-
8/13/2019 Glaucoma Essay
1/5
The Role of Biomechanics in Glaucoma
The human eye is a remarkable organ with a complex anatomy. It
is responsible for detecting,
focussing and subsequently, converting photons into
electrochemical signals that are then transmitted
to the brain. The eye is roughly spherical and approximately one
inch in diameter. Its outermost layer
is made of two tough connective tissues; the cornea and the
sclera. The middle layer consists of theiris, ciliary body and the
choroid. The choroid contains blood vessels that nourish the
retinal cells, and
facilitate metabolite exchange. The iris is responsible for the
changing size of the pupil to ensure that
the right amount of light reaches the retina. Finally, the
ciliary body, made up of the ciliary processes
and the ciliary muscle is responsible for the production of
aqueous humor and the accommodation of
the lens to adapt to changing focal distances, respectively. The
innermost layer of the eye, the retina,
is the sensory layer containing neurons, and photoreceptors
neurons known as rods and cones that
convert the incident light into neuron firings that are
transmitted to the brain via the optic nerve. The
eyeball is divided into the anterior and posterior chambers,
filled with aqueous humor and the vitreous
body, filled with vitreous humor. In the absence of any bony
processes, the eyeball maintains its
rigidity by maintaining a small positive pressure with respect
to the surroundings. This positivepressure is known as the
Intraocular Pressure (IOP). The IOP is transmitted throughout the
eye by
the vitreous humor. Therefore, the eye remains spherical and
rigid, and a stable distance between the
lens and the retina is always maintained. The normal mean value
of IOP for the human eye is 15.5
2.6 mm Hg(Ethier & Simmons, 2007).
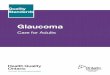
Figure 1: Image of the anatomy of the human eye (Bonnick,
2013)
A normal IOP is essential to functioning of the human eye. How
is this IOP produced and why?Aqueous humor is responsible for the
IOP. In the cornea and the lens, because of the need for
optical
-
8/13/2019 Glaucoma Essay
2/5
transparency, metabolite exchange with blood via perfusion is
not possible. Therefore, clear and
colourless aqueous humor also serves as a medium for nutrient
exchange. Secreted by epithelial cells
in the ciliary processes, the aqueous humor perfuses the lens
and then moves into the anterior chamber
of the eye. From here, it drains out of the eye through special
channels in the angle formed by the iris
and the cornea known as the angle of the anterior chamber. The
rate of production of aqueous humor
by the ciliary processes is very slow (2.4 0.6 l/min in the
normal human eye). However, the
resistance to outflow of aqueous humor during its drainage is
what causes the considerable positive
pressure. The drainage of aqueous humor in the eye occurs
through two channels; the conventional
route and the unconventional route. The unconventional route or
the uveo-scleral route carries only
10% of the outflow, and does not account as the primary site for
flow resistance. Majority of the
aqueous humor drains through the conventional route; a series of
specialised tissues: the trabecular
meshwork, the canal of Schlemm, and the collector
channels/aqueous veins. These are the main cause
of the outflow resistance to aqueous humor (approximately 3-4mm
Hg/l/min). Once aqueous humor
leaves the aqueous veins, it drains back into the right side of
the heart after joining the episcleral
veins. At the normal values of outflow resistance, the IOP
remains at a value of 15.5 mm Hg, which is
normal.
Ocular hypertensionis a condition where the IOP is elevated
beyond its normal value, in the absence
of optic nerve damage or visual field loss. Ocular hypertension
is the most important risk factor for
glaucoma and thus, functions as a valuable screening tool for
glaucoma. According to Casson et al
(2012) glaucomamay be described as:
..a group of ocular disorders of multifactorial aetiology united
by a clinically characteristic optic
neuropathy with potentially progressive, clinically visible
changes at the optic nerve head (ONH),
comprising focal or generalized thinning of the neuroretinal rim
with excavation and enlargement of
the optic cup, representing neurodegeneration of retinal
ganglion cell axons and deformation of the
lamina cribrosa; corresponding diffuse and localized
nerve-fibre-bundle pattern visual field loss maynot be detectable
in early stages; while visual acuity is initially spared,
progression can lead to
complete loss of vision..
Chronically elevated IOPis indicated in the development as well
as the progression of glaucoma. A
patients IOP may be considered elevated if it is greater than
97.5 percentile of the population
(Casson et al, 2012). It may affect the pressure sensitive cells
and tissues in the eye viz. the trabecular
meshwork (TM), the optic nerve head (ONH) including the lamina
cribrosa cells and optic nerve head
astrocytes, the peripapillary sclera around the optic nerve
head, retinal ganglion cells (RGC) and RGC
axons in the retinal nerve fibre layer (Clark, 2012). This
increase in IOP is caused by an increase in
outflow resistance. In a glaucomatous eye, the resistance to
outflow maybe as high as or greater than
triple the normal value. There are also some forms of glaucoma
in which this increase in IOP is not
due to the increase in outflow resistance. These are categorized
as angle-closure glaucoma, which
occurs due to the iris pivoting forward and blocking the access
to the drainage structures in the angle
of the anterior chamber. This may be caused due to an anatomic
predisposition.
A few hypotheses have been put forth to explain the resistance
to outflow in the conventional route
for drainage:
1) Collapse of Canal of Schlemm - Channel collapse is governed
by two factors. Theunderlying elastic TM tends to keep the Canal of
Schlemm open. Whereas, the pressure drop
across the TM and the inner wall of the canal tends to make it
close. On solving the resultingequations drawn up to conserve mass,
pressure drop and deformation it was found that for
-
8/13/2019 Glaucoma Essay
3/5
typical values of input parameters, the resistance due to the
canal of Schlemm would be
negligible, except at very high pressures such as 50mm Hg where
the canal collapses. Even
with a collapsed Canal of Schlemm the outflow resistance is not
as high as a glaucomatous
eye. Therefore, channel collapse can be ruled out as a cause of
Glaucoma (Ethier & Simmons,
2007).
Figure 2: Scanning Electron Micrograph showing an overview of
conventional tissues
for aqueous humor drainage(Ethier & Simmons, 2007)
2) Experimental evidence supports the conclusion that the source
of normal and increasedoutflow resistance in glaucoma is
attributable to the inner wall endothelium, its basement
membrane, the juxtacanalicular connective tissue (JCT), or some
combination of all three of
these (Johnson, 2006). Like other epithelial basement membranes
in the body, the basement
membrane in the inner wall of the canal of Schlemm may be
responsible for the generation of
outflow resistance. However, due to the discontinuous nature of
the membrane in the human
eye, this resistance may not account for a large fraction. The
porous nature of the JCT as
evinced by transmission electron microscopy shows large open
spaces, which may not cause
significant outflow resistance. However, if these spaces were to
contain glycosaminoglycansat physiological concentrations, then the
flow resistance due to the JCT would be
considerable. Upon further investigation using quick freeze/deep
etch electron microscopy
that may preserve GAGs in the sample, similar pores were still
seen. Therefore, it remains
unclear whether GAGs account for the outflow resistance, and if
yes, till what extent. In the
inner wall, the endothelial cells form a continuous layer
attached to each other using tight
junctions. The unique feature of these cells is the formation of
vacuoles that are invaginations
of the endothelium into the lumen of the canal of Schlemm,
caused by the pressure drop
across the endothelium. These invaginations may account for the
outflow resistance. These
vacuoles also contain membrane lined pores that connect the
apical and basal side of the cell.
A study has shown that the pore density in the glaucomatous eye
is significantly reduced,
-
8/13/2019 Glaucoma Essay
4/5
which may mean that these pores account for the increase in
outflow resistance as
experienced in glaucoma (Overby, Stamer & Johnson,
2008).
Figure 3: Scanning Electron Micrograph of the inner wall of
Schlemms Canal
(Johnson, 2006)
Apart from the elevated outflow resistance, glaucoma causes
extensive and progressive neuropathy.
ONH cupping caused by the death of the neurons in the optic
nerve is a clinical feature of glaucoma
(Downs, Roberts & Sigal, 2012). RGC axons converge to form
the optic nerve that pierces the sclera
to join the brain. Since this is a weak point of discontinuity
in the otherwise continuous sclera, it is
additionally susceptible to concentration of stresses. The
lamina cribrosa is the porous connective
tissue that spans the sclera canal and supports the RGC axons as
they leave the eye as the optic nerve.
Two theories attempt to explain the damage to the RGCs. The
mechanical theory of glaucomatous
optic neuropathypostulates that the increased mechanical
stresses acting in lamina cribrosa cause
axonal damage. This damage may be mediated through astrocytes.
The astrocytes divide and form a
glial scar and fail to provide nutrition and guidance the
neurons, thus leading to neuronal death. The
second theory, vasogenic theory, states that the glaucomatous
insult results from inadequate vascular
perfusion in the laminar cribrosa, resulting in insufficient
oxygen delivery. The resulting ischemia
triggers neuronal cell death (Ethier & Simmons, 2007).
In conclusion, glaucoma is a progressive eye pathology caused by
chronically elevated IOP that leads
to irreversible vision loss and if left untreated, blindness.
Since the effects may not be clear till they
have progressed considerably, early screening is a must. Once
diagnosed, the treatment for glaucoma
involves reduction of the IOP via medication, or surgical
treatment. In addition to IOP and ONHbiomechanics, the biomechanics
of the cornea and the corneal thickness may also play a role in
the
development of glaucoma, especially the progression of ocular
hypertension into full fledged
glaucoma (Brown & Congdon, 2006). Therefore, further
research into the biomechanics of glaucoma
will help identify risk, early diagnosis, treatment modalities
as well as patient prognosis.
-
8/13/2019 Glaucoma Essay
5/5
References
Bonnick (2013) CSEC - The Eye - functions of the various parts.
Biologs. Weblog. [Online].
Available
fromhttp://thebiologs.blogspot.co.uk/2013/09/csec-eye.html.Accessed
24th October 2013.
Brown, K. E. & Congdon, N. G. (2006) Corneal structure and
biomechanics: impact on the diagnosis
and management of glaucoma. Current Opinion in Ophthalmology.17
(4), 338-343.
Casson, R. J., Chidlow, G., Wood, J. P., Crowston, J. G. &
Goldberg, I. (2012) Definition of
glaucoma: clinical and experimental concepts. Clinical &
Experimental Ophthalmology. 40 (4), 341-
349.
Clark, A. F. (2012) The cell and molecular biology of glaucoma:
biomechanical factors in
glaucoma.Investigative Ophthalmology & Visual Science. 53
(5), 2473-2475.
Crawford Downs, J., Roberts, M. D. & Sigal, I. A. (2011)
Glaucomatous cupping of the lamina
cribrosa: a review of the evidence for active progressive
remodeling as a mechanism.Experimental
Eye Research. 93 (2), 133-140.
Ethier, C. R., Johnson, M. & Ruberti, J. (2004) Ocular
biomechanics and biotransport.Annual Review
of Biomedical Engineering. 6, 249-273.
Ethier, C. R. & Simmons, C. A. (2007)Introductory
biomechanics: from cells to
organisms. Cambridge texts in biomedical engineering. Cambridge,
Cambridge University Press.
Johnson, M. (2006) 'What controls aqueous humour outflow
resistance?'.Experimental Eye
Research. 82 (4), 545-557.
Overby, D. R., Stamer, W. D. & Johnson, M. (2009) The
changing paradigm of outflow resistancegeneration: towards
synergistic models of the JCT and inner wall
endothelium.Experimental Eye
Research. 88 (4), 656-670.
http://thebiologs.blogspot.co.uk/2013/09/csec-eye.htmlhttp://thebiologs.blogspot.co.uk/2013/09/csec-eye.htmlhttp://thebiologs.blogspot.co.uk/2013/09/csec-eye.htmlhttp://thebiologs.blogspot.co.uk/2013/09/csec-eye.html