Embed Size (px)
Citation preview

ORIGINAL ARTICLE
GJB2, SLC26A4 and mitochondrial DNA A1555G mutations inprelingual deafness in Northern Chinese subjects
YU-FEN GUO1,*, XIAO-WEN LIU1,*, JING GUAN1,3, MING-KUN HAN2,
DA-YONG WANG2, YA-LI ZHAO4, SHAO-QI RAO2,5 & QIU-JU WANG2
1Department of Otolaryngology-Head and Neck Surgery, Second Hospital of Lanzhou University, Lanzhou, 2Department of
Otolaryngology-Head and Neck Surgery, Chinese People’s Liberation Army Institute of Otolaryngology, Chinese People’s
Liberation Army General Hospital, Beijing, 3Department of Otolaryngology-Head and Neck Surgery and 4Department of
Biochemistry and Molecular Biology, Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences and Peking
Union Medical College, Beijing and 5Department of Bioinformatics, Harbin Medical University, Harbin, China
AbstractConclusion. This genetic epidemiological study demonstrated that 26.65% of the prelingual deafness in Northern Chinesepatients can be detected at younger ages by genetic testing of three common hearing loss genes (GJB2, SLC26A4 andmtDNA A1555G), and thus, early intervention measures could be undertaken to help them in language acquisition.Objectives. The GJB2, SLC26A4 and mtDNA A1555G mutations are the prevalent causes of prelingual deafness worldwide.Numerous studies have revealed that the forms and frequencies of the mutations in the three genes are largely dependent onthe ethnic or geographic origins. Hence, this study aimed to characterize the mutation profiles of the three genes inprelingual deafness in Northern Chinese patients. Subects and methods. An investigation of 514 patients with prelingualdeafness and 117 controls with normal hearing was conducted. Bidirectional sequencing (or enzyme digestion) was appliedto identify sequence variations. Results. This study revealed that 26.65% patients had two mutated alleles (homozygote orcompound heterozygote) of GJB2 (9.14%) or SLC26A4 (8.95%) and/or an mtDNA A1555G (8.56%) mutation. In detail,19.26% patients carried GJB2 mutations including 10.12% single mutant carriers. 235delC was the most common type,making up 69.18% of all mutants for GJB2. The mutant carrier rate for SLC26A4 was 15.2%, including 6.23% singlemutant carriers. The two most common types (IVS7-2A�G and H723R) accounted for 51.61% and 33.06% mutations,respectively. Forty-five patients had mtDNA A1555G, giving a frequency of 8.75%. In the control group with normalhearing, 2.56%, 1.71% and 0% of the subjects carried a single mutant for GJB2, SLC26A4 and mtDNA A1555G,respectively.
Keywords: Prelingual deafness, non-syndromic hearing loss, genetic testing, Chinese
Introduction
Severe or profound prelingual deafness occurs in
approximately 1 per 1000 newborns [1,2]. The
affected children usually suffer from delayed lan-
guage acquisition and can experience social isolation.
Prelingual deafness can be caused by many genetic
and environmental factors, and at least half of the
cases are thought to be genetically determined [3].
Recent advances in genetic studies of hearing loss
have provided a better understanding of the genetic
mutations that cause prelingual deafness [4]. There
have been reports revealing that prelingual severe or
profound hearing loss is mainly due to recessive
inheritance, and mutations in GJB2 (DNFB1,
OMIM: 121011) and SLC26A4 (DFNB4, OMIM:
600791) genes are thought to be the major causes of
autosomal recessive non-syndromic deafness [5].
GJB2 gene is currently recognized as the gene
notably responsible for non-syndromic autosomal
recessive and sporadic prelingual deafness [6,7].
Mutations in the SLC26A4 gene have been identified
as a major cause of non-syndromic hearing loss
Correspondence: Qiu-Ju Wang, MD, PhD, Prof., Department of Otolaryngology-Head and Neck Surgery and Institute of Otolaryngology, Chinese People’s
Liberation Army General Hospital, Beijing, China. Tel: �86 10 68172228. Fax: �86 10 68156974. E-mail: [email protected] or [email protected]
*The first two authors contributed equally to this work.
Acta Oto-Laryngologica, 2008; 128: 297�303
(Received 5 September 2007; accepted 25 October 2007)
ISSN 0001-6489 print/ISSN 1651-2551 online # 2008 Taylor & Francis
DOI: 10.1080/00016480701767382
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
onas
h U
nive
rsity
on
11/0
2/14
For
pers
onal
use
onl
y.

associated with enlarged vestibular aqueduct (EVA)
and Pendred syndrome [8,9]. The 1555A�G mito-
chondrial mutation in the highly conserved coding
region of the mitochondrial 12S rRNA gene has been
found to be the most prevalent mitochondrial muta-
tion associated with both aminoglycoside-induced
and non-syndromic sensorineural hearing loss
(OMIM: 561000) in subjects of many ethnic origins
[10,11].
The forms of GJB2 and SLC26A4 mutations are
largely dependent on either ethnic or geographic
origins of the populations [12�15]. Mutation 35delG
in GJB2 is the most common type in sporadic or
familial Caucasian patients [16,17]. Mutation
167delT is the leading type in Israeli patients [18].
Mutation 235delC is the major type in Japanese,
Chinese and Korean patients [19]. In China, by
studying 118 probands from 60 simplex and 58
multiplex families, Liu et al. [20] estimated that the
GJB2 mutation rate in the non-syndromic hearing
loss patients was 27.5%. The 235delC mutation
accounted for 81% of the pathogenic alleles in
multiplex cases and 67% in simplex cases.
Numerous studies indicate that the SLC26A4
mutation(s) is associated with a congenital inner
ear malformation, EVA, which often accompanies
sensorineural hearing loss [8,9]. Prasad et al. [21]
reported that about 1�8% of the patients with
congenital hearing loss in a Western population
had EVA caused by SLC26A4 mutation(s). To
date, there are 100 reported mutations in
SLC26A4. However, the mutation hot spots were
also found to be race-specific [22�24]. In Northern
Europe, T416P and IVS8�1G�A are the most
common mutation types [24]; in Japan and South
Korea H723R is the most common type [22,23]. In
contrast to Japan, there is one additional common
type, IVS7-2A�G, in South Korea [23]. In Taiwan,
Wu et al. [25] screened SLC26A4 in 38 Chinese
families with EVA and found 8 mutation types in 33
families. IVS7-2A�G is most common, accounting
for 84% of all the alleles. Very recently, Hu et al. [26]
reported the results for 15 patients with deafness and
EVA in 13 unrelated Chinese families recruited to
the study from the Central South area of China.
IVS7-2A�G is most common among 15 pathogenic
mutations identified, accounting for 22.3% of all the
mutant alleles. In our recent study of 107 Chinese
patients with EVA and/or Mondini dysplasia in 101
familes (95 simplex and 6 multiplex familes) ascer-
tained by the Department of Otolaryngology, Chi-
nese People’s Liberation Army General Hospital
(Beijing, China), IVS7-2A�G was the most com-
mon form, accounting for 57.63% of all the mutant
alleles [27].
Discovery of the association between mtDNA 12S
rRNA A1555G and hearing loss is attributed to work
by Prezant et al. in 1993, who investigated three
families with aminoglycoside antibiotic-induced
deafness [10]. Now, the mtDNA A1555G mutation
has been estimated in different races all over the
world, which again indicates that the frequency of
the mutant in non-syndromic hearing loss is depen-
dent on racial or geographic origins. The frequency
estimates for this mutation are 2.4%, 0.7%, 1.8%
and 2.4% for Danes, Germans, Hungarians and
Poles, respectively [28,29]. In Asia, the frequency
estimates are 3.0%, 5.3% and 3.43% for Japanese,
Indonesians and Chinese subjects, respectively
[30,31].
Overall, these data show that significant differ-
ences in both frequencies and types in the three
genes can be observed in either different ethnic or
geographic origins. In particular, in the Chinese,
who make up approximately one-fifth of the world
population, high genetic heterogeneity may be pre-
sent among geographic origins. For instance, it is
known that Chinese in southern and northern areas
have distinct ancestral origins, with Malay and
Mongolian lineages, respectively. Therefore, this
study aimed to define the forms and frequencies of
the three well-known hearing loss genes in Northern
Chinese using a large sample of 514 patients with
prelingual deafness and 117 controls with normal
hearing.
Subjects and methods
Subjects and phenotyping
In this study, 514 patients (292 males and 222
females), whose ages ranged from 5 to 22 years, were
ascertained from the students at 3 schools for deaf
and dumb subjects in Gansu Province, Northern
China. As a control, 117 subjects with normal
hearing were recruited from the same region as this
study. Information consent, blood samples and
clinical evaluations were obtained from all the
participants according to the protocols approved by
the collectors’ institution review boards of the ethics
committees. Their clinical data, hearing test data
(including pure tone audiometry, acoustic immit-
tance, and auditory-evoked brainstem response),
and blood were collected by the Department of
Otorhinolaryngology & Head and Neck Surgery in
the Second Affiliated Hospital of Lanzhou Univer-
sity. The examinations demonstrated that these
students had severe or profound prelingual non-
syndromic hearing loss. Their ages of onset were less
than 3 years, and as a result they were only able to
communicate using sign language. Furthermore,
298 Y.-F. Guo et al.
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
onas
h U
nive
rsity
on
11/0
2/14
For
pers
onal
use
onl
y.

children in whom with SLC26A4 homozygous or
compound heterozygous mutations were detected
underwent high-resolution computed tomography
(HRCT) scan of petrous temporal bone to examine
for bilateral EVA. The criterion for classifying the pa-
tients with EVA was defined as a diameter ]1.5 mm
for the midpoint between the common crus and the
external aperture in the HRCT scanning [32].
General procedures for DNA isolation and sequencing
Genomic DNA from peripheral blood leukocytes
was obtained by the phenol/chloroform method. All
PCR amplified products for the target fragments of
three genes were purified with the Millipore plate,
and were then sequenced with an ABI 3730
Sequencer (Applied Biosystems, Foster City, CA,
USA). The sequence data were analyzed by aligning
with the reference sequences in NCBI (NC_000013
for GJB2, NT_007933 for SLC26A and AC_000021
for mtDNA 12S rRNA A1555G) using the DNAS-
tar 5.0 and BioEdit software. Mutations or poly-
morphisms were identified according to the
reference sequences.
GJB2 mutation screening
The GJB2 gene has two exons, and the coding
region is in exon 2. With the use of the Primer 5.0
software package, the primer pair � forward primer
(GJB2-F): TGCTTACCCAGACTCGAGAA and
reverse primer (GJB2-R): CGACTGAGCCTTGA-
CAGCTGA � were designed for the coding region of
GJB2, and the PCR product was an 864 bp
fragment. To amplify the exon, Touch-down PCR
with annealing temperatures of T1�688C (10
cycles) and T2�638C (25 cycles) was carried out
in an ABI 9700 thermal cycler.
SLC26A4 mutation screening
The SLC26A4 gene contains an open reading frame
of 2343 bp, and encompasses 21 exons. Mutations in
exons 8, 19, 10, 17 and 15 were often found in non-
syndromic hearing loss associated with EVA in
Chinese subjects [27]. Hence, the following sequen-
tial procedures were used to systematically detect
mutations in the SLC26A4 gene. PCR amplifications
of five exons (8, 19, 10, 17 and 15) were first
performed; if a mutation was not detected in these
five exons, the DNA sample was further screened for
mutations in exons 3, 4, 5, 7, 11, 12 and 14,
respectively.
Exons 3, 5, 8 and 15 were amplified using the
primer pairs displayed in Table I, which were
designed using the online Primer 3.0 software. For
exons 4, 7, 10, 11, 12, 14, 17 and 19, the primer
pairs were designed based on those in Coucke et al.
[33]. All the primer pairs were synthesized by
Shanghai Sangon Biological Engineering Technol-
ogy and Services (Shanghai, China). Touch-down
PCR with conditions shown in Table I was con-
ducted for amplifying exons 3, 5, 8 and 15 in an ABI
9700 thermal cycler. The other exons were amplified
according to the reaction conditions described by
Coucke et al. [33].
Mitochondrial DNA A1555G mutation screening
PCR amplication. With the use of the primer pair
synthesized by Shanghai Sangon Biological Engi-
neering Technology and Services � forward primer
(M-F): TCAACCTCACCACCTCTT and reverse
primer (M-R): TTTGTCGCCTCTACCTAT � a
767 bp mtDNA fragment (nt 1229�nt 1995) was
amplified using an annealing temperature of 628Cfor 30 cycles.
Alw26I digestion analysis. For detecting mtDNA
A1555G, 6.0 ml of the PCR product was mixed with
2.0 ml of buffer and 0.2 ml of Alw26I restriction
enzyme (Tango, Shanghai, China). ddH2O was
added to the mixture until the volume reached
25.0 ml. The reaction mixture was incubated at
378C for 150 min. The electrophoresis on the 2%
agarose gel was run to examine the digested product.
If the digested product showed the specific band for
Table I. Primer pairs and PCR conditions for exons 3, 5, 8 and 15 of SLC26A4 gene.
Temperature (8C)
Exon Primer sequence T1 T2 Size (bp)
3 5?GGCAAAAGCATGGTAAGCAC3?3?AGGGTAAGCAACCATCTGTCA5?
61 54 400
5 5?CAAAGTGCTGCGGTTACAGA3?3?AATTTTGGGTTCCAGGAAAT5?
59 52 480
8 5?AAGTTCAGCATTATTTGGTTGACA3?3?TGGTTGTTTCTTCCAGATCACA5?
60 53 305
15 5?GCTCCTCTGAGCAACTGTGA3?3?GGGTCTAGGGCCTATTCCTG5?
67 60 302
GJB2, SLC26A4 and mtDNA A1555G mutations in Chinese 299
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
onas
h U
nive
rsity
on
11/0
2/14
For
pers
onal
use
onl
y.

mtDNA A1555G, the PCR product was verified by
direct sequencing.
Results
GJB2 mutations
Fifteen different DNA sequence variations were
detected in 514 patients, as shown in Table II.
Among the variations, 11 types had already been
reported, including 6 mutations (35delG, R32C,
E47K, 176-191del16, 235delC and 299�300delAT)
[6,34�36], 5 polymorphisms (V37I, V27I, E141G,
G160S and I203T) and 4 novel variants (T18I,
Y68C, A78T and T86R), all situated in a highly
conserved region in GJB2. In comparison, among
117 controls, only 2 subjects were 235delC carriers
(heterozygotes) and 1 subject was a 299�300delAT
carrier (a heterozygote), which gave an estimate of
2.56% (3/117) for mutant carrier rate in the group
with normal hearing.
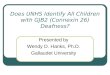
In all, 99 of 514 patients with hearing loss
(99/514, 19.26%) were found to have a GJB2
mutation(s), and the total number of mutant alleles
was 146 (Figure 1), of which 52 (52/514, 10.12%)
patients had only 1 mutant allele and the remaining
patients (47/514, 9.14%) had two mutant GJB2
alleles, in either homozygous or compound hetero-
zygous states. 235delC was most common, account-
ing for 69.18% (101/146) of the mutant alleles
(Figure 1), and next was 299�300delAT, with a
frequency of 11.64%.
SLC26A4 mutations
Seventy-eight patients carried a SLC26A4 muta-
tion(s), of which 46 had 2 mutant alleles (either
homozygotes or compound heterozygotes), making
up 8.95% of 514 patients, and the remaining
32 patients had single mutant allele. Ten mutations
were IVS7-2A�G, IVS10-12T�A, IVS15�5G
�A, N392Y, R409H, T410M, V659L, L676Q,
I714K and H723R (Figure 2). The two leading
variants, IVS7-2A�G and H723R, accounted for
51.61% and 33.06% of mutations, respectively.
Twenty-five patients who were detected with
SLC26A4 homozygous or compound heterozygous
mutations underwent an HRCT scan on their
petrous temporal bones and 24 patients showed
evidence of EVA, indicating that almost all of the
hearing-impaired patients with such SLC26A4 mu-
tation configurations suffered from some inner ear
malformations such as EVA. Among 117 controls,
only 2 mutant alleles were identified in 2 IVS7-2A
�G heterozygotes, which gave an estimate of 1.71%
of the mutant carrier rate.
Mitochondrial DNA A1555G mutation
Forty-five patients in the cohort had mtDNA
A1555G, of which 23 (23/45, 51.11%) had a history
of being prescribed aminoglycosides. Interestingly, a
few patients also had either GJB2 or SLC26A4
Table II. DNA variations detected in GJB2 gene.
Codon Nucleotide change Case (1028 alleles) Control (234 alleles) Mutation type
35delG 35delG 4 � Frameshift
T18I 53C�T 1 � Novel variation
V27I 79G�A 297 76 Polymorphism
R32C 94C�T 1 � Synonymous
V37I 109G�A 22 12 Polymorphism
E47K 139G�A 1 � Missense
176�191del16 176�191del16 1 � Frameshift
Y68C 203A�G 1 � Novel variation
A78T 232G�A 1 � Novel variation
235delC 235delC 101 2 Frameshift
T86R 257C�G 2 � Novel variation
299�300delAT 299�300delAT 17 1 Frameshift
E114G 341A�G 205 59 Polymorphism
G160S 478G�A 1 � Polymorphism
I203T 608T�C 20 � Polymorphism
101
17
4 1 1 10
20
40
60
80
100
120
235delC 299-300delAT
35delG R32C E47K 176-191del16
Num
ber
of M
utan
t Alle
les
Figure 1. Distribution of GJB2 mutant alleles.
300 Y.-F. Guo et al.
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
onas
h U
nive
rsity
on
11/0
2/14
For
pers
onal
use
onl
y.

mutations (Table III). For example, one subject who
carried mtDNA A1555G was a GJB2_235delC
homozygote. Another subject who carried mtDNA
A1555G was a SLC26A4-D661E heterozygote. Ac-
cording to the current perspective that mtDNA
A1555G may exacerbate the severity of hearing
loss associated with GJB2 [35], we reclassified the
patient who carried both mtDNA A1555G and two
GJB2 mutants into the hearing loss group associated
with GJB2. As a result, the estimate of the carrier
rate for mtDNA A1555G becomes 8.56% (44/514).
However, mtDNA A1555G was not found in 117
subjects with normal hearing.
Discussion
Severe or profound prelingual deafness has a nega-
tive impact on language acquisition in patients.
Many prelingual deafness cases were not discovered
at early stages of the disease development, and thus
lost opportunities for early interventions, such as
wearing hearing aids and receiving speech training.
Consequently, these patients had to communicate
by sign language, which often led to social isolation.
Needless to say, early diagnosis of prelingual
deafness is fundamental to prevent such an undesir-
able outcome. This study involved 514 patients with
prelingual deafness from Northern China. We found
that 26.65% of the patients had two mutant alleles in
either GJB2 (9.14%) or SLC26A4 (8.95%), and/or
with mtDNA A1555G (8.56%). Based on the
recessive inheritance mode, the results suggest that
by conducting a proper DNA test, more than one-
quarter of the prelingual deafness cases may be
identified at a younger age, which would allow early
intervention measures to be undertaken to help them
acquire timely language skills.
However, designing an efficient genetic test for the
ear clinic may become complicated because of high
genetic heterogeneity in hereditary deafness and the
further complication of a need to screen numeruous
exons such as SLC26A4, which can be very time-
consuming. A more effective approach is to only
screen the pathogenic mutations of high frequencies.
In this study, we found seven previously reported
GJB2 mutations in the patients. Of the mutations,
235delC (72.14%) and 299�300delAT (12.14%)
were most common, and jointly accounted for
84.28% of GJB2 mutations in the studied cohort.
It is likely that IVS7-2A�G (51.61%) and H723R
(33.06%) jointly accounted for 84.67% of SLC26A4
mutations. If considering the 8.56% of patients
who carried mtDNA A1555G, we reasonably
believe that screening five mutations, i.e GJB2_
235delC, GJB2_299�300delAT, SLC26A4_H723R,
SLC26A4_IVS7-2A�G and mtDNA A1555G, may
be sufficient to identify most cases of prelingual
deafness in Northern Chinese patients at an earlier
age.
Due to its very high mutation load in either
recessively inherited or sporadic hearing loss, defini-
tion of the mutation rate and types of GJB2 in
populations of different racial or geographic origins
has become an intensely studied aspect of the
64
41
5 4 3 2 2 1 1 10
10
20
30
40
50
60
70
IVS7-
2A>G
H723R
L676
Q
IVS10
-12T
>A
R409H
N392Y
V659L
IVS15
+5G>A
T410M
D661E
Num
ber
of M
utan
t Alle
les
Figure 2. Distribution of SLC26A4 mutant alleles.
Table III. Frequencies of the subjects who had both mtDNA A1555G and GJB2 or SLC26A4 mutations.
Gene/locus
mtDNA A1555G GJB2 SLC26A4 Number of subjects
A1555G 79G�A /wt � 7
A1555G 79G�A /wt;341A�G/wt � 5
A1555G 79G�A/79G�A; 341A�G/wt � 2
A1555G 79G�A /79G�A; 341A�G/ 341A�G � 1
A1555G 235delC /235delC � 1
A1555G 235delC/wt � 2
A1555G 341A�G /341A�G � 1
A1555G 478 G�A/wt � 1
A1555G 79G�A /wt;608T�C /wt � 2
A1555G 109G�A/wt � 1
A1555G 608T�C/wt � 2
A1555G 79G�A/wt;341A�G /wt D661E/wt 1
GJB2, SLC26A4 and mtDNA A1555G mutations in Chinese 301
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
onas
h U
nive
rsity
on
11/0
2/14
For
pers
onal
use
onl
y.

molecular epidemiology of hearing loss. Several
studies revealed that European or American peoples
(e.g. Caucasians [16,17] and Jewish [18]) have
distinct GJB2 mutation types or rates from Mon-
golians (e.g. Chinese, Japanese and Koreans) in East
Asia [19,20]. In this study, the GJB2 mutant carriers
made up 19.26% (99/514) of all prelingual hearing
loss cases recruited from Northern China. Mutation
235delC was the most common type, accounting for
69.18% of mutated alleles; next was 299�300delAT
accounting for 11.64%. It is interesting to note that
the most common mutation type, 35delG, in Cau-
casians accounted only 2.74% mutated alleles and
167delT, the most common in Jewish subjects, was
not detected in the Chinese cohort. Based on the
present study and previous studies of Japanese,
Korean and Chinese subjects [19,20], 235delC is
the leading variant in all three races, despite its rates
varied.
For SLC26A4, two leading types, IVS7-2A�G
(51.61%) and H723R (33.06%), made up 84.67%
of pathogenic mutants in the prelingual hearing loss
cohort recruited in Northern China; these results of
mutation types and frequencies are unique to the
large cohort of Northern Chinese subjects. In
comparison with other races, T416P and IVS8�1G�A are most frequent in Northern Europeans
[24], and in Japanese and Koreans, H723R (53%
and 40%, respectively) is the most frequent
SLC26A4 mutation [22,23]. Even within the same
broad category of race � Chinese � Hu et al. [26]
reported markedly different results in a Chinese
cohort from the Central South area of China, in
which the leading variant IVS7-2A�G accounted
for 22.3% of all the mutant alleles, and H723R was
infrequent. These data suggest that there are sig-
nificant differences not only between different races,
but also within a same broad racial category (e.g.
Chinese cohorts of different geographic or ancestral
origins).
A number of racial populations over the world
have been screened for locus mtDNA A1555G,
again indicating markedly different mutation rates
among different geographic or racial origins. In
Caucasians living in Europe or America, the rates
are 0.7�2.4%; in Japanese, it is 3.0%; and in
Indonesians, a rate of 5.3% was observed [30]. In
Chinese, based on genetic screening of 1836 non-
syndromic hearing loss subjects, Liu et al. [31] gave
an estimate of 3.43%, which is lower than the
estimate (8.35%) obtained in this study, the highest
rate reported so far. The following reasons may
contribute to this fact. First, there may be a founder
effect. Northern Chinese are largely derived from
Mongolian lineage, which is quite different from the
ancestor(s) for Caucasians in European countries. It
should also be noted that Southern Chinese are
mainly derived from Malay (Southeast Asian race),
which appear to have a lower mutation rate than
Northern Chinese according to this study and the
study conducted by Liu et al. [31]. Second, China is
a large country inhabited by numerous nationalities.
Especially in Northern China where several mino-
rities live, marriages between Han and other races
can increase genetic diversity in this region. Third,
Northern China is a less developed region and 80%
of subjects among 514 deaf school students came
from the countryside. Thus, it is not surprising that
the incidence of deafness can be higher, because of
the poor (or improper) medical care (e.g. the wide
use of aminoglycoside antibiotics [37]) and lack of
the relevant knowledge of genetics.
In conclusion, in this study the epidemiological
characteristics for the three most important patho-
genic genes were investigated by using a large cohort
of prelingually deaf subjects recruited from Northern
China. These data show that more than one-quarter
of the deaf cases can potentially be detected at an
earlier age using the proposed genetic screening, so
that some timely intervention procedures could be
provided to help them develop their language ability.
Acknowledgements
This research was supported in part by the National
High-Tech R&D Project (grant no. 2006AA02
Z181), National Natural Science Foundation of
China (grant nos 30570424, 30672310, 30771203
and 30771857), Beijing Science & Technology
Major Project (grant nos D0906005040291 and
7070002), and National Outstanding PhD Thesis
Grant (grant no. 200463), National 973 Project
(2007CB507400) and Heilongjiang Province De-
partment of Education Outstanding Overseas Scien-
tist grant (grant no. 1055HG009) and Gansu
Province grant for Young and Middle-Aged Scien-
tists (grant no. 3YS061-A25-012).
References
[1] Marazita ML, Ploughman LM, Rawlings B, Remington E,
Arnos KS, Nance WE. Genetic epidemiological studies of
early-onset deafness in the U.S. school-age population. Am J
Med Genet 1993;46:486�91.
[2] Morton NE. Genetic epidemiology of hearing impairment.
Ann N Y Acad Sci 1991;630:16�31.
[3] Denoyelle F, Marlin S, Weil D, Moatti L, Chauvin P,
Garabedian EN, et al. Clinical features of the prevalent
form of childhood deafness, DFNB1, due to a connexin-26
gene defect: implications for genetic counselling. Lancet
1999;353:1298�303.
[4] Schrijver I, Gardner P. Hereditary sensorineural hearing loss:
advances in molecular genetics and mutation analysis.
Expert Rev Mol Diagn 2006;6:375�86.
302 Y.-F. Guo et al.
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
onas
h U
nive
rsity
on
11/0
2/14
For
pers
onal
use
onl
y.

[5] Gurtler N, Lalwani AK. Etiology of syndromic and non-
syndromic sensorineural hearing loss. Otolaryngol Clin
North Am 2002;35:891�908.
[6] Kudo T, Ikeda K, Kure S, Matsubara Y, Oshima T,
Watanabe K, et al. Novel mutations in the connexin 26
gene (GJB2) responsible for childhood deafness in the
Japanese population. Am J Med Genet 2000;90:141�5.
[7] Zelante L, Gasparini P, Estivill X, Melchionda S, D’Agruma
L, Govea N, et al. Connexin26 mutations associated with the
most common form of non-syndromic neurosensory auto-
somal recessive deafness (DFNB1) in Mediterraneans. Hum
Mol Genet 1997;6:1605�9.
[8] Abe S, Usami S, Hoover DM, Cohn E, Shinkawa H,
Kimberling WJ. Fluctuating sensorineural hearing loss
associated with enlarged vestibular aqueduct maps to 7q31,
the region containing the Pendred gene. Am J Med Genet
1999;82:322�8.
[9] Usami S, Abe S, Weston MD, Shinkawa H, Van Camp G,
Kimberling WJ. Non-syndromic hearing loss associated with
enlarged vestibular aqueduct is caused by PDS mutations.
Hum Genet 1999;104:188�92.
[10] Prezant TR, Agapian JV, Bohlman MC, Bu X, Oztas S, Qiu
WQ, et al. Mitochondrial ribosomal RNA mutation asso-
ciated with both antibiotic-induced and non-syndromic
deafness. Nat Genet 1993;4:289�94.
[11] Li R, Xing G, Yan M, Cao X, Liu XZ, Bu X, et al.
Cosegregation of C-insertion at position 961 with the
A1555G mutation of the mitochondrial 12S rRNA gene in
a large Chinese family with maternally inherited hearing loss.
Am J Med Genet A 2004;124:113�17.
[12] Morell RJ, Kim HJ, Hood LJ, Goforth L, Friderici K, Fisher
R, et al. Mutations in the connexin 26 gene (GJB2) among
Ashkenazi Jews with nonsyndromic recessive deafness. N
Engl J Med 1998;339:1500�5.
[13] Fuse Y, Doi K, Hasegawa T, Sugii A, Hibino H, Kubo T.
Three novel connexin26 gene mutations in autosomal
recessive non-syndromic deafness. Neuroreport 1999;10:
1853�7.
[14] Gasparini P, Rabionet R, Barbujani G, Melchionda S,
Petersen M, Brondum-Nielsen K, et al. High carrier
frequency of the 35delG deafness mutation in European
populations. Genetic Analysis Consortium of GJB2 35delG.
Eur J Hum Genet 2000;8:19�23.
[15] Hutchin T, Coy NN, Conlon H, Telford E, Bromelow K,
Blaydon D, et al. Assessment of the genetic causes of
recessive childhood non-syndromic deafness in the UK �implications for genetic testing. Clin Genet 2005;68:506�12.
[16] Dent KM, Kenneson A, Palumbos JC, Maxwell S, Eichwald
J, White K, et al. Methodology of a multistate study of
congenital hearing loss: preliminary data from Utah new-
born screening. Am J Med Genet C Semin Med Genet
2004;125:28�34.
[17] Tekin M, Arnos KS, Pandya A. Advances in hereditary
deafness. Lancet 2001;358:1082�90.
[18] Sobe T, Vreugde S, Shahin H, Berlin M, Davis N, Kanaan
M, et al. The prevalence and expression of inherited
connexin 26 mutations associated with nonsyndromic hear-
ing loss in the Israeli population. Hum Genet 2000;106:
50�7.
[19] Abe S, Usami S, Shinkawa H, Kelley PM, Kimberling WJ.
Prevalent connexin 26 gene (GJB2) mutations in Japanese.
J Med Genet 2000;37:41�3.
[20] Liu XZ, Xia XJ, Ke XM, Ouyang XM, Du LL, Liu YH,
et al. The prevalence of connexin 26 ( GJB2) mutations in
the Chinese population. Hum Genet 2002;111:394�7.
[21] Prasad S, Kolln KA, Cucci RA, Trembath RC, Van Camp
G, Smith RJ. Pendred syndrome and DFNB4-mutation
screening of SLC26A4 by denaturing high-performance
liquid chromatography and the identification of eleven novel
mutations. Am J Med Genet A 2004;124:1�9.
[22] Tsukamoto K, Suzuki H, Harada D, Namba A, Abe S,
Usami S. Distribution and frequencies of PDS (SLC26A4)
mutations in Pendred syndrome and nonsyndromic hearing
loss associated with enlarged vestibular aqueduct: a unique
spectrum of mutations in Japanese. Eur J Hum Genet
2003;11:916�22.
[23] Park HJ, Lee SJ, Jin HS, Lee JO, Go SH, Jang HS, et al.
Genetic basis of hearing loss associated with enlarged
vestibular aqueducts in Koreans. Clin Genet 2005;67:160�5.
[24] Campbell C, Cucci RA, Prasad S, Green GE, Edeal JB,
Galer CE, et al. Pendred syndrome, DFNB4, and PDS/
SLC26A4 identification of eight novel mutations and
possible genotype-phenotype correlations. Hum Mutat
2001;17:403�11.
[25] Wu CC, Yeh TH, Chen PJ, Hsu CJ. Prevalent SLC26A4
mutations in patients with enlarged vestibular aqueduct and/
or Mondini dysplasia: a unique spectrum of mutations in
Taiwan, including a frequent founder mutation. Laryngo-
scope 2005;115:1060�4.
[26] Hu H, Wu L, Feng Y, Pan Q, Long Z, Li J, et al. Molecular
analysis of hearing loss associated with enlarged vestibular
aqueduct in the mainland Chinese: a unique SLC26A4
mutation spectrum. J Hum Genet 2007;52:492�7.
[27] Wang Q-J, Zhao Y-L, Rao S-Q, Guo Y-F, Yuan H, Zong L,
et al. A distinct spectrum of SLC26A4 mutations in patients
with enlarged vestibular aqueduct in China. Clin Genet
2007;72:245�54.
[28] Ostergaard E, Montserrat-Sentis B, Gronskov K, Brondum-
Nielsen K. The A1555G mtDNA mutation in Danish
hearing-impaired patients: frequency and clinical signs.
Clin Genet 2002;62:303�5.
[29] Kupka S, Toth T, Wrobel M, Zeissler U, Szyfter W, Szyfter
K, et al. Mutation A1555G in the 12S rRNA gene and its
epidemiological importance in German, Hungarian, and
Polish patients. Hum Mutat 2002;19:308�9.
[30] Malik SG, Pieter N, Sudoyo H, Kadir A, Marzuki S.
Prevalence of the mitochondrial DNA A1555G mutation
in sensorineural deafness patients in island Southeast Asia.
J Hum Genet 2003;48:480�3.
[31] Liu X, Dai P, Huang DL, Yuan HJ, Li WM, Cao JY, et al.
[Large-scale screening of mtDNA A1555G mutation in
China and its significance in prevention of aminoglycoside
antibiotic induced deafness.] Zhonghua Yi Xue Za Zhi
2006;86:1318�22 (in Chinese).
[32] Valvassori GE, Clemis JD. The large vestibular aqueduct
syndrome. Laryngoscope 1978;88:723�8.
[33] Coucke PJ, Van Hauwe P, Everett LA, Demirhan O,
Kabakkaya Y, Dietrich NL, et al. Identification of two
different mutations in the PDS gene in an inbred family
with Pendred syndrome. J Med Genet 1999;36:475�7.
[34] Park HJ, Hahn SH, Chun YM, Park K, Kim HN.
Connexin26 mutations associated with nonsyndromic hear-
ing loss. Laryngoscope 2000;110:1535�8.
[35] Abe S, Kelley PM, Kimberling WJ, Usami SI. Connexin 26
gene (GJB2) mutation modulates the severity of hearing loss
associated with the 1555A��G mitochondrial mutation.
Am J Med Genet 2001;103:334�8.
[36] Wang YC, Kung CY, Su MC, Su CC, Hsu HM, Tsai CC,
et al. Mutations of Cx26 gene (GJB2) for prelingual deafness
in Taiwan. Eur J Hum Genet 2002;10:495�8.
[37] Hu DN, Qui WQ, Wu BT, Fang LZ, Zhou F, Gu YP, et al.
Genetic aspects of antibiotic induced deafness: mitochon-
drial inheritance. J Med Genet 1991;28:79�83.
GJB2, SLC26A4 and mtDNA A1555G mutations in Chinese 303
Act
a O
tola
ryng
ol D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y M
onas
h U
nive
rsity
on
11/0
2/14
For
pers
onal
use
onl
y.