Embed Size (px)
Citation preview
Glucose homeostasis, Glucose homeostasis, pathophysiology of pathophysiology of
diabetes & ADA diabetes & ADA GuidelinesGuidelines
JC LynchJC Lynch
PHPT 726PHPT 726
20072007
Glucose homeostasisGlucose homeostasis
Glycogenolysis & Glycogenolysis & GlucoeogenesisGlucoeogenesis
Hepatic Glucose OutputHepatic Glucose Output
GlycogenolysisGlycogenolysis– Catabolism of Catabolism of
glycogen.glycogen.
GluconeogenesisGluconeogenesis– Production of Production of
glucose from glucose from carbohydrates or carbohydrates or proteins.proteins.
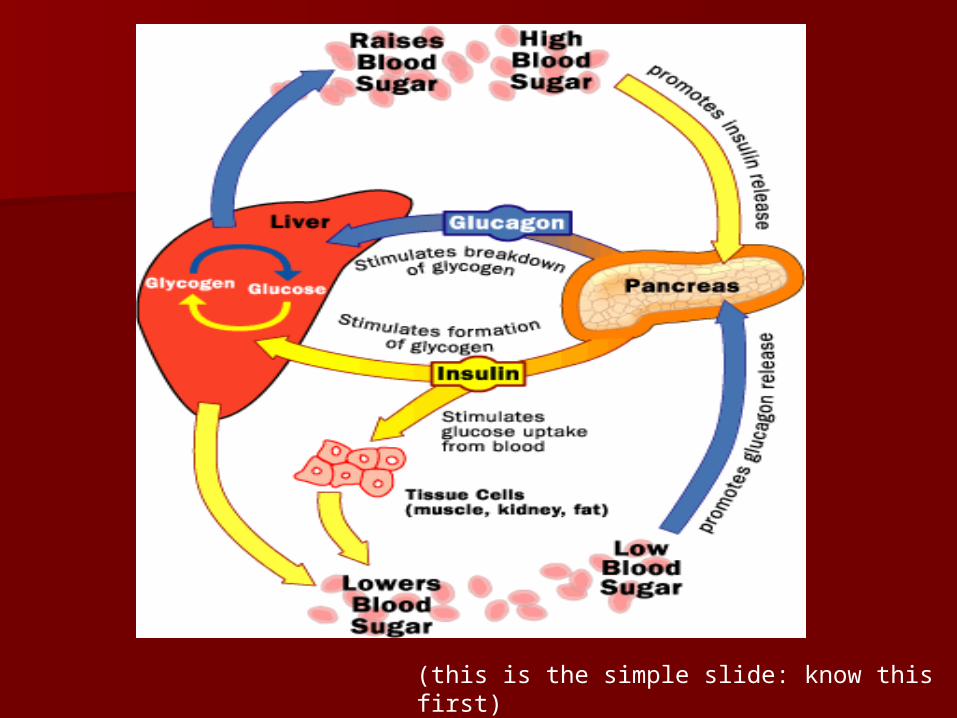
(this is the simple slide: know this first)
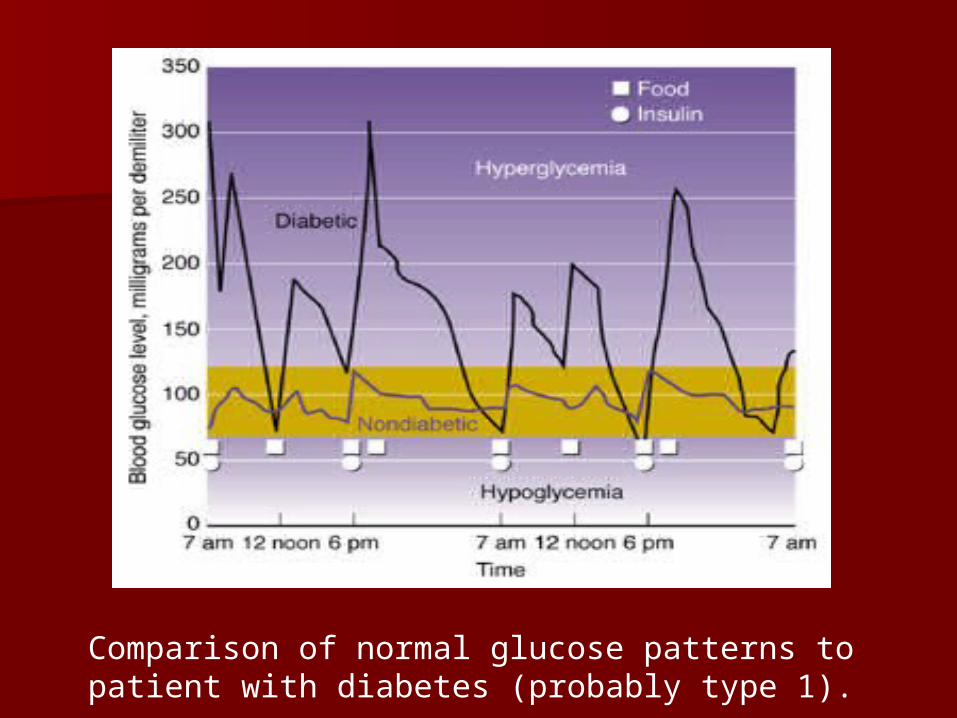
Comparison of normal glucose patterns to patient with diabetes (probably type 1).
Direct Effects of InsulinDirect Effects of Insulin
Glucose metabolismGlucose metabolism Lipoprotein metabolismLipoprotein metabolism Ketone metabolismKetone metabolism Protein metabolismProtein metabolism
Insulin Action: DefinitionsInsulin Action: Definitions
Insulin SensitivityInsulin SensitivityAbility of insulin to lower Ability of insulin to lower
circulating glucose circulating glucose concentrationsconcentrations
Insulin ResistanceCondition of low insulin sensitivity
Glucose MetabolismGlucose Metabolism
Major Metabolic Major Metabolic Effects of InsulinEffects of Insulin
Consequences of Consequences of Insulin Insulin
DeficiencyDeficiencyStimulates Stimulates glucose uptake glucose uptake into muscle and into muscle and adipose cellsadipose cells
Inhibits hepatic Inhibits hepatic glucose glucose production production
HyperglycemiaHyperglycemia osmotic diuresis osmotic diuresis and dehydrationand dehydration
Lipoprotein MetabolismLipoprotein Metabolism
Major Metabolic Major Metabolic Effects of InsulinEffects of Insulin
Consequences of Consequences of Insulin Insulin DeficiencyDeficiency
Inhibits Inhibits breakdown of breakdown of triglycerides triglycerides (lipolysis) in (lipolysis) in adipose tissueadipose tissue
Elevated FFA Elevated FFA levelslevels
Ketone MetabolismKetone Metabolism
Major Metabolic Major Metabolic Effects of InsulinEffects of Insulin
Consequences of Consequences of Insulin Insulin
DeficiencyDeficiencyInhibits Inhibits ketogenesis ketogenesis
Ketogenesis: is the Ketogenesis: is the process by which process by which ketone bodies are ketone bodies are produced as a result produced as a result of fatty acid of fatty acid breakdown. breakdown.
KetoacidosisKetoacidosis
Protein MetabolismProtein Metabolism
Major Metabolic Major Metabolic Effects of InsulinEffects of Insulin
Consequences Consequences of Insulin of Insulin DeficiencyDeficiency
Stimulates amino Stimulates amino acid uptake and acid uptake and protein synthesisprotein synthesis
Inhibits protein Inhibits protein degradation degradation
Regulates gene Regulates gene transcription transcription
Muscle wastingMuscle wastingOthersOthers
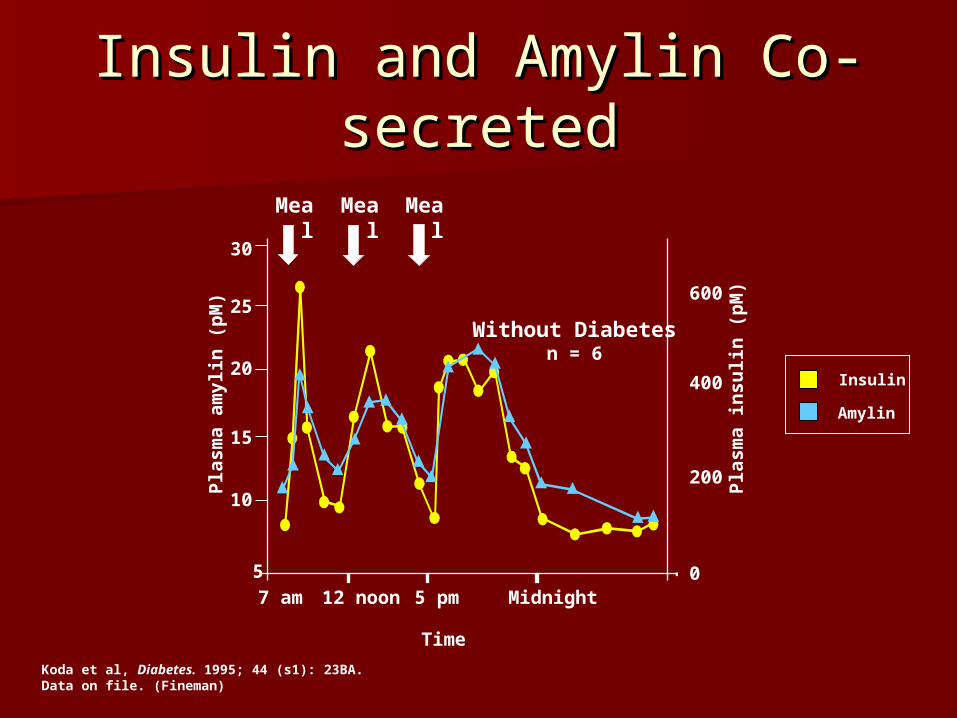
Insulin and Amylin Co-Insulin and Amylin Co-secretedsecreted
Amylin
Insulin
Without Diabetesn = 6
Pla
sma
insu
lin
(p
M)
Pla
sma
am
ylin
(p
M)
30
25
20
15
10
5
7 am Midnight5 pm12 noon
Time
600
400
200
0
Meal Meal Meal
Koda et al, Diabetes. 1995; 44 (s1): 23BA.Data on file. (Fineman)
AmylinAmylin
Secreted by pancreatic beta-cellsSecreted by pancreatic beta-cells An anorectic hormoneAn anorectic hormone Works on the brain to stimulate the Works on the brain to stimulate the
feeling of satiety.feeling of satiety. This results in decreased G.I. This results in decreased G.I.
motility, slowed carbohydrate motility, slowed carbohydrate absorption, and decreased appetite.absorption, and decreased appetite.
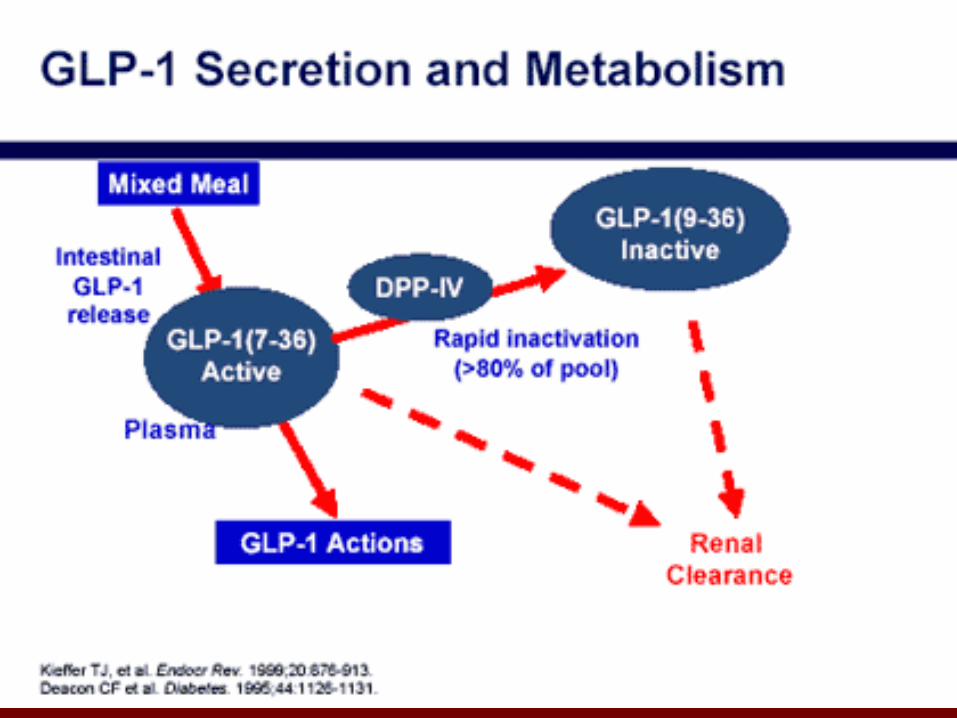
GLP-1GLP-1 ““Incretin” hormone secreted by jejunal Incretin” hormone secreted by jejunal
and ileal L cells in response to a mealand ileal L cells in response to a meal Stimulates insulin secretionStimulates insulin secretion Decreases glucagon secretionDecreases glucagon secretion Slows gastric emptyingSlows gastric emptying Reduces fuel intake (increases satiety)Reduces fuel intake (increases satiety) Improves insulin sensitivityImproves insulin sensitivity Increases Increases -cell mass and improves -cell mass and improves --
cell function (animal studies)cell function (animal studies)
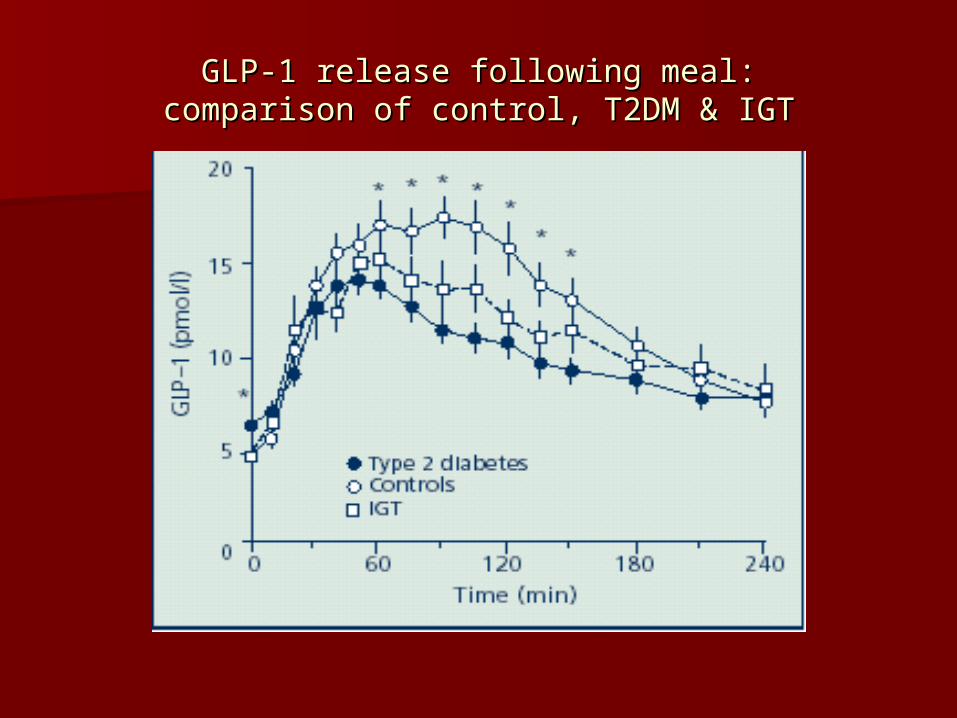
GLP-1 release following meal:GLP-1 release following meal:comparison of control, T2DM & IGTcomparison of control, T2DM & IGT
Diabetes Diabetes PathophysiologyPathophysiology
Diabetes is a Diabetes is a Multi-Hormonal DiseaseMulti-Hormonal Disease
Pancreatic hormonesPancreatic hormones– Insulin (Insulin (-cell)-cell)– Glucagon (Glucagon (-cell)-cell)– Amylin (Amylin (-cell)-cell)
Intestinal Hormones (Incretins) Intestinal Hormones (Incretins) – GLP-1 (L-cells)GLP-1 (L-cells)– GIP (K-cells)GIP (K-cells)
Type 1 Diabetes: Type 1 Diabetes: PathophysiologyPathophysiology
Impaired insulin secretionImpaired insulin secretion– Absolute insulin deficiencyAbsolute insulin deficiency
T1DMT1DM
Typically autoimmune (~90%)Typically autoimmune (~90%) Beta-cells destroyed by multiple Beta-cells destroyed by multiple
antibodies.antibodies. Can occur at any age (but more in kids)Can occur at any age (but more in kids) Fast progression (the older the slower)Fast progression (the older the slower) Related to ketones @ Related to ketones @
– Urine ketonesUrine ketones– KetoacidosisKetoacidosis
Weight loss, N&V, lethargyWeight loss, N&V, lethargy
KetogenesisKetogenesis
Normal physiological responses to Normal physiological responses to carbohydrate shortages cause the carbohydrate shortages cause the liver to increase the production of liver to increase the production of ketone bodies from the acetyl-CoA ketone bodies from the acetyl-CoA generated from fatty acid oxidation. generated from fatty acid oxidation.
Allows the heart and skeletal Allows the heart and skeletal muscles primarily to use ketone muscles primarily to use ketone bodies for energy, thereby bodies for energy, thereby preserving the limited glucose for preserving the limited glucose for use by the brain use by the brain
HoneymooningHoneymooning
The ability of the failing b-cells to The ability of the failing b-cells to become hyper-productive and become hyper-productive and compensate for failing insulin compensate for failing insulin
response.response.
T2DMT2DMDiagnosis characteristicsDiagnosis characteristics
InsidiousInsidious Obesity (almost always), or weight gainObesity (almost always), or weight gain Related to other IRS signsRelated to other IRS signs
– Hyperlipidemia, acanthosis nigricansHyperlipidemia, acanthosis nigricans Older (Older (↑Obesity = ↓Age; fatter = ↑Obesity = ↓Age; fatter =
youngeryounger)) Ethnic linksEthnic links Family history of T2DMFamily history of T2DM No ketonesNo ketones
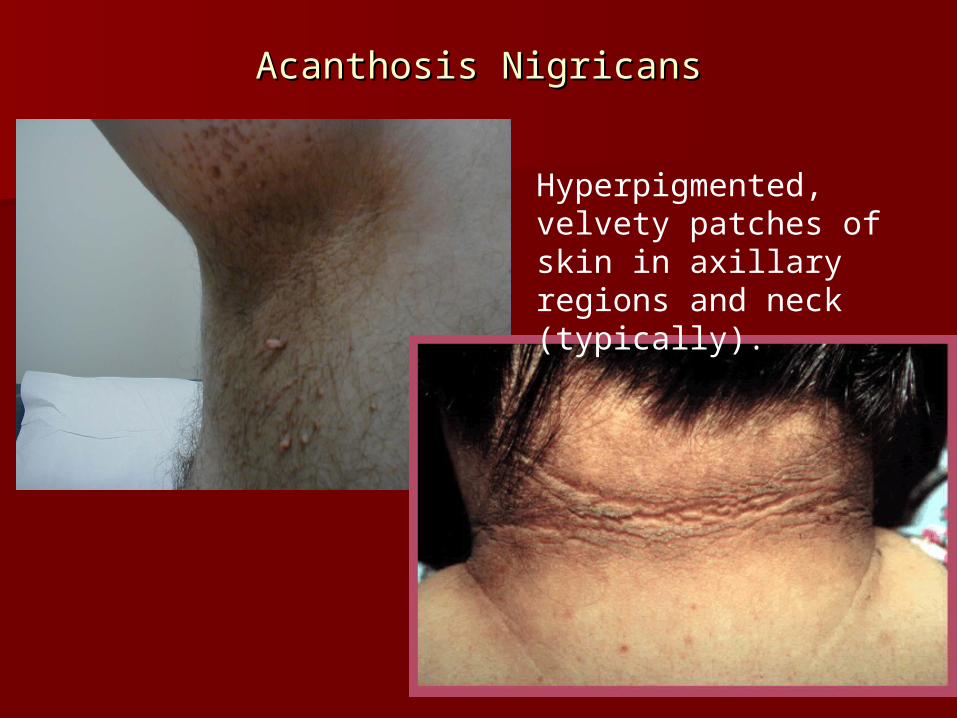
Acanthosis NigricansAcanthosis Nigricans
Hyperpigmented, velvety patches of skin in axillary regions and neck (typically).
Type 2 Diabetes: Type 2 Diabetes: PathophysiologyPathophysiology
Impaired insulin secretionImpaired insulin secretion– Absolute or Absolute or relativerelative insulin insulin
deficiencydeficiency
Impaired insulin action Impaired insulin action (sensitivity)(sensitivity)– Insulin resistanceInsulin resistance
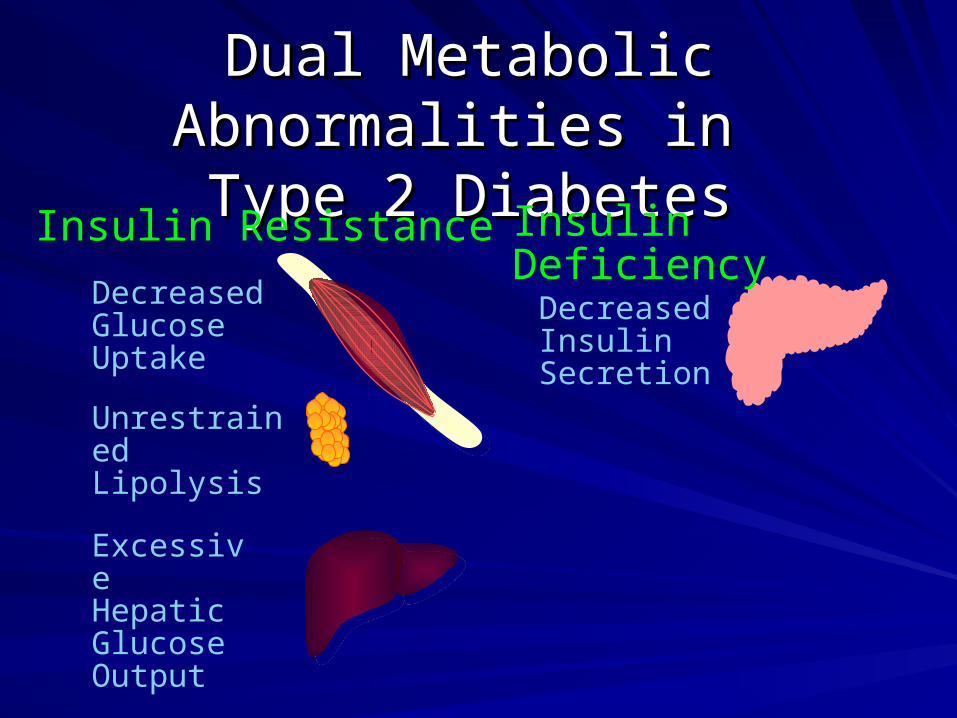
Dual Metabolic Abnormalities in Dual Metabolic Abnormalities in
Type 2 DiabetesType 2 Diabetes
Excessive HepaticGlucose Output
Decreased Glucose Uptake
Insulin DeficiencyInsulin Resistance
Decreased Insulin Secretion
Unrestrained Lipolysis
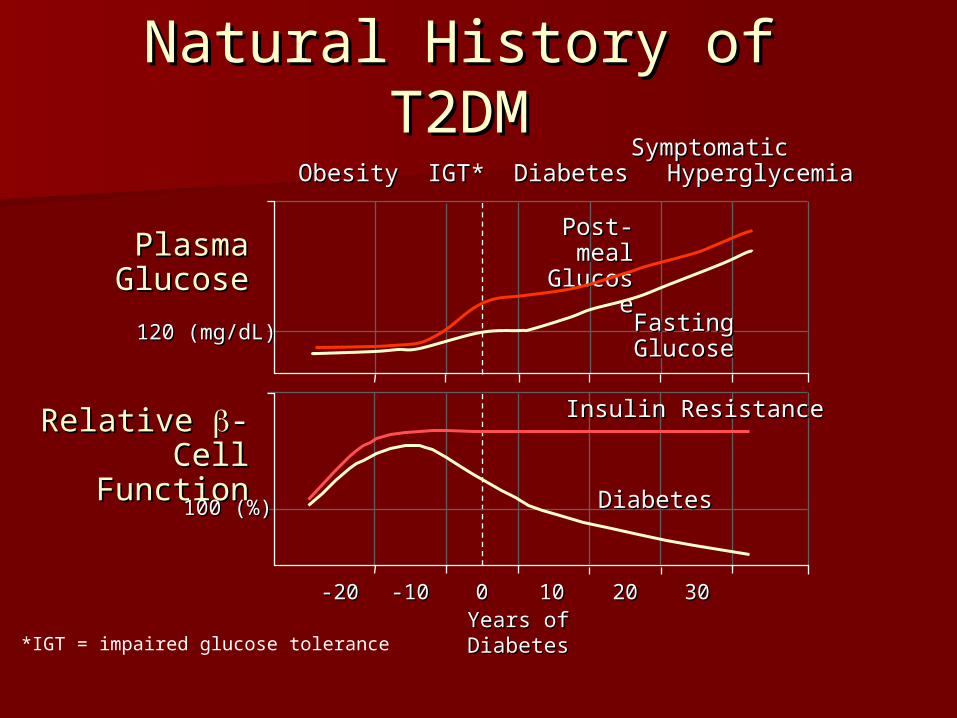
Natural History of T2DMNatural History of T2DM
*IGT = impaired glucose toleranceYears of Years of DiabetesDiabetes
SymptomaticSymptomatic Obesity Obesity IGT* Diabetes IGT* Diabetes HyperglycemiaHyperglycemia
Relative Relative -Cell -Cell FunctionFunction
100 (%)100 (%)
-20-20 -10-10 00 1010 2020 3030
PlasmaPlasmaGlucoseGlucose
Insulin ResistanceInsulin Resistance
DiabetesDiabetes
120 (mg/dL)120 (mg/dL) Fasting Fasting GlucoseGlucose
Post-Post-meal meal
GlucoseGlucose
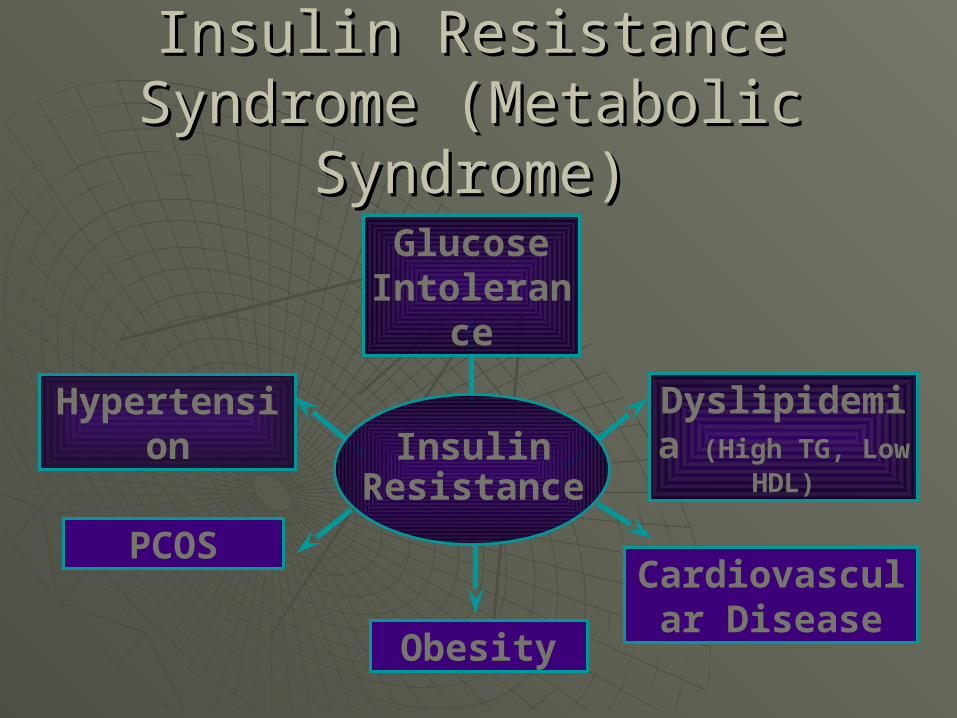
InsulinResistance
Glucose Intolerance
Obesity
Dyslipidemia (High TG, Low HDL)
Cardiovascular Disease
Hypertension
PCOS
Insulin Resistance Syndrome Insulin Resistance Syndrome (Metabolic Syndrome)(Metabolic Syndrome)
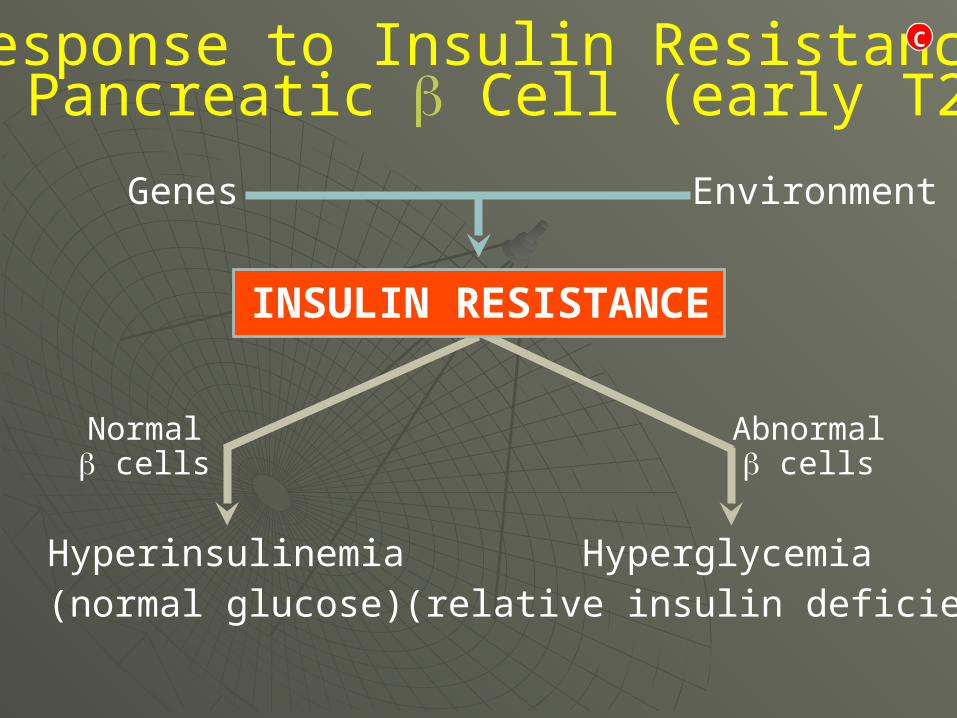
Response to Insulin Resistance:The Pancreatic Cell (early T2DM)
EnvironmentGenes
INSULIN RESISTANCE
Hyperglycemia(relative insulin deficiency)
Hyperinsulinemia(normal glucose)
Normal cells
Abnormal cells
C
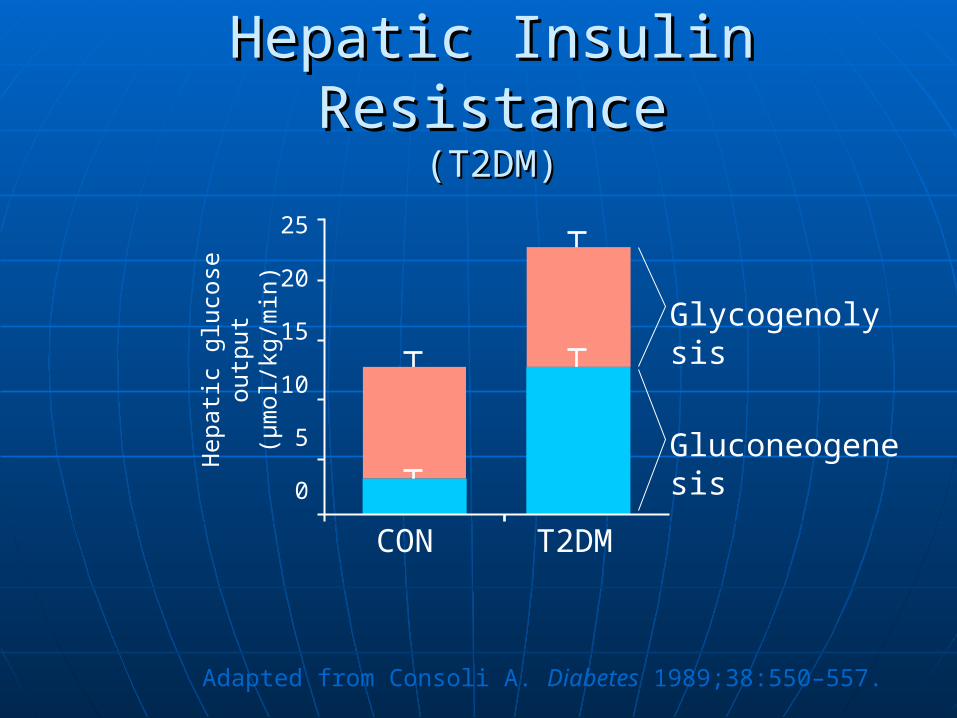
Hepatic Insulin ResistanceHepatic Insulin Resistance(T2DM)(T2DM)
Adapted from Consoli A. Diabetes 1989;38:550–557.
Hep
atic
glu
cose
out
put
(µm
ol/k
g/m
in)
CON
25
20
15
10
5
0
T2DM
Glycogenolysis
Gluconeogenesis
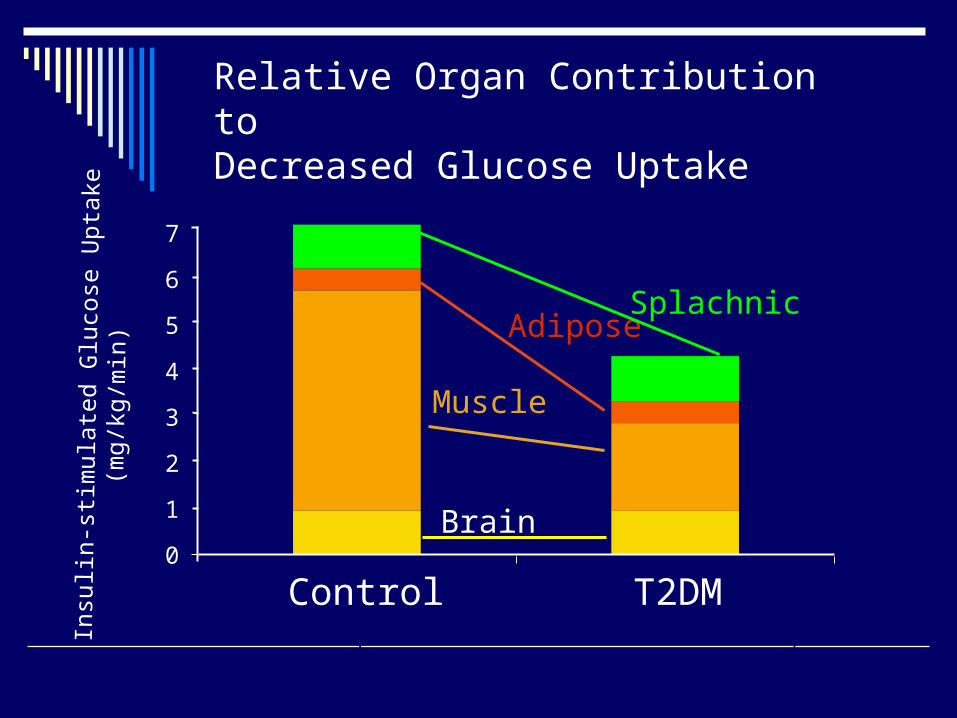
Relative Organ Contribution to Decreased Glucose Uptake
Control T2DM
Adapted from DeFronzo RA. Diabetes 1988;37:667–687.
Brain
Muscle
Adipose
7
6
5
4
3
2
1
0
Splachnic
Insu
lin-
stim
ulat
ed G
luco
se U
ptak
e(m
g/kg
/min
)
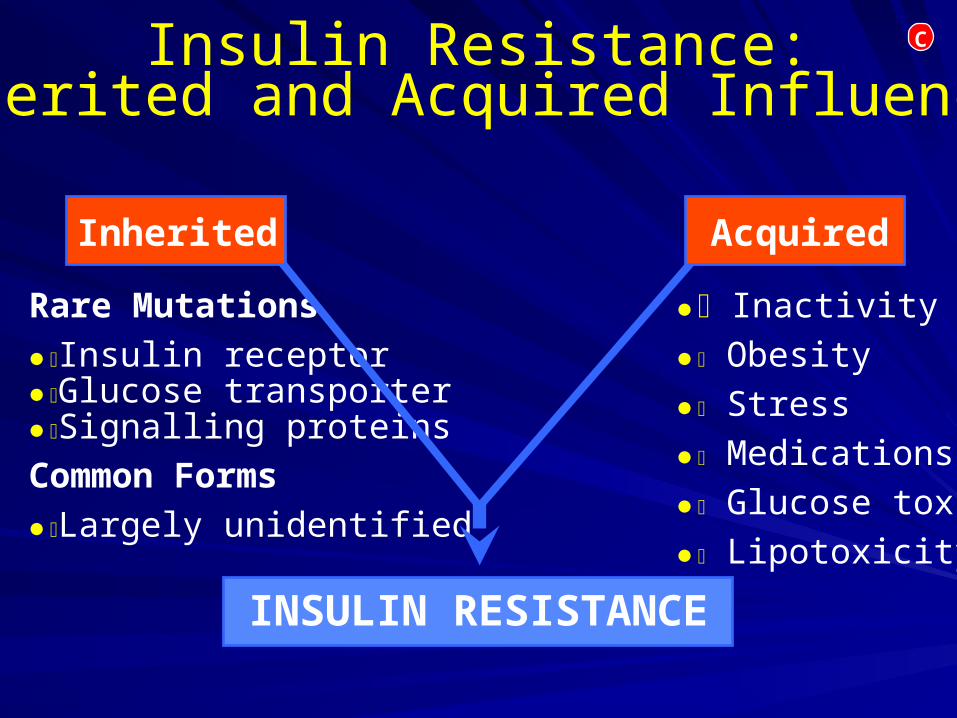
Insulin Resistance:Inherited and Acquired Influences
Rare Mutations
Insulin receptorGlucose transporterSignalling proteins
Common Forms
Largely unidentified
Inactivity
Obesity
Stress
Medications
Glucose toxicity
Lipotoxicity
INSULIN RESISTANCE
AcquiredInherited
C
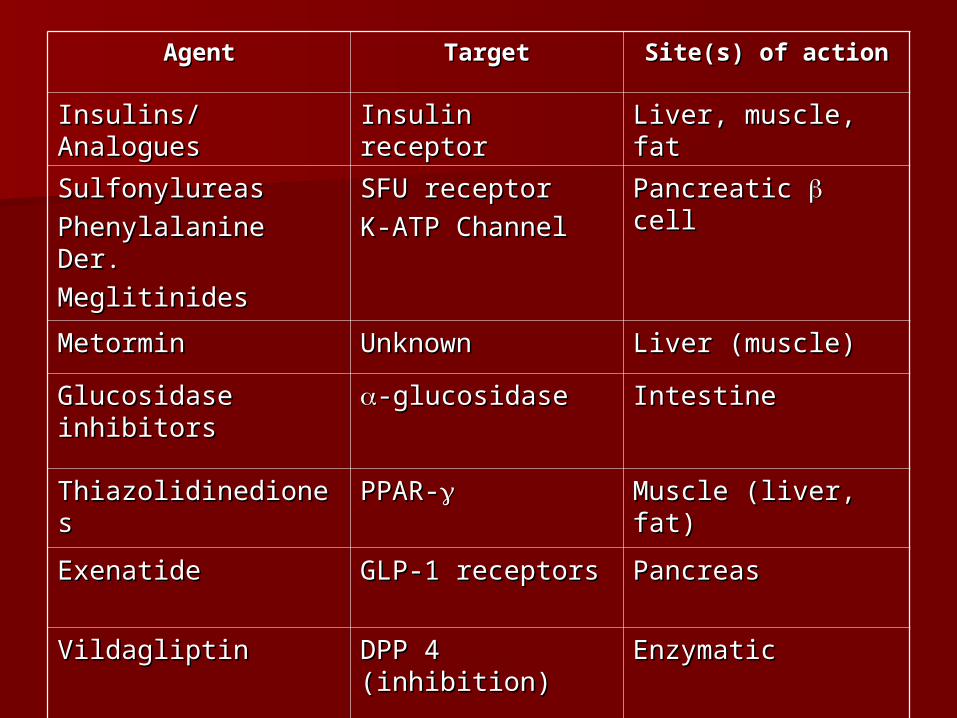
AgentAgent TargetTarget Site(s) of actionSite(s) of action
Insulins/AnaloguesInsulins/Analogues Insulin receptorInsulin receptor Liver, muscle, fatLiver, muscle, fat
SulfonylureasSulfonylureas
Phenylalanine Der.Phenylalanine Der.
MeglitinidesMeglitinides
SFU receptorSFU receptor
K-ATP ChannelK-ATP ChannelPancreatic Pancreatic cell cell
MetorminMetormin UnknownUnknown Liver (muscle)Liver (muscle)
Glucosidase Glucosidase inhibitorsinhibitors
-glucosidase-glucosidase IntestineIntestine
ThiazolidinedionesThiazolidinediones PPAR-PPAR- Muscle (liver, fat)Muscle (liver, fat)
ExenatideExenatide GLP-1 receptorsGLP-1 receptors PancreasPancreas
VildagliptinVildagliptin DPP 4 (inhibition)DPP 4 (inhibition) EnzymaticEnzymatic
Atypical diabetesAtypical diabetes
Idiopathic type 1 diabetesIdiopathic type 1 diabetes
Also known as “Flatbush diabetes”Also known as “Flatbush diabetes” African American and Asian men (18-African American and Asian men (18-
25)25) Fluctuating insulin secretionFluctuating insulin secretion No antibodiesNo antibodies Many honeymoonsMany honeymoons
LADALADA Latent autoimmune diabetes of Latent autoimmune diabetes of
adulthoodadulthood Like type 1 but diagnosed after age 25.Like type 1 but diagnosed after age 25. ~20% of those with diagnosis of T2 may ~20% of those with diagnosis of T2 may
actually have LADA.actually have LADA. Slower onset than type 1 dm.Slower onset than type 1 dm. Positive antibodies.Positive antibodies. Low or no c-peptideLow or no c-peptide No family historyNo family history
MODYMODY
Maturity Onset Diabetes of the YoungMaturity Onset Diabetes of the Young A collection of many (at least 6) A collection of many (at least 6)
inherited diseases affecting insulin inherited diseases affecting insulin secretion.secretion.
Dominant inheritance characteristicsDominant inheritance characteristics Normal insulin sensitivityNormal insulin sensitivity Impaired insulin secretion (but still Impaired insulin secretion (but still
some).some). Diagnosis confirmed by genetic testing.Diagnosis confirmed by genetic testing.
Pancreatic DiabetesPancreatic Diabetes
Results from a failure of the pancreas Results from a failure of the pancreas as a whole.as a whole.
May be secondary to ETOH abuse, May be secondary to ETOH abuse, trauma, repeat pancreatitis.trauma, repeat pancreatitis.
Exocrine pancreas generally fails Exocrine pancreas generally fails before endocrine pancreas.before endocrine pancreas.
Will need pancreatic enzyme Will need pancreatic enzyme replacement as well as insulin.replacement as well as insulin.
Gestational diabetesGestational diabetes
Any glucose intolerance first Any glucose intolerance first diagnosed during pregnancydiagnosed during pregnancy– Some definitions require return to Some definitions require return to
normal following end of pregnancy.normal following end of pregnancy.
Closely related to T2DMClosely related to T2DM Treat only with insulinTreat only with insulin
– Some data support the use of SUs & Some data support the use of SUs & metformin.metformin.
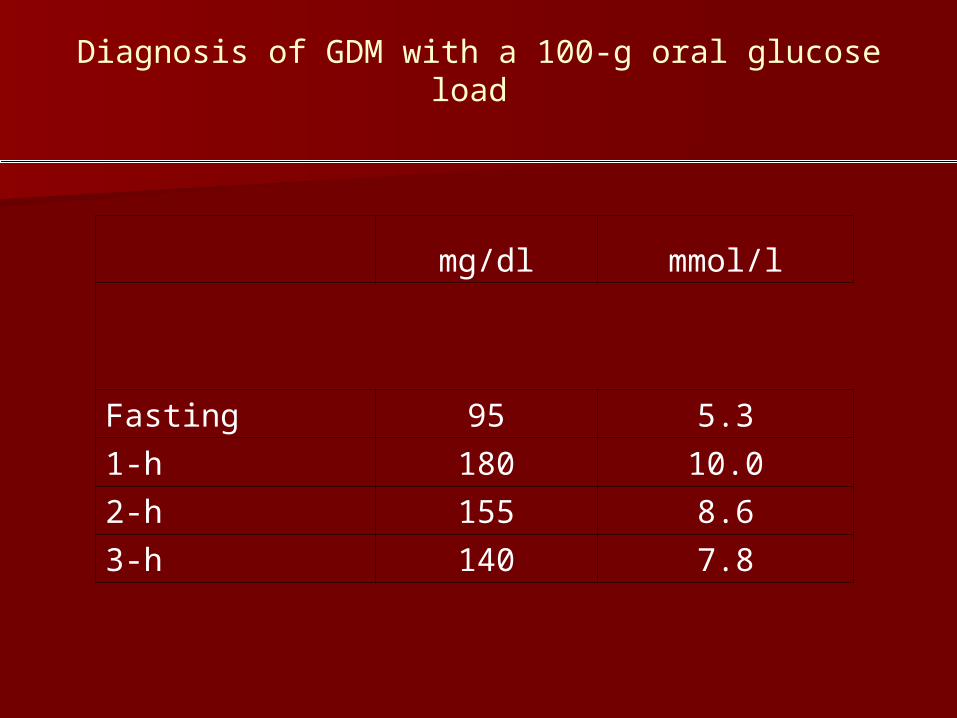
mg/dl mmol/l
Fasting 95 5.3
1-h 180 10.0
2-h 155 8.6
3-h 140 7.8
Diagnosis of GDM with a 100-g oral glucose load
A1C monitoringA1C monitoring
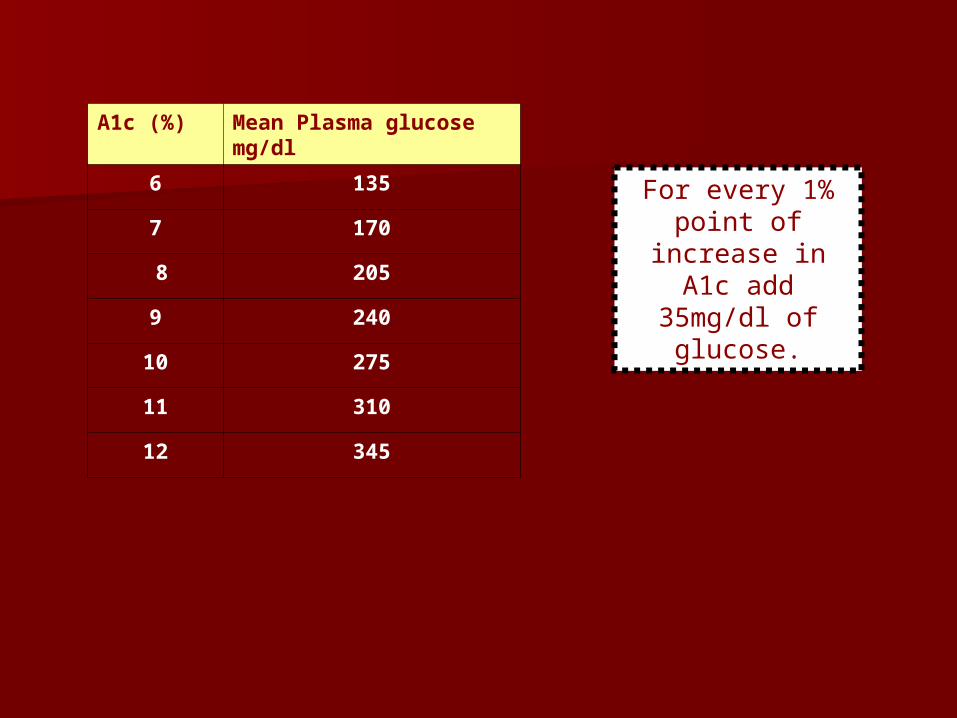
For every 1% point of increase in A1c
add 35mg/dl of glucose.
A1c (%) Mean Plasma glucose mg/dl
6 135
7 170
8 205
9 240
10 275
11 310
12 345
False A1C ReadingsFalse A1C Readings
ElevatedElevated– Iron deficiency Iron deficiency
anemiaanemia– SplenectomySplenectomy
DecreasedDecreased– Hemolytic anemiaHemolytic anemia– Sickle cell anemiaSickle cell anemia– TransfusionTransfusion
ADA GuidelinesADA Guidelines
http://www.diabetes.org/http://www.diabetes.org/
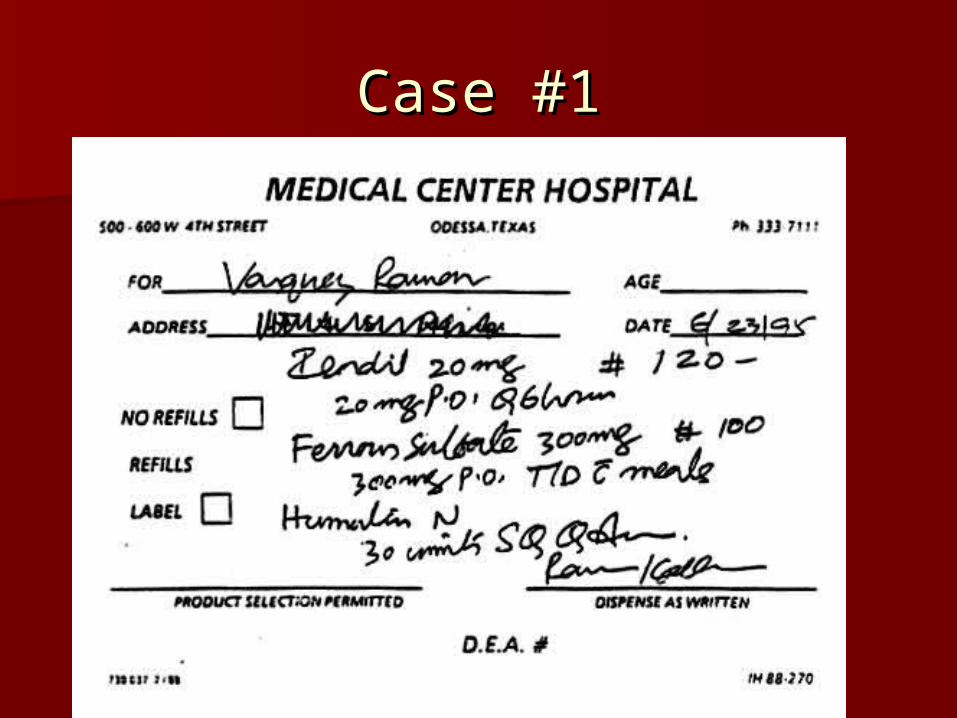
Case #1Case #1