Embed Size (px)
Citation preview
·:{iC0Fp'16ACOFP 53rd Annual Convention & Scientific Seminars
Goal Setting in Advanced Illness
Marianne Holler, DO
3/17/2016
1
Goal Setting in Advanced Illnesses: The “How to” of Having Difficult Conversations
Marianne M Holler, DO, FACOIMedical Director Hospice and Palliative Programs
VNA Health Group, Red Bank, NJ
Purpose
• To provide tools for discussing goal setting with patients and their families in the face of advanced illnesses
Objectives
• Identify the two most important questions to ask when assisting patients in setting goals in the face of advanced illness
• Describe two things that patients with serious illnesses want
3/17/2016
2
Thoughts for the Day
• “I learned a lot of things in medical school, but mortality wasn’t one of them.”
• Physicians view death less as a human norm and more as a medical defeat.
• “The way we saw it, and the way our professors saw it, the purpose of medical schooling was to teach how to save lives, not how to tend to patient’s demise” Gawande 2014
History Lesson
• 1914 People died at home surrounded by loved ones and supported by the family physician
• Society pitied those who had to die in an institution (hospital or nursing home) surrounded by strangers
• It was thought those individuals lacked family and loved ones who truly cared about them
Dying at Home Historically a good death

3/17/2016
3
History Lesson
• 2014 People now die in institutions despite many studies showing that most individuals prefer to die at home peacefully
• If you die at home there is an underlying cultural sentiment: “Didn’t you want everything done for your mother?”
So What Happened?
• “It is time to contemplate the unintended consequences of medical technology’s frighteningly successful war on natural death and its banishment of the “Good Death” our ancestors so prized”Butler 2013
3/17/2016
4
More History
• 25% of Medicare’s $560 billion budget is spent in annual outlays covers medical care in the last year of life! (Roughly $140 billion)
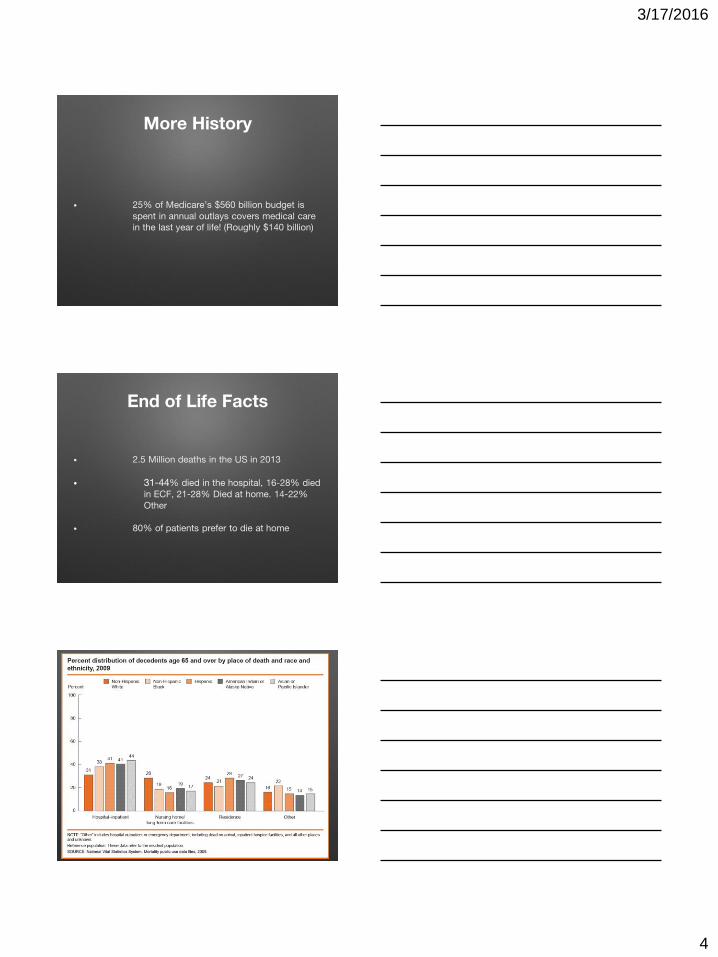
End of Life Facts
• 2.5 Million deaths in the US in 2013
• 31-44% died in the hospital, 16-28% died in ECF, 21-28% Died at home. 14-22% Other
• 80% of patients prefer to die at home
3/17/2016
5
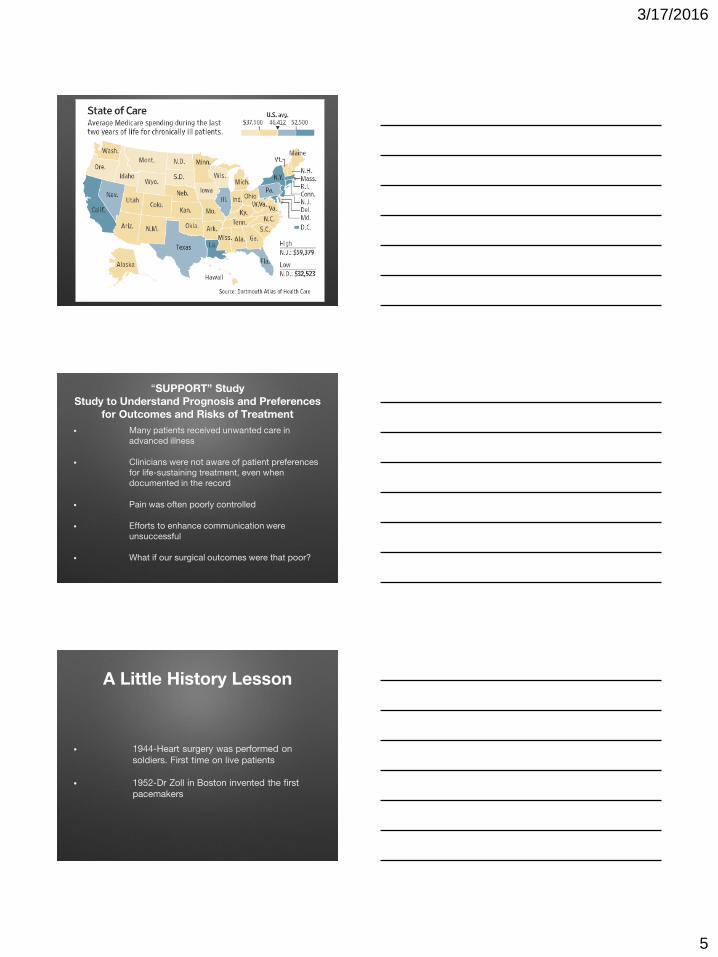
“SUPPORT” StudyStudy to Understand Prognosis and Preferences
for Outcomes and Risks of Treatment
• Many patients received unwanted care in advanced illness
• Clinicians were not aware of patient preferences for life-sustaining treatment, even when documented in the record
• Pain was often poorly controlled
• Efforts to enhance communication were unsuccessful
• What if our surgical outcomes were that poor?
A Little History Lesson
• 1944-Heart surgery was performed on soldiers. First time on live patients
• 1952-Dr Zoll in Boston invented the first pacemakers
3/17/2016
6
1953
• North Carolina Memorial Hospital in Chapel Hill established the first ICU
• Original ICU criteria admission excluded dying patients
• Many hospitals made the distinction between critical and terminal. It was also found to be important to guard against the admission of non-salvageable patients
ICUs
• An article by an administrator and a surgeon at Mary Hitchcock Hospital in New Hampshire stated “To maintain good morale among the nurses working in an ICU there must be some possibility of a successful outcome to crown their strenuous labors. Loading the unit with terminal cases is the best way to extinguish the optimistic spirit and drive so essential for good nursing care” Abel 2013
ICU Cont
• Primitive respirators based on the design of vacuum cleaners were used
• Dialysis was transformed from emergent to chronic care with implanted shunts
• the nations first “crash carts” were developed to hold all new equipment and meds that could be rushed to the bedside. (Designed after carts in sheet-metal and auto shops)
• CPR came into being around 1961 just as these units were blossoming
3/17/2016
7
1971
• The 911 system came into being on a national level
• Between ICUs, CPR and 911, lives of hardy people in their primes were saved who had suffered a heart attack, overdose, head-on collision, drowned, been stabbed, shot or accidentally poisoned.
• No doubt MIRACULOUS, no doubt important, no doubt transformative
A New Paradigm
Because a doctor CAN do something never means they SHOULDWe have learned so much about what to do no one is spending
time to discuss when we should and shouldn’t do
The Rise of the “Treatment Train” Berlin 2016
3/17/2016
8
Is it Me?
• ML 87yo F, Jan 2015
• Mild cognitive impairment, rectal bleeding. Found to have Met Rectal CA. Not a candidate for Tx. Diverting palliative colostomy performed and sent home with VNA
• Returns to ED July ’15 with “change in mental status”. Admitted to hospital, hospitalist places her on telemetry. Pauses are noted on the monitor, hospitalist consults Cardio. Cardio suggests pacer, family not sure. Cardio returns the next day, talks to family again and pacer is placed the following day.
Is it Me?
• Patient returns home. Readmitted 3 weeks later with infected pacer site.
• Palliative Care is consulted to discuss goals.
Is it Me?
• 88yo M. End stage Dementia. Bed bound, non verbal, total care, admitted to hospital with FTT. Record reveals four hospitalizations for Asp PNA this year alone. GI consulted to place feeding tube. GT is attempted and during scope GI malignancy is identified and GT cannot be placed. Surgery is then consulted to place J tube. Which is successful. Pt returns to the hospital 2 weeks later with infected stage IV sacral wound.
• Palliative Care is consulted to discuss goals of care.
3/17/2016
9
Is it Me?
• 59yo female, Stage 4 Ovarian Ca. Failed fourth line interventions and clinical trials. Now presents with bowel obs not a candidate for surgical intervention. Decompression G-Tube is placed for palliative reasons to prevent intractable N-V. Surgery is concerned the patient will have no nutrition and arranges for home TPN.
Is it me?
• 62 yo female found down in the field. Transported to ED in full arrest. Palliative Care is consulted on the day of admission. Review of medical records reveals 7 hospitalizations over the past 4 months and the following history:
• Stage 4 lung ca at dx 18 months ago, now on salvage chemo, cardiomyopathy with EF <10%, advanced O2 dependent COPD at the time of cancer dx.
• No family (well documented on previous admissions that there was no family)
• No documented conversations about goals or end of life care at office of Cardio, Heme/Onc, Pulm or PCP or on any of the previous admissions.
Why we do these things
• As practitioners we are taught HOW to do but not WHEN to use that HOW judiciously.
• It makes us feel better and more comfortable that we DID something.
• Realize that doing nothing in some situations is the best you can offer that particular patient and family.
3/17/2016
10
Treatment Train
• Who is the conductor? (Patient vs system vs Family vs doctor)
• What is the destination?
• When is it time to re-route?
Discussing Goals in Advanced Illness
• What are the two most important questions that must be asked to start theconversation?
QUESTION #1
• What is your understanding of what is happening with your (your family members) health at this time? (Ask, tell, ask)
3/17/2016
11
QUESTION #2
• Based on that information what is the GOAL? Now and if your health worsens?
More Questions
• What are your fears going forward with this illness?
• Patients often say to me “I want to live as long as I can”
Last Question
• What are the trade-offs you are willing to make and not willing to make?
3/17/2016
12
“REMAP” method for addressing goals of care
• 1) Reframe why the status quo isn’t working
• 2) Expect emotion and empathize
• 3) Map the future
• 4) Align with the patient’s values
• 5) Plan medical treatments that match the patient values
Reframe with the status quo is not working
• You may need to discuss serious news (scan results, bx results, echo, etc) first. Show them X-rays, scans, etc, visuals help)
• “Given this news, it seems like a good time to talk about what to do now”
• “We are in a different place”
Expect emotion and empathize
• “It’s hard to deal with all this”
• “I can see you are really concerned about….
• “Tell me more about that——what are you worried about?”
• “Is it ok for us to talk about what this means”
3/17/2016
13
Map the future
• “Given this situation, what’s the most important for you”
• When you think about the future, are there things you want to do?”
• As you think towards the future, what concerns you?”
Align with the patient’s values
• “ As I listen to you, it sounds the most important things are (xyz)
• Do not see “God is going to heal him” as a barrier but as an opportunity.
Plan medical treatments that match patient values
• Here’s what I can do now that will help you do those important things. What do you think about it?
3/17/2016
14
Expect questions about more treatment
• “Here are the benefits and burdens of what you are asking about”
• Overall, my experience tells me that (more chemo, surgery etc) would do more harm than good at this point”
• Everything in medicine comes with a benefit and burden. Only the patient/family can define that.
Talk about services that would help before introducing hospice• “We’ve talked about wanting to conserve your energy
for important things. One thing that can help us is having a nurse come to your house to help us adjust your medicines so you don’t have to come in to the office/hospital”
• “The best way I have to do that is to call hospice, because they can provide this service for us, and more”
• Do not feel that you are “hand-cuffing” a patient to a decision. People can change their mind, come off hospice, pursue a different direction if they choose.
Something to remember
• DYING IS A PROCESS
• DEATH IS AN EVENT
3/17/2016
15
Something to remember
• If we fail to understand and recognize the process we cannot prepare our patients and their families for the event.
When Caring for patients with
advanced illness remember:
“don’t just do something, stand
there”NY Times Editorial 9/2014
As much as we owe our patients the depth and the breadth of our skill and knowledge
We also owe them the chance for a peaceful and meaningful death
3/17/2016
16
References
• Butler, Katy: KNOCKING ON HEAVEN’S DOOR a path to a better way of death, 2013
• Abel, Emily; The Inevitable Hour: A History of Caring for Dying Patients in America
• Oxford Textbook of Palliative Medicine 4th Edition 2010
• Harrison’s Principles of Internal Medicine 18th Edition 2012
• Gawande, Atul: BEING MORTAL Medicine and What Matters in the End, 2014
• Health, United States, 2010 US Dept of Health and Human Services, CDC National Center for Health Statistics
• Dartmouth Atlas of Health Care 2015





