Embed Size (px)
Citation preview

Global Journal of Oral Science, 2017, 3, 27-32 27
E-ISSN-2414-2050 © 2017 Global Journal of Oral Science
Management of Natal Teeth in a Preterm Neonate - A Case Report
Saleha Shah*
Aga Khan University Karachi, Karachi, Pakistan Abstract: A 24 day old preterm neonate was referred to the dental clinic by his paediatrician. Subsequent to an extra and intra oral clinical assessment he was diagnosed with an erupted, grade III mobile mandibular right natal tooth and an unerupted mandibular left natal tooth. Subsequently the right natal tooth was extracted, preventive advice imparted and a follow up for extraction of the erupted left natal tooth was advised. Hence this case report elucidates the identification of natal teeth in neonates and highlights the clinical management of natal teeth with respect to their underlying systemic considerations.
Keyword: Infant, Haematology, Natal teeth, Premature birth.
1. INTRODUCTION
Paediatric dentistry delivers primary and compre- hensive preventive and therapeutic oral health care for infants and children through adolescence, inclusive of special health care need [1]. The purpose of a child’s dental examination entails disease identification in con- junction with assessment of growth and development in physical, cognitive and psychosocial spheres. Dentists are often the first clinicians to recognize significant disease and anomalies [2] and decide on an appro- priate treatment. In addition emergency care for infants, children and adolescents is essential for every dentist [3].
Natal teeth are defined as teeth, which are present at birth whereas neonatal teeth are those erupting during the first 30 days of life [4,5] and the anterior natal and neonatal teeth are a part of the normal set of dentition [4,5]. The teeth erupting earlier are also referred to as congenital teeth, fetal teeth, predecidual teeth and dentitia praecox [6,7]. They diverge from 1:6000 to 1:800 cases with an incidence from 1:700 to 1:30,000 with a predilection for females [8]. Natal teeth are three times more common than neonatal teeth with the localization being the mandibular region of central incisors (85%), followed by maxillary incisors (11%), mandibular cuspids or molars (3%) and maxillary cusp- ids or molars (1%). Natal teeth are a rare manifestation [9]. A strong predilection for the lower central incisors is their normal eruption sequence. Clinical features like mobility raise concerns about possible ingestion or aspiration by infants during nursing. Full infant care during the first year of life maintains child oral health and addresses the dental needs in a more preventive conduct.
*Address correspondence to this author at the Aga Khan University Karachi, Karachi, Pakistan; E-mail: [email protected]
It is important to understand the difference between early eruption and premature eruption. Although seve- ral theories exist about why the teeth erupt prema- turely, none of the current studies have been able to confirm a causal relationship with any of the theories suggested. The most accepted possibility seems to be the superficial tooth germ position associated with a hereditary factor [5]. Natal and neonatal teeth can present a challenge when deciding on appropriate treatment. Hence medically necessary dental care prevents and eliminates pain, infection and orofacial disease, restores dentition form and function and corrects facial disfiguration or dysfunction. This not only increases the probability of good health and wellbeing but also decreases unfavorable outcomes [10].
This case is unique with reference to the relevant literature because it apprises that a paediatric dentist should be able to prudently identify full term and preterm infants with prematurely erupted teeth with underlying systemic consideration; aptly assess, examine, diagnose, treat and manage a preterm child with heritable dental developmental anomalies with due hematological considerations and parental counseling for the holistic wellbeing of a child.
CLINICAL CASE
A 24 day old preterm Asian boy referred to the AKUH Dental Clinic by his pediatrician at AKUH attended with parental concerns of a baby tooth since birth and an external feeding tube. Medical history indicated a single live born preterm baby boy delivered by a cesarean section at 33-34 weeks of gestation weighing 1.16kg with Apgar scores 7 at the 1st minute and 9 at the 5th minute. Other conditions associated with preterm birth comprised of an intra-ventricular hemorrhage Grade 1, sepsis of new born, neonatal hypoglycemia, transitory tachypnea of newborn and an undescended testis and neonatal jaundice after 24

28 Global Journal of Oral Science, 2017, Vol. 3 Saleha Shah
hours. The baby was shifted from the Operating Room to Neonatal Intensive Care Unit for low birth weight and care of prematurity. Oxygen inhalation was initiated and tapered off. The 1st dose of IV antibiotics and dexamethasone were administered twenty three hours later, single phototherapy for neonatal jaundice and low platelets, polycythemia, hypernatremia and sepsis of new born were managed by a par enteral parenteral infusion of concentrated nutritional substances, Ome- prazole 5MG/SYR, Domperidone 1MG/ML, Normal Saline vial 25ML/vial and cefotaxime and amikacin sulphate 50, G/ML AMP. Feeding commenced after shifting to step down. Cot was shifted after the incu- bator trial and he was discharged on attaining stability. Social history indicated a middle income background and a history of consanguineous parents.
The baby was placed supine and assessed clin- ically. An erupted right mandibular incisor prenatal tooth with a pale translucent crown, grade III mobility with a risk of aspiration and an unerupted left mandi- bular natal tooth were noticed on intraoral examination. His head was stabilized by his mother and the mouth opened with gentle but firm digital pressure. A gauze was placed lingual to the natal tooth, Topical Benzo- caine 20% applied locally on the gingiva surrounding the mobile right mandibular prenatal tooth to achieve
analgesia and the root less tooth extracted to allay risk of aspiration Hemostasis was achieved by gentle digital pressure on moist gauze. A follow up for the extraction of lower left mandibular prenatal tooth subsequent to its eruption was advised. Preventive advice included appropriate oral hygiene instructions as the primary teeth begin to erupt and dietary recommendations to ensure good general health, nutritional, developmental, psychological, social, economic, and environmental advantages and decreasing risk of acute and chronic diseases. The parents however did not comply for a follow up visit despite a telephonic reminder.
DISCUSSION
Premature/Preterm children are born in less than 37 weeks of gestation whereas full term is birth in 37- 42 weeks of gestation or after 42 weeks. About 5-10 % of all childbirths are preterm. Causes of low birth weight may include primary predictors: infection, severe ane- mia, heart and renal disease, multiple pregnancies, maternal smoking, preeclampsia, diabetes, stress, fam- ily history, domestic violence, young mothers, low BMI and low socioeconomic status. Secondary indicators include IVF, low maternal weight, multiple fetuses, hydroaminosis, inadequate fetal care and other causes [34].
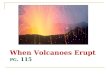
Figure 1: Extraoral view of a natal tooth.

Management of Natal Teeth in a Preterm Neonate Global Journal of Oral Science, 2017, Vol. 3, 29
Problems in Preterm and low birth weight depend on the degree of prematurity. They may suffer from apnoea or irregular breathing (hyaline membrane dis- ease and respiratory insufficiency), hyperbilirubinemia, necrotizing enterocolitis, cerebral intraventricular haemorrhage, oxygen retinopathy, inactivity, weak cry, poor feeding, lanugo (shiny wrinkled skin with fine body hair), flexible ear cartilage, enlarged clitoris or small scrotum, less able to maintain body temperature and hemostasis. Long term sequelae include low IQ, co- ordination problems, respiratory problems, behavioral disorders and feeding problems [11,12].
Preterm underlying systemic disturbances often lead to typical clinical manifestations which have to be identified and managed accordingly. Hyperbilirubinemia leads to intrinsic tooth staining, trauma from intubation (laryngoscopy) causes enamel hypoplasia/ hypocalci- fication in the maxillary central incisors typically while chronological opacities or hypoplasia manifest as an alteration in amelogenesis, hypoglycaemia & hypocal- cemia with pseudohyperparathyroidism. Children have multiplecomplex problems as their dental conditions affect both form and function and can have significant psychological impact. These conditions may present early in life and require both immediate intervention and management of a protracted nature including coordination of multi-disciplinary care [12].
Any physical, developmental, mental, sensory, be- havioral, cognitive, or emotional impairment or limiting
condition are considered as special health care needs requiring medical management, health care interven- tion, and/or use of specialized services or programs [13]. Perinatal health commences with the completion of 20th through 28th week of gestation and concludes one to four weeks after birth. It depends on the overall health and well-being of pregnant women [14]. Infant oral health is a fundamental upon which age-appro- priate preventive education and dental care must be built to augment the prospect for a lifetime free from preventable oral disease. By the age of six months an infant should receive oral health risk assessment from primary health care providers or qualified health care professionals to evaluate the patient’s risk of develop- ing oral diseases of soft hard tissues, include caries-risk assessment, provide education on infant oral health and evaluate and improve fluoride exposure [14,15].
Developmental abnormalities and syndromes inclu- ding Ellis-van Creveld (chondroectodermal dysplasia), pachyonychia congenita (Jadassohn-Lewandowsky), Hallerman-Streiff (occulo-mandibulo dyscephaly with hypotrichosis), Rubinstein-Taybi, steatocystoma multi- plex, Pierre-Robin, cyclopia, Pallister-Hall, short rib-polydactyly type II, Wiedeman-Rautenstrauch (neonatal progeria), cleft lip and palate, Pfeiffer, ectodermal dys- plasia, craniofacial dysostosis, multiple steacystoma, Sotos, adrenogenital, epidermolysis bullosa simplex including van der Woude and Walker-Warburg Synd- romes are frequently associated with natal and neo- natal teeth [16-23].
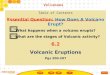
Figure 2: Setup for extraction of a natal tooth.

30 Global Journal of Oral Science, 2017, Vol. 3 Saleha Shah
Morphologically natal teeth are conical or maybe of usual size and shape, brown-yellowish/whitish opaque in color and immature with enamel hypoplasia and small root formation. The crown is smaller than primary teeth and attached to soft tissue above the alveolar ridge, maybe covered by mucosa with resultant magnified crown mobility. Degree of maturity by Spoug and Feasby (1966) defines a mature natal tooth as fully developed in shape and comparable to primary tooth morphology with a good prognosis for maintenance whereas an immature tooth having an incomplete structure and development with poor prognosis. The eruption time is not as important as their degree of maturity hence a mature natal tooth has better prognosis than an immature tooth as does a tooth stable beyond four months. If the mobility exceeds 2 mm natal teeth necessitate an extraction [24-26]. If the tooth mobility is not marked or leads to feeding problems it should be conserved and maintained in a healthy condition [27]. Close monitoring is indicated to ensure that the tooth remains stable.
Classification of natal teeth is literature based into four clinical categories [26,28]:
1. Shell-shaped crown fixed poorly to the alveolus by gingival tissue and absence of a root.
2. Solid crown fixed poorly to the alveolus by gingival tissue and little or no root.
3. Eruption of crown incisal margin through the gingival tissues.
4. Edematous gingival tissue with an unerupted but palpable tooth.
Histologically thin enamel with varying degrees of mineralization and/or hypoplastic to total absence of enamel is present. Alteration in amelogenesis due to premature tooth eruption results in metaplastic altera- tion of the normal columnar epithelium to stratified squamous epithelium [29,30]. Dentine is normal except some irregular dentinal tubules in the cervical third. Osteodentin formed via stimulation by tooth movement may cause a gradual decrease in the number of den- tinal tubules from the crown to the cervical region and degeneration of Hertwigs sheath which prevents root development and stabilization [23]. Increased mobility causes lack of cementum development. The pulp shows normal development however pulp cavity and the radicular canals are wider [24]. Weil's zone and cell-rich zone are missing [28]. Posterior natal tooth should be investigated for other systemic conditions,
syndromes or anomalies [31]. The literature reflects the association of natal teeth with reactive fibrous hyper- plasia [28] congenital hydrocephalus associated with congenital glaucoma Walker Warburg syndrome, [32] bilateral mandibular hamartomas, [32] pyogenic gra- nuloma, [33] peripheral ossifying fibroma, eruption cyst, [8] gingival fibrous hamartoma [34]. It is also important to consider other lesions like cysts and developmental disturbances in neonates hence a complete oral examination is recommended in newborns, in order to establish the differential diagnosis.
Clinical and radiographic diagnosis of natal and neonatal determines whether the teeth belong to the normal dentition or are supernumerary to avoid indis- criminate extractions [35]. Natal correspond to normal primary dentition in 95% of cases whereas 5% are supernumerary [6]. They are located in the lower incisor region usually [36]. Multiple natal teeth are extremely rare however some report involvement of natal molars and canines in the literature [30,37]. Other oral lesions similar to them include cysts of the dental lamina and Bohn nodules. A correct diagnosis for the maintenance of natal and neonatal teeth of the normal dentition prevents premature primary tooth loss, which may cause space loss and collapse of the developing mandibular arch with a resultant malocclusion in the permanent dentition [26].
The treatment plan in the presence of natal and neonatal teeth may contribute a doubt in deciding retention versus extraction. Various factors like degree of mobility, inconvenient suckling, interference with breast feeding and possibility of traumatic injury ascer- tain whether the tooth is part of the normal dentition or is supernumerary [38]. When well implanted, they should be left in the arch. Their removal should be indicated only if they interfere with feeding, are highly mobile with a risk of dislocation and consequent aspiration or if they have a potential for traumatic injury to the baby’s tongue and/or to the maternal breast, soft tissue growth and caries [39-41].
Riga-Fede disease is caused by the mobile natal or neo-natal tooth rubbing the ventral surface of the tongue during feeding, leading to ulcerative lesion [42]. Inability to diagnose and treat may result in dehydration and inadequate infant nutritional intake [43]. Treatment should be conservative and create round, smooth incisal margins to prevent wounding of the maternal breast during breast-feeding. If conservative treatment does not correct the condition, extraction is the treatment of choice [44].

Management of Natal Teeth in a Preterm Neonate Global Journal of Oral Science, 2017, Vol. 3, 31
Potential for hemorrhage is an important considera- tion when deciding to extract a natal or neonatal tooth. Extraction is contraindicated in newborns due to risk of hemorrhage [35]. However unless the child is at least 10 days old consultation with the pediatrician regarding adequate hemostasis may be indicated prior to tooth extraction to assess the need for vitamin K admin- istration. The general health and wellbeing of the baby should be evaluated as well as and care must be taken to avoid unnecessary gingival trauma, damage to per- manent tooth buds, prevent residual remnants of the dental papillae from proliferating and allay aspiration risk during a tooth extraction. The airway is protected with gauze since teeth may easily drop or dislodge, spencer welis forep provides a firm grip for removal. Alternatively a finger may also be used for extraction. A periodic follow-up by a pediatric dentist to ensure preventive oral health care is very essential [33].
This waiting period prior to a tooth extraction is for the intestinal commensal flora to become established and start vitamin K production essential for the pro- ducing prothrombin in the liver [35,39]. If it is not possible to wait for 10 days then valuate the need for administration of vitamin K with a pediatrician. If vitamin K is not medicated immediately after birth in the newborn then vitamin k (0.5-1.0 mg) is administered intramuscularly to prevent hemorrhagic disease of the newborn as part of immediate medical care [45]. Lite- rature has reported cases of spontaneous tooth exfoliation as well [46]. Teeth stable past four months have a good prognosis even if they are not pleasing esthetically due to discoloration [47].
Other factors to consider are the genetic blue print which indicate the rate at which a baby's teeth come through [48]. Hereditary transmission of a dominant autosomal gene is another important factor to be considered [28,49]. Bodenhoff and Gorlin show that 15% of children with natal and neonatal teeth had a history of the same presenting condition in either their parents, siblings or close relatives [24]. Endocrine dis- turbances are thought to be due to excessive secretion of the pituitary, thyroid or gonads. Osteoblastic activity within the area of the tooth germ may be contributory [24,49]. Infections such as Congenital syphilis could to a varying degree accelerate or decelerate early erup- tion including nutritional deficiency such as hypovita- minosis [49]. Fever, exanthemata during pregnancy tend to accelerate eruption as they do in various other processes. Superficial position of tooth germ alongside [49] environmental factors such as Polychlorinated biphenyls (PCB) and dibenzofurans seem to increase the incidence of natal teeth [50].
CONCLUSION
Professional care for oral health maintenance and risk assessment is an integral part of contemporary preventive care for infants, children, adolescents, and persons with special health care needs. A paediatric dentist should be able to prudently identify full term and preterm infants with prematurely erupted teeth with underlying systemic consideration; be able to appro- priately assess, examine, diagnose, treat and manage a preterm baby with heritable dental developmental anomalies with due hematological considerations and parental counseling for the holistic wellbeing of a child. For future reference studies should be planned to enable the understanding of etiology, anatomical con- siderations and type of dentition of natal teeth.
ERUDITION
Natal and neonatal teeth are a rare manifestation in the oral cavity of a neonate.
Differentiation between natal and primary teeth matters for subsequent management.
The treatment decision on retention versus extrac- tion of a natal and/or neonatal tooth is based on clinical presentation, evidence based practice and parental consent.
Radiographic examination where possible augments differential diagnosis between supernumerary pri- mary teeth and teeth of the normal dentition.
Potential for hemorrhage due to hypoprothrombi- nemia is an important consideration when deciding to extract a natal or neonatal tooth
Teeth from primary dentition should be maintained in a healthy oral cavity.
REFERENCES
[1] American Dental Association Commission on Dental Accreditation. Accreditation standards for advanced spe-cialty education programs in pediatric dentistry. Chicago, Ill.; 2013.
[2] Goncalves FA, Birmani EG, Sugayai NN, Melo AM. Natal teeth: Review of literature and report of an unusual case. Braz Dent J. 1998; 9: 53-6.
[3] American Dental Association. Principles of Ethics and Code of Professional Conduct. Available at: “http://www. ada.org/sections/about/pdfs/code_of_ethics_2012. pdf ” Accessed June 24, 2012.
[4] Cunha RF, Boer FA, Torriani DD, Frossard WT. Natal and neonatal teeth: Review of the literature. Pediatr Dent. 2001; 23(2): 158-62.
[5] Leung A, Robson W. Natal teeth: A review. J Natl Med Assoc. 2006; 98(2): 226-8.
[6] Massler M, Savara BS. Natal and neonatal teeth: a review of 24 cases reported in the literature. J Pediatr. 1950; 36: 349-359.

32 Global Journal of Oral Science, 2017, Vol. 3 Saleha Shah
[7] Anegundi RT, Sudha P, Kaveri H, Sadanand K. Natal and neonatal teeth: A report of four cases. J Indian Soc Pedo Prev Dent. 2002; 20: 86-92.
[8] Singh S, Subbba Reddy VV, Dhananjaya G, Patil R. Reactive fibrous hyperplasia associated with a natal tooth: A case report. J Indian Soc Pedo Prev Dent. 2004; 22: 183-6.
[9] Bigeard L, Hemmerle J, Sommermater JI. Clinical and ultrastructural study of the natal tooth: enamel and dentin assessments. J Dent Child 1996; 63: 23-31.
[10] Definition of Medically Necessary Care, American Academy of Paediatric Dentistry Oral Health Policy, 2014.
[11] Crispian Scully, Oral Health Issues; Age and Gender issues; Chapter 25; Medical Problems in Denstistry; 6th Edition, Elsevier.
[12] American Academy of Paediatric Dentistry, Guideline on Dental Management of Heritable Dental Development, Reference Manual 2013; 36(6): 14-15.
[13] American Academy of Pediatrics: Guideline on Infant Oral Health Care; Reference Manual 2014; 36(6): 14-1.
[14] American Academy of Pediatric Dentistry. Guideline on periodicity of examination, preventive dental services, anticipatory guidance/counseling, and oral treatment for infants, children, and adolescents. Pediatr Dent. 2010; 32(special issue): 93-100.
[15] American Academy of Pediatrics. Policy on oral health risk assessment timing and establishment of the dental home. Pediatrics 2003; 111(5Pt1): 1113-6.
[16] Portela MB, Damasceno L, Primo LG. Unusual case of multiple natal teeth. J Clin Pediatr Dent. 2004; 29: 37-9.
[17] Darwish S, Sastry RH, Ruprecht A. Natal teeth, bifid tongue and deaf mutism. J Oral Med. 1987; 42: 49-53.
[18] Mandal AK, Hornby SJ, Jones RB. Congenital hydrocephalus associated with congenital glaucoma and natal teeth. Indian J Ophthalmol. 2002; 50: 322-3.
[19] Rao BB, Mamatha GR, Jameera KM, Hegde RB. Natal and neonatal teeth: A case report. J Indian Soc Pedo Prev Dent. 2001; 19: 110-2.
[20] Hersh JH, Verdi GD. Natal teeth in monozygotic twins with vander Woude Syndrome. Cleft Palate Craniofac J. 1992; 29: 279-81.
[21] Leachman SA, Kaspar RL, Fleckman P, Florell SR, Smith FJ, McLean WH, et al. Clinical and pathological features of Pachyonychia Congenita. J Investig Dermatol Symp Proc. 2005; 10: 3-17.
[22] Ziai MN, Bock DJ, Da Silveira A, Daw JL. Natal teeth: A potential impediment to nasoalveolar molding in infants with cleft lip and palate. J Craniofac Surg. 2005; 16: 262-6.
[23] Masatomi Y, Abe K, Ooshima T. Unusual multiple natal teeth: Case report. Pediatr Dent. 1991; 13: 170-172.
[24] Delbem AC, Faraco IM, Percinoto C, Delbem AC. Natal teeth: Case report. J Clin Pediatr Dent. 1996; 20: 325-7.
[25] Chow MH. Natal and neonatal teeth. JADA 1980; 100: 215-216.
[26] Hebling J, Zuanon ACC, Vianna DR. Dente Natal—A case of natal teeth. Odontol Clín. 1997; 7: 37-40.
[27] Galassi MS, Santos-Pinto L, Ramalho T. Natal maxillary primary molars: Case report. J Clin Pediatr Dent. 2004; 29(1): 41-44.
[28] Anegundi RT, Sudha P, Kaveri H, Sadanand K. Natal and neonatal teeth: A report of four cases. J Indian Soc Pedo Prev Dent. 2002; 20: 86-92.
[29] Anderson RA. Natal and neonatal teeth: histologic investigation of two black females. J Dent Child 1982; 49: 300-303.
[30] Friend GW, Mincer HH, Carruth KR, Jones JE. Natal primary molar: case report. Pediatr Dent. 1991; 13: 173-175.
[31] Aldred MJ. et al. Dental Anomalies,Chapter 9, Handbook of Paediatric Dentistry, 3rd Edition, Mosby Elsevier.
[32] Sigal MJ, Mock D, Weinberg S. Bilateral mandibular hamartomas and familial natal teeth. Oral Surg Oral Med Oral Pathol. 1988; 65: 731-5.
[33] Muench MG, Layton S, Wright JM. Pyogenic granuloma associated with a natal tooth: Case report. Pediatr Dent. 1992; 14: 265.
[34] Oliveira LB, Tamay TK, Wanderley MT, Rodrigues RM, Barboza CA, de Souza SO. Gingival fibrous hamartoma associated with natal teeth. J Clin Pediatr Dent. 2005; 29: 249-52.
[35] Rusmah M. Natal and neonatal teeth: a clinical and histological study. J Clin Ped Dent. 1991; 15:251-253.
[36] Bodenhoff J. Natal and neonatal teeth. Dental Abstr. 1960; 5: 485-488.
[37] Tay WM. Natal canine and molar in an infant. Oral Surg Oral Med Oral Pathol. 1970; 29: 598-602.
[38] Magitot E. Anomalies in the erupton of the teeth in man. Br J Dent Sc. 1883; 26: 640-641.
[39] Allwright WC. Natal and neonatal teeth. British Dent J. 1958; 105: 163-172.
[40] Leung AKC. Management of natal teeth (letter). JADA 1987; 114: 762.
[41] Leung AKC. Natal teeth. Am J Dis Child 1986; 140: 249-251. [42] Kara C. Evaluation of patient perceptions of frenectomy: A
comparison of Nd:YAG laser and conventional tech-niques. Photomed Laser Surg. 2008; 26(2): 147-52.
[43] Slayton RL. Treatment alternatives for sublingual traumatic ulceration (RigaFede disease). Pediatr Dent 2000; 22(5): 413-4.
[44] Goho C. Neonatal sublingual traumatic ulceration (Riga- Fede disease): Report of cases. J Dent Child 1996; 63(5): 362-4.
[45] Stein S, Paller A, Haut P, Mancini A. Langerhans cell his-tiocytosis presenting in the neonatal period: A retrospective case series. Arch Pediatr Adolesc Med. 2001; 155(7): 778-83.
[46] Ooshima T, Mihara J, Saito T, Sobue S. Eruption of tooth like structure following the exfoliation of natal tooth: report of case. J Dent Child 1986; 2013: 275-8.
[47] Last updated on 2007 Nov. 9. Available from: http://www.newdao.com/natal-teeth-baby-born.html.
[48] Singh S, Subbba Reddy VV, Dhananjaya G, Patil R. Reactive fibrous hyperplasia associated with a natal tooth: A case report. J Indian Soc Pedo Prev Dent. 2004; 22: 183-6.
[49] McDonald RD, Avery DR, Dean JA. 8th ed. Missouri: Mosby; 2004. Dentistry for the Child and Adolescent.
[50] Alaluusua S, Kiviranta H, Leppäniemi A, Hölttä P, Lukinmaa PL, Lope L, et al. Natal and neonatal teeth in relation to environmental toxicants. Pediatr Res. 2002; 52: 652-5.
Received on 30-11-2017 Accepted on 11-12-2017 Published on 16-12-2017 © 2017 Saleha Shah; Licensee Global Journal of Oral Science. This is an open access article licensed under the terms of the Creative Commons Attribution Non-Commercial License (http: //creativecommons.org/licenses/by-nc/3.0/), which permits unrestricted, non-commercial use, distribution and reproduction in any medium, provided the work is properly cited.



























![birth to 6 months [before teeth erupt] thumb sucking](https://img.pdfslide.us/doc/110x75/6261ef10b9a606740d49a8da/birth-to-6-months-before-teeth-erupt-thumb-sucking-.jpg)