Embed Size (px)
Citation preview

1/20/2014
1
“Establishing realistic treatment objectives for adult patients”
Goals of presentation
I. Describe uniqueness of adult ortho patients
II. Clarify the meaning of “realistic treatment objectives” for 21st century orthodontics
III. Describe a standardized method of communication that helps patients and providers achieve their objectives
IV. Reduce risks of adverse legal action and at the same time enhance internal marketing
A few “warm-up” questions & a “do-it-yourself” survey:
1. In your experience please rate, in order of importance (1—being most important), which of the following most frequently limits the achievement of the treatment goals in adults patients?
( ) IDT teamwork failure of communication ( ) Pre-existing periodontal disease ( ) Cost of the Interdisciplinary treatment plan-- unable to be
completed ( ) Lack of patient compliance with treatment (missed appointments,
Oral Hygiene, lack of elastic wear, etc.) ( ) Underlying surgical skeletal imbalance and Orthognathic surgery is
denied by insur. or refused by pt. ( ) Patient treatment expectation beyond what is feasible ( ) Other_________________________________________
2. In your experience with adult IDT patients which of the following interdisciplinary treatments result in the least predictable outcomes?
a) Orthodontics and restorative
b) Orthodontics and Orthognathic surgery
c) Orthodontics and periodontics
d) Orthodontics, periodontics, & estorative
e) Orthodontics, periodontics, restorative and orthognathic surgery
f) Any combination of the above and TMJ symptoms
at treatment start
3. For your answer to question #2, what do you think is the most likely cause of outcome deficiency?
a) Lack of IDT teamwork among doctors
b) Lack of IDT teamwork among office staff and treatment coordinators
c) Frequency of unexpected complications
d) Lack of insurance coverage resulting in treatment compromises
e) Patient “burn-out” as they go through the treatment process
f) Other___________________________________
4. Which of the following technologic advances have allowed reduction in treatment limitations of your adult IDT patients?
a) Additional diagnostic information from 3-D cone beam
radiographic assessment b) The use of removable aligners (Invisalign, Clear Choice,
etc.) c) Utilization of TADS to provide more predictable anchorage
and control d) Utilization of methods of accelerated tooth movement
(Wilkodontics, Surg Facilitated Ortho Tx, etc.) e) IDT study club meetings in which each specialty is
represented f) Other, Please
list_____________________________________________
5. In your treatment of complex, IDT patients, what specific measures have you taken to minimize limitations of treatment outcomes?_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Survey answers from experienced orthodontist at end of presentation.

1/20/2014
2
Cases and concepts “Perio and too old for treatment”
Previous tx, but unhappy!
“Only way to treat is w jaw
surgery”
“25 and considering dentures”
“Two stage surgery? Cost
and coverage?”
Significant variation in adults challenges “adult label”
Adult orthodontic patients— 19-80 yrs. Age/social factors 1. 19-29 still in transition to independence
2. 30-39 pressure, pregnancy, stress, $$$, TMJ
3. 40-49 time for self; before it’s too late
4. 50-65 use insurance, prepare for retirement, other health issues— “stay younger longer”
5. 65-80 preserve and restore; role of implants!
Doctors/Staff/
IDT Team
Insurance/
Legal
System
Biologic System/Patient
Biologic System/Patient
Intrinsic factors
• Periodontal
• Skeletal
• Dental
• Neuromuscular
• Psychological
• Financial—2007—2014 and beyond
• Capacity to commit to tx duration & plan
10
Case #1--70 y old Female: What is her chief concern? What are her kids chief concern?
“Establishing realistic treatment objectives for adult patients”
Goals of presentation ”
I. Describe uniqueness of adult ortho patients
II. Clarify the meaning of “realistic treatment
objectives” for 21st century orthodontics

1/20/2014
3
What is your/your patient’s concept of acceptable treatment goals?
F unction (Optimal)
R2 eliable/Realistic
E2 sthetic/Economic
S2 tability/Satisfaction
H ealth--dental/physical/mental
Who determines which goal is prioritized? Examples
1. Is function more important than facial esthetics?
i. e. canine rise vs. flattened upper lip and
accelerated facial “aging?”
2. Is total cost of treatment a consideration—eg.
missing laterals—space opening or closure?
3. Surgical risks, costs, coverage and borderline
surgical cases?
4. Is it acceptable to push boundaries of stability to
achieve a more esthetic outcome?
Template guided diagnosis and treatment planning—Chapter 24
For adult orthodontic patients, realistic treatment objectives…..
1. …are determined through a thorough diagnostic process and thoughtful conversation;
2. …most important objectives are the primary treatment goals of the patient;
3. …are sensitive to the age of the patient and realizes that ideal goals that are possible may not be desirable;
4. …more that 75% of the time require interdisciplinary teamwork to achieve reliable outcomes.
16
Goals of presentation Establishing realistic treatment objectives for adult patients
I. Describe uniqueness of adult ortho patients
II. Clarify the meaning of “realistic treatment objectives” for 21st century orthodontics
III. Describe a method of communication that helps patients and providers achieve their objectives
8 Step Discipline® System of operation Framework for patient care Mechanism for providing consistency Internal marketing/External Marketing Medicolegal protection System in which all senior staff can be TC ‘s
1
2
3
4
5
6
7
8 Feedback review Initial Phone Contact
First Dr. meeting
Tx. Conference Rpt.
Progress Rpt.
Retention/Stabilization Rpt.
Completion Summary
Creating referrals

1/20/2014
4
The 8 Step Discipline Step 2: First Office Contact
Concept: Good “first impression” is essential.
Trust can be gained or lost during the telephone interview.
Check List: Will you…
4. Have mission statement reflected in the receptionist’s skills? Is the practice mission part of “shared vision” of doctors and staff?
5. Follow-up with welcome letter, brochure, etc.? Is your welcome genuine and shared by all of the staff?
The 8 Step Discipline Step 4: Tx Planning Conference/*Report
Concept: Presentation of plan with options and empathy is
critical. Try to provide a meaningful discretionary experience.
Check List: Will you…(Keep good practice stats.)
9. Review records? 10. Illustrate possible outcomes?
11. Review consent form? 12. Tx. Plan report to DDS & patient?
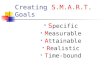
Adult Orthodontic Treatment (Ages 20 – 75)
Before After
Before After
Is there anything special about adult orthodontic treatment? Yes, the jaw structure of adults is no longer growing which limits correction of certain types of bite problems. Additionally, adults are more at risk for periodontal problems and adults have more missing and damaged teeth. However, adult orthodontic patients cooperate better than their adolescent counter-parts and as a result their time in orthodontic treatment is frequently shorter.
Interdisciplinary Treatment
Missing Posterior Teeth
Missing posterior teeth: Loss of molars and congentially absent posterior
teeth contribute to jaw “over closure” Jaw over closure is also called “bite collapse” and
can accelerate progressive tooth loss through incisor trauma which is secondary to over closure and to an anterior deep bite
The most predictable correction is accomplished through: o Reversal of the “bite collapse” with tooth
movement (orthodontic treatment) o Periodontal re-evaluation of tissue response o Reopen spaces in preparation for
restoration o Stabilization with tooth replacement—
implant if possible to preserve bone and to reduce crown preparation
Interdisciplinary dentofacial therapy (IDT): 80% of adult patients require dental teamwork: Tooth loss and wear allow dental migration Dental arch collapse requires “reversal” (uprighting)
through orthodontic treatment If adequate bone exists—implants will replace roots
and crowns will replace the top portion of the tooth Restored function, health and esthetics are
achieved Dentofacial “aging” is reversed
Musich & Busch DDS, Ltd. 2006 ©
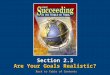
Surgical Orthodontic Treatment
Before After
Before After
Why is jaw surgery part of some orthodontic treatment plans? The “facial form” is part of a complex genetic interaction of teeth and bones. In about 15-20% of the adult patients who seek orthodontic correction, the
jaw structure needs to be corrected. Therefore, the combined treatment of orthodontics and orthognathic surgery is required to achieve an ideal bite.
Lower Jaw Excess
Severe Jaw / Chin Deficiency
Lower jaw excess with upper jaw deficiency: In this jaw imbalance, the lower jaw appears too
large to match the upper There is frequently an “underbite” and incisor
trauma There is frequently upper jaw width deficiency
and crowding Braces usually precede the jaw surgery by 12 to
18 months to prepare tooth position to match the planned surgical correction of the jaw relationship (see milestones)
Severe jaw and chin deficiency: This jaw growth imbalance, gives the
appearance of little or no chin The bite is characterized by a large overjet and
frequent upper and lower crowding “Late onset” lower jaw deficiency may be related
to degenerative joint disease Braces are needed to prepare the teeth for
appropriate surgical correction of the jaws Braces usually precede the jaw surgery by 12 to
18 months to prepare tooth position to match the planned surgical correction of the jaw relationship (see milestones)
Musich & Busch DDS, Ltd. 2006 © 22
Case #5: Skel Class III, spacing, impacted #11, perio, + attitude
The 8 Step Discipline Step 5: Progress Conference/ Report (JCO<10%)
Concept: Patients & parents are curious about progress and have questions. This conference gives you chance to inform, & build trust. Reduce risk management issues.
Check List: Will you… 13. Take a panoramic x-ray + other needed records (?) about two-
thirds of the way through treatment?
14. Send a Progress Report to the DDS (including x-ray) with a copy
to the patient/parent?
15. Have educational materials to help patients understand options such as implants, plasties, exposures, gingival grafts, Class III growth & jaw surgery, verify restorative plan and future steps.

1/20/2014
5
The 8 Step Discipline Step 6: Retention/Stabilization: Report-JCO<16%
Concept: Formal conference to review original
goals and the emphasize the importance of “after
care”(retention). Also, discuss case limitations.
Check List: Will you…
16. Have patients complete a questionnaire assessing
their orthodontic experience?
17. Provide the patient/parent with a post-treatment
report with a copy to their dentist?
18. Celebrate the patient’s accomplishment & provide
before and after photos?
Long-term fixed retainers are not without problems!
“Establishing realistic treatment objectives for adult patients”
Goals of presentation
Describe uniqueness of adult ortho patients
Clarify the meaning of “realistic treatment objectives” for
21st century orthodontics
Describe a standardized method of communication that
helps patients and providers achieve their objectives
IV. Reduce risks of adverse legal action while
enhancing internal marketing
10 important tips from medical/defense attorneys:
1. Be selective in taking on new patients (Step #1; #2; #3)
2. Good communication—informed consent & tx plan;
billing & finances (Step #2; #3; #4; #5: #6)
3. Document good care provided & comm w other providers (#4;#5:#6)
4. ALWAYS document informed pt refusals in detail
5. Do not allow patients to dictate care
1.

1/20/2014
6
10 important tips from medical/defense attorneys:
(continued)
6. Do not criticize the care of another provider to the patient
7. Have a good system of standardized practices for tx plan,
progress repts, emergency, reminders, etc. (All of 8 Step)
8. Acknowledge limitations to your expertise; refer to others when needed.
9. Treat staff and relatives in same manner as all other pts. T
10. Maintain a team approach and good working relationship w other providers (#1, #2, #3—plus study club effort)
32
Case #5: Skel Class III, spacing, impacted #11, perio, + attitude
Note relative stability in 15 year follow-up
Achieving Objectives: Successes or Failures?
“…more logical to categorize patients as ‘responders (R) or non-responders (NR).’”
In addition, post-treatment relapse patients should be categorized as “adapters (A) and non-adapters (NA).”
Bell shaped curve—most favorable A and R at one end and most unfavorable NR and NA at the other end of a normal distribution curve. Ackerman, JL
34
Variables that made this person a non-responder-
smoker, perio disease susceptibility, poor mechanics, no progress rpt Outcome: • All upper incisors were extracted • Implants needed to replace • $350,000 insurance settlement • License suspended