-
Gluteus Maximus Preactivation Using
a Thera-Band Alters Gluteus Maximus
Muscle Activity and the Anterior Pelvic
Tilt Angle During Bridging Exercise
Silah Choi
The Graduate School
Yonsei University
Department of Physical Therapy
-
Gluteus Maximus Preactivation Using
a Thera-Band Alters Gluteus Maximus
Muscle Activity and the Anterior Pelvic
Tilt Angle During Bridging Exercise
Silah Choi
The Graduate School
Yonsei University
Department of Physical Therapy
-
Gluteus Maximus Preactivation Using
a Thera-Band Alters Gluteus Maximus
Muscle Activity and the Anterior Pelvic
Tilt Angle During Bridging Exercise
A Masters Thesis Submitted to the Department of Physical
Therapy
and the Graduate School of Yonsei University in partial
fulfillment of the requirements
for the degree of Master of Science
Silah Choi
December 2013
-
This certifies that the masters thesis of Silah Choi is
approved.
Thesis Supervisor: Heonseock Cynn
Ohyun Kwon: Thesis Committee Member #1
Chunghwi Yi: Thesis Committee Member #2
The Graduate School Yonsei University
December 2013
-
Acknowledgements
First, I would like to express my gratitude to my supervisor,
Professor Heonseock
Cynn. He continuously gave me confidence and always supported
me. He devoted a
great deal of time to discussing and sharing opinions about my
research. With his
assistance and encouragement, I was able to improve my research
and expand my
knowledge. His inspiration exceeded the academic aspects of my
life; he also taught
me to have a sense of responsibility and to consider principles
and beliefs in order to
become a respectable person. I feel honored to have met him and
I am delighted to
have been his student.
I would also like to thank my thesis committee members.
Professor Chunghwi Yi
helped to improve the quality of my thesis with his detailed and
insightful comments.
He always treated me with kindness and made me feel very
comfortable in my school
life. Professor Ohyun Kwon offered me opportunities to obtain
experience in the
clinical field and taught me practical skills and scientific
methods. He also took the
time to listen to my vision for the future and provide sincere
advice. He was
tremendous help in designing my future and furthering my
self-development. I would
also like to express my deep appreciation to Professor Sanghyun
Cho, Professor
Hyeseon Jeon, and Professor Sunghyun Yu for their
thoughtfulness, encouragement,
and assistance during my master’s course.
-
I would like to thank all the members of the applied kinesiology
and ergonomic
technology laboratory: Taelim Yoon, Jihyun Lee, Kyungmi Park,
Woojeong Choi,
Changhee Ko, and Hyojeong Jung. In their kindness, they have
been like sisters and
brothers to me, cheering me on, working together, and sharing
discussions. Their
heartfelt advice and intellectual support encouraged me to
complete my master’s
course. I would also like to express my gratitude to all members
of the graduate
school, department of physical therapy, who were always kind and
caring in daily
life—especially when I needed help with my research. I will have
many happy
memories of Sungdae Choung, Onebin Lim, and Sunyoung Kang, who
continuously
motivated me and helped me to adapt to school life from
beginning to end.
Additionally, I want to thank all of my junior colleagues who
participated in my
research, helped me to carry out data collection, and empathized
with me.
Finally, I thank my family. They have shown me infinite love and
support. It would
have been impossible for me to finish this work without my
family. I promise to
reward you with good achievements. I love you very much.
Although my grandfather
is no longer on this earth, he would have been very happy and
proud of my
accomplishments. I miss you.
I could not have completed my thesis without the contribution
and encouragement
of many people. I deeply appreciate all those who made this work
possible. Please
know that I will continue to thirst for knowledge and develop my
skills.
Thank you.
-
-i-
Table of Contents
List of Figures
························································································
iii
List of Tables
·························································································
iv
Abstract
··································································································
v
Introduction
·····························································································
1
Methods
··································································································
4
1. Subjects
···························································································
4
2. Instrumentation
················································································
6
2.1 Surface Electromyography
························································· 6
3. Experimental Procedures
·································································
8
3.1 Bridging Without Isometric Hip Abduction
································ 9
3.2 Bridging With Isometric Hip Abduction
··································· 12
3.3 Measurement of Anterior Pelvic Tilt Angle
······························ 14
4. Statistical Analysis
········································································
16
Results
··································································································
17
1. Subjects
·························································································
17
2 Electromyographic Data
·································································
18
2.1 Gluteus Maximus, Hamstrings, and Erector Spinae Muscle
Activity
····································································································
18
2.2 Gluteus Maximus/Hamstrings and Gluteus Maximus/Erector
Spinae
Muscle Activity Ratios
·······························································
20
-
-ii-
2.3 Anterior Pelvic Tilt Angle
·························································· 21
Discussion
·····························································································
23
Conclusion
····························································································
29
References
····························································································
30
Abstract in Korean
················································································
38
-
-iii-
List of Figures
Figure 1. Starting position of bridging exercise
············································ 9
Figure 2. Bridging without isometric hip abduction
··································· 11
Figure 3. Bridging with isometric hip abduction using the
Thera-Band ···· 13
Figure 4. Measurement of anterior pelvic tilt angle
·································· 15
Figure 5. Comparison of gluteus maximus muscle activity between
bridging
exercise with and without isometric hip abduction
······················ 19
Figure 6. Comparison of anterior pelvic tilt angle between
bridging exercise
with and without isometric hip abduction
··································· 22
-
-iv-
List of Tables
Table 1. General characteristics of
subjects·············································· 17
Table 2. Comparison of muscle activity in the gluteus maximus,
hamstrings,
and erector spinae between two conditions of bridging
exercise
································································································
18
Table 3. Comparison of gluteus maximus/hamstrings and gluteus
maximus/
erector spinae ratios between g two conditions of bridging
exercise
··································································································
20
Table 4. Comparison of anterior pelvic tilt angle between two
conditions of
bridging exercise
·······································································
21
-
-v-
ABSTRACT
Gluteus Maximus Preactivation Using a Thera-Band Alters
Muscle Activity and the Anterior Pelvic Tilt Angle
During Bridging Exercise
Silah Choi Dept. of Physical Therapy
The Graduate School
Yonsei University
The gluteus maximus (GM) is frequently weak and lengthened
because many
people spend a great amount of time remaining seated. Hamstring
(HAM) tightness
and excessive anterior pelvic tilt with dominant erector spinae
(ES) can be observed
as a compensatory mechanism for a weak GM. The purpose of this
study was to
investigate the effects of bridging with isometric hip abduction
(IHA) using the
Thera-Band on GM, HAM, and ES muscle activity; GM/HAM and GM/ES
ratios;
and the anterior pelvic tilt angle in healthy subjects.
Twenty-one subjects participated
in this study and all subjects performed bridging with and
without IHA. Surface EMG
-
-vi-
was used to collect EMG data of GM, HAM, and ES muscle
activities, and Image J
software was used to measure anterior pelvic tilt angle. A
paired t-test was used to
compare GM, HAM, and ES muscle activity; the GM/HAM and GM/ES
ratios; and
the anterior pelvic tilt angle with and without IHA during the
bridging exercise. GM
muscle activity increased significantly and the anterior pelvic
tilt angle decreased
significantly during bridging with IHA using the Thera-Band (p
< 0.05). However,
there were no significant differences in the activity of the HAM
and ES and the
GM/HAM and GM/ES ratios between bridging with and without IHA (p
> 0.05). The
results of this study suggest that bridging with IHA using the
Thera-Band can be
implemented as an effective method to facilitate GM muscle
activity and reduce the
anterior pelvic tilt angle.
Key words: Bridging, Gluteus maximus, Preactivation,
Thera-Band.
-
-1-
Introduction
The gluteus maximus (GM) is one of the largest and strongest
muscles in the body.
The GM originates from the posterior sacrum and coccyx as well
as the posterior
gluteal line of the ilium and inserts on the iliotibial tract
and gluteal tuberosity of the
femur (Frank and Netter, 1987). The GM is a powerful extensor
and external rotator
of the hip, and the superior part of the GM acts as a hip
abductor because muscle
fibers in the GM are directed downward and outward (Frank and
Netter, 1987; Long
et al., 1993). Hip extensors, especially the GM, are important
for many functional
activities of daily living such as moving from sitting to
standing, climbing stairs, and
maintaining an upright posture during walking (Winter, 1991).
Because the direction
of the GM muscle fibers, especially deep sacral fibers of the
GM, are perpendicular to
the sacroiliac (SI) joint, GM contraction improves SI joint
stability and plays a part in
force transmission from the lower extremity to the pelvis during
ambulation (Hossain
and Nokes, 2005; Leinonen et al., 2000; Mooney et al.,
2001).
However, the GM is frequently weak and lengthened because many
people spend a
great amount of time remaining seated (Sahrmann, 2002).
Decreased activity of the
GM is one cause of low back pain (LBP) and results in SI joint
instability and
dysfunction (van Wingerden et al., 2004). In addition, hamstring
(HAM) tightness can
be observed as a compensatory mechanism for a weak GM (Massoud
et al., 2011; van
Wingerden et al., 2004). Also, excessive anterior pelvic tilt,
lumbar lordosis with
-
-2-
dominant erector spinae (ES), and lumbar rotation occur in place
of a weak GM or
delayed GM activation during hip extension (Chaitow, 1996;
Sahrmann, 2002).
There are various exercises to strengthen the hip extensors,
including the squat,
lunge, and prone hip extension (Distefano et al., 2009; Kang et
al., 2013; Wagner et
al., 2010). Among these exercises, bridging exercises are the
most commonly used by
people with weak hip extensors and trunk muscles in physical
therapy programs.
Bridging exercises are closed-chain weight-bearing exercises
that support the body
weight against gravity. They activate the hip extensors and
trunk muscles to a greater
extent than the abdominal muscles and are useful for lumbopelvic
stabilization and
the control of pelvic motion (Ekstrom et al., 2007; Mori A,
2004; O'Sullivan and
Schimitz, 2007; Richardson, 1995). In addition, bridging
exercises can be easily
modified and applied in diverse ways, including single-leg
bridging, ball bridging,
and bridging with different knee positions (Ekstrom et al.,
2008; Stevens et al., 2006).
However, bridging exercises are associated with a risk of
dominant HAM and ES
activity and excessive anterior pelvic tilt as a compensation
for GM weakness
regardless of the type of bridging exercise performed.
Therefore, bridging exercise
with isometric hip abduction (IHA) using a Thera-Band (Hygenic
Corp., Akron, OH,
USA) was devised in this study. The Thera-Band is a useful and
portable clinical tool
for increasing strength, mobility, and function in multi-planar
movements and various
part of the body (Mikesky et al., 1994; Selkowitz et al.,
2013).
No previous studies have compared GM with HAM and ES muscle
activity and
pelvic kinematics during bridging with IHA using the Thera-Band.
Thus, the purpose
-
-3-
of this study was to investigate the effects of bridging with
IHA using the Thera-Band
on GM, HAM, and ES muscle activity; GM/HAM and GM/ES ratios; and
the anterior
pelvic tilt angle in healthy subjects. It was hypothesized that
bridging with IHA using
the Thera-Band would result in increased GM muscle activity,
increased GM/HAM
and GM/ES ratios, and a decreased anterior pelvic tilt
angle.
-
-4-
Methods
1. Subjects
Prior to recruiting subjects for this study, a power analysis
was performed with
G*power software ver. 3.1.2 (Franz Faul, University of Kiel,
Kiel, Germany) using
the results of a pilot study involving five subjects. The
calculation of sample size was
carried out with a power of 0.80, alpha level of 0.05, and
effect size of 0.89. This
provided a necessary sample size of ten subjects for this
study.
Twenty-one healthy subjects were recruited from a university
population. The
exclusion criteria were: (1) limitations in range of motion of
the bilateral hip, knee,
and ankle joints; (2) a history of LBP or lower extremity
dysfunctions such as
iliotibial band friction syndrome, patellofemoral pain syndrome,
anterior cruciate
ligament sprains, or chronic ankle instability (Cichanowski et
al., 2007; Fredericson
et al., 2000; Friel et al., 2006; Hewett et al., 2006; Ireland
et al., 2003) in the past 12
months; (3) iliopsoas, rectus femoris, or tensor fasciae latae
tightness as evidenced by
the Thomas test, Ely’s test, or modified Ober’s test,
respectively (Kendall, 2005;
Magee, 2007); and (4) lumbopelvic instability demonstrated by
performing the active
straight leg raising test with a pressure biofeedback unit
(Liebenson, 2004; Mens et al.,
1999).
-
-5-
Prior to collecting data, the examiner informed the subjects of
the study procedures
and each subject completed an informed consent form. The study
protocol was
approved by the Yonsei University Wonju Institutional Review
Board.
-
-6-
2. Instrumentation
2.1 Surface Electromyography
Electromyographic (EMG) data were collected using a TeleMyo DTS
(Noraxon
Inc., Scottsdale, AZ, USA) and analyzed using MyoResearch 1.08
XP software
(Noraxon Inc.). The electrode sites were shaved and then rubbing
alcohol was used to
reduce skin impedance. Two surface electrodes were positioned at
an interelectrode
distance of 2㎝ bilaterally.
EMG data were collected for the GM, HAM, and ES. The upper
fibers of the GM
represented the GM in this study. The electrode for the GM was
placed half the
distance between the trochanter and sacral vertebrae in the
middle of the muscle at an
oblique angle at the level of the trochanter. For general
recordings of the HAM, the
electrode for the HAM was placed parallel to the muscle in the
center of the back of
the thigh, approximately half the distance from the gluteal fold
to the back of the knee.
The electrode for the ES was placed parallel to the spine at the
level of the iliac crest,
approximately 2 ㎝ apart from the spine over the muscle mass
(Criswell, 2010).
EMG signals were sampled at 1000㎐. Notch filter was preset to
reject 60㎐. A band
pass filter was used between 20 and 450 ㎐. The raw data were
processed into the
root mean square (RMS) with a window of 50㎳.
Normalization was needed to minimize variables or differences
between different
recoding sites and individuals. The maximal voluntary isometric
contraction (MVIC)
-
-7-
normalization method was applied to each tested muscle and MVIC
was recorded
during a manual muscle test (MMT) in the positions described by
Kendall et al.
(2005). To collect MVIC data, subjects maintained the MMT
position of each tested
muscle against manual resistance for 5 s. The middle 3-s
contraction, excluding each
1 s at the beginning and end, was used for data analysis, and a
30-s rest was given
between the two trials. The mean value of the two trials for the
maximal contraction
in each muscle was taken as the MVIC. All EMG data collected
were expressed as an
RMS-processed percentage of the MVIC (%MVIC).
-
-8-
3. Experimental Procedures
Subjects were informed of the standardized position of the
bridging exercise in this
study and underwent a familiarization period of approximately 20
min to achieve a
proper exercise performance capability. When subjects failed to
perform the
standardized position and maintain the position during the
exercise period, data
collection was immediately stopped. Bridging without IHA was
followed by bridging
with IHA to minimize the learning effect. The mean value of two
trials of each
bridging exercise was used for data analysis. A 5-min rest
between the two conditions
and a 1-min rest between every two trials was given to avoid
muscle fatigue.
-
-9-
3.1 Bridging Without Isometric Hip Abduction
The subjects were placed in a supine position. Both knees were
flexed at 90°, the
feet were hip-width apart while resting on the floor, and the
toes were facing forward.
The arms were crossed over the chest to minimize arm support
(Figure 1).
Figure 1. Starting position of bridging exercise.
-
-10-
Two plastic poles were placed vertically along the lateral
aspect of the bilateral knee
joint to maintain hip abduction of 30°. A wooden target bar was
placed at the height
of the middle point of the thigh between the greater trochanter
and femoral condyle
when the trunk, pelvis, and thigh were aligned in a straight
line (hip extension of 0°).
A universal goniometer was used for knee and hip angle
measurements. The subject
was instructed to lift his pelvis comfortably at a self-selected
speed while maintaining
contact between the lateral aspects of the bilateral knee joint
and vertically placed
plastic poles. When both thighs touched the wooden target bar
during bridging, the
subject was asked not to lift his pelvis further and to hold the
bridging position for 5 s
without pelvic or thigh movement. After 5 s of bridging, the
subject lowered his
pelvis (Figure 2).
-
-11-
Figure 2. Bridging without isometric hip abduction.
-
-12-
3.2 Bridging With Isometric Hip Abduction
Bridging with IHA followed the same procedure as bridging
without IHA, with the
exception of the application of a blue-colored Thera-Band, which
is recommended by
the manufacturer for an intermediate or advanced workout level.
The Thera-Band was
wrapped around both thighs just proximal to the knees, providing
consistent
resistance to IHA. Tension was controlled by lengthening or
shortening the Thera-
Band. The tension in the Thera-Band was determined when the
subject was able to
perform more than ten repetitions of hip abduction of 30° in
hook-lying position
using the Thera-Band (Decker et al., 1999; Park et al., 2013)
(Figure 3).
-
-13-
Figure 3.Bridging with isometric hip abduction using the
Thera-Band.
-
-14-
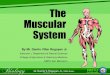
3.3 Measurement of Anterior Pelvic Tilt Angle
To obtain pelvic kinematic data, two reflective markers were
placed on specific
anatomical landmarks; namely, the anterior superior iliac spine
(ASIS) and posterior
superior iliac spine (PSIS). In this study, the anterior pelvic
tilt was defined as an
angle between a line joining the ASIS, PSIS, and the vertical
line from the ASIS
(Figure 4). The examiner took a picture of the subject’s pelvis
with a digital camera
when the subject maintained the position under two conditions of
bridging exercises.
The location of the digital camera and distance from the digital
camera to the subject
were consistent. These pictures were then transferred to Image J
software (National
Institutes of Health, Bethesda, MD, USA) and used to measure the
anterior pelvic tilt
angle.
-
-15-
Figure 4. Measurement of anterior pelvic tilt angle.
-
-16-
4. Statistical Analysis
A Kolmogorov-Smirnov Z-test was performed to confirm a normal
distribution. A
paired t-test was used to compare GM, HAM, and ES muscle
activity; the GM/HAM
and GM/ES ratios; and the anterior pelvic tilt angle with and
without IHA during the
bridging exercise. Statistical significance was set at 0.05. All
statistical analyses were
performed using PASW Statistics ver. 18.0 (SPSS, Inc., Chicago,
IL, USA).
-
-17-
Results
1. Subjects
The general characteristics of the 21 subjects, including age,
height, weight, and
body mass index, are shown in Table 1.
Table 1.General characteristics of subjects (N=21)
Parameters Mean±SD
Age (years) 22.5 ± 1.0
Height (㎝) 165.3 ± 7.1
Weight (㎏) 57.5 ± 8.7
BMIa (㎏/㎡) 20.9 ± 1.8 aBMI: Body mass index.
-
-18-
2. Electromyographic Data
All dependent variables were found to approximate a normal
distribution
(Kolmogorov-Smirnov Z-test, p > 0.05).
2.1 Gluteus Maximus, Hamstrings, and Erector Spinae Muscle
Activity
In terms of muscle activity, GM muscle activity increased
significantly during
bridging with IHA using the Thera-Band (p < 0.05) (Figure 5).
However, there were
no significant differences in the activity of the HAM and ES (p
> 0.05) between
bridging with and without IHA (Table 2).
Table 2. Comparison of muscle activity in the gluteus maximus,
hamstrings, and
erector spinae between two conditions of bridging exercise
(N=21)
Muscles Bridging without IHAa Bridging with IHA t p
GMb 21.06 ± 12.16e 25.50 ± 13.01 -3.016 0.007
HAMc 37.96 ± 16.89 42.97 ± 20.22 -2.040 0.055
ESd 52.93 ± 4.23 54.18 ± 4.01 -0.565 0.578 aIHA: Isometric hip
abduction. bGM: Gluteusmaximus. cHAM: Hamstrings. dES:
Erectorspinae. eMean ±Standard deviation of % maximal voluntary
isometric contraction.
-
-19-
Figure 5. Comparison of gluteus maximus muscle activity between
bridging exercise
with and without isometric hip abduction.
IHA: Isometric hip abduction.
* p < 0.05.
-
-20-
2.2 Gluteus Maximus/Hamstrings and Gluteus Maximus/Erector
Spinae Muscle Activity Ratios
In terms of muscle ratios, the GM/HAM and GM/ES ratios were not
significantly
different between bridging with and without IHA (p > 0.05)
(Table 3).
Table 3. Comparison of gluteus maximus/hamstrings and gluteus
maximus/erector
spinae ratios between g two conditions of bridging exercise
(N=21)
Ratio Bridging without IHAa Bridging with IHA t p
GM/HAMb 0.72 ± 0.67d 0.73 ± 0.52 -0.119 0.906
GM/ESc 0.45 ± 0.34 0.49 ± 0.23 -0.748 0.463 aIHA: Isometric hip
abduction. bGM/HAM: Gluteus maximus/hamstrings. cGM/ES: Gluteus
maximus/erector spinae. dMean ± Standard deviation.
-
-21-
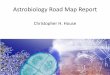
2.3 Anterior Pelvic Tilt Angle
With regard to pelvic kinematics, the anterior pelvic tilt angle
decreased
significantly during bridging with IHA using the Thera-Band (p
< 0.05) (Table 4)
(Figure 6).
Table 4. Comparison of anterior pelvic tilt angle between two
conditions of bridging
exercise (N=21)
Pelvic Kinematics Bridging without IHAa Bridging with IHA t
p
Anterior pelvic
tilt angle 7.65 ± 2.36b 6.08 ± 2.28 3.055 0.006
aIHA: Isometric hip abduction. bMean ± Standard deviation
(°)
-
-22-
Figure 6. Comparison of anterior pelvic tilt angle between
bridging exercise with and
without isometric hip abduction.
IHA: Isometric hip abduction.
* p < 0.05.
-
-23-
Discussion
The aim of this study was to determine whether GM, HAM, and ES
muscle
activity; the GM/HAM and GM/ES ratios; and the anterior pelvic
tilt angle could be
altered when IHA using the Thera-Band was applied during
bridging in healthy
subjects. To my knowledge, this study is the first to evaluate
the effect of IHA with
the Thera-Band on GM muscle preactivation and pelvic kinematics
during a bridging
exercise. The results partially supported the research
hypothesis.
GM activity increased significantly by 21.1% during bridging
with IHA using the
Thera-Band, supporting the research hypothesis. A possible
explanation is that
applying IHA with the Thera-Band during bridging and maintaining
hip abduction of
30° induced preactivation of the GM before initiation of the
bridging movement,
consequently increasing GM muscle activity. Isometric exercises
have been used to
develop static muscle strength or muscular endurance and
facilitate muscle firing to
reestablish neuromuscular control (Kisner and Cloby, 2007). Our
present finding is in
agreement with those of previous studies demonstrating the
effect of muscle
preactivation on muscle firing or force. Linnamo et al. (2003)
investigated motor unit
activation patterns in concentric and eccentric contractions
with and without isometric
preactivation at different force levels. At the highest force
level, when movement was
initiated with preactivation, the mean spike amplitude in
concentric contraction was
higher than that in eccentric contraction, while no significant
difference in mean spike
amplitude was shown between concentric and eccentric
contractions during
-
-24-
movement without preactivation. Kyrolaïnen et al. (1999)
emphasized the importance
of the preactivation of leg extensor muscles for increasing
running speed. Specifically,
this finding determined that preactivity of the gastrocnemius
muscle functioned as a
preparatory requirement to enhance muscle activity and the
timing of muscular action
with respect to ground contact during the running cycle.
Mrdakovic et al. (2008)
confirmed that when a knee extensor bench exercise was performed
before (or
preceded by) a leg press exercise by means of muscle
preactivation, an increased
EMG signal was recorded from the vastus lateralis muscle. This
result indicates that
preactivation performance by a single-joint exercise increases
the number of motor
units recruited during a multi-joint exercise.
The GM is quadrilateral in shape, and its fibers are obliquely
directed inferiorly
and laterally. It functions not only as a hip extensor, but also
as a hip abductor and
external rotator (Frank and Netter, 1987; McAndrew et al.,
2006). In this study, hip
abduction of 30° was sustained by two plastic poles placed
vertically along the lateral
aspect of the bilateral knee joints. Such hip abduction during
bridging might facilitate
GM activity in terms of the action of the GM as a hip abductor
and external rotator. In
a previous study, Kang et al. (2013) reported that the GM EMG
amplitude was
greatest at 30° of hip abduction during prone hip extension with
knee flexion.
Because the GM is a fusiform muscle that is optimized when the
direction of muscle
pull is parallel to the muscle fiber, hip abduction during prone
hip extension with
knee flexion leads to an increased EMG amplitude of the GM.
-
-25-
It was expected that HAM and ES activity would be reduced when
GM activity
was increased by applying IHA with the Thera-Band during
bridging exercise. This
hypothesis was based on the findings of previous studies
demonstrating that
synergistic muscles work together to perform the same range of
motion. For example,
increased or decreased changes in the activity of one muscle can
lead to opposing
changes in activity of another synergistic muscle (Jonkers et
al., 2003; Kang et al.,
2013; Park et al., 2013). Based on these findings, synergistic
muscles during bridging
(i.e., trunk extensors such as the GM, HAM, and ES) can affect
one another during
bridging: increased GM activity could reduce HAM and ES
activity. However, the
present study also produced findings that are inconsistent with
the hypothesis.
Although GM activity was significantly increased, it failed to
elicit changes in the
GM/HAM and GM/ES ratios. The GM/HAM and GM/ES ratios did not
reach
statistical significance between bridging with and without
IHA.
The unexpected findings in this study may be the result of
several differences from
previous studies. First, in contrast to the subjects in previous
studies, healthy subjects
participated in the present study and exhibited HAM or ES
activity that was dominant
to (or greater than) the GM activity at the beginning of the
study. In many previous
studies that investigated GM activity during various bridging or
prone hip extension
exercises in healthy subjects, the mean activity levels of the
ES and HAM at baseline
(i.e., before the intervention) were less than or similar to the
mean value for the GM
(Ekstrom et al., 2007; Ekstrom et al., 2008; Kang et al., 2013;
Sakamoto et al., 2009).
However, in this study, especially for the ES, the mean value of
ES activity was twice
-
-26-
the mean value reported previously (García-Vaquero et al., 2012;
Imai et al., 2010;
Lehman et al., 2005; Okubo et al., 2010). In addition, because
the mean value of
HAM and ES muscle activity was about 1.8 and 2.5 times that of
the GM,
respectively, during bridging without IHA in this study (without
intervention or at
entry), bridging with IHA would not likely lead to significant
decreases in the
dominant HAM and ES in a cross-sectional study.
Second, because a wooden target bar was used to control pelvic
lift during bridging,
increased activation of the HAM and ES was not likely to occur
in the present study.
No previous studies have recommended the most appropriate level
of pelvic lifting
during bridging, and over-lifting the lumbopelvis during
bridging can be
disadvantageous due to potential overactivation of the
already-dominant HAM and
ES; thus, a wooden target bar was placed to provide contact,
cueing the subjects not
to over-lift the pelvis while performing the two types of
bridging. However, this valid
use of a wooden target bar could have limited the level of the
lumbopelvis and
consequently might have prevented overactivation of the HAM and
ES during
bridging. Thus, HAM and ES activity may have differed if the
subjects had performed
bridging without a wooden target bar.
The anterior pelvic tilt angle decreased significantly by 20.5%
during bridging with
IHA using the Thera-Band, supporting the research hypothesis.
Although the change
of anterior pelvic tilt angle was small, it could be a
meaningful result in consideration
of measurement position because anterior pelvic tilt was
measured in bridging
position in this study. Lembeck et al. (2005) reported that
average pelvic tilt angle in
-
-27-
the lying position was lower than standing position. Thus,
bridging with IHA using a
Thera-Band resulted in preactivation of the GM, and the
increased GM activity could
have contributed to reduce anterior pelvic tilt. In other words,
when the femur was
fixed, such as bridging position, contraction of the GM induced
the pelvis to move
posteriorly and decrease anterior pelvic tilt and lumbar
lordosis. Many previous
studies have emphasized that an important function of the GM is
to maintain pelvic
stability. Oh et al. (2007) suggested that performance of the
abdominal drawing-in
maneuver during prone hip extension encouraged activation of the
hip extensors
while decreasing activation of the ES and reducing the anterior
pelvic tilt. They
explained that increased GM muscle activity could be affected by
biomechanical
alterations such as a reduced anterior pelvic tilt. Tateuchi et
al. (2012) focused on
improvements in hip muscle balance between agonists and
antagonists, which could
reduce the anterior pelvic tilt. An altered balance in muscle
activation, especially a
hip flexor (tensor fasciae latae) dominant to the hip extensors
(GM and
semitendinosus), during prone hip extension resulted in abnormal
movement patterns,
such as anterior pelvic tilt and excessive lumbar extension.
The present study has several limitations. First, measurement
errors were likely to
have occurred when measuring the pelvic kinematics because this
study used only
two-dimensional image processing software. A three-dimensional
motion analysis
system or real-time measuring system will be needed to improve
the precision of
measurement in future studies. Second, the findings of this
study are difficult to
generalize to the entire patient population because only healthy
and young subjects
-
-28-
participated. Subjects with a broad age range and clinical
symptoms such as GM
weakness should be investigated in future to strengthen the
clinical implications of
this study. Finally, this study used a cross-sectional design
and could not identify the
long-term effects of preactivation of the GM on HAM and ES
activity. Future
longitudinal studies are necessary to show distinct differences
in GM, HAM, and ES
muscle activity and anterior pelvic tilt angle.
-
-29-
Conclusion
This study investigated the effects of bridging with IHA using a
Thera-Band on
GM, HAM, and ES activity; the GM/HAM and ES ratios; and the
anterior pelvic tilt
angle. GM muscle activity increased significantly and the
anterior pelvic tilt angle
decreased significantly during bridging with IHA using a
Thera-Band. These findings
indicate that the application of a Thera-Band preactivates the
GM before the initiation
of bridging, enhances GM activity, and prevents excessive
anterior pelvic tilt during
bridging. Therefore, bridging with IHA using the Thera-Band can
be implemented as
an effective method to facilitate GM muscle activity and reduce
the anterior pelvic tilt
angle.
-
-30-
References
Chaitow L. Muscle Energy Techniques. London, UK: Churchill
Livingstone, 1996.
Cichanowski HR, Schmitt JS, Johnson RJ, Niemuth PE. Hip strength
in collegiate
female athletes with patellofemoral pain. Med Sci Sports
Exerc.
2007;39(8):1227-1232.
Criswell E. Cram’s Introduction to Surface Electromyography. 2nd
ed. Sudbury, MA:
Jones and Bartlett Publishers, 2011.
Decker MJ, Hintermeister RA, Faber KJ, Hawkins RJ. Serratus
anterior muscle
activity during selected rehabilitation exercises. Am J Sports
Med.
1999;27(6):784-791.
Distefano LJ, Blackburn JT, Marshall SW, Padua DA. Gluteal
muscle activation
during common therapeutic exercises. J Orthop Sports Phys
Ther.
2009;39(7):532-540.
Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of
core trunk, hip,
and thigh muscles during 9 rehabilitation exercises. J Orthop
Sports Phys Ther.
2007;37(12):754-762.
-
-31-
Ekstrom RA, Osborn RW, Hauer PL. Surface electromyographic
analysis of the low
back muscles during rehabilitation exercises. J Orthop Sports
Phys Ther. 2008
Dec;38(12):736-745.
Frank H and Netter R. The CIBA Collection of Medical
Illustrations: vol 8.
Musculoskeletal system. Summit, NJ: Ciba-Geigy Corp, 1987.
Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC,
Oestreicher N,
Sahrmann SA. Hip abductor weakness in distance runners with
iliotibial band
syndrome. Clin J Sport Med. 2000;10(3):169-175.
Friel K, McLean N, Myers C, Caceres M. Ipsilateral hip abductor
weakness after
inversion ankle sprain. J Athl Train. 2006;41(1):74-78.
García-Vaquero MP, Moreside JM, Brontons-Gil E, Peco-González N,
Vera-Garcia
FJ. Trunk muscle activation during stabilization exercises with
single and double
leg support. J Electromyogr Kinesiol. 2012;22(3):398-406.
Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries
in female
athletes: Part 1, mechanisms and risk factors. Am J Sports Med.
2006;34(2):299-
311.
-
-32-
Hossain M, Nokes LD. A model of dynamic sacroiliac joint
instability from
malrecruitment of gluteus maximus and biceps femoris muscles
resulting in low
back pain. Med Hypotheses. 2005;65(2):278-281.
Imai A, Kaneoka K, Okubo Y, Shiina I, Tatsumura M, Izumi S,
Shiraki H. Trunk
muscle activity during lumbar stabilization exercises on both a
stable and
unstable surface. J Orthop Sports Phys Ther.
2010;40(6):369-75.
Ireland ML, Willson JD, Ballantyne BT, Davis IM. Hip strength in
females with and
without patellofemoral pain. J Orthop Sports Phys Ther.
2003;33(11):671-676.
Jonkers I, Stewart C, Spaepen A. The complementary role of the
plantar flexors,
hamstrings and gluteus maximus in the control of stance limb
stability during
gait. Gait Posture. 2003;17:264-72.
Kang SY, Jeon HS, Kwon O, Cynn HS, Choi BR. Activation of the
gluteus maximus
and hamstring muscles during prone hip extension with knee
flexion in three hip
abduction positions. Man Ther. 2013;18(4):303-307.
Kendall FP, McCreary EK, Provance PG. Muscles: Testing and
Function With
Posture and Pain. 5th ed. Baltimore, MD: Lippincott Williams
& Wilkins, 2005.
-
-33-
Kisner C and Colby LA. Therapeutic Exercise: Foundations and
techniques. 5th ed.
Philadelphia, PA: F.A. Davis Co., 2007.
Kyrolaïnen H, Komi P V, and Belli A. Changes in Muscle Activity
patterns and
kinetics with increasing running speed. J Strength Cond Res.
1999;13(4):400-
406.
Lehman GJ, Hoda W, Oliver S. Trunk muscle activity during
bridging exercises on
and off a Swiss ball. Chiropr Osteopat. 2005;30:13-14.
Leinonen V, Kankaanpää M, Airaksinen O, Hänninen O. Back and hip
extensor
activities during trunk flexion/extension: Effects of low back
pain and
rehabilitation. Arch Phys Med Rehabil. 2000;81(1):32-37.
Lembeck B, Mueller O, Reize P, Wuelker N. Pelvic tilt makes
acetabular cup
navigation inaccurate. Acta Orthop. 2005:76(4):517-523.
Liebenson C. The relationship of the sacroiliac joint,
stabilization musculature, and
lumbo-pelvic instability. J Bodyw Mov Ther. 2004;8(1):43-45.
-
-34-
Linnamo V, Moritani T, Nicol C, Komi PV. Motor unit activation
patterns during
isometric, concentric and eccentric actions at different force
levels. J
Electromyogr Kinesiol. 2003;13(1):93-101.
Long WT, Dorr LD, Healy B, Perry J. Functional recovery of
noncemented total hip
arthroplasty. Clin Orthop Relat Res. 1993;(288):73-77.
Magee DJ. Orthopedic Physical Assessment. 5th ed, St. Louis, MO:
Saunders, 2007.
Massoud Arab A, Reza Nourbakhsh M, Mohammadifar A. The
relationship between
hamstring length and gluteal muscles trength in individuals with
sacroiliac joint
dysfunction. J Man Manip Ther. 2011;19(1):5-10.
McAndrew D, Gorelick M, Brown JMM. Muscles within muscles: A
mechanomyographic analysis of muscle segment contractile
properties within
human gluteus maximus. J Musculoskelet Res. 2006;10:23-35.
Mens JM, Vleeming A, Snijders CJ, Stam HJ, Ginai AZ. The active
straight leg
raising test and mobility of the pelvic joints. Eur Spine J.
1999;8(6):468-473.
-
-35-
Mikesky AE, Topp R, Wigglesworth JK, Harsha DM, Edwards JE.
Efficacy of a
home-based training program for older adults using elastic
tubing. Eur J Appl
Physiol Occup Physiol. 1994;69:316-320.
Mooney V, Pozos R, Vleeming A, Gulick J, Swenski D. Exercise
treatment for
sacroiliac pain. Orthopedics. 2001;24(1):29-32.
Mori A. Electromyographic activity of selected trunk muscles
during stabilization
exercises using a gymball. Electromyogr Clin Neurophysiol.
2004;44(1):57-64.
Mrdakovic V, Ilic DB, Jankovic N, Rajkovic Z, Stefanovic D.
Pre-activity
modulation of lower extremity muscles within different types and
heights of
deep jump. J Sports Sci Med. 2008;7(2):269-278.
O'Sullivan SB and Schmitz TJ. Physical Rehabilitatio. 5th ed.
Philadelphia, PA: F.A.
Davis Co., 2007.
Oh JS, Cynn HS, Won JH, Kwon OY, Yi CH. Effects of performing an
abdominal
drawing-in maneuver during prone hip extension exercises on hip
and back
extensor muscle activity and amount of anterior pelvic tilt. J
Orthop Sports Phys
Ther. 2007;37(6):320-324.
-
-36-
Okubo Y, Kaneoka K, Imai A, Shiina I, Tatsumura M, Izumi S,
Miyakawa S.
Electromyographic analysis of transversus abdominis and lumbar
multifidus
using wire electrodes during lumbar stabilization exercises. J
Orthop Sports
Phys Ther. 2010;40(11):743-50
Park KM, Cynn HS, Yi CH, Kwon OY. Effect of isometric horizontal
abduction on
pectoralis major and serratus anterior EMG activity during three
exercises in
subjects with scapular winging. J Electromyogr Kinesiol.
2013;23(2):462-468.
Richardson CA, Jull GA. Muscle control-pain control. What
exercises would you
prescribe? Man Ther. 1995;1(1):2-10.
Sahrmann SA. Diagnosis and Treatment of Movement Impairment
Syndromes. 1st ed.
St. Louis, MO: Mosby, 2002.
Sakamoto ACL, Teixeira-Salmela LF, Rodrigues De Paula F,
Guimarães, CQ, Faria
CDCM. Gluteus maximus and semitendinosus activation during
active prone hip
extension exercises. Braz J PhysTher. 2009;13(4):335-342.
Selkowitz DM, Beneck GJ, Powers CM. Which exercises target the
gluteal muscles
while minimizing activation of the tensor fascia lata?
Electromyographic
-
-37-
assessment using fine-wire electrodes. J Orthop Sports Phys
Ther.
2013;43(2):54-64.
Stevens VK, Bouche KG, Mahieu NN, Coorevits PL, Vanderstraeten
GG, Danneels
LA. Trunk muscle activity in healthy subjects during bridging
stabilization
exercises. BMC MusculoskeletDisord. 2006;20:7:75.
Tateuchi H, Taniguchi M, Mori N, Ichihashi N. Balance of hip and
trunk muscle
activity is associated with increased anterior pelvic tilt
during prone hip
extension. J Electromyogr Kinesiol. 2012;22(3):391-397.
van Wingerden JP, Vleeming A, Buyruk HM, Raissadat
K.Stabilization of the
sacroiliac joint in vivo: Verification of muscular contribution
to force closure of
the pelvis. Eur Spine J. 2004 ;13(3):199-205.
Wagner T, Behnia N, Ancheta WK, Shen R, Farrokhi S, Powers CM.
Strengthening
and neuromuscular reeducation of the gluteus maximus in a
triathlete with
exercise-associated cramping of the hamstrings. J Orthop Sports
Phys Ther.
2010;40(2):112-9.
Winter DA. The Biomechanics and Motor Control of Human Gait:
Normal, Elderly
and Pathological. 2nd ed. Kitchener, ON: Waterloo Biomechanics.
1991.
-
-38-
국문 요약
교각운동 시 세라밴드를 이용한 대둔근의 전활성화가
대둔근의 근활성도와 골반의 전방경사
각도에 미치는 영향
연세대학교 대학원
물리치료학과
최 슬 아
대둔근은 많은 사람들이 상당한 시간을 앉아서 생활하면서 쉽게
약화되고 늘어나게 된다. 약화된 대둔근에 대한 보상작용으로 슬괵근의
단축, 우세한 척추기립근과 함께 나타나는 과도한 골반의 전방경사가 관찰
되기도 한다. 따라서 본 연구의 목적은 교각운동 시 세라밴드를 이용한
등척성 고관절 외전이 대둔근, 슬괵근, 척추기립근의 근활성도와
대둔근/슬괵근, 대둔근/척추기립근의 근활성비, 그리고 골반의 전방경사
각도에 미치는 영향을 알아보는 것이다. 본 연구를 위해 21명의 건강한
-
-39-
대상자가 참여하였고 모든 대상자는 세라밴드를 이용하여 등척성 고관절
외전을 적용한 교각운동과 그렇지 않은 교각운동을 실시하였다. 대둔근,
슬괵근, 척추기립근의 근활성도 자료를 수집하기 위해 표면 근전도를
사용하였고, 골반의 전방경사 각도는 이미지 제이 소프트웨어를 이용하여
측정하였다. 대둔근, 슬괵근, 척추기립근의 근활성도와 대둔근/슬괵근,
대둔근/척추기립근 근활성비, 그리고 골반의 전방경사 각도를 등척성
고관절 외전을 적용한 교각운동과 그렇지 않은 교각운동에서 비교하기
위해 짝비교 t-검정을 하였다.
세라밴드를 이용하여 등척성 고관절 외전을 적용한 교각운동에서
대둔근의 근활성도는 유의하게 증가하였고 골반의 전방경사 각도는
유의하게 감소하였다. 하지만 슬괵근, 척추기립근의 근활성도와
대둔근/슬괵근, 대둔근/척추기립근의 근활성비에서는 유의한 차이를
보이지 않았다. 본 연구의 결과를 바탕으로, 교각운동 시 세라밴드를
이용한 등척성 고관절 외전이 대둔근의 근활성도를 증진시키고 골반의
전방경사 각도를 감소시키는 데 효과적인 방법이 될 수 있음을 시사한다.
핵심 되는 말: 교각운동, 대둔근, 전활성화, 세라밴드.