Embed Size (px)
Citation preview

Original article | Published 06 July 2017 | doi104414smw201714459Cite this as Swiss Med Wkly 2017147w14459
Glycaemic blood pressure and lipid goalattainment and chronic kidney disease stage oftype 2 diabetic patients treated in primary carepracticesCorcillo Antonellaa Pivin Edwardb Lalubin Fabriceb Pitteloud Nellya Burnier Michelb Zanchi Anneab
a Service of Endocrinology Diabetes and Metabolism Department of Internal Medicine Centre Hospitalier Universitaire Vaudois Lausanne Switzerlandb Service of Nephrology and Hypertension Department of Internal Medicine Centre Hospitalier Universitaire Vaudois Lausanne Switzerland
Summary
INTRODUCTION The prevalence of chronic kidney dis-ease and diabetes is rising in Europe These patients areat high cardiovascular and renal risk and need a challeng-ing multifactorial therapeutic approach
METHOD The goal of this cross-sectional study was toexamine the treatment and attainments of goals related tocardiovascular risk factors within chronic kidney diseasestages in type 2 diabetic patients followed up by primarycare physicians in Switzerland Each participating physi-cian entered into a web database the anonymised data ofup to 15 consecutive diabetic patients attending herhis of-fice between December 2013 and June 2014 Diabeteshypertension and lipid lowering therapies were analysedas well as glycated haemoglobin (HbA1c) blood pressureand low-density lipoprotein-cholesterol (LDL-c) levels andgoal attainments by KDIGO chronic kidney disease stage1 to 4
RESULTS A total of 1359 patients (mean age 665plusmn124years) were included by 109 primary care physiciansChronic kidney disease stages 0ndash2 3a 3 b and 4 werepresent in 776 139 61 and 24 respectivelyAverage HbA1c was independent of chronic kidney dis-ease stage and close to 7 more than half of the patientsreached the HbA1c goal Eighty-four percent of patientswere hypertensive and only 182 reached the then cur-rent Swiss or American Diabetes Association 2013 bloodpressure goals Despite loosening of blood pressure goalsin 2015 only half of the patients reached them and mostneeded multiple therapies Increased body mass indexand advanced chronic kidney disease stage decreasedthe chance of reaching blood pressure goals Lipid low-ering therapy was prescribed in 621 of cases with av-erage LDL-c levels similar across chronic kidney diseasestages Only 42 of patients reached the LDL-c goal oflt25 mmoll in primary prevention and 32 reached lt18mmoll in secondary prevention Younger patients were
treated significantly less aggressively than older patients(ge68 years median age) for HbA1c LDL-c and diastolicblood pressure control
CONCLUSION This cross-sectional study demonstratesthat blood pressure and lipid goals are less often achievedthan blood glucose control in type 2 diabetic patients fol-lowed up by primary care physicians in Switzerland Goalattainments for HbA1c and LDL-c were not influenced bychronic kidney disease stages in contrast to blood pres-sure Reaching all three goals was rare (22) Thereis a need for improvement in blood pressure control inadvanced chronic kidney disease whereas HbA1c goalsmay be loosened in the elderly and in advanced chronickidney disease
Key words diabetes chronic kidney disease goal attain-ments HbA1c blood pressure LDL-cholesterol
Introduction
Type 2 diabetes is a complex disease requiring a multifac-torial approach Since 1989 specific goals for blood glu-cose blood pressure and lipid control have been elaboratedby diabetes associations [1ndash3] Recently these goals havebeen adapted to diabetic patients with chronic kidney dis-ease (CKD) in recommendations from the Kidney DiseaseOutcomes Quality Initiative (KDOQI) [4] Kidney Dis-ease Improving Global Outcomes (KDIGO) [5] Ameri-can Diabetes Association (ADA) and European Associa-tion for the Study of Diabetes (EASD) [1ndash3] Less strin-gent goals for HbA1c are now recommended in CKD pa-tients The Steno study was the first to emphasise theefficacy of a multifactorial approach in type 2 diabetes [6]The group receiving intensified intervention on modifiablerisk factors for cardiovascular disease had lower cardiovas-cular and microvascular events by around 50 comparedwith those receiving usual care In the intensive therapygroup goals for HbA1c (goal lt65) systolic blood pres-sure (goal lt130 mm Hg) diastolic blood pressure (goallt80 mm Hg) and total cholesterol (goal lt175 mmoll) were
Author contributionsA Corcillo Vionnet and EPivin contributed equallyand are both first authorsCorrespondenceAnne Zanchi MD Serviceof Nephrology Endocrinol-ogy and Diabetes Depart-ment of Medicine LausanneUniversity Hospital CentreHospitalier UniversitaireVaudois CH-1011 Lau-sanneannezanchi[at]chuvch
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 1 of 12
reached in approximately 15 45 70 and 70 of cas-es respectivelyPrimary care physicians (PCPs) often complain about thedifficulty in reaching all goals as time dedicated to thecare of patients in an outpatient setting is confined Goalattainments following recommendations have recentlybeen examined in the US in Italy in Finland and in Canadawith heterogeneous results [7ndash10] For example in a USsurvey although testing rates in family practices forHbA1c blood pressure and low-density lipoprotein cho-lesterol (LDL-c) were high (992 100 and 939 re-spectively) goal attainment was not optimal Goals wereonly attained in 389 for HbA1c (goal lt7) in 595for blood pressure (goal lt13080 mm Hg) and in 718for LDL-c (goal lt26 mmoll) This was a retrospectiveobservational study done in a single area showing goodadherence to ADA recommendations of practitioners inclinics at Michigan State University Although some coun-tries have registries for diabetic patients this are lackingin Switzerland Thus surveys with primary care physiciansare needed to examine this issue
Objective and methods
The objective of this cross-sectional study was to examinethe treatment the CKD stages and goal attainments of type2 diabetic patients followed up by PCPs in SwitzerlandPCPs in German- (n = 16) and French-speaking (n = 4)cantons were approached for this purposeData were collected from December 2013 to June 2014 bymeans of a cross-sectional survey of ambulatory patientsvisiting their physicians The randomisation of the par-ticipating physicians was as follows for the German andFrench linguistic regions of Switzerland physicians wererecruited randomly among PCPs until about 110 physi-cians were recruited No physician from the Italian part ofSwitzerland was recruited PCPs were asked to collect thedata from up to 15 consecutive patients with type 2 dia-betes without selection of enrolled patients The data wereintroduced anonymously into a web database elaborated byPNN AG (wwwpnnch) Informed consent was obtainedfrom each patient Type 1 diabetes was an exclusion crite-rionDemographic and clinical data complications related todiabetes detailed antidiabetic antihypertensive and lipidlowering therapies and aspirin treatment were collectedin a standardised web questionnaire Estimated glomerularfiltration rate (eGFR) was calculated with the Chronic Kid-ney Disease Epidemiology Collaboration (CKD-EPI) for-mula [5] As data on albuminuria were available for onlya minority of patients an eGFR ge60 mlmin173m2 wasclassified as CKD stage 0ndash2 Detailed antidiabetic therapyand CKD stages have been presented in a separate article[11] Here we present the data for attainment of HbA1cblood pressure and LDL-c goalsThe study was accepted by the Ethics Committee of theCanton of Vaud
Data analysis for goal attainments
Blood glucose controlThe most recent values for HbA1c creatinine and antidi-abetic therapy were introduced into the database Mean
HbA1c values by KDIGO CKD stages [5] and age (lt68 orge68 years) were examined At initiation of the study exist-ing goals for HbA1c were individualised from lt7 in pa-tients at low risk of hypoglycaemia to lt8 in patients witha history of severe hypoglycaemia limited life expectan-cy advanced microvascular complications and extensivecomorbid conditions [5 12] Based on these recommen-dations we examined HbA1c goal attainments of lt7 inCKD stage 0ndash2 and lt8 in CKD stage 3a 3b and 4 Fac-tors involved in attainment of HbA1c goals were assessed
Blood pressure controlThe most recent office blood pressure reading and antihy-pertensive therapy were entered into the database Subjectswere stratified by KDIGO CKD stage and the number ofantihypertensive classes analysed accordinglyAt initiation of the study existing goals from the Swiss Hy-pertension Society were lt13080 mm Hg in diabetes [13]Factors involved in blood pressure goal attainment wereexamined Systolic and diastolic blood pressure levels byKDIGO CKD stages and age (lt68 or ge68 years) were ex-aminedBecause blood pressure goal recommendations have sub-stantially changed during recent years [14] and differedfrom Swiss recommendations at the time of the study weanalysed the data according to a ldquohistoricalrdquo goal of lt13080 mm Hg [13] ADA 2013 goal of lt14080 mm Hg [12]European Society of Hypertension (ESH) 2013 goal oflt14085 mm Hg [15] and the recent ADA 2015 goal oflt14090 mm Hg [2]
LDL-cholesterol goalsThe most recent lipid profile and lipid lowering therapywere entered into the database Mean LDL-c levels wereanalysed by KDIGO CKD stage and median age (lt68 orge68 years) At the initiation of the study existing Swissgoals for LDL-c in diabetes were lt18 mmoll in the caseof end-organ damage or other cardiovascular risk factorsand lt25 mmoll in uncomplicated type 2 diabetes [16]We chose a goal of lt18 mmoll for patients with diabetesand a positive history of coronary heart disease atheroscle-rosis cerebrovascular disease and an eGFRlt60mlmin Agoal of lt25 mmoll was chosen for others
StatisticsStatistical analyses were conducted using STATAreg version14 (StataCorp College Station TX) Continuous and cate-gorical variables were expressed as mean plusmn standard devi-ation (SD) and as number () of participants respectivelyStatistical significance was a 2-sided p-value of less than005 We used Pearsonrsquos correlation to assess associationsbetween continuous variables T-tests were performed tocompare continuous variables between goal attainers andgoal nonattainers To compare the frequency of goal attain-ers across CKD stages we used the Pearsonrsquos chi-squaredtest We used a logistic regression to assess the associa-tions between independent variables and goal attainmentTo compare continuous variables across CKD stages weperformed the nonparametric test for trend across orderedgroups developed by Cuzick which is an extension of theWilcoxon rank-sum test [17]
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 2 of 12
Results
A total of 109 PCPs from 20 German- or French-speakingcantons participated in the study with a total of 1359 pa-tients included for analysis Detailed geographic distribu-tion of PCP offices has been described previously [11] (fig1)Characteristics of participants according to CKD stage arepresented in table 1 There were a majority of male Cau-casian patients Average age was of 665plusmn124 years (meanplusmn standard deviation) with most (575) in the 60ndash80 yeargroup Mean duration of diabetes was 93 years and meanbody mass index (BMI) 302 kgm2 An eGFR ge60 mlmin was found in 776 of the patients and 139 61
Figure 1 Percentage and number of type 2 diabetic patients en-rolled by cantonZH = Zuumlrich SG = St Gallen GE = Genegraveve Vaud= VD VS = Valais BS = Basel-Stadt BL = Basel-Landschaft GR= Graubuumlnden LU = Luzern TG = Thurgau FR = Freiburg SZ =Schwyz SH = Schaffhausen AG = Aargau OW = Obwalden NE= Neuchacirctel ZG = Zug SO = Solothurn AL = Appenzell
and 24 respectively were in CKD stage 3a 3b and4 Hypertension dyslipidaemia and atherosclerosis werethe three most reported comorbidities present in 8468 and 26 of cases respectively Age duration of di-abetes sex smoking status diastolic blood pressure an-tihypertensive therapy lipid lowering therapy neuropathyretinopathy history of atherosclerosis cerebrovascular dis-ease coronary heart disease and heart failure differed sig-nificantly by CKD stageDetails of antidiabetic antihypertensive lipid loweringand aspirin therapies are presented in Table 2
Treatment and goal attainments
Glycated haemoglobinHbA1c was available for 1357 patients Only 625 ofsubjects were on nonpharmacological therapy The major-ity of subjects were on mono- (377) or dual therapy(383) with a clear preference for metformin (table 2)Mean (plusmn SD) HbA1c was 712 plusmn 122 716 plusmn 113716 plusmn 12 and 718 plusmn 10 respectively in subjects withstage 0ndash2 3a 3b and 4 CKD (table 1) The goal of lt7was reached in 53 of subjects with CKD stage 0ndash2 (andin 488 with CKD stage 3andash4) the goal of lt8 wasreached in 791 of patients with CKD stage 3andash4 Factorsinvolved in HbA1c goal attainment are presented in table3 Nonsmoking status fewer comorbidities increased age
Table 1 Characteristics of participants according to stage of chronic kidney disease (n = 1359)
CKD stageVariable
0ndash2 3a 3b 4
Miss p-value Total
Categorical n ()
Total 1057 (781) 183 (135) 84 (62) 30 (22) 5 1359
Women 430 (407) 81 (443) 45 (536) 19 (633) 2 001 577 (425)
Non-Caucasian 17 (16) 1 (05) 2 (24) 1 (33) 0 053 21 (15)
Smoking (yes) 136 (148) 22 (128) 7 (89) 0 (00) 158 006 165 (137)
Hypertension (yes) 757 (826) 151 (878) 73 (924) 26 (867) 158 006 1201 (841)
Antihypertensive TTT (yes) 782 (740) 165 (902) 77 (917) 29 (967) 0 lt001 1056 (777)
Dyslipidaemia (yes) 630 (688) 110 (640) 56 (709) 23 (767) 158 042 822 (684)
Lipid lowering TTT (yes) 632 (598) 122 (667) 64 (762) 23 (767) 0 lt001 844 (621)
Obesity (yes) 471 (446) 91 (497) 36 (429) 13 (433) 0 059 612 (450)
Neuropathy (yes) 111 (121) 34 (198) 21 (266) 12 (400) 158 lt001 178 (148)
Retinopathy (yes) 52 (57) 18 (105) 11 (139) 4 (133) 158 lt001 85 (71)
Atherosclerosis (yes) 206 (225) 62 (360) 34 (430) 16 (533) 158 lt001 318 (265)
CV disease (yes) 47 (51) 17 (99) 15 (190) 5 (167) 158 lt001 84 (70)
CHD (yes) 147 (160) 45 (262) 23 (291) 13 (433) 158 lt001 228 (190)
Heart failure (yes) 29 (32) 19 (110) 12 (152) 8 (267) 158 lt001 68 (57)
Urogenital disease (yes) 23 (25) 9 (52) 5 (63) 1 (33) 158 010 38 (32)
Continuous (meanplusmnSD)
Age yr 640plusmn119 745plusmn90 768plusmn92 790plusmn94 0 lt001 665plusmn124
Duration of DB yr 89plusmn87 109plusmn97 104plusmn63 125plusmn108 1 lt001 93plusmn88
Number of DB drugs 172plusmn088 160plusmn083 173plusmn094 143plusmn090 0 010 169plusmn088
Body mass index kgm2 302plusmn58 304plusmn53 302plusmn56 303plusmn53 1 055 302plusmn57
Diastolic BP mm Hg 808plusmn99 788plusmn113 778plusmn121 737plusmn92 0 lt001 802plusmn103
Systolic BP mm Hg 136plusmn14 137plusmn15 138plusmn14 138plusmn16 0 011 137plusmn14
eGFR mlmin173 m2 870plusmn153 527plusmn39 374plusmn42 238plusmn44 5 ndash 779plusmn224
LDL mmoll 262plusmn095 266plusmn100 256plusmn125 265plusmn119 394 068 263plusmn098
HDL mmoll 126plusmn040 132plusmn044 124plusmn037 125plusmn044 270 097 127plusmn040
Triglyceride mmoll 198plusmn112 192plusmn100 216plusmn107 192plusmn089 275 061 197plusmn109
HbA1c 712plusmn122 716plusmn113 716plusmn120 718plusmn100 2 040 712plusmn120
BP = blood pressure CHD = coronary heart disease CKD = chronic kidney disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rateHbA1c = glycated haemoglobin HDL = high density lipoprotein LDL = low density lipoprotein Miss = number of missing values SD = standard deviation TTT = treatment p-value for chi-square test of independence for categorical variables for a trend across CKD stages for continuous variables
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 3 of 12
shorter duration of diabetes lower BMI higher HDL-c andimpaired renal function were factors associated with im-proved HbA1c goal attainment Mean HbA1c was 72 inthe group aged lt68 y and 70 in the group aged ge68yand differed significantly (p lt001)
Blood pressureOverall blood pressure values were available for 1359 pa-tients Angiotensin II receptor blockers (ARBs) diureticsand ACE inhibitors (ACEIs) were the most prescribed an-tihypertensive classes (46 457 and 397 respective-ly) followed by beta-blockers and calcium channel block-ers (CCBs) (335 and 316 respectively) (table 2)Among the 262 patients on dual therapy the preferredoption was ARBdiuretic (285) followed by ACEIdi-uretic (197) and ARBCCB (144) Two patients wereon inappropriate ARBACEI therapy With the progression
of CKD stages the number of antihypertensive classes in-creased A total of 2341108 (21) of patients with bloodpressure ge13080 mm Hg were not on antihypertensivetherapy (fig 2) The number of antihypertensive drugs wasthe same in blood pressure goal attainers and nonattainers(160 vs 156 p = 06) In blood pressure goal attainers thenumber of antihypertensive drugs increased with advanc-ing CKD stage (p lt0001) After stratifying for two agegroups mean systolic and diastolic blood pressure were1361 mm Hg and 826 mm Hg respectively in the pa-tients aged lt68 years and 1370 mm Hg and 778 mmHg respectively in those aged ge68 years (median age)for diastolic blood pressure the difference was significant(plt001)Estimated GFR was negatively associated with systolicblood pressure (p lt001) and positively associated withdiastolic blood pressure (plt001) Systolic blood pressuredid not differ by CKD stage however diastolic blood pres-
Table 2 Antidiabetic antihypertensive lipid lowering and aspirin therapies
n
Antidiabetic therapy 1359 100
Healthy way of life 1037 7631
Pharmacological therapy 1274 9375
Metformin 1006 7403
DPP-4 inhibitor 465 3422
Sulphonylurea 279 2053
Glitazone 41 302
Glinide 28 206
Alpha glucosidase inhibitor 4 029
GLP-1 agonist 85 625
Insulin 393 2892
Long acting insulin 273 2009
Short and long acting insulin 182 1339
Number of classes prescribed
0 85 625
1 513 378
2 521 383
3 214 158
4 26 19
Antihypertensive therapy 1056 (777) answers
ACE inhibitor 420 397
Angiotensin receptor blocker 486 460
Calcium antagonist 334 316
Diuretic 483 457
Beta-blocker 354 335
Other 56 53
Number of classes prescribed
1 385 365
2 356 337
3 228 216
4 83 79
5 4 04
Lipid lowering therapy 844 (621) answers
Statin 793 940
Fibrate 18 213
Inhibitor of cholesterol absorption 28 33
Other 39 46
Number of classes prescribed
1 810 960
2 34 40
Aspirin 1066 (784) answers
575 539
ACE = angiotensin converting enzyme DPP-4 = dipeptidyl peptidase-4 GLP-1 = glucagon-like peptide-1
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 4 of 12
sure was lower at advanced CKD stage (nptrend p lt0001table 3) The blood pressure goal of lt13080 mmg Hg wasreached in only 182 of patients Of interest a bloodpressure goal le13080 mmg Hg was reached in 30 of cas-es illustrating a clear digit preference for numbers endingin zeroFactors involved in blood pressure goal attainment are pre-sented in table 4 Presence of atherosclerosis coronaryheart disease and congestive heart disease increased goalattainment Low BMI and low LDL-c levels were factorsassociated with improved blood pressure goal attainment
Figure 2 Number and of anti-hypertensive therapy by chronickidney disease (CKD) stage
Recommendations for blood pressure goals have consid-erably changed recently and have differed between dia-betes or hypertension associations For better clarity fig-ure 3 presents different goals and goal attainments by CKDstage Goal attainment increased with less stringent goalsbut however decreased with more advanced CKD For ex-ample the less stringent ADA 2015 goal of a blood pres-sure lt14090 mm Hg was reached by only 546 519476 40 respectively of patients in CKD stages 0ndash23a 3b and 4 Goal attainment was significantly lower inadvanced CKD
Figure 3 Mean blood pressure and number () of patientsachieving blood pressure goals according to guidelinesADA =American Diabetes Association BP = blood pressure ESH = Eu-ropean Society of Hypertension
Table 3 Odd ratios for glycated haemoglobin goal attainment in univariate analysis (n = 1352)
HbA1c goal attainment
CKD stages 0ndash2(n = 1055) CKD stages 3a 3b and 4(n = 297)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidence interval) p-value
Categorical
Women 108 (084ndash138) 056 090 (051ndash159) 073
Non-Caucasian 048 (018ndash130) 015 025 (003ndash183) 017
Smoking (yes) 051 (035ndash075) lt001 122 (044ndash335) 070
Hypertension (yes) 055 (039ndash078) lt001 120 (049ndash294) 070
Antihypertensive TTT (yes) 058 (044ndash077) lt001 148 (059ndash370) 040
Dyslipidaemia (yes) 079 (060ndash105) 011 070 (037ndash135) 029
Lipid lowering TTT (yes) 068 (053ndash088) lt001 099 (054ndash184) 098
Obesity (yes) 067 (052ndash085) lt001 065 (037ndash114) 013
Neuropathy (yes) 047 (031ndash071) lt001 119 (058ndash241) 064
Retinopathy (yes) 040 (022ndash073) lt001 044 (020ndash098) 004
Atherosclerosis (yes) 078 (057ndash106) 011 113 (062ndash207) 069
CV disease (yes) 082 (046ndash148) 051 063 (028ndash139) 025
CHD (yes) 083 (058ndash118) 031 091 (048ndash173) 078
Heart failure (yes) 182 (084ndash397) 013 096 (041ndash222) 092
Urogenital disease (yes) 049 (021ndash118) 011 100 (027ndash365) 099
Continuous
Age 10 yr 118 (106ndash131) lt001 117 (087ndash158) 030
Duration of DB yr 097 (096ndash099) lt001 097 (095ndash100) 006
Number of DB drugs 044 (037ndash051) lt001 051 (037ndash072) lt001
Body mass index 5 kgm2 088 (079ndash098) 002 082 (064ndash106) 013
Diastolic BP 10 mmHg 093 (082ndash105) 024 076 (059ndash098) 003
Systolic BP 10 mmHg 092 (084ndash100) 005 084 (069ndash102) 008
eGFR 10 mlmin173 m2 089 (082ndash097) lt001 113 (087ndash146) 036
LDL mmoll 096 (083ndash112) 062 123 (085ndash180) 027
HDL mmoll 153 (108ndash217) 002 278 (109ndash714) 003
Triglyceride mmoll 076 (067ndash087) lt001 058 (043ndash079) lt001
HbA1c ndash ndash ndash ndash
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 5 of 12
LipidsOverall LDL-c values were available in 965 patientsAmong the 621 of patients on lipid lowering therapy94 were taking a statin LDL-c values were similaracross CKD stages of (mean plusmn SD) 262 plusmn 095 mmoll266 plusmn 10 mmoll 256 plusmn 125 mmoll and 265 plusmn 119mmoll respectively in subjects with CKD stages 0ndash2 3a3b and 4 (table 1) In patients qualifying for primary pre-vention (n = 473) an LDL-c goal of lt25 mmoll wasreached in 42 (n = 198) of cases For those qualifyingfor secondary prevention (n = 407) an LDL-c goal of lt18mmoll was reached in 32 of cases (n = 130) (fig 4)LDL-c goal attainments did not change across all CKDstages
Figure 4 Mean low-density lipoprotein- cholesterol levels andnumber () of patients achieving goals in primary and secondarypreventionCKD = chronic kidney disease LDL = low-densitylipoprotein
Factors involved in LDL-c goal attainment are presentedin table 5 Gender smoking status and co-morbidities ageduration of diabetes DBP were factors associated with im-proved LDL goal attainment Mean LDL-c was of 276mmoll in patients aged lt68 years and 25 mmoll in thoseaged ge68 years and differed significantly between the twoage groups (p lt001)In this study HbA1c blood pressure and lipid goals wereall achieved in only 30 patients (22) (fig 5) Charac-teristics by goal attainment are available in supplementarytable S1 (appendix)
Discussion
The European prevalence of CKD is rising in diabetic sub-jects [18] and is the leading cause of end-stage renal dis-
Figure 5 Percentage of patients reaching glycated haemoglobinblood pressure and low-density lipoprotein-cholesterol goalsBP =blood pressure CKD = chronic kidney disease stage HbA1c = gly-cated haemoglobin
Table 4 Odd ratios for blood pressure goal attainment in univariate analysis (n = 1354)
Independent variables Odds ratio(95 confidence interval) p-value
Categorical
Women 110 (083ndash145) 052
Non-Caucasian 075 (022ndash256) 064
Smoking (yes) 112 (074ndash171) 058
Hypertension (yes) 048 (033ndash068) lt001
Antihypertensive TTT (yes) 072 (052ndash098) 004
Dyslipidaemia (yes) 116 (084ndash161) 037
Lipid lowering TTT (yes) 109 (082ndash146) 054
Obesity (yes) 058 (044ndash078) lt001
Neuropathy (yes) 158 (108ndash231) 002
Retinopathy (yes) 167 (101ndash279) 005
Atherosclerosis (yes) 164 (120ndash225) lt001
CV disease (yes) 138 (081ndash235) 024
CHD (yes) 213 (152ndash299) lt001
Heart failure (yes) 332 (199ndash553) lt001
Urogenital disease (yes) 086 (035ndash208) 073
Continuous
Age 10 yr 103 (092ndash115) 059
Duration of DB yr 102 (101ndash104) lt001
Number of DB drugs 107 (091ndash125) 041
Body mass index 5 kgm2 078 (069ndash090) lt001
Diastolic BP 10 mmHg ndash ndash
Systolic BP 10 mmHg ndash ndash
eGFR 10 mlmin173 m2 096 (091ndash103) 025
LDL mmoll 074 (062ndash088) lt001
HDL mmoll 077 (052ndash115) 021
Triglyceride mmoll 086 (073ndash101) 006
HbA1c 094 (083ndash106) 030
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 6 of 12
ease (ESRD) The presence of nephropathy considerablyamplifies cardiovascular risk and mortality A multifacto-rial approach is thus necessary to decrease the renal func-tion decline and cardiovascular risk In accordance guide-lines have been released by many societies [1ndash4 19] andthe goal of this study was to examine whether goal attain-ments were reached in a primary care setting in Switzer-landThe average patient age sex distribution HbA1c systolicblood pressure and LDL-c level in this survey was similarto results of other Swiss diabetic surveys [20 21] Our datacan therefore be considered as representative of the Swissdiabetic population To our knowledge this is the first sur-vey analysing the care of Swiss type 2 diabetic patients byCKD stage Overall this study demonstrates that the ma-jority of subjects with type 2 diabetes are men with hy-pertension and lipid abnormalities HbA1c goals are mostoften reached but blood pressure goals are achieved lessfrequently especially in advanced CKD stages Amongthose qualifying for secondary prevention only a thirdreached the recommended LDL-c goalThe demographic characteristics of the population in thissurvey are similar to other studies in Europe in termsof age group sex and ethnicity but differ from the USstudy in which sexes were equally represented and ethnic-ity more diverse [7ndash10]
HbA1c and glycaemic controlIn our study average HbA1c was independent of CKDstage and close to 7 This was similar to the Finnishstudy in which HbA1c ranged between 69 and 73 atCKD stages 2ndash5 [9] Thus Swiss physicians may not dif-ferentiate their goals by CKD stage in spite of KDOQI2012 recommendations [4] Furthermore older subjects(71ndash90 years old) were treated significantly more aggres-sively than younger subjects with an average HbA1c lt7Hence these results highlight the need to improve physi-cian awareness of the risk of hypoglycaemia in CKD andin the elderly [22]Tight glycaemic control is beneficial in the primary pre-vention of nephropathy in type 1 [23 24] and type 2 dia-betes [25ndash27] with a decrease in the incidence of microal-buminuria and progression to macroalbuminuria but itseffect in secondary prevention is less well established In-deed the effect on renal function decline has been demon-strated in type 1 diabetes in the 22-year Diabetes Controland Complications Trial Epidemiology of Diabetes In-terventions and Complications (DCCTEDIC) study [28]and in subjects with type 2 diabetes after 10 years in theUK Prospective Diabetes Study (UKPDS) study [25] Yetboth studies involved intensive glucose control early in thecourse of diabetes The cardiovascular and renal efficacyand safety of tight glycaemic control in type 2 diabetespatients at high cardiovascular risk needs to be careful-
Table 5 Odd ratios for low-density lipoprotein goal attainment in univariate analysis (n = 937)
LDL goal attainment
CKD stages 0ndash2 n = 748) CKD stages 3a 3b and 4(n = 189)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidenceinterval)
p-value
Categorical
Women 067 (049ndash091) 001 055 (028ndash107) 008
Non-Caucasian 068 (024ndash195) 047
Smoking (yes) 056 (035ndash088) 001 099 (030ndash325) 098
Atherosclerosis (yes) ndash ndash ndash ndash
Hypertension (yes) 115 (077ndash172) 048 112 (038ndash326) 084
Antihypertensive TTT (yes) 204 (139ndash299) lt001 450 (057ndash3555) 015
Dyslipidaemia (yes) 131 (094ndash183) 011 062 (031ndash124) 017
Lipid lowering TTT (yes) 285 (203ndash401) lt001 178 (079ndash400) 016
Obesity (yes) 129 (096ndash173) 010 117 (061ndash225) 063
Neuropathy (yes) 199 (126ndash315) lt001 147 (067ndash324) 033
Retinopathy (yes) 255 (129ndash506) 001 240 (089ndash649) 008
CV disease (yes) ndash ndash ndash ndash
CHD (yes) ndash ndash ndash ndash
Heart failure (yes) 219 (092ndash519) 008 180 (070ndash465) 022
Urogenital disease (yes) 115 (042ndash313) 078 188 (051ndash697) 034
Continuous
Age 10 yr 120 (105ndash138) 001 119 (080ndash177) 040
Duration of DB yr 102 (101ndash104) 001 101 (098ndash104) 054
Number of DB drugs 118 (100ndash140) 006 086 (059ndash125) 042
Body mass index 5 kgm2 112 (099ndash127) 008 115 (086ndash153) 034
Diastolic BP 10 mm Hg 077 (066ndash091) lt001 082 (060ndash110) 019
Systolic BP 10 mm Hg 099 (089ndash111) 089 079 (063ndash101) 006
eGFR 10 mlmin173 m2 092 (084ndash102) 010 078 (059ndash104) 009
LDL mmoll ndash ndash ndash ndash
HDL mmoll 104 (072ndash151) 084 063 (027ndash148) 029
Triglyceride mmoll 099 (082ndash120) 091 097 (064ndash146) 087
HbA1c 096 (085ndash109) 051 120 (091ndash159) 019
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment Too few (4) non-Caucasian participants with CKD stages 3a 3b and 4 to perform a univariateanalysis
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 7 of 12
ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

reached in approximately 15 45 70 and 70 of cas-es respectivelyPrimary care physicians (PCPs) often complain about thedifficulty in reaching all goals as time dedicated to thecare of patients in an outpatient setting is confined Goalattainments following recommendations have recentlybeen examined in the US in Italy in Finland and in Canadawith heterogeneous results [7ndash10] For example in a USsurvey although testing rates in family practices forHbA1c blood pressure and low-density lipoprotein cho-lesterol (LDL-c) were high (992 100 and 939 re-spectively) goal attainment was not optimal Goals wereonly attained in 389 for HbA1c (goal lt7) in 595for blood pressure (goal lt13080 mm Hg) and in 718for LDL-c (goal lt26 mmoll) This was a retrospectiveobservational study done in a single area showing goodadherence to ADA recommendations of practitioners inclinics at Michigan State University Although some coun-tries have registries for diabetic patients this are lackingin Switzerland Thus surveys with primary care physiciansare needed to examine this issue
Objective and methods
The objective of this cross-sectional study was to examinethe treatment the CKD stages and goal attainments of type2 diabetic patients followed up by PCPs in SwitzerlandPCPs in German- (n = 16) and French-speaking (n = 4)cantons were approached for this purposeData were collected from December 2013 to June 2014 bymeans of a cross-sectional survey of ambulatory patientsvisiting their physicians The randomisation of the par-ticipating physicians was as follows for the German andFrench linguistic regions of Switzerland physicians wererecruited randomly among PCPs until about 110 physi-cians were recruited No physician from the Italian part ofSwitzerland was recruited PCPs were asked to collect thedata from up to 15 consecutive patients with type 2 dia-betes without selection of enrolled patients The data wereintroduced anonymously into a web database elaborated byPNN AG (wwwpnnch) Informed consent was obtainedfrom each patient Type 1 diabetes was an exclusion crite-rionDemographic and clinical data complications related todiabetes detailed antidiabetic antihypertensive and lipidlowering therapies and aspirin treatment were collectedin a standardised web questionnaire Estimated glomerularfiltration rate (eGFR) was calculated with the Chronic Kid-ney Disease Epidemiology Collaboration (CKD-EPI) for-mula [5] As data on albuminuria were available for onlya minority of patients an eGFR ge60 mlmin173m2 wasclassified as CKD stage 0ndash2 Detailed antidiabetic therapyand CKD stages have been presented in a separate article[11] Here we present the data for attainment of HbA1cblood pressure and LDL-c goalsThe study was accepted by the Ethics Committee of theCanton of Vaud
Data analysis for goal attainments
Blood glucose controlThe most recent values for HbA1c creatinine and antidi-abetic therapy were introduced into the database Mean
HbA1c values by KDIGO CKD stages [5] and age (lt68 orge68 years) were examined At initiation of the study exist-ing goals for HbA1c were individualised from lt7 in pa-tients at low risk of hypoglycaemia to lt8 in patients witha history of severe hypoglycaemia limited life expectan-cy advanced microvascular complications and extensivecomorbid conditions [5 12] Based on these recommen-dations we examined HbA1c goal attainments of lt7 inCKD stage 0ndash2 and lt8 in CKD stage 3a 3b and 4 Fac-tors involved in attainment of HbA1c goals were assessed
Blood pressure controlThe most recent office blood pressure reading and antihy-pertensive therapy were entered into the database Subjectswere stratified by KDIGO CKD stage and the number ofantihypertensive classes analysed accordinglyAt initiation of the study existing goals from the Swiss Hy-pertension Society were lt13080 mm Hg in diabetes [13]Factors involved in blood pressure goal attainment wereexamined Systolic and diastolic blood pressure levels byKDIGO CKD stages and age (lt68 or ge68 years) were ex-aminedBecause blood pressure goal recommendations have sub-stantially changed during recent years [14] and differedfrom Swiss recommendations at the time of the study weanalysed the data according to a ldquohistoricalrdquo goal of lt13080 mm Hg [13] ADA 2013 goal of lt14080 mm Hg [12]European Society of Hypertension (ESH) 2013 goal oflt14085 mm Hg [15] and the recent ADA 2015 goal oflt14090 mm Hg [2]
LDL-cholesterol goalsThe most recent lipid profile and lipid lowering therapywere entered into the database Mean LDL-c levels wereanalysed by KDIGO CKD stage and median age (lt68 orge68 years) At the initiation of the study existing Swissgoals for LDL-c in diabetes were lt18 mmoll in the caseof end-organ damage or other cardiovascular risk factorsand lt25 mmoll in uncomplicated type 2 diabetes [16]We chose a goal of lt18 mmoll for patients with diabetesand a positive history of coronary heart disease atheroscle-rosis cerebrovascular disease and an eGFRlt60mlmin Agoal of lt25 mmoll was chosen for others
StatisticsStatistical analyses were conducted using STATAreg version14 (StataCorp College Station TX) Continuous and cate-gorical variables were expressed as mean plusmn standard devi-ation (SD) and as number () of participants respectivelyStatistical significance was a 2-sided p-value of less than005 We used Pearsonrsquos correlation to assess associationsbetween continuous variables T-tests were performed tocompare continuous variables between goal attainers andgoal nonattainers To compare the frequency of goal attain-ers across CKD stages we used the Pearsonrsquos chi-squaredtest We used a logistic regression to assess the associa-tions between independent variables and goal attainmentTo compare continuous variables across CKD stages weperformed the nonparametric test for trend across orderedgroups developed by Cuzick which is an extension of theWilcoxon rank-sum test [17]
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 2 of 12
Results
A total of 109 PCPs from 20 German- or French-speakingcantons participated in the study with a total of 1359 pa-tients included for analysis Detailed geographic distribu-tion of PCP offices has been described previously [11] (fig1)Characteristics of participants according to CKD stage arepresented in table 1 There were a majority of male Cau-casian patients Average age was of 665plusmn124 years (meanplusmn standard deviation) with most (575) in the 60ndash80 yeargroup Mean duration of diabetes was 93 years and meanbody mass index (BMI) 302 kgm2 An eGFR ge60 mlmin was found in 776 of the patients and 139 61
Figure 1 Percentage and number of type 2 diabetic patients en-rolled by cantonZH = Zuumlrich SG = St Gallen GE = Genegraveve Vaud= VD VS = Valais BS = Basel-Stadt BL = Basel-Landschaft GR= Graubuumlnden LU = Luzern TG = Thurgau FR = Freiburg SZ =Schwyz SH = Schaffhausen AG = Aargau OW = Obwalden NE= Neuchacirctel ZG = Zug SO = Solothurn AL = Appenzell
and 24 respectively were in CKD stage 3a 3b and4 Hypertension dyslipidaemia and atherosclerosis werethe three most reported comorbidities present in 8468 and 26 of cases respectively Age duration of di-abetes sex smoking status diastolic blood pressure an-tihypertensive therapy lipid lowering therapy neuropathyretinopathy history of atherosclerosis cerebrovascular dis-ease coronary heart disease and heart failure differed sig-nificantly by CKD stageDetails of antidiabetic antihypertensive lipid loweringand aspirin therapies are presented in Table 2
Treatment and goal attainments
Glycated haemoglobinHbA1c was available for 1357 patients Only 625 ofsubjects were on nonpharmacological therapy The major-ity of subjects were on mono- (377) or dual therapy(383) with a clear preference for metformin (table 2)Mean (plusmn SD) HbA1c was 712 plusmn 122 716 plusmn 113716 plusmn 12 and 718 plusmn 10 respectively in subjects withstage 0ndash2 3a 3b and 4 CKD (table 1) The goal of lt7was reached in 53 of subjects with CKD stage 0ndash2 (andin 488 with CKD stage 3andash4) the goal of lt8 wasreached in 791 of patients with CKD stage 3andash4 Factorsinvolved in HbA1c goal attainment are presented in table3 Nonsmoking status fewer comorbidities increased age
Table 1 Characteristics of participants according to stage of chronic kidney disease (n = 1359)
CKD stageVariable
0ndash2 3a 3b 4
Miss p-value Total
Categorical n ()
Total 1057 (781) 183 (135) 84 (62) 30 (22) 5 1359
Women 430 (407) 81 (443) 45 (536) 19 (633) 2 001 577 (425)
Non-Caucasian 17 (16) 1 (05) 2 (24) 1 (33) 0 053 21 (15)
Smoking (yes) 136 (148) 22 (128) 7 (89) 0 (00) 158 006 165 (137)
Hypertension (yes) 757 (826) 151 (878) 73 (924) 26 (867) 158 006 1201 (841)
Antihypertensive TTT (yes) 782 (740) 165 (902) 77 (917) 29 (967) 0 lt001 1056 (777)
Dyslipidaemia (yes) 630 (688) 110 (640) 56 (709) 23 (767) 158 042 822 (684)
Lipid lowering TTT (yes) 632 (598) 122 (667) 64 (762) 23 (767) 0 lt001 844 (621)
Obesity (yes) 471 (446) 91 (497) 36 (429) 13 (433) 0 059 612 (450)
Neuropathy (yes) 111 (121) 34 (198) 21 (266) 12 (400) 158 lt001 178 (148)
Retinopathy (yes) 52 (57) 18 (105) 11 (139) 4 (133) 158 lt001 85 (71)
Atherosclerosis (yes) 206 (225) 62 (360) 34 (430) 16 (533) 158 lt001 318 (265)
CV disease (yes) 47 (51) 17 (99) 15 (190) 5 (167) 158 lt001 84 (70)
CHD (yes) 147 (160) 45 (262) 23 (291) 13 (433) 158 lt001 228 (190)
Heart failure (yes) 29 (32) 19 (110) 12 (152) 8 (267) 158 lt001 68 (57)
Urogenital disease (yes) 23 (25) 9 (52) 5 (63) 1 (33) 158 010 38 (32)
Continuous (meanplusmnSD)
Age yr 640plusmn119 745plusmn90 768plusmn92 790plusmn94 0 lt001 665plusmn124
Duration of DB yr 89plusmn87 109plusmn97 104plusmn63 125plusmn108 1 lt001 93plusmn88
Number of DB drugs 172plusmn088 160plusmn083 173plusmn094 143plusmn090 0 010 169plusmn088
Body mass index kgm2 302plusmn58 304plusmn53 302plusmn56 303plusmn53 1 055 302plusmn57
Diastolic BP mm Hg 808plusmn99 788plusmn113 778plusmn121 737plusmn92 0 lt001 802plusmn103
Systolic BP mm Hg 136plusmn14 137plusmn15 138plusmn14 138plusmn16 0 011 137plusmn14
eGFR mlmin173 m2 870plusmn153 527plusmn39 374plusmn42 238plusmn44 5 ndash 779plusmn224
LDL mmoll 262plusmn095 266plusmn100 256plusmn125 265plusmn119 394 068 263plusmn098
HDL mmoll 126plusmn040 132plusmn044 124plusmn037 125plusmn044 270 097 127plusmn040
Triglyceride mmoll 198plusmn112 192plusmn100 216plusmn107 192plusmn089 275 061 197plusmn109
HbA1c 712plusmn122 716plusmn113 716plusmn120 718plusmn100 2 040 712plusmn120
BP = blood pressure CHD = coronary heart disease CKD = chronic kidney disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rateHbA1c = glycated haemoglobin HDL = high density lipoprotein LDL = low density lipoprotein Miss = number of missing values SD = standard deviation TTT = treatment p-value for chi-square test of independence for categorical variables for a trend across CKD stages for continuous variables
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 3 of 12
shorter duration of diabetes lower BMI higher HDL-c andimpaired renal function were factors associated with im-proved HbA1c goal attainment Mean HbA1c was 72 inthe group aged lt68 y and 70 in the group aged ge68yand differed significantly (p lt001)
Blood pressureOverall blood pressure values were available for 1359 pa-tients Angiotensin II receptor blockers (ARBs) diureticsand ACE inhibitors (ACEIs) were the most prescribed an-tihypertensive classes (46 457 and 397 respective-ly) followed by beta-blockers and calcium channel block-ers (CCBs) (335 and 316 respectively) (table 2)Among the 262 patients on dual therapy the preferredoption was ARBdiuretic (285) followed by ACEIdi-uretic (197) and ARBCCB (144) Two patients wereon inappropriate ARBACEI therapy With the progression
of CKD stages the number of antihypertensive classes in-creased A total of 2341108 (21) of patients with bloodpressure ge13080 mm Hg were not on antihypertensivetherapy (fig 2) The number of antihypertensive drugs wasthe same in blood pressure goal attainers and nonattainers(160 vs 156 p = 06) In blood pressure goal attainers thenumber of antihypertensive drugs increased with advanc-ing CKD stage (p lt0001) After stratifying for two agegroups mean systolic and diastolic blood pressure were1361 mm Hg and 826 mm Hg respectively in the pa-tients aged lt68 years and 1370 mm Hg and 778 mmHg respectively in those aged ge68 years (median age)for diastolic blood pressure the difference was significant(plt001)Estimated GFR was negatively associated with systolicblood pressure (p lt001) and positively associated withdiastolic blood pressure (plt001) Systolic blood pressuredid not differ by CKD stage however diastolic blood pres-
Table 2 Antidiabetic antihypertensive lipid lowering and aspirin therapies
n
Antidiabetic therapy 1359 100
Healthy way of life 1037 7631
Pharmacological therapy 1274 9375
Metformin 1006 7403
DPP-4 inhibitor 465 3422
Sulphonylurea 279 2053
Glitazone 41 302
Glinide 28 206
Alpha glucosidase inhibitor 4 029
GLP-1 agonist 85 625
Insulin 393 2892
Long acting insulin 273 2009
Short and long acting insulin 182 1339
Number of classes prescribed
0 85 625
1 513 378
2 521 383
3 214 158
4 26 19
Antihypertensive therapy 1056 (777) answers
ACE inhibitor 420 397
Angiotensin receptor blocker 486 460
Calcium antagonist 334 316
Diuretic 483 457
Beta-blocker 354 335
Other 56 53
Number of classes prescribed
1 385 365
2 356 337
3 228 216
4 83 79
5 4 04
Lipid lowering therapy 844 (621) answers
Statin 793 940
Fibrate 18 213
Inhibitor of cholesterol absorption 28 33
Other 39 46
Number of classes prescribed
1 810 960
2 34 40
Aspirin 1066 (784) answers
575 539
ACE = angiotensin converting enzyme DPP-4 = dipeptidyl peptidase-4 GLP-1 = glucagon-like peptide-1
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 4 of 12
sure was lower at advanced CKD stage (nptrend p lt0001table 3) The blood pressure goal of lt13080 mmg Hg wasreached in only 182 of patients Of interest a bloodpressure goal le13080 mmg Hg was reached in 30 of cas-es illustrating a clear digit preference for numbers endingin zeroFactors involved in blood pressure goal attainment are pre-sented in table 4 Presence of atherosclerosis coronaryheart disease and congestive heart disease increased goalattainment Low BMI and low LDL-c levels were factorsassociated with improved blood pressure goal attainment
Figure 2 Number and of anti-hypertensive therapy by chronickidney disease (CKD) stage
Recommendations for blood pressure goals have consid-erably changed recently and have differed between dia-betes or hypertension associations For better clarity fig-ure 3 presents different goals and goal attainments by CKDstage Goal attainment increased with less stringent goalsbut however decreased with more advanced CKD For ex-ample the less stringent ADA 2015 goal of a blood pres-sure lt14090 mm Hg was reached by only 546 519476 40 respectively of patients in CKD stages 0ndash23a 3b and 4 Goal attainment was significantly lower inadvanced CKD
Figure 3 Mean blood pressure and number () of patientsachieving blood pressure goals according to guidelinesADA =American Diabetes Association BP = blood pressure ESH = Eu-ropean Society of Hypertension
Table 3 Odd ratios for glycated haemoglobin goal attainment in univariate analysis (n = 1352)
HbA1c goal attainment
CKD stages 0ndash2(n = 1055) CKD stages 3a 3b and 4(n = 297)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidence interval) p-value
Categorical
Women 108 (084ndash138) 056 090 (051ndash159) 073
Non-Caucasian 048 (018ndash130) 015 025 (003ndash183) 017
Smoking (yes) 051 (035ndash075) lt001 122 (044ndash335) 070
Hypertension (yes) 055 (039ndash078) lt001 120 (049ndash294) 070
Antihypertensive TTT (yes) 058 (044ndash077) lt001 148 (059ndash370) 040
Dyslipidaemia (yes) 079 (060ndash105) 011 070 (037ndash135) 029
Lipid lowering TTT (yes) 068 (053ndash088) lt001 099 (054ndash184) 098
Obesity (yes) 067 (052ndash085) lt001 065 (037ndash114) 013
Neuropathy (yes) 047 (031ndash071) lt001 119 (058ndash241) 064
Retinopathy (yes) 040 (022ndash073) lt001 044 (020ndash098) 004
Atherosclerosis (yes) 078 (057ndash106) 011 113 (062ndash207) 069
CV disease (yes) 082 (046ndash148) 051 063 (028ndash139) 025
CHD (yes) 083 (058ndash118) 031 091 (048ndash173) 078
Heart failure (yes) 182 (084ndash397) 013 096 (041ndash222) 092
Urogenital disease (yes) 049 (021ndash118) 011 100 (027ndash365) 099
Continuous
Age 10 yr 118 (106ndash131) lt001 117 (087ndash158) 030
Duration of DB yr 097 (096ndash099) lt001 097 (095ndash100) 006
Number of DB drugs 044 (037ndash051) lt001 051 (037ndash072) lt001
Body mass index 5 kgm2 088 (079ndash098) 002 082 (064ndash106) 013
Diastolic BP 10 mmHg 093 (082ndash105) 024 076 (059ndash098) 003
Systolic BP 10 mmHg 092 (084ndash100) 005 084 (069ndash102) 008
eGFR 10 mlmin173 m2 089 (082ndash097) lt001 113 (087ndash146) 036
LDL mmoll 096 (083ndash112) 062 123 (085ndash180) 027
HDL mmoll 153 (108ndash217) 002 278 (109ndash714) 003
Triglyceride mmoll 076 (067ndash087) lt001 058 (043ndash079) lt001
HbA1c ndash ndash ndash ndash
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 5 of 12
LipidsOverall LDL-c values were available in 965 patientsAmong the 621 of patients on lipid lowering therapy94 were taking a statin LDL-c values were similaracross CKD stages of (mean plusmn SD) 262 plusmn 095 mmoll266 plusmn 10 mmoll 256 plusmn 125 mmoll and 265 plusmn 119mmoll respectively in subjects with CKD stages 0ndash2 3a3b and 4 (table 1) In patients qualifying for primary pre-vention (n = 473) an LDL-c goal of lt25 mmoll wasreached in 42 (n = 198) of cases For those qualifyingfor secondary prevention (n = 407) an LDL-c goal of lt18mmoll was reached in 32 of cases (n = 130) (fig 4)LDL-c goal attainments did not change across all CKDstages
Figure 4 Mean low-density lipoprotein- cholesterol levels andnumber () of patients achieving goals in primary and secondarypreventionCKD = chronic kidney disease LDL = low-densitylipoprotein
Factors involved in LDL-c goal attainment are presentedin table 5 Gender smoking status and co-morbidities ageduration of diabetes DBP were factors associated with im-proved LDL goal attainment Mean LDL-c was of 276mmoll in patients aged lt68 years and 25 mmoll in thoseaged ge68 years and differed significantly between the twoage groups (p lt001)In this study HbA1c blood pressure and lipid goals wereall achieved in only 30 patients (22) (fig 5) Charac-teristics by goal attainment are available in supplementarytable S1 (appendix)
Discussion
The European prevalence of CKD is rising in diabetic sub-jects [18] and is the leading cause of end-stage renal dis-
Figure 5 Percentage of patients reaching glycated haemoglobinblood pressure and low-density lipoprotein-cholesterol goalsBP =blood pressure CKD = chronic kidney disease stage HbA1c = gly-cated haemoglobin
Table 4 Odd ratios for blood pressure goal attainment in univariate analysis (n = 1354)
Independent variables Odds ratio(95 confidence interval) p-value
Categorical
Women 110 (083ndash145) 052
Non-Caucasian 075 (022ndash256) 064
Smoking (yes) 112 (074ndash171) 058
Hypertension (yes) 048 (033ndash068) lt001
Antihypertensive TTT (yes) 072 (052ndash098) 004
Dyslipidaemia (yes) 116 (084ndash161) 037
Lipid lowering TTT (yes) 109 (082ndash146) 054
Obesity (yes) 058 (044ndash078) lt001
Neuropathy (yes) 158 (108ndash231) 002
Retinopathy (yes) 167 (101ndash279) 005
Atherosclerosis (yes) 164 (120ndash225) lt001
CV disease (yes) 138 (081ndash235) 024
CHD (yes) 213 (152ndash299) lt001
Heart failure (yes) 332 (199ndash553) lt001
Urogenital disease (yes) 086 (035ndash208) 073
Continuous
Age 10 yr 103 (092ndash115) 059
Duration of DB yr 102 (101ndash104) lt001
Number of DB drugs 107 (091ndash125) 041
Body mass index 5 kgm2 078 (069ndash090) lt001
Diastolic BP 10 mmHg ndash ndash
Systolic BP 10 mmHg ndash ndash
eGFR 10 mlmin173 m2 096 (091ndash103) 025
LDL mmoll 074 (062ndash088) lt001
HDL mmoll 077 (052ndash115) 021
Triglyceride mmoll 086 (073ndash101) 006
HbA1c 094 (083ndash106) 030
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 6 of 12
ease (ESRD) The presence of nephropathy considerablyamplifies cardiovascular risk and mortality A multifacto-rial approach is thus necessary to decrease the renal func-tion decline and cardiovascular risk In accordance guide-lines have been released by many societies [1ndash4 19] andthe goal of this study was to examine whether goal attain-ments were reached in a primary care setting in Switzer-landThe average patient age sex distribution HbA1c systolicblood pressure and LDL-c level in this survey was similarto results of other Swiss diabetic surveys [20 21] Our datacan therefore be considered as representative of the Swissdiabetic population To our knowledge this is the first sur-vey analysing the care of Swiss type 2 diabetic patients byCKD stage Overall this study demonstrates that the ma-jority of subjects with type 2 diabetes are men with hy-pertension and lipid abnormalities HbA1c goals are mostoften reached but blood pressure goals are achieved lessfrequently especially in advanced CKD stages Amongthose qualifying for secondary prevention only a thirdreached the recommended LDL-c goalThe demographic characteristics of the population in thissurvey are similar to other studies in Europe in termsof age group sex and ethnicity but differ from the USstudy in which sexes were equally represented and ethnic-ity more diverse [7ndash10]
HbA1c and glycaemic controlIn our study average HbA1c was independent of CKDstage and close to 7 This was similar to the Finnishstudy in which HbA1c ranged between 69 and 73 atCKD stages 2ndash5 [9] Thus Swiss physicians may not dif-ferentiate their goals by CKD stage in spite of KDOQI2012 recommendations [4] Furthermore older subjects(71ndash90 years old) were treated significantly more aggres-sively than younger subjects with an average HbA1c lt7Hence these results highlight the need to improve physi-cian awareness of the risk of hypoglycaemia in CKD andin the elderly [22]Tight glycaemic control is beneficial in the primary pre-vention of nephropathy in type 1 [23 24] and type 2 dia-betes [25ndash27] with a decrease in the incidence of microal-buminuria and progression to macroalbuminuria but itseffect in secondary prevention is less well established In-deed the effect on renal function decline has been demon-strated in type 1 diabetes in the 22-year Diabetes Controland Complications Trial Epidemiology of Diabetes In-terventions and Complications (DCCTEDIC) study [28]and in subjects with type 2 diabetes after 10 years in theUK Prospective Diabetes Study (UKPDS) study [25] Yetboth studies involved intensive glucose control early in thecourse of diabetes The cardiovascular and renal efficacyand safety of tight glycaemic control in type 2 diabetespatients at high cardiovascular risk needs to be careful-
Table 5 Odd ratios for low-density lipoprotein goal attainment in univariate analysis (n = 937)
LDL goal attainment
CKD stages 0ndash2 n = 748) CKD stages 3a 3b and 4(n = 189)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidenceinterval)
p-value
Categorical
Women 067 (049ndash091) 001 055 (028ndash107) 008
Non-Caucasian 068 (024ndash195) 047
Smoking (yes) 056 (035ndash088) 001 099 (030ndash325) 098
Atherosclerosis (yes) ndash ndash ndash ndash
Hypertension (yes) 115 (077ndash172) 048 112 (038ndash326) 084
Antihypertensive TTT (yes) 204 (139ndash299) lt001 450 (057ndash3555) 015
Dyslipidaemia (yes) 131 (094ndash183) 011 062 (031ndash124) 017
Lipid lowering TTT (yes) 285 (203ndash401) lt001 178 (079ndash400) 016
Obesity (yes) 129 (096ndash173) 010 117 (061ndash225) 063
Neuropathy (yes) 199 (126ndash315) lt001 147 (067ndash324) 033
Retinopathy (yes) 255 (129ndash506) 001 240 (089ndash649) 008
CV disease (yes) ndash ndash ndash ndash
CHD (yes) ndash ndash ndash ndash
Heart failure (yes) 219 (092ndash519) 008 180 (070ndash465) 022
Urogenital disease (yes) 115 (042ndash313) 078 188 (051ndash697) 034
Continuous
Age 10 yr 120 (105ndash138) 001 119 (080ndash177) 040
Duration of DB yr 102 (101ndash104) 001 101 (098ndash104) 054
Number of DB drugs 118 (100ndash140) 006 086 (059ndash125) 042
Body mass index 5 kgm2 112 (099ndash127) 008 115 (086ndash153) 034
Diastolic BP 10 mm Hg 077 (066ndash091) lt001 082 (060ndash110) 019
Systolic BP 10 mm Hg 099 (089ndash111) 089 079 (063ndash101) 006
eGFR 10 mlmin173 m2 092 (084ndash102) 010 078 (059ndash104) 009
LDL mmoll ndash ndash ndash ndash
HDL mmoll 104 (072ndash151) 084 063 (027ndash148) 029
Triglyceride mmoll 099 (082ndash120) 091 097 (064ndash146) 087
HbA1c 096 (085ndash109) 051 120 (091ndash159) 019
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment Too few (4) non-Caucasian participants with CKD stages 3a 3b and 4 to perform a univariateanalysis
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 7 of 12
ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

Results
A total of 109 PCPs from 20 German- or French-speakingcantons participated in the study with a total of 1359 pa-tients included for analysis Detailed geographic distribu-tion of PCP offices has been described previously [11] (fig1)Characteristics of participants according to CKD stage arepresented in table 1 There were a majority of male Cau-casian patients Average age was of 665plusmn124 years (meanplusmn standard deviation) with most (575) in the 60ndash80 yeargroup Mean duration of diabetes was 93 years and meanbody mass index (BMI) 302 kgm2 An eGFR ge60 mlmin was found in 776 of the patients and 139 61
Figure 1 Percentage and number of type 2 diabetic patients en-rolled by cantonZH = Zuumlrich SG = St Gallen GE = Genegraveve Vaud= VD VS = Valais BS = Basel-Stadt BL = Basel-Landschaft GR= Graubuumlnden LU = Luzern TG = Thurgau FR = Freiburg SZ =Schwyz SH = Schaffhausen AG = Aargau OW = Obwalden NE= Neuchacirctel ZG = Zug SO = Solothurn AL = Appenzell
and 24 respectively were in CKD stage 3a 3b and4 Hypertension dyslipidaemia and atherosclerosis werethe three most reported comorbidities present in 8468 and 26 of cases respectively Age duration of di-abetes sex smoking status diastolic blood pressure an-tihypertensive therapy lipid lowering therapy neuropathyretinopathy history of atherosclerosis cerebrovascular dis-ease coronary heart disease and heart failure differed sig-nificantly by CKD stageDetails of antidiabetic antihypertensive lipid loweringand aspirin therapies are presented in Table 2
Treatment and goal attainments
Glycated haemoglobinHbA1c was available for 1357 patients Only 625 ofsubjects were on nonpharmacological therapy The major-ity of subjects were on mono- (377) or dual therapy(383) with a clear preference for metformin (table 2)Mean (plusmn SD) HbA1c was 712 plusmn 122 716 plusmn 113716 plusmn 12 and 718 plusmn 10 respectively in subjects withstage 0ndash2 3a 3b and 4 CKD (table 1) The goal of lt7was reached in 53 of subjects with CKD stage 0ndash2 (andin 488 with CKD stage 3andash4) the goal of lt8 wasreached in 791 of patients with CKD stage 3andash4 Factorsinvolved in HbA1c goal attainment are presented in table3 Nonsmoking status fewer comorbidities increased age
Table 1 Characteristics of participants according to stage of chronic kidney disease (n = 1359)
CKD stageVariable
0ndash2 3a 3b 4
Miss p-value Total
Categorical n ()
Total 1057 (781) 183 (135) 84 (62) 30 (22) 5 1359
Women 430 (407) 81 (443) 45 (536) 19 (633) 2 001 577 (425)
Non-Caucasian 17 (16) 1 (05) 2 (24) 1 (33) 0 053 21 (15)
Smoking (yes) 136 (148) 22 (128) 7 (89) 0 (00) 158 006 165 (137)
Hypertension (yes) 757 (826) 151 (878) 73 (924) 26 (867) 158 006 1201 (841)
Antihypertensive TTT (yes) 782 (740) 165 (902) 77 (917) 29 (967) 0 lt001 1056 (777)
Dyslipidaemia (yes) 630 (688) 110 (640) 56 (709) 23 (767) 158 042 822 (684)
Lipid lowering TTT (yes) 632 (598) 122 (667) 64 (762) 23 (767) 0 lt001 844 (621)
Obesity (yes) 471 (446) 91 (497) 36 (429) 13 (433) 0 059 612 (450)
Neuropathy (yes) 111 (121) 34 (198) 21 (266) 12 (400) 158 lt001 178 (148)
Retinopathy (yes) 52 (57) 18 (105) 11 (139) 4 (133) 158 lt001 85 (71)
Atherosclerosis (yes) 206 (225) 62 (360) 34 (430) 16 (533) 158 lt001 318 (265)
CV disease (yes) 47 (51) 17 (99) 15 (190) 5 (167) 158 lt001 84 (70)
CHD (yes) 147 (160) 45 (262) 23 (291) 13 (433) 158 lt001 228 (190)
Heart failure (yes) 29 (32) 19 (110) 12 (152) 8 (267) 158 lt001 68 (57)
Urogenital disease (yes) 23 (25) 9 (52) 5 (63) 1 (33) 158 010 38 (32)
Continuous (meanplusmnSD)
Age yr 640plusmn119 745plusmn90 768plusmn92 790plusmn94 0 lt001 665plusmn124
Duration of DB yr 89plusmn87 109plusmn97 104plusmn63 125plusmn108 1 lt001 93plusmn88
Number of DB drugs 172plusmn088 160plusmn083 173plusmn094 143plusmn090 0 010 169plusmn088
Body mass index kgm2 302plusmn58 304plusmn53 302plusmn56 303plusmn53 1 055 302plusmn57
Diastolic BP mm Hg 808plusmn99 788plusmn113 778plusmn121 737plusmn92 0 lt001 802plusmn103
Systolic BP mm Hg 136plusmn14 137plusmn15 138plusmn14 138plusmn16 0 011 137plusmn14
eGFR mlmin173 m2 870plusmn153 527plusmn39 374plusmn42 238plusmn44 5 ndash 779plusmn224
LDL mmoll 262plusmn095 266plusmn100 256plusmn125 265plusmn119 394 068 263plusmn098
HDL mmoll 126plusmn040 132plusmn044 124plusmn037 125plusmn044 270 097 127plusmn040
Triglyceride mmoll 198plusmn112 192plusmn100 216plusmn107 192plusmn089 275 061 197plusmn109
HbA1c 712plusmn122 716plusmn113 716plusmn120 718plusmn100 2 040 712plusmn120
BP = blood pressure CHD = coronary heart disease CKD = chronic kidney disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rateHbA1c = glycated haemoglobin HDL = high density lipoprotein LDL = low density lipoprotein Miss = number of missing values SD = standard deviation TTT = treatment p-value for chi-square test of independence for categorical variables for a trend across CKD stages for continuous variables
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 3 of 12
shorter duration of diabetes lower BMI higher HDL-c andimpaired renal function were factors associated with im-proved HbA1c goal attainment Mean HbA1c was 72 inthe group aged lt68 y and 70 in the group aged ge68yand differed significantly (p lt001)
Blood pressureOverall blood pressure values were available for 1359 pa-tients Angiotensin II receptor blockers (ARBs) diureticsand ACE inhibitors (ACEIs) were the most prescribed an-tihypertensive classes (46 457 and 397 respective-ly) followed by beta-blockers and calcium channel block-ers (CCBs) (335 and 316 respectively) (table 2)Among the 262 patients on dual therapy the preferredoption was ARBdiuretic (285) followed by ACEIdi-uretic (197) and ARBCCB (144) Two patients wereon inappropriate ARBACEI therapy With the progression
of CKD stages the number of antihypertensive classes in-creased A total of 2341108 (21) of patients with bloodpressure ge13080 mm Hg were not on antihypertensivetherapy (fig 2) The number of antihypertensive drugs wasthe same in blood pressure goal attainers and nonattainers(160 vs 156 p = 06) In blood pressure goal attainers thenumber of antihypertensive drugs increased with advanc-ing CKD stage (p lt0001) After stratifying for two agegroups mean systolic and diastolic blood pressure were1361 mm Hg and 826 mm Hg respectively in the pa-tients aged lt68 years and 1370 mm Hg and 778 mmHg respectively in those aged ge68 years (median age)for diastolic blood pressure the difference was significant(plt001)Estimated GFR was negatively associated with systolicblood pressure (p lt001) and positively associated withdiastolic blood pressure (plt001) Systolic blood pressuredid not differ by CKD stage however diastolic blood pres-
Table 2 Antidiabetic antihypertensive lipid lowering and aspirin therapies
n
Antidiabetic therapy 1359 100
Healthy way of life 1037 7631
Pharmacological therapy 1274 9375
Metformin 1006 7403
DPP-4 inhibitor 465 3422
Sulphonylurea 279 2053
Glitazone 41 302
Glinide 28 206
Alpha glucosidase inhibitor 4 029
GLP-1 agonist 85 625
Insulin 393 2892
Long acting insulin 273 2009
Short and long acting insulin 182 1339
Number of classes prescribed
0 85 625
1 513 378
2 521 383
3 214 158
4 26 19
Antihypertensive therapy 1056 (777) answers
ACE inhibitor 420 397
Angiotensin receptor blocker 486 460
Calcium antagonist 334 316
Diuretic 483 457
Beta-blocker 354 335
Other 56 53
Number of classes prescribed
1 385 365
2 356 337
3 228 216
4 83 79
5 4 04
Lipid lowering therapy 844 (621) answers
Statin 793 940
Fibrate 18 213
Inhibitor of cholesterol absorption 28 33
Other 39 46
Number of classes prescribed
1 810 960
2 34 40
Aspirin 1066 (784) answers
575 539
ACE = angiotensin converting enzyme DPP-4 = dipeptidyl peptidase-4 GLP-1 = glucagon-like peptide-1
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 4 of 12
sure was lower at advanced CKD stage (nptrend p lt0001table 3) The blood pressure goal of lt13080 mmg Hg wasreached in only 182 of patients Of interest a bloodpressure goal le13080 mmg Hg was reached in 30 of cas-es illustrating a clear digit preference for numbers endingin zeroFactors involved in blood pressure goal attainment are pre-sented in table 4 Presence of atherosclerosis coronaryheart disease and congestive heart disease increased goalattainment Low BMI and low LDL-c levels were factorsassociated with improved blood pressure goal attainment
Figure 2 Number and of anti-hypertensive therapy by chronickidney disease (CKD) stage
Recommendations for blood pressure goals have consid-erably changed recently and have differed between dia-betes or hypertension associations For better clarity fig-ure 3 presents different goals and goal attainments by CKDstage Goal attainment increased with less stringent goalsbut however decreased with more advanced CKD For ex-ample the less stringent ADA 2015 goal of a blood pres-sure lt14090 mm Hg was reached by only 546 519476 40 respectively of patients in CKD stages 0ndash23a 3b and 4 Goal attainment was significantly lower inadvanced CKD
Figure 3 Mean blood pressure and number () of patientsachieving blood pressure goals according to guidelinesADA =American Diabetes Association BP = blood pressure ESH = Eu-ropean Society of Hypertension
Table 3 Odd ratios for glycated haemoglobin goal attainment in univariate analysis (n = 1352)
HbA1c goal attainment
CKD stages 0ndash2(n = 1055) CKD stages 3a 3b and 4(n = 297)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidence interval) p-value
Categorical
Women 108 (084ndash138) 056 090 (051ndash159) 073
Non-Caucasian 048 (018ndash130) 015 025 (003ndash183) 017
Smoking (yes) 051 (035ndash075) lt001 122 (044ndash335) 070
Hypertension (yes) 055 (039ndash078) lt001 120 (049ndash294) 070
Antihypertensive TTT (yes) 058 (044ndash077) lt001 148 (059ndash370) 040
Dyslipidaemia (yes) 079 (060ndash105) 011 070 (037ndash135) 029
Lipid lowering TTT (yes) 068 (053ndash088) lt001 099 (054ndash184) 098
Obesity (yes) 067 (052ndash085) lt001 065 (037ndash114) 013
Neuropathy (yes) 047 (031ndash071) lt001 119 (058ndash241) 064
Retinopathy (yes) 040 (022ndash073) lt001 044 (020ndash098) 004
Atherosclerosis (yes) 078 (057ndash106) 011 113 (062ndash207) 069
CV disease (yes) 082 (046ndash148) 051 063 (028ndash139) 025
CHD (yes) 083 (058ndash118) 031 091 (048ndash173) 078
Heart failure (yes) 182 (084ndash397) 013 096 (041ndash222) 092
Urogenital disease (yes) 049 (021ndash118) 011 100 (027ndash365) 099
Continuous
Age 10 yr 118 (106ndash131) lt001 117 (087ndash158) 030
Duration of DB yr 097 (096ndash099) lt001 097 (095ndash100) 006
Number of DB drugs 044 (037ndash051) lt001 051 (037ndash072) lt001
Body mass index 5 kgm2 088 (079ndash098) 002 082 (064ndash106) 013
Diastolic BP 10 mmHg 093 (082ndash105) 024 076 (059ndash098) 003
Systolic BP 10 mmHg 092 (084ndash100) 005 084 (069ndash102) 008
eGFR 10 mlmin173 m2 089 (082ndash097) lt001 113 (087ndash146) 036
LDL mmoll 096 (083ndash112) 062 123 (085ndash180) 027
HDL mmoll 153 (108ndash217) 002 278 (109ndash714) 003
Triglyceride mmoll 076 (067ndash087) lt001 058 (043ndash079) lt001
HbA1c ndash ndash ndash ndash
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 5 of 12
LipidsOverall LDL-c values were available in 965 patientsAmong the 621 of patients on lipid lowering therapy94 were taking a statin LDL-c values were similaracross CKD stages of (mean plusmn SD) 262 plusmn 095 mmoll266 plusmn 10 mmoll 256 plusmn 125 mmoll and 265 plusmn 119mmoll respectively in subjects with CKD stages 0ndash2 3a3b and 4 (table 1) In patients qualifying for primary pre-vention (n = 473) an LDL-c goal of lt25 mmoll wasreached in 42 (n = 198) of cases For those qualifyingfor secondary prevention (n = 407) an LDL-c goal of lt18mmoll was reached in 32 of cases (n = 130) (fig 4)LDL-c goal attainments did not change across all CKDstages
Figure 4 Mean low-density lipoprotein- cholesterol levels andnumber () of patients achieving goals in primary and secondarypreventionCKD = chronic kidney disease LDL = low-densitylipoprotein
Factors involved in LDL-c goal attainment are presentedin table 5 Gender smoking status and co-morbidities ageduration of diabetes DBP were factors associated with im-proved LDL goal attainment Mean LDL-c was of 276mmoll in patients aged lt68 years and 25 mmoll in thoseaged ge68 years and differed significantly between the twoage groups (p lt001)In this study HbA1c blood pressure and lipid goals wereall achieved in only 30 patients (22) (fig 5) Charac-teristics by goal attainment are available in supplementarytable S1 (appendix)
Discussion
The European prevalence of CKD is rising in diabetic sub-jects [18] and is the leading cause of end-stage renal dis-
Figure 5 Percentage of patients reaching glycated haemoglobinblood pressure and low-density lipoprotein-cholesterol goalsBP =blood pressure CKD = chronic kidney disease stage HbA1c = gly-cated haemoglobin
Table 4 Odd ratios for blood pressure goal attainment in univariate analysis (n = 1354)
Independent variables Odds ratio(95 confidence interval) p-value
Categorical
Women 110 (083ndash145) 052
Non-Caucasian 075 (022ndash256) 064
Smoking (yes) 112 (074ndash171) 058
Hypertension (yes) 048 (033ndash068) lt001
Antihypertensive TTT (yes) 072 (052ndash098) 004
Dyslipidaemia (yes) 116 (084ndash161) 037
Lipid lowering TTT (yes) 109 (082ndash146) 054
Obesity (yes) 058 (044ndash078) lt001
Neuropathy (yes) 158 (108ndash231) 002
Retinopathy (yes) 167 (101ndash279) 005
Atherosclerosis (yes) 164 (120ndash225) lt001
CV disease (yes) 138 (081ndash235) 024
CHD (yes) 213 (152ndash299) lt001
Heart failure (yes) 332 (199ndash553) lt001
Urogenital disease (yes) 086 (035ndash208) 073
Continuous
Age 10 yr 103 (092ndash115) 059
Duration of DB yr 102 (101ndash104) lt001
Number of DB drugs 107 (091ndash125) 041
Body mass index 5 kgm2 078 (069ndash090) lt001
Diastolic BP 10 mmHg ndash ndash
Systolic BP 10 mmHg ndash ndash
eGFR 10 mlmin173 m2 096 (091ndash103) 025
LDL mmoll 074 (062ndash088) lt001
HDL mmoll 077 (052ndash115) 021
Triglyceride mmoll 086 (073ndash101) 006
HbA1c 094 (083ndash106) 030
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 6 of 12
ease (ESRD) The presence of nephropathy considerablyamplifies cardiovascular risk and mortality A multifacto-rial approach is thus necessary to decrease the renal func-tion decline and cardiovascular risk In accordance guide-lines have been released by many societies [1ndash4 19] andthe goal of this study was to examine whether goal attain-ments were reached in a primary care setting in Switzer-landThe average patient age sex distribution HbA1c systolicblood pressure and LDL-c level in this survey was similarto results of other Swiss diabetic surveys [20 21] Our datacan therefore be considered as representative of the Swissdiabetic population To our knowledge this is the first sur-vey analysing the care of Swiss type 2 diabetic patients byCKD stage Overall this study demonstrates that the ma-jority of subjects with type 2 diabetes are men with hy-pertension and lipid abnormalities HbA1c goals are mostoften reached but blood pressure goals are achieved lessfrequently especially in advanced CKD stages Amongthose qualifying for secondary prevention only a thirdreached the recommended LDL-c goalThe demographic characteristics of the population in thissurvey are similar to other studies in Europe in termsof age group sex and ethnicity but differ from the USstudy in which sexes were equally represented and ethnic-ity more diverse [7ndash10]
HbA1c and glycaemic controlIn our study average HbA1c was independent of CKDstage and close to 7 This was similar to the Finnishstudy in which HbA1c ranged between 69 and 73 atCKD stages 2ndash5 [9] Thus Swiss physicians may not dif-ferentiate their goals by CKD stage in spite of KDOQI2012 recommendations [4] Furthermore older subjects(71ndash90 years old) were treated significantly more aggres-sively than younger subjects with an average HbA1c lt7Hence these results highlight the need to improve physi-cian awareness of the risk of hypoglycaemia in CKD andin the elderly [22]Tight glycaemic control is beneficial in the primary pre-vention of nephropathy in type 1 [23 24] and type 2 dia-betes [25ndash27] with a decrease in the incidence of microal-buminuria and progression to macroalbuminuria but itseffect in secondary prevention is less well established In-deed the effect on renal function decline has been demon-strated in type 1 diabetes in the 22-year Diabetes Controland Complications Trial Epidemiology of Diabetes In-terventions and Complications (DCCTEDIC) study [28]and in subjects with type 2 diabetes after 10 years in theUK Prospective Diabetes Study (UKPDS) study [25] Yetboth studies involved intensive glucose control early in thecourse of diabetes The cardiovascular and renal efficacyand safety of tight glycaemic control in type 2 diabetespatients at high cardiovascular risk needs to be careful-
Table 5 Odd ratios for low-density lipoprotein goal attainment in univariate analysis (n = 937)
LDL goal attainment
CKD stages 0ndash2 n = 748) CKD stages 3a 3b and 4(n = 189)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidenceinterval)
p-value
Categorical
Women 067 (049ndash091) 001 055 (028ndash107) 008
Non-Caucasian 068 (024ndash195) 047
Smoking (yes) 056 (035ndash088) 001 099 (030ndash325) 098
Atherosclerosis (yes) ndash ndash ndash ndash
Hypertension (yes) 115 (077ndash172) 048 112 (038ndash326) 084
Antihypertensive TTT (yes) 204 (139ndash299) lt001 450 (057ndash3555) 015
Dyslipidaemia (yes) 131 (094ndash183) 011 062 (031ndash124) 017
Lipid lowering TTT (yes) 285 (203ndash401) lt001 178 (079ndash400) 016
Obesity (yes) 129 (096ndash173) 010 117 (061ndash225) 063
Neuropathy (yes) 199 (126ndash315) lt001 147 (067ndash324) 033
Retinopathy (yes) 255 (129ndash506) 001 240 (089ndash649) 008
CV disease (yes) ndash ndash ndash ndash
CHD (yes) ndash ndash ndash ndash
Heart failure (yes) 219 (092ndash519) 008 180 (070ndash465) 022
Urogenital disease (yes) 115 (042ndash313) 078 188 (051ndash697) 034
Continuous
Age 10 yr 120 (105ndash138) 001 119 (080ndash177) 040
Duration of DB yr 102 (101ndash104) 001 101 (098ndash104) 054
Number of DB drugs 118 (100ndash140) 006 086 (059ndash125) 042
Body mass index 5 kgm2 112 (099ndash127) 008 115 (086ndash153) 034
Diastolic BP 10 mm Hg 077 (066ndash091) lt001 082 (060ndash110) 019
Systolic BP 10 mm Hg 099 (089ndash111) 089 079 (063ndash101) 006
eGFR 10 mlmin173 m2 092 (084ndash102) 010 078 (059ndash104) 009
LDL mmoll ndash ndash ndash ndash
HDL mmoll 104 (072ndash151) 084 063 (027ndash148) 029
Triglyceride mmoll 099 (082ndash120) 091 097 (064ndash146) 087
HbA1c 096 (085ndash109) 051 120 (091ndash159) 019
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment Too few (4) non-Caucasian participants with CKD stages 3a 3b and 4 to perform a univariateanalysis
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 7 of 12
ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

shorter duration of diabetes lower BMI higher HDL-c andimpaired renal function were factors associated with im-proved HbA1c goal attainment Mean HbA1c was 72 inthe group aged lt68 y and 70 in the group aged ge68yand differed significantly (p lt001)
Blood pressureOverall blood pressure values were available for 1359 pa-tients Angiotensin II receptor blockers (ARBs) diureticsand ACE inhibitors (ACEIs) were the most prescribed an-tihypertensive classes (46 457 and 397 respective-ly) followed by beta-blockers and calcium channel block-ers (CCBs) (335 and 316 respectively) (table 2)Among the 262 patients on dual therapy the preferredoption was ARBdiuretic (285) followed by ACEIdi-uretic (197) and ARBCCB (144) Two patients wereon inappropriate ARBACEI therapy With the progression
of CKD stages the number of antihypertensive classes in-creased A total of 2341108 (21) of patients with bloodpressure ge13080 mm Hg were not on antihypertensivetherapy (fig 2) The number of antihypertensive drugs wasthe same in blood pressure goal attainers and nonattainers(160 vs 156 p = 06) In blood pressure goal attainers thenumber of antihypertensive drugs increased with advanc-ing CKD stage (p lt0001) After stratifying for two agegroups mean systolic and diastolic blood pressure were1361 mm Hg and 826 mm Hg respectively in the pa-tients aged lt68 years and 1370 mm Hg and 778 mmHg respectively in those aged ge68 years (median age)for diastolic blood pressure the difference was significant(plt001)Estimated GFR was negatively associated with systolicblood pressure (p lt001) and positively associated withdiastolic blood pressure (plt001) Systolic blood pressuredid not differ by CKD stage however diastolic blood pres-
Table 2 Antidiabetic antihypertensive lipid lowering and aspirin therapies
n
Antidiabetic therapy 1359 100
Healthy way of life 1037 7631
Pharmacological therapy 1274 9375
Metformin 1006 7403
DPP-4 inhibitor 465 3422
Sulphonylurea 279 2053
Glitazone 41 302
Glinide 28 206
Alpha glucosidase inhibitor 4 029
GLP-1 agonist 85 625
Insulin 393 2892
Long acting insulin 273 2009
Short and long acting insulin 182 1339
Number of classes prescribed
0 85 625
1 513 378
2 521 383
3 214 158
4 26 19
Antihypertensive therapy 1056 (777) answers
ACE inhibitor 420 397
Angiotensin receptor blocker 486 460
Calcium antagonist 334 316
Diuretic 483 457
Beta-blocker 354 335
Other 56 53
Number of classes prescribed
1 385 365
2 356 337
3 228 216
4 83 79
5 4 04
Lipid lowering therapy 844 (621) answers
Statin 793 940
Fibrate 18 213
Inhibitor of cholesterol absorption 28 33
Other 39 46
Number of classes prescribed
1 810 960
2 34 40
Aspirin 1066 (784) answers
575 539
ACE = angiotensin converting enzyme DPP-4 = dipeptidyl peptidase-4 GLP-1 = glucagon-like peptide-1
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 4 of 12
sure was lower at advanced CKD stage (nptrend p lt0001table 3) The blood pressure goal of lt13080 mmg Hg wasreached in only 182 of patients Of interest a bloodpressure goal le13080 mmg Hg was reached in 30 of cas-es illustrating a clear digit preference for numbers endingin zeroFactors involved in blood pressure goal attainment are pre-sented in table 4 Presence of atherosclerosis coronaryheart disease and congestive heart disease increased goalattainment Low BMI and low LDL-c levels were factorsassociated with improved blood pressure goal attainment
Figure 2 Number and of anti-hypertensive therapy by chronickidney disease (CKD) stage
Recommendations for blood pressure goals have consid-erably changed recently and have differed between dia-betes or hypertension associations For better clarity fig-ure 3 presents different goals and goal attainments by CKDstage Goal attainment increased with less stringent goalsbut however decreased with more advanced CKD For ex-ample the less stringent ADA 2015 goal of a blood pres-sure lt14090 mm Hg was reached by only 546 519476 40 respectively of patients in CKD stages 0ndash23a 3b and 4 Goal attainment was significantly lower inadvanced CKD
Figure 3 Mean blood pressure and number () of patientsachieving blood pressure goals according to guidelinesADA =American Diabetes Association BP = blood pressure ESH = Eu-ropean Society of Hypertension
Table 3 Odd ratios for glycated haemoglobin goal attainment in univariate analysis (n = 1352)
HbA1c goal attainment
CKD stages 0ndash2(n = 1055) CKD stages 3a 3b and 4(n = 297)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidence interval) p-value
Categorical
Women 108 (084ndash138) 056 090 (051ndash159) 073
Non-Caucasian 048 (018ndash130) 015 025 (003ndash183) 017
Smoking (yes) 051 (035ndash075) lt001 122 (044ndash335) 070
Hypertension (yes) 055 (039ndash078) lt001 120 (049ndash294) 070
Antihypertensive TTT (yes) 058 (044ndash077) lt001 148 (059ndash370) 040
Dyslipidaemia (yes) 079 (060ndash105) 011 070 (037ndash135) 029
Lipid lowering TTT (yes) 068 (053ndash088) lt001 099 (054ndash184) 098
Obesity (yes) 067 (052ndash085) lt001 065 (037ndash114) 013
Neuropathy (yes) 047 (031ndash071) lt001 119 (058ndash241) 064
Retinopathy (yes) 040 (022ndash073) lt001 044 (020ndash098) 004
Atherosclerosis (yes) 078 (057ndash106) 011 113 (062ndash207) 069
CV disease (yes) 082 (046ndash148) 051 063 (028ndash139) 025
CHD (yes) 083 (058ndash118) 031 091 (048ndash173) 078
Heart failure (yes) 182 (084ndash397) 013 096 (041ndash222) 092
Urogenital disease (yes) 049 (021ndash118) 011 100 (027ndash365) 099
Continuous
Age 10 yr 118 (106ndash131) lt001 117 (087ndash158) 030
Duration of DB yr 097 (096ndash099) lt001 097 (095ndash100) 006
Number of DB drugs 044 (037ndash051) lt001 051 (037ndash072) lt001
Body mass index 5 kgm2 088 (079ndash098) 002 082 (064ndash106) 013
Diastolic BP 10 mmHg 093 (082ndash105) 024 076 (059ndash098) 003
Systolic BP 10 mmHg 092 (084ndash100) 005 084 (069ndash102) 008
eGFR 10 mlmin173 m2 089 (082ndash097) lt001 113 (087ndash146) 036
LDL mmoll 096 (083ndash112) 062 123 (085ndash180) 027
HDL mmoll 153 (108ndash217) 002 278 (109ndash714) 003
Triglyceride mmoll 076 (067ndash087) lt001 058 (043ndash079) lt001
HbA1c ndash ndash ndash ndash
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 5 of 12
LipidsOverall LDL-c values were available in 965 patientsAmong the 621 of patients on lipid lowering therapy94 were taking a statin LDL-c values were similaracross CKD stages of (mean plusmn SD) 262 plusmn 095 mmoll266 plusmn 10 mmoll 256 plusmn 125 mmoll and 265 plusmn 119mmoll respectively in subjects with CKD stages 0ndash2 3a3b and 4 (table 1) In patients qualifying for primary pre-vention (n = 473) an LDL-c goal of lt25 mmoll wasreached in 42 (n = 198) of cases For those qualifyingfor secondary prevention (n = 407) an LDL-c goal of lt18mmoll was reached in 32 of cases (n = 130) (fig 4)LDL-c goal attainments did not change across all CKDstages
Figure 4 Mean low-density lipoprotein- cholesterol levels andnumber () of patients achieving goals in primary and secondarypreventionCKD = chronic kidney disease LDL = low-densitylipoprotein
Factors involved in LDL-c goal attainment are presentedin table 5 Gender smoking status and co-morbidities ageduration of diabetes DBP were factors associated with im-proved LDL goal attainment Mean LDL-c was of 276mmoll in patients aged lt68 years and 25 mmoll in thoseaged ge68 years and differed significantly between the twoage groups (p lt001)In this study HbA1c blood pressure and lipid goals wereall achieved in only 30 patients (22) (fig 5) Charac-teristics by goal attainment are available in supplementarytable S1 (appendix)
Discussion
The European prevalence of CKD is rising in diabetic sub-jects [18] and is the leading cause of end-stage renal dis-
Figure 5 Percentage of patients reaching glycated haemoglobinblood pressure and low-density lipoprotein-cholesterol goalsBP =blood pressure CKD = chronic kidney disease stage HbA1c = gly-cated haemoglobin
Table 4 Odd ratios for blood pressure goal attainment in univariate analysis (n = 1354)
Independent variables Odds ratio(95 confidence interval) p-value
Categorical
Women 110 (083ndash145) 052
Non-Caucasian 075 (022ndash256) 064
Smoking (yes) 112 (074ndash171) 058
Hypertension (yes) 048 (033ndash068) lt001
Antihypertensive TTT (yes) 072 (052ndash098) 004
Dyslipidaemia (yes) 116 (084ndash161) 037
Lipid lowering TTT (yes) 109 (082ndash146) 054
Obesity (yes) 058 (044ndash078) lt001
Neuropathy (yes) 158 (108ndash231) 002
Retinopathy (yes) 167 (101ndash279) 005
Atherosclerosis (yes) 164 (120ndash225) lt001
CV disease (yes) 138 (081ndash235) 024
CHD (yes) 213 (152ndash299) lt001
Heart failure (yes) 332 (199ndash553) lt001
Urogenital disease (yes) 086 (035ndash208) 073
Continuous
Age 10 yr 103 (092ndash115) 059
Duration of DB yr 102 (101ndash104) lt001
Number of DB drugs 107 (091ndash125) 041
Body mass index 5 kgm2 078 (069ndash090) lt001
Diastolic BP 10 mmHg ndash ndash
Systolic BP 10 mmHg ndash ndash
eGFR 10 mlmin173 m2 096 (091ndash103) 025
LDL mmoll 074 (062ndash088) lt001
HDL mmoll 077 (052ndash115) 021
Triglyceride mmoll 086 (073ndash101) 006
HbA1c 094 (083ndash106) 030
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 6 of 12
ease (ESRD) The presence of nephropathy considerablyamplifies cardiovascular risk and mortality A multifacto-rial approach is thus necessary to decrease the renal func-tion decline and cardiovascular risk In accordance guide-lines have been released by many societies [1ndash4 19] andthe goal of this study was to examine whether goal attain-ments were reached in a primary care setting in Switzer-landThe average patient age sex distribution HbA1c systolicblood pressure and LDL-c level in this survey was similarto results of other Swiss diabetic surveys [20 21] Our datacan therefore be considered as representative of the Swissdiabetic population To our knowledge this is the first sur-vey analysing the care of Swiss type 2 diabetic patients byCKD stage Overall this study demonstrates that the ma-jority of subjects with type 2 diabetes are men with hy-pertension and lipid abnormalities HbA1c goals are mostoften reached but blood pressure goals are achieved lessfrequently especially in advanced CKD stages Amongthose qualifying for secondary prevention only a thirdreached the recommended LDL-c goalThe demographic characteristics of the population in thissurvey are similar to other studies in Europe in termsof age group sex and ethnicity but differ from the USstudy in which sexes were equally represented and ethnic-ity more diverse [7ndash10]
HbA1c and glycaemic controlIn our study average HbA1c was independent of CKDstage and close to 7 This was similar to the Finnishstudy in which HbA1c ranged between 69 and 73 atCKD stages 2ndash5 [9] Thus Swiss physicians may not dif-ferentiate their goals by CKD stage in spite of KDOQI2012 recommendations [4] Furthermore older subjects(71ndash90 years old) were treated significantly more aggres-sively than younger subjects with an average HbA1c lt7Hence these results highlight the need to improve physi-cian awareness of the risk of hypoglycaemia in CKD andin the elderly [22]Tight glycaemic control is beneficial in the primary pre-vention of nephropathy in type 1 [23 24] and type 2 dia-betes [25ndash27] with a decrease in the incidence of microal-buminuria and progression to macroalbuminuria but itseffect in secondary prevention is less well established In-deed the effect on renal function decline has been demon-strated in type 1 diabetes in the 22-year Diabetes Controland Complications Trial Epidemiology of Diabetes In-terventions and Complications (DCCTEDIC) study [28]and in subjects with type 2 diabetes after 10 years in theUK Prospective Diabetes Study (UKPDS) study [25] Yetboth studies involved intensive glucose control early in thecourse of diabetes The cardiovascular and renal efficacyand safety of tight glycaemic control in type 2 diabetespatients at high cardiovascular risk needs to be careful-
Table 5 Odd ratios for low-density lipoprotein goal attainment in univariate analysis (n = 937)
LDL goal attainment
CKD stages 0ndash2 n = 748) CKD stages 3a 3b and 4(n = 189)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidenceinterval)
p-value
Categorical
Women 067 (049ndash091) 001 055 (028ndash107) 008
Non-Caucasian 068 (024ndash195) 047
Smoking (yes) 056 (035ndash088) 001 099 (030ndash325) 098
Atherosclerosis (yes) ndash ndash ndash ndash
Hypertension (yes) 115 (077ndash172) 048 112 (038ndash326) 084
Antihypertensive TTT (yes) 204 (139ndash299) lt001 450 (057ndash3555) 015
Dyslipidaemia (yes) 131 (094ndash183) 011 062 (031ndash124) 017
Lipid lowering TTT (yes) 285 (203ndash401) lt001 178 (079ndash400) 016
Obesity (yes) 129 (096ndash173) 010 117 (061ndash225) 063
Neuropathy (yes) 199 (126ndash315) lt001 147 (067ndash324) 033
Retinopathy (yes) 255 (129ndash506) 001 240 (089ndash649) 008
CV disease (yes) ndash ndash ndash ndash
CHD (yes) ndash ndash ndash ndash
Heart failure (yes) 219 (092ndash519) 008 180 (070ndash465) 022
Urogenital disease (yes) 115 (042ndash313) 078 188 (051ndash697) 034
Continuous
Age 10 yr 120 (105ndash138) 001 119 (080ndash177) 040
Duration of DB yr 102 (101ndash104) 001 101 (098ndash104) 054
Number of DB drugs 118 (100ndash140) 006 086 (059ndash125) 042
Body mass index 5 kgm2 112 (099ndash127) 008 115 (086ndash153) 034
Diastolic BP 10 mm Hg 077 (066ndash091) lt001 082 (060ndash110) 019
Systolic BP 10 mm Hg 099 (089ndash111) 089 079 (063ndash101) 006
eGFR 10 mlmin173 m2 092 (084ndash102) 010 078 (059ndash104) 009
LDL mmoll ndash ndash ndash ndash
HDL mmoll 104 (072ndash151) 084 063 (027ndash148) 029
Triglyceride mmoll 099 (082ndash120) 091 097 (064ndash146) 087
HbA1c 096 (085ndash109) 051 120 (091ndash159) 019
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment Too few (4) non-Caucasian participants with CKD stages 3a 3b and 4 to perform a univariateanalysis
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 7 of 12
ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12
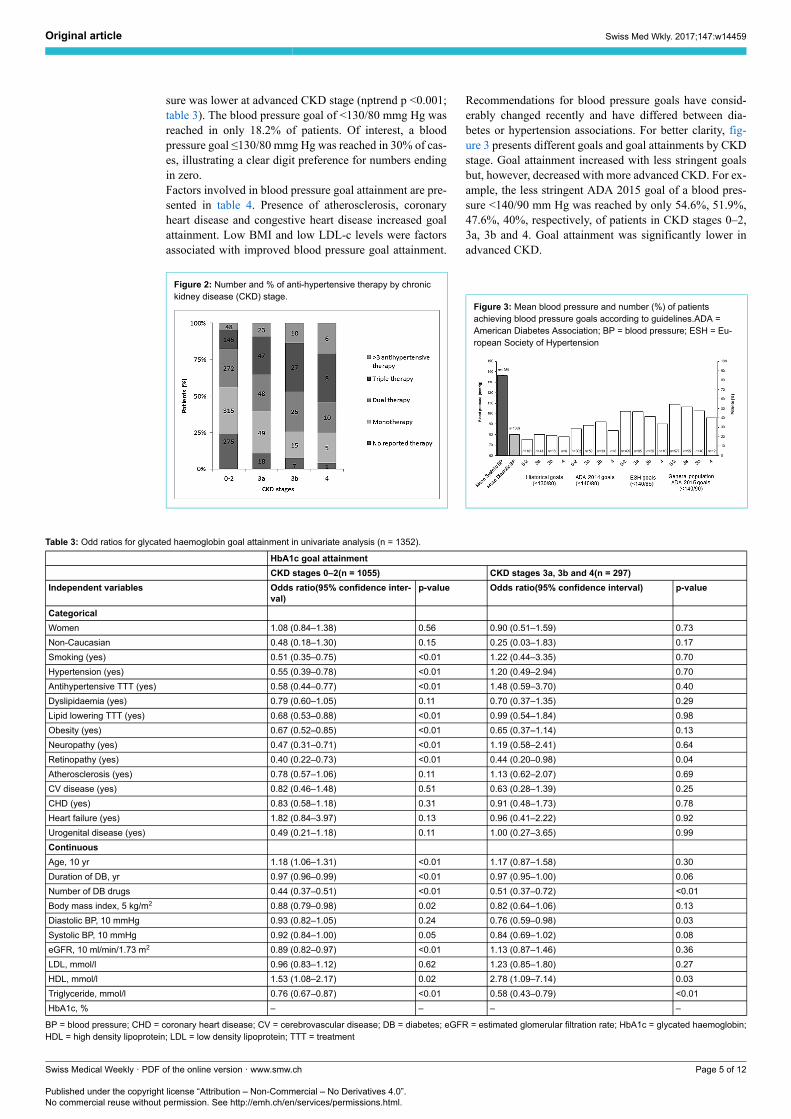
sure was lower at advanced CKD stage (nptrend p lt0001table 3) The blood pressure goal of lt13080 mmg Hg wasreached in only 182 of patients Of interest a bloodpressure goal le13080 mmg Hg was reached in 30 of cas-es illustrating a clear digit preference for numbers endingin zeroFactors involved in blood pressure goal attainment are pre-sented in table 4 Presence of atherosclerosis coronaryheart disease and congestive heart disease increased goalattainment Low BMI and low LDL-c levels were factorsassociated with improved blood pressure goal attainment
Figure 2 Number and of anti-hypertensive therapy by chronickidney disease (CKD) stage
Recommendations for blood pressure goals have consid-erably changed recently and have differed between dia-betes or hypertension associations For better clarity fig-ure 3 presents different goals and goal attainments by CKDstage Goal attainment increased with less stringent goalsbut however decreased with more advanced CKD For ex-ample the less stringent ADA 2015 goal of a blood pres-sure lt14090 mm Hg was reached by only 546 519476 40 respectively of patients in CKD stages 0ndash23a 3b and 4 Goal attainment was significantly lower inadvanced CKD
Figure 3 Mean blood pressure and number () of patientsachieving blood pressure goals according to guidelinesADA =American Diabetes Association BP = blood pressure ESH = Eu-ropean Society of Hypertension
Table 3 Odd ratios for glycated haemoglobin goal attainment in univariate analysis (n = 1352)
HbA1c goal attainment
CKD stages 0ndash2(n = 1055) CKD stages 3a 3b and 4(n = 297)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidence interval) p-value
Categorical
Women 108 (084ndash138) 056 090 (051ndash159) 073
Non-Caucasian 048 (018ndash130) 015 025 (003ndash183) 017
Smoking (yes) 051 (035ndash075) lt001 122 (044ndash335) 070
Hypertension (yes) 055 (039ndash078) lt001 120 (049ndash294) 070
Antihypertensive TTT (yes) 058 (044ndash077) lt001 148 (059ndash370) 040
Dyslipidaemia (yes) 079 (060ndash105) 011 070 (037ndash135) 029
Lipid lowering TTT (yes) 068 (053ndash088) lt001 099 (054ndash184) 098
Obesity (yes) 067 (052ndash085) lt001 065 (037ndash114) 013
Neuropathy (yes) 047 (031ndash071) lt001 119 (058ndash241) 064
Retinopathy (yes) 040 (022ndash073) lt001 044 (020ndash098) 004
Atherosclerosis (yes) 078 (057ndash106) 011 113 (062ndash207) 069
CV disease (yes) 082 (046ndash148) 051 063 (028ndash139) 025
CHD (yes) 083 (058ndash118) 031 091 (048ndash173) 078
Heart failure (yes) 182 (084ndash397) 013 096 (041ndash222) 092
Urogenital disease (yes) 049 (021ndash118) 011 100 (027ndash365) 099
Continuous
Age 10 yr 118 (106ndash131) lt001 117 (087ndash158) 030
Duration of DB yr 097 (096ndash099) lt001 097 (095ndash100) 006
Number of DB drugs 044 (037ndash051) lt001 051 (037ndash072) lt001
Body mass index 5 kgm2 088 (079ndash098) 002 082 (064ndash106) 013
Diastolic BP 10 mmHg 093 (082ndash105) 024 076 (059ndash098) 003
Systolic BP 10 mmHg 092 (084ndash100) 005 084 (069ndash102) 008
eGFR 10 mlmin173 m2 089 (082ndash097) lt001 113 (087ndash146) 036
LDL mmoll 096 (083ndash112) 062 123 (085ndash180) 027
HDL mmoll 153 (108ndash217) 002 278 (109ndash714) 003
Triglyceride mmoll 076 (067ndash087) lt001 058 (043ndash079) lt001
HbA1c ndash ndash ndash ndash
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 5 of 12
LipidsOverall LDL-c values were available in 965 patientsAmong the 621 of patients on lipid lowering therapy94 were taking a statin LDL-c values were similaracross CKD stages of (mean plusmn SD) 262 plusmn 095 mmoll266 plusmn 10 mmoll 256 plusmn 125 mmoll and 265 plusmn 119mmoll respectively in subjects with CKD stages 0ndash2 3a3b and 4 (table 1) In patients qualifying for primary pre-vention (n = 473) an LDL-c goal of lt25 mmoll wasreached in 42 (n = 198) of cases For those qualifyingfor secondary prevention (n = 407) an LDL-c goal of lt18mmoll was reached in 32 of cases (n = 130) (fig 4)LDL-c goal attainments did not change across all CKDstages
Figure 4 Mean low-density lipoprotein- cholesterol levels andnumber () of patients achieving goals in primary and secondarypreventionCKD = chronic kidney disease LDL = low-densitylipoprotein
Factors involved in LDL-c goal attainment are presentedin table 5 Gender smoking status and co-morbidities ageduration of diabetes DBP were factors associated with im-proved LDL goal attainment Mean LDL-c was of 276mmoll in patients aged lt68 years and 25 mmoll in thoseaged ge68 years and differed significantly between the twoage groups (p lt001)In this study HbA1c blood pressure and lipid goals wereall achieved in only 30 patients (22) (fig 5) Charac-teristics by goal attainment are available in supplementarytable S1 (appendix)
Discussion
The European prevalence of CKD is rising in diabetic sub-jects [18] and is the leading cause of end-stage renal dis-
Figure 5 Percentage of patients reaching glycated haemoglobinblood pressure and low-density lipoprotein-cholesterol goalsBP =blood pressure CKD = chronic kidney disease stage HbA1c = gly-cated haemoglobin
Table 4 Odd ratios for blood pressure goal attainment in univariate analysis (n = 1354)
Independent variables Odds ratio(95 confidence interval) p-value
Categorical
Women 110 (083ndash145) 052
Non-Caucasian 075 (022ndash256) 064
Smoking (yes) 112 (074ndash171) 058
Hypertension (yes) 048 (033ndash068) lt001
Antihypertensive TTT (yes) 072 (052ndash098) 004
Dyslipidaemia (yes) 116 (084ndash161) 037
Lipid lowering TTT (yes) 109 (082ndash146) 054
Obesity (yes) 058 (044ndash078) lt001
Neuropathy (yes) 158 (108ndash231) 002
Retinopathy (yes) 167 (101ndash279) 005
Atherosclerosis (yes) 164 (120ndash225) lt001
CV disease (yes) 138 (081ndash235) 024
CHD (yes) 213 (152ndash299) lt001
Heart failure (yes) 332 (199ndash553) lt001
Urogenital disease (yes) 086 (035ndash208) 073
Continuous
Age 10 yr 103 (092ndash115) 059
Duration of DB yr 102 (101ndash104) lt001
Number of DB drugs 107 (091ndash125) 041
Body mass index 5 kgm2 078 (069ndash090) lt001
Diastolic BP 10 mmHg ndash ndash
Systolic BP 10 mmHg ndash ndash
eGFR 10 mlmin173 m2 096 (091ndash103) 025
LDL mmoll 074 (062ndash088) lt001
HDL mmoll 077 (052ndash115) 021
Triglyceride mmoll 086 (073ndash101) 006
HbA1c 094 (083ndash106) 030
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 6 of 12
ease (ESRD) The presence of nephropathy considerablyamplifies cardiovascular risk and mortality A multifacto-rial approach is thus necessary to decrease the renal func-tion decline and cardiovascular risk In accordance guide-lines have been released by many societies [1ndash4 19] andthe goal of this study was to examine whether goal attain-ments were reached in a primary care setting in Switzer-landThe average patient age sex distribution HbA1c systolicblood pressure and LDL-c level in this survey was similarto results of other Swiss diabetic surveys [20 21] Our datacan therefore be considered as representative of the Swissdiabetic population To our knowledge this is the first sur-vey analysing the care of Swiss type 2 diabetic patients byCKD stage Overall this study demonstrates that the ma-jority of subjects with type 2 diabetes are men with hy-pertension and lipid abnormalities HbA1c goals are mostoften reached but blood pressure goals are achieved lessfrequently especially in advanced CKD stages Amongthose qualifying for secondary prevention only a thirdreached the recommended LDL-c goalThe demographic characteristics of the population in thissurvey are similar to other studies in Europe in termsof age group sex and ethnicity but differ from the USstudy in which sexes were equally represented and ethnic-ity more diverse [7ndash10]
HbA1c and glycaemic controlIn our study average HbA1c was independent of CKDstage and close to 7 This was similar to the Finnishstudy in which HbA1c ranged between 69 and 73 atCKD stages 2ndash5 [9] Thus Swiss physicians may not dif-ferentiate their goals by CKD stage in spite of KDOQI2012 recommendations [4] Furthermore older subjects(71ndash90 years old) were treated significantly more aggres-sively than younger subjects with an average HbA1c lt7Hence these results highlight the need to improve physi-cian awareness of the risk of hypoglycaemia in CKD andin the elderly [22]Tight glycaemic control is beneficial in the primary pre-vention of nephropathy in type 1 [23 24] and type 2 dia-betes [25ndash27] with a decrease in the incidence of microal-buminuria and progression to macroalbuminuria but itseffect in secondary prevention is less well established In-deed the effect on renal function decline has been demon-strated in type 1 diabetes in the 22-year Diabetes Controland Complications Trial Epidemiology of Diabetes In-terventions and Complications (DCCTEDIC) study [28]and in subjects with type 2 diabetes after 10 years in theUK Prospective Diabetes Study (UKPDS) study [25] Yetboth studies involved intensive glucose control early in thecourse of diabetes The cardiovascular and renal efficacyand safety of tight glycaemic control in type 2 diabetespatients at high cardiovascular risk needs to be careful-
Table 5 Odd ratios for low-density lipoprotein goal attainment in univariate analysis (n = 937)
LDL goal attainment
CKD stages 0ndash2 n = 748) CKD stages 3a 3b and 4(n = 189)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidenceinterval)
p-value
Categorical
Women 067 (049ndash091) 001 055 (028ndash107) 008
Non-Caucasian 068 (024ndash195) 047
Smoking (yes) 056 (035ndash088) 001 099 (030ndash325) 098
Atherosclerosis (yes) ndash ndash ndash ndash
Hypertension (yes) 115 (077ndash172) 048 112 (038ndash326) 084
Antihypertensive TTT (yes) 204 (139ndash299) lt001 450 (057ndash3555) 015
Dyslipidaemia (yes) 131 (094ndash183) 011 062 (031ndash124) 017
Lipid lowering TTT (yes) 285 (203ndash401) lt001 178 (079ndash400) 016
Obesity (yes) 129 (096ndash173) 010 117 (061ndash225) 063
Neuropathy (yes) 199 (126ndash315) lt001 147 (067ndash324) 033
Retinopathy (yes) 255 (129ndash506) 001 240 (089ndash649) 008
CV disease (yes) ndash ndash ndash ndash
CHD (yes) ndash ndash ndash ndash
Heart failure (yes) 219 (092ndash519) 008 180 (070ndash465) 022
Urogenital disease (yes) 115 (042ndash313) 078 188 (051ndash697) 034
Continuous
Age 10 yr 120 (105ndash138) 001 119 (080ndash177) 040
Duration of DB yr 102 (101ndash104) 001 101 (098ndash104) 054
Number of DB drugs 118 (100ndash140) 006 086 (059ndash125) 042
Body mass index 5 kgm2 112 (099ndash127) 008 115 (086ndash153) 034
Diastolic BP 10 mm Hg 077 (066ndash091) lt001 082 (060ndash110) 019
Systolic BP 10 mm Hg 099 (089ndash111) 089 079 (063ndash101) 006
eGFR 10 mlmin173 m2 092 (084ndash102) 010 078 (059ndash104) 009
LDL mmoll ndash ndash ndash ndash
HDL mmoll 104 (072ndash151) 084 063 (027ndash148) 029
Triglyceride mmoll 099 (082ndash120) 091 097 (064ndash146) 087
HbA1c 096 (085ndash109) 051 120 (091ndash159) 019
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment Too few (4) non-Caucasian participants with CKD stages 3a 3b and 4 to perform a univariateanalysis
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 7 of 12
ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

LipidsOverall LDL-c values were available in 965 patientsAmong the 621 of patients on lipid lowering therapy94 were taking a statin LDL-c values were similaracross CKD stages of (mean plusmn SD) 262 plusmn 095 mmoll266 plusmn 10 mmoll 256 plusmn 125 mmoll and 265 plusmn 119mmoll respectively in subjects with CKD stages 0ndash2 3a3b and 4 (table 1) In patients qualifying for primary pre-vention (n = 473) an LDL-c goal of lt25 mmoll wasreached in 42 (n = 198) of cases For those qualifyingfor secondary prevention (n = 407) an LDL-c goal of lt18mmoll was reached in 32 of cases (n = 130) (fig 4)LDL-c goal attainments did not change across all CKDstages
Figure 4 Mean low-density lipoprotein- cholesterol levels andnumber () of patients achieving goals in primary and secondarypreventionCKD = chronic kidney disease LDL = low-densitylipoprotein
Factors involved in LDL-c goal attainment are presentedin table 5 Gender smoking status and co-morbidities ageduration of diabetes DBP were factors associated with im-proved LDL goal attainment Mean LDL-c was of 276mmoll in patients aged lt68 years and 25 mmoll in thoseaged ge68 years and differed significantly between the twoage groups (p lt001)In this study HbA1c blood pressure and lipid goals wereall achieved in only 30 patients (22) (fig 5) Charac-teristics by goal attainment are available in supplementarytable S1 (appendix)
Discussion
The European prevalence of CKD is rising in diabetic sub-jects [18] and is the leading cause of end-stage renal dis-
Figure 5 Percentage of patients reaching glycated haemoglobinblood pressure and low-density lipoprotein-cholesterol goalsBP =blood pressure CKD = chronic kidney disease stage HbA1c = gly-cated haemoglobin
Table 4 Odd ratios for blood pressure goal attainment in univariate analysis (n = 1354)
Independent variables Odds ratio(95 confidence interval) p-value
Categorical
Women 110 (083ndash145) 052
Non-Caucasian 075 (022ndash256) 064
Smoking (yes) 112 (074ndash171) 058
Hypertension (yes) 048 (033ndash068) lt001
Antihypertensive TTT (yes) 072 (052ndash098) 004
Dyslipidaemia (yes) 116 (084ndash161) 037
Lipid lowering TTT (yes) 109 (082ndash146) 054
Obesity (yes) 058 (044ndash078) lt001
Neuropathy (yes) 158 (108ndash231) 002
Retinopathy (yes) 167 (101ndash279) 005
Atherosclerosis (yes) 164 (120ndash225) lt001
CV disease (yes) 138 (081ndash235) 024
CHD (yes) 213 (152ndash299) lt001
Heart failure (yes) 332 (199ndash553) lt001
Urogenital disease (yes) 086 (035ndash208) 073
Continuous
Age 10 yr 103 (092ndash115) 059
Duration of DB yr 102 (101ndash104) lt001
Number of DB drugs 107 (091ndash125) 041
Body mass index 5 kgm2 078 (069ndash090) lt001
Diastolic BP 10 mmHg ndash ndash
Systolic BP 10 mmHg ndash ndash
eGFR 10 mlmin173 m2 096 (091ndash103) 025
LDL mmoll 074 (062ndash088) lt001
HDL mmoll 077 (052ndash115) 021
Triglyceride mmoll 086 (073ndash101) 006
HbA1c 094 (083ndash106) 030
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 6 of 12
ease (ESRD) The presence of nephropathy considerablyamplifies cardiovascular risk and mortality A multifacto-rial approach is thus necessary to decrease the renal func-tion decline and cardiovascular risk In accordance guide-lines have been released by many societies [1ndash4 19] andthe goal of this study was to examine whether goal attain-ments were reached in a primary care setting in Switzer-landThe average patient age sex distribution HbA1c systolicblood pressure and LDL-c level in this survey was similarto results of other Swiss diabetic surveys [20 21] Our datacan therefore be considered as representative of the Swissdiabetic population To our knowledge this is the first sur-vey analysing the care of Swiss type 2 diabetic patients byCKD stage Overall this study demonstrates that the ma-jority of subjects with type 2 diabetes are men with hy-pertension and lipid abnormalities HbA1c goals are mostoften reached but blood pressure goals are achieved lessfrequently especially in advanced CKD stages Amongthose qualifying for secondary prevention only a thirdreached the recommended LDL-c goalThe demographic characteristics of the population in thissurvey are similar to other studies in Europe in termsof age group sex and ethnicity but differ from the USstudy in which sexes were equally represented and ethnic-ity more diverse [7ndash10]
HbA1c and glycaemic controlIn our study average HbA1c was independent of CKDstage and close to 7 This was similar to the Finnishstudy in which HbA1c ranged between 69 and 73 atCKD stages 2ndash5 [9] Thus Swiss physicians may not dif-ferentiate their goals by CKD stage in spite of KDOQI2012 recommendations [4] Furthermore older subjects(71ndash90 years old) were treated significantly more aggres-sively than younger subjects with an average HbA1c lt7Hence these results highlight the need to improve physi-cian awareness of the risk of hypoglycaemia in CKD andin the elderly [22]Tight glycaemic control is beneficial in the primary pre-vention of nephropathy in type 1 [23 24] and type 2 dia-betes [25ndash27] with a decrease in the incidence of microal-buminuria and progression to macroalbuminuria but itseffect in secondary prevention is less well established In-deed the effect on renal function decline has been demon-strated in type 1 diabetes in the 22-year Diabetes Controland Complications Trial Epidemiology of Diabetes In-terventions and Complications (DCCTEDIC) study [28]and in subjects with type 2 diabetes after 10 years in theUK Prospective Diabetes Study (UKPDS) study [25] Yetboth studies involved intensive glucose control early in thecourse of diabetes The cardiovascular and renal efficacyand safety of tight glycaemic control in type 2 diabetespatients at high cardiovascular risk needs to be careful-
Table 5 Odd ratios for low-density lipoprotein goal attainment in univariate analysis (n = 937)
LDL goal attainment
CKD stages 0ndash2 n = 748) CKD stages 3a 3b and 4(n = 189)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidenceinterval)
p-value
Categorical
Women 067 (049ndash091) 001 055 (028ndash107) 008
Non-Caucasian 068 (024ndash195) 047
Smoking (yes) 056 (035ndash088) 001 099 (030ndash325) 098
Atherosclerosis (yes) ndash ndash ndash ndash
Hypertension (yes) 115 (077ndash172) 048 112 (038ndash326) 084
Antihypertensive TTT (yes) 204 (139ndash299) lt001 450 (057ndash3555) 015
Dyslipidaemia (yes) 131 (094ndash183) 011 062 (031ndash124) 017
Lipid lowering TTT (yes) 285 (203ndash401) lt001 178 (079ndash400) 016
Obesity (yes) 129 (096ndash173) 010 117 (061ndash225) 063
Neuropathy (yes) 199 (126ndash315) lt001 147 (067ndash324) 033
Retinopathy (yes) 255 (129ndash506) 001 240 (089ndash649) 008
CV disease (yes) ndash ndash ndash ndash
CHD (yes) ndash ndash ndash ndash
Heart failure (yes) 219 (092ndash519) 008 180 (070ndash465) 022
Urogenital disease (yes) 115 (042ndash313) 078 188 (051ndash697) 034
Continuous
Age 10 yr 120 (105ndash138) 001 119 (080ndash177) 040
Duration of DB yr 102 (101ndash104) 001 101 (098ndash104) 054
Number of DB drugs 118 (100ndash140) 006 086 (059ndash125) 042
Body mass index 5 kgm2 112 (099ndash127) 008 115 (086ndash153) 034
Diastolic BP 10 mm Hg 077 (066ndash091) lt001 082 (060ndash110) 019
Systolic BP 10 mm Hg 099 (089ndash111) 089 079 (063ndash101) 006
eGFR 10 mlmin173 m2 092 (084ndash102) 010 078 (059ndash104) 009
LDL mmoll ndash ndash ndash ndash
HDL mmoll 104 (072ndash151) 084 063 (027ndash148) 029
Triglyceride mmoll 099 (082ndash120) 091 097 (064ndash146) 087
HbA1c 096 (085ndash109) 051 120 (091ndash159) 019
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment Too few (4) non-Caucasian participants with CKD stages 3a 3b and 4 to perform a univariateanalysis
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 7 of 12
ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

ease (ESRD) The presence of nephropathy considerablyamplifies cardiovascular risk and mortality A multifacto-rial approach is thus necessary to decrease the renal func-tion decline and cardiovascular risk In accordance guide-lines have been released by many societies [1ndash4 19] andthe goal of this study was to examine whether goal attain-ments were reached in a primary care setting in Switzer-landThe average patient age sex distribution HbA1c systolicblood pressure and LDL-c level in this survey was similarto results of other Swiss diabetic surveys [20 21] Our datacan therefore be considered as representative of the Swissdiabetic population To our knowledge this is the first sur-vey analysing the care of Swiss type 2 diabetic patients byCKD stage Overall this study demonstrates that the ma-jority of subjects with type 2 diabetes are men with hy-pertension and lipid abnormalities HbA1c goals are mostoften reached but blood pressure goals are achieved lessfrequently especially in advanced CKD stages Amongthose qualifying for secondary prevention only a thirdreached the recommended LDL-c goalThe demographic characteristics of the population in thissurvey are similar to other studies in Europe in termsof age group sex and ethnicity but differ from the USstudy in which sexes were equally represented and ethnic-ity more diverse [7ndash10]
HbA1c and glycaemic controlIn our study average HbA1c was independent of CKDstage and close to 7 This was similar to the Finnishstudy in which HbA1c ranged between 69 and 73 atCKD stages 2ndash5 [9] Thus Swiss physicians may not dif-ferentiate their goals by CKD stage in spite of KDOQI2012 recommendations [4] Furthermore older subjects(71ndash90 years old) were treated significantly more aggres-sively than younger subjects with an average HbA1c lt7Hence these results highlight the need to improve physi-cian awareness of the risk of hypoglycaemia in CKD andin the elderly [22]Tight glycaemic control is beneficial in the primary pre-vention of nephropathy in type 1 [23 24] and type 2 dia-betes [25ndash27] with a decrease in the incidence of microal-buminuria and progression to macroalbuminuria but itseffect in secondary prevention is less well established In-deed the effect on renal function decline has been demon-strated in type 1 diabetes in the 22-year Diabetes Controland Complications Trial Epidemiology of Diabetes In-terventions and Complications (DCCTEDIC) study [28]and in subjects with type 2 diabetes after 10 years in theUK Prospective Diabetes Study (UKPDS) study [25] Yetboth studies involved intensive glucose control early in thecourse of diabetes The cardiovascular and renal efficacyand safety of tight glycaemic control in type 2 diabetespatients at high cardiovascular risk needs to be careful-
Table 5 Odd ratios for low-density lipoprotein goal attainment in univariate analysis (n = 937)
LDL goal attainment
CKD stages 0ndash2 n = 748) CKD stages 3a 3b and 4(n = 189)
Independent variables Odds ratio(95 confidence inter-val)
p-value Odds ratio(95 confidenceinterval)
p-value
Categorical
Women 067 (049ndash091) 001 055 (028ndash107) 008
Non-Caucasian 068 (024ndash195) 047
Smoking (yes) 056 (035ndash088) 001 099 (030ndash325) 098
Atherosclerosis (yes) ndash ndash ndash ndash
Hypertension (yes) 115 (077ndash172) 048 112 (038ndash326) 084
Antihypertensive TTT (yes) 204 (139ndash299) lt001 450 (057ndash3555) 015
Dyslipidaemia (yes) 131 (094ndash183) 011 062 (031ndash124) 017
Lipid lowering TTT (yes) 285 (203ndash401) lt001 178 (079ndash400) 016
Obesity (yes) 129 (096ndash173) 010 117 (061ndash225) 063
Neuropathy (yes) 199 (126ndash315) lt001 147 (067ndash324) 033
Retinopathy (yes) 255 (129ndash506) 001 240 (089ndash649) 008
CV disease (yes) ndash ndash ndash ndash
CHD (yes) ndash ndash ndash ndash
Heart failure (yes) 219 (092ndash519) 008 180 (070ndash465) 022
Urogenital disease (yes) 115 (042ndash313) 078 188 (051ndash697) 034
Continuous
Age 10 yr 120 (105ndash138) 001 119 (080ndash177) 040
Duration of DB yr 102 (101ndash104) 001 101 (098ndash104) 054
Number of DB drugs 118 (100ndash140) 006 086 (059ndash125) 042
Body mass index 5 kgm2 112 (099ndash127) 008 115 (086ndash153) 034
Diastolic BP 10 mm Hg 077 (066ndash091) lt001 082 (060ndash110) 019
Systolic BP 10 mm Hg 099 (089ndash111) 089 079 (063ndash101) 006
eGFR 10 mlmin173 m2 092 (084ndash102) 010 078 (059ndash104) 009
LDL mmoll ndash ndash ndash ndash
HDL mmoll 104 (072ndash151) 084 063 (027ndash148) 029
Triglyceride mmoll 099 (082ndash120) 091 097 (064ndash146) 087
HbA1c 096 (085ndash109) 051 120 (091ndash159) 019
BP = blood pressure CHD = coronary heart disease CV = cerebrovascular disease DB = diabetes eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobinHDL = high density lipoprotein LDL = low density lipoprotein TTT = treatment Too few (4) non-Caucasian participants with CKD stages 3a 3b and 4 to perform a univariateanalysis
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 7 of 12
ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

ly investigated [26 27] The ACCORD (Action to Con-trol Cardiovascular Risk in Diabetes) ADVANCE (Actionin Diabetes and Vascular Disease Preterax and DiamicronMR Controlled Evaluation) and VADT (Veterans AffairsDiabetes Trial) trials showed an improvement in the pre-vention and progression of albuminuria with tight gly-caemic control but no benefits on renal function declinein high risk subjects with type 2 diabetes and cardiovas-cular disease These studies however excluded subjectswith creatinine levels over 130 to 140 micromoll Eventuallya post hoc analysis of the ADVANCE trial did show a sig-nificant reduction in the risk of ESRD although numberswere low and the number needed to treat (NNT) was 445to prevent one case of ESRD in 5 years [29] This wasrecently confirmed in the ADVANCE-ON follow-up trialwhich found an NNT of 109 for CKD stages 1ndash2 and 393for CKD stages 3 or greater to prevent one case of ESRDover 99 years of follow-up [30] A recent and importantstudy demonstrated a decrease in new onset or worseningof nephropathy in patients with diabetes and establishedcardiovascular disease treated with empagliflozin a sodi-um-glucose cotransporter 2 (SGLT-2) inhibitor [31] Mostexperts agree that the nephroprotection provided by em-pagliflozin is not due to the mild improvement in bloodglucose but to many other hemodynamic and metaboliceffects currently under investigation [32] As SGLT-2 in-hibitors reached the market in mid-2014 no patients in thisstudy were on this treatmentCKD is associated with an increased risk of hypogly-caemia [33] which could increase mortality [34 35] TheACCORD study was prematurely stopped because of in-creased all-cause mortality rate in the intensive interven-tion arm (HbA1c goal lt6) [33] Consequently the KDO-QI clinical practice guidelines published in 2012 recom-mend not targeting an HbA1c of lt7 in CKD patientsat risk of hypoglycaemia [4] Likewise the ADA recom-mends a personalised target based on age comorbiditiesdisease duration life expectancy risk of hypoglycaemiapatient attitude and patient resource [1] In our study goalattainment was obviously easier to reach in CKD stages 3to 4 because it was loosened to lt8
Blood pressureSimilar to the Finnish and Canadian surveys in this surveythe large majority of subjects were hypertensive [9 10] andonly half reached the ADA 2015 goals for blood pressureand even fewer the more stringent ADA 2013 goals pre-vailing during the study [2] Advanced CKD stage was as-sociated with multiple antihypertensive drugs and reducedADA 2015 goal attainment as found in the Finnish popu-lation [9] Last digit preference suggests that PCPs roundmeasured values which can significantly bias the analysisfor goal attainment if lt or le are chosen for blood pressuretarget values This phenomenon has been described whenphysicians use manual as well as automatic blood pressuremeasuring devices [36]Targeting blood pressure levels is a priority in the care ofpatients with type 2 diabetes Reduction in cardiovascularevents with lower blood pressure has been demonstratedin a large number of randomised control trials includingdiabetic patients [37] Tight systolic blood pressure con-trol (le130 mm Hg) decreased stroke and overt nephropa-thy but not all-cause mortality whereas less tight control
(le135 mm Hg) decreased all-cause mortality [38] Otherstudies showed a decrease in the incidence and progressionof nephropathy with systolic blood pressure lt140 mm Hg[39ndash41] Therefore blood pressure goals have been loos-ened from lt13080 mm Hg before 2013 to lt14090 mmHg (or lt13080 mm Hg in case of stage A2ndashA3 albu-minuria) in 2015 [2] Our study demonstrates that despiteloosening of goals only half of patients reach them andmost needed multiple therapies The fact that a fifth of pa-tients not at goal were not on antihypertensive drug thera-py emphasises the problem of medical inertia and the needof continual PCP educationIn our study blockade of the renin angiotensin system withARBs or ACE inhibition and diuretics were clearly the pre-ferred options for antihypertensive therapy The KDIGO2012 and KDOQI recommendations propose an ARB orACEI as first line therapy in diabetic hypertensive subjectswith albuminuria (stage A2 or more) [4 42] Nephropro-tection with irbesartan and losartan has been demonstratedin CKD type 2 diabetic patients independent of blood pres-sure reduction [41 43] Although the KDIGO guidelinesdo not recommend specific second-line therapy amlodip-ine could be preferred to hydrochlorothiazide because ofsuperior efficacy in the reduction of cardiovascular eventsand the progression of CKD in hypertensive subjects athigh cardiovascular risk on ACE inhibition [44] In ourstudy we showed that multiple drug regimens were neededmore with advanced CKD stages as already demonstrat-ed in a cross-sectional observational Swiss survey includ-ing diabetic and CKD patients visiting PCPs [45] Multi-medication and comorbidities are a cause of nonadherenceto treatment [46] which could be improved by single pillcombination therapy and clinical pharmacist evaluation ofadverse effects and drug interactions [45]
LipidsLipid lowering therapy was prescribed in 621 of our pa-tients similarly to the Finnish study [9] and fewer than halfof the patients reached the goal of lt25 mmoll for primaryprevention This rate fell to a third for those qualifying forsecondary prevention Interestingly CKD was not a limit-ing factor for lipid goal attainment Better results were re-ported in the Canadian survey with 82 of type 2 diabet-ic patients taking lipid-lowering therapy and 57 attainingthe defined LDL-c goal of le20 mmoll [10] To explainthese low rates of success low adherence to treatment pa-tient education andor limited access to medical care werehighlighted Likewise in a Swiss survey including 197of diabetics diabetes was a predictor for treatment non-adherence Also although diabetes was as a positive pre-dictor for diagnostic adherence it was not a predictor foroverall guideline adherence highlighting the difficulty inreaching lipid treatment goals in diabetes [47]Patients with diabetes and CKD represent a very high car-diovascular risk group [48 49] The Study of Heart andRenal Protection (SHARP) demonstrated a decrease in car-diovascular events for stage 3andash5 CKD patients who wereon statinezetimibe combination therapy However no sig-nificant effect was observed for mortality or the progres-sion of renal disease [50] Statin or statinezetimibe com-bination is recommended as the first line LDL-c therapyregardless of the baseline values in nondialysis diabeticCKD patients [2 51] Current recommendations for pa-
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 8 of 12
tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

tients with diabetes and CKD do not specify any LDL-cgoal [2 51] However after initiating lipid lowering thera-py measuring LDL-c is optional to assess patient drug ad-herence Doses of lipid lowering agents should be adaptedto renal function as side effects are more prevalent and se-rious in this population [52]Interestingly this study showed that patients aged gt68years have significantly lower levels of LDL-c comparedwith younger patients An Italian survey among diabeticCKD patients also showed that LDL-c goal was attainedless often by younger adults than older adults [8] Drug ad-herence is known to be lowest in younger adults specif-ically in younger men Recently another Italian surveydemonstrated a higher all-cause mortality and cardiovascu-lar mortality in younger (lt75 years) CKD diabetic patients[53] which may be due to a difficulty in reaching goals forcardiovascular risk factors in this younger population Thiswill need further investigation
Limitations of the studyAs our sampling method was not truly random (ie ran-domly choosing participating physicians) but based on thewillingness of physicians to participate to the study thesample studied may not be representative of the populationas found in a population-based cohort study We cannot ex-clude the possibility that physicians agreeing to participatein the study were more compliant with current recommen-dations than those who refused Furthermore patients se-lected for the data collection obviously represent a groupmore adherent to visits to physician offices and men in thiscase may be underrepresented This may have created aconsiderable bias in selection The observational design ofthis study does not allow the reasons why targets were notachieved to be identified Finally in this study it was notpossible to differentiate between non-CKD patients andpatients with CKD stage 1 to 2 because of insufficient re-porting of albuminuria Devices for blood pressure mea-surements and the number of blood pressure measurementswere not standardised Because of the known white coateffect the percentage of patients attaining blood pressuregoals might have been underestimated Laboratory mea-surements were not standardised and based on single val-uesIdeally the results of this study should be compared withthose found in a population-based cohort study Further-more barriers to patient and physician compliance shouldbe assessed in order to implement strategies to improvegoal attainments
Conclusion
This cross-sectional study demonstrates that blood pres-sure and lipid goal attainments are less often achieved thanblood glucose control in type 2 diabetic patients followedup by PCPs in Switzerland Reaching all goals current in2013 was close to impossible Goal attainments for HbA1cand LDL-c were not influenced by CKD stage HbA1cand LDL-c were less well controlled in younger individu-als There is a need for improvement in cardiovascular riskcontrol in the younger population blood pressure controlin advanced CKD whereas HbA1c goals may be loosenedin the elderly and in advanced CKD
Disclosure statementThis study was supported by Boehringer Ingelheim and Lilly for thelogistics of data collection but not for data analysis and manuscriptpreparation which was performed independently by the authors Par-ticipating physicians received 30 CHF per included patient to cover thetime of data collection
References1 American Diabetes Association (6) Glycemic targets Diabetes Care
2015(Suppl_1)S33ndash40 httpdxdoiorg102337dc15-S009 PubMed2 American Diabetes Association (8) Cardiovascular disease and risk
management Diabetes Care 2015(Suppl_1)S49ndash57 httpdxdoiorg102337dc15-S011 PubMed
3 Rydeacuten L Grant PJ Anker SD Berne C Cosentino F Danchin N et althe Task Force on diabetes pre-diabetes and cardiovascular diseases ofthe European Society of Cardiology (ESC) and developed in collabora-tion with the European Association for the Study of Diabetes (EASD)ESC Guidelines on diabetes pre-diabetes and cardiovascular diseasesdeveloped in collaboration with the EASD Eur Heart J2013(39)3035ndash87 Available at httpdxdoiorg101093eurheartjeht108 PubMed
4 National Kidney Foundation KDOQI Clinical Practice Guideline forDiabetes and CKD 2012 Update Am J Kidney Dis 2012(5)850ndash86httpdxdoiorg101053jajkd201207005 PubMed
5 KDIGO Board KDIGO 2012 Clinical Practice Guideline for the Evalu-ation and Management of Chronic Kidney Disease Kidney Int 2013(1suppl)1ndash150
6 Gaede P Vedel P Larsen N Jensen GV Parving HH Pedersen O Mul-tifactorial intervention and cardiovascular disease in patients with type 2diabetes N Engl J Med 2003(5)383ndash93 httpdxdoiorg101056NE-JMoa021778 PubMed
7 Rao DT Sunio LK Lo YJ Gossain VV Comparison of the adherenceto the american diabetes association guidelines of diabetes care in pri-mary care and subspecialty clinics J Diabetes Metab Disord2015(1)35 httpdxdoiorg101186s40200-015-0158-x PubMed
8 De Cosmo S Viazzi F Pacilli A Giorda C Ceriello A Gentile S et alAMD-Annals Study Group Achievement of therapeutic targets in pa-tients with diabetes and chronic kidney disease insights from the Asso-ciazione Medici Diabetologi Annals initiative Nephrol Dial Transplant2015(9)1526ndash33 httpdxdoiorg101093ndtgfv101 PubMed
9 Metsaumlrinne K Broumlijersen A Kantola I Niskanen L Rissanen A Appel-roth T et al STages of NEphropathy inType 2 Diabetes Study Investi-gators High prevalence of chronic kidney disease in Finnish patientswith type 2 diabetes treated in primary care Prim Care Diabetes2015(1)31ndash8 httpdxdoiorg101016jpcd201406001 PubMed
10 Leiter LA Berard L Bowering CK Cheng AY Dawson KG Ekoeacute JMet al Type 2 diabetes mellitus management in Canada is it improvingCan J Diabetes 2013(2)82ndash9 httpdxdoiorg101016jjcjd201302055 PubMed
11 Lamine F Lalubin F Pitteloud N Burnier M Zanchi A Chronic kidneydisease in type 2 diabetic patients followed-up by primary care physi-cians in Switzerland prevalence and prescription of antidiabetic drugsSwiss Med Wkly 2016w14282 PubMed
12 American Diabetes Association Standards of medical care in dia-betes--2013 Diabetes Care 2013(Suppl 1)S11ndash66 httpdxdoiorg102337dc13-S011 PubMed
13 Swiss Society of Hypertension (SSH) Guidelines 2009httpwwwswisshypertensionchguidelineshtm
14 Fox CS Golden SH Anderson C Bray GA Burke LE de Boer IH etal American Heart Association Diabetes Committee of the Council onLifestyle and Cardiometabolic Health Council on Clinical CardiologyCouncil on Cardiovascular and Stroke Nursing Council on Cardiovas-cular Surgery and Anesthesia Council on Quality of Care and OutcomesResearch American Diabetes Association Update on Prevention of Car-diovascular Disease in Adults With Type 2 Diabetes Mellitus in Light ofRecent Evidence A Scientific Statement From the American Heart As-sociation and the American Diabetes Association Diabetes Care2015(9)1777ndash803 httpdxdoiorg102337dci15-0012 PubMed
15 Mancia G Fagard R Narkiewicz K Redon J Zanchetti A Boumlhm M etal 2013 ESHESC guidelines for the management of arterial hyperten-sion the Task Force for the Management of Arterial Hypertension of theEuropean Society of Hypertension (ESH) and of the European Societyof Cardiology (ESC) Eur Heart J 2013(28)2159ndash219httpdxdoiorg101093eurheartjeht151 PubMed
16 Reiner Z Catapano AL De Backer G Graham I Taskinen MR Wik-lund O et al European Association for Cardiovascular Prevention ampRehabilitation ESC Committee for Practice Guidelines (CPG)2008-2010 and 2010-2012 Committees ESCEAS Guidelines for the
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 9 of 12
management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

management of dyslipidaemias the Task Force for the management ofdyslipidaemias of the European Society of Cardiology (ESC) and theEuropean Atherosclerosis Society (EAS) Eur Heart J2011(14)1769ndash818 Available at httpdxdoiorg101093eurheartjehr158 PubMed
17 Cuzick J A Wilcoxon-type test for trend Stat Med 1985(1)87ndash90httpdxdoiorg101002sim4780040112 PubMed
18 Kainz A Hronsky M Stel VS Jager KJ Geroldinger A Dunkler D etal Prediction of prevalence of chronic kidney disease in diabetic pa-tients in countries of the European Union up to 2025 Nephrol DialTransplant 2015(Suppl 4)iv113ndash8 httpdxdoiorg101093ndtgfv073 PubMed
19 Bilo H Coentrao L Couchoud C Covic A De Sutter J Drechsler C etal Guideline development group Clinical Practice Guideline on man-agement of patients with diabetes and chronic kidney disease stage 3b orhigher (eGFR lt45 mLmin) Nephrol Dial Transplant 2015(Suppl2)ii1ndash142 httpdxdoiorg101093ndtgfv100 PubMed
20 Frei A Herzog S Woitzek K Held U Senn O Rosemann T et al Char-acteristics of poorly controlled Type 2 diabetes patients in Swiss primarycare Cardiovasc Diabetol 2012(1)70 httpdxdoiorg1011861475-2840-11-70 PubMed
21 Kaiser A Vollenweider P Waeber G Marques-Vidal P Prevalenceawareness and treatment of type 2 diabetes mellitus in Switzerland theCoLaus study Diabet Med 2012(2)190ndash7 httpdxdoiorg101111j1464-5491201103422x PubMed
22 Bodmer M Meier C Kraumlhenbuumlhl S Jick SS Meier CR Metformin sul-fonylureas or other antidiabetes drugs and the risk of lactic acidosis orhypoglycemia a nested case-control analysis Diabetes Care2008(11)2086ndash91 httpdxdoiorg102337dc08-1171 PubMed
23 Nathan DM Genuth S Lachin J Cleary P Crofford O Davis M et alDiabetes Control and Complications Trial Research Group The effect ofintensive treatment of diabetes on the development and progression oflong-term complications in insulin-dependent diabetes mellitus N EnglJ Med 1993(14)977ndash86 httpdxdoiorg101056NE-JM199309303291401 PubMed
24 de Boer IH Rue TC Cleary PA Lachin JM Molitch ME Steffes MWet al Diabetes Control and Complications TrialEpidemiology of Dia-betes Interventions and Complications Study Research Group Long-term renal outcomes of patients with type 1 diabetes mellitus and mi-croalbuminuria an analysis of the Diabetes Control and ComplicationsTrialEpidemiology of Diabetes Interventions and Complications cohortArch Intern Med 2011(5)412ndash20 httpdxdoiorg101001archintern-med201116 PubMed
25 UK Prospective Diabetes Study (UKPDS) Group Intensive blood-glu-cose control with sulphonylureas or insulin compared with conventionaltreatment and risk of complications in patients with type 2 diabetes(UKPDS 33) Lancet 1998(9131)837ndash53 httpdxdoiorg101016S0140-6736(98)07019-6 PubMed
26 Ismail-Beigi F Craven T Banerji MA Basile J Calles J Cohen RM etal ACCORD trial group Effect of intensive treatment of hypergly-caemia on microvascular outcomes in type 2 diabetes an analysis of theACCORD randomised trial Lancet 2010(9739)419ndash30httpdxdoiorg101016S0140-6736(10)60576-4 PubMed
27 Patel A MacMahon S Chalmers J Neal B Billot L Woodward M etal ADVANCE Collaborative Group Intensive blood glucose controland vascular outcomes in patients with type 2 diabetes N Engl J Med2008(24)2560ndash72 httpdxdoiorg101056NEJMoa0802987PubMed
28 de Boer IH Sun W Cleary PA Lachin JM Molitch ME Steffes MW etal DCCTEDIC Research Group Intensive diabetes therapy andglomerular filtration rate in type 1 diabetes N Engl J Med2011(25)2366ndash76 httpdxdoiorg101056NEJMoa1111732PubMed
29 Shurraw S Tonelli M Intensive glycemic control in type 2 diabetics athigh cardiovascular risk do the benefits justify the risks Kidney Int2013(3)346ndash8 httpdxdoiorg101038ki2012431 PubMed
30 Wong MG Perkovic V Chalmers J Woodward M Li Q Cooper ME etal ADVANCE-ON Collaborative Group Long-term Benefits of Inten-sive Glucose Control for Preventing End-Stage Kidney Disease AD-VANCE-ON Diabetes Care 2016(5)694ndash700 httpdxdoiorg102337dc15-2322 PubMed
31 Wanner C Inzucchi SE Lachin JM Fitchett D von Eynatten MMattheus M et al EMPA-REG OUTCOME Investigators Em-pagliflozin and Progression of Kidney Disease in Type 2 Diabetes NEngl J Med 2016(4)323ndash34 httpdxdoiorg101056NEJ-Moa1515920 PubMed
32 Heerspink HJ Perkins BA Fitchett DH Husain M Cherney DZ Sodi-um Glucose Cotransporter 2 Inhibitors in the Treatment of DiabetesMellitus Cardiovascular and Kidney Effects Potential Mechanisms and
Clinical Applications Circulation 2016(10)752ndash72 httpdxdoiorg101161CIRCULATIONAHA116021887 PubMed
33 Miller ME Bonds DE Gerstein HC Seaquist ER Bergenstal RMCalles-Escandon J et al ACCORD Investigators The effects of base-line characteristics glycaemia treatment approach and glycated haemo-globin concentration on the risk of severe hypoglycaemia post hoc epi-demiological analysis of the ACCORD study BMJ 2010(jan081)b5444 httpdxdoiorg101136bmjb5444 PubMed
34 Bonds DE Miller ME Bergenstal RM Buse JB Byington RP CutlerJA et al The association between symptomatic severe hypoglycaemiaand mortality in type 2 diabetes retrospective epidemiological analysisof the ACCORD study BMJ 2010(jan08 1)b4909 httpdxdoiorg101136bmjb4909 PubMed
35 McCoy RG Van Houten HK Ziegenfuss JY Shah ND Wermers RASmith SA Increased mortality of patients with diabetes reporting severehypoglycemia Diabetes Care 2012(9)1897ndash901 httpdxdoiorg102337dc11-2054 PubMed
36 Burnier M Gasser UE End-digit preference in general practice a com-parison of the conventional auscultatory and electronic oscillometricmethods Blood Press 2008(2)104ndash9 httpdxdoiorg10108008037050801972881 PubMed
37 Law MR Morris JK Wald NJ Use of blood pressure lowering drugs inthe prevention of cardiovascular disease meta-analysis of 147 ran-domised trials in the context of expectations from prospective epidemio-logical studies BMJ 2009(may19 1)b1665 httpdxdoiorg101136bmjb1665 PubMed
38 Bangalore S Kumar S Lobach I Messerli FH Blood pressure targets insubjects with type 2 diabetes mellitusimpaired fasting glucose observa-tions from traditional and bayesian random-effects meta-analyses of ran-domized trials Circulation 2011(24)2799ndash810 9 810httpdxdoiorg101161CIRCULATIONAHA110016337 PubMed
39 UK Prospective Diabetes Study Group Tight blood pressure control andrisk of macrovascular and microvascular complications in type 2 dia-betes UKPDS 38 BMJ 1998(7160)703ndash13 httpdxdoiorg101136bmj3177160703 PubMed
40 Zoungas S de Galan BE Ninomiya T Grobbee D Hamet P Heller S etal ADVANCE Collaborative Group Combined effects of routine bloodpressure lowering and intensive glucose control on macrovascular andmicrovascular outcomes in patients with type 2 diabetes New resultsfrom the ADVANCE trial Diabetes Care 2009(11)2068ndash74httpdxdoiorg102337dc09-0959 PubMed
41 Bakris GL Weir MR Shanifar S Zhang Z Douglas J van Dijk DJ etal RENAAL Study Group Effects of blood pressure level on progres-sion of diabetic nephropathy results from the RENAAL study Arch In-tern Med 2003(13)1555ndash65 httpdxdoiorg101001arch-inte163131555 PubMed
42 Chapter 4 Blood pressure management in CKD ND patients with dia-betes mellitus Kidney Int Suppl (2011) 2012(5)363ndash9httpdxdoiorg101038kisup201254 PubMed
43 Lewis EJ Hunsicker LG Clarke WR Berl T Pohl MA Lewis JB et alCollaborative Study Group Renoprotective effect of the angiotensin-re-ceptor antagonist irbesartan in patients with nephropathy due to type 2diabetes N Engl J Med 2001(12)851ndash60 httpdxdoiorg101056NEJMoa011303 PubMed
44 Bakris GL Sarafidis PA Weir MR Dahloumlf B Pitt B Jamerson K et alACCOMPLISH Trial investigators Renal outcomes with differentfixed-dose combination therapies in patients with hypertension at highrisk for cardiovascular events (ACCOMPLISH) a prespecified sec-ondary analysis of a randomised controlled trial Lancet2010(9721)1173ndash81 httpdxdoiorg101016S0140-6736(09)62100-0 PubMed
45 Roas S Bernhart F Schwarz M Kaiser W Noll G Antihypertensivecombination therapy in primary care offices results of a cross-sectionalsurvey in Switzerland Int J Gen Med 2014549ndash56 PubMed
46 Stemer G Zehetmayer S Lemmens-Gruber R Evaluation of risk factormanagement of patients treated on an internal nephrology ward a pilotstudy BMC Clin Pharmacol 2009(1)15 httpdxdoiorg1011861472-6904-9-15 PubMed
47 Bally K Martina B Halter U Isler R Tschudi P Barriers to Swissguideline-recommended cholesterol management in general practiceSwiss Med Wkly 2010(19-20)280ndash5 PubMed
48 Fox CS Matsushita K Woodward M Bilo HJ Chalmers J HeerspinkHJ et al Chronic Kidney Disease Prognosis Consortium Associationsof kidney disease measures with mortality and end-stage renal disease inindividuals with and without diabetes a meta-analysis Lancet2012(9854)1662ndash73 httpdxdoiorg101016S0140-6736(12)61350-6 PubMed
49 Tonelli M Muntner P Lloyd A Manns BJ Klarenbach S Pannu N etal Alberta Kidney Disease Network Risk of coronary events in people
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 10 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12
with chronic kidney disease compared with those with diabetes a popu-lation-level cohort study Lancet 2012(9844)807ndash14 httpdxdoiorg101016S0140-6736(12)60572-8 PubMed
50 Baigent C Landray MJ Reith C Emberson J Wheeler DC Tomson Cet al SHARP Investigators The effects of lowering LDL cholesterolwith simvastatin plus ezetimibe in patients with chronic kidney disease(Study of Heart and Renal Protection) a randomised placebo-controlledtrial Lancet 2011(9784)2181ndash92 httpdxdoiorg101016S0140-6736(11)60739-3 PubMed
51 Wanner C Tonelli M Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members KDIGO ClinicalPractice Guideline for Lipid Management in CKD summary of recom-
mendation statements and clinical approach to the patient Kidney Int2014(6)1303ndash9 httpdxdoiorg101038ki201431 PubMed
52 Tonelli M Wanner C Kidney Disease Improving Global OutcomesLipid Guideline Development Work Group Members Lipid manage-ment in chronic kidney disease synopsis of the Kidney Disease Im-proving Global Outcomes 2013 clinical practice guideline Ann InternMed 2014(3)182ndash9 httpdxdoiorg107326M13-2453 PubMed
53 Tancredi M Rosengren A Svensson AM Kosiborod M Pivodic AGudbjoumlrnsdottir S et al Excess Mortality among Persons with Type 2Diabetes N Engl J Med 2015(18)1720ndash32 httpdxdoiorg101056NEJMoa1504347 PubMed
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 11 of 12
Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12

Appendix Supplementary table
Table S1 Patient characteristics by goal attainment
Hba1c goal attained BP goal attained LDL goal attained
Independent variables No Yes No Yes No Yes
Categorical
Total 557 795 1110 249 607 332
Women 228 346 467 110 280 116
Men 329 449 643 139 327 216
Continuous
Age yr 641plusmn120 683plusmn123 664plusmn120 667plusmn137 670plusmn126 682plusmn104
Body mass index kgm2 307plusmn 53 299plusmn 59 305plusmn 57 290plusmn 55 299plusmn 58 307plusmn 57
Diastolic BP mm Hg 81plusmn10 79plusmn 10 82plusmn 10 70plusmn 6 80plusmn 10 78plusmn10
Systolic BP mm Hg 138plusmn15 136plusmn14 140plusmn12 119plusmn7 136plusmn14 136plusmn14
eGFR mlmin173 m2 835plusmn205 738plusmn228 782plusmn222 764plusmn231 777plusmn225 790plusmn207
LDL mmoll 263plusmn102 263plusmn095 268plusmn100 241plusmn086 314plusmn082 171plusmn045
HDL mmoll 122plusmn040 130plusmn041 127plusmn041 124plusmn037 128plusmn037 126plusmn046
Triglyceride mmoll 218plusmn117 184plusmn102 200plusmn110 184plusmn106 183plusmn074 182plusmn083
HbA1c 818plusmn110 639plusmn055 714plusmn123 704plusmn110 704plusmn121 704plusmn110
BP = blood pressure eGFR = estimated glomerular filtration rate HbA1c = glycated haemoglobin HDL = high-density lipoprotein LDL = low-density lipoprotein
Original article Swiss Med Wkly 2017147w14459
Swiss Medical Weekly middot PDF of the online version middot wwwsmwch
Published under the copyright license ldquoAttribution ndash Non-Commercial ndash No Derivatives 40rdquoNo commercial reuse without permission See httpemhchenservicespermissionshtml
Page 12 of 12