Embed Size (px)
Citation preview

Journal of the Neurological Sciences xxx (2013) xxx–xxx
JNS-12813; No of Pages 3
Contents lists available at ScienceDirect
Journal of the Neurological Sciences
j ourna l homepage: www.e lsev ie r .com/ locate / jns
Short communication
Glycine receptor and myelin oligodendrocyte glycoprotein antibodies in Turkishpatients with neuromyelitis optica
Mark Woodhall a,1, Arzu Çoban b,⁎,1, Patrick Waters a, Esme Ekizoğlu b, Murat Kürtüncü b, Erkingul Shugaiv b,Recai Türkoğlu c, Gulsen Akman-Demir b, Mefkure Eraksoy b, Angela Vincent a, Erdem Tüzün d
a Neuroimmunology Group, Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, University of Oxford, Oxford, UKb Department of Neurology, Istanbul Faculty of Medicine, Istanbul University, Istanbul, Turkeyc Department of Neurology, Haydarpasa Numune Education and Research Hospital, Istanbul, Turkeyd Department of Neuroscience, Institute for Experimental Medical Research (DETAE), Istanbul University, Istanbul, Turkey
⁎ Corresponding author at: Istanbul University, Istanbulof Neurology, Millet cad., Capa, 34390 Istanbul, Turkey. Te212 5334393.
E-mail address: [email protected] (A. Çoban1 Mark Woodhall and Arzu Çoban are equally contribut
0022-510X/$ – see front matter © 2013 Published by Elsehttp://dx.doi.org/10.1016/j.jns.2013.08.034
Please cite this article as: Woodhall M, et aneuromyelitis optica, J Neurol Sci (2013), ht
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 21 July 2013Accepted 27 August 2013Available online xxxxKeywords:Aquaporin-4Myelin oligodendrocyte glycoproteinGlycine receptorAntibodyNeuromyelitis opticaSera
Background: Seronegative NMO is highly prevalent in non-Western countries implying the presence of as yet un-known antibodies (Ab).We investigated potential novel Ab in aquaporin-4 Ab (AQP-4-Ab) positive and negativeNMO patients.Methods: Sera of 20 NMO patients were examined for AQP-4, myelin oligodendrocyte glycoprotein (MOG) andglycine receptor (GlyR) Ab by cell-based assays.Results: AQP-4-Ab was identified in 10 NMO patients, MOG-Ab was detected only in one AQP-4-Ab positivepatient andGlyR-Abwas detected in twoAQP-4-Ab negative patients. GlyR-Ab positive patients displayed simul-taneous optic neuritis and transverse myelitis attacks and relatively low disability, whereas MOG and AQP-4-Abdouble positive patient had a significantly increased disability.Conclusion: This study showed for the first time the presence of GlyR-Ab in Turkish NMO patients. In contrastwith previous reports, MOG Ab does not appear to be a distinctive marker for Turkish AQP-4-Ab negative
NMO patients.© 2013 Published by Elsevier B.V.
1. Introduction
Neuromyelitis optica (NMO)-IgG, a serum immunoglobulin autoan-tibody to aquaporin-4 (AQP-4-Ab), is a pathological effector in NMO. Al-though NMO IgG/AQP-4-Ab has been detected in more than 80% ofNMOpatients in severalWestern countries [1,2], in certain geographicalregions the prevalence of this antibody is less than 70% [3–5]. However,plasma exchange is useful in the treatment of seronegative NMO patients[6] and sera from seronegativeNMOpatients have been shown to activatethe complement system [7], indicating the presence of pathogenic anti-bodies. Furthermore, the lack of a significant difference between the clin-ical features of AQP-4-Ab positive and negative cases [4] has suggestedthat AQP-4-Ab is only one of many anti-neuronal antibodies causingNMO and there might be other unknown antibodies responsible forNMO pathogenesis.
Faculty of Medicine, Departmentl.: +90 212 4142000; fax: +90
).ing joint first authors.
vier B.V.
l, Glycine receptor and myeltp://dx.doi.org/10.1016/j.jns.2
Although myelin oligodendrocyte glycoprotein (MOG)-Ab are pre-dominantly found in pediatric patients with acute disseminated en-cephalomyelitis and multiple sclerosis [8,9], among NMO spectrumdisorders, MOG-Ab has been defined mostly in AQP-4-Ab negativeNMO, optic neuritis (ON) or transverse myelitis (TM) patients [10,11].Glycine receptor antibody (GlyR-Ab) has been shown in progressiveencephalomyelitis with rigidity and myoclonic jerks (PERM), a rareautoimmune disorder with brainstem and spinal cord involvementjust like NMO [12]. To examine whether antibodies to these spinalcord disease associated autoantigens could be involved in seronegativeNMO, we investigated MOG-Ab and GlyR-Ab in our NMO cohort.
2. Methods
2.1. Patients
Twenty (16 female, 4 male) consecutive NMO patients fulfillingWingerchuk's revised diagnostic criteria [1] were included. Clinicaland demographic characteristics of each patientwere collected. Patientsgave informed consent for inclusion in the study, which was approvedby the local medical research ethics committee. All sera were obtainedfor routine diagnostic purposes, immediately centrifuged, stored inaliquots at −70 °C. All sera were collected during an attack prior totreatment with steroids.
in oligodendrocyte glycoprotein antibodies in Turkish patients with013.08.034
2 M. Woodhall et al. / Journal of the Neurological Sciences xxx (2013) xxx–xxx
2.2. Antibody testing
Sera of all patients were examined by cell-based assays usingcultured HEK293 cells transfected with plasmids containing humanM23-AQP4, GlyR α1 subunit or MOG. The antibody binding was scoredvisually in a range from 0 (negative) to 4 (very strong), as in previousstudies [2,11–13].
3. Results
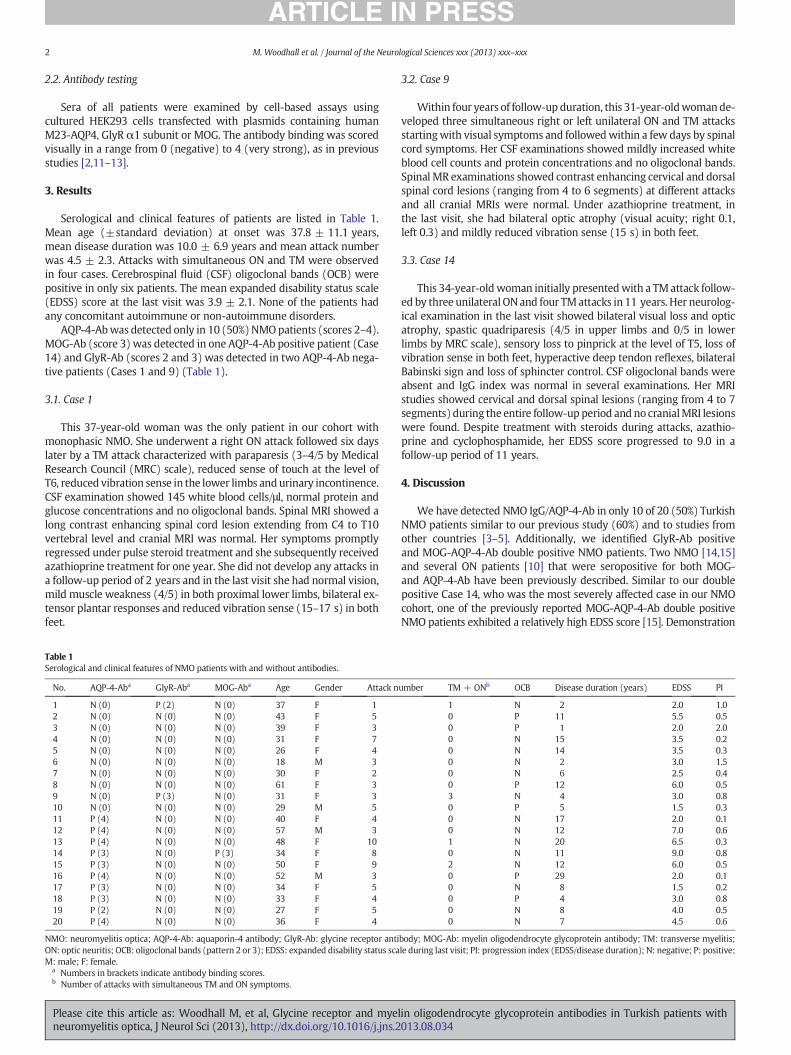
Serological and clinical features of patients are listed in Table 1.Mean age (±standard deviation) at onset was 37.8 ± 11.1 years,mean disease duration was 10.0 ± 6.9 years and mean attack numberwas 4.5 ± 2.3. Attacks with simultaneous ON and TM were observedin four cases. Cerebrospinal fluid (CSF) oligoclonal bands (OCB) werepositive in only six patients. The mean expanded disability status scale(EDSS) score at the last visit was 3.9 ± 2.1. None of the patients hadany concomitant autoimmune or non-autoimmune disorders.
AQP-4-Abwas detected only in 10 (50%)NMOpatients (scores 2–4).MOG-Ab (score 3) was detected in one AQP-4-Ab positive patient (Case14) and GlyR-Ab (scores 2 and 3) was detected in two AQP-4-Ab nega-tive patients (Cases 1 and 9) (Table 1).
3.1. Case 1
This 37-year-old woman was the only patient in our cohort withmonophasic NMO. She underwent a right ON attack followed six dayslater by a TM attack characterized with paraparesis (3–4/5 by MedicalResearch Council (MRC) scale), reduced sense of touch at the level ofT6, reduced vibration sense in the lower limbs andurinary incontinence.CSF examination showed 145 white blood cells/μl, normal protein andglucose concentrations and no oligoclonal bands. Spinal MRI showed along contrast enhancing spinal cord lesion extending from C4 to T10vertebral level and cranial MRI was normal. Her symptoms promptlyregressed under pulse steroid treatment and she subsequently receivedazathioprine treatment for one year. She did not develop any attacks ina follow-up period of 2 years and in the last visit she had normal vision,mild muscle weakness (4/5) in both proximal lower limbs, bilateral ex-tensor plantar responses and reduced vibration sense (15–17 s) in bothfeet.
Table 1Serological and clinical features of NMO patients with and without antibodies.
No. AQP-4-Aba GlyR-Aba MOG-Aba Age Gender Attack n
1 N (0) P (2) N (0) 37 F 12 N (0) N (0) N (0) 43 F 53 N (0) N (0) N (0) 39 F 34 N (0) N (0) N (0) 31 F 75 N (0) N (0) N (0) 26 F 46 N (0) N (0) N (0) 18 M 37 N (0) N (0) N (0) 30 F 28 N (0) N (0) N (0) 61 F 39 N (0) P (3) N (0) 31 F 310 N (0) N (0) N (0) 29 M 511 P (4) N (0) N (0) 40 F 412 P (4) N (0) N (0) 57 M 313 P (4) N (0) N (0) 48 F 1014 P (3) N (0) P (3) 34 F 815 P (3) N (0) N (0) 50 F 916 P (4) N (0) N (0) 52 M 317 P (3) N (0) N (0) 34 F 518 P (3) N (0) N (0) 33 F 419 P (2) N (0) N (0) 27 F 520 P (4) N (0) N (0) 36 F 4
NMO: neuromyelitis optica; AQP-4-Ab: aquaporin-4 antibody; GlyR-Ab: glycine receptor antiON: optic neuritis; OCB: oligoclonal bands (pattern 2 or 3); EDSS: expanded disability status scaM: male; F: female.
a Numbers in brackets indicate antibody binding scores.b Number of attacks with simultaneous TM and ON symptoms.
Please cite this article as: Woodhall M, et al, Glycine receptor and myeneuromyelitis optica, J Neurol Sci (2013), http://dx.doi.org/10.1016/j.jns.2
3.2. Case 9
Within four years of follow-up duration, this 31-year-oldwomande-veloped three simultaneous right or left unilateral ON and TM attacksstartingwith visual symptoms and followedwithin a few days by spinalcord symptoms. Her CSF examinations showed mildly increased whiteblood cell counts and protein concentrations and no oligoclonal bands.Spinal MR examinations showed contrast enhancing cervical and dorsalspinal cord lesions (ranging from 4 to 6 segments) at different attacksand all cranial MRIs were normal. Under azathioprine treatment, inthe last visit, she had bilateral optic atrophy (visual acuity; right 0.1,left 0.3) and mildly reduced vibration sense (15 s) in both feet.
3.3. Case 14
This 34-year-oldwoman initially presentedwith a TMattack follow-ed by three unilateral ONand four TMattacks in 11 years. Her neurolog-ical examination in the last visit showed bilateral visual loss and opticatrophy, spastic quadriparesis (4/5 in upper limbs and 0/5 in lowerlimbs by MRC scale), sensory loss to pinprick at the level of T5, loss ofvibration sense in both feet, hyperactive deep tendon reflexes, bilateralBabinski sign and loss of sphincter control. CSF oligoclonal bands wereabsent and IgG index was normal in several examinations. Her MRIstudies showed cervical and dorsal spinal lesions (ranging from 4 to 7segments) during the entire follow-up period and no cranialMRI lesionswere found. Despite treatment with steroids during attacks, azathio-prine and cyclophosphamide, her EDSS score progressed to 9.0 in afollow-up period of 11 years.
4. Discussion
We have detected NMO IgG/AQP-4-Ab in only 10 of 20 (50%) TurkishNMO patients similar to our previous study (60%) and to studies fromother countries [3–5]. Additionally, we identified GlyR-Ab positiveand MOG-AQP-4-Ab double positive NMO patients. Two NMO [14,15]and several ON patients [10] that were seropositive for both MOG-and AQP-4-Ab have been previously described. Similar to our doublepositive Case 14, who was the most severely affected case in our NMOcohort, one of the previously reported MOG-AQP-4-Ab double positiveNMO patients exhibited a relatively high EDSS score [15]. Demonstration
umber TM + ONb OCB Disease duration (years) EDSS PI
1 N 2 2.0 1.00 P 11 5.5 0.50 P 1 2.0 2.00 N 15 3.5 0.20 N 14 3.5 0.30 N 2 3.0 1.50 N 6 2.5 0.40 P 12 6.0 0.53 N 4 3.0 0.80 P 5 1.5 0.30 N 17 2.0 0.10 N 12 7.0 0.61 N 20 6.5 0.30 N 11 9.0 0.82 N 12 6.0 0.50 P 29 2.0 0.10 N 8 1.5 0.20 P 4 3.0 0.80 N 8 4.0 0.50 N 7 4.5 0.6
body; MOG-Ab: myelin oligodendrocyte glycoprotein antibody; TM: transverse myelitis;le during last visit; PI: progression index (EDSS/disease duration); N: negative; P: positive;
lin oligodendrocyte glycoprotein antibodies in Turkish patients with013.08.034

3M. Woodhall et al. / Journal of the Neurological Sciences xxx (2013) xxx–xxx
of MOG-Ab in patients with higher disability might suggest thatthese antibodies develop as a result of increased release of myelinproteins into the circulation due to accumulating myelin destructionin the advanced stages of the disease. Moreover, in contrast with pre-vious studies conducted inWestern countries [11,14], MOG antibodycould not be identified in any of the AQP-4-Ab negative patients.
In a previous study [10], MOG-Ab has been reported in 6 of 23 pa-tients (26%) with AQP-4-Ab positive ON. Similar to our Case 14, thesedouble positive patients gave poor response to immunotherapy,whereas in the MOG-Ab negative group, visual acuity improvedsignificantly. Overall, these findings suggest that MOG-AQP-4-Abdouble seropositivity might be a marker of a dismal outcome inNMO and NMO spectrum disorders. In contrast, in another study, 4AQP-4-Ab negative NMO/NMO spectrum disorder patients withMOG-Ab have been reported to give good response to immunother-apy and have a more favorable clinical outcome as compared to AQP-4-Ab positive patients [11]. A limitation of the study by Kezuka et al.[10] was that MOG-Ab was measured by an ELISA method usingrecombinant MOG produced in bacteria. Our study utilizing a cellbased assay for MOG-Ab detection substantiates the notion that innon-Western countries MOG-Ab positivity might have differentprognostic implications indicating an immunogenetic backgroundinfluence on MOG immunity.
Presence of serum antibodies to GlyR, which is abundantlyexpressed in the spinal cord [16], suggests possible involvement ofthese antibodies in NMO pathogenesis. Moreover, a GlyR-Ab positivepatient with steroid-responsive vision loss, optic atrophy and inflam-matory CSF findings has been recently described [17], corroboratingthe link between GlyR-Ab and NMO spectrum disorders. The onlydistinguishing clinical feature of GlyR-Ab positive patients was that inevery attack they had presentedwith simultaneous ON andTMfindings.Notably one of the GlyR-Ab positive patients had a monophasic diseasecourse. Also, the EDSS scores and attack numbers of these patientstended to be low and their disease durations were relatively shorter,suggesting that GlyR-Ab might be emerging in the earlier stages ofNMO and then disappearing during the disease course. Two additionalAQP-4-Ab single positive patients (Cases 13 and 15) also had displayedsimultaneous ON and TM attacks during their clinical course. Therefore,whether these clinical associations are genuine or simply coincidental,the exact frequency of Gly-R-Ab positivity in NMO and NMO spectrumdisorders andwhether this antibody can be used as a diagnostic markeras AQP-4-Ab remain to be clarified in future studies performed withlarger NMO cohorts.
Please cite this article as: Woodhall M, et al, Glycine receptor and myelneuromyelitis optica, J Neurol Sci (2013), http://dx.doi.org/10.1016/j.jns.2
Conflict of interest
The authors report no conflict of interest.
References
[1] Wingerchuck DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Reviseddiagnostic criteria for neuromyelitis optica. Neurology 2006;66:1485–9.
[2] Waters P, Jarius S, Littleton E, Leite MI, Jacob S, Gray B, et al. Aquaporin-4 antibodiesin neuromyelitis optica and longitudinally extensive transverse myelitis. ArchNeurol 2008;65:913–9.
[3] Cabrera-Go'mez JA, Bonnan M, Gonza'lez-Quevedo A, Saiz-Hinarejos A, Marignier R,Olindo S, et al. Neuromyelitis optica positive antibodies confer a worse course inrelapsing–neuromyelitis optica in Cuba and French West Indies. Mult Scler2009;15:828–33.
[4] Akman-Demir G, Tüzün E,Waters P, Içöz S, KürtüncüM, Jarius S, et al. Prognostic im-plications of aquaporin-4 antibody status in neuromyelitis optica patients. J Neurol2011;258:464–70.
[5] Yoshimura S, Isobe N, Matsushita T, Yonekawa T, Masaki K, Sato S, et al. South JapanMultiple Sclerosis Genetics Consortium. Distinct genetic and infectious profiles inJapanese neuromyelitis optica patients according to anti-aquaporin 4 antibody sta-tus. J Neurol Neurosurg Psychiatry 2013;84:29–34.
[6] Bonnan M, Valentino R, Olindo S, Mehdaoui H, Smadja D, Cabre P. Plasma exchangein severe spinal attacks associated with neuromyelitis optica spectrum disorder.Mult Scler 2009;15:487–92.
[7] Sabater L, Giralt A, Boronat A, Hankiewicz K, Blanco Y, Llufriu S, et al. Cytotoxic effectof neuromyelitis optica antibody (NMO-IgG) to astrocytes: an in vitro study. JNeuroimmunol 2009;215:31–5.
[8] O'Connor KC, McLaughlin KA, De Jager PL, Chitnis T, Bettelli E, Xu C, et al. Self-antigentetramers discriminate between myelin autoantibodies to native or denatured pro-tein. Nat Med 2007;13:211–7.
[9] Pröbstel AK, Dornmair K, Bittner R, Sperl P, Jenne D, Magalhaes S, et al. Antibodies toMOG are transient in childhood acute disseminated encephalomyelitis. Neurology2011;77:580–8.
[10] Kezuka T, Usui Y, Yamakawa N, Matsunaga Y, Matsuda R, MasudaM, et al. Relationshipbetween NMO-antibody and anti-MOG antibody in optic neuritis. J Neuroophthalmol2012;32:107–10.
[11] Kitley J, Woodhall M, Waters P, Leite MI, Devenney E, Craig J, et al. Myelin-oligodendrocyte glycoprotein antibodies in adults with a neuromyelitis optica phe-notype. Neurology 2012;79:1273–7.
[12] Hutchinson M, Waters P, McHugh J, Gorman G, O'Riordan S, Connolly S, et al. Pro-gressive encephalomyelitis, rigidity, and myoclonus: a novel glycine receptor anti-body. Neurology 2008;71:1291–2.
[13] LeiteMI, Jacob S, Viegas S, Cossins J, Clover L,Morgan BP, et al. IgG1 antibodies to ace-tylcholine receptors in ‘seronegative’ myasthenia gravis. Brain 2008;131:1940–52.
[14] Mader S, Gredler V, Schanda K, Rostasy K, Dujmovic I, Pfaller K, et al. Complementactivating antibodies to myelin oligodendrocyte glycoprotein in neuromyelitisoptica and related disorders. J Neuroinflammation 2011;8:184.
[15] Xu Y, Zhang Y, Ye J, Peng B, Wang JM, Cui LY. Successful treatment of a woman withrelapsing neuromyelitis optica by interferon beta. Neurol Sci 2012;33:911–3.
[16] Rajendra S, Lynch JW, Schofield PR. The glycine receptor. Pharmacol Ther1997;73:121–46.
[17] McKeon A, Martinez-Hernandez E, Lancaster E, Matsumoto JY, Harvey RJ, McEvoyKM, et al. Glycine receptor autoimmune spectrum with stiff-man syndrome pheno-type. JAMA Neurol 2013;70:44–50.
in oligodendrocyte glycoprotein antibodies in Turkish patients with013.08.034















![Myelin oligodendrocyte glycoprotein-specific antibodies from ......protein (MBP)] used to induce experimental autoimmune encephalomyelitis (EAE) in rodent models through induction](https://img.pdfslide.us/doc/110x75/60ff0b7639f1f130b4007123/myelin-oligodendrocyte-glycoprotein-specific-antibodies-from-protein-mbp.jpg)












