than one brood can be producedin a summer, and as many as 2,000 offspring may be produced during a year. If theysurvive the winter, females may produce egg sacs the following year, and they may liveup to 3 years.
Widow spiders typically will be seen hanging upside down in their web, waiting forprey which includes many types of arthropods including insects and other spiders. Theprey’s contact with the web and subsequent struggle to free itself produces vibrations
Figure 6Widow spiders: dorsal view of Latrodectus mactans adult female, normal (A), and variantpattern (B), Latrodectus mactans adult female, ventral view (C). Dorsal view of L. variolus (D)and underside of L. variolus (E). Dorsal view of L. mactans male (F) and L. mactans immaturefemale (G).

321
Spiders
that the spider follows to locate the prey. The spider then seizes and bites the prey,injecting venom to paralyze and kill it so that it can be consumed. Venom is producedin two glands located in the basal segment of the chelicerae and is injected througha tiny hole in each of the two fangs.
Widow spiders are reclusive; they usually will not bite humans unless provoked.When their web is disturbed, they attempt to escape, but if teased or pursued, they willbite in self-defense.
E. Treatment of Bites
First aid for Latrodectus envenomization consists of cleansing the wound thoroughlyand applying ice packs to slow absorption of the venom. Incision of the wound andsuction to remove venom should not be attempted.
Cramps can usually be helped with muscle relaxants. If pain is severe, there is oftenquick response to sustained i.v. calcium gluconate; i.m. calcium gluconate is notadvisable, especially in infants and children. Calcium gluconate is used in preferenceto calcium chloride, because the gluconate lessens the danger of tissue necrosis fromaccidental extravasation. Tetanus vaccine status should be assessed. Physicians shouldmonitor for shock and treat as necessary. Antivenin is available for severe cases(especially Australian cases due to the redback spider), but it may be of little help onceillness has progressed and unnecessarily risky if given routinely for mild bites. Russellet al.21 recommend the muscle relaxant methocarbamol for adult uncomplicated cases.Children, the very elderly, and persons with hypertensive disease or other medicalconditions of risk need special attention, including hospitalization and possible antive-nin. If antivenin is given, the content of one vial (be sure and check package insert)is usually administered i.m. after tests for serum sensitivity are made. Symptoms shouldstart to subside in 0.5 to 3 h after administration of the antivenin.
Maretic,15 on the other hand, recommends i.v. administration of calcium salts andspecific antivenin. He says that during i.v. administration of calcium salts there is atypical feeling of warmth accompanied by the disappearance of pain, muscle cramps,and rigidity. However, the symptoms usually return within 20 min to a few hours. If,immediately after the injection of calcium, antivenin is also given i.v. (after appropriateeye or skin tests), the pain will not return.
IV. HOBO SPIDERSA. General and Medical Importance
Hobo spiders have only recently been recognized as causing necrotic lesions. Necroticspider bites in the states of Washington, Oregon, and Idaho have steadily increased infrequency during the last 20 years. At first, these were attributed to the brown reclusespider, but intensive efforts to find brown recluses in/near patients’ homes werefruitless. It is now believed that local effects of hobo spider (formerly called theaggressive house spider) envenomization are similar to those of brown recluse bites,and that the hobo spider is indeed the culprit.22,23 Akre and Myhre24 recorded 52 seriousbites from this species, Tegenaria agrestis, between 1989 and 1994.
Hobo spider bites are usually painless at first. Induration may appear within 30 min,surrounded by an area of expanding erythema that may reach a diameter of 5 to 15cm. Blisters develop within 15 to 35 h, subsequently rupturing with a serous exudate

322
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
encrusting the cratered wound. An eschar may develop with underlying necrosis andeventual sloughing of affected tissues. Lesions may require up to 3 years to heal if thebite occurred in fatty tissue.23 Systemic symptoms include headache (often prolonged),nausea, weakness, fatigue, memory loss, and vision impairment. Protracted and severesystemic effects may rarely lead to death.23
B. General Description
Hobo spiders are large, very fast-running specimens, about 45 mm in length (includinglegs), with distinct chevron stripes on the abdomen. They have eight eyes with boththe anterior and posterior eye rows in straight lines and have solid, light brown legs(not banded).
C. Geographic Distribution
Hobo spiders are native to Europe and were probably introduced into the Seattle areain the 1920s. They now occur from central Utah north to the Alaskan panhandle(Figure 4).
D. Biology/Behavior
Hobo spiders build funnel-shaped webs in or near houses. Common sites include rockwalls, along house foundations, in garages, piles of debris, and stacks of firewood. Bothmales and females build webs, and both may be in a single web in the late summerand fall. Mature males leave their webs in the fall to search for females. Male hobospiders enter houses in large numbers in the fall, but are usually restricted to basementsor ground floor rooms since they are poor climbers. Males are more venomous thanfemales, and are responsible for most bites.24
E. Treatment of Bites
Optimal treatment for necrotic spider bites is not well defined23 (see previous discus-sion under Violin Spiders for current ideas).
V. FUNNEL WEB SPIDERSA. General and Medical Importance
The Sydney funnel web spider, Atrax robustis, is Australia’s most dangerous spider,capable of causing death in as little as 15 min.25 There are several relatives of the Sydneyfunnel web which are also sometimes dangerous to humans. In many cases, little orno venom is injected during the biting event and no symptoms develop. If envenom-ization does occur, the bite site becomes extremely painful. Systemic symptoms maydevelop within minutes due to the toxin’s direct effect on somatic and autonomicnerves leading to widespread release of neurotransmitter. Progressive hypotension andapnea may ensue.

323
Spiders
B. General Description
The Sydney funnel web is a large, dark-colored aggressive spider with prominent fangs(Figure 7). The carapace is glossy dark brown to black, while the abdomen is usuallydark plum to black. The spiders often range in size from 45 to 60 mm (including legs);body length alone ranges from 15 to 45 mm. Males are smaller than females. Spinneretsare obvious, finger-like, and at the end of the abdomen.
C. Geographic Distribution
Sydney funnel web spiders are only found within about a 160-km radius of Sydney,Australia.25 Specifically, they occur from Newcastle to Nowra and west to Lithgow.Other related funnel webs occur all along the east coast of Australia.
D. Biology/Behavior
Sydney funnel webs live in burrows, rotting logs, tree holes, or crevices in rocks wherethey build (as their name implies) a funnel-shaped web. The web characteristicallycontains irregular silken trap lines radiating out from the burrow entrance. Coloniesmay consist of more than 100 spiders. Males may wander in search of females intohouses during summer, especially during rainy weather.
E. Treatment of Bites
Immediate first aid should be administered for bites by any large black spider alongthe east coast of Australia, but especially in the Sydney area. A pressure bandage canbe applied and the bitten limb immobilized using a splint. The spider should becaptured, if possible, for identification.
At a hospital, patients are usually carefully monitored for signs and symptoms for4 h25 (little or no venom may have been injected during the bite). If signs and symptomsoccur such as mouth numbness, tongue spasms, nausea, vomiting, profuse sweating,
Figure 7Sydney funnel web spider.

324
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
salivation, and other muscle spasms, administration of antivenom is indicated (perpackage insert instructions). Patients should be monitored closely for development ofallergic reactions to the antivenom.
VI. TARANTULA SPIDERSA. General and Medical Importance
Spiders in the family Theraphosidae are commonly called tarantulas in the U.S.;however, in other parts of the world this name is shared with other spiders, leadingto confusion. Because of their great size and reputation, tarantulas are sometimesfeared. This fear is unfounded. Tarantulas attack only when roughly handled ordeliberately provoked, and their bite is relatively minor (except in the case of a fewtropical species which have more toxic venom). Bites of the North American speciesvary from being almost painless to a deep, throbbing pain that may last for hours.Baerg26 allowed himself to be bitten twice, and reported mild pain (like that of pinpricks) lasting 15 to 30 min, not accompanied by inflammation or swelling. Hypersen-sitive individuals could have more severe reactions. Tarantula venom consists mainlyof hyaluronidase and a protein that is toxic to cockroaches and other arthropods forwhich it is intended.
Many tarantulas occurring in the Western Hemisphere have urticarial hairs on thedorsal surface of the abdomen. These hairs are “flicked off” by the spiders as adefensive mechanism.17 Urticarial hairs do not occur on African or Oriental species.Contact with these urticarial hairs on the skin or mucous membranes may result inpruritic papular lesions lasting for weeks. If the hairs get into the eyes, complicationscan arise with symptoms similar to ophthalmia nodosa.
B. General Description
Tarantulas are large hairy spiders. Their jaws (chelicerae) are attached on front of thehead and can move up and down, opening parallel to the long axis of the body (Figure8). Species native to the U.S. have a leg span of about 18 cm, but some South Americanjungle species have a span of 24 cm.
C. Geographic Distribution
About 30 species of tarantulas occur in the U.S., mostly in the southwestern states. Noneoccur east of the Mississippi River. Due to their popularity as pets, they can be foundin captivity all across the U.S. The majority of tarantulas sold in pet stores in the U.S.are imported species of Aphonopelma, which are especially attractive as pets becauseof their bright colors.
D. Biology/Behavior
Tarantulas hatch from eggs into spiderlings that look like a miniature version of theadult. They mature in 10 to 12 years. A male tarantula usually does not live longer thana year after becoming sexually mature, but the female life span may exceed 15 to 20years. In their native habitats, tarantulas dig burrows to rest in during the day. These

325
Spiders
burrows are often dug under large stones foundin open hillside areas among mixed desert flora.Tarantulas are sluggish during daytime and mayhibernate through the winter in colder areas.They emerge at night to hunt, usually rangingonly a few yards from the burrow. During themating season, males travel long distances fromtheir burrows in search of females, but femalesand immatures remain near their burrow through-out their life. Tarantulas have extremely pooreyesight and detect their prey by vibrations.Their diet consists of arthropods and small ver-tebrates.
E. Treatment of Bites
Treatment of tarantula bites consists of washingthe bite site thoroughly, keeping the affectedarea elevated, and administering systemic anal-gesics if the wound is painful. Because tarantulamouthparts are dirty, tetanus vaccine statusshould be assessed. Treatment for urticaria pro-duced by the abdominal hairs includes topicalcorticosteroids and oral antihistamines. If severeand widespread lesions occur, a short course of1 or 2 weeks of oral corticosteroids may beconsidered.
REFERENCES1. Carpenter, T. L., Bernacky, B. J., and Stabell,
E. E., Human envenomization by Plectreurystristis: a case report, J. Med. Entomol., 28, 477,1991.
2. King, L. E., Jr., Spider bites, Arch. Dermatol.,123, 41, 1987.
3. Atkins, J. A., Wingo, C. W., and Sodeman, W.A., Probable cause of necrotic spider bite inthe Midwest, Science, 126, 73, 1957.
4. Atkins, J. A., Wingo, C. W., Sodeman, W. A.,and Flynn, J. E., Necrotic arachnidism, Am. J.Trop. Med. Hyg., 7, 165, 1958.
5. Masters, E. J. and King, L. E., Jr., Differentiatingloxoscelism from Lyme disease, Emer. Med.,Aug. 1994, p. 48.
6. DeLozier, J. B., Reaves, L., King, L. E., Jr., andRees, R. S., Brown recluse spider bites of theupper extremity, S. Med. J., 81, 181, 1988.
TARANTULASPIDERS
Figure 8Adult female tarantula. (Photo courtesy of theRoss E. Hutchins Photograph Collection,Mississippi Entomological Museum, MississippiState University.)
ImportancePainful bites; urticating hairs
DistributionU.S., Central and South America, Africa
LesionBites — generally just pin prick type
lesions; abdominal hairs — maycause itchy pruritic lesions
Disease TransmissionNone
Key ReferenceBaerg, W. J., Sci. Month, 14, 482, 1922
TreatmentBites — analgesics, tetanus prophylaxis;
urticarial lesions — corticosteroidsand antihistamines

326
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
7. Murray, L.M. and Seger, D. L., Hemolytic anemia following a presumptive brown reclusespider bite, Clin. Toxicol., 32, 451, 1994.
8. Bey, T. A., Walter, F.G., Lober, W., Schmidt, J., Spark, R., and Schlievert, P.M., Loxoscelesarizonica bite associated with shock, Ann. Emerg. Med., 30, 701, 1997.
9 Rees, R., Campbell, D., Rieger, E., and King, L. E., Jr., The diagnosis and treatment ofbrown recluse spider bites, Ann. Emerg. Med., 16, 945, 1987.
10. Rees, R.S., Altenbern, D.P., Lynch, J.B., and King, L.E., Jr., Brown recluse spider bites: acomparison of early surgical excision versus dapsone and delayed surgical excision, Ann.Surg., 202, 659, 1985.
11. King, L.E., Jr. and Rees, R.S., Dapsone treatment of a brown recluse bite, J.A.M.A., 250, 648, 1983.
12. Nonavinakere, V.K., Stamm, P.L. and Early, J.L. II, A case study of brown recluse spider bite: roleof the community pharmacist in achieving a successful outcome, J. Agromed., 3, 37, 1996.
13. Phillips, S., Kohn, M., Baker, D., Vander Leest, R., Gomez, H., McKinney, P., McGoldrick,J. and Brent, J., Therapy of brown spider envenomation: a controlled trail of hyperbaricoxygen, dapsone, and cyproheptadine, Ann. Emerg. Med., 25, 363, 1995.
14. Masters, E., Sams, H. and King, L.E., Jr., Loxoscelism, N. Engl. J. Med. 339, 1945, 1998.
15. Maretic´, Z., Latrodectism: variations in clinical manifestations provoked by Latrodectusspecies of spiders, Toxicon, 21, 457, 1983.
16. Wingo, C. W., Poisonous spiders, Mo. Agri. Exp. Sta. Bull. No. 738, 1960.
17. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 14.
18. Sutherland, S.K., Australian Animal Toxins: The Creatures, Their Toxins, and Care of thePoisoned Patient, Melbourne, Oxford University Press, 1983, p. 275.
19. Wiener, S., Spider bite in Australia: an analysis of 167 cases, Med. J. Austr., 48, 44, 1961.
20. Horton, P., Redback spider is now established in Japan: bites can be recognized by aunique sign, Br. Med. J., 314, 1484, 1997.
21. Russell, F. E., Wainschel, J., and Gertsch, W. J., Bites of spiders and other arthropods, inCurrent Therapy, Conn, H. F., Ed., W. B. Saunders, Philadelphia, 1973, 868.
22. Vest, D.K., Necrotic arachnidism in the northwest United States and its probable relationshipto Tegenaria agrestis spiders, Toxicon, 25, 175, 1987.
23. CDC, Necrotic arachnidism – Pacific Northwest, 1988-1996, CDC, Morbidity and MortalityWeekly Rep., 45, 1, 1996.
24. Akre, R.D. and Myhre, E.A., The great spider whodunit, Pest Control Technology, AprilIssue, pg. 44, 1994.
25. Hawdon, G.M. and Winkel K.D., Spider bite: a rational approach, Austral. Fam. Phys., 26,1380, 1997.
26. Baerg, W. J., Regarding the habits of tarantulas and the effects of their poison, Sci. Month.,14, 482, 1922.

327
Ticks
CHAPTER 30
TICKS
TABLE OF CONTENTS
I. General and Medical Importance ...................................................................327A. Lyme Borreliosis ..........................................................................................329B. Rocky Mountain Spotted Fever ..................................................................332C. Other Spotted Fever Group Rickettsiae ....................................................334D. Ehrlichiosis ...................................................................................................335E. Babesiosis ....................................................................................................336F. Tularemia .....................................................................................................337G. Colorado Tick Fever ...................................................................................338H. Relapsing Fever ...........................................................................................339I. Tick-Borne Encephalitis ..............................................................................339J. Tick Paralysis ...............................................................................................340
II. General Biology/Ecology ................................................................................341
III. Tick Identification ............................................................................................346
IV. Discussion of Some of the Common U.S. Species .......................................348
V. Discussion of Some Major Pest Species in Other Areas ofthe World .........................................................................................................361
References ......................................................................................................................383
I. GENERAL AND MEDICAL IMPORTANCE
Ticks are blood-sucking ectoparasites which are efficient vectors of several differenttypes of disease agents such as bacteria, viruses, rickettsiae, and protozoans (see ColorFigure 30-26). In fact, they are second only to mosquitoes as arthropod vectors ofhuman disease. Listed in Table 1 are 13 of the common diseases produced by tick-

328
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Table 1Major Tick-Borne Diseases Worldwide
CausativeDisease Agent Where Occurs Tick Vectors
Lyme disease Spirochete U.S., Europe, Japan, Primarily Ixodes ricinus China, Australia complex
Rocky mountain Rickettsia U.S., Canada, Mexico, Dermacentor variabilis, spotted fever Central and South D. andersoni, others
AmericaSiberian tick Rickettsia Asiatic Russia, some Primarily D. marginatus, typhus islands in Sea of D. silvarum, D. nuttalli
JapanBoutonneuse fever Rickettsia Southern Europe, India, Rhipicephalus sanguineus,
Mediterranean area, R. appendiculatus, Africa Haemaphysalis leachi, others
Tularemia Bacterium U.S., Europe, Russia, Amblyomma americanum, Japan, Canada, D. variabilis, D. nuttalli, Mexico I. ricinus
Colorado tick fever Virus Mountain states of Primarily D. andersoni western U.S., British Columbia, Canada
Human tick-borne Rickettsia Mainly eastern and A. americanum, I. scapularis ehrlichiosis (Ehrlichia) central U.S.American Protozoan U.S., in Massachusetts I. scapularis babesiosis and New York areaTick paralysis Salivary toxin U.S., particularly D. andersoni, D. variabilis,
Montana, British I. holocyclus Columbia border, Australia
Relapsing fever Spirochete Almost worldwide, in Ornithodoros spp., U.S. cases U.S., primarily in mostly from O. hermsi Washington, Oregon, California
Tick-borne Virus Eastern and western I. ricinus, I. persulcatus, encephalitis Europe D. marginatus, othersCrimean Congo Virus Former U.S.S.R., Hyalomma marginatum, hemorrhagic Pakistan, Bulgaria, H. anatolicum fever Iraq, Yugoslavia,
ChinaKyasanur forest Virus India, especially H. spinigera disease Karnataka State

329
Ticks
transmitted agents, and a discussion of the major ones is provided below. The readeris referred to other references1-5 for more complete information on the natural history,epidemiology, and treatment of these diseases.
A. Lyme borreliosis
Lyme borreliosis (LB), caused by the spirochete, Borrelia burgdorferi (there are at least3 “genospecies” of this organism), is a systemic tick-borne illness with many clinicalmanifestations that occurs over much of the world in temperate zones. Although rarelyfatal, the disease may be long and debilitating with cardiac, neurologic, and joint
OFTEN ASKED QUESTION
HOW DO TICKS GET ON PEOPLE?
There is considerable confusion among the public as to how ticks get on people. Folklorehas it that they live in pine thickets, hide under bark, and/or fall out of trees on unsuspectingpassersby. Frequently, park rangers or other outdoor workers erroneously recommend a hatfor protection against ticks (presumably to guard against falling ticks). But ticks cannot fly,jump, or swim. They “quest” for host animals by climbing vegetation and passively waiting.The height of questing varies by species and life stage, but usually is 3 ft or less (often justa few inches). If environmental conditions are favorable, they may stay atop the vegetationfor hours or even days. When a potential host approaches, signaled by vibrations or carbondioxide, questing ticks may wave their legs (Figure 1) or move around on the plant tryingto get on the animal. Once on the host, they crawl around for some time looking for asuitable place to feed. Since ticks often attach in the scalp of humans, it is falsely assumedthat they fall out of trees.
Figure 1Ticks crawl up blades of grass to “quest” for passing hosts.

330
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
involvement. Initial symptoms include a flu-like syndrome with headache, stiff neck,myalgias, arthralgias, malaise, and low-grade fever. Often, a more or less circular,painless, macular dermatitis is present at the bite site called erythema migrans (EM).The EM lesion is often said to be pathognomonic for LB, although not all patientsdevelop it. EM lesions may steadily increase in size with subsequent central clearing.Untreated EM and associated symptoms usually resolve in 3 to 4 weeks. However, thedisease often disseminates within weeks or months, resulting in cardiac, neurologic,and joint manifestations. Symptoms may include Lyme carditis, cranial neuropathy,radiculopathy, diffuse peripheral neuropathy, meningitis, and asymmetric oligoarticulararthritis. The number of reported LB cases in the U.S. continues to increase. There were17,730 cases reported to the CDC in 2000.6 In the U.S., the vast majority of cases arefrom the northeastern and northcentral states (Figure 1).
Lyme borreliosis is solely tick-borne. In the U.S., Ixodes scapularis is the primaryvector in the East, and Ixodes pacificus in the West. In Europe, I. ricinus and I.
CASE HISTORYTICK ON MAN’S EARDRUM
One week after sleeping on the ground near Mexican Hat, Utah, a man began to havesevere pain in his right ear. After a few days, lymphadenitis developed in the neck regionsurrounding the ear. He was seen by a family physician approximately seven days later,who referred him to an ENT. Four days later (and 18 days after camping) the ENT examinedhis eardrum, found a small, “crab-like” creature attached, and removed it (Figure 1). Sincenone of the physicians in the medical group knew exactly what the creature was, the patient— with specimen in hand — was referred to a parasitologist at the University of MississippiMedical Center. The parasitologist identified the specimen as a “tick”, and referred thepatient to the Mississippi Department of Health for more specific identification. The tickwas identified as a nymphal spinose ear tick, Otobius megnini. The patient recovereduneventfully.
Comment: This tick belongs to the soft tick family. Most ticks seen by people are hard ticks— the ones that attach to a vertebrate host such as a dog or deer and remain attached fora week or so. Soft ticks are classified in another entire tick family since they differ from hardticks in appearance and behavior. Soft ticks have little sexual dimorphism, have a wrinkled,granulated integument, and the mouthparts are generally not visible when the specimen isviewed from above. Soft ticks are especially adapted to dry climates or dry conditionswithin wet climates, and generally only feed on their vertebrate hosts for a short time (onehour or less), not remaining attached for days. Most soft tick species in the U.S. occur inthe West. The tick involved in this particular case differs from other soft ticks in that thelarval and nymphal stages will invade ears of cattle, horses, sheep, deer, and other wildanimals and remain attached for long periods of time. There have been records of thisspecies remaining in the ears of animals for as long as 121 days. The scientific literaturecontains several records of this species being found in the ears of humans.
This case is interesting and illuminates several issues. For one thing, people travel and maybring back with them all sorts of parasites or microbes. Species that normally do not occurin an area may be seen from time to time by practicing physicians. Second, none of thephysicians knew that this creature was a tick. To their credit, the physicians knew that thespecimen was some sort of parasite, and referred the man to a parasitologist. The parasi-tologist — a broadly trained, organismal-level scientist knowing a wide range of internaland external parasites on sight — immediately knew it was a tick. The medical community

331
Ticks
needs such scientists, especially in light of rapid, modern travel methods and immigration(both legal and illegal). In the last 20 years or so, there has been a drift away fromorganismal-level training, with increasing emphasis on molecular biology. But there willalways be a need for scientists who can “eyeball” a specimen and place it in its appropriatetaxonomic group. A key to treatment strategies in such cases is knowledge of the biology/behavior of the parasite and what diseases, if any, it transmits.
Figure 1Tick removed from patient’s eardrum.
persulcatus serve as principal vectors of the Borrelia. In Asia, vectors include I.persulcatus, I. ovatus, I. granulatus, I. moschiferi, and a few Haemaphysalis species.
Two important aspects of vector-borne disease ecology are host availability anddiversity. If immature ticks feed on hosts that are refractory to infection with the LBspirochete, then overall prevalence of the disease agent in an area will decline. On theother hand, if an abundant host is available that also is able to be infected with B.burgdorferi producing long and persistent spirochetemias, then prevalence of tickinfection increases. This is precisely the case in the northeastern and upper midwesternU.S. In those areas the primary host for immature I. scapularis is the white-footedmouse which is capable of infecting nearly 100% of larval ticks during feeding. Sinceinfection can be transferred from tick stage to tick stage, this obviously leads to highnumbers of infected nymphs and adults. In the West and South, tick infection rates aremuch lower (and hence, lower numbers of LB cases). This is attributed to the fact thatimmature stages of I. scapularis and I. pacificus feed primarily on lizards which are

332
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
incompetent as reservoirs and incapable of infecting ticks. Another factor affecting thedynamics of LB is the fact that nymphal I. scapularis are the stage primarily bitingpeople and transmitting the disease agent in the Northeast, whereas in the South,nymphal I. scapularis rarely, if ever, bite humans. Adult ticks are certainly capable oftransmitting the LB agent in all areas — North, South, or West — but adult ticks arelarge enough to be easily seen and removed by people. Nymphs, on the other hand,are about the size of the head of a pin and may be easily overlooked or confused witha freckle.
Other tick species may be involved in the ecology of Lyme borreliosis in the U.S.Alterrnatively, there may be several, as of yet undescribed, Borrelia species whichcause Lyme-like illness. In the southern U.S. there have been reports for years aboutan LB-like illness which other researchers have voiced doubts about — doubts as towhether or not it is true LB. Also, it has been widely known for some time that 1 to3% of lone star ticks, Amblyomma americanum, harbor spirochetes that react withreagents prepared against B. burgdorferi. Recent evidence has shed light on thiscontroversy, revealing that the lone star tick spirochetes are a true Borrelia species(called lonestari), but distinct from the LB agent.7 Therefore, some cases of LB-likeillness in the southeastern and southcentral U.S. may be due to this new spirochete andnot true B. burgdorferi. At least one case of erythema migrans has been caused by B.lonestari.7a
B. Rocky Mountain spotted fever
Ticks may transmit a wide variety of rickettsial organisms, classified by scientists intoseveral distinct groups. The spotted fever group (SFG) contains rickettsial species
Figure 1Reported number of Lyme disease cases by county — United States, 2000 (CDC figure).

333
Ticks
Table 2Epidemiologic Information on Six Spotted Fever Group Rickettsiae
Rickettsia Disease Tick/Mite Vectors Distribution
R. rickettsii RMSF Primarily ticks Dermacentor Western hemispherevariabilis and D. andersoni
R. conorii Boutonneuse Fever Primarily ticks in genera Africa, MediterraneanRhipicephalus, Hyalomma, area, Middle Eastand Haemaphysalis
R. siberica North Asian Tick Primarily ticks in genera Siberia, central Asia,Typhus (Siberian Dermacentor and Hyalomma MongoliaTick Typhus)
R. australis Queensland Tick Tick, Ixodes holocyclus AustraliaTyphus
R. africae African Tick Bite Tick, Amblyomma hebraeum Sub-Saharan AfricaFever
R. japonica Japanese Spotted Haemaphysalis flava, JapanFever H. longicornis, Ixodes ovatus
related to the agent of Rocky mountain spotted fever, Rickettsia rickettsii. But there aremany other rickettsial species in the spotted fever group; it contains at least 6 diseaseagents and 15 others with low or no pathogenicity to humans. Table 2 presents somedistributional and epidemiologic information on six human disease-causing SFG rick-ettsiae. Rocky Mountain spotted fever (RMSF) is the most frequently reported rickettsialdisease in the U.S. with about 600 cases reported each year.8 Probably many more casesoccur but go unreported. If an unusual febrile illness is treated successfully with oneof the tetracyclines, there may be little interest in follow-up and reporting. At the timeof initial presentation, there is often the classic triad of RMSF — fever, rash, and historyof tick bite. Other characteristics are malaise, severe headache, chills, and myalgias.Sometimes gastrointestinal symptoms such as abdominal pain and diarrhea are re-ported. The rash, appearing on the third day or after, usually begins on the extremitiesand then spreads to the rest of the body. However, there have been confirmed caseswithout rash. Mental confusion, coma, and death may occur in severe cases. Untreated,the mortality rate is about 20%; even with treatment the rate is 4%.
Laboratory findings may include hyponatremia (20 to 50% of cases), thrombocytope-nia (30 to 50% of cases), anemia (5 to 25% of cases), and mildly elevated aminotrans-ferase levels (40 to 60% of cases). There are no widely available, specific laboratorytests for the diagnosis of RMSF, although serological tests such as IFA may help confirmthe disease later. Diagnosis and treatment decisions for RMSF are based onclinical and epidemiologic clues and should never be delayed pending labora-tory confirmation.
RMSF is usually transmitted by the bite of an infected tick (Figure 2). Not all tickspecies are effective vectors of the rickettsia, and, even in the vector species, not allticks are infected. Therefore, the presence of an infected tick in an area is like a needlein a haystack. Generally, only 1 to 5% of vector ticks in an area are infected. Severaltick vectors may transmit RMSF organisms, but the primary ones are the American dogtick, Dermacentor variabilis (Color Figure 30-27) in the eastern U.S., and D. andersoni

334
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
in the West. Adults of both species feed on a variety of medium to large mammals andhumans. Ticks are often brought into close contact with people via pet dogs or cats(dog ticks may also feed on cats).
C. Other spotted fever group rickettsioses
Boutonneuse Fever. Boutonneuse fever (BF), or Mediterranean spotted fever, causedby Rickettsia conorii, is widely distributed in Africa, areas surrounding the Mediterra-nean, southern Europe, and India. The name is derived from the black, button-likelesion (eschar) at the site of tick bite. BF resembles a mild form of RMSF, characterizedby mild to moderately severe fever and a rash usually involving the palms and soles.Several tick species serve as vectors of the agent to humans, but especially Rhipiceph-alus sanguineus, R. appendiculatus, and Amblyomma hebraeum.
African Tick-Bite Fever. African tick-bite fever (ATBF), caused by a newly describedspotted fever group rickettsia, Rickettsia africae, is clinically similar to BF with theexception that there is usually an absence of rash in ATBF patients.8a, 8b ATBF alsoproduces an eschar. The disease has been recognized in sub-Sharan Africa, and isbelieved to be transmitted by Amblyomma hebraeum ticks.
Siberian Tick Typhus. Siberian tick typhus (STT), or North Asian tick typhus, causedby Rickettsia siberica, is very similar clinically to RMSF with fever, headache, and rash.The disease can be mild to severe, but is seldom fatal. STT was first recognized in theSiberian forests and steppes in the 1930s, but now is known to occur in many areasof Asiatic Russia and on islands in the Sea of Japan. Various hard ticks are vectors ofthe agent, but especially Dermacentor marginatus, D. silvarum, D. nuttalli, andHaemaphysalis concinna.
Queensland Tick Typhus. Queensland tick typhus (QTT), caused by Rickettsiaaustralis, occurs along the east coast of Australia and is named after the northeastern
Figure 2Life cycle of Rocky Mountain spotted fever.

335
Ticks
Australian state of Queensland. It is primarily restricted to dense forests interspersedwith grassy savanna or secondary scrub. Most patients have fever, headache, and rashthat may be vesicular and petechial — even pustular. Commonly, there is an escharat the site of the tick bite. The agent of QTT is transmitted to humans by the bite ofan infected Ixodes holocyclus tick.
D. Ehrlichiosis
Ehrlichia organisms are rickettsiae which primarily infect circulating leukocytes. Muchof the knowledge gained concerning ehrlichiae has come from the veterinary scienceswith intensive studies on Anaplasma marginale (cattle disease agent), Ehrlichia(Cowdria) ruminantium (cattle, sheep, goats), Ehrlichia equi (horses), and Anaplasma(Ehrlichia) phagocytophila (sheep, cattle, deer). Canine ehrlichiosis, caused by Ehrlichiacanis, wiped out 200 to 300 military working dogs during the Vietnam War.9 In the U.S.,human cases of ehrlichiosis were unknown until a report in March 1986 of a 51-year-old man who had been bitten by a tick in Arkansas and was sick for 5 days before beingadmitted to a hospital in Detroit.10 He had malaise, fever, headache, myalgia, pancy-topenia, abnormal liver function, renal failure, and high titers of E. canis antibodies thatfell sharply during convalescence. The patient was thought to have the dog disease.It turned out not to be the case. For this reason, in the literature there are several reportsof human infection with E. canis, when, in fact, human ehrlichiosis is caused by otherclosely related Ehrlichia organisms. As of this writing, there are three ehrlichial diseaseagents infecting humans in the U.S.* One, Ehrlichia chaffeensis, the causative agent ofhuman monocytic ehrlichiosis (HME), occurs mostly in the southern and south-centralU.S., and infects mononuclear phagocytes in blood and tissues.11 Another, Anaplasma(Ehrlichia) (near) phagocytophila, infects granulocytes and causes human granulocyticehrlichiosis (HGE); it is mostly reported from the upper midwest and northeastern U.S.The reason the HGE organism is sometimes called (near) phagocytophila is because itis could be a new species, but closely related to phagocytophila. The third, E. ewingii,causes a clinical illness similar to the other two, but thus far, has only been identifiedin a few patients, most of whom were immune compromised.11a Therefore, much is yetunknown about human infection with this agent.
Clinical and laboratory manifestations of infection with HME or HGE are similar. Thepatient usually presents with fever, headache, myalgia, progressive leukopenia (oftenwith a left shift), thrombocytopenia, and anemia. In addition, there may be moderateelevations in levels of hepatic transaminases. Sometimes there is a cough, gastroenteri-tis, or meningitis. Rarely is there a rash, so ehrlichiosis is often called “spotless” RMSF.Illness due to HME is thought by some to be milder than with HGE; reported fatalityrates are 2 to 5% and 7 to 10% for HME and HGE, respectively. Some research hasindicated that both ehrlichial agents alter the patient’s immune system, allowingopportunistic infections such as fungal pneumonia to occur. Diagnosis depends mainlyon clinical findings, although IFA tests may be used to detect antibodies against therespective ehrlichial agent.
* Note: Recent reclassification of these organisms has moved the HGE agent from genes Ehrlichia to Ana-plasma. This will likely lead to confusion since Anaplasma organisms have traditionally been associatedwith cattle disease. In this section, we will continue to call infection with HGE agent “ehrlichiosis” and not“anaplasmosis.”

336
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Ehrlichiosis is transmitted to humans via the bite of an infected tick. HME, primarilyoccurring within the geographic distribution of the lone star tick, Amblyommaamericanum, seems to have a close association with that tick and the white-tailed (WT)deer. Lone star ticks (LST) generally occur from central Texas east to the Atlantic Coastand north to approximately Iowa and New York. WT deer, possibly along with dogsor small rodents, serve as reservoir hosts for the agent, and LSTs are the likely vectors.However, detection of the HME agent in other tick vectors and a few cases outside thedistribution of LST may indicate that additional vectors occur.
The ecology of HGE is not well known at this time. It has been diagnosed mostlyin patients from the upper midwest and northeastern U.S., although cases have beenreported in Florida, Arkansas, and California. The tick vector is Ixodes scapularis, thesame species that transmits the agent of Lyme borreliosis; thus, there is the possibilityof co-infection with Lyme borreliosis and HGE (and even babesiosis). Possible animalreservoirs of the HGE agent include deer and small rodents.
E. Babesiosis
Human babesiosis is a tick-borne disease primarily associated with two protozoa of thefamily Piroplasmordia: Babesia microti and Babesia divergens, although other, newlyrecognized species may also cause human infection. The disease is a malaria-likesyndrome characterized by fever, fatigue, and hemolytic anemia lasting from severaldays to a few months. In terms of clinical manifestations, babesiosis may vary widely,from asymptomatic infection to a severe, rapidly fatal disease. The first demonstratedcase of human babesiosis in the world was reported in Europe in 1957.12 Since then,there have been at least 28 additional cases in Europe.12 Most European cases occurredin asplenic individuals and were with Babesia divergens, a cattle parasite. In the U.S.there have been hundreds of cases of babesiosis (most with intact spleens), mainlycaused by Babesia microti, mostly from southern New England, and specificallyNantucket, Martha’s Vineyard, Shelter Island, Long Island, and Connecticut.13, 14 The tickvector in Europe is believed to be the European castor bean tick, Ixodes ricinus, oneof the most commonly encountered ticks in central and western Europe. In the U.S.,cases of human infection by Babesia microti are caused by bites from the same tickthat transmits the agent of Lyme borreliosis, Ixodes scapularis.
Babesiosis is very similar clinically to malaria; in fact, confusion between the twodiseases is often reported in the scientific literature. Headache, fever, chills, nausea,vomiting, myalgia, altered mental status, disseminated intravascular coagulation, ane-mia with dyserythropoiesis, hypotension, respiratory distress, and renal insufficiencyare common to both diseases. However, the symptoms of babesiosis do not showperiodicity. The incubation period varies from 1 to 4 weeks. Physical exam of patientsis generally unremarkable, although the spleen and liver may be palpable. Diagnosisof babesiosis is based upon recognition of the organism within erythrocytes in Giemsa-stained blood smears.
Babesial parasites, along with members of the genus Theileria, are called piroplasmsbecause of their pear-shaped intraerythrocytic stages. There are at least 100 species oftick-transmitted Babesia, parasitizing a wide variety of vertebrate animals. Somenotorious ones are as follows: Babesia bigemina, the causative agent of Texas cattlefever; B. canis and B. gibsoni, canine pathogens; B. equi, a horse pathogen thatoccasionally infects humans; B. divergens, a cattle parasite that infects humans; and B.microti, a rodent parasite that infects humans. Recently, new Babesia species have been

337
Ticks
recovered from ill humans and have tentatively been variously designated as the WA1agent, the CA1 agent, or the MO1 agent.12, 15 The WA1 agent, isolated from a patientin Washington State, was particularly interesting because the man was only 41 yearsold, had an intact spleen, and was immunocompetent.15 Although the parasites weremorphologically identical to Babesia microti, the patient did not develop a substantialantibody to Babesia microti antigens. Subsequent DNA sequencing of the organismindicated that it was most closely related to the canine pathogen Babesia gibsoni.Obviously, there is much to be learned about the many and varied Babesia species,and their complex interactions in nature.
F. Tularemia
Tularemia, sometimes called rabbit fever or deer fly fever, is a bacterial zoonosis thatoccurs throughout temperate climates of the northern hemisphere. Approximately 150to 300 cases occur in the U.S. each year, but most cases occur in Arkansas, Missouri,and Oklahoma (Figure 3).8 The causative organism, Francisella tularensis, is a small,gram-negative, non-motile cocco-bacillus named after Sir Edward Francis (who did theclassical early studies on the organism) and Tulare, California (where it was firstisolated). The disease may be contracted in a variety of ways — food, water, mud,articles of clothing, and (particulary) arthropod bites. Arthropods involved in transmis-sion of tularemia include ticks, biting flies, and possibly even mosquitoes. Ticksaccount for more than 50% of all cases, especially west of the Mississippi River.Tularemia may present as several different clinical syndromes, including glandular,ulceroglandular, oculoglandular, oropharangeal, pneumonic, and typhoidal. In general,the clinical course is characterized by an influenza-like attack with severe initial fever,
Figure 3Reported number of tularemia cases — United States, 1990–2000 (CDC figure).

338
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
temporary remission, and a subsequent febrile period of at least two weeks. Later, alocal lesion with or without glandular involvement may occur. Additional symptomsvary depending upon the method of transmission and form of the disease (seediscussion below). Untreated, the mortality rate for tularemia is about 8%; earlydiagnosis and treatment can reduce that to 1 to 2%.
Depending upon the route of entry of the causative organism, tularemia may beclassified in several ways. The most common is ulceroglandular — resulting fromcutaneous inoculation — characterized by an ulcer with sharp undetermined bordersand a flat base. Location of the ulcers may help identify the mode of transmission.Ulcers on the upper extremities are often a result of exposure to infected animals,whereas ulcers on the lower extremities, back, or abdomen most often reflect arthropodtransmission. When there is lymphadenopathy without an ulcerative lesion, the clas-sification glandular tularemia is used. If the tularemia bacterium enters via the conjunc-tivae, oculoglandular tularemia may result. Oropharyngeal tularemia results fromingestion of contaminated food or water. If airborne transmission of the agent isinvolved, the pneumonic form occurs. These patients often present with fever, a non-productive cough, dyspnea, and chest pain. Finally, tularemia may be classified astyphoidal, characterized by disseminated infection mimicking typhoid fever, brucello-sis, tuberculosis, or some of the Rocky Mountain spotted fever-type infections.
In ticks, tularemia infection occurs in both the gut and body tissues and hemolymphfluid (tick blood). Infection is known to persist for many months and even years insome species. Tularemia organisms may be passed from tick stage to tick stage, andto the offspring of infected female ticks. The three major North American ticks involvedin transmission of tularemia organisms are the lone star tick, Amblyomma americanum,the Rocky Mountain wood tick, Dermacentor andersoni, and the American dog tick,Dermacentor variabilis. Both the lone star tick and the American dog tick occur overmuch of the eastern U.S.; the Rocky Mountain wood tick occurs in the West. All threeof these tick species are avid human biters. In Central and Western Europe, Ixodesricinus is probably a vector. Dermacentor nuttalli may be a vector in Russia. Derma-centor dagestanicus (=niveus) and Rhipicephalus pumilio may be vectors in Kazakhstan.
G. Colorado tick fever
Colorado tick fever (CTF) is a generally moderate, acute, self-limited, febrile illnesscaused by an Orbivirus in the Reoviridae. Typically, onset of CTF is sudden, with chillysensations, high fever, headache, photophobia, mild conjunctivitis, lethargy, myalgias,and arthralgias. The temperature pattern may be biphasic, with a 2- to 3-day febrileperiod, a remission lasting 1 to 2 days, then another 2 to 3 days of fever, sometimeswith more severe symptoms.16 Rarely, the disease may become severe in children withencephalitis, myocarditis, or tendency to bleed. Infrequently, a transient rash mayaccompany infection. Recovery is usually prompt, but a few fatal cases have beenreported. CTF occurs in areas above 4,000 feet in at least 11 western states (SouthDakota, Montana, Wyoming, Colorado, New Mexico, Utah, Idaho, Nevada, Washing-ton, Oregon, and California) and in British Columbia and Alberta, Canada. Exact casenumbers are hard to ascertain since many cases may be so mild that ill persons fail toseek medical care, but approximately 200 to 400 cases are reported in the U.S. annually.Peak incidence is during April and May at lower elevations and during June and Julyat higher elevations. The virus is maintained in nature by cycles of infection amongvarious small mammals and the ticks which parasitize them. Infection in humans is by

339
Ticks
the bite of an infected tick. Several tick species have been found infected with the virus,but Dermacentor andersoni is by far the most common. This tick is especially prevalentwhere there is brushy vegetation to provide good protection for small mammalian hostsof immature ticks and yet with sufficient forage to attract large hosts required for theadults.
H. Relapsing fever
Tick-borne (endemic) relapsing fever (TBRF) is a systemic spirochetal disease charac-terized by periods of fever lasting 2 to 9 days alternating with afebrile periods of 2 to4 days. The total number of relapses can vary from 1 to 10 or more, lasting two or threeweeks. Transitory petechial rashes are common during the initial febrile period.Untreated, the mortality rate is between 2 and 10%. Several hundred cases are reportedworldwide each year, with approximately 30 to 50 of those being diagnosed in the U.S.(primarily in Washington, Oregon, and northern California).
TBRF is caused by Borrelia recurrentis, or various tick-adapted strains of thisorganism (many authors maintain that each tick-adapted strain is a distinct species) (seeColor Figure 30-28). The spirochetes are transmitted to humans by several species ofsoft ticks in the genus Ornithodoros. Since soft ticks generally feed for only a shortperiod of time (30 min or so), the victim may be unaware of any recent tick bites.Rodents serve as a natural source of infection for ticks, and transmission is by tick bite(saliva) and also sometimes through contamination of the bite wound with infectivecoxal fluid produced by feeding ticks just before they detach. Transstadial andtransovarial transmission of the agent occurs readily; thus, the ticks are reservoirs ofinfection. The disease is endemic across central Asia, northern Africa, tropical Africa,parts of the Middle East, and North and South America.17 Foci of infection are restrictedto Ornithodoros-infested areas such as huts, caves, log cabins, cattle barns, anduninhabited houses. Outbreaks in the western U.S. have most often been associatedwith mountain cabins or rented state or federal park cabins.18, 19
I. Tick-borne encephalitis
Tick-borne encephalitis (TBE) should be considered a general term encompassing atleast three diseases caused by similar flaviviruses spanning from the British Isles(Louping ill), across Europe (Central European tick-borne encephalitis), to far-easternRussia (Russian spring-summer encephalitis [RSSE]). The three diseases also differ inseverity — Louping ill being the mildest and RSSE the worst. In Central Europe thetypical case has a biphasic course with an early, viremic, flu-like stage, followed abouta week later by the appearance of signs of meningoencephalitis.20 CNS disease isrelatively mild, but occasional severe motor dysfunction and permanent disabilityoccur. The case fatality rate is 1 to 5%.21 RSSE (sometimes referred to as the “far easternform”) is characterized by violent headache, high fever, nausea, and vomiting. De-lirium, coma, paralysis, and death may follow; the mortality rate is about 25 to 30%.A recent report showed that new variants of TBE virus in Russia may produce ahemorrhagic syndrome.21a Louping ill — named after a Scottish sheep disease — inhumans also displays a biphasic pattern and is generally mild.1 As mentioned, the virusinfects sheep; few cases are actually ever reported in humans. Reported case numbersfor TBE (excluding the few Louping ill cases) is between 500 and 1000. Transmissionto humans is mostly by the bite of an infected tick; however, infection may also be

340
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
acquired via consuming infected milk and uncooked milk products. The distributionand seasonal incidence of TBE is closely related to the activity of the tick vectors —Ixodes ricinus in western and central Europe, and I. persulcatus in central and easternEurope (there is overlap of the two species). Ixodes ricinus is most active in spring andautumn. Two peaks of activity may be observed: one in late March to early June, andone from August to October. Ixodes persulcatus is usually active in spring and earlysummer. Apparently, I. persulcatus is more cold hardy than I. ricinus, thus inhabitingharsher, more northern areas.
Powassan encephalitis (POW) — also in the TBE subgroup — is a rare infection ofhumans that mostly occurs in the northeastern U.S. and adjacent regions of Canada.Characteristically, there is sudden onset of fever with temperature up to 40°C along withconvulsions. Also, accompanying encephalitis is usually severe, characterized byvomiting, respiratory distress, and prolonged, sustained fever. Only about 20 cases ofPOW have been reported in North America.22 Recognized cases have occurred inchildren and adults, with a case fatality rate of approximately 50%. POW is transmittedin an enzootic cycle among ticks (primarily Ixodes cookei) and rodents and carnivores.Ixodes cookei only occasionally bites people — this may explain the low case numbers.Antibody prevalence to POW in residents of affected areas is less than 1%, indicatingthat human exposure to the virus life cycle is a rare event.
J. Tick paralysis
Tick paralysis is characterized by an acute, ascending, flaccid motor paralysis that mayterminate fatally if the tick is not located and removed. The causative agent is believedto be a salivary toxin produced by ticks when they feed. In the strictest sense, tickparalysis is not a zoonosis; however, many contend that zoonoses should include notonly infections that humans acquire from animals, but also diseases induced by non-infective agents such as toxins and poisons.23 The disease is more common than onemight think. In North America, hundreds of cases have been documented from theMontana–British Columbia region.24, 25 It occurs in the southeastern U.S. as well. Tickparalysis is also especially common in Australia. Sporadic cases may occur in Europe,Africa, and South America.
The site of tick bite in a case of tick paralysis looks no different from that in caseswithout paralysis. There is a latent period of 4 to 6 days before the patient becomesrestless and irritable. Within 24 h there is an acute ascending lower motor neuronparalysis of the Landry type. It usually begins with weakness of the lower limbs,progressing in a matter of hours to falling down and obvious incoordination, which isprincipally due to muscle weakness, although rarely there may also be true ataxia.Finally, cranial nerve weakness with dysarthria and dysphagia leads to bulbar paralysis,respiratory failure, and death. In children, presenting features may include restlessness,irritability, malaise, and sometimes anorexia and/or vomiting. A tick may usually befound attached to the patient, usually on the head or neck. Some controversy occursover whether or not severity of symptoms is related to the proximity of the attachedtick to the patient’s brain. In one study, the case fatality rate in patients with ticksattached to the head or neck was higher than that in patients with ticks attachedelsewhere; however, the difference was not statistically significant. Although tickscausing paralysis are often attached to the head or neck, it must be noted that casesof paralysis may occur from tick bites anywhere on the body (published examples —external ear, breast, groin, and back26). Once the tick is found and removed, all

341
Ticks
symptoms usually disappear rapidly (there are exceptions to this, especially in Australiawith Ixodes holocyclus).
As many as 43 tick species in 10 genera have been incriminated in tick paralysis inhumans, other mammals, and birds.27 However, human cases of the malady mostlyoccur in only a few geographic regions, caused by three main tick species. In theNorthwestern U.S. and British Columbia region of North America, the Rocky Mountainwood tick, Dermacentor andersoni, is the principal tick involved. In the southeasternU.S. a related species, Dermacentor variabilis, known as the American dog tick, is themain cause of tick paralysis. Human cases in Australia are due to the Australianparalysis tick, Ixodes holocyclus.
Interestingly, not all feeding female ticks — even of the species known to causeparalysis — produce paralysis. Why, out of hundreds of tick bites, does one result inparalysis? There is some evidence that in cattle, sheep, and dogs numerous ticks feedingsimultaneously (to reach a minimum dose) is necessary to elicit paralysis. In humans,however, one tick is usually involved. Most researchers believe that tick paralysis iscaused by a toxin, but its nature is not well characterized. Generally, it is thought thatthe toxin is produced in the salivary glands of the female tick as she feeds. Onealternative view would be that the toxin is produced in tick ovaries and subsequentlypasses to the salivary glands during later stages of tick engorgement. Although the vastmajority of cases are due to female ticks, there are reports of male ticks causing limitedparalysis. This fact seems to argue against the ovary toxin theory. There are othertheories for the cause of the paralysis such as host reactions to components of the ticksaliva or possibly symbiotic rickettsial organisms commonly found in tick salivaryglands.
II. GENERAL BIOLOGY/ECOLOGY
There are three families of ticks recognized in the world today: (1) Ixodidae (hard ticks),(2) Argasidae (soft ticks), and (3) Nuttalliellidae (a small, curious, little-known group withsome characteristics of both hard and soft ticks). The terms hard and soft refer to thepresence of a dorsal scutum or “plate” in the Ixodidae, which is absent in the Argasidae.
Hard ticks display sexual dimorphism, males and females look obviously different(Figure 4), and the blood-fed females are capable of enormous expansion. Theirmouthparts are anteriorly attached and visible from dorsal view (Figures 5 and 6B).When eyes are present, they are located dorsally on the sides of the scutum.
Soft ticks are leathery and nonscutate, without obvious sexual dimorphism. Theirmouthparts are subterminally attached (in adult and nymphal stages) and not visiblefrom dorsal view (Figure 6A). Eyes, when present, are located laterally in folds abovethe legs.
There are major differences in the biology of hard and soft ticks. Some hard tickspecies have a one host life cycle, wherein engorged larvae and nymphs remain onthe host after feeding; they then molt, and the subsequent stages reattach and feed. Theadults mate on the host, and only engorged females drop off to lay eggs on the ground.While some hard ticks complete their development on only one or two hosts, mostcommonly encountered ixodids have a three-host life cycle. In this case, adults mateon a host (except for some Ixodes spp.) and the fully fed female drops from a hostanimal to the ground and lays from 2,000 to 18,000 eggs, after which she dies. The eggshatch in about 30 days into a six-legged seed tick (larval) stage, which feeds

342
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
predominantly on small animals. The fully fedseed ticks drop to the ground and transforminto eight-legged nymphs. These nymphs seekan animal host, feed, and drop to the ground(see Color Figure 30-29 for ticks on a hostanimal). They then molt into adult ticks, thuscompleting the life cycle. Figure 7A shows allthe motile life stages of hard ticks.
Many hard tick species “quest” for hosts,whereby they climb blades of grass or weedsand remain attached, forelegs outstretched,awaiting a passing host. For this reason, drag-ging a white flannel cloth through brushy areasworks well for collecting ticks (Figure 8). Theymay travel up a blade of grass (to quest) andback down to the leaf litter where humidity ishigh (to rehydrate) several times a day. Also,hard ticks will travel toward a CO2 source. Adultticks are more adept at traveling through veg-etation than the minute larvae. Studies haveshown that adult lone star ticks may travel upto 10 m (33 ft) to a CO2 source, but otherspecies such as I. scapularis will only traveldistances of 1 to 2 m (3.3 to 6.6 ft) toward a CO2
source. Goddard28 demonstrated minimal (<2 ft)lateral movement by questing adult I. scapularisin a mark–release–recapture study.
Ticks feed by cutting a small hole into thehost epidermis with their chelicerae and insert-ing the hypostome into the cut, thereby attach-ing to the host. Blood flow is presumably main-tained with the aid of an anticoagulant from thesalivary glands. Some hard ticks secure theirattachment to the host by forming a cementcone around the mouthparts and surroundingskin. Two phases are recognized in the feedingof nymphal and female hard ticks: (1) a growthfeeding stage characterized by slow continuousblood uptake and (2) a rapid engorgementphase occurring during the last 24 h or so ofattachment.
The biology of soft ticks differs from hardticks in several ways (see Figure 7B for lifestages). Adult female soft ticks feed and lay eggsseveral times during their lifetime. Soft tickspecies may also undergo more than onenymphal molt before reaching the adult stage.With the exception of larval stages of somespecies, soft ticks do not firmly attach to their
TICKS
Figure 4Female and male hard ticks (from: USAF Publ.USAFSAM-SR-89-2).
ImportanceAnnoyance; disease transmission; tick
paralysis
DistributionNumerous species worldwide
LesionRed papule with erythema; sometimes
nodular
Disease TransmissionLyme disease, rocky mountain spotted
fever, tularemia, relapsing fever,tickborne encephalitis, ehrlichiosis,and others
Key ReferenceArthur, D. R., Pergamon Press, New
York, 445 pp., 1962
TreatmentGenerally none needed for bites other
than palliatives after tick removal;watch for development of tick-bornedisease

343
Ticks
Figure 5Hard tick showing dorsal (A) and ventral (B)aspects (National Institutes of Health photocourtesy Dr. Jim Keirans).
A
B
hosts for several days like the Ixodidae. They are adapted to feeding rapidly and leavingthe host promptly.
The expansion capability of hard ticks sometimes causes confusion among nonspe-cialists. I have often been sent fully engorged hard ticks removed from dogs withinstructions to “identify enclosed soft tick”; this misconception is because engorgedixodids do sometimes appear “soft.” Another common misconception is that flat,unengorged hard ticks and engorged hard ticks represent different species. Ranchersoften speak of two “species” on their cattle; “the large swollen species” and the “smallflat, brown species.”

344
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 7Motile life stages of hard ticks (A) and soft ticks (B) (from:USAF Publ. USAFSAM-SR-89-2).
Figure 6Comparison of soft (A) and hard (B) ticks (from: USAFPubl. USAFSAM-SR-89-2).
Hard ticks and soft ticks occur in different habitats. In general, hard ticks occur inbrushy, wooded, or weedy areas containing numerous deer, cattle, dogs, smallmammals, or other hosts. Soft ticks are generally found in animal burrows or dens, batcaves, dilapidated or poor-quality human dwellings (huts, cabins, etc.), or animalrearing shelters. Many soft tick species thrive in hot and dry conditions, whereas ixodidsare more sensitive to desiccation (the genus Hyalomma may be an exception) and,therefore, usually found in areas providing protection from high temperatures, lowhumidities, and constant breezes.
Most hard ticks, being sensitive to desiccation, must practice water conservation anduptake. Their epicuticle contains a wax layer which prevents water movement throughthe cuticle. Water can be lost through the spiracles; therefore, resting ticks keep their

345
Ticks
Figure 8Tick collecting by dragging or flagging with a white flannel cloth.
spiracles closed most of the time (opening them only one or two times an hour). Tickmovement and its resultant rise in CO2 production cause the spiracles to open about15 times an hour with a corresponding water loss.
Development, activity, and survival of hard ticks is influenced greatly by temperatureand humidity within the tick microhabitat. Lancaster29 found that lone star tick eggsreared in an environment of <75% humidity would not hatch. Lees30 demonstrated thatI. ricinus died within 24 h if kept in a container of 0% RH, but survived 2 to 3 monthsat 90% RH. Because of their temperature and humidity requirements, as well as hostavailability, hard ticks tend to congregate in areas providing those factors. Ecotonalareas (ecological interface areas such as between forests and fields) are excellenthabitats for hard ticks. Open meadows/prairies, along with climax forest areas, supportthe fewest lone star ticks. Ecotone areas and small openings in the woods are usuallyheavily infested. In a study by Semtner et al.,31 lone star tick populations decreased withan increase in distance from the ecotone. Studies in Virginia demonstrated thatAmerican dog ticks tend to be especially abundant along trails, roadsides, and forestboundaries surrounding old fields or other clearings.32-34

346
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 9Deer heavily infested with lone star ticks (Tennessee Valley Authority photo by Denise Schmittou).
Deer and small mammals thrive in ecotonal areas, thus providing blood meals forticks. In fact, deer are often heavily infested with hard ticks in the spring and summermonths (Figure 9). The optimal habitat of white tail deer has been reported to be theforest ecotone, since the area supplies a wide variety of browse and frequently offersthe greatest protection from their natural enemies. Many favorite deer foods are alsofound in the low trees of an ecotone, including greenbrier, sassafras, grape, oaks, andwinged sumac.
Ticks are not evenly distributed in the wild; instead, they are localized in areasproviding their necessary temperature, humidity, and host requirements. These biologiccharacteristics of ticks, when known, may enable us to avoid the parasites.
III. TICK IDENTIFICATION
Ticks look like large mites, with both having eight legs and one (apparent) disk-shapedbody region. However, ticks differ from mites in having a toothed hypostome and noclaws on their palps. Like those of many other arthropod groups, tick morphologicalstructures have been assigned rather long and somewhat confusing names. Figures 10and 11 are provided to acquaint the reader with those terms. Some identification keysare well written and relatively easy to use (a good example is the pictorial key to adulthard ticks east of the Mississippi River35). However, tick identification to the specieslevel is probably best accomplished by an expert to avoid misinformation. In a “study”that the author was asked to review, more than 30% of the ticks collected and identifiedfrom Mississippi did not even occur in this country.

347
Ticks
Figure 10Diagnostic characters of soft ticks (from: Strickland et al.34a).

348
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
IV. DISCUSSION OF SOME OF THE COMMON U.S. SPECIES*
Ornithodoros hermsi Wheeler, Herms, and Meyer
Medical Importance: Primary vector of tick-borne relapsing fever (TBRF) spiro-chetes in the Rocky Mountain and Pacific Coast states, U.S; implicated in several TBRFoutbreaks18,19
Figure 11Diagnostic characters of hard ticks (from: Strickland et al.34a).
* The descriptions for each tick species are only general comments about their macroscopic appearance. Tickidentification to the species level is quite difficult, utilizing a number of microscopic characteristics. Specificidentifications should be performed by specialists at institutions that routinely handle such requests(universities, extension services, state health departments, the military, etc.).

349
Ticks
Description: Typical-looking soft tick about 10 mm long, gray in color, and coveredwith numerous bumplike projections (mammillae); as with all soft ticks, head (mouth-parts in this case) not visible from dorsal view; foreleg depicted in Figure 12
Distribution: California, Nevada, Idaho, Oregon, Utah, Arizona, Washington, andColorado, as well as in British Columbia, Canada (Figure 13)
Host: Rodents and humans
Seasonality: Varies with geographic location, hosts, and habitat
Remarks: Often found infesting corners and crevices of vacation or summer cabins;larvae only remain attached to a host for about 15 to 20 min; usually four nymphalmolts; cycle from egg to egg takes about 4.5 months; often found in coniferous forestsat elevations above 1,000 m
Figure 12Larva (A), foreleg (B), and adult (C) of Ornithodoros hermsi (from: USAF Publ. USAFSAM-SR-89-2).
Figure 13Approximate geographic distribution of Ornithodoros hermsi (from: USAF Publ. USAFSAM-89-2).

350
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 14Larva (A), foreleg (B), and adult (C), of Ornithodoros turicata (from: USAF Publ. USAFSAM-89-2).
Relapsing Fever TickOrnithodoros turicata (Duges)
Medical Importance: May produce an intense irritation and edema at the bite sitein humans; serves as a vector of relapsing fever spirochetes in portions of Kansas,Oklahoma, Texas, and other southwestern states
Description: About 10 mm long, gray in color, and covered with bumplike projec-tions (mammillae); foreleg depicted in Figure 14
Distribution: Texas, New Mexico, Oklahoma, Kansas, California, Colorado, Arizona,Florida, and Utah; reported from Mexico in the states of Aguascalientes, Coahuila,Gunanjuato, Morelos, Queretaro, San Luis Potosi, and Sinaloa (Figure 15); also report-edly found in Venezuela, Honduras, Bolivia, Chile, and Argentina; records from Centraland South America probably incorrect
Figure 15Approximate geographic distribution of Ornithodoros turicata (from: USAF Publ. USAFSAM-89-2).

351
Ticks
Hosts: Collected from rattlesnakes, turtles, birds, rodents, rabbits, sheep, cattle,horses, pigs, and humans
Seasonality: Varies with geographic location, hosts, and habitat; may be active inwarmer geographic areas throughout year
Remarks: Often found in burrows used by rodents or burrowing owls; bite is painlessbut may be followed in a few hours by intense local irritation and swelling; subsequently,subcutaneous nodules may form and persist for months; three to five nymphal stages;time required for development from larva to adult is approximately 6 months.
Lone Star TickAmblyomma americanum (Linnaeus)
Medical Importance: Transmits the pathogen of tularemia to humans; a knownvector of agent of human ehrlichiosis — Ehrlichia chaffensis;9 reported to transmit theagents of Lyme borreliosis and Rocky Mountain spotted fever (RMSF) (Goddard36
provided a detailed review of the disease potential of this species; however, studiesindicate that A. americanum may not be an important vector of RMSF37,38); Lyme-borreliosis-like spirochetes have been recovered from this species;7 found naturallyinfected with Rickettsia parkeri38 and Ehrlichia ewingii.38a
Description: Reddish-brown tick species; adult stages have long mouthparts visiblefrom above (in contrast to the soft ticks); adult females have distinct single white spoton their back (scutum); males have no single spot, instead have inverted horseshoe-shaped markings at the posterior edge of their dorsal side (Figure 16)
Figure 16Adult female (A), male (B), nymph (C), and dorsal view of capitulum (D) of Amblyommaamericanum (from: USAF Publ. USAFSAM-89-2).

352
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Distribution: Central Texas east to the Atlantic Coast and north to approximatelyIowa and New York; reported from Mexico in the northern states of Coahuila, NuevoLeon, and Tamaulipas (Figure 17); also occasionally reported from Panama, Venezuela,Argentina, Guatemala, Guayana, and Brazil (however, Central and South Americanrecords of this species may not be valid)
Hosts: Extremely aggressive and nonspecific in its feeding habits; all three motile lifestages will feed on a wide variety of mammals (including humans) and ground-feedingbirds
Seasonality: Adults and nymphs generally active from early spring through midsum-mer, with larvae being active from late summer into early fall
Remarks: Probably the most annoying and commonly encountered tick occurring inthe southern U.S.; in some rural areas almost every person has been bitten by theseticks at one time or another; the “seed ticks” occurring in late summer in the southernU.S. are most often this species (Figure 18); lone star ticks especially found in
Figure 17Approximate geographic distribution of Amblyomma americanum (from: USAF Publ. USAFSAM-89-2).
Figure 18Larval lone star tick showing extremely small size.

353
Ticks
interfacing zones between forested and open (meadow) areas, especially where thereis an abundance of deer or other hosts; they seldom occur in high numbers in themiddle of pastures or meadows because of low humidities and high daytime tempera-tures present in those areas; larvae may survive from 2 to 9 months, nymphs and adults4 to 15 months each; females usually deposit 3,000 to 8,000 eggs
Female often falsely referred to as the “spotted fever tick” because of the single whitespot visible on its back; however, this spot has nothing to do with the presence or absenceof RMSF organisms; adults have very long mouthparts and can produce painful bites
Gulf Coast TickAmblyomma maculatum (Koch)
Medical Importance: Nuisance effects due to painful bites; found naturally infectedwith Rickettsia parkeri
Description: Macroscopically, somewhat similar to American dog tick, except withmetallic markings (instead of white) and long mouthparts typical of all Amblyomma;large tick species with long mouthparts visible from above; adult females with metallicwhite or gold markings on scutum (Figure 19); males with numerous, mostly con-nected, linear spots of golden white
Distribution: Portions of Atlantic and Gulf coast areas (generally 100 to 200 milesinland) and south into Mexico and portions of Central and South America (Figure 20)
Figure 20Approximate geographic distribution of Amblyomma maculatum.
Figure 19Adult female (A) and male (B) Amblyomma maculatum.

354
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Hosts: Adults on large animals including deer, cattle, sheep, and humans; larvae andnymphs on small mammals and ground-feeding birds such as rabbits, fox, meadowlarks, and bobwhite quail
Seasonality: Variable depending upon geographic location; larvae generally outfrom June through October; nymphs active from July through October; adults can befound from March through September, usually peaking in activity during August
Remarks: Increasingly a pest in the southern U.S.; large ticks often found in the earsof cattle, producing great irritation, destruction of cartilage, and drooping, called“gotched” ears
Rocky Mountain Wood TickDermacentor andersoni Stiles
Medical Importance: Primary vector of RMSF in the Rocky Mountain states and alsoknown to transmit the causative agents of Colorado tick fever and tularemia; producescases of tick paralysis in the U.S. and Canada each year39
Description: Adults have shorter mouthparts than the Amblyomma species and areusually dark brown or black with bright white markings on the scutum (see Figure 21for pattern).
Distribution: Found from the western counties of Nebraska and the Black Hills ofSouth Dakota to the Cascade and Sierra Nevada Mountains; also reported from northernArizona and northern New Mexico to British Columbia, Alberta, and Saskatchewan,Canada (Figure 22)
Figure 21Adult female (A), male (B), nymph (C), and dorsal view of capitulum (D) of Dermacentorandersoni (from: USAF Publ. USAFSAM-89-2).

355
Ticks
Hosts: Immatures prefer many species of small mammals such as chipmunks andground squirrels, whereas adults feed mostly on cattle, sheep, deer, man, and otherlarge mammals
Seasonality: Larvae feed throughout the summer and adults usually appear in March,disappearing by July; nymphs may continue to be present, although in diminishingnumbers, until late summer
Remarks: Especially prevalent where there is brushy vegetation to provide goodprotection for small mammalian hosts of immatures and with sufficient forage to attractlarge hosts required by adults; unfed larvae may live for 1 to 4 months, nymphs for10 months or more, and adults 14 months or longer; females deposit about 4,000 eggs
American Dog TickDermacentor variabilis (Say)
Medical Importance: One of the most medically important ticks in the U.S.; primaryvector of RMSF in the East; also transmits tularemia and may cause tick paralysis39,40
Description: Adults are dark brown or black with short, rounded mouthparts; dullor bright white markings on the scutum (see Figure 23 for pattern)
Distribution: Throughout the U.S. except in parts of the Rocky Mountain region; alsoestablished in Nova Scotia, Manitoba, and Saskatchewan, Canada; reported in Mexicofrom Chiapas, Gunajuato, Hidalgo, Oaxaca, Puebla, San Luis Potosi, Sonora, Tamaulipas,and Yucatan (Figure 24)
Hosts: Immatures feed primarily on small mammals (particularly rodents); adultsprefer the domestic dog, but will readily bite humans
Seasonality: Adults active from about mid-April to early September; nymphs predomi-nate from June to early September; larvae active from about late March through July
Remarks: Principal vector of RMSF in the central and eastern U.S. (should be avoidedwhenever possible); deticking dogs important mode of RMSF transmission that may be
Figure 22Approximate geographic distribution of Dermacentor andersoni (from: USAFPubl. USAFSAM-89-2).

356
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 23Adult female (A), male (B), nymph (C), and dorsal view of capitulum (D) of Dermacentorvariabilis (from: USAF Publ. USAFSAM-89-2).
overlooked (handpicking D. variabilis from dogs is dangerous because infected ticksecretions on the hands may be transmitted through contact with the eyes, mucousmembranes, etc.); unfed larvae may live up to 15 months, nymphs 20 months, andadults up to 30 months or longer; females deposit 4,000 to 6,500 eggs
Western Black-Legged TickIxodes pacificus Cooley and Kohls
Medical Importance: Known to be a vector of Lyme borreliosis spirochetes; most,if not all, cases of Lyme borreliosis occurring in California transmitted by this tick;
Figure 24Approximate geographic distribution of Dermacentor variabilis (from: USAF Publ. USAFSAM-89-2).

357
Ticks
reports of Type I (IgE-mediated) hypersensitivity reactions in humans as a result of bitesby this species
Description: No white markings on their dorsal side, no eyes or festoons (Figure 25)(like other members of genus); adults dark brown in color with moderately longmouthparts; looks almost identical to I. scapularis
Distribution: Along the Pacific coastal margins of British Columbia, Canada, andU.S., possibly extending into Baja, California and other parts of Mexico (Figure 26); alsoreported from at least one area in Arizona
Figure 25Adult female (A), male (B), nymph (C), and dorsal view of capitulum (D) of Ixodes pacificus(from: USAF Publ. USAFSAM-89-2).
Figure 26Approximate geographic distribution of Ixodes pacificus (from: USAF Publ. USAFSAM-89-2).

358
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Hosts: Immatures feed on numerous species of small mammals, birds, and lizards;in certain areas of California, predominance of feeding on lizards; adults feed primarilyon Columbian black-tailed deer
Seasonality: Adults primarily active from fall to late spring with immatures active inthe spring and summer
Remarks: Adults, like I. scapularis, have long mouthparts, enabling them to beespecially painful parasites of humans; adults most abundant in the early spring;infection rates with Lyme borreliosis spirochetes usually in the range of 1 to 5%compared to rates of 25 to 75% in the northern form of I. scapularis (effect may be relatedto vector competence or host preferences of the immatures); immatures will bite people
Black-Legged TickIxodes scapularis Say
Taxonomic Note: For several years, the northern form of Ixodes scapularis wasthought to be a distinct species named Ixodes dammini (see Goddard41 for a discussionof this issue). Subsequently, evidence was produced indicating that the two are onespecies.42 Morphologically, the two are almost identical. However, there are someimportant behavioral differences, especially in the immature stages. In this book, Ixodesdammini is considered a synonym and is included under I. scapularis. However, the formerI. dammini will be referred to occasionally in the text as “the northern form of I. scapularis.”
Medical Importance: Northern form primary vector of the causative agent of Lymeborreliosis, especially in the northeastern and upper midwestern areas of the U.S.;vector of the protozoan, Babesia microti, also in the Northeast and Upper Midwest; alsoa vector of agent of human granulocytic ehrlichiosis (HGE); southern form of Ixodesscapularis a vector of Lyme borreliosis spirochetes,43 however, infection rates lowerthan in the northeastern U.S.
Description: Adults have no eyes, festoons, or white markings on their dorsal side(Figure 27), dark brown in color (occasionally the abdomen from dorsal view is lightbrown or orangish)
Distribution: Northern form in the New England states and New York, south intoNew Jersey, Virginia, and Maryland; also found in upper midwest and Ontario, Canada;southern form found in the southern Atlantic Coast states and throughout the Southincluding Texas and Oklahoma; also reported from the Mexican states of Jalisco andTamaulipas (Figure 28)
Hosts: Immatures feed on lizards, small mammals, and birds; adults prefer deer butwill bite people; in Mexico, additional host records from dogs, cattle, and jaguar
Seasonality: In U.S., adults active in fall, winter, and spring (Figure 29) (seasonalactivity pattern interesting, since most people do not think of ticks being active in thedead of winter); immatures active in spring and summer
Remarks: Congregates along paths, trails, and roadways in various types of forestedareas such as those exhibiting mature pine hardwoods with dogwood, wild blueberry,

359
Ticks
Figure 27Adult female (A), male (B), nymph (C),and dorsal view of capitulum (D), ofIxodes scapularis (from: USAF Publ.USAFSAM-89-2).
Figure 28Approximate geographic distribution of Ixodes scapularis (from: USAF Publ.USAFSAM-89-2).
Figure 29Seasonal activity of adult I. scapularis in Mississippi,as determined by dragging vegetation with a whiteflannel cloth.

360
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
privet, blackberry, huckleberry, and sweetgum; inflicts a painful bite; adult males rarelybite; nymphs of northern form bite people aggressively during summer months and canbe collected with a drag cloth; nymphs of southern form rarely, if ever, bite people andcan rarely be collected with drag cloths; majority of hard ticks acquired by persons inthe south central and southeastern states in the winter months are of this species; inone study,44 most often collected questing at around 20°C, but were collected on daysas cold as 6.9°C
Brown Dog TickRhipicephalus sanguineus (Latreille)
Medical Importance: Reported to transmit the agent of RMSF in Mexico; in southernEurope and Africa, known vector of Rickettsia conorii, the causative agent of boutonneusefever
Description: Light to dark brown in color, with no white markings on the dorsum(Figure 30); they have both festoons and eyes
Distribution: Probably the most widely distributed of all ticks, being found almostworldwide (Figure 31); in Western Hemisphere, records from most of U.S. andsoutheastern and southwestern parts of Canada; reported from most of Mexico,Argentina, Venezuela, Colombia, Brazil, Nicaragua, Panama, Uruguay, Paraguay,Galapagos Islands, Surinam, British Guiana, French Guiana, Peru, Costa Rica, Carib-bean islands of Cuba, Jamaica, and Bahamas; also widely distributed throughoutEurasia, Africa, and Australian region
Figure 30Adult female (A), male (B), nymph (C), and dorsal view of capitulum (D) of Rhipicephalussanguineus (from: USAF Publ. USAFSAM-89-2).

361
Ticks
Hosts: Dog is principal host, although in immature stages sometimes attacks numer-ous other animals; humans historically only occasionally bitten in U.S.; could bebecoming more anthropophilic45,46
Seasonality: May be active in the warmer parts of its range year-round; however, intemperate zones adults and immatures primarily active from late spring to early fall
Remarks: Most often found indoors in and around pet bedding areas; strongtendency to crawl upward and often seen climbing the walls of infested houses;associated with homes and yards of pet owners and seldom found out in the middleof a forest or uninhabited area; unfed larvae may survive as long as 8.5 months, nymphs6 months, and adults 19 months; females usually lay 2,000 to 4,000 eggs
V. DISCUSSION OF SOME MAJOR PEST SPECIES INOTHER AREAS OF THE WORLD
Eyeless TampanOrnithodoros moubata (Murray)
Medical Importance: Known vector of African tick-borne relapsing fever spiro-chetes in eastern, central, and southern Africa
Description: Like many other soft ticks, about 9 to 12 mm long in adult stage; bumpyintegument (mammillated) and protuberances on the tarsi (Figure 32)
Distribution: Throughout eastern Africa and the northern portions of southernAfrica, extending into the drier parts of central Africa (Figure 33)
Hosts: Humans, warthogs, domestic pigs, antbears, and porcupines
Seasonality: Varies with geographic location, hosts, and habitat
Remarks: Often found in cracks in walls and in earthen floors of huts, female usually
Figure 31Approximate geographic distribution of Rhipicephalus sanguineus (from:USAF Publ. USAFSAM-89-2).

362
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
lays six to seven batches of eggs (several hundred per batch) during her lifetime; larvaedo not feed; nymphs engorge in about 20 to 25 min; usually four nymphal molts formales and five for the females; able to live up to 5 years without feeding
Carios rudis (includes venezuelensis) Karsch[Klompen47 has determined that several
Ornithodoros species should be placed in the genus Carios]
Medical Importance: Most important vector of relapsing fever spirochetes in Panama,Colombia, Venezuela, and Ecuador
Description: Unlike some of the other soft ticks, has no dorsal humps on legs (seeFigure 34)
Distribution: Panama, Paraguay, Colombia, Venezuela, Peru, and Ecuador (Figure 35)
Hosts: Domestic birds and humans
Seasonality: Varies with geographic location, hosts, and habitat; may be active inwarmer areas throughout year
Figure 32Dorsal (A) and ventral (B) view of Ornithodoros moubata (from: USAF Publ. USAFSAM-89-2).
Figure 33Approximate geographic distribution of Ornithodoros moubata (from: USAF Publ. USAFSAM-89-2).

363
Ticks
Remarks: Appears especially adapted as parasite of humans but feeds on otheranimals; night feeder with the larval stages engorging rapidly; three to four nymphalstages; developmental time from larvae to adult is about 3 months
Carios talaje (Guerin-Meneville)47
Medical Importance: Transmits the agent of relapsing fever to humans in Guate-mala, Panama, and Colombia
Description: Typical-looking soft tick with large discs (round spots mostly on thedorsal side of the integument) and no humps on tarsi (Figure 36)
Figure 34Larva (A), foreleg (B), and adult (C) of Carios (=Ornithodoros) rudis (from: USAF Publ.USAFSAM-89-2).
Figure 35Approximate geographic distribution of Carios (=Ornithodoros) rudis (from: USAF Publ. USAFSAM-89-2).

364
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Distribution: Reported in Florida, Texas, Arizona, Nevada, Kansas, New Mexico, andCalifornia (however, Hoogstraal48 maintains that in the U.S. it has only been reportedfrom Kansas and California); occurs in Mexico in the states of Baja California, Chiapas,Guerrero, Morelos, Oaxaca, Puebla, Sinaloa, Sonora, Veracruz, and Yucatan; alsoreported from Venezuela, Uruguay, Brazil, French Guiana, Panama, Ecuador, and Chile.Hoffmann49 notes this species also reported from Guatemala, Colombia, Argentina, andGalapagos Islands (although according to Keirans et al.,50 the O. talaje reported fromGalapagos Islands actually is O. galapagensis) (Figure 37)
Hosts: Rodents (principally) and humans, as well as birds, bats, pigs, cattle, horses,opossums, and snakes
Seasonality: Varies with geographic location, hosts, and habitat; may be active inwarmer geographic areas throughout year
Figure 36Larva (A), foreleg (B), and adult (C) of Carios talaje(from: USAF Publ. USAFSAM-89-2).
Figure 37Approximate geographic distribution of Carios talaje (from: USAF Publ.USAFSAM-89-2).

365
Ticks
Remarks: Adults seldom observed in dwellings and not avid parasites of humans;larvae remain attached to a host for several days; three to four nymphal stages;developmental time from larva to adult is about 8 months
Cayenne TickAmblyomma cajennense (Fabricius)
Medical Importance: Probably most commonly encountered and aggressive of allCentral and South American ticks; considered vector of RMSF rickettsiae in Mexico,Panama, Colombia, and Brazil
Description: Long mouthparts, eyes, and festoons similar to that of A. americanum;males have weblike ornamentation radiating from the center of the scutum; femalesalso have extensive ornamentation and festoons with tubercules at the posterior edge(Figure 38)
Distribution: Extreme southern Texas, south throughout Mexico and Central Americainto parts of South America; most of Mexico, Panama, several Caribbean islandsincluding Cuba and Jamaica, Brazil, Honduras, Venezuela, Costa Rica, Uruguay,Ecuador, Nicaragua, and Bolivia (Figure 39); Hoffmann49 states it also occurs inGuatemala, Colombia, Guayana, Paraguay, and Argentina
Hosts: All active stages commonly attack people, domestic and wild animals, andground-frequenting birds
Figure 38Adult female (A), male (B), nymph (C), and dorsalview of capitulum (D) of Amblyomma cajennense(from: USAF Publ. USAFSAM-89-2).

366
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Seasonality: May be active in tropical areas year-round; may be reduced activity inmidwinter in the cooler areas at the northernmost and southernmost extent ofdistribution
Remarks: Very similar to A. americanum in aggressiveness and nonspecific feedinghabits; basically, where southernmost distribution of A. americanum stops, A. cajennensepicks up and continues southward throughout Central and South America; longevity oflarvae, nymphs, and adults, as well as numbers of eggs laid by engorged females,similar to that of A. americanum; as with A. americanum, A. cajennense have longmouthparts and produce painful bites
Bont TickAmblyomma hebraeum Koch
Medical Importance: One of several ixodid vectors of Rickettsia conorii, the agentof boutonneuse fever; vector of African tick-bite fever organisms
Description: Long mouthparts, eyes, and festoons typical of other Amblyomma spp.(Figure 40); males have black or brown stripes and spots on a pale greenish-whitebackground; females have dark markings confined to the scutum
Distribution: Distributed throughout southern Africa, specifically Angola, Botswana,Cameroon, Mozambique, Madagascar, Kenya, Nigeria, Somalia, South Africa, Swaziland,Tanzania, Zaire, Zambia, and Zimbabwe; accidentally introduced into U.S. on severaloccasions (primarily on rhinoceroses), but each time has been successfully eliminated(Figure 41)
Hosts: Immatures feed on many medium- and large-sized mammals, particularly wildhares; adults parasitize a variety of domestic and wild mammals but seem to prefercattle and antelopes; all life stages will bite people
Seasonality: Active in spring, summer, and fall months; in South Africa, adults mostabundant on hosts during the late summer and autumn51
Figure 39Approximate geographic distribution of Amblyomma cajennense (from:USAF Publ. USAFSAM-89-2).

367
Ticks
Remarks: Larvae, like U.S. cousins, lone star ticks, troublesome pests of people; attachthemselves in large numbers on legs and about waist, causing intense irritation, rashlikelesions, and occasional pustules; unfed larvae may live for up to 11 months, nymphs for8 months or more, and adults 22 months or longer; females deposit about 15,000 eggs
Haemaphysalis concinna Koch
Medical Importance: Vector of Siberian tick typhus rickettsia and viruses in the tick-borne encephalitis complex; may be a vector of Lyme borreliosis spirochetes in Asia.
Description: As a group, small inornate ticks with festoons but without eyes (Figure42); second palpal segment projecting beyond lateral margin of basis capitulum (givespalpi appearance of being triangular — should not be confused with basis capitulumbeing angular, as in the Rhipicephalus ticks); males have pincerlike palps; females havea hypostome dentition of 6/6 and scutum is broadest in middle
Figure 40Adult female (A) and male (B) Amblyomma hebraeum (from: USAF Publ. USAFSAM-89-2).
Figure 41Approximate geographic distribution of Amblyomma hebraeum (from: USAFPubl. USAFSAM-89-2).

368
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Distribution: Widely distributed in forests of temperate Eurasia, including most ofCentral Europe, Estonia, Latvia, Belarus, Ukraine, Russia, Kazakhstan, Uzbekistan,Turkmenistan, China, Japan, Korea, and Vietnam (Figure 43)
Hosts: Adults feed on large wild and domestic mammals; immatures infest smallermammals and birds, sometimes even reptiles; both adults and nymphs will bite people
Seasonality: All stages active from spring to autumn; peak adult activity in June
Remarks: Found chiefly in deciduous and mixed forests, grass tussock swamps,birch–aspen groves, and alpine taiga forests; reported abundant in low-lying areas withhigh humidities
Yellow Dog TickHaemaphysalis leachi (Audouin) (Including H. l. muhsami)
Medical Importance: Vector of boutonneuse fever rickettsia (human infection withrickettsia may also be acquired by contamination of skin and eyes with infectious tickfluids from crushing while deticking dogs)
Figure 42Female (A) and male (B) Haemaphysalis concinna (from: USAF Publ.USAFSAM-89-2).
Figure 43Approximate geographic distribution of Haemaphysalis concinna (from:USAF Publ. USAFSAM-89-2).

369
Ticks
Description: Typical-looking Haemaphysalis sp. (Figure 44) characteristically ap-pears to have large, wedge-shaped mouthparts as viewed from above (personsidentifying these specimens should be careful not to confuse them with brown dog tick,R. sanguineus)
Distribution: Primarily in tropical and southern Africa (although there are recordsfrom Algeria, Libya, and Egypt); records from India and Southeast Asia probablyrepresent related but distinct species (Figure 45)
Hosts: Immatures usually parasitize field rodents; adults commonly bite domesticdogs but will bite people readily; subspecies H. leachi muhsami prefers small carni-vores (mongooses, wildcats, etc.) instead of canines
Seasonality: Most active from late spring to early fall
Remarks: Very common on dogs; in some areas more prevalent on dogs than R.sanguineus; usually two generations produced each year; unfed larvae may survive atleast 169 days, nymphs 52 days, and adults 210 days; females lay up to 5,000 eggs
Figure 44Female (A) and male (B) Haemaphysalis leachi (from: USAF Publ. USAFSAM-89-2).
Figure 45Approximate geographic distribution of Haemaphysalis leachi (from: USAF Publ. USAFSAM-89-2).

370
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 46Female (A) and male (B) Haemaphysalis spinigera (from: USAF Publ.USAFSAM-89-2).
Haemaphysalis spinigera Neumann
Medical Importance: Primary vector of the virus of Kyasanur Forest disease (KFD)in India
Description: Apart from usual generic characteristics of Haemaphysalis (inornate, noeyes, festoons present, triangular-shaped second palpal segment), males have longspurs on coxae I and IV and poorly developed spurs on coxae II and III (Figure 46);females have no spurs on the trochanters
Distribution: Widely distributed in central and southern India; also reported fromsoutheast Asia and Indonesia (Figure 47)
Hosts: Immatures parasitize wide range of small mammals and birds; adults preferlarge mammals such as cattle, monkeys, bears, and tigers; nymphs avidly bite humans
Seasonality: Generally active in the spring, summer, and fall; immatures peak innumbers from September to November
Figure 47Approximate geographic distribution of Haemaphysalis spingera (from:USAF Publ. USAFSAM-89-2).

371
Ticks
Remarks: People in the KFD endemic areas (Mysore State, India) turn from agricul-tural pursuits to wood gathering in the forests during the season of peak immatureactivity; activity greatly increases human–tick contact; Hoogstraal52 reported tick popu-lation increases in India because of recent increased cattle grazing practices in andbeside forests; immatures thrive on numerous small vertebrates hiding in dense lantanathickets where sections of forests cleared
Asiatic HyalommaHyalomma asiaticum Schulze and Schlottke
Medical Importance: Vector of agent of Siberian tick typhus
Description: In general, scant ornamentation, long mouthparts, eyes present, and festoons(although festoons not always clearly delineated); often legs appear banded (Figure 48);females have scutum longer than wide; both sexes have white or yellowish bands on legs
Distribution: Generally found in Russia, Georgia, Azerbaijan, Kazakhstan, Uzbekistan,Turkmenistan, China, Afghanistan, Pakistan, Iran, and Iraq (Figure 49)
Figure 48Female (A) and male (B) Hyalomma asiaticum (from: USAF Publ. USAFSAM-89-2).
Figure 49Approximate geographic distribution of Hyalomma asiaticum (from: USAFPubl. USAFSAM-89-2).

372
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Hosts: Adults parasitize all domestic animals, especially camels, cattle, horses, andsheep; people, hares, boars, and hedgehogs less frequently attacked; immatures feedon hedgehogs, rodents, hares, cats, and dogs
Seasonality: Most active in spring and summer throughout range
Remarks: In southwestern Kirghiz (former U.S.S.R.), foci of Siberian tick typhusoccur where southern steppes give way to foothill semidesert zone; in these areas,associated with red-tailed jirds along dry waterways overgrown with shrubs and alongirrigation canals5
Small Anatolian HyalommaHyalomma anatolicum Koch
(Including H. a. anatolicum and H. a. excavatum)
Medical Importance: Vector of virus of Crimean–Congo hemorrhagic fever
Description: Usual characteristics of all Hyalomma ticks (scant ornamentation, eyespresent, long mouthparts, banded legs); small and similar in appearance to H.asiaticum (Figure 50)
Distribution: Throughout northern Africa, portions of the Near East, Asia Minor,southern Europe, Russia, Ukraine, Georgia, Azerbaijan, Armenia, Kazakhstan, Uzbekistan,Turkmenistan, and India (Figure 51)
Hosts: All stages observed feeding on hares in forest near Casablanca;53 also avidparasite of humans and many domestic animals
Seasonality: Varies with latitude throughout range; in general, adults infest domesticanimals from March to October, and larvae and nymphs from July to September; allstages most abundant in early August
Figure 50Female (A) and male (B) Hyalomma anatolicum (from: USAF Publ. USAFSAM-89-2).

373
Ticks
Remarks: Engorged larvae and unfed adults usual overwintering stages; hibernate incracks and crevices in wooden animal shelters in Russian climate and in rodent burrowsin African desert conditions; larvae may survive up to 241 days, nymphs up to 246 days,and adults over 1 year
Hyalomma marginatum Koch(Including Several Subspecies)
Medical Importance: Ticks of this complex efficient vectors of the Crimean–Congohemorrhagic fever virus
Description: Complex includes several subspecies; in general, large with bandedlegs (Figure 52)
Distribution: Most common in southeastern Europe, including Russia, Ukraine,Belarus, Georgia, Azerbaijan, Armenia, Kazakhstan, Uzbekistan, Turkmenistan; also
Figure 51Approximate geographic distribution of Hyalomma anatolicum (from: USAFPubl. USAFSAM-89-2).
Figure 52Female (A) and male (B) Hyalomma marginatum (from: USAF Publ. USAFSAM-89-2).

374
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
occurs in India and Indochina, westward throughout southern Europe, into the NearEast and Africa; specific countries include Egypt, Libya, Tunisia, Morocco, Algeria,Nigeria, Sudan, Kenya, South Africa, Cameroon, Southwest Africa, Mauritania, Senegal,Israel, Syria, Lebanon, Jordan, Turkey, Cyprus, Iran, Iraq, Yemen, Spain, Portugal,France, Italy, Yugoslavia, Romania, Greece, Bulgaria, countries of former U.S.S.R.,India, and China (Figure 53)
Hosts: Adults attack humans and most domestic animals, especially cattle and horses;immatures may also be found on domestic animals but prefer small wild mammals andbirds
Seasonality: According to Hoogstraal,53 rarely seen in winter throughout much ofdistribution, but begin to appear in March and continue until October; maximumdensities reached in April, May, and June; nymphs active throughout summer
Remarks: Extremely hardy, often existing under varied conditions of cold, heat, andaridity; often occurs in high numbers; an aggressive human parasite; may act as eithera two-host or three-host tick; unfed adults can survive over 2 years; females depositbetween 4,000 and 15,000 eggs
Dermacentor marginatus Sulzer
Medical Importance: Primary vector of Siberian tick typhus rickettsia in Eurasia;vector of viruses in the tick-borne encephalitis complex; possible vector of Omskhemorrhagic fever virus
Description: Usually ornate specimens with both eyes and festoons present (Figure54); rectangular basis capituli dorsally; males have weakly defined spur on posterodorsalmargin of second palpal segment and mixture of both large and small punctations overscutum; females have small ventral spurs on trochanters II and III
Distribution: Many areas of western and central Europe; specific countries includeAfghanistan, Albania, Bulgaria, Czech Republic, Portugal, Slovakia, Spain, France,Germany, Greece, Hungary, Romania, Switzerland, Iran, Iraq, Poland, Italy, Turkey,
Figure 53Approximate geographic distribution of Hyalomma marginatum (from:USAF Publ. USAFSAM-89-2).

375
Ticks
Yugoslavia, Russia, Belarus, Ukraine, Kazakhstan, Uzbekistan, Kyrgyzstan, Georgia,Azerbaijan, and Armenia (Figure 55)
Hosts: Adults parasitize horses, cattle, sheep, people, dogs, buffalo, swine, camels,and hedgehogs; immatures feed most frequently on small mammals, especially rodents
Seasonality: Adults generally active in spring and again in autumn; larvae usuallypeak in activity in June and July, nymphs in July and August
Remarks: Inhabits shrubby areas, low forests, marshes, lowlands, alpine steppes,and semidesert areas; in southeastern France, found in close association with woodswhere oaks, Quercus pubescens, predominated54
Dermacentor nuttalli Olenev
Medical Importance: One of several known vectors of Siberian tick typhus; alsovector of agent of tularemia in northern Eurasia
Figure 54Female (A) and male (B) Dermacentor marginatus (from: USAF Publ.USAFSAM-89-2).
Figure 55Approximate geographic distribution of Dermacentor marginatus (from:USAF Publ. USAFSAM-89-2).

376
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Description: Characteristics common to all members of genus Dermacentor; femaleshave no internal spurs on coxa IV and no cornua (Figure 56)
Distribution: Through central and eastern Siberia, Asiatic Russia, northern Mongolia,and China (Figure 57); occasionally reported from Ukraine and Kazakhstan
Hosts: Immatures generally parasitize small mammals such as field mice, rats,marmots, hamsters, hares, cats, and dogs; adults feed predominantly on larger hostssuch as horses, cattle, camels, sheep, dogs, and humans
Seasonality: Larvae and nymphs active from mid-June to mid-August with adultsactive primarily in the spring (peaking in mid-May); Splisteser and Tyron55 reportedhigh population numbers of adult D. nuttalli in steppe regions of Mongolia from mid-March to late May
Remarks: Seems especially associated with high grasslands; generally not found indense forests, river lowlands, or hilly wooded country; unfed adults usually overwinterin cracks in soil and occasionally in burrows of rodents; cease questing and becomeinactive at temperatures below 10°C (50°F)55
Figure 56Female (A) and male (B) Dermacentor nuttalli (from: USAF Publ. USAFSAM-89-2).
Figure 57Approximate geographic distribution of Dermacentor nuttalli (from: USAFPubl. USAFSAM-89-2).

377
Ticks
Dermacentor silvarum Olenev
Medical Importance: Vector of Siberian tick typhus rickettsia in Eurasia and Asia,as well as viruses in the tick-borne encephalitis complex; may be a vector of Lymeborreliosis spirochetes in Asia
Description: Males have ornamentation similar to that in Figure 58B; prominentdorsal spur on trochanter I; females have coxa IV without internal spurs; cornua presentand ventral spurs lacking on basis capituli
Distribution: Primarily in eastern and far eastern Russia and northern Mongolia; alsoreported from Belarus, Ukraine, Lithuania, Latvia, Estonia, Georgia, Kazakhstan,Uzbekistan, Turkmenistan, Kyrgyzstan, Romania, and Yugoslavia (Figure 59)
Hosts: Adults collected from people, horses, cattle, sheep, dogs, fox, and deer; larvaeand nymphs feed on numerous species of small mammals
Figure 58Female (A) and male (B) Dermacentor silvarum (from: USAF Publ.USAFSAM-89-2).
Figure 59Approximate geographic distribution of Dermacentor silvarum (from: USAFPubl. USAFSAM-89-2).

378
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Seasonality: Bimodal pattern of seasonal activity of adults with one peak in earlyJune and another in early September;56 larvae most active in June and July and nymphsfrom June to mid-August
Remarks: Inhabitant of forest steppe zones; most numerous in birch–aspen marshes,glades in mixed forests, cultivated areas in taiga forests, and other localized dense shrubareas and secondary growth forest
Australian Paralysis TickIxodes holocyclus Neumann
Medical Importance: Primary cause of tick paralysis cases in Australia;39 bite alsoknown to cause Type I hypersensitivity reactions in humans
Description: Inornate with no eyes or festoons (Figure 60); males have legs I andIV reddish, legs II and III yellowish; females have scutum broadest posterior to middle,with numerous punctations of varying sizes; coxae are large and trapezoid shaped
Distribution: Primarily in New Guinea and along eastern coastal areas of Australia(Figure 61)
Hosts: Parasitizes humans, other mammals, and birds; seems to especially prefersheep, cattle, dogs, cats, and bandicoots
Seasonality: Active in warmer months of year
Remarks: Primarily in heavily vegetated rain forest areas of eastern coastal Australia;bandicoot is natural host (bandicoot populations increasing near urban areas due tocontrol campaigns against dingoes and foxes57)
Figure 60Female (A) and male (B) Ixodes holocyclus (from: USAF Publ. USAFSAM-89-2).

379
Ticks
Taiga TickIxodes persulcatus Schulze
Medical Importance: Vector of virus of Russian spring–summer encephalitis andLyme borreliosis spirochete in Europe and Asia
Description: Characteristics common to all species in genus Ixodes; very similar inappearance to commonly encountered European castor bean tick, I. ricinus (Figure 62)
Distribution: Central and eastern Europe, Russia, Ukraine, Belarus, Kazakhstan,Uzbekistan, Kyrgyzstan, China, and Japan (Figure 63)
Hosts: Larvae and nymphs feed on wide variety of small forest mammals and birds;adults parasitize larger wild and domestic mammals; readily bites people
Seasonality: Found on hosts in late spring and summer months (Zemskaya58 foundthat, after overwintering, adults usually resumed activity in eastern part of Russian Plainduring last 10 days of April, when upper soil layers warmed up to 5 to 10°C (41 to 50°F)and remained active for 65 to 95 days
Figure 61Approximate geographic distribution of Ixodes holocyclus (from: USAFPubl. USAFSAM-89-2).
Figure 62Female (A) and male (B) Ixodes persulcatus (from: USAF Publ. USAFSAM-89-2).

380
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Remarks: Apparently more cold-hardy than I. ricinus, thus inhabiting harsher, morenorthern areas; inhabits small-leaved forests near primary coniferous forests, such asspruce–basswood combinations (commonly referred to as taiga)
European Castor Bean TickIxodes ricinus (Linnaeus)
Medical Importance: Primary vector of Lyme borreliosis spirochetes in Europe; alsoknown to transmit viruses of tick-borne encephalitis complex
Description: Long mouthparts and dark brown to black in color (females may haveportion posterior to scutum orangish) (Figure 64); resembles and closely related toAmerican species I. scapularis
Distribution: Common throughout most of Europe, including the British Isles (Fig-ure 65); also found in scattered locations in northern Africa and parts of Asia
Figure 63Approximate geographic distribution of Ixodes persulcatus (from: USAFPubl. USAFSAM-89-2).
Figure 64Female and male Ixodes ricinus (USAF photo).

381
Ticks
Hosts: Immatures recorded from lizards, small mammals, and birds; adults feedmostly on sheep, cattle, dogs, horses, and deer; adults avid parasites of humans
Seasonality: In temperate regions of range, most active in spring and autumn; twopeaks of activity may be observed: late March to early June, August to October; innorthern Africa most active in winter51
Remarks: One of most commonly encountered ticks in central and western Europe;more than 90% of tick bites in England and Ireland are from I. ricinus nymphs; as longas 3 years usually required to complete the life cycle: larvae feed first year, nymphssecond year, and adults third year; females deposit 2,000 to 3,000 eggs
Brown Ear TickRhipicephalus appendiculatus Neumann
Medical Importance: One of several vectors of boutonneuse fever rickettsia
Description: Usually inornate with both eyes and festoons present (Figure 66); looksimilar to cosmopolitan R. sanguineus; males have distinctly pointed dorsal projectionon coxa I; females have flat eyes (not obviously convex)
Distribution: Throughout southern Africa up to about 10°N latitude (Figure 67)
Hosts: Cattle primarily (for adult ticks as well as immatures); also humans, domesticanimals, and wild game such as antelope and buffalo
Seasonality: Larvae most abundant on hosts from May to July; nymphs occur onhosts from June to September; adults most active from November to March
Remarks: May be one to three generations occurring annually, depending on lengthand number of rainy seasons in range; seems especially sensitive to desiccation; duringconsecutive dry years tends to die out; unfed larvae may survive as long as 10 months,nymphs 15 months, and adults 24 months; females lay up to 6,000 eggs
Figure 65Approximate geographic distribution of Ixodes ricinus (from: USAF Publ.USAFSAM-89-2).

382
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Figure 67Approximate geographic distribution of Rhipicephalus appendiculatus (from:USAF Publ. USAFSAM-89-2).
Figure 66Male Rhipicephalus appendiculatus (Specimen provided by Dr. K. Y. Mumcuoglu, Hebrew University,Jerusalem).

383
Ticks
REFERENCES1. Benenson, A.S. (Ed.), Control of Communicable Diseases Manual, 16th edn., American
Public Health Association, Washington, DC, 1995.
2. Goddard, J., Ticks and Tick-borne Diseases Affecting Military Personnel, U.S. Air Force,School of Aerospace Medicine, San Antonio, TX, 1989.
3. Burgdorfer, W., A review of Rocky Mountain spotted fever: its agent, and its vectors inthe U.S, J. Med. Entomol., 12, 269, 1975.
4. Hoogstraal, H., Ticks in relation to human diseases caused by viruses, Ann. Rev. Entomol.,11, 261, 1966.
5. Hoogstraal, H., Ticks in relation to human diseases caused by Rickettsia species, Ann. Rev.Entomol., 12, 377, 1967.
6. CDC, Summary of notifiable diseases, 2000, MMWR, 49, 7, 2002.
7. Barbour, A. G., Maupin, G. O., Teltow, G. J., Carter, C. J. and Piesman, J., Identificationof an uncultivable Borrelia species in the hard tick Amblyomma americanum: Possibleagent of a Lyme disease-like illness, J. Infect. Dis., 173, 403, 1996.
7a. James, A. M., Liveris, D., Wormser, G. P., Schwartz, I., Montecalvo, M. A., and Johnson,B. J. B., Borrelia lonestari infection after a bite by an Amblyomma americanum tick, J.Infect. Dis., 183, 1810, 2001.
8. Spach, D. H., Liles, W. C., Campbell, G. L., Quick, R. E., Anderson, D. E. J. and Fritsche,T. R., Tick-borne diseases in the United States, N. Engl. J. Med., 329, 936, 1993.
8a. Kelly, P.J., Beati, L., Matthewman, L.A., Mason, P.R., Dasch, G.A., and Raoult, D., A newpathogenic spotted fever group rickettsia from Africa, J. Trop. Med. Hyg. 97, 129, 1994.
8b. Kelly, P.J., Beati, L., Mason, P.R., Matthewman, L.A., Roux, V., and Raoult, D., Rickettsiaafricae sp. nov., the agent of African tick bite fever, Int. J. Syst. Bacteriol. 46, 611, 1996.
9. Walker, D. and Dumler, J. S., Emergence of the ehrlichioses as human health problems,Emerg. Infect. Dis., 2, 18, 1996.
10. Maeda, K., Markowitz, N., Hawley, R. C., Ristic, M., Cox, D. and McDade, J. E., Humaninfection with Ehrlichia canis a leukocytic rickettsia, N. Engl. J. Med., 316, 853, 1987.
11. Dumler, J. S. and Bakken, J. S., Ehrlichial diseases of humans: Emerging tick-borneinfections, Clin. Infect. Dis., 20, 1102, 1995.
11a. Buller, R. S., Arens, M., Hmiel, S. P., Paddock, C. D., Sumner, J. W., Rikihisa, Y., Unver,A., Gaudreault-Keener, M., Manian, F. A., Liddell, A. M., Schmulewitz, N., and Storch,G. A., Ehrlichia ewingii: a newly recognized agent of human ehrlichiosis, New Eng. J.Med., 341, 148, 1999.
12. Gorenflot, A., Moubri, K., Precigout, E., Carcy, B. and Schetters, T. P., Human babesiosis,Ann. Trop. Med. Parasitol., 92, 489, 1998.
13. Markell, E. K., Voge, M. and John, D. T., Medical Parasitology, 7th edn., W.B. SaundersCo., Philadelphia, 1992.
14. CDC, Babesiosis — Connecticut. MMWR, 38, 649-650.
15. Thomford, J. W., Conrad, P. A., Telford, S. R., III, Mathiesen, D., Eberhard, M. L., Herwaldt,B. L., Quick, R. E. and Persing, D. H., Cultivation and phylogenetic characterization of anewly recognized human pathogenic protozoan, J. Infect. Dis., 169, 1050, 1994.
16. Emmons, R. W., Colorado tick fever, in Viral Zoonoses, Vol. I, Steel, J. H. Ed., CRC Press,Boca Raton, FL, 1979, 113.
17. Varma, M.G.R., Ticks and mites, in Medical Insects and Arachnids, Lane, R.P. andCrosskey, R.W. Eds., Chapman and Hall, London, 1993, chap. 18.
18. CDC, Outbreak of relapsing fever — Grand Canyon National Park, Arizona, 1990. MMWR40, 296-297.

384
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
19. Thompson, R. S. and Russell, R., Outbreak of tick-borne relapsing fever in SpokaneCounty, Washington, J.A.M.A., 210, 1045, 1969.
20. Monath, T. M. and Johnson, K. M., Diseases transmitted primarily by arthropod vectors,in Public Health and Preventive Medicine, Last, J. M. and Wallace, R. B. Eds., 13th edn.,Appleton and Lange, Norwalk, CT, 1992, 223.
21. Gresikova, M. and Calisher, C. H., Tick-borne encephalitis, in The Arboviruses: Epidemiologyand Ecology, Vol. IV, Monath, T. P. Ed., CRC Press, Boca Raton, FL, 1989, 177.
21a. Loktev, V. B., Ternovoy, V. A., Kurgukov, G. P., Sokolov, Y. V., Ivanov, G. Y., Loktev,A. U., Ryder, R., Netesov, S. V., New variants of tick-borne encephalitis discovered byretrospective investigation of fatal cases of tick-borne encephalitis with hemorrhagicsyndrome occurring in Novosibirsk Region (Russia) during summer of 1999, (Abstract)Intl. Conf. on Emerg. Infect. Dis., Atlanta, March 24–27, 2002, p. 11 (suppl.), board 40.
22. Nuttall, P. A. and Labuda, M., Tick-borne encephalitis subgroup, in Ecological Dynamicsof Tick-Borne Zoonoses, Sonenshine, D. E. and Mather, T. N. Eds., Oxford University Press,New York, 1994, 351.
23. Kocan, A. A., Tick paralysis, JAVMA, 192, 1498, 1988.
24. Gregson, J. D., Tick paralysis: an appraisal of natural and experimental data. Canada Dept.Agri. Monograph No. 9, 1973.
25. Schmitt, N., Bowmer, E. J. and Gregson, J. D., Tick paralysis in British Columbia, Canad.Med. Ass. J., 100, 417, 1969.
26. Stanbury, J. B. and Huyck, J. H., Tick paralysis: a critical review, Medicine, 24, 219, 1945.
27. Gothe, R., Kunze, K. and Hoogstraal, H., The mechanisms of pathogenicity in the tickparalysis, J. Med. Entomol., 16, 357, 1979.
28. Goddard, J., Ecological studies of Ixodes scapularis in Mississippi: lateral movement ofadult ticks, J. Med. Entomol., 30, 824, 1993.
29. Lancaster, J. L., Control of the lone star tick. University of Arkansas Agr. Exp. Sta. Rep.Ser. No. 67, 1957.
30. Lees, A. D., The water balance in Ixodes ricinus and certain other species of ticks,Parasitol., 37, 1, 1946.
31. Semtner, P. J., Howell, D. E. and Hair, J. A., The ecology and behavior of the lone startick. I. The relationship between vegetative habitat type and tick abundance and distributionin Cherokee Co., Oklahoma, J. Med. Entomol., 8, 329, 1971.
32. Sonenshine, D. E., Atwood, E. L. and Lamb, J. T., The ecology of ticks transmitting RockyMountain spotted fever in a study area in Virginia, Ann. Entomol. Soc. Am., 59, 1234, 1966.
33. Sonenshine, D. E., The Ticks of Virginia. Virginia Polytechnic Institute and State UniversityRes. Div. Bull. No. 139, 1979.
34. Sonenshine, D. E. and Levy, G. F., Ecology of the American dog tick, Dermacentorvariabilis in a study area in Virginia. II. Distribution in relation to vegetative types, Ann.Entomol. Soc. Am., 65, 1175, 1972.
34a. Strickland, R.K., Gerrish, R.R., Hourrigan, J.L., and Schubert, G.O., Ticks of veterinaryimportance, USDA, APHIS, Agri. Hndbk. No. 485, U.S. Department of Agriculture,Washington, D.C., 1976.
35. Keirans, J. E. and Litwak, T. R., Pictorial key to the adults of hard ticks, family Ixodidae,J. Med. Entomol., 26, 435, 1989.
36. Goddard, J., A review of the disease agents harbored and transmitted by the lone star tick,Southwest. Entomol., 12, 158, 1987.
37. Burgdorfer, W., Tick-borne diseases in the United States: Rocky Mountain spotted feverand Colorado tick fever, Acta Tropica, 34, 103, 1977.

385
Ticks
38. Goddard, J. and Norment, B. R., Spotted fever group rickettsiae in the lone star tick, J.Med. Entomol., 23, 465, 1986.
38a. Wolf, L., McPherson, T., Harrison, B., Engber, B., Anderson, A., and Whiti, P., Prevalenceof Ehrlichia ewingii in Amblyomma americanum in North Carolina, J. Clin. Microbiol.,38, 2795, 2000.
39. Goddard, J., Tick paralysis, Infect. Med., 15, 28, 1998.
40. Goddard, J., Arthropod transmission of tularemia, Infect. Med., 15, 306, 1998.
41. Goddard, J., Ticks and Lyme disease, Infect. Med., 14, 698, 1997.
42. Oliver, J. H., Owsley, M. R., Hutcheson, H. J., James, A. M., Chunsheng, C., Irby, W. S.,Dotson, E. M. and Mclain, D. K., Conspecificity of the ticks Ixodes scapularis and I.dammini, J. Med. Entomol., 30, 54, 1993.
43. Piesman, J. and Sinksky, R. J., Ability of Ixodes scapularis, Dermacentor variabilis, andAmblyomma americanum to acquire, maintain, and transmit Lyme disease spirochetes,J. Med. Entomol., 25, 336, 1988.
44. Goddard, J., Ecological studies of adult Ixodes scapularis in central Mississippi: Questingactivity in relation to time of year, vegetation type, and meteorologic conditions, J. Med.Entomol., 29, 501, 1992.
45. Goddard, J., Focus of human parasitism by the brown dog tick, Rhipicephalus sanguineus,J. Med. Entomol., 26, 628, 1989.
46. Carpenter, T. L., McMeans, M. C. and McHugh, C. P., Additional instances of humanparasitism by the brown dog tick, J. Med. Entomol., 27, 1065, 1990.
47. Klompen, J. S. H. and Oliver, J. H. J., Systematic relationships in the soft ticks, Sys.Entomol., 18, 313, 1993.
48. Hoogstraal, H., Argasid and nuttalliellid ticks as parasites and vectors, Adv. Parasitol., 24,135, 1985.
49. Hoffmann, A., Monografia de los Ixodoidea de Mexico, I parte, Rev. Soc. Mex. Hist. Nat.,23, 191, 1962.
50. Keirans, J. E., Clifford, C. M. and Hoogstraal, H., Ornithodoros yunkeri, new species fromseabirds and nesting sites in the Galapagos Islands, J. Med. Entomol., 21, 344, 1984.
51. Strickland, R. K., Gerrish, R. R., Hourrigan, J. L. and Schubert, G. O., Ticks of VeterinaryImportance. U.S. Department of Agriculture, APHIS, Agri. Hndbk. No. 485, 1976.
52. Hoogstraal, H., Changing patterns of tick-borne diseases in modern society, Ann. Rev.Entomol., 26, 75, 1981.
53. Hoogstraal, H., African Ixodoidea. I. Ticks of the Sudan. U.S. Navy, Bur. Med. Sur.,Washington, D.C., Res. Rep. NM 005-050. 29.07, 1956.
54. Gilot, B. and Pautou, G., Distribution and ecology of Dermacentor marginatus in thefrench alps and their piedmont, Acarologia, 24, 261, 1983.
55. Splisteser, H. and Tyron, U., Studies on the ecology and behavior of Dermacentor nuttalliin the Mongolian Republic, Monat. Veter., 41, 126, 1986.
56. Pomerantzev, B. I. and Serdyukova, G. V., Ecological observations of ticks of the familyIxodidae, vectors of spring-summer encephalitis in the Far East, Parazit. Sborn. Zool. Inst.Akad. Nauk. USSR, 9, 47, 1947.
57. Bagnall, B. G. and Doube, B. M., The Australian paralysis tick, Ixodes holocyclus, Aust.Vet. J., 51, 151, 1975.
58. Zemskaya, A. A., Seasonal activity of adult ticks Ixodes persulcatus in the eastern part ofthe Russian plain, Folia Parasitol., 31, 269, 1984.


387
Wasps (Yellowjackets, Hornets, and Paper Wasps)
CHAPTER 31
WASPS (YELLOWJACKETS,HORNETS, AND
PAPER WASPS)
TABLE OF CONTENTS
I. Yellowjackets ....................................................................................................388A. General and Medical Importance ..............................................................388B. General Description ....................................................................................388C. Geographic Distribution .............................................................................388D. Biology/Behavior .........................................................................................389E. Treatment of Stings .....................................................................................391
II. Hornets .............................................................................................................391A. General and Medical Importance ..............................................................391B. General Description ....................................................................................391C. Geographic Distribution .............................................................................394D. Biology/Behavior .........................................................................................394E. Treatment of Stings .....................................................................................394
III. Paper Wasps .....................................................................................................394A. General and Medical Importance ..............................................................394B. General Description ....................................................................................394C. Geographic Distribution .............................................................................394D. Biology/Behavior .........................................................................................394E. Treatment of Stings .....................................................................................396
References ......................................................................................................................396

388
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
ImportancePainful stings; allergic RXNS
DistributionNumerous species almost worldwide
LesionCentral white spot with erythematous
halo; amount of local swelling isvariable
Disease TransmissionNone
Key ReferenceAkre, R. D., et al., USDA, SEA, Agri.
Handbk., #552, 1981.
TreatmentPain relievers, antipruritic lotions for
local RXNS; systemic RXNS mayrequire antihistamines, epinephrine,and other supportive measures
YELLOWJACKETS
Figure 2Worker yellowjacket (from: U.S. DHEW, PHS,CDC, Pictorial Keys).
I. YELLOWJACKETSA. General and Medical Importance
Venomous wasps in the genera Vespula,Paravespula, and Dolichovespula are calledyellowjackets and comprise about 26 species(some entomologists still do not recognize thegeneric status of Paravespula and would groupthem with Vespula). Some species nest near (inthe ground) or in human dwellings and can bea nuisance and health threat to people (Figure1). Yellowjackets produce painful stings andmay cause death due to sting allergy (see Chap-ter 2). Cellulitis may occur following stings bysome scavenger yellowjackets. Foragingyellowjackets are particularly numerous aroundrecreation areas and refuse collection sites, wherethey are attracted to meats, sweet carbohy-drates, soda pop, etc.
B. General Description
The name “yellowjacket” refers to the typicalyellow and black bands on the abdomen (Fig-ure 2), although some species are actually blackand white, such as the baldfaced hornet. Thepattern of markings on the yellowjacket gaster(most prominent portion of the abdomen) isoften diagnostic as to species (Figure 3). Mostspecies are smaller than paper wasps (1.5 to 2.0cm) and more robust in appearance like honey-bees. Wasps, yellowjackets, and hornets haveinconspicuous hairs on their bodies that are notfeathered (when observed under magnification).
C. Geographic Distribution
Paravespula maculifrons, the easternyellowjacket, occurs from Minnesota to Texasand eastward. It is probably the most trouble-some yellowjacket in the eastern and southeast-ern U.S. Paravespula vulgaris, the commonyellowjacket, is Holarctic, being widely distrib-uted across Europe, Asia, and North America.Vespula squamosa, the southern yellowjacket,occurs from Wisconsin to Texas and southeast-ward to the Atlantic Coast. Yellowjackets thathave been introduced into nonnative habitats

389
Wasps (Yellowjackets, Hornets, and Paper Wasps)
seem to be especially troublesome pests. The introduced German yellowjacket, P.germanica, is rapidly becoming a problem in the northeastern U.S. as well as theMidwest. Also, the western yellowjacket, P. pennsylvanica, is a severe pest in thewestern U.S. In certain years this species appears in such great numbers that itsurpasses mosquitoes and flies as an annoyance to campers.1 In addition, this specieshas been introduced into Hawaii where it builds perennial colonies and is a pest insugar cane fields.
D. Biology/Behavior
Yellowjackets of the genus Dolichovespula build aerial nests. This is the case for thelarge black and white species called the “baldfaced hornet” (D. maculata). Actually,
Figure 1Yellowjacket workers tending nest (photo courtesy Dr. James Jarratt, Entomology Department,Mississippi State University).
Figure 3Gaster patterns of some yellowjackets; not drawn to scale (from: USDA Agri. Hndbk. No. 552).

390
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
this species is not a hornet and should be called an aerial yellowjacket (see Section IIof this chapter). The other genera of yellowjackets, Vespula and Paravespula, usuallybuild nests in underground sites. Yellowjacket nests are multicombed with a surround-ing paper envelope (Figure 4 and Color Figure 31-30). The mature size of yellowjacketcolonies in temperate regions ranges from 500 cells in 2 combs in some Vespula sp.to 15,000 cells in 8 to 10 combs in some Paravespula sp.
Mature colonies may have from as few as 75 to over 5,000 worker yellowjackets. Mostyellowjackets typically have annual nesting cycles, but in some of the southernmost areasof their distribution, perennial colonies of V. squamosa and P. maculifrons have beenreported. This has led to discovery of 6 to 9 feet tall nests in Florida containing over100,000 cells. See Color Figure 31-31 for a picture of a 4-foot tall yellowjacket nest foundin Mississippi. A single overwintered queen yellowjacket initiates and builds a colonywithout aid from other queens. After the first brood of workers emerge, the queen ceasesforaging and building activities and becomes the egg layer. At that point she rarely leavesthe colony. The queen is much larger than her workers (1.5 to 3 times worker size). Ayellowjacket colony usually survives until late fall (September to November), dependingupon the species and locality. There is rapid colony growth during late summer. Thehundreds of new queens that emerge from the colony mate with males (which were alsoproduced in the fall), and each inseminated queen hibernates in a protected place untilthe following spring when the cycle is repeated. Some species, typically in the genusParavespula, scavenge for decaying protein and carbohydrates at carrion, garbage cans,rotting fruit, picnic areas, and meat processing plants. This seems to be a problem
Figure 4Yellowjacket nest showing multiple combs and paper envelope (from: Mississippi CooperativeExtension Service).

391
Wasps (Yellowjackets, Hornets, and Paper Wasps)
especially in the fall, resulting in a serious sting-ing hazard to people.
E. Treatment of Stings
The treatment recommendations given foryellowjacket stings is generally that recom-mended for all stinging wasps.
Local treatment of yellowjacket stings in-volves using ice packs and/or pain relievers tominimize pain, washing the wound to lessenthe chances of secondary infection, and admin-istering oral antihistamines to counteract thedirect release of histamine (not IgE-mediated).In the case of a large local reaction, rest andelevation of the affected arm or leg may also beneeded.
For allergic reactions, administration of epi-nephrine, antihistamines, and other supportivetreatment may be required (see Chapter 2).
II. HORNETS
A. General and Medical Importance
In the U.S., the term “hornet” is often misap-plied to the yellowjacket, D. maculata, be-cause it is large with white and black markingsand it builds large aerial nests. True hornetsare represented in North America by only onespecies, Vespa crabro, the brown hornet orEuropean hornet (Figure 5). This large hornetproduces a very painful sting and may produceallergic reactions in sensitive individuals (seealso Chapter 2).
B. General Description
Again, it is important to mention that the com-monly called “baldfaced hornet” that producesa large, egg-shaped aerial nest is not a truehornet — it is a yellowjacket. V. crabro (theonly true U.S. hornet) is a distinctive wasp witha large, robust body (2.5 to 3.5 cm long) andcharacteristic brown, orange, and red colora-tion. They have the head swollen behind theeyes and ocelli (small, simple eyes) remotefrom the margin of the head.
ImportancePainful stings; allergic RXNS
DistributionSeveral species almost worldwide; only
one U.S. species: Vespa crabro
LesionCentral white spot with erythematous
halo; amount of local swelling isvariable
Disease TransmissionNone
Key ReferenceAkre, R. D. and Davis, H. G. Ann. Rev.
Entomol., 23, 215, 1978
TreatmentPain relievers, antipruritic lotions for
local RXNS; systemic RXNS mayrequire antihistamines, epinephrine,and other supportive measures
HORNETS
Figure 5Worker hornet, Vespa crabro.

392
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
OFTEN ASKED QUESTION
HOW DO YELLOWJACKETS BUILD A NEST IN THE GROUND?
People often encounter yellowjackets when cutting grass, hiking, playing golf, or otheroutdoor activities during late summer. Unfortunately, they may fly up the pants legs whenemerging from their holes in the ground. Stinging events can be quite severe with multiplestings possible. Why do these little pests come out of a hole in the ground? How do theyconstruct a nest underground? First of all, the hole in the ground is just an entrance to anest underground. Even though the nests are underground, they are still paper nests withthe familiar combs and a paper envelope surrounding them. Raw materials gathered byyellowjackets to construct the “paper” include wood or vegetable fibers mixed with salivarysecretions. They may even utilize human products such as blankets, newspapers, orcardboard. The queen yellowjacket selects a site (usually already a hole, crack, or cavernin the ground) and builds the first few nest cells. Almost simultaneously, she constructs apaper envelope around the developing nest (Figures 1 and 2). When the first batch ofworkers emerge, the queen then switches from provisioning/building the nest to solely egg-laying. Workers then take over the jobs of foraging for food and nest building. Nest buildingis continuous from the time the first workers emerge until the colony declines (usually fall).Accordingly, underground nests may get quite large in late summer, containing thousandsof workers. As the nest grows, yellowjackets excavate dirt to enlarge the undergroundcavity. Most of the evacuated earth is carried outside the burrow and dropped. As summerends and fall approaches, yellowjackets generally (there are exceptions) produce newqueens and the colony dies. Newly formed queens spend the winter in hollow trees,stumps, wall voids of houses, etc. waiting to emerge in the spring and start the process allover again.

393
Wasps (Yellowjackets, Hornets, and Paper Wasps)
Figure 2Early stages of yellowjacket nest (left) and baldfaced hornet nest (right).
Figure 1Yellowjacket nest in early stages of development (with individual block of cells removed frominside).

394
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
C. Geographic Distribution
The true hornets belong to the genus Vespa and occur in Europe and Asia. The onlyspecies in the U.S. is V. crabro, which was accidentally introduced into the eastern U.S.around 1850. It now occurs sparsely in the Atlantic seaboard states into the South.
D. Biology/Behavior
Vespa crabro is very similar in its biology to yellowjackets. They produce annual,single-female colonies usually housed in a multiple-combed nest with a thick brownenvelope in sheltered aerial locations such as hollow trees, attics, and wall voids ofhouses. This brown paper nest is easily distinguishable from the typical gray papernests of other wasps and baldfaced hornets (Color Figure 31-32). The nests aregenerally large due to the large individual cells and contain about 1,500 to 3,000 cellsin 6 to 9 combs with 200 to 400 workers. Hornets hunt insects, and several speciesattack honeybee colonies.2 Although not usually scavengers, they do occasionallypuncture the skin of ripe fruits and feed on them.
E. Treatment of Stings
Hornet stings are treated the same as yellowjacket stings.
III. PAPER WASPSA. General and Medical Importance
This large and diverse wasp group is usually divided into two major divisionsdepending on lifestyle: solitary or social. Of the 15,000 or so species of stinging waspsworldwide, 95% are solitary species that are not aggressive toward people. The socialwasps, on the other hand, form large colonies and can pose serious threats to humans.The most common social groups in temperate regions are the yellowjackets and hornets(subfamily Vespinae) and the paper wasps (Polistes). Paper wasps have a great affinityfor building their nests on or around buildings; therefore, human encounters, and thusstinging incidents, are common.
B. General Description
Paper wasps have elongate, slim bodies (2 to 2.5 cm long) and are variously coloredyellow, black, brown, and red depending on the species. Some are striped, yellowishor white and brown, and are occasionally confused with yellowjackets. Males of manypaper wasps have more yellow on the “face” (frons and clypeus) than females of thesame species.
C. Geographic Distribution
Paper wasps in the genus Polistes include about 200 species distributed worldwide intemperate and tropical regions. Polistes rubiginosa (now broken into two species, P.carolina and P. perplexus) is a bright red-orange wasp that is common throughout thesouthern U.S. (Figure 6A). P. exclamans (Figure 6B), also commonly found in the

395
Wasps (Yellowjackets, Hornets, and Paper Wasps)
southern U.S., is the striped species most oftenmislabeled as “yellowjackets.” P. annularis is alarge, dark red paper wasp that nests nearpermanent bodies of water. It is common in thesouthern U.S. In the western U.S. and California,P. aurifer and P. apachus are significant pests.P. fuscatus is a commonly encountered waspfound throughout Canada and the U.S. (Figure6D). P. gallicus is a species occurring widelythroughout southern France and Italy. Polistesspecies common in Japan include P. smelleniand P. jadwigae.
D. Biology/Behavior
Paper wasps build a nest consisting of a single,open-faced comb of gray paper. The nest isattached to various substrates (buildings, trees,shrubs) by a single petiole. Polistes wasps feedon any extrafloral juices, plant sap, sweets, andvarious arthropods. They catch caterpillars tofeed their brood. In temperate regions eachinseminated queen hibernates in a protectedsite and emerges in the spring to initiate nestbuilding. Usually a single female, called afoundress, initiates the nest, but in some speciesother individual females, called cofoundresses,may join the original foundress and help buildand provision the nest. These multiplefoundresses (usually 2 to 6) compete for repro-ductive dominance in this small colony. Even-tually a dominance hierarchy or pecking orderdevelops with one foundress (i.e., queen), andit lays more of the eggs than the otherfoundresses. After emergence of the first broodof workers, the other foundresses lose theirreproductive status and the colony usually de-velops into a single queen (monogynous) soci-ety. The workers perform most colony tasks,especially nest building and foraging; however,reproduction remains the primary function ofthe queen. Although the queen is distinct inbehavior from the other colony members, she isnot usually discernibly different in appearancefrom the workers.
The colony grows rapidly through the sum-mer, and mature colony size is usually reachedin August or September. Typical mature Polistescolonies probably contain 30 to 75 adults and
PAPER WASPS
Paper wasp with nest. (Photo courtesythe Ross E. Hutchins photographcollection, Mississippi EntomologicalMuseum, Mississippi State University.)
ImportancePainful stings; allergic RXNS
DistributionNumerous species almost worldwide
LesionCentral white spot with erythematous
halo; amount of local swellingvariable
Disease TransmissionNone
Key ReferenceAkre, R. D. and Davis, H. G., Ann. Rev.
Entomol., 23, 215, 1978
TreatmentPain relievers, antipruritic lotions for
local RXNS; systemic RXNS mayrequire antihistamines, epinephrine,and other supportive measures

396
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
100 to 200 cells, although very large colonies of 150 to 200 adults and nests of 1,000to 1,900 cells have been reported. In late summer and early fall, males and reproductivefemales (future queens) are produced. The colony declines as workers die and thereproductives leave the nest to mate. After mating, males soon die or do not usuallysurvive the winter, whereas inseminated females seek out and survive in winterhibernation sites. Large aggregations of males and females are sometimes seen nearhibernation sites or in tall trees, towers, and buildings during late fall, on warm daysof winter, or in early spring. This “house dwelling” hibernation behavior of Polistes maylead to human stings any time of the year.3 The following spring, the annual cycle isrepeated as females emerge from hibernation to initiate a new nest.
E. Treatment of Stings
Paper wasp stings are treated the same as yellowjacket stings.
REFERENCES1. Ebeling, W., Urban Entomology, University of California, Division of Agricultural Science,
Los Angeles, 1978, 357.
2. Harwood, R. F. and James, M. T., Entomology in Human and Animal Health, 7th ed.,Macmillan, New York, 1979, chap. 17.
3. Alexander, J. O., Arthropods and Human Skin, Springer-Verlag, Berlin, 1984, chap. 10.
Figure 6Some common paper wasps: Polistes perplexus (A), P. exclamans (B), P. annularis (C), P. fuscatus(D) (from: U.S. DHEW, PHS, CDC Pictorial Keys).

PART IV
PERSONAL PROTECTIONMEASURES AGAINST
ARTHROPODS


399
Pros and Cons of Insect Repellents
CHAPTER 32
PROS AND CONS OFINSECT REPELLENTS
TABLE OF CONTENTS
I. Introduction ......................................................................................................400
II. Mosquito Repellents ........................................................................................400A. DEET Products ............................................................................................400B. Plant-Derived Substances ............................................................................401C. Permethrin ...................................................................................................402D. Skin-So-Soft® ................................................................................................403
III. Tick Repellents .................................................................................................403A. DEET Products ............................................................................................403B. Permethrin ...................................................................................................403
IV. Health Concerns Associated with DEET Products ........................................404A. Background..................................................................................................404B. Safe Application Rates/Methods .................................................................404
References ...............................................................................................................405

400
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
I. INTRODUCTION
Insect repellents are chemicals that cause insects to make directed, oriented movementsaway from the source of repellent. In light of disease transmission by insects and otherarthropods, chemical substances that have repellent effects or interfere with biting arewonderful because they enable us to go places and do things in insect/disease infestedareas. Undoubtedly, repellents have prevented thousands of cases of malaria, denguefever, encephalitis, and other mosquito-borne diseases. However, in recent years,concerns about the potential adverse health effects of insect repellents have increased,especially for those containing the active ingredient DEET. N,N-diethyl-3-methylbenzamide, also known as DEET, is the most effective and widely used insectrepellent available.1 It repels a variety of mosquitoes, chiggers, ticks, fleas, and bitingflies, and an estimated 50 to 100 million people in the U.S. use it each year.2,3 Therehave been a few reports of systemic reactions from repeated cutaneous exposure toDEET. For example, six girls, ranging in age from 17 months to 8 years, developedbehavioral changes, ataxia, encephalopathy, seizures, and/or coma after repeatedcutaneous exposure to DEET; three subsequently died.3 Additionally, episodes ofconfusion, irritability, and insomnia have been reported by Everglades National Parkemployees following repeated and prolonged use of DEET.3 However, a few reportsof adverse reactions to DEET should not be misconstrued to mean that repellents aredangerous and not to be used. All commercially available repellents are generally safewhen used according to their label instructions. This chapter discusses various chemicalrepellents, their modes of action, possible side effects, and precautions necessary toprevent adverse reactions.
II. MOSQUITO REPELLENTSA. DEET Products
Previously called N,N-diethyl-m-toluamide, N,N-diethyl-3-methylbenzamide (DEET)remains the gold standard of currently available insect repellents.1 The chemical wasdiscovered by USDA scientists and patented by the U.S. Army in 1946. It was registeredfor use by the public in 1957. Twenty years of empirical testing of more than 20,000other chemical compounds has not resulted in another marketed product with theduration of protection and broad-spectrum effectiveness of DEET.1 DEET is sold undernumerous brand names, and is formulated in various ways and concentrations —creams, lotions, sprays, extended-release formulations, etc. (Figure 1). Concentrationsof DEET range from about 5 to 100%, and, generally, products with higher concentra-tions of DEET have longer repellence times.4 However, at some point there is not adirect correlation between concentration and repellency. For example, in one study,50% DEET provided about 4 h of protection against Aedes aegypti mosquitoes, butincreasing the concentration to 100% provided only 1 additional hour of protection.5
When used, DEET is absorbed through the skin into the systemic circulation; one studyshowed that about 10 to 15% of each dose can be recovered from the urine.2 Otherstudies have shown lower skin absorption values in the range of 5.6 to 8.4%.1 Possibly,the solvent used in the product enhances absorption. One study showed that ethanolmay increase permeation of DEET.6 Regardless, the lowest concentration of DEETproviding the longest repellency should be chosen for use. Products containing 10 to35% DEET will provide adequate protection from biting insects under most circum-

401
Pros and Cons of Insect Repellents
stances. Small children should probably not use concentrations higher than 10%.1 TheU.S. military uses a polymer-based extended-release formulation containing 35% DEET,which is available to the general public through the 3M Corporation under the brandname Ultrathon®.
B. Plant-Derived Substances
Plant-derived substances which provide some repellency against mosquitoes includecitronella, cedar, verbena, pennyroyal, geranium, lavender, pine, cajeput, cinnamon,rosemary, basil, thyme, allspice, garlic, and peppermint. However, these productsgenerally only provide temporary protection, if any at all. One study testing DEET-based products against Buzz Away® (containing citronella, cedarwood, eucalyptus,lemongrass, alcohol, and water) and Green Ban® (containing citronella, cajuput,lavender, safrole-free saasfrass, peppermint, bergaptene-free bergamot, calendula, soy,and tea tree oils) demonstrated essentially no repellency against Aedes aegypti.4
However, other studies with Buzz Away® indicated that the product does haverepellency for about 2 h.1 One plant-based repellent that was released in the U.S. in1997, Bite Blocker®, (containing soybean oil, geranium oil, and coconut oil) has showngood repellency against Aedes mosquitoes for up to 3.5 h.1 Citronella candles have beenmarketed as backyard mosquito repellents for years. One study compared the abilityof commercially available 3% citronella candles, 5% citronella incense, and plaincandles to prevent bites by Aedes mosquitoes under field conditions.7 Persons near thecitronella candles had 42% fewer bites than controls, but ordinary candles provided a23% reduction. The efficacy of plain candles and citronella incense did not differ. The
Figure 1Several commercially available insect repellents — all but Natrapel® contain the active ingredientDEET.

402
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
ability of plain candles to decrease biting may be because they serve as a decoy sourceof warmth, moisture, and carbon dioxide.
C. Permethrin
Permethrin, actually a pesticide rather than a repellent, is a human-made syntheticpyrethroid available for use against mosquitoes, but can only be used on clothing. Theproduct is sold in lawn, garden, or sporting goods stores as an aerosol under the namePermanone® Repel or something similar (Figure 2). It is non-staining, nearly odorlessand resistant to degradation by light, heat, or immersion in water.2 Interestingly, it canmaintain its potency for at least 2 weeks, even through several launderings.1,8 Permethrincan be applied to clothing, tent walls, and mosquito nets. In fact, sleeping underpermethrin-impregnated mosquito nets has been tried extensively in malaria preven-tion campaigns in Africa, New Guinea, Pakistan, and Malaysia.9 For personal protection,the combination of permethrin-treated clothing and DEET-treated skin creates almost
Figure 2Permanone® tick repellent.

403
Pros and Cons of Insect Repellents
complete protection against mosquito bites. In field trials conducted in Alaska, personswearing permethrin-treated uniforms and 35% DEET (on exposed skin) had more than99.9% protection (1 bite/h) over 8 h, whereas unprotected persons received an averageof 1188 bites/h.10
D. Skin-So-Soft®
The bath oil, Avon Skin-So-Soft®, is often used as a mosquito repellent and is discussedhere because of its widespread use. Apparently, Skin-So-Soft® does have some transientrepellency for mosquitoes. Rutledge et al.11 reported that the bath oil exhibits repel-lency for Aedes aegypti, but the effect is short-lived. They reported that Skin-So-Soft®
is not nearly as effective as DEET (gram for gram). In another study, the Avon productprovided 0.64 h of protection from A. albopictus mosquito bites compared to >10 hprotection provided by 35% DEET.8 Avon now markets products under the Skin-So-Soft® label that contain an EPA-recognized repellent.
III. TICK REPELLENTSA. DEET Products
One study12 demonstrated that DEET on military uniforms provided between 10 and87.5% protection against ticks, depending upon species and life stage of the tick. Therewas an average of 59.8% protection against all species of ticks. Obviously, protectionlevels in the 50% range are less than desirable, considering the fact that only one tickcan transmit a tick-borne disease. In a U.S. Army repellent rating system, DEET isassigned a 2X value, whereas, permethrin is given a 3X rating.13 DEET products aresimply not as effective in protecting from tick infestation as permethrin products.12,14
However, the advantage is that DEET can be applied to human skin in places likelyto be encountered by ticks — ankles, legs, arms.
B. Permethrin
By far, the most effective tick repellent is permethrin (sold under various brand names,but especially Permanone® [Figure 2]), a synthetic pyrethroid pesticide with very lowmammalian toxicity.12-14 It is for clothing use only, not to be applied directly to humanskin. In one study, a pressurized spray of .5% permethrin was compared to 20% and30% DEET products on military uniforms in a highly infested tick area. A 1-minapplication of permethrin provided 100% protection, compared to 86% and 92%protection with the two DEET products, respectively.14 Additionally, permethrin hasbeen shown to remain in clothing, providing 100% protection against ticks after severalwashings.1,8,13 Generally, application of permethrin to clothing is done by a slow,sweeping application of the aerosol spray until clothing is slightly wet. Label instruc-tions should be followed. Some people take the clothing to be worn (needingprotection from ticks), hang it on a clothes line, spray it, and put it on after drying.When ticks subsequently crawl on the clothing treated with permethrin they are eitherkilled or repelled. Permethrin is extremely effective against New World ticks, but thereis some evidence that not all tick species are equally repelled by permethrin. One OldWorld species, the camel tick, actually showed a high tolerance to permethrin, and anincreased biting response when exposed to the product.15

404
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
IV. HEALTH CONCERNS ASSOCIATED WITH DEETPRODUCTS
A. Background
DEET has been used for over 30 years by millions of people worldwide. Although ithas an excellent safety record, there have been sporadic reports of adverse reactionsassociated with its use. Most of these have resulted from accidental exposure, such asswallowing, spraying into the eye, or repeated application, although at least one caseoccurred in an 18-month-old boy following brief exposure to low-strength (17.6%)DEET.16 While most complaints have involved transient minor skin or eye irritation, rarecases of toxic encephalopathy have been reported, especially in children. Adversereactions have included headache, nausea, behavioral changes, disorientation, muscleincoordination, irritability, confusion, difficulty sleeping, respiratory distress, and evenconvulsions and death. In one report, six girls, ranging in age from 17 months to 8years, developed behavioral changes, ataxia, encephalopathy, seizures, and/or comaafter repeated cutaneous exposure to DEET; three later died.3 However, if DEETproducts (preferably not the high concentration products such as 50 to 100%) areproperly applied and used according to their label directions, they are generallyconsidered safe. Use of DEET products according to EPA guidelines (next section) willgreatly reduce the possibilty of toxicity.
B. Safe Application Rates/Methods
Except under extraordinary conditions, high concentrations of DEET should not beused. Products with 10 to 35% DEET will provide adequate protection under mostconditions. For children, even lower concentrations may be warranted. The AmericanAcademy of Pediatrics recommends that repellents used on children contain no morethan 10% DEET.1 The following guidelines will help ensure safe use of DEET-basedrepellents. Remember, repellents should only be applied to clothing and/or exposedskin according to the product label directions.
DO:• Use aerosols or pump sprays for skin and for treating clothing. These products
provide even application.• Use liquids, creams, lotions, or sticks to apply more precisely to exposed skin.• After outdoor activity, wash DEET-covered skin with soap and water.• Always keep insect repellents out of the reach of small children.
DON’T:• Apply to eyes, lips or mouth, or over cuts, wounds, or irritated skin.• Over-apply or saturate skin or clothing.• Apply to skin under clothing.• Apply more often than directed on the product label.

405
Pros and Cons of Insect Repellents
REFERENCES1. Fradin, M.S., Mosquitoes and mosquito repellents: A clinician’s guide, Ann. Intern. Med.,
128, 931-940, 1998.
2. Abramowicz, M., Insect repellents, Medical Letter, 31, 45-47, 1989.
3. CDC, Seizures temporally associated with use of DEET insect repellent - New York andConnecticut, MMWR, 38, 678-680, 1989.
4. Chou, J.T., Rossignol, P.A. and Ayres, J.W., Evaluation of commercial insect repellents onhuman skin against Aedes aegypti, J. Med. Entomol., 34, 624-630, 1997.
5. Buescher, M.D., Rutledge, L.C., Wirtz, R.A. and Nelson, J.H., The dose-persistencerelationship of DEET against Aedes aegypti, Mosq. News, 43, 364-366, 1983.
6. Stinecipher, J. and Shah, J., Percutaneous permeation of N,N-diethyl-m-toluamide (DEET)from commercial mosquito repellents and the effect of solvent, J. Toxicol. Environ. Health,52, 119-135, 1997.
7. Lindsay, R.L., Surgeoner, G.A., Heal, J.D. and Gallivan, G.J., Evaluation of the efficacy of3% citronella candles and 5% citronella incense for protection against field populationsof Aedes mosquitoes, J. Am. Mosq. Control Assoc., 12, 293-294, 1996.
8. Schreck, C.E. and McGovern, T.P., Repellents and other personal protection strategiesagainst Aedes albopictus, J. Am. Mosq. Control Assoc., 5, 247-250, 1989.
9. Service, M.W., Mosquitoes. In R.P. Lane and R.W. Crosskey (Eds.), Medical Insects andArachnids, Chapman and Hall, London, 1993, pp. 120-240.
10. Lillie, T.H., Schreck, C.E. and Rahe, A.J., Effectiveness of personal protection againstmosquitoes in Alaska, J. Med. Entomol., 25, 475-478, 1988.
11. Rutledge, L.C., Wirtz, R.A. and Buescher, M.D., Repellent activity of a proprietary bath oil(Skin-So-Soft), Mosq. News, 42, 557-560, 1982.
12. Evans, S.R., Korch, G.W.J. and Lawson, M.A., Comparative field evaluation of permethrinand DEET-treated military uniforms for personal protection against ticks, J. Med. Entomol.,27, 829-834, 1990.
13. Evans, S., Personal protective techniques against insects and other arthropods of militarysignificance. U.S. Army Environmental Hygiene Agency, Aberdeen Proving Ground,Maryland, TG No. 174.
14. Schreck, C.E., Snoddy, E.L. and Spielman, A., Pressurized sprays of permethrin or deet onmilitary clothing for personal protection against Ixodes dammini, J. Med. Entomol., 23,396-399, 1986.
15. Fryauff, D.J., Shoukry, M.A. and Schreck, C.E., Stimulation of attachment in a camel tick,Hyalomma dromedarii: the unintended result of sublethal exposure to permethrin-treatedfabric, J. Med. Entomol., 31, 23-29, 1994.
16. Briassoulis, G., Narlioglou, M., and Hatzis, T., Toxic encephalopathy associated with useof DEET insect repellents: a case analysis of its toxicity in children, Hum. Exp. Toxicol.,20, 8, 2001.


407
Arthropod-Specific Personal Protection Techniques
CHAPTER 33
ARTHROPOD-SPECIFICPERSONAL PROTECTION
TECHNIQUES
TABLE OF CONTENTS
I. Protection from Mosquitoes ............................................................................408A. Avoidance ....................................................................................................408B. Screening......................................................................................................408C. Netting ..........................................................................................................408
II. Protection from Ticks ......................................................................................408A. Boots, Trousers, Tape .................................................................................408B. Unorthodox Methods ..................................................................................409C. Tick Removal ...............................................................................................409
III. Protection from Other Arthropods .................................................................412A. Biting Midges ...............................................................................................412B. Chiggers (Red Bugs) ...................................................................................413C. Kissing Bugs ................................................................................................413
References ...............................................................................................................414

408
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
I. PROTECTION FROM MOSQUITOES
A. Avoidance
Common sense, non-chemical, measures for mosquito avoidance include such thingsas limiting outdoor activity after dark during peak mosquito season and avoidingknown mosquito-infested areas (e.g., swamps, marshes, etc.) during those times aswell. In addition, persons who must be outdoors after dark during mosquito seasonshould wear long sleeves and long pants to physically limit mosquito biting.
B. Screening
Probably one of the most basic and effective sanitation measures to limit arthropod-human contact is that of screen wire windows and doors. Screens are constructed ofvarious metals or plastic and are ordinarily 16 × 16 × 20 mesh. They should be tightfitting over window openings. Screen doors should be hung so that they open outward.Being such a basic protection measure, screens are sometimes overlooked. However,their importance cannot be overemphasized. I personally investigated a fatality due toeastern equine encephalitis in which the family had no screens on the house. By theirown testimony the family members stated, “Mosquitoes eat us up every night!”
C. Netting
During mosquito season, persons camping out may sleep under mosquito nets forprotection from mosquitoes. This becomes essentially mandatory on safaris or othertrips to the tropics or subtropics for protection against disease-carrying mosquitoes.Ordinarily mosquito netting is made of cotton or nylon with 23 to 26 meshes per inch.Netting should not be allowed to lay loosely on the head since mosquitoes can feedthrough the net wherever it touches the skin. Generally, people construct a crude frameover the bed or end of the bed to fit the net over (Figure 1). For added protection, thenet can be sprayed lightly with permethrin (Permanone®) before getting inside. Thispermethrin treatment should be effective for several months if not rinsed or washedout.
II. PROTECTION FROM TICKSA. Boots, Trousers, Tape
Personal protection techniques for tick bites include avoiding tick-infested woods,tucking pant legs into boots or socks, and using repellents on pant legs and socks(Figures 2 and 3). Tucking trousers into boots or socks forces ticks to crawl up theoutside of one’s pants, thus making them easier to spot and remove. Wide masking tapemay be used to “tape down” pants legs at the ankles, or even placed around the anklesor thighs with the sticky side exposed to protect against ticks crawling up the legs(Figure 4). One research study showed that significantly fewer nymphal deer ticks werepicked up on 5-minute walks in the woods when boots were worn with ankles tapedthan when sneakers were worn with socks exposed.1

409
Arthropod-Specific Personal Protection Techniques
B. Unorthodox Methods
Many unorthodox (or questionable, at least) methods of tick protection are commonlyused by people. Flea collars worn around the ankles, Avon Skin-So-Soft®, vitamin C,garlic, sulfur powder, panty hose, and others have been reported to me as “great tickrepellents.” While these efforts may possibly provide some degree of protection,tucking the trousers with proper use of Permanone® is much more effective.2 Besides,using pet products such as flea collars may be dangerous due to absorption of pesticidethrough the skin (Figure 5); they have not been Food and Drug Administration (FDA)approved for human wear.
C. Tick Removal
“What is the best way to remove a tick after it gets on you?” The answers are varieddepending on who you ask and what part of the country you are in because manyfolklore methods are available. Hard ticks attach themselves firmly to a host for afeeding period of several days and are especially difficult to remove. Methods such astouching attached ticks with a hot match, coating them with mineral oil, petroleum jellyor some other substance, and/or “unscrewing” them are but a few of the homeremedies that supposedly induce them to “back out.”
The theory behind coating a tick with fingernail polish, petroleum jelly, or mineraloil is that covering the spiracles with a substance will interfere with their breathing and
Figure 1Bed netting for protection against mosquito bites (photo courtesy of Joseph Goddard).

410
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
make the ticks “back out”. However, ticks are able to shut off their spiracles (at leasttemporarily) and certainly do not breathe via the mouthparts. Even if coating a tick witha substance causes it to back out, the time required to accomplish this is unacceptable(usually 1 to 4 h).
Since the lengthy feeding period is an important factor in disease transmission byticks, it is crucial that a tick be removed as soon as possible to reduce chances ofinfection by disease organisms. During several years of field research with ticks, theauthor often had to remove them from himself or others, and pulling them straight offwith blunt forceps (tweezers) seemed to work best (Figure 6). There has been someresearch in this area. Glen Needham at Ohio State University did a very good study ofthis problem.3 He evaluated five methods commonly used for tick removal: (1)petroleum jelly, (2) fingernail polish, (3) 70% isopropyl alcohol, (4) hot kitchen match,and (5) forcible removal with forceps. Needham found that the commonly advocatedmethods are either ineffective, or worse, actually created greater problems. If petroleumjelly or some other substance causes the tick to back out on its own (and most often
Figure 2Tucking pant legs into socks for tick protection.

411
Arthropod-Specific Personal Protection Techniques
Figure 3Tucking pants legs into rubber boots for tick protection.
Figure 4“Taping up” with masking tape for tick protection. The last layer or two should be with the stickyside out.
it does not), the cement surrounding the mouthparts used for attachment remains inthe skin where it continues to cause irritation. Touching the tick with a hot match maycause it to burst, increasing risk of disease pathogen exposure. Furthermore, hot objectsmay induce ticks to salivate or regurgitate infected fluids into the wound. “Unscrewing”a tick is likely to leave broken mouthparts in the host’s skin.
Needham recommended the following procedure for tick removal: (a) use bluntforceps or tweezers; (b) grasp the tick as close to the skin surface as possible and pullupward with steady, even pressure; (c) take care not to squeeze, crush, or puncturethe tick; (d) do not handle the tick with bare hands because infectious agents may enter

412
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
via mucous membranes or breaks in the skin; and (e) after removing the tick, disinfectthe bite site and wash hands thoroughly with soap and water.
Many tick-borne diseases can be successfully treated with antibiotics in their initialstages; therefore, early diagnosis is imperative. For this reason, marking the day of atick bite on a calendar is a good idea. If unexplained disease symptoms occur within2 weeks from this day, persons should be reminded to see their physicians andspecifically inform him/her of the tick bite. This method has proven to be very helpfulin diagnosis of tick-borne disease. Although there are a number of well-known tickremoval methods (mostly folklore), the best one seems to be the simplest — pull themstraight off with blunt forceps and disinfect the bite site.
III. PROTECTION FROM OTHER ARTHROPODSA. Biting Midges
Biting midges (no-see-ums), the tiny slender gnats that are extremely common alongthe Atlantic and Gulf Coasts, are small enough to pass through ordinary screen wireused to cover windows and doors. Accordingly, a finer mesh screen wire must be usedto prevent entry of these flies into dwellings. Outdoors, DEET repellents and long-sleeved shirts and long pants can provide relief in infested areas. Avon Skin-So-Soft®
Figure 5Skin lesions from human use of animal flea collars for tick protection. (Photo courtesy S. Evansand R. Fitzsimmons, U.S. Army Env. Hyg. Agency.)

413
Arthropod-Specific Personal Protection Techniques
Figure 6Recommended method for tick removal: grab tick with forceps as close to the skin as possible andpull straight off. (From: USAF Publ. USAFSAM-SR-89-2)
is often used as a repellent for biting midges, and controlled studies indicate that theproduct provides some protection.4 However, the effectiveness is probably because theoiliness of Skin-So-Soft traps the tiny midges on the skin surface.
B. Chiggers (Red Bugs)
Chigger mites (sometimes called “red bugs”) occur in grass, weeds, or leaves and geton passing vertebrate hosts. Therefore, personal protection measures for chiggers aresimilar to those for ticks. Tucking pants legs into socks or boots and spraying clothingwith DEET-based repellents provide good protection. Clothing treatment with Permanone®
(permethrin) is also very effective against chiggers. After exposure to infested outdoorareas, hot soapy baths or showers will help remove any chiggers, attached orunattached.
C. Kissing Bugs
Kissings bugs (Triatoma species), the vectors of Chagas disease in Mexico and Centraland South America, are nocturnal insects that seek refuge by day in the cracks andcrevices in poorly constructed houses or in the loose roof thatching of huts. Personalprotection from the bugs involves avoidance (if possible) — not sleeping in thatched

414
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
roof huts in endemic areas — and exclusion methods such as bed nets. Prevention andcontrol of domestic species of triatomines can be accomplished by proper constructionof houses, wise choice of building materials, sealing cracks and crevices, and precision-targeting of insecticides within the home.
REFERENCES1. Carroll, J. F. and Kramer, M., Different activities and footwear influence exposure to host-
seeking nymphs of Ixodes scapularis and Amblyomma americanum, J. Med. Entomol., 38,596, 2001.
2. Evans, S. R., Korch, G. W. J. and Lawson, M. A., Comparative field evaluation ofpermethrin and DEET-treated military uniforms for personal protection against ticks, J.Med. Entomol., 27, 829, 1990.
3. Needham, G. R., Evaluation of five popular methods for tick removal, Pediatrics, 75, 997,1985.
4. Schreck, C. E. and Kline, D. L., Repellency determinations of four commercial productsagainst six species of ceratopogonid biting midges, Mosq. News, 41, 7, 1981.

PART V
FURTHER READING,GLOSSARY, AND INDEX


417
Suggestions for Further Reading
SUGGESTIONS FORFURTHER READING
Alexander, J.O. 1984. Arthropods and Human Skin. Springer-Verlag, Berlin.
Arnett, R.H. 2000. American Insects: A Handbook of the Insects of America North ofMexico, 2nd ed., CRC Press, Boca Raton, FL.
Borror, D.J., Triplehorn, C.A., and Johnson, N.F. 1989. An Introduction to the Study ofInsects, 6th ed. Saunders College Publishing, Philadelphia.
Burgess, N.R.H. and Cowan, G.O. 1993. A Color Atlas of Medical Entomology. Chapmanand Hall, London.
Busvine, J.R. 1980. Insects and Hygiene, 3rd ed. Chapman and Hall, London.
Eldridge, B.F. and Edman, J.D. 2000. Medical Entomology. Kluwer Academic Publishers,Dordrecht, Netherlands.
Gilles, H.M. and Warrell, D.A. 1993. Bruce-Chwatt’s Essential Malariology, 3rd ed.Arnold Publishing Co., London.
Goddard, J. 2000. Infectious Diseases and Arthropods. Humana Press, Totowa.
Lane, R.P. and Crosskey, R.W. 1996. Medical Insects and Arachnids. Chapman and Hall,London.
Guerrant, R.L., Walker, D.H., and Weller, P.F. 1999. Tropical Infectious Diseases:Principles, Pathogens, and Practice (Volumes I and II). Churchill Livingstone,Philadelphia.
Harwood, R.F. and James, M.T. 1979. Entomology in Human and Animal Health, 7thed. Macmillian Publishing Co., New York.
Joneja, J.M.V. and Bielory, L. Understanding Allergy, Sensitivity, and Immunity. RutgersUniversity Press, New Brunswick.

418
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Jones, S.L. 2000. Clinical Laboratory Pearls. Penn, Lippincott, Williams, and Wilkins,Philadelphia.
Mallis, A. 1997. Handbook of Pest Control, 8th ed. Mallis Textbook and TechnicalTraining Company (GIE Media), Cleveland, OH.
Markell, E.K., Voge, M., and John, D.T. 1992. Medical Parasitology, 7th ed. W.BSaunders Co., Philadelphia.
Mullen, G. and Durden, L.A. 2002. Medical and Veterinary Entomology. AcademicPress, New York.
Oldstone, M.B.A. 1998. Viruses, Plagues, and History. Oxford University Press, Oxford.
Palmer, S.R., Soulsby, L., and Simpson, D.I.H. 1998. Zoonoses: Biology, Clinical Prac-tice, and Public Health Control. Oxford University Press, Oxford.
Polis, G.A. 1990. The Biology of Scorpions. Stanford University Press, Stanford, CA.
Service, M.W. 1996. Medical Entomology for Students. Chapman and Hall, London.
Simon, H.U. 2000. CRC Desk Reference for Allergy and Asthma. CRC Press, Boca Raton,FL.
Smith, E.H. and Whitman, R.C. 1992. NPCA Field Guide to Structural Pests. National PestControl Association, Washington, DC.
Sonenshine, D.E. and Mather, T.N. 1994. Ecological Dynamics of Tick-Borne Zoonoses.Oxford University Press, Oxford.
Thaler, D.E., Hope, R.A., and Longmore, J.M. 1999. Oxford Handbook of ClinicalMedicine (American Edition). Oxford University Press, Oxford.

419
Glossary
GLOSSARY
Abdomen The hindmost of the three body divisions in insects.Acaracide A substance poisonous to ticks or mites.Aculeate Pertaining to the members of the order Hymenoptera, which sting — the
bees, wasps, and ants.Alate Winged form; in ants alates are the winged reproductive forms.Anal The posterior wing veins.Antennae (sing. Antenna) A pair of sensory segmented appendages located on the
head above the mouthparts.Anterior Toward the front end.Anthropophilic Describes any bloodsucking arthropod that prefers humans to lower
animals as its food source.Apiary Any place where honeybees are kept.Apical At the tip or end.Apterous Without wings.Arbovirus An arthropod-borne virus.Arista A large bristle located on the last antennal segment of some flies.Atopy IgE-dependent allergy often arising from an unknown exposure to an antigen.Babesiosis Infection with a protozoan organism in the genus Babesia; often a malaria-
like illness.Basis capitulum Basal portion of the capitulum on which the tick mouthparts are
attached. May be of various shapes (hexagonal, rectangular, subtriangular, etc.)in hard ticks.
Beak The proboscis of a sucking insect.Bifid Clearly divided into two parts.Brood All the immature members of a colony including eggs, larvae, and pupae.Brood Cell A cell made by a worker bee in which to lay an egg.Bubo An enlargement of a lymph gland caused by an infection.Bug Loosely used to denote any arthropod; technically only meaning members of the
insect order Hemiptera.Cantharidin A chemical produced by certain beetles (especially family Meloidae) that
causes blistering on the skin of humans.

420
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Calypter A basal lobe or lobes on the posterobasal portion of the axillary membraneof the wings of some Diptera
Carapace The sclerotized (hardened) plate forming the dorsal surface of an arachnidcephalothorax.
Carnivorous Feeding upon animals.Caste A group of morphologically distinct individuals within a colony often having
distinctive behavior (e.g., workers, queens, and males).Caterpillar The larva of a butterfly or moth having a cylindrical body, a well-
developed head, and thoracic legs and abdominal prolegs.Cell Terminology used in describing areas of an insect wing. An area of the wing
enclosed by veins.Cephalothorax Head and thorax combined; characteristic of arachnids.Cerci (sing. Cercus) Paired appendages at the posterior end of the abdomen, as in
a cockroach.Chelae (sing. Chela) The second pair of appendages (pedipalps) of scorpions and
pseudoscorpions; modified into pincers.Chelicerae Paired appendages of an arachnid, highly variable in shape and size. In
scorpions they are short, chelate, and lacking a poison gland; in spiders they terminatein a sharp tip with a venom duct; and in ticks they lie dorsally to the hypostome,completing the cylindrical mouthparts that are inserted when a tick feeds.
Chitin A complex nitrogenous carbohydrate forming the main skeletal substance ofarthropods.
Class A grouping used in classification. A division of a phylum.Classification The arrangement of species in a hierarchical system of categories and
taxa.Clypeus That part of the insect head below the front to which the labrum is attached.Cocoon A silken enclosure secreted by a larva just before pupation.Colony Individuals, other than a single mated pair, which cooperate to build a nest
or rear offspring.Complete metamorphosis Type of insect development in which there are egg, larva
(caterpillar), pupa (resting stage), and adult stages.Compound eye Insect eye composed of many individual elements represented
externally by hexagonal facets.Contiguous Touching one another.Cornua Small projections extending from the dorsal, posterolateral angles of basis
capituli in ticks.Costa The thickened anterior vein of the insect wing.Coxae (sing. Coxa) Basal segments of the leg. In ticks, small sclerotized plates on the
venter representing the first segment of the leg to which the trochanters aremovably attached. From anterior to posterior, the coxae are designated by Romannumerals I, II, III, and IV. Bifid coxae are those that are cleft, divided, or forked.
Dentition Refers to the presence and arrangement of denticles (teeth). In ticks, thenumerical arrangement of the rows of denticles on the ventral side of thehypostome is expressed by dentition formulas. Thus, dentition 3/3 means thatthere are three longitudinal rows of denticles on each side of the median line ofthe hypostome.
Dermatitis Inflammation or eruption of the skin.

421
Glossary
Desensitization (also called immunotherapy) Elimination or reduction of allergicsensitivity; usually accomplished through a programmed course of antigen treat-ment.
Deutonymph The third stage of a mite.Dichotomous Divided into two parts. Insect identification keys are often kichotomous,
giving the reader two choices after each question.Diurnal Active in the daytime.Dorsal Pertaining to the back or top of the body.Ecdysis The process of shedding the skin or exoskeleton.Ectoparasite A parasite that feeds on the surface of the body and is usually blood-
sucking.Ehrlichiosis Disease caused by one of several rickettsial organisms in the genus
Ehrlichia.Elytra Thick or leathery front wing of beetles.Envenomization (also called Envenomation) The poisonous effects caused by the
bites, stings, secretions, or stinging hairs of insects, other arthropods, and certaininvertebrate animals, or the bites of reptiles.
Enzootic Disease of animals constantly present in an area.Epizootic Describes any disease of animals, the number of cases of which exceeds
that normally expected.Erucism Urtication caused by moth or butterfly larvae.Exuvium The cast exoskeleton of an arthropod.Eyes In insects, may be simple (singular) or compound variously arranged on the
head. In ticks, eyes, when present, are located on the edges of the scutum. Theyare about even with the site of leg I attachment in hard ticks; soft ticks may haveeyes on their lateral margins near coxae I and II.
Facet The external surface of one of the individual units of a compound eye, as inthe fly.
Family A category in the hierarchy of classification. A division of an order.Femur The third leg segment outward from the insect body.Festoons Uniform rectangular areas, separated by distinct grooves, located on the
posterior margin of most genera of hard ticks.Filariasis Disease caused by filarial worms (Nematodes) which invade lymphatic
tissues and are transmitted by mosquitoes.Flagellum The third and succeeding segments of most antennae.Flagellomere A division of the flagellum of the antennae.Foci (sing. Focus) With reference to a disease, specific areas in which the disease is
prevalent.Foundress An individual, usually a fertilized female, that founds a new colony. All
subsequent offspring are her daughters and sons.Galea Portion of some insect mouthparts. Specifically, the outer lobe of the maxilla.Gaster The prominent part of wasp or ant abdomen, separated from the other body
parts by a thin connecting segment called a petiole or pedicel.Genera (sing. Genus) Categories in the classification hierarchy to which species are
assigned.Gradual metamorphosis Type of insect development in which there are egg, nymph,
and adult stages; no worm-like larval stage present.Gravid Full of ripe eggs; ready to lay eggs.

422
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Grub Term used for a thick-bodied, sluggish, often white insect larva.Goblets Small, round structures located in the spiracular plate of ticks.Grooves On ticks, linear depressions or furrows, primarily on the ventral surface.Halteres (sing. Haltere) Small knoblike structures on each side of the thorax of a fly
immediately behind each wing.Haustellate Having mouthparts adapted for sucking blood.Head The anterior body region of an insect bearing eyes, antennae, and mouthparts.
Ticks and mites have no true head.Hemelytron The forewing of the true bugs (order: Hemiptera).Hemimetabolous Simple metamorphosis.Hemocoel The major body cavity of insects containing the blood.Hemolymph Arthropod blood.Hemolytic anemia Shortage of red blood cells due to their premature destruction;
sometimes a complication in brown recluse spider bite.Herbivorous Feeding on plants.Hibernation A period of lethargy or suspension of most bodily activities with a greatly
reduced resipiration rate, occurring mostly during periods of low temperature.Histamine Organic substance released from tissues during an allergic reaction to
injury or invasion by an antigen, causing dilation of local blood vessels.Holometabolous Complete metamorphosis.Holoptic In flies, the eyes touching above.Hood The anterior projection of the integument in soft ticks above and covering the
mouthparts.Hypognathus Head and mouthparts situated ventrally (pointed down).Hypopharynx Mouthpart structure, located medially, that is anterior to the labium. In
many sucking insects this structure contains the salivary channel.Hypostome In ticks, the median ventral structure of the mouthparts that lies parallel
to and between the palps. It bears the “recurved teeth” or denticles.Imago The adult stage of an insect.Infarction Formation of a localized area of necrosis produced by occlusion of the
arterial blood supply or venous drainage of a part.Inornate In ticks, the absence of a color pattern on the scutum.Instar An insect between successive molts.Joint An articulation. The area of flexion between sections of an appendage.Labellum Insect mouthpart; the tip of the labium.Labial palpi (sing. Labial palpus) Segmented sensory appendages of the labium of
insects.Labium “Lower lip” of insect mouthparts.Labrum “Upper lip” of insect mouthparts.Laciniae (sing. Lacinia) Insect mouthparts; the inner lobe of the maxilla.Large local reaction Reaction to sting or bite that is exaggerated, but still contiguous
with the sting site.Larvae (sing. Larva) An immature stage of an insect having complete metamorphosis
but excluding the egg or pupal stage. Also, a six-legged first instar mite or tick.Larviparous Method of reproduction by bringing forth larvae that have already
hatched in the female’s body.Lepidopterism Urtication caused by hairs, scales, or spines of adult moths or
butterflies.Lesion An injury to body tissue. Often a spot or mark.

423
Glossary
Maggot A legless larva (usually limited in usage to Diptera) that has no well developedhead region.
Malphigian tubules Long and slender blind tubes in the hemocoel that open into thebeginning of the hind intestine of insets. Excretory in function.
Mammillae (sing. Mammilla) Elevations of various forms found on the integumentof Ornithodoros tick species.
Mandibles The most anterior pair of two pairs of insect mouthpart structures.Maxillae (sing. Maxilla) The pair of mouthpart structures lying behind the mandibles.Maxillary palpi (sing. Maxillary palpus) Segmented sensory structures located on the
maxillae.Mesosoma The seven abdominal segments of scorpions.Metamorphosis The series of changes through which an insect passes in developing
from egg to adult.Metasoma The “tail” of scorpions.Molt The process of shedding the exoskeleton.Musciform Resembling a fly.Myiasis The invasion of human tissues by dipterous larvae.Nearctic One of the zoogeographical regions of the earth that includes Canada,
Alaska, Greenland, the United States, and the temperate northern part of Mexico.Neotropical South America, Central America (including Mexico), and the Antilles.Nits (sing. Nit) Eggs of lice.Nocturnal Being active during night.Nomenclature The scientific names of living organisms and the application of these
names.Nymph An immature insect that does not have a pupal stage (e.g., cockroach,
grasshopper, bed bug). Also, an eight-legged immature tick or mite.Obligate parasite A parasitic association in which the parasite cannot complete its life
cycle without a suitable host.Ocelli (sing. Ocellus) The simple eyes of arthropods.Oothecae (sing. Ootheca) Egg case in cockroaches.Opisthosoma The entire abdomen in arachnids.Opisthognathus Mouthparts situated and directed toward the posterior (backward).Order A division of a class in the hierarchy of categories.Ornate Definite enamel-like color pattern superimposed on the base color of the
integument in hard ticks.Ovipositor Tubular structure used by many insects to lay eggs; modified into a stinger
in the ants, wasps, and bees.Palpi (sing. Palpus or Palp) In insects, a segmented process on the maxillae or labium.
In ticks, paired articulated appendages located on the front and sides of the basiscapituli and lying parallel to the hypostome.
Papilloma Benign tumor derived from epithelium.Papules (sing. Papule) Small elevations of the skin which are usually inflamed.Parasite Any animal or plant that lives in or on, and at the expense of, another animal
or plant.Parthenogenesis Condition in which egg development can occur without fertilization.Pectines Feathery sensory organs of scorpions; believed to sense ground vibrations.Pedicel In spiders, the petiole (waist) between the cephalothorax and abdomen; in
ants and other Hymenoptera the stalk between thorax and abdomen.Pedipalps The second pair of appendages of an arachnid.

424
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Petechiae (sing. Petechia) Pinpoint, flat, round, purplish red spots.Petiole The narrowed portion of the abdomen of certain Hymenoptera.Pharynx In insects, the anterior region of the foregut, located between the mouth and
the esophagus.Pheromone A chemical produced by one individual that causes a specific reaction
by other members of the same species.Phylum A major division of the animal kingdom; a category.Plumose As in antennae, meaning feather-like.Prepupa The quiescent stage immediately before the pupal stage in insects.Proboscis A beak-like projection containing various arrangements of mouthparts and
their modifications.Prognathous With the head horizontal and the jaws directed forward.Pronotum Dorsal shield over the anterior segment of the thorax; in cockroaches the
pronotum looks like the head.Protonymph In mites, the second instar.Pubescent Covered with short, fine hairs; appearing hairy.Pupae (sing. Pupa) A nonfeeding and inactive stage (except mosquitoes) between the
larvae and adults.Puparium A shell or case produced by the hardening of the last larval skin.Quinones Caustic, highly volatile hydrocarbons secreted by some arthropods as a
defensive measure.Rickettsiae (sing. Rickettsia) Single-celled, very small, intracellular bacteria. Notorious
members of this group include the causative agents of Rocky Mountain spottedfever, Rickettsia rickettsii, and murine typhus, Rickettsia typhi.
Segment A ring or subdivision of the body or of an appendage between areas offlexibility, with muscles attached for movement.
Sclerite Hardened plate or portion of an insect body.Scutum The sclerotized dorsal plate posterior to the capitulum in hard ticks. It covers
almost the entire dorsal surface in the male and about one half the dorsal surfacein the unengorged female.
Sensillae (sing. Sensilla) Setae, bristles, or hairs having a sensing function.Sexual dimorphism Morphological differences between males and females of a
species.Species complex A group of closely related species, the taxonomic relationships of
which are sometimes unclear making precise identification difficult.Spiracle A breathing pore which marks the external opening of the tracheal system.Spurs In ticks, coxal spurs are projections from the posterior surface of the posterior
margin of the coxae; they may be rounded or pointed, large or small.Stylet A needlelike structure, especially the elongated portion of the peircing-sucking
type of insect mouthparts.Sylvatic Describes any disease usually acquired in forest or other uncultivated,
unoccupied areas rather than in an urban environment or other areas developedby humans.
Synonym Another name used for a species, or other taxon, invalid because it is eitherof a more recent date or invalidly proposed.
Systemic Affecting the entire body.Tarsi (sing. Tarsus) The terminal leg segments.Taxa (sing. Taxon) Groups of organisms classified together.

425
Glossary
Taxonomy The naming and arraning of species and groups into a system of classi-fication.
Telson In scorpions, the last segment of the “tail”; bears the sting.Thorax A body region in insects, located behind the head, that bears the legs and
wings.Tibia The fourth segment (from the body outward) of an insect leg.Trachea An internal respiratory tube.Transovarial transmission The production (by an infected vector) of infected eggs that
hatch into individuals likewise infected and capable of transmitting the infectingorganism.
Transstadial transmission The survival of parasites or pathogens through successivestages (larva — nymph — adult).
Trochanter The portion of the leg between the coxa and the femur.Trophallaxis Exchange of alimentary canal liquid among colony members of social
insectsUrticaria Intensely itchy wheals; also popularly called hives.Vein A tube running through the membrane of the wings of insects.Wheal A localized area of edema on the skin, often with severe itching. The typical
lesion of urticaria.Wigglers Mosquito larvae.Worker A member of a nonreproductive or sterile caste that contributes to a colony
welfare by rearing offspring of reproductives. In Hymenoptera, workers are theones that sting.
Zoogeographic regions The six divisions of the earth’s surface distinguished by majordifferences in animal and plant life.
Zoonoses (sing. Zoonosis) Diseases of animals that may be transmitted to humans.


427
Index
INDEX
A
Abdominal pain, 25, 314Acari, See also Mitesmorphology, 85mouthparts, 43-44, 85Acarus siro, 68-69, 240Acetylcholine, 35-36Acute toxic reaction (nonallergic), 14-15Adenopathy, 100Aedes, 252, 264-265, 267, 268-273
A. aegypti, 252-254, 264, 268-269A. albopictus, 252-254, 264, 270-271A. vexans, 252, 272-273
Aerial yellowjacket, 389-390Africanized (“killer”) honey bees, 117-118African sleeping sickness, 180-181African tick-bite fever, 328, 334Aggressive house spider, 321-322. See also Hobo
spiderAIDS/HIV transmission by insects, 251Allergens, 5-6
antigen binding sites, 6cockroach parts and feces, 22-25dust mites, 22-25ingested, 25inhaled, 22salivary secretions, 25-26venom constituents, 35-38
Allergic reactions, 5-8, 12-18. See alsoAnaphylaxis; Hypersensitivity reactions
bee stings, 14-16, 116biochemical mediators of, 6-7delayed, 8-9, 47fire ant stings, 12-16, 108-110hornet stings, 373-374house dust mites, 22-25, 232-233ingestion/inhalation of body parts, 25
lice bites, 216-222large local reactions, 14-17mechanisms, 6mortality, 15normal reactions, 14-15respiratory involvement in, 15-18, 21-25systemic reactions, 16-18treatment, 8, 16-18
long-term management, 18-21normal reactions, 15large local reactions, 16systemic reactions, 16-18venom immunotherapy, 18-19venom cross-reactivity 15
Allergic rhinitis, 7, 21-26, 232-233Allergy, See Allergic reactions; Hypersensitivity
reactionsbee sting, 14cockroach inhalent, 22-25house dust mite, 22-25, 232-233long-term management of, 18-19, 233
Triatoma, 20Allodermanyssus sanguineus, 234, 236-237Amblyomma, 335-337, 351-354, 366-367
A. americanum, 351-352. See also lone startick
A. cajennense, 365-366A. hebraeum, 366-367A. maculatum, 353-354
American babesiosis, 328, 336American cockroach, 150-152American dog tick, 328, 333, 341, 355-356American house dust mite, 232American trypanosomiasis, 130-133. See also
Chagas’ diseaseAmphipod, 159Anaphe, 59Anaplasma phagocytophila, 335

428
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Anaplasmosis, 335Anaphylaxis (anaphylactic shock), 5,7, 12,15
death from, 7,15fire ant sting, 12-13, 108-109second phase (biphasic), 18signs and symptoms, 16-17treatment and management, 16-18
Anatomy, See Morphology; Identification ofarthropods
AndroctonusA. amoreuxi, 305-306A. australis, 305-306A. bicolor, 305A. crassicauda, 305-306A. mauritanicus, 305
Anemia, 100, 311-313hemolytic, 313from brown recluse spider bite, 311-313
Angioedema, 7, 15Anopheles, 250, 252, 264-265, 268, 274
A. albimanus, 279-280A. arabiensis, 281A. balabacensis, 282A. bwambae, 281A. crucians, 242A. darlingi, 280-281A. dirus, 282A. flavirostris, 283A. freeborni, 242A. funestus, 283A. gambiae, 281-282A. leucosphyrus, 282-283A. melas, 281A. merus, 281A. minimus, 283A. pseudopunctipennis, 284-285A. quadriannulatus, 281A. quadrimaculatus, 252, 273-274A. stephensi, 285-286
Anopheline mosquito larvae, 263Ants, 108-114
fire, 108-110harvester, 110-113list of stinging ants, 108stinger morphology, 33-34stinging behavior, 31stings, 31-38, 108velvet, 113-114
Antibody-mediated hypersensitivity reactions, 5Anticholinesterase ointments, 223Antihistamine treatment, 4,8,25
histamine overload from numerous stings, 4,14-15
Ant stings, See also each specific antallergic reactions, 33-38, 108fire ant, 12-13, 107-109harvester ant, 110-113incidence, 13lymphatic reactions, 111
mortality, 13pustular lesions, 12, 37velvet ant, 113-114venom constituents, 35-37venom cross-reactivity, 15venom immunotherapy, 18-19
Apamin, 35Aphonopelma, 324Apis mellifera, 116. See also Honey BeeAppendicitis-like symptoms, 314Arachidonic acid, 7Arachnida, See also Mites; Ticks; Scorpions;
Spidersmorphology, 82-85
Araneae, 82. See also Spidersmorphology of, 82-85
Arboviruses, 252-255, 258-263Argasidae, 341-345. See also Soft TicksArilus cristatus, 134Artificial container mosquitoes, 252, 264Ash-gray blister beetles, 122-123Asian cockroach, 150Asian tiger mosquito, 252, 264, 270-271Asian hyalomma, 371-372Assassin bugs, 129-132
bites, 129description and distribution, 130-131mouthparts, 40-42
Asthma, 22-23, 100chironomid midges and, 23cockroaches and, 22-24house dust mites and, 22-24mosquitoes and, 16
Astigmata, 233Atylotus incisuralis, 168Arthralgia, 262-263Auchmeromyia luteola (senegalensis), 200-201Aural myiasis, 61, 208-209Australian cochroach, 150Australian paralysis tick, 341, 378-379Austroconops macmillani, 170Automeris, 138
A. io, 138-143. See also IO moth larvaeAvon Skin-so-Soft, 403Axillary pain, 100, 111
B
Babesia spp., 336-337Babesia bigemina, 336Babesia canis, 336Babesia divergens, 336Babesia equi, 336Babesia gibsoni, 336Babesia microti, 336-337MO1 agent, 337WA1 agent, 337
Babesiosis, 328, 336-337Bacillary dysentary, 180

429
Index
Baker’s mite, 69Baldfaced hornet, 389Bancroftian filariasis, 255-256Bark scorpions, 307Bartonella bacilliformis, 171Bartonellosis, 171Basophils, 6Bed bugs, 126-128
biology/behavior, 128bites, 46
allergic reactions, 14lesion patterns, 46-54location on body, 46-54number of lesions, 46-54treatment, 128
cutaneous sequelae, 54description and geographic distribution, 126HIV transmission by, 251method of blood feeding, 40mouthparts, 40mysterious bites and, 69signs of, 46-54treatment, 128
Bees, 116-120bumble bees, 118-120carpenter, 119control and avoidance, 19-20honey bees, 116-117killer (Africanized), 117-118nests (hives),117stings, 116-117 See Bee stingsstinging behavior, 31
Bee stings,allergy, 14histamine overdosage, 4, 14-15lethal dose, 4mortality, 15stinger, 116
morphology of, 31removal, 117
systemic reactions, 14-17treatment,
Africanized (killer) bees, 4, 14-15bumble bees, 14-15honey bees, 14-15
venom components, 35-36venom cross-reactivity, 15
Beetlesblister, See Blister beetleslarvae of, 122
diarrhea caused by, 25food contamination, 25-26
staphylinid, 56Belle Glade, Florida, 251Benzodiazepine, 307Benzyl benzoate, 25Beta-2 agonists, 8Biopsies, of papules or nodules, 44-45
Bites, 39-54 See also each specific arthropodbed bug, 40, 46centipede, 48cutaneous sequelae, 54diagnostic patterns, 53direct effects, 4flea, 47fly, 43, 47hypersensitivity reactions, 14imaginary, 69infectious complications, 45lesion characteristics, 52-54lice, 40, 46location on body, 52-54method of blood feeding, 40midge, 43, 46mite, 49mosquito, 47mouthpart types, 40-42mysterious, 68-69number of lesions, 52-54pathology and diagnosis, 44-45recognizing, 52-54salivary secretions and, 44spider, 48, 310-314 See Spider bitessystemic reactions, 14tick, 49true bugs, 46
Biting flies,black flies, 164-165deer flies, 166-167horse flies, 168-169midges, 169-170sand flies, 171-176stable flies, 178-180tsetse flies, 180-183
Biting gnats, 169. See also Biting midgesavoidance and protection, 394bites, 47
lesion patterns, 52-54location on body, 52-54number of lesions, 52-54
description and geographic distribution, 169life history and behavior, 170mouthparts, 43treatment, 170
Black blow fly, 211, 211-214,Black Caucasian honeybee, 116Black flies, 48, 159
bites, 48, 52lesion patterns, 52-54location on body, 52-54number of lesions, 52-54reactions, 164systemic reactions, 14, 158treatment, 165
description and geographic distribution, 164life history, 165

430
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
method of blood feeding, 40mouthparts, 43onchocerciasis vectors, 165
Black imported fire ant, 109Black-legged tick, 340Black soldier fly, 62
myiasis from, 62, 209Black widow spider, 314. See also Widow spiders
antivenin, 321bite effects, 314-315bite mortality, 316case history, 319description, 317geographic distribution, 317-318habitats and life history, 318hourglass marking, 317neurotoxic venom, 314species of, 317-318treatment of bites, 321
Blatella, 149-151B. asahinae,150B. germanica, 150-151
Blatta orientalis, 151Blatteria, 149 See also CockroachesBlepharitis, 221Blister beetles, 121-123
cantharidin toxin, 56, 121ingestion of, 56management/treatment, 57, 123medical significance, 56, 121
Blisters, 56, 123Blood-feeding arthropods
AIDS/HIV transmission, 251methods of blood feeding, 40mouthpart types, 40
Bloodworms, 191Blow flies, 188-190
biology/behavior, 188Congo floor maggot, 200descriptions, 188larvae of, 188myiasis, 205
treatment, 213screwworm flies, 198Tumbu fly, 202
Bluebottle fly, 188Bluish spots, 221Body lice, 216-217
bite lesion patterns, 52-54bite locations, 52-54cutaneous sequelae, 54description, 216differentiating from head lice, 218disease transmission, 216eggs, 216primary sensitization, 216treatment, 217
Boils or boil-like lesions, 196, 202, 204-205Bombus, 117
Bont tick, 366Bot fly, 196-198. See also Human bot fliesBoutonneuse fever, 334Bradykinin activator, 7Breakbone fever, 253Bronchial hyperreactivity, 22Bronchodilators, 18, 25Brown banded cockroach, 150-151Brown cockroach, 150Brown dog tick, 360-361Brown ear tick, 381-382Brown hornet, 391Brown recluse spider, 310-314
antivenin, 313biology/behavior, 312-313description and geographic distribution, 312necrotic skin lesions, 311treatment of bites, 313venom, 9violin-shaped markings, 312
Browntail moth larvae, 58-60Brugia, 255
B. malayi, 255Brugian filariasis, 255Brumptomyia, 176Bryobia praetiosa, 238Bubonic plague, 156Buffalo gnats, 164Bugs, See True bugsBulldog ants, 108Bumble bees, 118-119
biology/behavior, 119treatment of stings, 119
Burrowing flea (chigoe), 158-160Buthidae, 302 See ScorpionsButhus, 305
B. minax, 305B. occitanus, 305-306
Butterflies, 291larvae, See Urticating caterpillars
C
Cable mites, 74Caddisflies, 23Calabar swellings, 166Calcium chloride, 321Calcium gluconate, 321California group encephalitis, 260-262California harvester ant, 111Calliphora, 188
C. cadaverina, 80C. vicina, 188, 208-209C. vomitoria, 80
Calliphoridae, 188myiasis, 205
Canine scabies, 241Cantharidin, 56, 121Carios, 362

431
Index
C. rudis, 362-363C. talaje,363-364
Carpenter bees, 119Carpets, 25. See also House dust mitesCarrion’s disease, 171Castor bean tick, 380-381Caterpillars, 58. See also Urticating caterpillars
stings, 58-59treatment, 59
Cat flea, 157Cayenne tick, 365CD4+ cells, 6Cellulitis, 45Centipedes, 145
bite lesion patterns, 52-54, 145-146description, 146differentiating from millipedes, 85-86morphology, 81, 85treatment, 148
Centruroides, 301-307 See also ScorpionsC. elegans, 305C. exilicauda, 301-307C. gertschi, 304C. infamatus, 305C. limpidus, 305C. noxius, 305C. sculpturatus, 301-307C. suffussus, 305C. vittatus, 301-307
Ceratopogonidae, 169bites, 169protection from, 412treatment, 170
Chagas’ disease, 129-130Cheese skipper, 62Chelicerae, 44Chewing mouthparts, 40Cheyletiella, 239
C. blakei, 51, 239C. furmani, 51C. parasitivorax, 239C. yasguri, 51, 239
Chicken mite, 236Chigger mites, 230-232
bites, 230location on body, 52-54, 230number of lesions, 52-54pattern of lesions, 52-54
cutaneous sequelae, 54treatment, 231
Chigoe flea, 158Chilopoda, 85Chironomidae, 191-192
larvae, 192respiratory problems from, 22-25
Chironomus, 191C. decorus, 191C. plumosus, 22-23
Chloropidae, 190
Chondroitin monosulfate, 6Chrysomya
C. albiceps, 211C. bezziana, 199C. chloropyga, 211C. rufifacies, 63
ChrysopsC. atlanticus, 166-167C. dimidiata, 166C. discalis, 166C. silacea, 166
Chyluria, 100Cimex
hemipterous, 128lectularis, 126. See also Bed bugs
Cladotanytarsus lewisi, 22-25Clothing treatment,
for lice, 215for scabies, 243
Clover mites, 238Cnephia pecuarum, 164Cochliomyia
C. hominivorax, 198-200C. macellaria, 208-209
Cockroaches,allergens, 22-25allergies, 22-25descriptions, 150disease transmission, 149food contamination, 25geographic distribution, 150medical importance, 149prevention/control, 150species, 150
Cockroach inhalent allergy, 22-25management and treatment, 22-23
Coleoptera, 80Colorado tick fever, 338Coma, 100Computer mites, 74Conenose bugs, 128-129. See also Assassin bugs;
Kissing bugsallergic reactions to bites, 14Chagas’s disease from, 129
Congo floor maggot, 199treatment/prevention, 200
Conjunctivitis, 57-59, 101Contact dermatitis, 232Convulsions, 286Copra itch, 239Coquillettidia perturbans, 252, 258Cordylobia anthropophaga, 202Cow killers, 113Crab lice, 221. See also Pubic liceCrimean-Congo hemorrhagic fever, 328Cromolyn sodium, 8, 26Cross-reactivity among venoms, 15Crotamiton, 244Crustacea, 95

432
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
CtenocephalidesC. canis, 157C. felis, 157
Culex, 252, 274-277, 286-287C. annulirostris, 287C. nigripaplus, 252, 274-275C. pipiens, 252, 275-276C. quinquefasciatus, 252, 275-276C. restuans, 252C. salinarius, 252, 276-277C. tarsalis, 252, 277-278C. tritaeniorhynchus, 286
Culicinae, 263Culicoides
C. furens, 169-170C. pulicaris, 169-170
CulisetaC. inornata, 252C. melanura, 252
Cutaneous leishmaniasis, 171Cuterebra, 205-206Cyanide secretions, 225Cytokines, 6Cynomyopsis cadaverina, 80
D
Daddy longlegs, 84Dapsone, 10, 313 See also Brown recluse spidersDark rice field mosquitoes, 278Dasymutilla occidentalis, 114Deer flies, 166-167
bites, 166number of lesions, 52-54reactions, 166systemic reactions, 14treatment of bites, 167
disease transmission, 166method of blood feeding, 40mouthparts, 40-42
DEET (insect repellent), 400, 403-404Delayed-type hypersensitivity reactions, 7-8, 44Delousing, 217, 220, 222Delusions of parasitosis, 67-74
possible real arthropod causes, 68-69treatment, 73-74typical complaints, 69-70workplace infestations, 74
DemodexD. brevis, 245D. folliculorum, 245
Dengue fever, 253mosquito vectors, 255
Dengue hemorrhagic fever (DHF), 255Dermacentor
D. andersoni, 333, 340-341, 354-355D. dagestanicus (=niveus), 338D. marginatus, 374-375D. nuttalli, 375-376
D. silvarum, 377-378D. variabilis, 333, 340-341, 355-356
Dermanyssus gallinae, 236Dermaptera, 154 See also EarwigsDermatitis. See also specific manifestations,
symptomsadult moth exposure (lepidopterism), 57, 291-
294blister beetle exposure, 56-57caterpillar exposure, 57, 137-143chigger bites, 230mites and, 234possible causes, 100
Dermatobia hominis, 196Dermatophagoides,
D. farinae, 232-233D. pteronyssinus, 232-233
Dermestidae, 22-23, 25Diarrhea,
ingested larvae and, 25digestive tract, larvae in, 22-25possible causes, 100
Diapause, 265Diphenhydramine hydrochloride, 16-18Diphylidium caninum, 157Diplopoda, 85-86. See also MillipedesDirect effects, 4. See also Bites; Myiasis; StingsDirofilaria, 256-257
D. immitis, 256D. tenuis, 257D. repens, 257
Disease vectorsAfrican sleeping sickness, 180American babesiosis, 319bartonellosis (Carrion’s disease), 170boutonneuse fever, 328Chagas’ disease, 130cockroaches, 149-150Colorado tick fever, 328Crimean-Congo hemorrhagic fever, 328dengue fever, 253-255dysentery, 186ehrlichiosis, 328encephalitis (mosquito-borne), 258-262encephalitis (tick-borne), 328loiasis, 166malaria, 250-251mosquitoes, 250-252onchocerciasis, 164pinkeye, 190plague, 156relapsing fever, 328rickettsialpox, 232Rocky mountain spotted fever, 328sandfly fever, 171scrub typhus, 230Siberian tick typhus, 328Simbu group arboviruses, 169tapeworm, 157

433
Index
tick paralysis, 328ticks, 328-340trypanosomiasis, 130, 180tularemia, 166, 326typhus, 216West Nile virus, 258-260venereal diseases, 221yaws, 190yellow fever, 253-254
Dog fleas, 157Dog flies, 178Dog heartworm, 255-258Dog tapeworm, 157Dog ticks, 355, 360, 368Dolichovespula, 388-391
D. maculata, 389, 391Dopamine, 35-36Douglas fir tussock moth, 291-294Dried fruit dermatitis, 69Dried fruit mite, 69Dust mites, 232-233
allergies, 22-25, 232-233treatment/control, 233
E
Earsearwigs and, 154imaginary mites in, 69larval infestation, 202-203ticks in, 314
Earwigs, 154-155Eastern equine encephalitis (EEE), 258
mosquito vectors, 258Eastern yellowjacket, 388Echidnophaga gallinacea, 158Eczema,
mite-induced, 232Edema, typical sting effects, 14Eggs
flea, 160lice (nits), 218removal of, 220mosquito, 252-253
Ehrlichiosis, 328, 335Ehrlichia chaffeensis, 335
E. ewingii, 335E. phagocytophila, 335E. equi, 335
Elephantiasis, 101Emergency treatment for systemic reactions, 16-17Encephalitis, 258-262
California group, 260-262case history, 257, 261eastern equine, 258Japanese, 262LaCrosse, 260mosquito vectors, 258-262
Russian summer-spring, 339St. Louis, 258tick vectors, 339Venezuelan, 262West Nile, 258western equine, 260
Encephalitis mosquito, 277Entomological inspection, 73-74Entomological terminology, 79-80Entomophobia, 67-68Eosinophil chemotactic factor (ECF), 6Eosinophilia, 101Eosinophilia cerebrospinal fluid pleocytosis, 101Epicauta
E. fabricii, 122E. vittata, 122
Epidemic typhus, 216Epididymitis, 101Epinephrine, 16-18Eristalis tenax, 62, 208-209Erucism, 57Erythema migrans (or erythema chronicum
migrans), 330Eschar, 101European castor-bean tick, 380European earwig, 154European hornet, 391European house dust mite, 232Eutrombicula
E. alfreddugesi, 231E. sarcina, 231
Excoriation, neurotic, 70, 100tarantula hairs, 324
Eye gnats, 184Eye pathology
caterpillar exposure, 58eye gnats and, 190millipede exposure, 227moth-associated conjunctivitis, 292
Eyebrow or eyelash infestations, lice, 221
F
Face, bites on, 52-54Facultative myiasis, 63-64Fannia, 62, 208-209
F. canicularis, 202-204F. scalaris, 202-204
Fascicle, 40-42Fat-tailed scorpion, 306Fc receptor, 6Feet, bites on, 52-54Fever symptoms, 95, 250-263
from mosquito-borne diseases, 250-263Fiddleback spider, 310-314Filariasis, 254
mosquito vectors, 254Filth flies, 186-189. See also Blow flies

434
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
control of, 189description, 186disease transmission, 186larvae, 187life history and behavior, 188-189mouthparts, 40-42myiasis, 205
Fingers, bites between, 52-54Fire ants, 108-110
aggressive behavior, 108biology/behavior, 110geographic distribution, 109hypersensitivity, 12-13, 108nests and colonies, 110, 113queens, 110red and black forms, 109stings, 108incidence, 12-13lesions, 30-31, 108reactions, 30treatment, 110venom, 37venom immunotherapy, 18-19
Firebrats, 91Flannel moth, 138-142Flea(s), 155-161
biology and behavior, 160bites, 47. See Flea bitesburrowing, 158cat and dog, 157chigoe, 158control, 160disease transmission, 155-156eggs and larvae, 160-161geographic distribution, 160head morphology, 160human, 158method of blood feeding, 40mouthparts, 40-42northern rat, 158oriental rat, 157removal of, 160sand, 159species, 155-161sticktight, 158treatment of bites, 161
Flea bites,lesion patterns, 52-54, 156locations, 52-54mysterious bites and, 69number of lesions, 52-54skin reaction, 156treatment, 161
Flea collars, 409, 412Flesh flies, 186-189
biology/behavior, 188description, 186-187larvae, 187
Fliesbites, see Fly bites biting; Black flies; Deer
flies; Horse flies; Midges; Stable flies;Black flies
causing myiasis, 196-214. See also underMyiasis
deer flies, 166disease transmission, 164, 166, 171, 180horse flies, 168method of blood feeding, 40mouthparts, 40-42nonbiting, 186-193. See also Filth flies; House
fliesSpanish fly, 122. See Blister beetles species
namesFloodwater mosquitoes, 252, 264-265Flour mites, 239Fly larvae, see also Myiasis
biting midges, 170black fly, 165blow flies, 187causing myiasis, 196-214Congo floor maggot, 2019Cuterebra (animal bot fly), 205human bot fly, 196occasional, facultative species, 205, 208-209posterior spiracles, 211sarcophagids (Wohlfahrtia) flies, 204screwworm flies, 198in urinary tract, 203, 208-209
Flying teeth, 169Follicle mite, 245-246Food contamination,
beetle larvae, 25cockroaches, 25filth flies, 186fly larvae, accidental enteric, 60Indian meal moths, 24prevention, 25-26
Forcipomyia (Lasiohelea) taiwana, 170Formicidae, 108-114. See also Ant(s)Foundress, 395Furuncular myiasis, 196, 202, 204-205
G
Gangrenous spot, 312Genital lesions, 52-54German cockroach, 150-152German yellowjacket, 389Glossina, 180-183. See also Tsetse flies
G. fuscipes, 180G. morsitans, 182G. pallidipes, 182G. palpalis, 180G. swynnertoni, 182G. tachinoides, 180

435
Index
Glucose-6-phosphate dehydrogenase (G6PD)deficiency, 313
Gnathosoma, 43-44Gnats biting, 169. See also Black flies; Biting
midgesGolubatz fly, 164Grain mites, 239Gray Caucasian honey bee, 116Green flies, 186-189, 205Green nimiti midge, 22-25Grocer’s itch, 239Grocer’s itch mite, 239Ground scorpions, 307G6PD deficiency, 313Guard bees, 116Gulf coast tick, 353-354Gypsy moth, 137-142
H
Hadrurus, 301Haemaphysalis
H. concinna, 367-368H. leachi, 368-369H. leachi mubsami, 368H. spinigera, 370-371
Hair follicle mites, 245-246Ham mite, 239-240Hand
bites on, 52-54scabies infestation of, 241
Hard ticks, 341-346diagnostic characters, 348
Harvester ants, 110-113biology/behavior, 111description and geographic distribution, 111lymphatic system reactions, 111nests, 111treatment of stings, 111venom components, 35-37
Harvestmen, 84Hastisetae, 22Head lice, 218-221
description, 218lesion patterns, 52-54life cycle, 218-219nits, 218treatment, 220
Hematemesis, 101Hematuria, 311Hemileuca, 142Hemoglobinuria, 101Heparin, 6Hermetia illucens, 62, 208-209Hexapoda, characteristics of, 81Hippelates, 190Histamine,
bee sting-induced overdosage, 4, 14-15
in caterpillars, 58in venom, 35-37
HIV, 251Hives, 101Honey bee, 116-117
Africanized (“killer”), 117Caucasian races, 116Gold Italian race, 116
nests, 117venom cross-reactivity, 15
Honey bee stingsmortality, 15stinger, 116removal, 117treatment of, 14-15venom constituents, 35-37
Hornetsbaldfaced, 388venom, 35-37
Horse flies, 168-169bites, 168-169
lesion patterns, 52-54systemic reactions, 14treatment, 169
method of blood feeding, 40mouthparts, 40-42, 168number of lesions, 52-54
Hourglass marking, 314, 320Hourglass spider, 314House dust allergy, 22-25, 232-233House dust mite, 232-233
allergy, 22-25, 232-233immunotherapy, 22, 233management and treatment, 22-25, 232-233
House flies, 186-189. See also Filth fliesbiology/behavior, 188control of, 189description, 186larvae, 187
House mouse mite, 236Human bot flies, 196-198
geographic distribution, 197life history and behavior, 197treatment, 197-198
Human flea, 158Human follicle mite, 245Human granulocytic ehrlichiosis, 328Human immunodeficiency virus (HIV), 251Human itch mite, 241 See Scabies mitesHundred leggers, 145-148. See also CentipedesHyalomma, 371-374
H. analoticum, 372H. asiaticum, 371H. marginatum, 373
Hydrocele, 101Hylesia, 292Hymenoptera, see also Ant(s); Bee(s); Wasps
Fire ant venom cross-reactivity, 15

436
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Sting-associated fatalities, 15Hyperpigmentation, 54Hypersensitivity reactions, 7-8, 12-18. See also
Allergic reactionsbiochemical mediators involved in, 5-7delayed (late), 8histamine involvement, 6IgE responses, 6immediate, 5local, 7mosquito bites, 47pharmacological mediators, 5-7respiratory, insect inhalant allergy, 22-25systemic, 14-15 See also Systemic reactionstick bites, 14, 351-352, 378treatment principles, 8
Hypotension, 15management, 16-17
Hypoxia, 16
I
Identification of arthropods, 79-97centipedes and millipedes, 85insects, 81keys, 87larval morphology, 83morphology review, 80-87mites and ticks, 85scorpions, 85spiders, 82naming principles, 79-80outside help, 80questions to ask, 96
IgE responses, 6Imaginary arthropods, 67-74. See also Delusions of
parasitosisImmediate hypersensitivity, 5Immunoglobulin E (IgE) response, 6Immunotherapy, 18-19Imported fire ants (IFA), 108-110. See also Fire
antsvenom constituents, 37
Indian meal moth, 24Indirect effects, 4. See also Allergic reactionsInflammation, 4
histamine and, 4Insect repellents, 400-404
dangers from use, 404DEET products, 400natural repellents, 401permethrin (Permanone), 402plant derived substances, 401
Institutional settingspreventing myiasis (fly infestations), 63-64scabies infestations, 244
International Commission on zoologicalNomenclature, 80
Invalid infestationsmyiasis, 63scabies, 244
I0 moth caterpillar, 138-143Itching, differential diagnosis, 234, 241Ixodes
I. dammini, 358I. granulatus, 331I. holocyclus, 378I. pacificus, 356-357I. persulcatus, 379I. ovatus, 331I. ricinus, 380I. scapularis, 358
Ixodidae, 341
J
Japanese encephalitis, 262Japanese spotted fever, 333Jigger, 158
K
Kala azar (visceral leishmaniasis), 173Kerititis, 101Killer bees, 117-118
biology and behavior, 118description, 118geographic distribution, 118treatment of stings, 118
Kinins, 36-37Kissing bugs, 129-133
allergic reactions, 14bites,129-130classification of, 129description and geographic distribution, 130-
131disease transmission, 130method of blood feeding, 130mouthparts, 40-42systemic reactions, 14
Kolumbtz flies, 164Kwell, 220, 224, 243Kyasanur Forest disease, 328
L
Labium, 40LaCrosse encephalitis (LAC), 260Laelaps echidnina, 236Lancets, 33-34Large local reactions, 7, 14-16
treatment, 16Late cutaneous allergic reactions, 7-8, 44Late hypersensitivity reactions, 7Latrodectism, 314-321Latrodectus, see also Widow spiders

437
Index
L. bishopi, 318L. geometricus, 318L. hesperus, 317L. mactans, 314-319. See also Black widow
spiderL. mactans cinctus, 318L. mactans hasselti, 318L. mactans menavodi, 318L. mactans tredecimquttatus, 318L. variolus, 317, 320
Legs, bites on, 52-54Leishmania
L. braziliensis, 173L. chagasi, 173L. donovani, 171-173L. infantum, 173L. major, 173L. mexicana, 173L. tropica, 173
Leishmaniasis, 171-177Leiurus quinquestriatus, 305-306Lepidoptera, 291Lesions, see also Bites
arthropod bites,boil-like, 194, 202, 204,
Lethal dose, 4Leukocytosis, 101Leukopenia, 101Lice, 216-223
bites, 216, 217lesion patterns, 52-54locations, 52-54number of lesions, 52-54
body, 216. See also Body liceclothing or bedding treatments, 217, 220crab, 221 See also Pubic licecutaneous sequelae, 54delousing equipment, 217disease transmission, 216head, 218 See also Head licemysterious bites or dermatitis, 69nits or eggs, 218, 220removal of, 220pubic, 221. See also Pubic liceskin reactions, 46treatment, 220, 223
Lindane-based products, 220, 223, 244Liponyssoides sanguineus, 236Loa loa, 166Loiasis, 166Lone star tick, 351-352Loxosceles, 310-313. See also Violin spiders
L. arizonica, 311L. deserta, 311L. devia, 312L. laeta, 311-312L. rufescens, 311-312
Loxoscelism (systemic effects from brown reclusebites), 310-311
LutzomyiaL. anthophora, 177L. diabolica, 177L. longipalpis, 176L. olmeca, 176L. peruensis, 176L. trapidoi, 176L. verrucarum, 176L. ylephiletrix, 176
Lymantria dispar, 138Lymantriidae, 292Lyme disease, 329Lymph node pain, 137Lymphadenitis, 101Lymphangitis, 101Lymphocytosis, 101Lytta vesicatoria, 122
M
Maculae caruleae, 221Maggots, 81, 200-209. See also Fly larvae tissue
infestation by; MyiasisMalaria, 250, 254
mosquito vectors, 252, 273, 279-284Malaria mosquito, 273Malayan filariasis, 254Mange mites, 241. See Scabies mitesMansonia
M. annulifera, 288Mast cells, 6Mayflies, 22-25MCD peptide, 35Meat tenderizer, (for use on stings), 15Medic-Alert, 18Megabombus, 118Megalopyge, 137-143
M. opercularis, 138Megaselia
M. scalaris, 208-210Melittin, 35-38Meloe, 121-122Meloidae, 121-123. See also Blister beetlesMeningoencephalitis, 102Mesostigmata, 235Metamorphosis, 81-82Midges, 169, 191
avoidance and protection, 394bites, 47
lesion patterns, 52-54locations, 52-54number of lesions, 52-54
chironomid, 190-192description and geographic distribution,
191larvae, 191-192life history and behavior, 191respiratory allergens, 22-25

438
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Millipedes, 225-227characteristics, 225-226morphology, 85poisonous secretions, 225treatment, 227
Mitesallergens, 22-25, 232-233baker’s, 69bite locations, 52-54
number of lesions, 52-54bites, 49characteristics, 85cheyletiellids, 239chigger, 230-231clover, 238dermatitis from, 230-244disease vectors, 230dried fruit, 69flour, 239follicle, 245fowl, 235grain, 239grocer’s itch, 239ham, 239house dust, 232-233human biting species, 234-244humidity requirements, 233identifying characteristics, 85imaginary, 233. See also Delusions
of parasitosislife history, 234-235management and treatment, 231, 233, 243-244morphology, 85mouse, 236mouthparts, 43-44opportunistic infestations, 241rat, 235respiratory allergic reactions, 22-24, 232-233scabies, 241-244 See Scabies mitesstraw itch, 238workplace infestations, 74
Monomorium bicolor, 108Morphology, 80-87Mosquito bites
allergic reactions, 14-16, 47lesion patterns, 52-54number of lesions, 52-54secondary infection, 45transmission of fly larvae, 197
Mosquitoesartificial container/tree hole breeders, 264avoidance, 408biology and ecology, 263-265breeding sites, 265common U.S. species, 268-279description, 265-268disease transmission, 250-262
dengue fever, 253
encephalitis vectors, 258-262. See alsoEncephalitis
filariasis, 254HIV/AIDS virus, 251malaria vectors, 252, 273, 279-284West Nile vectors, 260yellow fever, 253
eggs, 264floodwater breeders, 265head and appendages, 266, 268larvae and pupae, 263-264life history, 263-264major foreign pest species, 279-289mouthparts, 40-42permanent water breeders, 264-265repellents, 400screening or netting, 408species characteristics (table), 252
Mothsexposure to hair or scales, 291-294
management/treatment, 294gypsy, 138-143larvae (caterpillars), 57-59. See also Urticating
caterpillars, 57lepidopterism, 291management/treatment, 294species with irritating hairs or scales, 291-294urticating setae, 57-58tussock, 292-294
Mouthpartspiercing-sucking, 40-43scissor-like, 43
Mule killers, 113-114Murine typhus, 156Musca
M. crassirostris, 211M. domestica, 186-187. See also House fliesM. sorbens, 211
Muscidae, 186Muscina stabulans, 208-209, 211Muscular spasm, 302Mutillid wasps, 113-114Myiasis
accidental, 62-63aural, 61, 208-209blow flies, 211-214Congo floor maggot, 201Cuterebra (animal bot fly), 205facultative, 63filth flies, 186-189furuncular or boil-like lesions, human bot fly,
196in invalids or elderly, 63locations on body, 208-209maggot removal, 197-198posterior spiracles of some offending larvae,
211prevention, 64

439
Index
rectal, 208sarcophagids (Woblfabrtia) flies, 204screwworm flies, 198-200species involved in, 208-209
occasional species, 205treatment, 64-65, 197, 200-201, 204-205, 213traumatic, 61Tumbo or Mango fly, 202urinary, 61, 196, 208-209
Myocarditis, 102Myrmecia, 106
N
Naming of arthropods, 79-80Narceus, 226Natural insect repellents, 401Neck, bites on, 52-54Necrosis, 102
recluse spider bites, 310-313treatment principles, 313
Necrotic venoms, 9Neotrombicula autumnalis, 231Netting, 408Neuritis, 102Neurotic excoriation, 70Neurotoxic venoms, 9, 314-321New World screwworm, 198-199Nits
head lice, 218removal of, 220pubic lice, 222
No-see-ums, 169Nodules, 49, 54, 102Northern fowl mite, 236Northern rat flea, 158Nosopsyllus fasciatus, 158Nursing homes, scabies infestations, 244Nutalliellidae, 341Nymphs, 81. See also Metamorphosis
O
Obligate myiasis, 63-64Ochlerotatus
O. dorsalis, 252O. melanimon, 252O. mitchellae, 252O. nigromaculis, 252O. solicitans, 252, 271O. taeniorhynchus, 252O. triseriatus, 252, 260O. trivittatus, 252
Off repellent, 400-401, 403-404Oil beetle, 122-123Old World screwworm, 198-199Omsk hemorrhagic fever, 374Onchocerca volvulus, 164
Onchocerciasis, 164Onchocercoma, 102Opiliones, 84Optic neuritis, 30Orchitis, 102Oriental cockroach, 150Oriental rat flea, 157Oriental sore, 171-173Ornithodoros
O. hermsi, 339, 348-349O. moubata, 361-362O. rudis (=Carios rudis), 362-363O. talaje (=Carios talaje), 363-364O. turicata, 350-351O. venezuelensis, 362
OrnitbonyssusO. bacoti, 233O. bursa, 233O. sylviarum, 234
Oropouche virus, 169Orthoptera, 149-151. See also CockroachesOtobius megnini (in human ear), 330-331Ovipositor, 33Oxygen therapy, 16
P
PaederusP. gemellus, 122P. limnophilus, 122
Painaxillary, caterpillar sting, 137centipede bite, 145lymph node, 137spider bite, 294tarantula bite, 308
Pandinus, 301Panstrongylus megistus, 131Papain, 15Paper mites, 74Paper wasps, 394-396Papular urticaria, 156Papules
biopsies of, 44-45black fly bites, 48differential diagnosis, 44-45, 48on genitalia, 52tarantula hair exposure, 324
ParabuthusP. transvaalensis, 305P. triradulatus, 305P. villosus, 305
Paralysis symptoms, 102, 340Parasitosis, delusory, 67-74. See Delusions of
parasitosisParavespula, 388-391
P. maculifrons, 388P. vulgaris, 388-389

440
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
Peanut brittle, 24Pediculicidal products, 217, 220, 223Pediculosis pubis, 223Pediculus
P. humanus capitis, 217. See also Head liceP. humanus corporis, 216. See also Body lice
Pedipalpi, 84Pellagra, 73Penis, papules on, 241Pentastomes, 297-299Periplaneta
P. americana, 150-152P. australasiae, 150P. brunnea, 150P. fuliginosa, 150-152
Permanone, 402Permethrin, 402Personal protection measures against arthropods,
408-414avoidance, 408bed nets, 408flea collars, 409insect repellents, 400-402screening, 408taping up, 408tucking pants legs, 408
PhaeniciaP. caeruleiviridis, 211P. cuprina, 208P. sericata, 208-213
Phlebotomus, 171-178P. argentipes, 176P. caucasicus, 176P. papatasi, 176-177P. pedifer, 176P. peruensis, 176
Phormia regina, 208-213Phospholipase A, 9, 36-38Phosphlipases, sphingomyelinase D, 9Phthiraptera, 94 See also LicePiercing-sucking mouthparts, 40-43Piloerection, 314Pimozide, 73Pinkeye, 190Piperidines, 37Plague, 156Plasmodium, 250, 254
P. falciparum, 250P. malariae, 250P. ovale, 250P. vivax, 250
Platelet activating factor (PAF), 6-7Pogonomyrmex, 110Poison sac, 33Po-ko-moo spider, 314Polistes, 394
P. annularis, 395P. aurifer, 395
P. carolina, 394P. exclamans, 394P. fuscatus, 395P. gallicus, 395P. jadwigae, 395P. perplexus, 394P. rubiginosa, 394P. smelleni, 395
Predaceous insect bites, 134Prionurus crassicauda, 306Proboscis, 40Prosimuliim mixtum, 164Prostigmata, 238-239Proteinuria, 102Protozoans, 250Pseudomyiasis, 62Psorophora, 252, 264-265, 267
P. columbiae, 252, 278-279P. discolor, 252
Pthiriasis, 221Pthirus pubis, 221-223. See also Pubic lice
Pubic lice, 221-223biology/behavior, 222bites, 221lesion patterns, 52-54locations, cutaneous sequelae, 54medical importance, 221sexual contact and, 221venereal diseases and, 221
Pulex irritans, 158Puncta, 102Pupae, mosquito, 263-264Purpuric spots, 54Puss caterpillar, 138-141. See also Urticating
caterpillarsPustular lesions, fire ant stings, 31Pyemotes tritici, 238Pyrobombus, 118
Q
Queensland tick typhus, 333-334Questing behavior, 342Quinones, 225
R
Rash, 102. See also Rocky Mountain spotted feverRat-tailed maggot, 62, 208-210Recluse spider, 310-313. See Brown recluse spiderRectal myiasis, 208-209Red bugs, 230-232Red bulldog ant, 108Red harvester ant, 111Red imported fire ant, 108-110Red mite of poultry, 236Reduviidae, 129. See also Assassin bugs;
Kissing bugs, 129-132

441
Index
Relapsing fever, 339louse vector, 216tick vectors, 339
Relapsing fever tick, 350-351Repellents
mosquito, 400-402tick, 403
Respiratory allergies, 22-25Respiratory distress, 16-17Respiratory failure, 7, 15, 16-17Rhinitis, 7, 21-25, 102, 232-233Rhipicephalus
R. appendiculatus, 381-382R. sanguineus, 360-361R. pumilio, 338
Rickettsia, 333R. conorii, 334R. prowazeki, 216
Rickettsialpox, 234Ringlegged earwig, 154River blindness, 164Roaches, 149-152 See CockroachesRocky Mountain spotted fever, 332-334Rocky Mountain wood tick, 354-355Romana’s sign, 102Ross River Disease, 262Russian summer-spring encephalitis, 339
S
Saddleback caterpillar, 137-143Salivary secretions, 5,14
hypersensitivity reactions, 14Salivation symptoms, 302Salt marsh mosquito, 271-272Sandfleas, 159Sand flies, 171-177
biology/behavior, 177bites, 171
locations, 52-54number of lesions, 52-54treatment of, 177
disease vectors, 171Sand fly fever, 171Sarcophaga, 187-188
S. citellivora, 211S. crassipaipis, 211S. haemorrhoidalis, 187, 211
Sarcophagidae, 187-188, 211myiasis, 208-209
Sarcoptes scabei mites, 241Scabicides, 243-245Scabies mites, 241-245
bites and lesions, 52-54, 241locations, 52-54, 241number of lesions, 52-54, 241patterns, 52-54, 241
burrows, 241
description and geographic distribution, 242in institutions or nursing homes, 244lindane-resistant, 244mouthparts, 43-44races (animal forms), 241sexual transmission, 242skin scraping, 243treatment, 243
Scissorlike mouthparts, 47Scolopendra, 145-146
S. cingulata, 146S. heros, 146S. polymorpha, 146
Scorpions, 301-308biology and behavior, 304characteristics, 302dangerous species (table), 305description, 302geographic distribution, 304medical importance, 301-302morphology, 83
Scorpion stingsstinger morphology, 303-304systemic reactions, 301-302treatment, 307venoms, 301-302
Screwworm flies, 198-200description and geographic distribution, 199life cycle and behavior, 199treatment, 200
Scrub typhus, 230Scutigera coleoptrata, 146Secondary infection, from bites, 45Seed tick, 352Serotonin, 35Serum sickness, 5Sexually-transmitted infestations
pubic (crab) lice, 221scabies, 241
Shampoos, pediculicidal, 217, 220, 222Shock, 5,7, 102. See also AnaphylaxisShoe button spider, 314Shuni virus, 169Siberian tick typhus, 328Sibine stimulae, 138Simbu group arboviruses, 169Simple metamorphosis, 81Simuliim, see also Black flies
S. colombaschense, 165S. damnosum, 165S. equinum, 165S. erythrocephalum, 165S. metallicum, 165S. neavi, 165S. ochraceum, 165S. ornatum, 165S. reptans, 165S. venustum, 164

442
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
S. vittatum, 164Siphonaptera, 155-161. See also Fleas(s)Skin lesions, see LesionsSkin manifestations, see specific typesSkin pigmentation
lice bites, 46, 54millipede secretions, 225
Skin samples submitted, 70-71Skin scrapings, 243Skin-So-Soft, 403Sleeping sickness, 180-182Small Anatolian hyalomma, 372Smoky brown cockroach, 150Soft ticks, 341-342
diagnostic characters, 347Solenophagy, 40Solenopsis
S. geminata, 108S. invicta, 108-110S. richteri, 108-110S. xyloni,108
Southern fire ant, 108-109Southern house mosquito, 275-276Spanish fly, 122. See also Blister beetles;
CantharidinSpicisetae, 25Spider(s),
characteristics, 82-84medical importance, 310morphology, 80mouthparts, 43-44urticarial hairs, 324
Spider bites, 310-323 See also specific spiderscase history, 319locations, 52-54necrotic, 310-313, 321-323lesions, 310-323venoms, 9, 310-323
neurotoxic venoms, 8-9, 314number of lesions, 52-54
tetanus risk considerations, 324treatment, 310, 313, 321-323, 325. See also
Treatment, bitesSpine removal, 59-60Spiny rat mite, 236Splenomegaly, 102Sponging mouthparts, 40Spotted fever tick, 353Stable flies, 178-180
biology and behavior, 179mouthparts, 43treatment of bites, 180
Staphylinidae, 121Sticktight flea, 158Stingers, 34-35
honey bee, 115-117morphology, 34-35removal, 117
scorpion, 288Stinging behavior, 31Sting kits, 18Stings, 29-38St. Louis encephalitis (SLE), 258Stomoxys calcitrans, 178-180. See also Stable fliesStraw itch mite, 238Striped blister beetle, 122Stylets, 40-42Sucking lice, 216-223Supella longipalpa, 150-151Syrphid fly larvae, 62, 208-210Systemic reactions, 16-18
bee stings, 15-17black fly bites, 164black widow bite, 314brown recluse spider bites, 310caterpillar stings, 137deer fly bites, 14horse fly bites, 14scorpion stings, 301-302
T
T-lymphocytes, 6Tabanidae, 166-169Tabanus
T. atratus, 168T. lineola, 168T. punctifer, 168T. similis, 168
Tachycardia, 102Taiga tick, 379-380Tan assassin bug, 131Tanytarsus lewisi, 22-25Tapeworm, 157Tarantula spiders, 324-325
treatment of bites, 325Taxonomic nomenclature, 79-80Tegenaria agrestis, 321-322. See also Hobo spiderTelmophagy, 40Termites, 90Tetanus prophylaxis, 325Theraphosidae, 324Thousand leggers, 225-227. See also MillipedesTick(s)
attachment to humans, 342biology/ecology, 341bites, 52-54, 342
cutaneous sequelae, 54locations, 52-54number of lesions, 52-54
characteristics, 346-348common U.S. species, 348-360diagnostic characters, 347-348disease vectors, 328, 329-341expansion capacity, 342-343field collection, 345

443
Index
habitats, 345-346hard (Ixodidae), 341humidity requirements, 344-345hypersensitivity reactions, 14, 356-357, 378larvae, 352morphology, 81mouthparts, 40-43Nuttalliellidae, 341personal protection measures, 408-409questing behavior, 342removal of, 413repellents, 403sexual dimorphism, 341soft (Argasidae), 341species outside of the U.S., 361
Tick-borne encephalitis, 339Tick paralysis, 340Tissue infestation, by fly larvae (maggots), see
MviasisTityus
T. bahiensis, 305T. cambridgei, 305T. serrulatus, 305-306T. transvaalensis, 306T. trinitatis, 305
Toes, flea infestation, 158Tree hole mosquitoes, 252, 260-261Trench fever, 216Triatoma
T. dimidiata, 131T. gerstaeckeri, 132-133T. infestans, 132-133T. protracta, 132-133T. rubida, 133T. rubrofasciata, 133T. sanguisuga, 132-133
Triatominae, 129-131Triatominae, classification of, 129Triatominae, distribution, 133Trombiculidae, 231Tropical fowl mite, 235Tropical rat mite, 235True bugs, 126-135. See also Assassin bugs; Bed
bugs; Kissing bugs; Wheel bugsTrypanosoma
T. cruzi, 130T. gambiense, 180T. rhodesiense, 180
Trypanosomiasis, 130, 180. See also Chagas’disease
Tsetse flies, 180-183description and geographic distribution, 182method of blood feeding, 40treatment of bites, 183trypanosomiasis vector, 180
Tularemia, 166, 337deer fly vector, 166tick vectors, 338
Tumblers, 264Tumbu fly, 202Tunga penetrans, 158Turkey gnats, 164Tussock moths, 291-294Typhus vectors, 155, 216
U
Ulcers, cutaneous, 103Uloboridae, 310Ultraviolet light traps, 189Urinary myiasis, 208-209Urticaria
adult moth exposure, 291-294setae, 58tarantula hair exposure, 324-325
Urticating caterpillars, 137-143biology/behavior, 141descriptions, 138eye lesions from, 137-138geographic distribution, 138-139species, 138-142spine removal, 142treatment and management, 142-143spine or hair removal, 142venom, 58
UV traps, 189
V
Vagabond’s syndrome, 216Vanillism, 239Vasculitis, 30Velvet ants, 113-114
treatment of stings, 114Venezuelan encephalitis (VEE), 262Venom, see also Bites; Stings
alkaloidal, 37allergens in, 5-7antivenins, 307, 313, 321, 323black widow, 321components, 35-37cross-reactivity, 15hypersensitivity reactions, 8necrotic, 9neurotoxic, 9scorpion, 9spider, 9wasp, bee, and hornet, 35-37
Venom immunotherapy, 18-19Venom skin tests, 19Vespa crabro, 391Vespula, 3388
V. squamosa, 3390Viente-cuatro hora hormiga, 108Violin-shaped marking, 312Violin spiders, 310-312 See also Brown recluse
spider

444
Physician’s Guide to Arthropods of Medical Importance, 4th Edition
biology/behavior, 312bites, 310description and geographic distribution, 312necrotic effects, 310treatment of bites, 313venoms, 9
Visceral leishmaniasis, 171-174
W
Warehouse beetle larvae, 23Wasps, see also Hornets; Yellowjackets
control and avoidance, 19-20nests, 19, 390-392paper wasps, 3394-396stinger morphology, 33-34
Wasp stingseffects, 28-29treatment, 15-18venom, 35-37
West Nile virus, 258Western black-legged tick, 356-357Western equine encephalitis (WEE), 260Western harvester ant, 111Wheel bugs, 134
bites, 134geographic distribution, 134
Wheezing symptoms, 18-19, 22-25White-marked tussock moth, 291-294Widow spiders, 314-321 See also Black widow
spiderantivenin, 3321bites, 314description, 317geographic distribution, 317habitats and life history, 318species, 314-315
Winterbottom’s sign, 105Wigglers, 263Wiggle tails, 263Wohlfahrtia
W. magnifica, 204-205W. vigil, 204-205
Workplace infestations, 74Wounds, larval infestation of, 61, 63. See also
MyiasisWucheria
W. bancrofti, 254W. malayi, 254
X
Xenopsylla cheopis, 157
Y
Yaws, 200Yellow dog tick, 368-369Yellow fever, 253Yellow fever mosquito, 252, 268-269. See also
Aedes aegyptiYellowjackets, 388-391
avoidance, 19-20description and geographic distribution, 388-
389treatment of stings, 391venom components, 32-34venom cross-reactivity, 15
Yersinia pestis, 156
Z
Zoonosis, obligate myiasis, 64