Embed Size (px)
Citation preview

Glycemic Index: The State of the Science, Part 1:
The Measure and Its Variability
PART1
51D Red Fox LaneRidgway, CO 81432
Phone: 970.626.9828Fax: 970.626.3686
www.wheatfoods.org

Glycemic Index: The State of the Science, Part 1:The Measure and Its Variability
Author: Julie M. Jones, Ph.D. Professor Emeritus St. Catherine University 4030 Valentine Ct. Arden Hills, MN 55112 Phone: 651-636-2275 Fax: 651-636-2394 email: [email protected]
Address for Reprints: Wheat Foods Council 19201 E. Mainstreet, Suite 103 Parker, CO 80134
Running Title: Glycemic Index: The Measure and Its Variability
Sources of Support: Wheat Foods Council
Short Biography of Author:
Julie Miller Jones, PhD, L.N., C.N.S., is a food science and nutrition professional with extensive academic experience as a faculty member, author of several books, speaker at many conferences nationally and internationally, scientific advisor to many groups including the Carbohydrate Committee of the International Life Sciences Institute, and a leader in scientific food and nutrition organizations.

2G
lyce
mic
In
de
x
AbstractThe carbohydrate (CHO) quality of food has recently been added to essential criteria used in selection of foods for the diet. The glycemic index (GI), and its cousin glycemic load (GL), are recommended by some as useful for this purpose. Others argue that these measures are too variable. Variability of the measures is caused by many food factors including the content and type of sugars, the proportion of the two starch moieties – amylose and amylopectin and whether the starch is raw or gelatinized, the kind and degree of cooking and processing, the presence of other ingredients and macronutrients, whether the food is eaten hot or cold or alone or with other foods. Characteristics of the person eating the food also affect the measure including: foods eaten a day or more prior to the test, the degree of chewing, and the speed of ingestion and whether glucose and insulin secretion are normal. For some, the measure is not clearly understood. Some think it compares equal amounts of food or equal amounts of CHO and fail to grasp that it compares 50g of available CHO from the test food compared with 50g of glucose. Thus, markedly different amounts of food are tested if foods are high in dietary fiber (unavailable CHO) or water. Further, the fact that labeled values may not relate to what is actually eaten makes use of the GI difficult for consumer and patient education. Finally, diets that are low GI or GL can be constructed in markedly different ways, making it seem quite reasonable that conclusions about such diverse diets on various health outcomes are often extremely variable.

Gly
cem
ic Ind
ex
3
IntroductionCarbohydrate (CHO) in foods, after languishing nearly a half century in the shadow of dietary fat, has emerged as one more factor to consider when deciding how much and which type of food to include in the diet. As is the case with fat, there is no universal agreement regarding either the optimal amount and type of CHO or the measurement of CHO quality.
Two proposed measures for assessing CHO quality are the glycemic index (GI) and its cousin–glycemic load (GL). These measures were suggested because scientific literature, albeit contradictory, associated high GI and GL diets with overweight, diabetes, coronary heart disease and other chronic diseases. Adherents promoted the use of this measure in a myriad of books and blogs. The American Diabetes Association (1), as part of its recent evidence-based review, suggested that GI might be useful adjunct to carbohydrate counting and other proven dietary strategies for those with diabetes. In contrast, opponents and the 2010 Dietary Guidelines Advisory Committee in their preliminary report express concern that the data are associational and contradictory. Many scientists question the use of these concepts for meal planning because of the lack of accuracy and precision of the measurement.
This is the first in a series of articles about GI and GL, and it will address the following: (1) definition and measurement; (2) variability caused by food parameters and by subjects and (3) problems associated with its use in mixed meals and (4) common misconceptions about the measure and its use. Thus, this background
will set the stage for the subsequent articles on the relationship of the GI and GL on various aspects of chronic disease. These future articles will deal with strengths and weaknesses of the science associating the GI and GL with (1) overweight, weight loss and cancer risk, (2) markers of inflammation, and glycemic control and diabetes, and (3) lipid profiles and attendant coronary disease risk.
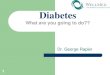
Carbohydrate, the Blood GlucoseResponse and the GIIt is well known that various CHOs cause different blood glucose responses. Nutrition doctrine for much of the last century espoused that simple CHOs delivered glucose to the bloodstream rapidly with a sharp rise followed by a steep drop. In contrast, complex CHOs delivered blood glucose slowly and steadily with neither a sharp peak nor a dramatic drop (Figure 1A). Despite inklings as early as the 1930s that this might be wrong, it was not until studies in the 1970s affirmed that some complex CHOs such as potatoes gave a blood glucose curve akin to those observed with simple sugars, and some simple CHOs such as fructose gave a blood glucose curve akin to those observed with complex CHOs (Figure 1B).
Figure 1A Old Paradigm of Glucose Response Curves - Pre 1970
Figure 1B Actual Glucose Response Curves
Sugars
StarchesLegumes
Fructose
PotatoGlucose
Time
Bloo
d G
luco
se
Bloo
d G
luco
se
Time
Legend Figure 1A Schematics of 2-hour Blood Glucose Curves representing the old paradigm of simple sugars causing a blood glucose peak and complex carbohydrates causing a more steady glucose.
Legend Figure 1B Schematics of 2-hour Blood Glucose Curves representing the old paradigm of blood glucose curve of potato (a complex carbohydrate) as similar to that of glucose. Further, there is a blood glucose curve for the simple sugar fructose causing a more steady glucose rise similar to complex carbohydrates.

4G
lyce
mic
In
de
x
In the 1980s, David Jenkins and colleagues developed the GI concept to compare the blood glucose response of various CHOs to a standard amount of glucose. Specifically, the 2-hour blood glucose excursion after ingesting 50g of available CHO from the test food (as measured by area under the curve (AUC)) was compared to that observed after ingesting 50g of glucose. The GI is the ratio of the two AUCs. The GI for 50g of glucose standard curve was arbitrarily assigned a value of 100.
Several points regarding GI and GL must be made. When the GI is measured, often the gram amounts of food are very different in order to reach required 50g of available CHO (Table 1). The GL was proposed to consider the gram amount of food. It is calculated by multiplying the amount of CHO in a given serving of food by the glycemic index of that same food and then dividing that number by 100. Table 2 shows a comparison of the GI and the GL and shows that some foods with a high GI have a low GI. The GL has also been applied to whole diets and foods eaten in combination.
Both concepts were developed for use in research. However, they have made their way from the laboratory to popular press. Their use outside of research has created much controversy because of the variability, both of the measure itself and of the results from studies using it.
Variability of the MeasureDue to Aspects of the FoodProperties of food including carbohydrate and other macronutrient composition, biological variability due to species, variety and cultivar, and degree and method of processing all impact the GI of the food. Further the following impact the GI: (1) chemical properties and amount of the sugars and starch, (2) the proportion of amylose versus amylopectin in the starch, (3) the structure of the starch granule and the extent of crystallization of the starch chains in the granule, (4) whether the starch is raw or cooked and the degree of gelatinization, (5) the food matrix and physical structure, and (6) the presence of other macronutrients and ingredients in or eaten with the food.
Sugars and GI – The specific type and amount of sugars in a food impact the GI. For example, foods which are formulated with high amounts of glucose will have a high GI, while those with fructose, a low one. Foods with sucrose (table sugar) and high fructose corn syrup will have an intermediate GI because these sweeteners are approximately half glucose and half fructose.
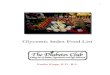
Starch, Amylose and Amylopectin and GI –
Starch, a large polymer of glucose, exists in two forms. In the amylose form, it is a long, straight
Table 1: Amount of Food to Yield 50g of Available CHO
Food Grams of Food for 50g CHO Amount of Food in Consumer Units
Glucose 50 ~ 4 TbspConverted rice, dry 61 1/3 cup dry (1 cup cooked)Russet potato, raw 317 1 large potatoWhole kernel corn 279 1¾ cup (cooked, drained)Enriched white bread 102 ~ 2¾ slicesWhole grain bread 120 ~ 4 slicesCarrots 896 ~ 7 cups, shredded raw or ~ 5 cups cookedWatermelon 636 4.5 cups
Data from Crapo et al i and USDA Tables of Food Composition

Gly
cem
ic Ind
ex
5
chain; while in the amylopectin form is highly branched with a structure similar to glycogen (Figure 2). Since the starch-digesting enzyme, amylase, attaches only to one end of starch molecule, the speed of glucose release from the two starch entities is dramatically different. From amylose, sugar units are split slowly from the lone end of the starch chain. However, from amylopectin with its numerous ends, many sugar units can be split off simultaneously. Hence, foods with a high proportion of amylopectin show a much more rapid rise in blood glucose and a higher GI than foods with a high proportion of amylose. For example, long grain basmati rice, naturally higher in amylose, has a lower GI than many other rices. (Table 3 gives some amylose and amylopectin contents of a sampling of foods.)
The sugar-starch balance changes with ripening - The GI of a food changes as the amount of sugar and starch changes as a food ripens. For instance, green bananas contain very few free sugars and much resistant starch (RS), hence they are low GI. Fully ripe ones contain many free sugars and little RS, hence they are high GI.
Starch granules and resistant starch - Starch granules in different species, varieties and cultivars have different structures, and this can affect the GI. Large granules usually have more surface area and more amylopectin, hence, a higher GI.
Starch that is tightly encased in the whole grain or embedded in the food matrix is shielded from action of the amylase. In fact, such starch may escape digestion in the small intestine and becomes RS type 1. This not only results in less available starch and a lower GI, it contributes dietary fiber.
Raw, cooked and cooled starch and the GI - Whether starch is eaten raw or cooked (gelatinized) has a large impact on GI. Uncooked starches, such as those in the raw oats of muesli, have a low GI because amylase does not readily attack it. In contrast,
Table 2: Comparison of GI and GL in a Sampling of Foods
Food GI Serving GL Shredded wheat cereal 69 30g 57.0Bagel 72 55g 38.4Cornflakes 84 30g 72.7Rice, brown 66 1 cup 23 Rice, white 83 1 cup 30Beets, boiled 64 ½ cup 6.3Bananas 53 1 small 12.1Sweet Potatoes 54 ½ cup 13.1Carrots 71 l large 7.2Watermelon 72 ½ cup 4
www.glycemicindex.com
Table 3: Amylose and Amylopectin Content of Common Starches
Starch Amylose % Amylopectin %
Corn 24 76Corn, waxy <1 99Corn, high amylose 70 30Potato and tapioca 20 80Wheat 22 88Barley starch 29 71Barley, waxy 2 98Barley, high amylose 45 55Rice, short grain 15-20 80-85Rice, medium grain 18-26 74-77Rice, long grain 23-26 74-77Pea 30 70
Adapted from Griswold, RM. The Experimental Study of Foods, p. 289 Houghton & Mifflin, New York.
Figure 2 A schematic of the branched chain structure of amylopectin

6G
lyce
mic
In
de
x
gelatinized starch is readily attacked by the amylase resulting in a higher GI than raw starches. Starch in food that has been heated and allowed to cool has a much lower GI than freshly gelatinized starches because starch chains line up and re-crystallize (retrograde) upon cooling (2, 3). The crystallized starch impedes amylase activity. Thus, a warm boiled potato has a much higher GI than the same potato eaten cold (Table 4) (4).
Physical structure and GI - A food’s physical structure impacts the GI. Dense, compact foods such as nuts, pasta, and legumes and viscous foods digest more slowly. This slows glucose release into the bloodstream and results in a lower GI. Such foods are sometimes described as delivering slowly available glucose or SAG (5). On the other hand, amylases can readily reach and rapidly break down the CHO in porous foods such as bread or in non-viscous liquids. The result is a rapid release of glucose into the bloodstream. The foods in this category are sometimes referred to as delivering rapidly available glucose or RAG (6). An example of the density effect is shown comparing the same dough baked into a bagel (traditionally baked at half-proof) and loaf of bread (fully proofed). The bagel has a lower GI than the bread (7).
Milling and processing and GI - Milling, particle size, grain type and intactness, processing, and fiber
type all affect the GI. Finely milled particles of many grains have higher GIs than intact or larger particles, since starch may be more available to the enzymes (8, 9). Instantizing of starches to make products that hydrate with hot or cold liquid markedly raises the GI. Puffing or popping of grains opens the grain structure and enables amylase access to the starch raising the GI (10).
Not all processes raise the GI. Extrusion can both lower and raise the GI, depending on the pressure and temperature of extrusion, the specific product and its resultant shape. Parboiling rice prior to removing bran in the manufacture of converted rice yields rice with a somewhat lower GI than regular rice. Toasting, freezing or defrosting, or toasting following freezing and defrosting, all lower the GI of bread products by promoting the re-crystallization of the starch chains (11).
Other macronutrients and ingredients and the GI - The macronutrient composition and the presence of other ingredients in the food affect the GI. Fat in food generally lowers the GI because it slows gastric emptying and impedes interaction of the CHO-digesting enzymes and their substrates. Thus, relatively high fat foods such as
Table 5: GI and Fat Content of Some Foods
Food GI Fat/svCarrots, raw 92 <1Rice crackers/cakes 77-80 1Whole wheat bread 75 1Mars Bar 65 9Oatmeal 58 2Potato chips 56 10Pound cake 54 6Snickers candy bar 40 14Chocolate cake and chocolate frosting 38 11Lentils 32 <1Fructose 15
GI values from www.glycemicindex.com Fat from USDA food composition data.
Table 4: GI of Selected US Potatoes and Cooking Methods
Potato type and cooking method GI Boiled red potatoes 89 Boiled red potatoes, eaten cold 56 Roasted California white potatoes 72Baked US Russet potatoes 77French fries 75Instant mashed potatoes 88
Adapted from Fernandes G, Velangi A, Wolever TM. Glycemic index of potatoes commonly consumed in North America. JADA. 2005;105:557-62

Gly
cem
ic Ind
ex
7
ice cream, candy bars and iced chocolate cake have fairly low GI values. French fries have a lower GI than boiled potatoes, due in part to the fat content (12). Table 5 gives selected foods their GI and their fat content. Fibers, especially viscous ones, thicken the gut’s unstirred layer. This slows amylase action and lowers GI. Protein stimulates insulin secretion and hastens glucose clearance from the bloodstream in both those with normal glucose tolerance and diabetics (13, 14). Addition or formation of acid (as in the sourdough process) lowers the GI of high GI foods (15).
Mixed meal effects on the GI – Eating a food as part of a mixed dish or meal changes the GI. For example, the addition of nuts can drop the GI of a food by as much as half. Toppings as diverse as cheese, chili con carne, baked beans or tuna on baked potatoes, pasta or toast lowered the GI of these foods (16). Such changes raise questions about the usefulness of GI for individual foods since most consumers eat foods in combination (17, 18). In fact, a recent review called into question the utility of GI and GL when used in the context of a usual diet (19). Table 6 shows that the GI of rice and Chinese steamed bread is lowered as other foods mix with the meal (20).
Proponents for the GI concept report that the relative rankings of GI remain the same in a mixed meal. Further, some data show that total CHO and GI explained approximately 90 percent of the variability in glucose and insulin response irrespective of calories, protein, or fat in a meal (21).
The Accuracy and Precisionof the GI Measurement Beyond, the variability caused by the food, the accuracy and precision of the method itself is the subject of much controversy. First, there is large within and among subject variation. Table 7 shows the GI with their standard deviations. In some cases these are so large as to make the assignment of foods into categories of low, medium and high GI both difficult and quite arbitrary.
Even in controlled settings with rigid dietary and other protocols, glycemic responses vary from day-to-day even in the same subject (22). Further, there exists a high degree of variability among subjects, even when the analyses are conducted by experienced laboratories (23). For example, triplicate analysis of the GI values for white bread compared to the 50g glucose standard in 23 adult subjects showed that there were marked differences on different days for the same subject. The coefficient of variation was 17.8% for inter-individual values, while the intra-individual variation was 42.8%. These data show that the day-to-day variation in the same subject is often greater than variation among subjects.
Factors that affect the variation among and within subjects – A number of factors affect the GI accounting for some of the variability observed. These include: the degree of mastication, quantity
Table 6: Changes in Glycemic Index as Foods are Added
Food Glycemic IndexRice 83.2Rice and stir-fry pork 72.0Rice and stir-fry pork and celery 57.1 Rice and stir-fry garlic sprout 57.9Rice and stir-fry garlic sprout and eggs 62.8 Steamed bread 80.1Steamed bread and butter 68.0Steamed bread and beef 49.4
Adapted from ref. 21
Table 7: Glycemic Index and Standard Deviations from Interlab Studies of GI GI ± std dev
White bread 72.5 ± 35.8Instant mashed potatoes 84.5 ± 32.7Long grain rice 71.1 ± 38.2White spaghetti 46.9 ± 26.7Pot barley 34.7 ± 24.7
Adapted from ref 22

8G
lyce
mic
In
de
x
of food ingested at any one time, the time period of eating and frequency of eating, the accompanying foods and foods eaten at prior meals and on prior days. For instance, inclusion of legumes or barley in the evening meal lowers the glycemic response at breakfast, the so-called ‘lente CHO’ effect. In like manner, low GI foods at breakfast lower the GI of a CHO food at lunch (24). Different mechanisms are thought to be involved. The decreased GI of foods eaten the morning after low GI food eaten the night before is attributed to the production of short chain fatty acids produced through colonic fermentation. Whereas, the lowered glycemic response 3-4 hours after a low GI meal is thought to be due to changes in free fatty acid concentration in the blood stream (25). The blood sugar and insulin status of the individual have tremendous impact on the measure. Thus, the GI measure itself is quite variable with its variability dependent not only on the properties of the food and its handling, but also on how it is eaten, what else is in the diet, and the glucose tolerance of the subjects eating it.
Misconceptions and Misuseof the GI and GLSome diet books and blogs fail to understand the concept of available CHO. Therefore, they suggest that the GI measure compares 50g of test food to 50g of glucose. This misunderstanding makes users of the GI concept unaware that higher gram amounts of the test food are needed if the food is either high in dietary fiber (unavailable CHO) or water as in watermelon or carrots. Table 1 shows the gram amount of some selected foods needed to reach 50g of available CHO. Note while white bread and whole wheat bread have relatively similar GIs, more whole wheat bread is eaten to reach the 50g of available CHO. Also note that large servings of foods such as carrots or watermelon are needed for the 50g of available CHO. These latter foods, while they have high GIs, have low GLs. Table 2 compares the GI and GL of selected foods.
GI is sometimes applied to the diet. This is also a misuse of the concept. GL is the appropriate

Gly
cem
ic Ind
ex
9
measure. However, critics of GL claim that it takes an imprecise measure, the GI, and amplifies the error by multiplying it by the grams of CHO.
GI and GL and Diet QualityCombinations of foods resulting in a low GI diet can create diets of markedly different nutritional quality. Diets can be high in fruits and vegetables, nuts, low-fat dairy, and can include lower GI options amongst carbohydrate containing foods. Alternately, they may have almost no carbohydrate foods, be high in meat saturated fats, include snacks such as bacon rinds and crustless cheesecake, and utilize low GI sweeteners such as agave. Thus, both the macro- and micro-nutrients and food groups included differ dramatically. Thus, when both diets are included in a study as low GI or GL, it is not surprising that the outcomes of studies with respect to associations with a certain health effect are frequently unclear or contradictory.
ConclusionsDetermination of the GI of a food, even in closely controlled laboratory conditions by experienced analysts, creates large standard deviations even for a single individual, so the measure’s precision and accuracy are subject to question. In like manner, determination of the dietary GI or GL from food frequency also has many potential sources of error. This is compounded by the fact that table values for GI may not accurately reflect what was eaten in terms of variety, cooking method, amounts and processing. Further, diet quality may vary markedly and still have the same low GI or GL score, making conclusions about the health effects of such diets inconsistent from study to study.
Proponents contend that, despite the variability, using the GI/GL concept is important in making diet selections, and that GI/GL should be controlled for both treatment and prevention of chronic diseases. Detractors contend that selection of foods only by using the GI could cause people to choose bacon rinds over watermelon or candy bars over carrots. Further, they argue that the measure’s variability makes its use valuable only in a laboratory setting and question the results when applied to food frequencies (26). Thus, they find little supporting evidence its use outside the laboratory or its use as a tool to help address key nutritional problems. Subsequent articles will address the state of the literature and the strength of the associations of GI and GL and chronic diseases.

10G
lyce
mic
In
de
x
References1. American Diabetes Association, Bantle JP, Wylie-Rosett J, Albright AL, Apovian CM, Clark NG, Franz MJ, Hoogwerf BJ, Lichtenstein AH, Mayer-Davis E, Mooradian AD, Wheeler ML. Nutrition recommendations and interventions for diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2008;31 Suppl 1:S61-78.
2. Björck I, Granfeldt Y, Liljeberg H, Tovar J, Asp NG. Food properties affecting the digestion and absorption of carbohydrates. Am J Clin Nutr. 1994;59(3 Suppl):699S-705S. 3. Jenkins DJ, Jenkins AL, Wolever TM, Collier GR, Rao AV, Thompson LU. Starchy foods and fiber: reduced rate of digestion and improved carbohydrate metabolism. Scand J Gastroenterol Suppl. 1987;129:132-41.
4. Fernandes G, Velangi A, Wolever TM. Glycemic index of potatoes commonly consumed in North America. J Am Diet Assoc. 2005;105:557-62.
5. Araya H, Pak N, Vera G, Alviña M. Digestion rate of legume carbohydrates and glycemic index of legume-based meals. Int J Food Sci Nutr. 2003;54:119-26.
6. Englyst KN, Englyst HN, Hudson GJ, Cole TJ, Cummings JH. Rapidly available glucose in foods: an in vitro measurement that reflects the glycemic response. Am J Clin Nutr. 1999;69:448-54.
7. Burton P, Lightowler HJ. Influence of bread volume on glycaemic response and satiety. Br J Nutr. 2006;96:877-82.
8. Jenkins DJ, Wesson V, Wolever TM, Jenkins AL, Kalmusky J, Guidici S, Csima A, Josse RG, Wong GS. Wholemeal versus wholegrain breads: proportion of whole or cracked grain and the glycaemic response. BMJ. 1988;297:958-60.
9. Ross SW, Brand JC, Thorburn AW, Truswell AS. Glycemic index of processed wheat products. Am J Clin Nutr. 1987;46:631-5. 10. Holm J, Hagander B, Björck I, Eliasson AC, Lundquist I. The effect of various thermal processes on the glycemic response to whole grain wheat products in humans and rats. J Nutr. 1989;119:1631-8.
11. Burton P, Lightowler HJ. The impact of freezing and toasting on the glycaemic response of white bread. Eur J Clin Nutr. 2008 May;62(5):594-9.
12. Leeman M, Ostman E, Björck I. Glycaemic and satiating properties of potato products. Eur J Clin Nutr. 2008;62:87-95.
13. Davidson CJ, Zderic TW, Byerley LO, Coyle EF. Different glycemic indexes of breakfast cereals are not due to glucose entry into blood but to glucose removal by tissue. Am J Clin Nutr. 2003;78:742-8.
14. Gannon MC, Nuttall FQ, Saeed A, Jordan K, Hoover H. An increase in dietary protein improves the blood glucose response in persons with type 2 diabetes. Am J Clin Nutr. 2003;78:734-41.
15. Johnston CS, Buller AJ. Vinegar and peanut products as complementary foods to reduce postprandial glycemia. J Am Diet Assoc. 2005;105:1939-42.
16. Henry CJ, Lightowler HJ, Kendall FL, Storey M. The impact of the addition of toppings/fillings on the glycaemic response to commonly consumed carbohydrate foods. Eur J Clin Nutr. 2006;60:763-9.
17. Hollenbeck CB, Coulston AM. The clinical utility of the GI and its application to mixed meals. Can J Physiol Pharmacol. 1991;69:100-7.
18. Wolever TM. Glycemic index and mixed meals. Am J Clin Nutr. 1990;51:1113-4.
19. Wheeler ML, Pi-Sunyer FX. Carbohydrate issues: type and amount. J Am Diet Assoc. 2008;108(4 Suppl 1):S34-9.
20. Cui H, Yang Y, Bian L, He M. Effect of food composition of mixed food on glycemic index. Wei Sheng Yan Jiu. 1999;28:356-8. 21. Wolever TM, Yang M, Zeng XY, Atkinson F, Brand-Miller JC. Food glycemic index, as given in glycemic index tables, is a significant determinant of glycemic responses elicited by composite breakfast meals. Am J Clin Nutr. 2006;83:1306-12.
22. Wolever TM, Vorster HH, Bjorck I, Brand-Miller J, Brighenti F, Mann JI, Ramdath DD, Granfeldt Y, Holt S, Perry TL, Venter C, Xiaomei Wu. Determination of the glycaemic index of foods: interlaboratory study. Eur J Clin Nutr. 2003, 57:475-82.
23. Vega-López S, Ausman LM, Griffith JL, Lichtenstein AH. Interindividual variability and intra-individual reproducibility of glycemic index values for commercial white bread. Diabetes Care. 2007;30:1412-7.
24. Wolever TM, Jenkins DJ, Ocana AM, Rao VA, Collier GR. Second-meal effect: low-glycemic-index foods eaten at dinner improve subsequent breakfast glycemic response. Am J Clin Nutr. 1988;48:1041-7.
25. Nilsson A, Granfeldt Y, Ostman E, Preston T, Björck I. Effects of GI and content of indigestible carbohydrates of cereal-based evening meals on glucose tolerance at a subsequent standardised breakfast. Eur J Clin Nutr. 2006;60:1092-9.
26. van Bakel MM, Slimani N, Feskens EJ, Du H, Beulens JW, van der Schouw YT, Brighenti F, Halkjaer J, Cust AE, Ferrari P, Brand-Miller J, Bueno-de-Mesquita HB, Peeters P, Ardanaz E, Dorronsoro M, Crowe FL, Bingham S, Rohrmann S, Boeing H, Johansson I, Manjer J, Tjonneland A, Overvad K, Lund E, Skeie G, Mattiello A, Salvini S, Clavel-Chapelon F, Kaaks R. Methodological challenges in the application of the glycemic index in epidemiological studies using data from the European Prospective Investigation into Cancer and Nutrition. J Nutr. 2009;139:568-75.